adv. microbiology case study
TRANSCRIPT

Case study created by : Robert Patrick Fredal II
I C. Diff-iculty Ahead

PATIENT HISTORY
A 67 year old female presented to the hospital because of ongoing
watery diarrhea that occurred up to 7 times a day for the past five
days. Signs of dehydration were noted and she has also been
complaining of moderate to severe abdominal pain, fever, nausea,
and loss of appetite. Upon further investigation this patient was
treated with antibiotics a week prior due to a nosocomial urinary tract
infection acquired after her lengthy hospital stay for a broken hip.
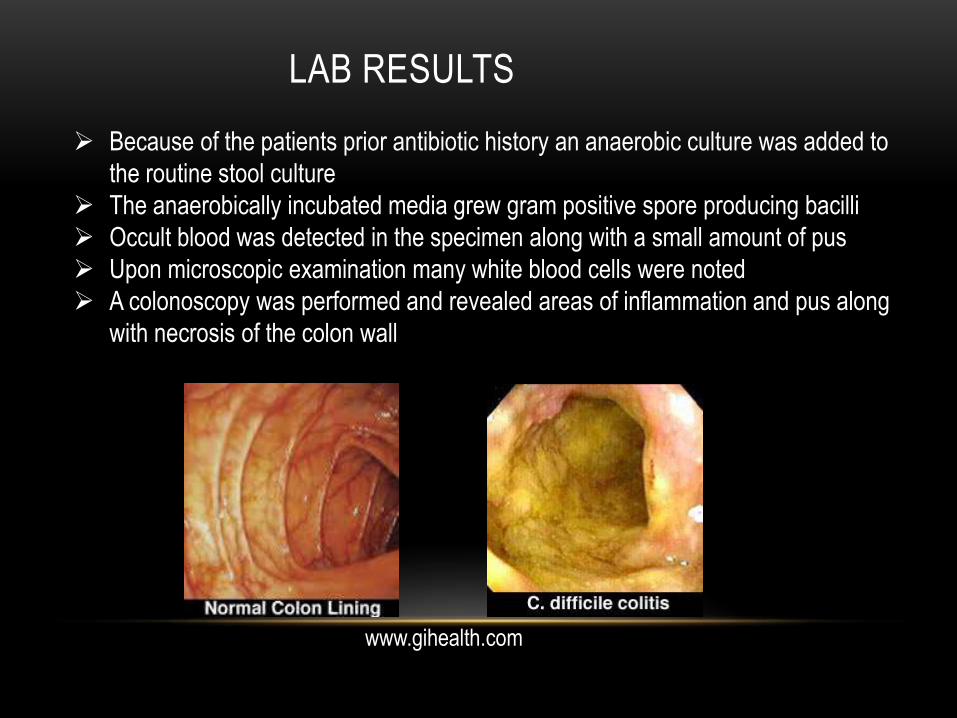
LAB RESULTS
Because of the patients prior antibiotic history an anaerobic culture was added to
the routine stool culture
The anaerobically incubated media grew gram positive spore producing bacilli
Occult blood was detected in the specimen along with a small amount of pus
Upon microscopic examination many white blood cells were noted
A colonoscopy was performed and revealed areas of inflammation and pus along
with necrosis of the colon wall
www.gihealth.com

What is the possible diagnosis of this patient?
What organism could be causing this?
She was diagnosed with pseudomembranous colitis,
confirmatory tests were done and came up positive for
Clostridium difficile
Other pathogenic species of the Clostridium genus
include: C. botulinium (botulism) this organism produces an
active neurotoxin and can have CNS involvement such
as blurred vision
C. perfringens ( gas gangrene) cause of amputations in
diabetics
Clostridium tetani (tetanus) which causes painful muscle
spasms that can often lead to respiratory complications

Clostridium difficile: the basics
It is One of the most serious nosocomial infections
worldwide
Associated with antibiotic associated diarrhea
(20-30% of all cases)
can range from self limiting diarrhea and flu-
like symptoms to life-threatening colitis
It can be a small part of an adults normal gut flora
More than half a million people become ill a year
because of this organism
In recent years C. difficile has because more
frequent than ever before, more severe, and
even more difficult to treat
The most virulent strain (BI/NAP1/027) has
increased toxin production and drug resistance
http://www.vancocin-us.com/healthcareprofessionals/aboutcdifficile

Cultural characteristics
Gram positive bacilli
They can look club shaped with a bulge at
each end
Forms endospores
Strict anaerobe
Grows well on SBA at 37 degrees celcius
Colony morphology; Glossy, gray/white , circular
colonies with a rough edge, fluoresce green-
yellow under UV light, non-hemolytic, and a
characteristic farmyard smell
peritrichous flagella
http://lancastria.net/blog/new-drug-to-treat-c-diff.html
http://depts.washington.edu/molmicdx/mdx/tests/cdiff.shtml

Culture media
Cycloserine Cefoxitine Fructose Agar (CCFA)
Selective medium used for C. difficile
D-cycloserine and cefoxitine antibiotics are added to inhibit most other
organisms
Colonies appear large, flat, yellow , ground glass look , and a filamentous
edge can be observed
Spores are absent when grown on artificial media along with reduced
motility
Has a characteristic “Farmyard” smell
http://www.cdc.gov/media/dpk/2014/dpk-hai.html
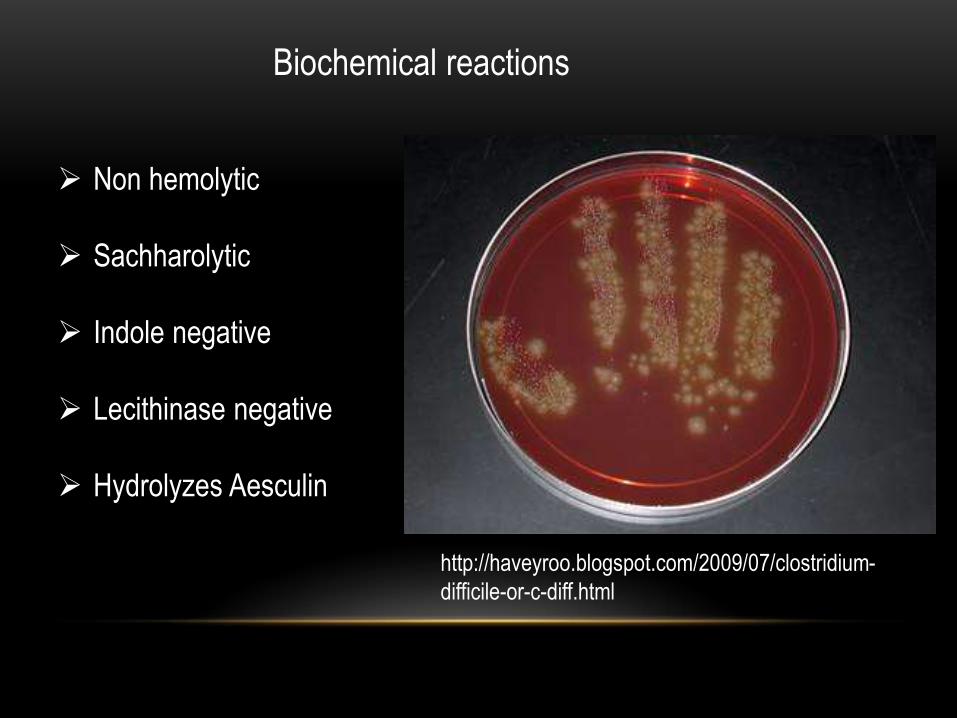
Biochemical reactions
Non hemolytic
Sachharolytic
Indole negative
Lecithinase negative
Hydrolyzes Aesculin
http://haveyroo.blogspot.com/2009/07/clostridium-
difficile-or-c-diff.html

Identification
Cell cytotoxicity assays are considered the gold standard
test for detection of C. difficile toxin by observing the
cytopathic effects of the toxin in cell culture
Enzyme ImmunoAssays (EIA) and Enzyme-Linked
Immunosorbent Assay (ELISA) tests are available for use
and can detect toxins A and B
PCR is also now starting to be used

Clinical Significance
Antibiotic associated diarrhea
Colitis
Pseudomembranous colitis
Perforated colon
Inflammatory bowel disease
Paralytic ileus
Toxic mega colon
Sepsis
Death

Virulence factors
Enterotoxin (Toxin A)
Stimulates chemotaxis and induces cytokine production that leads to
hyper secretion of fluids from the bowel
Cytotoxin ( Toxin B)
Causes depolymerization of actin accompanied by loss of the cellular
cytoskeleton (cytopathic effect)
Binary toxin
It is unclear the role of this toxin but it may synergistically increase the
virulence of toxins A & B
Adhesion factor
Aids in binding to cells in the colon
Hyaluronidase ( produces hydrolytic activity)
Spore formation
Allows for the organism to remain viable under harsh conditions and for
long periods of time

Pathogenic Mechanisms
Antibiotics reduce normal flora which allows for C. diff to start
to multiply and begin to overtake the normal gut bacteria
Toxins are produced and cause degradation of the cell
cytoskeleton
This causes loss of cell shape and decreased adherence
to eachother
Fluid leaks occur which leads to the watery diarrhea
The toxins can also erode away the colon membrane and
in severe cases can cause bowel perforation

http://www.cdiff-support.co.uk/about.htm
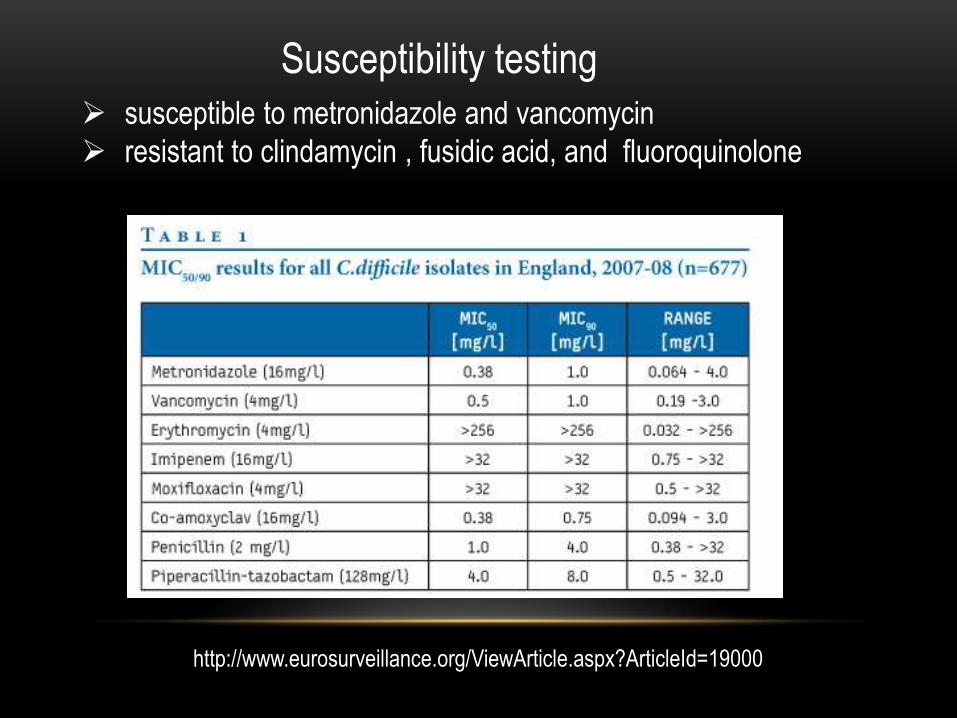
Susceptibility testing
susceptible to metronidazole and vancomycin
resistant to clindamycin , fusidic acid, and fluoroquinolone
http://www.eurosurveillance.org/ViewArticle.aspx?ArticleId=19000

Treatment
First you should discontinue taking antibiotics that likely caused the
infection
Keep thoroughly hydrated
Normally oral metronidazole is given(DOC), but in more complicated
infections oral vancomycin is administered
Human micro biota transplants (poo transplant)
Repopulates the gut and suppresses the growth of C. diff
Probiotics
Surgery may be needed depending on the damage to the bowel (
colectomy)
Prevention and disease control
WASH YOUR HANDS with soap and
water
Alcohol-based hand cleansers do
not kill C.diff spores
Patient is isolated in a room that includes
an attached bathroom
Contact precautions
Cleansing with bleach to disinfect any
potentially contaminated surfaces
http://www.nanobugs.com/shop/sposters.html