advances in the analysis of cerebrospinal fluid in the analysis of cerebrospinal fluid*! ... and in...
TRANSCRIPT

ANNALS O F CLIN IC A L AND LABORATORY SC IE N C E, Vol. 27, No. 2 Copyright © 1997, Institute for Clinical Science, Inc.
Advances in the Analysis of Cerebrospinal Fluid*!JOSEPH A. KNIGHT, M.D.
Department o f Pathology and Laboratory Medicine,Salt Lake VAMC,
andDepartment o f Pathology,
University o f Utah School o f Medicine, Salt Lake City, UT 84132
ABSTRACTThe laboratory examination of cerebrospinal fluid (CSF) continues to play an
important role in the clinical diagnosis and treatm ent of various disorders of the central nervous system (CNS). The major conditions currently include, as they have in the past, infectious diseases, neoplastic processes, multiple sclerosis, other demyelinating disorders, and intracerebral hemorrhage. Recent publications suggest a variety of new laboratory tests that may be useful in the evaluation of patients with both primary and metastatic malignancies, Alzheimer’s disease, Creutzfeld- Jacob disease, global ischemia, various psychiatric disorders, CSF otorrhea and rhi- norrhea, and in the differential diagnosis of cortical vs lacunar stroke, among others. Examples of these recent developments and their possible clinical usefulness are discussed.
IntroductionThe laboratory examination of cerebro
spinal fluid (CSF) for diagnosis and treatment of various CNS disorders has been clinically useful for over 100 years. Interestingly, the “routine” testing of CSF during this period, consisting of CSF pressure measurement, total and differential leukocyte count, glucose
* Presented in part at the Association of Clinical Scientists 43rd Annual Applied Seminar entitled "Neurological and Psychiatric Diseases: Molecular Basis and Diagnostic Approaches”, Louisville, KY, 31 October to 3 November, 1996.
tS end reprint requests to: Joseph A. Knight, M.D., Department of Pathology, University of Utah School of Medicine, Salt Lake City, UT 84132.
and protein quantitation, Gram stain, and bacterial culture, is still the mainstay of the CSF examination. However, all of these tests are not necessary in most cases.1,2'3 In selected cases, cultures for tuberculosis and testing for CNS syphilis are also useful. More recently improved techniques in protein analysis, especially high resolution protein electrophoresis and isoelectric focusing to detect oligoclonal bands, are of considerable help in the diagnosis of multiple sclerosis. However, the presence of oligoclonal banding occurs in a wide variety of other CNS disorders.4 Since numerous studies have been published on this subject,5’6,7'8’9'10’11,12 as well as measurements of IgG synthetic rate13 and the IgG/albumin index,14 these topics will not be discussed here.
930091-7370/97/0300-0093 $02.00 © Institute for Clinical Science, Inc.
94 KNIGHT
Over the past quarter of a century, significant advances have been made in our understanding of the various CNS disease processes. As a result, there has been a corresponding interest in developing CSF tests that may be useful in the diagnosis of these disorders. In this report, some of the recent advances in laboratory analysis of CSF will be addressed.Cytological Examination
Cytologic examination for malignancies metastatic to the meninges is very useful since malignant cells are identified, on average, in about 70 percent of these patients.2 In these cases, the CSF usually shows an increase in mononuclear leukocytes, modest increase in CSF protein concentration, and a normal or slightly decreased glucose level. Therefore, a finding of normal cell count and protein level generally excludes the presence of a lep- tomeningeal malignancy, making further examination unnecessary.2
The CNS is a sanctuary for leukemic cells. That is, about 60 percent of patients with acute myeloblastic leukemia and 80 percent of patients with acute lymphoblastic leukemia have leukemic cells in their CSF at some time during their disease.4 Here, the morphologic examination of CSF for leukemic cells is critical in many cases. When leukemic cells are identified, other studies may include cytochemistry, immunophenotyping, DNA studies by flow cytometry, and beta-2-microglobulin levels.15Biochemical Markers o f Malignancy
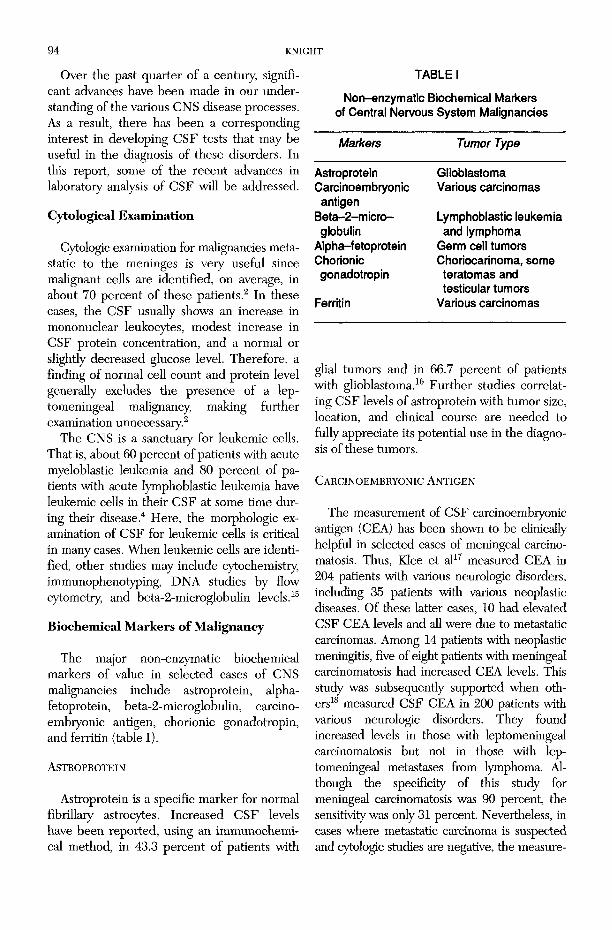
The major non-enzymatic biochemical markers of value in selected cases of CNS malignancies include astroprotein, alpha- fetoprotein, beta-2-microglobulin, carcino- embryonic antigen, chorionic gonadotropin, and ferritin (table I).A s t r o p r o t e in
Astroprotein is a specific marker for normal fibrillary astrocytes. Increased CSF levels have been reported, using an immunochemical method, in 43.3 percent of patients with
TABLE I
Non-enzymatic Biochemical Markers of Central Nervous System Malignancies
Markers Tumor Type
Astroprotein GlioblastomaCarcinoembryonic Various carcinomas
antigenBeta-2-m icro- Lymphoblastic leukemiaglobulin and lymphoma
Alpha-fetoprotein Germ cell tumorsChorionic Choriocarinoma, somegonadotropin teratomas and
testicular tumorsFerritin Various carcinomas
glial tumors and in 66.7 percent of patients with glioblastoma.16 Further studies correlating CSF levels of astroprotein with tumor size, location, and clinical course are needed to fully appreciate its potential use in the diagnosis of these tumors.
C a r c in o e m r r y o n ic A n t ig e n
The measurement of CSF carcinoembryonic antigen (CEA) has been shown to be clinically helpful in selected cases of meningeal carcinomatosis. Thus, Klee et al17 measured CEA in 204 patients with various neurologic disorders, including 35 patients with various neoplastic diseases. Of these latter cases, 10 had elevated CSF CEA levels and all were due to metastatic carcinomas. Among 14 patients with neoplastic meningitis, five of eight patients with meningeal carcinomatosis had increased CEA levels. This study was subsequently supported when others18 measured CSF CEA in 200 patients with various neurologic disorders. They found increased levels in those with leptomeningeal carcinomatosis but not in those with leptomeningeal metastases from lymphoma. Although the specificity of this study for meningeal carcinomatosis was 90 percent, the sensitivity was only 31 percent. Nevertheless, in cases where metastatic carcinoma is suspected and cytologic studies are negative, the measure

ADVANCES IN ANALYSIS OF CEREBROSPINAL FLUID 95ment of CEA will usually be elevated in those tumors known to commonly produce CEA (breast, colon, stomach, some lung cancers).
Beta-2-microglobulin
Beta-2-microglobulin ((32-M), an 11,800 dalton protein, appears on the surface of all nucleated cells as part of the histocompatibility antigen (HLA) antigens. Elevated levels of P2-M are common in certain inflammatory disorders, especially those where lymphocytes are prominent. In this regard, the measurement of (32-M has been reported to be useful to detect early CNS relapse in patients with acute lymphoblastic leukemia or lymphoma.19 These authors noted significantly higher levels in patients with CNS involvement than in those without this complication. Furthermore, serial measurements correlated well with the clinical appearance and disappearance of CNS involvement suggesting that serial serum and CSF p2-M measurements may be useful in early diagnosis and management in these patients. Hallgren et al20 also reported increased CSF (32-M levels in patients with both primary and metastatic malignant brain tumors. Im portantly normal levels were present in those with benign tumors. It should also be noted that CNS involvement with leukemia or lymphoma is more likely when CSF (32-M levels exceed simultaneous serum levels.20
Alpha-fetoprotein
Alpha-fetoprotein (AFP) is a glycoprotein synthesized by yolk sac elements. Elevated CSF levels of AFP have been reported in some patients with metastatic germ cell tumors.21 Furthermore, the 3-subunit of human chorionic gonadotropin ((3-HCG) has been reported to be increased in those with CSF involvement with metastatic choriocarcinomas, germinal cell testicular carcinomas, and gonadotropin-producing teratomas.22 These latter authors noted that (3-HCG levels were generally related to tumor activity during therapy; elevated levels were often noted before clinical or radiologic evidence of metastases.
F erritin
Another non-enzymatic marker for malignancy is ferritin. Zandman-Goddard et al23 quantified CSF ferritin levels in patients with benign inflammatory and non-inflammatoiy neurologic disorders and in patients with various malignancies, both metastatic and nonmetastatic to the brain. They found increased CSF ferritin levels in most CNS inflammatory and metastatic malignant disorders but not in those with non-metastatic tumors or in those with non-inflammatoiy neurologic disorders. Thus, CSF ferritin levels showed high sensitivity for brain tumors and inflammatory disorders but demonstrated very low specificity.
EnzymesNumerous studies have been published to
determine the possible usefulness of measuring enzyme activity in various CNS disorders (table II). In general, the literature is somewhat conflicting regarding the usefulness of measuring enzymes, except in selected cases.
TABLE II
Cerebrospinal Fluid Enzymes in Neurologic Disorders
EnzymeCentral Nervous
System Disorders)
Lactate Leukemia, lymphoma,dehydrogenase primary and metastatic
carcinomas, strokeAspartate Lacunar vs cortical stroke
aminotransferaseCreatine kinase Global ischemia, lacunar
vs cortical strokeLysozyme Primary and metasatic
tumors, myeloblastic and monocytic leukemias, sarcoidosis
Adenosine Tuberculous meningitisdeaminase
Acetylcholinesterase Alzheimer's diseaseNeuron-specific Creutzfeldt-Jacob
enolase disease

96 KNIGHT
It is these latter cases that will be discussed in which various enzyme measurements may be useful.
L a cta te D e h y d r o g e n a s e
Cerebrospinal fluid lactate dehydrogenase (LD) has probably been studied more than any other enzyme. Normal CSF values are about 10 percent of the corresponding serum levels.24 Since LD is ubiquitous, it is elevated in numerous disorders, making it a highly sensitive marker for a variety of diseases. Conversely, total LD has very low specificity and is extremely active in erythrocytes (100 or more times the activity of serum). As a result, the presence of blood or hemolysis results in elevated levels. Nevertheless, total LD may be useful in the early differential diagnosis between bacterial and viral meningitis. In this regard, viral meningitis is usually associated with normal or mildly elevated LD levels while bacterial meningitis is associated with significantly higher levels, including those cases that have been partially treated.24,25
On the other hand, LD isoenzymes significantly improve specificity and may be very useful in meningeal carcinomatosis since most carcinomas show a predominance of LD5. In this regard, Fleisher et al26 reported that the ratio of LD5 to total LD was increased (above 10 percent to 15 percent) in leptomeningeal infiltration by metastatic carcinoma (breast, lung, and malignant melanoma). This pattern is also present in bacterial meningitis since neutrophils have a predominance of LDg. However, in the absence of bacterial meningitis, an elevated LD5 is supportive of a metastatic carcinoma. Lymphomas and lymphoblastic leukemia show a “tenting” pattern with relatively low LDj and LD5 but an increase in LD3 and LD4.4
In addition to these conditions, Lampl and associates27 compared CSF LD levels in patients with transient ischemic attacks (TIA) and early stroke with a control group. They found significantly increased LD levels in those with stroke (mean 40.9 U/L) compared with the TIA (mean 11.8 U/L) and control
(mean 11.2 U/L) groups. In an earlier report Donnan et al28 measured CSF levels of LD, asparate aminotransferase (AST), and creatine kinase (CK) in an attempt to differentiate between lacunar and cortical infarcts. Since cortical infarcts are generally due to embolic phenomena, a search for a proximal site of embolization with carotid angiography is warranted. Conversely, lacunar strokes are usually secondary to small vessel hypertensive disease in which angiography is not helpful. These workers showed a significant increase in at least one of the three enzymes in 80 percent of cortical stroke patients while no increased CK or AST activity was present in patients with lacunar stroke and only a mild LD elevation was seen in some of these patients.
A spartate A m in o t r a n s f e r a s e
Aspartate aminotransferase (AST), similar to LD, is widely distributed. Although not as rich in red cells as LD, mild hemolysis results in elevated levels since they contain about 10 to 15 times the plasma level, which is also significantly higher than it is in CSF. Although AST has been measured in a wide variety of CSF studies, its measurement has not generally been useful except as noted previously in the discussion of LD in which its measurement, along with LD and CK, was considered useful in the differential diagnosis between lacunar and cortical infarcts.28
C r e a t in e K in a se
The brain is rich in creatine kinase (CK). As a result, increased CSF CK levels have been reported in a wide variety of CNS disorders including subarachnoid hemorrhage, hydrocephalus, various brain tumors, cerebral infarction, and in other conditions associated with increased intracranial pressure.29 Total CSF CK levels have also been noted to correlate with the degree of head trauma. Here, Florez et al30 found correspondingly higher CSF CK activity as the severity increased from mild to moderate to severe concussions. In addition, serum CK levels were increased,

ADVANCES IN ANALYSIS OF CEREBROSPINAL FLUID 9 7
depending on the degree of extracranial damage.
The measurement of CSF CK isoenzymes is probably even more helpful in selected CNS conditions since they are more specific owing to the presence of CK-BB, the major isoenzyme in the brain. Chandler et al31,32 studied CSF CK isoenzymes in some detail and recently reviewed this subject33 and came to the following conclusions:(1) Brain tissue contains both CK-BB and
mitochondrial (CK-mt) isoenzymes, the latter making up about 10 percent of the total. Both CK-MM and CK-MB are not normally present.
(2) The presence of CK-MM in CSF is usually secondary to blood contamination. W hen present, CK-MB is usually due to an equilibrium between CK-MM and CK-BB.
(3) Creatine kinase-BB is increased in CSF about 6 hours following an ischemic or anoxic insult. Global brain ischemia, following respiratory or cardiac arrest, results in diffuse cerebral injury with peak CK-BB levels in about 48 hours.
(4) The level of CK-BB gives an estimate of overall brain damage and prognosis for patients suffering global ischemia or anoxia.33 Thus, CSF CK-BB less than 5 U/L indicates little or no neurologic injury; 5 to 20 U/L is associated with mild to moderate neurologic damage; few patients with levels between 21 and 50 U/L awaken and most die; death occurs in almost all patients with CSF CK-BB levels greater than 50 U/L.
(5) Brain damage also results in the release of CK-mt. However, there is poor correlation between CK-mt and CK-BB; measurement of the former is not useful.
Lyso zy m e
Lysozyme (muramidase), a low molecular mass protein (14,300 daltons), catalyzes the depolymerization of mucopolysaccharides. This enzyme is rich in neutrophil and
macrophage lysosomes. Normal CSF contains very little lysozyme activity but markedly elevated levels are present in acute bacterial meningitis. Increased activity has also been reported in cerebral atrophy, various tumors, multiple sclerosis, intracranial hemorrhage, and epilepsy.4
With respect to brain tumors, Newman and associates34 noted prominently increased enzyme activity in patients with both primary and metastatic brain tumors; the degree of elevation reflected the extent of tum or involvement. However, increased levels were not noted in CNS Hodgkins disease or Guillain-Barre syndrome. Elevated lysozyme levels are also common in acute myeloblastic and monocytic leukemia, as well as in various granulomatous disorders, including sarcoidosis.35
A d e n o s in e D e a m in a s e
Adenosine deaminase (AD) catalyzes the irreversible conversion of adenosine to inosine. This enzyme is particularly rich in T-lym- phocytes. Several recent studies suggest that AD measurements in the various body fluids may be useful in the early diagnosis of tuberculosis.36 These authors not only showed that tuberculous effusions have significantly higher AD levels than various other disorders (e.g., tumors, bacterial and viral infections), but they described a rapid method for AD measurement. They found that patients with tuberculous meningitis had a mean enzyme level of 8 U/L, a value over twice that seen in bacterial or viral meningitis, malignancy, subarachnoid hemorrhage, or other disorders. Levels greater than 6 U/L were generally associated with tuberculous meningitis. Mann et al37 reported similar results in children. They noted that CSF AD levels had a sensitivity of 87 percent, specificity of 84 percent, and a predictive value of 87 percent for CNS tuberculosis.
On the other hand, others reported that CSF AD measurements were less helpful. For example, Donald and co-workers38 measured AD in both plasma and CSF in four groups of children: (1) those studied for meningitis but

98 KNIGHT
found to be unaffected (controls); (2) those with aseptic meningitis; (3) those with bacterial meningitis; and (4) those with tuberculous meningitis. They found that both the CSF/plasma AD ratio and CSF AD activity were increased in both tuberculous and bacterial meningitis but not in viral meningitis or the control group. The authors stressed that although AD levels could distinguish viral from tuberculous and bacterial meningitis, its measurement was not useful in separating bacterial from tuberculous meningitis.
A l z h e im e r ’s D is e a s e
In Alzheimer’s disease, there is a regional brain loss in the activity of enzyme markers in the cholinergic system. For example, Atack et al39 measured acetylcholinesterase (AChE) and butylcholinesterase (BChE) activities and protein concentration in the CSF of 26 healthy controls aged 20 to 86 years, 27 patients with dementia of Alzheimer’s type, and 10 patients with dementia of Alzheimer’s type with extrapyramidal signs. Their results confirmed earlier studies that a cholinergic deficit is present in patients with Alzheimer’s dementia. However, AChE activity did not correlate with the severity of the dementia nor was there any significant change over an 18 month period. They concluded that the usefulness of CSF AChE measurements is limited as a diagnostic marker.
D e m e n t ia
More recently, Navaratnam and associates40 studied CSF obtained at autopsy from patients with clinical dementia, possible dementia, and a control group without dementia. Using isoelectric focusing in polyacrylamide gel, they demonstrated an additional AChE band in 19 of 23 patients with a pathologic diagnosis of Alzheimer’s disease but in none of the 19 control subjects. The extra AChE band was also present in 4 of 8 patients with possible dementia but without the histopathologic criteria for Alzheimer’s disease.
C r e u t z f e l d t -Ja c o b
Creutzfeldt-Jacob (C-J) disease is a rapidly progressive disorder caused by an infectious prion agent. A specific diagnosis can be made only by microscopic examination of brain tissue (spongioform encephalopathy). Early studies suggested that increased levels of CSF neuron-specific enolase (NSE) are present in the early disease phase. In a recent report, Zerr et al41 studied 58 patients with C-J disease and found NSE levels to be significantly higher than in 26 control subjects (median 94.0 ng/mL vs 9.5 ng/mL). Using a cut-off of 35 ng/mL, the test sensitivity was 80 percent and the specificity 92 percent.
Other enzymes that have been studied in the CSF in an attempt to correlate their levels with various disease processes include beta- glucuronidase, adenylate kinase, ribonucle- ase, arginine esterase, and dopamine-beta- hydroxylase.4
Amines and Amino AcidsVarious amines and amino acids have been
measured in the CSF and their levels correlated with a wide variety of CNS disorders (table III).
G l u t a m in e
Central nervous system glutamine is synthesized from ammonia and glutamic acid. Increased glutamine concentrations have been reported in hepatic encephalopathy,42 up to 75 percent of children with Reyes syndrome,43 and in patients with septic encephalopathy.44 Importantly, CSF glutamine reference intervals are method-dependent.4
P o ly am in es
The polyamines consist of spermidine, spermine, and their precursor putrescine. These amines form complexes with polyanionic substances such as deoxyribonucleic acid (DNA) and ribonucleic acid (RNA) as well as with structures and membranes which contain nu-

ADVANCES IN ANALYSIS OF CEREBROSPINAL FLUID 99
Measurement of Cerebrospinal Fluid Amines and Amino Acids in
Central Nervous System Disorders
Amine/ Central NervousAmino Add System Disorder(s)
TABLE III
Glutamine
Polyamines Biogenic amines3
Gamma-amino- butyric acid
Homocarnosine
Reye's syndrome, various encephalopathies Medulloblastoma Organic dementia, schizophrenia, autism, depressive psychoses Huntington's disease, migraine, startle disease
Homocarnosinosis
“Metabolites include 5-hydroxyindoleacetic acid, homovanillic acid, phenylacetic acid, 3-methoxy-4-hydroxyphenylethylene glycol.
cleic acids. Polyamines are widely distributed and numerous studies have linked them to cellular proliferation. As a result, they are reportedly elevated in rapidly growing tissues. For example, Marton and associates45 measured CSF polyamines in children with medulloblastoma. O f the 16 children with this malignancy, 15 had polyamine levels that correlated well with the clinical course. On the other hand, Smith et al46 measured polyamine levels in children with acute leukemia and found them to be of limited value as a screening test for early detection of CNS involvement.
B io g e n ic A m in e s
The CNS biogenic amines include serotonin, phenylethylamine, dopamine and norepinephrine. The CSF has been extensively studied with regards to its concentration of these compounds as well as with their major metabolites, 5-hydroxy-indoleacetic acid (5-HIAA), phenylacetic acid (PA), homovanillic acid (HVA), and 3-methoxy-4-hydroxyphenyl- ethylene glycol (MHPG), respectively. Over
the past quarter of a centuiy, numerous studies have been reported on the role these compounds might play in parkinsonism, Huntingtons chorea, dystonia, and other organic dementias.
In addition, there has been an intensive investigation into the role of the biogenic amines in schizophrenia, affective disorders, manic-depressive psychosis, and autism. This extensive topic has been recently reviewed4 and will not be discussed here except for a more recent publication not included in that review. Here, Cooper and co-workers47 found low concentrations of 5-HIAA in the CSF of schizophrenic patients with suicidal behavior. In this study, 30 schizophrenics in a drug-free state were followed for 11 years during which time 10 of them attempted suicide. These suicide attempters had significantly lower CSF 5-HIAA levels at initial evaluation than the non-attempters. This study provides additional evidence for the probable relationship between suicide and defective serotonin production.
A m in o A c id s
The measurement of CSF amino acids has been greatly facilitated since the introduction of chromatographic techniques, especially liquid chromatography as well as the availability of automated amino acid analyzers. Fishman48 has summarized information regarding the presence of free amino acids in both children and adults. He noted that CSF free amino acids are relatively increased in infants less than 30 days of age but are particularly high in children with febrile convulsions and bacterial meningitis. In addition, CSF amino acids apparently increase with age. Gjessing et al49 reported that CSF amino acid concentration in a group of older individuals (mean age, 70 years) was significantly higher than a group of young adults (mean age, 38 years).
G a m m a -a m in o b u t y r ic A c id
Gamma-aminobutyric acid (GABA) is a major inhibitoiy transmitter in the brain and

100 KNIGHT
spinal cord. Normally, the CSF concentration of this amino acid is low (mean about 150 pmol/mL).50,51 Its concentration in GABA- containing neurons in the basal ganglia is decreased by about 50 percent of normal in patients with Huntingtons disease.50,51 The CSF levels are also decreased in some of these patients.51 These results are consistent with the finding that glutamic acid decarboxylase, the enzyme that catalyzes the synthesis of GABA from glutamic acid, is decreased in Huntingtons disease.51 Decreased GABA levels have also been reported in patients with Alzheimer’s disease.50
Welch and associates52 measured CSF GABA in patients during migraine attacks and compared the results with a group of patients with tension headaches and a control group without headaches. With the analytical method they used, GABA was undetectable in the latter two groups but readily measureable levels were present in all patients with migraine.
The pathophysiology of startle disease (hy- perekplexia), an inherited autosomal dominant disorder, is usually characterized very early in neonatal life either with “stiff baby syndrome” or with a seizure disorder. A recent report53 of an infant with this disorder showed significantly decreased CSF levels of GABA. These authors emphasized that the measurement of CSF GABA is not only helpful in the diagnosis of this rare disorder but that the GABA neurotransmitter system is implicated in its pathogenesis.
Homocarnosinosis is an inherited metabolic disorder of homoeamosine metabolism. It is characterized by spastic paraplegia, progressive mental deterioration, and retinal pigmentation. The CSF levels of homoeamosine, a dipeptide composed of histidine and GABA, are increased in this disorder, averaging about 20 times the normal concentration.54
Since these and other amines and amino acids are not commonly measured, their possible importance is generally unappreciated. However, they are important in our understanding of the pathogenesis of the several CNS disorders.
ProteinsElevation of CSF total protein is probably
the most common single laboratory abnormality in CNS disorders. However, measurement of total protein has very limited clinical value since it is so nonspecific. However, the measurement of specific proteins may be very useful in selected disorders (table IV).
More than 300 different proteins have been detected in CSF using bidirectional electrophoresis: the first dimension is isoelectric focusing and the second is polyacrylamide gel in the presence of sodium dodecyl sulfate. Electrophoresis is followed by highly sensitive silver staining. Using this technique, Harrington et al55 identified four abnormal proteins in the CSF of all patients with Creutzfeldt-Jacob (C-J) disease, a fatal form of dementia caused by an infectious prion agent. Two of these proteins (molecular mass about 40,000 daltons each) were also present in some, although not all, patients with multiple sclerosis (MS), herpes encephalitis, schizophrenia, Parkinson’s disease, and the Guillain-Barre syndrome. They were not present in several other neurological disorders nor in any of the 100 normal control samples. The other two proteins (molecular masses about 26,000 and 29,000 daltons) were also identified in five of the 10 cases of herpes simplex encephalitis but in none of the controls or other CNS disorders.
TABLE IV
Specific Proteins in Central Nervous Disorders
ProteinsCentral Nen/ous
System Disorder(s)
Amyloid beta-protein Alzheimer's diseaseprecursor
26,000-40,000 Creutzfeldt-Jacobdalton proteins disease
Microtubule-associated Alzheimer’s diseasetau
Fibronectin Lymphoblastic, leukemia, bacterial meningitis, AIDS

ADVANCES IN ANALYSIS OF CEREBROSPINAL FLUID 101A l z h e im e r ’s D is e a se
Alzheimer’s disease (AD) is characterized by pathological lesions known as neurofibrillary tangles and senile plaques. The intracellular neurofibrillary tangles are composed principally of microtubule-associated protein tau while the extracellular senile plaques consist primarily of amyloid beta-protein, a fragment of amyloid beta-protein precursor. Several researchers have shown that increased CSF levels of microtubule-associated tau protein might be useful in the diagnosis of AD.56'57 In support of this suggestion, Terajima and associates58 recently reported two probable AD cases in the early stage of disease in which the CSF tau levels were markedly elevated.
A m y l o id B eta - p r o t e in P r e c u r s o r
Cerebrospinal fluid amyloid beta-protein precursor (APP) has also been studied as a possible marker for AD.59,60 These authors used an antibody assay to measure CSF APP levels in 16 healthy controls, 13 patients with probable AD, and 18 patients with non-AD dementia. Their measurements showed that APP levels in AD patients were about 3.5 times lower than both of the other groups. They concluded that in AD there is abnormal processing of the protein that forms amyloid deposits. Similar levels of APP have been reported in patients with hereditary (presenile) AD.61
F ib r o n e c t in
Fibronectin is a large glycoprotein with a molecular mass of about 420,000 daltons. It is present in essentially all body tissues and fluids as well as in the extracellular matrix. Its primary action is in the process of adhesion and phagocytosis.62 In children with acute lymphoblastic leukemia, increased CSF fi- bronectin levels observed at the time of diagnosis were associated with a poor prognosis and subsequent CNS leukemia.63 In addition, Torre et al64 noted increased CSF fibronectin levels in acute bacterial meningitis but normal
levels in viral meningitis. This latter finding could be clinically useful in the early differential diagnosis of these two infectious diseases since they are frequently indistinguishable by other markers. Interestingly, a significant decrease in fibronectin concentrations has been reported in the CSF of patients with AIDS dementia complex.65 These authors suggest that the mechanism for the decreased levels might be due to fibronectin binding to the HIV virus or to viral proteins; alternatively, in some cases it might bind to opportunistic microorganisms.
Transferrin and CSF LeakageTransferrin is an iron-binding glycoprotein
with a molecular mass of about 77,000 daltons. This glycoprotein, which contains four negatively charged sialic acid groups, is synthesized primarily in the liver. In the CSF, two isoforms are present, the major one (beta-1- transferrin) migrating on electrophoresis exactly as in serum. The second isoform (beta-2- transferrin), not present in serum, migrates cathodally to the major isoform. Beta-2-trans- ferrin is formed in the CSF by the action of neuraminidase on beta-l-transferrin. By the use of CSF electrophoresis and immunofixa- tion, both isoforms are readily identified. In this regard, several recent publications have shown that CSF rhinorrhea and otorrhea can be readily diagnosed using immunofixation to demonstrate the presence of both transferrin isoforms.66,67,68 Non-CSF fluids show only a single band.
This technique is, therefore, extremely valuable in verification of CSF leakage in those rare cases of skull fracture in which there is leakage from the nose or ear. The only alternative definitive diagnostic procedure in these cases involves a highly expensive and labor intense radiologic isotopic technique.
Tests for Bleeding Following Negative Computed Tomography
Most cases of significant subarachnoid or other CNS hemorrhage are readily diagnosed
102 KNIGHT
by computed tomography (CT) scans. However, there is a small group of these patients with negative CT scans or whose presentation is unusual. In these cases, various laboratory tests have been suggested to detect visually negative specimens or to differentiate minor brain hemorrhage from the common traumatic tap. In fact, routine spectrophortomet- ric analysis of all CSF samples has been recently proposed in order to detect small cerebral and subdural hematomas, minimal subarachnoid hemorrhage, blood seepage from aneurysms and neoplasms, and in small cerebral infarcts.69 These authors described a highly sensitive spectrophotometric method to detect methemoglobin in trace amounts of hemoglobin mixture (< 0.3 umol/L). They found methemoglobin in 9 percent of 454 patients with cerebrovascular pathology and in 4 percent of 449 patients with other neurological disorders.
Others70 studied a small group of patients with negative CT scans by measuring bilirubin, ferritin, D-dimers, and erythrophages in the CSF of patients suspected of having subarachnoid hemorrhage. They concluded that measurement of neither ferritin nor D-dimer adds significantly to information provided by a CT scan and spectrophotometry.
References1. Marton KI, Gean AD. The spinal tap: a new look at
an old test. Ann Intem Med 1986;104:840-8.2. Position Paper, Health and Public Policy Committee,
American College of Physicians. The diagnostic spinal tap. Ann Intem Med 1986;104:880-5.
3. Hayward RA, Shapiro MF, Oye RK. Laboratory testing on cerebrospinal fluid. A reappraisal. Lancet 1987;1:1-4.
4. Kjeldsberg C, Knight J. Body Fluids, 3rd ed., American Society Clinical Pathologists, Chicago. 1993: 65-157.
5. Laterre EC, Callewaert A, Heremans JF, et al. Electrophoretic morphology of gamma globulins in cerebrospinal fluid of multiple sclerosis and other diseases of the nervous system. Neurology 1970;20:982-90.
6. Link H, Muller R. Immunoglobulins in multiple sclerosis and infections of the nervous system. Arch Neurol 1971;25:326-44.
7. Johnson KP, Arrigo SC, Nelson BJ, et al. Agarose electrophoresis of cerebrospinal fluid in multiple sclerosis. Neurology 1977;27:273-7.
8. Link H, Kostulas V. Utility of isoelectric focusing of cerebrospinal fluid and serum on agarose evaluated for neurological patients. Clin Chem 1983;29:810-5.
9. Lane JR, Bowles KJ, Normansell DE. The detection of oligoclonal IgG bands in unconcentrated cerebrospinal fluid by isoelectric focusing on thin-layer agarose gels and silver staining. Arch Pathol Lab Med 1986;110:26-9.
10. Poser CM, Paty DW, Scheinberg L, et al. New diagnostic criteria for multiple sclerosis: guidelines for research proposals. Ann Neurol 1983;13:227-31.
11. Bentz J. Laboratory investigation of multiple sclerosis. Lab Med 1995;26:393-9.
12. Zeman A, McLean B, Keir G, Sharief M, Thompson E. The significance of serum oligoclonal bands in neurological diseases. J Neurol Neurosurg Psychiatry 1993;56:32-5.
13. Tibbling G, Link H, Ohman S. Principles of albumin and IgG analyses in neurological disorders. I. Establishment of reference values. Scand J Clin Lab Invest 1977;37:385-90.
14. Tourtellotte WW, Potvin AR, Fleming JO, et al. Multiple sclerosis measurement and validation of central nervous system IgG synthesis rate. Neurology 1980;30:240-4.
15. Lauer SJ, Kirchner PA, Camitta BM. Identification of leukemic cells in the cerebrospinal fluid from children with acute lymphoblastic leukemia: advances and dilemmas. Am J Pediatr Hematol Oncol 1989;11:64-73.
16. Hayakawa T, Morimoto K, Ushio Y, et al. Levels of as- troprotein (an astrocyte-specific cerebroprotein) in cerebrospinal fluid of patients with brain tumors. J Neurosurg 1980;52:229-33.
17. Klee GG, Tallman RD, Goellner JR, et al. Elevation of carcinoembryonic antigen in cerebrospinal fluid among patients with meningeal carcinomatosis. Mayo Clin Proc 1986;61:9-13.
18. Twijnstra A, Nooyen WJ, van Zanten AP, et al. Cerebrospinal fluid carcinoembryonic antigen in patients with metastatic and nonmetastatic neurological diseases. Arch Neurol 1986;43:269-72.
19. Mavligit GM, Studkey SE, Cabanillas FF, et al. Diagnosis of leukemia or lymphoma in central nervous system by betaj-microglobulin determination. N Engl J Med 1980;303:718-22.
20. Hallgren R, Terent A, Venge P. Lactoferrin, lysozyme, and ß2-microglobulin levels in cerebrospinal fluid. Inflammation 1982;6:291-304.
21. Allen JC, Nisselbaum J, Epstein C, et al. Alpha-feto- protein and human chorionic gonadotropin determination in cerebrospinal fluid: an aid to the diagnosis and management of intracranial germ-cell tumors. J Neurosurg 1979;57:368-74.
22. Bagshawe KD, Harland S. Immunodiagnosis and monitoring of gonadotrophin-producing metastases in the central nervous system. Cancer 1976;38:112-8.
23. Zandman-Goddard G, Matzner Y, Konijn AM, et al. Cerebrospinal fluid ferritin in malignant CNS involvement. Cancer 1986;58:1146-9.
24. Knight JA, Dudek SM, Haymond RE. Early (chemical) diagnosis of bacterial meningitis: cerebrospinal fluid glucose, lactate, and lactate dehydrogenase compared. Clin Chem 1981;27:1431^.
25. Feldman WE. Cerebrospinal fluid lactic acid dehy

ADVANCES IN ANALYSIS OF CEREBROSPINAL FLUID 103drogenase activity: Levels in untreated and partially antibiotic-treated meningitis. Am J Dis Child 1975; 129:77-80.
26. Fleisher M, Wasserstrom WR, Schold SC, et al. Lactic dehydrogenase isoenzymes in the cerebrospinal fluid of patients with systemic cancer. Cancer 1981;47:2654-9.
27. Lampl Y, Paniri Y, Eshel Y, et al. Cerebrospinal fluid lactate dehydrogenase levels in early stroke and transient ischemic attacks. Stroke 1990;21:854-7.
28. Donnan GA, Zapf P, Doyle AE, et al. CSF enzymes in lacunar and cortical stroke. Stroke 1983;14:266-9.
29. Savory J, Brody JP. Measurement and diagnostic value of cerebrospinal fluid enzymes. Ann Clin Lab Sci 1979;9:68-79.
30. Florez G, Cabeza A, Gonzalez JM, et al. Changes in serum and cerebrospinal fluid enzyme activity after head injury. Acta Neurochir 1976;35:3-13.
31. Chandler WL, Clayson KJ, Longstreth WT Jr, Fine JS. Creatine kinase isoenzymes in human cerebrospinal fluid and brain. Clin Chem 1984;30:1804-6.
32. Chandler WL, Clayson KJ, Longstreth WT Jr, Fine JS. Mitochondrial and BB isoenzymes of creatine kinase in cerebrospinal fluid from patients with hypoxic-ischemic brain damage. Am J Clin Pathol 1986;86:533-7.
33. Chandler WL. Cerebrospinal fluid creatine kinase. Chicago IL, American Society of Clinical Pathologists Check Sample 1990;30:CC90-8.
34. Newman J, Cacatian A, Josephson AS, et al. Spinal fluid lysozyme in the diagnosis of central nervous system tumours. Lancet 1974;1:756-9.
35. Mason DY, Robert-Thomson P. Spinal fluid lysozyme in diagnosis of central nervous system tumours. Lancet 1974;2:952-3.
36. Blake J, Berman P. The use of adenosine deaminase in the diagnosis of tubersclerosis. S Afr Med J 1982; 62:19-22.
37. Mann MD, Macfarlane CM, Verburg CJ, et al. The bromide partition test and CSF adenosine deaminase activity in the diagnosis of tuberculous meningitis in children. S Afr Med J 1982;62:432-3.
38. Donald PR, Malan C, van der Walt A, et al. The simultaneous determination of cerebrospinal fluid and plasma adenosine deaminase activity as a diagnostic aid in tuberculous meningitis. S Afr Med J 1986;69:505-7.
39. Atack JR, May C, Kay JA, et al. Cerebrospinal fluid cholinesterase in aging and in dementia of the Alzheimer’s type. Ann Neurol 1988;23:161-7.
40. Navaratnam DS, Priddle JD, McDonald B, et al. Anomalous molecular form of acetylcholinesterase in cerebrospinal fluid in histologically diagnosed Alzheimer’s disease. Lancet 1991;337:447-50.
41. Zerr I, Bodemer M, Racker S, Grosche S, Poser S, Kretzschmar HA, Weber T. Cerebrospinal fluid concentration of neuron-specific enolase in diagnosis of Creutzfeldt-Jacob disease. Lancet 1995;345:1609-10.
42. Hourani B, Hamlin EM, Reynolds TB. Cerebrospinal fluid glutamine as a measure of hepatic encephalopathy. Arch Intern Med 1971;172:1033-6.
43. Glasgow AM, Dhiensiri K. Improved assay for spinal fluid glutamine, and values for children with Reyes syndrome. Clin Chem 1974;20:642-4.
44. Mizock BA, Rackow EC, Burke GS. Elevated cere
brospinal fluid glutamine in septic encephalopathy. J Clin Gastroenterol 1989;11:362-3.
45. Marton LJ, Heby O, Levin VA, et al. The relationship of polyamines in cerebrospinal fluid to the presence of central nervous system tumors. Cancer Res 1976; 36:973-7.
46. Smith J, Lee S, Sabio H, et al. Cerebrospinal fluid polyamines in childhood leukemia. Ann Clin Lab Sci 1984;14:225-31.
47. Cooper SJ, Kelly CB, King DJ. 5-hydroxyindoleacetic acid in cerebrospinal fluid and prediction of suicidal behaviour in schizophrenia. Lancet 1992;340:940-1.
48. Fishman RA. Cerebrospinal Fluid in Diseases of the Nervous System. Philadelphia: WB Saunders, 1980: 168-252.
49. Gjessing LR, Gjesdahl P, Dietrichson P, et al. Free amino acids in the cerebrospinal fluid in old age and in Parkinson’s disease. Eur Neurol 1974;12:33-7.
50. Enna SJ, Stem LZ, Wastek GJ, et al. Cerebrospinal fluid fS-aminobutyric acid variations in neurological disorders. Arch Neurol 1977;34:683-5.
51. Manyam NVB, Hare TA, Katz L, et al. Huntington’s disease. Arch Neurol 1978;35:728-30.
52. Welch KMA, Chabi E, Bartosh K, et al. Cerebrospinal fluid P-aminobutyric acid levels in migraine. Br Med J 1975;3:515-7.
53. Dubowitz LMS, Bouza H, Hird MF, Jaeken J. Low cerebrospinal fluid concentration of free gamma- aminobutyric acid in startle disease. Lancet 1992;340: 80-1.
54. Sjaastad O, Berstad J, Gjesdahl P, et al. Homocarnosi- nosis, II. A familial metabolic disorder associated with spastic paraplegia, progressive mental deficiency, and retinal pigmentation. Acta Neurol Scand 1976;53: 275-90.
55. Harrington MG, Merrill CR, Asher DM, et al. Abnormal proteins in the cerebrospinal fluid of patients with Creutzfeldt-Jacob disease. N Engl J Med 1986; 315:279-83.
56. Arai H, Terajima T, Miura M, et al. Tau in cerebrospinal fluid: A potential diagnostic marker of Alzheimer’s disease. Ann Neurol 1995;35:649-52.
57. Vigo-Pelfrey C, Seubert P, Barbour R, et al. Elevations of microtubule-associated protein tau in the cerebrospinal fluid of patients with Alzheimer’s disease. Neurology 1995;45:788-93.
58. Terajima M, Arai H, Itabashi S, Hyuchi M, Zhu C, Kosaka Y, Nakagawa T, Sasaki H. Elevated cerebrospinal fluid tau levels: Implications for the early diagnosis of Alzheimer’s disease. J Am Geriatr Soc 1996;44:1012-3.
59. Van Nostrand WE, Wagner SL, Shankle WR, et al. Decreased levels of soluble amyloid beta-protein precursor in cerebrospinal fluid of live Alzheimer’s patients. Proc Natl Acad Sci USA 1992;89:2251-5.
60. Erickson D. Doomsday diagnostic? Sci Amer 1992;267:120.
61. Farlow M, Ghetti B, Benson MD, Farrow JS, van Nostra.'*cl WE, Wagner SL. Low cerebrospinal-fluid concentrations of soluble amyloid beta-protein precursor in hereditary Alzheimer’s disease. Lancet 1992;340:453-4.
62. Ruoslahti E, Engvall E, Hayman EG. Fibronectin: current concepts of its stmcture and functions. Coll Res 1981;1:95-128.

104 KNIGHT
63. Rautonen J, Koskiniemi M, Siimes MA, et al. Elevated cerebrospinal fluid fibronectin concentration indicates poor prognosis in children with acute lymphoblastic leukemia. Int J Cancer 1989;43:32-7.
64. Torre D, Zeroli C, Issi M, et al. Cerebrospinal fluid concentration of fibronectin in meningitis. J Clin Pathol 1991;44:783-4.
65. Torre D, Zeroli C, Ferrario G, Bonetta G, Fiori GP, Martegani R. Cerebrospinal fluid concentration of fibronectin in HIV-1 infection and central nervous system disorders. J Clin Pathol 1993;46:1039^11.
66. Iijala K, Suonpaa J, Laurent B. Identification of CSF leakage by immunofixation. Arch Otolaryngal 1979; 105:447-8.
67. Rouah E, Rogers BB, Buffone GJ. Transferrin analysis by immunofixation as an aid in the diagnosis of
cerebrospinal fluid otorrhea. Arch Pathol Lab Med 1987;111:756-7.
68. Zaret DL, Morrison N, Gulbranson R, Keren DF. Immunofixation to quantify ß2-transferrin in cerebrospinal fluid to detect leakage of cerebrospinal fluid from skull injury. Clin Chem 1992;38:1909-12.
69. Trbojevic-Cepe M, Vogrinc Z, Brinar V. Diagnostic significance of methemoglobin determination in colorless cerebrospinal fluid. Clin Chem 1992;38: 1404-8.
70. Page KB, Howell SJ, Smith CML, Dabbs DJW, Malia RG, Porter NR, Thickett KJ, Wilkinson GM. Bilirubin, ferritin, D-dimers and erythrophages in the cerebrospinal fluid of patients with suspected subarachnoid haemorrhage but negative computed tomography scans. J Clin Pathol 1994;47:986-9.