ajodo-2013_zhang_144_5_726
DESCRIPTION
articleTRANSCRIPT

CASE REPORT
Early orthodontic intervention followed by fixedappliance therapy in a patient with a severeClass III malocclusion and cleft lip and palate
He Zhang,a Feng Deng,b Huaqiao Wang,a Qianqian Huang,a and Yi Zhangc
Chongqing, China
FromDiseaChinaaStaffbProfecDirecAll auPotenAddreHospiCentetrict,Subm0889-Copyrhttp:/
726
This case report describes the treatment of a girl, age 11 years 10 months, with a cleft lip and palate and a post-surgical scar. The clinical examination showed a concave profile, a retrusivemaxilla, an asymmetric face, severedental crowding, a Class III dental relationship, and a complete dental crossbite. Maxillary expansion anddistraction, chincap, and high-pull headgear were used to moderate the skeletal discrepancy. These ap-proaches, combined with tooth extraction and fixed orthodontic appliances, finally established a functionaland esthetic occlusal relationship, normal overjet and overbite, and a well-balanced facial appearance. (Am JOrthod Dentofacial Orthop 2013;144:726-36)
Askeletal Class III malocclusion has beenacknowledged to be the most challengingproblem confronting orthodontists, especially
when it is associated with cleft lip and palate.1 Primarilybecause of the unpredictable and potentially abnormalgrowth in patients with this skeletal pattern, treatmentplanning for most young patients with Class III maloc-clusion has been directed at growth modification.2
Although early treatment of these patients commonlyachieves a relatively more normal jaw relationship,there have been few case reports of early interventionfor a Class III malocclusion in a patient with cleft lipand palate.3
Most patients with cleft lip and palate have alteredand deficient maxillary growth as a result of postsurgicalscar contraction or anatomic anomalies, and even mayhave dental arch deformities. Our aims of orthodontictreatment for these patients are to solve or moderate
the Affiliated Hospital of Stomatology, Chongqing Research Center for Oralses and Biomedical Science, Chongqing Medical University, Chongqing,.orthodontist.ssor and hospital director.tor, Department of Orthodontics.thors have completed and submitted the ICMJE Form for Disclosure oftial Conflicts of Interest, and none were reported.ss correspondence to: Yi Zhang, Department of Orthodontics, Affiliatedtal of Stomatology, Chongqing Medical University, Chongqing Researchr for Oral Diseases and Biomedical Science, 5 Shangqingsi Rd, Yuzhong Dis-Chongqing 400015, P. R. China; e-mail, [email protected], April 2012; revised and accepted, November 2012.5406/$36.00ight � 2013 by the American Association of Orthodontists./dx.doi.org/10.1016/j.ajodo.2012.11.028
these deformities and to establish an ideal maxilloman-dibular relationship.4 This case report describes thetreatment of a girl, age 11 years 10 months, with cleftlip and palate and a postsurgical scar, a Class III maloc-clusion, maxillary anterior crowding, and a completedental crossbite.
DIAGNOSIS AND ETIOLOGY
The girl and her parents came for orthodontic treat-ment with chief complaints of a crossbite and an unes-thetic smile. She had received surgery at the age of 4years and had no contraindication to orthodontic ther-apy. The pretreatment examination (Fig 1) and thedental casts (Fig 2) showed a concave profile (suggestingmaxillary retrusion) and an asymmetric face (suggestingmandibular deviation).
There was severe dental crowding (13 mm), and a leftdeciduous second molar remained in the maxilla; in themandible, the deciduous second molars remained onboth sides, with mild dental crowding. She had a ClassIII dental relationship on the left side and a Class I rela-tionship on the right, as well as a complete dental cross-bite. The maxillary midline deviated 3 mm to the rightfrom the facial midline, and the mandibular midlinewas shifted 1 mm to the left.
The cephalometric tracing (Fig 3) and analysis (Table)showed a vertical skeletal pattern (MP-FH, 34�; PFH,64.1�; AFH, 105.1�; FHI, 0.6) and a Class III skeletal rela-tionship with maxillary retrusion (SNA, 81.2�; SNB, 84.1�;ANB, �2.9�). The mandibular incisors were retroclined(IMPA, 77.5�; 1.NB, 20�; 1-NB, 3.8 mm). The concave

Fig 1. Pretreatment photographs.
Fig 2. Pretreatment dental casts.
Zhang et al 727
American Journal of Orthodontics and Dentofacial Orthopedics November 2013 � Vol 144 � Issue 5
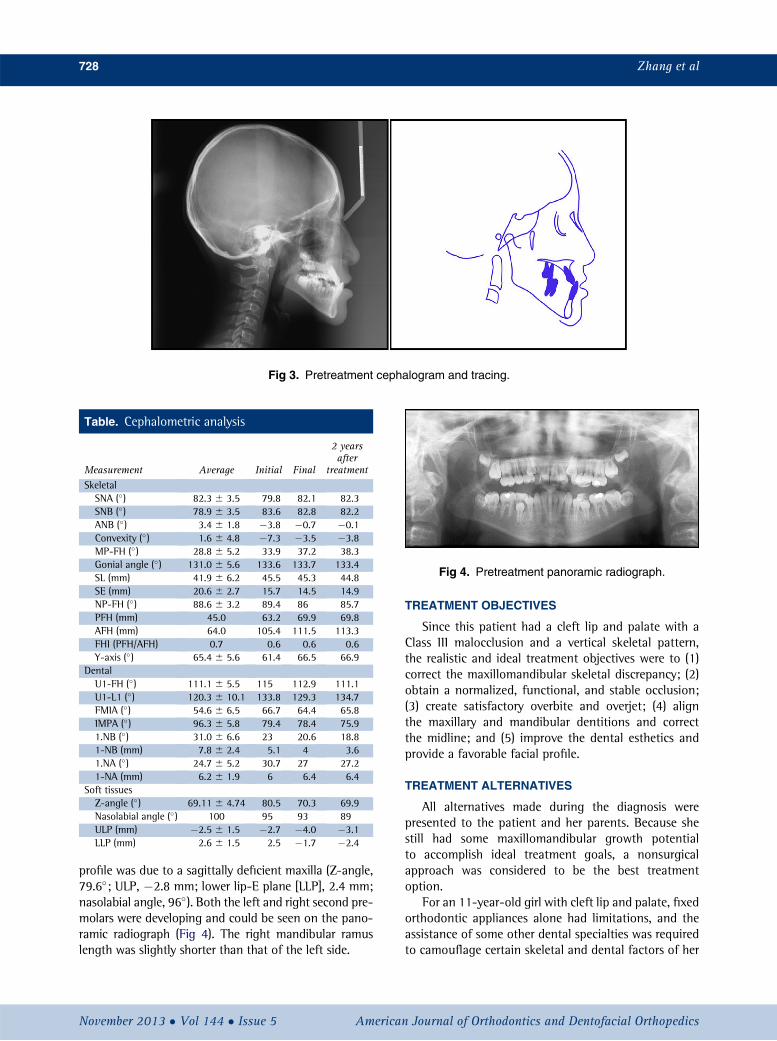
Fig 3. Pretreatment cephalogram and tracing.
Table. Cephalometric analysis
Measurement Average Initial Final
2 yearsafter
treatmentSkeletalSNA (�) 82.3 6 3.5 79.8 82.1 82.3SNB (�) 78.9 6 3.5 83.6 82.8 82.2ANB (�) 3.4 6 1.8 �3.8 �0.7 �0.1Convexity (�) 1.6 6 4.8 �7.3 �3.5 �3.8MP-FH (�) 28.8 6 5.2 33.9 37.2 38.3Gonial angle (�) 131.0 6 5.6 133.6 133.7 133.4SL (mm) 41.9 6 6.2 45.5 45.3 44.8SE (mm) 20.6 6 2.7 15.7 14.5 14.9NP-FH (�) 88.6 6 3.2 89.4 86 85.7PFH (mm) 45.0 63.2 69.9 69.8AFH (mm) 64.0 105.4 111.5 113.3FHI (PFH/AFH) 0.7 0.6 0.6 0.6Y-axis (�) 65.4 6 5.6 61.4 66.5 66.9
DentalU1-FH (�) 111.1 6 5.5 115 112.9 111.1U1-L1 (�) 120.3 6 10.1 133.8 129.3 134.7FMIA (�) 54.6 6 6.5 66.7 64.4 65.8IMPA (�) 96.3 6 5.8 79.4 78.4 75.91.NB (�) 31.0 6 6.6 23 20.6 18.81-NB (mm) 7.8 6 2.4 5.1 4 3.61.NA (�) 24.7 6 5.2 30.7 27 27.21-NA (mm) 6.2 6 1.9 6 6.4 6.4
Soft tissuesZ-angle (�) 69.11 6 4.74 80.5 70.3 69.9Nasolabial angle (�) 100 95 93 89ULP (mm) �2.5 6 1.5 �2.7 �4.0 �3.1LLP (mm) 2.6 6 1.5 2.5 �1.7 �2.4
Fig 4. Pretreatment panoramic radiograph.
728 Zhang et al
profile was due to a sagittally deficient maxilla (Z-angle,79.6�; ULP, �2.8 mm; lower lip-E plane [LLP], 2.4 mm;nasolabial angle, 96�). Both the left and right second pre-molars were developing and could be seen on the pano-ramic radiograph (Fig 4). The right mandibular ramuslength was slightly shorter than that of the left side.
November 2013 � Vol 144 � Issue 5 American
TREATMENT OBJECTIVES
Since this patient had a cleft lip and palate with aClass III malocclusion and a vertical skeletal pattern,the realistic and ideal treatment objectives were to (1)correct the maxillomandibular skeletal discrepancy; (2)obtain a normalized, functional, and stable occlusion;(3) create satisfactory overbite and overjet; (4) alignthe maxillary and mandibular dentitions and correctthe midline; and (5) improve the dental esthetics andprovide a favorable facial profile.
TREATMENT ALTERNATIVES
All alternatives made during the diagnosis werepresented to the patient and her parents. Because shestill had some maxillomandibular growth potentialto accomplish ideal treatment goals, a nonsurgicalapproach was considered to be the best treatmentoption.
For an 11-year-old girl with cleft lip and palate, fixedorthodontic appliances alone had limitations, and theassistance of some other dental specialties was requiredto camouflage certain skeletal and dental factors of her
Journal of Orthodontics and Dentofacial Orthopedics

Fig 5. Treatment progress: A, maxillary expansion, with a jackscrew expansion appliance;B, construction used for protraction; C, 5 months after maxillary expansion and protraction.
Zhang et al 729
malocclusion and to help improve esthetics and func-tion. The options considered included (1) maxillary andmandibular first premolar extractions, compensationmechanics, and further occlusal adjustment with ClassIII elastics; (2) rapid maxillary expansion and distractionas well as a high-pull chincap to moderate or correct theClass III skeletal relationship, with extraction of themaxillary and mandibular first premolars to correct thecrowding, overjet, and anterior crossbite; and (3) com-bined therapy of orthodontic-orthognathic surgery aftershe reached 18 years old.
TREATMENT PROGRESS
Treatment began with maxillary expansion using ajackscrew expansion appliance soldered to 2 bandedteeth per side (Fig 5, A). The appliance was activatedat a rate of 0.5 mm per day for 15 days, until the poste-rior crossbite had been moderated.
The facemask and the construction used for protrac-tion were connected with anterior hooks in the canineregion for elastics (Fig 5, B). A 400-g to 500-g protrac-tion force was transferred to the hooks per side, with theelastics adjusted to provide a forward and downward
American Journal of Orthodontics and Dentofacial Orthoped
pull at 30� to the occlusal plane to minimize the sideeffect of counterclockwise rotation. The patient worethe facemask for at least 12 hours a day, and it wasstarted after 4 weeks of maxillary expansion. The ante-rior crossbite was corrected 3 months later (Fig 5, C).The transverse expansion and protraction of the maxillawas maintained for 5 months to limit the relapse causedby the scar contraction and the increased muscletension.
A chincap and high-pull headgear were used to limitthe excessive mandibular anterior facial height, and Tip-Edge brackets (TP Orthodontics, La Porte, Ind) werebonded to the teeth (Fig 6). With sequential nickel-titanium archwires, dental alignment and leveling wereobserved in 3 months. We placed an 0.018 3 0.025-instainless steel wire and an Australian wire, respectively,in the maxillary and mandibular dental arches. Thennickel-titanium coil springs (Fig 7, A) and Class III elas-tics (Fig 7, B) were used for space adjustment and distalmovement of the mandibular dental arch.
Then the Tip-Edge brackets were replaced by pread-justed 0.022-in brackets (MBT; 3M Unitek, Monrovia,Calif). Australian wire and 0.183 0.025-in stainless steelarchwires were used to align the teeth more precisely. At
ics November 2013 � Vol 144 � Issue 5

Fig 6. Combination of high-pull chincap and Tip-Edge brackets.
Fig 7. Treatment progress: A, nickel-titanium coil springs for space adjustment;B,Class III elastics formandibular dental retrusion; C, Tip-Edge brackets replaced by MBT brackets and mini-implant formidline correction.
730 Zhang et al
November 2013 � Vol 144 � Issue 5 American Journal of Orthodontics and Dentofacial Orthopedics

Zhang et al 731
the third stage, to correct the maxillary midline, a mini-implant (1.6 3 9 mm; Medicon, Tuttlingen, Germany)was placed between the roots of the maxillary rightlateral incisor and canine, 3 mm occlusally to the vestib-ular groove (Fig 7, C). The treatment lasted 3 years 2months. It took over 12 months to establish Class I molarrelationships, including maxillary expansion, protrac-tion, and tooth movement, and 6 months to correctthe midline.
TREATMENT RESULTS
The posttreatment facial photographs (Fig 8) anddental casts (Fig 9) indicated a noteworthy improvementin the lower facial profile from the pronounced retrac-tion of the mandibular anterior teeth. The lower lipmoved backward, shown by LLP, resulting in an opti-mized lip relationship. Because of the better mandibularincisor and lower lip positions, the soft-tissue profilebecame more convex, the Z-angle decreased signifi-cantly, and the nasolabial angle also decreased slightly.Meanwhile, the crossbite had been corrected, and ClassI canine and molar relationships were achieved withnormal overbite and overjet.
The lateral cephalometric tracing and analysis (Fig10, Table) were consistent with the clinical results. Verti-cally, lower facial height increased as shown by MP-FH,PFH, and AFH, yet the facial height ratio was main-tained. Sagittally, the skeletal discrepancy between themaxilla and the mandible was remarkably moderated,as confirmed by the SNA, SNB, and ANB angles. Themandible tilted down and backward because of the pres-sure exerted on the chin. Although the treatment for thispatient was a compromise, satisfactory results were ob-tained. In addition, her facial convexity was significantlyimproved as shown by NP-FH and y-axis. The mandib-ular incisors moved backward to a more acceptableposition as shown by 1.NB, 1-NB, FMIA, IMPA, andthe interincisal angle. The maxillary incisors were alsoretruded as shown by U1-FH and 1-NA.
The soft-tissue profile changes between pretreatmentand posttreatment, as well as the skeletal profileimprovement and tooth movement, were clearly evidenton the superimposition of the cephalometric tracings(Fig 11). It also shows that no change was observed inthe position of the condyle relative to basion and the go-nial angle; this was confirmed by the cephalometric anal-ysis. The level of interradicular bone was relatively stableafter treatment as seen on the panoramic radiograph (Fig12). There is a bony apophysis appearing obviously alongthe lower border of the mandible, close to the chin.
The treatment plan was a satisfactory nonsurgicalalternative, and a functional and esthetic occlusal
American Journal of Orthodontics and Dentofacial Orthoped
relationship was established. The more favorablemandibular incisor inclination resulted in normal overjetand overbite, and a well-balanced facial appearance wasachieved. Correction of the malocclusion and improve-ment of her facial profile were accomplished with bothdentoalveolar and skeletal changes.
After 2 years of retention, the posttreatment occlu-sion and anterior overjet continued to be stable (Fig13). The skeletal (Fig 14) and soft-tissue (Fig 15) facialprofile were also satisfactory, and there was no signifi-cant change shown on the panoramic radiograph(Fig 16).
DISCUSSION
Midface retrusion and malocclusion are concerns forpatients with operated cleft lip and palate. Because ofthe possible influence of cleft severity on the growthof the maxilla, cleft lip and palate patients can have arelatively retruded maxillary position with a tendencyfor a Class III malocclusion, even after palatoplasty.1,5,6
The tension of the scar contraction resulting from thepalatal repair could adversely affect maxillary growth.Most cleft lip and palate patients require a LeFort Iosteotomy after completion of skeletal growth toreposition the maxilla. This type of surgery might alsorequire rigid fixation, bone grafting, and mandibularsetback.6,7 However, these treatments are quite invasive.
Maxillary expansion and distraction osteogenesis areconsidered an attractive alternative to correct the maloc-clusion in cleft lip and palate patients,6,8,9 although achincap and high-pull headgear have also been advo-cated in the treatment of Class III malocclusion.10 Labialtipping of the maxillary incisors could not be avoidedbecause the maxillary anterior teeth were used as an an-chor for the distraction forces. Because of the first pre-molar extraction, proclination of the maxillary anteriorteeth had been slightly decreased. The pronouncedimprovement of the patient’s facial profile and occlusalrelationship suggested that orthognathic surgery wasunnecessary for correcting her skeletal discrepancies. Inaddition, because of her unesthetic facial appearanceand unattractive smile, the patient and her parents didnot want to wait another 10 years to have surgical treat-ment. Also, the malocclusion could have become worsewith time if it were not corrected. Therefore, orthog-nathic surgery was finally abandoned after carefulconsideration.
The esthetic improvement obtained in this cleft lipand palate patient was impressive as a result of favorablemaxillary advancement and mandibular incisor retru-sion, which were achieved by maxillary protraction,mandibular growth inhibition, and premolar extraction.
ics November 2013 � Vol 144 � Issue 5

Fig 8. Posttreatment photographs.
Fig 9. Posttreatment dental casts.
732 Zhang et al
November 2013 � Vol 144 � Issue 5 American Journal of Orthodontics and Dentofacial Orthopedics

Fig 10. Posttreatment cephalogram and tracing.
Fig 11. Superimposed tracings. Blue lines, pretreatmenttracing; red lines, posttreatment tracing.
Fig 12. Posttreatment panoramic radiograph.
Zhang et al 733
Early intervention by protracting the maxilla was inten-tionally controlled. One side effect of facemask protrac-tion is unexpected proclination of the maxillary anteriorteeth; this would cause undesirable profile changes(concave facial profile with maxillary incisor proclina-tion). Hence, premolar extraction was necessary tokeep her maxillary incisors upright. Although most ClassIII patients have retroclined anterior mandibular teeth,retraction of the mandibular incisors still helps to deepenthe labiomental fold, which is flat in most Class III pa-tients. This further contributes to the improvement ofthe facial profile. Our results are similar to those of Lin
American Journal of Orthodontics and Dentofacial Orthoped
and Gu,11 who suggested that by treating Class IIIpatients with compensatory mechanics, remarkablesoft-tissue changes can be observed when the facial pro-file changes from concave to straight.12 However, otherfactors such as the patient’s age, skeletal growth pattern,individual growth potential, and cooperation are alsoimportant in producing the entire treatment effect.13
The age of the skull is an essential element that af-fects the mechanical property of the skeletal suture.14,15
So, timing is crucial to achieve successful orthodontictreatment. Beginning treatment at the correct time ina patient with growth potential has a significantinfluence on correcting the discrepancy in the sagittal,vertical, and transverse planes. It is recommended thattreatment directed at promoting or inhibiting maxillaryor mandibular growth should be performed before thepubertal growth spurt.16 Normally, midface growth upto the age of 7 years is attributed to the increasing sizeof the anterior cranial base, orbits, and nasal septum.All facial bones move forward and downward fromgrowth of the synchondroses.17 However, normal
ics November 2013 � Vol 144 � Issue 5

Fig 13. Photographs 2 years after treatment.
Fig 14. Cephalogram and tracing 2 years after treatment.
734 Zhang et al
forward and downward growth was not expectedbecause of the underdeveloped maxilla, especially inthis patient with cleft lip and palate. Consequently,
November 2013 � Vol 144 � Issue 5 American
expansion and protraction therapy was considered forher. But the space provided by the rapid maxillary expan-sion was not enough to correct the dental crowding;
Journal of Orthodontics and Dentofacial Orthopedics

Fig 15. Superimposed tracings of posttreatment and 2years after treatment. Red lines, posttreatment tracing;black lines, 2 years posttreatment tracing.
Fig 16. Panoramic radiograph 2 years after treatment.
Zhang et al 735
therefore, tooth extraction was a reasonable solution.Luckily, the patient’s cleft deformity was not unilateral.Thus, the risk of a nonaverage distribution of heavy or-thodontic force caused by the asymmetric structure ofthe skull was greatly reduced.14
Chincap, high-pull headgear, and maxillary protrac-tion appliances have been reported to achieve favorablechanges in patients with Class III malocclusion.13,18 Yetwhether it is possible to alter the congenital growthpattern significantly and permanently requires furtherinvestigation.13 Interestingly, the apophysis along thelower border of the mandible shown in the posttreamentprofile was not found on the cephalometric tracingbefore the chincap was applied. The effects of the chin-cap were more concentrated on backward repositioningof the mandible, the direction and inhibition of mandib-ular growth, and the stress distributions on thecondyle.19 Remodeling of the mandibular shape and
American Journal of Orthodontics and Dentofacial Orthoped
morphologic changes have been rarely reported.Although similar bone apophysis might also be observedin other clinical cases in which the chincap was used,further study related to its mechanical properties shouldbe conducted.
The posttreatment results show good stability aftermore than 2 years. The prevention of posterior and ante-rior crossbite by maxillary expansion and distraction,and the long-term chin growth inhibition with the chin-cup seemed to contribute to this stability.
CONCLUSIONS
A definitive analysis and treatment plan should bemade for each patient. In those with cleft lip and palatewho are undergoing a growth spurt, orthodontic treat-ment objectives should be restoratively realistic,economical, and low risk. In this case report, the final oc-clusion was esthetic, functional, healthy, and stable. Theearly orthodontic intervention combined with the sec-ond phase of treatment (fixed orthodontic appliances)efficiently achieved a satisfactory result, and the patientbenefited by gaining self-esteem and improvedesthetics.
REFERENCES
1. Burns NR, Musich DR, Martin C, Razmus T, Gunel E, Ngan P. ClassIII camouflage treatment: what are the limits? Am J Orthod Den-tofacial Orthop 2010;137:9.e1-9.e13; discussion, 9-11.
2. Singh GD, Rivera-Robles J, de Jesus-Vinas J. Longitudinal cranio-facial growth patterns in patients with orofacial clefts: geometricmorphometrics. Cleft Palate Craniofac J 2004;41:136-43.
3. Macdonald KE, Kapust AJ, Turley PK. Cephalometric changes afterthe correction of class III malocclusion with maxillary expansion/facemask therapy. Am J Orthod Dentofacial Orthop 1999;116:13-24.
4. Aikawa T, Haraguchi S, Tanaka S, Uematsu S, Ishibashi M,Kogo M, et al. Rotational movement of the anterior maxillarysegment by hybrid distractor in patients with cleft lip and palate.Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2010;110:292-300.
5. Chiu YT, Liao YF, Chen PK. Initial cleft severity and maxillarygrowth in patients with complete unilateral cleft lip and palate.Am J Orthod Dentofacial Orthop 2011;140:189-95.
6. Swennen G, Colle F, De May A, Malevez C. Maxillary distraction incleft lip palate patients: a review of six cases. J Craniofac Surg1999;10:117-22.
7. Epker BN, Stella JP, Fish LC. Dentofacial deformities associatedwithcleft lip andpalate. In: Epker BN, editor. Dentofacial deformities: in-tegrated orthodontic and surgical correction. St Louis: Mosby;1995.
8. Trindade IE, Castilho RL, Sampaio-Teixeira AC, Trindade-Suedam IK, Silva-Filho OG. Effects of orthopedic rapid maxillaryexpansion on internal nasal dimensions in children with cleft lipand palate assessed by acoustic rhinometry. J Craniofac Surg2010;21:306-11.
9. Zemann W, Pichelmayer M. Maxillary segmental distraction inchildren with unilateral clefts of lip, palate, and alveolus. Oral
ics November 2013 � Vol 144 � Issue 5

736 Zhang et al
Surg Oral Med Oral Pathol Oral Radiol Endod 2011;111:688-92.
10. Gautam P, Valiathan A, Adhikari R. Stress and displacement pat-terns in the craniofacial skeleton with rapid maxillary expansion:a finite element method study. Am J Orthod Dentofacial Orthop2007;132:5.e1-5.e11.
11. Lin J, Gu Y. Preliminary investigation of nonsurgical treatment ofsevere skeletal Class III malocclusion in the permanent dentition.Angle Orthod 2003;73:401-10.
12. Maruo H, Maruo IT, Saga AY, Camargo ES, Guariza Filho O,Tanaka OM. Orthodontic-prosthetic treatment of an adult with asevere Class III malocclusion. Am J Orthod Dentofacial Orthop2010;138:820-8.
13. Shanker S, Ngan P, Wade D, Beck M, Yu C, H€agg U, et al. Cephalo-metric A point changes during and after maxillary protraction andexpansion. Am J Orthod Dentofacial Orthop 1996;110:423-30.
14. Wang D, Cheng L, Wang C, Qian Y, Pan X. Biomechanical analysisof rapid maxillary expansion in the UCLP patient. Med Eng Phys2009;31:409-17.
November 2013 � Vol 144 � Issue 5 American
15. Henderson JH, Longaker MT, Carter DR. Sutural bone depositionrate and strain magnitude during cranial development. Bone2004;34:271-80.
16. Franchi L, Baccetti T, De Toffol L, Polimeni A, Cozza P. Phases of thedentition for the assessment of skeletal maturity: a diagnostic perfor-mance study. Am J Orthod Dentofacial Orthop 2008;133:395-400.
17. Sade Hoefert C, Bacher M, Herberts T, Kimmel M, Reinert S, Goz G.3D soft tissue changes in facial morphology in patients with cleftlip and palate and class III malocclusion under therapy with rapidmaxillary expansion and delaire facemask. J Orofac Orthop 2010;71:136-51.
18. Liu ZP, Li CJ, Hu HK, Chen JW, Li F, Zou SJ. Efficacy of short-termchincup therapy for mandibular growth retardation in Class IIImalocclusion. Angle Orthod 2011;81:162-8.
19. Tanne K, Tanaka E, Sakuda M. Stress distribution in the temporo-mandibular joint produced by orthopedic chincup forces applied invarying directions: a three-dimensional analytic approach with thefinite elementmethod. Am J Orthod Dentofacial Orthop 1996;110:502-7.
Journal of Orthodontics and Dentofacial Orthopedics