aesthetic surgery journal malar fat pad …...facial surgery malar fat pad repositioning, which...
TRANSCRIPT

FacialSurgery
Malar fat pad repositioning, which restores the shape and volume of the face, is a fundamental step in facial rejuve-nation procedures. Recent studies show that malar fat pad aging occurs on two levels. In the upper level, aging is primarily caused by ptosis of the fibroadipose layer attached to the skin. In the lower level, atrophy or osseous rotation of the muscle is a more significant factor than changes to the superficial muscular aponeurotic system and periosteum.1,2 In traditional facial rejuvenation, the malar fat pad is repositioned with upper-lateral traction, which may be ineffective in light of recent research regard-ing the anatomy of the area. The upward vector of the malar fat pad should be vertical; in the periorbital region, the vectors should be concentric.3-5 The proper fixation of this suspension in rigid tissue is important as well.6-8 To that end, we present a simple technique of suspension and fixation of the midface, specifically in the orbital and malar regions, the nasolabial and labiomandibular folds, and the jawline. This technique lends itself well to
concurrent procedures and can complement additional upper or lower facial rejuvenation techniques.
MethodS
From January 2007 to January 2009, the technique described below was applied to 10 consecutive patients over a two-year period in the senior author’s (CYC) clinic. All patients
Malar Fat Pad Repositioning in Facelifting: A Simple Technique of Suspension and Fixation
Chang Yung Chia, MD; Marcelo Wilson Rocha Almeida, MD; Patrícia Durgante Ritter, MD; and Erik de Aquino Nery, MD
AbstractBackground: Aging in the malar fat pad is mainly caused by ptosis of the fibroadipose layer. In the lower level of the face, atrophy or osseous rotation may contribute to the signs and symptoms of facial aging.Objectives: The senior author (CYC) describes his simple technique of suspension and fixation of the malar fat pad and the jowl during facial rejuvenation surgery.Methods: Ten patients underwent facial rejuvenation, the technique of which consists of sustaining and elevating the ptotic malar tissue and the jowl with four slings of monofilament nylon suture. The sutures are fixed medially in an artificial orifice dissected on the frontal process of the maxilla, above the alar groove. The sutures are distributed evenly on the face, directly supporting the jowl, the malar fat pad, and the periorbital tissue. Laterally, the loops are fixed under tension on the temporal fascia and the periosteum of the lateral orbital rim. The vector of tissue displacement is upward and concentric, opposing the vector of the aging process, and the fixation is consistent.Results: Postoperative complications included moderate and transitory pain; patients reported no major complications or recidivisms during the follow-up period of two years. Results showed aesthetic improvement for all patients.Conclusions: The present technique has proven simple and effective in a small cohort over two years. A longer follow-up period with more patients would be valuable in further documenting the procedure.
Keywordsface lifting, rhytidoplasty, facial rejuvenation
Accepted for publication July 27, 2010.
Dr. Chia is a plastic surgeon in private practice in Rio de Janiero, Brazil, and a member of the Brazilian Society of Plastic Surgery.Drs. Almeida, Ritter, and de Aquino Nery are plastic surgery students at the Ivo Pitanguy Institute, Rio de Janiero, Brazil.
Corresponding Author:Dr. Marcelo Wilson Rocha Almeida, Rua São Clemente, 182, apto 201, Rio de Janeiro, RJ, 22260-000, Brazil.E-mail: [email protected]
Aesthetic Surgery Journal30(6) 790 –797© 2010 The American Society for Aesthetic Plastic Surgery, Inc.Reprints and permission: http://www .sagepub.com/journalsPermissions.navDOI: 10.1177/1090820X10381878www.aestheticsurgeryjournal.com
INTE
RNAT
IONAL CONTRIBUTION

Chia et al 791
within the extension of the neck detachment. The lateral platysma and medial platysma superficial muscular apone-urotic system were treated. Access to the midface was gained through conventional inferior blepharoplasty, tak-ing care to limit the orbicularis muscular incision to the lateral half, thus preserving the motor innervations.9 The dissection plane at the malar region was infraorbicular and supraperiosteal.
A 2-mm stab incision was then made with a No. 11 blade at the upper part of the alar crease. Dissection with sharp scissors proceeded to the bone at the piriform aper-ture, just above the nasal wing (Figure 2). Through the stab incision, the bone and nasal mucosa were transfixed with a 3-cm threaded curved needle of 2-0 monofilamen-tar nylon. Exiting outward through the naris, the needle crossed the osseous opening and then retroceded in a cau-dal direction, passing through the piriform opening edge
Figure 1. This illustration of preoperative planning (left) and postoperative results (right) shows the position of the four sutures inserted during the procedure: green (nylon 2-0), along the mandibular line; purple (nylon 2-0), along the caudal malar fat region; blue (nylon 4-0), along the medial malar region; and red (nylon 4-0), along the cranial malar region. The postoperative hemiface shows the traced wires suspending the malar fat pad, with their respective fixations: green and purple, in the temporal fascia; blue, in the parietal region; and red, in the lateral orbital edge.
Figure 2. (A) A 2-mm incision is placed in the nasal wing groove close to the bone edge of the piriform opening. (B) Dissected facial-cervico lifting and the trajectories of the marked wires are shown in the mandibular, malar, and periorbital regions.
were women. Each underwent facelift and necklift proce-dures along with blepharoplasty. Seven (70%) were pri-mary cases and three (30%) were secondary.
Surgical Technique
Before the procedure began, each patient was examined in the orthostatic position; the structures to be treated were identified and the location where each suture would be placed was marked (Figure 1). Once the patient had undergone preoperative preparation and antisepsis, gen-eral anesthesia was administered, with local infiltration of the face and nasal lateral mucosa with vasoconstrictor solution. A preauricular incision was made, and limited detachment of the face was completed, after which retro-auricular and mastoidal incisions were made as necessary

792 Aesthetic Surgery Journal 30(6)
and finally exiting through the cutaneous incision, thereby binding the bone (Figure 3). A 4-0 monofilament nylon was secured to the previously-placed 2-0 suture, resulting
in four fixed sutures at the malar region (Figure 4). A long, curved, blunt needle was then passed from the preauricular and periorbital region to the nasal incision; it was continued
Figure 3. (A, B) The opening in the bone of the nasal process of the maxilla. (C, D) The bone and nasal mucosa are transfixed. (E, F) The needle crosses the bone and the mucosa, then retrocedes and returns through the incision, binding the bone edge.
Chia et al 793
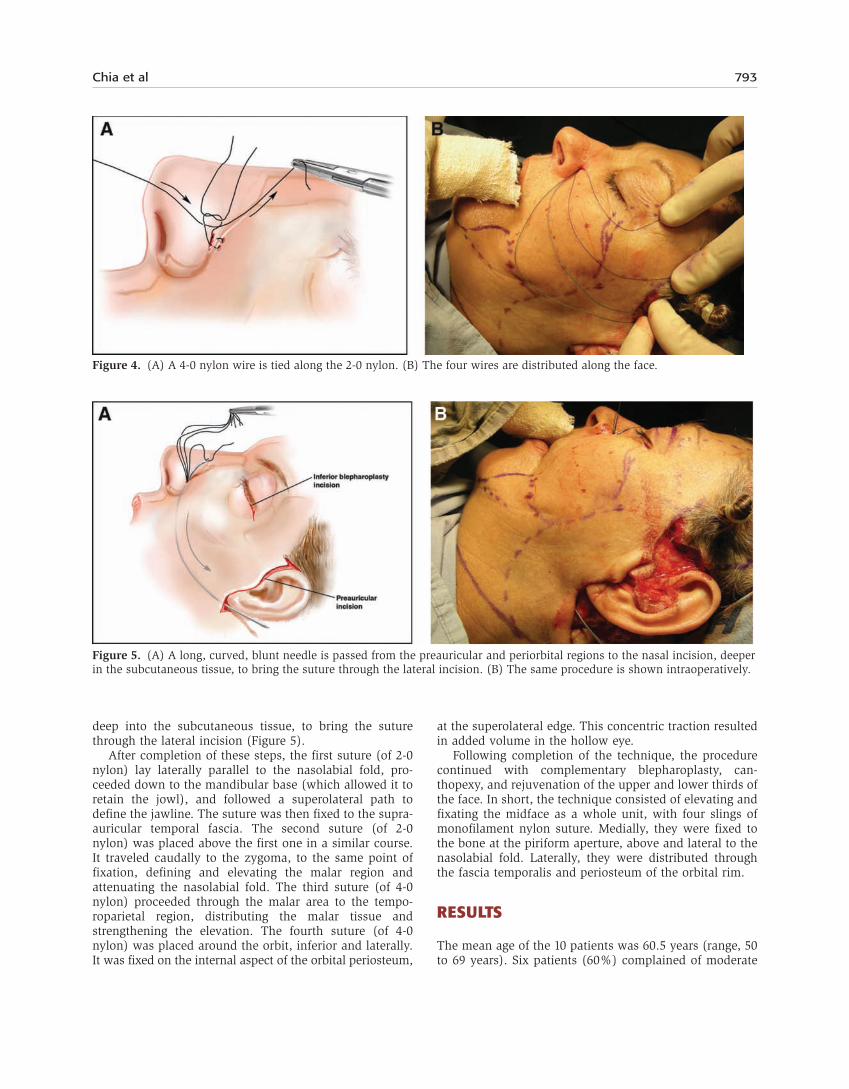
deep into the subcutaneous tissue, to bring the suture through the lateral incision (Figure 5).
After completion of these steps, the first suture (of 2-0 nylon) lay laterally parallel to the nasolabial fold, pro-ceeded down to the mandibular base (which allowed it to retain the jowl), and followed a superolateral path to define the jawline. The suture was then fixed to the supra-auricular temporal fascia. The second suture (of 2-0 nylon) was placed above the first one in a similar course. It traveled caudally to the zygoma, to the same point of fixation, defining and elevating the malar region and attenuating the nasolabial fold. The third suture (of 4-0 nylon) proceeded through the malar area to the tempo-roparietal region, distributing the malar tissue and strengthening the elevation. The fourth suture (of 4-0 nylon) was placed around the orbit, inferior and laterally. It was fixed on the internal aspect of the orbital periosteum,
at the superolateral edge. This concentric traction resulted in added volume in the hollow eye.
Following completion of the technique, the procedure continued with complementary blepharoplasty, can-thopexy, and rejuvenation of the upper and lower thirds of the face. In short, the technique consisted of elevating and fixating the midface as a whole unit, with four slings of monofilament nylon suture. Medially, they were fixed to the bone at the piriform aperture, above and lateral to the nasolabial fold. Laterally, they were distributed through the fascia temporalis and periosteum of the orbital rim.
ReSultS
The mean age of the 10 patients was 60.5 years (range, 50 to 69 years). Six patients (60%) complained of moderate
Figure 4. (A) A 4-0 nylon wire is tied along the 2-0 nylon. (B) The four wires are distributed along the face.
Figure 5. (A) A long, curved, blunt needle is passed from the preauricular and periorbital regions to the nasal incision, deeper in the subcutaneous tissue, to bring the suture through the lateral incision. (B) The same procedure is shown intraoperatively.

794 Aesthetic Surgery Journal 30(6)
temporal pain postoperatively, lasting up to seven days. There were no major complications such as hematomas, seromas, facial nerve branch compression or lesion, ischemia, or alopecia in any of the patients in this series.
Figures 6–8 show representative clinical results of facial rejuvenation with our technique of malar fat pad suspen-sion. As these results suggest, both surgeon and patients deemed the repositioning and definition at the malar and orbital regions, jawline, and nasolabial fold very satisfactory.
diScuSSion
Current techniques in facial surgery emphasize volume redistribution and restoration of natural contours.10 The middle third of the face is primarily responsible for the most noticeable signs of aging. It encompasses the inferior lid and periorbital region, areas that demonstrate symp-toms such as the hollow eye (the V deformity), skele-tonization of the malar bone, intensification of nasolabial fold, tear trough deformities, and the emergence of fes-toons.11 Recent studies have revealed that the main changes
occur in facial volume as a result of the descent of the subcutaneous fat and bone atrophy. Changes in muscle aponeurosis seem to be irrelevant and traction on the superficial muscular aponeurotic system does not work; in some cases, these procedures may even accentuate the nasolabial fold, given that it is formed by the insertion of the zygomatic muscles.12-14 Therefore, the preferred plane for undermining is subcutaneous and the treatment/ repositioning of malar fibroadipose thickening is key.1
The direction of traction is another point of interest. The medial third of the midface falls inferiorly and medi-ally; the central third, inferiorly; and the lateral third, inferiorly and laterally. As such, to combat the signs of aging, the medial third should be pulled superiorly and laterally; the central third, superiorly; and the lateral third, superiorly and medially.3 When the sutures are pulled, as proposed by the technique we describe, the force of traction is perpendicular to the sling parabola. Therefore, the resulting vector of elevation is superior and vertical.15
Obtaining strong and lasting results in tissue mobiliza-tion or suspension depends on observing several well-established principles: tissue undermining, elimination or
Figure 6. (A) This 69-year-old woman presented for facial rejuvenation. (B) One year after facial-cervico lift and blepharoplasty, with malar and periorbital repositioning, as well as jaw line definition.

Chia et al 795
attenuation of opposing forces (myotomies, myectomies), elimination of excess tissue, fixation to immobile struc-tures, placement of an adequate number of sutures, and direct approach to the structure when it has elastic proper-ties.6,8,16 (According to the nonlinear elastic deformation property, the proximal part absorbs most of the pulling forces, and the distal part is only minimally mobilized.)
Among the many midface suspension techniques,17-19 most feature superolateral traction. Some authors employ transpalpebral vertical traction and fix the graft in the periosteum of the infraorbital edge—or, when the perios-teum is thin, they perforate two or three openings with a drill in the orbital edge, taking care to protect the ocular globe.20 However, the existing literature lacks description of a simple surgical technique of reliable fixation with a vertical ascension vector. In our technique, the sutures directly sustain the ptotic tissue. Because the sutures are fixed to the bone medially and distributed over the orbital rim and fascia temporalis laterally, there are several con-centric traction forces, allowing total reshaping and vol-ume restoration in the midface.
Two limitations of our study are its small sample size and its relatively short follow-up period. To truly determine
the long-term safety and efficacy of this procedure, follow-ing a larger cohort for an extended period would be helpful.
concluSionS
Our technique of malar fat pad repositioning for facial reju-venation has proven simple, safe, versatile, and reversible, with no major complications in a cohort of 10 patients. The multidirectionality of the suture placement, elevation, and suspension make this approach unique and contributes to its overall reliability. Furthermore, it can be successfully per-formed alongside other rejuvenation procedures.
disclosures
The author declared no conflicts of interest with respect to the authorship and publication of this article.
FundingThe authors received no financial support for the research and authorship of this article.
Figure 7. (A) This 60-year-old woman presented for facial rejuvenation. (B) Two years after facial-cervico lift and blepharoplasty, with malar and periorbital repositioning.

796 Aesthetic Surgery Journal 30(6)
ReFeRenceS
1. Gosain AK, Amarante MT, Hyde JS, Yousif NJ. A dynamic analysis of changes in the nasolabial fold using mag-netic resonance imaging: implications for facial rejuve-nation and facial animation surgery. Plast Reconstr Surg 1996;98(4):622-636.
2. Pessa JE. An algorithm of facial aging: verification of Lambros’s theory by three-dimensional stereolithog-raphy, with reference to the pathogenesis of midfacial aging, scleral show, and the lateral suborbital trough deformity. Plast Reconstr Surg 2000;106(2):479-490.
3. Hamra ST. Frequent face lift sequelae: hollow eyes and the lateral sweep: cause and repair. Plast Reconstr Surg 1998;102(5):1658-1666.
4. Hinderer UT. Vertical preperiosteal rejuvenation of the frame of the eyelids and midface. Plast Reconstr Surg 1999;104(5):1482-1501.
5. Le Louarn C, Buthiau D, Buis J. The face recurve con-cept: medical and surgical applications. Aesthetic Plast Surg 2007;31(3):219-232.
6. Hudson DA, Fernandes DB. Caveats for the use of suspension sutures. Aesthetic Plast Surg 2004;28(3):170-173.
7. Barton FE Jr, Kenkel JM. Direct fixation of the malar pad. Clin Plast Surg 1997;24(2):329-335.
8. Owsley JQ Jr, Zweifler M. Midface lift of the malar fat pad: technical advances. Plast Reconstr Surg 2002;110(2): 674-685.
9. Lowe JB 3rd, Cohen M, Hunter DA, Mackinnon SE. Anal-ysis of the nerve branches to the orbicularis oculi muscle of the lower eyelid in fresh cadavers. Plast Reconstr Surg 2005;116(6):1743-1751.
10. Little JW. Volumetric perceptions in midfacial aging with altered priorities for rejuvenation. Plast Reconstr Surg 2000;105(1):252-266.
11. Goldberg RA. The three periorbital hollows: a para-digm for periorbital rejuvenation. Plast Reconstr Surg 2005;116(6):1796-1804.
12. Gosain AK, Klein MH, Sudhakar PV, Prost RW. A volu-metric analysis of soft-tissue changes in the aging midface using highresolution MRI: implications for facial rejuve-nation. Plast Reconstr Surg 2005;115(4):1143-1155.
13. Shaw RB Jr, Kahn DM. Aging of the midface bony ele-ments: a three-dimensional computed tomographic study. Plast Reconstr Surg 2007;119(2):675-683.
14. Barton FE Jr, Gyimesi IM. Anatomy of the nasolabial fold. Plast Reconstr Surg 1997;100(5):1276-1280.
Figure 8. (A) This 50-year-old woman presented for facial rejuvenation. (B) Facial-cervico lift and blepharoplasty, with malar and periorbital repositioning, as well as jaw line definition and treatment of her naso- and labiomandibular folds.

Chia et al 797
15. Yousif NJ, Matloub MDH, Summers AN. The midface sling: a new technique to rejuvenate the midface. Plast Reconstr Surg 2002;110(6):1541-1557.
16. Finger ER. A 5-year study of the transmalar subperiosteal midface lift with minimal skin and superficial musculo-aponeurotic system dissection: a durable, natural-appear-ing lift with less surgery and recovery time. Plast Reconstr Surg 2001;107(5):1273-1284.
17. Sasaki GH, Cohen AT. Meloplication of the malar fat pads by percutaneous cable-suture technique for mid-face rejuvenation: outcome study (392 cases, 6 years’ experience). Plast Reconstr Surg 2002;110(2):635-654.
18. De Cordier BC, de la Torre JI, Al-Hakeem MS, et al. Reju-venation of the midface by elevating the malar fat pad: review of technique, cases, and complications. Plast Recon-str Surg 2002;110(6):1526-1536.
19. Sulamanidze MA, Fournier PF, Paikidze TG, Sulamanidze GM. Removal of facial soft tissue ptosis with special threads. Dermatol Surg 2002;28(5):367-371.
20. Fuente-del-Campo A. Centrofacial lifting, up to date. Aes-thetic Plast Surg 2001;25(1):29-34.