agenda item: tb 195/11 subject: assurance framework report board/trust board documents... · agenda...
TRANSCRIPT
AGENDA ITEM: TB 195/11
SUBJECT: Assurance Framework Report
DATE OF MEETING: 06 December 2011
PREPARED BY: Jane Burke, Assistant Company Secretary
FOIA STATUS: No exemption Choose an item.
Part exemption applies to page:
REVIEW DATE: 06 December 2012
LINK TO VALUES: Accountability
LINK TO STRATEGIC PRIORITIES: 6. Quality & Governance
LINK TO NHS CONSTITUTION: Quality of Care & Environment
LINK TO BOARD RISK REGISTER: 8. Maintain an effective system of internal control
1.0 BOARD ACTION The Board are asked to review the Assurance Framework and to confirm agreement with the content and the assurances described.
2.0 INTRODUCTION The paper provides the revised Assurance Framework which outlines the high level risks to the organisations strategic objectives.
Effective governance and assurance arrangements are essential to providing confidence that the organisation is focused effectively on the delivery of its objectives. Boards are required to seek regular assurance to satisfy them that systems of internal control are functioning effectively to manage risks to delivery of objectives.
The Board Assurance Framework is a key document whose purpose is to provide the Board with reasonable assurance around the management of strategic risks and that internal control systems are functioning effectively.
The Department of Health guidance, Building an Assurance Framework (2003) describes how Boards should seek assurances against the effectiveness of the controls in place to mitigate key risks The maintenance and monitoring of the Board Assurance Framework will provide confidence that there are robust risk management arrangements, that these arrangements are subject to appropriate scrutiny and that the Board can be confident that there is evidence that risks to achieving its objectives are appropriately managed.
3.0 BACKGROUND
During 2009 the Board led the overall programme of work to embed the Enterprise Assurance Management approach within the Trust. This commenced with the Board identifying its risk appetite and defining risk tolerances across key areas of Business Activity.
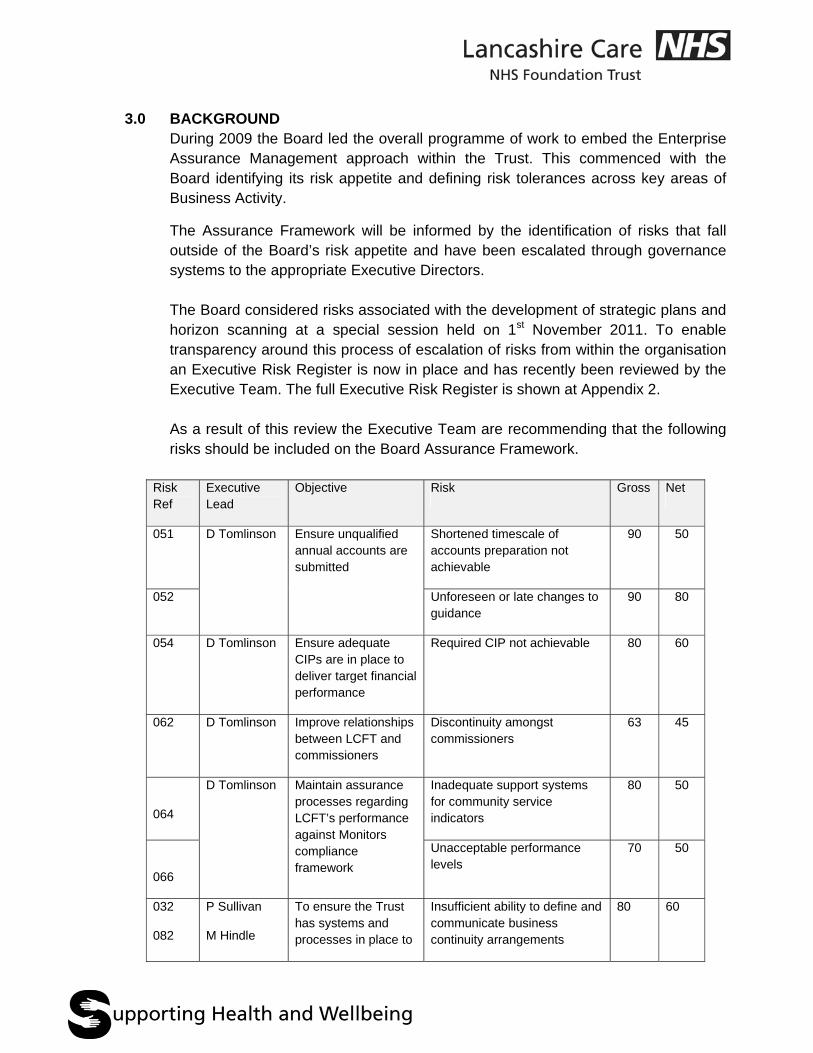
The Assurance Framework will be informed by the identification of risks that fall outside of the Board’s risk appetite and have been escalated through governance systems to the appropriate Executive Directors. The Board considered risks associated with the development of strategic plans and horizon scanning at a special session held on 1st November 2011. To enable transparency around this process of escalation of risks from within the organisation an Executive Risk Register is now in place and has recently been reviewed by the Executive Team. The full Executive Risk Register is shown at Appendix 2. As a result of this review the Executive Team are recommending that the following risks should be included on the Board Assurance Framework.
Risk Ref
Executive Lead
Objective Risk Gross Net
051 D Tomlinson Ensure unqualified annual accounts are submitted
Shortened timescale of accounts preparation not achievable
90 50
052 Unforeseen or late changes to guidance
90 80
054
D Tomlinson Ensure adequate CIPs are in place to deliver target financial performance
Required CIP not achievable 80 60
062
D Tomlinson Improve relationships between LCFT and commissioners
Discontinuity amongst commissioners
63 45
064
D Tomlinson Maintain assurance processes regarding LCFT’s performance against Monitors compliance framework
Inadequate support systems for community service indicators
80 50
066
Unacceptable performance levels
70 50
032
082
P Sullivan
M Hindle
To ensure the Trust has systems and processes in place to
Insufficient ability to define and communicate business continuity arrangements
80 60
support Emergency Planning and business continuity
Table 1
The starting point for any assurance framework is the identification of the organisation’s goals/priorities and key objectives for the year. The previous Assurance Framework reported to the Board in June 2011 has been revised to clearly map risks to the current priorities.
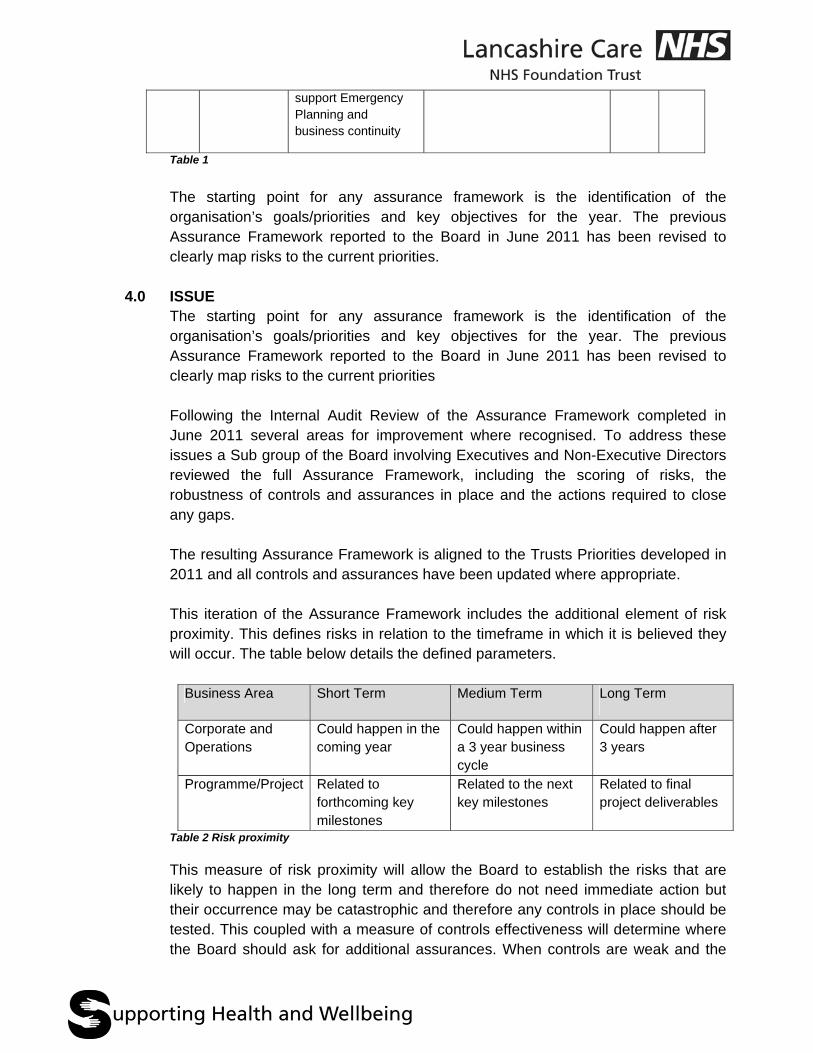
4.0 ISSUE The starting point for any assurance framework is the identification of the organisation’s goals/priorities and key objectives for the year. The previous Assurance Framework reported to the Board in June 2011 has been revised to clearly map risks to the current priorities Following the Internal Audit Review of the Assurance Framework completed in June 2011 several areas for improvement where recognised. To address these issues a Sub group of the Board involving Executives and Non-Executive Directors reviewed the full Assurance Framework, including the scoring of risks, the robustness of controls and assurances in place and the actions required to close any gaps. The resulting Assurance Framework is aligned to the Trusts Priorities developed in 2011 and all controls and assurances have been updated where appropriate. This iteration of the Assurance Framework includes the additional element of risk proximity. This defines risks in relation to the timeframe in which it is believed they will occur. The table below details the defined parameters.
Business Area Short Term Medium Term Long Term
Corporate and Operations
Could happen in the coming year
Could happen within a 3 year business cycle
Could happen after 3 years
Programme/Project
Related to forthcoming key milestones
Related to the next key milestones
Related to final project deliverables
Table 2 Risk proximity
This measure of risk proximity will allow the Board to establish the risks that are likely to happen in the long term and therefore do not need immediate action but their occurrence may be catastrophic and therefore any controls in place should be tested. This coupled with a measure of controls effectiveness will determine where the Board should ask for additional assurances. When controls are weak and the
net risk is high, the Board should consider this exposure and require appropriate controls to be demonstrated.
5.0 FUTURE REPORTING Through the development of an IT platform to support the roll out of Enterprise Assurance Management future reports will contain greater detail and allow the Board to gain confidence that Enterprise Assurance Management is becoming embedded throughout the Trust. Appendix 3 demonstrates the current figures of risk reporting via the EAM system however this should be seen as illustrative of the future reporting that will be available to the Board. At this stage the data is not yet validated and further progress has been made since the report was created. It is planned to report progress to the Board in March 2012 together with the revised Assurance Framework.
6.0 SUMMARY AND CONCLUSIONS The Assurance Framework has now been reviewed in full. It includes risks relevant to the enlarged organisation. The introduction of risk proximity will provide the Board with an additional dimension to risk management focussing attention on controls when impacts are high or risks are faced in the short term. This approach allows the Board to gain assurance that its strategic aims are deliverable as risks in the long term are also identified and controlled appropriately.
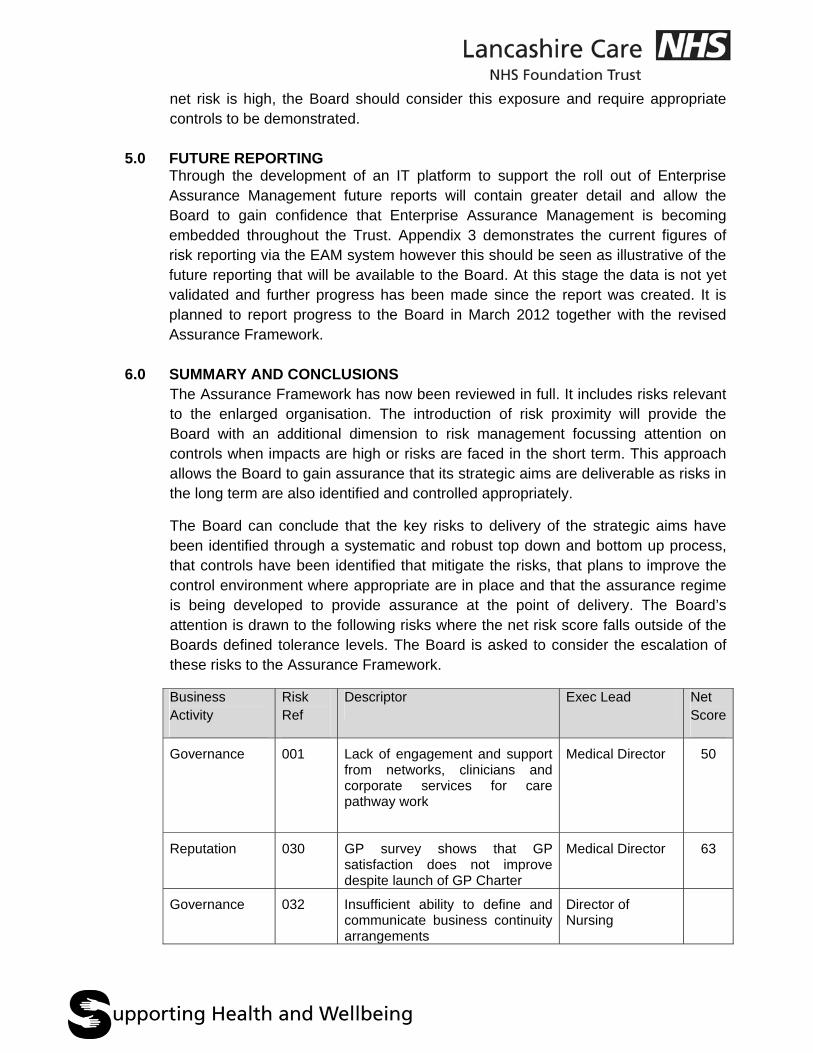
The Board can conclude that the key risks to delivery of the strategic aims have been identified through a systematic and robust top down and bottom up process, that controls have been identified that mitigate the risks, that plans to improve the control environment where appropriate are in place and that the assurance regime is being developed to provide assurance at the point of delivery. The Board’s attention is drawn to the following risks where the net risk score falls outside of the Boards defined tolerance levels. The Board is asked to consider the escalation of these risks to the Assurance Framework.
Business Activity
Risk Ref
Descriptor Exec Lead Net Score
Governance 001 Lack of engagement and support from networks, clinicians and corporate services for care pathway work
Medical Director 50
Reputation 030 GP survey shows that GP satisfaction does not improve despite launch of GP Charter
Medical Director 63
Governance 032 Insufficient ability to define and communicate business continuity arrangements
Director of Nursing
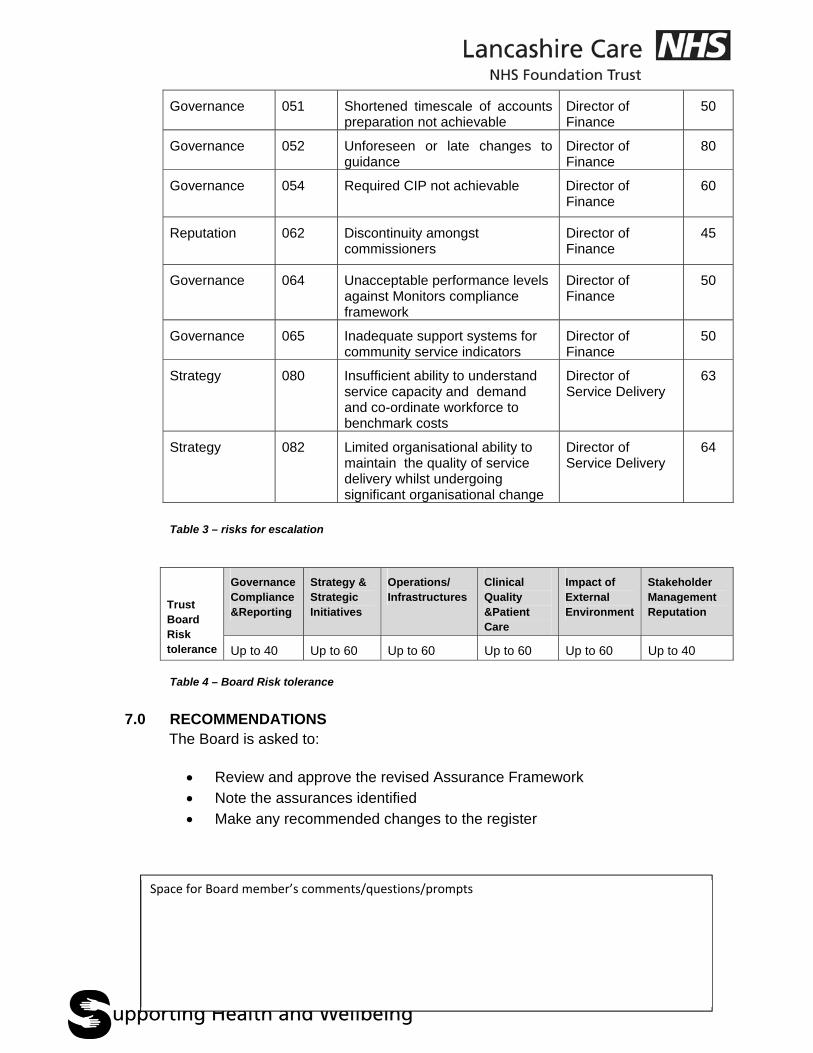
Governance 051 Shortened timescale of accounts preparation not achievable
Director of Finance
50
Governance 052 Unforeseen or late changes to guidance
Director of Finance
80
Governance 054 Required CIP not achievable Director of Finance
60
Reputation 062 Discontinuity amongst commissioners
Director of Finance
45
Governance 064 Unacceptable performance levels against Monitors compliance framework
Director of Finance
50
Governance 065 Inadequate support systems for community service indicators
Director of Finance
50
Strategy 080 Insufficient ability to understand service capacity and demand and co-ordinate workforce to benchmark costs
Director of Service Delivery
63
Strategy 082 Limited organisational ability to maintain the quality of service delivery whilst undergoing significant organisational change
Director of Service Delivery
64
Table 3 – risks for escalation
Trust Board Risk tolerance
Governance Compliance &Reporting
Strategy & Strategic Initiatives
Operations/ Infrastructures
Clinical Quality &Patient Care
Impact of External Environment
Stakeholder Management Reputation
Up to 40 Up to 60 Up to 60 Up to 60 Up to 60 Up to 40 Table 4 – Board Risk tolerance
7.0 RECOMMENDATIONS
The Board is asked to:
Review and approve the revised Assurance Framework Note the assurances identified Make any recommended changes to the register
Space for Board member’s comments/questions/prompts
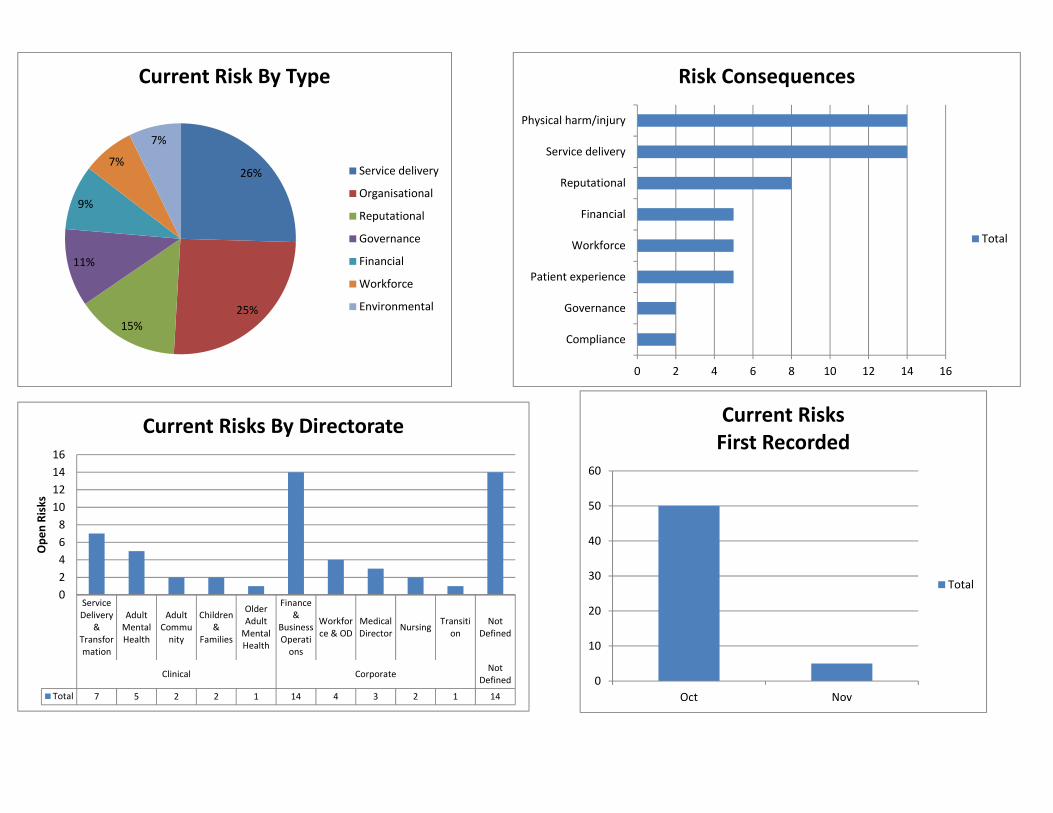
26%
25%
15%
11%
9%
7%
7%
Current Risk By Type
Service delivery
Organisational
Reputational
Governance
Financial
Workforce
Environmental
0 2 4 6 8 10 12 14 16
Compliance
Governance
Patient experience
Workforce
Financial
Reputational
Service delivery
Physical harm/injury
Risk Consequences
Total
ServiceDelivery
&Transformation
AdultMentalHealth
AdultCommunity
Children&
Families
OlderAdultMentalHealth
Finance&
BusinessOperations
Workforce & OD
MedicalDirector
NursingTransition
NotDefined
Clinical CorporateNot
Defined
Total 7 5 2 2 1 14 4 3 2 1 14
0
2
4
6
8
10
12
14
16
Ope
n Risks
Current Risks By Directorate
0
10
20
30
40
50
60
Oct Nov
Current RisksFirst Recorded
Total
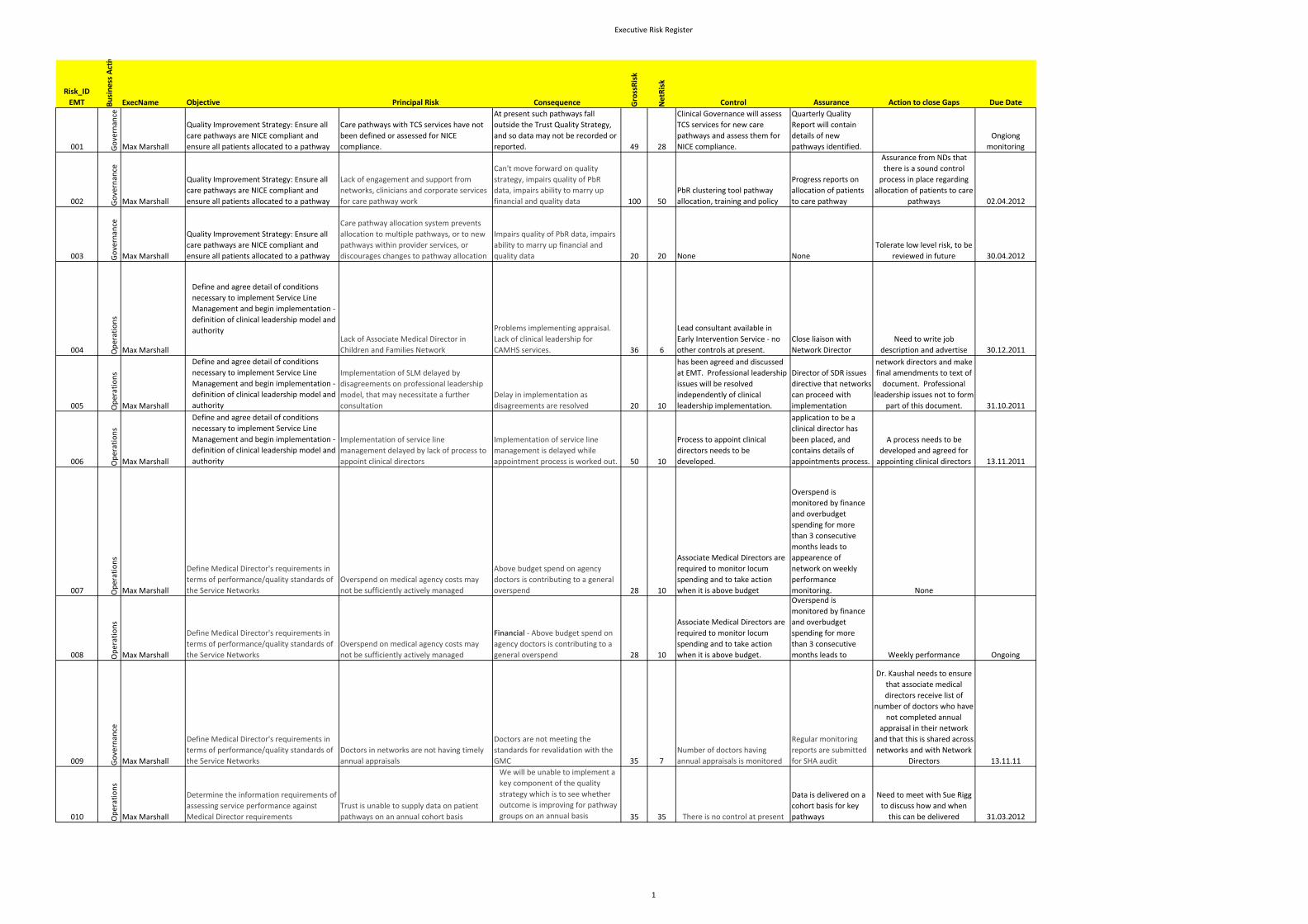
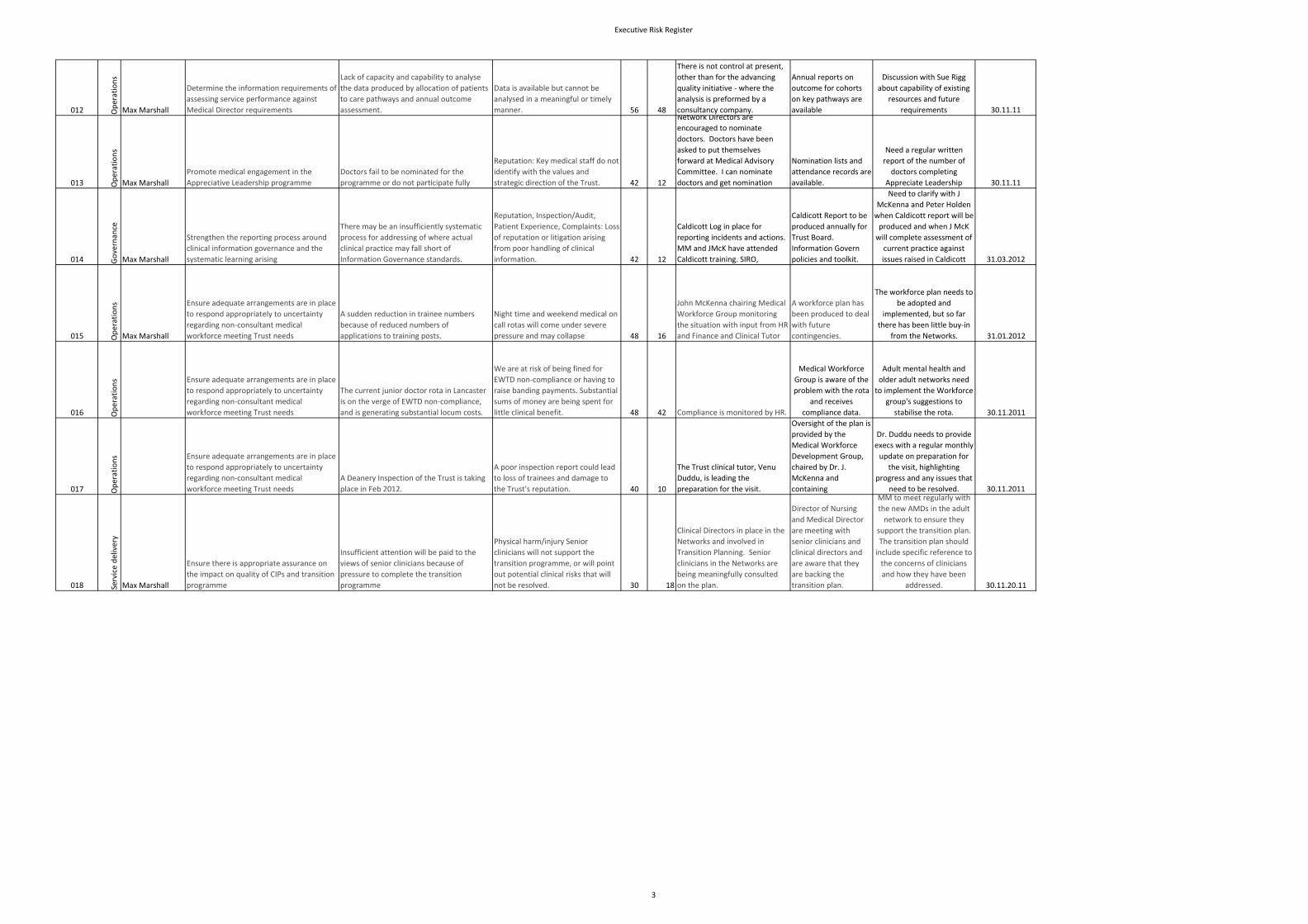
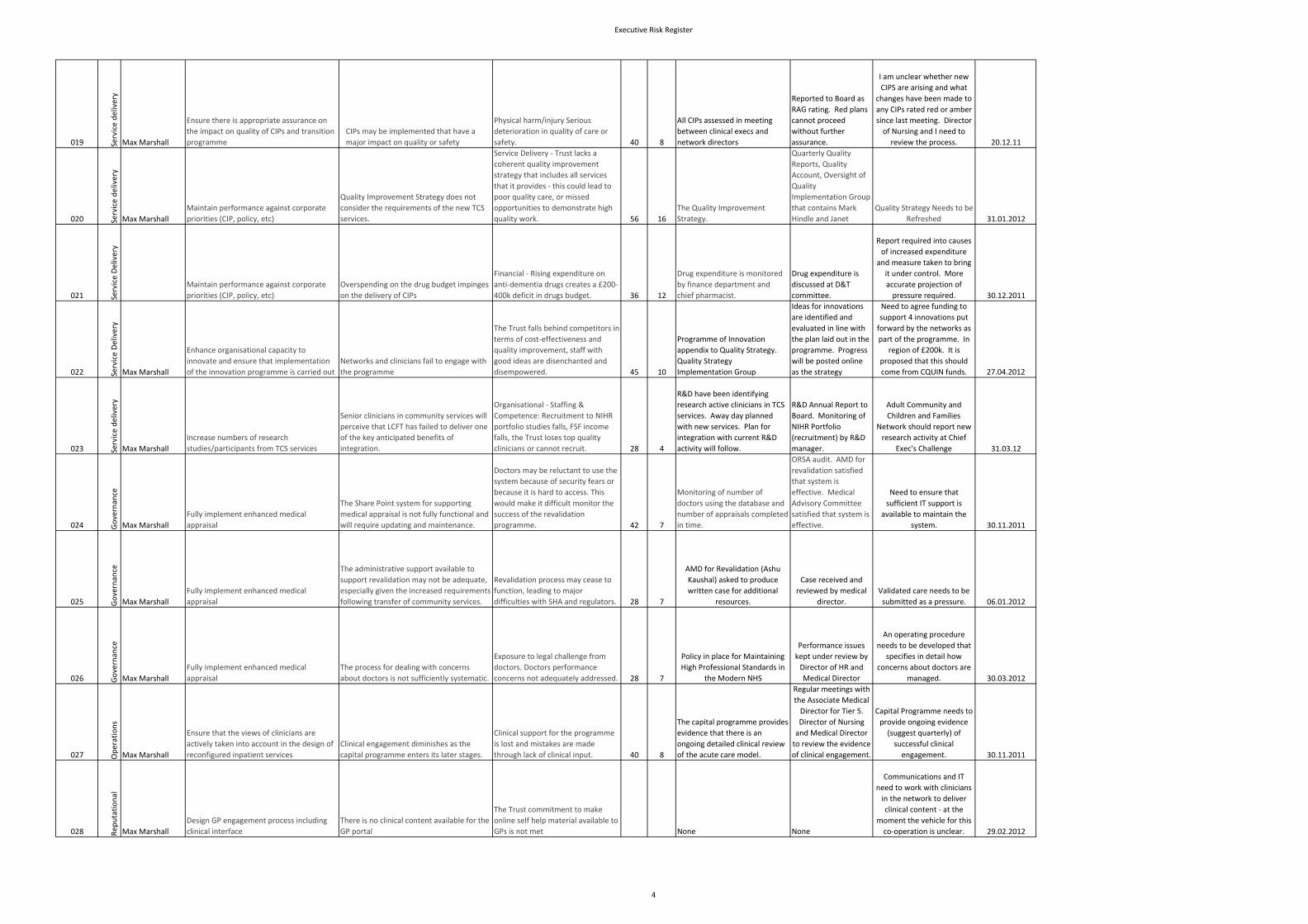
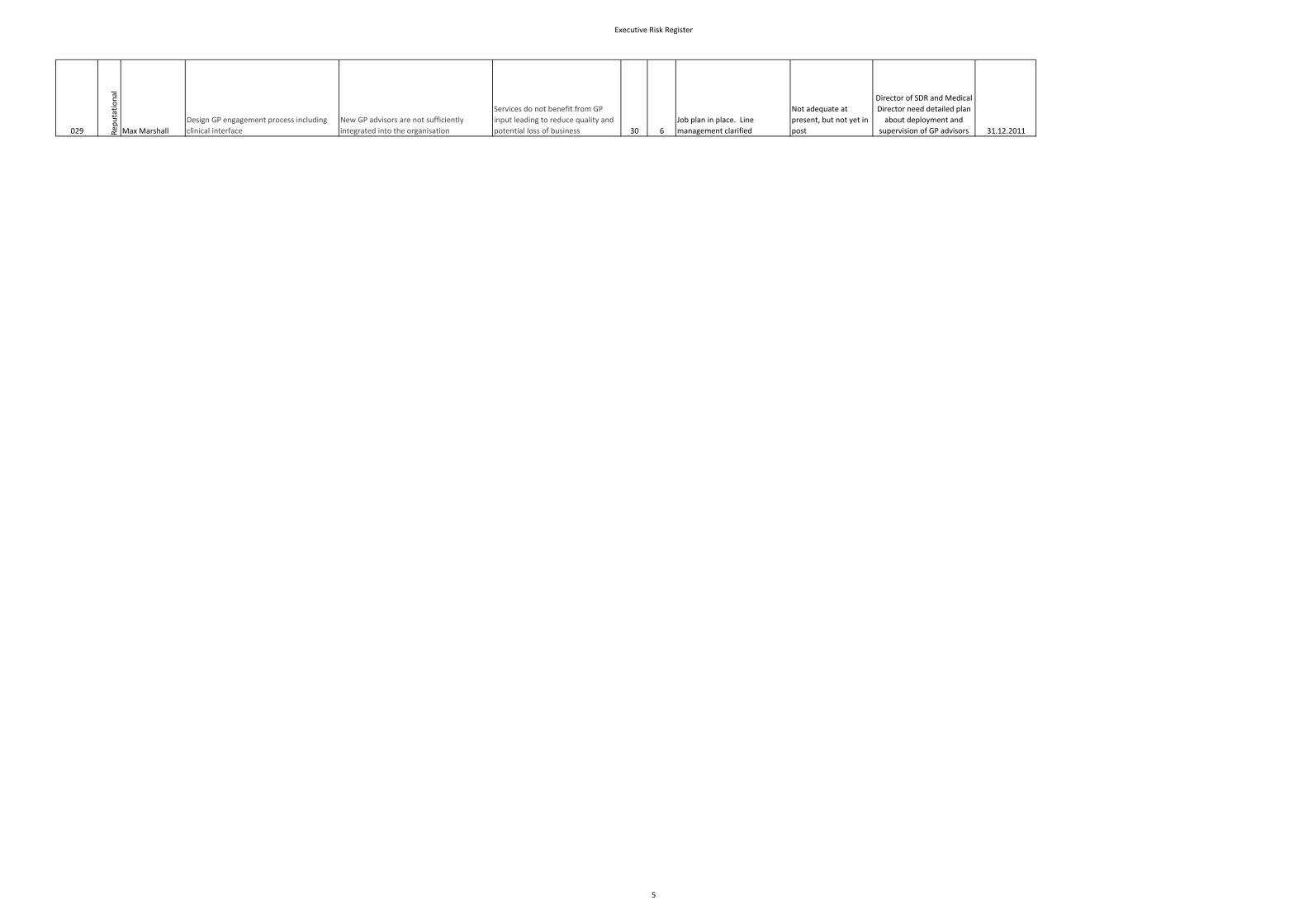
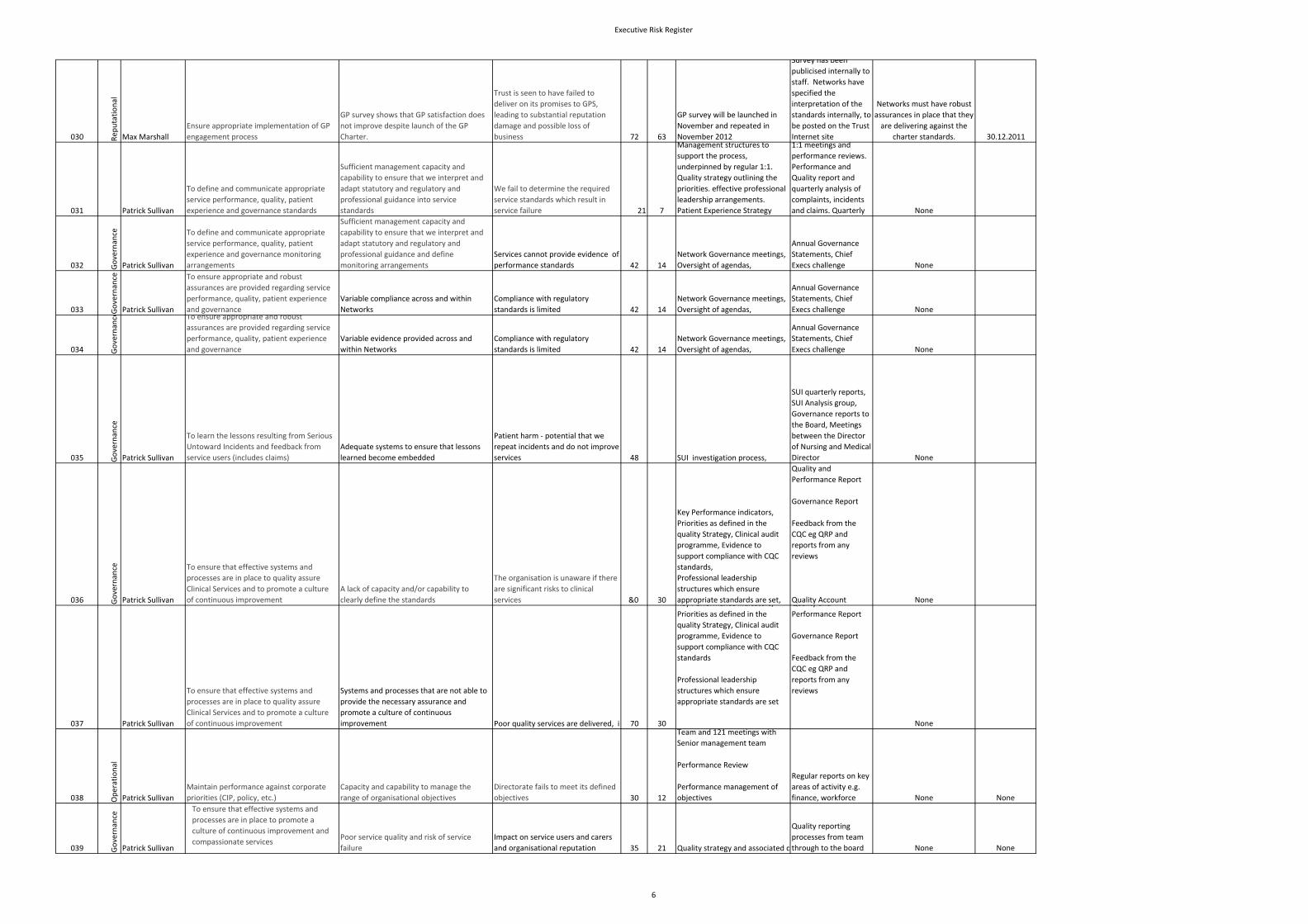
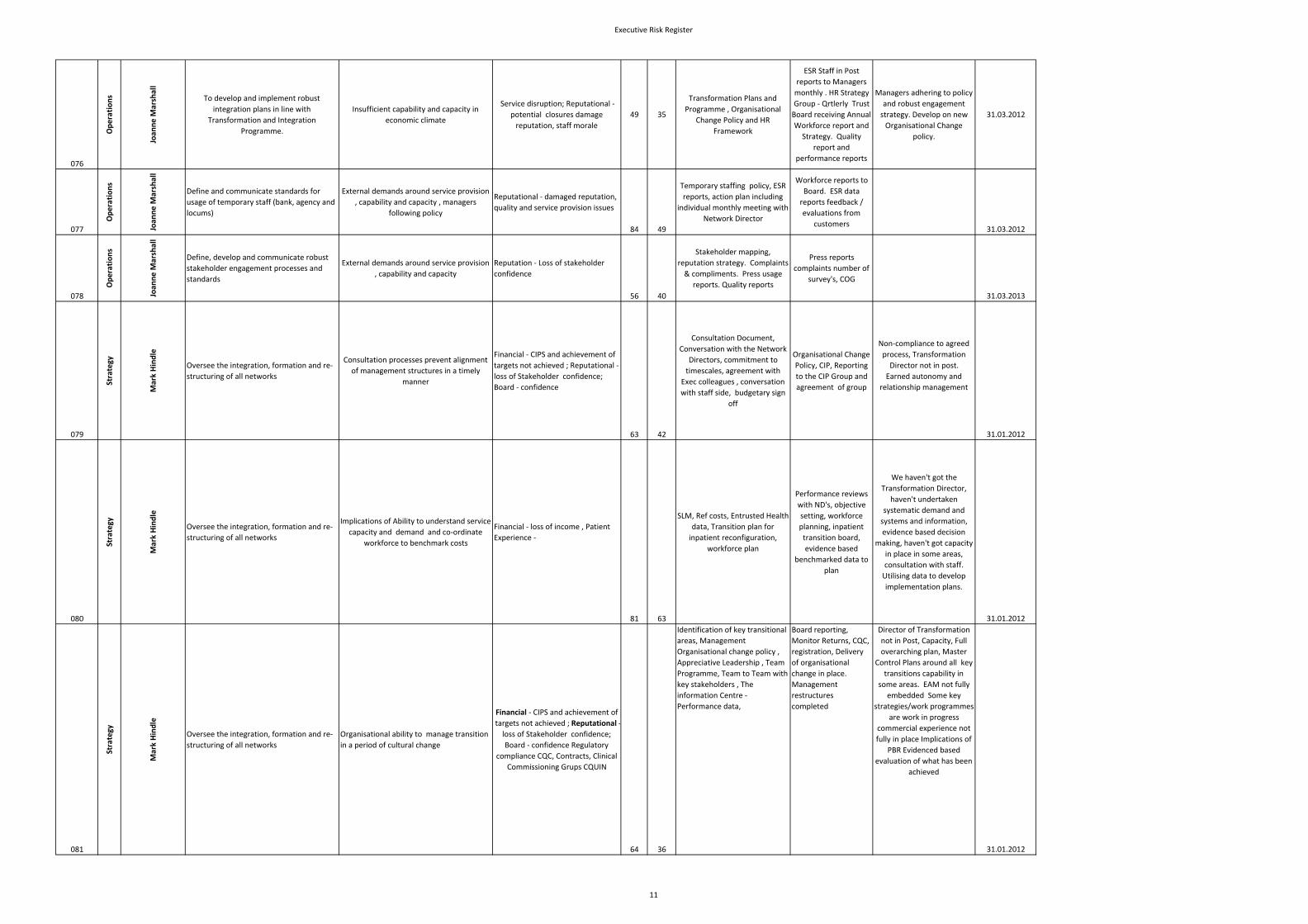
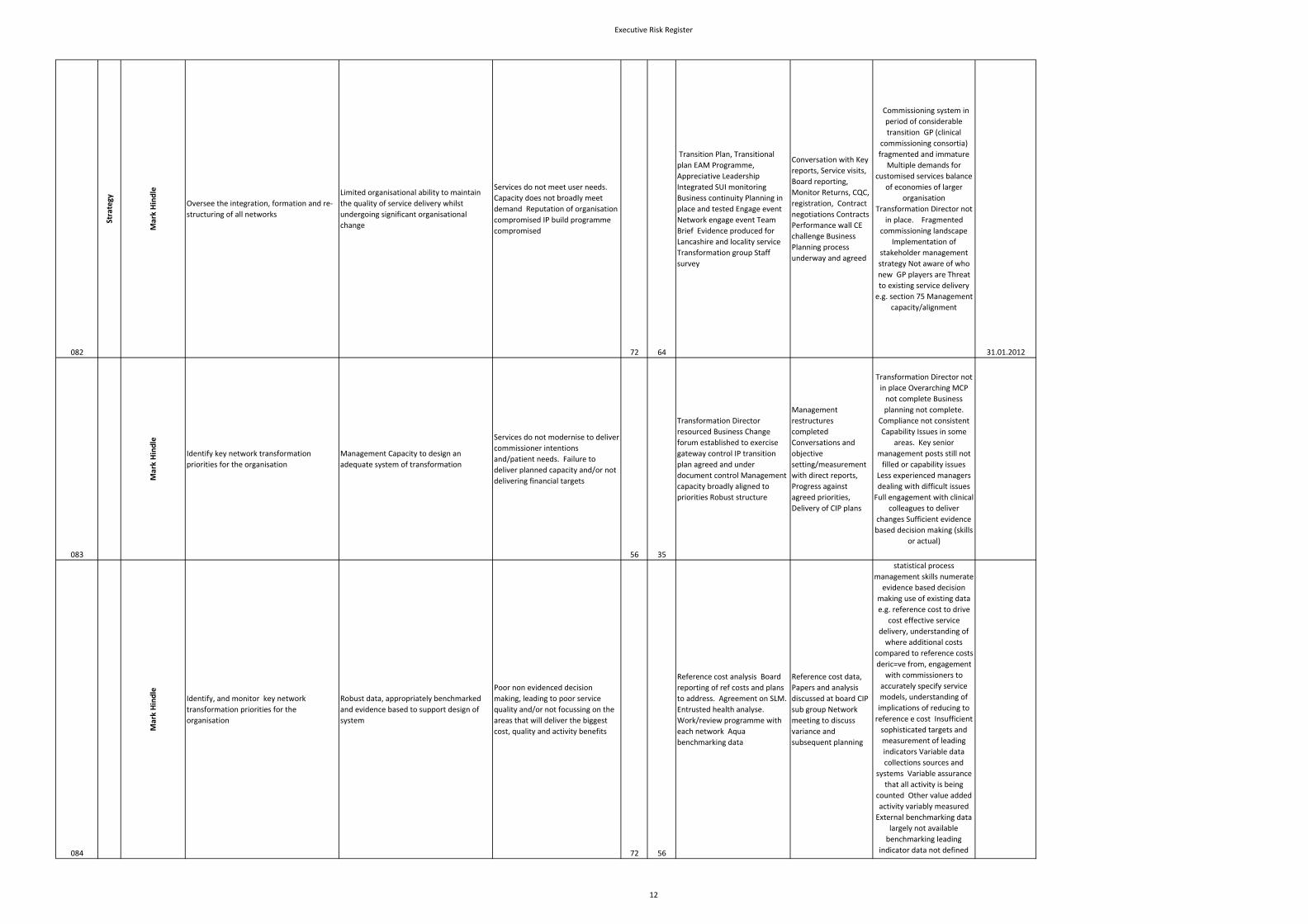
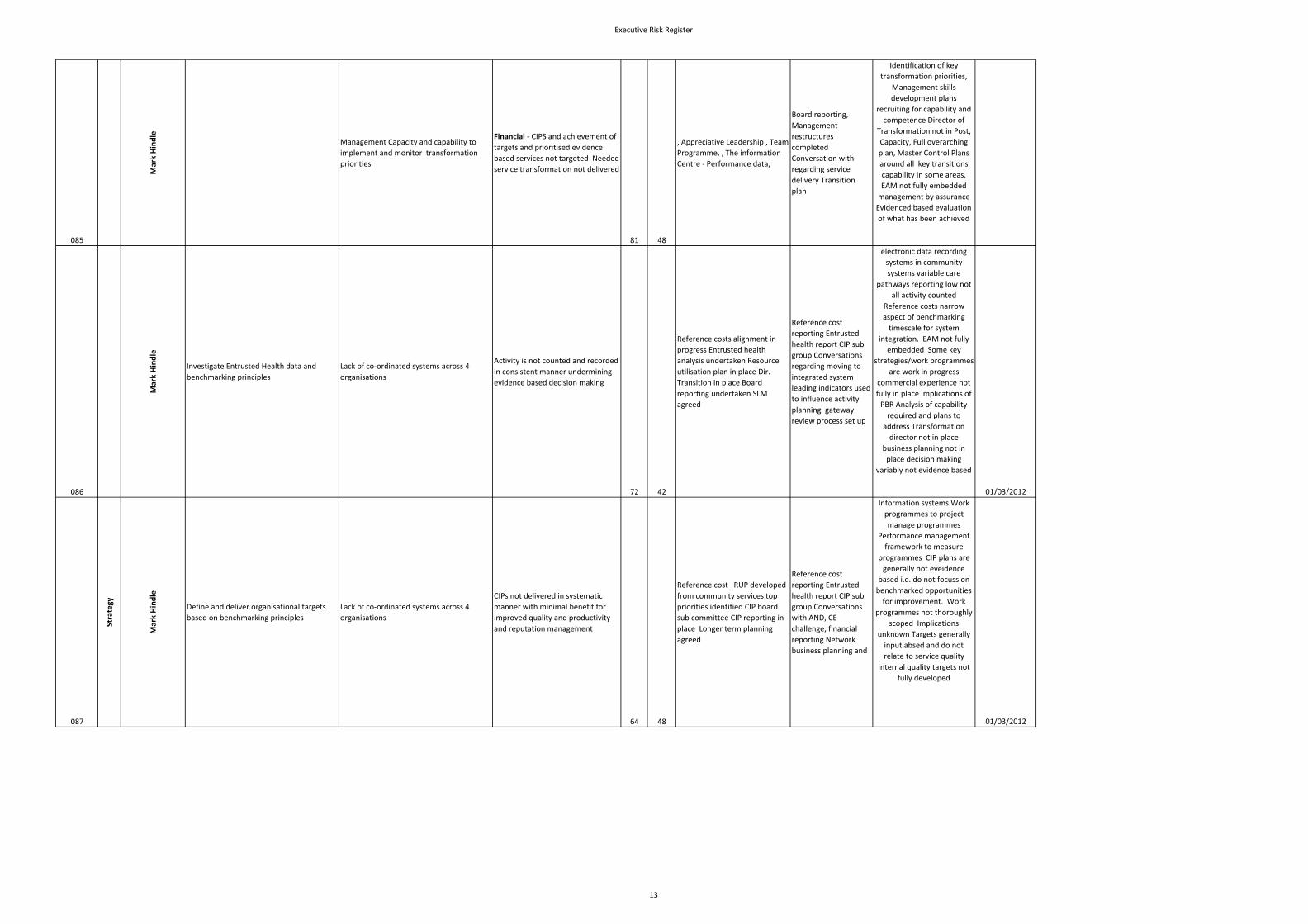
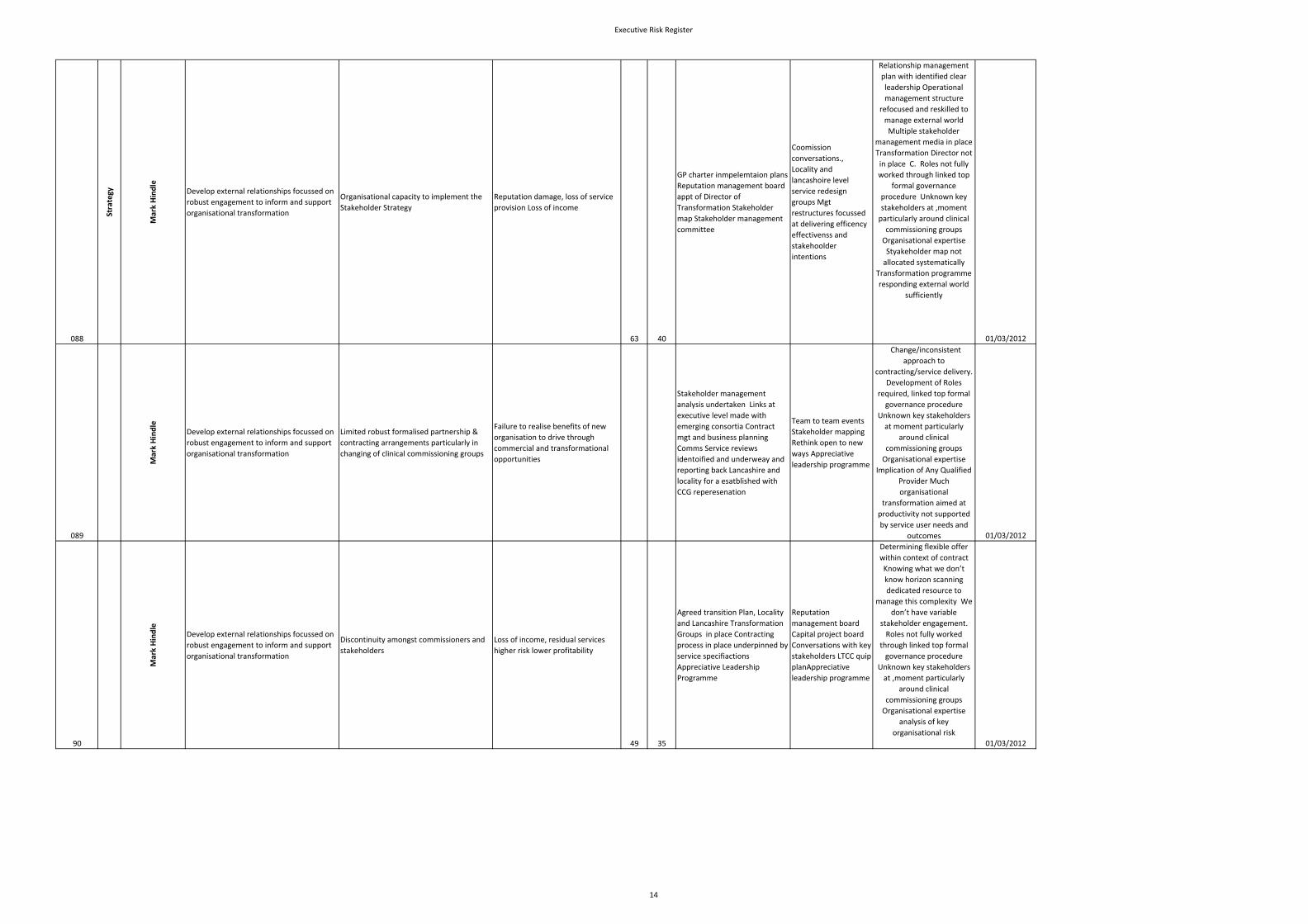
Executive Risk Register
Risk_ID EMT Bu
sine
ss Activ
ExecName Objective Principal Risk Consequence GrossRisk
NetRisk
Control Assurance Action to close Gaps Due Date
001 Governan
ce
Max Marshall
Quality Improvement Strategy: Ensure all
care pathways are NICE compliant and
ensure all patients allocated to a pathway
Care pathways with TCS services have not
been defined or assessed for NICE
compliance.
At present such pathways fall
outside the Trust Quality Strategy,
and so data may not be recorded or
reported. 49 28
Clinical Governance will assess
TCS services for new care
pathways and assess them for
NICE compliance.
Quarterly Quality
Report will contain
details of new
pathways identified.
Ongiong
monitoring
002 Governan
ce
Max Marshall
Quality Improvement Strategy: Ensure all
care pathways are NICE compliant and
ensure all patients allocated to a pathway
Lack of engagement and support from
networks, clinicians and corporate services
for care pathway work
Can't move forward on quality
strategy, impairs quality of PbR
data, impairs ability to marry up
financial and quality data 100 50
PbR clustering tool pathway
allocation, training and policy
Progress reports on
allocation of patients
to care pathway
Assurance from NDs that
there is a sound control
process in place regarding
allocation of patients to care
pathways 02.04.2012
003 Governan
ce
Max Marshall
Quality Improvement Strategy: Ensure all
care pathways are NICE compliant and
ensure all patients allocated to a pathway
Care pathway allocation system prevents
allocation to multiple pathways, or to new
pathways within provider services, or
discourages changes to pathway allocation
Impairs quality of PbR data, impairs
ability to marry up financial and
quality data 20 20 None None
Tolerate low level risk, to be
reviewed in future 30.04.2012
004 Operations
Max Marshall
Define and agree detail of conditions
necessary to implement Service Line
Management and begin implementation ‐
definition of clinical leadership model and
authorityLack of Associate Medical Director in
Children and Families Network
Problems implementing appraisal.
Lack of clinical leadership for
CAMHS services. 36 6
Lead consultant available in
Early Intervention Service ‐ no
other controls at present.
Close liaison with
Network Director
Need to write job
description and advertise 30.12.2011
005 Operations
Max Marshall
Define and agree detail of conditions
necessary to implement Service Line
Management and begin implementation ‐
definition of clinical leadership model and
authority
Implementation of SLM delayed by
disagreements on professional leadership
model, that may necessitate a further
consultation
Delay in implementation as
disagreements are resolved 20 10
has been agreed and discussed
at EMT. Professional leadership
issues will be resolved
independently of clinical
leadership implementation.
Director of SDR issues
directive that networks
can proceed with
implementation
network directors and make
final amendments to text of
document. Professional
leadership issues not to form
part of this document. 31.10.2011
006 Operations
Max Marshall
Define and agree detail of conditions
necessary to implement Service Line
Management and begin implementation ‐
definition of clinical leadership model and
authority
Implementation of service line
management delayed by lack of process to
appoint clinical directors
Implementation of service line
management is delayed while
appointment process is worked out. 50 10
Process to appoint clinical
directors needs to be
developed.
application to be a
clinical director has
been placed, and
contains details of
appointments process.
A process needs to be
developed and agreed for
appointing clinical directors 13.11.2011
007 Operations
Max Marshall
Define Medical Director's requirements in
terms of performance/quality standards of
the Service Networks
Overspend on medical agency costs may
not be sufficiently actively managed
Above budget spend on agency
doctors is contributing to a general
overspend 28 10
Associate Medical Directors are
required to monitor locum
spending and to take action
when it is above budget
Overspend is
monitored by finance
and overbudget
spending for more
than 3 consecutive
months leads to
appearence of
network on weekly
performance
monitoring. None
008 Operations
Max Marshall
Define Medical Director's requirements in
terms of performance/quality standards of
the Service Networks
Overspend on medical agency costs may
not be sufficiently actively managed
Financial ‐ Above budget spend on agency doctors is contributing to a
general overspend 28 10
Associate Medical Directors are
required to monitor locum
spending and to take action
when it is above budget.
Overspend is
monitored by finance
and overbudget
spending for more
than 3 consecutive
months leads to Weekly performance Ongoing
009 Governan
ce
Max Marshall
Define Medical Director's requirements in
terms of performance/quality standards of
the Service Networks
Doctors in networks are not having timely
annual appraisals
Doctors are not meeting the
standards for revalidation with the
GMC 35 7
Number of doctors having
annual appraisals is monitored
Regular monitoring
reports are submitted
for SHA audit
Dr. Kaushal needs to ensure
that associate medical
directors receive list of
number of doctors who have
not completed annual
appraisal in their network
and that this is shared across
networks and with Network
Directors 13.11.11
010 Operations
Max Marshall
Determine the information requirements of
assessing service performance against
Medical Director requirements
Trust is unable to supply data on patient
pathways on an annual cohort basis
We will be unable to implement a
key component of the quality
strategy which is to see whether
outcome is improving for pathway
groups on an annual basis 35 35 There is no control at present
Data is delivered on a
cohort basis for key
pathways
Need to meet with Sue Rigg
to discuss how and when
this can be delivered 31.03.2012
1
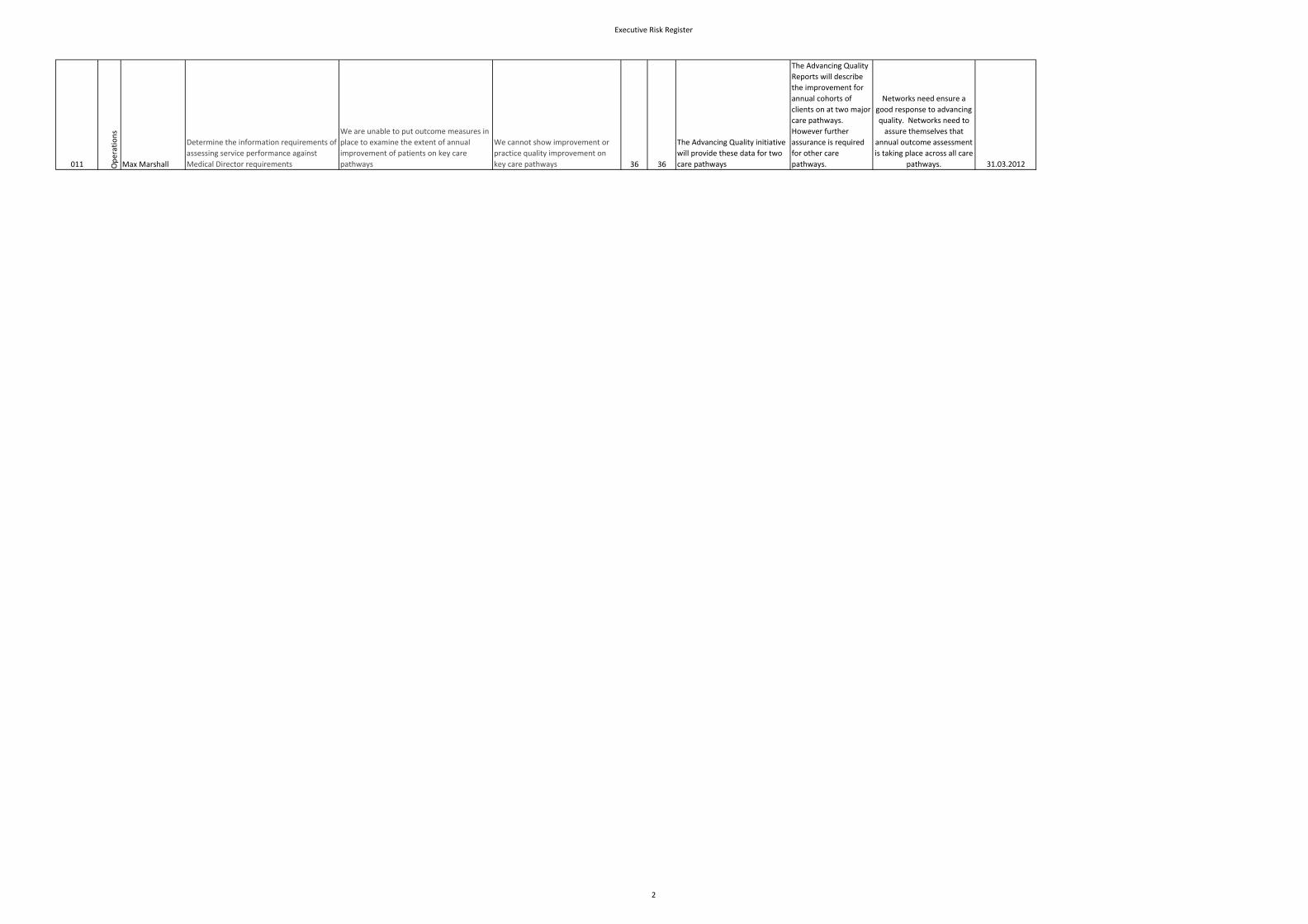
Executive Risk Register
011 Operations
Max Marshall
Determine the information requirements of
assessing service performance against
Medical Director requirements
We are unable to put outcome measures in
place to examine the extent of annual
improvement of patients on key care
pathways
We cannot show improvement or
practice quality improvement on
key care pathways 36 36
The Advancing Quality initiative
will provide these data for two
care pathways
The Advancing Quality
Reports will describe
the improvement for
annual cohorts of
clients on at two major
care pathways.
However further
assurance is required
for other care
pathways.
Networks need ensure a
good response to advancing
quality. Networks need to
assure themselves that
annual outcome assessment
is taking place across all care
pathways. 31.03.2012
2
Executive Risk Register
012 Operations
Max Marshall
Determine the information requirements of
assessing service performance against
Medical Director requirements
Lack of capacity and capability to analyse
the data produced by allocation of patients
to care pathways and annual outcome
assessment.
Data is available but cannot be
analysed in a meaningful or timely
manner. 56 48
There is not control at present,
other than for the advancing
quality initiative ‐ where the
analysis is preformed by a
consultancy company.
Annual reports on
outcome for cohorts
on key pathways are
available
Discussion with Sue Rigg
about capability of existing
resources and future
requirements 30.11.11
013 Operations
Max Marshall
Promote medical engagement in the
Appreciative Leadership programme
Doctors fail to be nominated for the
programme or do not participate fully
Reputation: Key medical staff do not
identify with the values and
strategic direction of the Trust. 42 12
Network Directors are
encouraged to nominate
doctors. Doctors have been
asked to put themselves
forward at Medical Advisory
Committee. I can nominate
doctors and get nomination
Nomination lists and
attendance records are
available.
Need a regular written
report of the number of
doctors completing
Appreciate Leadership 30.11.11
014 Governan
ce
Max Marshall
Strengthen the reporting process around
clinical information governance and the
systematic learning arising
There may be an insufficiently systematic
process for addressing of where actual
clinical practice may fall short of
Information Governance standards.
Reputation, Inspection/Audit,
Patient Experience, Complaints: Loss
of reputation or litigation arising
from poor handling of clinical
information. 42 12
Caldicott Log in place for
reporting incidents and actions.
MM and JMcK have attended
Caldicott training. SIRO,
Caldicott Report to be
produced annually for
Trust Board.
Information Govern
policies and toolkit.
Need to clarify with J
McKenna and Peter Holden
when Caldicott report will be
produced and when J McK
will complete assessment of
current practice against
issues raised in Caldicott 31.03.2012
015 Operations
Max Marshall
Ensure adequate arrangements are in place
to respond appropriately to uncertainty
regarding non‐consultant medical
workforce meeting Trust needs
A sudden reduction in trainee numbers
because of reduced numbers of
applications to training posts.
Night time and weekend medical on
call rotas will come under severe
pressure and may collapse 48 16
John McKenna chairing Medical
Workforce Group monitoring
the situation with input from HR
and Finance and Clinical Tutor
A workforce plan has
been produced to deal
with future
contingencies.
The workforce plan needs to
be adopted and
implemented, but so far
there has been little buy‐in
from the Networks. 31.01.2012
016 Operations Ensure adequate arrangements are in place
to respond appropriately to uncertainty
regarding non‐consultant medical
workforce meeting Trust needs
The current junior doctor rota in Lancaster
is on the verge of EWTD non‐compliance,
and is generating substantial locum costs.
We are at risk of being fined for
EWTD non‐compliance or having to
raise banding payments. Substantial
sums of money are being spent for
little clinical benefit. 48 42 Compliance is monitored by HR.
Medical Workforce
Group is aware of the
problem with the rota
and receives
compliance data.
Adult mental health and
older adult networks need
to implement the Workforce
group's suggestions to
stabilise the rota. 30.11.2011
017 Operations Ensure adequate arrangements are in place
to respond appropriately to uncertainty
regarding non‐consultant medical
workforce meeting Trust needs
A Deanery Inspection of the Trust is taking
place in Feb 2012.
A poor inspection report could lead
to loss of trainees and damage to
the Trust's reputation. 40 10
The Trust clinical tutor, Venu
Duddu, is leading the
preparation for the visit.
Oversight of the plan is
provided by the
Medical Workforce
Development Group,
chaired by Dr. J.
McKenna and
containing
Dr. Duddu needs to provide
execs with a regular monthly
update on preparation for
the visit, highlighting
progress and any issues that
need to be resolved. 30.11.2011
018 Service delivery
Max Marshall
Ensure there is appropriate assurance on
the impact on quality of CIPs and transition
programme
Insufficient attention will be paid to the
views of senior clinicians because of
pressure to complete the transition
programme
Physical harm/injury Senior
clinicians will not support the
transition programme, or will point
out potential clinical risks that will
not be resolved. 30 18
Clinical Directors in place in the
Networks and involved in
Transition Planning. Senior
clinicians in the Networks are
being meaningfully consulted
on the plan.
Director of Nursing
and Medical Director
are meeting with
senior clinicians and
clinical directors and
are aware that they
are backing the
transition plan.
MM to meet regularly with
the new AMDs in the adult
network to ensure they
support the transition plan.
The transition plan should
include specific reference to
the concerns of clinicians
and how they have been
addressed. 30.11.20.11
3
Executive Risk Register
019 Service delivery
Max Marshall
Ensure there is appropriate assurance on
the impact on quality of CIPs and transition
programme
CIPs may be implemented that have a
major impact on quality or safety
Physical harm/injury Serious
deterioration in quality of care or
safety. 40 8
All CIPs assessed in meeting
between clinical execs and
network directors
Reported to Board as
RAG rating. Red plans
cannot proceed
without further
assurance.
I am unclear whether new
CIPS are arising and what
changes have been made to
any CIPs rated red or amber
since last meeting. Director
of Nursing and I need to
review the process. 20.12.11
020 Service delivery
Max Marshall
Maintain performance against corporate
priorities (CIP, policy, etc)
Quality Improvement Strategy does not
consider the requirements of the new TCS
services.
Service Delivery ‐ Trust lacks a
coherent quality improvement
strategy that includes all services
that it provides ‐ this could lead to
poor quality care, or missed
opportunities to demonstrate high
quality work. 56 16
The Quality Improvement
Strategy.
Quarterly Quality
Reports, Quality
Account, Oversight of
Quality
Implementation Group
that contains Mark
Hindle and Janet
Quality Strategy Needs to be
Refreshed 31.01.2012
021 Service Delivery
Maintain performance against corporate
priorities (CIP, policy, etc)
Overspending on the drug budget impinges
on the delivery of CIPs
Financial ‐ Rising expenditure on
anti‐dementia drugs creates a £200‐
400k deficit in drugs budget. 36 12
Drug expenditure is monitored
by finance department and
chief pharmacist.
Drug expenditure is
discussed at D&T
committee.
Report required into causes
of increased expenditure
and measure taken to bring
it under control. More
accurate projection of
pressure required. 30.12.2011
022 Service Delivery
Max Marshall
Enhance organisational capacity to
innovate and ensure that implementation
of the innovation programme is carried out
Networks and clinicians fail to engage with
the programme
The Trust falls behind competitors in
terms of cost‐effectiveness and
quality improvement, staff with
good ideas are disenchanted and
disempowered. 45 10
Programme of Innovation
appendix to Quality Strategy.
Quality Strategy
Implementation Group
Ideas for innovations
are identified and
evaluated in line with
the plan laid out in the
programme. Progress
will be posted online
as the strategy
Need to agree funding to
support 4 innovations put
forward by the networks as
part of the programme. In
region of £200k. It is
proposed that this should
come from CQUIN funds. 27.04.2012
023 Service delivery
Max Marshall
Increase numbers of research
studies/participants from TCS services
Senior clinicians in community services will
perceive that LCFT has failed to deliver one
of the key anticipated benefits of
integration.
Organisational ‐ Staffing &
Competence: Recruitment to NIHR
portfolio studies falls, FSF income
falls, the Trust loses top quality
clinicians or cannot recruit. 28 4
R&D have been identifying
research active clinicians in TCS
services. Away day planned
with new services. Plan for
integration with current R&D
activity will follow.
R&D Annual Report to
Board. Monitoring of
NIHR Portfolio
(recruitment) by R&D
manager.
Adult Community and
Children and Families
Network should report new
research activity at Chief
Exec's Challenge 31.03.12
024 Governan
ce
Max Marshall
Fully implement enhanced medical
appraisal
The Share Point system for supporting
medical appraisal is not fully functional and
will require updating and maintenance.
Doctors may be reluctant to use the
system because of security fears or
because it is hard to access. This
would make it difficult monitor the
success of the revalidation
programme. 42 7
Monitoring of number of
doctors using the database and
number of appraisals completed
in time.
ORSA audit. AMD for
revalidation satisfied
that system is
effective. Medical
Advisory Committee
satisfied that system is
effective.
Need to ensure that
sufficient IT support is
available to maintain the
system. 30.11.2011
025 Governan
ce
Max Marshall
Fully implement enhanced medical
appraisal
The administrative support available to
support revalidation may not be adequate,
especially given the increased requirements
following transfer of community services.
Revalidation process may cease to
function, leading to major
difficulties with SHA and regulators. 28 7
AMD for Revalidation (Ashu
Kaushal) asked to produce
written case for additional
resources.
Case received and
reviewed by medical
director.
Validated care needs to be
submitted as a pressure. 06.01.2012
026 Governan
ce
Max Marshall
Fully implement enhanced medical
appraisal
The process for dealing with concerns
about doctors is not sufficiently systematic.
Exposure to legal challenge from
doctors. Doctors performance
concerns not adequately addressed. 28 7
Policy in place for Maintaining
High Professional Standards in
the Modern NHS
Performance issues
kept under review by
Director of HR and
Medical Director
An operating procedure
needs to be developed that
specifies in detail how
concerns about doctors are
managed. 30.03.2012
027 Operations
Max Marshall
Ensure that the views of clinicians are
actively taken into account in the design of
reconfigured inpatient services
Clinical engagement diminishes as the
capital programme enters its later stages.
Clinical support for the programme
is lost and mistakes are made
through lack of clinical input. 40 8
The capital programme provides
evidence that there is an
ongoing detailed clinical review
of the acute care model.
Regular meetings with
the Associate Medical
Director for Tier 5.
Director of Nursing
and Medical Director
to review the evidence
of clinical engagement.
Capital Programme needs to
provide ongoing evidence
(suggest quarterly) of
successful clinical
engagement. 30.11.2011
028 Reputational
Max Marshall
Design GP engagement process including
clinical interface
There is no clinical content available for the
GP portal
The Trust commitment to make
online self help material available to
GPs is not met None None
Communications and IT
need to work with clinicians
in the network to deliver
clinical content ‐ at the
moment the vehicle for this
co‐operation is unclear. 29.02.2012
4
Executive Risk Register
029 Reputational
Max Marshall
Design GP engagement process including
clinical interface
New GP advisors are not sufficiently
integrated into the organisation
Services do not benefit from GP
input leading to reduce quality and
potential loss of business 30 6
Job plan in place. Line
management clarified
Not adequate at
present, but not yet in
post
Director of SDR and Medical
Director need detailed plan
about deployment and
supervision of GP advisors 31.12.2011
5
Executive Risk Register
030 Reputational
Max Marshall
Ensure appropriate implementation of GP
engagement process
GP survey shows that GP satisfaction does
not improve despite launch of the GP
Charter.
Trust is seen to have failed to
deliver on its promises to GPS,
leading to substantial reputation
damage and possible loss of
business 72 63
GP survey will be launched in
November and repeated in
November 2012
Survey has been
publicised internally to
staff. Networks have
specified the
interpretation of the
standards internally, to
be posted on the Trust
Internet site
Networks must have robust
assurances in place that they
are delivering against the
charter standards. 30.12.2011
031 Patrick Sullivan
To define and communicate appropriate
service performance, quality, patient
experience and governance standards
Sufficient management capacity and
capability to ensure that we interpret and
adapt statutory and regulatory and
professional guidance into service
standards
We fail to determine the required
service standards which result in
service failure 21 7
Management structures to
support the process,
underpinned by regular 1:1.
Quality strategy outlining the
priorities. effective professional
leadership arrangements.
Patient Experience Strategy
1:1 meetings and
performance reviews.
Performance and
Quality report and
quarterly analysis of
complaints, incidents
and claims. Quarterly None
032 Governan
ce
Patrick Sullivan
To define and communicate appropriate
service performance, quality, patient
experience and governance monitoring
arrangements
Sufficient management capacity and
capability to ensure that we interpret and
adapt statutory and regulatory and
professional guidance and define
monitoring arrangements
Services cannot provide evidence of
performance standards 42 14
Network Governance meetings,
Oversight of agendas,
Annual Governance
Statements, Chief
Execs challenge None
033 Governan
ce
Patrick Sullivan
To ensure appropriate and robust
assurances are provided regarding service
performance, quality, patient experience
and governance
Variable compliance across and within
Networks
Compliance with regulatory
standards is limited 42 14
Network Governance meetings,
Oversight of agendas,
Annual Governance
Statements, Chief
Execs challenge None
034 Governan
ce To ensure appropriate and robust
assurances are provided regarding service
performance, quality, patient experience
and governance
Variable evidence provided across and
within Networks
Compliance with regulatory
standards is limited 42 14
Network Governance meetings,
Oversight of agendas,
Annual Governance
Statements, Chief
Execs challenge None
035 Governan
ce
Patrick Sullivan
To learn the lessons resulting from Serious
Untoward Incidents and feedback from
service users (includes claims)
Adequate systems to ensure that lessons
learned become embedded
Patient harm ‐ potential that we
repeat incidents and do not improve
services 48 SUI investigation process,
SUI quarterly reports,
SUI Analysis group,
Governance reports to
the Board, Meetings
between the Director
of Nursing and Medical
Director None
036 Governan
ce
Patrick Sullivan
To ensure that effective systems and
processes are in place to quality assure
Clinical Services and to promote a culture
of continuous improvement
A lack of capacity and/or capability to
clearly define the standards
The organisation is unaware if there
are significant risks to clinical
services &0 30
Key Performance indicators,
Priorities as defined in the
quality Strategy, Clinical audit
programme, Evidence to
support compliance with CQC
standards,
Professional leadership
structures which ensure
appropriate standards are set,
Quality and
Performance Report
Governance Report
Feedback from the
CQC eg QRP and
reports from any
reviews
Quality Account None
037 Patrick Sullivan
To ensure that effective systems and
processes are in place to quality assure
Clinical Services and to promote a culture
of continuous improvement
Systems and processes that are not able to
provide the necessary assurance and
promote a culture of continuous
improvement Poor quality services are delivered, im 70 30
Key Performance indicators,
Priorities as defined in the
quality Strategy, Clinical audit
programme, Evidence to
support compliance with CQC
standards
Professional leadership
structures which ensure
appropriate standards are set
Quality and
Performance Report
Governance Report
Feedback from the
CQC eg QRP and
reports from any
reviews
None
038 Operational
Patrick Sullivan
Maintain performance against corporate
priorities (CIP, policy, etc.)
Capacity and capability to manage the
range of organisational objectives
Directorate fails to meet its defined
objectives 30 12
Team and 121 meetings with
Senior management team
Performance Review
Performance management of
objectives
Regular reports on key
areas of activity e.g.
finance, workforce None None
039 Governan
ce
Patrick Sullivan
To ensure that effective systems and
processes are in place to promote a
culture of continuous improvement and
compassionate servicesPoor service quality and risk of service
failure
Impact on service users and carers
and organisational reputation 35 21 Quality strategy and associated q
Quality reporting
processes from team
through to the board None None
6
Executive Risk Register
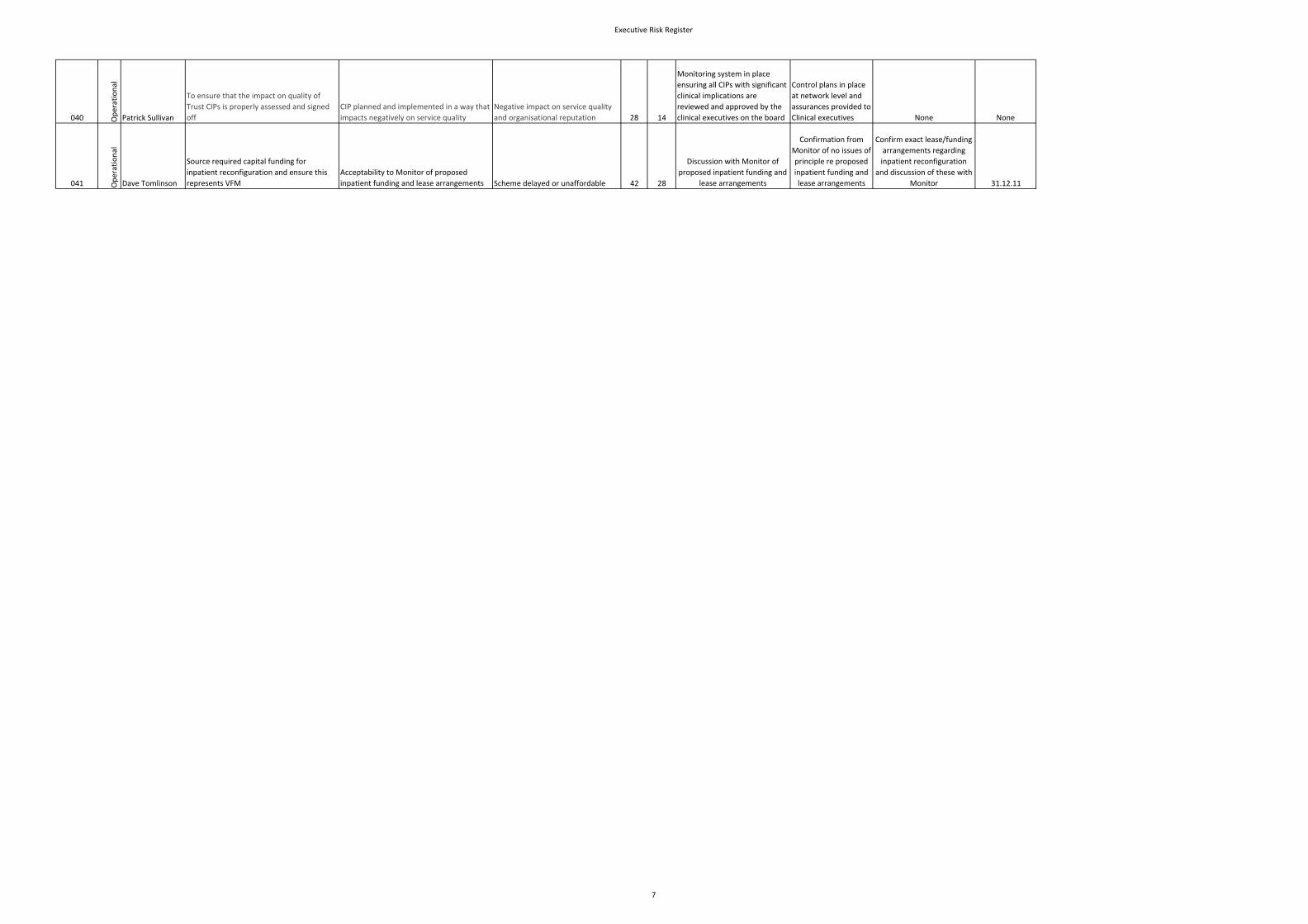
040 Operational
Patrick Sullivan
To ensure that the impact on quality of
Trust CIPs is properly assessed and signed
off
CIP planned and implemented in a way that
impacts negatively on service quality
Negative impact on service quality
and organisational reputation 28 14
Monitoring system in place
ensuring all CIPs with significant
clinical implications are
reviewed and approved by the
clinical executives on the board
Control plans in place
at network level and
assurances provided to
Clinical executives None None
041 Operational
Dave Tomlinson
Source required capital funding for
inpatient reconfiguration and ensure this
represents VFM
Acceptability to Monitor of proposed
inpatient funding and lease arrangements Scheme delayed or unaffordable 42 28
Discussion with Monitor of
proposed inpatient funding and
lease arrangements
Confirmation from
Monitor of no issues of
principle re proposed
inpatient funding and
lease arrangements
Confirm exact lease/funding
arrangements regarding
inpatient reconfiguration
and discussion of these with
Monitor 31.12.11
7
Executive Risk Register
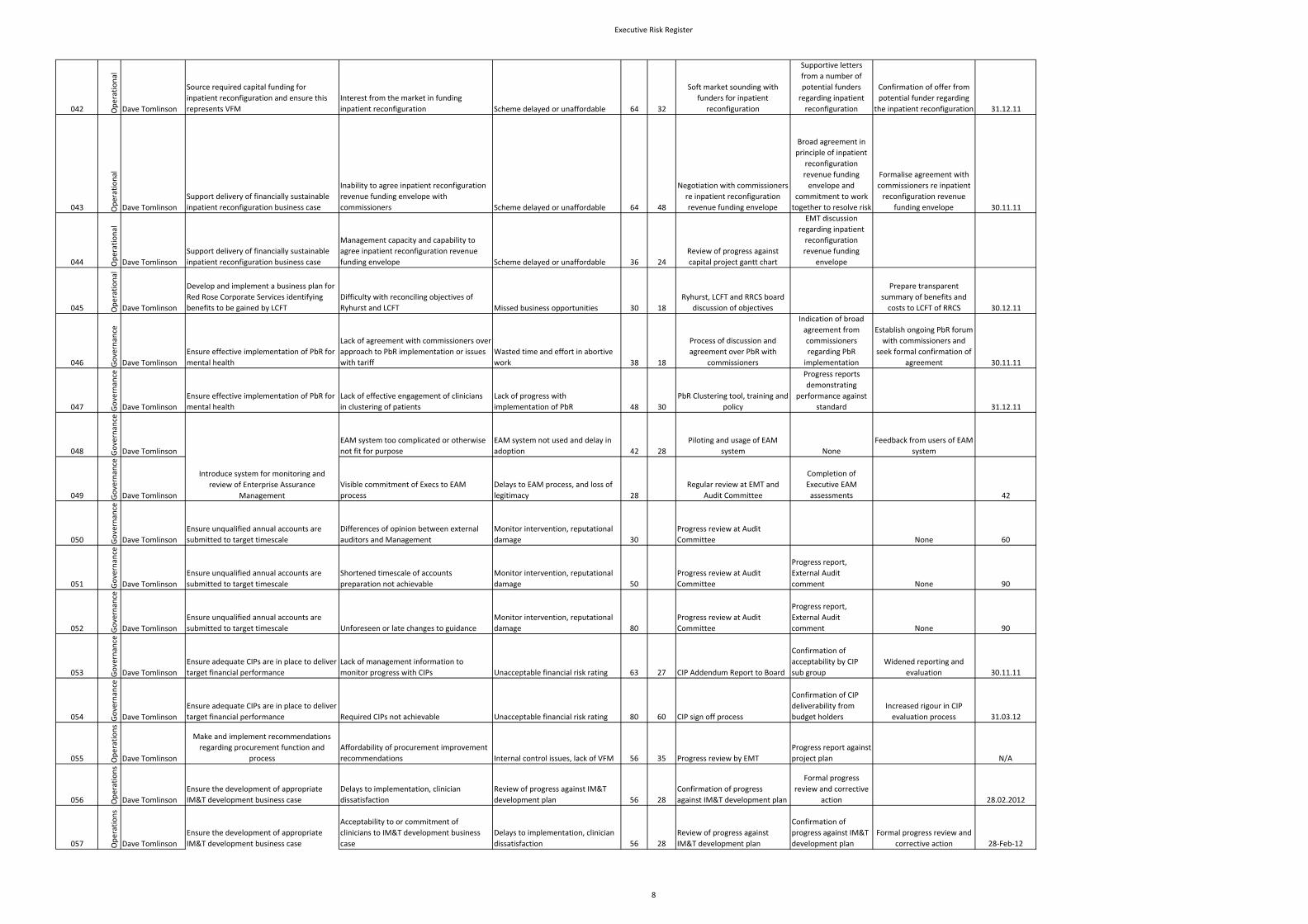
042 Operational
Dave Tomlinson
Source required capital funding for
inpatient reconfiguration and ensure this
represents VFM
Interest from the market in funding
inpatient reconfiguration Scheme delayed or unaffordable 64 32
Soft market sounding with
funders for inpatient
reconfiguration
Supportive letters
from a number of
potential funders
regarding inpatient
reconfiguration
Confirmation of offer from
potential funder regarding
the inpatient reconfiguration 31.12.11
043 Operational
Dave Tomlinson
Support delivery of financially sustainable
inpatient reconfiguration business case
Inability to agree inpatient reconfiguration
revenue funding envelope with
commissioners Scheme delayed or unaffordable 64 48
Negotiation with commissioners
re inpatient reconfiguration
revenue funding envelope
Broad agreement in
principle of inpatient
reconfiguration
revenue funding
envelope and
commitment to work
together to resolve risk
Formalise agreement with
commissioners re inpatient
reconfiguration revenue
funding envelope 30.11.11
044 Operational
Dave Tomlinson
Support delivery of financially sustainable
inpatient reconfiguration business case
Management capacity and capability to
agree inpatient reconfiguration revenue
funding envelope Scheme delayed or unaffordable 36 24
Review of progress against
capital project gantt chart
EMT discussion
regarding inpatient
reconfiguration
revenue funding
envelope
045 Operational
Dave Tomlinson
Develop and implement a business plan for
Red Rose Corporate Services identifying
benefits to be gained by LCFT
Difficulty with reconciling objectives of
Ryhurst and LCFT Missed business opportunities 30 18
Ryhurst, LCFT and RRCS board
discussion of objectives
Prepare transparent
summary of benefits and
costs to LCFT of RRCS 30.12.11
046 Governan
ce
Dave Tomlinson
Ensure effective implementation of PbR for
mental health
Lack of agreement with commissioners over
approach to PbR implementation or issues
with tariff
Wasted time and effort in abortive
work 38 18
Process of discussion and
agreement over PbR with
commissioners
Indication of broad
agreement from
commissioners
regarding PbR
implementation
Establish ongoing PbR forum
with commissioners and
seek formal confirmation of
agreement 30.11.11
047 Governan
ce
Dave Tomlinson
Ensure effective implementation of PbR for
mental health
Lack of effective engagement of clinicians
in clustering of patients
Lack of progress with
implementation of PbR 48 30
PbR Clustering tool, training and
policy
Progress reports
demonstrating
performance against
standard 31.12.11
048 Governan
ce
Dave Tomlinson
EAM system too complicated or otherwise
not fit for purpose
EAM system not used and delay in
adoption 42 28
Piloting and usage of EAM
system None
Feedback from users of EAM
system
049 Governan
ce
Dave Tomlinson
Visible commitment of Execs to EAM
process
Delays to EAM process, and loss of
legitimacy 28
Regular review at EMT and
Audit Committee
Completion of
Executive EAM
assessments 42
050 Governan
ce
Dave Tomlinson
Ensure unqualified annual accounts are
submitted to target timescale
Differences of opinion between external
auditors and Management
Monitor intervention, reputational
damage 30
Progress review at Audit
Committee None 60
051 Governan
ce
Dave Tomlinson
Ensure unqualified annual accounts are
submitted to target timescale
Shortened timescale of accounts
preparation not achievable
Monitor intervention, reputational
damage 50
Progress review at Audit
Committee
Progress report,
External Audit
comment None 90
052 Governan
ce
Dave Tomlinson
Ensure unqualified annual accounts are
submitted to target timescale Unforeseen or late changes to guidance
Monitor intervention, reputational
damage 80
Progress review at Audit
Committee
Progress report,
External Audit
comment None 90
053 Governan
ce
Dave Tomlinson
Ensure adequate CIPs are in place to deliver
target financial performance
Lack of management information to
monitor progress with CIPs Unacceptable financial risk rating 63 27 CIP Addendum Report to Board
Confirmation of
acceptability by CIP
sub group
Widened reporting and
evaluation 30.11.11
054 Governan
ce
Dave Tomlinson
Ensure adequate CIPs are in place to deliver
target financial performance Required CIPs not achievable Unacceptable financial risk rating 80 60 CIP sign off process
Confirmation of CIP
deliverability from
budget holders
Increased rigour in CIP
evaluation process 31.03.12
055 Operations
Dave Tomlinson
Make and implement recommendations
regarding procurement function and
process
Affordability of procurement improvement
recommendations Internal control issues, lack of VFM 56 35 Progress review by EMT
Progress report against
project plan N/A
056 Operations
Dave Tomlinson
Ensure the development of appropriate
IM&T development business case
Delays to implementation, clinician
dissatisfaction
Review of progress against IM&T
development plan 56 28
Confirmation of progress
against IM&T development plan
Formal progress
review and corrective
action 28.02.2012
057 Operations
Dave Tomlinson
Ensure the development of appropriate
IM&T development business case
Acceptability to or commitment of
clinicians to IM&T development business
case
Delays to implementation, clinician
dissatisfaction 56 28
Review of progress against
IM&T development plan
Confirmation of
progress against IM&T
development plan
Formal progress review and
corrective action 28‐Feb‐12
Introduce system for monitoring and
review of Enterprise Assurance
Management
8
Executive Risk Register
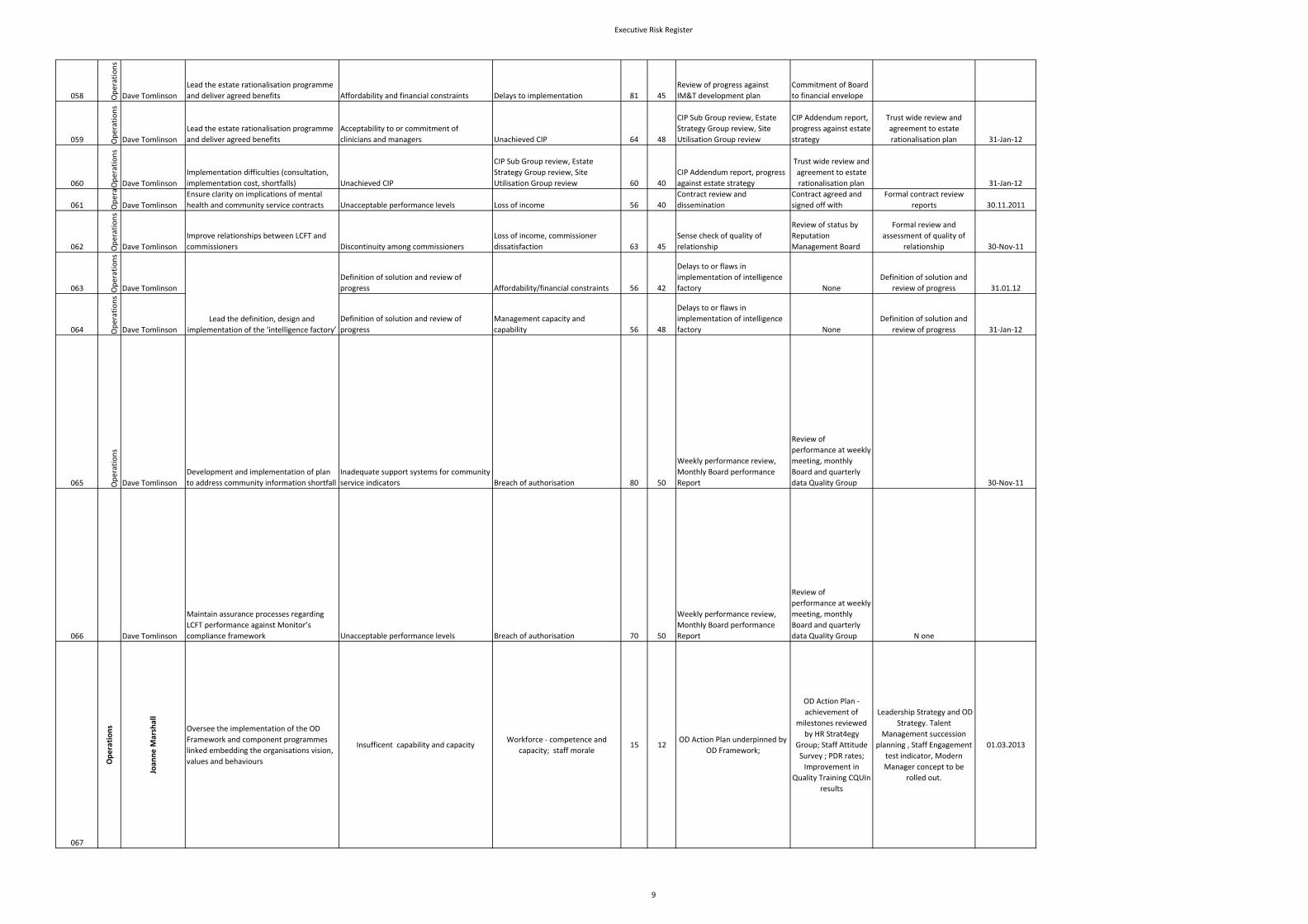
058 Operations
Dave Tomlinson
Lead the estate rationalisation programme
and deliver agreed benefits Affordability and financial constraints Delays to implementation 81 45
Review of progress against
IM&T development plan
Commitment of Board
to financial envelope
059 Operations
Dave Tomlinson
Lead the estate rationalisation programme
and deliver agreed benefits
Acceptability to or commitment of
clinicians and managers Unachieved CIP 64 48
CIP Sub Group review, Estate
Strategy Group review, Site
Utilisation Group review
CIP Addendum report,
progress against estate
strategy
Trust wide review and
agreement to estate
rationalisation plan 31‐Jan‐12
060 Operations
Dave Tomlinson
Implementation difficulties (consultation,
implementation cost, shortfalls) Unachieved CIP
CIP Sub Group review, Estate
Strategy Group review, Site
Utilisation Group review 60 40
CIP Addendum report, progress
against estate strategy
Trust wide review and
agreement to estate
rationalisation plan 31‐Jan‐12
061 Opera
Dave Tomlinson
Ensure clarity on implications of mental
health and community service contracts Unacceptable performance levels Loss of income 56 40
Contract review and
dissemination
Contract agreed and
signed off with
Formal contract review
reports 30.11.2011
062 Operations
Dave Tomlinson
Improve relationships between LCFT and
commissioners Discontinuity among commissioners
Loss of income, commissioner
dissatisfaction 63 45
Sense check of quality of
relationship
Review of status by
Reputation
Management Board
Formal review and
assessment of quality of
relationship 30‐Nov‐11
063 Operations
Dave Tomlinson
Definition of solution and review of
progress Affordability/financial constraints 56 42
Delays to or flaws in
implementation of intelligence
factory None
Definition of solution and
review of progress 31.01.12
064 Operations
Dave Tomlinson
Definition of solution and review of
progress
Management capacity and
capability 56 48
Delays to or flaws in
implementation of intelligence
factory None
Definition of solution and
review of progress 31‐Jan‐12
065 Operations
Dave Tomlinson
Development and implementation of plan
to address community information shortfall
Inadequate support systems for community
service indicators Breach of authorisation 80 50
Weekly performance review,
Monthly Board performance
Report
Review of
performance at weekly
meeting, monthly
Board and quarterly
data Quality Group 30‐Nov‐11
066 Dave Tomlinson
Maintain assurance processes regarding
LCFT performance against Monitor’s
compliance framework Unacceptable performance levels Breach of authorisation 70 50
Weekly performance review,
Monthly Board performance
Report
Review of
performance at weekly
meeting, monthly
Board and quarterly
data Quality Group N one
067
Ope
ratio
ns
Joan
ne M
arshall
Oversee the implementation of the OD
Framework and component programmes
linked embedding the organisations vision,
values and behaviours
Insufficent capability and capacity Workforce ‐ competence and
capacity; staff morale 15 12
OD Action Plan underpinned by
OD Framework;
OD Action Plan ‐
achievement of
milestones reviewed
by HR Strat4egy
Group; Staff Attitude
Survey ; PDR rates;
Improvement in
Quality Training CQUIn
results
Leadership Strategy and OD
Strategy. Talent
Management succession
planning , Staff Engagement
test indicator, Modern
Manager concept to be
rolled out.
01.03.2013
Lead the definition, design and
implementation of the ‘intelligence factory’
9
Executive Risk Register
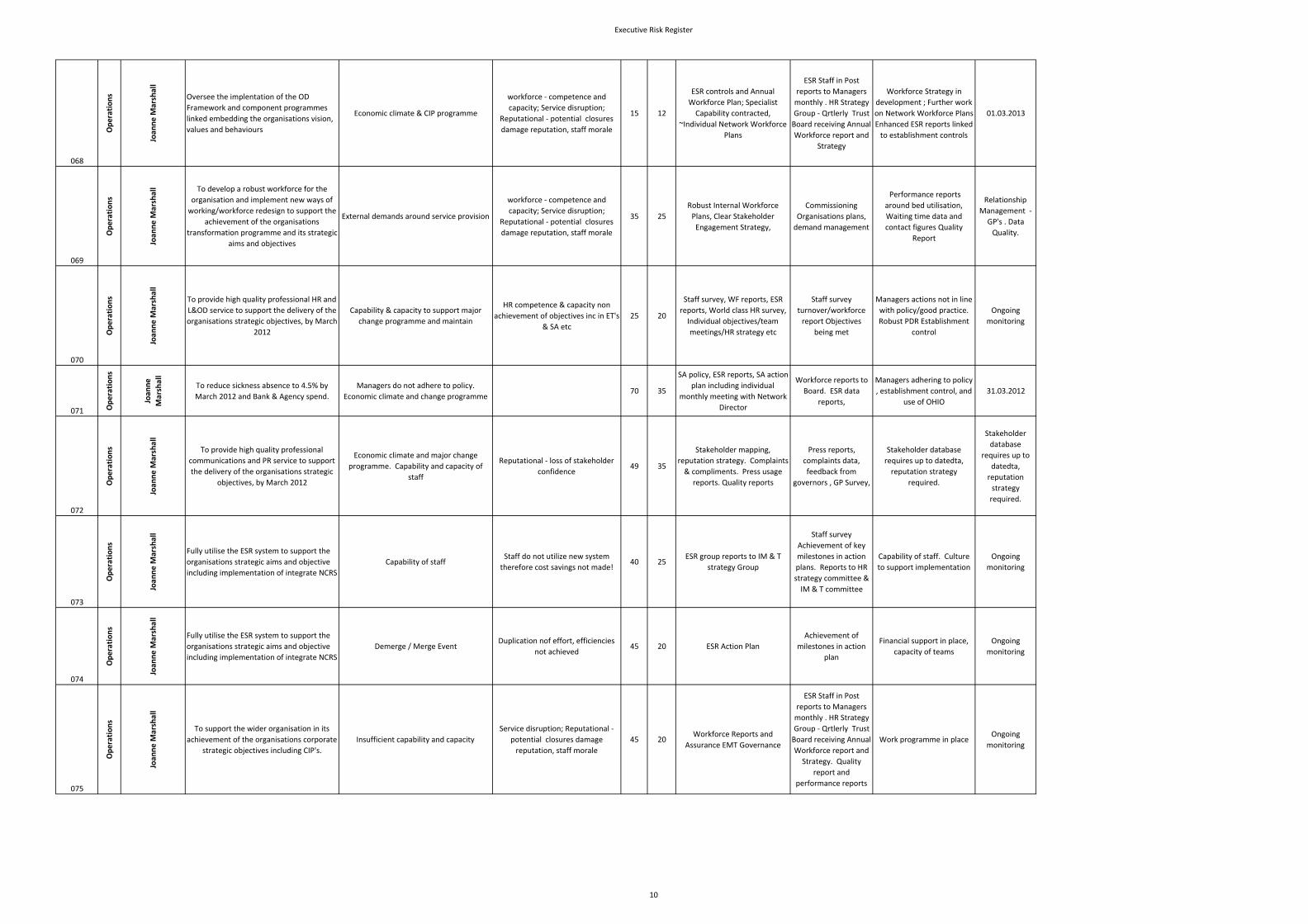
068
Ope
ratio
ns
Joan
ne M
arshall
Oversee the implentation of the OD
Framework and component programmes
linked embedding the organisations vision,
values and behaviours
Economic climate & CIP programme
workforce ‐ competence and
capacity; Service disruption;
Reputational ‐ potential closures
damage reputation, staff morale
15 12
ESR controls and Annual
Workforce Plan; Specialist
Capability contracted,
~Individual Network Workforce
Plans
ESR Staff in Post
reports to Managers
monthly . HR Strategy
Group ‐ Qrtlerly Trust
Board receiving Annual
Workforce report and
Strategy
Workforce Strategy in
development ; Further work
on Network Workforce Plans
Enhanced ESR reports linked
to establishment controls
01.03.2013
069
Ope
ratio
ns
Joan
ne M
arshall To develop a robust workforce for the
organisation and implement new ways of
working/workforce redesign to support the
achievement of the organisations
transformation programme and its strategic
aims and objectives
External demands around service provision
workforce ‐ competence and
capacity; Service disruption;
Reputational ‐ potential closures
damage reputation, staff morale
35 25
Robust Internal Workforce
Plans, Clear Stakeholder
Engagement Strategy,
Commissioning
Organisations plans,
demand management
Performance reports
around bed utilisation,
Waiting time data and
contact figures Quality
Report
Relationship
Management ‐
GP's . Data
Quality.
070
Ope
ratio
ns
Joan
ne M
arshall
To provide high quality professional HR and
L&OD service to support the delivery of the
organisations strategic objectives, by March
2012
Capability & capacity to support major
change programme and maintain
HR competence & capacity non
achievement of objectives inc in ET's
& SA etc
25 20
Staff survey, WF reports, ESR
reports, World class HR survey,
Individual objectives/team
meetings/HR strategy etc
Staff survey
turnover/workforce
report Objectives
being met
Managers actions not in line
with policy/good practice.
Robust PDR Establishment
control
Ongoing
monitoring
071 Ope
ratio
ns
Joan
ne
Marshall
To reduce sickness absence to 4.5% by
March 2012 and Bank & Agency spend.
Managers do not adhere to policy.
Economic climate and change programme70 35
SA policy, ESR reports, SA action
plan including individual
monthly meeting with Network
Director
Workforce reports to
Board. ESR data
reports,
Managers adhering to policy
, establishment control, and
use of OHIO
31.03.2012
072
Ope
ratio
ns
Joan
ne M
arshall
To provide high quality professional
communications and PR service to support
the delivery of the organisations strategic
objectives, by March 2012
Economic climate and major change
programme. Capability and capacity of
staff
Reputational ‐ loss of stakeholder
confidence 49 35
Stakeholder mapping,
reputation strategy. Complaints
& compliments. Press usage
reports. Quality reports
Press reports,
complaints data,
feedback from
governors , GP Survey,
Stakeholder database
requires up to datedta,
reputation strategy
required.
Stakeholder
database
requires up to
datedta,
reputation
strategy
required.
073
Ope
ratio
ns
Joan
ne M
arshall
Fully utilise the ESR system to support the
organisations strategic aims and objective
including implementation of integrate NCRS
Capability of staffStaff do not utilize new system
therefore cost savings not made!40 25
ESR group reports to IM & T
strategy Group
Staff survey
Achievement of key
milestones in action
plans. Reports to HR
strategy committee &
IM & T committee
Capability of staff. Culture
to support implementation
Ongoing
monitoring
074
Ope
ratio
ns
Joan
ne M
arshall
Fully utilise the ESR system to support the
organisations strategic aims and objective
including implementation of integrate NCRS
Demerge / Merge EventDuplication nof effort, efficiencies
not achieved 45 20 ESR Action Plan
Achievement of
milestones in action
plan
Financial support in place,
capacity of teams
Ongoing
monitoring
075
Ope
ratio
ns
Joan
ne M
arshall
To support the wider organisation in its
achievement of the organisations corporate
strategic objectives including CIP's.
Insufficient capability and capacity
Service disruption; Reputational ‐
potential closures damage
reputation, staff morale
45 20Workforce Reports and
Assurance EMT Governance
ESR Staff in Post
reports to Managers
monthly . HR Strategy
Group ‐ Qrtlerly Trust
Board receiving Annual
Workforce report and
Strategy. Quality
report and
performance reports
Work programme in place Ongoing
monitoring
10
Executive Risk Register
076
Ope
ratio
ns
Joan
ne M
arshall
To develop and implement robust
integration plans in line with
Transformation and Integration
Programme.
Insufficient capability and capacity in
economic climate
Service disruption; Reputational ‐
potential closures damage
reputation, staff morale
49 35
Transformation Plans and
Programme , Organisational
Change Policy and HR
Framework
ESR Staff in Post
reports to Managers
monthly . HR Strategy
Group ‐ Qrtlerly Trust
Board receiving Annual
Workforce report and
Strategy. Quality
report and
performance reports
Managers adhering to policy
and robust engagement
strategy. Develop on new
Organisational Change
policy.
31.03.2012
077
Ope
ratio
ns
Joan
ne M
arshall
Define and communicate standards for
usage of temporary staff (bank, agency and
locums)
External demands around service provision
, capability and capacity , managers
following policy
Reputational ‐ damaged reputation,
quality and service provision issues
84 49
Temporary staffing policy, ESR
reports, action plan including
individual monthly meeting with
Network Director
Workforce reports to
Board. ESR data
reports feedback /
evaluations from
customers 31.03.2012
078
Ope
ratio
ns
Joan
ne M
arshall
Define, develop and communicate robust
stakeholder engagement processes and
standards
External demands around service provision
, capability and capacity
Reputation ‐ Loss of stakeholder
confidence
56 40
Stakeholder mapping,
reputation strategy. Complaints
& compliments. Press usage
reports. Quality reports
Press reports
complaints number of
survey's, COG
31.03.2013
079
Strategy
Mark Hindle
Oversee the integration, formation and re‐
structuring of all networks
Consultation processes prevent alignment
of management structures in a timely
manner
Financial ‐ CIPS and achievement of
targets not achieved ; Reputational ‐
loss of Stakeholder confidence;
Board ‐ confidence
63 42
Consultation Document,
Conversation with the Network
Directors, commitment to
timescales, agreement with
Exec colleagues , conversation
with staff side, budgetary sign
off
Organisational Change
Policy, CIP, Reporting
to the CIP Group and
agreement of group
Non‐compliance to agreed
process, Transformation
Director not in post.
Earned autonomy and
relationship management
31.01.2012
080
Strategy
Mark Hindle
Oversee the integration, formation and re‐
structuring of all networks
Implications of Ability to understand service
capacity and demand and co‐ordinate
workforce to benchmark costs
Financial ‐ loss of income , Patient
Experience ‐
81 63
SLM, Ref costs, Entrusted Health
data, Transition plan for
inpatient reconfiguration,
workforce plan
Performance reviews
with ND's, objective
setting, workforce
planning, inpatient
transition board,
evidence based
benchmarked data to
plan
We haven't got the
Transformation Director,
haven't undertaken
systematic demand and
systems and information,
evidence based decision
making, haven't got capacity
in place in some areas,
consultation with staff.
Utilising data to develop
implementation plans.
31.01.2012
081
Strategy
Mark Hindle
Oversee the integration, formation and re‐
structuring of all networks
Organisational ability to manage transition
in a period of cultural change
Financial ‐ CIPS and achievement of
targets not achieved ; Reputational ‐loss of Stakeholder confidence;
Board ‐ confidence Regulatory
compliance CQC, Contracts, Clinical
Commissioning Grups CQUIN
64 36
Identification of key transitional
areas, Management
Organisational change policy ,
Appreciative Leadership , Team
Programme, Team to Team with
key stakeholders , The
information Centre ‐
Performance data,
Board reporting,
Monitor Returns, CQC,
registration, Delivery
of organisational
change in place.
Management
restructures
completed
Director of Transformation
not in Post, Capacity, Full
overarching plan, Master
Control Plans around all key
transitions capability in
some areas. EAM not fully
embedded Some key
strategies/work programmes
are work in progress
commercial experience not
fully in place Implications of
PBR Evidenced based
evaluation of what has been
achieved
31.01.2012
11
Executive Risk Register
082
Strategy
Mark Hindle
Oversee the integration, formation and re‐
structuring of all networks
Limited organisational ability to maintain
the quality of service delivery whilst
undergoing significant organisational
change
Services do not meet user needs.
Capacity does not broadly meet
demand Reputation of organisation
compromised IP build programme
compromised
72 64
Transition Plan, Transitional
plan EAM Programme,
Appreciative Leadership
Integrated SUI monitoring
Business continuity Planning in
place and tested Engage event
Network engage event Team
Brief Evidence produced for
Lancashire and locality service
Transformation group Staff
survey
Conversation with Key
reports, Service visits,
Board reporting,
Monitor Returns, CQC,
registration, Contract
negotiations Contracts
Performance wall CE
challenge Business
Planning process
underway and agreed
Commissioning system in
period of considerable
transition GP (clinical
commissioning consortia)
fragmented and immature
Multiple demands for
customised services balance
of economies of larger
organisation
Transformation Director not
in place. Fragmented
commissioning landscape
Implementation of
stakeholder management
strategy Not aware of who
new GP players are Threat
to existing service delivery
e.g. section 75 Management
capacity/alignment
31.01.2012
083
Mark Hindle
Identify key network transformation
priorities for the organisation
Management Capacity to design an
adequate system of transformation
Services do not modernise to deliver
commissioner intentions
and/patient needs. Failure to
deliver planned capacity and/or not
delivering financial targets
56 35
Transformation Director
resourced Business Change
forum established to exercise
gateway control IP transition
plan agreed and under
document control Management
capacity broadly aligned to
priorities Robust structure
Management
restructures
completed
Conversations and
objective
setting/measurement
with direct reports,
Progress against
agreed priorities,
Delivery of CIP plans
Transformation Director not
in place Overarching MCP
not complete Business
planning not complete.
Compliance not consistent
Capability Issues in some
areas. Key senior
management posts still not
filled or capability issues
Less experienced managers
dealing with difficult issues
Full engagement with clinical
colleagues to deliver
changes Sufficient evidence
based decision making (skills
or actual)
084
Mark Hindle
Identify, and monitor key network
transformation priorities for the
organisation
Robust data, appropriately benchmarked
and evidence based to support design of
system
Poor non evidenced decision
making, leading to poor service
quality and/or not focussing on the
areas that will deliver the biggest
cost, quality and activity benefits
72 56
Reference cost analysis Board
reporting of ref costs and plans
to address. Agreement on SLM.
Entrusted health analyse.
Work/review programme with
each network Aqua
benchmarking data
Reference cost data,
Papers and analysis
discussed at board CIP
sub group Network
meeting to discuss
variance and
subsequent planning
statistical process
management skills numerate
evidence based decision
making use of existing data
e.g. reference cost to drive
cost effective service
delivery, understanding of
where additional costs
compared to reference costs
deric=ve from, engagement
with commissioners to
accurately specify service
models, understanding of
implications of reducing to
reference e cost Insufficient
sophisticated targets and
measurement of leading
indicators Variable data
collections sources and
systems Variable assurance
that all activity is being
counted Other value added
activity variably measured
External benchmarking data
largely not available
benchmarking leading
indicator data not defined
12
Executive Risk Register
085
Mark Hindle
Management Capacity and capability to
implement and monitor transformation
priorities
Financial ‐ CIPS and achievement of
targets and prioritised evidence
based services not targeted Needed
service transformation not delivered
81 48
, Appreciative Leadership , Team
Programme, , The information
Centre ‐ Performance data,
Board reporting,
Management
restructures
completed
Conversation with
regarding service
delivery Transition
plan
Identification of key
transformation priorities,
Management skills
development plans
recruiting for capability and
competence Director of
Transformation not in Post,
Capacity, Full overarching
plan, Master Control Plans
around all key transitions
capability in some areas.
EAM not fully embedded
management by assurance
Evidenced based evaluation
of what has been achieved
086
Mark Hindle
Investigate Entrusted Health data and
benchmarking principles
Lack of co‐ordinated systems across 4
organisations
Activity is not counted and recorded
in consistent manner undermining
evidence based decision making
72 42
Reference costs alignment in
progress Entrusted health
analysis undertaken Resource
utilisation plan in place Dir.
Transition in place Board
reporting undertaken SLM
agreed
Reference cost
reporting Entrusted
health report CIP sub
group Conversations
regarding moving to
integrated system
leading indicators used
to influence activity
planning gateway
review process set up
electronic data recording
systems in community
systems variable care
pathways reporting low not
all activity counted
Reference costs narrow
aspect of benchmarking
timescale for system
integration. EAM not fully
embedded Some key
strategies/work programmes
are work in progress
commercial experience not
fully in place Implications of
PBR Analysis of capability
required and plans to
address Transformation
director not in place
business planning not in
place decision making
variably not evidence based
01/03/2012
087
Strategy
Mark Hindle
Define and deliver organisational targets
based on benchmarking principles
Lack of co‐ordinated systems across 4
organisations
CIPs not delivered in systematic
manner with minimal benefit for
improved quality and productivity
and reputation management
64 48
Reference cost RUP developed
from community services top
priorities identified CIP board
sub committee CIP reporting in
place Longer term planning
agreed
Reference cost
reporting Entrusted
health report CIP sub
group Conversations
with AND, CE
challenge, financial
reporting Network
business planning and
Information systems Work
programmes to project
manage programmes
Performance management
framework to measure
programmes CIP plans are
generally not eveidence
based i.e. do not focuss on
benchmarked opportunities
for improvement. Work
programmes not thoroughly
scoped Implications
unknown Targets generally
input absed and do not
relate to service quality
Internal quality targets not
fully developed
01/03/2012
13
Executive Risk Register
088
Strategy
Mark Hindle
Develop external relationships focussed on
robust engagement to inform and support
organisational transformation
Organisational capacity to implement the
Stakeholder Strategy
Reputation damage, loss of service
provision Loss of income
63 40
GP charter inmpelemtaion plans
Reputation management board
appt of Director of
Transformation Stakeholder
map Stakeholder management
committee
Coomission
conversations.,
Locality and
lancashoire level
service redesign
groups Mgt
restructures focussed
at delivering efficency
effectivenss and
stakehoolder
intentions
Relationship management
plan with identified clear
leadership Operational
management structure
refocused and reskilled to
manage external world
Multiple stakeholder
management media in place
Transformation Director not
in place C. Roles not fully
worked through linked top
formal governance
procedure Unknown key
stakeholders at ,moment
particularly around clinical
commissioning groups
Organisational expertise
Styakeholder map not
allocated systematically
Transformation programme
responding external world
sufficiently
01/03/2012
089
Mark Hindle
Develop external relationships focussed on
robust engagement to inform and support
organisational transformation
Limited robust formalised partnership &
contracting arrangements particularly in
changing of clinical commissioning groups
Failure to realise benefits of new
organisation to drive through
commercial and transformational
opportunities
Stakeholder management
analysis undertaken Links at
executive level made with
emerging consortia Contract
mgt and business planning
Comms Service reviews
identoified and underweay and
reporting back Lancashire and
locality for a esatblished with
CCG reperesenation
Team to team events
Stakeholder mapping
Rethink open to new
ways Appreciative
leadership programme
Change/inconsistent
approach to
contracting/service delivery.
Development of Roles
required, linked top formal
governance procedure
Unknown key stakeholders
at moment particularly
around clinical
commissioning groups
Organisational expertise
Implication of Any Qualified
Provider Much
organisational
transformation aimed at
productivity not supported
by service user needs and
outcomes 01/03/2012
90
Mark Hindle
Develop external relationships focussed on
robust engagement to inform and support
organisational transformation
Discontinuity amongst commissioners and
stakeholders
Loss of income, residual services
higher risk lower profitability
49 35
Agreed transition Plan, Locality
and Lancashire Transformation
Groups in place Contracting
process in place underpinned by
service specifiactions
Appreciative Leadership
Programme
Reputation
management board
Capital project board
Conversations with key
stakeholders LTCC quip
planAppreciative
leadership programme
Determining flexible offer
within context of contract
Knowing what we don’t
know horizon scanning
dedicated resource to
manage this complexity We
don’t have variable
stakeholder engagement.
Roles not fully worked
through linked top formal
governance procedure
Unknown key stakeholders
at ,moment particularly
around clinical
commissioning groups
Organisational expertise
analysis of key
organisational risk
01/03/2012
14
Executive Risk Register
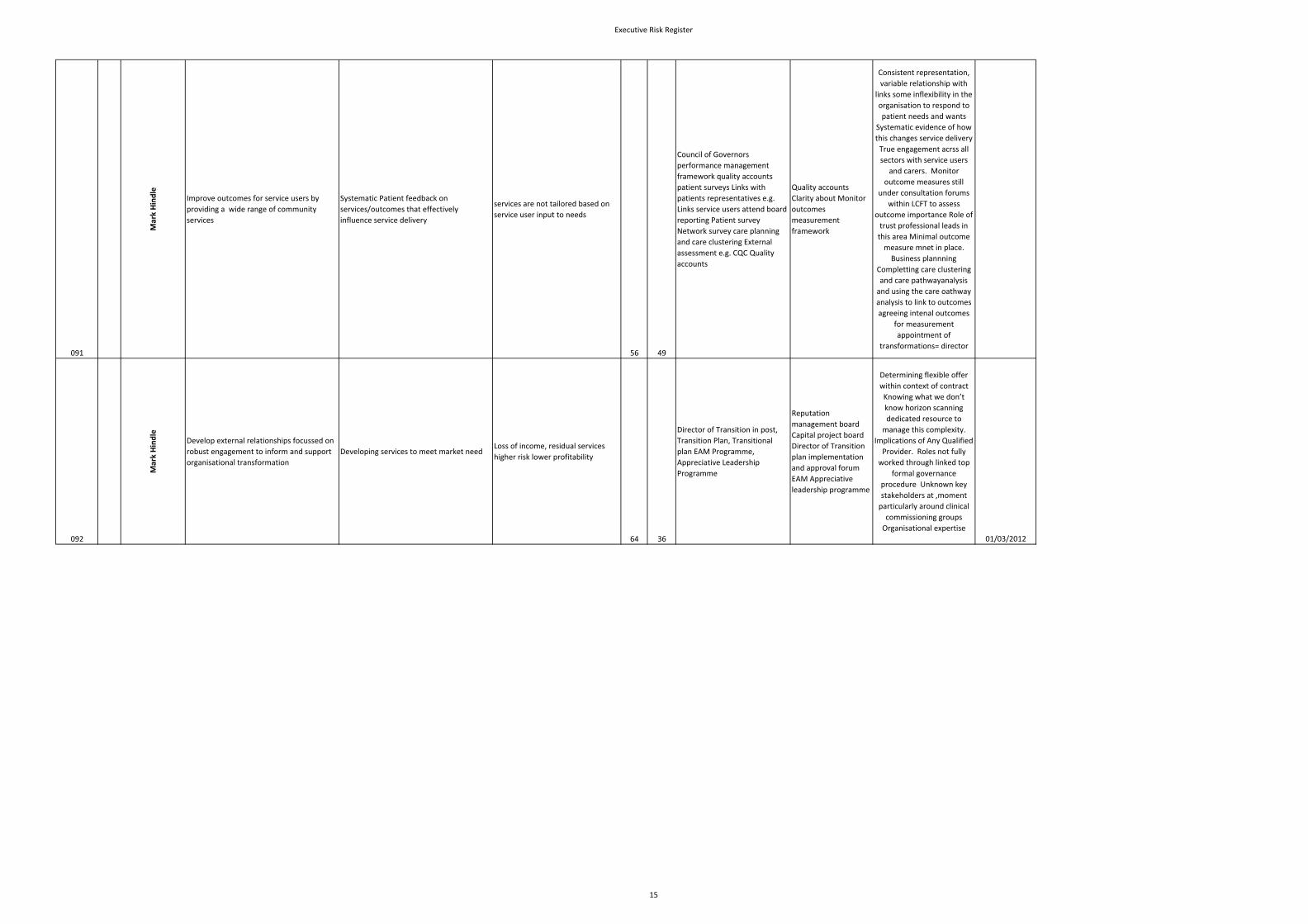
091
Mark Hindle
Improve outcomes for service users by
providing a wide range of community
services
Systematic Patient feedback on
services/outcomes that effectively
influence service delivery
services are not tailored based on
service user input to needs
56 49
Council of Governors
performance management
framework quality accounts
patient surveys Links with
patients representatives e.g.
Links service users attend board
reporting Patient survey
Network survey care planning
and care clustering External
assessment e.g. CQC Quality
accounts
Quality accounts
Clarity about Monitor
outcomes
measurement
framework
Consistent representation,
variable relationship with
links some inflexibility in the
organisation to respond to
patient needs and wants
Systematic evidence of how
this changes service delivery
True engagement acrss all
sectors with service users
and carers. Monitor
outcome measures still
under consultation forums
within LCFT to assess
outcome importance Role of
trust professional leads in
this area Minimal outcome
measure mnet in place.
Business plannning
Completting care clustering
and care pathwayanalysis
and using the care oathway
analysis to link to outcomes
agreeing intenal outcomes
for measurement
appointment of
transformations= director
092
Mark Hindle
Develop external relationships focussed on
robust engagement to inform and support
organisational transformation
Developing services to meet market needLoss of income, residual services
higher risk lower profitability
64 36
Director of Transition in post,
Transition Plan, Transitional
plan EAM Programme,
Appreciative Leadership
Programme
Reputation
management board
Capital project board
Director of Transition
plan implementation
and approval forum
EAM Appreciative
leadership programme
Determining flexible offer
within context of contract
Knowing what we don’t
know horizon scanning
dedicated resource to
manage this complexity.
Implications of Any Qualified
Provider. Roles not fully
worked through linked top
formal governance
procedure Unknown key
stakeholders at ,moment
particularly around clinical
commissioning groups
Organisational expertise
01/03/2012
15
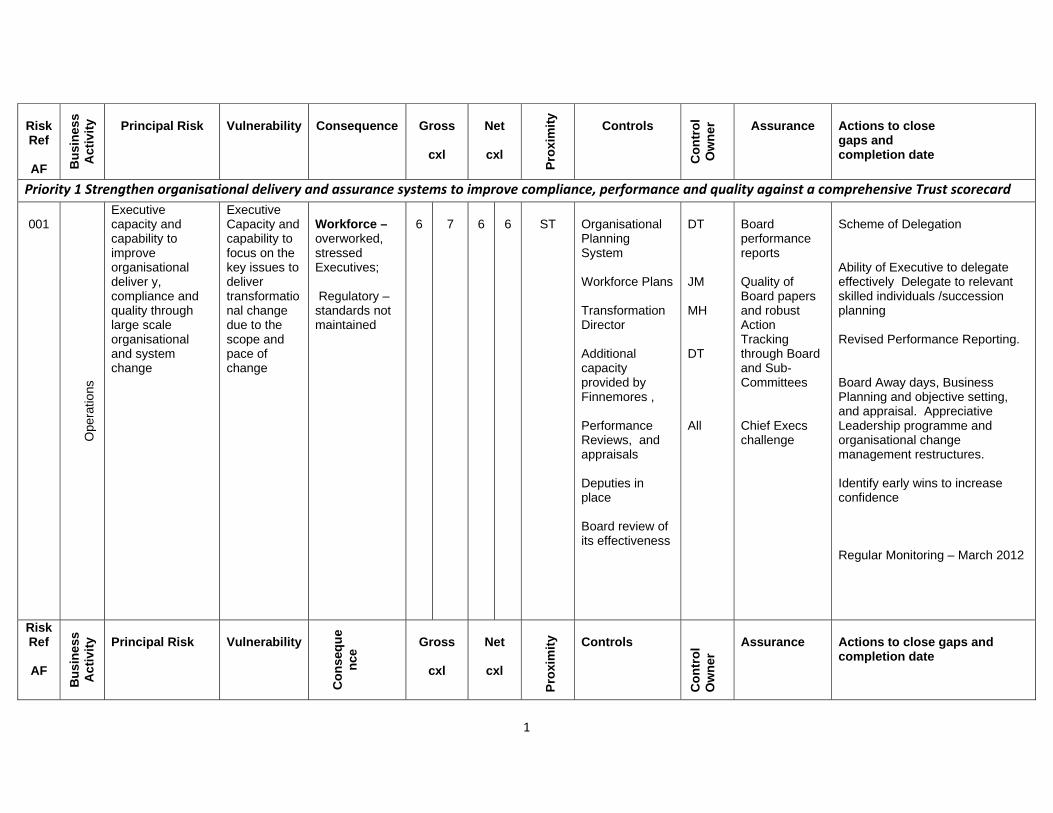
1
Risk Ref
AF B
usi
nes
s A
ctiv
ity
Principal Risk
Vulnerability Consequence Gross
cxl
Net
cxl
P
roxi
mit
y Controls
Co
ntr
ol
Ow
ner
Assurance Actions to close gaps and completion date
Priority 1 Strengthen organisational delivery and assurance systems to improve compliance, performance and quality against a comprehensive Trust scorecard
001
O
pera
tions
Executive capacity and capability to improve organisational deliver y, compliance and quality through large scale organisational and system change
Executive Capacity and capability to focus on the key issues to deliver transformational change due to the scope and pace of change
Workforce – overworked, stressed Executives; Regulatory – standards not maintained
6
7
6
6
ST
Organisational Planning System Workforce Plans Transformation Director Additional capacity provided by Finnemores , Performance Reviews, and appraisals Deputies in place Board review of its effectiveness
DT JM MH DT All
Board performance reports Quality of Board papers and robust Action Tracking through Board and Sub- Committees Chief Execs challenge
Scheme of Delegation Ability of Executive to delegate effectively Delegate to relevant skilled individuals /succession planning Revised Performance Reporting. Board Away days, Business Planning and objective setting, and appraisal. Appreciative Leadership programme and organisational change management restructures. Identify early wins to increase confidence Regular Monitoring – March 2012
Risk Ref
AF
Bu
sin
ess
Ac
tivi
ty
Principal Risk Vulnerability
C
on
seq
ue
nce
Gross
cxl
Net
cxl
P
roxi
mit
y Controls
Co
ntr
ol
Ow
ner
Assurance Actions to close gaps and completion date
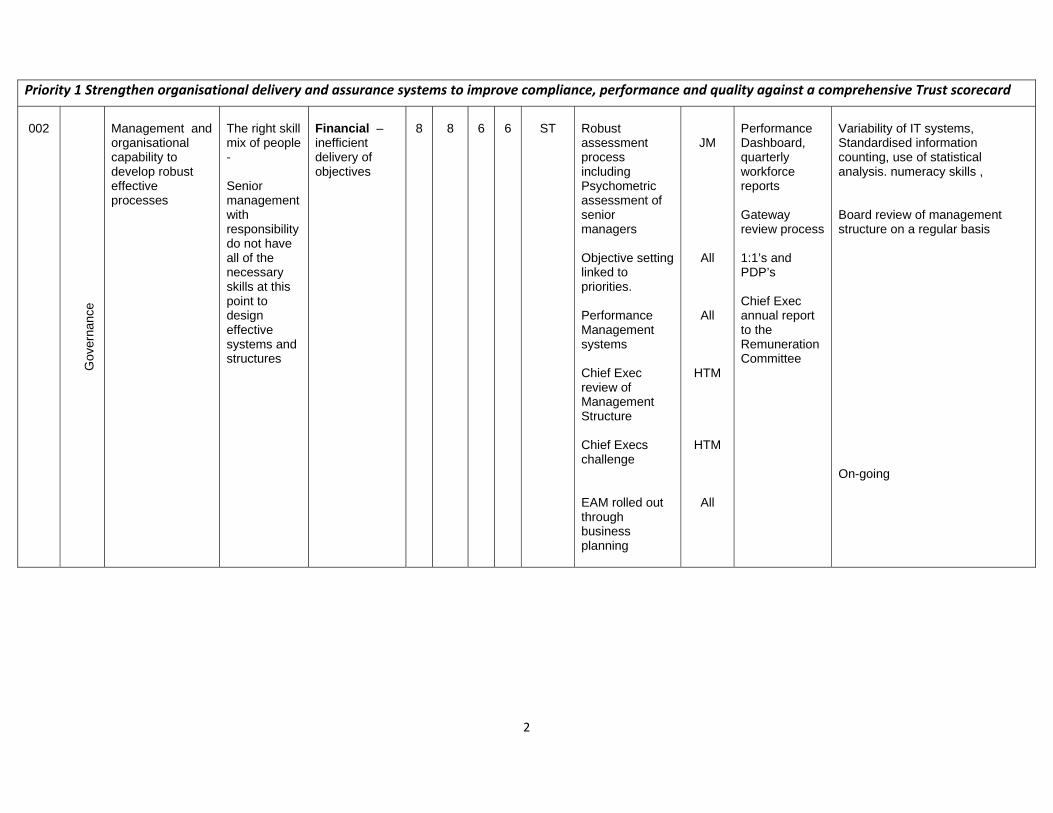
2
Priority 1 Strengthen organisational delivery and assurance systems to improve compliance, performance and quality against a comprehensive Trust scorecard
002
G
over
nanc
e
Management and organisational capability to develop robust effective processes
The right skill mix of people - Senior management with responsibility do not have all of the necessary skills at this point to design effective systems and structures
Financial – inefficient delivery of objectives
8
8
6
6
ST
Robust assessment process including Psychometric assessment of senior managers Objective setting linked to priorities. Performance Management systems Chief Exec review of Management Structure Chief Execs challenge EAM rolled out through business planning
JM
All
All
HTM
HTM
All
Performance Dashboard, quarterly workforce reports Gateway review process 1:1’s and PDP’s Chief Exec annual report to the Remuneration Committee
Variability of IT systems, Standardised information counting, use of statistical analysis. numeracy skills , Board review of management structure on a regular basis On-going
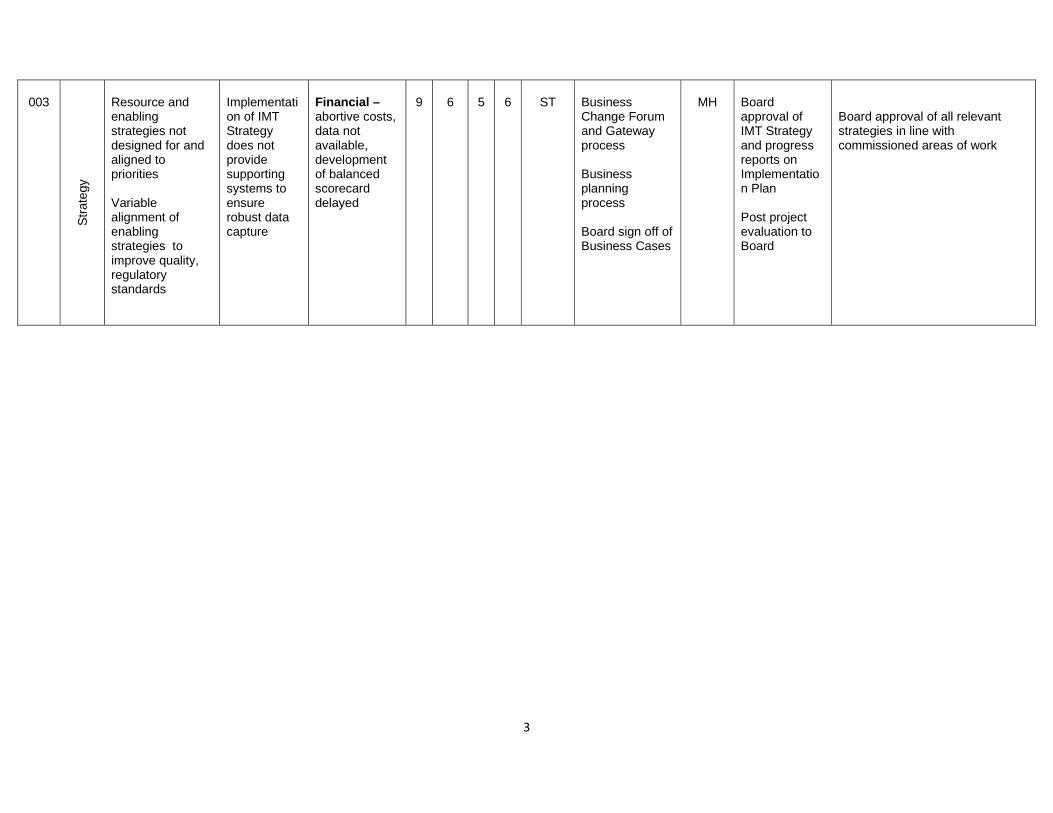
3
003
Str
ateg
y Resource and enabling strategies not designed for and aligned to priorities Variable alignment of enabling strategies to improve quality, regulatory standards
Implementation of IMT Strategy does not provide supporting systems to ensure robust data capture
Financial – abortive costs, data not available, development of balanced scorecard delayed
9
6
5
6
ST
Business Change Forum and Gateway process Business planning process Board sign off of Business Cases
MH
Board approval of IMT Strategy and progress reports on Implementation Plan Post project evaluation to Board
Board approval of all relevant strategies in line with commissioned areas of work
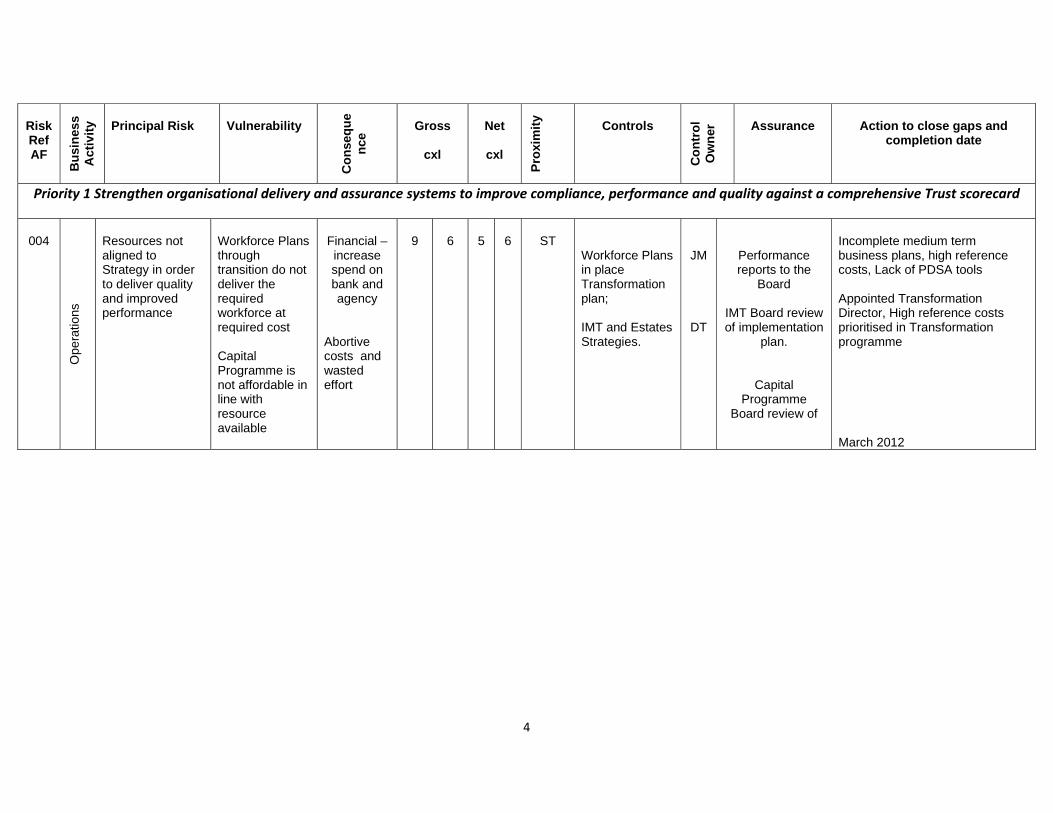
4
Risk Ref AF
Bu
sin
ess
Act
ivit
y
Principal Risk
Vulnerability
C
on
seq
ue
nce
Gross
cxl
Net
cxl
Pro
xim
ity
Controls
Co
ntr
ol
Ow
ner
Assurance Action to close gaps and completion date
Priority 1 Strengthen organisational delivery and assurance systems to improve compliance, performance and quality against a comprehensive Trust scorecard
004
Ope
ratio
ns
Resources not aligned to Strategy in order to deliver quality and improved performance
Workforce Plans through transition do not deliver the required workforce at required cost Capital Programme is not affordable in line with resource available
Financial – increase spend on bank and agency
Abortive costs and wasted effort
9
6
5
6
ST
Workforce Plans in place Transformation plan; IMT and Estates Strategies.
JM
DT
Performance reports to the
Board
IMT Board review of implementation
plan.
Capital Programme
Board review of
Incomplete medium term business plans, high reference costs, Lack of PDSA tools Appointed Transformation Director, High reference costs prioritised in Transformation programme March 2012
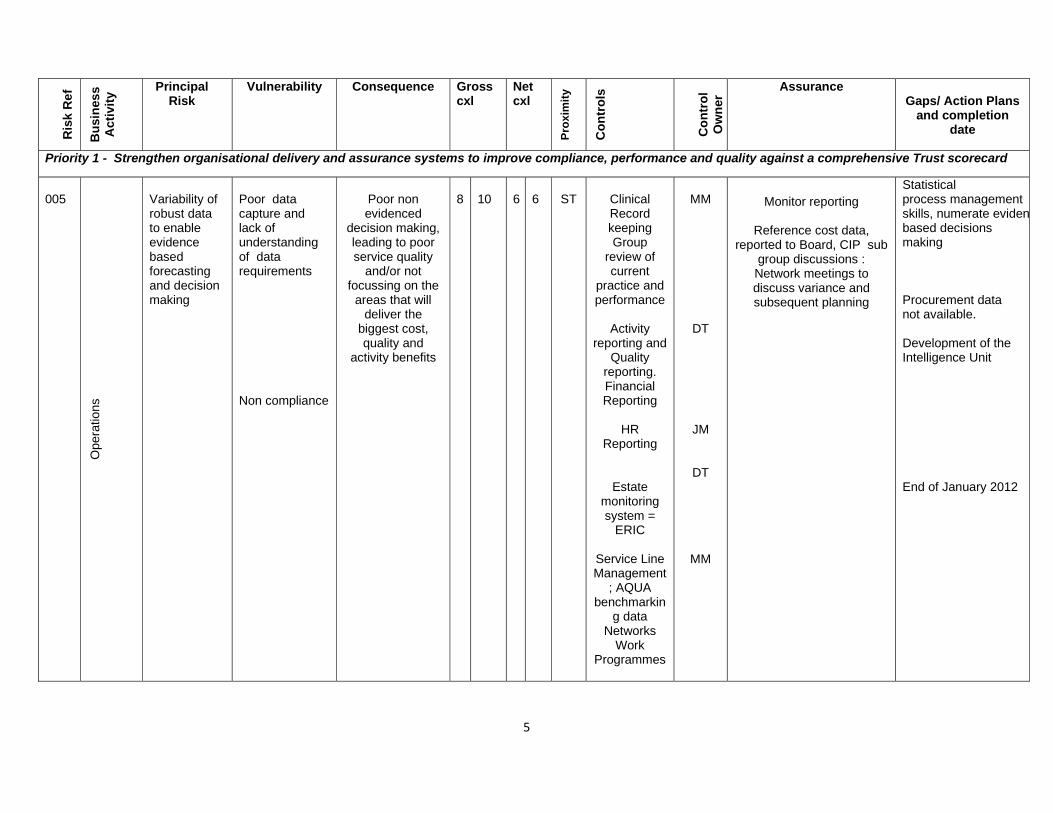
5
R
isk
Re
f
Bu
sin
ess
Act
ivit
y Principal
Risk Vulnerability Consequence Gross
cxl Netcxl
Pro
xim
ity
Co
ntr
ols
C
on
tro
l O
wn
er Assurance
Gaps/ Action Plans and completion
date
Priority 1 - Strengthen organisational delivery and assurance systems to improve compliance, performance and quality against a comprehensive Trust scorecard
005
Ope
ratio
ns
Variability of robust data to enable evidence based forecasting and decision making
Poor data capture and lack of understanding of data requirements Non compliance
Poor non evidenced
decision making, leading to poor service quality
and/or not focussing on the
areas that will deliver the
biggest cost, quality and
activity benefits
8
10
6
6
ST
Clinical Record keeping Group
review of current
practice and performance
Activity
reporting and Quality
reporting. Financial Reporting
HR
Reporting
Estate monitoring system =
ERIC
Service Line Management
; AQUA benchmarkin
g data Networks
Work Programmes
MM
DT
JM
DT
MM
Monitor reporting
Reference cost data, reported to Board, CIP sub
group discussions : Network meetings to discuss variance and subsequent planning
Statistical process management skills, numerate evidenbased decisions making Procurement data not available. Development of the Intelligence Unit End of January 2012
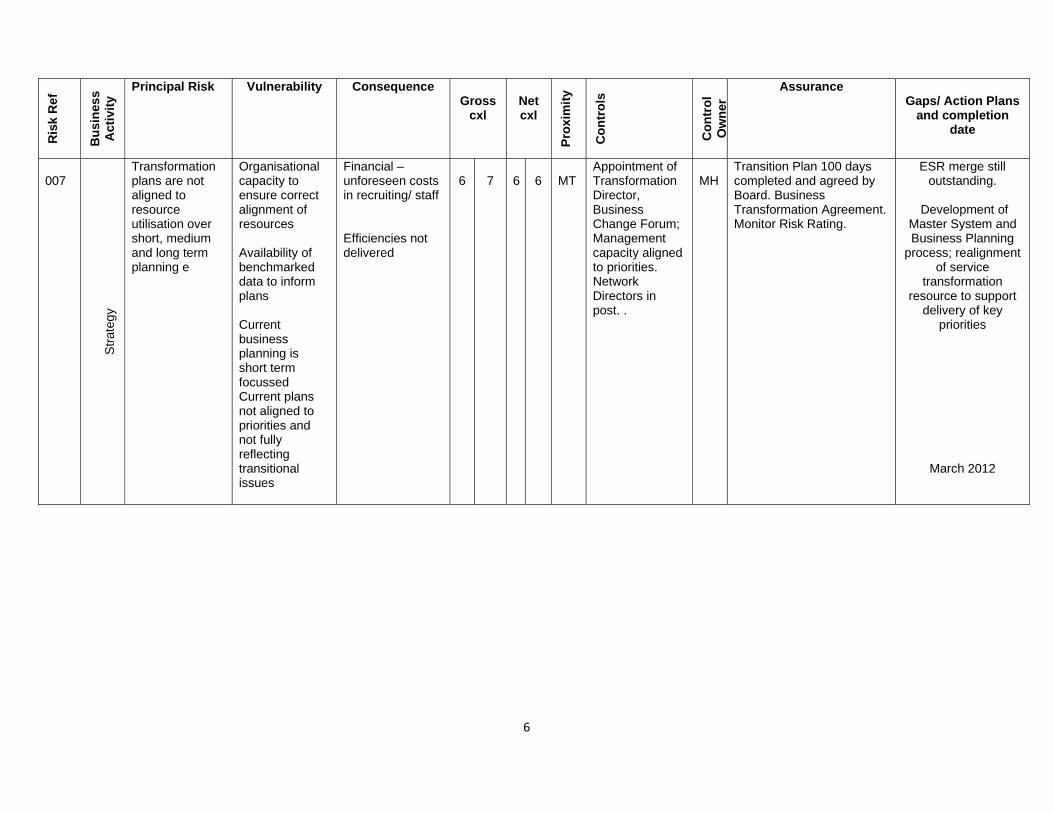
6
Ris
k R
ef
Bu
sin
ess
Act
ivit
y Principal Risk Vulnerability Consequence
Gross cxl
Net cxl
Pro
xim
ity
Co
ntr
ols
Co
ntr
ol
Ow
ner
Assurance Gaps/ Action Plans
and completion date
007
S
trat
egy
Transformation plans are not aligned to resource utilisation over short, medium and long term planning e
Organisational capacity to ensure correct alignment of resources Availability of benchmarked data to inform plans Current business planning is short term focussed Current plans not aligned to priorities and not fully reflecting transitional issues
Financial – unforeseen costs in recruiting/ staff Efficiencies not delivered
6
7
6
6
MT
Appointment of Transformation Director, Business Change Forum; Management capacity aligned to priorities. Network Directors in post. .
MH
Transition Plan 100 days completed and agreed by Board. Business Transformation Agreement. Monitor Risk Rating.
ESR merge still outstanding.
Development of
Master System and Business Planning
process; realignment of service
transformation resource to support
delivery of key priorities
March 2012
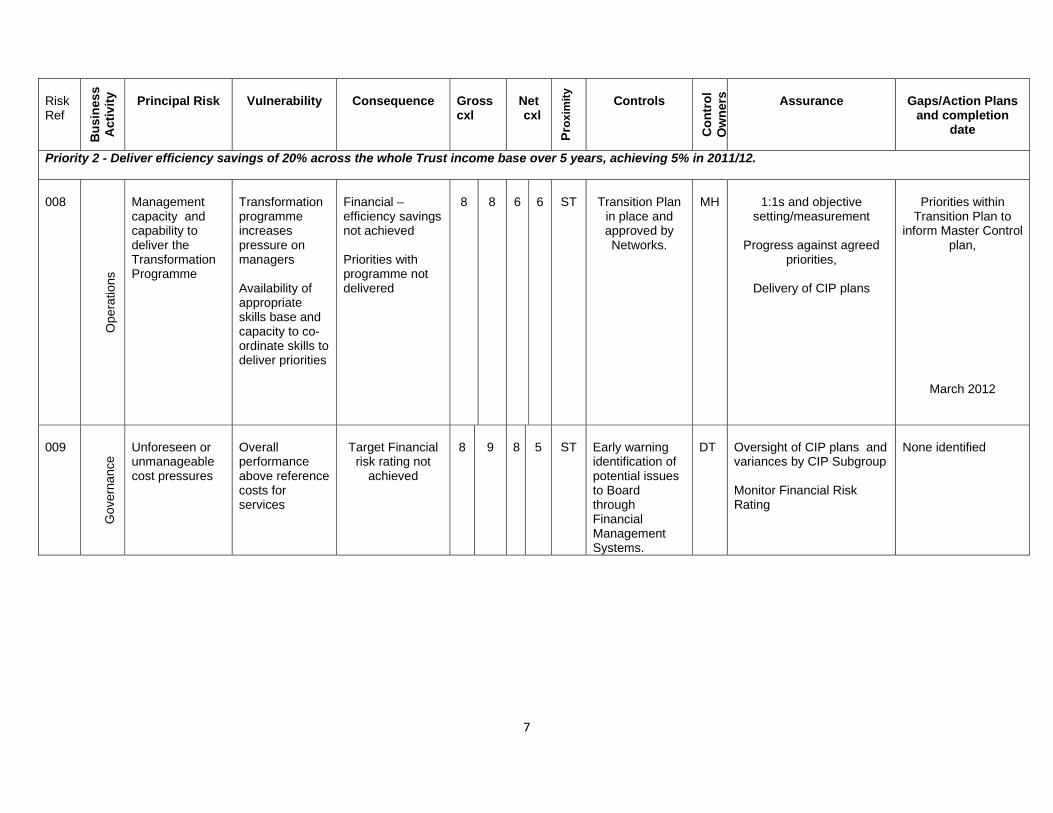
7
Risk Ref
Bu
sin
ess
Act
ivit
y
Principal Risk
Vulnerability Consequence Gross cxl
Net cxl
Pro
xim
ity
Controls
Co
ntr
ol
Ow
ner
s Assurance Gaps/Action Plans and completion
date
Priority 2 - Deliver efficiency savings of 20% across the whole Trust income base over 5 years, achieving 5% in 2011/12.
008
O
pera
tions
Management capacity and capability to deliver the Transformation Programme
Transformation programme increases pressure on managers Availability of appropriate skills base and capacity to co-ordinate skills to deliver priorities
Financial – efficiency savings not achieved Priorities with programme not delivered
8
8
6
6
ST
Transition Plan
in place and approved by Networks.
MH
1:1s and objective
setting/measurement
Progress against agreed priorities,
Delivery of CIP plans
Priorities within
Transition Plan to inform Master Control
plan,
March 2012
009
G
over
nanc
e
Unforeseen or unmanageable cost pressures
Overall performance above reference costs for services
Target Financial
risk rating not achieved
8
9
8
5
ST
Early warning identification of potential issues to Board through Financial Management Systems.
DT
Oversight of CIP plans and variances by CIP Subgroup Monitor Financial Risk Rating
None identified
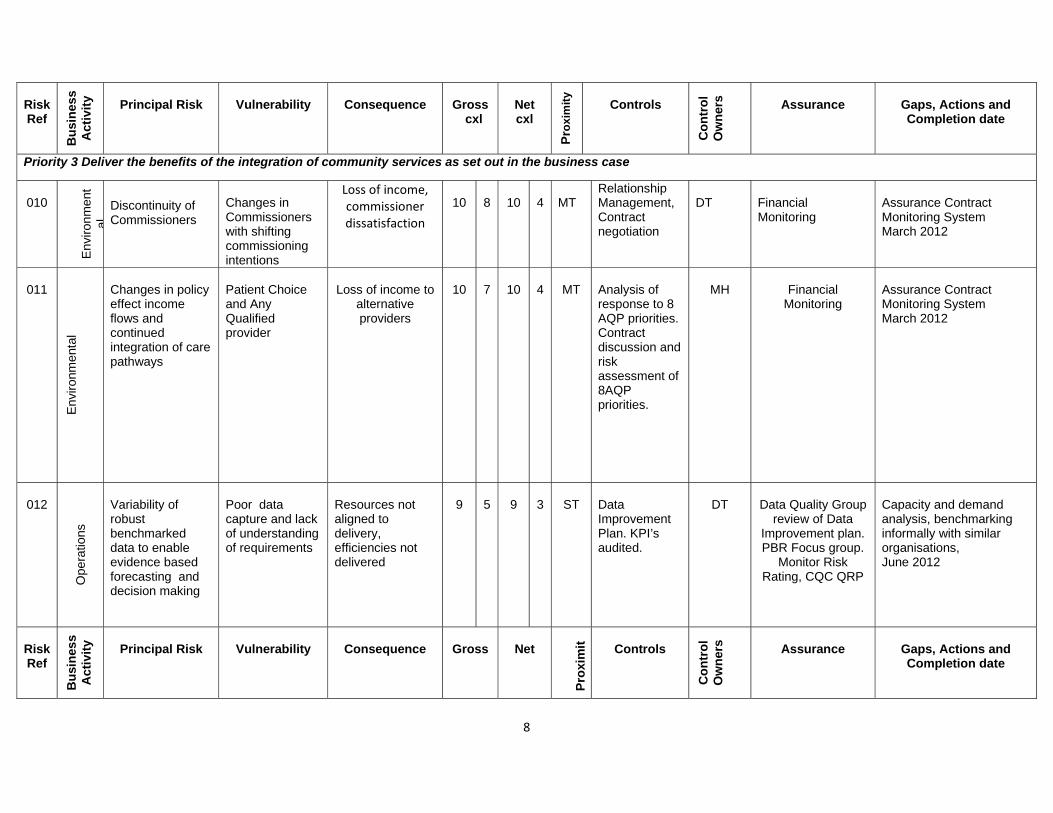
8
Risk Ref
Bu
sin
ess
Act
ivit
y
Principal Risk
Vulnerability Consequence Gross cxl
Net cxl
Pro
xim
ity
Controls
Co
ntr
ol
Ow
ner
s Assurance Gaps, Actions and Completion date
Priority 3 Deliver the benefits of the integration of community services as set out in the business case
010
E
nviro
nmen
tal
Discontinuity of Commissioners
Changes in Commissioners with shifting commissioning intentions
Loss of income, commissioner dissatisfaction
10
8
10
4
MT
Relationship Management, Contract negotiation
DT
Financial Monitoring
Assurance Contract Monitoring System March 2012
011
Env
ironm
enta
l
Changes in policy effect income flows and continued integration of care pathways
Patient Choice and Any Qualified provider
Loss of income to
alternative providers
10
7
10
4
MT
Analysis of response to 8 AQP priorities. Contract discussion and risk assessment of 8AQP priorities.
MH
Financial
Monitoring
Assurance Contract Monitoring System March 2012
012
Ope
ratio
ns
Variability of robust benchmarked data to enable evidence based forecasting and decision making
Poor data capture and lack of understanding of requirements
Resources not aligned to delivery, efficiencies not delivered
9
5
9
3
ST
Data Improvement Plan. KPI’s audited.
DT
Data Quality Group
review of Data Improvement plan. PBR Focus group.
Monitor Risk Rating, CQC QRP
Capacity and demand analysis, benchmarking informally with similar organisations, June 2012
Risk Ref
Bu
sin
ess
Act
ivit
y
Principal Risk
Vulnerability Consequence Gross Net
Pro
xim
it
Controls
Co
ntr
ol
Ow
ner
s Assurance Gaps, Actions and Completion date
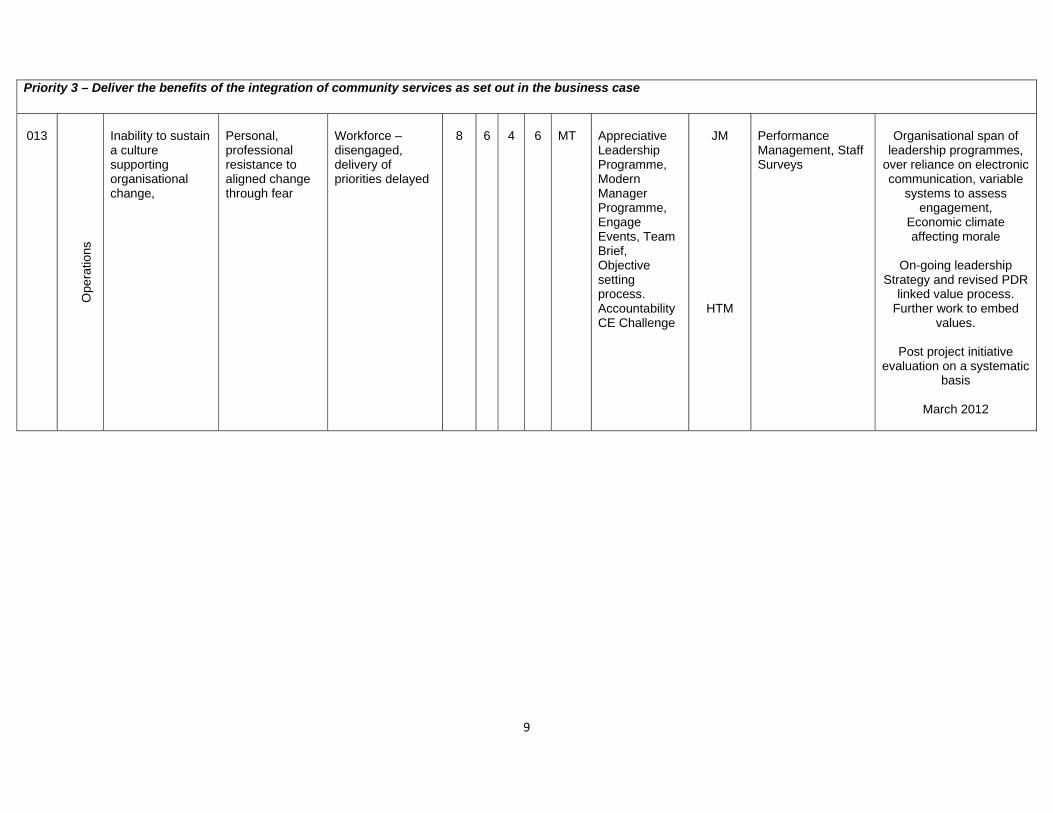
9
Priority 3 – Deliver the benefits of the integration of community services as set out in the business case
013
O
pera
tions
Inability to sustain a culture supporting organisational change,
Personal, professional resistance to aligned change through fear
Workforce – disengaged, delivery of priorities delayed
8
6
4
6
MT
Appreciative Leadership Programme, Modern Manager Programme, Engage Events, Team Brief, Objective setting process. Accountability CE Challenge
JM
HTM
Performance Management, Staff Surveys
Organisational span of
leadership programmes, over reliance on electronic communication, variable
systems to assess engagement,
Economic climate affecting morale
On-going leadership
Strategy and revised PDR linked value process.
Further work to embed values.
Post project initiative
evaluation on a systematic basis
March 2012
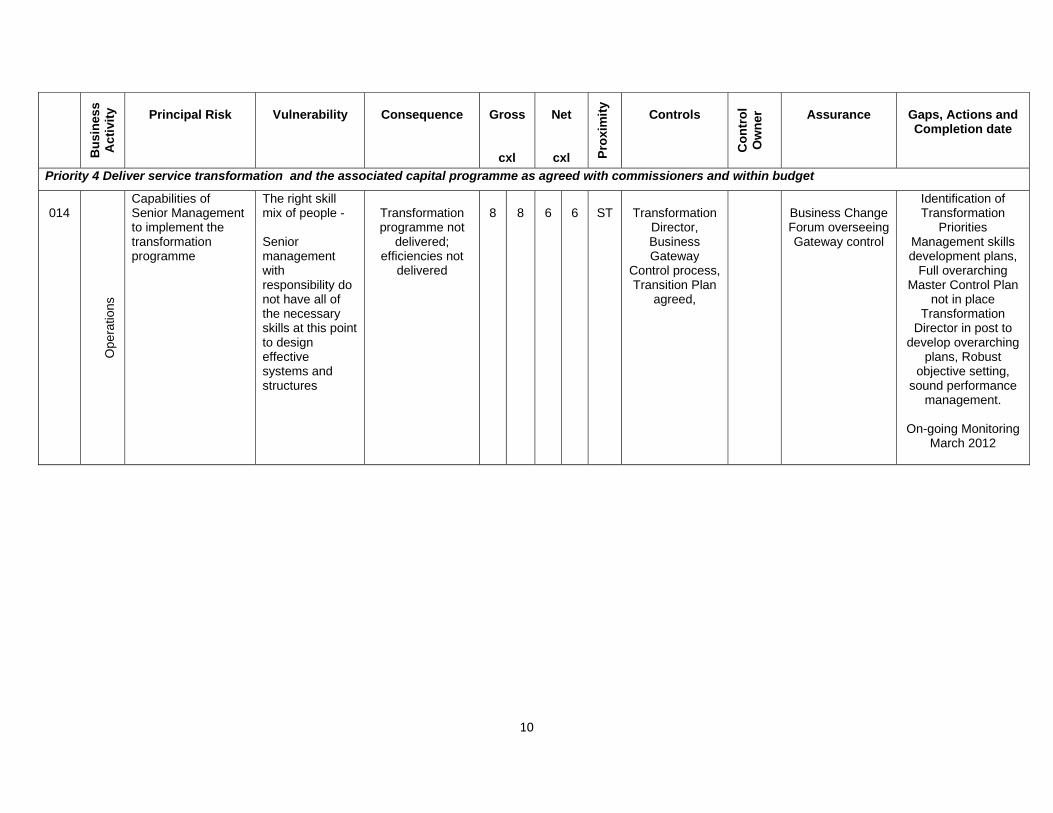
10
Bu
sin
ess
Ac
tivi
ty
Principal Risk
Vulnerability Consequence Gross
cxl
Net
cxl Pro
xim
ity
Controls
Co
ntr
ol
Ow
ner
Assurance Gaps, Actions and Completion date
Priority 4 Deliver service transformation and the associated capital programme as agreed with commissioners and within budget
014
O
pera
tions
Capabilities of Senior Management to implement the transformation programme
The right skill mix of people - Senior management with responsibility do not have all of the necessary skills at this point to design effective systems and structures
Transformation programme not
delivered; efficiencies not
delivered
8
8
6
6
ST
Transformation
Director, Business Gateway
Control process, Transition Plan
agreed,
Business Change Forum overseeing Gateway control
Identification of Transformation
Priorities Management skills development plans,
Full overarching Master Control Plan
not in place Transformation
Director in post to develop overarching
plans, Robust objective setting,
sound performance management.
On-going Monitoring
March 2012
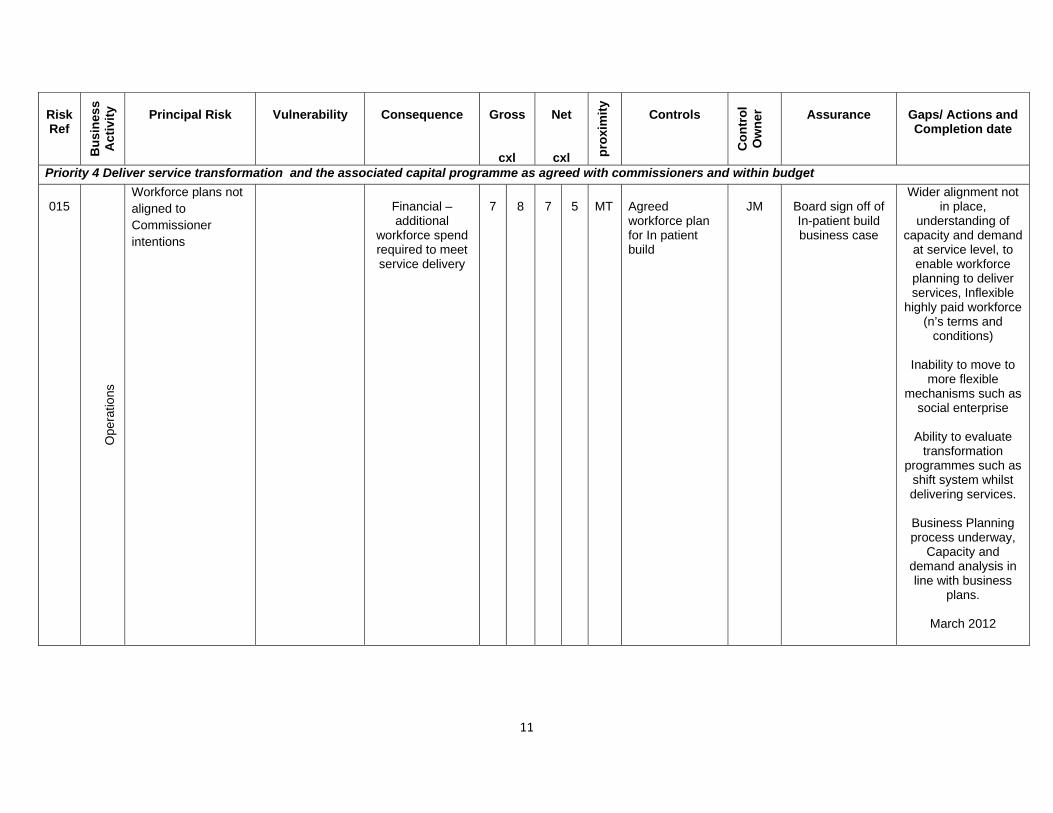
11
Risk Ref
Bu
sin
ess
Act
ivit
y
Principal Risk
Vulnerability Consequence Gross
cxl
Net
cxl pro
xim
ity
Controls
Co
ntr
ol
Ow
ner
Assurance Gaps/ Actions and Completion date
Priority 4 Deliver service transformation and the associated capital programme as agreed with commissioners and within budget
015
O
pera
tions
Workforce plans not aligned to Commissioner intentions
Financial – additional
workforce spend required to meet service delivery
7
8
7
5
MT
Agreed workforce plan for In patient build
JM
Board sign off of In-patient build business case
Wider alignment not in place,
understanding of capacity and demand
at service level, to enable workforce planning to deliver services, Inflexible
highly paid workforce (n’s terms and
conditions)
Inability to move to more flexible
mechanisms such as social enterprise
Ability to evaluate
transformation programmes such as
shift system whilst delivering services.
Business Planning process underway,
Capacity and demand analysis in line with business
plans.
March 2012
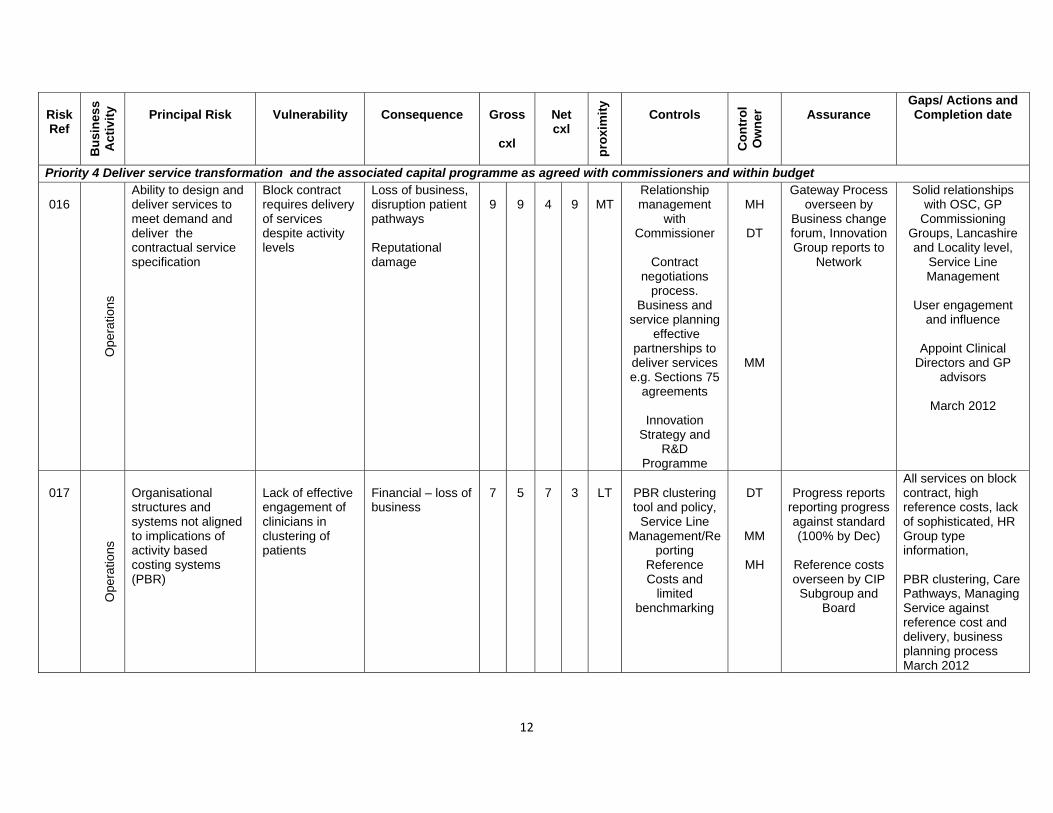
12
Risk Ref
Bu
sin
ess
Act
ivit
y
Principal Risk
Vulnerability Consequence Gross
cxl
Net cxl
pro
xim
ity
Controls
Co
ntr
ol
Ow
ner
Assurance Gaps/ Actions and Completion date
Priority 4 Deliver service transformation and the associated capital programme as agreed with commissioners and within budget
016
O
pera
tions
Ability to design and deliver services to meet demand and deliver the contractual service specification
Block contract requires delivery of services despite activity levels
Loss of business, disruption patient pathways Reputational damage
9
9
4
9
MT
Relationship management
with Commissioner
Contract
negotiations process.
Business and service planning
effective partnerships to deliver services e.g. Sections 75
agreements
Innovation Strategy and
R&D Programme
MH
DT
MM
Gateway Process overseen by
Business change forum, Innovation Group reports to
Network
Solid relationships with OSC, GP
Commissioning Groups, Lancashire and Locality level,
Service Line Management
User engagement
and influence
Appoint Clinical Directors and GP
advisors
March 2012
017
O
pera
tions
Organisational structures and systems not aligned to implications of activity based costing systems (PBR)
Lack of effective engagement of clinicians in clustering of patients
Financial – loss of business
7
5
7
3
LT
PBR clustering tool and policy,
Service Line Management/Re
porting Reference Costs and
limited benchmarking
DT
MM
MH
Progress reports
reporting progress against standard (100% by Dec)
Reference costs overseen by CIP
Subgroup and Board
All services on block contract, high reference costs, lack of sophisticated, HR Group type information, PBR clustering, Care Pathways, Managing Service against reference cost and delivery, business planning process March 2012
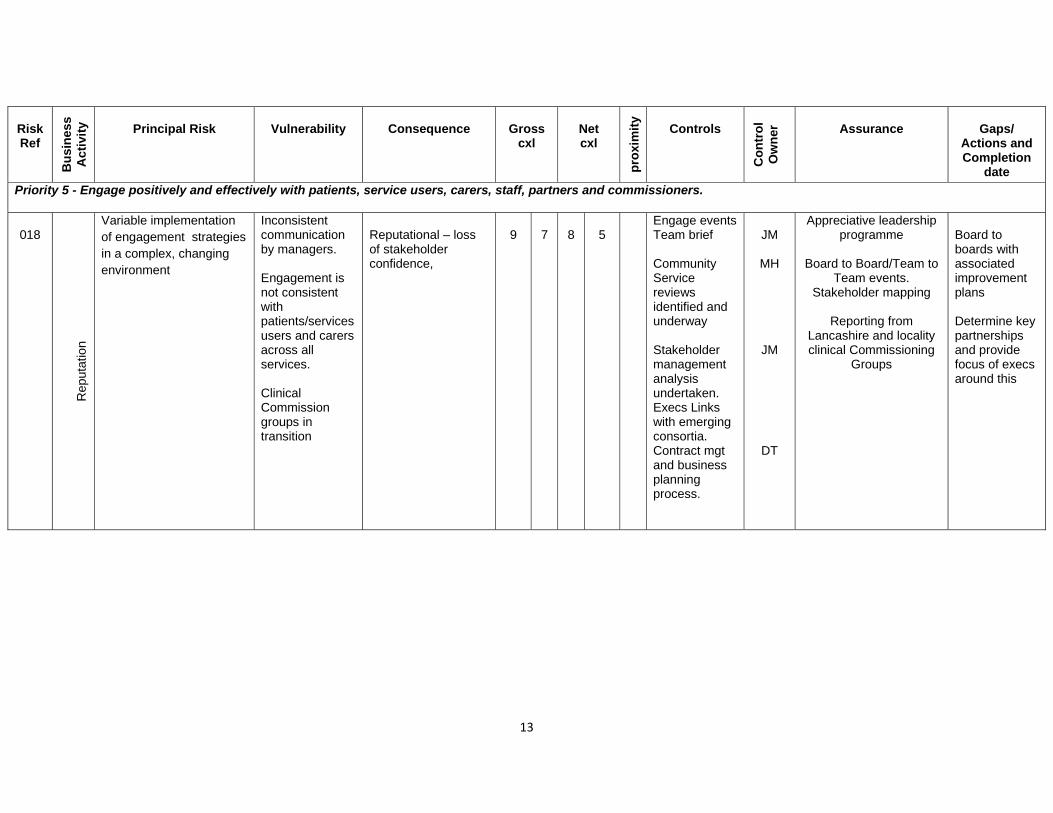
13
Risk Ref
Bu
sin
ess
Ac
tivi
ty
Principal Risk
Vulnerability Consequence Gross cxl
Net cxl
pro
xim
ity
Controls
Co
ntr
ol
Ow
ner
Assurance
Gaps/ Actions and Completion
date
Priority 5 - Engage positively and effectively with patients, service users, carers, staff, partners and commissioners.
018
R
eput
atio
n
Variable implementation of engagement strategies in a complex, changing environment
Inconsistent communication by managers. Engagement is not consistent with patients/services users and carers across all services. Clinical Commission groups in transition
Reputational – loss of stakeholder confidence,
9
7
8
5
Engage events Team brief Community Service reviews identified and underway Stakeholder management analysis undertaken. Execs Links with emerging consortia. Contract mgt and business planning process.
JM
MH
JM
DT
Appreciative leadership programme
Board to Board/Team to
Team events. Stakeholder mapping
Reporting from
Lancashire and locality clinical Commissioning
Groups
Board to boards with associated improvement plans Determine key partnerships and provide focus of execs around this
14
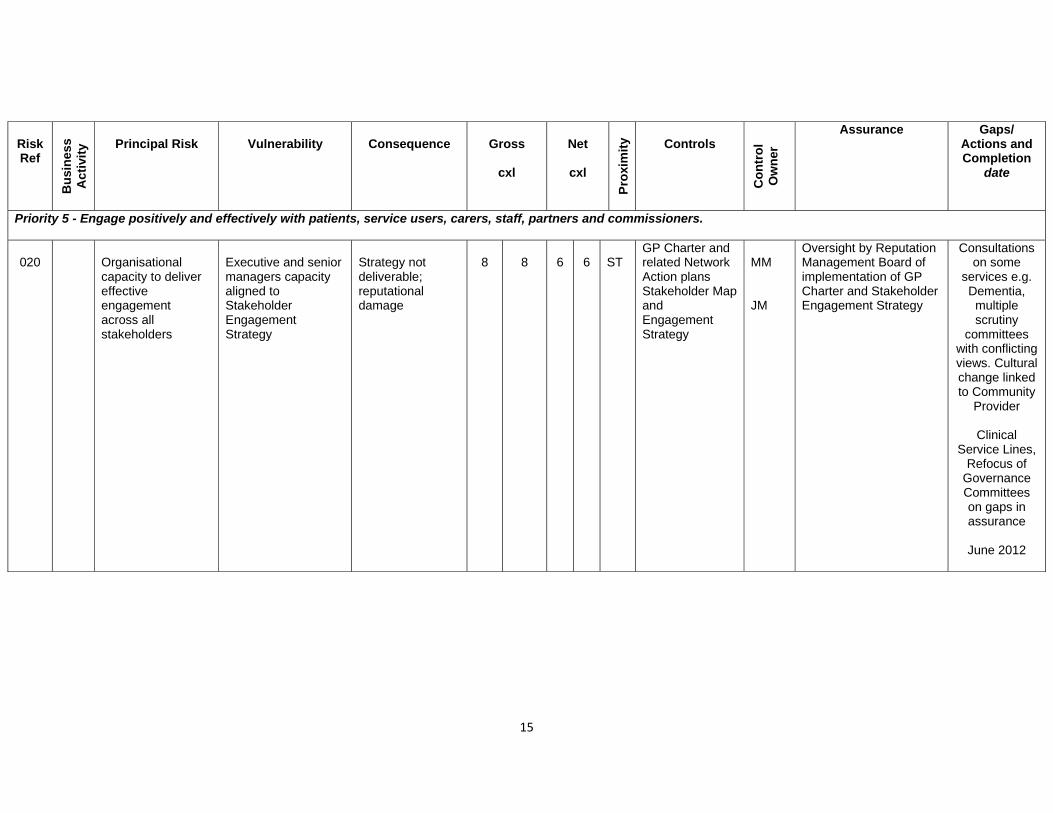
15
Risk Ref
Bu
sin
ess
Ac
tivi
ty
Principal Risk
Vulnerability Consequence Gross
cxl
Net
cxl
Pro
xim
ity Controls
Co
ntr
ol
Ow
ner
Assurance
Gaps/ Actions and Completion
date
Priority 5 - Engage positively and effectively with patients, service users, carers, staff, partners and commissioners.
020
Organisational capacity to deliver effective engagement across all stakeholders
Executive and senior managers capacity aligned to Stakeholder Engagement Strategy
Strategy not deliverable; reputational damage
8
8
6
6
ST
GP Charter and related Network Action plans Stakeholder Map and Engagement Strategy
MM JM
Oversight by Reputation Management Board of implementation of GP Charter and Stakeholder Engagement Strategy
Consultations on some
services e.g. Dementia, multiple scrutiny
committees with conflicting views. Cultural change linked to Community
Provider
Clinical Service Lines,
Refocus of Governance Committees on gaps in assurance
June 2012
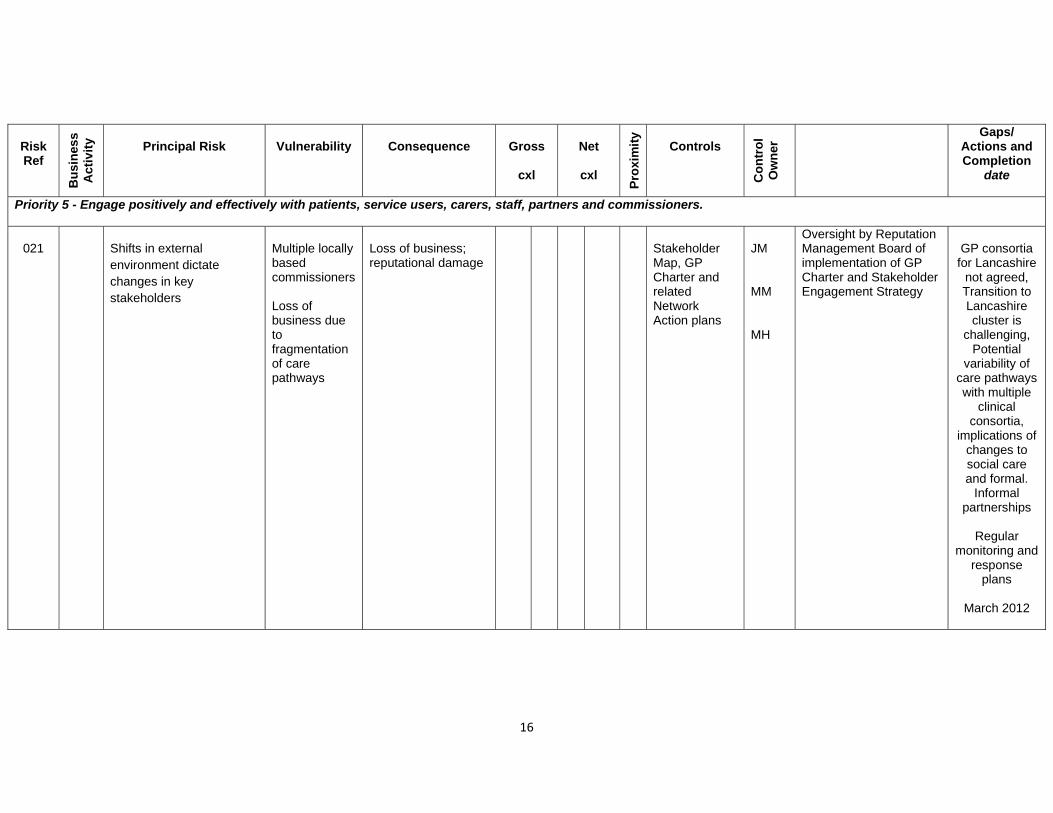
16
Risk Ref
Bu
sin
ess
Act
ivit
y
Principal Risk
Vulnerability Consequence Gross
cxl
Net
cxl P
roxi
mit
y
Controls
Co
ntr
ol
Ow
ner
Gaps/ Actions and Completion
date
Priority 5 - Engage positively and effectively with patients, service users, carers, staff, partners and commissioners.
021
Shifts in external environment dictate changes in key stakeholders
Multiple locally based commissioners Loss of business due to fragmentation of care pathways
Loss of business; reputational damage
Stakeholder Map, GP Charter and related Network Action plans
JM MM MH
Oversight by Reputation Management Board of implementation of GP Charter and Stakeholder Engagement Strategy
GP consortia for Lancashire
not agreed, Transition to Lancashire cluster is
challenging, Potential
variability of care pathways with multiple
clinical consortia,
implications of changes to social care and formal.
Informal partnerships
Regular
monitoring and response
plans
March 2012
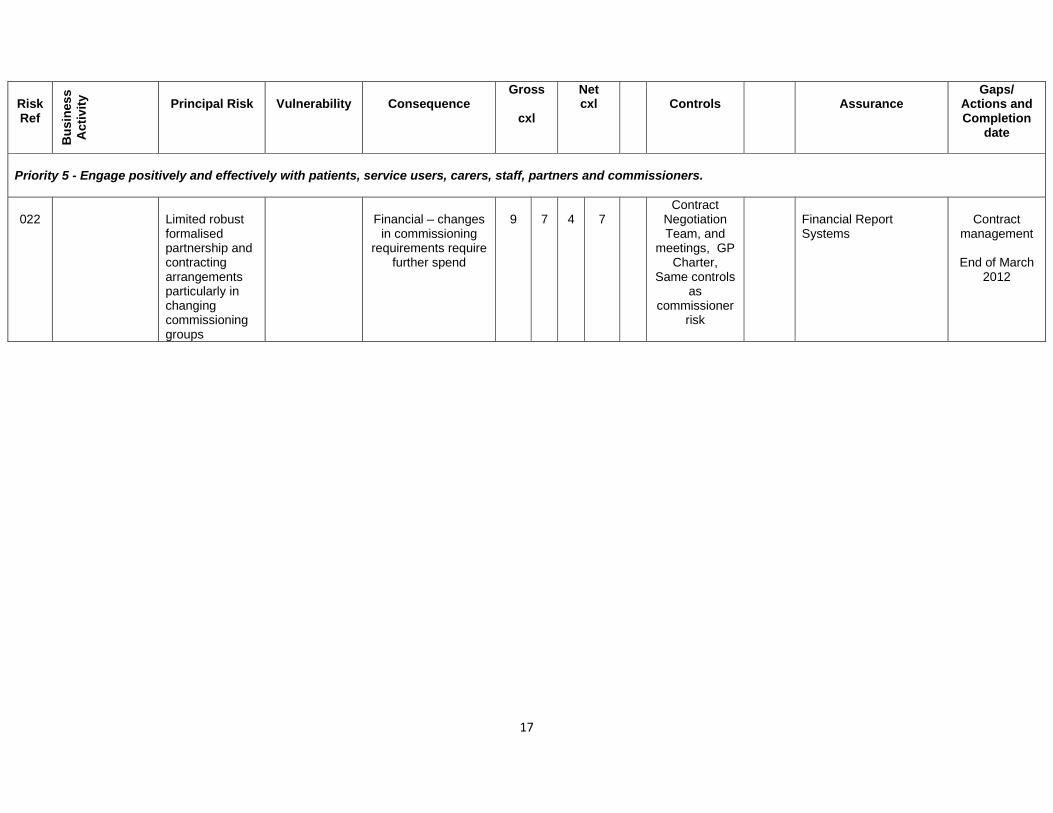
17
Risk Ref
Bu
sin
ess
Act
ivit
y
Principal Risk
Vulnerability Consequence Gross
cxl
Net cxl
Controls
Assurance
Gaps/ Actions and Completion
date
Priority 5 - Engage positively and effectively with patients, service users, carers, staff, partners and commissioners.
022
Limited robust formalised partnership and contracting arrangements particularly in changing commissioning groups
Financial – changes
in commissioning requirements require
further spend
9
7
4
7
Contract Negotiation Team, and
meetings, GP Charter,
Same controls as
commissioner risk
Financial Report Systems
Contract
management
End of March 2012
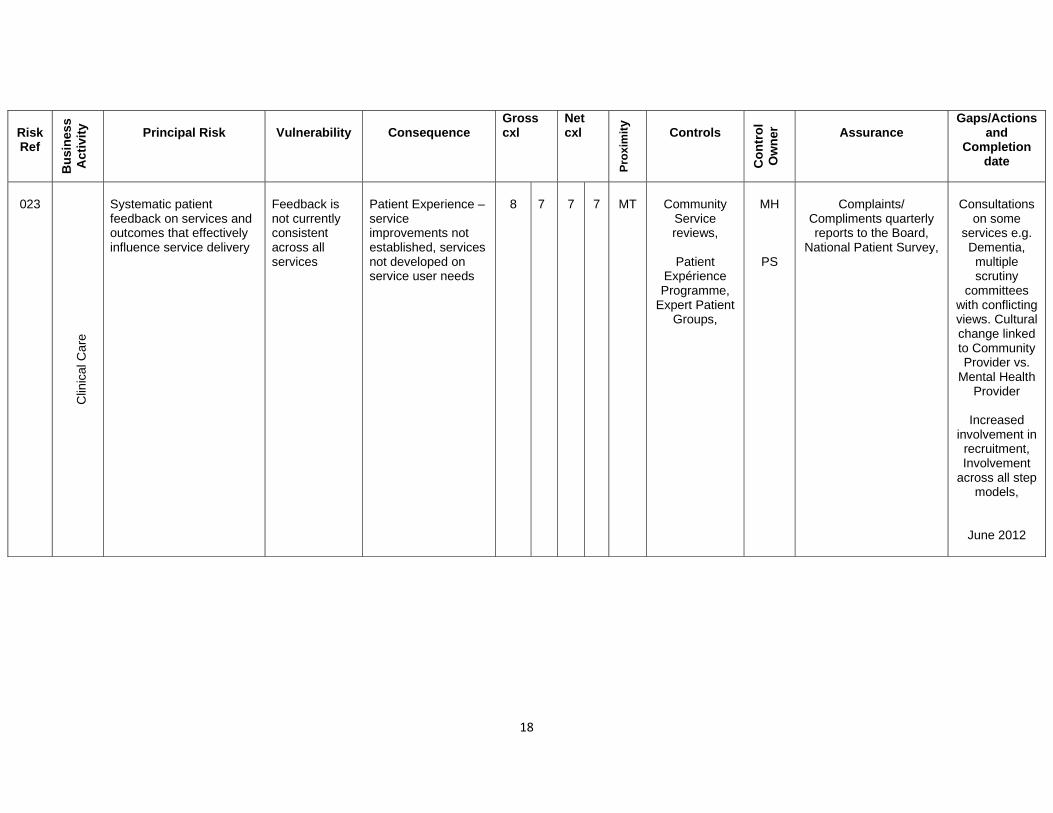
18
Risk Ref
Bu
sin
ess
Act
ivit
y
Principal Risk
Vulnerability Consequence Gross cxl
Netcxl
Pro
xim
ity
Controls
Co
ntr
ol
Ow
ner
Assurance Gaps/Actions
and Completion
date
023
C
linic
al C
are
Systematic patient feedback on services and outcomes that effectively influence service delivery
Feedback is not currently consistent across all services
Patient Experience – service improvements not established, services not developed on service user needs
8
7
7
7
MT
Community
Service reviews,
Patient
Expérience Programme,
Expert Patient Groups,
MH
PS
Complaints/
Compliments quarterly reports to the Board,
National Patient Survey,
Consultations
on some services e.g. Dementia, multiple scrutiny
committees with conflicting views. Cultural change linked to Community Provider vs.
Mental Health Provider
Increased
involvement in recruitment, Involvement
across all step models,
June 2012
19