adrenal & parathyroid
TRANSCRIPT

ENDOCRINE SYSTEM:ADRENAL
NMT 431
1UAB
Adrenal Imaging
Clinical Indications
Radiopharmaceutical used
Dosage & Administration
Technique
The Normal Scan
The Abnormal Scan
Artifacts & Pitfalls
Anatomy / Physiology
2UAB

Anatomy• Located bilaterally on
superior poles of both kidneys
• Each gland weighs only 6-7 grams
• Each gland consists of two parts:– Cortex (outer layer)– Medulla (inner layer)
Anatomy / Physiology
3UAB

Cortex (outer layer) produces steroid hormones:AldosteroneCortisolAndrogens
Medulla (inner layer) produces catecholamines:Epinephrine (adrenaline)NorepinephrineDopamine
Anatomy / Physiology
dopamine
4UAB

Hypothalamus - Pituitary – Adrenal cortex- feedback loop
• Hypothalamus synthesize and secrete corticotropin-releasing hormone (CRH) and vasopressin
• CRH and vasopressin stimulate the secretion of adrenocorticotropic hormone (ACTH) from anterior pituitary
• In response to stimulation by ACTH the adrenal cortices produce cortisol
• Cortisol in turn act back on the hypothalamus and pituitary (to suppress CRH and ACTH production) in a negative feedback cycle.
5UAB

Adrenal Cortex:
• Adrenal cortical pathology causing excessive production of one or more steroid hormones:
Hyperplasia (a proliferation of normal cells)Adenoma (a benign tumor)Carcinoma (a malignant tumor)
Clinical Indications
6UAB

Adrenal Cortex:• Adrenal cortical imaging indicated when source of
overproduction of steroid hormones is unknown in the presence of the following symptoms:– Increased level of cortisol (Cushing’s syndrome)– Increased level of aldosterone– Increased virilization
• Rule out adenoma; differentiate adenoma from hyperplasia
Clinical Indications
7UAB

Adrenal Medulla
Clinical indication: rule out pheochromocytoma
Clinical Indications
• Pheochromocytoma: a benign or malignant tumor of the adrenal medulla that secretes increased levels of epinephrine or norepinephrine
• Symptoms include unexplained hypertension, elevated levels of catecholamines, epinephrine, norepinephrine
8UAB

Adrenal Cortex: Radiopharmaceutical
• I-131 cholesterol (6-beta-iodomethyl-19-norcholesterol) (I-131 NP-59)
• Cholesterol is a precursor of steroid hormones; radiolabeled cholesterol when administered IV is incorporated into newly synthesized steroid hormones
• Investigational drug
Radiopharmaceutical used
9UAB

Adrenal Medulla: Radiopharmaceutical
• I-131 iobenguane (MIBG = methyliodobenzylguanidine)
• MIBG is structurally similar to norepinephrine
Radiopharmaceutical used
10UAB

Adrenal Cortex: Clinical Procedure
1) Patient preparation:
Dexamethasone (synthetic cortisol) may be given to suppress function of normal ACTH dependent adrenal tissue (by negative feedback) for approximately 4 days before receiving the tracer
Lugol’s solution (supersaturated solution of potassium iodide) to prevent uptake of free iodine by thyroid gland for several days before receiving the tracer
Signed consent required – investigational radiopharmaceutical
Dosage & Administration
Technique
11UAB

Adrenal Cortex: Clinical Procedure
2) IV administration of I-131 cholesterol: 0.5-1 mCi
3) Image 2-4 days following tracer administration
Posterior abdominal view
Dosage & Administration
Technique
12UAB

Adrenal Medulla: Clinical Procedure1) Patient preparation:
Lugol’s solution several days prior to tracer administration
2) IV administration of I-131 MIBG: ≈ 0.5 mCi
3) Image anterior and posterior head, thorax and abdomen 24-48 hrs post tracer administration; later images as indicated/needed
Dosage & Administration
Technique
13UAB

Adrenal CortexNormal tracer biodistribution:
- liver
- tracer excretion into bile then bowel
- normal adrenal tissue not visualized (if pretreated with
Dexamethasone)
- Right adrenal is slightly superior to the left
The Normal Scan
(without dexamethasone suppression)
Principles & Practice of Nuclear Medicine – Early & Sodee
14UAB

Adrenal Cortex
Abnormal:
- increased tracer uptake in abnormal gland
The Abnormal Scan
NP-59 uptake in adrenal adenoma
Endocrine Surgery - By Schwartz, Pertsemlidis, Gagner
15UAB

Adrenal Medulla:
Normal tracer biodistribution:
heart, liver, spleen, salivary glands and bladder; no adrenal medulla uptake or only faintly visualized at 24 hrs
The Normal Scan
Principles & Practice of Nuclear Medicine – Early & Sodee16UAB

Adrenal Medulla:Abnormal:
- intense uptake in tumor - significant uptake persists
in later images
- in the case of a malignant tumor, uptake may be seen in liver, bone, lymph nodes, heart, lungs, etc. (metastases from primary tumor)
The Abnormal Scan
PheochromocytomaMIR teaching file
MIR teaching file
Metastatic pheochromocytoma17UAB

• Interfering Gall bladder activity (may image post fatty meal)
• Colonic activity (cathartics may be used)
• Many drugs interfere or promote MIBG uptake (careful medication hx needed; ideally, drugs withheld 2-3 weeks before test)
Artifacts & Pitfalls
MIBG uptake in the muscles due to drug interference; Study was non-diagnostic
MIR teaching file
18UAB

19
Dexamethasone pre-treatment is done in order to:
a. stimulate normal adrenal tissueb. stimulate abnormal adrenal tissue c. inhibit normal adrenal tissued. inhibit abnormal adrenal tissue
UAB

Lugol’s solution is given before adrenal medulla imaging in order to block:
a. adrenal cortexb. adrenal medullac. thyroidd. parathyroid
20UAB

ENDOCRINE SYSTEM:PARATHYROID
NMT 431
21UAB

Parathyroid Imaging
Clinical Indications
Radiopharmaceutical used
Dosage & Administration
Technique
The Normal Scan
The Abnormal Scan
Artifacts & Pitfalls
Anatomy / Physiology
22UAB

Anatomy
• Located beside, beneath, or within thyroid gland tissue
• Other locations: within thymus gland or mediastinum or among the great vessels
Anatomy / Physiology
Some common ectopic parathyroid sites
Wikipedia
23UAB

Parathyroid Hormone (PTH)• Regulates calcium &
phosphate metabolism
– Bone: stimulates osteoclastic activity to increase bone resorption to make calcium & phosphorous available to other tissue
– Kidney: decreases
excretion of Ca & increases excretion of phosphorous
– GI tract: enhances calcium & phosphate absorption from bowel
Linus Pauling Institute, Oregon State University
Anatomy / Physiology
24UAB

Thyroid – Parathyroid – feedback for calcium homeostasis
• Synthesis/secretion regulated by plasma Ca++ level by negative feedback mechanism
Anatomy / Physiology
25UAB

Pathophysiology
• Hypoparathyroidism– Failure to respond to
lowered serum calcium levels resulting in hypocalcemia (muscle spasm, cardiac arrhythmia)
Anatomy / Physiology
Hypoparathyroidism
26UAB

Pathophysiology
• Hyperparathyroidism– Primary
hyperparathyroidism: increased synthesis and release of PTH
– Major symptoms: kidney stones, osteoporosis, neurological disorders & abdominal pain)
Anatomy / Physiology
Symptoms of
hyperparathyroidism
Adam, Inc.
27UAB

1) Localize hyperfunctioning parathyroid tissue (adenoma or hyperplasia) in primary hyperparathyroidism. May help surgeon identify lesion.
2) Localize hyperfunctioning parathyroid tissue (usually adenoma) in patients with persistent or recurrent disease
Clinical Indications
28UAB

Dual tracer technique
Tc-99m pertechnetate Tc-99m sestamibi (99mTc-MIBI)
Radiopharmaceutical used
Single tracer technique
Tc-99m sestamibi (99mTc-MIBI)
29UAB

Clinical Procedure1) ID patient; verify physician’s order; review clinical
indication for imaging
2) Explain procedure to patient; obtain relevant medical history
Dosage & Administration
Technique
30UAB

Relevant Medical History
• Lab results: serum calcium, PTH levels; urine calcium level
• History of thyroid disease• Results of other imaging procedures• Physical exam findings (neck palpation)
Dosage & Administration
Technique
31UAB

Clinical Procedure (cont’d)
3) Patient preparation - No special preparation - Assess patient’s ability to lie still
4) Administer radiopharmaceutical
Dosage & Administration
Technique
32UAB

Clinical Procedure (cont’d)5a) Injection & Imaging – Dual tracer Subtraction technique
Patient must remain in position for all images Tc-99m pertechnetate: 4-5 mCi IV Position patient as for thyroid imaging; image neck
20-30 min later, Tc-99m sestamibi (MIBI): 20-25 mCi IV 30 min after sestamibi injection, image neck
Image mediastinum to rule out ectopic tissue
Dosage & Administration
Technique
Subtraction technique
(Sestamibi thyroid image) – (99mTc-Pertechnetate image) = areas of abnormal tracer accumulation in parathyroid
33UAB

Clinical Procedure (cont’d)
5b) Injection & Imaging – Single tracer technique Patient injected and positioned as for thyroid imaging
Image neck at 30 min and 90-120 min
Image mediastinum to rule out ectopic tissue
Dosage & Administration
Technique
34UAB

The Normal Scan
Radiographics 19 (3): 601. (1999)
(upper left) 99mTc pertechnetate image
(upper right) the early Tc- sestamibi image
(Lower left) Computer-subtraction image
Dual tracer Subtraction Technique
Single tracer delayed washout method
THE JOURNAL OF NUCLEAR MEDICINE; Vol. 38 No.6 June 1997
35UAB

The Abnormal Scan
Patient with a parathyroid carcinoma involving the left
upper thyroid gland
(Upper left) Technetium-99m-pertechnetate image(upper right) early Tc-sestamibi image
(lower left) computer-subtraction image
THE JOURNAL OF NUCLEAR MEDICINE; Vol. 38 No.6 June 1997
Dual tracer Subtraction Technique
36UAB
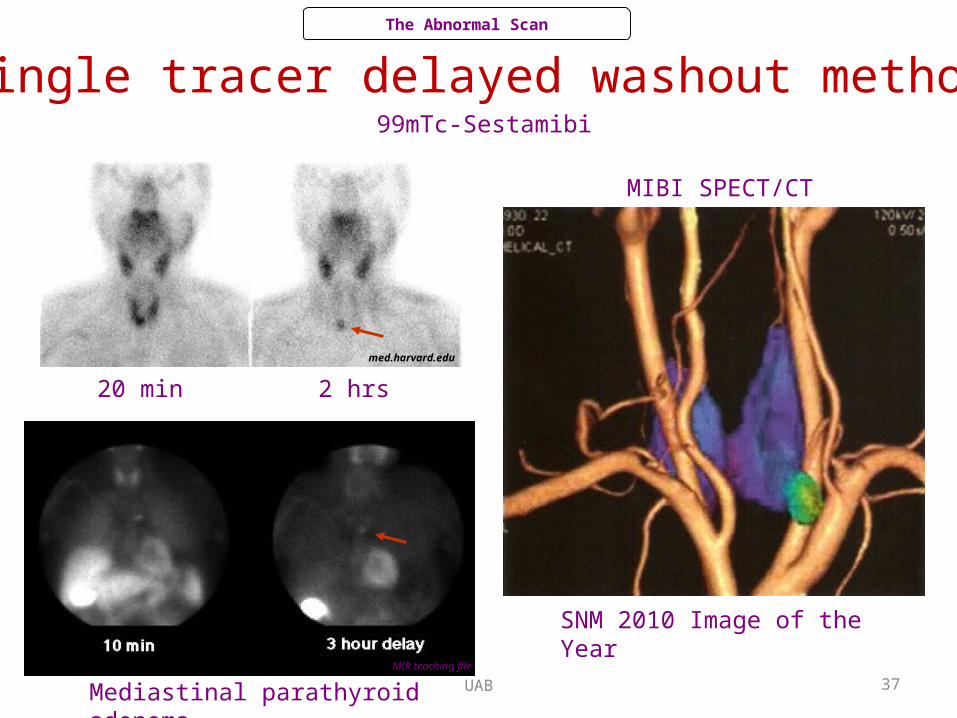
20 min 2 hrs
MIBI SPECT/CT
Mediastinal parathyroid adenoma
Single tracer delayed washout method
MIR teaching file
med.harvard.edu
The Abnormal Scan
SNM 2010 Image of the Year
99mTc-Sestamibi
37UAB

Sources of Error• Patient motion• Image misregistration• Small adenomas/hyperplastic/ectopic glands may be
difficult to detect• Thyroid adenomas/carcinomas may be
indistinguishable from parathyroid adenomas
Artifacts & Pitfalls
38UAB