adverse drug reaction - farmacja.umed.wroc.pl · 1 adverse drug reaction anna wielaanna...
TRANSCRIPT

1
ADVERSE DRUG REACTIONADVERSE DRUG REACTION
Anna WielaAnna Wiela--HojeńskaHojeńska
Ewa JaźwińskaEwa Jaźwińska--TarnawskaTarnawska
Department of Clinical Pharmacology Department of Clinical Pharmacology
Wroclaw Medical UniversityWroclaw Medical University
1
ADVERSE DRUG REACTIONADVERSE DRUG REACTION
as defined by WHO:as defined by WHO:
–– aanyny response to a drug which is response to a drug which is noxiousnoxious and and
unintendedunintended and which occurs at doses used in and which occurs at doses used in
man for prophylaxis, diagnosis or therapy.man for prophylaxis, diagnosis or therapy.
Directive Directive 2010/84/EU2010/84/EU of the of the EuropeanEuropean
ParliamentParliament and of the and of the CouncilCouncil
of 15 of 15 DecemberDecember 20102010amendingamending, as , as regardsregards pharmacovigilancepharmacovigilance, Directive , Directive
2001/83/EC on the 2001/83/EC on the CommunityCommunity codecode relatingrelating to to medicinalmedicinal
products for products for humanhuman useuse
aadversedverse reactionreaction –– noxiousnoxious and and unintendedunintended effectseffects
resultingresulting not not onlyonly for the for the authorisedauthorised useuse of a of a medicinalmedicinal
productproduct atat normalnormal dosesdoses, but , but alsoalso from from medicationmedication errorserrors
and and usesuses outsideoutside the the termsterms of the marketing of the marketing
authorisationauthorisation, , includingincluding the the misusemisuse and and abuseabuse of the of the
medicinalmedicinal productproduct
•• aacutecute
within 60 minuteswithin 60 minutes
•• ssubub--acuteacute
1 to 24 hours1 to 24 hours
•• llatentatent
> 2 days> 2 days
Onset of reactionOnset of reaction
•• mmildild
bothersome but requires no change in bothersome but requires no change in therapytherapy
•• mmoderateoderate
requires change in therapy, additional requires change in therapy, additional treatment, hospitalization treatment, hospitalization
•• ssevereevere
disabling or lifedisabling or life--threateningthreatening
SSeverityeverity of reactionof reaction
-- rresultesult in deathin death
–– llifeife--threateningthreatening
–– rrequireequire hospitalizationhospitalization
–– pprolongrolongeded hospitalizationhospitalization
–– ccauseause disabilitydisability
–– ccauseause congenital anomaliescongenital anomalies
–– medicallymedically significantsignificant
Serious ADRSerious ADR

2
ExamplesExamples of of seriousserious reactionsreactions
BloodBlood: : bonebone marrowmarrow dyscrasiasdyscrasias, ,
coagulopathiescoagulopathies, , haemolitichaemolitic anaemiasanaemias
CardiovascularCardiovascular: : arrhythmiasarrhythmias, ,
cardiaccardiac arrestarrest, , cardiaccardiac failurefailure, ,
hypertensionhypertension
Central Central nervousnervous systemsystem: : depressiondepression, , epilepsyepilepsy, , myastheniamyasthenia
GastrointestinalGastrointestinal: : colitis, colitis, hepatichepatic
cirrhosiscirrhosis, , hepatichepatic dysfunctiondysfunction, , hepatichepatic
fibrosisfibrosis, , pancreatitispancreatitis
ImmunologicaImmunologicall:: anaphylaxisanaphylaxis, , drugdrug
feverfever, , graftgraft tejectiontejection, , vasculitisvasculitis
MetabolicMetabolic: : acidosisacidosis, , adrenaladrenal
dysfunctiondysfunction, , diabetesdiabetes, , hypercalcaemiahypercalcaemia, ,
hyperkalaemiahyperkalaemia, , hypokalaemiahypokalaemia, ,
hyponatraemiahyponatraemia
MusculoskeletalMusculoskeletal: : arthopathyarthopathy, ,
asepticaseptic bonebone necrosisnecrosis, ,
osteomalaciaosteomalacia
RenalRenal: : renalrenal dysfunctiondysfunction, ,
urinaryurinary retentionretention
ReproductionReproduction: : spontaneousspontaneous
abortionabortion, , congenitalcongenital abnormalitiesabnormalities, ,
eclampsiaeclampsia, , infertilityinfertility, , uterineuterine
haemorrhagehaemorrhage//perforationperforation
RespiratoryRespiratory: : bronchospasmbronchospasm, ,
pneumonitispneumonitis, respiratory , respiratory failurefailure, ,
thromboembolismthromboembolism
SkinSkin: : angioedemaangioedema, , bullousbullous
eruptionseruptions, , epidrmalepidrmal necrolysisnecrolysis, ,
exfoliationexfoliation
Special Special sensessenses: : cataractcataract
Classifications of ADRClassifications of ADR
Type:Type:
AA ((AAugmented)ugmented)
BB ((BBizzare)izzare)
CC ((CContinuous)ontinuous)
DD ((DDelayed)elayed)
EE ((EEnding Use)nding Use)
FF ((FFailure of Efficacy)ailure of Efficacy)
Type AType A reactionsreactions
aaugmentedugmented
Type B reactionsType B reactions
bbizzareizzare

3
Type C Reactions Type C Reactions
ccontinuontinuinging
llong term effects are usually related to the ong term effects are usually related to the dosedose and and duration of treatmentduration of treatment
eexamplexampless:: eethambutol thambutol –– optical neuropathyoptical neuropathy, bisphosphonates , bisphosphonates –– osteonecrosisosteonecrosis
Type D reactionsType D reactions
ddelayedelayed
become apparent some time after the use of a medicinebecome apparent some time after the use of a medicine
examples: leucopoenia, which can occur up to six weeks after a dose of lomustineexamples: leucopoenia, which can occur up to six weeks after a dose of lomustine
Type E ReactionsType E Reactions
eend of nd of uusese
associated wassociated withith the withthe withdrawal drawal of a medicineof a medicine
examples: bexamples: barbiturates arbiturates –– restlessness, mental confusion, convulsionrestlessness, mental confusion, convulsion, c, clonidine lonidine –– rebound rebound
hypertensionhypertension, o, opioids pioids –– narcotic withdrawalnarcotic withdrawal, benzodiazepins , benzodiazepins –– insomnia, anxiety, perceptual insomnia, anxiety, perceptual
disturbancesdisturbances
Type F ReactionsType F Reactions
ffailure of ailure of eefficacyfficacy
can be attributed to lack of efficacy of drug productscan be attributed to lack of efficacy of drug products
eexamples:xamples: ffailure to control infection (microbial resistance)ailure to control infection (microbial resistance), u, uncontrolled hypertensionncontrolled hypertension, ,
iintractable painntractable pain
Limitations of Clinical TrialsLimitations of Clinical Trials
•• tootoo small small number of patientsnumber of patients-- averageaverage 1500 patients1500 patientsif a medicine has a risk that only occurs if a medicine has a risk that only occurs onceonce in in every 5.000every 5.000 patients you would patients you would
have to give the medicine to have to give the medicine to 15.00015.000 patients during the trials to be patients during the trials to be reasonably sure of identifying itreasonably sure of identifying it
•• tootoo sstrict trict conditionsconditions -- use patients without complications, use patients without complications,
other medicalother medical conditionsconditions
•• tootoo narrownarrow -- limited indicationslimited indications
•• tootoo brief brief -- limited timelimited time
•• tootoomedianmedian -- very old/very young patients, very old/very young patients,
pregnapregnant nt women not includedwomen not included
Drug administered
Pt develops a new condition/symptoms
Drug suspected?
Yes
Check literature
Documented ?– (for the product or similar class of products)
Yes
Highly suggestive of ADR
Not documented in literature
Drug continued Drug discontinued
Worsening of symptoms Symptoms improve (+ve dechallenge)
Drug restarted
Symptoms recur(+ve rechallenge)
Any other possible causes?• Concomitant therapy• Underlying conditions

4
PharmacovigilancePharmacovigilance
drug safety monitoringdrug safety monitoringWHOWHO
European Medicines AgencyEuropean Medicines Agency
iis the science and activities relating to the s the science and activities relating to the
detectiondetection, , assessmentassessment, , understandingunderstanding and and
preventionprevention of of adverse effectsadverse effects andand other other
medicinemedicine--related problemsrelated problems
The European Union system of pThe European Union system of pharmacovigilanceharmacovigilance
European Medicines Agency, EMA/186974/2012European Medicines Agency, EMA/186974/2012
www.ema.europa.euwww.ema.europa.euNew EU pharmacovigilance legislation New EU pharmacovigilance legislation –– Key conceptsKey concepts
oversees the safety of medicines on the European marketoversees the safety of medicines on the European market
it has been established for a number of yearsit has been established for a number of years
this processes have evolved over timethis processes have evolved over time
The European CommissionThe European Commission has reviewed the current system has reviewed the current system and proposed and proposed new EU pharmacovigilance legislationnew EU pharmacovigilance legislation
This new legislation This new legislation was adoptedwas adopted by the by the European ParliamentEuropean Parliamentand and European CouncilEuropean Council in in December 2010December 2010 and will enter into and will enter into force in force in July 2012July 2012
EMAEMA, together with the , together with the European Member StatesEuropean Member States is responsible is responsible for implementing much of a new legislationfor implementing much of a new legislation
The European Union system of pThe European Union system of pharmacovigilanceharmacovigilance
European Medicines Agency, EMA/186974/2012European Medicines Agency, EMA/186974/2012
www.ema.europa.euwww.ema.europa.euNew EU pharmacovigilance legislation New EU pharmacovigilance legislation –– Key conceptsKey concepts
every country within the European Union has a every country within the European Union has a department department or or agency responsibleagency responsible for for national national pharmacovigilancepharmacovigilance
the reports that the national competent authorities the reports that the national competent authorities receive receive are transferredare transferred to a to a databasedatabase called called EudraVigilanceEudraVigilance and and evaluatedevaluated, together with additional , together with additional sources of information such as sources of information such as clinical trial dataclinical trial data, , medical literaturemedical literature or or data from international regulatorsdata from international regulators, , in order to identify new safety inormationsin order to identify new safety inormations
Aims of drug safety monitoringAims of drug safety monitoring
(pharmacovigilance)(pharmacovigilance)
collection, monitoring, discovering of ADRcollection, monitoring, discovering of ADR
analysisanalysis of all information related to ADR, of all information related to ADR, confirmationconfirmation or or
negationnegation of hypothesis of their occurence, of hypothesis of their occurence, evaluation of riskevaluation of risk
identification of risk factors identification of risk factors and and estimation estimation of probability of their of probability of their
occurrenceoccurrence
determinationdetermination of of increased risk increased risk of ADRof ADR
making decisions making decisions regarding changes in the therapyregarding changes in the therapy
propagationpropagation of information about ADR to physicians, of information about ADR to physicians,
pharmacists, patientspharmacists, patients
Pharmacovigilance by pharmaceutical
companies
www.ema.europa.eu
the company that holds the marketing
authorisation for a medicine has legal
obligations to continuously collect data and
conduct pharmacovigilance
data have to be transmitted to the authorities
within defined timelines, and any emerging
concern about the benefit-risk balance has to
be notified immediately
SPONTANEOUS REPORTINGSPONTANEOUS REPORTING
AdvantagesAdvantages
–– large population/not large population/not
specific pts groupsspecific pts groups
–– all medicinesall medicines
–– hospital and outhospital and out--patient patient
carecare
–– mmay generate rapid alertsay generate rapid alerts
–– lleast likely to influence east likely to influence
prescribing behaviourprescribing behaviour
–– llow setow set--up/costsup/costs
DisadvantagesDisadvantages
–– underreportingunderreporting
–– difficult to detectdifficult to detect
delayed reactionsdelayed reactions
reactions with high reactions with high
background incidencebackground incidence
–– number of exposed number of exposed
unknownunknown
–– biasbias

5
What does the What does the �������� black triangle mean?black triangle mean?
The Black Triangle indicates a medicine The Black Triangle indicates a medicine under under
additional monitoringadditional monitoring, a system to identify , a system to identify
medicines that are being monitored particularly medicines that are being monitored particularly
closely by regulatory authoritiesclosely by regulatory authorities
itit isis assigned toassigned to a medicine if:a medicine if:–– it contains a it contains a new new active substanceactive substance
–– it is a biological medicine, such as a vaccine or a medicine derived from it is a biological medicine, such as a vaccine or a medicine derived from
plasmaplasma
–– it has been given a conditional approval (where the company that it has been given a conditional approval (where the company that
markets the medicine must provide more data about it) or approved markets the medicine must provide more data about it) or approved
under exceptional circumstances (where there are specific reasons wht under exceptional circumstances (where there are specific reasons wht
the company cannot provide a comprehensive set of data)the company cannot provide a comprehensive set of data)
–– the company that markets the medicine is required to carry out additional the company that markets the medicine is required to carry out additional
studiesstudies
List of Black Triangle List of Black Triangle medicinesmedicines
hashas beenbeen publishedpublished by the by the EuropeanEuropean MedicinesMedicines
AgencyAgency
was was firstfirst publishedpublished in in AprilApril 2013 2013 and and willwill be be
reviewedreviewed everyevery monthmonth by the by the
PharmacovigilancePharmacovigilance RiskRisk AssessmentAssessment
CommitteeCommittee (PRAC)(PRAC)
tthe he upup--toto--datedate list of list of medicinesmedicines underunder additionaladditional
monitoring monitoring isis publishedpublished eacheach monthmonth on the on the
MHRAMHRA websitewebsite
mmedicinesedicines willwill be be typicallytypically assignedassigned a Black a Black
Triangle for a period of Triangle for a period of five five yearsyears
If in doubt
Fill a card out!
The The YellowYellow Card Card SchemeSchemeMHRA, http://www.mhra.gov.ukMHRA, http://www.mhra.gov.uk
wwas as introducedintroduced in 1964 in 1964
afterafter thalidomidethalidomide tragedytragedy
highlightedhighlighted the the urgenturgent needneed for for routineroutine
monitoring of monitoring of medicinesmedicines
pprincipallyrincipally actsacts as as anan earlyearly--warningwarning system system for for
identyfyingidentyfying previouslypreviously unrecognisedunrecognised ADRsADRs
pprovidesrovides valuablevaluable informationinformation on on recognisedrecognised
ADRsADRs, , allowingallowing to to identifyidentify and and refinerefine the the
understandingunderstanding of of riskrisk factorsfactors thatthat maymay affectaffect the the
clinicalclinical management of management of patientspatients
What information must I have to What information must I have to
complete a Yellow Card?complete a Yellow Card?
55 critical pieces of information are neededcritical pieces of information are needed::
11. Patient details (anonymised). Patient details (anonymised)
22. Suspect. Suspecteded drugdrug(s) (s)
33. Suspect. Suspecteded reactionreaction(s)(s)
4.4. Other drug(s) (including selfOther drug(s) (including self--medication andmedication and
complementary remedies)complementary remedies)
55. Reporter details. Reporter details
Do not delay reportingDo not delay reporting,,
even if you are in doubt even if you are in doubt
about causalityabout causality

6
ADRsADRs findingsfindings cancan leadlead to to changeschanges in the in the
marketing marketing authorisationauthorisation of the of the medicinemedicine, , suchsuch as:as:
restrictionsrestrictions in in useuse
changeschanges in the in the specified dose specified dose of the medicineof the medicine
introductionintroduction of specific of specific warningswarnings of sideof side--effects effects
in the product informationin the product information
updatingupdating patient information patient information leafletsleaflets (PILs) and (PILs) and
Summaries of Product Characteristics Summaries of Product Characteristics (SPCs)(SPCs)
Yellow Card reports have helped identify:
Year Medicine Adverse Reaction Resulting action or
advice
August 2012 Simvastatin Drug interactions Updated warnings and
contraindications with
maximum dose
recommendations
July 2012 Dabigatran
(Pradaxa)
Serious haemorrhages Contraindications clarified
and reminder to monitor
renal function
April 2012 Proton pomp
inhibitors
Hypomagnesaemia Long-terms use warnings
and measurement of
magnesium levels
December 2011 Citalopram and
escitalopram
QT interval
prolongation
New maximum daily dose
restrictions (including in
elderly patients),
contraindications, and
warnings
SUMMARYSUMMARY
AAnyny drug can produce some form of ADRdrug can produce some form of ADR
Significant untoward risks, costs, and increased Significant untoward risks, costs, and increased
hospital stays associated with ADRshospital stays associated with ADRs
Allergy, Allergy, atopyatopy, or asthma p, or asthma paattientsients have been have been
suggested to be at an increased risksuggested to be at an increased risk
SUMMARY (2)SUMMARY (2)
Antibiotics, blood products, drug preservatives (sulfites Antibiotics, blood products, drug preservatives (sulfites
and methylparabens) and polypeptides (ie, aprotinin, and methylparabens) and polypeptides (ie, aprotinin,
latex, and protamine) may be associated with a higher latex, and protamine) may be associated with a higher
incidence of reactionsincidence of reactions
Drug avoidance whenever possible is still the best Drug avoidance whenever possible is still the best
method to avoid an ADRmethod to avoid an ADR
Undesirable drug interactions Undesirable drug interactions
in clinical practicein clinical practice
Department of Clinical Pharmacology Department of Clinical Pharmacology
Wroclaw Medical UniversityWroclaw Medical University
Criteria for clinical significanceCriteria for clinical significance
of interactionof interaction
hazard of interaction consequenceshazard of interaction consequences –– for for instance, mutual displacement of two drugs instance, mutual displacement of two drugs featuring high therapeutic range from protein featuring high therapeutic range from protein binding seldom leads to dangerous binding seldom leads to dangerous consequences, while the same phenomenon consequences, while the same phenomenon observed in the case of drugs characterized by observed in the case of drugs characterized by narrow therapeutic index is of considerable narrow therapeutic index is of considerable clinical significance (97% of warfarin bounds clinical significance (97% of warfarin bounds with proteins, displacement of merely 3% of the with proteins, displacement of merely 3% of the drug from these bonds increases the effect drug from these bonds increases the effect twice)twice)

7
Criteria for clinical significance Criteria for clinical significance
of interactionof interaction (continuation)(continuation)
the degree of support by documentary evidence of particular interaction in clinical material –– it is important if this it is important if this interaction has been confirmed in patientsinteraction has been confirmed in patients
Criteria for clinical significance Criteria for clinical significance
of interactionof interaction (continuation)(continuation)
the frequency of particular interaction the frequency of particular interaction
in determined population of patientsin determined population of patients
(the factor is very useful for prognosis)(the factor is very useful for prognosis)
Criteria for clinical significance Criteria for clinical significance
of interactionof interaction (continuation)(continuation)
the frequency and degree of interaction the frequency and degree of interaction
documentationdocumentation –– mainly depends on how mainly depends on how
often a determined combination of drugs often a determined combination of drugs
is applied in medical practiceis applied in medical practice
Risk factors increasing the Risk factors increasing the
probability of undesirable interactionprobability of undesirable interaction
ppololypharmacotherapyypharmacotherapy –– the number of the number of
undesired interactions increases proportionally undesired interactions increases proportionally
to the number of drugs prescribed to one to the number of drugs prescribed to one
patient patient (4 or (4 or 5 5 drugs simultaneusly).drugs simultaneusly).
When When more than 5 drugsmore than 5 drugs are used at the same are used at the same
time, the time, the number of interactions increasesnumber of interactions increases, ,
excessing the proportional wayexcessing the proportional way
Risk factors increasing the Risk factors increasing the
probability of undesirable interactionprobability of undesirable interaction(continuation)(continuation)
administration of drugs featuringadministration of drugs featuring
strong effects strong effects andand narrow therapeutic narrow therapeutic
indexindex, , as well asas well as the the drugsdrugs determined determined
as substances thatas substances that potentially potentially
endanger the highest interaction riskendanger the highest interaction risk
Risk factors increasing the Risk factors increasing the
probability of undesirable interactionprobability of undesirable interaction(continuation)(continuation)
thethe useuse ofof drugsdrugs characterizedcharacterized byby nonnon--linearlinear
kineticskinetics,, ee..gg.. ttheophyllineheophylline,, phenytoinphenytoin
coexistence of other diseasescoexistence of other diseases, , especially especially
those disturbing the function of organs those disturbing the function of organs
eliminating drugs, like the liver or/and kidneyseliminating drugs, like the liver or/and kidneys

8
Risk factors increasing the Risk factors increasing the
probability of undesirable interactionprobability of undesirable interaction(continuation)(continuation)
advancedadvanced oror veryvery youngyoung ageage ofof patients,patients,
accompaniedaccompanied byby adequateadequate physiologicalphysiological
differencesdifferences inin thethe functionfunction ofof thethe circulatorycirculatory andand
centralcentral nervousnervous system,system, liver,liver, kidneyskidneys
elderlyelderly patientspatients sufferingsuffering fromfrom manymany diseasesdiseases
andand thereforetherefore takingtaking manymany drugsdrugs atat thethe samesame
timetime,, areare mostmost endangeredendangered byby undesirableundesirable drugdrug
interactionsinteractions
Risk factors increasing the Risk factors increasing the
probability of undesirable interactionprobability of undesirable interaction(continuation)(continuation)
polytherapypolytherapy in critically ill patients taking in critically ill patients taking
many drugs, when the symptoms of the many drugs, when the symptoms of the
disease are difficult to differentiate from disease are difficult to differentiate from
complications resulting from drug therapy complications resulting from drug therapy
which becomes not tolerated by the which becomes not tolerated by the
patientspatients
Risk factors increasing the Risk factors increasing the
probability of undesirable interactionprobability of undesirable interaction(continuation)(continuation)
therapy conducted by several doctorstherapy conducted by several doctors and and
the lack of detailed interview regarding the the lack of detailed interview regarding the
drugs administered previouslydrugs administered previously
takingtaking contraceptivecontraceptive drugsdrugs whichwhich cancan bebe thethe
reasonreason ofof theirtheir interactioninteraction withwith thethe drugsdrugs usedused
atat thethe samesame timetime
Risk factors increasing the Risk factors increasing the
probability of undesirable probability of undesirable
interactioninteraction
drug advertisingdrug advertising in mass mediain mass media
general accessibility of drugsgeneral accessibility of drugs, , especially especially
those fromthose from OTCOTC ((OOver ver TThe he CCounter) ounter) group, group,
sold without doctor’s prescriptionsold without doctor’s prescription
dangerous phenomenon of dangerous phenomenon of patients’ patients’ selfself--
treatmenttreatment
Consequences of drug interactionsConsequences of drug interactions
Decrease in pharmacological drug effect Decrease in pharmacological drug effect
by:by:
pharmacodynamic antagonism,pharmacodynamic antagonism,
reduced absorption (decrease in reduced absorption (decrease in
bioavailability),bioavailability),
induction of metabolic processes,induction of metabolic processes,
increased excretion.increased excretion.
Consequences of drug interactionsConsequences of drug interactions
Increase in pharmacological drug effect Increase in pharmacological drug effect
by:by:
pharmacodynamic synergism,pharmacodynamic synergism,
displacement of drugs from protein displacement of drugs from protein
binding,binding,
inhibition of metabolic processes,inhibition of metabolic processes,
decreased excretion.decreased excretion.

9
Drug absorption interactions Drug absorption interactions
after oral administrationafter oral administration
changes in gastrointestinal pHchanges in gastrointestinal pH
adsorbtion, chelation, complexes formation, adsorbtion, chelation, complexes formation,
malabsorption syndromemalabsorption syndrome
changes in gastrointestinal motilitychanges in gastrointestinal motility
inhibiting activity of CYP3A cytochrom P450 inhibiting activity of CYP3A cytochrom P450
enzymes responsible for metabolism of the first enzymes responsible for metabolism of the first
passage in the intesine wallpassage in the intesine wall
Inhibiting activity of CYP3A cytochrome Inhibiting activity of CYP3A cytochrome
P450 enzymes responsible for the first P450 enzymes responsible for the first
pass metabolism in the intestine wallpass metabolism in the intestine wallThe components of The components of grapefruit grapefruit (naringenine, (naringenine, dihydroksybergamotine) inhibiting activity of CYP3A4 dihydroksybergamotine) inhibiting activity of CYP3A4 cytochrome P450 isoenzyme cytochrome P450 isoenzyme –– increase absorption increase absorption from intestines of from intestines of calcium channel blockerscalcium channel blockers((nifedipine, felodipine, isradipine, lacidipine, nifedipine, felodipine, isradipine, lacidipine, lercanidipine, nicardipine, nimodipine, verapamil), lercanidipine, nicardipine, nimodipine, verapamil), immunosuppressantsimmunosuppressants (cyclosporine, sirolimus, (cyclosporine, sirolimus, tacrolimus), tacrolimus), entocort which contains budesonide for entocort which contains budesonide for Crohn’s diseasCrohn’s diseas, , statinsstatins ((simvastatin, atorvastatinsimvastatin, atorvastatin), ), medicines used in the tratment of cancerousmedicines used in the tratment of cancerous((crizotinib, lapatinib, linotinib, sunitinibcrizotinib, lapatinib, linotinib, sunitinib, , everolimuseverolimus), ), aliskiren aliskiren which is used to which is used to treat high blood pressuretreat high blood pressure ––drugs undergoing first pass metabolism in the drugs undergoing first pass metabolism in the intestinal wallintestinal wall
amlodipine and grepefruit interactionamlodipine and grepefruit interaction
a male patient drank a male patient drank grapefrit juicegrapefrit juice three times three times
a day whilst taking a day whilst taking amlodipineamlodipine, prescribed for , prescribed for
high blood pressure, reported high blood pressure, reported severe swelling severe swelling
to his legs and feetto his legs and feet
the swelling resolved when he stoped drinking the swelling resolved when he stoped drinking
grapefruit juicegrapefruit juice
Drug transport interaction by cell membranes. Drug transport interaction by cell membranes.
Drugs effects on PDrugs effects on P--glicoprotein activity (Pglicoprotein activity (P--gp)gp)
PP--glycoproteinglycoprotein is a largeis a large--molecule protein molecule protein
detected in cell membranes of different detected in cell membranes of different
organs, which, by active transport organs, which, by active transport
(„pump”) push drugs out of the cells, („pump”) push drugs out of the cells,
preventing their accumulation.preventing their accumulation.
Induction of PInduction of P--gp activitygp activity
RifampicinRifampicin can inducecan induce PP--gp activity in gp activity in
intestinal epithelium cells, increasing the intestinal epithelium cells, increasing the
elimination of digoxin to the intestine elimination of digoxin to the intestine
lumen, what causes the decrease of its lumen, what causes the decrease of its
concentration in blood serum concentration in blood serum
Inhibition of PInhibition of P--gp activitygp activity
CiclosporinCiclosporin inhibits Pinhibits P--gp activity within gp activity within
the kidney tubule cells so that the amount the kidney tubule cells so that the amount
of digoxin pushed out into urine is of digoxin pushed out into urine is
reduced, therefore causing a rise in reduced, therefore causing a rise in
plasma digoxin levelsplasma digoxin levels

10
Drug displacement (proteinDrug displacement (protein--binding) binding)
interactionsinteractions
Drugs of high affinity to blood proteins, soDrugs of high affinity to blood proteins, so--
called „called „displacing drugsdisplacing drugs" " –– the compounds of the compounds of
acidic propertiesacidic properties –– acetylsalicylic acid, acetylsalicylic acid,
ibuprofen, diclofenac, phenylbutazone, some ibuprofen, diclofenac, phenylbutazone, some
sulfonamides, chloral hydrate, trichloroacetic sulfonamides, chloral hydrate, trichloroacetic
acid, clofibrate, ethacrynic acid, quinidine, acid, clofibrate, ethacrynic acid, quinidine,
verapamil, amiodaroneverapamil, amiodarone
Drug metabolism interactionsDrug metabolism interactionsSubstances inhibiting metabolism of other drugs, Substances inhibiting metabolism of other drugs,
soso--calledcalled „„enzyme inhibitorsenzyme inhibitors”:”:
–– allopurinol allopurinol
–– amiodarone amiodarone
–– qunidine qunidine
–– chloramphenicol chloramphenicol
–– cimetidine cimetidine
–– ciprofloxacin ciprofloxacin
–– diltiazem diltiazem
–– disulfiram disulfiram
–– enoxacinenoxacin
–– erythromycin erythromycin
–– phenylbutazone phenylbutazone
–– fluconazolefluconazole
__-- fluoxetinefluoxetine
–– isoniazidisoniazid
–– indynavirindynavir
–– ketoconazole ketoconazole
–– clarithromycin clarithromycin
–– omeprazoleomeprazole
–– metronidazolemetronidazole
–– rytonavirrytonavir
–– sulfinpyrazone sulfinpyrazone
–– verapamil verapamil
–– alcohol once in high amountalcohol once in high amount
–– grapefruit juicegrapefruit juice
warfarin and cranberry juice interactionwarfarin and cranberry juice interaction
warfarin warfarin + + cranberry juicecranberry juice
interaction interaction -- ↑↑ International Normalised Ratio International Normalised Ratio
(INR), (INR), bleeding bleeding episodesepisodes
Cranberry juice Cranberry juice contains various antioxidants contains various antioxidants
including flavinoid, which inhibit CYP2C9, including flavinoid, which inhibit CYP2C9,
enzyme used to metabolise warfarin enzyme used to metabolise warfarin
Drug metabolism interactionsDrug metabolism interactions
Substances inducing metabolism of other drugs, Substances inducing metabolism of other drugs,
soso--called called „„enzyme inductorsenzyme inductors”:”:
barbiturates, especially phenobarbital barbiturates, especially phenobarbital
aminoglutethimide aminoglutethimide
carbamazepinecarbamazepine
phenytoin phenytoin
rifampicin rifampicin
griseofulvin griseofulvin
preparations of St. John’s wortpreparations of St. John’s wort (Hypericum (Hypericum perforatum)perforatum)
alcoholalcohol abused for a long timeabused for a long time
carbohydrates present in tobacco smokecarbohydrates present in tobacco smoke
Drug excretion interactionsDrug excretion interactions
changes in urinary pH changes in urinary pH
changes in active kidney tubule excretionchanges in active kidney tubule excretion
changes in kidney blood flowchanges in kidney blood flow
Drugs most commonly causing adverse Drugs most commonly causing adverse effects of interactionseffects of interactions
anticoagulantsanticoagulants
antidiabeticsantidiabetics
nonsteroidal antinonsteroidal anti--inflammatory drugs (NSAIDs)inflammatory drugs (NSAIDs)
drugs used in the diseases of circulatory systems, like: drugs used in the diseases of circulatory systems, like: cardiac insufficiency, cardiac ischemia, arterial cardiac insufficiency, cardiac ischemia, arterial hypertension, allorhythmia, (especially cardiac hypertension, allorhythmia, (especially cardiac glycosides, betaglycosides, beta--adrenolytic drugs, diuretics, adrenolytic drugs, diuretics, angiotensin converting enzyme inhibitors, antagonists , antagonists of angiotensin II receptors, calcium canal blockers, of angiotensin II receptors, calcium canal blockers, antiarrhythmic drugs, dilatators of peripheral vesselsantiarrhythmic drugs, dilatators of peripheral vessels––nitrates),nitrates),
hypolipemic drugshypolipemic drugs
antibacterial, antiviral and antifungal drugsantibacterial, antiviral and antifungal drugs
11
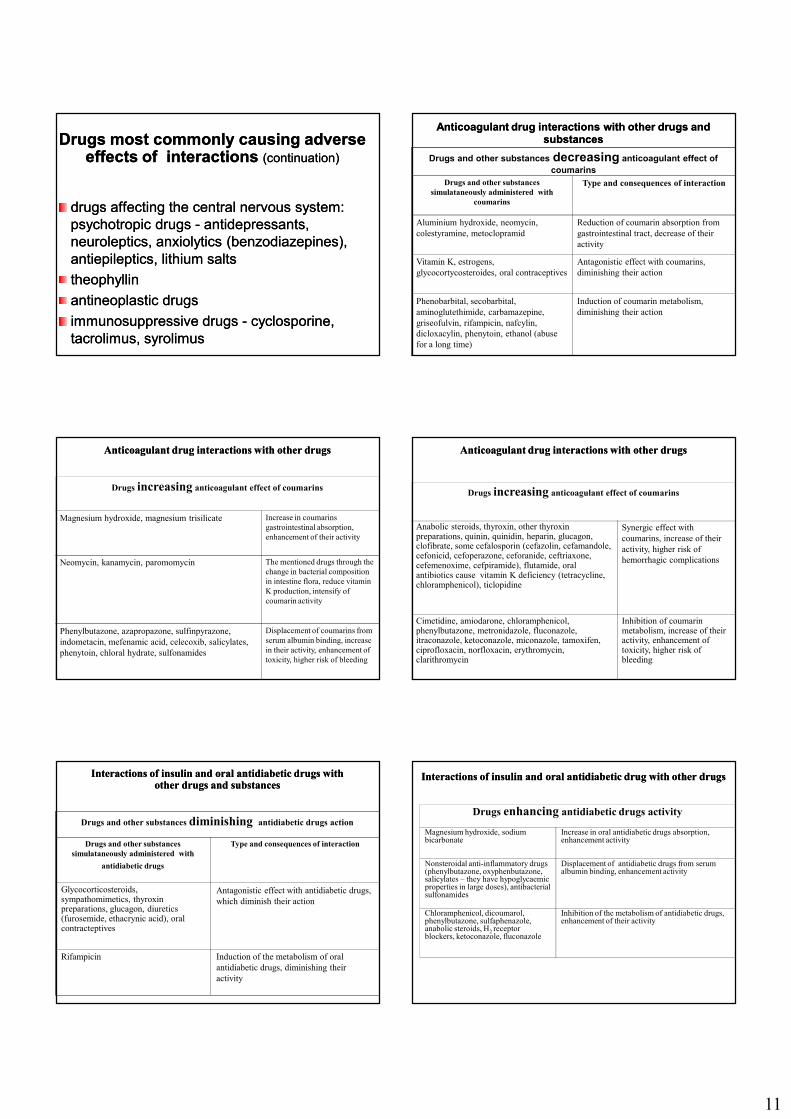
Drugs most commonly causing adverse Drugs most commonly causing adverse effects of interactions effects of interactions (continuation)(continuation)
drugs affecting the central nervous system: drugs affecting the central nervous system:
psychotropic drugs psychotropic drugs -- antidepressants, antidepressants,
neuroleptics, anxiolytics (benzodiazepines), neuroleptics, anxiolytics (benzodiazepines),
antiepileptics, lithium saltsantiepileptics, lithium salts
theophyllintheophyllin
antineoplastic drugsantineoplastic drugs
immunosuppressive drugs immunosuppressive drugs -- cyclosporine, cyclosporine,
tacrolimus, syrolimus tacrolimus, syrolimus
Anticoagulant drugAnticoagulant drug interactionsinteractions with other drugs and with other drugs and substancessubstances
Drugs and other substances decreasing anticoagulant effect ofcoumarins
Drugs and other substances
simulataneously administered with
coumarins
Type and consequences of interaction
Aluminium hydroxide, neomycin,
colestyramine, metoclopramid
Reduction of coumarin absorption from
gastrointestinal tract, decrease of their
activity
Vitamin K, estrogens,
glycocortycosteroides, oral contraceptives
Antagonistic effect with coumarins,
diminishing their action
Phenobarbital, secobarbital,
aminoglutethimide, carbamazepine,
griseofulvin, rifampicin, nafcylin,
dicloxacylin, phenytoin, ethanol (abuse
for a long time)
Induction of coumarin metabolism,
diminishing their action
Anticoagulant drugAnticoagulant drug interactions with other drugs interactions with other drugs
Drugs increasing anticoagulant effect of coumarins
Magnesium hydroxide, magnesium trisilicate Increase in coumarins
gastrointestinal absorption,
enhancement of their activity
Neomycin, kanamycin, paromomycin The mentioned drugs through the
change in bacterial composition
in intestine flora, reduce vitamin
K production, intensify of
coumarin activity
Phenylbutazone, azapropazone, sulfinpyrazone,
indometacin, mefenamic acid, celecoxib, salicylates,
phenytoin, chloral hydrate, sulfonamides
Displacement of coumarins from
serum albumin binding, increase
in their activity, enhancement of
toxicity, higher risk of bleeding
Anticoagulant drugAnticoagulant drug interactions with other drugsinteractions with other drugs
Drugs increasing anticoagulant effect of coumarins
Anabolic steroids, thyroxin, other thyroxin preparations, quinin, quinidin, heparin, glucagon, clofibrate, some cefalosporin (cefazolin, cefamandole, cefonicid, cefoperazone, ceforanide, ceftriaxone, cefemenoxime, cefpiramide), flutamide, oral antibiotics cause vitamin K deficiency (tetracycline, chloramphenicol), ticlopidine
Synergic effect with
coumarins, increase of their
activity, higher risk of
hemorrhagic complications
Cimetidine, amiodarone, chloramphenicol, phenylbutazone, metronidazole, fluconazole, itraconazole, ketoconazole, miconazole, tamoxifen, ciprofloxacin, norfloxacin, erythromycin, clarithromycin
Inhibition of coumarinmetabolism, increase of theiractivity, enhancement of toxicity, higher risk of bleeding
Interactions of iInteractions of insulin nsulin andand oral antidiabetic drugsoral antidiabetic drugs with with other drugs and substancesother drugs and substances
Drugs and other substances diminishing antidiabetic drugs action
Drugs and other substances
simulataneously administered with
antidiabetic drugs
Type and consequences of interaction
Glycocorticosteroids, sympathomimetics, thyroxin preparations, glucagon, diuretics(furosemide, ethacrynic acid), oral contracteptives
Antagonistic effect with antidiabetic drugs,
which diminish their action
Rifampicin Induction of the metabolism of oral
antidiabetic drugs, diminishing their
activity
InteractionsInteractions of of iinsulinnsulin andand oral antidiabetic drugoral antidiabetic drug with other drugswith other drugs
Drugs enhancing antidiabetic drugs activity
Magnesium hydroxide, sodium bicarbonate
Increase in oral antidiabetic drugs absorption, enhancement activity
Nonsteroidal anti-inflammatory drugs(phenylbutazone, oxyphenbutazone, salicylates – they have hypoglycaemicproperties in large doses), antibacterial sulfonamides
Displacement of antidiabetic drugs from serum albumin binding, enhancement activity
Chloramphenicol, dicoumarol, phenylbutazone, sulfaphenazole, anabolic steroids, H2 receptor blockers, ketoconazole, fluconazole
Inhibition of the metabolism of antidiabetic drugs, enhancement of their activity

12
InteractionsInteractions of of iinsulinnsulin and and oral antidiabetic drugoral antidiabetic drug with other drugswith other drugs
Drugs enhancing antidiabetic drugs activity
Beta-adrenolytic drugs(propranolol)
Synergic effect with antidiabetic drugs, enhancement of their activity
Salicylates, allopurinol Displacement of antidiabetic drugs from kidney tubular transport systems
�SAIDs�SAIDs phphaarmacodynamicrmacodynamic iinteraction nteraction of highest clinical significanceof highest clinical significance
Drugs and other substances simultaneously administered with
�SAIDs
Type and consequences of interaction
Hypotensive drugs (beta-adrenolytics, angiotensin converting enzyme inhibitors, diuretics)
Reduction of hypotensive effect of these drugs due to increase in synthesis of vasodilatory prostaglandins by NSAIDs
Anticoagulant drugs (coumarin derivatives)
Higher risk of bleeding from gastrointestinal tract due to inhibition of platelets activity and prothrombin synthesis
Antidiabetic drugs Intensification of hypoglycemic activity by hypoglycemic action of some of NSAIDs
Fluoroquinolones Intensification of toxic effect on CNS
Cyclosporine, tacrolimus, angiotensin converting enzyme inhibitors
Enhancement of nephrotoxicity by NSAIDs
Lithium carbonate Enhancement of toxicity by NSAIDs
Alcohol Higher risk of bleeding from gastrointestinal tract
Thrombocyte aggregation inhibitors(ticlopidine, clopidogrel)
Higher risk of bleeding, synergic effect
�SAIDs�SAIDs pharmacokinetic interactionspharmacokinetic interactions
oof highest clinical significancef highest clinical significance
Drugs simultaneously administered with �SAIDs
Type and consequences of interaction
Anticoagulant drugs(coumarin derivatives)
Higher risk of bleeding from gastrointestinal tract due tocoumarins displacement from blood protein binding
Antidiabetic drugs (oral, especially sulphonylureas derivatives)
Enhancement of hypoglicemic activity, by displacement ofantidiabetic drugs from blood protein binding and inhibition oftheir metabolism
Methotrexate Enhancement of methotrexate toxicity as a result of its displacement from protein binding and impairment of renal tubular secretion of this drug
Cardiac drugs (digoxin) Increase in digoxin concentration as a result of its displacementfrom protein binding and reduction of kidney excretion, leading to intensification of its activity and causing risk of adverse effects
�SAIDs�SAIDs phpharmaarmaccookkinetinetiic ic interactionsnteractions
of highest clinical significanceof highest clinical significance
Drugs simultaneously administered with �SAIDs
Type and consequences of interaction
Aminoglycosides Increase in aminoglycosides concentration in serum leading to higher risk of adverse effects due to inhibition of their glomerular filtration, enhancement of oto- andnephrotoxicity
Drugs affecting CNS(phenytoin, valproic acid)
Increase in phenytoin and valproic acid concentration due to inhibition of their metabolism and their displacement fromblood protein binding
Corticosteroids Increase in cortycosteroids concentration due to decrease in their renal excretion, gastropathy, bleeding from gastrointestinal tract
Tricyclic antidepressants,selective serotonin reuptake inhibitors, neuroleptics, antiarrhythmic drugs
Increase in activity as a result of metabolism inhibition of the mentioned drugs by NSAIDs (celecoxib)
Cardiac Cardiac glglycycoosisiddeses interactioninteraction with other drugs and substanceswith other drugs and substances
Drugs and substances simultaneously
administered with cardiac glicosidesType and consequences of
interaction
Hypercalcemia: calcium compounds
Hypokalemia: diuretics (furosemide, etacrynic
acid), indapamide, glicocorticosteroids, laxatives,
amphotericin B, polymyxins
Enhancement of cardiac glycosides
activity and their arrhythmogenic effect
Hyperkalemia: potassium compounds
Hypokalcemia: sodium versenate, sodium citrate
Reduction of cardiac glycosides activity
Epinephrine, norepinephrine, reserpine,
monoamine oxidase inhibitors (MAOI)
Possibility of cardiac arrhythmia
Cardiac glycosidesCardiac glycosides interactions with other drugs and substancesinteractions with other drugs and substances
Drugs and substances simultaneously
administered with cardiac glycosidesType and consequences of
interaction
Drugs diminishing digoxin absorption from
gastrointestinal tract: activated charcoal,
metoclopramide, colestyramine, colestipol,
neomycin, sulphasalazine, aminosalicylic acid
Reduction of digoxin activity
Drugs stimulating cardiac glycosides
biotransformation: phenobarbital, phenylbutazone,
rifampicin, phenytoin, St. John’s wort (Hypericum
perforatum)
Reduction of cardiac glycosides activity
Drugs increasing plasma digoxin concentration:
verapamil, diltiazem, niphedypine, quinidine, amiodarone, indomethacin, spironolactone, trimethoprim, gentamicin, cefradine, tetracycline, erythromycin, clarithromycin, propafenone, cyclosporine, itraconazole
Decrease in digoxin renal clearance, inhibition of P-glicoprotein activityresponsible for renal and intestinal digoxin transport, intensification of digoxin activity

13
BetaBeta--adrenolytic drugadrenolytic drug interactionsinteractions with other drugs with other drugs
BetaBeta--adrenolytic adrenolytic
drugs (DBA)drugs (DBA)
Simultaneously administered Simultaneously administered
other drugs other drugs
Type and consequences of interaction
Lipofilic DBA Lipofilic DBA
(propranolol, (propranolol,
metoprolol)metoprolol)
Quinidine, amiodarone, Quinidine, amiodarone,
propafenone, encainide, propafenone, encainide,
flecainide, hydralazineflecainide, hydralazine
InhibitionInhibition of DBA of DBA metabolismmetabolism, increase , increase
in DBA blood concentration, hypotonia, in DBA blood concentration, hypotonia,
bradycardia, ventricular arrhythmiasbradycardia, ventricular arrhythmias
TimololTimolol Quinidine, cimetidineQuinidine, cimetidine IncreaseIncrease in cardiac action frequency, in cardiac action frequency,
reduction of intraocular pressurereduction of intraocular pressure
PropranololPropranolol Propafenone, lidocainePropafenone, lidocaine IncreaseIncrease in propafenone, lidocaine in propafenone, lidocaine
bioavailabilitybioavailability, enhancement their , enhancement their
activityactivity
MetoprololMetoprolol PropafenonePropafenone InhibitionInhibition of metoprolol of metoprolol metabolismmetabolism, ,
increase in metoprolol concentration, increase in metoprolol concentration,
enhancement activity (hypotonia, enhancement activity (hypotonia,
bradycardia)bradycardia)
BetaBeta--adrenolytic drugadrenolytic drug interactionsinteractions with other drugs with other drugs
BetaBeta--adrenolytic adrenolytic
drugs (DBA)drugs (DBA)
Simultaneously Simultaneously
administered other drugs administered other drugs
Type and consequences of
interaction
Metoprolol, Metoprolol,
carvedilol, carvedilol,
propranolol, propranolol,
timololtimolol
Antidepressive drugs: Antidepressive drugs:
amitriptyline, nortriptyline, amitriptyline, nortriptyline,
fluoxetinefluoxetine
InhibitionInhibition of DBA of DBA metabolismmetabolism, ,
increase in DBA activity, hypotoniaincrease in DBA activity, hypotonia
DBA (acebutolol, DBA (acebutolol,
atenolol,esmolol, atenolol,esmolol,
metoprolol, metoprolol,
timolol)timolol)
AlphaAlpha--adrenolytic drugs: adrenolytic drugs:
prazosin, doxazosinprazosin, doxazosin
Orthostatic hypotoniaOrthostatic hypotonia
Propranolol, Propranolol,
labetalollabetalol
ClonidineClonidine Rebound hypertension after clonidine Rebound hypertension after clonidine
discontinuationdiscontinuation
DBADBA Werapamil, diltiazemWerapamil, diltiazem EnhancementEnhancement of negative dromothropic of negative dromothropic
effect the mentioned drugs, Aeffect the mentioned drugs, A--V block, V block,
hypotoniahypotonia
BetaBeta--adrenolytic drugadrenolytic drug interactionsinteractions with other drugs with other drugs
BetaBeta--adrenolytic adrenolytic
drugs (DBA)drugs (DBA)
Simultaneously Simultaneously
administered other drugs administered other drugs
Type and consequences of
interaction
DBADBA DigoxinDigoxin Enhancement Enhancement of depressive influence of depressive influence
the mentioned drugs on cardiac impulsthe mentioned drugs on cardiac impuls--
conductive system, bradycardia, conductive system, bradycardia,
impairments of transmissionimpairments of transmission
DBA DBA Indomethacin, acetylsalicylic Indomethacin, acetylsalicylic
acidacid
InhibitionInhibition of prostaglandins synthesis, of prostaglandins synthesis,
increase in DBA hypotensive effectincrease in DBA hypotensive effect
PropranololPropranolol Oral hypoglycaemic drugsOral hypoglycaemic drugs InhibitionInhibition of insulin secretion, of insulin secretion,
reduction of insulinreduction of insulin--susceptibility susceptibility
tissues, worsening of diabetes tissues, worsening of diabetes
metabolic control, masking of metabolic control, masking of
hypoglycaemic symptoms by DBA, hypoglycaemic symptoms by DBA,
higher risk of hypoglycaemiahigher risk of hypoglycaemia
DiureticDiuretic interactionsinteractions with other drugs with other drugs
DiureticDiuretic Simultaneously administered Simultaneously administered
other drugs other drugs
Type and consequences of interaction
Loop diuretics Loop diuretics
(furosemide, (furosemide,
ethacrynic acid)ethacrynic acid)
Aminoglycosides, Aminoglycosides,
cephalosporinscephalosporins
IncreaseIncrease in aminoglycosides, in aminoglycosides,
cephalosporins cephalosporins nephrotoxicitynephrotoxicity, ,
aminoglycosides aminoglycosides otoxicityotoxicity
Amiloride Amiloride CiclosporinCiclosporin IncreaseIncrease in ciclosporin in ciclosporin nephrotoxicitynephrotoxicity
AmilorideAmiloride QuinidineQuinidine QT interval prolonging effects, QT interval prolonging effects, enhanced enhanced
proarythmic quinidine activityproarythmic quinidine activity, ,
ventricular tachycardia episodes of ventricular tachycardia episodes of
torsade de pointestorsade de pointes typetype
IndapamideIndapamide Quinidine, disopyramide, Quinidine, disopyramide,
amiodarone, bretylium, sotalol, amiodarone, bretylium, sotalol,
bepridil, erythromycin, bepridil, erythromycin,
pentamidinepentamidine
QT interval prolonging effects, QT interval prolonging effects,
ventricular tachycardia episodes of ventricular tachycardia episodes of
torsade de pointestorsade de pointes typetype
Diuretic Diuretic interactionsinteractions with other drugs with other drugs
DiureticDiuretic Simultaneously administered Simultaneously administered
other drugs other drugs
Type and consequences of interaction
FurosemideFurosemide Valproic acidValproic acid
PhenytoinPhenytoin
Displacement Displacement of furosemide of furosemide from proteinfrom protein
bindingbinding, increase in furosemide , increase in furosemide
concentration, enhancement its diuretic concentration, enhancement its diuretic
activityactivity
DecreaseDecrease in furosemide in furosemide diuretic activitydiuretic activity
Loop diuretics Loop diuretics
(furosemide, (furosemide,
torasemide, torasemide,
bumetanide)bumetanide)
NSAIDs NSAIDs –– indometacin, indometacin,
diclofenac, piroxicam, diclofenac, piroxicam,
naproxen, acetylsalicylic acidnaproxen, acetylsalicylic acid
Decrease in diuretic effectDecrease in diuretic effect
IndapamideIndapamide Indometacin, tienilic acidIndometacin, tienilic acid Acute renal insufficiencyAcute renal insufficiency
Interactions ofInteractions of angiotensin converting enzyme angiotensin converting enzyme
(ACE) inhibitors (ACE) inhibitors with other drugs with other drugs
and substancesand substances
Angiotensin Angiotensin
converting enzyme converting enzyme
(ACE) inhibitors(ACE) inhibitors
Simultaneously administered Simultaneously administered
other drugs other drugs
and substances and substances
Type and consequences of interaction
Captopril, enalapril, Captopril, enalapril,
lisinopril, lisinopril,
perindopril perindopril
NSAIDs (acetylosalicylic acid, NSAIDs (acetylosalicylic acid,
indometacin, naproxen)indometacin, naproxen)
ReductionReduction of hypotensive action, of hypotensive action,
hemodynamic effects of ACE inhibitorshemodynamic effects of ACE inhibitors
ACE inhibitors ACE inhibitors Hypoglycaemic agentsHypoglycaemic agents DecreaseDecrease in glucose blood concentration in glucose blood concentration
in patients with diabetesin patients with diabetes
CaptoprilCaptopril General anesthetic agentsGeneral anesthetic agents ExcessiveExcessive reduction of blood pressurereduction of blood pressure
ACE inhibitorsACE inhibitors AllopurynolAllopurynol Neurologic disturbances, StevensNeurologic disturbances, Stevens--
Johnson syndrom, anaphylactic reactions, Johnson syndrom, anaphylactic reactions,
neutropenianeutropenia

14
Interactions ofInteractions of angiotensin converting enzyme angiotensin converting enzyme
(ACE) inhibitors (ACE) inhibitors with other drugs with other drugs
and substancesand substances
Angiotensin Angiotensin
converting enzyme converting enzyme
(ACE) inhibitors(ACE) inhibitors
Simultaneously administered Simultaneously administered
other drugs other drugs
and substances and substances
Type and consequences of interaction
ACE inhibitors ACE inhibitors
(captopril, (captopril,
cilizapril, cilizapril,
trandolapril)trandolapril)
Immunosuppressant drugs Immunosuppressant drugs
(azathioprine), cytostatics(azathioprine), cytostatics
NeutropeniaNeutropenia
ACE inhibitors ACE inhibitors CiclosporinCiclosporin Symptoms of acute renal insufficiencySymptoms of acute renal insufficiency
in patients after kidney transplantationin patients after kidney transplantation
ACE inhibitorsACE inhibitors Lithium saltsLithium salts Increase in lithium carbonate blood Increase in lithium carbonate blood
concentration, enhancement its toxicityconcentration, enhancement its toxicity
Captopril, enalaprilCaptopril, enalapril Chlorpromazine, clozapineChlorpromazine, clozapine Hypotonia, orthostatic syncopeHypotonia, orthostatic syncope
Interactions ofInteractions of angiotensin converting enzyme angiotensin converting enzyme
(ACE) inhibitors (ACE) inhibitors with other drugs with other drugs
and substancesand substances
Angiotensin Angiotensin
converting enzyme converting enzyme
(ACE) inhibitors(ACE) inhibitors
Simultaneously administered Simultaneously administered
other drugs other drugs
and substances and substances
Type and consequences of interaction
ACE inhibitors ACE inhibitors Thiazides, chlortalidone, Thiazides, chlortalidone,
furosemide, etacrynic acid furosemide, etacrynic acid
Rapid hypotension, acute renal Rapid hypotension, acute renal
insufficiencyinsufficiency
ACE inhibitors ACE inhibitors Diuretics potassiumDiuretics potassium--sparing sparing
(amiloride, triamterene, (amiloride, triamterene,
spironolactone)spironolactone)
Dangerous, sometimes lifeDangerous, sometimes life--threatening threatening
hyperkalemic symptomshyperkalemic symptoms
ACE inhibitorsACE inhibitors DiureticsDiuretics Increase in urea blood concentrationIncrease in urea blood concentration
Captopril at the Captopril at the
dose of 25 mgdose of 25 mg
FurosemideFurosemide Reduction of furosemide diuretic effectReduction of furosemide diuretic effect
Interactions ofInteractions of calciumcalcium--channel blockers channel blockers with other with other
drugs and substancesdrugs and substances
CalciumCalcium--channel channel
blockersblockers
Simultaneously administered Simultaneously administered
other drugs other drugs
and substances and substances
Type and consequences of interaction
Amlodipine, Amlodipine,
felodipine, felodipine,
isradipine, isradipine,
nicardipine, nicardipine,
nifedipine, nifedipine,
verapamil verapamil
Erythromycin, itraconazole, Erythromycin, itraconazole,
ketoconazole, cimetidine, ketoconazole, cimetidine,
indinavir, ritonavir, saquinavir, indinavir, ritonavir, saquinavir,
grapefruit juice grapefruit juice
InhibitionInhibition of of metabolismmetabolism, increase in , increase in
calciumcalcium--channel blockers blood channel blockers blood
concentration, enhancement of concentration, enhancement of
hypotonia, dizziness, headache, circular hypotonia, dizziness, headache, circular
edema edema
Diltiazem, Diltiazem,
verapamil, verapamil,
nifedipine nifedipine
Rifampicin, phenobarbitalRifampicin, phenobarbital AccelerationAcceleration of of metabolismmetabolism, decrease in , decrease in
calciumcalcium--channel blockers blood channel blockers blood
concentration, reduction of their activityconcentration, reduction of their activity
Werapamil, Werapamil,
diltiazemdiltiazem
Qinidine, disopyramide, Qinidine, disopyramide,
amiodaroneamiodarone
InhibitionInhibition of werapamil, diltiazem of werapamil, diltiazem
metabolismmetabolism, increase in their , increase in their
concentration, bradycardia, hypotonia, concentration, bradycardia, hypotonia,
enhancement of cardiac failure enhancement of cardiac failure
symptomssymptoms
Interactions ofInteractions of calciumcalcium--channel blockers channel blockers with other with other
drugs and substancesdrugs and substances
CalciumCalcium--channel channel
blockersblockers
Simultaneously administered Simultaneously administered
other drugs other drugs
and substances and substances
Type and consequences of interaction
Diltiazem, Diltiazem,
amlodipine, amlodipine,
nifedipine, nifedipine,
verapamil verapamil
Ciclosporin, tacrolimus, Ciclosporin, tacrolimus,
sirolimussirolimus
InhibitionInhibition of of metabolismmetabolism, increase in , increase in
ciclosporin, tacrolimus, sirolimus blood ciclosporin, tacrolimus, sirolimus blood
concentration, enhancement of their concentration, enhancement of their
activityactivity
Diltiazem, Diltiazem,
verapamil, verapamil,
nifedipine nifedipine
Rifampicin, phenobarbitalRifampicin, phenobarbital AccelerationAcceleration of of metabolismmetabolism, decrease in , decrease in
calciumcalcium--channel blockers blood channel blockers blood
concentration, reduction of their activityconcentration, reduction of their activity
Werapamil, Werapamil,
diltiazemdiltiazem
Lovastatin, simvastatin, Lovastatin, simvastatin, InhibitionInhibition of of statins metabolismstatins metabolism, increase , increase
in their plasma concentration, higher risk in their plasma concentration, higher risk
of myopathy or rhabdomyolysisof myopathy or rhabdomyolysis
Interactions ofInteractions of calciumcalcium--channel blockers channel blockers with other with other
drugs and substancesdrugs and substances
CalciumCalcium--channel channel
blockersblockers
Simultaneously administered Simultaneously administered
other drugs other drugs
and substances and substances
Type and consequences of interaction
Diltiazem, Diltiazem,
verapamil verapamil
Carbamazepine, phenytoinCarbamazepine, phenytoin Inhibition Inhibition of carbamazepine, phenytoin of carbamazepine, phenytoin
metabolismmetabolism, increase in their blood , increase in their blood
concentration, enhancement of their concentration, enhancement of their
neurotoxicityneurotoxicity
Diltiazem, Diltiazem,
verapamilverapamil
BetaBeta--adrenolitic drugsadrenolitic drugs EnhancementEnhancement of negative dromothropic of negative dromothropic
effect the mentioned drugs, Aeffect the mentioned drugs, A--V block, V block,
arrhythmogenic effect of arrhythmogenic effect of torsade de torsade de
pointespointes typetype
CalciumCalcium--channel channel
blockersblockers
Tubocurarine, atracurium, Tubocurarine, atracurium,
vecuroniumvecuronium
Increase, prolongIncrease, prolong in muscle relaxant in muscle relaxant
effecteffect
Drugs prolonging Drugs prolonging QT QT interval in interval in EECCG G with the highest risk with the highest risk of of induinducing cing ventricular tachycardia episodes of ventricular tachycardia episodes of torsade de pointestorsade de pointes typetype
Antiarrhythmic drugs
Amiodarone, disopyramide, dofetilide, qunidine, sotalol
Antihistaminic drug
Ebastine
Antibacterial drugs
Erythromycin, clarithromycin, spiramycin, ciprofloxacin, gatifloxacin, norfloxacin, sparfloxacin, co-trimoxazole
Antimycotic drug
Ketoconazole
Antiprotozoan drugsMetronidazole, pentamidine, quinine, chloroquine
Antidepressant drugs
Tricyclic antidepressant drugs, fluoxetine, maprotiline
Antipsychotic drugsChlorpromazine, haloperidol, droperidol, thioridazine, mesoridazine, lithium carbonate, pimozide, sertindole
Calcium channel blocking drugs
Bepridil, prenylamine
Opiate receptor agonists
Methadone, levomethadyl
Other drugs
Chloral hydrate, ketanserin, succinylocholine, tamoxyfen, tacrolimus, vasopressin

15
StatinsStatins interactionsinteractions with other drugs and substanceswith other drugs and substances
StatinsStatins Simultaneously administered Simultaneously administered
other drugs other drugs
and substances and substances
Type and consequences of interaction
LovastatinLovastatin FoodFood IncreaseIncrease in in absorptionabsorption (50%), (50%),
enhancement of activityenhancement of activity
Simvastatin, Simvastatin,
lovastatin, lovastatin,
atorvastatinatorvastatin
Erythromycin, clarithromycin, Erythromycin, clarithromycin,
itraconazole, ketoconazole, itraconazole, ketoconazole,
fluconazole, diltiazem, fluconazole, diltiazem,
verapamil, ciclosporinverapamil, ciclosporin
InhibitionInhibition of CYP3A4 isoenzyme of CYP3A4 isoenzyme
activity responsible for statins first pass activity responsible for statins first pass
metabolism in the intestine wall, metabolism in the intestine wall,
enhancement of their activity, higher enhancement of their activity, higher
risk of myopathy, rhabdomyolysisrisk of myopathy, rhabdomyolysis
Simvastatin, Simvastatin,
lovastatin, lovastatin,
atorvastatinatorvastatin
Grapefruit juiceGrapefruit juice InhibitionInhibition of CYP3A4 isoenzyme of CYP3A4 isoenzyme
activity responsible for statins first pass activity responsible for statins first pass
metabolism in the intestine wall, metabolism in the intestine wall,
enhancement of their activity, higher enhancement of their activity, higher
risk of myopathy, rhabdomyolysisrisk of myopathy, rhabdomyolysis
StatinsStatins interactionsinteractions with other drugs and substanceswith other drugs and substances
StatinsStatins Simultaneously administered Simultaneously administered
other drugs other drugs
and substances and substances
Type and consequences of interaction
Simvastatin, Simvastatin,
lovastatin, lovastatin,
atorvastatinatorvastatin
Fibrates (especially Fibrates (especially
gemfibrozil), niacingemfibrozil), niacin
DecreaseDecrease in statins in statins eliminationelimination, increase , increase
in concentration, enhancement of in concentration, enhancement of
activity, higher risk of myopathy, activity, higher risk of myopathy,
rhabdomyolysisrhabdomyolysis
FluvastatinFluvastatin WarfarinWarfarin InhibitionInhibition of warfarin of warfarin metabolismmetabolism by by
fluvastatin, enhancement of warfarin fluvastatin, enhancement of warfarin
activityactivity
Simvastatin, Simvastatin,
lovastatin, lovastatin,
atorvastatin, atorvastatin,
pravastatin, pravastatin,
fluvastatinfluvastatin
Pectin, colestyraminePectin, colestyramine ReductionReduction of statinsof statins absorptionabsorption, , decrease decrease
in their activityin their activity
StatinsStatins interactionsinteractions with other drugs and substanceswith other drugs and substances
StatinsStatins Simultaneously administered Simultaneously administered
other drugs other drugs
and substances and substances
Type and consequences of interaction
Simvastatin, Simvastatin,
lovastatin, lovastatin,
atorvastatinatorvastatin
Rifampicin, barbituratesRifampicin, barbiturates AccelerationAcceleration of CYP3A4 isoenzyme of CYP3A4 isoenzyme
activity responsible for statins activity responsible for statins
metabolism, reduction of their activitymetabolism, reduction of their activity
FluvastatinFluvastatin RifampicinRifampicin AccelerationAcceleration of fluvastatin of fluvastatin metabolismmetabolism
by rifampicin, reduction of its activityby rifampicin, reduction of its activity
AtorvastatinAtorvastatin Norethisterone, estradiolNorethisterone, estradiol IncreaseIncrease inin hormoneshormones plasma plasma
concentration, enhancement of their concentration, enhancement of their
activityactivity
Rules of antibiotic combinationRules of antibiotic combination
Do not combineDo not combine antibiotics with each other or antibiotics with each other or
antibiotics with other drugs antibiotics with other drugs featuring similar featuring similar
toxic propertiestoxic properties or mutually altering the or mutually altering the
destination in organism, thus affecting destination in organism, thus affecting
pharmacokinetic properties.pharmacokinetic properties.
Rules of antibiotic combination Rules of antibiotic combination (continuation)(continuation)
Antibiotic doses administered in combination Antibiotic doses administered in combination
can not be lowercan not be lower than the doses of these drugs than the doses of these drugs
administered individually.administered individually.
Rules of antibiotic combinationRules of antibiotic combination(continuation)(continuation)
CombinationCombination of of bactericidalbactericidal chemotherapeutics, which chemotherapeutics, which require effectively growing bacteria cells for their require effectively growing bacteria cells for their activity (penicillins, cephalosporins, aminoglycosides, activity (penicillins, cephalosporins, aminoglycosides, rifampicin, isoniazid, fluoroquinolones, polymyxins, rifampicin, isoniazid, fluoroquinolones, polymyxins, vancomycin, bacitracin, nitrofurans, macrolides at vancomycin, bacitracin, nitrofurans, macrolides at higher doses) with higher doses) with bacteriostaticbacteriostatic drugs (sulfonamides, drugs (sulfonamides, tetracyclines, macrolides, chloramphenicol, tetracyclines, macrolides, chloramphenicol, lincosamides, trimethoprim, ethambutol), inhibiting lincosamides, trimethoprim, ethambutol), inhibiting bacteria growth, at great sensitivity of microbacteria growth, at great sensitivity of micro--organism organism can leadcan lead to undesirable to undesirable antagonistic effectantagonistic effect; the ; the ranknest example of drug combination is that of ranknest example of drug combination is that of penicillins with tetracyclines, macrolides or penicillins with tetracyclines, macrolides or chloramphenicol.chloramphenicol.

16
Aminoglicoside antibioticsAminoglicoside antibiotics interaction with other interaction with other
drugs and substancesdrugs and substances
Drugs and substances simultaneously Drugs and substances simultaneously
administered with aminoglicosidesadministered with aminoglicosidesType and consequences of interaction
Neuromuscular blockers (tubocurarine, Neuromuscular blockers (tubocurarine,
gallamine, pancuronium) gallamine, pancuronium)
Increase Increase inin muscle relaxation, prolong muscle muscle relaxation, prolong muscle
paralysis, resulting in possible fatal respiratory paralysis, resulting in possible fatal respiratory
depressiondepression
Furosemide, etacrynic acidFurosemide, etacrynic acid Increase Increase inin ototoxicity ototoxicity
Cefalotin, cefradine, vancomycin, Cefalotin, cefradine, vancomycin,
amphotericin, furosemide, etacrynic acid, amphotericin, furosemide, etacrynic acid,
methoxyflurane, cisplatin, ciclosporin methoxyflurane, cisplatin, ciclosporin
Increase Increase in nephrotoxicity in nephrotoxicity
Phenothiazines (thiethylperazine, Phenothiazines (thiethylperazine,
chlorpromazine, dimenhydrinate) chlorpromazine, dimenhydrinate)
Masking Masking ofof aminoglycosides aminoglycosides
ototoxic symptoms ototoxic symptoms
TetracyclinsTetracyclins interaction with other drugs and interaction with other drugs and
substancessubstances
Drugs and substances simultaneously Drugs and substances simultaneously
administered with tetracyclinesadministered with tetracyclinesType and consequences of interaction
Drugs containing the ions of calcium, iron, Drugs containing the ions of calcium, iron,
magnesium, aluminium, bismuth, zinc, copper, magnesium, aluminium, bismuth, zinc, copper,
milk, bases milk, bases
ReductionReduction of tetracyclins of tetracyclins absorptionabsorption from from
gastrointestinal tract, decrease in their activitygastrointestinal tract, decrease in their activity
Phenytoin, barbiturates, carbamazepine Phenytoin, barbiturates, carbamazepine InductionInduction of teracyclins of teracyclins metabolismmetabolism ––
doxycycline, diminishing of their activitydoxycycline, diminishing of their activity
Phenothiazines (chlorpromazine) Phenothiazines (chlorpromazine) IncreaseIncrease in in hepatotoxic activityhepatotoxic activity of tetracyclins of tetracyclins
Warfarin, phenindioneWarfarin, phenindione IncreaseIncrease in in anticoagulant drug activityanticoagulant drug activity due to due to
dysbacteriosis, decrease in vitamin K synthesis dysbacteriosis, decrease in vitamin K synthesis
by intestinal bacteria and decrease in by intestinal bacteria and decrease in
prothrombin concentrationprothrombin concentration
Digoxin, insulin Digoxin, insulin Tetracyclins enhancement of digoxin and Tetracyclins enhancement of digoxin and
insulin activityinsulin activity
Macrolides antibioticsMacrolides antibiotics interaction with other drugsinteraction with other drugs
AntibioticAntibiotic Type and consequences of interaction
Group IGroup I
Old genetation macrolides Old genetation macrolides
erythromycin, troleandomycin erythromycin, troleandomycin
EnhancementEnhancement of warfarin, digoxin, of warfarin, digoxin,
theophylline, ebastine, methylprednisolone, theophylline, ebastine, methylprednisolone,
carbamazepine, ciclosporin, disopyramide, carbamazepine, ciclosporin, disopyramide,
felodipine, benzodiazepines (triazolam, felodipine, benzodiazepines (triazolam,
midazolam) and bromocriptine midazolam) and bromocriptine activity activity due to due to
inhibitioninhibition of their of their metabolismmetabolism and and excretionexcretion
Group IIGroup II
josamycin, roxithromycin, josamycin, roxithromycin,
clarithromycin, flurythromycin, clarithromycin, flurythromycin,
miokamycin, midekamycin miokamycin, midekamycin
Enhancement Enhancement ofof theophylline, ebastine, theophylline, ebastine,
carbamazepine, coumarin derivatives, carbamazepine, coumarin derivatives,
bromocriptine, ciclosporin bromocriptine, ciclosporin activityactivity due to due to
inhibitioninhibition of their of their metabolismmetabolism
Group IIIGroup III
azythromycin, spiramycin,azythromycin, spiramycin,
dirithromycin, rokitamycin dirithromycin, rokitamycin
So far clinically significant interactions have So far clinically significant interactions have
not been observed in peoplenot been observed in people
FluoroquinolonesFluoroquinolones interactions with other drugsinteractions with other drugs
Drugs simultaneously Drugs simultaneously
administered with administered with
fluoroquinolonesfluoroquinolones
Type and consequences of interaction
Theophyllin Theophyllin InhibitionInhibition of theophyllin of theophyllin metabolismmetabolism by enoxacin, by enoxacin,
pipemidic acid, in a less degree by ciprofloxacin, pipemidic acid, in a less degree by ciprofloxacin,
pefloxacin, norfloxacin, increase in theophyllin pefloxacin, norfloxacin, increase in theophyllin
concentration, concentration, enhancementenhancement in its activity and adverse in its activity and adverse
effects effects
Antihistaminic drugs Antihistaminic drugs
(ebastine) (ebastine)
EnhancementEnhancement of cardiotoxic effect by ciprofloxacin, of cardiotoxic effect by ciprofloxacin,
norfloxacin, sparfloxacin, prolongation of QT interval, norfloxacin, sparfloxacin, prolongation of QT interval,
risk of ventricular tachycardia episodes of risk of ventricular tachycardia episodes of torsade de torsade de
pointespointes typetype
FluoroquinolonesFluoroquinolones interactions with other drugsinteractions with other drugs
Drugs simultaneously administered Drugs simultaneously administered
with fluoroquinoloneswith fluoroquinolones
Type and consequences of interaction
Anticoagulant drugs, NSAIDs, Anticoagulant drugs, NSAIDs,
antidiabetic drugs, cytostatic drugs antidiabetic drugs, cytostatic drugs --
substrates for isoenzyme CYP1A2 substrates for isoenzyme CYP1A2
and CYP3A4and CYP3A4
InhibitionInhibition of drug of drug metabolismmetabolism, which are , which are
substrates for isoenzyme CYP1A2 and substrates for isoenzyme CYP1A2 and
CYP3A4 by fluoroquinolones, enhancement of CYP3A4 by fluoroquinolones, enhancement of
their activity their activity
Antacids containing aluminium, Antacids containing aluminium,
magnesium, calcium, zinc, iron magnesium, calcium, zinc, iron
salts, sucralfate, salts, sucralfate,
ReductionReduction of fluoroquinolones of fluoroquinolones absorptionabsorption from from
gastrointestinal tract gastrointestinal tract
Tuberculostatic drugTuberculostatic drug interactions with other drugs interactions with other drugs
and substances and substances
Tuberculostatic drugsTuberculostatic drugs Drugs and substances simultaneously Drugs and substances simultaneously
administered administered
Type and consequences
of interaction
Rifampicin Rifampicin Antifungal drugs (itraconazole, Antifungal drugs (itraconazole,
ketoconazole), antiviral drugs ketoconazole), antiviral drugs
(indinavir, saquinavir, nelfinavir), (indinavir, saquinavir, nelfinavir),
immunosuppressant drugs immunosuppressant drugs
(ciclosporin, tacrolimus), (ciclosporin, tacrolimus),
theophylline, narcotic analgesics theophylline, narcotic analgesics
(methadone), contraceptives, (methadone), contraceptives,
coumarins derivatives, oral coumarins derivatives, oral
antidiabetics, tricyclic antidiabetics, tricyclic
antidepressant drugs, antipsychotic antidepressant drugs, antipsychotic
drug (haloperidol), drug (haloperidol),
antihypertensive drug (enalapril), antihypertensive drug (enalapril),
corticosteroids corticosteroids
InductionInduction of the of the
mentioned drugs mentioned drugs
and substances and substances
metabolismmetabolism by by
rifampicin, rifampicin,
reduction of their reduction of their
activityactivity

17
Tuberculostatic drugTuberculostatic drug interactions with other interactions with other
drugsdrugs
Tuberculostatic Tuberculostatic
drugsdrugs
Simultaneously Simultaneously
administered other administered other
drugsdrugs
Type and consequences
of interaction
Rifampicin Rifampicin Digoxin Digoxin Decrease Decrease in digoxin in digoxin
concentration by rifampicin concentration by rifampicin
inductioninduction of of PP--glicoproteinglicoprotein
activity activity in gut epithelium cells, in gut epithelium cells,
reduction of digoxin activity reduction of digoxin activity
Antifungal drugAntifungal drug interactions with other drugs interactions with other drugs
and substancesand substances
Antifungal Antifungal
drugsdrugs
Simultaneously Simultaneously
administered drugs administered drugs
and substances and substances
Type and consequences of
interaction
Ketoconazole Ketoconazole Drugs prolonging QT intervalDrugs prolonging QT interval IncreasedIncreased risk ofrisk of lifelife--threateningthreatening
dysrrhythmia of dysrrhythmia of torsade de pointestorsade de pointes
typetype
Ketoconazole Ketoconazole Alcohol Alcohol Symptoms of alcohol Symptoms of alcohol intoleranceintolerance, ,
disulfiramdisulfiram--like reaction like reaction
Ketoconazole, Ketoconazole,
fluconazole, fluconazole,
itraconazole, itraconazole,
woriconazole woriconazole
Phenytoin, rifampicin, Phenytoin, rifampicin,
phenobarbital phenobarbital
InductionInduction of antifungal drugs of antifungal drugs
metabolismmetabolism by phenytoin, rifampicin, by phenytoin, rifampicin,
phenobarbital, reduction of antifungal phenobarbital, reduction of antifungal
drugs activity drugs activity
Ketoconazole, Ketoconazole,
fluconazole, fluconazole,
itraconazole, itraconazole,
woriconazole woriconazole
Drugs administered in Drugs administered in
chronic peptic ulcer disease, chronic peptic ulcer disease,
antagonists of H2 receptors, antagonists of H2 receptors,
omeprazol, sucralfate omeprazol, sucralfate
DecreaseDecrease in antifungal drugs in antifungal drugs
absorptionabsorption from gastrointestinal tractfrom gastrointestinal tract
Antifungal drugAntifungal drug interactions with other drugs interactions with other drugs
and substancesand substances
Antifungal drugsAntifungal drugs Simultaneously Simultaneously
administered drugs administered drugs
and substances and substances
Type and consequences of
interaction
Griseofulvin Griseofulvin Anticoagulants, ciclosporin, Anticoagulants, ciclosporin,
oral contraceptives oral contraceptives
InductionInduction of the above drugs of the above drugs
metabolismmetabolism by griseofulvin, decrease by griseofulvin, decrease
in their activityin their activity
Griseofulvin Griseofulvin Barbiturates Barbiturates InductionInduction of griseofulvin of griseofulvin metabolism metabolism
by barbiturates, reduction of its by barbiturates, reduction of its
antifungal activity antifungal activity
Griseofulvin Griseofulvin Alcohol Alcohol IntensificationIntensification of alcohol effectof alcohol effect
Ketoconazole, Ketoconazole,
fluconazole, fluconazole,
itraconazole, itraconazole,
woriconazole woriconazole
Phenytoin, ciclosporin, Phenytoin, ciclosporin,
statins, anticoagulants, statins, anticoagulants,
antihistamines H1 II antihistamines H1 II
generation, cardiac generation, cardiac
glycosides, calcium channel glycosides, calcium channel
blocker drugsblocker drugs
Inhibition Inhibition of the above drugs of the above drugs
metabolismmetabolism by ketoconazole, by ketoconazole,
fluconazole, itraconazole, fluconazole, itraconazole,
woriconazole, enhancement of their woriconazole, enhancement of their
activity and toxicityactivity and toxicity
TheophyllineTheophylline interactions with other drugs and substancesinteractions with other drugs and substances
Simultaneously administered drugs Simultaneously administered drugs
and substancesand substances
Type and consequences of interaction
Macrolides Macrolides –– erythromycin, erythromycin,
clarithromycin, josamycin; clarithromycin, josamycin;
fluoroquinolones fluoroquinolones –– enoxacin, enoxacin,
pipemidic acid, ciprofloxacin, pipemidic acid, ciprofloxacin,
pefloxacin, norfloxacin; moreover pefloxacin, norfloxacin; moreover
cimetidine, zileuton, oral cimetidine, zileuton, oral
contraceptivescontraceptives
InhibitionInhibition of theophyllin of theophyllin metabolismmetabolism
Enzyme inductors Enzyme inductors -- barbiturates, barbiturates,
rifampicin, phenytoin, St John’s wortrifampicin, phenytoin, St John’s wort
InductionInduction of theophyllin of theophyllin metabolismmetabolism, ,
reductionreduction ofof its pharmacological activityits pharmacological activity
Methotrexate Methotrexate interactions with other drugsinteractions with other drugs
Drugs simultaneously administered Drugs simultaneously administered
with MTXwith MTX
Type and consequences of interaction
Cholestyramine, neomycin, Cholestyramine, neomycin,
paromomycin paromomycin
DecreaseDecrease in MTX gastrointestinal in MTX gastrointestinal
absorptionabsorption, diminishing MTX action, diminishing MTX action
Hydrocortisone, prednisone, cefalotin Hydrocortisone, prednisone, cefalotin ReductionReduction of MTX of MTX cell uptakecell uptake, ,
diminishing of MTX activitydiminishing of MTX activity
Griseofulvin, rifampicin, phenobarbital Griseofulvin, rifampicin, phenobarbital Induction Induction of MTX of MTX metabolismmetabolism, ,
diminishing of MTX action diminishing of MTX action
Asparaginase Asparaginase Antagonistic effectAntagonistic effect in relation to MTX, in relation to MTX,
diminishing of MTX activitydiminishing of MTX activity
Kanamycin Kanamycin IncreaseIncrease in MTX gastrointestinal in MTX gastrointestinal
absorptionabsorption, increase in its bioavailability, , increase in its bioavailability,
enhancement of MTX activity enhancement of MTX activity
MethotrexateMethotrexate interactionsinteractions with other drugswith other drugs
Drugs simultaneously administered Drugs simultaneously administered
with MTXwith MTX
Type and consequences of interaction
NSAIDs, sulfonamides, probenecidNSAIDs, sulfonamides, probenecid DisplacementDisplacement of of MTX from MTX from serum serum
albumin bindingalbumin binding, increase in its activity, , increase in its activity,
enhancement of MTX toxicityenhancement of MTX toxicity
Salicylates, sulfonamides, cefalotin, Salicylates, sulfonamides, cefalotin,
penicillin, probenecid penicillin, probenecid
Competitive Competitive impairmentimpairment of renal tubular of renal tubular
secretion of MTX, increase in activity, secretion of MTX, increase in activity,
enhancement of toxicity enhancement of toxicity
Aminoglycosides, cisplatin, Aminoglycosides, cisplatin,
ciclosporin, procarbazin ciclosporin, procarbazin
Impairment Impairment of kidney function, decrease of of kidney function, decrease of
MTX excretion, increase in MTX MTX excretion, increase in MTX
pharmacological activity, enhancement of pharmacological activity, enhancement of
MTX toxicityMTX toxicity

18
MethotrexateMethotrexate interactions with other drugsinteractions with other drugs
Drugs simultaneously administered Drugs simultaneously administered
with MTXwith MTX
Type and consequences of interaction
CisplatinCisplatin DamageDamage of renal tubules, of renal tubules, decrease decrease in MTX in MTX
and folic acid reabsorptionand folic acid reabsorption, decrease in , decrease in
effectiveness of leucovorin rescueeffectiveness of leucovorin rescue
Phenylbutazone, amidopirinePhenylbutazone, amidopirine EnhancementEnhancement of MTX bone marrow of MTX bone marrow
depressiondepression
Azathioprine, sulfasalazineAzathioprine, sulfasalazine Increase Increase in hepatotoxicity riskin hepatotoxicity risk
Mercaptopurine Mercaptopurine InhibitionInhibition of mercaptopurine of mercaptopurine metabolismmetabolism by by
MTX, enhancement of mercaptopurine MTX, enhancement of mercaptopurine
activityactivity
Immunosuppressant drugImmunosuppressant drug interactions interactions ––
ciclosporin, tacrolimus, sirolimus with other drugsciclosporin, tacrolimus, sirolimus with other drugs
Immunosuppressant Immunosuppressant
drugsdrugs
Other simultaneously Other simultaneously
administered drugsadministered drugs
Type and consequences of interaction
Ciclosporin, Ciclosporin,
tacrolimustacrolimus
Macrolides Macrolides --
erythromycin, erythromycin,
clarithromycin, clarithromycin,
josamycin josamycin
Inhibition Inhibition of ciclosporin andof ciclosporin and
tacrolimus tacrolimus metabolismmetabolism by macrolides, increaseby macrolides, increase in in
immunosuppressant drugsimmunosuppressant drugs effecteffect
Ciclosporin Ciclosporin Antifungal drugs Antifungal drugs --
ketoconazole, ketoconazole,
fluconazole, fluconazole,
itraconazoleitraconazole
InhibitionInhibition of ciclosporin of ciclosporin metabolismmetabolism by by
antifungal drugs, increaseantifungal drugs, increase inin itsits activity. activity.
Necessity of 85% reduction in ciclosporin Necessity of 85% reduction in ciclosporin
dosages during simultaneous therapy with dosages during simultaneous therapy with
ketoconazole, and of 50% ketoconazole, and of 50% -- during therapy with during therapy with
fluconazolefluconazole
Tacrolimus Tacrolimus Fluconazole Fluconazole InhibitionInhibition of tacrolimus of tacrolimus metabolismmetabolism by by
fluconazole, enhancement of tacrolimus activity. fluconazole, enhancement of tacrolimus activity.
Necessity of 50% reduction in tacrolimus Necessity of 50% reduction in tacrolimus
dosages during simultaneously therapy with dosages during simultaneously therapy with
fluconazolefluconazole
Sirolimus Sirolimus Ketoconazole Ketoconazole Inhibition Inhibition of sirolimus of sirolimus metabolismmetabolism by by
ketoconazole, enhancement of sirolimusketoconazole, enhancement of sirolimus activityactivity
Immunosuppressant drugImmunosuppressant drug interactions interactions ––
ciclosporin, tacrolimus, sirolimus with other drugsciclosporin, tacrolimus, sirolimus with other drugs
Immunosuppressant Immunosuppressant
drugsdrugs
Other simultaneously Other simultaneously
administered drugsadministered drugs
Type and consequences of interaction
Ciclosporin, Ciclosporin,
tacrolimus, tacrolimus,
sirolimussirolimus
Diltiazem Diltiazem InhibitionInhibition of immunosupressant drugs of immunosupressant drugs
metabolismmetabolism by diltiazem, increase in their by diltiazem, increase in their
activityactivity
CiclosporinCiclosporin Verapamil Verapamil InhibitionInhibition of ciclosporin of ciclosporin metabolismmetabolism by by
verapamil, enhancement of ciclosporin activityverapamil, enhancement of ciclosporin activity
TacrolimusTacrolimus Nifedipine, Nifedipine,
antiviral drugs antiviral drugs ––
protease inhibitors protease inhibitors
(nelfinavir, (nelfinavir,
ritonavir, ritonavir,
saquinavir) saquinavir)
InhibitionInhibition of tacrolimus of tacrolimus metabolismmetabolism by the by the
above drugs, enhancement of its activityabove drugs, enhancement of its activity
Ciclosporin, Ciclosporin,
tacrolimustacrolimus
Grapefruit juiceGrapefruit juice InhibitionInhibition of ciclosporin and tacrolimus of ciclosporin and tacrolimus first first
pass metabolismpass metabolism in intestine, increase of in intestine, increase of
bioavailability, enhancement of activitybioavailability, enhancement of activity
Immunosuppressant drugImmunosuppressant drug interactions interactions ––
ciclosporin, tacrolimus, sirolimus with other drugsciclosporin, tacrolimus, sirolimus with other drugs
Immunosuppressant Immunosuppressant
drugsdrugs
Other simultaneously Other simultaneously
administered drugsadministered drugs
Type and consequences of interaction
Ciclosporin Ciclosporin Phenobarbital, Phenobarbital,
rifampicin, rifampicin,
phenytoin, phenytoin,
carbamazepine, carbamazepine,
St John’s wortSt John’s wort
Induction Induction of ciclosporinof ciclosporin metabolismmetabolism by the by the
above drugs, diminishing its activity, above drugs, diminishing its activity,
danger of graft rejectiondanger of graft rejection
Tacrolimus Tacrolimus Rifampicin, Rifampicin,
phenytoinphenytoin
InductionInduction ofof tacrolimus tacrolimus metabolismmetabolism by the by the
above drugs, diminishing its activity, above drugs, diminishing its activity,
danger of graft rejectiondanger of graft rejection
Sirolimus Sirolimus RifampicinRifampicin Induction Induction of sirolimus of sirolimus metabolismmetabolism by by
rifampicin, diminishing its activity, danger rifampicin, diminishing its activity, danger
of graft rejectionof graft rejection
Immunosuppressant drugImmunosuppressant drug interactions interactions ––
ciclosporin, tacrolimus, sirolimus with other drugsciclosporin, tacrolimus, sirolimus with other drugs
Immunosuppressant Immunosuppressant
drugsdrugs
Other simultaneously Other simultaneously
administered drugsadministered drugs
Type and consequences of interaction
Ciclosporin, Ciclosporin,
tacrolimustacrolimus
Aminoglycosides, Aminoglycosides,
NSAIDs, amiloride, NSAIDs, amiloride,
sirolimus, other sirolimus, other
nephrotoxic drugsnephrotoxic drugs
IncreaseIncrease inin nephrotoxicity as a result nephrotoxicity as a result
of of additive effectadditive effect of these drugsof these drugs
CiclosporinCiclosporin Digoxin Digoxin Increase Increase inin digoxin concentration in digoxin concentration in
organism, enhancement of its activityorganism, enhancement of its activity
Some websitesSome websites
www.ema.europa.euwww.ema.europa.eu
www.adrreports.euwww.adrreports.eu
yellowcard.yellowcard.mhra.mhra.gov.ukgov.uk
www.dsru.orgwww.dsru.org
www.mhra.gov.ukwww.mhra.gov.uk
www.cks.nks.uk/adversewww.cks.nks.uk/adverse drug reactionsdrug reactions

19
Literature Sources for ADR InformationLiterature Sources for ADR Information
WHO PublicationWHO Publication
-- Pharmacovigilance A to ZPharmacovigilance A to Z
-- Dictionary of PharmacovigilanceDictionary of Pharmacovigilance
-- Stephen’s Detection of New Adverse Stephen’s Detection of New Adverse
Drug ReactionsDrug Reactions
-- To Heal and HarmTo Heal and Harm
-- WHO Pharmaceutical NewsletterWHO Pharmaceutical Newsletter
-- Signal Signal –– Analyses of ADR in WHO DatabaseAnalyses of ADR in WHO Database
Electronic Reference SearchesElectronic Reference Searches
EE--mail Alerts mail Alerts –– USFDA MedwatchUSFDA Medwatch
Electronic Table of Content (EElectronic Table of Content (E--ToC)ToC)
-- Lancet (Lancet (http://thelancet.comhttp://thelancet.com))
-- BMJ (BMJ (http://www.bmj.comhttp://www.bmj.com))
-- NEJM (NEJM (http://content.nejm.orghttp://content.nejm.org))
SCIRUS SCIRUS –– for scientific information onlyfor scientific information only
((http://www.scirus.com/srsapphttp://www.scirus.com/srsapp))
Free medical journalFree medical journal
((http://www.freemedicaljournals.comhttp://www.freemedicaljournals.com))
PLoS MedicinePLoS Medicine
((http://medicine.plosjournals.orghttp://medicine.plosjournals.org))
Medscape Medscape
((http://www.medscape.comhttp://www.medscape.com))
Medical �ews TodayMedical �ews Today
((http://www.medicalnewstoday.comhttp://www.medicalnewstoday.com))
Medsafe, �ew ZealandMedsafe, �ew Zealand
((http://www.medsafe.govt.nzhttp://www.medsafe.govt.nz))
Lareb Lareb -- �etherland Pharmacovigilance �etherland Pharmacovigilance
((www.lareb.comwww.lareb.com))
WHO WHO –– Vigisearch, Vigibase, Vigimed Vigisearch, Vigibase, Vigimed
(Sorry!!! This is for members only(Sorry!!! This is for members only))