alessandra fabi brain metastases: current and future options brain metastases: current and future...
TRANSCRIPT

Alessandra FabiAlessandra Fabi
Brain Metastases: current and future options
Brain Metastases: current and future options
Roma, 16 Novembre 2006Roma, 16 Novembre 2006


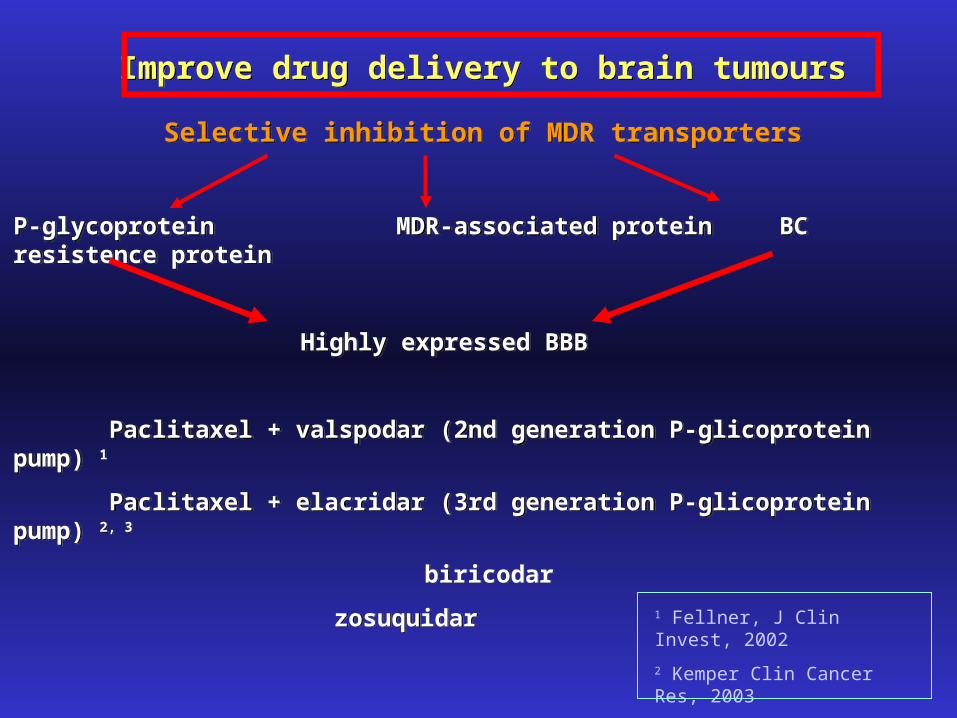
Improve drug delivery to brain tumoursImprove drug delivery to brain tumours
Selective inhibition of MDR transporters
P-glycoprotein MDR-associated protein BC resistence protein
Highly expressed BBB
Paclitaxel + valspodar (2nd generation P-glicoprotein pump) 1
Paclitaxel + elacridar (3rd generation P-glicoprotein pump) 2, 3
biricodar
zosuquidar
Selective inhibition of MDR transporters
P-glycoprotein MDR-associated protein BC resistence protein
Highly expressed BBB
Paclitaxel + valspodar (2nd generation P-glicoprotein pump) 1
Paclitaxel + elacridar (3rd generation P-glicoprotein pump) 2, 3
biricodar
zosuquidar
1 Fellner, J Clin Invest, 2002
2 Kemper Clin Cancer Res, 2003
3 Robert, J Med Chem, 2003

Primary tumors with a frequent brain diffusion and
chemosensitiveGERM-CELL TUMOURS
PEB regimen (Heinorm)
SCLC
PE regimen (Italian Oncology Group)
BREAST CANCER
(CMF, PE, Taxane-including regimen)
Can BBB not to be a cause of chemoresistence but the biological characteristics of primary tumour ?

Incidence
10 -16 % (30% autopsies)
prevalent site: supratentorial
2-5 % leptomeningeal metastases
2% metastasis sincron at diagnosis
median PFS 34 months
Incidence
10 -16 % (30% autopsies)
prevalent site: supratentorial
2-5 % leptomeningeal metastases
2% metastasis sincron at diagnosis
median PFS 34 months
Breast cancer and brain metastasesBreast cancer and brain metastases

Risk Factors
Age (Tsukada 2003)
Hormonal Receptors (Samaan 1984)
ER - vs ER+ : 10% vs 4%
Overespression HER2 and Trastuzumab (Kallionemi 1991,
Burstain 2003)
- predictor of site of first relapse : 4.3% vs 0.4%
- increase incidence of BM in HER2 + T treated pts
- higher incidence in trastuzumab (28-43%)
Adjuvant chemiotherapy vs no treatment (Carey BCRT
2001)
50% vs 26% (p=0.012)
Risk Factors
Age (Tsukada 2003)
Hormonal Receptors (Samaan 1984)
ER - vs ER+ : 10% vs 4%
Overespression HER2 and Trastuzumab (Kallionemi 1991,
Burstain 2003)
- predictor of site of first relapse : 4.3% vs 0.4%
- increase incidence of BM in HER2 + T treated pts
- higher incidence in trastuzumab (28-43%)
Adjuvant chemiotherapy vs no treatment (Carey BCRT
2001)
50% vs 26% (p=0.012)
Breast cancer and brain metastasesBreast cancer and brain metastases

Prognostic FactorsPrognostic Factors724 pz724 pz
3-yrs S: 27% vs 44%5-yrs S: 11% vs 28%3-yrs S: 27% vs 44%5-yrs S: 11% vs 28%
HR+ HR-
3-yrs S: 33% vs 60%5-yrs S: 14% vs 38%
3-yrs S: 14% vs16%5-yrs S: 4% vs 8%
Andre et al.
JCO 2004
Andre et al.
JCO 2004
Median Survival ’87-’93/ ’94-’00= 28 mos vs 45 mos
Median Survival ’87-’93/ ’94-’00= 28 mos vs 45 mos

SURGERY
RADIOTHERAPY (WBRT, RS)
CHEMOTHERAPY
SURGERY
RADIOTHERAPY (WBRT, RS)
CHEMOTHERAPY

SURGERYSURGERY
Patchell ’90 48 pts (10% breast primary)
Surgery alone vs Surgery ->WBRT
functional independence 8 vs 38 weeks
Recurrence 18% vs 70%
Survival 15 vs 40 weeks
Noordijk ’94 63 pts (19% breast primary)
Surgery alone vs Surgery ->WBRT
Survival 18 vs 36 weeks
Benefit of combined therapy seen only in pts with stable or absent extracranial disease
Mintz ‘96
Surgery alone vs Surgery ->WBRT
Survival no difference
Patchell ’90 48 pts (10% breast primary)
Surgery alone vs Surgery ->WBRT
functional independence 8 vs 38 weeks
Recurrence 18% vs 70%
Survival 15 vs 40 weeks
Noordijk ’94 63 pts (19% breast primary)
Surgery alone vs Surgery ->WBRT
Survival 18 vs 36 weeks
Benefit of combined therapy seen only in pts with stable or absent extracranial disease
Mintz ‘96
Surgery alone vs Surgery ->WBRT
Survival no difference
Surgical resection should be considered seriously in pts with single metastases
and stable or absent extracranial disease
Surgical resection should be considered seriously in pts with single metastases
and stable or absent extracranial disease

Stereotactic RadiosurgeryStereotactic Radiosurgery
Single metastases
Median Survival after brain diagnosis 15-18 months
Median Survival after SRS 7-13 months
Retrospective analysis (SRS vs Surgery) (15% breast primary)
Conflicting results for single metastases
RTOG 95-08 ’02 333 pts (1-3 metastases)
SRS + WBRT vs WBRT alone
Survival no difference
Improvement KPS 43% vs 27% (p=0.03)
Local tumor control (1 yr) 82% vs 71% (p=0.01)
Single metastases
Median Survival after brain diagnosis 15-18 months
Median Survival after SRS 7-13 months
Retrospective analysis (SRS vs Surgery) (15% breast primary)
Conflicting results for single metastases
RTOG 95-08 ’02 333 pts (1-3 metastases)
SRS + WBRT vs WBRT alone
Survival no difference
Improvement KPS 43% vs 27% (p=0.03)
Local tumor control (1 yr) 82% vs 71% (p=0.01)
In most cases seem resonable to limit SRS to
with 1 to 3 brain metastases and who have controlled extracranial disease and
adequate performance status
In most cases seem resonable to limit SRS to
with 1 to 3 brain metastases and who have controlled extracranial disease and
adequate performance status

Therapeutical Possibility
Chemotherapy alone
Chemotherapy concurrently with WBRT
Radiosensitizing Agents
Target Therapy
Chemotherapy alone
Chemotherapy concurrently with WBRT
Radiosensitizing Agents
Target Therapy
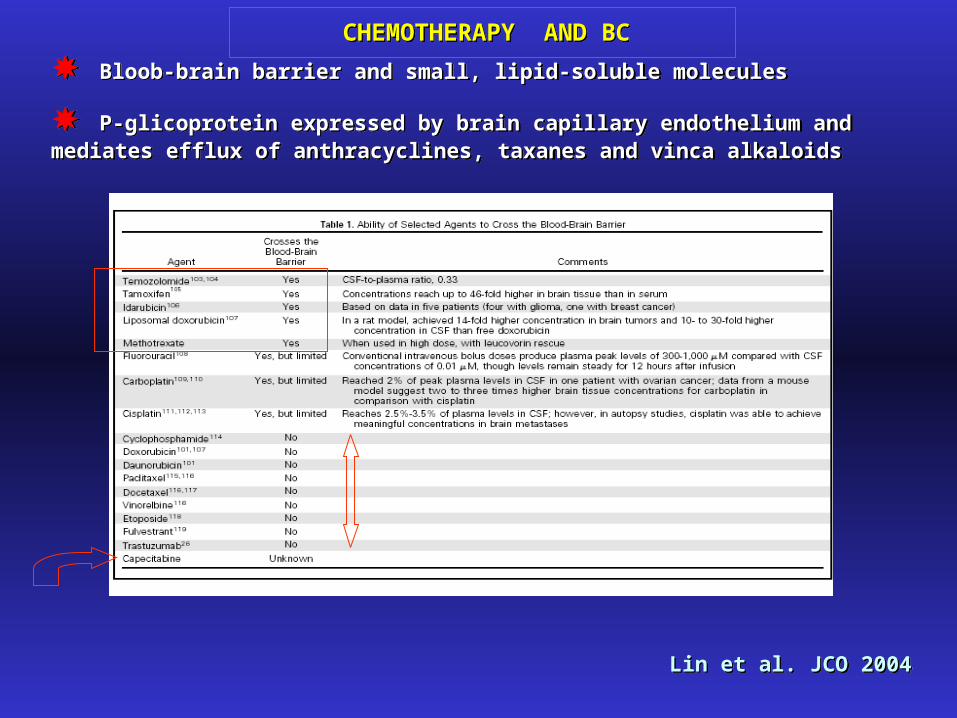
CHEMOTHERAPY AND BCCHEMOTHERAPY AND BC
Bloob-brain barrier and small, lipid-soluble molecules
P-glicoprotein expressed by brain capillary endothelium and mediates efflux of anthracyclines, taxanes and vinca alkaloids
Bloob-brain barrier and small, lipid-soluble molecules
P-glicoprotein expressed by brain capillary endothelium and mediates efflux of anthracyclines, taxanes and vinca alkaloids
Lin et al. JCO 2004Lin et al. JCO 2004

Capecitabine, breast cancer and brain metastases response
Fabi et al., Anticancer Research 2006

Rosner et al.
100 pts ( Rr 50% - median duration 7 months)
Boogerd et al
22 pts (Rr 59%)
Rosner et al.
100 pts ( Rr 50% - median duration 7 months)
Boogerd et al
22 pts (Rr 59%)
WBRT +/-TMZ
Rr 96% vs 67% (p=0.017)
WBRT +/-TMZ
Rr 96% vs 67% (p=0.017)
Durable remission in leptomenigeal metastasesDurable remission in leptomenigeal metastases
Rr 38% - 55%
CHEMOTHERAPY, BREAST CANCER AND BRAIN METASTASES

Chemotherapy alone and activity on BM Chemotherapy alone and activity on BM
Langer et Metha, JCO 2005Langer et Metha, JCO 2005

Chemotherapy concurrently with WBRT
Langer et Metha, JCO 2005Langer et Metha, JCO 2005
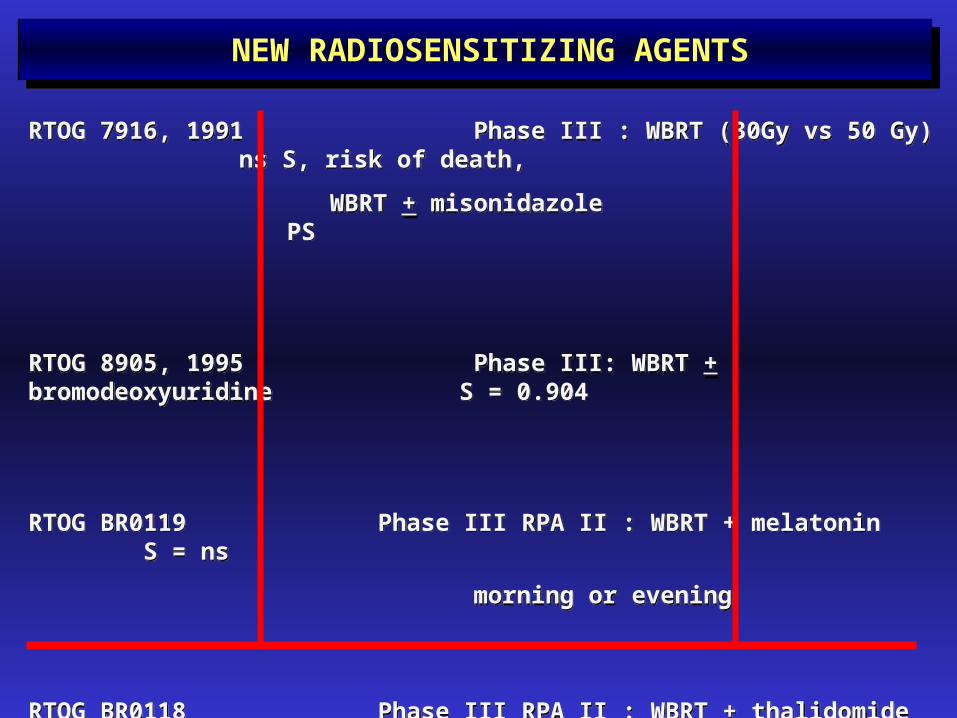
RTOG 7916, 1991 Phase III : WBRT (30Gy vs 50 Gy) ns S, risk of death,
WBRT + misonidazole PS
RTOG 8905, 1995 Phase III: WBRT + bromodeoxyuridine S = 0.904
RTOG BR0119 Phase III RPA II : WBRT + melatonin S = ns
morning or evening
RTOG BR0118 Phase III RPA II : WBRT + thalidomide ongoing
RTOG 7916, 1991 Phase III : WBRT (30Gy vs 50 Gy) ns S, risk of death,
WBRT + misonidazole PS
RTOG 8905, 1995 Phase III: WBRT + bromodeoxyuridine S = 0.904
RTOG BR0119 Phase III RPA II : WBRT + melatonin S = ns
morning or evening
RTOG BR0118 Phase III RPA II : WBRT + thalidomide ongoing
NEW RADIOSENSITIZING AGENTS
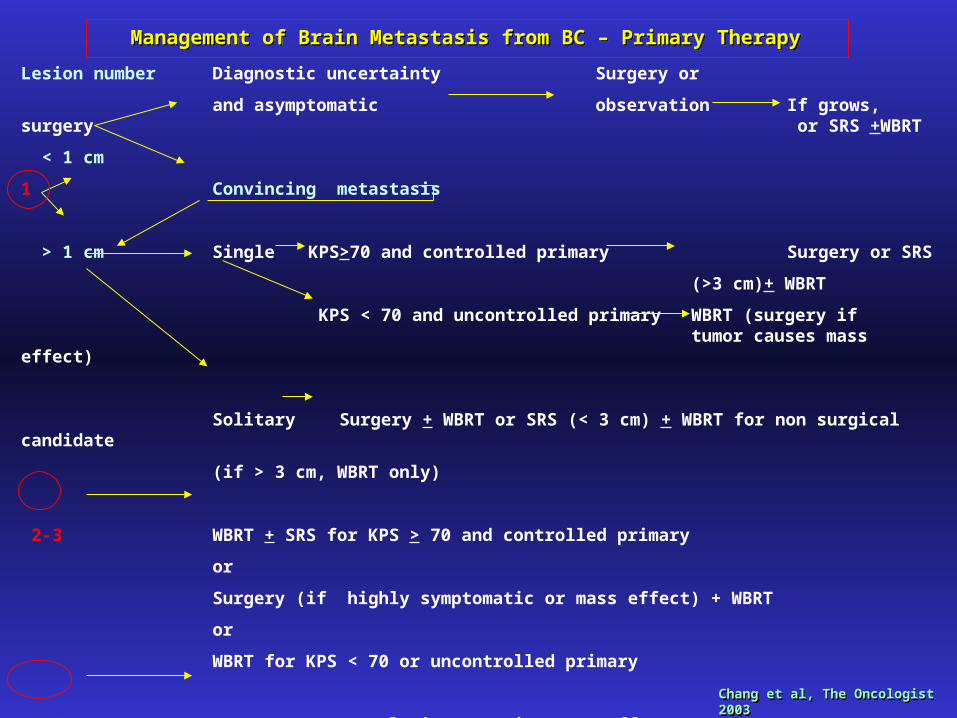
Lesion number Diagnostic uncertainty Surgery or
and asymptomatic observation If grows, surgery or SRS +WBRT
< 1 cm
1 Convincing metastasis
> 1 cm Single KPS>70 and controlled primary Surgery or SRS
(>3 cm)+ WBRT
KPS < 70 and uncontrolled primary WBRT (surgery if tumor causes mass effect)
Solitary Surgery + WBRT or SRS (< 3 cm) + WBRT for non surgical candidate
(if > 3 cm, WBRT only)
2-3 WBRT + SRS for KPS > 70 and controlled primary
or
Surgery (if highly symptomatic or mass effect) + WBRT
or
WBRT for KPS < 70 or uncontrolled primary
> 3 WBRT (surgery to lesions causing mass effect)
Management of Brain Metastasis from BC – Primary Therapy Management of Brain Metastasis from BC – Primary Therapy
Chang et al, The Oncologist 2003Chang et al, The Oncologist 2003

BRAIN METASTASES FROM DIFFERENT TUMOR TYPES: A SURVEY ANALISYS FROM A
MULTIDISCIPLINARY EXPERIENCE
A.Fabi, A.Felici, A.Mirri, I.Sperduti, E.Bria, F.Serraino, G.Lanzetta, G.Mansueto,
L.Moscetti, A.Pace, S.Telera, and CM.Carapella
(the Latium Neuro-Oncology Group)
A.Fabi, A.Felici, A.Mirri, I.Sperduti, E.Bria, F.Serraino, G.Lanzetta, G.Mansueto,
L.Moscetti, A.Pace, S.Telera, and CM.Carapella
(the Latium Neuro-Oncology Group)
Varese, AINO 2004
Edimburgo, EANO 2005
Varese, AINO 2004
Edimburgo, EANO 2005

END-POINTS
Primary
• To define a multidisciplinary approach based on the primary tumor stage, prognostic class and chemo and/or radio-sensitivity
• To clarify the commonly employed therapeutic strategies and to indicate the most effective approach arising from a multidisciplinary experience Fabi et al, EANO
2005

PRIMARY SITE (%)
0
10
20
30
40
50
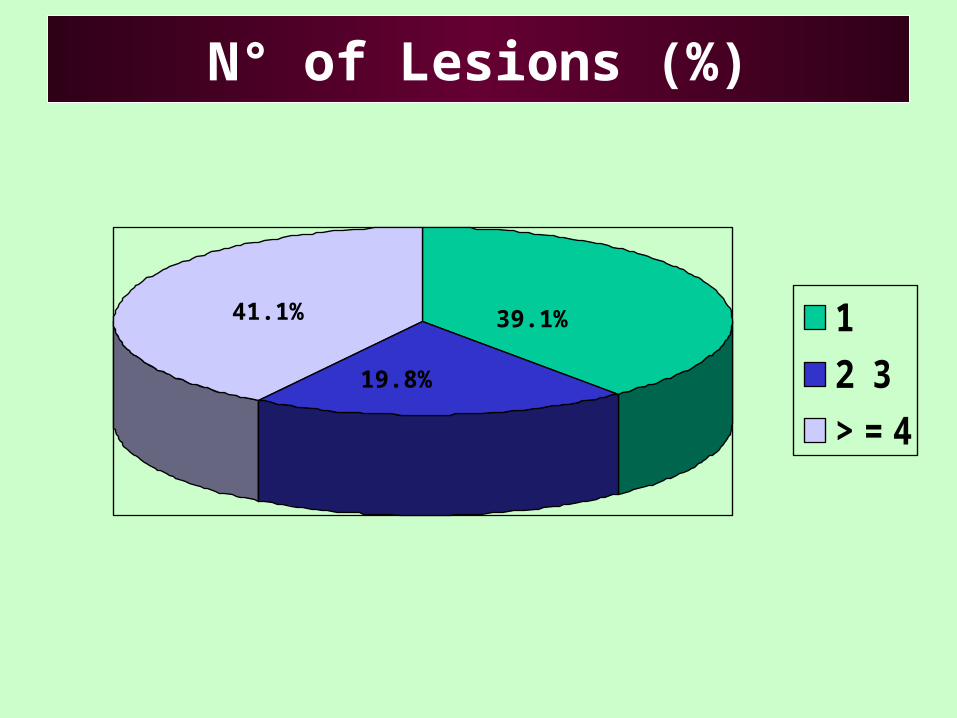
N° of Lesions (%)
1
2 3
> = 4
39.1%
19.8%
41.1%
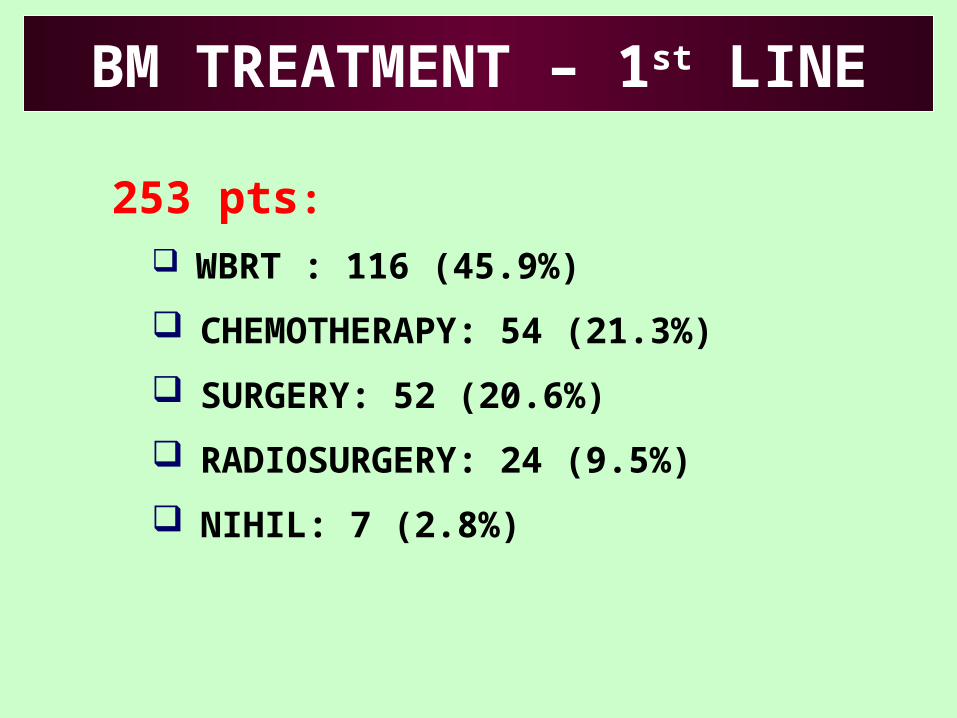
253 pts: WBRT : 116 (45.9%)
CHEMOTHERAPY: 54 (21.3%)
SURGERY: 52 (20.6%)
RADIOSURGERY: 24 (9.5%)
NIHIL: 7 (2.8%)
BM TREATMENT – 1st LINE

134 pts: CHEMOTHERAPY: 72 (53.7%)
WBRT: 47 (35%)
SURGERY: 10 (7.4%)
RADIOSURGERY: 5 (3.7%)
BM TREATMENT – 2nd LINE

0
20
40
60
80
100
0 4 8 12 16 20 24 28 32 36
0
20
40
60
80
100
0 4 8 12 16 20 24 28 32 36
12 %12 %
3- yrs Overall Survival3- yrs Overall Survival
Median OS = 13 months
( 95% C.I. 10-16 )
Months
%50.9 %50.9 %
28.1 %28.1 %

0
20
40
60
80
100
0 2 4 6 8 10 12 colon- rectumbreastmelanomalung
29.1 %29.1 %
1-yr Overall Survival1-yr Overall Survival
months
%
13.4 %13.4 %
51.4 %51.4 %
56.0 %56.0 %
p =0.03

0
20
40
60
80
100
0 4 8 12 16 20 24 1 lesion2-3 lesions>=4 lesions
15.0 %15.0 %
2-yrs Overall Survival2-yrs Overall Survival
months
%
29.0 %29.0 %
40.3 %40.3 %
p <.0001
0
20
40
60
80
100
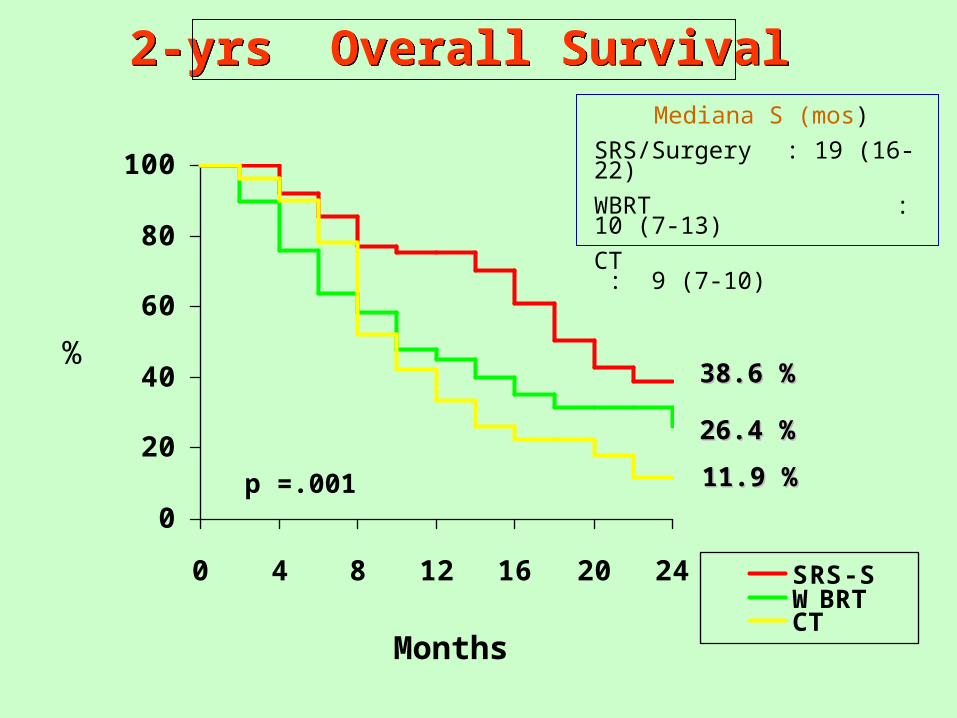
0 4 8 12 16 20 24 SRS- SWBRTCT
11.9 %11.9 %
2-yrs Overall Survival2-yrs Overall Survival
Months
%
26.4 %26.4 %
38.6 %38.6 %
p =.001
Mediana S (mos)
SRS/Surgery : 19 (16-22)
WBRT : 10 (7-13)
CT : 9 (7-10)

BRAIN METASTASES FROM BREAST CANCER
BRAIN METASTASES FROM BREAST CANCER

0
20
40
60
80
100
0 4 8 12 16 20 24
0
20
40
60
80
100
0 4 8 12 16 20 24
43.0 %43.0 %
Breast Cancer and Brain Metastases 2-yrs Overall Survival
Breast Cancer and Brain Metastases 2-yrs Overall Survival
Median OS = 17 months
( 95% C.I. 6-29 )
Months
%56.0 %56.0 %

0
20
40
60
80
100
0 4 8 12 16 20 24 1 lesion2-3 lesions>=4 lesions
15.9 %15.9 %
Breast Cancer and Brain Metastases
2-yrs Overall Survival
Breast Cancer and Brain Metastases
2-yrs Overall Survival
months
%58.3 %58.3 %
90.0 %90.0 %
p =.007

0
20
40
60
80
100
0 4 8 12 16 20 24 SRS- SRT WBCT
37.5 %37.5 %
Breast Cancer and Brain Metastases2-yrs Overall Survival
Breast Cancer and Brain Metastases2-yrs Overall Survival
Months
%58.3 %58.3 %
40.0 %40.0 %


LAPATINIB



Increasing of incidence because increasing of survival
Higher survival because more therapeutic approches
Early diagnosis allows an improvement of survival for the possibility to a local therapy
The need for more effective CNS-directed treatments may become more pressing becouse improvements in systemic treatment for breast cancer could lead to a greater incidence of BM
Radiation therapy remains the mainstay of treatment for BM
SRS and surgery can benefit patients with limited metastatic brain disease and good KPS
Increasing of incidence because increasing of survival
Higher survival because more therapeutic approches
Early diagnosis allows an improvement of survival for the possibility to a local therapy
The need for more effective CNS-directed treatments may become more pressing becouse improvements in systemic treatment for breast cancer could lead to a greater incidence of BM
Radiation therapy remains the mainstay of treatment for BM
SRS and surgery can benefit patients with limited metastatic brain disease and good KPS
Chemotherapy could be a first therapeutical option in case of multiple lesions and uncontrolled extracranial disease or failure to local treatment
The patient with brain metastases can now be treated
Future areas of research:
- Characterization of risk factors and molecular mechanism
- Evaluation of radiologic screening strategies
- More optimization of indication for timing of surgery, WBRT and SRS
- Development of novel chemotherapeutic and biological targeted approaches
Chemotherapy could be a first therapeutical option in case of multiple lesions and uncontrolled extracranial disease or failure to local treatment
The patient with brain metastases can now be treated
Future areas of research:
- Characterization of risk factors and molecular mechanism
- Evaluation of radiologic screening strategies
- More optimization of indication for timing of surgery, WBRT and SRS
- Development of novel chemotherapeutic and biological targeted approaches
