adult survivors of childhood and adolescent cancer anna t. meadows, md children’s hospital of...
TRANSCRIPT

Adult Survivors of Childhood and Adolescent
Cancer
Anna T. Meadows, MD
Children’s Hospital of Philadelphia
University of PA School of Medicine


0
10
20
30
40
50
60
70
80
90
100
0 2 4 6 8 10 12 14 16 18 20 22
Years from Diagnosis
Pro
po
rtio
n S
urv
ivin
g
1976
1990
1985
1980
• Over 250,000 childhood cancer survivors in the US • 1 in 1,000 is a childhood cancer survivor• 1 in 570 is a childhood cancer survivor (ages 20 to 34 yr.)
Cancer Survival, 0-14 Years of AgeCancer Survival, 0-14 Years of AgeSEER Program 1976-1997SEER Program 1976-1997

Advances in Treatment forPediatric Cancer
• Chemotherapy responsiveness
• Multi-agent chemotherapy protocols
• Adjuvant and neoadjuvant therapy
• Improvements in surgery and anaesthesia
• Supportive therapies: Blood products,
broad spectrum antibiotics, antifungals

Late MortalityLate MortalitySex-specific survival (CCSS)Sex-specific survival (CCSS)
5 10 15 20 250.80
0.84
0.88
0. 92
0.96
1.00
Years since diagnosis
Su
rviv
al f
un
ctio
n e
stim
ate
US Female
Male
Female
US Male
•Relapse•Treatment-related•Non-treatment-related

Mortality in Survivors of Childhood Cancer
• Surveillance and End Results data for 5 years survivors
• Diagnosis 1974-1980– 7% mortality
• Diagnosis 1995-2000– 4% mortality

Evolution of Survivorship Research
• Anecdotal Reports
• Case Series
• Prospective Studies
• Multivariate Analyses
• Mathematical Modeling
• Surveillance and Counseling
• Intervention

Late Complications of Childhood Cancer Therapy
• Growth and Development– linear growth– intellectual function– sexual maturation
• Reproduction– fertility– health of offspring
• Vital Organ Function– cardiac– pulmonary– renal– gastrointestinal
• Second Neoplasms– benign– malignant
• Psychosocial adjustment



Neurocognitive Late Effects
• Radiation induced– dose related– age related
• Chemotherapy induced– Methotrexate– Intrathecal therapy:
• Triples > single agent
• Surgical resection

Prevention of Cognitive Dysfunction
• Eliminate or reduce cranial irradiation
• Substitute chemotherapy with CNS penetration
• Avoid parenteral methotrexate after radiation
• Monitor educational performance
• Provide early intervention

Gonadal Failure
• Males and females are different• Fertility and hormone production are not
synchronous males, unlike females • Radiation and alkylator agent
chemotherapy (cyclophosphamide, ifosfamide, cisplatin, procarbazine, nitrosoureas, mustard) are responsible; doses are critical
Prevention of Gonadal Toxicity
• Eliminate or reduce radiation to the gonads
• Design gender-specific protocols
• For males, avoid or reduce total dose
of alkylating agents

Cardiac Late Effects
• Anthracyclines• Gender• Age• Dose• Latency
• Radiation• > 25 - 30 Gy
• Cardiomyopathy• Ventricular
dysfunction• Pericarditis• Rhythm
abnormalities• Pericardial damage• CAD

Prevention of Cardiac Toxicity
• Limit total dose of anthracyclines
• Infuse anthracyclines slowly
• Evaluate cardiac function during therapy
• Avoid concomitant radiotherapy
• Use the cardioprotectant dexrazoxane

Factors Predisposing to Second Neoplasms
• Treatment– radiation therapy
– chemotherapy: alkylating agents; epipodophyllotoxins
• Genetic Conditions– genetic retinoblastoma
– neurofibromatosis
– Li-Fraumeni Syndrome

Radiation Therapy and Second Neoplasms
• bone and soft tissue sarcomas – doses >40Gy; adolescents
• carcinomas of the breast – doses >30Gy; adolescents
• thyroid adenomas and carcinomas – young children; dose-effect
• basal cell carcinomas
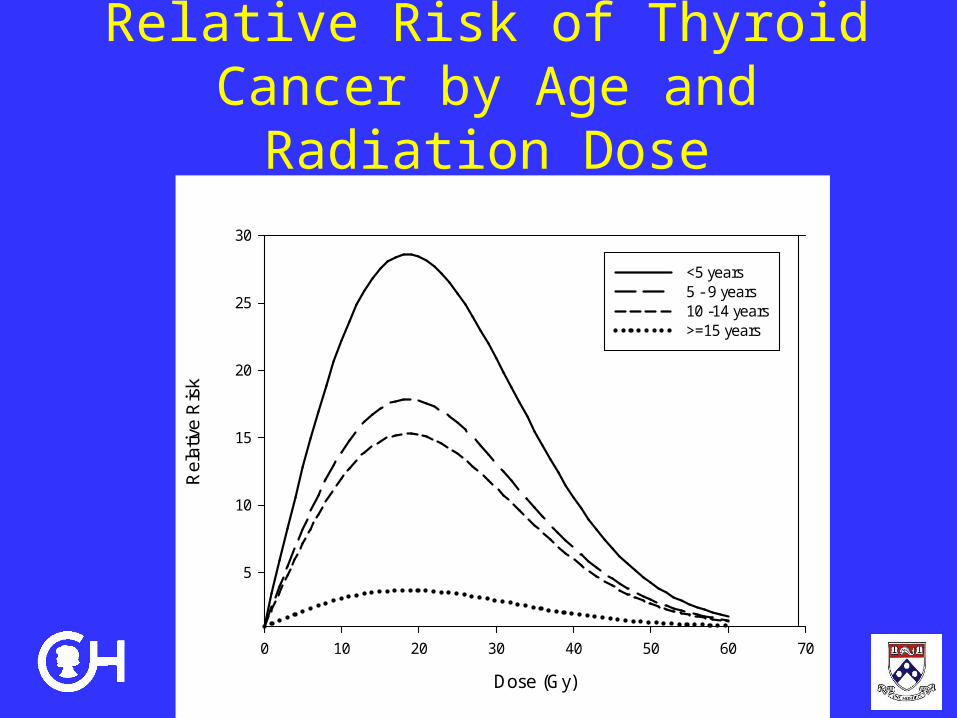
Relative Risk of Thyroid Cancer by Age and Radiation Dose
Dose (Gy)
0 10 20 30 40 50 60 70
Rel
ativ
e R
isk
5
10
15
20
25
30
<5 years5 - 9 years10 -14 years>=15 years

Chemotherapy and Second Neoplasms
• Alkylators: myeloid leukemia and MDS– chromosomes 5 and 7 abnormalities
– latent period 3 to 7 years
– dose relationship
• Epipodophyllotoxin:monocytic leukemia – chromosome 11q23 abnormality
– dose and schedule dependent
– short latent period

Years since diagnosis
Cu
mu
lativ
e in
cid
en
ce
0.0 10.0 20.0 30.0
0.0
0.1
00
.20
0.3
0LESG - Second Malignant NeoplasmsLESG - Second Malignant Neoplasms

Subsequent Neoplasms following Subsequent Neoplasms following update of LESG cohortupdate of LESG cohort
0
50
100
150
200
250
All Neoplams Solid Tumors AML/NHL
1985 1994 2000

Breast Cancer After Thoracic Radiation in Childhood
• MEDLINE, EMBASE, Cochrane Library and CINAHL search – 1966 to 2008
• Cumulative incidence 40-45 years 13-20% • SIR 13.3-55.5• Incidence increased linearly with RT dose• ~13% Bilateral; most metachronous• Benefits of targeted surveillance screening

Second Cancers in Genetic Retinoblastoma
• Pineal gland
- familial cases at greater risk
• Bone and soft tissue sarcomas
- 6 to 10% up to 20 years without radiation
- increasing frequency with time after
radiation
• Malignant melanoma; leiomyosarcoma

0
10
20
30
40
0 10 20 30 40 50Time After Retinoblastoma Diagnosis, yrs
Per
cen
t C
um
ula
tive
Inci
den
ce, %
Hereditary
963 760 615 401 14730
Non-Hereditary
638 570 500 317 13446
Number of Patients at Risk
36.0%
5.69%
Cumulative Incidence of a Second Cancer
Hereditary Retinoblastoma
Non-Hereditary Retinoblastoma
0
10
20
30
40
0 10 20 30 40
Survival (Years)
Pe
rce
nt
Cu
mu
lati
ve
Inc
ide
nc
e
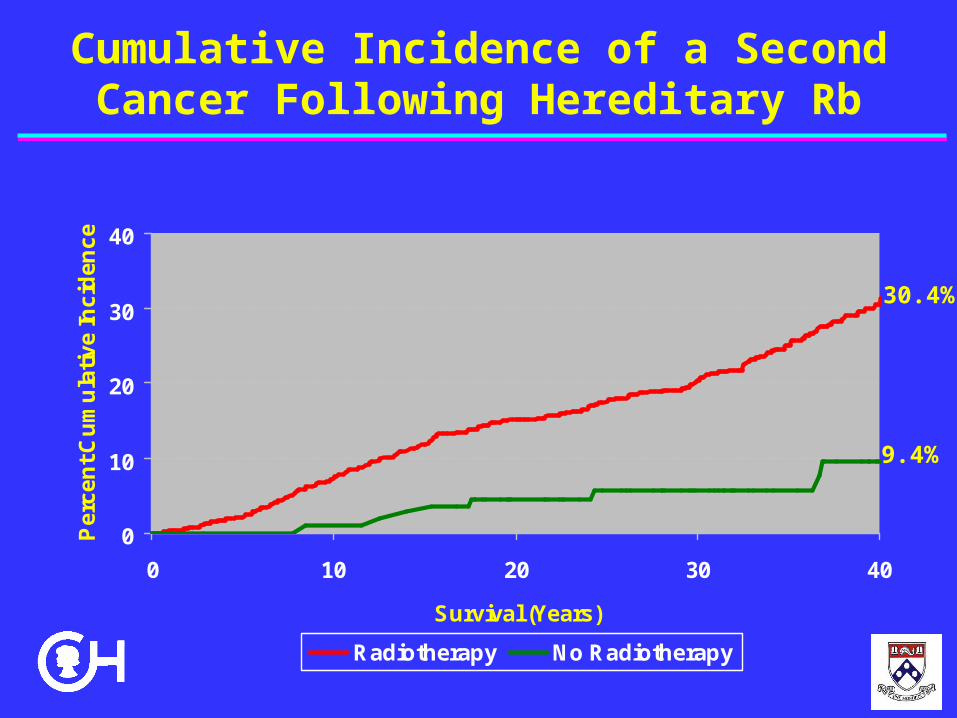
Radiotherapy No Radiotherapy
Cumulative Incidence of a Second Cancer Following Hereditary Rb
30.4%
9.4%

NEUROFIBROMATOSIS TYPE 1

GORLIN SYNDROMERadiation for Medulloblastoma
Psychosocial Late Effects
• Fear of recurrence and death• Adjustment to physiological late effects• Sexuality/intimacy issues• Changes in social support• Employment discrimination• Insurance discrimination• Financial issues• Quality of life issues

Symptoms of PTSD
• Hypervigilance for threat
• Avoidance of traumatic reminders
• Recurrent intrusive memories
• Reckless behavior
• Regressive dependency
• Affective blunting/numbing
• Irritability
• Sense of isolation

Positive Psychosocial Late Effects
• Greater appreciation for life
• Increased life satisfaction
• Renewed spirituality or religiosity
• Improved self-acceptance & self-awareness
• Strengthened relationships with significant
others
• Increased ability to cope with adversity
• Present-centered awareness

Reduction in Psychosocial Morbidity
• Individual and group support during therapy
• Incorporate family members in education and counseling
• Identify families at high risk requiring additional intervention
• Continue support after completion of therapy

Survivors’ Needs• Education
• Treatment• Risk factors• Surveillance
• Surveillance • Early detection of problems• Anticipatory guidance• Modifiable risk factors
• Empowerment/Advocacy • Education• Awareness

Transition from Pediatrics to Adult Focused Care
• Determining readiness for transition
• Providing comprehensive care that is user-friendly in an adult-centered environment
• Transmitting information from pediatrics to adult setting
• Development of a stable infrastructure for ongoing care and research

Ideal Follow-up Program
• Coordinated, comprehensive care
• Multidisciplinary; culturally and socially appropriate
• Health education and anticipatory guidance based on therapy and other risk factors
• Transition to adult health care system

Survivor Intervention to Reduce
Late Effects• Health education re: exercise, diet,
sun, smoking cessation
• Reproductive counseling
• Psychosocial support
• Education regarding previous disease history
• Discussion of risks associated with treatment

Provider Education to Reduce Late Effects
• Increase knowledge of late effects of cancer therapy
• Improve ability to recognize and treat subclinical late effects
• Detect second cancers early– Screening of high risk patients for
RT-associated cancers– Counseling of survivors with
genetic predisposition

Transitional Care Models
• Disease Specific: disease specific where individuals move from pediatric specialist to adult specialist.
• Generic: adolescent focused, move from pediatric, adolescent to adult services with disease specialist as part of the team.
• Primary Care: use a family practitioner, with specialist as consultants*
• Single Site: use same clinical environment and moves from pediatric to adult with specialist as consultants

Obstacles to TransitionPatient
• Dependent Behavior; Immaturity• Severe Illness/Disability• Lack of support systems• Lack of trust in caregivers• Poor adherence to treatment regimes• Psychological Issues

Obstacles to TransitionFamily
• Emotional dependency
• Excessive need to control
• Heightened perception of disability
• Lack of trust in caregivers
• Mistaken perception of potential survival
• Psychological Issues

Obstacles to TransitionPediatric Caregiver
• Concerns about the program
• Emotional bond with patient and family
• Perceptions of own skill as caregiver
• Distrust of adult caregiver
• Ambivalence towards transition
• Economic concerns

Obstacles to TransitionAdult Caregiver
• Lack of familiarity with childhood cancer and late effects
• Heightened perception of care demands
• Lack of institutional support
• Economic concerns

Research Questions
• Incidence and prevalence of late effects of cancer treatment
• Relationship between treatment modality, including dose, and late effects
• Ways to reduce the physiological and psychosocial morbidity of cancer treatment
• Interventions to improve the quality of survival throughout the lifespan
Research Questions• How best to provide comprehensive care
throughout the life span of survivors• What is the best venue for follow-up care• Will insurance cover necessary care• How to monitor changes in survivors as they
age• How to determine readiness to transition• Does systematic evaluation and follow-up
care reduce late effects

Research Principles
Hypotheses• Supported by clinical observations• Involve important outcomes• Availability of preliminary information
Methods• Retrospective or prospective• Availability of necessary sample size • Avoidance of selection bias • Sufficient resources for completion of study• Follow-up is adequate

Clinical Care/Research Conflicts
• Procedures– Interventions based on clinical need
• Reimbursement for studies– Some not clinically indicated
• Investigator interest, time, expertise– Acute care needs take priority

Conclusions
As survivors enter the third and fourth decade of life they will need to
cope with the normal demands of young adulthood while dealing
with possible physical and psychological effects of their cancer
treatment.
Transition programs for young adult survivors should determine
readiness for transition, develop/interpret guidelines, and provide
research opportunities that test the appropriate venues for care
and the effectiveness and efficiency of surveillance guidelines.


