advances in pulse oximetry samuel y. ash, m.d. resident, department of internal medicine university...
TRANSCRIPT

Advances in Pulse Oximetry
Samuel Y. Ash, M.D.Resident, Department of Internal
MedicineUniversity of Washington Medical Center

Disclosures
• No financial disclosures.• Research presented is unfunded.
Outline
• Background and Technological Review
• Limitations of Traditional Pulse Oximetry
• Next Generation Pulse Oximetry– Pulse CO-Oximetry
• Applications of Pulse CO-Oximetry• Conclusions• Future Areas of Research

Background and Technological Review
• Beer-Lambert Law:– by knowing the absorptive properties of
a solution or tissue, one can determine the relative concentrations of the solutes in that solution or tissue

Background and Technological Review
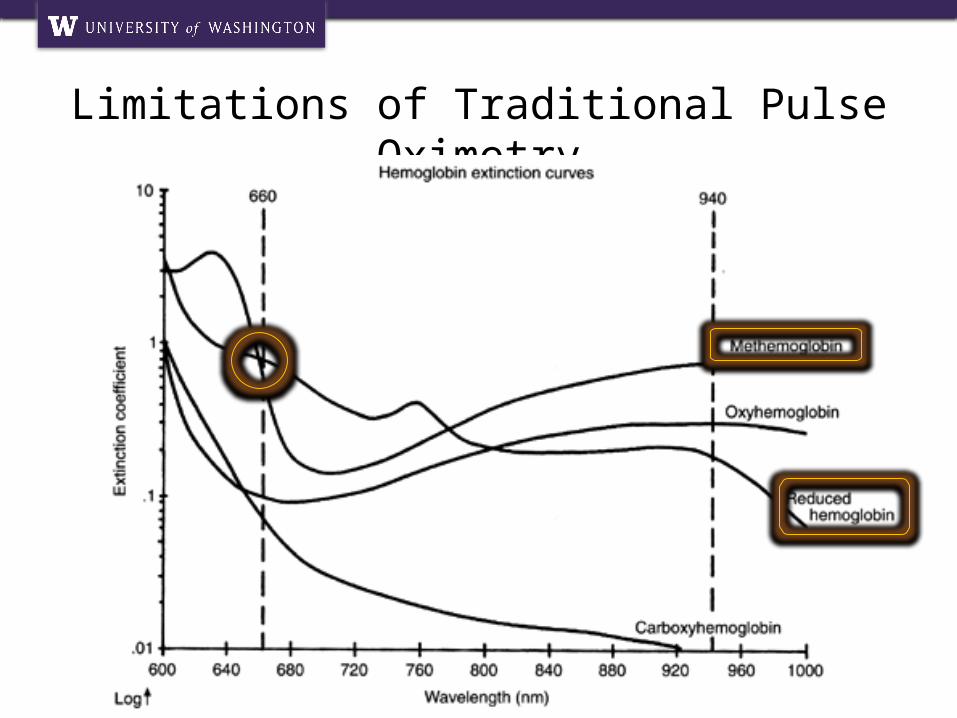
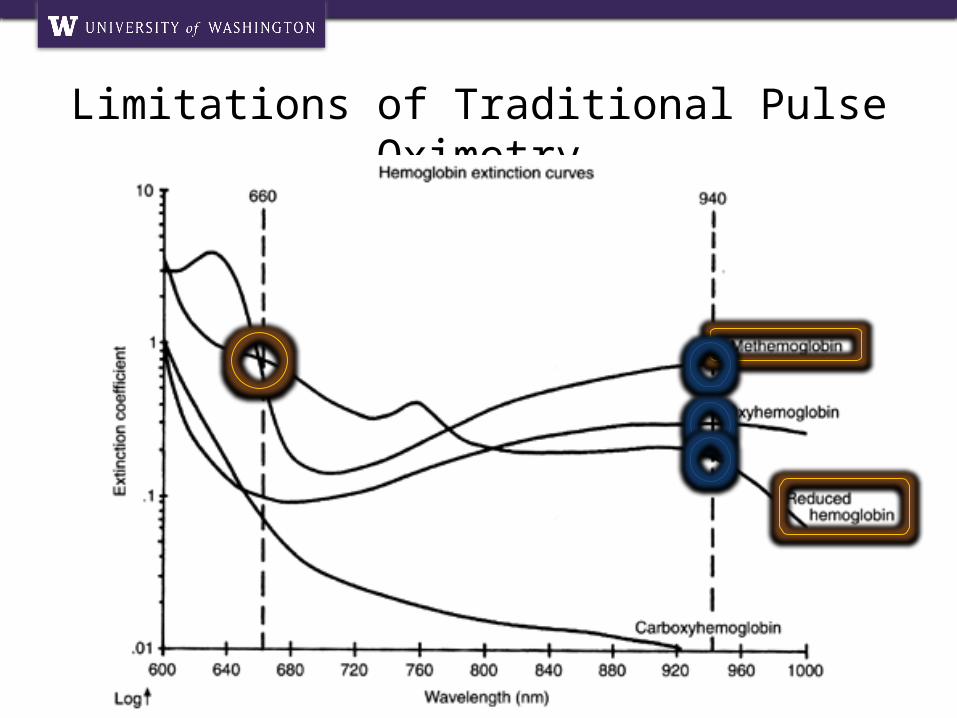
• Traditional Pulse Oximetry:– 940nm
• Near-infrared• Oxyhemoglobin
– 660nm• Red• Deoxyhemoglobi
n
Image source: Isenhour JL and Slovis CM. Arterial Blood Gas Analysis. J Respir Dis 2008. 29;2: epub.
Limitations of Traditional Pulse Oximetry
• Calibration assumptions– Measurements in young volunteers– Use of empirical calibration curves
• Optical interference– Dyshemoglobinemias– Bilirubin and intravenous dyes
• Signal artifact– False signal– Low signal to noise ratio
FunctionalOxyhemoglobinDeoxyhemoglobin
Limitations of Traditional Pulse Oximetry
Dyshemoglobinemias
Non-functionalCarboxyhemoglobinMethemoglobin
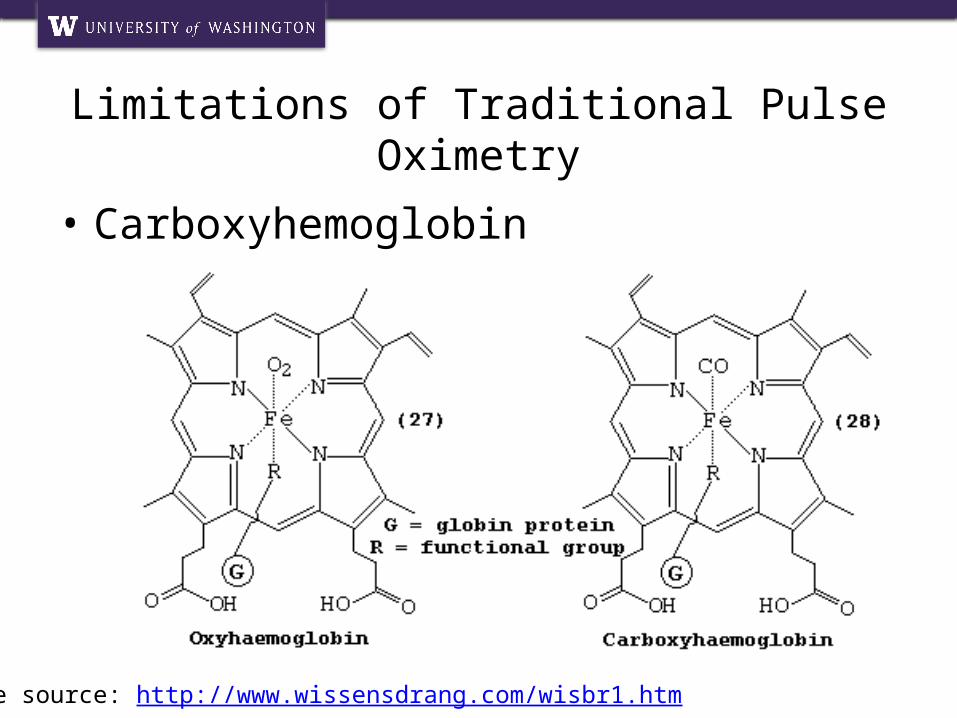
• Carboxyhemoglobin
Limitations of Traditional Pulse Oximetry
Image source: http://www.wissensdrang.com/wisbr1.htm
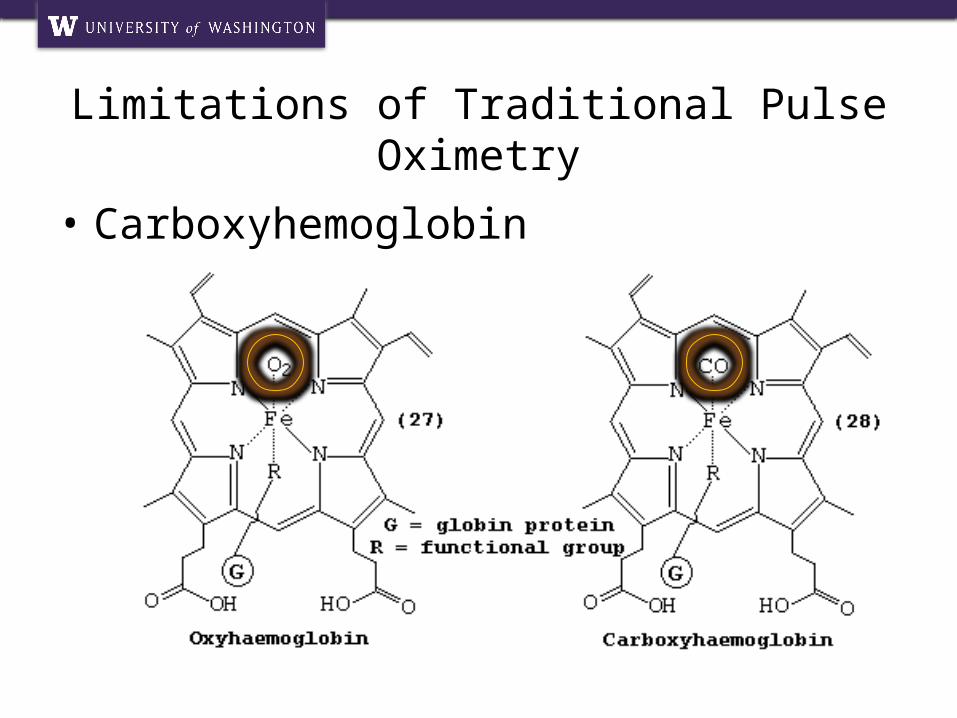
• Carboxyhemoglobin
Limitations of Traditional Pulse Oximetry
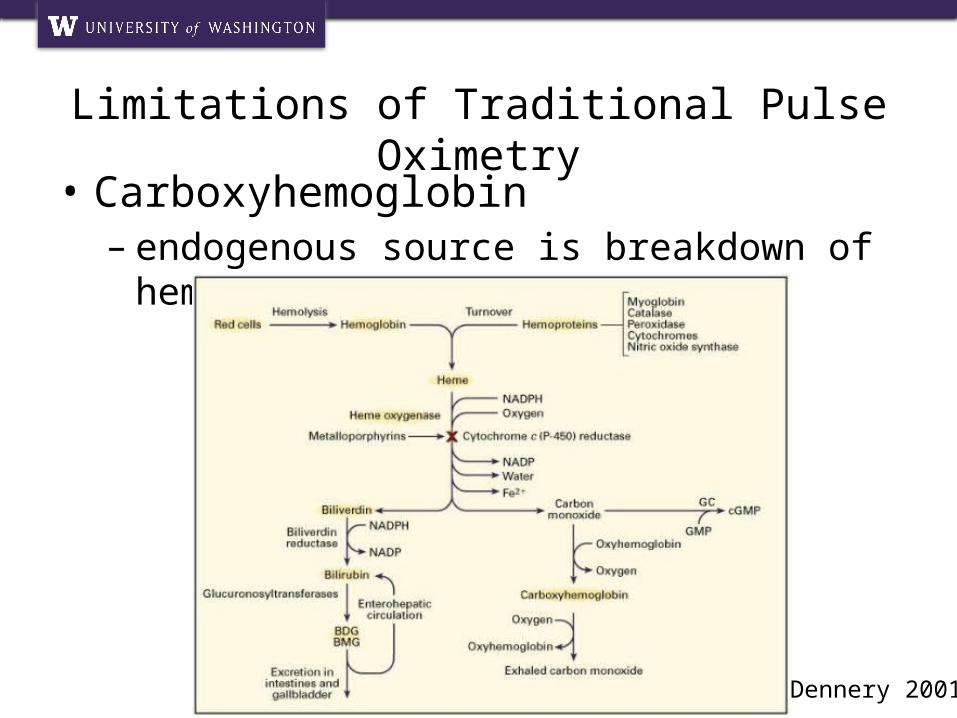
• Carboxyhemoglobin– endogenous source is breakdown of
heme
Limitations of Traditional Pulse Oximetry
Dennery 2001
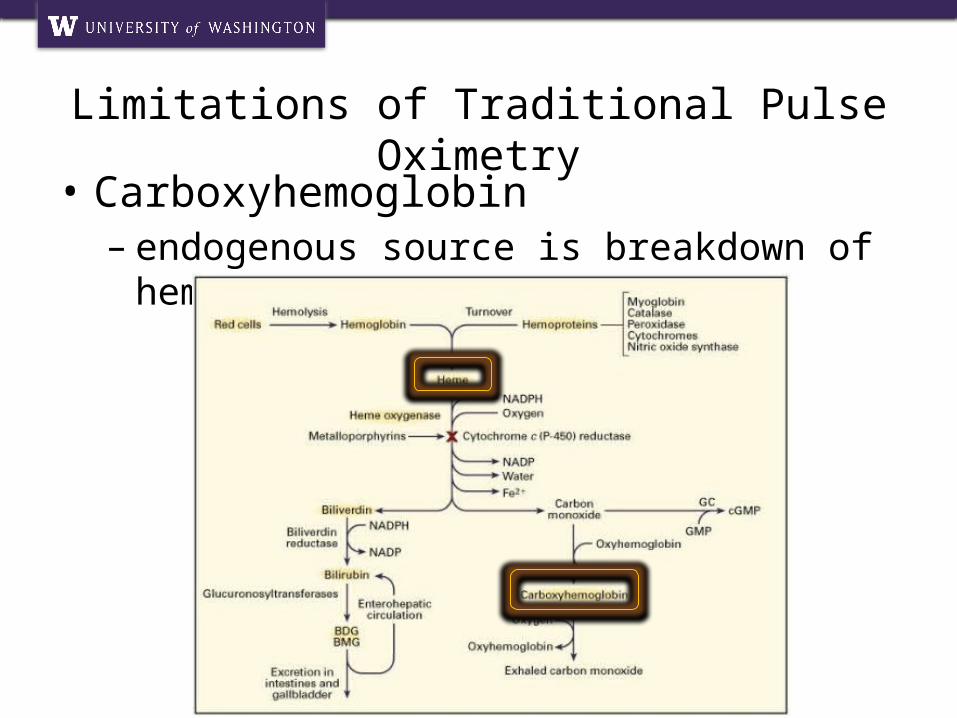
• Carboxyhemoglobin– endogenous source is breakdown of
heme
Limitations of Traditional Pulse Oximetry

• Carboxyhemoglobin– Typically associated with exposure to
exogenous carbon monoxide– Levels in most non-smokers: 1-2%– Levels in heavy smokers: up to 10-20%– Increased in cirrhosis by 2%
Limitations of Traditional Pulse Oximetry
Image sources: townipproject.wikispaces.com, tobaccofreewny.com, woodstove.net

Limitations of Traditional Pulse Oximetry
Image source: http://web.squ.edu.om/med-Lib/MED_CD/E_CDs/anesthesia/site/content/v03/030220r00.HTM
Limitations of Traditional Pulse Oximetry
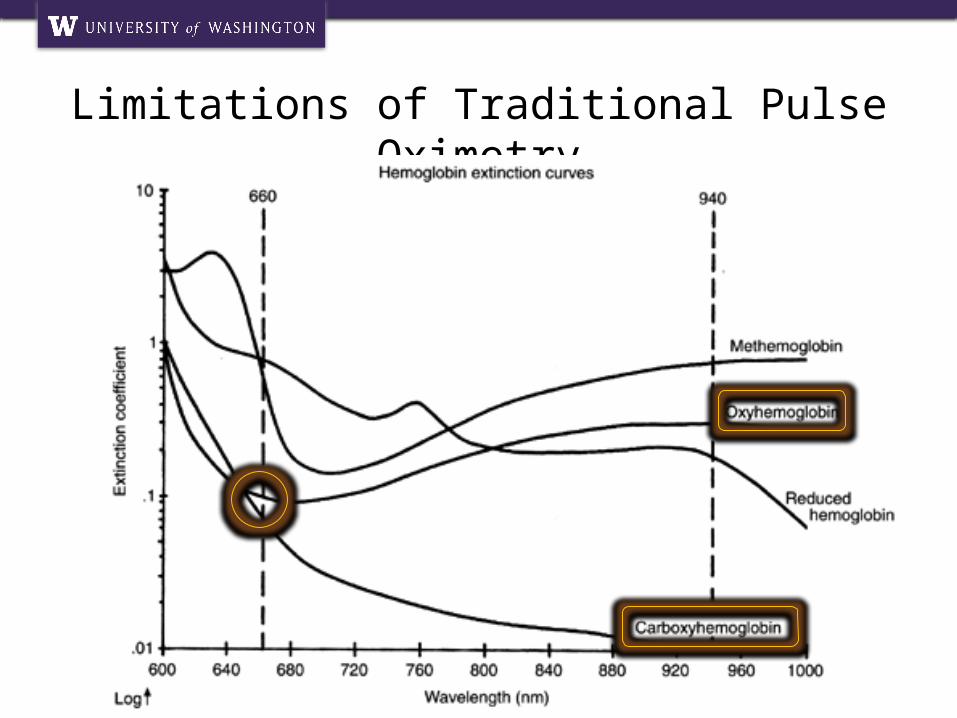
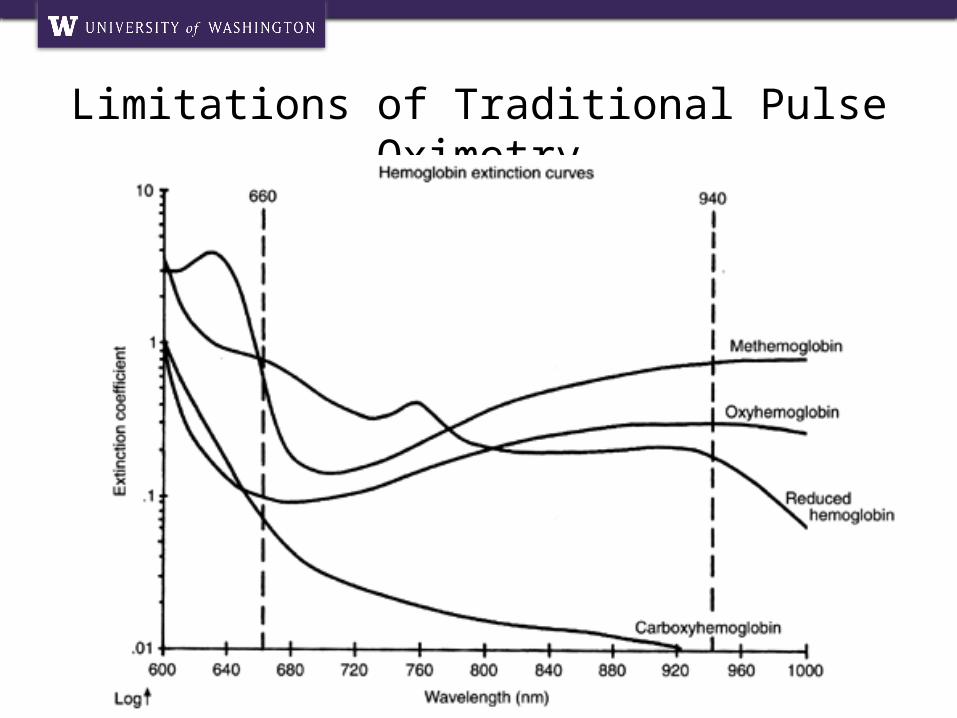
• Carboxyhemoglobin– Absorbs light at 660nm much like
oxyhemoglobin– Effect on measured oxygen saturation
(SpO2) is to overestimate true oxygen saturation
– Overestimation is approximately proportional to the carboxyhemoglobin level (COHb)
• SpO2 = SaO2 + %COHb
Limitations of Traditional Pulse Oximetry

• Carboxyhemoglobin– causes relative hypoxia due to carbon
monoxide’s affinity for hemoglobin– triggers inflammation through multiple
pathways resulting in cardiac and neurologic injury
Limitations of Traditional Pulse Oximetry
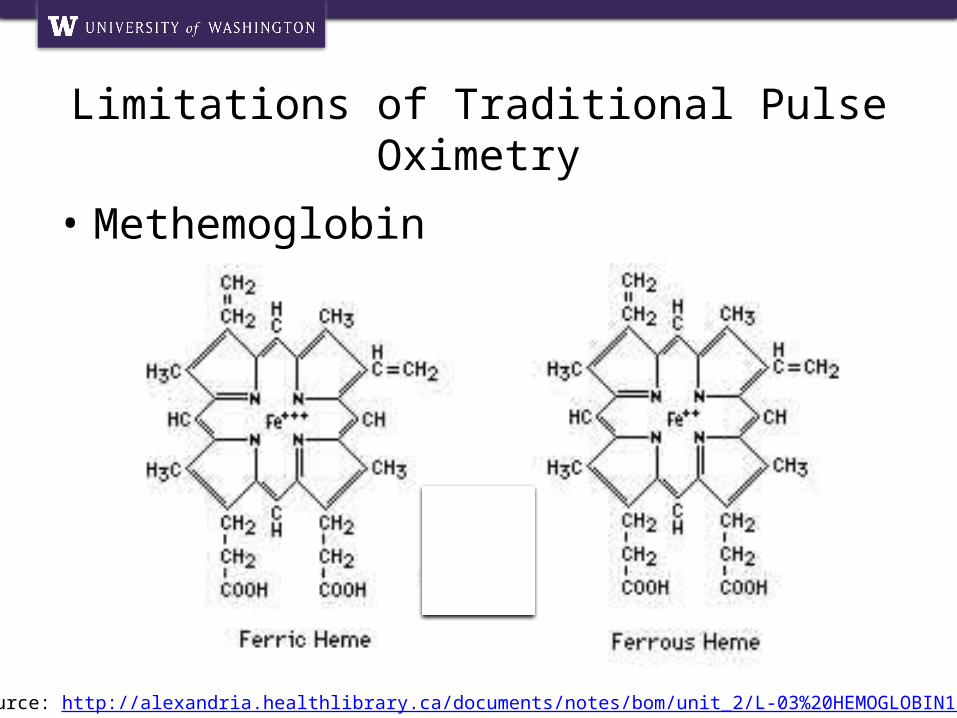
• Methemoglobin
Limitations of Traditional Pulse Oximetry
Image source: http://alexandria.healthlibrary.ca/documents/notes/bom/unit_2/L-03%20HEMOGLOBIN1.xml

• Methemoglobin
Limitations of Traditional Pulse Oximetry

• Methemoglobin– Congenital– Exposure to a number of different
agents• Antibiotics – especially sulfa• Local anesthetics• Nitrates
Limitations of Traditional Pulse Oximetry
Limitations of Traditional Pulse Oximetry
Limitations of Traditional Pulse Oximetry
Limitations of Traditional Pulse Oximetry
• Methemoglobin– Increases both numerator and
denominator of the ratio of relative absorbances
– Drives ratio toward 1 which results in measured SpO2 of 85%
Limitations of Traditional Pulse Oximetry
Pulse CO-Oximetry
• Masimo Rainbow® SET Pulse CO-Oximetry– Introduced in 2005– Rainbow: uses 8 wavelengths of light– SET: Signal Extraction Technology
• Masimo Radical 7
Pulse CO-Oximetry
Pulse CO-Oximetry
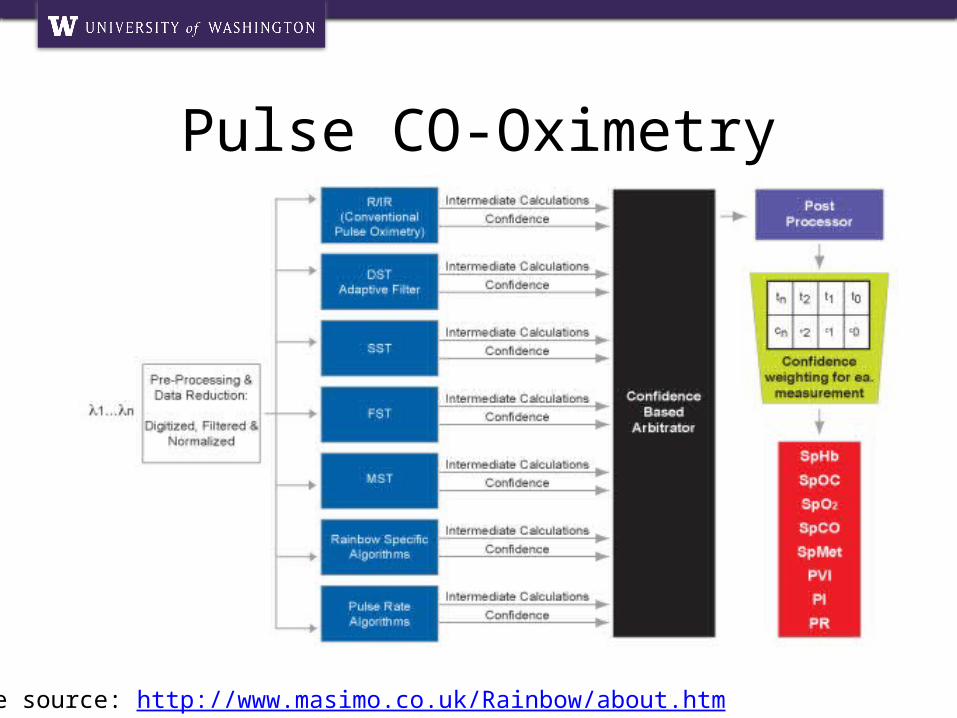
Image source: http://www.masimo.co.uk/Rainbow/about.htm
Pulse CO-Oximetry
• Measurements– Total hemoglobin (SpHb)– Oxygen content (SpOC)– Oxygen saturation (SpO2)– Carboxyhemoglobin (SpCO)– Methemoglobin (SpMet)– Photoplethysmographic (Pleth)
variability index (PVI)– Perfusion index (PI)– Pulse rate (PR)
Pulse CO-Oximetry
• Measurements– Total hemoglobin (SpHb)– Oxygen content (SpOC)– Oxygen saturation (SpO2)– Carboxyhemoglobin (SpCO)– Methemoglobin (SpMet)– Photoplethysmographic (Pleth)
variability index (PVI)– Perfusion index (PI)– Pulse rate (PR)
Pulse CO-Oximetry
• Measurements– Total hemoglobin (SpHb)– Oxygen content (SpOC)– Oxygen saturation (SpO2)– Carboxyhemoglobin (SpCO)– Methemoglobin (SpMet)– Photoplethysmographic (Pleth)
variability index (PVI)– Perfusion index (PI)– Pulse rate (PR)
Applications of Pulse CO-Oximetry
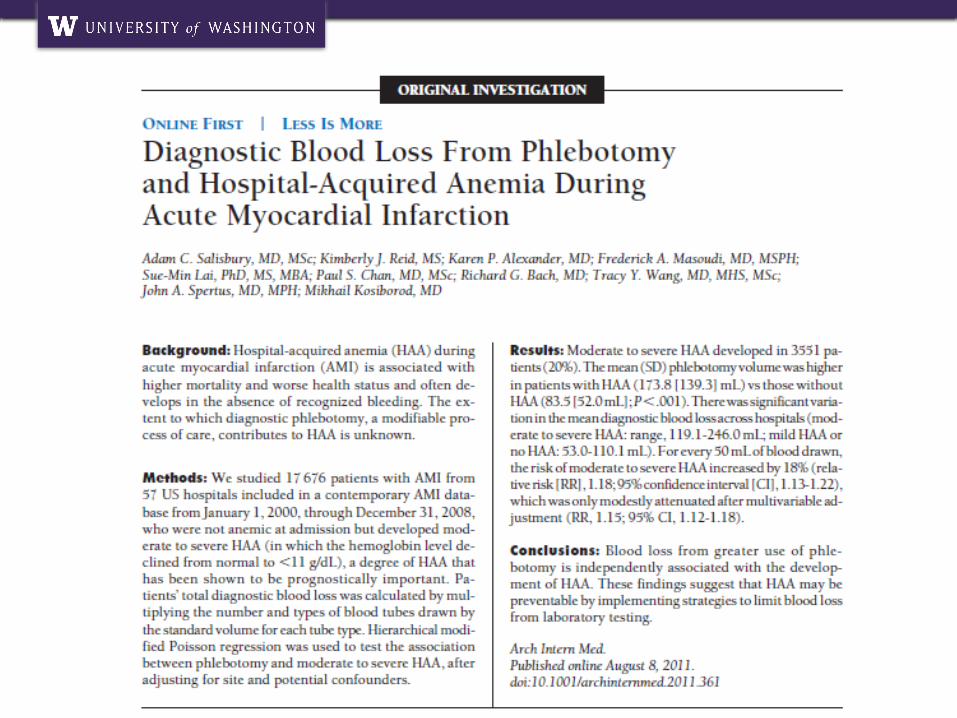
• Total hemoglobin – need– Among the most commonly checked
laboratory values– Current methods invasive, time
consuming and intermittent– Blood draws result in significant hospital
acquired anemia
• Total hemoglobin – evidence for– Macket 2007: first clinical validation
study– Macket 2010: pulse co-oximetry based
SpHb is accurate within 1.0 g/dL in health volunteers undergoing hemodilution
– Causey 2011: appears accurate in general surgery population
– Frasca 2011: pulse co-oximetry based SpHb in ICU patients without ongoing bleeding
Applications of Pulse CO-Oximetry

• Total hemoglobin – evidence against– Lamhaut 2011:
• Small systematic bias• Significant lack of precision• Significant number of outliers
– Gayat 2011: • Moderate systematic bias• Difficulty obtaining in “sicker” patients
Applications of Pulse CO-Oximetry

• Total hemoglobin – evidence for further research– Miller 2011:
• Not accurate enough for all clinical scenarios• Accuracy appears to improve with time
Applications of Pulse CO-Oximetry
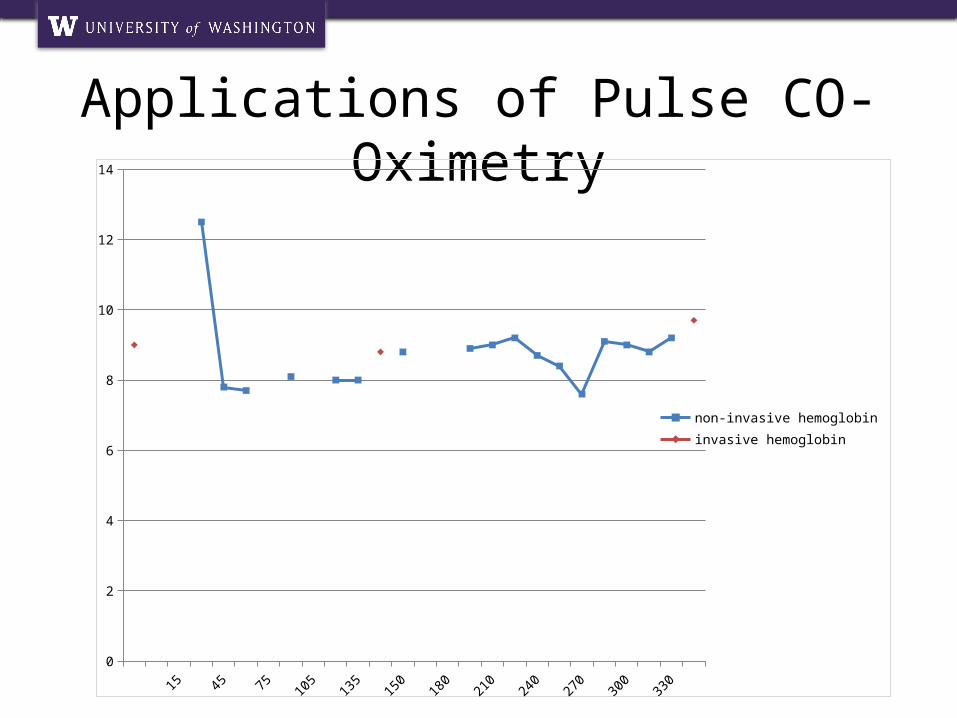
• Total hemoglobin – ongoing work– Non-invasive measurement of total
hemoglobin in the ICU setting• Blinded• Prospective• ICU patients receiving blood transfusion• Ongoing subject enrollment• Preliminary results suggest significant
lack of precision in noninvasive measurements due to outliers*
– *Preliminary data
Applications of Pulse CO-Oximetry
Applications of Pulse CO-Oximetry
-213
0 15 30 45 60 75 90 105 120 135 147 150 165 180 195 210 225 240 255 270 285 300 315 330 4160
2
4
6
8
10
12
14
non-invasive hemoglobininvasive hemoglobin

Applications of Pulse CO-Oximetry
-213
0 15 30 45 60 75 90 105 120 135 147 150 165 180 195 210 225 240 255 270 285 300 315 330 4160
2
4
6
8
10
12
14
non-invasive hemoglobininvasive hemoglobin

• Carboxyhemoglobin – toxicity– causes relative hypoxia due to carbon
dioxide’s affinity for hemoglobin– triggers inflammation through multiple
pathways resulting in cardiac and neurologic injury
– Symptoms are nonspecific: • mild headache, nausea, confusion, dizziness• MI, stroke, death
Applications of Pulse CO-Oximetry
• Carboxyhemoglobin – evidence for– Case reports of noninvasive
measurement resulting in diagnosis• Crawford 2008: CO poisoning onboard
submarine• Roth 2009: CO poisoning due to water
heater
– Roth 2011: acceptable bias and precision for screening for CO poisoning in ED
– Suner 2007: acceptable correlation for screening for CO poisoning in ED
Applications of Pulse CO-Oximetry
• Carboxyhemoglobin – evidence against– Touger 2010: sensitivity of only 43% for
patients with lab values of COHb greater than 15%
• NB: enrollment was for suspected CO poisoning
Applications of Pulse CO-Oximetry
• Carboxyhemoglobin – transfusion– Reports of alarming levels of
carboxyhemoglobin in banked blood– Large volume transfusion may lead to
prolonged increases in COHb levels
Applications of Pulse CO-Oximetry
• Carboxyhemoglobin – ongoing research– Non-invasive measurement of
carboxyhemoglobin in the ICU setting• Blinded• Prospective• ICU patients receiving blood transfusion• Ongoing subject enrollment• Inadequate data for preliminary results
Applications of Pulse CO-Oximetry

• Carboxyhemoglobin – DLCO– ATS/ERS Task Force on Standardization
of Lung Function Testing recommended adjusting DLCO for total hemoglobin and COHb
• COHb in particular increases “back pressure”
– Mahoney 2007: noninvasive COHb measurements may affect categorization of DLCO impairment
• Retrospective• No laboratory correlation
Applications of Pulse CO-Oximetry
• Carboxyhemoglobin – DLCO– Effect of noninvasively assessed
carboxyhemoglobin levels on diffusing capacity measured during pulmonary function testing
• Prospective• Spot observation at time of PFT
– Both SpHb and COHb– Frequent laboratory correlation
• Ongoing subject enrollment• Preliminary results suggest that lack of
precision in noninvasive measurements limits utility of device
Applications of Pulse CO-Oximetry
Conclusions
• Pulse co-oximetry represents a significant advancement in oximetry technology
• Noninvasive measurement of total hemoglobin in particular requires further investigation and validation prior to widespread use
• Pulse co-oximetry may provide useful screening information in low risk populations
Future Areas of Research
• Sensor technology– Rev E resposable sensor– Rev G resposable sensor

Future Areas of Research
• Total hemoglobin– Guidance of blood transfusion in
patients with GI bleed– Screening for anemia prior to blood
donation
• Pleth variability index– Comparison to pulse variability index
monitors

Acknowledgements• VA Puget Sound Health Care System
–Erik Swenson, M.D.–Richard Goodman, M.D.–Robin Boland–Christopher Click–Diane Houk–Barb–Shelly
Acknowledgements• UW Internal Medicine Residency
– D. Scott Weigle, M.D.– Christopher Knight, M.D.– Tyler Albert, M.D.
• Masimo– Jolene Hagin, R.N.– Serop Gharibian
• Family– Katie Ash Greenzang, M.D.– Sarah Ash, Ph.D.
References• Barker and Badal. The Measurement of Dyshemoglobins and Total Hemoglobin by
Pulse Oximetry. Curr Opin Anaesthesiol 21:805-810.• Barker SJ, Tremper KK, Hyatt J: Effects of Methemoglobinemia on Pulse Oximetry and
Mixed Venous Oximetry. Anesthesiology 1989;70:112-117.• Causey MW et al. Validation of noninvasive hemoglobin measurements using the
Masimo Radical-7 SpHb Station. Am J Surg 2011; 201:592-8.• Crawford DM and Hampson NB. Fire and Ice: Diagnosis of Carbon Monoxide Poisoning
in a Remote Environment. Emerg Med J 2008; 25:235-236.• Dennery PA, Seidman DS and Stevenson DK. Neonatal Hyperbilirubinemia. N Engl J
Med 2001; 344:581-590.• Ehlers M, Labaze G, Hanakova M, McCloskey D and Wilner G. Alarming Levels of
Carboxyhemoglobin in Banked Blood. J Cardiothorac Vasc Anesth 2009; 23:336-338.• Ernst A and Zibrak JD. Carbon Monoxide Poisoning. N Eng J Med 1998; 339:1603-
1608.• Frasca D et al. Accurace of a Continuous Noninvasive Hemoglobin Monitor in
Intensive Care Unit Patients. Crit Care Med 2011; 39(10):1-6.• Gayat E et al. Performance Evaluation of a Noninvasive Hemoglobin Monitoring
Device. Ann Emerg Med 2011; 57:330-333.• Lamhaut L et al. Comparison of the Accuracy of Noninvasive Hemoglobin Monitoring
by Spectrophotometry (SpHb) and HemoCue® with Automated Laboratory Hemoglobin Measurement. Anesthesiology 2011; 115:548-54.

References• Macket MR, Allard M, Applegate RL and Rook J. The Accuracy of Noninvasive and
Continuous Total Hemoglobin Measurement by Pulse CO-Oximetry in Human Subjects Undergoing Hemodilution. Anesth Analg 2010; 111:1424-1167.
• Mahoney AM, Stimpson CL, Scott KL and Hampson NB. Noninvasive Measurement of Carboxyhemoglobin Levels for Adjustment of Diffusion Capacity Measured During Pulmonary Function Testing. Resp Care 2007; 52:1741-1743.
• Miller et al. A Comparison of Three Methods of Hemoglobin Monitoring in Patients Undergoing Spine Surgery. Anesth Analg 2011; 112:858–863.
• Ortega R, Hansen CJ, Elterman K and Woo W. Videos in Clinical Medicine: Pulse Oximetry. N Eng J Med 2011;364:e33.
• Roth et al. Accuracy of Noninvasive Multiwave Pulse Oximetry Compared With Carboxyhemoglobin from Blood Gas Analysis in Unselected Emergency Department Patients. Ann Emerg Med 2011; 58:74-79.
• Roth et al. Victim of Carbon Monoxide Poisoning Identified by Carbon Monoxide Oximetry. J Emerg Med 2009; 40:640-642.
• Salisbury AC et al. Diagnostic Blood Loss From Phlebotomy and Hospital-Acquired Anemia During Acute Myocardial Infarction. Arch Int Med 2011; Epub ahead of print.
• Scheller MS, Unger RJ, Kelner MJ. Effects of Intravenously Administered Dyes on Pulse Oximetry Readings. Anesthesiology 1986;65:550-552.
References• Severinghaus JW. Takuo Aoyagi: Discovery of Pulse Oximetry. Anesth and Analg
2007;105:S1-4.• Sinex JE. Pulse Oximetry: Principles and Limitation;17:59-65.• Suner et al. Non-Invasive Pulse CO-Oximetry Screening in the Emergency
Department Identifies Occult Carbon Monoxide Toxicity. J Emerg Med 2007; 34:441-450.
• Touger et al. Performance of the RAD-57 Pulse CO-Oximeter Compared with Standard Laboratory Carboxyhemoglobin Measurement. Ann Emerg Med 2010; 20(10):1-7.
• Tram TT et al. Carboxyhemoglobin and Its Correlation to Disease Severity in Cirrhotics. J Clin Gastroenterol 2007; 41:211-215.
• Ziemann-Gimmel P and Schwartz DE. Increased Carboxyhemoglobin in a Patient with a Large Retroperitoneal Hematoma. Anesth Analg 2004;99:1800-1802.
The University of Washington is one of the world’s preeminent universities and a recognized leader in
educating the next generation of leaders, thinkers and doers. A multi-campus institution comprising UW Seattle,
UW Tacoma and UW Bothell, as well as a world-class academic medical center, the UW is a focal point of the
Puget Sound region’s intellectual and cultural life and a key contributor to Washington’s increasingly global reputation as a center of innovation and change. A progressive and
quintessentially Northwest institution with a uniquely innovative and creative culture, the UW is driven to lead by successfully integrating the full assets of the university and
its rich environs to address key issues of pressing human concern that make a lasting difference in the Northwest and
around the world.