aged care, disability and diabetes susan carbone diabetes ... · pdf filehelp to keep the...
TRANSCRIPT

Aged care, disability and diabetes
Susan Carbone
Diabetes Educator

Key Learnings
• Principles of diabetes
• Awareness of risk of clients developing diabetes
• Key considerations for clients living with diabetes
• Possible short and long term complications and prevention strategies

Diabetes In Australia
• Diabetes is Australia’s fastest growing chronic disease
• More than 3 million or one in four Australian adults over the age of 25 have either diabetes or impaired glucose tolerance (pre-diabetes)

The Cost of Diabetes

Age Distribution of Diabetes

What is Diabetes?
• Too much glucose (sugar) in the blood due to:
• Pancreas not producing any insulin
or
• Pancreas not producing enough insulin and/or insulin action is blocked

Types of diabetes
• Type 1
• Type 2
• Gestational Diabetes (GDM)
• Impaired fasting glucose (IFG)/impaired glucose
tolerance (IGT)

Type 1 diabetes
Can NOT be prevented or cured
• Pancreas does not produce any insulin
• Insulin producing cells destroyed by the body’s own immune system
• Commonly diagnosed in children and young adults

Type 2 diabetes
May be prevented but not cured
• The pancreas does not produce enough insulin and/or the insulin produced does not work properly (insulin resistance)
• 85-90% of all people with diabetes
Type 1: 15%
Type 2: 85%

10
Eat (any food)
Digest
Glucose levels in
bloodstream rise
Pancreas releases insulin
Cells accept glucose
BGLs fall
Pancreas stops insulin production
Simplified normal process
Body has a complex set of mechanisms and cross checks to maintain BGLs within a very tight tolerance

No diabetes
What would happen if there was no insulin in this picture?

12
Eat (any food)
Digest
Glucose levels in
bloodstream rise
Pancreas releases insulin
Cells accept glucose
BGLs fall
Pancreas stops insulin production
Type 1
• No cure, no
prevention • Auto-immune • Pancreas does
not produce insulin
• Rapid onset • Insulin is the
only therapy • @ 15% of
diagnoses • Growing at 3%
Type 1 diabetes overview

13
Eat (any food)
Digest
Glucose levels in
bloodstream rise
Pancreas releases insulin
Cells accept glucose
BGLs fall
Pancreas stops insulin production
Type 2
• Insulin resistance • Typically older onset • Progressive • Multiple therapies • @ 85% of diagnoses • Growing at 7% p.a • May be prevented or delayed in @ 60%
Type 2 diabetes
Changeable risk factors
What can’t we change?

Risk factors…unchangeable
Age Family history PCOS
GDM Ethnicity

Assessing the risk
• www.health.gov.au/preventionoftype2diabetes

Signs and Symptoms
• Excessive thirst
• Feeling tired
• Frequent urination
• Excessive hunger
• Blurred vision
• Leg cramps
• Headache
• Itching
• Mood swings
• Slow wound healing
• Repeated infections

IFG and IGT
• Previously known as pre-diabetes
• BGLs are not high enough to diagnose diabetes, but higher than normal.
• Healthy lifestyle changes can prevent or delay progression to diabetes
• Higher risk of heart disease
Gestational Diabetes
• Effects 5-8% of Australian pregnancies
• Temporary form of diabetes
• Risk factors = family history, increased maternal
age, overweight, ethnicity,
• Increased risk of Type 2 diabetes to mother and
baby in future

Why worry about diabetes? Chronic Complications
High blood glucose levels over time may cause:
• Cardiovascular disease
• Damage to the eyes (retinopathy)
• Damage to the kidneys (nephropathy)
• Damage to the nerves (neuropathy)
• Problems with the feet
• Infections and slow healing
• Problems with the teeth and gums
• Erectile dysfunction

Complications of diabetes
ACUTE CHRONIC
What are the consequences of these complication?
Symptomatic Hyperglycaemia
BGL > 15mmol/L
• Heart
• Brain
• Nerves
• Eyes
• Kidneys
• Feet
• Teeth and gums
4
10
15
Hypoglycaemia BGL < 4mmol/L

How can I help to manage his/her diabetes?
• Help the person adopt a number of healthy lifestyle behaviours
• Assist in the correct administration of medications and/or insulin
• Assist and encourage the person to attend annual reviews with diabetes team
Help to keep the daily BGL within the target range

Why manage diabetes?
• To reduce the risk of diabetes complications
• To prevent falls or stroke due to hypo or acute
hyperglycaemia
• To improve general health status
• To improve daily quality of life
Acute complications
Acute (Short Term)
• Hypoglycaemia ‘Hypo’ less than 4mmol/L
• Hyperglycaemia ‘Hyper’ more than 15mmol/L

Blood glucose monitoring

• Use different fingers
• Ensure hands are clean and dry
• Don’t prick on tip of finger...more painful!
• Single use lancet needles
(?retractable lancets required)
Is the BGL within resident target range??
Record BGL levels. Notify if any concerns
NDSS
Blood Glucose Monitoring

Lancets & Pen needles are for single use only.
Pain & discomfort Infection risk Lipohypertrophy Scarring & callouses Dose inaccuracy

When to test

Hypoglycaemia Signs and Symptoms
• Dizziness
• Light headedness
• Weakness, trembling or shaking
• Sweaty
• Headache
• Tingling lips, fingers
• Tearful/crying
• Irritability
• Lack of concentration or behaviour change
• Hunger
• Slurred speech
• Unconscious/
fitting

Causes of Hypoglycaemia
• Delaying or missing a meal or snack
• Not eating enough carbohydrate
• Too much insulin or diabetes tablets
• Unplanned physical activity
• More strenuous exercise than usual
• Drinking alcohol
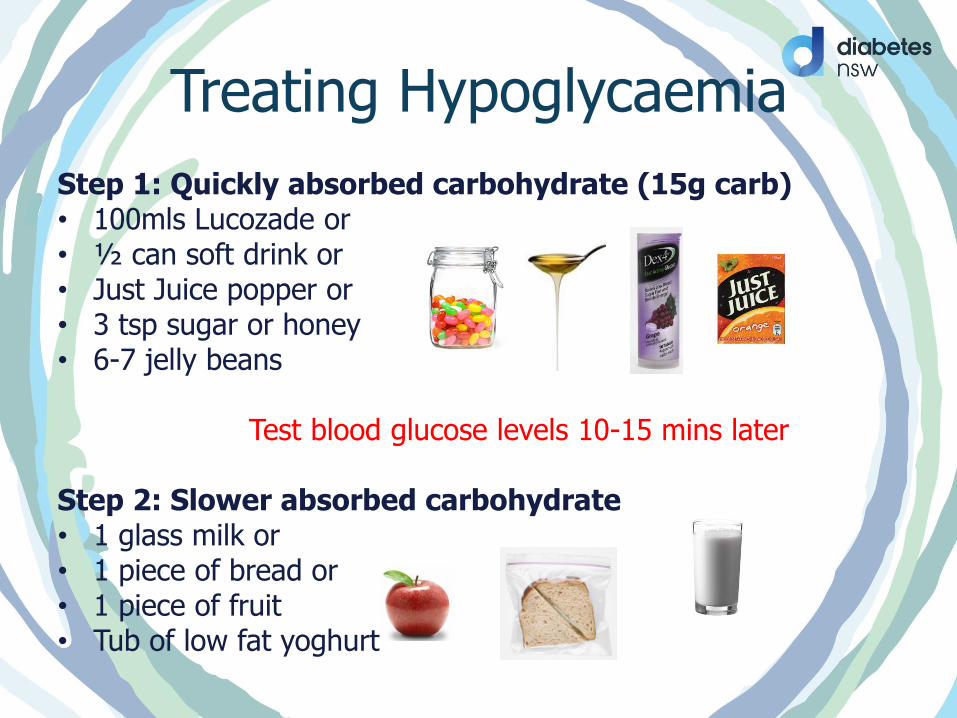
Treating Hypoglycaemia
Step 1: Quickly absorbed carbohydrate (15g carb) • 100mls Lucozade or • ½ can soft drink or • Just Juice popper or • 3 tsp sugar or honey • 6-7 jelly beans
Test blood glucose levels 10-15 mins later
Step 2: Slower absorbed carbohydrate • 1 glass milk or • 1 piece of bread or • 1 piece of fruit • Tub of low fat yoghurt

Severe Hypoglycaemia
• Call an ambulance if the person is unconscious
• Recovery position
• Stay with person
Administer Glucagon if trained

Hypoglycaemia in the elderly or disability
• Increased risk of hypos in the elderly
• Impaired hypo awareness
• Impaired ability of body to respond and recover from a hypo
• Polypharmacy increases risk of hypo’s
• Difficulty communicating
Hyperglycaemia

When a high is too high
• Type 1 – high may be due to insulin deficiency, increasing the risk of DKA – life threatening
• Type 2 - Hyperosmolar Osmotic Non-ketoacidosis (HONK) Treat underlying cause • Refer to sick day management plan: • Do not withhold insulin – may need dose altered • Testing blood glucose levels every 2 – 4 hours • Drinking extra non sweetened fluids to avoid dehydration • If uncertain contact doctor or diabetes educator

May not be able to tell you when they are having chest pain or a heart attack. They may not even feel it due to nerve damage to heart.
Coronary Heart Disease

Cardiovascular Disease
• Cardiovascular disease accounts for >50% of deaths in Type 2 diabetes
• People with diabetes at greater risk of developing cardiovascular disease
• Maintaining blood pressure, cholesterol and BGL levels within target range decreases risk
Care of People with Diabetes, 3rd ed. Dunning, 2009.

• Diabetes is the major cause of kidney disease in Australia
• Uncontrolled or poorly managed diabetes damages the nephrons -filtration units
• Kidney disease can lead to kidney failure requiring dialysis
Insulin is metabolised by kidneys and excreted in urine. As kidneys age and become less efficient they metabolise insulin more slowly – meaning insulin stays in the system for longer. Older people with renal impairment may need a reduction in dose.
Kidney Disease

Vision affected by Retinopathy
Diabetic Retinopathy
Falls risk !!!! Reduced ability to perform ADL including BGL testing

Peripheral Neuropathy High BGLs can damage the nerve transmission affecting the impulse to the brain e.g. if a person walks barefoot and treads on a nail/pin, a healthy nerve would send a signal to the brain ‘telling’ the person to take the foot off the pin and check the affected area. However, in a person with neuropathy the signal to the brain is impaired/lost and the person might not feel any pain. What would happen as a consequence? First symptoms of neuropathy can be pins and needles in the feet or legs (less commonly arms, fingers), tingling, hot and cold feet, cramps and/or numbness. Can also contribute to:
• Impotence in men • Digestion problems • Incontinence

Other complications
• Teeth and gums: gum infections more common in people with diabetes.
• Susceptibility to infection
• Liver: Non Alcoholic Fatty Liver Disease (NAFLD) associated with insulin resistance and increased waist measurement.
• Depression: affects approximately 50% of people with a chronic disease.

Wounds: Feet and Legs

Foot Care
• The daily foot hygiene time is the perfect opportunity to check feet thoroughly and identify any problems
• Self care capabilities:
– Can the resident see their feet
– Can the resident reach their feet
– Can the resident cut toenails & provide care as necessary
– Does the resident want to care for their own feet

What to look for?

High Risk Feet • Had a foot ulcer in the past
• Had an amputation in the past
• An ulcer at present
• Decreased sensation
• Corn and calluses
• Deformed thick toenails or discoloured nails
• Foot deformities such as bunions, hammer toes, bony prominences
• Any resident with diabetes should see a podiatrist immediately if they have a high risk foot and develop problems

Blood Supply
• Inadequate blood supply:
– Cold feet
– Frequent leg cramps
– Infections and ulceration
– Pain and/or aching when walking
– Changes to the skin colour of the feet
– Numbness, burning and/or tingling

Footwear
• Socks
Natural fibre socks such as wool or cotton are best
Fit correctly
If the seams are prominent, wear socks inside out
Ensure top of sock is not too tight around the leg
• Shoes
Natural materials such as canvas and leather are best
Enough room in the shoe
Firm heel grip, holds the foot securely
Fastened with laces, buckles, or velcro

Medications
• Classes of Medications – Biguanides
– Sulphonylureas
– Thiazolidinediones (Glitazones)
– Alpha Glucose Inhibitors
– DPP-4 Inhibitors
– Incretin Mimetics
– SGLT2 Inhibitors
– Combinations

Side Effects of Biguanides
• Nausea, diarrhoea, constipation, metallic taste in the mouth • Must be ceased immediately prior to surgery and
immediately after surgery, or any procedures that require radio-opaque dye
• Always take during or after food • Caution for elderly:
– Reduced appetite – Severe renal, heart, and liver disease – Small risk of hypoglycaemia

Biguanides
• Metformin, Diabex, Diabex XR, Diaformin, Diaformin XR, Glucobete, Formet, Glocomet, Glucophage, Metex
• Help lower the BGL by:
– Reducing the amount of stored glucose released by the liver
– Slowing absorption of glucose from the gut
– Helping the body to become more sensitive to insulin

Sulphonylurea • Gliclazide: Diamicron, Diamicron MR,
Glyade, Glyade MR, Genrx
Glibenclamide: Doanil, Glimel
Glipizide: Melizide, Minidiab
Glimepiride: Amaryl, Dimirel, Aylide
• Helps lower BGL by stimulating the pancreas
to release more insulin
• Take just prior to the meal

Side Effects of Sulphonylurea
• Hypoglycaemia, weight gain, skin rashes, stomach
upset (nausea and diarrhoea), jaundice
• Caution for elderly:
– Some sulphonylureas have a long half-life therefore increasing the risk of Hypoglycaemia,
such as Daonil.

Thiazolidinediones (Glitizones) • Rosiglitizone: Avandia
• Pioglitizone: Actos
• Help to lower BGL’s by increasing the effect of your own insulin especially on muscle and fat cells, they improve insulin resistance
• Low risk of hypoglycaemia

Side effects of Glitizones
• Weight gain, fluid accumulation, not to be taken by people who have liver disease
• Caution in elderly
– Avoid in people with heart failure
– Regular checks of liver function

Alpha Glucosidase Inhibitors
• Acarbose: Glucobay
• Help to slow down the digestion and
absorption of some dietary carbohydrates
in the gut
• Risk of hypoglycaemia low
• Must be taken just before a meal

Side Effects of Alpha Glucosidase Inhibitors
• Flatulence, bloating, diarrhoea
• They need to be started at low doses and increased slowly
• Caution in elderly:
– Diarrhoea and fluid loss

DPP-4 Inhibitors
• Linagliptin: Trajenta
• Saxagliptin: Onglyza
• Sitagliptin: Januvia
• Vildagliptin: Galvus
• Alogliptin: Nesina
• Help to inhibit the enzyme DPP-4 which
enhances the levels of active incretin hormones
• Incretin hormones increase insulin secretion
and decrease glucagon secretion

Side Effects of DPP-4 Inhibitors
• Few side effects
• Low risk of Hypoglycaemia
• Not likely to cause weight gain
• Caution in elderly:
– Consider lower doses if there are
kidney or liver problems

Incretin Mimetics
• Exanatide: Byetta
• Injected medication
• Helps to lower BGL’s by:
– Stimulating the pancreas to release more insulin in response to eating carbohydrates
– Reducing the amount of glucagon released from the pancreas after the meal
– Slow down the passage of food from the stomach to the gut so food is absorbed more slowly
– Increases a feeling of fullness after eating
– Inject twice a day within 1 hour of breakfast & dinner & at least 6 hours apart.

Side Effects of Incretin Mimetics
• Nausea, vomiting, constipation, diarrhoea
effect other medication passing through
the stomach
• Allergic reactions may occur
• Caution in elderly:
– Not recommended for people with severe gastrointestinal disease or severe kidney disease

SGLT2 Inhibitor
• Canagliflozin: Invokana
• Dapagliflozin: Forxiga
• Selectively inhibit SGLT2 in the kidney
• Lowers renal threshold for glucose and
reduces glucose reabsorption
• Increases urinary glucose excretion

Side Effects of SGLT2 Inhibitors
• Hypoglycaemia, thrush, UTI, frequent urination, balanoposthitis (inflammation of the glans and foreskin of the penis), thirst
• Caution in elderly
– All of the above
– Postural hypotension, dehydration, syncope
– Not recommended in people with severe kidney disease

Combination Medications

What is insulin?
• Insulin is a hormone that is produced by the pancreas
• It lowers blood glucose levels
• The insulin you inject works the same way as the insulin made by the body
• Insulin is the key that opens the cells in our body so they
can store glucose and use it for energy

Insulin

How to store insulin
DO
Store unopened insulin at the front of the door shelves of the refrigerator
Store opened insulin at room temperature
(below 25 degrees)
Store insulin in a cooler bag if living in a hot climate or travelling
DO NOT
X Leave insulin in the car or where it will get hot
X Store insulin in the freezer or at the back of the fridge
X Shake insulin too hard
X Use insulin after its expiry date

Where to inject insulin?

Different Insulin • Novonordisk
Levemir
Novorapid
Actrapid
Novomix 30
Mixtard 30/70
Mixtard 50/50
Protaphane
• Lilly
Humalin R
Humalin NPH
Humamix 25
Humamix 50
Humalin 30/70
Sanofi Aventis Lantus Apidra



Summary
• There are a number of considerations when
managing diabetes in the elderly and/or disability
• Individual care plans are essential to provide
accurate treatment on a range of areas
• Target BGLs
• Sick day management plans
• Hypo treatments
• Insulin administration – timing is vital
When in doubt – speak to GP and CDE
