ameloblastoma in children
TRANSCRIPT

Surgical Management of Ameloblastoma in Children

AuthorsI-Yueh Huang, DDS, MS,a Sheng-
Tsung Lai, DDS,b Chung-Ho Chen, DDS,c
Chun-Ming Chen, DDS, MS,d Chung-Wei Wu, DDS, MS,e and Yee-Hsiung Shen, DDS,f
Kaohsiung, TaiwanKAOHSIUNG MEDICAL
UNIVERSITY

Objective
The purpose of this study was to report experience in the treatment of ameloblastoma in Taiwanese children and to discuss the treatment regimen
Study design
Fifteen patients, all younger than 18 years of age, with a diagnosis of ameloblastoma in our department between January 1991 and December 2004 were selected for study. Data included sex, age at surgery, tumor type, size and site of lesion, primary surgical methods, use of adjuvant therapy, complications, recurrences, and course of follow-up.
ResultsAges ranged from 9 to 17 (average was 13.7
years). Nine were male, 6 were female; the sex ratio was 1.5:1.
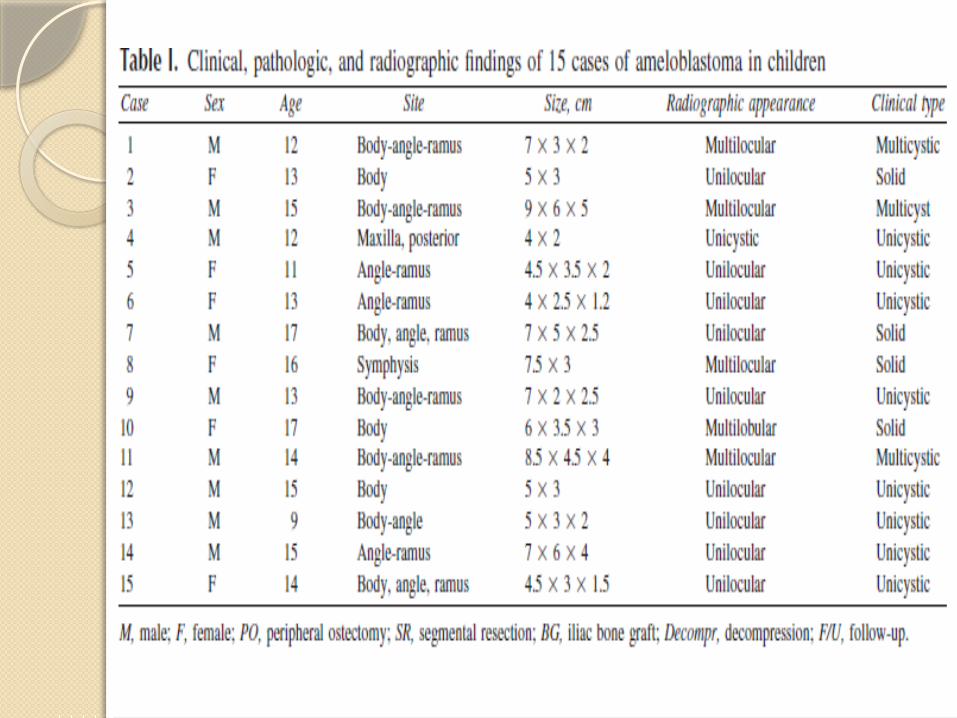
Fourteen lesions were in the mandible (1 in the symphysis, 13 in the mandibular posterior area) and only 1 was in the maxilla. The size of the lesions ranged from 4*2.5 cm to 8*8 cm. Clinical typing included 8 unicystic type, 3 multicystic type, and 4 solid types. Of the histologic types, 5 were plexiform, 3 were mixed type, and 3 were acanthomatous type. Complications included numbness of the lower lip and contour defect of the face. Three cases (20%) were recurrent, and 1 patient had 2 recurrences.
Conclusions Good results can be achieved in the
treatment of ameloblastoma in children using conservative surgery.
In the event of recurrence, a second surgery can be successful. Patient compliance and careful follow-up are important.
(Oral Surgery Oral Medicine Oral Pathology Oral Radiology Endodontology 2007;104:478-85)

Ameloblastoma is the most common aggressive benign odontogenic tumor of the jaws.
The tumor is often asymptomatic, presenting as a slowly enlarging facial swelling or an incidental finding on a radiograph. The physical presence of the tumor may cause symptoms such as pain, malocclusion, loosening of teeth, or ulceration. Ameloblastoma is a locally destructive tumor with a propensity for recurrence if not entirely excised.
A few cases of malignant change with distant metastasis have been reported in the literature.
It occurs in all age groups but the lesion is most commonly diagnosed in the third and fourth decades.
The tumor is considered a rarity in the young, but the tumor grows slowly and probably starts to develop in childhood
The treatment for ameloblastoma is stillcontroversial and poses some special
problems in children.Because of growth of the jaw, the
different incidence,behavior, and prognosis of the tumor make the surgical consideration different from adults. Some reports have encouraged aggressive resection for ameloblastoma in children, and some studies showed simple curettage had good results.

The aim of this study was to review a series of ameloblastoma in Taiwanese children, and to present our experience of surgical treatment in this pediatric group. We hope this report may contribute to further meta-analysis and develop a more rational surgical protocol for ameloblastoma in children.

PATIENTS AND MATERIALS
Of 223 patients with ameloblastoma, 15 (6.8%) were 18 years or younger when presenting to our department, and surgery was performed during the period January1991 to December 2004. We reviewed patient age and sex, anatomical distribution and size of the lesions, histologic types, clinical types, surgical methods, recurrence, complications, and outcome.

All patients underwent incisional biopsy before the surgery. Three surgical techniques were used:
(1) Enucleation with peripheral ostectomy,
(2) Decompression before enucleation with peripheral ostectomy, and
(3) Segmental resection with immediate iliac bone graft.
Enucleation with peripheral ostectomy
Enucleation with peripheral ostectomy was performed from an intraoral approach; the lesion being removed along the junction of the lesion and bone, and then peripheral bone was carefully trimmed off for 3 to 5 mm with a large round bone burr, including any septa for multicystic and solid types. The wound was packed open for 2 weeks, then the obturator was constructed and the patient instructed to irrigate the cavity with boiled water or normal saline. The wound was then allowed to heal secondarily or the cavity was filled with artificial bone substitutes and primary closure.
Decompression before enucleation withperipheral ostectomy
Decompression before enucleation with peripheral ostectomy was used when the lesion was found to be cystlike on biopsy, and the pathology report confirmed ameloblastoma. After 1 week, when the patient returned for the biopsy report, the benefits and risks of this plan would be discussed; if the patient understood the plan and agreed to comply, decompression would be used as a first measure. Under local anesthesia, a mucoperiosteal flap would be reflected to expose the lesion, and a bony window made of adequate size to allow opening of every loculation.
A decompression plug would be inserted (Fig. 1), and the wound closed.
Patients were taught to irrigate the cavity through the hole in the plug after each meal. Follow-up was arranged monthly with radiographic follow-up at 3 months to evaluate change and bony regeneration.
From 6 to 12 months later, enucleation with peripheral ostectomy would be performed under general anesthesia.
Postoperative care was similar to that discussed in the previous section “Enucleation with peripheral ostectomy.”



Segmental resection with immediate iliacbone graft
In segmental resection with immediate iliac bone graft, the extraoral resection was made through the mandible with a 1-cm margin of healthy bone. The reconstruction plate and iliac bone graft were placed immediately for 6 weeks of intermaxillary fixation.
This technique was used for all solid-type and multicystic lesions with involvement of the lower border or posterior border of the mandible, and when patients and parents chose radical surgery to decrease the chance of recurrence

RESULTS
Of the 15 patients, 9 were male and 6 were female, a ratio of 1.5:1.
The mean age was 13.7 years (range from 9 to 17 years). The angle region (body-angleramus) was the most common site (10 of 15, or 66.6%), followed by
Mandibular body (3 of 15, or 20%), Symphysis(1 of 15, 6.7%), Maxilla (1 of 15, 6.7%). The clinical types were as
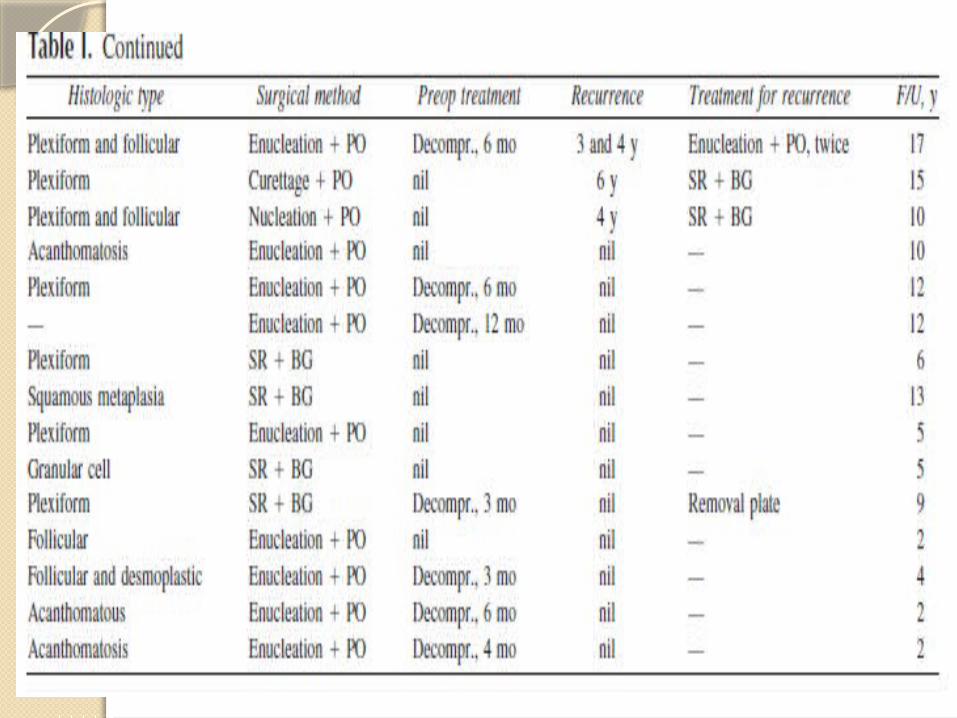
follows: 8 of 15 were unicystic (53.3%), 3 were multicystic (20%), and 4 were solid tumors (26.7%). Pathologic typing showed 5 to be plexiform, 3 mixed, and 3 were acanthomatous type. Sizes of the lesions ranged from 4*2 cm to 8*8 cm.
(Table I).

Treatments were direct enucleation and peripheral ostectomy for 5 cases (3 unicystic, 1 multicystic, and 1 solid type); decompression before enucleation with peripheral ostectomy for 6 cases (5 unicystic type and 1 multicystic type); and segmental resection and iliac bone graft for 4 cases (3 solid and 1 multicystic type, which had decompression surgery first, but did not respond to the treatment in 3 months and it was decided to initiate segmental resection and bone graft).
No unicystic type recurred
Two of 3 multicystic-type cases were recurrent. Of the 4 patients with solid type, 1 treated with enucleation and bone trimming was recurrent and then had segmental resection and bone graft 6 years later (when the patient was 19 years old), and no recurrence thereafter.
Another 3 solid types with segmental sectioning and bone grafts were not recurrent. In total, 3 cases had 4 recurrences

Radiographic findings showed 10 monolocular lesions and 5 multilocular radiolucent lesions. There were 2 solid-type lesions presented in monolocular and multilocular image groups. The follow-up period was from 2 years to 17 years. Complications, including mild facial deformity and permanent lip numbness were noted in all patients with segmental resection and bone grafts. Only 2 cases had permanent lip numbness after enucleation and peripheral ostectomy.
DISCUSSION Ameloblastoma is uncommon in the pediatric
population,with only 8.7% to 15% of all ameloblastomas in Western countries. The Asian and African reports show a higher percentage, ranging from 14.6% to 25%.3,10 Because ameloblastoma is uncommon, only a few surgeons have much experience in treating this lesion. The extent of surgical excision of mandibular ameloblastoma has been the subject of debate for many years. Many recent reports have warned of high recurrence rates (75%-90%) with conservative treatment, compared with recurrence rates of 15% to 25% after radical surgery.
One report shows a high success rate of tumor resection, reconstruction, and rehabilitation for pediatric patients, and declared that the current standard of care is en bloc resection with wide margins to prevent recurrence, with staged reconstruction with bone grafts and an implant-supported prosthesis.

Ameloblastoma is usually classified into 3 types:solid or multicystic, unicystic, and peripheral. Thecystic type of ameloblastoma is predominant in youngpatients. The multicystic and solid lesions are sometimesconsidered as one type because of similar behavior,with a locally invasive tumor and high recurrencerate, and are usually excised radically. We would ratherclassify ameloblastoma into 4 clinical types for pediatricpatients: solid, multicystic, unicystic, and peripheral.We suggest the multicystic type should be treatedconservatively as different lesions, especially for children.

For multicystic ameloblastoma, many reports suggest radical surgery where the buccal and lingual bone plates are sacrificed along with their periosteum and any suspicious surrounding soft tissue being removed. 3 patients with multicystic type were treated by 3 different methods. The first patient, a 12-year-old boy (Fig. 2), had decompression treatment for 6 months and then accepted enucleation and peripheral ostectomy.



The lesion recurred 3 years later (Fig. 4), and he had a secondary operation with enucleation and bone trimming. Four years after the second surgery (Fig. 5),



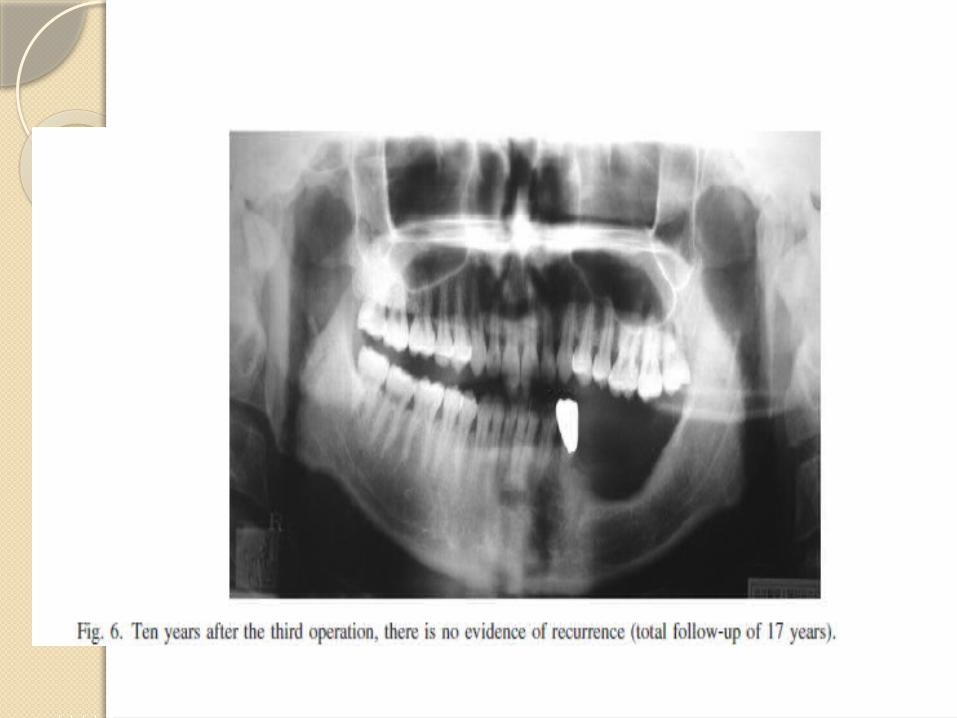
Four years after the second surgery (Fig. 5), it recurred again and he had a third operation (same procedures), and was monitored for another 10 years (Fig. 6), for a total of 17 years of follow-up. No recurrence has been noted so far. The first operation was performed under general anesthesia; the second and third operations were done under local anesthesia.
The patient and his parents were satisfied with the treatment, and there was no lip numbness, a limited number of teeth were removed, and there was no functional disturbance or esthetic problem.