alarms that deserve attention - amazon...
TRANSCRIPT

Alarms That Deserve AttentionMike Rayo3/29/2016

Tackling “Alarm Fatigue”
… With Sound Design
… With Policy
… By Sharpening
… With Multimodal Design
What I’ll becovering
2

3
Alarm fatigue is …
Too many alarms
Startle effect of alarms
Alarms are too loud
Patients can’t sleep
Can’t hear alarms
False alarms
Non-actionable alarms
Nuisance alarms
Annoying alarms
Can’t remember what alarm is for
Can’t discriminate alarms
Can’t identify alarm
Worn out by alarms
Desensitized
OverwhelmedTired

Alarm fatigue – words matterResearchers looked for alarm-induced fatigueResearchers FOUNDalarm-reduced fatigueHealthcare Informatics Research journal published findings
BUTOnly used 7 of the 77 questionsUnclear whether results are due to fatigue mechanism or something else
4
Cho et. al., 2016

So, what is the problem?Sensory discriminabilityCan I hear the alarms? Can I identify what events they are meant to signify?InformativenessHow often, historically, have the alarms (1) correctly identified a (2) hazardous eventAttentionDoes the clinician have sufficient attentional resources required to respond to the alarms?ResponseDoes the alarming system give the clinician sufficient information to respond appropriately to the event?
5

Addressing the alarm problem by making phone-based alerts discriminable and
identifiable
6
Cisco / connexall tones: current state
One tone associated with all eventsTelemetry low battery, Patient call, Asystole
Alerts often routed to multiple phones45% only go to primary phone35% go to a second phone20% go to second and third phone
7

Questions for intervention
How many tones should we have?Fewer: easier to rememberMore: less ambiguous what tone is signifyingAnswer: few tone families, variations within family
What should they be?Same – already learned them (or have we?), and we already have themDifferent – ability to improve them, but have to design them!
How do we improve when and how alerts are routed from phone to phone?How will we get the answers to these questions?
8

Quick-cycling for learning
9
Discovery
Analysis
DesignDevelopment
Implementation

Quickening the learning cycle
10
Large Implementation
Cycle length
Years
Months
Small Pilot
Weeks
“Research”Study
Heuristics
Days
Multiple tones project setup
Tone designResearch literature on memorability and encoding urgencyPast experience with emotional aspect of sounds and what they mean
Iterate!Learning experiment – 2 weeks, current against new setIterate!Pilot – comparing 2 units with new tones, escalation paths to “sister” units for 3 months (Ross 7 and James 18 new tones, Ross 5 and 7 stayed the same)Iterate!Implement! – Starting late March
11

Iterations of Cardiac Crisis
12
Initial Designs Sketches
Variations on Theme:CAR-DI-O-VAS-CU-LAR
After Learning Experiment

Iteration of Code Blue
13
Initial Designs
After Pilot
Then roughly 10 more sounds combined with 10 different human and synthetic voices
Learning Experiment
Pilot

Resultant tones
14
Cardiac CrisisAsystole, Vfib, Vtac)
Cardiac Other
Nurse Call
Technical High(Leads off, bed exit)
Technical Low(Low battery)
Code Blue Staff Assist

Listening experiment results - urgency
15

Listening experiment results -identification
16
*
*
*
*
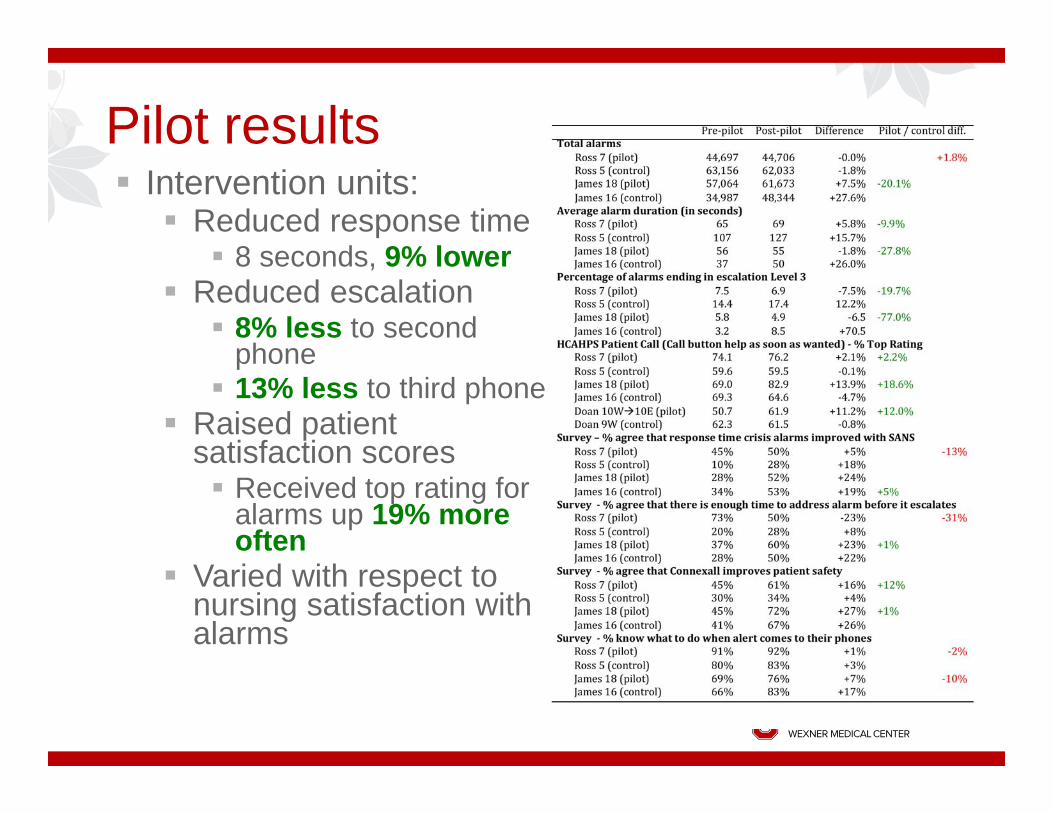
Pilot results Intervention units:
Reduced response time8 seconds, 9% lower
Reduced escalation8% less to second phone13% less to third phone
Raised patient satisfaction scores
Received top rating for alarms up 19% more often
Varied with respect to nursing satisfaction with alarms
Addressing the alarm problem by decreasing false and non-
actionable alarms
18

Cognitive Underpinnings of Alarm Problem
In high-tempo workplaces, many tasks and signals (e.g., alarms) compete for attention.Over time, clinicians determine (consciously and subconsciously) the informativeness of each of these signals.Informativeness is the likelihood that a signal is signifying what it is meant to signify (i.e., not false), and that what is signified is worthy of directing attention to (i.e., actionable).
Non-actionable Alarm: Correctly identified by the system, but it has no clinical significance and/or results in no change in plan of care—Asymptomatic Bradycardia)
False Alarm: A triggered event that is invalid or incorrect—Artifact; Asystole for a paced rhythm.
19

Informativeness
Informativeness drops quickly when:There are a lot of false alarmsThere are a lot of non-actionable alarmsGroup alarms
1 signal meant to alarm for multiple different reasons1 signal meant to alarm for multiple different urgencies
Drops in signal informativeness result in:Proportional reduction in clinician response (i.e., 80% false alarms predicts 20% clinician response)Lack of response examples include ignoring, overriding, and disabling alarms (turn off, lower volume)
NOTE: these responses are not due to a lack of vigilance or effort – similar responses have been seen in animals, machines, and proven mathematically
20

Performance with varying D’, resources
n=5 n=15
Addressing the alarm problem by decreasing false and non-
actionable alarms
… with Policy Changes
22

Policy: Low-risk patients off monitoring

Findings: Less Monitoring, False Alarms
MeasureFalse Alarm Rate
Fewer False AlarmsBefore After p Value18.8% 9.6% <0.001

Findings: Freed up Resources

Addressing the alarm problem by decreasing false and non-
actionable alarms
… With Configuration Changes
26

SpO2 Alarms: Pre & Post System Changes
33% actual reduction in Pulse Oximetry alerts in the Medical
Center
Another ~52,000 alarms triggered for SpO2 of 88%.
Future total reduction in Pulse Oximetry alerts in the Medical
Center will be ~61%!!!!

Reality check: Are we there yet?
SpO2 alarms default setting: less than 88% [2015]Results in heart hospital
3,400 alarms/day1.24M alarms/year
No, not there yet!


Addressing the alarm problem by decreasing false and non-
actionable alarms
… With Technology Design
30

Next steps: directly targeting informativeness!
Using heuristics, experiments, and pilots to improve alarm algorithms
Less false and non-actionable alarmsIdentifying hazardous events betterRouting to additional clinicians only when needed
Designing visual displays when sensor algorithms cannot get to high enough positive predictive value
31

Questions?
32

33