alzheimer’s disease and myelin
DESCRIPTION
Alzheimer’s Disease and Myelin. February 2012 Jason Su. Outline. WM degeneration in AD Connection between WM and GM New developments in WM/myelin imaging Myelin imaging in MS with mcDESPOT Highly sensitive to early changes The myelin hypothesis in AD - PowerPoint PPT PresentationTRANSCRIPT

Alzheimer’s Disease and Myelin
February 2012Jason Su

Outline
• WM degeneration in AD– Connection between WM and GM
• New developments in WM/myelin imaging• Myelin imaging in MS with mcDESPOT
– Highly sensitive to early changes• The myelin hypothesis in AD
– How might we design a study to prove or disprove it?

WM Damage in AD and Its Relationship to GM Atrophy
Agosta, Filippi, et. al. (Milan)
• AD is a disease that affects both GM and WM• Some WM loss may precedes GM: there may be a mix
of primary and secondary myelin degeneration involved in AD

Goals
• Use DTI to explore WM in probable AD patients and amnesic mild cognitive impairment (aMCI)– Correlate this with GM atrophy
• Previously, DTI has shown higher mean diffusivity (MD) and lower fractional anisotropy (FA) in AD– Temporal, parietal, and some frontal lobes– Are these changes primary or secondary to GM
atrophy?
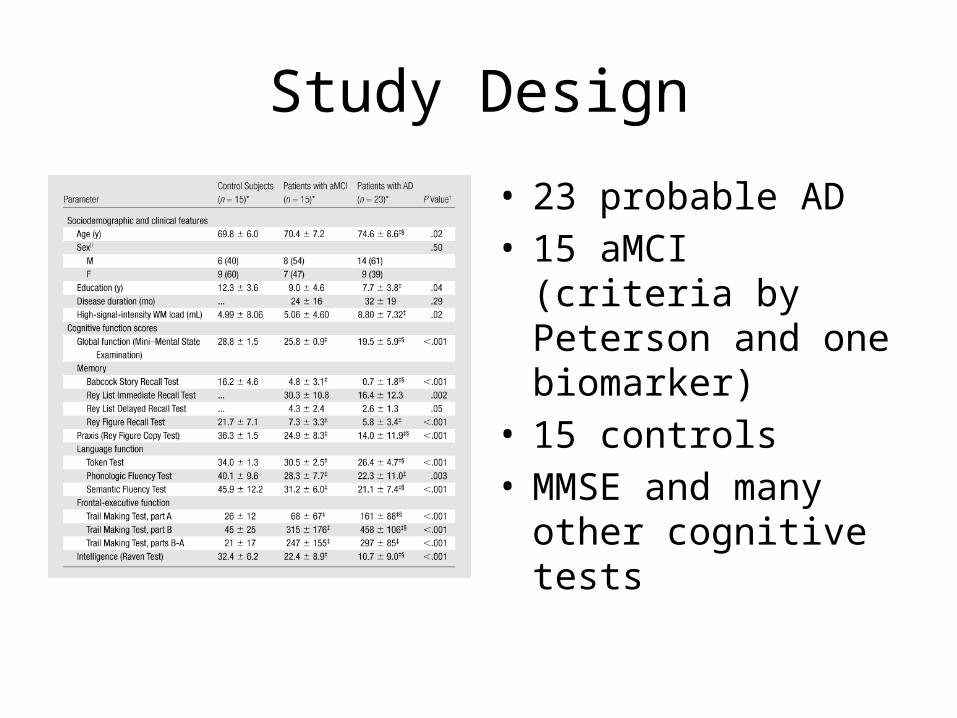
Study Design
• 23 probable AD• 15 aMCI (criteria by
Peterson and one biomarker)
• 15 controls• MMSE and many other
cognitive tests
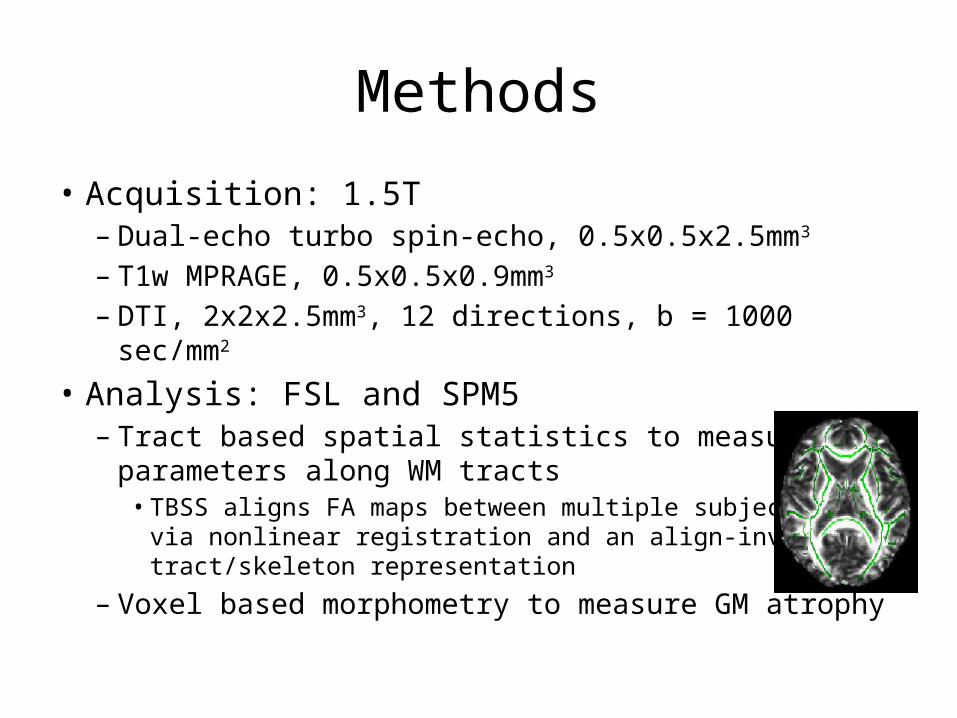
Methods
• Acquisition: 1.5T– Dual-echo turbo spin-echo, 0.5x0.5x2.5mm3
– T1w MPRAGE, 0.5x0.5x0.9mm3
– DTI, 2x2x2.5mm3, 12 directions, b = 1000 sec/mm2
• Analysis: FSL and SPM5– Tract based spatial statistics to measure DTI parameters
along WM tracts• TBSS aligns FA maps between multiple subjects
via nonlinear registration and an align-invariant tract/skeleton representation
– Voxel based morphometry to measure GM atrophy

Results – DTI• Probable AD vs Control
– MD: significant differences in all major WM tracts studied (limbic, cortico-cortical association, interhemispheric)
• Parahippocampal, inferior longitudinal fasciculus and splenium had most tract involvement– FA: no significant differences– Axial and radial: widespread differences, radial diffusivity changes in large portions
of tract• aMCI vs Control
– MD: no differences– FA: no differences– Axial: some differences in various fasciluci and corpus callosum but less tract
involvement than AD• AD vs aMCI
– No differences
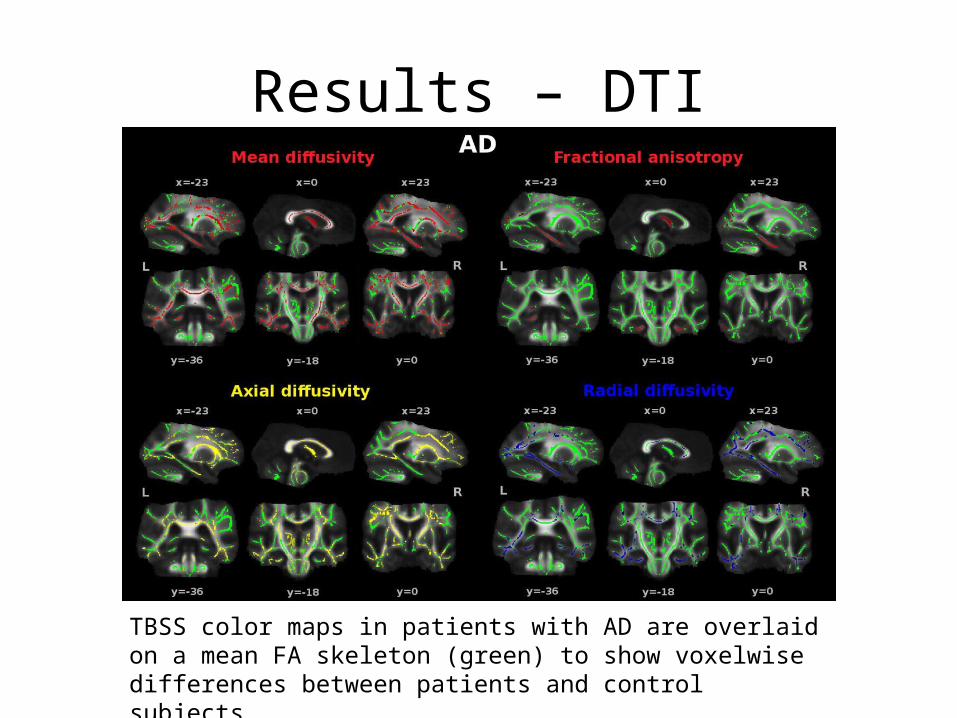
Results – DTI
TBSS color maps in patients with AD are overlaid on a mean FA skeleton (green) to show voxelwise differences between patients and control subjects.

Results – DTI
TBSS color maps in patients with aMCI are overlaid on a mean FA skeleton (green) to show voxelwise differences in axial diffusivity between groups.

Results – VBM
• AD vs Control– Significant loss in temporal lobes, thalami, bilateral
fontrol cortex, and left occipital cortex• aMCI vs Control
– Significant loss in left anterior hippocampus and fusiform gyrus
– Some loss in hippocampus and parahippocampal gyrus• AD vs aMCI
– No differences

Results – WM and GM
• AD: mean MD in splenium and parahippocampal tract correlated with hippocampus and parahippocampal gyrus volume
• aMCI: no correlation– Widespread increase in
axial diffusivity but GM is relatively spared
GM atrophy (cyan) and WM axial diffusivity changes (red).

Discussion
• Axial diffusivity is a potential early marker• Correlation of WM and GM in parahippocampus
consistent with secondary degeneration model• However, several WM tracts not correlated with
GM atrophy, especially in aMCI– May be indicative of primary WM degeneration– Perhaps some WM patterns are secondary, others
primary– Worthy further study!

Relaxation Based Myelin Imaging• DTI is not an ideal measure
of myelin (low resolution, crossing fibers problem)
• T2 (or R2) has been used in the past as a crude correlate of myelin– Myelination reduces water
content in brain, lower T2 – T2w FLAIR is used in MS to
highlight lesions– T2 mapping gives a more
sensitive indicator

Myelin Water FractionRecent methods have focused on a more specific measure: myelin water fraction (MWF)• Multiecho qT2 – vary TE, decomposes the
signal into a spectrum of T2 times (UBC, MacKay)
– Well validated way to produce MWF maps that represent myelin
– Few slices, long acquisition time• mcDESPOT – vary flip angle, models SPGR
and SSFP steady state signal– Also based on modeling relaxation and two pool
exchange– Validation in progress– High resolution, whole brain, but long
processing time (24 hours)
• Intra- and extra-cellular water, T2 ≈ 80ms
• Myelin water, T2 ≈ 20ms

FA vs MWF (UBC)
FA map (3.0 T), myelin-water (MW) map (3.0 T), MD map

mcDESPOT Maps in NormalT1single T1fast MWF
T2single T2slow
T1slow
T2fast Residence Time
0 – 0.234
0 – 137ms
0 – 555ms
0 – 9.26ms
0 – 1172ms
0 – 123ms
0 – 2345ms
0 – 328ms

MCDESPOT-DERIVED MWF IMPROVES EDSS PREDICTION IN MS PATIENTS COMPARED TO ATROPHY MEASURES ALONEJ.Su1, H.H.Kitzler2, M.Zeineh1, S.C.Deoni3, C.Harper-Little2, A.Leung2, M.Kremenchutzky2, and B.K.Rutt1
1Stanford U, CA, USA, 2TU Dresden, SN, Germany, 2U of Western Ontario, ON, Canada, 3Brown U, RI, USA
ISMRM 2011 E-POSTER #4643
• Highly sensitive to early changes in pre-MS patients, well before global atrophy is evident

Purpose
• To apply mcDESPOT, a whole-brain, myelin-selective, multi-component relaxometric imaging method, in a pilot MS study
• Assess if the method can explain differences in disease course and severity by uncovering the burden of disease in normal-appearing white matter (NAWM)
MCDESPOT-DERIVED MWF IMPROVES EDSS PREDICTION IN MS PATIENTS COMPARED TO ATROPHY MEASURES ALONEISMRM 2011 #4643

Study
Demographic Data Healthy Controls
All Patients CIS RRMS SPMS PPMS
N 26 26 10 5 6 5
Mean age, yr(SD)
42(13)
49(12)
41(12)
48(12)
58(7)
55(7)
Male/Female ratio 10/16 7/19 3/7 0/5 0/6 4/1
Mean disease duration, yr(SD)
—14
(13)2
(2)15
(10)28(8)
20(12)
Mean EDSS score(SD) —
3.6(2.4)
1.7(0.9)
2.0(1.7)
6.4(1.1)
5.6(1.1)
MCDESPOT-DERIVED MWF IMPROVES EDSS PREDICTION IN MS PATIENTS COMPARED TO ATROPHY MEASURES ALONEISMRM 2011 #4643

Processing Methods: Demyelination
• Non-linearly register mcDESPOT MWF maps to MNI152 standard space
• Combine normals together to form mean and standard deviation MWF volumes
• For each subject, calculate a z-score ([x – μ]/σ) at every voxel to determine if it is significantly demyelinated, i.e. MWF < -4σ below the mean
Demyelinated Voxels
MCDESPOT-DERIVED MWF IMPROVES EDSS PREDICTION IN MS PATIENTS COMPARED TO ATROPHY MEASURES ALONEISMRM 2011 #4643

Segmentations and DVFLAIR NAWM DAWM Lesions
MWF DemyelinatedVoxels
WM
DV in NAWM DV in DAWM DV in Lesions
MCDESPOT-DERIVED MWF IMPROVES EDSS PREDICTION IN MS PATIENTS COMPARED TO ATROPHY MEASURES ALONEISMRM 2011 #4643

Results: DVF in Compartments• Dotted line shows
demyelinated volume fraction in WM for healthy controls
• With DVF, all patient subclasses were significantly different from healthy controls
• PVF, however, fails to distinguish CIS and RR patients from normals
MCDESPOT-DERIVED MWF IMPROVES EDSS PREDICTION IN MS PATIENTS COMPARED TO ATROPHY MEASURES ALONEISMRM 2011 #4643

Characteristics of AD
• Afflicts >50% of people over 85• Age and ApoE4 allele are the primary risk factors for
late-onset AD• Deposition of extracellular Aβ plaques and
intracellular tau tangles– Aβ is produced by two acts of cleavage of APP, first by β-
site APP cleavage enzyme 1 (BACE1) then γ-secretase• Treatment of amyloid plaques has shown little
improvement of symptoms for Alzheimer’s patients

Alzheimer’s disease as homeostatic responses to age-related
myelin breakdown
George Bartzokis (UCLA)

The Myelin Hypothesis
• Myelin enables higher level functions in brain, AD is a disease where these facilities are progressively degraded
• Disruption in the myelin repair mechanism leads to a cascade resulting in the “Alzheimerization” of the brain– Repair failure caused by age (oligodendrocyte
vulnerability) or genetics (ApoE4)– Accumulation of plaques and tangles– Memory loss and language difficulty

Disrupted Myelin Repair
The Myelin Hypothesis: Myelin Breakdown
• Myelination in brain follows inverted-U shape, peaked at middle age
• Normal aging is strongly associated with myelin loss• Oligodendrocytes are uniquely vulnerable to
accumulation of toxins and free radicals with age because they consume 2-3x more energy than other brain cells
• Later myelinated temporal and frontal lobes are thinner: develop lesions first (recapitulation)

The Myelin Hypothesis: Failed Repair
• BACE1 accumulates, cleaves neuroregulin to signal oligodendrocytes to myelinate
• Repair of myelin depends on transport of cholesterol by ApoE, ApoE4 is poorer transporter than ApoE2/3
• Aβ and tau deposition are a byproduct of myelin repair processes that are failing to keep up with the “Alzheimerization” of the brain

The Myelin Hypothesis: Treatment
• Offers a unifying theme why traditional therapies that reduce amyloid are ineffective
• Treatments should be “upstream” of Aβ and tau formation: maintain myelin health and resilience, do not entirely inhibit BACE1

Myelin Imaging and AD• Many of the hypotheses derived from the myelin model need
further assessment in prospective studies to help determine causality– Aβ and tau deposits, the development and breakdown of myelin, as
well as important risk factors such as ferritin iron levels can be imaged with increasing specificity
• Questions we can explore with myelin imaging like mcDESPOT:– Can disease severity be linked to myelin (or MWF) loss, especially on a
spatial level? Cross-sectional– How closely does myelin loss follow the pattern of recapitulation?
Cross-sectional or longitudinal– How do existing treatments like BACE1 inhibitors affect myelin?
Longitudinal

ADmcDESPOT• Hypothesis: myelin loss is a precursor/predicts the development of
Aβ plaques and tau tangles• Longitudinal study, have to avoid CT or PET?• Imaging methods:
– MWF imaging via mcDESPOT– DTI– Amyloid PET?
• Aβ and tau concentrations in CSF as crude measures
• Questions– How active is plaque/tangle development in AD? How finely should we
sample in time?– Besides MMSE, what are vital cognitive measures?– What are the normal diagnostic imaging tools for AD?

References• Agosta F, Pievani M, Sala S, Geroldi C, Galluzzi S, Frisoni GB, Filippi M. “White matter
damage in Alzheimer disease and its relationship to gray matter atrophy.” Radiology. 2011 Mar;258(3):853-63. Epub 2010 Dec 21.
• Bartzokis G, Cummings JL, Sultzer D, Henderson VW, Nuechterlein KH, Mintz J. “White matter structural integrity in healthy aging adults and patients with Alzheimer disease: a magnetic resonance imaging study.” Arch Neurol. 2003 Mar;60(3):393-8.
• Mädler B, Drabycz SA, Kolind SH, Whittall KP, MacKay AL. “Is diffusion anisotropy an accurate monitor of myelination? Correlation of multicomponent T2 relaxation and diffusion tensor anisotropy in human brain.” Magn Reson Imaging. 2008 Sep;26(7):874-88. Epub 2008 Jun 4.
• Kitzler HH, Su J, Zeineh M, Harper-Little C, Leung A, Kremenchutzky M, Deoni SC, Rutt BK. “Deficient MWF mapping in multiple sclerosis using 3D whole-brain multi-component relaxation MRI.” Neuroimage. 2012 Feb 1;59(3):2670-7. Epub 2011 Sep 2.
• Bartzokis G. “Alzheimer's disease as homeostatic responses to age-related myelin breakdown.” Neurobiol Aging. 2011 Aug;32(8):1341-71. Epub 2009 Sep 22.