adult bed capacity management - wsh.nhs.uk · source: chief operating officer status: approved...
TRANSCRIPT

Source: Chief Operating Officer Status: Approved Document PP(13)302 Issue date: November 2013 Review date: September 2016 Page 1 of 18
Trust Policy and Procedure Document Ref. No: PP(13)302
Policy Name
For use in: All areas of the Trust
For use by: All Trust staff
For use for: Trust Wide
Document owner: Chief Operating Officer
Status: Approved
West Suffolk Hospital NHS Foundation Trust
Management Policy
for
Adult Bed Capacity

Source: Chief Operating Officer Status: Approved Document PP(13)302 Issue date: November 2013 Review date: September 2016 Page 2 of 18
Key Principles – ‘The 10 Golden Rules’
The ‘10 Golden Rules’ are critical to the Trust maintaining a high performing emergency pathway and effective capacity management regime for its patients – these are foundations upon which the trust builds effective and safe patient pathways and flows.
1. Patients who come into the hospital via the Emergency Department will be subject to
a system of rapid initial assessment and treatment by a senior clinician 2. GP referred patients will go to assessment areas when open; from there they will be
streamed to the appropriate ward or short stay area. The ED is strictly for diagnosis and routing of emergency patients only.
3. ED will have arrangements in place to assess emergency patients within an hour
and, if admission is obvious, a referral to the appropriate specialties should occur within 2 hours. No breaches will be caused by disputes between specialties about where a patient is to go. In the event of a dispute the ED Consultant will adjudicate in hours, the senior doctor out of hours.
4. We will not admit a patient likely to be able to go home or discharge a patient who needs urgent assessment/treatment primarily in order to avoid a transit time breach.
5. We will not admit for tests a patient who is well enough to go home and return for
those tests - and we will ensure those tests are available when required. 6. Once a decision to admit is made, the patient will not be re-reviewed in the ED
causing them to stay in the department for longer than 4 hours from their time of arrival. Such patients will be reviewed on the assessment units unless there is a change in their condition.
7. The creation of capacity in admission/assessment areas is a trust priority. 8. Patients will be accepted on to the assessment units prior to full clerking. Initial
documentation will be carried out by ED, and be checked by the speciality registrar. 9. Discharge planning will begin at the time a decision to admit is made. Each patient
will have a discharge plan with a clearly defined predicted date of discharge given within 12 hours of admission to be agreed with the medical team. Plans for the discharge of elective patients should start at the pre-assessment stage. The patient and their carers, where appropriate, must be involved in all stages of the process.
10. Clinicians are responsible for ensuring the following takes place: Daily ward/board rounds with prompt decision making, immediate prescribing of TTOs and ordering of tests. Once a decision has been made, explicit notes made to indicate suitability for nurse-led discharge.

Source: Chief Operating Officer Status: Approved Document PP(13)302 Issue date: November 2013 Review date: September 2016 Page 3 of 18
Contents
Key Principles – ‘The 10 Golden Rules’ ................................................................. 2
1. Introduction...................................................................................................... 4
1.1. Aim ................................................................................................................. 4
1.2. Objectives ....................................................................................................... 4
1.3. Scope ............................................................................................................. 4
2. Capacity Management – Corporate Approach and Priorities ....................... 5
3. Roles & Responsibilities ................................................................................. 6
3.1. Patient Flow Team .......................................................................................... 6
3.2. Escalation ....................................................................................................... 8
4. Elective Admissions ........................................................................................ 8
5. Emergency Admissions .................................................................................. 9
6. Outpatient and Other Urgent Admissions...................................................... 9
7. Internal & External Transfers .......................................................................... 9
8. Outlying .......................................................................................................... 10
9. Inpatient Referrals ......................................................................................... 11
9.1. Internal Referrals .......................................................................................... 11
9.2. External Referrals (Repatriations) ................................................................. 11
10. Discharges ..................................................................................................... 11
11. Intensive Care Unit – Capacity Management ............................................... 11
12. Bed Closures ................................................................................................. 13
General Principles ................................................................................................. 13
12.1. Reasons for consideration of bed closures ................................................ 13
12.1.1 Reduced staffing levels .......................................................................... 13
12.1.2 Case mix/patient acuity and dependency ............................................... 14
12.1.3 Infection outbreak or prevention............................................................. 14
12.1.4 Capital schemes/refurbishment/redecoration ......................................... 15
12.1.5 Same Sex Accommodation .................................................................... 15
13. Bed Configuration ......................................................................................... 16
14. Disputes ......................................................................................................... 16
Version Control ..................................................................................................... 17
Contributors .......................................................................................................... 17
Consultation .......................................................................................................... 17
Related documents ............................................................................................... 18

Source: Chief Operating Officer Status: Approved Document PP(13)302 Issue date: November 2013 Review date: September 2016 Page 4 of 18
1. Introduction
The effective management of the Trust’s Adult Bed Capacity and the appropriate clinical placement
of patients is a critical activity for our organisation. It is the key process which enables the hospital to maintain an effective flow of patients and minimise the operational pressures created by fluctuating demand for acute beds. Balancing the needs of the Trust with those of our patients requires the skills, knowledge and input of all functions across the Trust as well as the wider Suffolk health economy. This document is, in effect, the ABC by which the organisation runs its day to day operations. The policy acknowledges the importance of clinical engagement at the earliest opportunity in the patient journey to ensure that the patient pathway remains focused and decisions regarding placements and moves are clinically based and are made in the interest and safety of the patient. The effective management of bed capacity cannot be realised through adherence to this policy alone. It is vital that local operational polices for all clinical areas effectively dovetail with this policy and are adhered to at all times. All staff whose roles and responsibilities bring them into direct or indirect contact with activities related to capacity management are required to carry out their duties in accordance with this policy.
1.1. Aim
The aim of the Adult Bed Capacity Management Policy is to ensure the most efficient use of beds
within West Suffolk Hospital NHS Foundation Trust whilst ensuring that patients are placed appropriately and safely according to their clinical needs.
1.2. Objectives
The objectives of this policy are to
Make explicit the way in which the Trust manages its bed capacity on a day by day basis
Outline the key roles and responsibilities for those staff who are charged with effective use of the Trust’s capacity as part of their job remit
Underline the key elements and actions necessary to deliver effective and patient centred capacity management, these include;
Patient admission
Patient discharge
Patient transfers (internal and external)
Infection Control
Bed / Ward closure
Bed escalation
1.3. Scope
This policy is relevant to the management of all designated adult capacity within West Suffolk Hospital. Management of paediatric and maternity capacity is outside the scope of this document.

Source: Chief Operating Officer Status: Approved Document PP(13)302 Issue date: November 2013 Review date: September 2016 Page 5 of 18
2. Capacity Management – Corporate Approach and Priorities
The effective use of the Trusts capacity requires the following approaches to be enacted on a day to day basis
Operational Policies for individual clinical areas will be formulated to support this policy in sustaining the effective and efficient use of capacity.
Patients should only be physically admitted when their needs cannot be appropriately met within a day case setting or community environment.
All patients should have a comprehensive assessment of their health and social care needs completed within 12 hours of their admission to the hospital.
Patients should only be placed in an area that is adequately staffed with nursing and medical staff (according to number and acuity of patients) and that has the clinical equipment required to manage the presenting condition.
Patients will be accommodated in single-sexed bay areas. Where, due to urgent clinical need, this is not possible, the process for Breach of Single Sex Accommodation - Adults MUST be followed.
Following the initial move from an assessment area, a patient should not undergo any further moves unless clinical needs dictate otherwise. If it is necessary to move patients due to non-clinical or capacity reasons, Section 9; Outlying, of this policy the must be adhered to.
Clinical areas will inform the Patient Flow Team immediately it is known that a decision to discharge or transfer a patient is made. Clinical areas will ensure any patient administration or discharge tracking system is updated. Compliance with ‘real time’ updating of admissions, transfers and discharges is monitored and reported on a weekly basis.
Failure to declare vacant beds in a timely manner impacts negatively upon patient care and overall patient experience and may lead to potential disciplinary action under the Trust’s disciplinary procedure. The Clinical Duty Manager will highlight identified issues to the relevant Service Manager / Matron for investigation and appropriate action.
There will be daily Consultant or Registrar ward/board rounds across the Trust to
ensure all patients are reviewed and have a plan of treatment in place. Patients can then be discharged or have a discharge date set that can be /nurse led.
Daily board rounds will take place on every ward detailing actions/outcomes and
estimated dates of discharge. The Nurse in Charge for each area will be responsible for leading the board rounds and the documentation of the white boards.
All elective patients will be triaged in accordance with their clinical need. Any
admissions the day before surgery will be based on clinical evidence and best practice and will be audited within Surgery. On a daily basis the Clinical Duty Manager and relevant Service Manager(s) will validate the following day’s lists and then work together to ensure that all elective patients are admitted. At times of increasing demand on capacity they can ensure that the appropriate patients are admitted according to their clinical need. For example patients with cancer or whose clinical need is urgent, are placed appropriately along with patients who have management priorities (i.e. cancelled previously or if this would cause a risk to their 18 week pathway) and those requiring routine surgical procedures.

Source: Chief Operating Officer Status: Approved Document PP(13)302 Issue date: November 2013 Review date: September 2016 Page 6 of 18
All patient movements will be updated on the Patient Administration System (PAS) as soon as they occur. This is a key element of patient safety and provides the Clinical Patient
Flow Team with accurate information on which to base their decisions and planned actions regarding capacity and flow.
3. Roles & Responsibilities
3.1. Patient Flow Team
Clinical Bed Coordinators, supported by Clinical Duty Manager and working alongside Trust management and clinical teams, are responsible for the effective management and coordination of Adult Bed Capacity on a 24/7 basis, ensuring all emergency and elective admissions meet
both national and local standards and access targets. A key element of the Clinical Duty Manager role is to ensure that the trust is able to accommodate patients irrespective of their presentational route into the hospital. Outside of their clinical responsibilities, the Clinical Duty Manager remit includes the management of;
Emergency admissions
Elective admissions
Patient Flow
Repatriations between WSH and other Trusts/Specialist services
Patients under the ITU network agreement The team carry out these tasks by:
The coordination of on-site services out of hours, working with staff to ensure that all services are being delivered to an agreed standard. Ensure that all issues are referred to the correct clinical group if not resolved.
Monitoring of the capacity within the Trust; obtaining bed states from inpatient areas enabling the Team to pro-actively manage capacity and ensure that all available capacity is used appropriately and the appropriate configuration of beds is available at the earliest opportunity for patients requiring admission
Ensuring all capacity management decisions are based on an assessment of the current bed state, predicted admissions and discharges, the time of day and relevant information obtained from clinical colleagues.
Monitoring the progress of patients through ED, AMU & SAU using the Patient Administration System and visits to the department, and maintain an overview of the allocation of beds in the assessment/admission areas in a timely manner.
Assisting in removing any constraints to individual patient’s pathways and ensuring escalation of blockages to avoid breaches of the 4 hour standard, collaborating closely with the ED Shift Coordinator
Assuming overall responsibility for the hospital site out of hours with support from the Director on Call.
Working in partnership with Directorate colleagues to facilitate effective patient flow e.g. the admission of elective and emergency patients within the principles of the Admission and Waiting List policies, and minimizing patient transit times and cancellations.

Source: Chief Operating Officer Status: Approved Document PP(13)302 Issue date: November 2013 Review date: September 2016 Page 7 of 18
Ensuring that patient need, safety and experience remains central to the decisions taken in facilitating the patient’s journey.
Applying Clinical Quality Indicators to facilitate patient flow and safety incorporating the operating standards for the 4 and 12-hour access standards, ensuring that no patient is placed at risk due to the achievement of an access standard.
Effectively communicating with Trust-wide leads over bed availability to expedite patient flow decisions and ensure that escalation policies and procedures are invoked as necessary.
Working with the Nurse in Charge of wards and departments to facilitate patient flow, ensuring that the right patients are in the right place. This includes internal transfers from ward areas and the Intensive Therapy Unit to the appropriate specialty ward
Establishing an effective working relationship with ward nursing staff to ensure collection of accurate information regarding bed availability, discharges and potential discharges, daily cancellations and outlying patients; seeing that an overview of the status of bed availability is available at any given time.
Liaise with the Matrons, Service Managers and Clinicians regarding problems and assist with communicating these issues.
Lead Operational Capacity Meetings, providing accurate information on capacity issues to the appropriate managers.
Maintain constant communication with wards to obtain accurate bed information ensuring this is communicated effectively.
Liaise with the Bed Managers external to the trust regarding bed resources, and coordinate the transfer of tertiary waiters and repatriations in a timely fashion in accordance with Trust policies and protocols.
As required, liaise with Ambulance Service, Chief Operating Officer or their deputy (in hours) and the Director On Call (out of hours) to arrange ambulance diverts as per agreed and documented protocols.
Notify the Chief Operating Officer (in hours) or Director on Call (out of hours) of any pending difficulties and participate in development and delivery of action plans.
Declare the internal escalation status in line with the Internal Escalation Plan and ensure all relevant staff are advised at designated times throughout the day of updated bed states and expected/predicted/pending problems (See Section 4 – Communications).
Work in partnership with Director on Call to address issues, informing each other of risks to patient safety, and capacity.
Support ward colleagues by providing guidance in expediting timely discharge.
Conduct a face to face handover to the incoming Clinical Duty Manager and sign off agreed plans /actions.

Source: Chief Operating Officer Status: Approved Document PP(13)302 Issue date: November 2013 Review date: September 2016 Page 8 of 18
Maintain up to date lists of outliers, clinically stable patients and available community beds via information received from the wards.
Proactively manage elective admissions to accommodate emergency demands in conjunction with Surgery.
Proactively manage the discharge of patients out of critical care to inpatient beds.
Following the acceptance of a patient from another Trust, assume responsibility from the relevant Consultant for liaising with the referring Trust and placing the patient as soon as capacity allows.
3.2. Escalation
The Trust has an Internal Escalation Policy and Plan which enables the Trust to deal effectively with fluctuations in demand and capacity so that it can manage associated clinical risk within acceptable limits. The policy is designed to help mitigate the risk of further escalation and ensure an appropriate response from key staff members to contribute to a reduction in escalation status. The policy aims to maintain high standards of patient safety, patient experience and performance against key waiting time and quality standards of care. The processes and procedures in that Policy are to be used in conjunction with the Acute Bed Capacity Policy, given that the Escalation Policy is for use in identifying when, and if, exceptional measures are required. While emphasis and priorities may change, the fundamentals around maintaining safety and providing the most appropriate treatment are constant.
4. Elective Admissions
Elective lists are co-ordinated between Consultants, Service Managers, and the Admissions Team. Clinical priority is the main determination of when patients are admitted as inpatients. Patients of the same clinical priority should be seen in chronological order in line with their 18 week RTT date. These are indicated on the elective priority list. Potential shortfalls in bed availability for elective admissions are normally identified at ward level and communicated via the Service Manager to the Clinical Duty Manager. This information is used in conjunction with the elective priority list and forms part of the weekend plan which is used by Clinical Duty Managers to appropriately place outliers in surgery to avoid on the day cancellations. At times of extreme capacity pressures a decision is likely to be taken to reduce elective admissions. Cancellations will be made on the basis of the lowest clinical need, following consultation with the Service Manager for the area and relevant Consultant and Team(s). If potential cancellations will put the 18 week speciality level targets at risk then these cancellations must be authorised through the appropriate Service Manager after discussion with the COO or GM for Surgery. Every effort will be made by the appropriate Clinical Management Team to give patients sufficient notice prior to cancellation of an elective surgical procedure. Outside normal working hours, the responsibility for utilising empty beds rests with the Clinical Duty Manager following plans developed and communicated at the Handover meetings. It is acknowledged that, at times of severe capacity pressures, medical patients will be admitted to surgical areas. This will be kept to an absolute minimum and the placement of patients closely monitored.

Source: Chief Operating Officer Status: Approved Document PP(13)302 Issue date: November 2013 Review date: September 2016 Page 9 of 18
To maintain patient flow and optimise capacity, the following principles are followed for all elective admissions:
Discharge planning occurs at pre-assessment.
Patients who can be outlied are identified and notified to the Clinical Duty Manager
Day case rates are maximised
Patients are only admitted on the day before their surgery where it is clinically appropriate.
5. Emergency Admissions
Emergency Admission numbers will be monitored by the Clinical Duty Manager and communicated via the Capacity meetings trust-wide. Protocols relating to overall capacity management and clinical acuity will be applied against the principle outlined within the 10 Golden Rules.
6. Outpatient and Other Urgent Admissions
A request may be made for an urgent hospital admission (e.g. from out-patient clinics, the MacMillan Unit, MTU or the endoscopy unit) following a patient assessment by a Consultant (or their deputy). It is the responsibility of the admitting team to inform the Patient Flow Team via Bleep 358 of the need to admit the patient within an agreed waiting time as determined by the accepting Consultant team. If the patient requires same day admission the Patient Flow Team will identify an appropriate bed within the relevant speciality. If this is not possible then an alternative ward will be identified and the placement will be discussed with the referring clinical team so that any clinical risks are identified. For the comfort and benefit of patients, the Patient Flow Team will endeavour to allocate an inpatient bed immediately upon request. Patients therefore should not be transferred from an Out-patient area to the Emergency Department unless:
The patient’s condition is clinically unstable and an in-patient bed is not immediately available.
The referring area does not have appropriately skilled staff to care for the patient and an in-patient bed is not immediately available, following completion of appropriate risk assessments.
If the patient is clinically stable and is able to wait at home, the patients’ details will be placed on an urgent “to come in” (TCI) list and will advise the referring team when arrangements have been made to admit the patient. For trauma patients it is the responsibility of the trauma team to keep the patient informed and update Clinical Bed Co-ordinators on beds required as soon as possible.
7. Internal & External Transfers
Transferring patients between in-patient wards to create capacity should be seen as a last resort as it can constitute increased risk, poor experience and increased length of stay for patients. It is acknowledged however that at times it may be necessary for clinical and patient safety reasons.

Source: Chief Operating Officer Status: Approved Document PP(13)302 Issue date: November 2013 Review date: September 2016 Page 10 of 18
All patient transfers, including those from AMU and SAU must be recorded and reported to the Patient Flow Team (Bleep 358) immediately. To minimise any risks associated with out-of-hours transfers for the patient and to maintain comfort and well-being, patients should not be transferred between in-patient areas, for non-clinical reasons, between 21:00 hrs and 08:00 hrs except in exceptional circumstances. The exceptions to this are patients who require admission or transfer from the ward or the Emergency Department when “Treat and Transfer” is in progress. Transfers from these areas may take place as required in order that appropriate assessment capacity is maintained. All patient transfers, including those from AMU and SAU must be recorded and reported to the Patient Flow Team (Bleep 358) immediately.
Intended transfers should be discussed with the Patient Flow Team to ensure availability.
8. Outlying
Transferring patients between in-patient wards to create capacity should be seen as a last resort as it can constitute increased risk, poor experience and increased length of stay for patients. It is acknowledged however that at times it may be necessary for clinical and patient safety reasons. Acute Medical patients from AMU can be moved to any appropriate medical ward or to the surgical floor as long as they have been seen by (at least) the registrar, have a clear plan of management, do not have a high GCS or MEWS score, do not require NIV and are not cardiac in presentation. The Patient Flow Team should have a copy of the nursing handover It is reasonable to admit medical patients directly from A & E into any medical or surgical outlying beds provided the patient has had a registrar / middle grade or Consultant review with a clear plan and their location is made known to the team the following day as without this it will create potential patient safety gaps. Dementia / confusion is not a reason to outlie, nor is it a reason not to, except where such a move would endanger the safety of the individual or other patients. The Executive Director of Nursing may, from time to time publish a list of exceptions. Patients requiring high level, specialist medical care, such as those requiring NIV or are cardiac in presentation are not to be outlied.
Patients in side rooms for Infection Prevention reasons may only be moved following discussions between Exec on Call and the On Call Microbiologist. Outlying should be avoided wherever possible, however when it does have to be done every ward shares in the responsibility of ensuring that only the most appropriate patients are moved without delay. As part of the nursing assessment, staff should regularly assess and annotate whether a patient is suitable for outlying or not and if so, any conditions or criteria which need to be met. Similarly if a patient is not suitable for outlying, the reason(s) are to be clearly recorded in the nursing assessment. It is always preferable to have a multiple number of patients moved to ensure the safest treatment of all. However all concerned must remember that every move is disruptive to the patient(s) concerned and may detract from their treatment.

Source: Chief Operating Officer Status: Approved Document PP(13)302 Issue date: November 2013 Review date: September 2016 Page 11 of 18
9. Inpatient Referrals
9.1. Internal Referrals
Any patient admitted under the care of one Consultant who then requires the intervention of a different specialty will be referred on by the admitting team on the day of decision.
9.2. External Referrals (Repatriations)
External referrals (i.e. patients from other NHS Trusts) will be accepted by the appropriate Consultant (or their deputy in their absence). With the exception of CCS, NICU and Obstetrics, it is the responsibility of the accepting team to inform the Clinical Patient Flow Team of the need to transfer the patient. Arrangements for the transfer will be made by the Clinical Patient Flow Team who will take into account the patient’s medical condition as assessed by the clinical team, bed availability and the Isolation Guidelines relating to the acceptance of patients from other NHS Trusts.
10. Discharges
Discharge planning will begin at the time a decision to admit is made. Each patient will have a discharge plan with a clearly defined predicted date of discharge given within 12 hours of admission to be agreed with the medical team. Plans for the discharge of elective patients should start at the pre-assessment stage. The patient and their carers, where appropriate, must be involved in all stages of the process. The team will operate with 3 registered nurses and 3 discharge planning practitioners each weekday between the hours of 8-4pm and 1 registered nurse between the hours of 4pm to 7pm. This will allow the team to respond to urgent out of hours discharge planning issues and to assist during critical bed capacity.
11. Intensive Care Unit – Capacity Management
Intensive Care capacity is likely to be one of the scarcest resources within the Trust. With this in mind it is imperative that patients are discharged in a safe and timely manner to a clinical area that can meet their needs. Clinical Duty Managers will include Critical Care Services (ICU and HDU) within their rounds, liaising closely with the shift leader. The Consultant in charge of the Intensive Care Unit will be the gate keeper and prioritise patients for transfer to ward areas. Critical Care patients will be prioritised according to clinical need and the over-arching pressures within the Trust. The algorithm to facilitate the timely discharge of patients from Intensive Care to a ward below will be adhered to. The Clinical Duty Manger will endeavour to ensure that an empty staffed Critical Care bed is available at all times for emergency admissions. On filling the last empty bed, all attempts will be made to move a ‘fit for discharge Level 1’ patient on to an appropriate ward. In an emergency, the necessity to create a Critical Care bed for a patient of greater clinical need will require an identified patient to be discharged irrespective of the time of day/night. In all other instances patients will be

Source: Chief Operating Officer Status: Approved Document PP(13)302 Issue date: November 2013 Review date: September 2016 Page 12 of 18
discharged between 7.00 am and 10.00 pm. All transfers from Critical Care to a lower level of care between 22:00 hours and 07:00 hours will have a Datix completed. Transfer of a Critical Care patient to another Critical Care area in another hospital may sometimes be necessary either due to clinical need or due to lack of capacity within the Critical Care; these will be classed as clinical or non-clinical transfers respectively. This will take place in line with the Admission and Discharge Policy, which is located in the Critical Care Unit. Any patient transferred out of Critical Care to another hospital will use the Critical Care Network Transfer Form, which will accompany the patient upon their transfer. Intensive Care patients who are transferred outside the clinical network, due to capacity reasons, should be recorded and reported on the SITREP information system. It is the Clinical Duty Manager’s responsibility to ensure that any patient transferred outside of the clinical network is reported to the appropriate senior manager.
Patient on ICU identified as ready for discharge to ward.
ICU Doctor to contact appropriate medical team for ongoing care.
ICU Shift co-ordinator to assess level of urgency required to ascertain ward bed
ROUTINE
No immediate ICU capacity problems
ICU shift co-ordinator to contact Patient Flow team bleep 358 immediately to request bed
DESIGNATED BED AVAILABLE WITHIN 4 HOURS
Bed Allocated within 4 hours
(Clinical Duty Manager to keep ICU informed of progress 2 hours post-
request)
Patient transferred to
ward
URGENT
ICU capacity reached
ICU shift co-ordinator to contact Patient Flow ream immediately to
request bed
DESIGNATED BED AVAILABLE WITHIN 2 HOURS
CRITICAL- ICU Capacity reached
Patient requires urgent admission DELAY WILL POSE SIGNIFICANT
CLINICAL RISK
ICU shift co-ordinator to contact Patient Flow team bleep 358 immediately to request bed
Priority to be given over
DESIGNATED BED AVAILABLE IMMEDIATELY
Priority given over electives and ED
Admissions
Bed Allocated within 2 hours
(Clinical Duty Manager to keep ICU informed of progress 1 hour post-
request)
Allocates Bed immediately
Patient transferred to
ward
RECORD AS DELAYED DISCHARGE
ICU TO COMPLETE DATIX DELAY/SAME SEX ACCOMMODATION BREACH
ICU Admission to be cared for in safe
environment by Critical Care Team until
transfer occurs or non-clinical transfer out
YES NO
YES NO NO YES

Source: Chief Operating Officer Status: Approved Document PP(13)302 Issue date: November 2013 Review date: September 2016 Page 13 of 18
12. Bed Closures
General Principles
“Closure of beds” is taken to mean any decision to reduce the number of beds a ward operates, below the number it is normally expected to operate, or the need to restrict admissions/patient transfers due to potential or actual outbreaks of infection or skill mix/staffing issues or other factors. The Patient Flow Team retains the information relating to the total number of beds each ward operates with. Each ward has a responsibility in maximising bed capacity, in order to be able to undertake an appropriate proportion of the inpatient workload of the Trust. The Trust, as a whole, has a responsibility to maintain maximum overall bed capacity. The closure of beds should be the last option considered after all other options have been explored and implemented. In making judgements about the closure of beds, adequacy of care and level of risk to patients will necessarily be considered. However, levels of risk cannot be assessed in isolation, and account will have to be taken of levels of risk being managed in other parts of the Trust (e.g. Emergency Department, Critical Care Unit). As such, wards might be expected to manage higher levels of risk at times of severe pressure. For example, wards may be expected to keep beds open (when ideally they would be closed); if significant numbers of acutely unwell patients are being managed in less than ideal circumstances in the Emergency Department or delays in ambulance handover within the Emergency Department are occurring. In the context of Clinical Governance and Risk Management, the responsibility for managing risks of this sort rests with the Trust whilst individual ward managers and others involved in decision-making must act reasonably and professionally. In working hours, the Chief Operating Officer or Director of Nursing will authorise bed closures. Out of hours this will be authorised by the Director on call.
12.1. Reasons for consideration of bed closures
Reasons for bed closures include:
12.1.1 Reduced staffing levels Bed closures should not be contemplated in circumstances where normal levels of sickness absence are being experienced. Staffing establishments are set to allow for this level of sickness absence. Similarly annual leave and study leave should not be a cause for beds to be closed. Excessive levels of sickness absence/maternity leave/vacancies, which cannot be covered by the use of Bank or agency staff, may result in staffing levels which do not allow the normal number of beds to be open. The Trust will be innovative in maintaining bed capacity by redistributing nurses and other resources throughout the organisation. A formal risk assessment should be in place and recorded on the Datix system.

Source: Chief Operating Officer Status: Approved Document PP(13)302 Issue date: November 2013 Review date: September 2016 Page 14 of 18
12.1.2 Case mix/patient acuity and dependency In extreme circumstances, the management of particularly sick and unwell patients may require additional staff to be deployed. The need for this will be agreed between the Ward Manager, Service Manager, Matron and Head of Nursing in hours / Clinical Duty Manager (out-of-hours). This should be for a comparatively short period of time and should be reviewed by the Service Manager and Matron and the clinical area on a regular basis.
12.1.3 Infection outbreak or prevention It is essential to utilise beds in a way that minimises the risk of spreading of infections between patients whilst recognising that some patients are very vulnerable to specific infections. Every effort will be made to minimise the risk of locating such a vulnerable patient to a bed in close proximity to a patient who has a high risk of having MRSA or other potentially transmissible pathogenic organism. Close liaison between the Service Manager and the Patient Flow Team and the Infection Prevention and Control Team is essential to ensure the risks are minimised and closed beds are reviewed. All staff will adhere to relevant Trust Hospital Infection Control Policies and guidelines with regard to bed management and patient safety. These include:
Standard Principles for Preventing Hospital Acquired Infection CG10023
Major Outbreak of Infection: Control Plan CG10050
Infection Control Policy for the Orthopaedic Wards CG10121
Isolating Patients with Communicable Diseases Including Healthcare Associated Infection CG10135
Clostridium Difficile Control CG10021
MRSA Control: The Management of Infection and Colonisation by Methicillin Resistant Staphylococcus Aureus (MRSA) CG10004
Norovirus: Clinical Management CG10117
The Major Outbreak Policy PP(13)139
Certain groups of patients are at much higher risk of having MRSA than the general patient population. This includes:
Patients who have been previously MRSA positive
Patients who live in nursing and residential care homes
Patients transferred from other hospitals/ abroad
Patients who have had healthcare interventions or admissions within the previous 3 months.
Patients in these categories should be placed in locations where they are least likely to be in close proximity to patients who are most vulnerable to MRSA. Patients who should be regarded as more vulnerable to MRSA include those awaiting orthopaedic implant surgery, vascular surgery and plastic surgery. As detailed in the Major Outbreak Policy any patient who is admitted with acute diarrhoea and vomiting should be placed in isolation; if no single rooms are available the Infection Prevention and Control Team will be contacted for advice regarding the placement of the patient. When a decision has been made to close a ward or a bay area this decision must not be changed without consultation from the Infection Prevention and Control Team or, out of hours, the on call Microbiologist.

Source: Chief Operating Officer Status: Approved Document PP(13)302 Issue date: November 2013 Review date: September 2016 Page 15 of 18
When patients are transferred between wards there is a risk of unidentified infections being transferred with them. When patients need to be transferred to create capacity, efforts should be made to avoid transferring patients who are most likely to carry hospital acquired organisms. Patients should not be transferred between wards if they are known to be MRSA positive or have another transmissible infection (e.g. TB, meningitis, shingles, measles) or undiagnosed diarrhoea or vomiting unless going to a side room for isolation. A transfer referral checklist must be completed for all patients who are transferred between ward areas.
12.1.4 Capital schemes/refurbishment/redecoration All key stakeholders are to be involved in any decisions that will impact on patient flow prior to capital schemes, refurbishment and redecoration commencing.
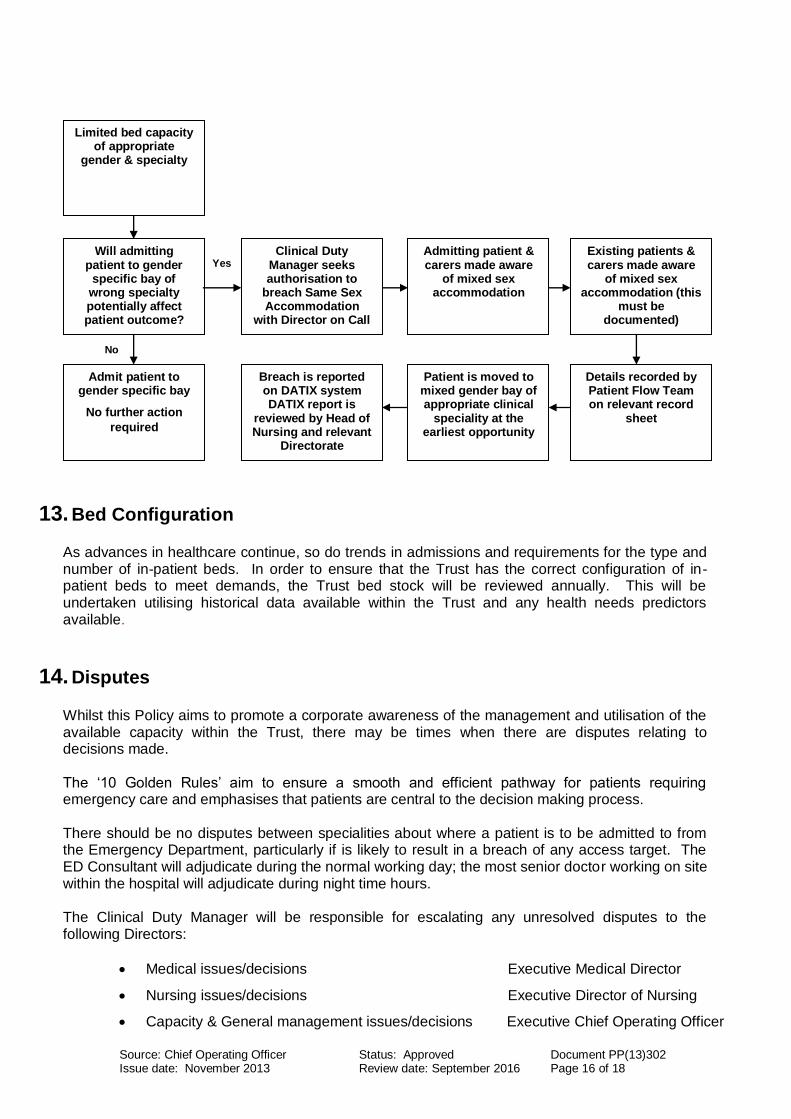
12.1.5 Same Sex Accommodation The Trust will make every effort to comply with Same Sex Accommodation related requirements. In the event all other avenues have been explored and the need arises to consider breaching, the Clinical Duty Manager must follow the process set out below.
Source: Chief Operating Officer Status: Approved Document PP(13)302 Issue date: November 2013 Review date: September 2016 Page 16 of 18
13. Bed Configuration
As advances in healthcare continue, so do trends in admissions and requirements for the type and number of in-patient beds. In order to ensure that the Trust has the correct configuration of in-patient beds to meet demands, the Trust bed stock will be reviewed annually. This will be undertaken utilising historical data available within the Trust and any health needs predictors available.
14. Disputes
Whilst this Policy aims to promote a corporate awareness of the management and utilisation of the available capacity within the Trust, there may be times when there are disputes relating to decisions made. The ‘10 Golden Rules’ aim to ensure a smooth and efficient pathway for patients requiring emergency care and emphasises that patients are central to the decision making process. There should be no disputes between specialities about where a patient is to be admitted to from the Emergency Department, particularly if is likely to result in a breach of any access target. The ED Consultant will adjudicate during the normal working day; the most senior doctor working on site within the hospital will adjudicate during night time hours. The Clinical Duty Manager will be responsible for escalating any unresolved disputes to the following Directors:
Medical issues/decisions Executive Medical Director
Nursing issues/decisions Executive Director of Nursing
Capacity & General management issues/decisions Executive Chief Operating Officer
Yes
No
Limited bed capacity of appropriate
gender & specialty
Will admitting patient to gender
specific bay of wrong specialty potentially affect patient outcome?
Admit patient to gender specific bay
No further action
required
Clinical Duty Manager seeks authorisation to
breach Same Sex Accommodation
with Director on Call
Admitting patient & carers made aware
of mixed sex accommodation
Existing patients & carers made aware
of mixed sex accommodation (this
must be documented)
Details recorded by Patient Flow Team on relevant record
sheet
Patient is moved to mixed gender bay of appropriate clinical
speciality at the earliest opportunity
Breach is reported on DATIX system DATIX report is
reviewed by Head of Nursing and relevant
Directorate

Source: Chief Operating Officer Status: Approved Document PP(13)302 Issue date: November 2013 Review date: September 2016 Page 17 of 18
Version Control
Version Number Date of Release Details
V1 29 October 2013 Agreed at Operational Steering Group
Contributors
The following people have contributed to the development of this plan
Name Role / Organisation
Jon Green Executive Chief Operating Officer
Gerald Kelly Patient Access Development Manager
Steve Myers General Manager, Surgery
Britt van-Rooyen General Manager, Clinical Support Services
Lesley Standring Project Manager, Emergency Care Workstreams 3 & 5
Paul Oats Service Manager, Theatres
Alice Troup Service Manager, Surgery
Consultation
The following people / roles were consulted prior to the ratification of this plan
Name
Lesley Roberts – Service Manager, Emergency Department

Source: Chief Operating Officer Status: Approved Document PP(13)302 Issue date: November 2013 Review date: September 2016 Page 18 of 18
Related documents
Plans / polices / procedures to be read in conjunction with this plan
Escalation Policy and Plan
ICU Admission & Discharge Policy
AMU Operational Policy
SAU Operational Policy
Patient Flow Team Operational Policy
Version & status 1
Date ratified 28 October 2013
Ratified by (name of committee) Operational Steering Group
Name of originator / author, job title & dept.
Jon Green, Executive Chief Operating Officer
Name of responsible committee Operational Steering Group
Issue date 29 October 2013
Review date 29 October 2014
Expiry date 29 October 2015
Impact assessed by Operational Steering Group