alterations in regional pulmonary flow in ... -...
TRANSCRIPT

Alterations in Regional Pulmonary BloodFlow in Patients with Congenital Heart
Disease Studied by Radioisotope ScanningBy WILLIAM F. FRIEDMIAN, M.D., EUGENE BRAUNWALD, M.D.,
AND ANDREW G. MoRRow, M.D.
SUMMARYExternal scintillation scanning of intravenously administered '31I-labeled macro-
aggregates of human serum albumin (1311-MAA) was employed to evaluate the dis-tribution of pulmonary arterial blood flow in 61 normal subjects and in 100 patientswith various congenital cardiovascular malformations. Intra-aortic administration of131I-MAA demonstrated that blood flow through subelavian-pulmonary artery anas-tomoses is directed principally to the lung on the side of the anastomosis; the relativeconcentration of 1311-MAA in each lung after intravenous injection provided an indexof the patency of the anastomosis or of the development of pulmonary atresia orpulmonary hypertension. In contrast to the findings in patients with a patent sub-clavian-pulmonary shunt, scans obtained from patients with a patent ductus arteriosusdid not reveal a separation of the systemic arterial and systemic venous inflows to thelungs. The patency of superior vena caval-right pulmonary arterial anastomosis couldbe assessed after injection of 13I-MAA into an upper-extremity vein.
Anomalies characterized by increased pulmonary blood flow or elevated pulmonaryarterial pressures, or both, increased the ratio of pulmonary blood flow in the lungapices relative to that in the dependent lung zones. Anomalies characterized by ele-vated pulmonary venous pressure, such as cor triatriatum and mitral regurgitation,were readily detected by demonstrating both a decrease in blood flow to the lungbases as well as an increase to the apices. Thus, in patients with known pulmonaryarterial hypertension (mean pressure, > 30 mm Hg) the ratio of upper to lower zoneblood flow was always significantly higher if the arterial hypertension was accompaniedby venous hypertension. For this reason, lung scans facilitated the screening of patientswith pulmonary arterial hypertension for surgically correctable lesions such as cortriatriatum and mitral stenosis.The method described is technically simple, without risk, easily applicable to large
numbers of patients, and provides clinically important information concerning manyforms of congenital heart disease.
Additional Indexing Words:'311-albumin macroaggregates Superior vena cava-pulmonary arterial anastomosisBronchial circulation Subclavian-pulmonary arterial anastomosis GravityPulmonary arterial hypertension Pulmonary venous hypertension
IT HAS recently become possible to deter- infusion of 1311-labeled macroaggregates ofmine the distribution of pulmonary blood human albumin (1311-MAA).1A In the present
flow in an accurate and reproducible manner study lung scans were employed to investigateby scintillation scanning of the lungs after the the patterns of regional pulmonary blood flow
(PBF) associated with a variety of congenitalFrom the Cardiology Branch and Clinic of Sur- cardiac malformations, to evaluate features of
gery, National Heart Institute, National Institutes of the bronchial circulation in selected patientsHealth, Bethesda, Maryland. with cyanotic heart disease, and to define theCirculation, Volume XXXVII, May 1968 747
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from

FRIEDMAN ET AL.
alterations in the patterns of pulmonary per-fusion which follow operations such as superi-or vena cava-pulmonary arterial anastomosisand subclavian-pulmonary arterial anastomo-sis.
It is recognized that, because of the influ-ence of gravity on the low pressure pulmo-nary vascular bed, normal erect subjects havegreater blood flow to the lung bases than tothe apices. In patients with pulmonary venoushypertension, there is a relative increase inblood flow to the apices and a decrease inperfusion to the lung bases, and it has beenshown that a linear relationship exists be-tween the magnitude of the shift of bloodflow toward the apices and the level of meanleft atrial pressure.2 Investigations utilizinginhaled or injected radioactive gases havedemonstrated that left-to-right circulatoryshunts also increase blood flow to the apicesand reduce the normal differences in perfu-sion between lung apex and base.5 6 Thus, thepresent investigation was also designed tostudy the distribution of PBF in patients withcongenital heart disease in an effort to dis-tinguish those with pulmonary arterial andvenous hypertension from those with pulmo-nary arterial hypertension alone.
MethodsScintillation scanning after administration of
13-11-MAA to patients in the supine position wasemployed to obtain data concerning the rela-tive PBFs to the right and left lungs. Exceptwhen specified, 131I-MAA was administered bythe intravenous route to all of the patients stud-ied. The relative perfusion between lung apexand base was determined after intravenous ad-ministration of MAA to patients who were inthe erect posture. Thyroid uptake of 1311 wasblocked with Lugol's solution which was ad-ministered for 10 days starting the evening priorto the injection of 1311-MAA. High specific ac-tivity (up to 3 mc/mg) radioalbumin aggregates(10-90 O) were used, providing count rates inexcess of 5,000 cpm above background. A doseof 10 to 300 pc was administered during a 5-minute period of quiet breathing. Less than 50,uc and 0.10 mg of protein was injected intra-venously into every patient in whom a right-to-left shunt was present or suspected, and in allinstances of left heart or aortic root injection.The particle distribution of '311-MAA provides
a precise delineation of pulmonary arterial bloodflow because the concentration of radioactivity thataccumulates in the lungs is directly proportionalto the blood flow.", 7 The particles of albuminare too large to pass through the pulmonarycapillary bed and are therefore trapped at thecapillary and precapillary levels. The pulmonaryextraction efficiency exceeds 80%, and an appre-ciable error is not introduced by recirculationbecause the particles not trapped by the lungsare extracted from the blood in the systemiccapillary bed.7 With intra-aortic injection, the13II-MAA reaches the lungs by way of thebronchial circulation unless a direct systemic-pulmonary arterial shunt is present. Significantmetabolic breakdown of the 1311-MAA does notoccur during the period of scanning. Considerabledata concerning the hemodynamic, immuno-logical, and radiation safety of the dose andpreparation have been collected." -10
Details concerning the method of displaying,recording, and quantifying the output of thescintillation detector have been described else-where.2 The scanning was performed within 1hour of 13'I-MAA injection with the patientsin the prone position and the detector mountedabove them. Although the patients lay pronethroughout scanning, the distribution of observedradioactivity in the lungs was that which waspresent at the time of injection. A conventionalradioisotope scanner and a focussed collimatorwere employed. Horizontal rectilinear scanningwas performed at a constant speed while theface of the detector was kept equidistant fromthe skin surface throughout the procedure. Thelevel of radioactivity recorded in any region ofthe scan image of the lung is proportional to theblood flow to that area. Therefore, the distribu-tion of blood flow to the lungs can be expressedas a percentage of the total activity of one orboth lungs.To compare the blood flows between the apex
and base, the right lung was divided into threeequal longitudinal segments from the apex to thetop of the diaphragmatic leaf. The ratio of con-centration of radioactivity between the upperand lower thirds, designated "U/L," was calcu-lated and taken to represent the ratio of bloodflow per unit of lung tissue in these two regions.Observations made for the vertical distributionof blood flow in the left lung were not analyzedin detail since the data from the patients withcongenital heart disease were compared withthose obtained from patients with mitral valvedisease in whorn a greatly enlarged heart oftenobscured the counting field in the left lung.The specific diagnosis was confirmed at car-
diac catheterization for each patient. Angio-Cifrc,a,ion, Volume XXXVII, May 1968
748
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from

REGIONAL PULMONARY BLOOD FLOW
cardiography and cardiac operation providedadditional confirmation in many of the patientsreported. The magnitude of intracardiac shuntingwas determined at cardiac catheterization byeither the 85Krypton inhalation test"1 or by ox-imetry. The ratio between the pulmonary andsystemic vascular resistances was calculatedfrom the formula:
PVR/SVR (%) = x LA Xx 100,QP/QsX SAM -RArn
where PVR = pulmonary vascular resistance;SVR = systemic vascular resistance; QP = pulmo-nary blood flow in L/min; QS = systemic bloodflow in L/min; PAm, LAm, SAm, and RAm =themean pressures in the pulmonary artery, leftatrium, systemic artery, and right atrium in mmHg, respectively.
ResultsDistribution of Pulmonary Blood Flow toBoth Lungs
In 48 normal subjects in whom 1311-MAAwas infused in the supine position, the aver-age distribution to the right lung was 53 +
2.3% (SD) of the total concentration of radio-activity. This partition of the PBF agreesclosely with data obtained from broncho-spirometry.'2 13
Peripheral Pulmonary Stenosis or Atresiaof One Pulmonary Artery
In five patients with unilateral stenosis ofthe right main pulmonary artery (mean pres-sure gradient in excess of 4 mm Hg), the
fraction of the total PBF to the right lungaveraged 47.1 + 2.5%, a value significantly lessthan normal (P <0.02). In one patient witha 5 mm Hg pressure gradient between thepulmonary trunk and the left main pulmonaryartery, the left lung received 41.2% of thetotal PBF (normal=47±2.4%). In four pa-tients in whom multiple bilateral sites of pul-monary arterial narrowing were detectedangiographically, blood flow to the right lungaveraged 51.1 ± 1.5%, a value not significantlydifferent from normal. Of interest was theobservation that in none of these four patientsdid the scans show ischemic areas similar tothose observed after pulmonary embolism,8suggesting that either pulmonary arterial col-lateral vessels provided adequate perfusionto the lung parenchyma distal to the sites ofstenosis or the ischemic areas were too smallto be detected by scanning (that is, < 2 cm2).
In two patients with pulmonary hyperten-sion and atresia of the left main pulmonaryartery, sequential intravenous and intra-aorticinjections of 1311-MAA clearly distinguishedpulmonary arterial from bronchial collateralflow (fig. 1). The scans following aortic in-jection showed considerable radioactivity inthe left lung, reflecting the large flow to thatside through bronchial arteries. Although theentire right ventricular output entered theright pulmonary artery in these patients, a
Figure 1
Chest roentgenogram and lung scans after intravenous (left) and aortic root (right) adminis-tration of 131I-MAA into a patient with atresia of the left main pulmonary artery and aventricular septal defect. The right lung receives all of the pulmonary arterial blood flow(left) while the left lung is supplied exclusively by the bronchial arterial collateral circulation.
Circulation, Volume XXXVII, May 1968
749
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from
FRIEDMAN ET AL.
80*
r40K
IRt. Luni2OF20_
PRE-OPERATIVETETRALOGY OF FALLOT
Ig
PatenPulmNon-Ana
Left Lungnt Anosti. Atresiafunct of a
-I~~~~~~~~~~~~~~~~~~~~~~~~~~POST- OPERATIVE
SUBCLAVIAN-PULMONARY ANAST.
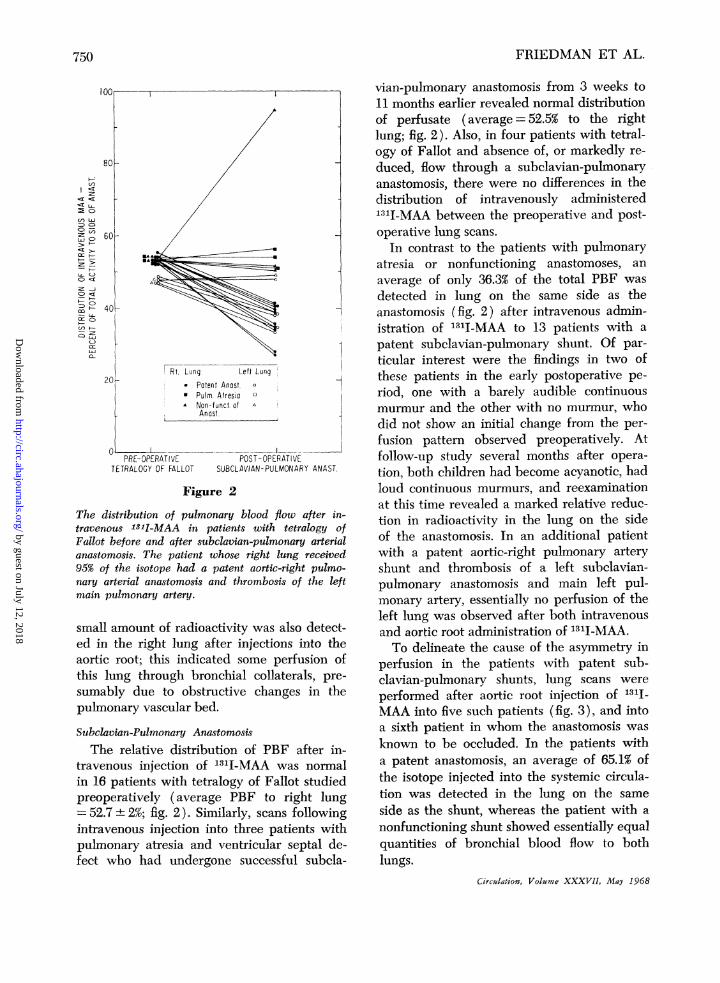
Figure 2
The distribution of pulmonary blood flow after in-
travenous 18-I-MAA in patients with tetralogy ofFallot before and after subclavian-pulmonary arterialanastomosis. The patient whose right lung received95% of the isotope had a patent aortic-right pulmo-nary arterial anastomosis and thrombosis of the leftmain pulmonary artery.
small amount of radioactivity was also detect-ed in the right lung after injections into the
aortic root; this indicated some perfusion ofthis lung through bronchial collaterals, pre-
sumably due to obstructive changes in thepulmonary vascular bed.
Subelavian-Pulmonary Anastomosis
The relative distribution of PBF after in-
travenous injection of 1311-MAA was normalin 16 patients with tetralogy of Fallot studiedpreoperatively (average PBF to right lung-52.7 L 2%; fig. 2). Similarly, scans followingintravenous injection into three patients withpulmonary atresia and ventricular septal de-fect who had undergone successful subcla-
vian-pulmonary anastomosis from 3 weeks to11 months earlier revealed normal distributionof perfusate (average = 52.5% to the rightlung; fig. 2). Also, in four patients with tetral-ogy of Fallot and absence of, or markedly re-duced, flow through a subelavian-pulmonaryanastomosis, there were no differences in thedistribution of intravenously administered1311-MAA between the preoperative and post-operative lung scans.
In contrast to the patients with pulmonaryatresia or nonfunctioning anastomoses, anaverage of only 36.3% of the total PBF wasdetected in lung on the same side as theanastomosis (fig. 2) after intravenous admin-istration of 1311-MAA to 13 patients with apatent subclavian-pulmonary shunt. Of par-ticular interest were the findings in two ofthese patients in the early postoperative pe-riod, one with a barely audible continuousmurmur and the other with no murmur, whodid not show an initial change from the per-fusion pattern observed preoperatively. Atfollow-up study several months after opera-tion, both children had become acyanotic, hadloud continuous murmurs, and reexaminationat this time revealed a marked relative reduc-tion in radioactivity in the lung on the sideof the anastomosis. In an additional patientwith a patent aortic-right pulmonary arteryshunt and thrombosis of a left subelavian-pulmonary anastomosis and main left pul-monary artery, essentially no perfusion of theleft lung was observed after both intravenousand aortic root administration of 1311-MAA.To delineate the cause of the asymmetry in
perfusion in the patients with patent sub-clavian-pulmonary shunts, lung scans wereperformed after aortic root injection of 131I-MAA into five such patients (fig. 3), and intoa sixth patient in whom the anastomosis wasknown to be occluded. In the patients witha patent anastomosis, an average of 65.1% ofthe isotope injected into the systemic circula-tion was detected in the lung on the sameside as the shunt, whereas the patient with anonfunctioning shunt showed essentially equalquantities of bronchial blood flow to bothlungs.
Circulation, Volume XXXVII, May 1968
-:
en LA-o C>
z o
-2 >-
U- (-)
O> <:Z n2O Ct~
-:: L,
C:
on r
750
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from

REGIONAL PULMONARY BLOOD FLOW7
Figure 3Chest roentgenogram and lung scans after aortic root (left) and intravenous (right) administra-tion of 131I-MAA; patient had tetralogy of Fallot and a patent right subclavian-pllmonaryarterial anastomosis. Shunted blood was distributed predominantly to the right lung (left),twhile systemic venous blood wvas diverted to the left lung (right).
Superior Vena Cava-Pulmonary AnastomosisIn a child with tetralogy of Fallot and a
patent superior vena cava-right pulmonaryanastomosis, the infusion of 131I-MAA, into anupper extremity vein resulted in distributionof radioactive particles to the lung on thesame side as the anastomosis; particles weredistributed almost entirely to the opposite lungafter injection of the isotope into a lowerextremity vein (fig. 4).
Patent Ductus ArteriosusIn nine patients with patent ductus arterio-
sus the right lung received 52.4 + 2.5%o of the131I-MAA after intravenous injection. In fiveof these patients, when 1311-MAA was in-jected into the left ventricle or aortic root atthe time of cardiac catheterization, 54.9 ±2lo'of the radioactivity was detected in the rightlung. Thus, the distribution of l3tI-MAA ad-ministered either intravenously or directlyinto the systemic circulation was not signifi-cantly different from the distribution of intra-venously administered 131I-MAA in normalsubjects. After intravenous administration of1311-MAA to a tenth patient with a patentductus, 65% of the total radioactivity was de-tected in the right lung; a similar distributionwas observed 6 months and again 1 year after
Circulation, Volume XXXVII, May 1968
successful closure of the ductus. In this patientstenosis of the left pulmonary artery had beenexcluded at cardiac catheterization. Thus, al-though markedly asymmetric flow to the lungexisted, unlike the patients with a patent sub-clavian-pulmonary anastomosis, it was not dueto a separation of the systemic arterial fromthe systemic venous inflows to the lungs.
After scanning the lungs of an eleventhpatient with a right-to-left shunt through aductus, we were prompted to examine thesystemic distribution of the '111-MAA. In suchpatients desaturated pulmonary arterial bloodis shunted into the descending aorta, so thatit would be anticipated that radioalbuminaggregates would be trapped selectively inthe systemic capillary bed of the lower, asopposed to the upper, extremities after in-travenous injection of 1311-MAA. In the afore-mentioned patient with a right-to-left shuntthrough a ductus, radioactivity emitted fromthe ventral metatarsal surface and the mid-palm of the hand was counted for 5 minuteswith a scintillation detector used routinely forthyroid counting, equipped with a 2-by-2 inchNal crystal (TI) and flat field collimator. Theaccumulated radioactivity in the lower ex-tremities was found to exceed that recordedfrom the upper extremities by an average of
751
I
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from

FRIEDMAN ET AL.
Figure 4
Diagrammatic representation (top), and lung scans and chest roentgenogram (lower) afterupper extremity (lower left) and lower extremity (lower right) administration of 131I-MAAin a patient with tetralogy of Fallot and a patent superior vena cava-right pulmonary arterialanastomosis. SVC = superior vena cava; RPA = right pulmonary artery; RPV = right pulmo-nary vein; RA = right atrium; IVC - inferior vena cava; RV = right ventricle; PA = pulmonaryartery; LPA = left pulmonary artery; LPV = left pulmonary vein; LA = left atrium; LV = leftventricle; Ao = aorta.
30 + 6%. In contrast, when the same techniquewas employed in 11 patients with right-to-leftintracardiac shunts and four patients withpatent ductus and left-to-right shunts, theuptake of radioactivity over the upper ex-
tremities was 24 + 7% higher than that over thelower extremities. Thus, it would appear thatshunt reversal through a ductus may be de-tected by simple counting of the radioactivitythat accumulates in the extremities.
Circulation, Volume XXXVII, May 1968
752
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from

REGIONAL PULMONARY BLOOD FLOW7
Table 1Data orn T'wenty-five Patients
PAm LAm SAm Qp, QsSubject Diagnosis U/L (mm Hg) (mm Hg) (mm Hg) (L/min)
1. R.F.2. A.A.3. L.D.4. J.L.5. R.R.6. G.S.7. L.S.8. M.V.9. M.K.
10. M.R.11. A.B.12. H.B.13. B.C.14. G.C.15. A.D.16. J.H.17. N.S.18. J.W.19. B.W.20. H.B.21. H.G.22. L.G.23. A.N.24. R.N.25. E.W.
ASDVSDASDASDASDASDASDASDVSDVSDASDASDASDASDVSDVSDASDVSDVSDVSDPPHPPHPPHPPHPPH
0.490.570.700.690.520.430.550.630.540.390.680.620.600.570.870.650.580.810.790.600.670.700.660.660.59
13171713191616201920477444327880507483828885447259
54458466551327482
85864
959088861148690768287909479987591707888829085808887
2.2/11.4/14.7/17.6/12/1
2.2/12.4/11.7/11.8/11.5/11.4/11.1/10.85/11.65/11.3/11.1/11.3/11.2/11.4/11.3/1
PVR iSVR(No)
41031465109
11356963157672537364728994407563
Abbreviations: U/L - upper/lower ratio; ASD = atrial septal defect; VSD = ventricular sep-tal defect; PPH = primary pulmonary hypertension; PAm, LAm, and SAm pulmonary-arterial, left atrial, and systemic arterial mean pressure, respectively; RAm = right atrial meanpressure; Qp/Qs = pulmonary/systemic flow ratio; PVR/SVR = pulmonary/systemic vascular
r tn PAmpQsm \10resistancet Qp/Qs X SAm-RAm X10J
Distribution of Pulmonary Blood FlowWithin One Lung
In 13 normal subjects in whom 138I-MAAwas infused during quiet respiration whilethey were erect, the ratio of isotope distribu-tion per unit of lung volume in the upperthird of the right lung to that in the lowerthird (U/L) was 0.43±0.08 (fig. 5). U/Laveraged 0.55 ± 0.09 in 10 patients with intra-cardiac left-to-right shunts and normal pul-monary arterial pressure, a value significantlyhigher than normal (P < 0.02; fig. 5, table1). In ten patients with intra-cardiac shuntsaccompanied by elevated pulmonary arterialmean pressures (in excess of 30 mm Hg) andpulmonary vascular resistances, U/L averagedCirculation, Volume XXXVII, May 1968
0.68 ± 0.10 (fig. 5, table 1), a value significant-ly higher than that obtained from the normalsubjects (P < 0.005) and from the patientswith left-to-right shunts and normal pulmo-nary arterial pressures (P < 0.01). In five pa-tients with idiopathic pulmonary hyperten-sion, U/L averaged 0.66 + 0.07 (fig. 5, table1). U/L was signfficantly lower in all of thepatients with pulmonary arterial hypertensionand normal levels of pulmonary venous pres-sure than in 25 patients reported on previous-ly2 with both pulmonary arterial and pul-monary venous hypertension (U/L = 1.09 +0.28) (P < 0.001; figs. 5 and 6). Moreover, U/Lnever exceeded 1.00 in the absence of pul-monary venous hypertension, regardless of the
753
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from

FRIEDMAN ET AL.
LI
::D
O
'r
O:
Z
1.,OD m_ DUZD
:DI
cr
2.0!
0. 6~~~~~~~~~~~
0.4 I _ _
<00p <0.
o H0L 8
II0.6
U.?- P<GCC? P< 10' P<O.OI___
III1
I
NORMA Lt R SHUNI L- R SHUN1 PRIMARY PULM VENOUS ANDSUBJECTS NORMAL PAP PULM. PULM. ARTERIAL
HYPERTENSION HYPERTENSION -HYPERTENSION
Figure 5U/L values after intravenous administration of 131I-MAA to patients in the erect posture. Horizontal barsrepresent mean values. L-R =left to right; PAP= pulmonary arterial pressure.
pulmonary arterial pressure. Thus, at any levelof mean pulmonary arterial pressure above 30mm Hg, U/L was significantly higher in thepatients with pulmonary venous hypertensionthan in those with pulmonary arterial hyper-tension alone (fig. 6).
DiscussionUntil recently, the accurate topographical
analysis of pulmonary perfusion necessitatedtechniques, such as pulmonary arteriography,bronchospirometry, and the injection or inhala-tion of radioactive gases. Inherent limitationsin each of these methods prevented their wide-spread application to clinical problems. Be-cause of its safety and technical simplicityscintillation scanning of the lungs has madeit possible to derive information concerningthe regional partition of pulmonary bloodflow in patients with a wide variety of cardio-pulmonary disorders. In the present investi-gation, lung scanning provided particularlyuseful information concerning the fate of pal-
I01 1-err,osy -Ie-,/ LAP
|1-INPX60rZefwso n oewgJ
I .) . S
08
..1 7
V 2 02 5_55 0 _ _C55 605 70 75 8G95 909 00
MEAN PULMONARY ARTERY0RESSURE (0.wH9)
Figure 6Relationship between U/L and mean pulmonary ar-tery pressure in patients with pulmonary hypertensionand normal (<15 mm Hg) and elevated (>15 mmHg) left atrial pressure (LAP). In the former groupare patients with primary pulmonary hypertenson,or intra or extra cardiac shunts, or both, with normalor elevated pulmonary vascular resistance. The diag-noses in the patients with left atrial hypertensioninclude congenital and acquired mitral stenosis orregurgitation, or both, and cor triatriatum. At anylevel of mean pulmonary artery pressure beyond 30mm Hg, U/L was significantly higher in the patientswith pulmonary venous hypertension than in thosewith pulmonary arterial hypertension alone.
liative systemic arterial or systemic venous-pulmonary arterial anastomoses in patientswith cyanotic heart disease and has allowedthe distinction of patients with pulmonaryarterial hypertension from those with bothpulmonary arterial and venous hypertension.
In 1962, Fragoyannis and Kardalinas14 com-pared the histological appearance of the smallpulmonary arteries in each lung after system-ic-pulmonary arterial anastomosis. They ob-served differences in the caliber and muscularcontent of the medial layer of these vesselswhich suggested that the lung on the sideof the anastomosis received the major portionof blood flowing through the artificially creat-ed shunt. Subsequently, Fort and associates'-demonstrated in animals with subclavian-pulmonary arterial anastomoses that the ma-jor proportion of the blood shunted from thesubclavian artery passed to the lung on theside of the anastomosis, and that the shuntflow diverted a major part of the right ven-tricular output to the lung on the side oppo-
Circulation, Volume XXXVII, May 1968
754
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from

REGIONAL PULMONARY BLOOD FLOW
Subclavian-Pulmonary Artery Anastomosis1. PATENT ANASTOMOSIS 2.NON-FUNCTION OFIANASTOMOSIS
Figure 7
Diagrammatic representation of the postoperative relation between systemic arterial andvenous blood supply to the lungs in patients with tetralogy of Fallot. (1) When a subclavian-pulmonary anastomosis is patent, the lung on the same side as the anastomosis receives mostof the oxygenated, shunted blood (solid black) while unsaturated, systemic venous blood(stippled gray) is diverted to the opposite lung. The development of a more symmetric dis-tribution of either venous or shunted blood suggests that the anastomosis is (2) thrombosed,(3) patent in the presence of pulmonary atresia, or (4) patent in the presence of pulmonaryhypertension. SVC =superior vena cava; IVC= inferior vena cava; RA=right atrium; RV= right ventricle; PA = pulmonary artery; LA = left atrium; LV = left ventricle; Ao = aorta.
site the anastomosis. This finding is consistentwith those reported in patients in an earliercommunication from this laboratory,3 as wellas by Tauxe and associates"6 and Massumi andco-workers.17The present study indicates that, together
with routine clinical assessment of the patient,intravenous lung scans obtained serially fol-lowing systemic-pulmonary anastomosis mayCirculation, Volume XXXVII, May 1968
provide information concerning the patency ofthe shunt, the severity of right ventricular out-flow obstruction, and the development of pul-monary hypertension (fig. 7). It would appearthat, although total pulmonary blood flow isincreased after subclavian-pulmonary anasto-mosis, the augmented flow to the lung on theside of the anastomosis is largely composedof oxygenated shunted blood, while the flow
755
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from

FRIEDMAN ET AL.
to the opposite lung is largely unsaturatedsystemic venous blood (fig. 7). In addition,a patent shunt changes the distribution ofblood entering the main pulmonary artery fromthe right ventricle, diverting most of the sys-temic venous return to the lung on the sideopposite the anastomosis. The distribution ofshunted blood becomes more symmetricalpostoperatively if the severity of right ven-tricular obstruction increases, or the shuntthrough the subclavian-pulmonary artery an-astomosis diminishes markedly or ceases (fig.7). The latter may occur if thrombosis de-velops at the anastomosis or if pulmonaryarteriolar vascular obstruction develops.'8These two possibilities may be differentiatedwith relative ease by determining the size ofthe pulmonary arteries on a plain chest roent-genogram. On the other hand, if symmetricaldistribution of intravenously injected particlesoccurs in patients who have maintained clini-cal improvement postoperatively, then it maybe assumed that an increase in the degree ofpulmonary stenosis has occurred.
It may be anticipated, therefore, that inany individual patient, serial lung scans willafford a simple means for following the pa-tient's condition postoperatively. It may alsobe anticipated that serial lung scans willpermit an estimate of the patency of superiorvena cava-pulmonary arterial anastomoses.If the anastomosis is patent, infusion of'311-MAA will produce a scintiscan of theright lung only; on the other hand, the leftlung will be visualized after an injection intoa vein in the lower extremity (fig. 4). Ob-struction at the site of the anastomosis leadsto the retrograde flow of superior caval bloodto the inferior vena cava via the hemiazy-gous venous pathway.'9 Thus, postoperative-ly, relative increases in the radioactivitydetected in the left lung after injection of1311-MAA into an upper extremity vein sug-gest that malfunction and perhaps imminentthrombosis of the anastomosis exist.Garfunkel and Kirkpatrick,20 and Whitley
and associates2' have observed patients withpatent ductus in whom decreased vascularityof the left lung was a prominent roentgeno-
graphic feature and both a primary decreasein perfusion, and unilateral overaeration havebeen postulated as being responsible for theasymmetric appearance of the lung fields.That the former may sometimes be the caseis suggested by our patient, mentioned earlier,in whom asymmetric pulmonary arterial bloodflow persisted after closure of a ductus. How-ever, it is also clear that in an occasionalpatient the ductus may insert at a moreperipheral site into the left pulmonary artery,and Ankeney22 and Tauxe and associates'6have each reported one such case in whichthe flow through the ductus entered the leftlung exclusively, with the blood ejected fromthe right ventricle being diverted into theright pulmonary artery.The clinical value of lung scanning in pa-
tients with pulmonary hypertension is basedon the well-known fact that the normal pul-monary circulation has a low perfusion pres-sure and the distribution of blood enteringthe lungs is considerably influenced by grav-ity.23' 24 Hence, in normal erect man there ismuch greater blood flow through the depen-dent zones of the lungs than through theapical regions. The present findings indicatethat when pulmonary blood flow increases,as it does in patients with left-to-right cardiacshunts, this difference in flow between theupper and lower pulmonary zones decreases,even if the pulmonary artery pressure remainsnormal. Patients with left-to-right shunts withpulmonary arterial hypertension and withoutpulmonary venous hypertension show a fur-ther reduction of the difference in flows be-tween the apical and dependent zones of thelungs, so that the blood flow per unit of lungvolume in the upper third of the lung is ap-proximately 70% of that in the lower third.In this regard, in several patients with trans-position of the great arteries in whom thepulmonary artery could not be entered atcardiac catheterization, lung scanning washelpful in distinguishing normal from ele-vated pulmonary arterial pressures. Whenboth pulmonary arterial and venous pressurerise, blood flow to the apices of the lung in-creases while flow to the bases diminishes; the
Circulation, Volume XXXVII, May 1968
756
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from

REGIONAL PULMONARY BLOOD FLOW
result is in an inversion of the pattern ob-served in normal erect subjects.2 25,26 Al-though pulmonary arterial hypertension aloneresults in elevated levels of U/L, the latterhas never been found to exceed 1.00 in theabsence of pulmonary venous hypertension.Hence, while relatively increased blood flowto the apices was found in our patients withleft-to-right shunts, the Eisenmenger syn-drome, and primary pulmonary hyperten-sion, lung scanning may be of diagnosticvalue, since at elevated levels of pulmonaryarterial pressure the shift of blood flow tothe apices is always significantly greater inpatients with both pulmonary arterial andvenous hypertension than in patients withpulmonary arterial hypertension alone. Forthis reason the technique has been helpfulin screening patients with known severe pul-monary arterial hypertension for potentiallycorrectable lesions such as cor triatriatumor mitral stenosis which are also associatedwith pulmonary venous hypertension.
References1. LOPEZ-MAJANO, V., CHERNICK, V., WAGNER,
H. N., JR., AND DUTTON, R. E.: Comparison ofradioisotope scanning and differential oxygenuptake of the lungs. Radiology 83: 697, 1964.
2. FRIEDMAN, W. F., AND BRAUNWALD, E.: Altera-tions in regional pulmonary blood flow inmitral valve disease studied by radioisotopescanning: Simple nontraumatic technique forestimation of left atrial pressure. Circulation34: 363, 1966.
3. FRIEDMAN, W. F., BRAUNWALD, E., AND MOR-ROw, A. C.: Diagnostic value of lung scanningin congenital heart disease. (Abstr.) Circula-tion 34 (suppl. III): III-105, 1966.
4. TAUXE, W. N., BURCHELL, H. B., CHAAPEL,D. W., AND SPRAU, A.: Quantitating the effectof gravity on lung scans of macroaggregatesof albumin-I131. J Appl Physiol 21: 1381, 1966.
5. DOLLERY, C. T., WEST, J. B., WILCKEN, D. E. L.,GOODWIN, J. F., AND HUGH-JONES, P.: Re-gional pulmonary blood flow in patients withcirculatory shunts. Brit Heart J 23: 225, 1961.
6. DOLLERY, C. T., WEST, J. B., WILCKEN, D. E. L.,AND HUGH-JONES, P.: Comparison of pulmo-nary blood flow between left and right lungsin normal subjects and patients with congenitalheart disease. Circulation 24: 617, 1961.
7. TOW, D. E., WAGNER, H. N., JR., LOPEZ-MA-JANO, V., SMITH, E. M., AND MIGITA, T.:
Circulation, Volume XXXVII, May 1968
Validity of measuring regional pulmonary ar-terial blood flow with macroaggregates ofhuman serum albumin. Amer J Roentgen96: 664, 1966.
8. WAGNER, H. N., JR., SABISTON, D. C., JR., MC-AFEE, J. G., Tow, D. E., AND STERN, H. S.:Diagnosis of massive pulmonary embolism inman by radioisotope scanning. New Eng JMed 271: 377, 1964.
9. COMIROE, J. H., JR.: Main functions of the pul-monary circulation. Circulation 33: 146, 1966.
10. MURPHY, E., CERVANTES, C., AND MAAS, R.: Fateof macroaggregates of radioalbumin in thelung. Amer J Clin Path 48: 18, 1967.
11. BRAUNWALD, E., COLDBLATT, A., LONG, R. T. L.,AND MORROW, A. G.: Krypton85 inhalation testfor the detection of left-to-right shunts. BritHeart J 24: 47, 1962.
12. GAENSLER, E. A.: Bronchospirometry: I. Reviewof the literature. J Lab Clin Med 39: 917,1952.
13. MATTSON, S. B., AND CARLENS, E.: Lobar ventila-tion and oxygen uptake in man: Influence ofbody position. J Thorac Surg 30: 676, 1955.
14. FRAGOYANNIS, S., AND KARDALINAS, A.: Congeni-tal heart disease with pulmonary ischemia:Study of the pulmonary vascular lesions beforeand after systemic pulmonary anastomosis.Amer Heart J 63: 335, 1962.
15. FORT, L., MORROW, A. G., PIERCE, G. E., SAIG-USA, M., AND MCLAUGHLIN, J. S.: Distributionof pulmonary blood flow after subelavian-pul-monary anastomosis. J Thorac Cardiov Surg50: 671, 1965.
16. TAUXE, W. N., BURCHELL, H. B., AND BLACK,L. F.: Clinical applications of lung scanning.Mayo Clin Proc 42: 473, 1967.
17. MASSUmI, R., JUST, G., RIOS, J., AND TAWAKKOL,A.: Retrograde lung scanning. J Thorac Car-diov Surg 54: 132, 1967.
18. Ross, R. S., TAUSSIG, H. B., AND EVANS, M. H.:Late hemodynamic complications of anastomot-ic surgery for treatment of the tetralogy ofFallot. Circulation 18: 553, 1958.
19. CANENT, R. V., JR., SPACH, M. S., AND YOUNG,W. G., JR.: Cardiopulmonary dynamics inpatients with anastomosis of the superior venacava to the right pulmonary artery. Circulation30: 47, 1964.
20. GARFUNKEL, J. M., AND KIRKPATRICK, J. A.:Overaeration of the left lung as a manifestationof patent ductus arteriosus. Circulation 24:937, 1961.
21. WHITLEY, J. E., RUDHE, V., AND HERZENBERG,H.: Decreased left lung vascularity in congeni-tal left-to-right shunts. Acta Radiol (Stock-holm) 1: 1125, 1963.
757
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from

7BFRIEDMAN ET AL.
22. ANKENEY, J. L.: Discussion. J Thorac CardiovSurg 50: 676, 1965.
23. WEST, J. B., DOLLERY, C. T., AND NAIMARK, A.:Distribution of blood flow in isolated lung:Relation to vascular and alveolar pressures.J Appl Physiol 19: 713, 1964.
24. WEST, J. B., AND DOLLERY, C. T.: Distributionof blood flow and the pressure-flow relationsof the whole lung. J Appl Physiol 20: 175,1965.
25. DOLLERY, C. T., AND WEST, J. B.: Regional up-take of radioactive oxygen, carbon monoxideand carbon dioxide in the lungs of patientswith mitral stenosis. Circulation Research 8:765, 1960.
26. WEST, J. B., DOLLERY, C. T., AND HEARD, B. E.:Increased pulmonary vascular resistance inthe dependent zone of the isolated dog lungcaused by perivascular edema. Circulation Re-search 17: 191, 1965.
(tE)
Bicentenary of Classic Description of AnginaCorrelation with Coronary Disease
It may seem surprising that Heberden did not take any active part in the pathologicalinvestigations and the controversy over the cause of angina which was already arisingin his lifetime. Jenner and Parry had both adopted the coronary theory by 1778, butdelayed its publication for fear of alarming John Hunter in whom Jenner had diagnosedangina in 1777, at Bath, and had written to Heberden about the case though apparentlythe letter was not received; it was published in Baron's Life of Jenner. Fothergi}l hadpublished a case of fatal gngina pectoris, in which Hunter found ossified coronaryarteries at necropsy in 1776, and Samuel Black of Newry had reported ossified coronariesin anginal cases in 1794.-D. EVAN BEDFORD: William Heberden's Contribution toCardiology. J Roy Coll Physicians (Lond) 2:132, 1968.
Circ,dation, Volume XXXVII, May 1968
758
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from

WILLIAM F. FRIEDMAN, EUGENE BRAUNWALD and ANDREW G. MORROWDisease Studied by Radioisotope Scanning
Alterations in Regional Pulmonary Blood Flow in Patients with Congenital Heart
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1968 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.37.5.747
1968;37:747-758Circulation.
http://circ.ahajournals.org/content/37/5/747located on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. and Rights Question and Answer
Permissionsthe Web page under Services. Further information about this process is available in thewhich permission is being requested is located, click Request Permissions in the middle column ofClearance Center, not the Editorial Office. Once the online version of the published article for
can be obtained via RightsLink, a service of the CopyrightCirculationoriginally published in Requests for permissions to reproduce figures, tables, or portions of articlesPermissions:
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from