aging and postural control. models of ageing two models of ageing (a) the concept that ageing...
TRANSCRIPT

Models of ageing
Two models of ageing
(a) The concept that ageing involves a linear decline in neuron function across all levels of the CNS. Primary aging model self limiting perceptions on the part of the older individuals regarding what they can do.
(b) The concept that during aging the CNS continues to function well until death, unless there is a catastrophe or disease that affects a specific part of the CNS. Secondary aging model optimistic view.

Interactions between Primary and Secondary factors
Primary and secondary factors may interact in the aging process
Example: genetic factors can include a genetic predisposition to a specific disease process.
Primary factors do not necessarily lead to a generalised decline in function, but rather to a loss of function within specific systems.
Secondary factors are more or less under our control. Some of these include nutrition, exercise, insults and pathologies that affect our mind and body.
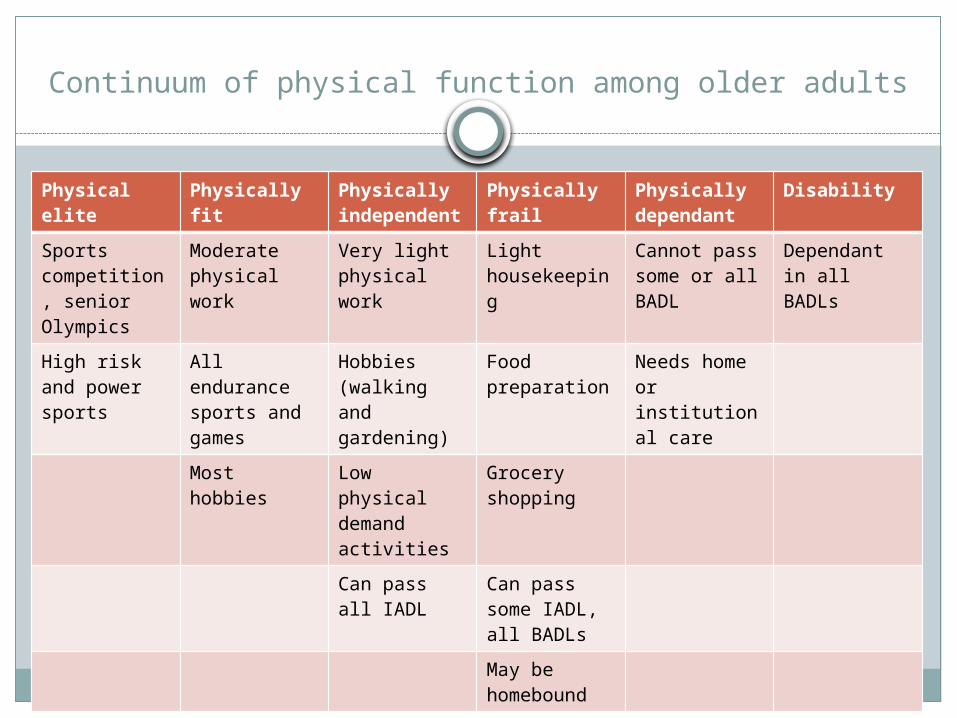
Continuum of physical function among older adults
Physical elite
Physically fit
Physically independent
Physically frail
Physically dependant
Disability
Sports competition, senior Olympics
Moderate physical work
Very light physical work
Light housekeeping
Cannot pass some or all BADL
Dependant in all BADLs
High risk and power sports
All endurance sports and games
Hobbies (walking and gardening)
Food preparation
Needs home or institutional care
Most hobbies Low physical demand activities
Grocery shopping
Can pass all IADL
Can pass some IADL, all BADLs
May be homebound
Behavioral indicators of instability
Definition of fall: At clinics: a fall is often defined as a
situation in which the older adult fall ground or is found lying on the ground. It is often defined as any unintended contact with a supporting surface, such as a chair, counter, or wall

Activity
Objective: To explore issues related to determining fall risk.
Procedure: Take a moment and ask yourself how many times you have fallen in the past 12 months. Think about and list the activities you were performing at the time you fell. What were the consequences of your falls? Were you injured? Since the fall, have y0ou been afraid or reluctant to return to those activities? Now, find an older adult living within the community or within a residential facility like an assisted living retirement center or skilled nursing facility. Ask this older adult the same set of questions. What is their fall rate? What activities were they performing when they fell? What was the environment like? Were they injured, and what was the psychological consequence of the fall? Were they more fearful and reluctant to return to their prior level of activity?
Risk factors for falls
11 Risk factors commonly associated with falls amongcommunity living older adults:
Muscle weakness History of falls Gait deficits Balance deficits Use of assistive device Visual deficits Arthritis Impaired ADL’s Depression Cognitive impairment Age (>80 years)
Falls continued
Environmental factors that increase fall risk:Presence of stairsThrow rugsSlippery surfacesPoor lighting
Falls continued
Falls are a great risk among hospitalised older adults and those
living in residential facilities. Many studies have examined risk
factors among hospitalised older adults and consistentlyIdentified the following factors: Gait instabilityLower extremity weaknessUrinary incontinence / frequency or need for assistance
in toileting. Impaired cognition – agitation, confusion, impaired
judgementHistory of fallsUse of certain medications, in particular centrally acting
sedatives
Risk factor assessment tools
Stratify Risk assessment tool for predicting falls inhospitalised elders1. Did the patient present to hospital with a fall, or has he or shefallen in the ward since admission? (Yes = 1, No = 0)2. Do you think the patient: (question 2-5)2.1 Is agitated? (yes = 1; no = 0)2.2 Is visually impaired to the extent that everyday function isaffected? (yes = 1; no = 0)2.3 Is in need of especially frequent toileting? (yes= 1; no=0)2.4 Has a transfer and mobility score* of 3 or 4(yes=1;no=0)
TOTAL SCORE (range 0-5) score ≥ 2 indicated increased risk for falls
* transfer score: 0 = unable; 1 = major help needed (one or two people, physical aids), 2 = minor help (verbal or physical), 3 = independent .
*mobility score: 0 = immobile, 1 = independent with aid/wheelchair, 2 = walks with help of one person, 3 = independent

Risk factors for fall continued
Older adults who fall after discharge have a significantly greater decline in independence in ADL and lower performance on balance and mobility measures.

Age related changes in the systems of postural control
Musculoskeletal SystemsMuscle strengthStrength or the amount of force a muscle produces,declines with age. Lower extremity muscle strengthcan be reduced by as much as 40% between the ages of30 and 80 years.Muscle strength reduction is more severe in oldernursing home residents with a history of falls – themean knee and ankle muscle strength was reducedtwofold and fourfold respectively, compared with thosewith no history of falls. Endurance – the capacity of the muscle to contract continuouslyat sub maximal levels also decreases with age. Endurance is betterpreserved with age than strength
Range of motionDecreased range of motion and loss of spinal
flexibilityin many older adults can lead to a
characteristicsflexed or stooped posture
ROM - continued
Spinal flexibility shows the greatest decline with age, compared with all other joints and spinal extension shows the greatest decline, with 50% less spinal mobility in 70 – 84 year olds compared with young adults of 20 – 29 years old.
Loss of spinal mobility can be associated with other changes in postural alignment, including a compensatory shift in the vertical displacement of center of body mass backward toward the heels.
Arthritis and other conditions can lead to decrease ROM in many joints throughout the body.
Pain may limit functional ROM
Neuromuscular system
The NMS contributes to postural control through the coordination of forces effective in controlling the body’s position in space.
Changes in quiet stance
Spontaneous swing during quiet stancePostural sway increases with each decade of
lifeGreatest increase in postural sway in older
adults with a history of falls.Velocity of sway greater in older adults with a
history of falls.Small decline in balance function in the older
adult.
Certain neurological disorders such as Parkinsons disease may have a normal or even a reduced swing in quiet stance due to increased stiffness and rigidity and this limits swing to smaller area during quiet stance.
Changes in motor strategies during perturbed stance
Is the older adult capable of activating muscle response synergies with appropriate timing, force and muscle response organisation when balance is threatened?
A study be Woolacott (1986) found that the motor strategies in younger adult and older adults were similar (ankle muscle and radiating to the muscles of the thigh).
The older adult group tended to co activate the antagonist muscles along with the agonist muscles at a given joint significantly more often than younger adults. Thus many of the elderly studied tended to stiffen the joints to a greater degree than younger adults when compensating for sway perturbations
Changes in motor strategies during perturbed stance
Several labs have found that many older adults used a strategy involving hip movements rather than ankle movements significantly more often than young adults (ankle muscle weakness? Loss of peripheral sensory function?)
This may increase falls, particularly those associated with slipping.
Changes in motor strategies during perturbed stance
In summary, both stable and unstable older adults show changes in the motor systems affecting postural control and that these can contribute significantly to an inability to maintain balance. Some of these changes include
- Muscle weakness- Impaired timing and organisation among
synergistic muscles activated in response to instability
- Limitations in the ability to adapt movements for balance in response to changing task and environment demands.
Anticipatory postural abilities
Postural adjustments are often used in a proactive manner, to stabilize the body before making a voluntary movement.
Many studies suggest that many older adults haave problems making anticipatory postural adjustments quickly and effectively, especially without prior practice.
This inability to stabilise the body in association with voluntary movement tasks such as lifting or carrying may be a major contributor to falls in many elderly.
Cognitive issues and postural control
The effect of fear of falling on the control of balance
There is now experimental evidence that anxiety and fear of falling affect the performance of older adults on tests of balance control.
