altered sensorimotor transformations for balance in
TRANSCRIPT
Altered Sensorimotor Transformations for Balance In Parkinson’s DiseaseJ. Lucas McKay and Lena H. TingWallace H. Coulter Department of Biomedical Engineering, Georgia Tech and Emory University, Atlanta, Georgia, USA
Long latency automatic postural responses to balance perturbations are often abnormal in Parkinson’s disease (PD) and may cause impaired balance and falls.•Antagonist and agonist muscles during long latency postural responses are often
coactivated in PD (Carpenter et al. 2004; Dimitrova et al. 2004; St George et al. 2012), which may increase rigidity and decrease stability. However, pathologic changes underlying abnormal postural responses are poorly understood, limiting our ability to develop improved therapies.
We have developed a mechanistic model of the sensorimotor feedback transformation underlying the magnitude and timing of muscle activation during postural responses: the sensorimotor response model (SRM).•We demonstrated that in behaving cats (Lockhart and Ting 2007) and in young
healthy individuals (Safavynia and Ting 2012; Welch and Ting 2009), postural responses are created through multisensory estimates of the motion of the body centerofmass(CoM)toactivatemusclesinanoptimaltradeoffbetweenposturalerrorandcontroleffort.
Here, we applied the SRM to investigate whether and how PD modifies the sensorimotor transformation during postural responses.•We compared postural responses to forward perturbations of the CoM in two
female patients: advanced PD (age, 75 y; Hoehn & Yahr stage 3; UPDRS-III score 43; daily falls, OFF medications), and mild PD (54 y; H & Y 1.5; UPDRS-III 24, no previous falls, OFF medications) with postural responses from healthy older (female, 70 y) and healthy young (female, 19 y) participants.
We hypothesize that pathologic changes in PD cause impaired inhibition of competing sensorimotor feedback motor programs during postural responses.•Mink has hypothesized that the basal ganglia provide “focused facilitation and
surround inhibition of motor mechanisms in thalamocortical and brainstem circuits” which is compromised in PD (Mink 2003).
•We predicted that in PD, antagonist muscles would be activated with increased magnitude,reflectedinincreasedSRMparametermagnitudes,andinadvancedPD, antagonists and agonists are also activated with abnormal timing, including shortenedburstsofinitialactivity,reflectedinincreasedvaluesofSRMparameterkJ, the feedback gain on the derivative of CoM acceleration.
Introduction
Methods
contact: [email protected]
• 3 backward perturbations (peak displacement: 7.5 cm displacement; 15 cm/s velocity; 0.1 g acceleration) within unpredictable multidirectional block
• Surface EMG recorded at 1,080 Hz from 16 leg and trunk muscles (Basmajian and Blumenstein 1980) and synchronized with kinematics and kinetics.
• EMG processed as in previous studies (hi-pass, 35 Hz, de-mean, rectify, low-pass, 40 Hz; bidirectional Butterworth filteringusedinallcasestoremovephaseartifacts).
• Average EMG in medial gastrocnemius (MGAS) and tibialis anterior (TA) analyzed.
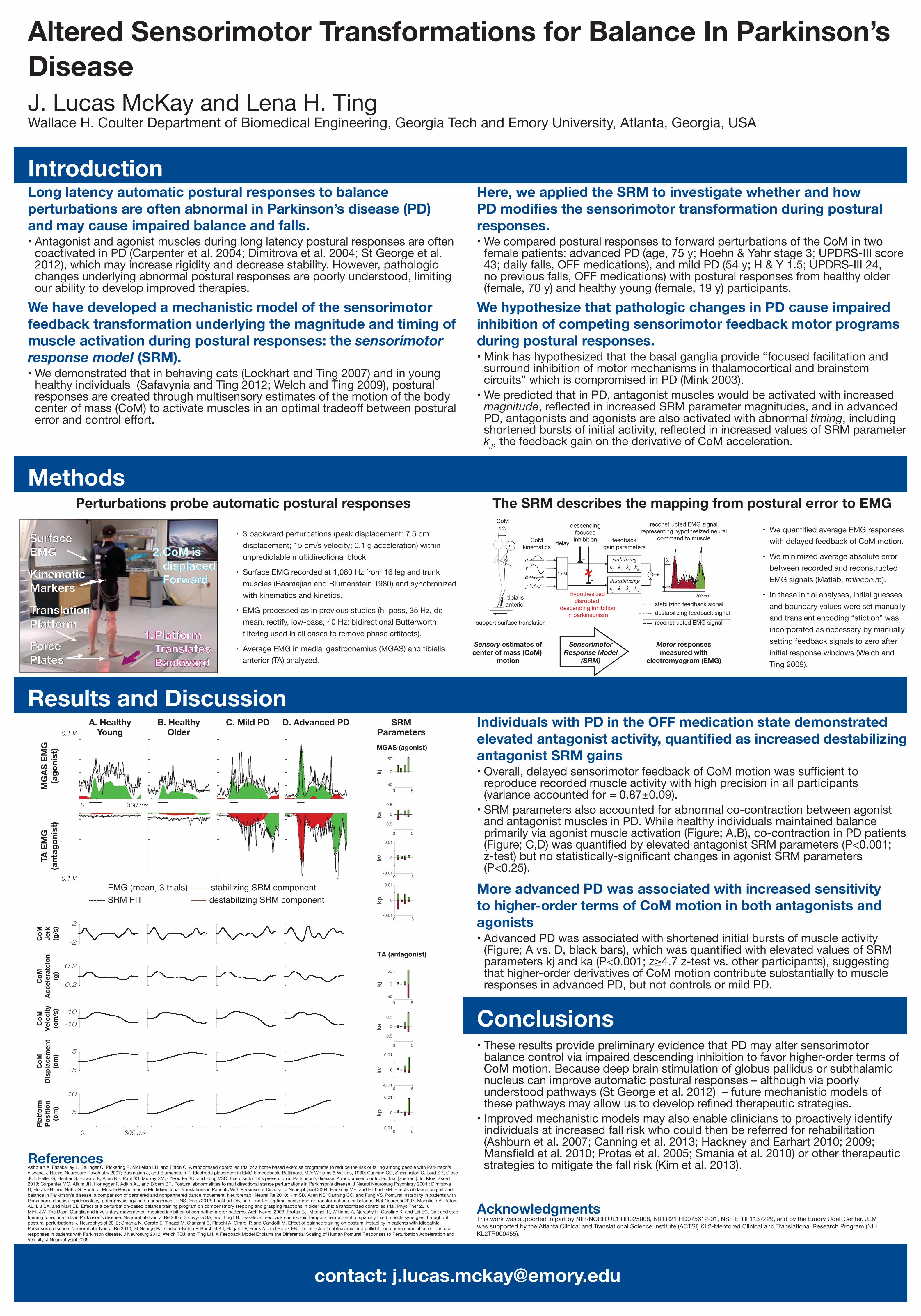
Individuals with PD in the OFF medication state demonstrated elevated antagonist activity, quantified as increased destabilizing antagonist SRM gains•Overall,delayedsensorimotorfeedbackofCoMmotionwassufficientto
reproduce recorded muscle activity with high precision in all participants (variance accounted for = 0.87±0.09).
•SRM parameters also accounted for abnormal co-contraction between agonist and antagonist muscles in PD. While healthy individuals maintained balance primarily via agonist muscle activation (Figure; A,B), co-contraction in PD patients (Figure;C,D)wasquantifiedbyelevatedantagonistSRMparameters(P<0.001;z-test)butnostatistically-significantchangesinagonistSRMparameters(P<0.25).
More advanced PD was associated with increased sensitivity to higher-order terms of CoM motion in both antagonists and agonists•Advanced PD was associated with shortened initial bursts of muscle activity (Figure;Avs.D,blackbars),whichwasquantifiedwithelevatedvaluesofSRMparameterskjandka(P<0.001;z≥4.7z-testvs.otherparticipants),suggestingthat higher-order derivatives of CoM motion contribute substantially to muscle responses in advanced PD, but not controls or mild PD.
ReferencesAshburn A, Fazakarley L, Ballinger C, Pickering R, McLellan LD, and Fitton C. A randomised controlled trial of a home based exercise programme to reduce the risk of falling among people with Parkinson’s disease. J Neurol Neurosurg Psychiatry 2007; Basmajian J, and Blumenstein R. Electrode placement in EMG biofeedback. Baltimore, MD: Williams & Wilkins, 1980; Canning CG, Sherrington C, Lord SR, Close JCT, Heller G, Heritier S, Howard K, Allen NE, Paul SS, Murray SM, O’Rourke SD, and Fung VSC. Exercise for falls prevention in Parkinson’s disease: A randomised controlled trial [abstract]. In: Mov Disord 2013; Carpenter MG, Allum JH, Honegger F, Adkin AL, and Bloem BR. Postural abnormalities to multidirectional stance perturbations in Parkinson’s disease. J Neurol Neurosurg Psychiatry 2004 ; Dimitrova D,HorakFB,andNuttJG.PosturalMuscleResponsestoMultidirectionalTranslationsinPatientsWithParkinson’sDisease.JNeurophysiol2004;HackneyME,andEarhartGM.Effectsofdanceongaitandbalance in Parkinson’s disease: a comparison of partnered and nonpartnered dance movement. Neurorehabil Neural Re 2010; Kim SD, Allen NE, Canning CG, and Fung VS. Postural instability in patients with Parkinson’sdisease.Epidemiology,pathophysiologyandmanagement.CNSDrugs2013;LockhartDB,andTingLH.Optimalsensorimotortransformationsforbalance.NatNeurosci2007;MansfieldA,PetersAL,LiuBA,andMakiBE.Effectofaperturbation-basedbalancetrainingprogramoncompensatorysteppingandgraspingreactionsinolderadults:arandomizedcontrolledtrial.PhysTher2010Mink JW. The Basal Ganglia and involuntary movements: impaired inhibition of competing motor patterns. Arch Neurol 2003; Protas EJ, Mitchell K, Williams A, Qureshy H, Caroline K, and Lai EC. Gait and step trainingtoreducefallsinParkinson’sdisease.NeurorehabNeuralRe2005;SafavyniaSA,andTingLH.Task-levelfeedbackcanexplaintemporalrecruitmentofspatiallyfixedmusclesynergiesthroughoutposturalperturbations.JNeurophysiol2012;SmaniaN,CoratoE,TinazziM,StanzaniC,FiaschiA,GirardiP,andGandolfiM.EffectofbalancetrainingonposturalinstabilityinpatientswithidiopathicParkinson’sdisease.NeurorehabilNeuralRe2010;StGeorgeRJ,Carlson-KuhtaP,BurchielKJ,HogarthP,FrankN,andHorakFB.TheeffectsofsubthalamicandpallidaldeepbrainstimulationonposturalresponsesinpatientswithParkinsondisease.JNeurosurg2012;WelchTDJ,andTingLH.AFeedbackModelExplainstheDifferentialScalingofHumanPosturalResponsestoPerturbationAccelerationandVelocity. J Neurophysiol 2009.
AcknowledgmentsThis work was supported in part by NIH/NCRR UL1 RR025008, NIH R21 HD075612-01, NSF EFRI 1137229, and by the Emory Udall Center. JLM was supported by the Atlanta Clinical and Translational Science Institute (ACTSI) KL2-Mentored Clinical and Translational Research Program (NIH KL2TR000455).
Results and Discussion
SurfaceEMG CoM is
displacedForwardKinematic
Markers
TranslationPlatform
ForcePlates
PlatformTranslatesBackward
1.
2.
Perturbations probe automatic postural responses The SRM describes the mapping from postural error to EMG• WequantifiedaverageEMGresponses
with delayed feedback of CoM motion.
• We minimized average absolute error between recorded and reconstructed EMG signals (Matlab, fmincon.m).
• In these initial analyses, initial guesses and boundary values were set manually, and transient encoding “stiction” was incorporated as necessary by manually setting feedback signals to zero after initial response windows (Welch and Ting 2009).
•These results provide preliminary evidence that PD may alter sensorimotor balance control via impaired descending inhibition to favor higher-order terms of CoM motion. Because deep brain stimulation of globus pallidus or subthalamic nucleus can improve automatic postural responses – although via poorly understood pathways (St George et al. 2012) – future mechanistic models of thesepathwaysmayallowustodeveloprefinedtherapeuticstrategies.
•Improved mechanistic models may also enable clinicians to proactively identify individuals at increased fall risk who could then be referred for rehabilitation (Ashburn et al. 2007; Canning et al. 2013; Hackney and Earhart 2010; 2009; Mansfieldetal.2010;Protasetal.2005;Smaniaetal.2010)orothertherapeuticstrategies to mitigate the fall risk (Kim et al. 2013).
Conclusions
δ(t-λ)
dvaj
delayCoMkinematics
feedbackgain parameters
reconstructed EMG signalrepresenting hypothesized neural
command to muscle
descendingfocusedinhibition
destabilizingkj ka kv kd
stabilizingkj ka kv kd
λ
stabilizing feedback signalhypothesized
disrupted descending inhibition
in parkinsonism
800 ms
+ destabilizing feedback signalreconstructed EMG signalsupport surface translation
Sensory estimates ofcenter of mass (CoM)
motion
SensorimotorResponse Model
(SRM)
Motor responsesmeasured with
electromyogram (EMG)
CoMx(t)
tibialisanterior
++--
-2
2
CoM Jerk
(g/s
)
MGAS (agonist)
TA (antagonist)
-0.2
0.2
CoM
Acc
eler
atci
on(g
)
-10
10
CoM
Velo
city
(cm
/s)
-5
5
CoM
Dis
plac
emen
t(c
m)
5
10
Plat
form
Posi
tion
(cm
)
EMG (mean, 3 trials)SRM FIT
stabilizing SRM componentdestabilizing SRM component
MG
AS E
MG
(ago
nist
)
0.1 V
0.1 V
0 800 ms
TA E
MG
(ant
agon
ist)
C. Mild PDA. HealthyYoung
D. Advanced PD SRMParameters
B. HealthyOlder
0 800 ms
0 5
kj
-50
0
50
0 5
ka
-0.5
0
0.5
0 5
kv
-0.01
0
0.01
0 5
kp
-0.01
0
0.01
0 5
kj
-50
0
50
0 5
ka
-0.5
0
0.5
0 5
kv
-0.01
0
0.01
0 5
kp
-0.01
0
0.01