advancing innovative therapies for neurological diseases
TRANSCRIPT

NYSE: BHVN© 2018 Biohaven Pharmaceuticals. All rights reserved.
November 01, 2018
Advancing Innovative Therapies for Neurological Diseases
Biohaven Investor Presentation
Disclaimer
This presentation contains forward-looking statements, including: statements about our plans to develop and commercialize our product candidates, our planned clinical trials for our rimegepant, BHV3500, troriluzole, BHV0223, BHV5000 and BHV3241 development programs, the timing of the availability of data from our clinical trials, the timing of our planned regulatory filings, the timing of and our ability to obtain and maintain regulatory approvals for our product candidates and the clinical utility of our product candidates, alone and as compared to other treatment options. These statements involve substantial known and unknown risks, uncertainties and other factors that may cause our actual results, levels of activity, performance or achievements to be materially different from the information expressed or implied by these forward-looking statements. We may not actually achieve the plans, intentions or expectations disclosed in our forward-looking statements, and you should not place undue reliance on our forward-looking statements. Actual results or events could differ materially from the plans, intentions and expectations disclosed in the forward-looking statements we make. The forward-looking statements in this presentation represent our views as of the date of this presentation. We anticipate that subsequent events and developments will cause our views to change. However, while we may elect to update these forward-looking statements at some point in the future, we have no current intention of doing so except to the extent required by applicable law. You should, therefore, not rely on these forward-looking statements as representing our views as of any date subsequent to the date of this presentation. For further information regarding these risks, uncertainties and other factors you should read the “Risk Factors” section of the Company’s Quarterly Report on Form 10-Q filed with the Securities and Exchange Commission (the ”SEC”) on August 14, 2018 and the Company’s other periodic reports filed with the SEC.
This presentation also contains market data and other statistical information that are based on independent industry publications, reports by market research firms or published independent sources. Some market data and statistical information are also based on the Company's good faith estimates, which are derived from management's knowledge of its industry and such independent sources referred to above. While the Company is not aware of any misstatements regarding the market and industry data presented herein, such data involve risks and uncertainties and are subject to change based on various factors.
NOVEMBER 2018 ADVANCING INNOVATIVE THERAPIES FOR NEUROLOGICAL DISEASES 2
NOVEMBER 2018 ADVANCING INNOVATIVE THERAPIES FOR NEUROLOGICAL DISEASES 3
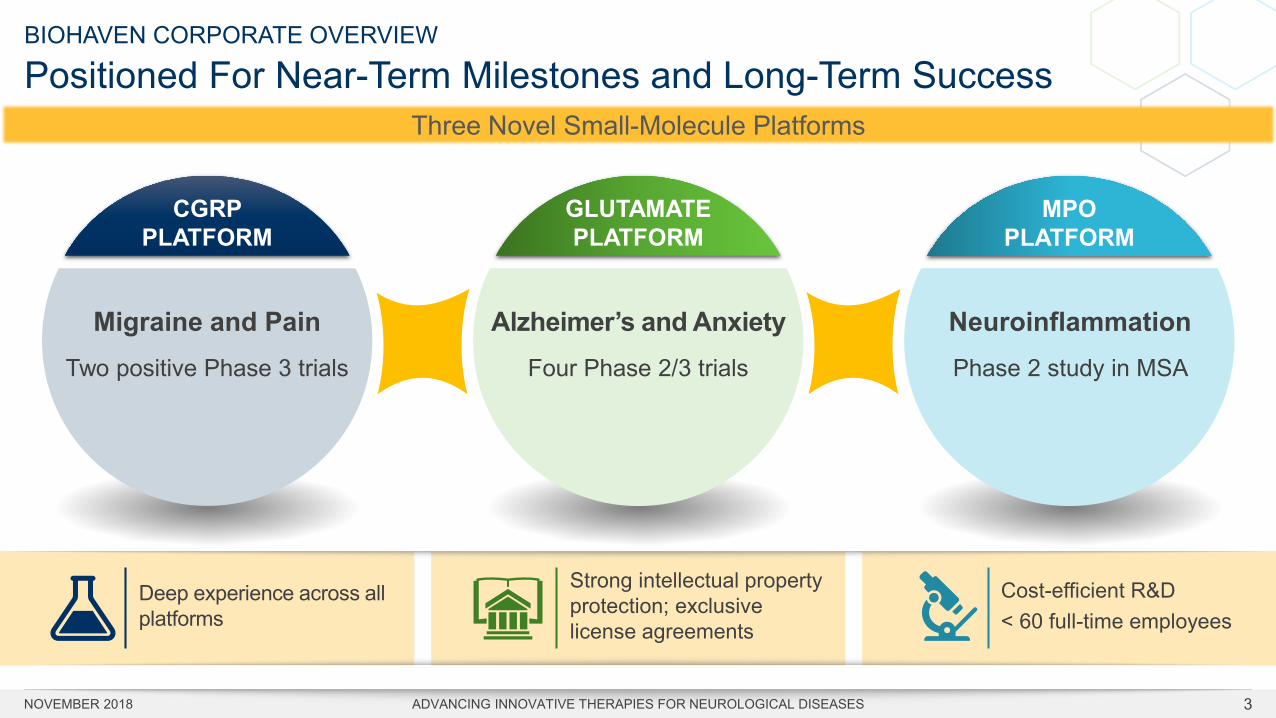
BIOHAVEN CORPORATE OVERVIEW
Positioned For Near-Term Milestones and Long-Term Success
CGRP PLATFORM
Three Novel Small-Molecule Platforms
GLUTAMATEPLATFORM
MPOPLATFORM
Migraine and Pain Two positive Phase 3 trials
Alzheimer’s and AnxietyFour Phase 2/3 trials
NeuroinflammationPhase 2 study in MSA
Strong intellectual property protection; exclusive license agreements
Deep experience across all platforms
Cost-efficient R&D< 60 full-time employees
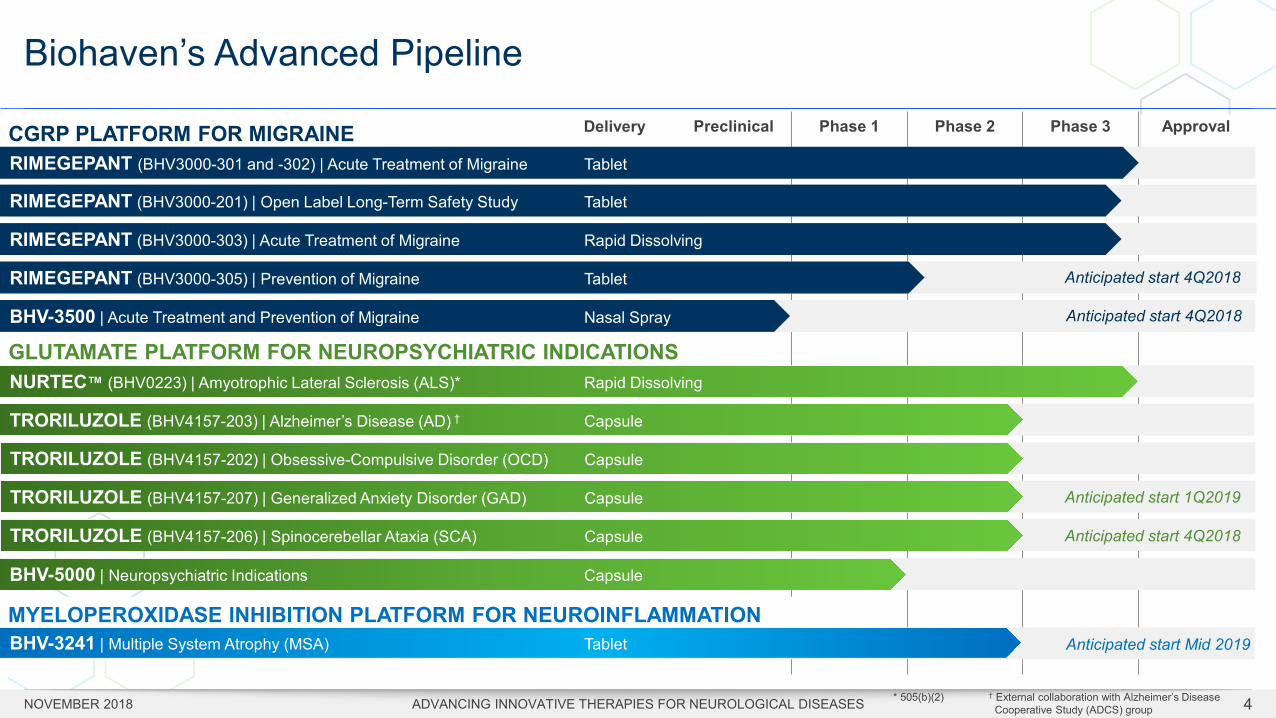
Biohaven’s Advanced Pipeline
NOVEMBER 2018 ADVANCING INNOVATIVE THERAPIES FOR NEUROLOGICAL DISEASES 4
Preclinical Phase 1 Phase 2 Phase 3 Approval
RIMEGEPANT (BHV3000-301 and -302) | Acute Treatment of Migraine Tablet
RIMEGEPANT (BHV3000-303) | Acute Treatment of Migraine Rapid Dissolving
Data inRIMEGEPANT (BHV3000-201) | Open Label Long-Term Safety Study Tablet
RIMEGEPANT (BHV3000-305) | Prevention of Migraine Tablet
NURTEC™ (BHV0223) | Amyotrophic Lateral Sclerosis (ALS)* Rapid Dissolving
TRORILUZOLE (BHV4157-203) | Alzheimer’s Disease (AD) † Capsule
TRORILUZOLE (BHV4157-202) | Obsessive-Compulsive Disorder (OCD) Capsule
TRORILUZOLE (BHV4157-206) | Spinocerebellar Ataxia (SCA) Capsule
BHV-5000 | Neuropsychiatric Indications Capsule
CGRP PLATFORM FOR MIGRAINE
GLUTAMATE PLATFORM FOR NEUROPSYCHIATRIC INDICATIONS
Delivery
BHV-3500 | Acute Treatment and Prevention of Migraine Nasal Spray
TRORILUZOLE (BHV4157-207) | Generalized Anxiety Disorder (GAD) Capsule Anticipated start 1Q2019
Anticipated start 4Q2018
Anticipated start 4Q2018
Anticipated start 4Q2018
MYELOPEROXIDASE INHIBITION PLATFORM FOR NEUROINFLAMMATION BHV-3241 | Multiple System Atrophy (MSA) Tablet
* 505(b)(2) † External collaboration with Alzheimer’s Disease Cooperative Study (ADCS) group
Anticipated start Mid 2019

CGRP PLATFORMTherapies for Migraine
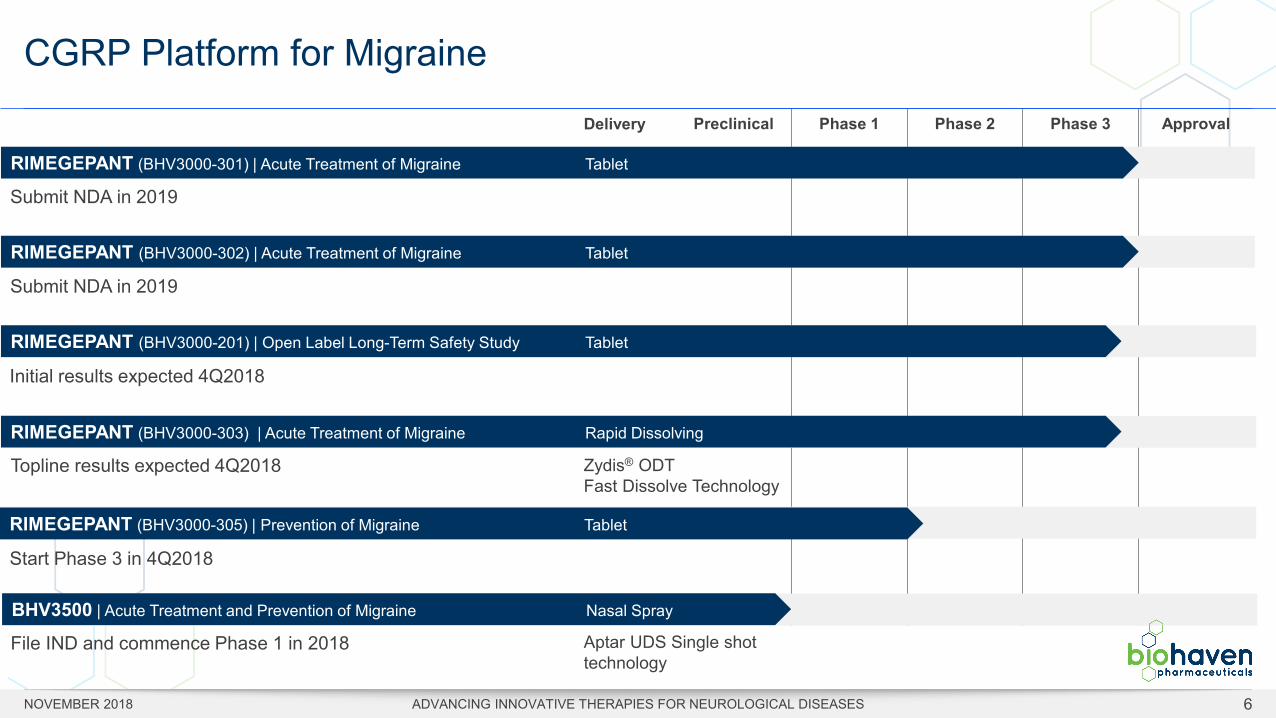
CGRP Platform for Migraine
NOVEMBER 2018 ADVANCING INNOVATIVE THERAPIES FOR NEUROLOGICAL DISEASES 6
Preclinical Phase 1 Phase 2 Phase 3 Approval
Data in
RIMEGEPANT (BHV3000-301) | Acute Treatment of Migraine Tablet
RIMEGEPANT (BHV3000-303) | Acute Treatment of Migraine Rapid Dissolving
RIMEGEPANT (BHV3000-302) | Acute Treatment of Migraine Tablet
RIMEGEPANT (BHV3000-201) | Open Label Long-Term Safety Study Tablet
RIMEGEPANT (BHV3000-305) | Prevention of Migraine Tablet
Delivery
Submit NDA in 2019
Submit NDA in 2019
Initial results expected 4Q2018
Topline results expected 4Q2018
Start Phase 3 in 4Q2018
Zydis® ODT Fast Dissolve Technology
BHV3500 | Acute Treatment and Prevention of Migraine Nasal Spray
File IND and commence Phase 1 in 2018 Aptar UDS Single shot technology
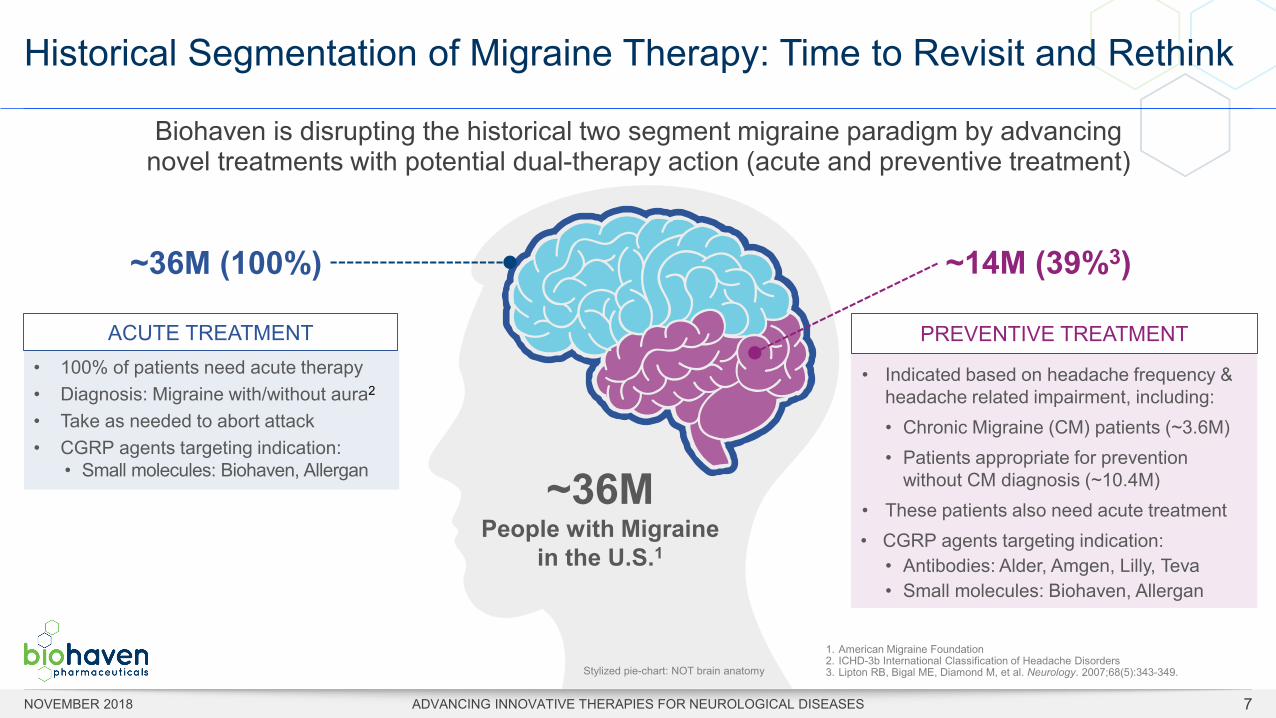
Historical Segmentation of Migraine Therapy: Time to Revisit and Rethink
ADVANCING INNOVATIVE THERAPIES FOR NEUROLOGICAL DISEASES
PREVENTIVE TREATMENT
• Indicated based on headache frequency & headache related impairment, including:• Chronic Migraine (CM) patients (~3.6M) • Patients appropriate for prevention
without CM diagnosis (~10.4M) • These patients also need acute treatment• CGRP agents targeting indication:
• Antibodies: Alder, Amgen, Lilly, Teva• Small molecules: Biohaven, Allergan
~36M People with Migraine
in the U.S.1
1. American Migraine Foundation2. ICHD-3b International Classification of Headache Disorders3. Lipton RB, Bigal ME, Diamond M, et al. Neurology. 2007;68(5):343-349.
~14M (39%3)~36M (100%)
ACUTE TREATMENT• 100% of patients need acute therapy• Diagnosis: Migraine with/without aura2
• Take as needed to abort attack• CGRP agents targeting indication:
• Small molecules: Biohaven, Allergan
Biohaven is disrupting the historical two segment migraine paradigm by advancing novel treatments with potential dual-therapy action (acute and preventive treatment)
Stylized pie-chart: NOT brain anatomy
NOVEMBER 2018 7
Multiple Formulations, Meeting Patient Needsfrom Acute Treatment to Prevention of Migraine
NOVEMBER 2018 ADVANCING INNOVATIVE THERAPIES FOR NEUROLOGICAL DISEASES 8
NOJECTION™ CGRP Drug Delivery Platform
* Exclusive World-Wide License with Catalent for use of Zydis® Fast Dissolve Technology in our migraine product candidates** Aptar Pharma Unit-Dose System (UDS) single shot nasal technology
Oral Rapid Dissolving* Intranasal**
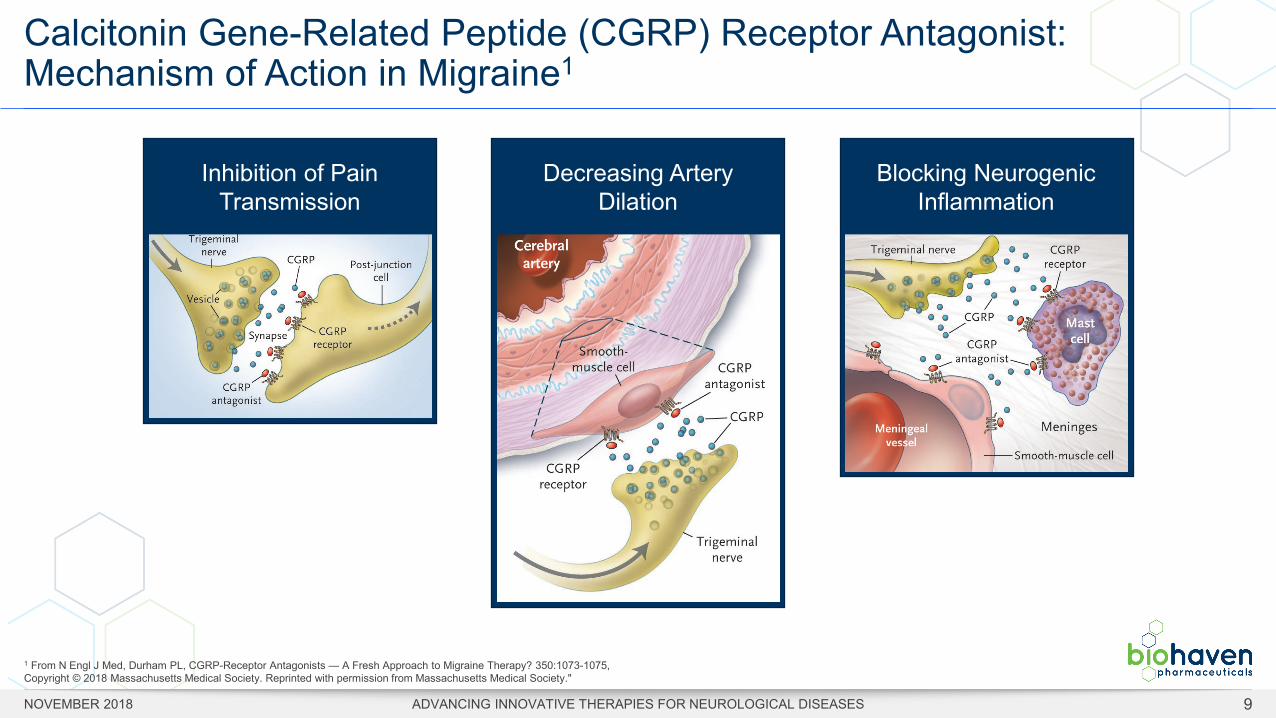
Calcitonin Gene-Related Peptide (CGRP) Receptor Antagonist: Mechanism of Action in Migraine1
Inhibition of Pain Transmission
Decreasing Artery Dilation
Blocking Neurogenic Inflammation
NOVEMBER 2018 ADVANCING INNOVATIVE THERAPIES FOR NEUROLOGICAL DISEASES 9
1 From N Engl J Med, Durham PL, CGRP-Receptor Antagonists — A Fresh Approach to Migraine Therapy? 350:1073-1075, Copyright © 2018 Massachusetts Medical Society. Reprinted with permission from Massachusetts Medical Society."
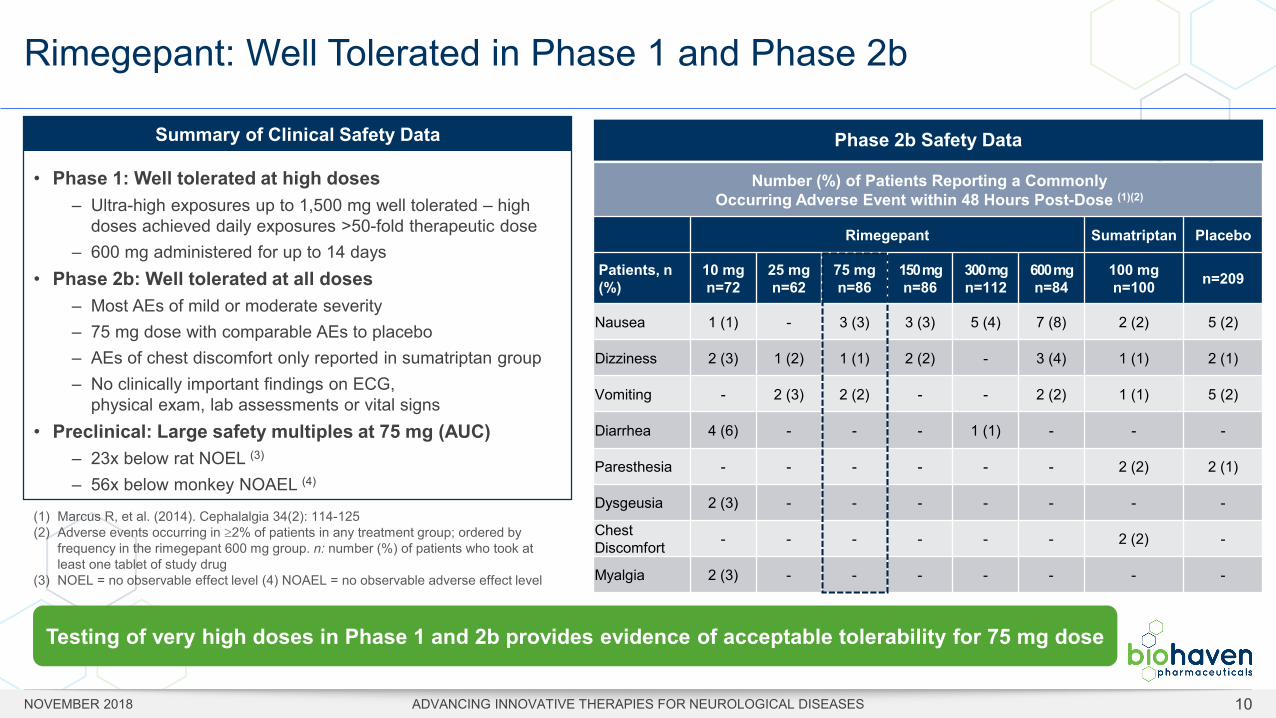
Rimegepant: Well Tolerated in Phase 1 and Phase 2b
10
Testing of very high doses in Phase 1 and 2b provides evidence of acceptable tolerability for 75 mg dose
Phase 2b Safety Data
• Phase 1: Well tolerated at high doses– Ultra-high exposures up to 1,500 mg well tolerated – high
doses achieved daily exposures >50-fold therapeutic dose– 600 mg administered for up to 14 days
• Phase 2b: Well tolerated at all doses– Most AEs of mild or moderate severity– 75 mg dose with comparable AEs to placebo– AEs of chest discomfort only reported in sumatriptan group– No clinically important findings on ECG,
physical exam, lab assessments or vital signs• Preclinical: Large safety multiples at 75 mg (AUC)
– 23x below rat NOEL (3)
– 56x below monkey NOAEL (4)
Number (%) of Patients Reporting a Commonly Occurring Adverse Event within 48 Hours Post-Dose (1)(2)
Rimegepant Sumatriptan Placebo
Patients, n (%)
10 mg n=72
25 mg n=62
75 mg n=86
150 mg n=86
300 mg n=112
600 mg n=84
100 mg n=100 n=209
Nausea 1 (1) - 3 (3) 3 (3) 5 (4) 7 (8) 2 (2) 5 (2)
Dizziness 2 (3) 1 (2) 1 (1) 2 (2) - 3 (4) 1 (1) 2 (1)
Vomiting - 2 (3) 2 (2) - - 2 (2) 1 (1) 5 (2)
Diarrhea 4 (6) - - - 1 (1) - - -
Paresthesia - - - - - - 2 (2) 2 (1)
Dysgeusia 2 (3) - - - - - - -
Chest Discomfort - - - - - - 2 (2) -
Myalgia 2 (3) - - - - - - -
(1) Marcus R, et al. (2014). Cephalalgia 34(2): 114-125(2) Adverse events occurring in ≥2% of patients in any treatment group; ordered by
frequency in the rimegepant 600 mg group. n: number (%) of patients who took at least one tablet of study drug
(3) NOEL = no observable effect level (4) NOAEL = no observable adverse effect level
Summary of Clinical Safety Data
NOVEMBER 2018 ADVANCING INNOVATIVE THERAPIES FOR NEUROLOGICAL DISEASES
Rimegepant: Comprehensive and Durable Treatment Effect Observed in Phase 2b
0
25
50
75
100
Placebo 10 25 75 150 300 6000
25
50
75
100
Placebo 10 25 75 150 300 600
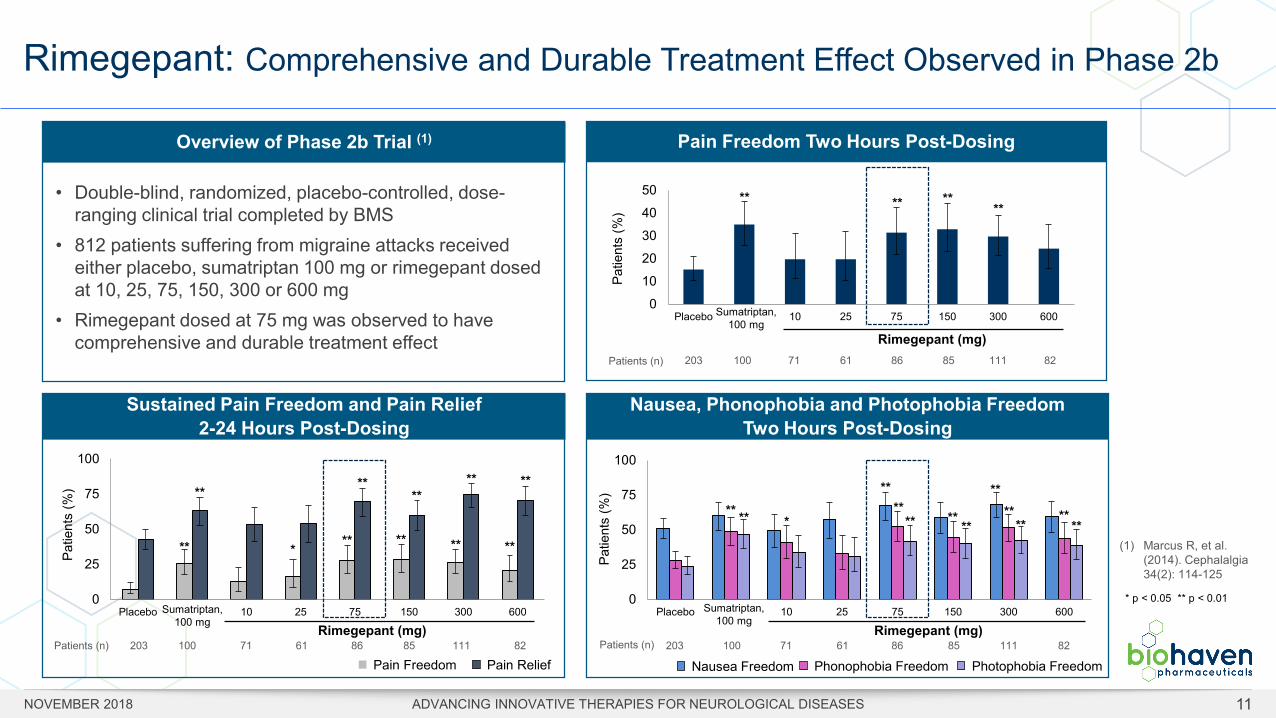
Overview of Phase 2b Trial (1)
• Double-blind, randomized, placebo-controlled, dose-ranging clinical trial completed by BMS
• 812 patients suffering from migraine attacks received either placebo, sumatriptan 100 mg or rimegepant dosed at 10, 25, 75, 150, 300 or 600 mg
• Rimegepant dosed at 75 mg was observed to have comprehensive and durable treatment effect
203 61 86 85 111 82100 71Patients (n)Rimegepant (mg)
**
Sustained Pain Freedom and Pain Relief 2-24 Hours Post-Dosing
**
**
**
**
**
****
**
**
*
**
Nausea, Phonophobia and Photophobia Freedom Two Hours Post-Dosing
203 61 86 85 111 82100 71Patients (n)
** ****
** ****
****
****
**
Patie
nts
(%)
Rimegepant (mg)203 61 86 85 111 82100 71Patients (n)
Pain Freedom Two Hours Post-Dosing
** **** **
Sumatriptan, 100 mg
Sumatriptan, 100 mg
Sumatriptan, 100 mg
Rimegepant (mg)
(1) Marcus R, et al. (2014). Cephalalgia 34(2): 114-125
*
* p < 0.05 ** p < 0.01
0
10
20
30
40
50
Placebo 10 25 75 150 300 600
Patie
nts
(%)
Pain Freedom Pain Relief
Patie
nts
(%)
Nausea Freedom Phonophobia Freedom Photophobia Freedom
11NOVEMBER 2018 ADVANCING INNOVATIVE THERAPIES FOR NEUROLOGICAL DISEASES
RIMEGEPANT (BHV-3000) PHASE 3 HIGHLIGHTS
Rimegepant Demonstrates Comprehensive and Durable Efficacy across Two Pivotal Phase 3 Trials with a Single Dose
NOVEMBER 2018 ADVANCING INNOVATIVE THERAPIES FOR NEUROLOGICAL DISEASES 12
• Primary endpoints achieved in two pivotal Phase 3 trials• Pain freedom at two hours• Freedom from most bothersome symptom (MBS) at two hours
• Clinically important drug benefit across multiple outcome measures• Majority of patients achieved pain relief within two hours (speed of onset)• Sustained efficacy out to 48 hours on multiple measures (durable benefit)• High proportion of patients achieving normal function• Low use of rescue meds
• Placebo-like safety and tolerability• Safety profile similar to placebo including liver function tests• Adverse events profile similar to placebo and favorable compared to historical triptan experience
• Consistent results across endpoints and efficacy trials
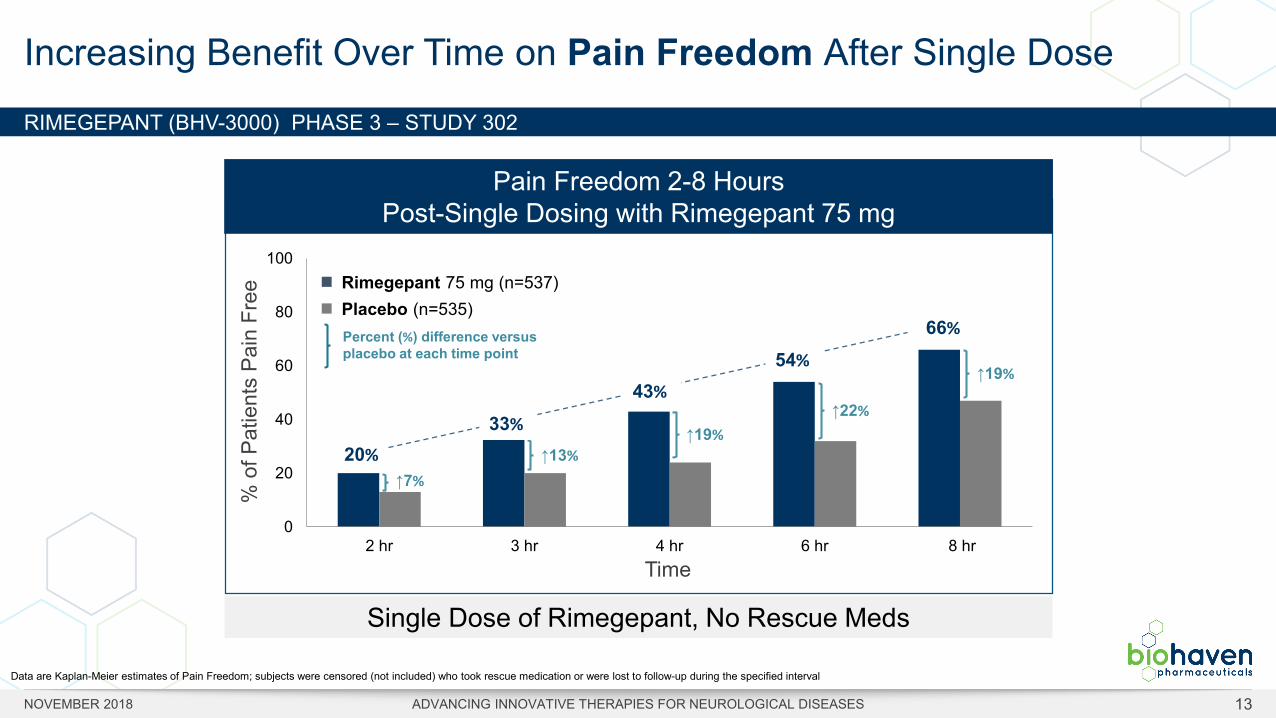
RIMEGEPANT (BHV-3000) PHASE 3 – STUDY 302
Increasing Benefit Over Time on Pain Freedom After Single Dose
NOVEMBER 2018 ADVANCING INNOVATIVE THERAPIES FOR NEUROLOGICAL DISEASES 13
Single Dose of Rimegepant, No Rescue Meds
0
20
40
60
80
100
2 hr 3 hr 4 hr 6 hr 8 hr
% o
f Pat
ient
s Pa
in F
ree
Pain Freedom 2-8 HoursPost-Single Dosing with Rimegepant 75 mg
Time
Rimegepant 75 mg (n=537)Placebo (n=535)
20%
66%
33%
43%
54%
Data are Kaplan-Meier estimates of Pain Freedom; subjects were censored (not included) who took rescue medication or were lost to follow-up during the specified interval
Single Dose of Rimegepant, No Rescue Meds
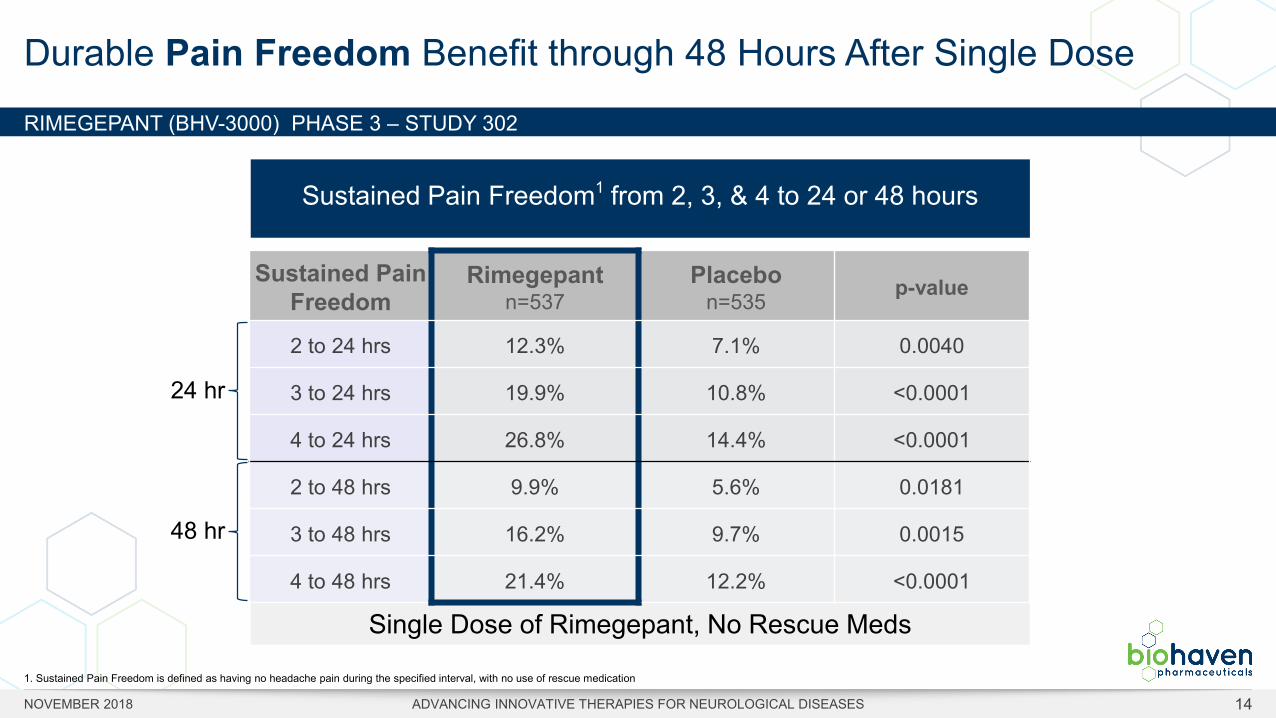
RIMEGEPANT (BHV-3000) PHASE 3 – STUDY 302
Durable Pain Freedom Benefit through 48 Hours After Single Dose
Sustained Pain Freedom
Rimegepant n=537
Placebo n=535 p-value
2 to 24 hrs 12.3% 7.1% 0.0040
3 to 24 hrs 19.9% 10.8% <0.0001
4 to 24 hrs 26.8% 14.4% <0.0001
2 to 48 hrs 9.9% 5.6% 0.0181
3 to 48 hrs 16.2% 9.7% 0.0015
4 to 48 hrs 21.4% 12.2% <0.0001
Sustained Pain Freedom1 from 2, 3, & 4 to 24 or 48 hours
24 hr
48 hr
NOVEMBER 2018 ADVANCING INNOVATIVE THERAPIES FOR NEUROLOGICAL DISEASES 14
1. Sustained Pain Freedom is defined as having no headache pain during the specified interval, with no use of rescue medication
RIMEGEPANT (BHV-3000) PHASE 3 – STUDY 302
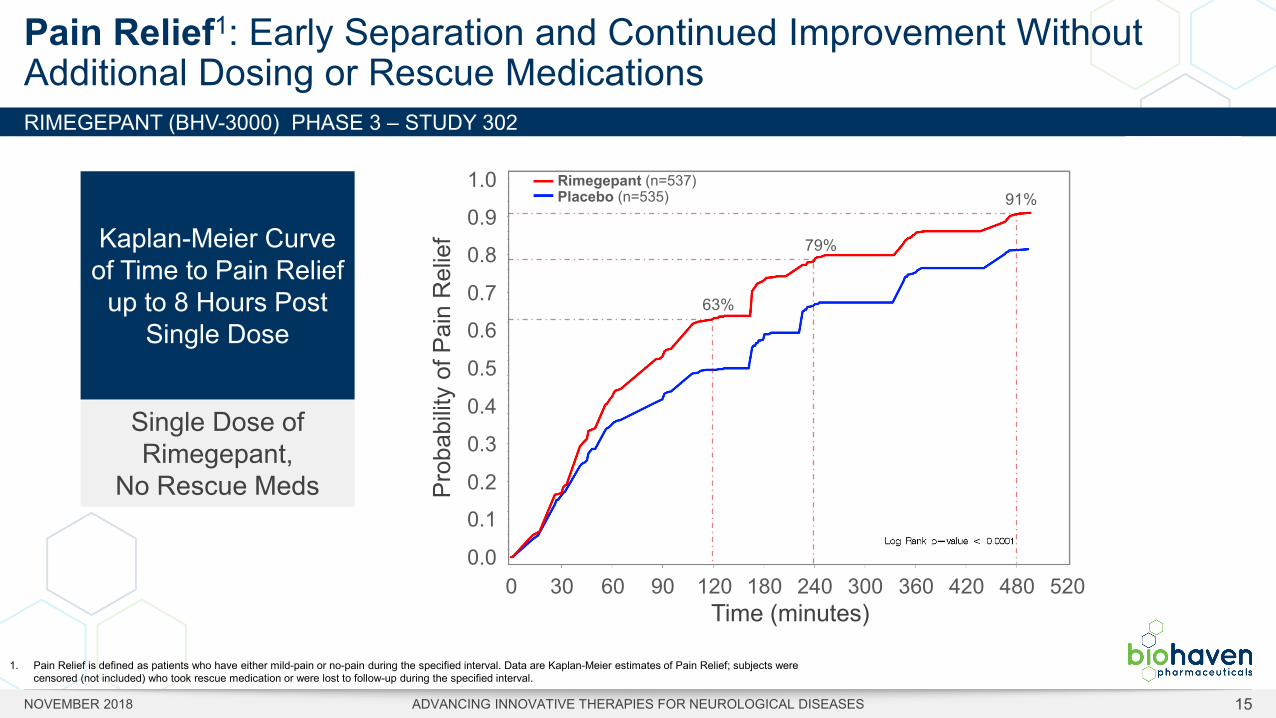
Pain Relief1: Early Separation and Continued Improvement Without Additional Dosing or Rescue Medications
Prob
abilit
y of
Pai
n R
elie
f
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0.00 30 60 90 120 180 240 300 360 420 480 520
Time (minutes)
Rimegepant (n=537)Placebo (n=535)
63%
79%
91%
Kaplan-Meier Curve of Time to Pain Relief
up to 8 Hours Post Single Dose
Single Dose of Rimegepant,
No Rescue Meds
NOVEMBER 2018 ADVANCING INNOVATIVE THERAPIES FOR NEUROLOGICAL DISEASES 15
1. Pain Relief is defined as patients who have either mild-pain or no-pain during the specified interval. Data are Kaplan-Meier estimates of Pain Relief; subjects were censored (not included) who took rescue medication or were lost to follow-up during the specified interval.
Single Dose of Rimegepant, No Rescue Meds
RIMEGEPANT (BHV-3000) PHASE 3 – STUDY 302
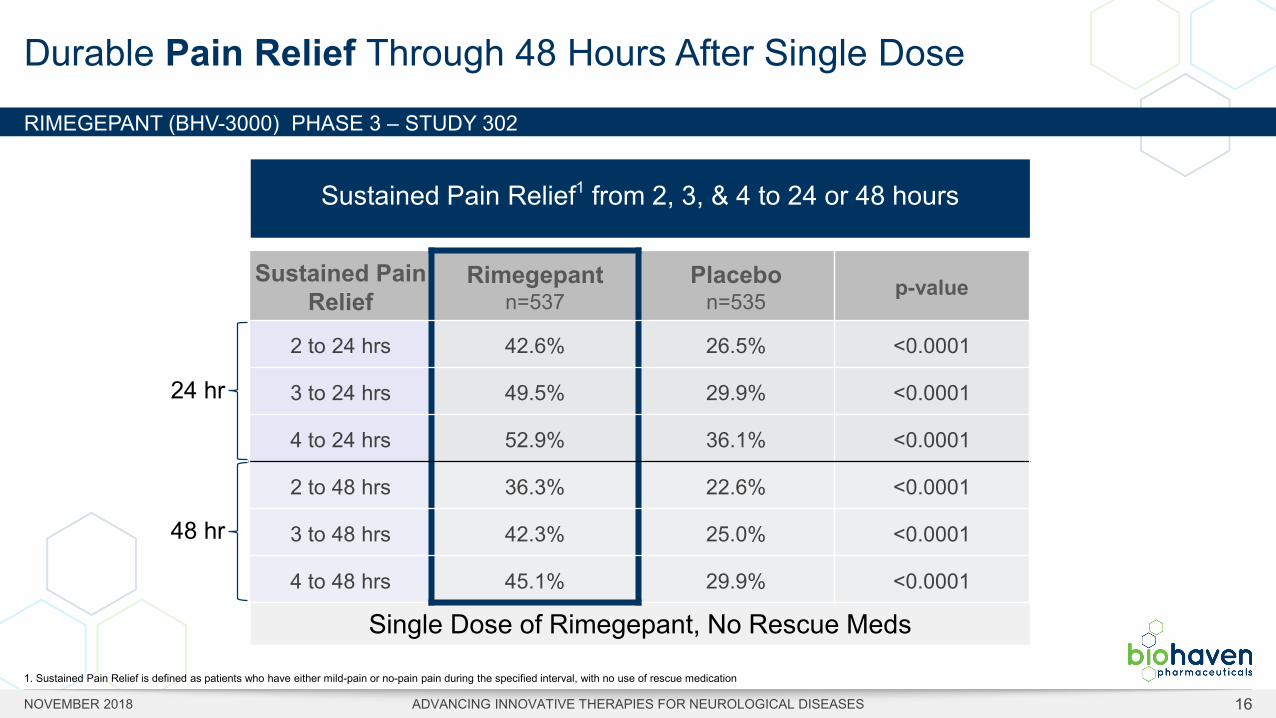
Durable Pain Relief Through 48 Hours After Single Dose
Sustained Pain Relief
Rimegepant n=537
Placebo n=535 p-value
2 to 24 hrs 42.6% 26.5% <0.0001
3 to 24 hrs 49.5% 29.9% <0.0001
4 to 24 hrs 52.9% 36.1% <0.0001
2 to 48 hrs 36.3% 22.6% <0.0001
3 to 48 hrs 42.3% 25.0% <0.0001
4 to 48 hrs 45.1% 29.9% <0.0001
Sustained Pain Relief1 from 2, 3, & 4 to 24 or 48 hours
24 hr
48 hr
NOVEMBER 2018 ADVANCING INNOVATIVE THERAPIES FOR NEUROLOGICAL DISEASES 16
1. Sustained Pain Relief is defined as patients who have either mild-pain or no-pain pain during the specified interval, with no use of rescue medication
RIMEGEPANT (BHV-3000) PHASE 3 – STUDY 302
NOVEMBER 2018 ADVANCING INNOVATIVE THERAPIES FOR NEUROLOGICAL DISEASES 17
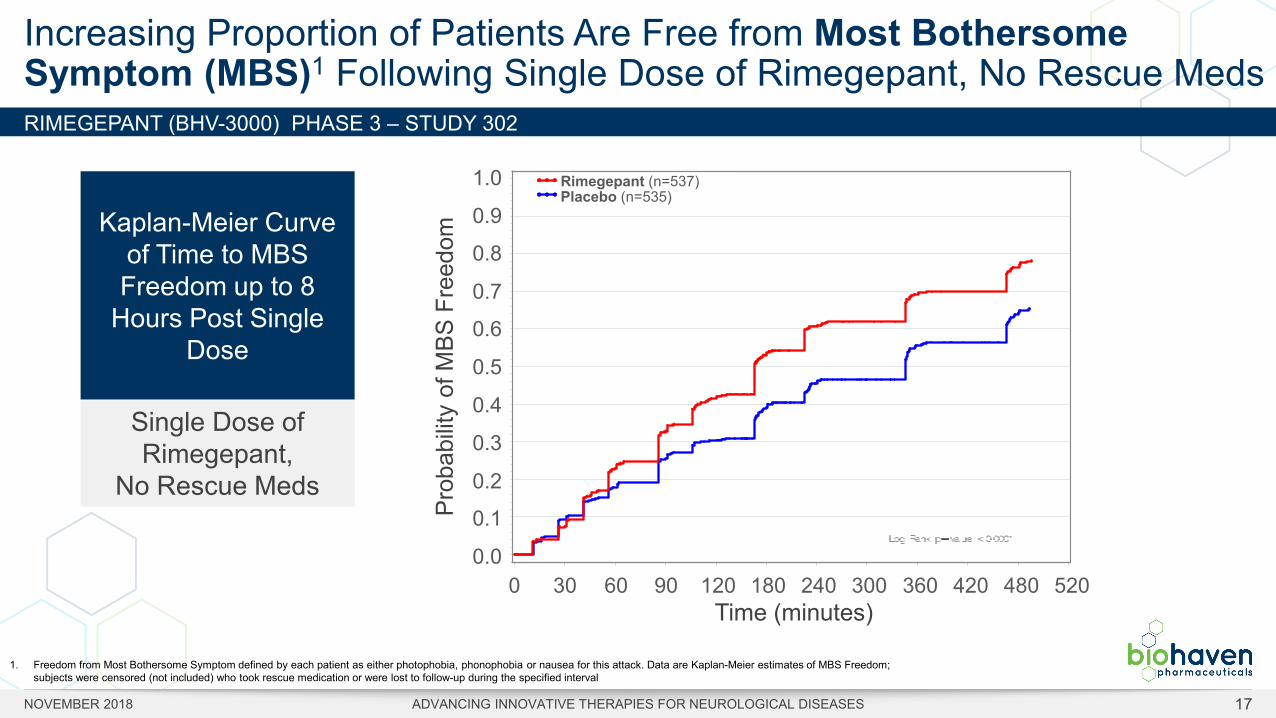
Increasing Proportion of Patients Are Free from Most Bothersome Symptom (MBS)1 Following Single Dose of Rimegepant, No Rescue Meds
Prob
abilit
y of
MBS
Fre
edom
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0.00 30 60 90 120 180 240 300 360 420 480 520
Time (minutes)
Rimegepant (n=537)Placebo (n=535)
Kaplan-Meier Curve of Time to MBS Freedom up to 8
Hours Post Single Dose
Single Dose of Rimegepant,
No Rescue Meds
1. Freedom from Most Bothersome Symptom defined by each patient as either photophobia, phonophobia or nausea for this attack. Data are Kaplan-Meier estimates of MBS Freedom; subjects were censored (not included) who took rescue medication or were lost to follow-up during the specified interval
RIMEGEPANT (BHV-3000) PHASE 3 – STUDY 302
NOVEMBER 2018 ADVANCING INNOVATIVE THERAPIES FOR NEUROLOGICAL DISEASES 18
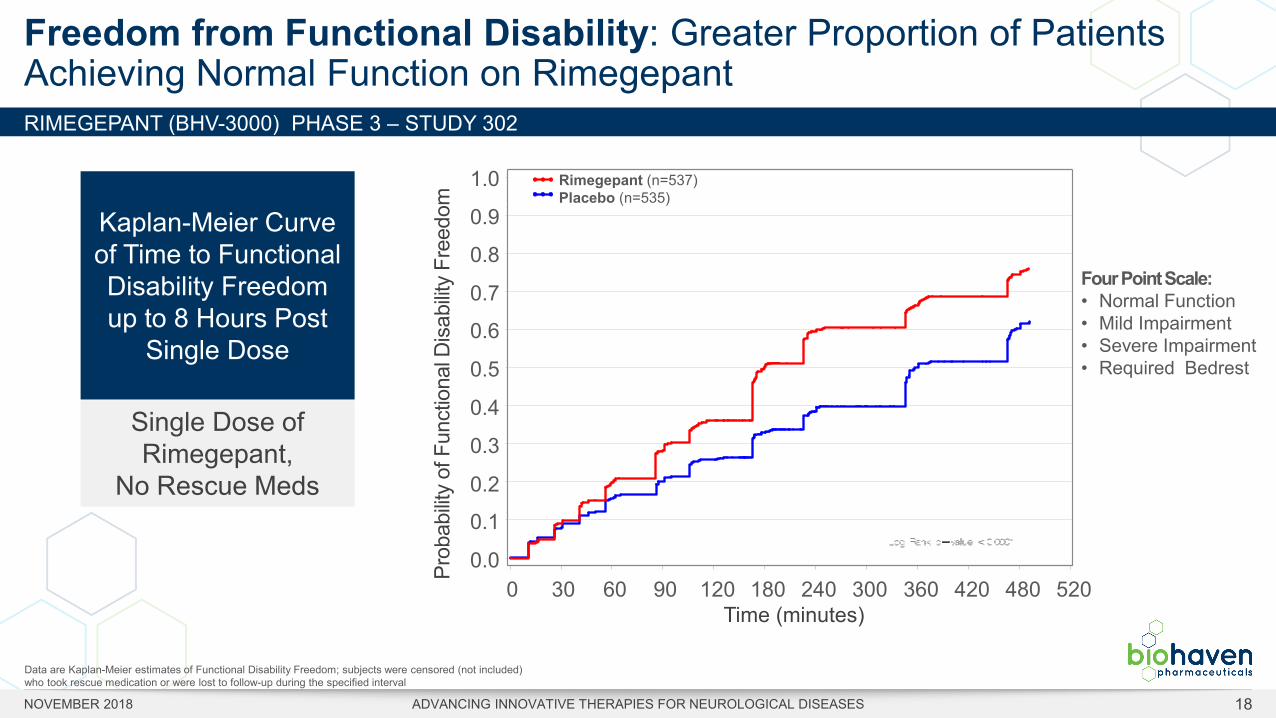
Freedom from Functional Disability: Greater Proportion of Patients Achieving Normal Function on Rimegepant
Data are Kaplan-Meier estimates of Functional Disability Freedom; subjects were censored (not included) who took rescue medication or were lost to follow-up during the specified interval
Four Point Scale: • Normal Function• Mild Impairment • Severe Impairment • Required Bedrest
Prob
abilit
y of
Fun
ctio
nal D
isab
ility
Free
dom
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0.00 30 60 90 120 180 240 300 360 420 480 520
Time (minutes)
Kaplan-Meier Curve of Time to Functional Disability Freedom up to 8 Hours Post
Single Dose
Single Dose of Rimegepant,
No Rescue Meds
Rimegepant (n=537)Placebo (n=535)
RIMEGEPANT (BHV-3000) PHASE 3 – STUDY 302
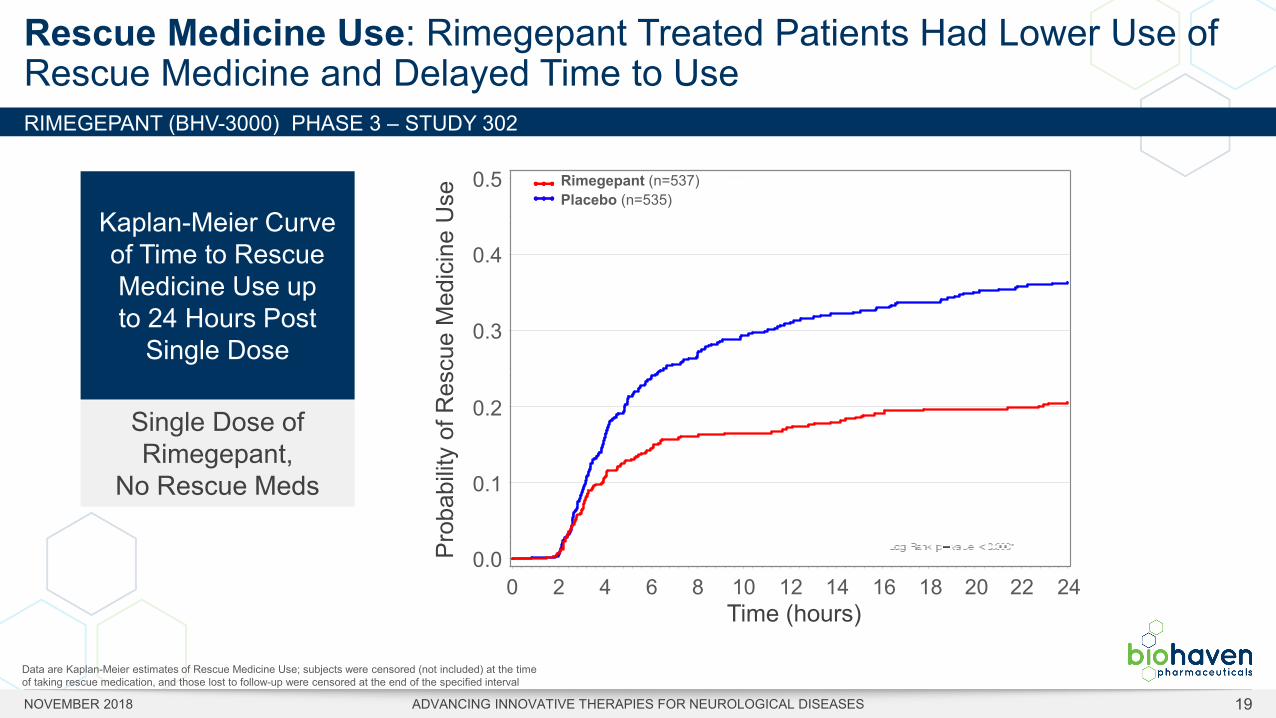
Rescue Medicine Use: Rimegepant Treated Patients Had Lower Use of Rescue Medicine and Delayed Time to Use
Data are Kaplan-Meier estimates of Rescue Medicine Use; subjects were censored (not included) at the time of taking rescue medication, and those lost to follow-up were censored at the end of the specified interval
Prob
abilit
y of
Res
cue
Med
icin
e U
se
0.5
0.4
0.3
0.2
0.1
0.00 2 4 6 8 10 12 14 16 18 20 24
Time (hours)
Rimegepant (n=537)Placebo (n=535)
22
Kaplan-Meier Curve of Time to Rescue Medicine Use up to 24 Hours Post
Single Dose
Single Dose of Rimegepant,
No Rescue Meds
NOVEMBER 2018 ADVANCING INNOVATIVE THERAPIES FOR NEUROLOGICAL DISEASES 19
RIMEGEPANT (BHV-3000) PHASE 3 – STUDY 302
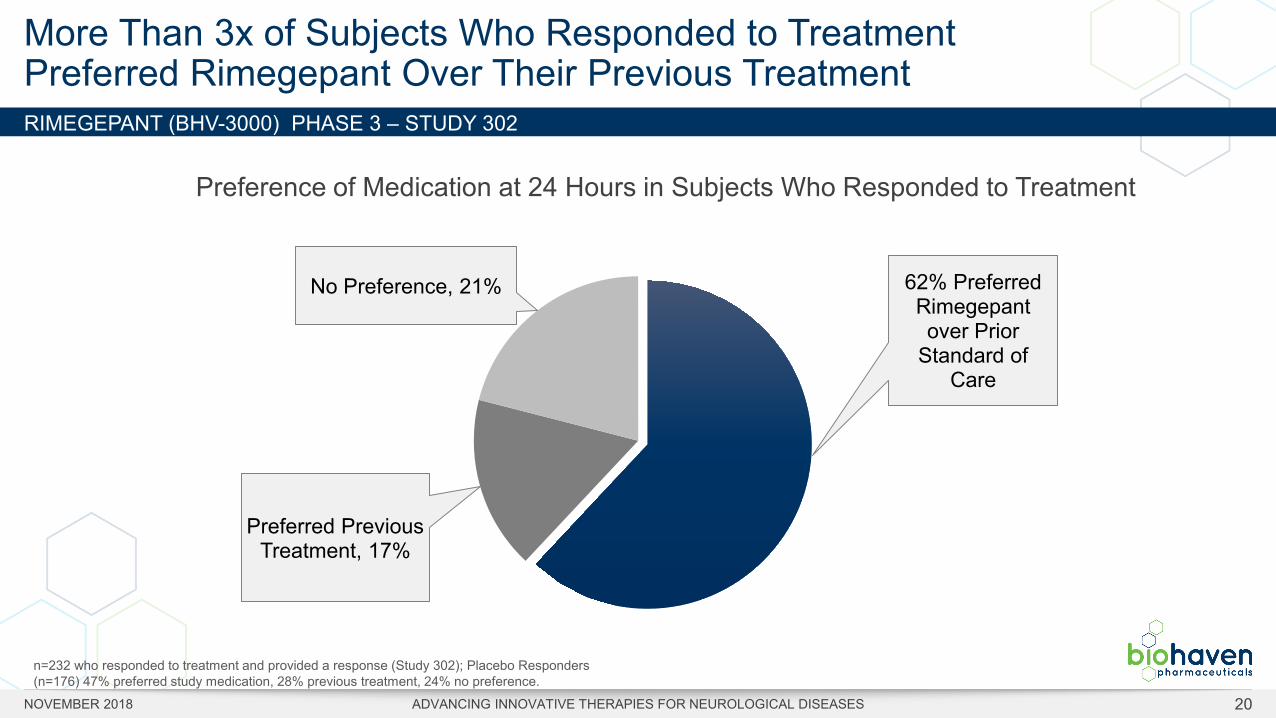
More Than 3x of Subjects Who Responded to TreatmentPreferred Rimegepant Over Their Previous Treatment
62% Preferred Rimegepant over Prior
Standard of Care
Preferred Previous Treatment, 17%
No Preference, 21%
n=232 who responded to treatment and provided a response (Study 302); Placebo Responders (n=176) 47% preferred study medication, 28% previous treatment, 24% no preference.
NOVEMBER 2018 ADVANCING INNOVATIVE THERAPIES FOR NEUROLOGICAL DISEASES 20
Preference of Medication at 24 Hours in Subjects Who Responded to Treatment
RIMEGEPANT (BHV-3000) PHASE 3 – STUDY 301 & 302
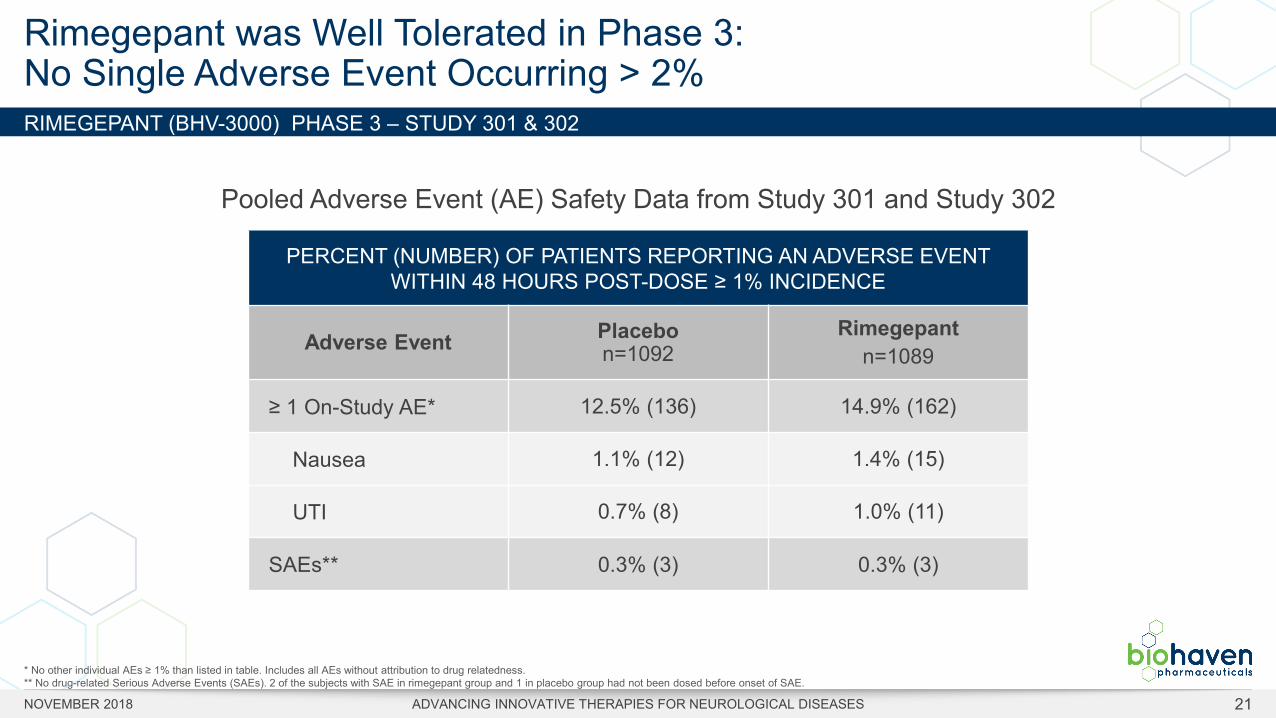
Rimegepant was Well Tolerated in Phase 3: No Single Adverse Event Occurring > 2%
PERCENT (NUMBER) OF PATIENTS REPORTING AN ADVERSE EVENT WITHIN 48 HOURS POST-DOSE ≥ 1% INCIDENCE
Adverse Event Placebon=1092
Rimegepantn=1089
≥ 1 On-Study AE* 12.5% (136) 14.9% (162)
Nausea 1.1% (12) 1.4% (15)
UTI 0.7% (8) 1.0% (11)
SAEs** 0.3% (3) 0.3% (3)
* No other individual AEs ≥ 1% than listed in table. Includes all AEs without attribution to drug relatedness. ** No drug-related Serious Adverse Events (SAEs). 2 of the subjects with SAE in rimegepant group and 1 in placebo group had not been dosed before onset of SAE.
Pooled Adverse Event (AE) Safety Data from Study 301 and Study 302
NOVEMBER 2018 ADVANCING INNOVATIVE THERAPIES FOR NEUROLOGICAL DISEASES 21
RIMEGEPANT (BHV-3000) PHASE 3 – STUDY 301 & 302
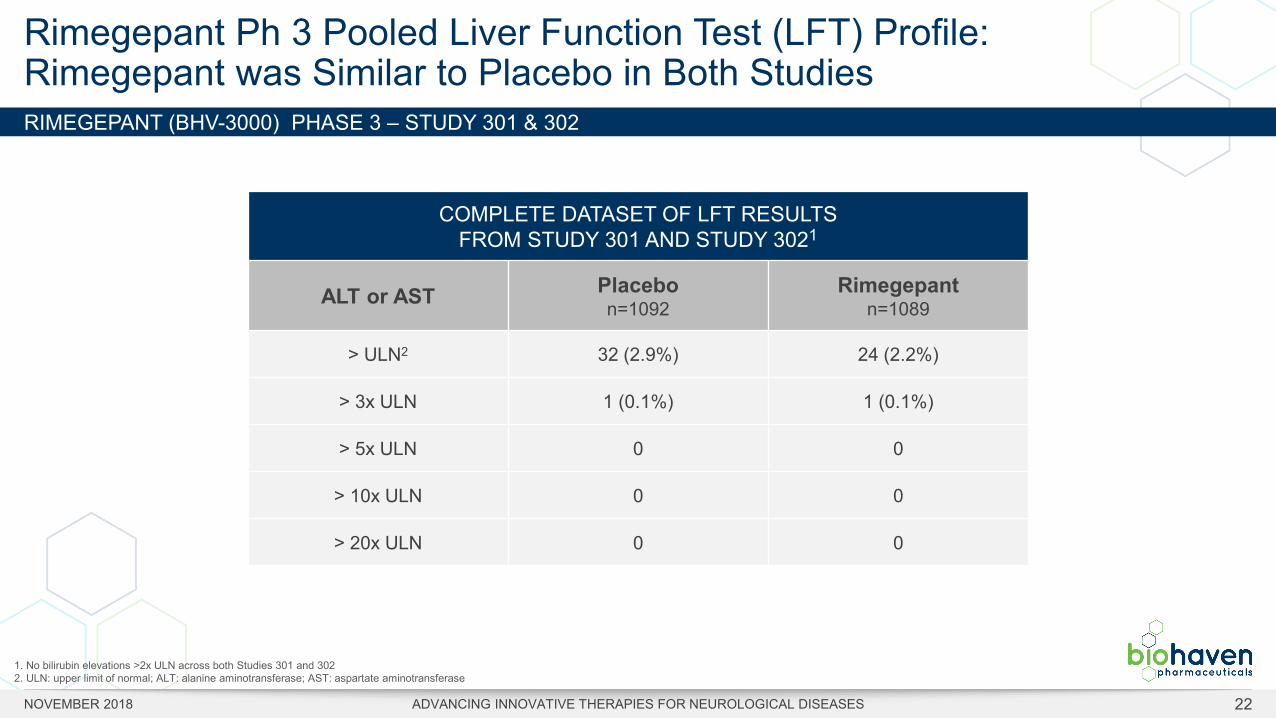
Rimegepant Ph 3 Pooled Liver Function Test (LFT) Profile: Rimegepant was Similar to Placebo in Both Studies
COMPLETE DATASET OF LFT RESULTSFROM STUDY 301 AND STUDY 3021
ALT or AST Placebo n=1092
Rimegepant n=1089
> ULN2 32 (2.9%) 24 (2.2%)
> 3x ULN 1 (0.1%) 1 (0.1%)
> 5x ULN 0 0
> 10x ULN 0 0
> 20x ULN 0 0
1. No bilirubin elevations >2x ULN across both Studies 301 and 3022. ULN: upper limit of normal; ALT: alanine aminotransferase; AST: aspartate aminotransferase
NOVEMBER 2018 ADVANCING INNOVATIVE THERAPIES FOR NEUROLOGICAL DISEASES 22
RIMEGEPANT (BHV-3000) PHASE 3 – STUDY 301 & 302
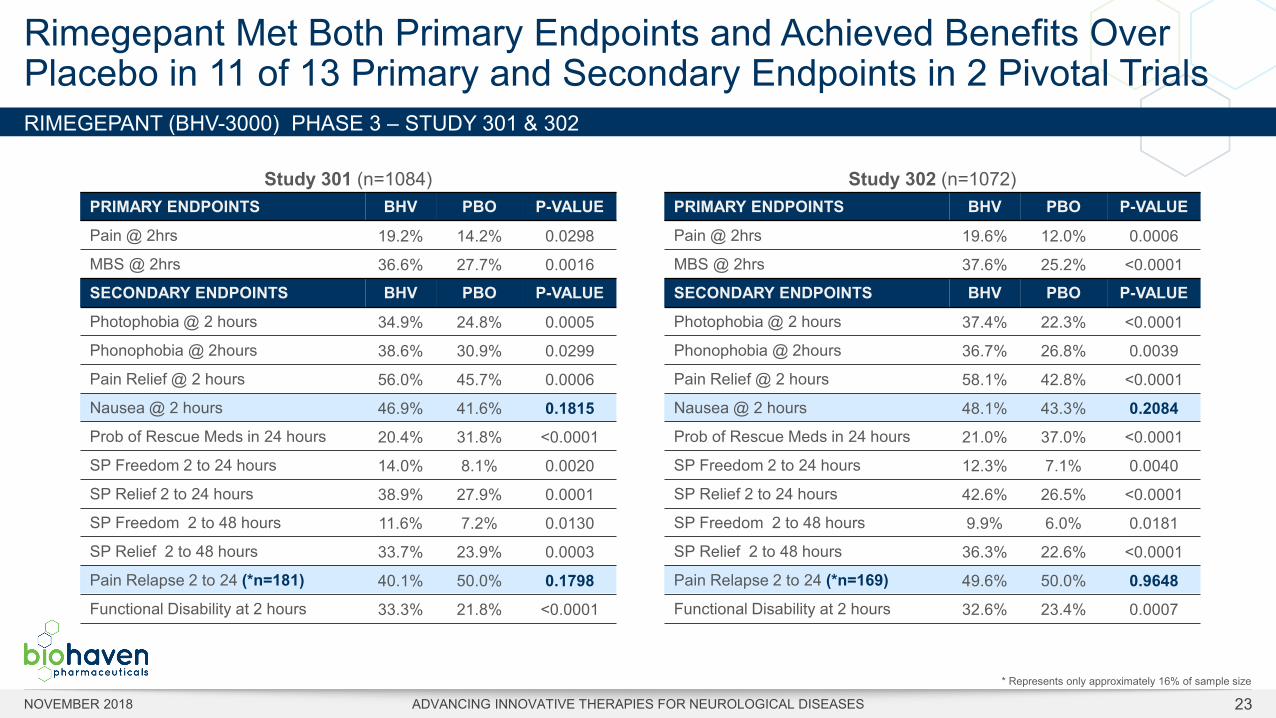
Rimegepant Met Both Primary Endpoints and Achieved Benefits Over Placebo in 11 of 13 Primary and Secondary Endpoints in 2 Pivotal Trials
Study 301 (n=1084)PRIMARY ENDPOINTS BHV PBO P-VALUE
Pain @ 2hrs 19.2% 14.2% 0.0298
MBS @ 2hrs 36.6% 27.7% 0.0016
SECONDARY ENDPOINTS BHV PBO P-VALUE
Photophobia @ 2 hours 34.9% 24.8% 0.0005
Phonophobia @ 2hours 38.6% 30.9% 0.0299
Pain Relief @ 2 hours 56.0% 45.7% 0.0006
Nausea @ 2 hours 46.9% 41.6% 0.1815Prob of Rescue Meds in 24 hours 20.4% 31.8% <0.0001
SP Freedom 2 to 24 hours 14.0% 8.1% 0.0020
SP Relief 2 to 24 hours 38.9% 27.9% 0.0001
SP Freedom 2 to 48 hours 11.6% 7.2% 0.0130
SP Relief 2 to 48 hours 33.7% 23.9% 0.0003
Pain Relapse 2 to 24 (*n=181) 40.1% 50.0% 0.1798Functional Disability at 2 hours 33.3% 21.8% <0.0001
Study 302 (n=1072)PRIMARY ENDPOINTS BHV PBO P-VALUE
Pain @ 2hrs 19.6% 12.0% 0.0006
MBS @ 2hrs 37.6% 25.2% <0.0001
SECONDARY ENDPOINTS BHV PBO P-VALUE
Photophobia @ 2 hours 37.4% 22.3% <0.0001
Phonophobia @ 2hours 36.7% 26.8% 0.0039
Pain Relief @ 2 hours 58.1% 42.8% <0.0001
Nausea @ 2 hours 48.1% 43.3% 0.2084Prob of Rescue Meds in 24 hours 21.0% 37.0% <0.0001
SP Freedom 2 to 24 hours 12.3% 7.1% 0.0040
SP Relief 2 to 24 hours 42.6% 26.5% <0.0001
SP Freedom 2 to 48 hours 9.9% 6.0% 0.0181
SP Relief 2 to 48 hours 36.3% 22.6% <0.0001
Pain Relapse 2 to 24 (*n=169) 49.6% 50.0% 0.9648Functional Disability at 2 hours 32.6% 23.4% 0.0007
* Represents only approximately 16% of sample size
NOVEMBER 2018 ADVANCING INNOVATIVE THERAPIES FOR NEUROLOGICAL DISEASES 23
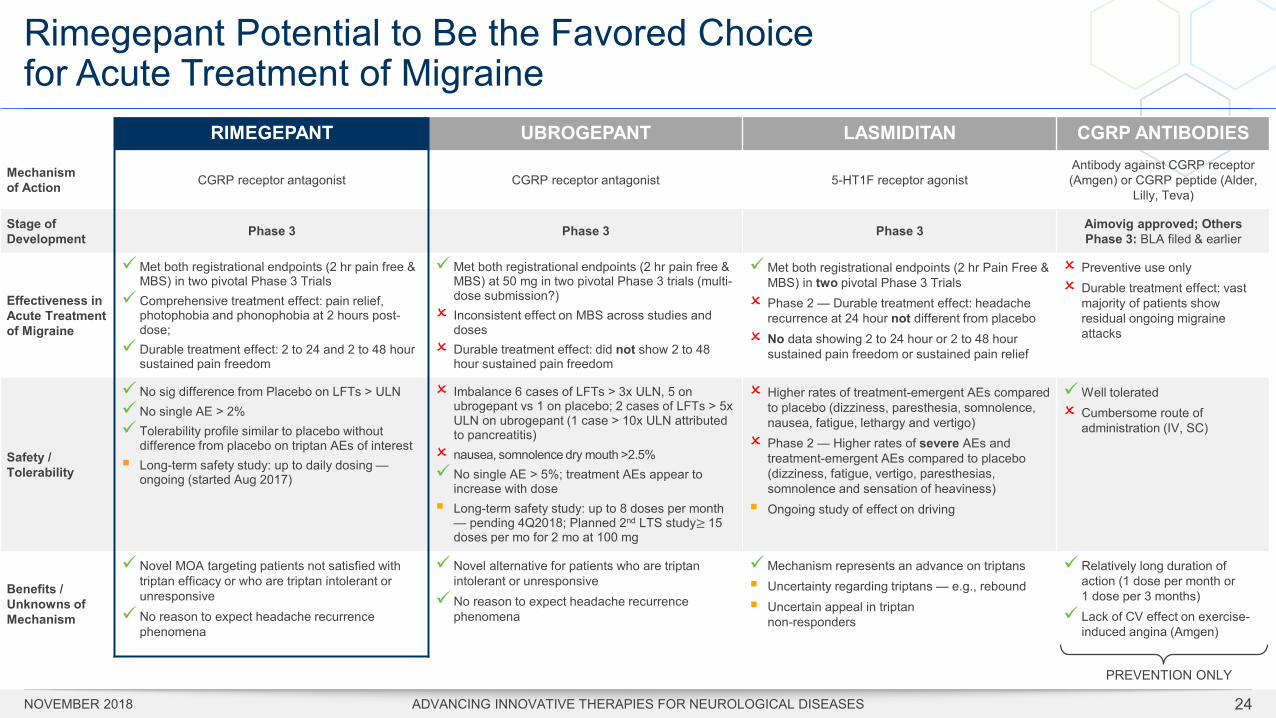
Rimegepant Potential to Be the Favored Choice for Acute Treatment of Migraine
NOVEMBER 2018 ADVANCING INNOVATIVE THERAPIES FOR NEUROLOGICAL DISEASES 24
RIMEGEPANT UBROGEPANT LASMIDITAN CGRP ANTIBODIES
Mechanism of Action CGRP receptor antagonist CGRP receptor antagonist 5-HT1F receptor agonist
Antibody against CGRP receptor (Amgen) or CGRP peptide (Alder,
Lilly, Teva)
Stage of Development Phase 3 Phase 3 Phase 3 Aimovig approved; Others
Phase 3: BLA filed & earlier
Effectiveness in Acute Treatment of Migraine
Met both registrational endpoints (2 hr pain free & MBS) in two pivotal Phase 3 Trials
Comprehensive treatment effect: pain relief, photophobia and phonophobia at 2 hours post-dose;
Durable treatment effect: 2 to 24 and 2 to 48 hour sustained pain freedom
Met both registrational endpoints (2 hr pain free & MBS) at 50 mg in two pivotal Phase 3 trials (multi-dose submission?)
Inconsistent effect on MBS across studies and doses
Durable treatment effect: did not show 2 to 48 hour sustained pain freedom
Met both registrational endpoints (2 hr Pain Free & MBS) in two pivotal Phase 3 Trials
Phase 2 — Durable treatment effect: headache recurrence at 24 hour not different from placebo
No data showing 2 to 24 hour or 2 to 48 hour sustained pain freedom or sustained pain relief
Preventive use only Durable treatment effect: vast
majority of patients show residual ongoing migraine attacks
Safety / Tolerability
No sig difference from Placebo on LFTs > ULN No single AE > 2% Tolerability profile similar to placebo without
difference from placebo on triptan AEs of interest Long-term safety study: up to daily dosing —
ongoing (started Aug 2017)
Imbalance 6 cases of LFTs > 3x ULN, 5 on ubrogepant vs 1 on placebo; 2 cases of LFTs > 5x ULN on ubrogepant (1 case > 10x ULN attributed to pancreatitis)
nausea, somnolence dry mouth >2.5% No single AE > 5%; treatment AEs appear to
increase with dose Long-term safety study: up to 8 doses per month
— pending 4Q2018; Planned 2nd LTS study≥ 15 doses per mo for 2 mo at 100 mg
Higher rates of treatment-emergent AEs compared to placebo (dizziness, paresthesia, somnolence, nausea, fatigue, lethargy and vertigo)
Phase 2 — Higher rates of severe AEs and treatment-emergent AEs compared to placebo (dizziness, fatigue, vertigo, paresthesias, somnolence and sensation of heaviness)
Ongoing study of effect on driving
Well tolerated Cumbersome route of
administration (IV, SC)
Benefits /Unknowns ofMechanism
Novel MOA targeting patients not satisfied with triptan efficacy or who are triptan intolerant or unresponsive
No reason to expect headache recurrence phenomena
Novel alternative for patients who are triptan intolerant or unresponsive
No reason to expect headache recurrence phenomena
Mechanism represents an advance on triptans Uncertainty regarding triptans — e.g., rebound Uncertain appeal in triptan
non-responders
Relatively long duration of action (1 dose per month or 1 dose per 3 months)
Lack of CV effect on exercise-induced angina (Amgen)
PREVENTION ONLY
Rimegepant Value Proposition
NOVEMBER 2018 ADVANCING INNOVATIVE THERAPIES FOR NEUROLOGICAL DISEASES 25
Oral Availability
Single dose & durable effect
Low cost of goods
Well tolerated
Effective on pain & MBS
Ultra-high potency
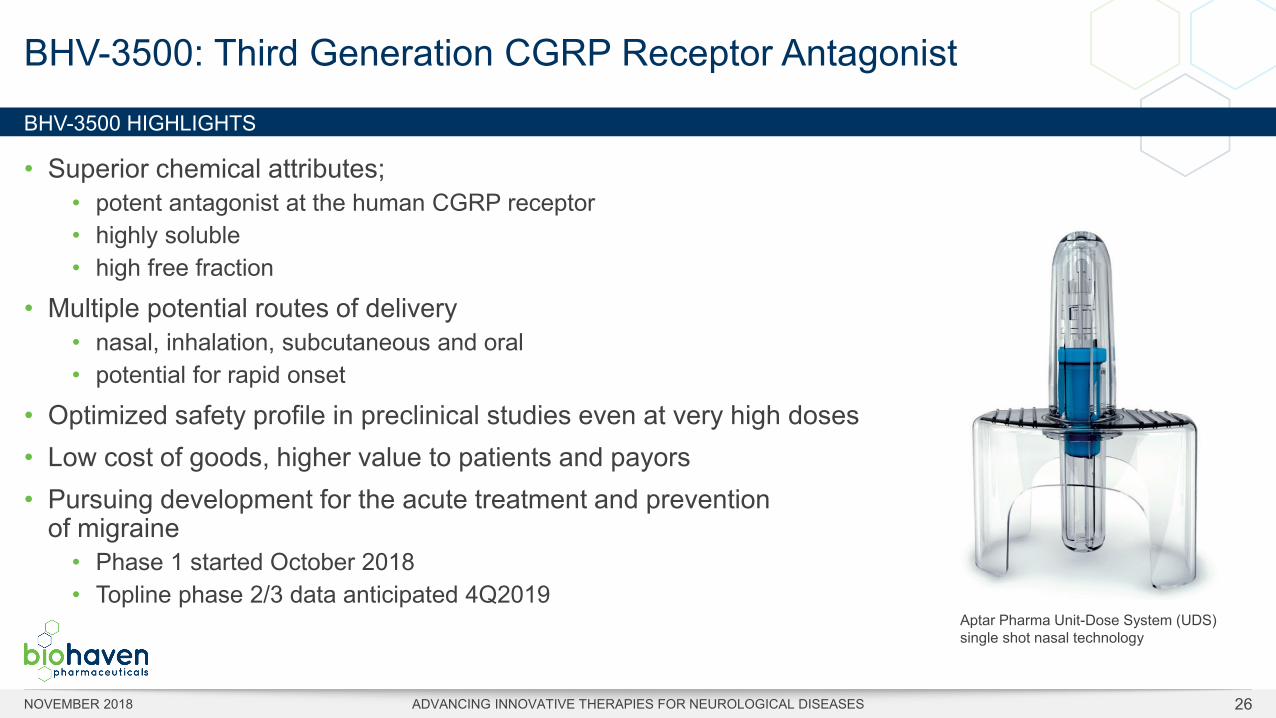
BHV-3500 HIGHLIGHTS
NOVEMBER 2018 ADVANCING INNOVATIVE THERAPIES FOR NEUROLOGICAL DISEASES 26
• Superior chemical attributes; • potent antagonist at the human CGRP receptor• highly soluble• high free fraction
• Multiple potential routes of delivery• nasal, inhalation, subcutaneous and oral• potential for rapid onset
• Optimized safety profile in preclinical studies even at very high doses• Low cost of goods, higher value to patients and payors• Pursuing development for the acute treatment and prevention
of migraine• Phase 1 started October 2018• Topline phase 2/3 data anticipated 4Q2019
BHV-3500: Third Generation CGRP Receptor Antagonist
Aptar Pharma Unit-Dose System (UDS) single shot nasal technology
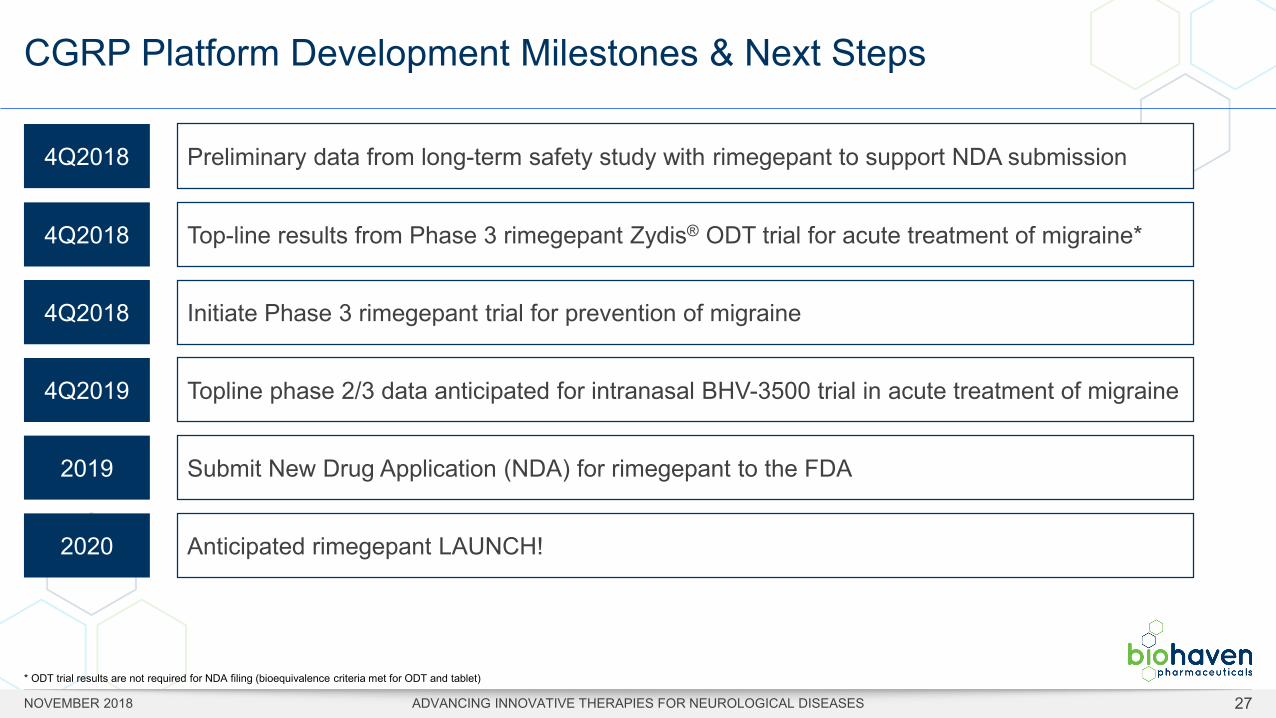
CGRP Platform Development Milestones & Next Steps
NOVEMBER 2018 ADVANCING INNOVATIVE THERAPIES FOR NEUROLOGICAL DISEASES 27
4Q2018 Preliminary data from long-term safety study with rimegepant to support NDA submission
4Q2018 Top-line results from Phase 3 rimegepant Zydis® ODT trial for acute treatment of migraine*
4Q2018 Initiate Phase 3 rimegepant trial for prevention of migraine
4Q2019 Topline phase 2/3 data anticipated for intranasal BHV-3500 trial in acute treatment of migraine
2019 Submit New Drug Application (NDA) for rimegepant to the FDA
2020 Anticipated rimegepant LAUNCH!
* ODT trial results are not required for NDA filing (bioequivalence criteria met for ODT and tablet)

GLUTAMATE PLATFORMTherapies for Neurologic and Neuropsychiatric Indications
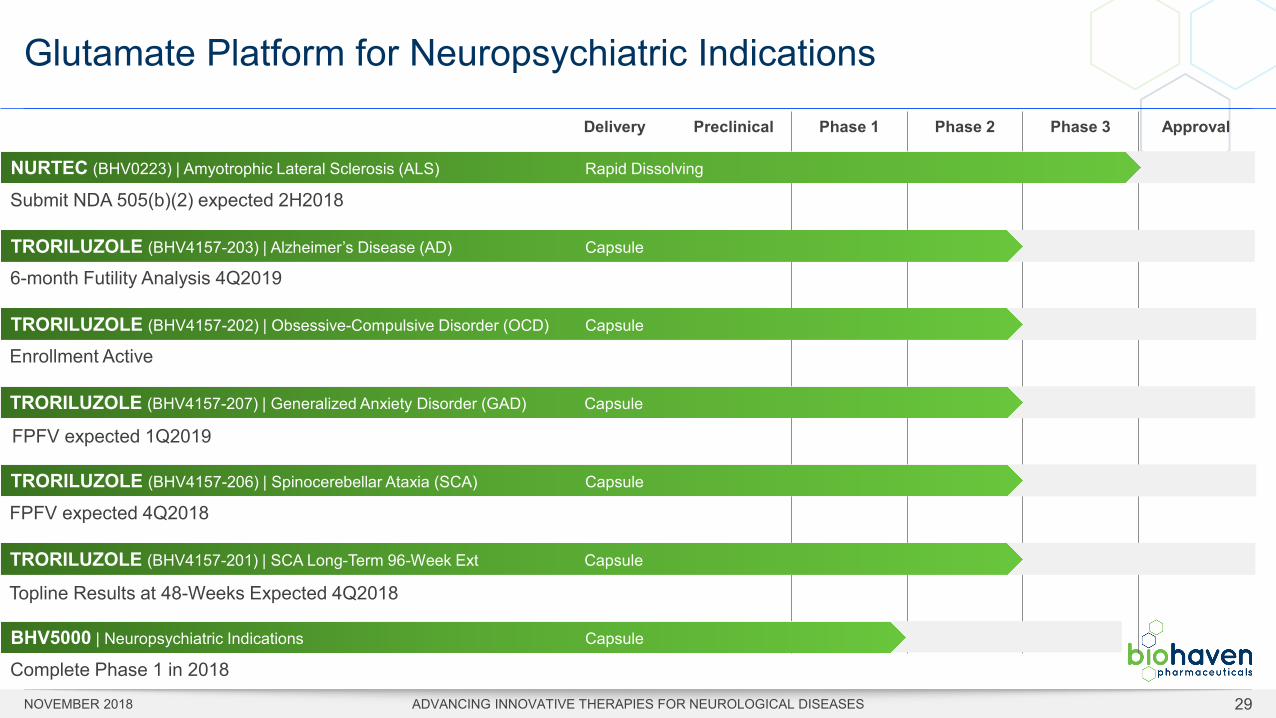
Glutamate Platform for Neuropsychiatric Indications
NOVEMBER 2018 ADVANCING INNOVATIVE THERAPIES FOR NEUROLOGICAL DISEASES 29
Preclinical Phase 1 Phase 2 Phase 3 ApprovalDelivery
NURTEC (BHV0223) | Amyotrophic Lateral Sclerosis (ALS) Rapid Dissolving
Submit NDA 505(b)(2) expected 2H2018
TRORILUZOLE (BHV4157-202) | Obsessive-Compulsive Disorder (OCD) Capsule
Enrollment Active
TRORILUZOLE (BHV4157-206) | Spinocerebellar Ataxia (SCA) Capsule
FPFV expected 4Q2018
TRORILUZOLE (BHV4157-203) | Alzheimer’s Disease (AD) Capsule
6-month Futility Analysis 4Q2019
BHV5000 | Neuropsychiatric Indications Capsule
Complete Phase 1 in 2018
TRORILUZOLE (BHV4157-207) | Generalized Anxiety Disorder (GAD) Capsule
FPFV expected 1Q2019
TRORILUZOLE (BHV4157-201) | SCA Long-Term 96-Week Ext Capsule
Topline Results at 48-Weeks Expected 4Q2018
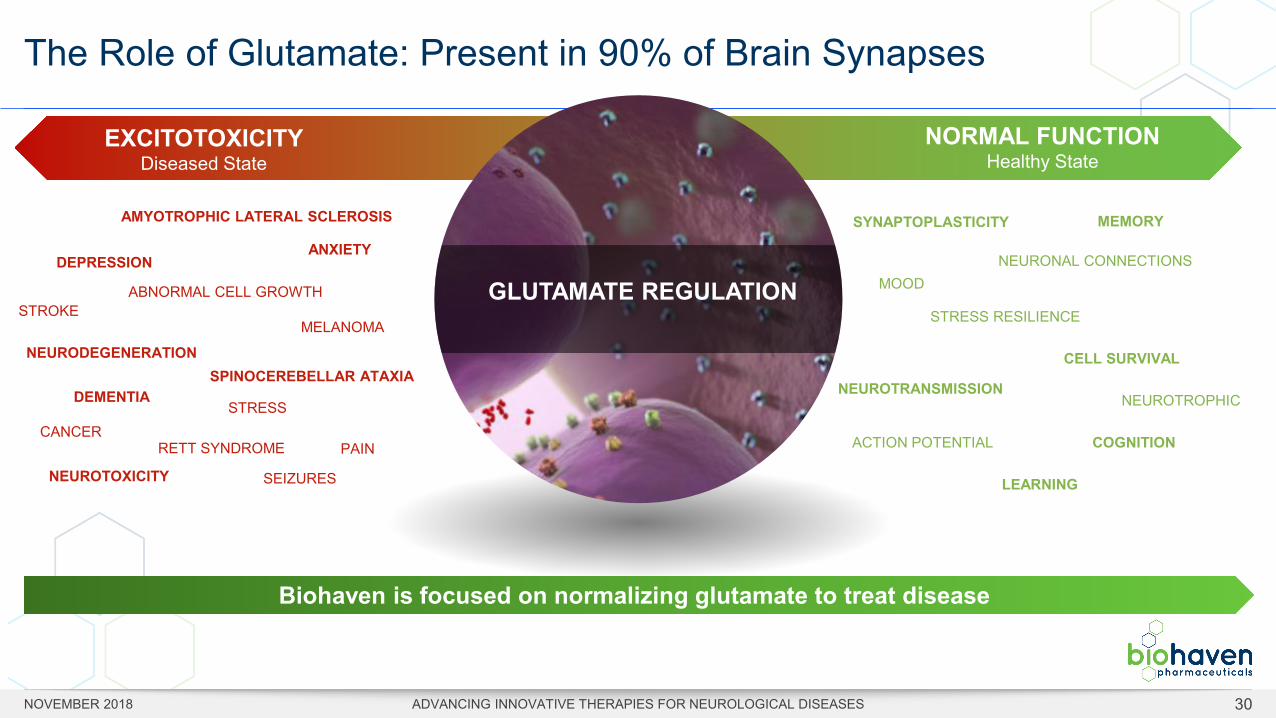
The Role of Glutamate: Present in 90% of Brain Synapses
NOVEMBER 2018 ADVANCING INNOVATIVE THERAPIES FOR NEUROLOGICAL DISEASES 30
Biohaven is focused on normalizing glutamate to treat disease
EXCITOTOXICITYDiseased State
NORMAL FUNCTIONHealthy State
GLUTAMATE REGULATION
AMYOTROPHIC LATERAL SCLEROSIS
SPINOCEREBELLAR ATAXIADEMENTIA
NEURODEGENERATION
NEUROTOXICITY SEIZURES
STRESS
DEPRESSION ANXIETY
STROKE
CANCERPAIN
MELANOMA
ABNORMAL CELL GROWTH
RETT SYNDROME
NEUROTRANSMISSION
MEMORY
CELL SURVIVAL
SYNAPTOPLASTICITY
LEARNING
NEUROTROPHIC
STRESS RESILIENCE
ACTION POTENTIAL COGNITION
MOODNEURONAL CONNECTIONS
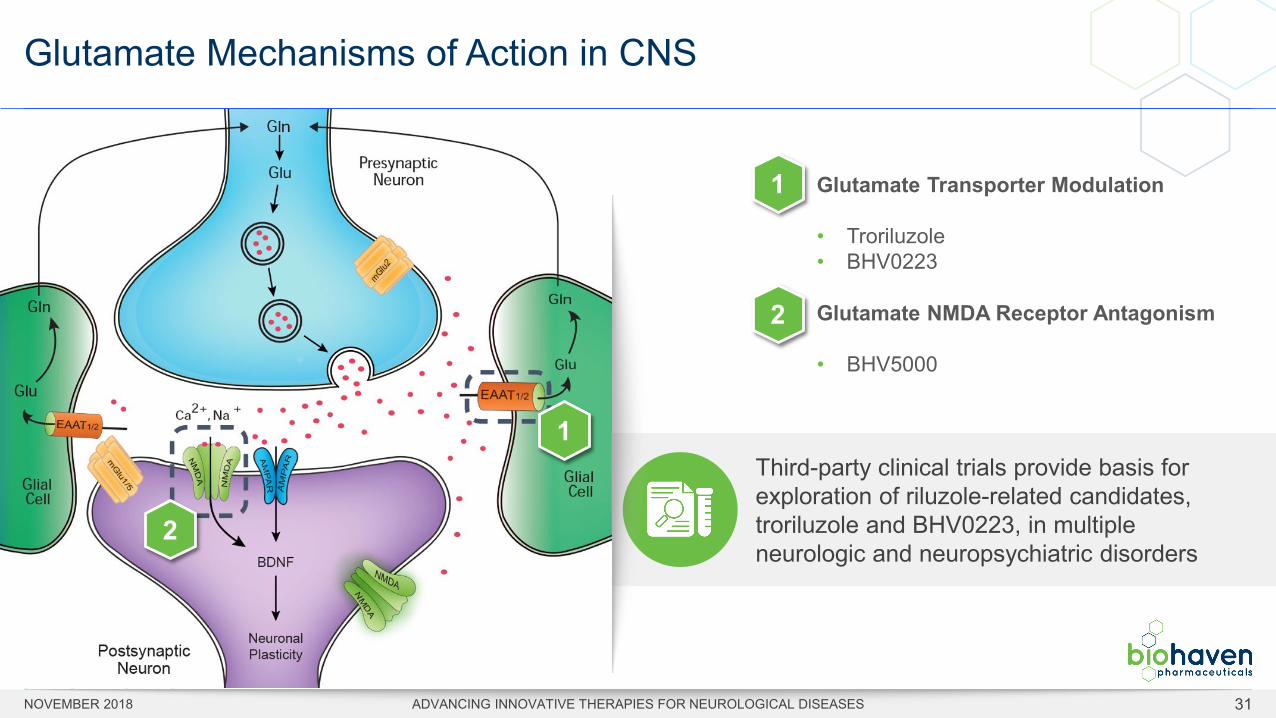
Glutamate Mechanisms of Action in CNS
NOVEMBER 2018 ADVANCING INNOVATIVE THERAPIES FOR NEUROLOGICAL DISEASES 31
Glutamate Transporter Modulation
• Troriluzole• BHV0223
Glutamate NMDA Receptor Antagonism
• BHV5000
Third-party clinical trials provide basis for exploration of riluzole-related candidates, troriluzole and BHV0223, in multiple neurologic and neuropsychiatric disorders
1
2
1
2
NOVEMBER 2018 ADVANCING INNOVATIVE THERAPIES FOR NEUROLOGICAL DISEASES 32
Riluzole is approved for the treatment of patients with amyotrophic lateral sclerosis (ALS) and proven to extend survival
• Originally marketed by Sanofi, Rilutek® (riluzole) received FDA approval in 1995
• In 2013, the FDA approved the first generic versions of riluzole
• Doses above 100 mg for efficacy not approved due to dose-dependent liver effects
BENEFITS Mechanism of action well understoodNeuroprotective, survival benefit in ALSWell tolerated, safe in clinical settings at approved dose
LIMITATIONS ✘Twice daily dosing, low bioavailability✘Fasting required for 6 hours/day,
can’t be taken with meals✘Dose dependent LFT liability(1)
✘Marked PK variability ✘High drug burden relative to efficacy(2)
✘Only one approved indication (ALS)
Riluzole: Use and Limitations
1. LFT = liver function test2. Poor oral bioavailability results in a high liver burden relative to efficacy as ~40% is either not absorbed or is metabolized in the liver
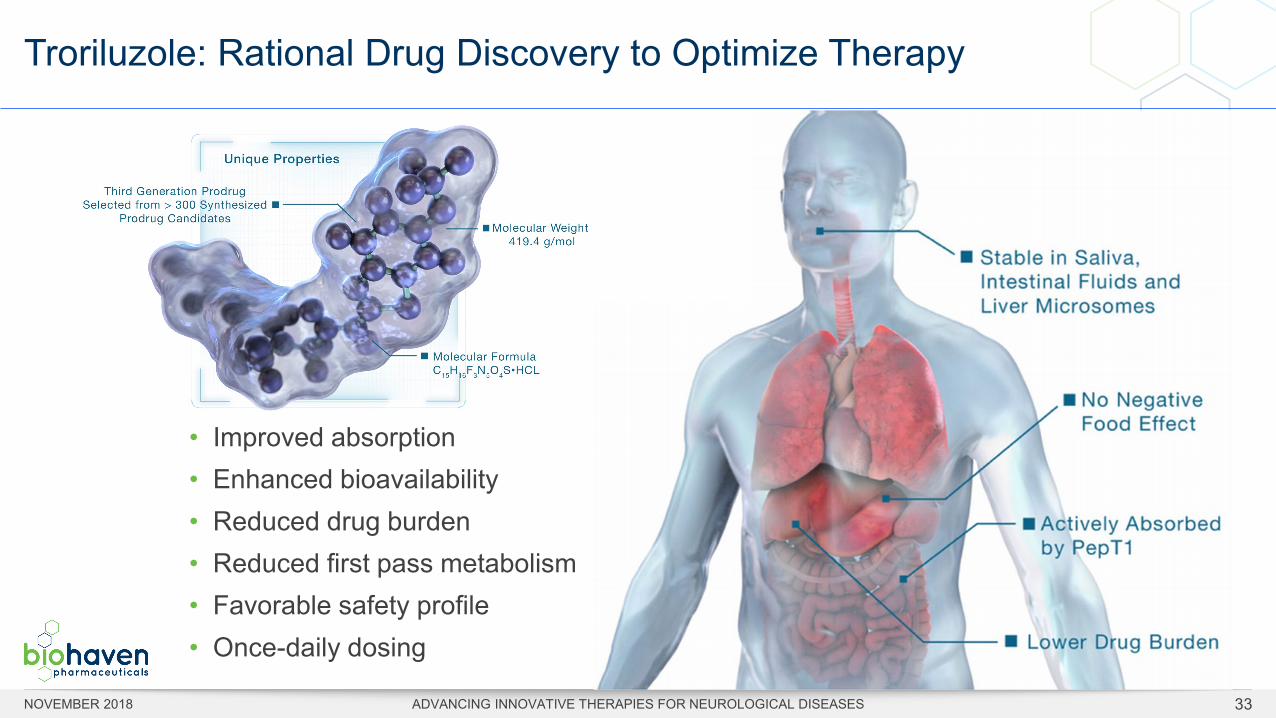
Troriluzole: Rational Drug Discovery to Optimize Therapy
NOVEMBER 2018 ADVANCING INNOVATIVE THERAPIES FOR NEUROLOGICAL DISEASES 33
• Improved absorption• Enhanced bioavailability• Reduced drug burden• Reduced first pass metabolism• Favorable safety profile• Once-daily dosing
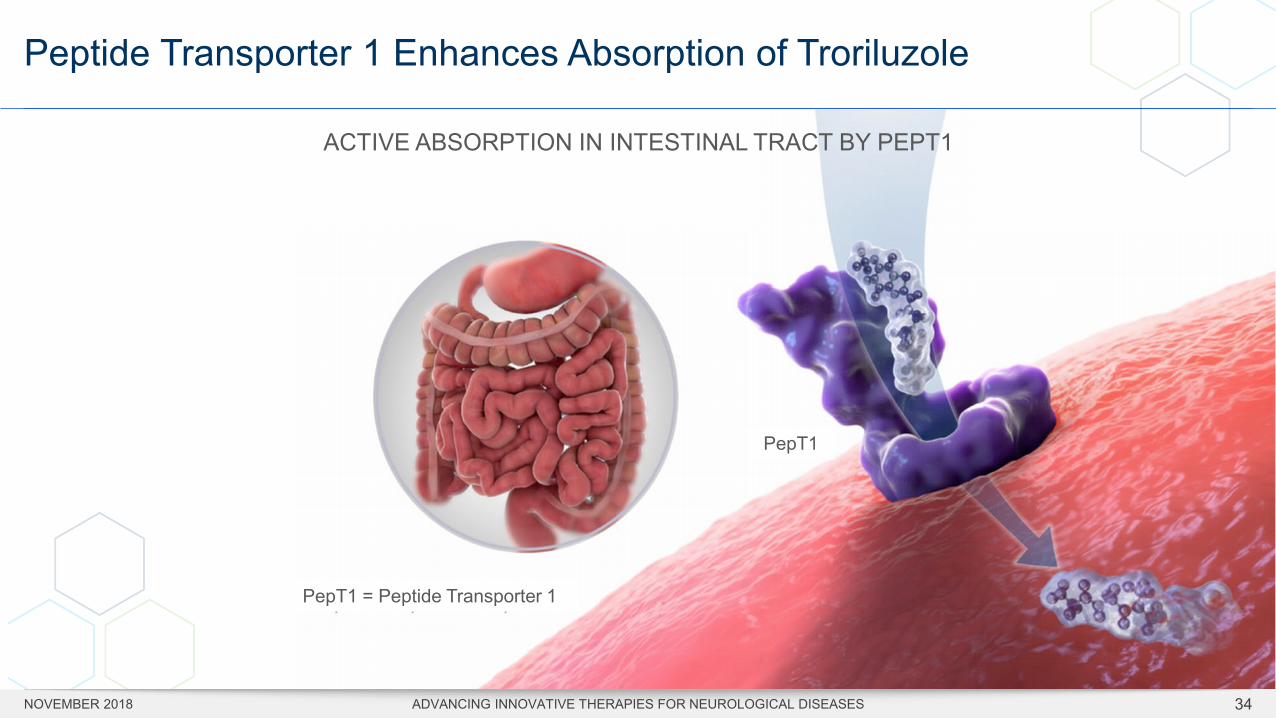
Peptide Transporter 1 Enhances Absorption of Troriluzole
PepT1
PepT1 = Peptide Transporter 1
ACTIVE ABSORPTION IN INTESTINAL TRACT BY PEPT1
NOVEMBER 2018 ADVANCING INNOVATIVE THERAPIES FOR NEUROLOGICAL DISEASES 34
TRORILUZOLE
NOVEMBER 2018 ADVANCING INNOVATIVE THERAPIES FOR NEUROLOGICAL DISEASES 35
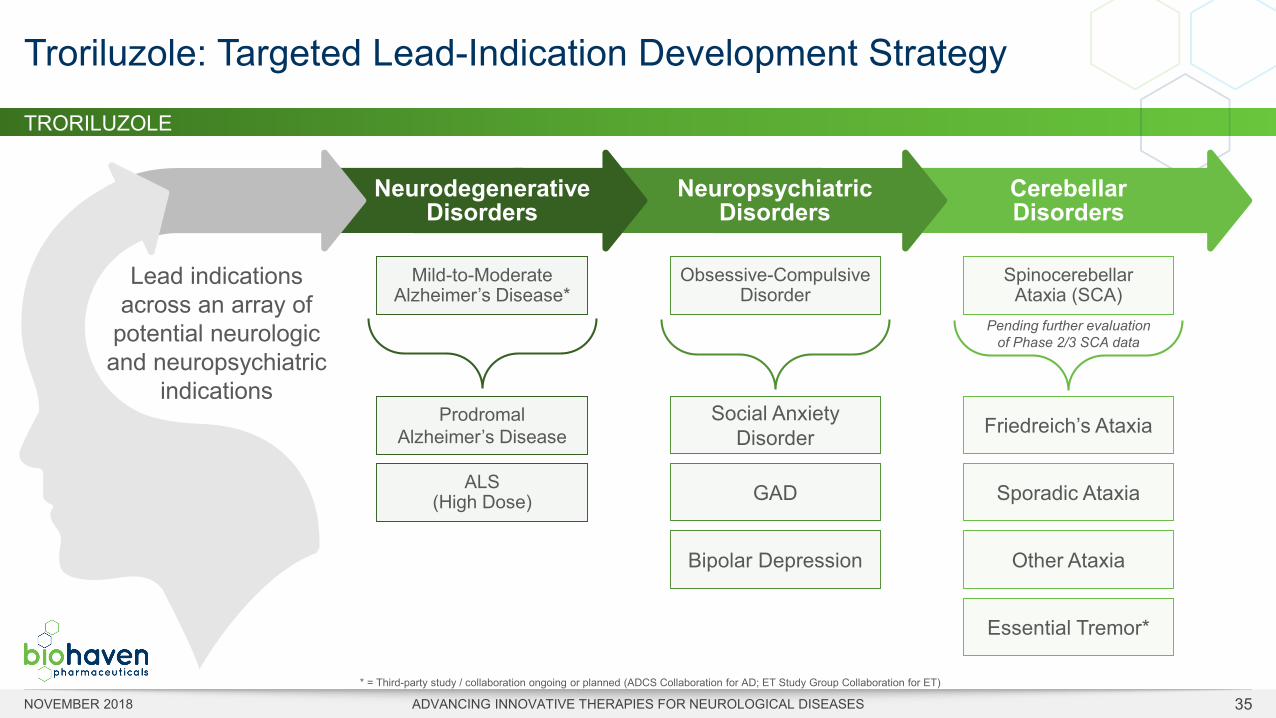
Troriluzole: Targeted Lead-Indication Development Strategy
* = Third-party study / collaboration ongoing or planned (ADCS Collaboration for AD; ET Study Group Collaboration for ET)
Pending further evaluation of Phase 2/3 SCA data
Lead indications across an array of
potential neurologic and neuropsychiatric
indications
Neurodegenerative Disorders
Mild-to-Moderate Alzheimer’s Disease*
Prodromal Alzheimer’s Disease
ALS (High Dose)
Neuropsychiatric Disorders
Obsessive-Compulsive Disorder
Social Anxiety Disorder
GAD
Bipolar Depression
Cerebellar Disorders
Spinocerebellar Ataxia (SCA)
Friedreich’s Ataxia
Sporadic Ataxia
Other Ataxia
Essential Tremor*
TRORILUZOLE
Rationale for Troriluzole in Alzheimer’s Disease (AD)
NOVEMBER 2018 ADVANCING INNOVATIVE THERAPIES FOR NEUROLOGICAL DISEASES 36
• Validated glutamate mechanism for treating neurodegenerative disease• Multimodal activity goes beyond simply targeting tau or amyloid• Therapeutic and pharmacologic effects of troriluzole in AD models
rescues cognitive symptoms and reverses hippocampal gene expression changes found in human AD tissue
• Potential to improve AD symptoms and reduce disease progression • Relevant to all stages of AD
Hallmarks of Human Alzheimer’s Disease• Cognitive and
behavioral symptoms• Loss of hippocampal
synapses (highly correlated with AD severity)
• Impairments in glutamate synapse structure and function
• Amyloid and tau pathology
GLIAL CELL FAILURE IS AN EARLY MARKER OF PATHOPHYSIOLGY
NOVEMBER 2018 ADVANCING INNOVATIVE THERAPIES FOR NEUROLOGICAL DISEASES 37
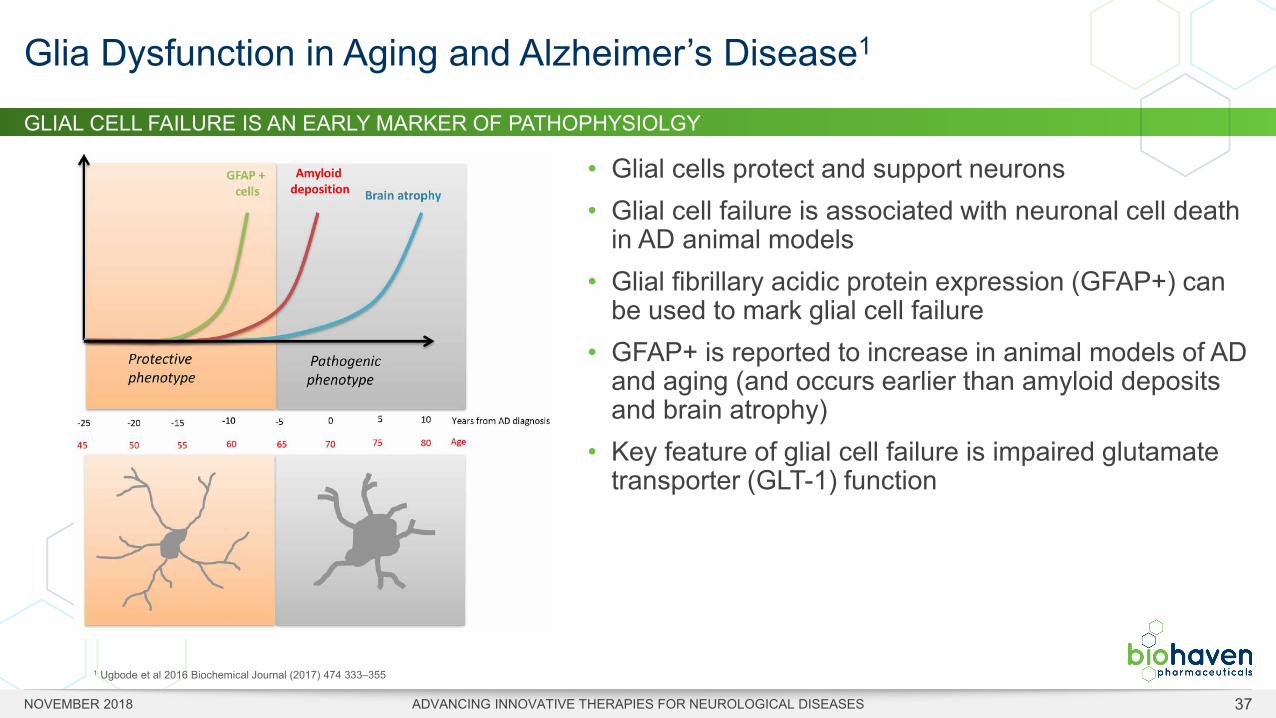
• Glial cells protect and support neurons• Glial cell failure is associated with neuronal cell death
in AD animal models• Glial fibrillary acidic protein expression (GFAP+) can
be used to mark glial cell failure• GFAP+ is reported to increase in animal models of AD
and aging (and occurs earlier than amyloid deposits and brain atrophy)
• Key feature of glial cell failure is impaired glutamate transporter (GLT-1) function
Glia Dysfunction in Aging and Alzheimer’s Disease1
1 Ugbode et al 2016 Biochemical Journal (2017) 474 333–355
NOVEMBER 2018 ADVANCING INNOVATIVE THERAPIES FOR NEUROLOGICAL DISEASES 38
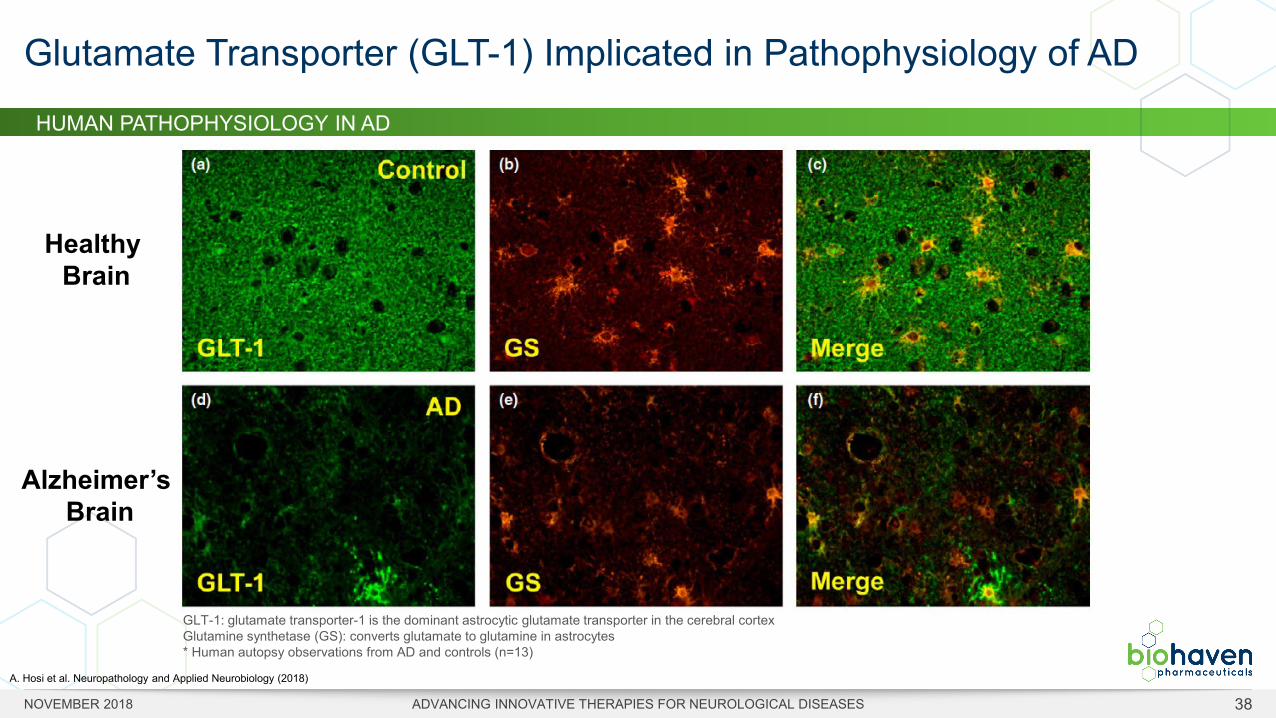
Glutamate Transporter (GLT-1) Implicated in Pathophysiology of AD
GLT-1: glutamate transporter-1 is the dominant astrocytic glutamate transporter in the cerebral cortexGlutamine synthetase (GS): converts glutamate to glutamine in astrocytes* Human autopsy observations from AD and controls (n=13)
A. Hosi et al. Neuropathology and Applied Neurobiology (2018)
HUMAN PATHOPHYSIOLOGY IN AD
Healthy Brain
Alzheimer’sBrain
NOVEMBER 2018 ADVANCING INNOVATIVE THERAPIES FOR NEUROLOGICAL DISEASES 39
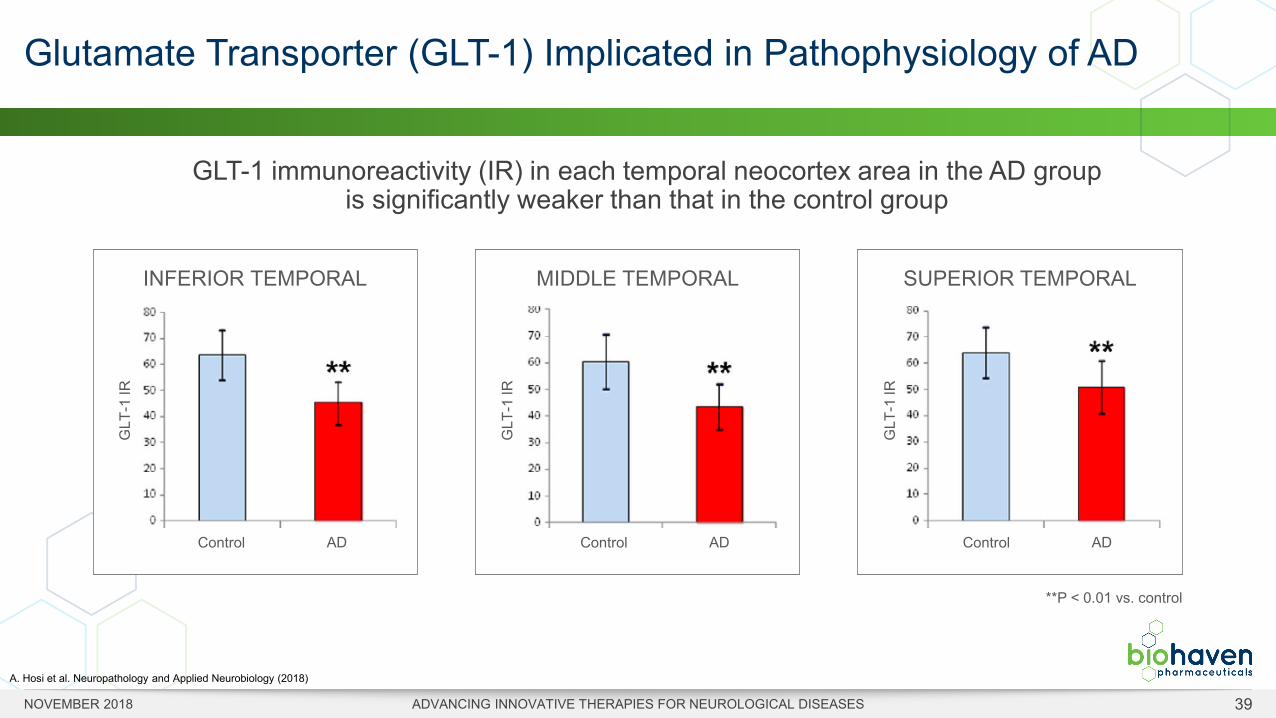
GLT-1 immunoreactivity (IR) in each temporal neocortex area in the AD group is significantly weaker than that in the control group
Glutamate Transporter (GLT-1) Implicated in Pathophysiology of AD
**P < 0.01 vs. control
GLT
-1 IR
Control AD
INFERIOR TEMPORAL
GLT
-1 IR
Control AD
MIDDLE TEMPORAL
GLT
-1 IR
Control AD
SUPERIOR TEMPORAL
A. Hosi et al. Neuropathology and Applied Neurobiology (2018)
I
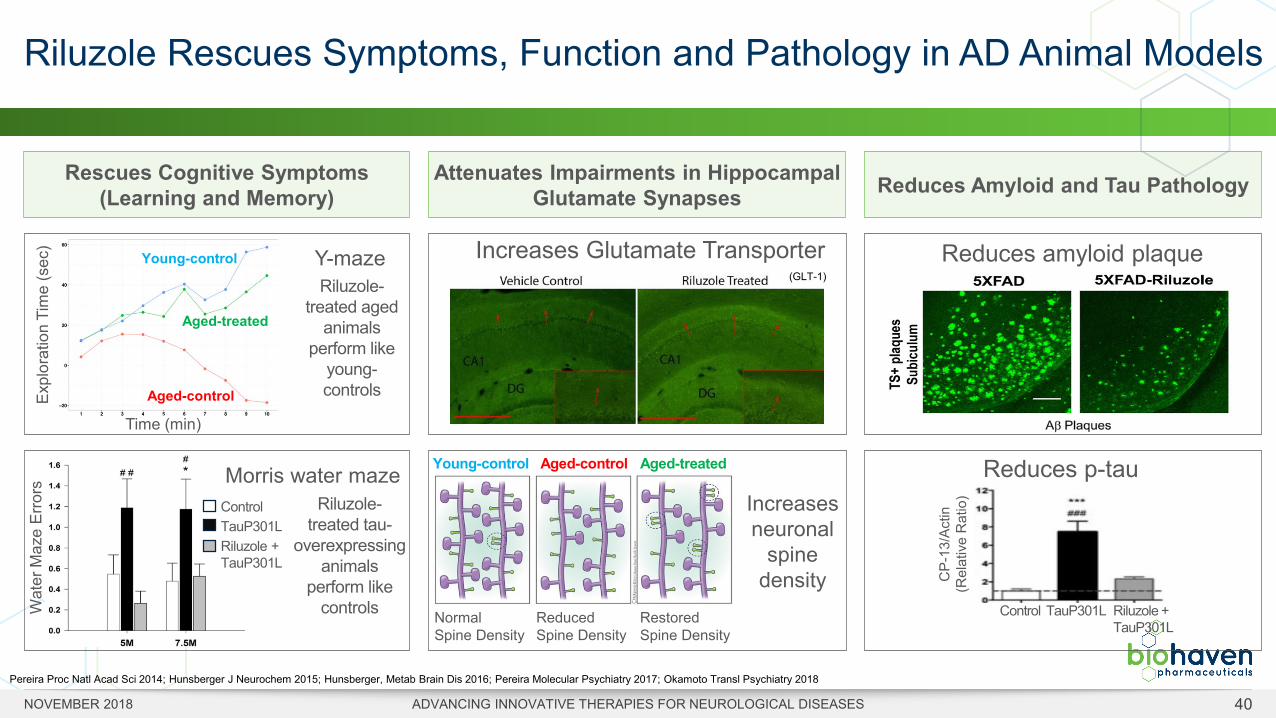
Attenuates Impairments in Hippocampal Glutamate Synapses
Rescues Cognitive Symptoms(Learning and Memory)
NOVEMBER 2018 ADVANCING INNOVATIVE THERAPIES FOR NEUROLOGICAL DISEASES 40
Riluzole Rescues Symptoms, Function and Pathology in AD Animal Models
Pereira Proc Natl Acad Sci 2014; Hunsberger J Neurochem 2015; Hunsberger, Metab Brain Dis 2016; Pereira Molecular Psychiatry 2017; Okamoto Transl Psychiatry 2018
Reduces Amyloid and Tau Pathology
Reduces amyloid plaque
Reduces p-tau
Increases Glutamate Transporter(GLT-1)
Control TauP301L Riluzole + TauP301L
CP-
13/A
ctin
(R
elat
ive
Rat
io)
Wat
er M
aze
Erro
rs
ControlTauP301LRiluzole + TauP301L
Morris water maze
Time (min)
Expl
orat
ion
Tim
e (s
ec)
Aged-control
Young-control
Aged-treated
Y-maze
Aged-controlYoung-control Aged-treated
Normal Spine Density
Reduced Spine Density
Restored Spine Density
Increases neuronal
spine density
Riluzole-treated aged
animals perform like
young-controls
Riluzole-treated tau-
overexpressing animals
perform like controls
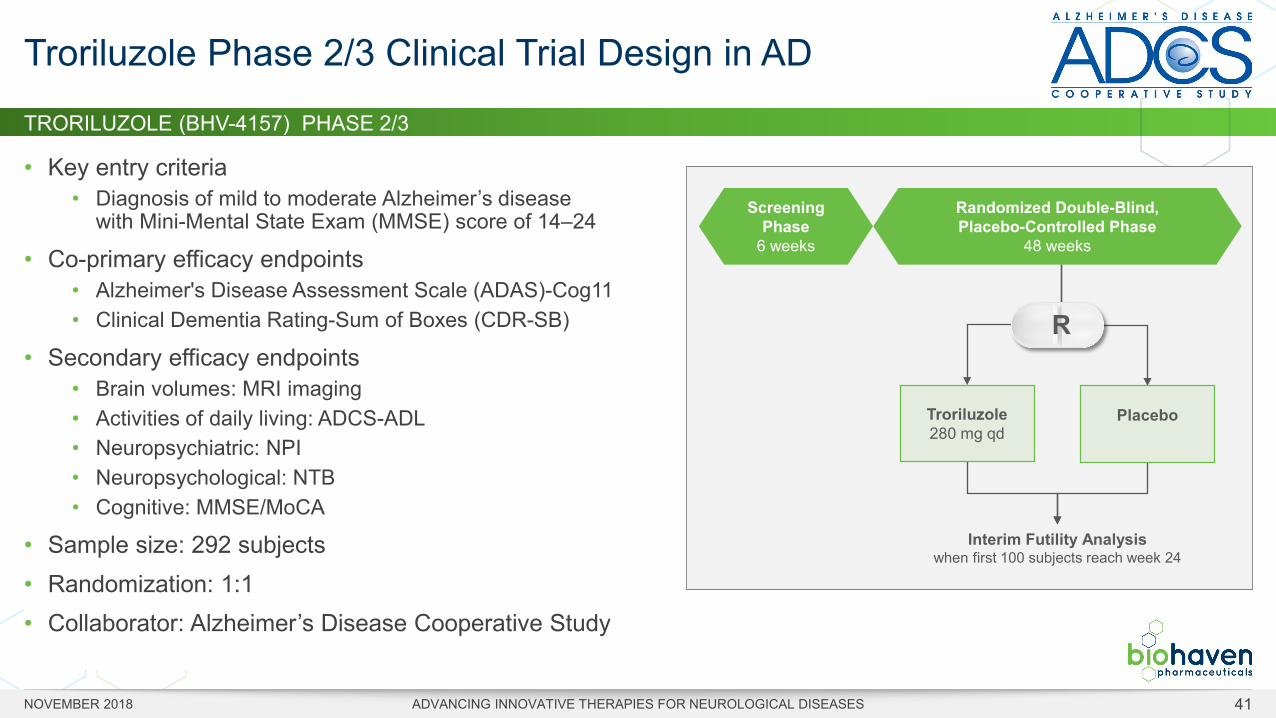
TRORILUZOLE (BHV-4157) PHASE 2/3
NOVEMBER 2018 ADVANCING INNOVATIVE THERAPIES FOR NEUROLOGICAL DISEASES 41
• Key entry criteria• Diagnosis of mild to moderate Alzheimer’s disease
with Mini-Mental State Exam (MMSE) score of 14–24
• Co-primary efficacy endpoints• Alzheimer's Disease Assessment Scale (ADAS)-Cog11• Clinical Dementia Rating-Sum of Boxes (CDR-SB)
• Secondary efficacy endpoints• Brain volumes: MRI imaging• Activities of daily living: ADCS-ADL• Neuropsychiatric: NPI• Neuropsychological: NTB• Cognitive: MMSE/MoCA
• Sample size: 292 subjects• Randomization: 1:1• Collaborator: Alzheimer’s Disease Cooperative Study
Troriluzole Phase 2/3 Clinical Trial Design in AD
Troriluzole280 mg qd
Placebo
Interim Futility Analysiswhen first 100 subjects reach week 24
Screening Phase
6 weeks
Randomized Double-Blind, Placebo-Controlled Phase
48 weeks
R
-2.00
-1.00
0.00
1.00
2.00
8 weeks
Cha
nge
in S
ARA
Scor
e
1. Ristori et al., Neurology 2010; 74: 839-845. 2. Romano et al., Lancet Neurol 2015; 14: 985–91. 3. Scale for the Assessment and Rating of Ataxia
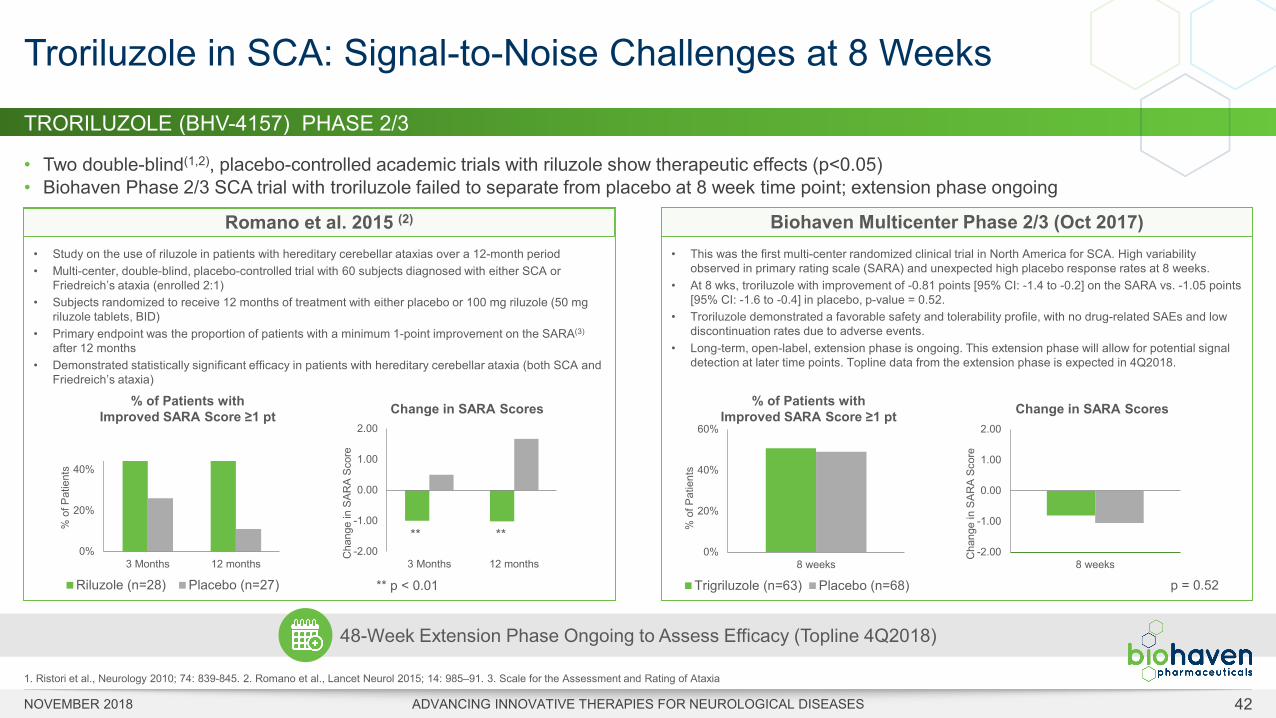
TRORILUZOLE (BHV-4157) PHASE 2/3
NOVEMBER 2018 ADVANCING INNOVATIVE THERAPIES FOR NEUROLOGICAL DISEASES 42
• Two double-blind(1,2), placebo-controlled academic trials with riluzole show therapeutic effects (p<0.05)• Biohaven Phase 2/3 SCA trial with troriluzole failed to separate from placebo at 8 week time point; extension phase ongoing
Troriluzole in SCA: Signal-to-Noise Challenges at 8 Weeks
• This was the first multi-center randomized clinical trial in North America for SCA. High variability observed in primary rating scale (SARA) and unexpected high placebo response rates at 8 weeks.
• At 8 wks, troriluzole with improvement of -0.81 points [95% CI: -1.4 to -0.2] on the SARA vs. -1.05 points [95% CI: -1.6 to -0.4] in placebo, p-value = 0.52.
• Troriluzole demonstrated a favorable safety and tolerability profile, with no drug-related SAEs and low discontinuation rates due to adverse events.
• Long-term, open-label, extension phase is ongoing. This extension phase will allow for potential signal detection at later time points. Topline data from the extension phase is expected in 4Q2018.
0%
20%
40%
60%
8 weeks
% o
f Pat
ient
s
Trigriluzole (n=63) Placebo (n=68)
% of Patients with Improved SARA Score ≥1 pt
p = 0.52
Change in SARA Scores
Biohaven Multicenter Phase 2/3 (Oct 2017)
-2.00
-1.00
0.00
1.00
2.00
3 Months 12 months
Cha
nge
in S
ARA
Scor
e
0%
20%
40%
60%
3 Months 12 months
% o
f Pat
ient
s
Riluzole (n=28) Placebo (n=27) ** p < 0.01
Romano et al. 2015 (2)
• Study on the use of riluzole in patients with hereditary cerebellar ataxias over a 12-month period• Multi-center, double-blind, placebo-controlled trial with 60 subjects diagnosed with either SCA or
Friedreich’s ataxia (enrolled 2:1) • Subjects randomized to receive 12 months of treatment with either placebo or 100 mg riluzole (50 mg
riluzole tablets, BID)• Primary endpoint was the proportion of patients with a minimum 1-point improvement on the SARA(3)
after 12 months• Demonstrated statistically significant efficacy in patients with hereditary cerebellar ataxia (both SCA and
Friedreich’s ataxia)
** **
% of Patients with Improved SARA Score ≥1 pt Change in SARA Scores
48-Week Extension Phase Ongoing to Assess Efficacy (Topline 4Q2018)
Num
ber o
f Sub
ject
s
Δ SARA [Screening SARA – Baseline SARA] Points
+ 2pt- 2pt
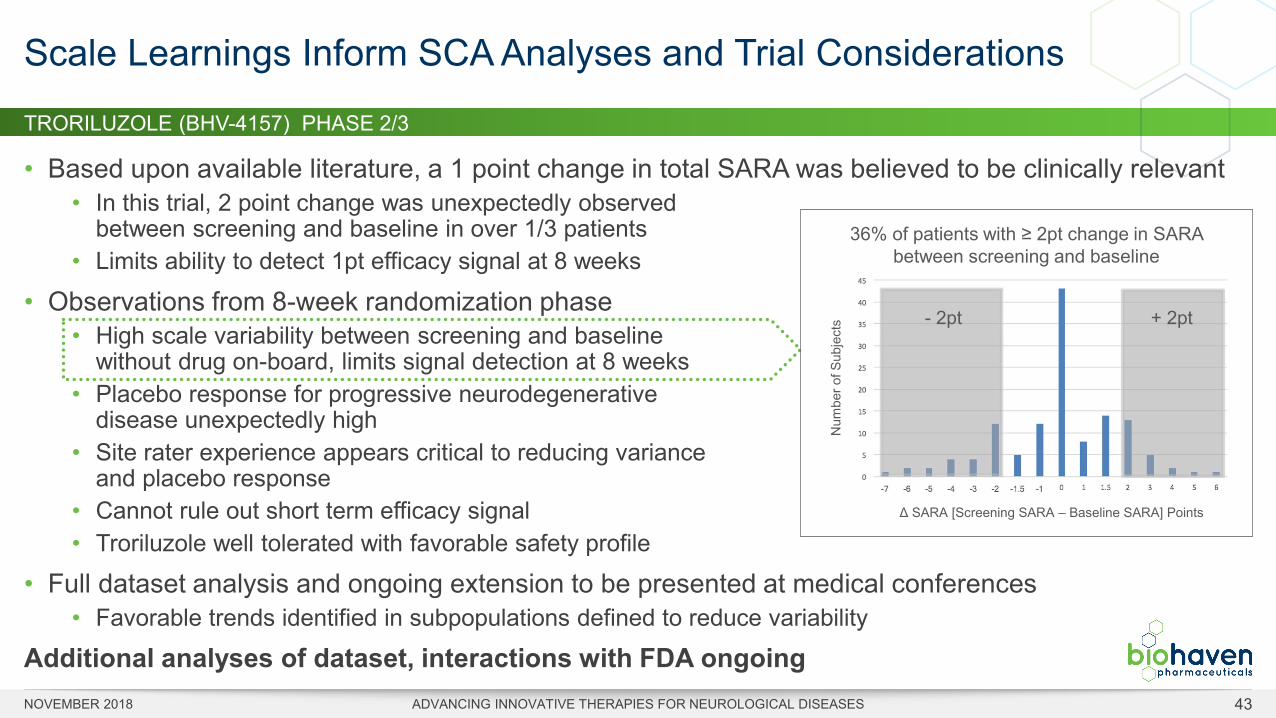
TRORILUZOLE (BHV-4157) PHASE 2/3
NOVEMBER 2018 ADVANCING INNOVATIVE THERAPIES FOR NEUROLOGICAL DISEASES 43
• Based upon available literature, a 1 point change in total SARA was believed to be clinically relevant • In this trial, 2 point change was unexpectedly observed
between screening and baseline in over 1/3 patients• Limits ability to detect 1pt efficacy signal at 8 weeks
• Observations from 8-week randomization phase• High scale variability between screening and baseline
without drug on-board, limits signal detection at 8 weeks• Placebo response for progressive neurodegenerative
disease unexpectedly high• Site rater experience appears critical to reducing variance
and placebo response• Cannot rule out short term efficacy signal• Troriluzole well tolerated with favorable safety profile
• Full dataset analysis and ongoing extension to be presented at medical conferences• Favorable trends identified in subpopulations defined to reduce variability
Additional analyses of dataset, interactions with FDA ongoing
Scale Learnings Inform SCA Analyses and Trial Considerations
36% of patients with ≥ 2pt change in SARA between screening and baseline
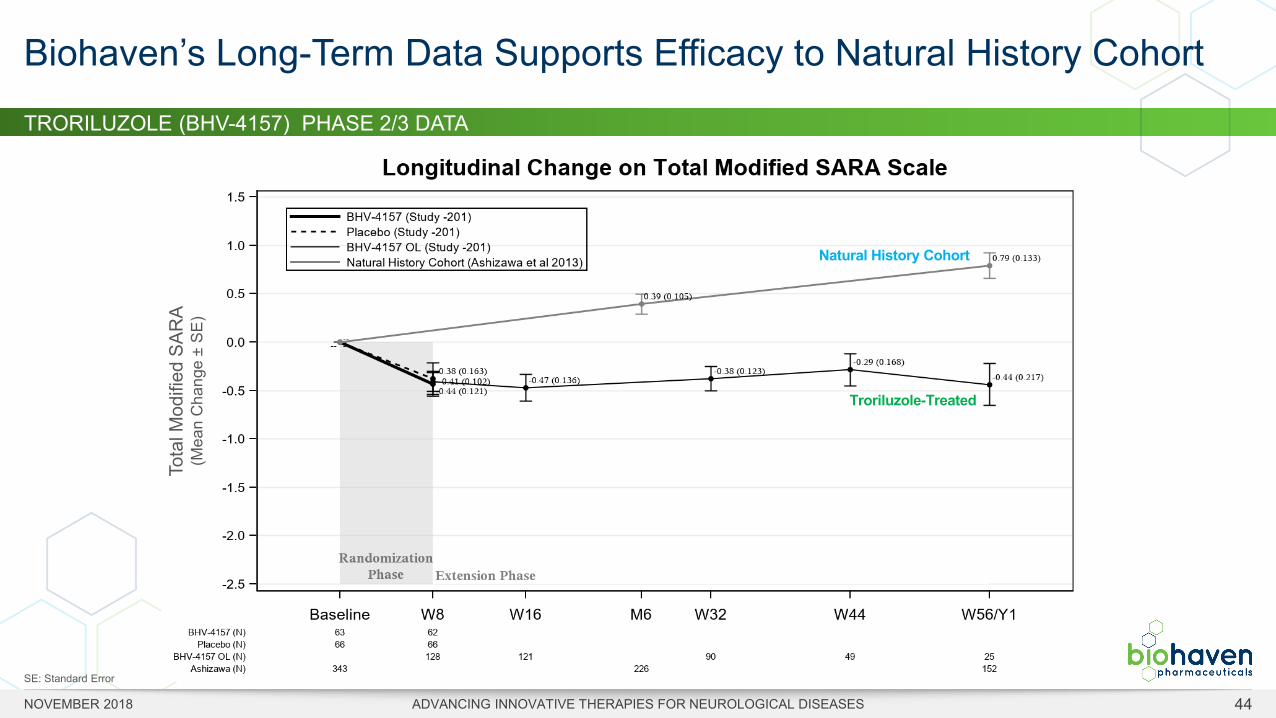
TRORILUZOLE (BHV-4157) PHASE 2/3 DATA
NOVEMBER 2018 ADVANCING INNOVATIVE THERAPIES FOR NEUROLOGICAL DISEASES 44
Biohaven’s Long-Term Data Supports Efficacy to Natural History Cohort
Natural History Cohort
Troriluzole-Treated
Tota
l Mod
ified
SAR
A(M
ean
Cha
nge
±SE
)
SE: Standard Error
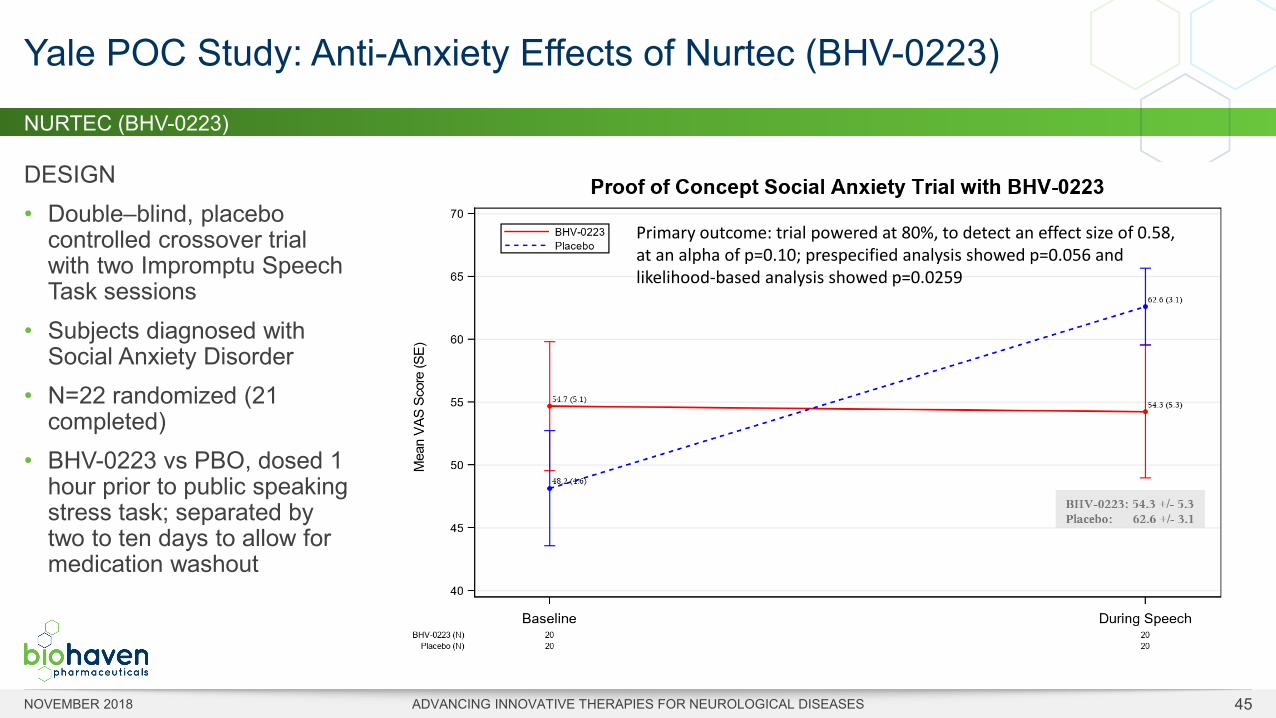
NURTEC (BHV-0223)
DESIGN • Double–blind, placebo
controlled crossover trial with two Impromptu Speech Task sessions
• Subjects diagnosed with Social Anxiety Disorder
• N=22 randomized (21 completed)
• BHV-0223 vs PBO, dosed 1 hour prior to public speaking stress task; separated by two to ten days to allow for medication washout
Yale POC Study: Anti-Anxiety Effects of Nurtec (BHV-0223)
Primary outcome: trial powered at 80%, to detect an effect size of 0.58, at an alpha of p=0.10; prespecified analysis showed p=0.056 and likelihood-based analysis showed p=0.0259
NOVEMBER 2018 ADVANCING INNOVATIVE THERAPIES FOR NEUROLOGICAL DISEASES 45
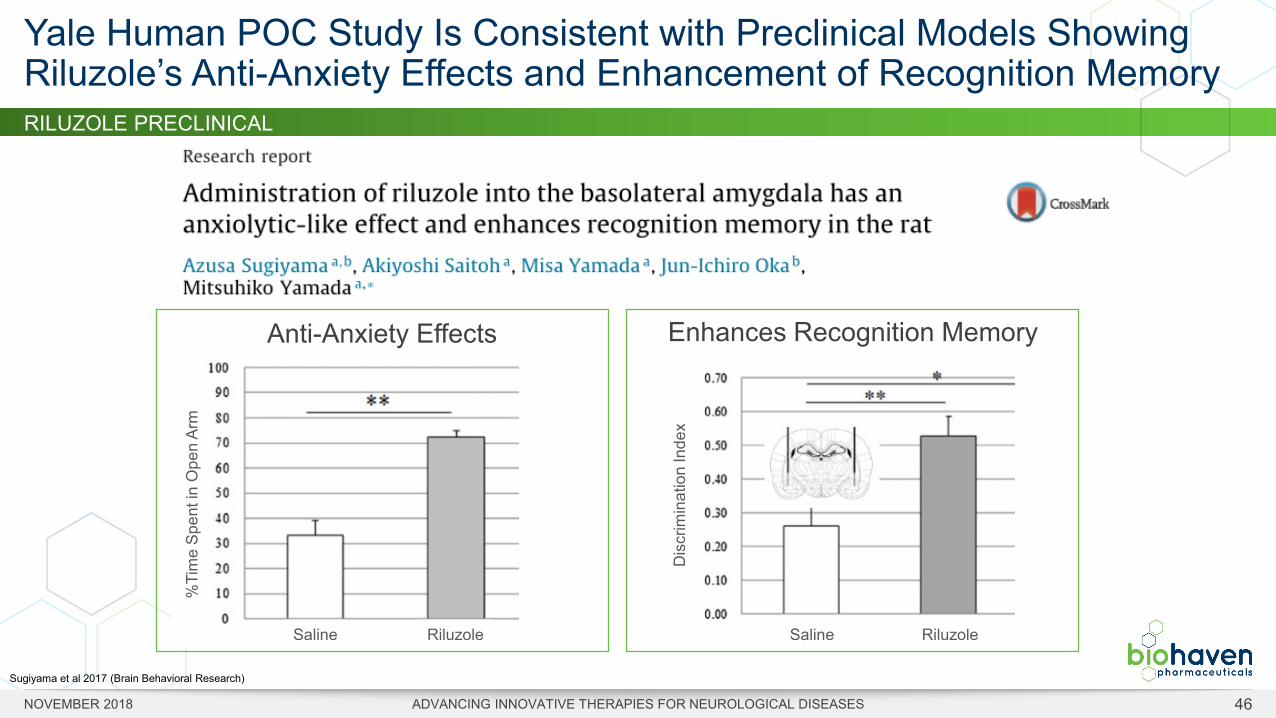
RILUZOLE PRECLINICAL
Yale Human POC Study Is Consistent with Preclinical Models Showing Riluzole’s Anti-Anxiety Effects and Enhancement of Recognition Memory
Sugiyama et al 2017 (Brain Behavioral Research)
NOVEMBER 2018 ADVANCING INNOVATIVE THERAPIES FOR NEUROLOGICAL DISEASES 46
Anti-Anxiety Effects
%Ti
me
Spen
t in
Ope
n Ar
m
Saline Riluzole
Enhances Recognition Memory
Dis
crim
inat
ion
Inde
x
Saline Riluzole
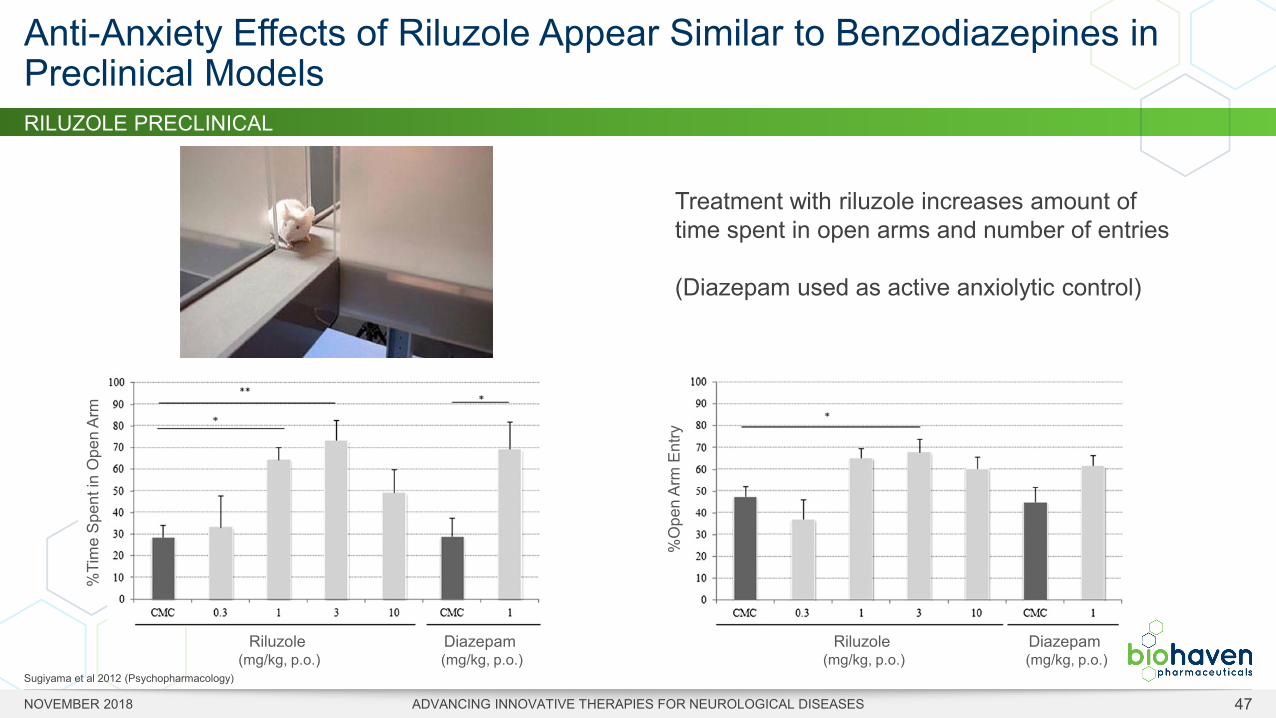
Treatment with riluzole increases amount of time spent in open arms and number of entries
(Diazepam used as active anxiolytic control)
Sugiyama et al 2012 (Psychopharmacology)
RILUZOLE PRECLINICAL
NOVEMBER 2018 ADVANCING INNOVATIVE THERAPIES FOR NEUROLOGICAL DISEASES 47
Anti-Anxiety Effects of Riluzole Appear Similar to Benzodiazepines in Preclinical Models
%Ti
me
Spen
t in
Ope
n Ar
m
%O
pen
Arm
Ent
ry
Riluzole(mg/kg, p.o.)
Diazepam (mg/kg, p.o.)
Riluzole(mg/kg, p.o.)
Diazepam (mg/kg, p.o.)
TRORILUZOLE (BHV-4157) PHASE 2/3 TRIAL DESIGN
GENERALIZED ANXIETY DISORDER
• Chronic or excessive worry, restlessness, fatigue, difficulty concentrating, insomnia
• Impairs ability to function socially or at work
• Irritable bowel-like gastrointestinal issues
• GAD has a 12-month prevalence in the United States of 3%
• 3,500,000 (est. treatment resistant in U.S.)
RILUZOLE PHASE 2/3 TRIAL DESIGN
• Multicenter (US only), randomized, double-blind, placebo-controlled trial in outpatients with GAD
• Troriluzole 140 mg QHS* & 60 mg QAM* vs Placebo BID*, N=260
• Primary Outcome: Change on HAM-A from baseline to Week 8
• Significant unmet need
• Yale IP protects riluzole in GAD, SAD & Panic Disorder
Expanding Biohaven’s glutamate modulating platform into Generalized Anxiety Disorder (GAD)
NBC New, 28-JUL-18
NOVEMBER 2018 ADVANCING INNOVATIVE THERAPIES FOR NEUROLOGICAL DISEASES 48
* QHS: every bedtime, QAM: every morning, BID: twice daily
NURTEC (BHV-0223)
NOVEMBER 2018 ADVANCING INNOVATIVE THERAPIES FOR NEUROLOGICAL DISEASES 49
• Amyotrophic Lateral Sclerosis (ALS) is a progressive neurodegenerative disease that causes muscle weakness, difficulties with breathing and swallowing and death
• Generic riluzole has been proven to extends survival in ALS• Yet, swallowing is a challenge for patients with ALS
• About 1/3 of patients have dysphagia at diagnosis; over 80% during advanced disease • Many crush riluzole tablet and mix with food, yet label cautions results in lower drug
levels• Fasting required 3 hours per dose (fast 2 hours before and one hour after meals)
• Nurtec is a proprietary, novel formulation of riluzole optimized for sublingual administration
• Nurtec rapidly dissolves when placed under tongue• Active ingredient efficiently absorbed by sublingual mucosa• No need to swallow tablet with liquid
NURTEC is Optimized to Address Riluzole Delivery Limitations for ALS
Only Riluzole Oral Dissolving Tablet meets needs with difficulty swallowing
Cau
tion:
New
Dru
g-L
imite
d by
Uni
ted
Stat
es la
w to
inve
stig
atio
nal u
se
NURTEC (BHV-0223)
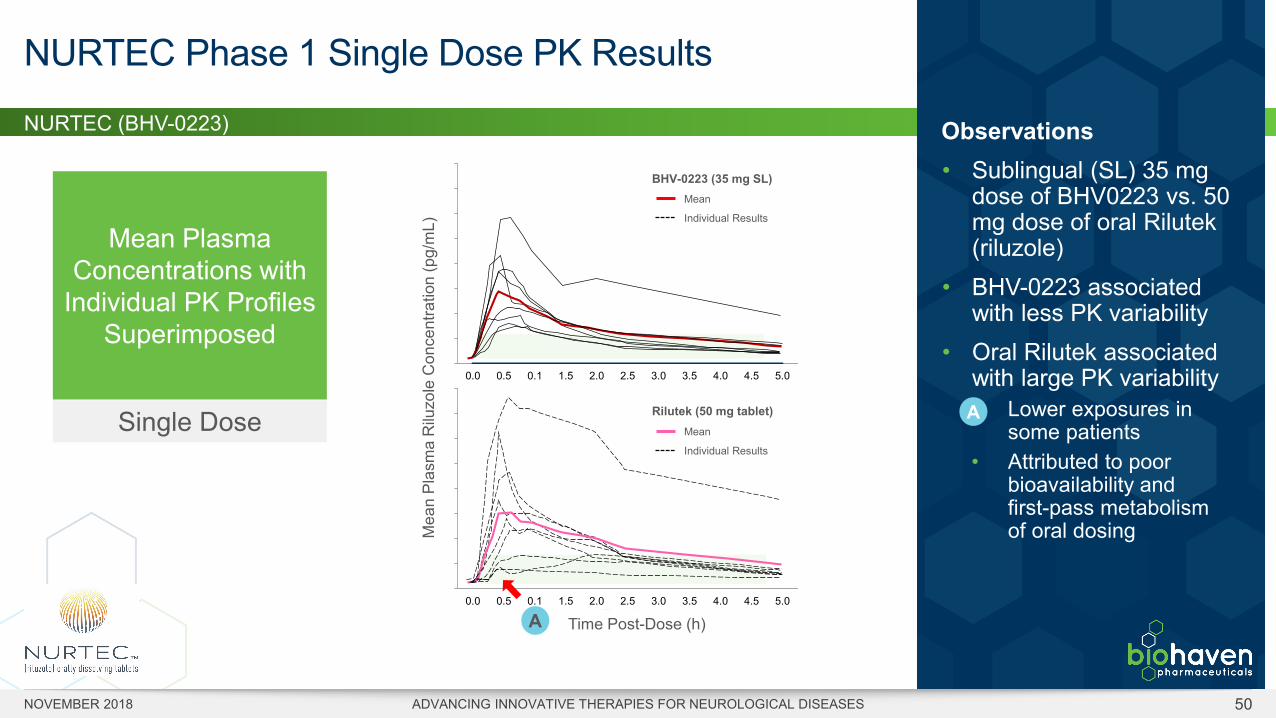
NURTEC Phase 1 Single Dose PK Results
NOVEMBER 2018 ADVANCING INNOVATIVE THERAPIES FOR NEUROLOGICAL DISEASES 50
Observations• Sublingual (SL) 35 mg
dose of BHV0223 vs. 50 mg dose of oral Rilutek(riluzole)
• BHV-0223 associated with less PK variability
• Oral Rilutek associated with large PK variability• Lower exposures in
some patients• Attributed to poor
bioavailability and first-pass metabolism of oral dosing
0
50000
100000
150000
200000
250000
300000
350000
400000
0.0 0.5 0.1 1.5 2.0 2.5 3.0 3.5 4.0 4.5 5.0
0
50000
100000
150000
200000
250000
300000
350000
400000
0.0 0.5 0.1 1.5 2.0 2.5 3.0 3.5 4.0 4.5 5.0
Rilutek (50 mg tablet)
BHV-0223 (35 mg SL)
Actual Time (h)A
Mea
n Pl
asm
a R
iluzo
leC
once
ntra
tion
(pg/
mL)
Mean
Individual Results
Mean
Individual Results
A
Mean Plasma Concentrations with
Individual PK Profiles Superimposed
Single Dose
Time Post-Dose (h)
NURTEC (BHV-0223)
NOVEMBER 2018 ADVANCING INNOVATIVE THERAPIES FOR NEUROLOGICAL DISEASES 51
EASE OF ADMINISTRATION • An early symptom of ALS is difficulty swallowing; makes use of riluzole
tablets challenging
• BHV0223 uses fast-dissolving technology that does not require swallowing or administration of liquids
NO FOOD EFFECT • Prescribing instructions for riluzole tablets state that it should be taken
at least an hour before, or two hours after, a meal to avoid food-related decreases in bioavailability
• Patients who do not strictly adhere to these fasting requirements or administer crushed riluzole in food, may not be obtaining desired therapeutic levels of riluzole
• BHV0223 was designed to be absorbed sublingually; since absorption of BHV0223 occurs in the vasculature under the tongue, fasting requirements are not anticipated
• This will be particularly beneficial to patients who require a continuous feeding tube for nutrition
NURTEC Offers Potential Advantages Over Conventional Riluzole Tablets for ALS Patients
MORE PREDICTABLE PHARMACOKINETIC PERFORMANCE • Some patients with ALS crush their solid riluzole tablets and
take with food to ease administration(1)
• With BHV0223, patients will not have to crush or alter the form of administration
• In Phase 1 trial, observed less pharmacokinetic variability with BHV0223 compared to 50 mg riluzole
REDUCED DRUG LOAD AND LIVER EXPOSURE • Riluzole associated with dose-dependent liver issues
resulting from high dose loads / extensive liver metabolism
• BHV0223 is sublingually absorbed, bypassing first-pass liver metabolism and reducing the dosage size that needs to be administered, thereby reducing potential risk for hepatic enzyme elevations
1. Leads to uncertain pharmacokinetic performance as well as oral numbness
BHV-5000
NOVEMBER 2018 ADVANCING INNOVATIVE THERAPIES FOR NEUROLOGICAL DISEASES 52
• Potential first-in-class, next-generation NMDA receptor antagonist • Exclusive license from AstraZeneca• Low-trapping agent • Orally bioavailable prodrug of the IV drug lanicemine
• NMDA modulation has the potential for applicability across a number of CNS disorders• BHV-5000 demonstrate markedly mitigated risk of dissociative effects in the clinic • Attributed to its distinct ability to uncouple from the NMDA receptor more freely than other agents
• Well tolerated in a Phase 1 single and multiple ascending dose trial• BHV-5000 doses up to 95 mg studied to date in Phase 1• Active metabolite, lanicemine, has been administered to ~770 subjects in single or multiple doses
in 18 clinical trials; generally well tolerated
BHV-5000: A Novel Low-Trapping NMDA Antagonist
BHV-5000 MOA
NOVEMBER 2018 ADVANCING INNOVATIVE THERAPIES FOR NEUROLOGICAL DISEASES 53
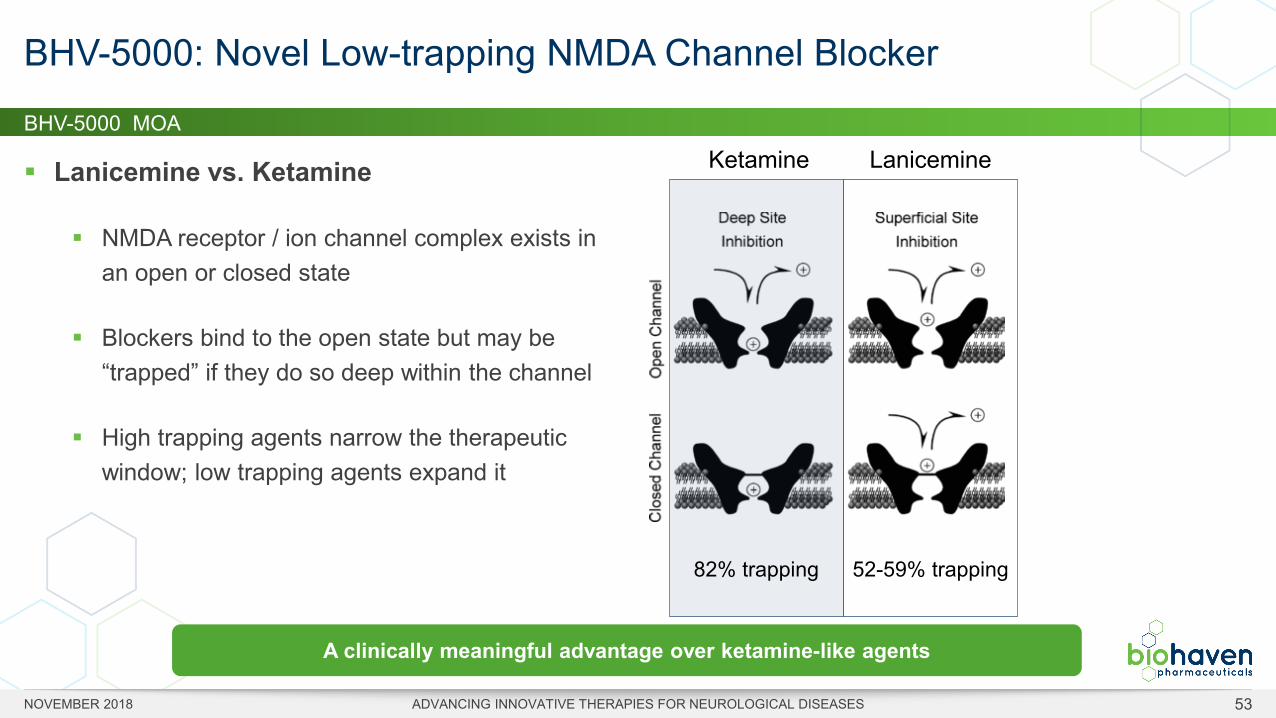
Lanicemine vs. Ketamine
NMDA receptor / ion channel complex exists in an open or closed state
Blockers bind to the open state but may be “trapped” if they do so deep within the channel
High trapping agents narrow the therapeutic window; low trapping agents expand it
BHV-5000: Novel Low-trapping NMDA Channel Blocker
82% trapping 52-59% trapping
LanicemineKetamine
A clinically meaningful advantage over ketamine-like agents
LANICEMINE
NOVEMBER 2018 ADVANCING INNOVATIVE THERAPIES FOR NEUROLOGICAL DISEASES 54
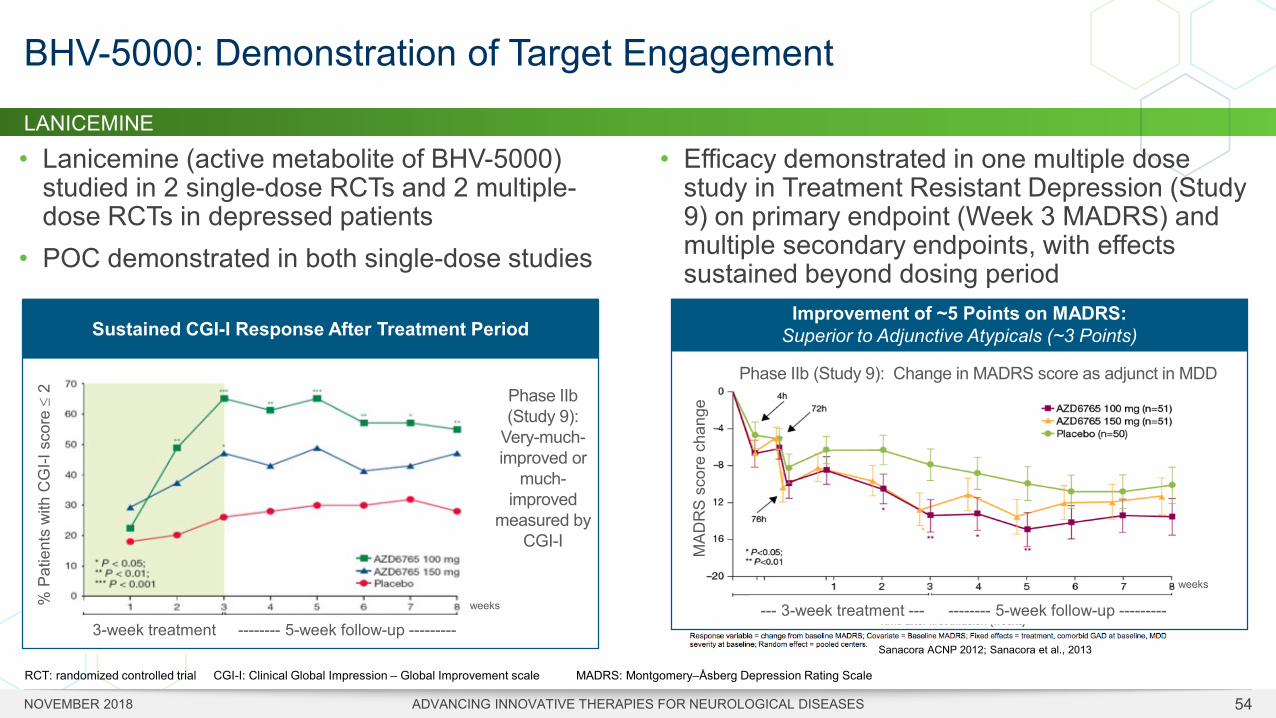
• Lanicemine (active metabolite of BHV-5000) studied in 2 single-dose RCTs and 2 multiple-dose RCTs in depressed patients
• POC demonstrated in both single-dose studies
BHV-5000: Demonstration of Target Engagement
Improvement of ~5 Points on MADRS:Superior to Adjunctive Atypicals (~3 Points)Sustained CGI-I Response After Treatment Period
RCT: randomized controlled trial
• Efficacy demonstrated in one multiple dose study in Treatment Resistant Depression (Study 9) on primary endpoint (Week 3 MADRS) and multiple secondary endpoints, with effects sustained beyond dosing period
% P
atie
nts
with
CG
I-I s
core
≤2
3-week treatment -------- 5-week follow-up ---------
Phase IIb (Study 9):
Very-much-improved or
much-improved
measured by CGI-I
CGI-I: Clinical Global Impression – Global Improvement scale
--- 3-week treatment --- -------- 5-week follow-up ---------
weeks
weeks
Phase IIb (Study 9): Change in MADRS score as adjunct in MDD
MAD
RS
scor
e ch
ange
MADRS: Montgomery–Åsberg Depression Rating Scale
Sanacora ACNP 2012; Sanacora et al., 2013
Glutamate Platform Development Milestones & Next Steps
NOVEMBER 2018 ADVANCING INNOVATIVE THERAPIES FOR NEUROLOGICAL DISEASES 55
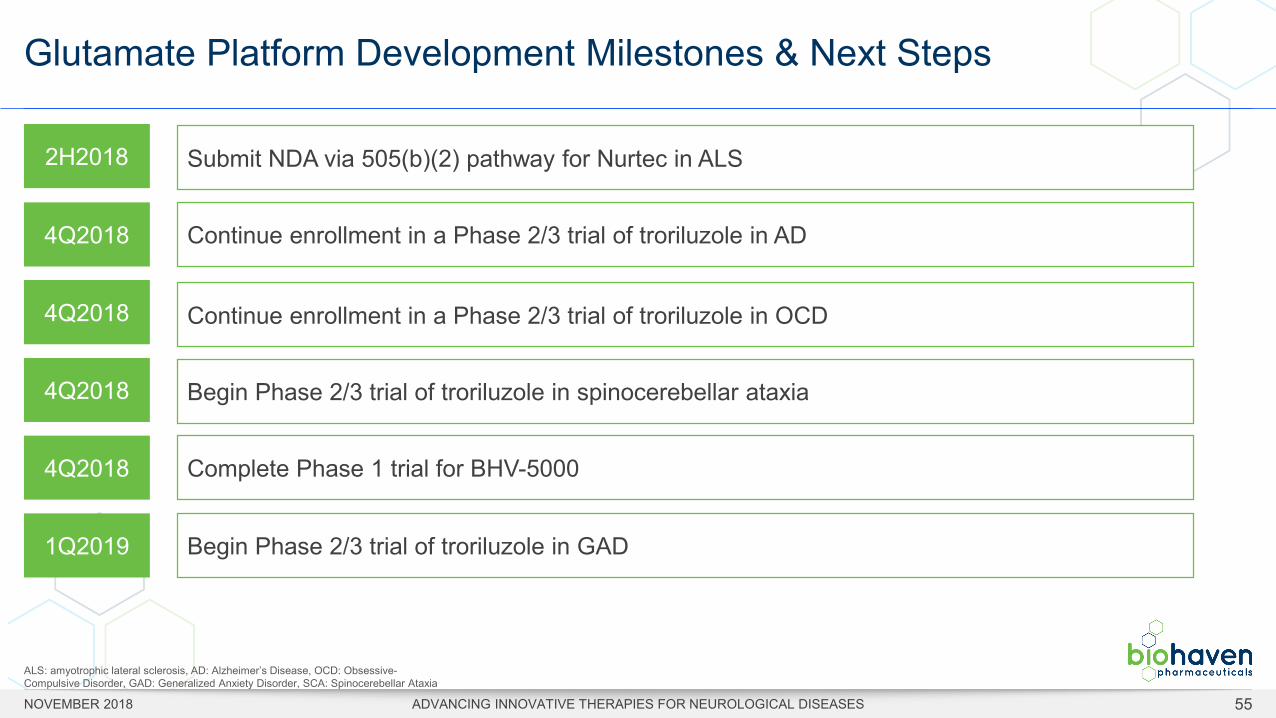
2H2018 Submit NDA via 505(b)(2) pathway for Nurtec in ALS
4Q2018 Continue enrollment in a Phase 2/3 trial of troriluzole in AD
4Q2018 Continue enrollment in a Phase 2/3 trial of troriluzole in OCD
4Q2018 Begin Phase 2/3 trial of troriluzole in spinocerebellar ataxia
4Q2018 Complete Phase 1 trial for BHV-5000
1Q2019 Begin Phase 2/3 trial of troriluzole in GAD
ALS: amyotrophic lateral sclerosis, AD: Alzheimer’s Disease, OCD: Obsessive-Compulsive Disorder, GAD: Generalized Anxiety Disorder, SCA: Spinocerebellar Ataxia

MPO PLATFORMTherapies for Neuroinflammation
BHV-3241
NOVEMBER 2018 ADVANCING INNOVATIVE THERAPIES FOR NEUROLOGICAL DISEASES 57
• Rare, rapidly progressive and fatal neurodegenerative disease • Clinical symptoms:
• Parkinsonism: characteristic tremor (not responsive to L-DOPA), rigidity, dysarthria, falls• Cerebellar ataxia• Autonomic failure: orthostatic hypotension, urinary dysfunction, erectile dysfunction• REM sleep behavior disorder
• Prevalence: 2–5 per 100,000• Pathology: glial cytoplasmic inclusions containing alpha-synuclein• Prognosis: more rapidly progressive than Parkinson’s disease
• Time to loss of ambulation: 3.5–5 years• Mean survival from symptom onset: 6–10 years
• No approved disease modifying treatments• Managed symptomatically
Multiple System Atrophy (MSA)
BHV-3241
NOVEMBER 2018 ADVANCING INNOVATIVE THERAPIES FOR NEUROLOGICAL DISEASES 58
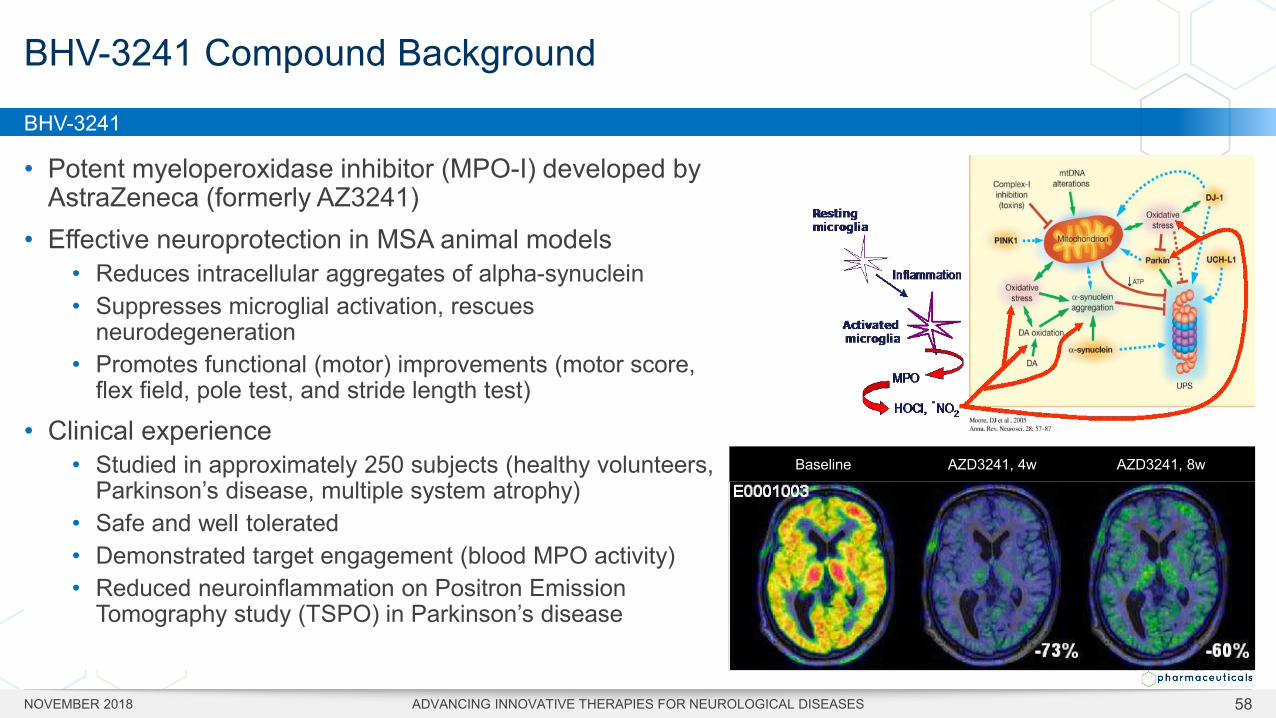
• Potent myeloperoxidase inhibitor (MPO-I) developed by AstraZeneca (formerly AZ3241)
• Effective neuroprotection in MSA animal models• Reduces intracellular aggregates of alpha-synuclein • Suppresses microglial activation, rescues
neurodegeneration • Promotes functional (motor) improvements (motor score,
flex field, pole test, and stride length test)
• Clinical experience• Studied in approximately 250 subjects (healthy volunteers,
Parkinson’s disease, multiple system atrophy)• Safe and well tolerated• Demonstrated target engagement (blood MPO activity)• Reduced neuroinflammation on Positron Emission
Tomography study (TSPO) in Parkinson’s disease
BHV-3241 Compound Background
Baseline AZD3241, 4w AZD3241, 8w
BHV-3241
NOVEMBER 2018 ADVANCING INNOVATIVE THERAPIES FOR NEUROLOGICAL DISEASES 59
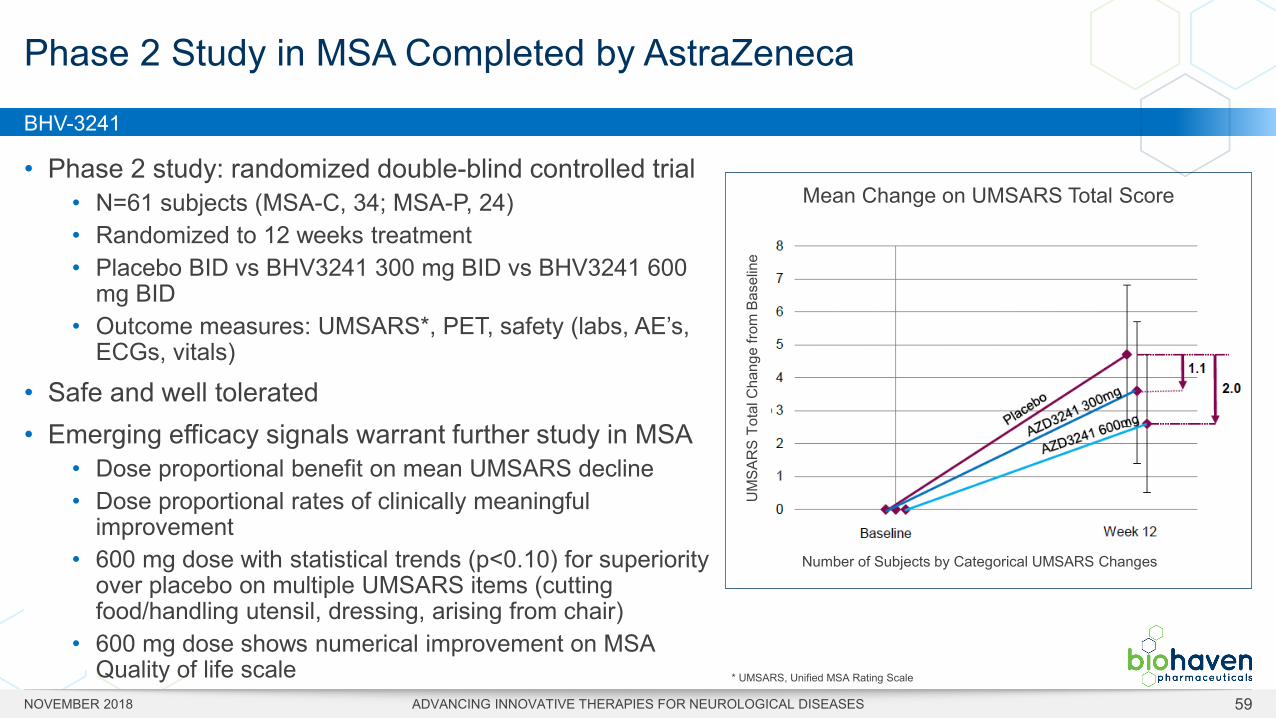
• Phase 2 study: randomized double-blind controlled trial• N=61 subjects (MSA-C, 34; MSA-P, 24)• Randomized to 12 weeks treatment • Placebo BID vs BHV3241 300 mg BID vs BHV3241 600
mg BID• Outcome measures: UMSARS*, PET, safety (labs, AE’s,
ECGs, vitals)
• Safe and well tolerated• Emerging efficacy signals warrant further study in MSA
• Dose proportional benefit on mean UMSARS decline• Dose proportional rates of clinically meaningful
improvement• 600 mg dose with statistical trends (p<0.10) for superiority
over placebo on multiple UMSARS items (cutting food/handling utensil, dressing, arising from chair)
• 600 mg dose shows numerical improvement on MSA Quality of life scale
Phase 2 Study in MSA Completed by AstraZeneca
* UMSARS, Unified MSA Rating Scale
Mean Change on UMSARS Total Score
Number of Subjects by Categorical UMSARS Changes
UM
SAR
S To
tal C
hang
e fro
m B
asel
ine

Driving Investor Value NYSE: BHVN

Biohaven’s Deep Therapeutic, Clinical and Commercial Experience
Robert Berman, M.D.Chief Medical Officer
Jim EngelhartChief Financial Officer
John TiltonChief Commercial Officer
Cliff BechtoldChief Operating Officer
Charlie Conway, Ph.D.Chief Scientific Officer
Robert Croop, M.D.Chief Development Officer —
Neurology
Elyse Stock, M.D.Chief Portfolio Strategy
and Development
Donnie McGrath, M.D. MPHChief of Corporate Strategy and
Business Development
NOVEMBER 2018 ADVANCING INNOVATIVE THERAPIES FOR NEUROLOGICAL DISEASES 61
Vlad Coric, M.D.Chief Executive Officer, Director
PRIOR PROFESSIONAL ROLES
SELECTED DEVELOPMENT EXPERIENCE
Licenses and Intellectual Property
• Founded on intellectual property from Yale University focused on glutamate modulation
• Licensed lanicemine prodrugs from AstraZeneca• Expanded glutamate patent portfolio with licenses from Rutgers, MGH
and ALSBiopharma• Licensed CGRP antagonist program from Bristol-Myers Squibb• Collaboration with Catalent on ZYDIS ODT technology across
glutamate and CGRP antagonist programs• Kleo Pharmaceuticals investment to develop small molecule
immuno-oncology platform
NOVEMBER 2018 ADVANCING INNOVATIVE THERAPIES FOR NEUROLOGICAL DISEASES 62
Financial Summary
IPO on NYSE at $17/share in May 2017
COMPANY OWNERSHIP• Top-tier institutional investors and company founders among
long-term shareholders• $500MM raised since inception
• raised $150M with Royalty Pharma CGRP platform transaction
• Cash on hand as of June 30, 2018 = $217.5M• Top 15 Institutional Investors (38%), Insiders (33%), Other (29%)1
NOVEMBER 2018 ADVANCING INNOVATIVE THERAPIES FOR NEUROLOGICAL DISEASES 631. Data based on latest available information per Thomson and SEC Filings; institutional investor ownership as of 4Q2017
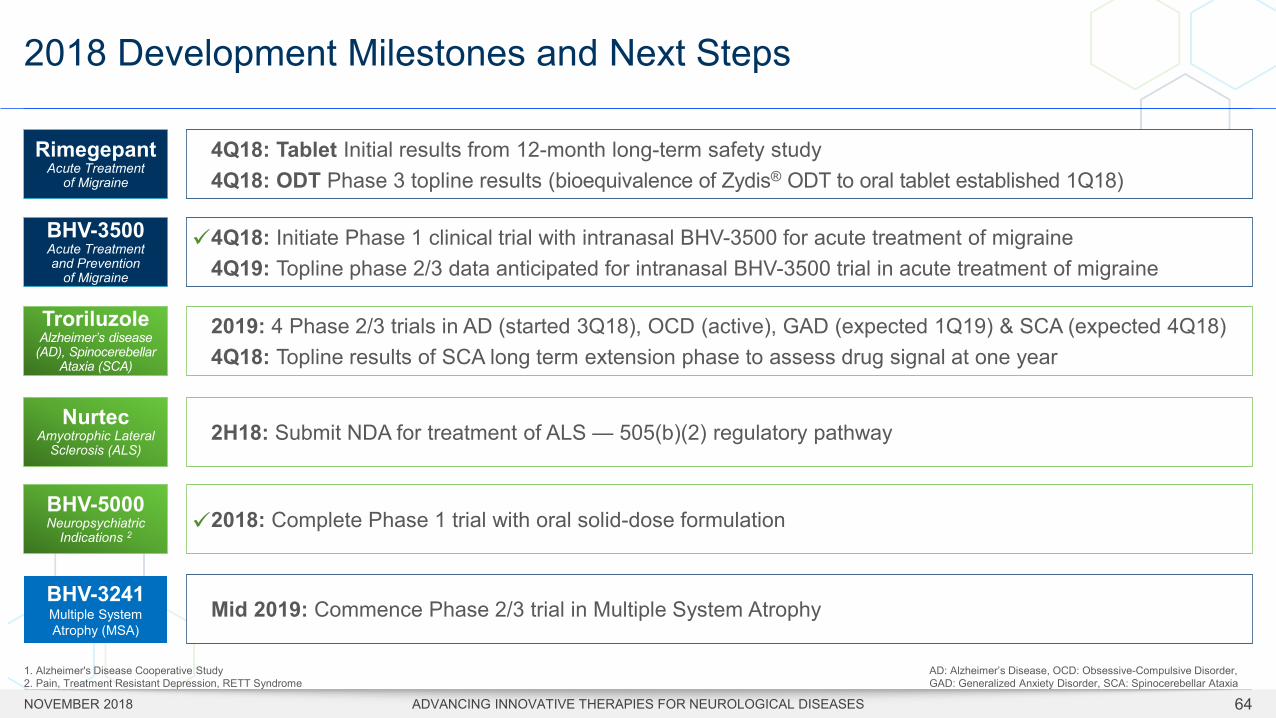
4Q18: Tablet Initial results from 12-month long-term safety study4Q18: ODT Phase 3 topline results (bioequivalence of Zydis® ODT to oral tablet established 1Q18)
RimegepantAcute Treatment
of Migraine
2018: Complete Phase 1 trial with oral solid-dose formulation BHV-5000Neuropsychiatric
Indications 2
4Q18: Initiate Phase 1 clinical trial with intranasal BHV-3500 for acute treatment of migraine4Q19: Topline phase 2/3 data anticipated for intranasal BHV-3500 trial in acute treatment of migraine
BHV-3500Acute Treatment and Prevention
of Migraine
2019: 4 Phase 2/3 trials in AD (started 3Q18), OCD (active), GAD (expected 1Q19) & SCA (expected 4Q18)4Q18: Topline results of SCA long term extension phase to assess drug signal at one year
TroriluzoleAlzheimer’s disease
(AD), Spinocerebellar Ataxia (SCA)
2H18: Submit NDA for treatment of ALS — 505(b)(2) regulatory pathwayNurtec
Amyotrophic Lateral Sclerosis (ALS)
1. Alzheimer's Disease Cooperative Study2. Pain, Treatment Resistant Depression, RETT Syndrome
2018 Development Milestones and Next Steps
NOVEMBER 2018 ADVANCING INNOVATIVE THERAPIES FOR NEUROLOGICAL DISEASES 64
BHV-3241Multiple System Atrophy (MSA)
Mid 2019: Commence Phase 2/3 trial in Multiple System Atrophy
AD: Alzheimer’s Disease, OCD: Obsessive-Compulsive Disorder, GAD: Generalized Anxiety Disorder, SCA: Spinocerebellar Ataxia
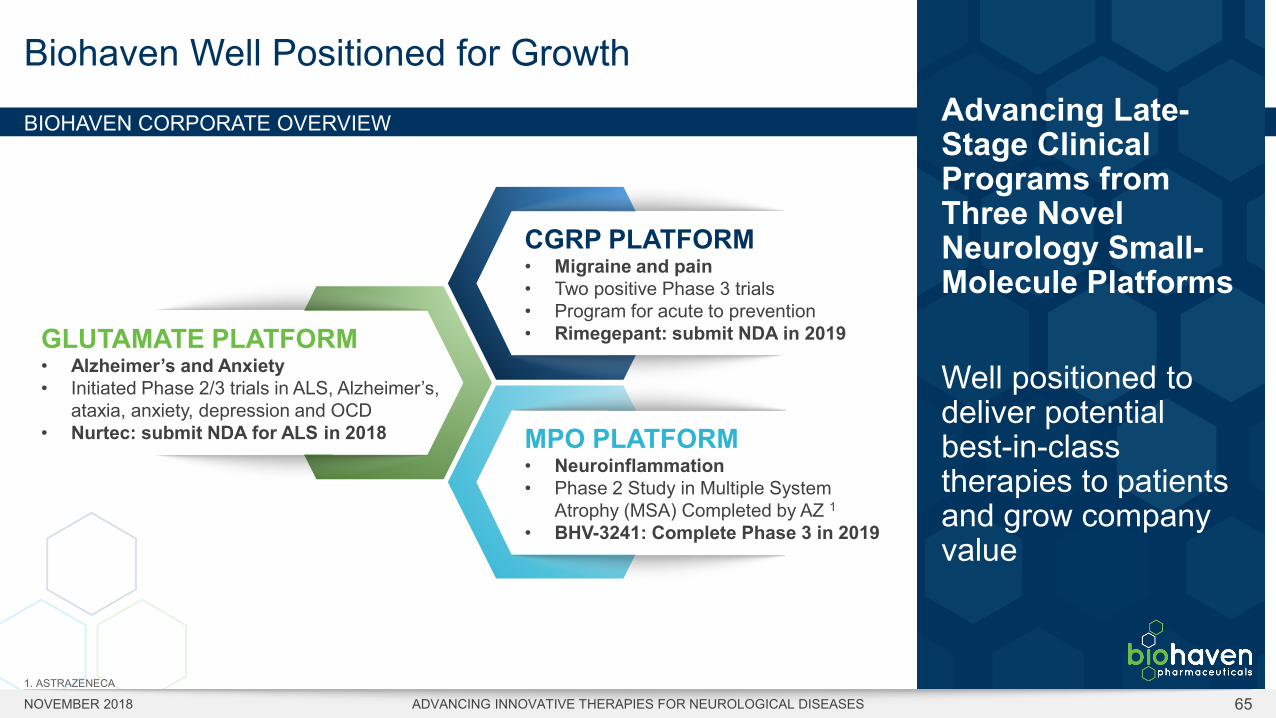
BIOHAVEN CORPORATE OVERVIEW
Biohaven Well Positioned for Growth
NOVEMBER 2018 ADVANCING INNOVATIVE THERAPIES FOR NEUROLOGICAL DISEASES 65
Advancing Late-Stage Clinical Programs from Three Novel Neurology Small-Molecule Platforms
Well positioned to deliver potential best-in-class therapies to patients and grow company value
GLUTAMATE PLATFORM• Alzheimer’s and Anxiety• Initiated Phase 2/3 trials in ALS, Alzheimer’s,
ataxia, anxiety, depression and OCD• Nurtec: submit NDA for ALS in 2018
CGRP PLATFORM• Migraine and pain • Two positive Phase 3 trials• Program for acute to prevention• Rimegepant: submit NDA in 2019
MPO PLATFORM• Neuroinflammation• Phase 2 Study in Multiple System
Atrophy (MSA) Completed by AZ 1• BHV-3241: Complete Phase 3 in 2019
1. ASTRAZENECA

NYSE: BHVN© 2018 Biohaven Pharmaceuticals. All rights reserved.
Thank You!
www.biohavenpharma.com