altitude and travel - winnipeg regional health authority · the dangers of altitude and acute...
TRANSCRIPT
Altitude and TravelAltitude and Travel
Philippe LagacPhilippe Lagacéé--WiensWiensMD, DTM&H, FRCPCMD, DTM&H, FRCPC
OutlineOutline
Basic physiology of altitude medicineBasic physiology of altitude medicineThe dangers of altitude and acute altitude The dangers of altitude and acute altitude illnesses.illnesses.Diagnosis of altitude related illnessesDiagnosis of altitude related illnessesTreatment of altitude related illnessesTreatment of altitude related illnessesPrevention of altitude illnesses.Prevention of altitude illnesses.Altitude illness in special populations.Altitude illness in special populations.


Altitude medicine Altitude medicine –– the basicsthe basics
Oxygen makes up roughly 21% of the gases Oxygen makes up roughly 21% of the gases in our atmosphere.in our atmosphere.Normal atmospheric pressure is 760 mm Normal atmospheric pressure is 760 mm Hg, Hg, –– Normal oxygen pressure is 159 mmHg.Normal oxygen pressure is 159 mmHg.As elevation increases, atmospheric As elevation increases, atmospheric pressure decreases (pressure decreases (oxygen concentration oxygen concentration stays the samestays the same).).
What does it mean?What does it mean?
In Winnipeg, oxygen pressure is 155 mmHg In Winnipeg, oxygen pressure is 155 mmHg ((““97%97%””))In Cusco, Peru oxygen pressure is : 100 mmHg In Cusco, Peru oxygen pressure is : 100 mmHg ((““65%65%””))In Lhasa, Tibet: 96 mmHg (In Lhasa, Tibet: 96 mmHg (““60%60%””))In La Paz, Bolivia: 92 mmHg (In La Paz, Bolivia: 92 mmHg (““58%58%””))Mt. Kilimanjaro: 73 mmHg (Mt. Kilimanjaro: 73 mmHg (““48%48%””))
Oxygen physiologyOxygen physiology
Haemoglobin carries oxygen from the lungs to the Haemoglobin carries oxygen from the lungs to the tissues.tissues.The amount of oxygen carried depends on the The amount of oxygen carried depends on the amount of oxygen in the lung and amount of amount of oxygen in the lung and amount of haemoglobin.haemoglobin.Haemoglobin is can be fully saturated as long as Haemoglobin is can be fully saturated as long as the atmospheric Othe atmospheric O2 2 pressure is over 115.pressure is over 115.–– Occurs at about 2500mOccurs at about 2500m
Adaptations to low oxygen pressureAdaptations to low oxygen pressure
Short term:Short term:–– HyperventilationHyperventilation
Increases oxygen in lungs by reducing COIncreases oxygen in lungs by reducing CO22
Also increases pHAlso increases pH
–– Renal acidRenal acid--base changes, disordered ventilationbase changes, disordered ventilationCompensates for pH increaseCompensates for pH increase
–– Local tissue responses to low oxygenLocal tissue responses to low oxygen
Long term:Long term:–– Not an issue in acute mountain sicknessNot an issue in acute mountain sickness–– Involves slow increase in oxygen carrying capacity.Involves slow increase in oxygen carrying capacity.
Dangers of altitude Dangers of altitude –– Many Many forms!forms!
Lower oxygen tensionLower oxygen tension–– Drops by 80 mm (~10 kPa) for each 1000 mDrops by 80 mm (~10 kPa) for each 1000 mIncreased UV radiationIncreased UV radiation–– Up 14% for each 1000mUp 14% for each 1000mLower temperaturesLower temperatures–– --6.56.5ººC for each 1000mC for each 1000m
Illnesses associated with altitudeIllnesses associated with altitudeOxygenOxygen--relatedrelated–– Acute hypoxiaAcute hypoxia–– AMSAMS–– HAPEHAPE–– HACEHACE–– Peripheral OedemaPeripheral Oedema–– PE/Thromboembolism/strokePE/Thromboembolism/stroke–– RetinopathyRetinopathy–– Disordered/periodic breathingDisordered/periodic breathing
Physical environment relatedPhysical environment related–– ExposureExposure–– SunburnSunburn–– Snow blindnessSnow blindness
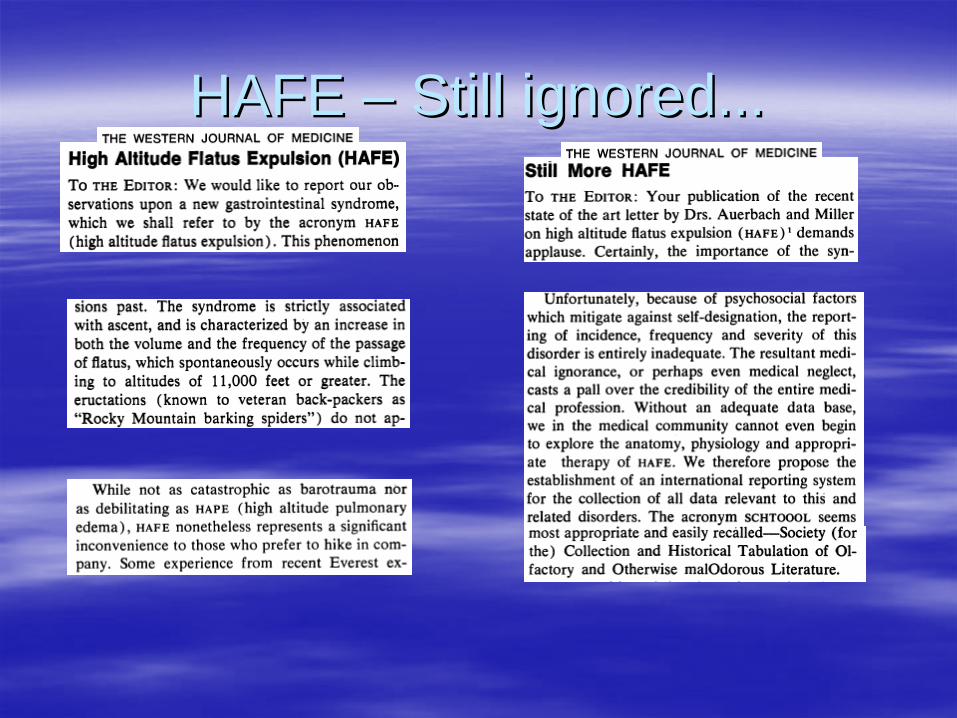
HAFE HAFE –– Still ignored...Still ignored...
Altitude associated illness Altitude associated illness –– Diagnosis and TreatmentDiagnosis and Treatment
Acute hypoxiaAcute hypoxiaAMS and HACEAMS and HACEHAPEHAPEDisordered breathingDisordered breathing
Acute hypoxiaAcute hypoxia
Rapid reaction to sudden drop in oxygen tension.Rapid reaction to sudden drop in oxygen tension.Occurs minutes to hours after exposureOccurs minutes to hours after exposureCan be triggered by exertion or other factors that Can be triggered by exertion or other factors that drop blood oxygen level while at altitude.drop blood oxygen level while at altitude.Dizziness, hallucinations, tinnitus, loss of Dizziness, hallucinations, tinnitus, loss of consciousness can occur.consciousness can occur.Almost guaranteed to occur in unacclimatized Almost guaranteed to occur in unacclimatized persons over ~5500mpersons over ~5500m
Acute hypoxia Acute hypoxia -- TreatmentTreatment
Descent and oxygen.Descent and oxygen.Correct causes or triggers of hypoxia.Correct causes or triggers of hypoxia.Encouraging hyperventilation can temporize.Encouraging hyperventilation can temporize.
Acute Mountain SicknessAcute Mountain Sickness
The bodyThe body’’s response to a sudden change in s response to a sudden change in oxygen pressure and subsequent modest oxygen pressure and subsequent modest hypoxaemia.hypoxaemia.Clinically differs from acute hypoxia.Clinically differs from acute hypoxia.–– Occurs 6 Occurs 6 –– 12 hours after elevation. 12 hours after elevation.
Results in a clinical syndrome characterized by:Results in a clinical syndrome characterized by:–– Headache which can progress to debilitating.Headache which can progress to debilitating.–– Fatigue which can progress to lassitude.Fatigue which can progress to lassitude.–– Insomnia, paroxysmal nocturnal breathing.Insomnia, paroxysmal nocturnal breathing.–– Poor appetite which can progress to vomitingPoor appetite which can progress to vomiting..
AMS AMS -- diagnosisdiagnosis
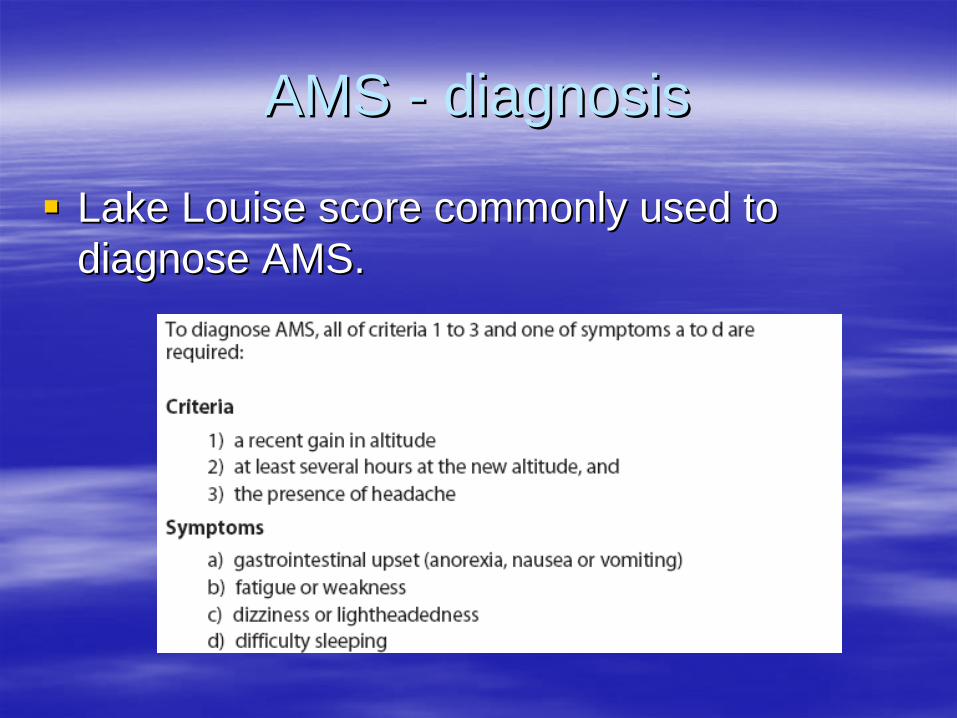
Lake Louise score commonly used to Lake Louise score commonly used to diagnose AMS.diagnose AMS.
Altitude headacheAltitude headache
Cardinal symptom of AMS.Cardinal symptom of AMS.–– Throbbing, frontal/bitemporalThrobbing, frontal/bitemporal–– Worse in morning and at night.Worse in morning and at night.–– PosturalPosturalSimilar to a Similar to a ““hangoverhangover”” headache in quality.headache in quality.
Disordered breathing and sleep Disordered breathing and sleep apneaapnea
Common finding at altitudes >3000mCommon finding at altitudes >3000mUsually in the form of periodic breathing and Usually in the form of periodic breathing and apnea during sleep.apnea during sleep.Leads to poor sleep, somnolence, Leads to poor sleep, somnolence, headache.headache.Caused by competing respiratory drives.Caused by competing respiratory drives.
High Altitude Cerebral EdemaHigh Altitude Cerebral Edema
HACE is endHACE is end--stage AMS:stage AMS:–– Hypoxia causes fluid leak into brain tissue, causing Hypoxia causes fluid leak into brain tissue, causing
brain swelling and inflammation.brain swelling and inflammation.
Symptoms are similar to AMS but more severe. Symptoms are similar to AMS but more severe. AMS with any of the following should be AMS with any of the following should be considered HACE.considered HACE.–– AtaxiaAtaxia–– ConfusionConfusion–– Altered consciousness/behaviourAltered consciousness/behaviour–– ComaComa–– Severe vomitingSevere vomiting
Treatment of AMSTreatment of AMS
The only 100% effective treatment for AMS The only 100% effective treatment for AMS is increasing oxygen pressure.is increasing oxygen pressure.–– This means This means descentdescent, , oxygen or a pressure chamber.oxygen or a pressure chamber.
Anybody with symptoms of HACE or severe Anybody with symptoms of HACE or severe AMS must descend!AMS must descend!–– Other modalities only adjunctiveOther modalities only adjunctive
Mild AMSMild AMS
Headache, nausea, fatigue, dizziness, insomnia Headache, nausea, fatigue, dizziness, insomnia can be treated symptomatically.can be treated symptomatically.–– NSAIDs and acetaminophen have been shown to be NSAIDs and acetaminophen have been shown to be
equivalent for headache.equivalent for headache.–– AntiAnti--emetics (prochlorperazine and promethazine)emetics (prochlorperazine and promethazine)–– Acetazolamide can be used to treat (250mg in two Acetazolamide can be used to treat (250mg in two
doses 8 hours apart)doses 8 hours apart)–– Sedatives or benzodiazepines may contribute to Sedatives or benzodiazepines may contribute to
disordered breathing.disordered breathing.
Severe AMSSevere AMS
Severe headache, vomiting, anorexia, Severe headache, vomiting, anorexia, peripheral oedema without HACE or HAPE.peripheral oedema without HACE or HAPE.–– Descent to lower altitude with acclimatization. Descent to lower altitude with acclimatization.
As little as 500 meters can be very helpful.As little as 500 meters can be very helpful.–– Acetazolamide 250mg then 250mg 8 hours Acetazolamide 250mg then 250mg 8 hours
later. later. –– Dexamethasone 4 mg every 6 hours.Dexamethasone 4 mg every 6 hours.
Combine with descent or acetazolamide!Combine with descent or acetazolamide!
–– Oxygen or pressure chamber to facilitate Oxygen or pressure chamber to facilitate descent.descent.
HACEHACE
Descent to lower altitude.Descent to lower altitude.Oxygen or pressure chamber to facilitate Oxygen or pressure chamber to facilitate descent.descent.Dexamethasone 4 mg every six hours after Dexamethasone 4 mg every six hours after 8mg loading dose.8mg loading dose.Furosemide and other diuretics can be Furosemide and other diuretics can be considered but quality evidence is lacking.considered but quality evidence is lacking.
High Altitude Pulmonary EdemaHigh Altitude Pulmonary Edema
Hypoxia and reduced pulmonary gas exchange Hypoxia and reduced pulmonary gas exchange increases pulmonary artery pressure and results in increases pulmonary artery pressure and results in capillaries leak into lungs.capillaries leak into lungs.–– Usually 2 Usually 2 –– 4 days after ascent.4 days after ascent.–– AMS not always coAMS not always co--existing.existing.–– Manifests as persistent dry cough, severe dyspnea and Manifests as persistent dry cough, severe dyspnea and
disproportionately limited exercise tolerance.disproportionately limited exercise tolerance.–– Fever (<38.5Fever (<38.5ººC), tachypnea and diffuse crackles are C), tachypnea and diffuse crackles are
common.common.–– Haemoptysis/pink sputum is late finding.Haemoptysis/pink sputum is late finding.
HAPE HAPE -- diagnosisdiagnosis
Two of: chest tightness, cough, dyspnea at Two of: chest tightness, cough, dyspnea at rest, and markedly decreased exercise rest, and markedly decreased exercise performance and...performance and...Two of: central cyanosis, pulmonary Two of: central cyanosis, pulmonary crackles, crackles, tachycardia >110 and tachypnea tachycardia >110 and tachypnea >20>20Caution with scoring systems!Caution with scoring systems!
HAPE HAPE -- TreatmentTreatment
Descent to lower altitude.Descent to lower altitude.Oxygen or pressure chamber to facilitate Oxygen or pressure chamber to facilitate descent.descent.Drugs play a small role in management.Drugs play a small role in management.–– Nifedipine XR 30mg BID, Nitric oxideNifedipine XR 30mg BID, Nitric oxide–– Furosemide with or without morphine (standard Furosemide with or without morphine (standard
of care for pulmonary oedema) remains of care for pulmonary oedema) remains controversial.controversial.
–– Role of dexamethasone is not clear.Role of dexamethasone is not clear.
Prediction and PreventionPrediction and Prevention
Who gets AMS?Who gets AMS?There is no way to predict who will get AMS.There is no way to predict who will get AMS.AMS does not typically occur below 2000m ASL.AMS does not typically occur below 2000m ASL.Faster ascents and group excursions more risky.Faster ascents and group excursions more risky.Younger people at highest risk.Younger people at highest risk.–– More vigorous ascents.More vigorous ascents.–– Less Less ““freefree”” intracranial space.intracranial space.
Personal history of AMS, HACE or HAPE.Personal history of AMS, HACE or HAPE.Residence below 900m.Residence below 900m.No apparent association with gender, physical No apparent association with gender, physical fitness, load.fitness, load.
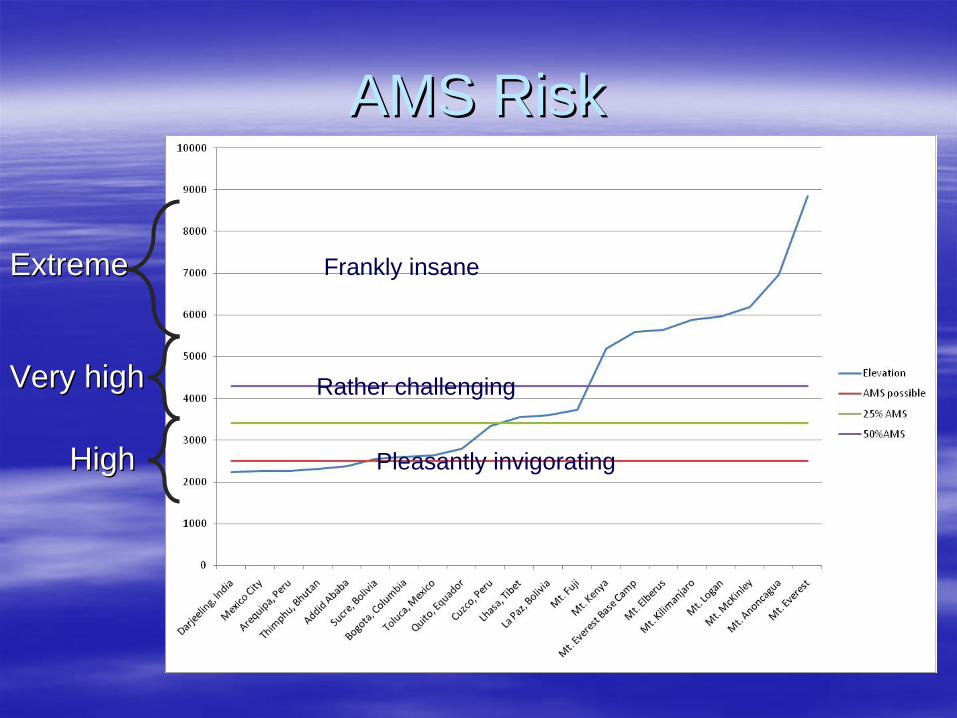
AMS RiskAMS Risk
HighHigh
Very highVery high
ExtremeExtreme
Pleasantly invigorating
Rather challenging
Frankly insane
Genetic basis of AMSGenetic basis of AMS
Genetically determined anatomical variations.Genetically determined anatomical variations.Activity of key enzymesActivity of key enzymes–– NO synthase in HAPENO synthase in HAPE–– ACE polymorphismsACE polymorphisms
Gender differences?Gender differences?–– Overall men more likely to get AMS Overall men more likely to get AMS –– behavioural.behavioural.–– No clear gender differences when other factors are No clear gender differences when other factors are
adjusted.adjusted.
Hereditary aspect of AMS.Hereditary aspect of AMS.
Prevention of AMS, HACE and Prevention of AMS, HACE and HAPEHAPE
BehaviourBehaviour–– Altering behaviour to reduce likelihood of AMS.Altering behaviour to reduce likelihood of AMS.PharmacologicalPharmacologicalPhysicalPhysical–– Methods to increase oxygen pressure.Methods to increase oxygen pressure.
BehaviouralBehavioural
Slow ascent with acclimatization points, especially Slow ascent with acclimatization points, especially at high altitude (>3000m).at high altitude (>3000m).–– 400m/ day is reasonable.400m/ day is reasonable.–– One acclimatization day for each 3 days of increase.One acclimatization day for each 3 days of increase.
NeverNever overnight at higher altitude than where overnight at higher altitude than where symptoms start. symptoms start. –– Climb high, sleep low.Climb high, sleep low.
Avoid sedatives or alcohol.Avoid sedatives or alcohol.Know the symptoms and ensure groups Know the symptoms and ensure groups understand individual variability. understand individual variability. Mild activity (no overexertion).Mild activity (no overexertion).
Diet?Diet?
High carbohydrate diet (carboHigh carbohydrate diet (carbo--loading) with >70% loading) with >70% of calories from carbohydrates reduces the risk of of calories from carbohydrates reduces the risk of AMS.AMS.Role of hydration and hyperhydration is in Role of hydration and hyperhydration is in question.question.–– Association exists between AMS and dehydration, but Association exists between AMS and dehydration, but
not apparently causal.not apparently causal.–– Dehydration can contribute to symptoms.Dehydration can contribute to symptoms.–– Adequate hydration probably helps acidAdequate hydration probably helps acid--base base
normalization.normalization.–– May prevent thromboembolic phenomena.May prevent thromboembolic phenomena.
Chemoprophylaxis of AMSChemoprophylaxis of AMS
AMSAMS–– Acetazolamide, dexamethasoneAcetazolamide, dexamethasoneHACEHACE–– Acetazolamide, dexamethasoneAcetazolamide, dexamethasoneHAPEHAPE–– Sildenafil, Tadadifil, Nifedipine, SalmeterolSildenafil, Tadadifil, Nifedipine, Salmeterol
AcetazolamideAcetazolamide
Carbonic anhydrase inhibitor.Carbonic anhydrase inhibitor.–– Increases renal output of bicarbonate causing metabolic Increases renal output of bicarbonate causing metabolic
acidosis.acidosis.–– Accelerates normal physiological changes in response Accelerates normal physiological changes in response
to altitude.to altitude.–– Stimulates ventilation (peripheral CA)Stimulates ventilation (peripheral CA)
125125--250mg po BID starting 24 hours pre250mg po BID starting 24 hours pre--ascent ascent and ending 48 hours after maximum altitude is and ending 48 hours after maximum altitude is effective for AMS prevention.effective for AMS prevention.Reduces severity of symptoms. Reduces severity of symptoms. –– Paroxysmal nocturnal breathing, insomnia, headacheParoxysmal nocturnal breathing, insomnia, headache..
AcetazolamideAcetazolamide
Indications:Indications:–– Rapid ascent to >3000m or rapid increase in sleep altitude (e.g.Rapid ascent to >3000m or rapid increase in sleep altitude (e.g.
4000 to 5000m in one day).4000 to 5000m in one day).–– Past history of AMS or HACE.Past history of AMS or HACE.
Side effects can be disturbing...Side effects can be disturbing...–– Annoying to painful paresthesias of fingers/toes.Annoying to painful paresthesias of fingers/toes.–– Taste alteration of carbonated beverages.Taste alteration of carbonated beverages.–– Diuresis, cloudy urine, nausea.Diuresis, cloudy urine, nausea.–– RARE: Myelosuppression, SJS, crytaluria.RARE: Myelosuppression, SJS, crytaluria.
Start with lowest effective dose (125 mg BID)Start with lowest effective dose (125 mg BID)People with sulfa allergy CAN take.People with sulfa allergy CAN take.
DexamethasoneDexamethasone
Considered second line due to side effects.Considered second line due to side effects.May prevent HACE and HAPE by reducing May prevent HACE and HAPE by reducing capillary leak and inflammation.capillary leak and inflammation.Reduces incidence of headache, vomiting.Reduces incidence of headache, vomiting.Is more effective when combined with Is more effective when combined with acetazolamide.acetazolamide.Dose for prevention is 4mg BID.Dose for prevention is 4mg BID.
NifedipineNifedipine
Should not be used to prevent HAPE.Should not be used to prevent HAPE.–– Only shown to be effective in preventing HAPE Only shown to be effective in preventing HAPE
in individuals with repeated history of HAPE in individuals with repeated history of HAPE going to high altitude.going to high altitude.
Recommended only in limited situations.Recommended only in limited situations.–– Individuals with recurrent HAPE and needing to Individuals with recurrent HAPE and needing to
go at high altitude without access to oxygen or go at high altitude without access to oxygen or ability for slow ascent.ability for slow ascent.
cGMP phosphodiesterase type 5 cGMP phosphodiesterase type 5 inhibitorsinhibitors
Sildenafil (ViagraSildenafil (Viagra™™) and Tadalafil (Cialis) and Tadalafil (Cialis™™) ) have been shown to be effective in have been shown to be effective in preventing HAPE and improving gas preventing HAPE and improving gas exchange and should be considered in exchange and should be considered in people with a history of HAPE who must people with a history of HAPE who must ascend rapidly.ascend rapidly.
ββ--adrenergic agonistsadrenergic agonists
Salmeterol, taken prophylactically at 125Salmeterol, taken prophylactically at 125μμg g every 12 hours reduced incidence of HAPE every 12 hours reduced incidence of HAPE by 50% in subjects with a previous episode by 50% in subjects with a previous episode of HAPE.of HAPE.
Other drugs for preventionOther drugs for prevention
Temazepam has been shown to reduce Temazepam has been shown to reduce periodic breathing.periodic breathing.Theophylline (caffeineTheophylline (caffeine--like analog) @ 250 like analog) @ 250 mg BID effective to reduce AMS.mg BID effective to reduce AMS.Sumatriptan reduced symptoms of AMS Sumatriptan reduced symptoms of AMS when taken prophylactically in one study.when taken prophylactically in one study.
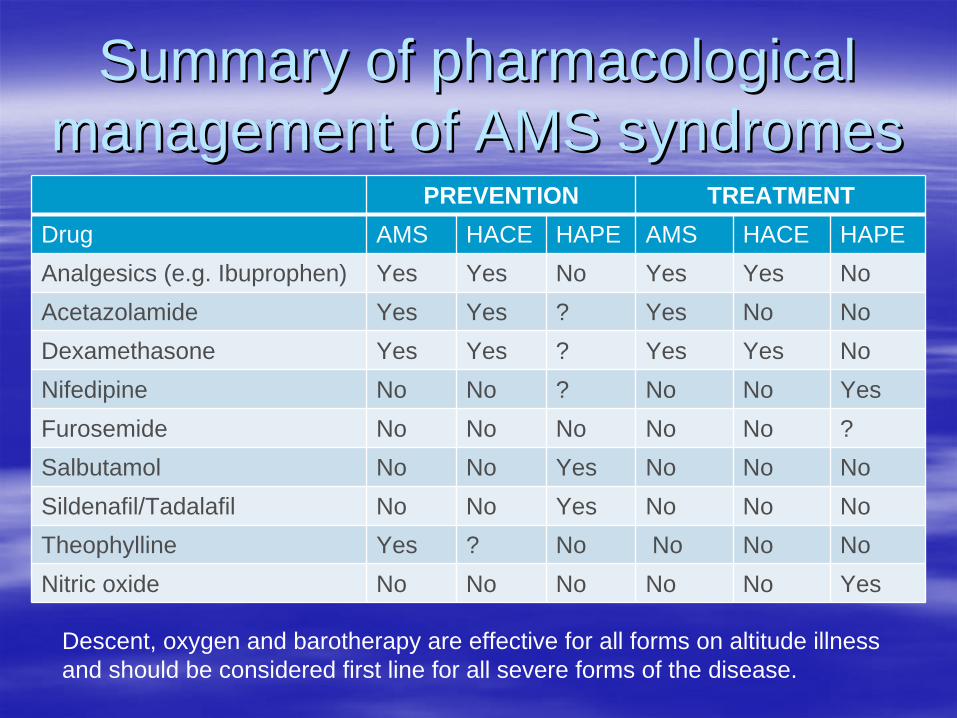
Summary of pharmacological Summary of pharmacological management of AMS syndromesmanagement of AMS syndromes
PREVENTION TREATMENTDrug AMS HACE HAPE AMS HACE HAPEAnalgesics (e.g. Ibuprophen) Yes Yes No Yes Yes NoAcetazolamide Yes Yes ? Yes No NoDexamethasone Yes Yes ? Yes Yes NoNifedipine No No ? No No YesFurosemide No No No No No ?Salbutamol No No Yes No No NoSildenafil/Tadalafil No No Yes No No NoTheophylline Yes ? No No No NoNitric oxide No No No No No Yes
Descent, oxygen and barotherapy are effective for all forms on altitude illness and should be considered first line for all severe forms of the disease.
Physical (oxygen)Physical (oxygen)
Use of oxygen as prevention for AMS is not Use of oxygen as prevention for AMS is not routine.routine.Used to prevent severe AMS at extreme Used to prevent severe AMS at extreme altitudesaltitudesUsed intermittently, nocturnally or Used intermittently, nocturnally or continuously.continuously.Used prophylactically on train to LhasaUsed prophylactically on train to Lhasa
Special populationsSpecial populations
Certain populations require special Certain populations require special considerations at high altitude:considerations at high altitude:–– ChildrenChildren–– Pregnant womenPregnant women–– DiabeticsDiabetics–– Underlying diseases of cardiovascular and Underlying diseases of cardiovascular and
respiratory system.respiratory system.
ChildrenChildren
May be more susceptible to AMS.May be more susceptible to AMS.–– Quality studies are lackingQuality studies are lackingDifficult to assess symptoms of AMS in Difficult to assess symptoms of AMS in young children.young children.Symptoms same in children over 8 years.Symptoms same in children over 8 years.–– Use Lake Louise ScoreUse Lake Louise ScoreModified Lake Louise score recommended Modified Lake Louise score recommended in children less than 8 years old.in children less than 8 years old.
Modified Lake Louise ScoreModified Lake Louise Score
Unexplained fussiness intensity and Unexplained fussiness intensity and amount.amount.How well child is eating.How well child is eating.How playful child is.How playful child is.How well child is sleeping.How well child is sleeping.
PregnancyPregnancy
Theoretical risks:Theoretical risks:–– Altitude = remotenessAltitude = remoteness
Access to care in case of complications, early Access to care in case of complications, early labour...labour...
–– Reduced oxygen delivery to foetusReduced oxygen delivery to foetus–– Dehydration and thrombosisDehydration and thrombosis
PregnancyPregnancy
Simulated altitude up to 2600 m doesnSimulated altitude up to 2600 m doesn’’t appear to t appear to harm the foetus.harm the foetus.–– Oxygen levels remain normal.Oxygen levels remain normal.–– Caution reasonable if there are complications.Caution reasonable if there are complications.
Women living at altitude have a higher than Women living at altitude have a higher than expected rate of miscarriage and LBW.expected rate of miscarriage and LBW.–– Reasons unclear, not significant in acute exposure.Reasons unclear, not significant in acute exposure.
Dehydration can exacerbate hypercoagulable Dehydration can exacerbate hypercoagulable state.state.Hypercoagulability after longHypercoagulability after long--term exposure.term exposure.
DiabetesDiabetes
Risk of AMS, HACE and HAPE appear no different.Risk of AMS, HACE and HAPE appear no different.Glycemic control is profoundly affected by exercise and Glycemic control is profoundly affected by exercise and altitude.altitude.–– Need very careful monitoring and expect poor control.Need very careful monitoring and expect poor control.–– Ketoacidosis can occurKetoacidosis can occur
Anorexia is common with altitude.Anorexia is common with altitude.
Temperature and environmental Temperature and environmental considerations.considerations.–– Medications, shivering etc...Medications, shivering etc...
Diabetes and AMS prophylaxisDiabetes and AMS prophylaxis
Acetazolamide can predispose individuals to Acetazolamide can predispose individuals to ketoacidosis.ketoacidosis.Dexamethosone causes hyperglycemia and Dexamethosone causes hyperglycemia and can lead to ketoacidosis.can lead to ketoacidosis.
COPDCOPD
Individuals with COPD and asthma cannot Individuals with COPD and asthma cannot compensate as well for hypoxia with compensate as well for hypoxia with hyperventilation.hyperventilation.With COPD, FEVWith COPD, FEV1 1 > 1.5L and expected > 1.5L and expected PaOPaO22 > 55mmHg> 55mmHg–– PaOPaO2Alt2Alt = (0.52PaO= (0.52PaO22 ) + (11.9FEV) + (11.9FEV11 ) ) –– 1.761.76
AsthmaAsthma
Patients with mild intermittent or mild persistent Patients with mild intermittent or mild persistent disease (controlled) may ascend to altitudes as disease (controlled) may ascend to altitudes as high as 5000 m.high as 5000 m.Caution patients with more severe disease against Caution patients with more severe disease against highhigh--altitude travel, particularly into remote areas.altitude travel, particularly into remote areas.–– Should have excellent controlShould have excellent control
Continue baseline medications and carry peak Continue baseline medications and carry peak flow meter and supply of rescue inhalers and flow meter and supply of rescue inhalers and prednisone for potential exacerbationsprednisone for potential exacerbationsConsider using balaclava or bandana over mouth Consider using balaclava or bandana over mouth to warm and humidify air in cold environments.to warm and humidify air in cold environments.
Pulmonary hypertensionPulmonary hypertension
Should be counselled against going to high Should be counselled against going to high altitude. altitude. No trials to assess risk, but theoretical risk No trials to assess risk, but theoretical risk of HAPE.of HAPE.If travel not avoidable, use HAPE If travel not avoidable, use HAPE prophylaxis, oxygen.prophylaxis, oxygen.
Angina, CAD and Heart FailureAngina, CAD and Heart Failure
No increased risk of AMS, HACE or HAPE.No increased risk of AMS, HACE or HAPE.Higher risk of effort angina and dysrythmia.Higher risk of effort angina and dysrythmia.Minimal exertion at moderate altitude in well Minimal exertion at moderate altitude in well compensated patients is low risk.compensated patients is low risk.RecommendationsRecommendations–– Gradual ascent. Gradual ascent. –– Ensure BP, heart rate/rhythm control. Ensure BP, heart rate/rhythm control. –– Limitation of activity to less than the symptomLimitation of activity to less than the symptom--limiting limiting
degree at sea level, especially during the first 1 to 3 degree at sea level, especially during the first 1 to 3 days.days.
Angina, CAD and Heart FailureAngina, CAD and Heart Failure
Counsel against high altitude if:Counsel against high altitude if:–– NewNew--onset or unstable angina. onset or unstable angina. –– Frequent or highFrequent or high--grade ventricular ectopy.grade ventricular ectopy.–– Severe or poorly controlled hypertension.Severe or poorly controlled hypertension.–– CoCo--existing pulmonary diseaseexisting pulmonary diseaseMyocardial infarction within several weeks Myocardial infarction within several weeks or months is a relative contraindication.or months is a relative contraindication.
Take home pointsTake home points
Altitude sickness is preventable.Altitude sickness is preventable.–– Behavioural and pharmacological approaches exist.Behavioural and pharmacological approaches exist.
People travelling to areas above 2500 m should People travelling to areas above 2500 m should be aware of altitude sickness.be aware of altitude sickness.People going to very high altitude, who are People going to very high altitude, who are anxious about altitude sickness or who are anxious about altitude sickness or who are pregnant or have underlying pulmonary, cardiac or pregnant or have underlying pulmonary, cardiac or chronic disease should be referred to an expert.chronic disease should be referred to an expert.
ReferencesReferences1.1. Basnyat B. High altitude cerebral and pulmonary edema. Travel MeBasnyat B. High altitude cerebral and pulmonary edema. Travel Med Infect Dis 2005;3:199d Infect Dis 2005;3:199--211.211.2.2. Basnyat B, Gertsch JH, Holck PS, et al. Acetazolamide 125 mg BD Basnyat B, Gertsch JH, Holck PS, et al. Acetazolamide 125 mg BD is not significantly different from 375 mg BD in the is not significantly different from 375 mg BD in the
prevention of acute mountain sickness: the prophylactic acetazolprevention of acute mountain sickness: the prophylactic acetazolamide dosage comparison for efficacy (PACE) trial. amide dosage comparison for efficacy (PACE) trial. High Alt Med Biol 2006;7:17High Alt Med Biol 2006;7:17--27.27.
3.3. Basnyat B, Hargrove J, Holck PS, et al. Acetazolamide fails to dBasnyat B, Hargrove J, Holck PS, et al. Acetazolamide fails to decrease pulmonary artery pressure at high altitude in ecrease pulmonary artery pressure at high altitude in partially acclimatized humans. High Alt Med Biol 2008;9:209partially acclimatized humans. High Alt Med Biol 2008;9:209--16.16.
4.4. Basnyat B, Murdoch DR. HighBasnyat B, Murdoch DR. High--altitude illness. Lancet 2003;361:1967altitude illness. Lancet 2003;361:1967--74.74.5.5. Basu M, Sawhney RC, Kumar S, Pal K, Prasad R, Selvamurthy W. GluBasu M, Sawhney RC, Kumar S, Pal K, Prasad R, Selvamurthy W. Glucocorticoids as prophylaxis against acute cocorticoids as prophylaxis against acute
mountain sickness. Clin Endocrinol (Oxf) 2002;57:761mountain sickness. Clin Endocrinol (Oxf) 2002;57:761--7.7.6.6. Brubaker PL. Adventure travel and type 1 diabetes: the complicatBrubaker PL. Adventure travel and type 1 diabetes: the complicating effects of high altitude. Diabetes Care ing effects of high altitude. Diabetes Care
2005;28:25632005;28:2563--72.72.7.7. Carlsten C, Swenson ER, Ruoss S. A doseCarlsten C, Swenson ER, Ruoss S. A dose--response study of acetazolamide for acute mountain sickness propresponse study of acetazolamide for acute mountain sickness prophylaxis hylaxis
in vacationing tourists at 12,000 feet (3630 m). High Alt Med Biin vacationing tourists at 12,000 feet (3630 m). High Alt Med Biol 2004;5:33ol 2004;5:33--9.9.8.8. Fischer R, Lang SM, Leitl M, Thiere M, Steiner U, Huber RM. TheoFischer R, Lang SM, Leitl M, Thiere M, Steiner U, Huber RM. Theophylline and acetazolamide reduce sleepphylline and acetazolamide reduce sleep--disordered disordered
breathing at high altitude. Eur Respir J 2004;23:47breathing at high altitude. Eur Respir J 2004;23:47--52.52.9.9. Gertsch JH, Basnyat B, Johnson EW, Onopa J, Holck PS. RandomisedGertsch JH, Basnyat B, Johnson EW, Onopa J, Holck PS. Randomised, double blind, placebo controlled comparison of , double blind, placebo controlled comparison of
ginkgo biloba and acetazolamide for prevention of acute mountainginkgo biloba and acetazolamide for prevention of acute mountain sickness among Himalayan trekkers: the prevention sickness among Himalayan trekkers: the prevention of high altitude illness trial (PHAIT). Bmj 2004;328:797.of high altitude illness trial (PHAIT). Bmj 2004;328:797.
10.10. Hackett PH, Rennie D, Levine HD. The incidence, importance, and Hackett PH, Rennie D, Levine HD. The incidence, importance, and prophylaxis of acute mountain sickness. Lancet prophylaxis of acute mountain sickness. Lancet 1976;2:11491976;2:1149--55.55.
11.11. Harris NS, Wenzel RP, Thomas SH. High altitude headache: efficacHarris NS, Wenzel RP, Thomas SH. High altitude headache: efficacy of acetaminophen vs. ibuprofen in a randomized, y of acetaminophen vs. ibuprofen in a randomized, controlled trial. J Emerg Med 2003;24:383controlled trial. J Emerg Med 2003;24:383--7.7.
12.12. Kotwal J, Apte CV, Kotwal A, Mukherjee B, Jayaram J. High altituKotwal J, Apte CV, Kotwal A, Mukherjee B, Jayaram J. High altitude: a hypercoagulable state: results of a prospective de: a hypercoagulable state: results of a prospective cohort study. Thromb Res 2007;120:391cohort study. Thromb Res 2007;120:391--7.7.
13.13. Kupper TE, Strohl KP, Hoefer M, Gieseler U, Netzer CM, Netzer NCKupper TE, Strohl KP, Hoefer M, Gieseler U, Netzer CM, Netzer NC. Low. Low--dose theophylline reduces symptoms of dose theophylline reduces symptoms of acute mountain sickness. J Travel Med 2008;15:307acute mountain sickness. J Travel Med 2008;15:307--14.14.
14.14. Leaf DE, Goldfarb DS. Mechanisms of action of acetazolamide in tLeaf DE, Goldfarb DS. Mechanisms of action of acetazolamide in the prophylaxis and treatment of acute mountain he prophylaxis and treatment of acute mountain sickness. J Appl Physiol 2007;102:1313sickness. J Appl Physiol 2007;102:1313--22.22.
15.15. Luks AM, Swenson ER. Travel to high altitude with preLuks AM, Swenson ER. Travel to high altitude with pre--existing lung disease. Eur Respir J 2007;29:770existing lung disease. Eur Respir J 2007;29:770--92.92.16.16. Maggiorini M, BrunnerMaggiorini M, Brunner--La Rocca HP, Peth S, et al. Both tadalafil and dexamethasone mayLa Rocca HP, Peth S, et al. Both tadalafil and dexamethasone may reduce the incidence of reduce the incidence of
highhigh--altitude pulmonary edema: a randomized trial. Ann Intern Med 200altitude pulmonary edema: a randomized trial. Ann Intern Med 2006;145:4976;145:497--506.506.17.17. Moraga FA, Flores A, Serra J, Esnaola C, Barriento C. Ginkgo bilMoraga FA, Flores A, Serra J, Esnaola C, Barriento C. Ginkgo biloba decreases acute mountain sickness in people oba decreases acute mountain sickness in people
ascending to high altitude at Ollague (3696 m) in northern Chileascending to high altitude at Ollague (3696 m) in northern Chile. Wilderness Environ Med 2007;18:251. Wilderness Environ Med 2007;18:251--7.7.18.18. Nerin MA, Palop J, Montano JA, Morandeira JR, Vazquez M. Acute mNerin MA, Palop J, Montano JA, Morandeira JR, Vazquez M. Acute mountain sickness: influence of fluid intake. ountain sickness: influence of fluid intake.
Wilderness Environ Med 2006;17:215Wilderness Environ Med 2006;17:215--20.20.19.19. Oelz O, Maggiorini M, Ritter M, et al. Nifedipine for high altitOelz O, Maggiorini M, Ritter M, et al. Nifedipine for high altitude pulmonary oedema. Lancet 1989;2:1241ude pulmonary oedema. Lancet 1989;2:1241--4.4.20.20. Rock PB, Johnson TS, Larsen RF, Fulco CS, Trad LA, Cymerman A. DRock PB, Johnson TS, Larsen RF, Fulco CS, Trad LA, Cymerman A. Dexamethasone as prophylaxis for acute examethasone as prophylaxis for acute
mountain sickness. Effect of dose level. Chest 1989;95:568mountain sickness. Effect of dose level. Chest 1989;95:568--73.73.21.21. Rodway GW, Hoffman LA, Sanders MH. HighRodway GW, Hoffman LA, Sanders MH. High--altitudealtitude--related disordersrelated disorders----Part II: prevention, special populations, and Part II: prevention, special populations, and
chronic medical conditions. Heart Lung 2004;33:3chronic medical conditions. Heart Lung 2004;33:3--12.12.22.22. Rodway GW, Hoffman LA, Sanders MH. HighRodway GW, Hoffman LA, Sanders MH. High--altitudealtitude--related disordersrelated disorders----Part I: Pathophysiology, differential diagnosis, Part I: Pathophysiology, differential diagnosis,
and treatment. Heart Lung 2003;32:353and treatment. Heart Lung 2003;32:353--9.9.23.23. Sartori C, Allemann Y, Duplain H, et al. Salmeterol for the prevSartori C, Allemann Y, Duplain H, et al. Salmeterol for the prevention of highention of high--altitude pulmonary edema. N Engl J Med altitude pulmonary edema. N Engl J Med
2002;346:16312002;346:1631--6.6.24.24. Schoene RB. Illnesses at high altitude. Chest 2008;134:402Schoene RB. Illnesses at high altitude. Chest 2008;134:402--16.16.25.25. Stream JO, Grissom CK. Update on highStream JO, Grissom CK. Update on high--altitude pulmonary edema: pathogenesis, prevention, and treatmenaltitude pulmonary edema: pathogenesis, prevention, and treatment. t.
Wilderness Environ Med 2008;19:293Wilderness Environ Med 2008;19:293--303.303.26.26. Swenson ER. Carbonic anhydrase inhibitors and hypoxic pulmonary Swenson ER. Carbonic anhydrase inhibitors and hypoxic pulmonary vasoconstriction. Respir Physiol Neurobiol vasoconstriction. Respir Physiol Neurobiol
2006;151:2092006;151:209--16.16.27.27. Swenson ER, Teppema LJ. Prevention of acute mountain sickness bySwenson ER, Teppema LJ. Prevention of acute mountain sickness by acetazolamide: as yet an unfinished story. J acetazolamide: as yet an unfinished story. J
Appl Physiol 2007;102:1305Appl Physiol 2007;102:1305--7.7.28.28. Wright A, Brearey S, Imray C. High hopes at high altitudes: pharWright A, Brearey S, Imray C. High hopes at high altitudes: pharmacotherapy for acute mountain sickness and highmacotherapy for acute mountain sickness and high--
altitude cerebral and pulmonary oedema. Expert Opin Pharmacotheraltitude cerebral and pulmonary oedema. Expert Opin Pharmacother 2008;9:1192008;9:119--27.27.29.29. Ziaee V, Yunesian M, Ahmadinejad Z, et al. Acute mountain sickneZiaee V, Yunesian M, Ahmadinejad Z, et al. Acute mountain sickness in Iranian trekkers around Mount Damavand ss in Iranian trekkers around Mount Damavand
(5671 m) in Iran. Wilderness Environ Med 2003;14:214(5671 m) in Iran. Wilderness Environ Med 2003;14:214--9.9.
