american association of immunologists recommendations for
TRANSCRIPT
an Undergraduate Course in ImmunologyAmerican Association of Immunologists Recommendations for
Swanson-Mungerson, Steven M. Varga and Julie M. JamesonEdith Porter, Eyal Amiel, Nandita Bose, Andrea Bottaro, William H. Carr, Michelle
http://www.immunohorizons.org/content/5/6/448https://doi.org/10.4049/immunohorizons.2100030doi:
2021, 5 (6) 448-465ImmunoHorizons
This information is current as of December 10, 2021.
Referenceshttp://www.immunohorizons.org/content/5/6/448.full#ref-list-1
, 1 of which you can access for free at: cites 13 articlesThis article
Email Alertshttp://www.immunohorizons.org/alertsReceive free email-alerts when new articles cite this article. Sign up at:
ISSN 2573-7732.All rights reserved.1451 Rockville Pike, Suite 650, Rockville, MD 20852The American Association of Immunologists, Inc.,
is an open access journal published byImmunoHorizons
by guest on Decem
ber 10, 2021http://w
ww
.imm
unohorizons.org/D
ownloaded from
by guest on D
ecember 10, 2021
http://ww
w.im
munohorizons.org/
Dow
nloaded from
American Association of Immunologists Recommendations foran Undergraduate Course in Immunology
Edith Porter,* Eyal Amiel,† Nandita Bose,‡ Andrea Bottaro,§ William H. Carr,{ Michelle Swanson-Mungerson,k
Steven M. Varga,#,**,†† and Julie M. Jameson‡‡
*Department of Biological Sciences, California State University Los Angeles, Los Angeles, CA; †Department of Biomedical and Health
Sciences, University of Vermont, Burlington, VT; ‡HiberCell, Inc., Roseville, MN; §Department of Biomedical Sciences, Cooper Medical School
of Rowan University, Camden, NJ; {Department of Biology, Medgar Evers College, City University of New York, Brooklyn, NY; kDepartment
of Microbiology and Immunology, Chicago College of Osteopathic Medicine, Midwestern University, Downers Grove, IL; #Department of
Microbiology and Immunology, University of Iowa, Iowa City, IA; **Interdisciplinary Graduate Program in Immunology, University of Iowa,
Iowa City, IA; ††Department of Pathology, University of Iowa, Iowa City, IA; and ‡‡Department of Biological Sciences, California State
University San Marcos, San Marcos, CA
ABSTRACT
Identifying the �essential� components of an undergraduate immunology lecture course can be daunting because of the varying
postgraduate pathways students take. The American Association of Immunologists Education Committee commissioned an Ad Hoc
Committee, representing undergraduate, graduate, and medical institutions as well as the biotechnology community, to develop core
curricular recommendations for teaching immunology to undergraduates. In a reiterative process involving the American Association of
Immunologists teaching community, 14 key topics were identified and expanded to include foundational concepts, subtopics and
examples, and advanced subtopics, providing a flexible list for curriculum development and avenues for higher-level learning.
Recommendations for inclusive and antiracist teaching that outline opportunities to meet the needs of diverse student populations were
also developed. The consensus recommendations can be used to accommodate various course settings and will bridge undergraduate
and graduate teaching and prepare diverse students for subsequent careers in the biomedical field. ImmunoHorizons, 2021, 5: 448–465.
INTRODUCTION
Immunology is challenging to teach in the undergraduate set-ting because of its rapidly advancing and expanding field ofknowledge. The task of defining the key components of anundergraduate curriculum in immunology can be overwhelm-ing to undergraduate educators, who are often challenged tocover the �essential� components of this vast field of sciencethrough a combination of smaller units in general biologycourses or within a single semester-long introductory course (1,2). Few resources are available that use a methodical approachto capture the key topics for inclusion in the course. In
recognition of the critical need for enhanced guidance onundergraduate immunology curricular development, severalrecent publications have begun the process of advocacy arounda more-unified approach to undergraduate immunology educa-tion (3, 4). Of note, a recent study that reported the results ofsurveyed immunology educators has helped identify currentcurricular practices by experienced instructors, which hashighlighted curricular priorities for both course and curriculumdesign for the field (5). All of these efforts are rooted in thepremise that broader attention to a cohesive set of key conceptsand evidence-based curriculum design leads to improved stu-dent understanding and outcomes (5, 6). Professional scientific
Received for publication March 25, 2021. Accepted for publication April 22, 2021.
Address correspondence and reprint requests to: Prof. Edith Porter, California State University Los Angeles, BS 143, 5151 State University Drive, Los Angeles,CA 90032. E-mail address: [email protected]
ORCIDs: 0000-0002-4656-5264 (E.P.); 0000-0002-1578-8705 (E.A.); 0000-0003-1712-6796 (A.B.); 0000-0003-1987-9070 (W.H.C.); 0000-0001-6384-6933(M.S.-M.); 0000-0001-7332-4290 (S.M.V.); 0000-0003-0727-4066 (J.M.J.).
Abbreviations used in this article: AAI, American Association of Immunologists; ITIG, Immunology Teaching Interest Group.
This article is distributed under the terms of the CC BY-NC-ND 4.0 Unported license.
Copyright © 2021 The Authors
448 https://doi.org/10.4049/immunohorizons.2100030
ImmunoHorizons is published by The American Association of Immunologists, Inc.
ON THE HORIZON
by guest on Decem
ber 10, 2021http://w
ww
.imm
unohorizons.org/D
ownloaded from
societies are uniquely poised to engage in broad curricular rec-ommendations for their field based on the breadth of theirmembership expertise and the depth of their communicationplatform to reach a broad section of researchers, educators, andprofessionals in the field (7, 8). In response to the perceivedneed among immunology educators, the American Associationof Immunologists (AAI) has undertaken a process to provide ageneral set of core recommendations for an undergraduate cur-riculum in the field of immunology. Ideally, curriculum guide-lines would be developed with a top-down strategy identifyingkey topics that could be covered in shorter course modules andexpanded subtopics that could be included in full-semestercourses. Additionally, educators at the next level of learning
(i.e., medical schools, graduate schools) or in the future workenvironment (i.e., biotechnology and pharmaceutical sectors)should have a seat at the table for decisions on key topics tomake the undergraduate curriculum relevant. This reverseengineering strategy will provide the knowledge needed in theundergraduate curriculum to succeed at these higher levels. Tomeet these goals, the AAI Education Committee has embarkedon a mission to gain broad community consensus on an under-graduate immunology curriculum that bridges undergraduateeducation and postgraduate education/career-relevant needs.
Starting in 2016, the AAI Education Committee initiated anew annual meeting session focused on improving immunologyeducation: the Immunology Teaching Interest Group (ITIG).This Education Committee--sponsored session has been dedi-cated to sharing novel teaching practices for immunology edu-cation at undergraduate, graduate, and medical schools. ITIGspeakers and attendees have included immunology educatorsspanning a range of institution types and serving students ofdifferent levels. The ITIG session has become a venue for theexchange of ideas and a way to provide suggestions to the AAIcommunity as a whole. The group has grown from 20 partici-pants in 2016 to more than 200 in 2020. Novel ideas and cut-ting-edge teaching strategies have been shared at the AAIAnnual Meeting and in a special section of the AAI Newsletterthat is dedicated to pedagogy. The rising interest in immunol-ogy education is also reflected in recently published articles,which have begun to highlight effective teaching pedagogiesand topics to cover (4, 9, 10).
The AAI Education Committee received input from theITIG highlighting a need for a comprehensive set of cur-ricular guidelines for teaching immunology at the under-graduate level. In 2019, the Education Committee formedan Ad Hoc Committee to establish recommendations forundergraduate immunology instruction with the goal ofproviding a guide for instructors in immunology that willbridge undergraduate and graduate teaching and preparestudents for subsequent careers in the biomedical andhealthcare fields as well as other areas applicable to immu-nology. The Ad Hoc Committee was composed of educa-tors from primarily undergraduate academic institutions,educators in various healthcare sectors, and a member ofthe biotechnology community. The recommendations wereinitially developed through consultation among the sub-committee members and then thoroughly vetted by ITIGmembers through a series of survey iterations, individualconsultation, and a virtual workshop. The strength of theserecommendations lies in the vetting and broad consensusachieved by engaging over 70 immunologists in a variety ofprofessional roles and the flexible structure to allow forinnovations and autonomy of topic emphasis within thecurriculum.
In this article, we first describe the methodology used forcurriculum content development, which may be useful for otherdisciplines aiming to develop curriculum recommendations forcomplex, interdisciplinary subjects. Then we present the
AHCKey topics
ITIGSurvey and
working groups
AHCRefinement
ITIGSurvey and workshop
AHCFinalization
AAI ECReview
AAI Council
Broader dissemination
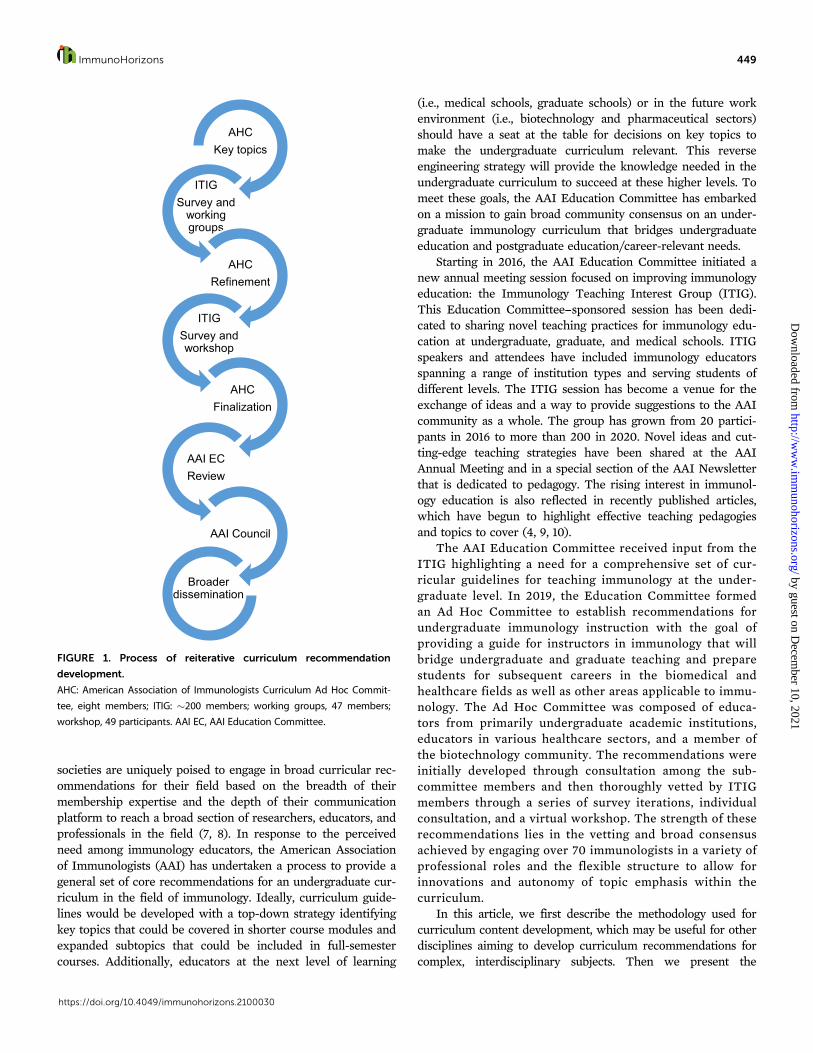
FIGURE 1. Process of reiterative curriculum recommendation
development.
AHC: American Association of Immunologists Curriculum Ad Hoc Commit-
tee, eight members; ITIG: �200 members; working groups, 47 members;
workshop, 49 participants. AAI EC, AAI Education Committee.
ImmunoHorizons 449
https://doi.org/10.4049/immunohorizons.2100030
by guest on Decem
ber 10, 2021http://w
ww
.imm
unohorizons.org/D
ownloaded from
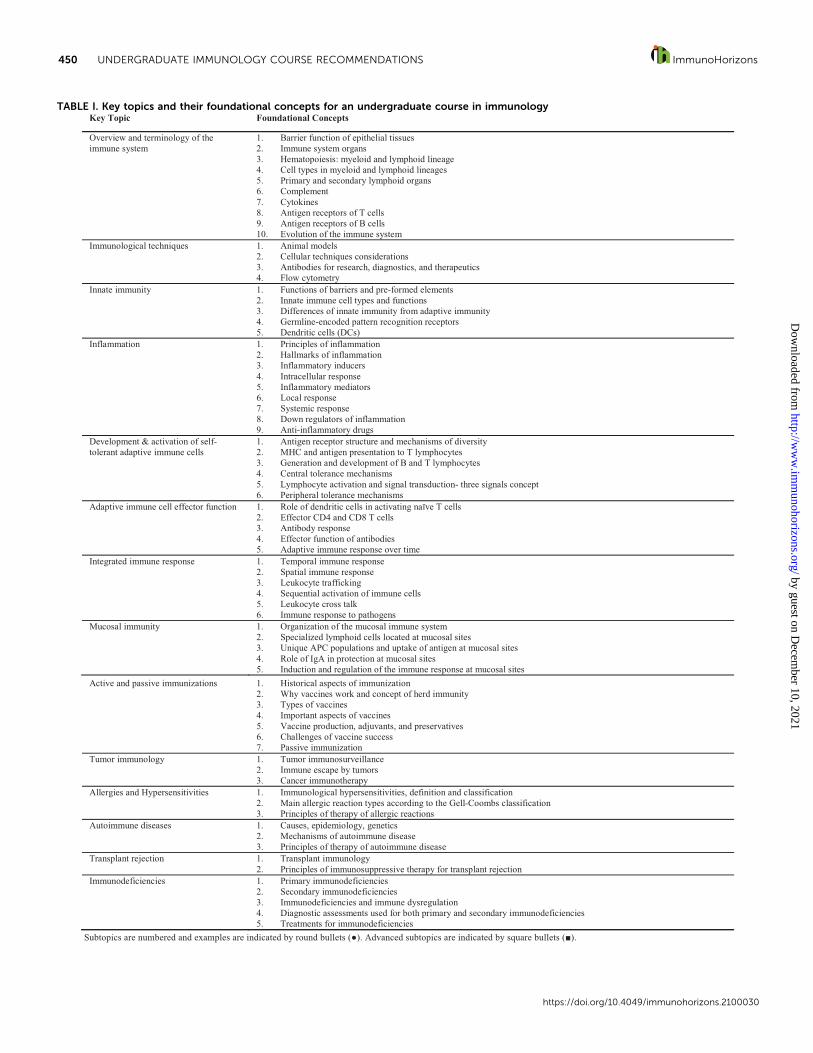
TABLE I. Key topics and their foundational concepts for an undergraduate course in immunologyKey Topic Foundational Concepts
Overview and terminology of the immune system
1. Barrier function of epithelial tissues 2. Immune system organs 3. Hematopoiesis: myeloid and lymphoid lineage 4. Cell types in myeloid and lymphoid lineages 5. Primary and secondary lymphoid organs 6. Complement 7. Cytokines 8. Antigen receptors of T cells 9. Antigen receptors of B cells 10. Evolution of the immune system
Immunological techniques 1. Animal models 2. Cellular techniques considerations 3. Antibodies for research, diagnostics, and therapeutics 4. Flow cytometry
Innate immunity 1. Functions of barriers and pre-formed elements 2. Innate immune cell types and functions 3. Differences of innate immunity from adaptive immunity 4. Germline-encoded pattern recognition receptors 5. Dendritic cells (DCs)
Inflammation 1. Principles of inflammation 2. Hallmarks of inflammation 3. Inflammatory inducers 4. Intracellular response 5. Inflammatory mediators 6. Local response 7. Systemic response 8. Down regulators of inflammation 9. Anti-inflammatory drugs
Development & activation of self-tolerant adaptive immune cells
1. Antigen receptor structure and mechanisms of diversity 2. MHC and antigen presentation to T lymphocytes 3. Generation and development of B and T lymphocytes 4. Central tolerance mechanisms 5. Lymphocyte activation and signal transduction- three signals concept 6. Peripheral tolerance mechanisms
Adaptive immune cell effector function 1. Role of dendritic cells in activating naïve T cells 2. Effector CD4 and CD8 T cells 3. Antibody response 4. Effector function of antibodies 5. Adaptive immune response over time
Integrated immune response 1. Temporal immune response 2. Spatial immune response 3. Leukocyte trafficking 4. Sequential activation of immune cells 5. Leukocyte cross talk 6. Immune response to pathogens
Mucosal immunity 1. Organization of the mucosal immune system 2. Specialized lymphoid cells located at mucosal sites 3. Unique APC populations and uptake of antigen at mucosal sites 4. Role of IgA in protection at mucosal sites 5. Induction and regulation of the immune response at mucosal sites
Active and passive immunizations 1. Historical aspects of immunization2. Why vaccines work and concept of herd immunity3. Types of vaccines4. Important aspects of vaccines5. Vaccine production, adjuvants, and preservatives6. Challenges of vaccine success7. Passive immunization
Tumor immunology 1. Tumor immunosurveillance2. Immune escape by tumors3. Cancer immunotherapy
Allergies and Hypersensitivities 1. Immunological hypersensitivities, definition and classification2. Main allergic reaction types according to the Gell-Coombs classification3. Principles of therapy of allergic reactions
Autoimmune diseases 1. Causes, epidemiology, genetics2. Mechanisms of autoimmune disease3. Principles of therapy of autoimmune disease
Transplant rejection 1. Transplant immunology2. Principles of immunosuppressive therapy for transplant rejection
Immunodeficiencies
Subtopics are numbered and examples are indicated by round bullets (●). Advanced subtopics are indicated by square bullets (■).
1. Primary immunodeficiencies2. Secondary immunodeficiencies3. Immunodeficiencies and immune dysregulation4. Diagnostic assessments used for both primary and secondary immunodeficiencies5. Treatments for immunodeficiencies
450 UNDERGRADUATE IMMUNOLOGY COURSE RECOMMENDATIONS ImmunoHorizons
https://doi.org/10.4049/immunohorizons.2100030
by guest on Decem
ber 10, 2021http://w
ww
.imm
unohorizons.org/D
ownloaded from
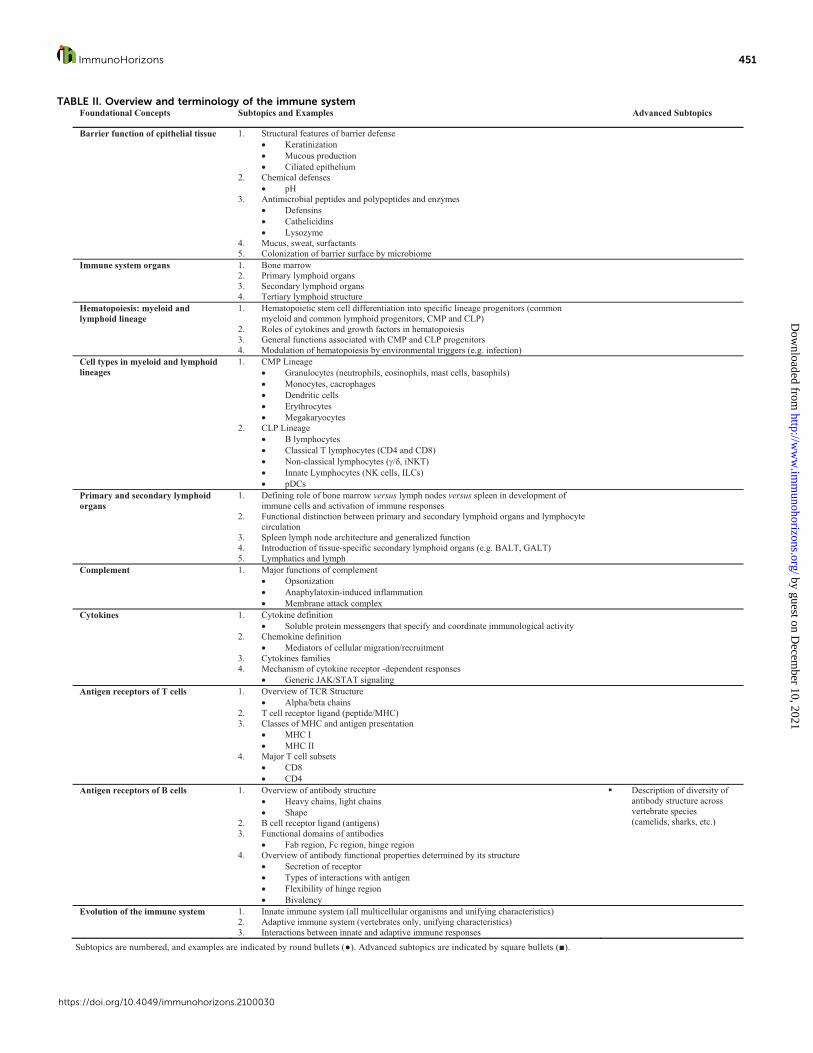
TABLE II. Overview and terminology of the immune systemFoundational Concepts Subtopics and Examples Advanced Subtopics
Barrier function of epithelial tissue 1. Structural features of barrier defense • Keratinization • Mucous production • Ciliated epithelium
2. Chemical defenses • pH
3. Antimicrobial peptides and polypeptides and enzymes • Defensins • Cathelicidins • Lysozyme
4. Mucus, sweat, surfactants 5. Colonization of barrier surface by microbiome
Immune system organs 1. Bone marrow 2. Primary lymphoid organs 3. Secondary lymphoid organs 4. Tertiary lymphoid structure
Hematopoiesis: myeloid and lymphoid lineage
1. Hematopoietic stem cell differentiation into specific lineage progenitors (common myeloid and common lymphoid progenitors, CMP and CLP)
2. Roles of cytokines and growth factors in hematopoiesis 3. General functions associated with CMP and CLP progenitors 4. Modulation of hematopoiesis by environmental triggers (e.g. infection)
Cell types in myeloid and lymphoid lineages
1. CMP Lineage • Granulocytes (neutrophils, eosinophils, mast cells, basophils) • Monocytes, cacrophages • Dendritic cells • Erythrocytes • Megakaryocytes
2. CLP Lineage • B lymphocytes • Classical T lymphocytes (CD4 and CD8) • Non-classical lymphocytes (γ/δ, iNKT) • Innate Lymphocytes (NK cells, ILCs) • pDCs
Primary and secondary lymphoid organs
1. Defining role of bone marrow versus lymph nodes versus spleen in development of immune cells and activation of immune responses
2. Functional distinction between primary and secondary lymphoid organs and lymphocyte circulation
3. Spleen lymph node architecture and generalized function 4. Introduction of tissue-specific secondary lymphoid organs (e.g. BALT, GALT) 5. Lymphatics and lymph
Complement
1. Major functions of complement • Opsonization • Anaphylatoxin-induced inflammation • Membrane attack complex
Cytokines 1. Cytokine definition • Soluble protein messengers that specify and coordinate immunological activity
2. Chemokine definition • Mediators of cellular migration/recruitment
3. Cytokines families 4. Mechanism of cytokine receptor -dependent responses
• Generic JAK/STAT signaling
Antigen receptors of T cells 1. Overview of TCR Structure • Alpha/beta chains
2. T cell receptor ligand (peptide/MHC) 3. Classes of MHC and antigen presentation
• MHC I • MHC II
4. Major T cell subsets • CD8 • CD4
Antigen receptors of B cells 1. Overview of antibody structure • Heavy chains, light chains • Shape
2. B cell receptor ligand (antigens) 3. Functional domains of antibodies
• Fab region, Fc region, hinge region 4. Overview of antibody functional properties determined by its structure
• Secretion of receptor • Types of interactions with antigen • Flexibility of hinge region • Bivalency
� Description of diversity of antibody structure across vertebrate species (camelids, sharks, etc.)
Evolution of the immune system 1. Innate immune system (all multicellular organisms and unifying characteristics) 2. Adaptive immune system (vertebrates only, unifying characteristics) 3. Interactions between innate and adaptive immune responses
Subtopics are numbered, and examples are indicated by round bullets (●). Advanced subtopics are indicated by square bullets (■).
ImmunoHorizons 451
https://doi.org/10.4049/immunohorizons.2100030
by guest on Decem
ber 10, 2021http://w
ww
.imm
unohorizons.org/D
ownloaded from

recommendations for curriculum content, as well as additionalresources for further classroom enrichment, compiled from asurvey of the AAI teaching community. Finally, we as educatorsare not only responsible for the scientific content in our coursesbut are also obligated by a responsibility to convey this contentin an equitable manner to serve a diverse student population aseffectively as possible. To speak to these principles, we haveincluded recommendations for antiracist and inclusive teachingwith a few examples of how to translate this desire into peda-gogy. The intent of the AAI Ad Hoc Committee and ITIG mem-bers is to provide a resource for new as well as seasonedundergraduate immunology instructors for curriculum develop-ment and curriculum improvement.
Process of recommendations developmentThe development of the recommendations was a highlyinclusive and reiterative process (Fig. 1) designed toensure that the recommendations would reflect topics thatimmunologists highly prioritize and bridge undergraduateand graduate immunology education. In October 2019, theAAI Education Committee formed an eight-member AdHoc Committee composed of current and former AAI Edu-cation Committee members representing undergraduate,graduate, and medical school educators as well as a mem-ber of the biotech industry. The Ad Hoc Committee cre-ated a list of key topics informed by current textbookcontent (11--16), other resources, requirements at the
graduate/medical school level, needs for biotechnologyand biomedical careers, and their own teaching experien-ces. These resources were selected based on individualexperiences and not from a targeted validation study.Absence from the sources cited in this article does notreflect an intentional decision against inclusion. In Decem-ber 2019, a survey was sent out to all members of the ITIG(203) for initial feedback to the suggested key topics (78responses) and to recruit team members (47 volunteered)to define foundational concepts, determine subtopics, andidentify examples in small working groups. Subsequently,in January 2020, working groups were formed with threeor four participants facilitated by one Ad Hoc Committeemember. Each working group included at least one under-graduate educator and one educator from a graduateschool. From April to May 2020, the Ad Hoc Committeemembers compiled the working group recommendations,removed redundancies, sequenced the individual topics,and uniformly formatted the document. A second surveywas sent out to the ITIG (10 responses) in June 2020, andthe Ad Hoc Committee further refined the recommenda-tions. Finally, the draft document was shared with theITIG, and the ITIG was invited to provide written feed-back and participate in a virtual workshop to further dis-cuss the recommendations. This 3-h workshop (49 ITIGattendees) took place on July 24, 2020. In breakout ses-sions dedicated to one or two key topics and facilitated by
TABLE III. Immunological techniquesFoundational Concepts Subtopics and Examples Advanced Subtopics
Animal models 1. Human studies: advantages versus disadvantages2. Brief overview of different animal models that can be used to study immunological
concepts • Knock-out• Knock-in
� Other types of animal models beyond k/o and knock in
� Specific model organisms (e.g., Drosophila mice, rats, Zebra fish, Xenopus, C. elegans, humanized mice)
� Non-model organisms
Cellular techniques considerations
1. Overview of sample preparation consideration2. Overview of assay sensitivity versus specificity3. in vitro, ex vivo, in vivo experiments - differences and techniques4. Isolation of immune cells from tissue5. Flow cytometry (see below)
� Next Generation Sequencing/bioinformatics
Antibodies for research, diagnostics, and therapeutics
1. Introduction2. Generation of antibodies for research and clinical use3. Immunoassays
• Pros and cons• Overview of technical concepts• Interpretation of Results• Examples
o ELISA/EIA/ELISPOTo Western Immunobloto Immunohistochemistry and immunofluorescenceo Microscopic imagingo Flow cytometry (see below)
� CyTOF � Noninvasive imaging techniques
(luminescence, PET/CT)
Flow cytometry 1. Overview of technical concepts• Overview of instrumentation• Controls for experiments• Sample preparation• Data acquisition
2. Interpretation of results 3. Cellular analysis versus cell sorting
� Multiparameter analysis� Statistics and data analysis in
immunology
Subtopics are numbered, and examples are indicated by round bullets (●). Advanced subtopics are indicated by square bullets (■).
452 UNDERGRADUATE IMMUNOLOGY COURSE RECOMMENDATIONS ImmunoHorizons
https://doi.org/10.4049/immunohorizons.2100030
by guest on Decem
ber 10, 2021http://w
ww
.imm
unohorizons.org/D
ownloaded from
the Ad Hoc Committee members, the current recommen-dations were further refined according to the survey com-ments, and in the following plenary session, a preferredsequence of the recommendations was discussed. InAugust 2020, the Ad Hoc Committee finalized the curricu-lum recommendations and developed a recommendationfor inclusive and antiracist teaching. These materials werethen presented in September 2020 to the AAI EducationCommittee, which approved the recommendations withsome minor edits and presented them to the AAI Council,which endorsed the recommendations and suggested abroader dissemination in November 2020.
The recommendationsThe curriculum recommendations provided are intended toserve a two-fold purpose: the first, to provide guidance forimmunology content selection and the second, to provide aframework for equity in the classroom (17--19). The curricularcontent recommendations are presented first (Tables I--XV),followed by the recommendations for inclusive and antiracistteaching.
Immunology content recommendationsThe format of the recommendations is layered, allowing educa-tors to start with key topics of immunology, which are furtherbroken down into foundational concepts that may be coveredin each section. Key topics represent critical categories recom-mended for inclusion in undergraduate immunology curricula,and the foundational concepts are embedded beneath the keytopics as important subcategories. If educators are interested inmore-specific guidance within the foundational concepts, theycan then refer to the subtopics and examples provided. Sub-topics and examples offer flexible opportunities to elaborateand work with students on the foundational concepts.Advanced subtopics are flexible opportunities to explore con-cepts more in depth in accordance with an instructor�s inter-ests, expertise, and available time. This layered approachprovides the instructor with flexibility in how much detail theywant to provide and allows the instructor to shape the curricu-lum according to the needs of their particular undergraduatestudents, the length of the module or course, and theinstructor�s individual expertise. The examples are intended fornew educators as a springboard for curriculum development in
TABLE IV. Innate immunityFoundational Concepts Subtopics and Examples Advanced Subtopics
Functions of barriers and pre-formed elements
1. Functions of anatomical & chemical barriers2. Functions of intrinsic mechanisms
• microRNA• CRISPR
3. Functions of complement (e.g., Ig clearance, MAC)
� Non-vertebrate innate immunity
� Regulation of complement activation
� Complement interaction with coagulation cascade and kallikrein system
� Blood brain barrier
Innate immune cell types and functions
1. Description of cell types• Epithelial cells• Neutrophils• Macrophages• Dendritic cells• NK cells• Basophils, Eosinophils, Mast cells
2. Characterization of effector functions by innate immune cells• Secretion of type I interferons • Antimicrobial peptides• Phagocytosis• Reactive oxygen and nitrogen radicals• Cell death induction
� Developmental origins of tissue resident and infiltrating phagocytes
� Neutrophil extracellular traps
� Maintenance of tissue homeostasis by macrophage
� Apoptosis pathways� Innate lymphoid cell
Differences of innate immunity from adaptive immunity
1. Rapid response time2. No memory 3. Generalized recognition of pathogens based on pathogen-associated molecular patterns
(PAMPs)
� Innate memory
Germline-encoded pattern recognition receptors
1. Pattern Recognition Receptors (PRR) • extracellular and intracellular (e.g., TLRs)• intracellular only (e.g., cytosolic or endosomal -NODs and RIGs)
2. PRR signaling 3. PRR ligands
• Bacterial• Viral• Host derived
4. PAMPs 5. DAMPs
� Fungal and protozoan PRR and PRR ligands
Dendritic cells 1. Survey, capture, migration, and processing of antigens2. Presentation of processed antigen to B cells and T cells in secondary lymphoid tissues
Subtopics are numbered, and examples are indicated by round bullets (●). Advanced subtopics are indicated by square bullets (■).
ImmunoHorizons 453
https://doi.org/10.4049/immunohorizons.2100030
by guest on Decem
ber 10, 2021http://w
ww
.imm
unohorizons.org/D
ownloaded from
their classroom. They are also intended for seasoned educatorsas a cross-check to modify course content or to add a newmodule to an existing course. Although the Ad Hoc Committeekey topics are intentionally arranged in their current orderbased on classroom experience, each key topic is self-standingand can be taught in any logical sequence according to theinstructor�s preference. Additionally, content from one keytopic may be distributed throughout the semester whenrelated content is discussed. This may be most appropri-ate for the final four topics (Tables XII--XV), which haveclinical relevance that may pique student interestthroughout the course in the form of case studies or activelearning projects. Although great effort was taken toremove unnecessary redundancy, some redundancy cannot
be avoided in a subject matter with so many intercon-nected facets. In some cases, it was determined that theredundancy was actually important and necessary to rein-force important topics. Finally, instructors may be limitedby the time they have available. Instructors are encour-aged to prioritize the foundational concepts. For minimumhours available, instructors could choose to only covermaterial listed in Table II. For a quarter system--basedcourse, instructors could plan to cover key topics listed inTables II to X and incorporate the clinical material pre-sented in Tables XI to XV in the form of case studiesthroughout the term, whereas a semester-long standaloneimmunology course could allow for incorporating all keytopics.
TABLE V. InflammationFoundational Concepts Subtopics and Examples Advanced Subtopics
Principles of inflammation 1. Protective response involving immune cells, blood vessels, protein and lipid-based mediators
2. Beneficial aspects
Hallmarks of inflammation 1. Calor, rubor, tumor, dolor, loss of function
Inflammatory inducers 1. Microbial productsPAMPs (e.g., LPS, bacterial DNA, viral nucleic acid)
2. Host associated products:DAMPs (e.g., ATP, nucleic acids, HMGB1, hyaluronic acid)Complement factor C5a
Intracellular response 1. Inflammasome 2. Pyroptosis
Inflammatory mediators 1. Cytokines (e.g., TNF, IL-1 , IL-6)2. Chemokines (e.g., IL-8)3. Lipids (e.g., prostaglandins, leukotrienes)
Local response 1. Cells involvedNeutrophilsMonocytes/M1 macrophagesEndothelial cells
2. Cell trafficking to the site of inflammation P-selectin, integrinsMargination, rolling adhesion, firm adhesion, transmigrationIL-8 and chemotaxis
Systemic response 1. Acute phaseHepatocyte involvementCRPIL-6
2. Fever response
BasophilsMast cellsEosinophils
Hypothalamus involvement3. Effect on bone marrow4. Other symptoms
PainLoss of appetiteMalaise
Down regulators of inflammation 1. Inhibitory cells M2 macrophagesTreg
2. Inhibitory biomoleculesResolvinsIL-10TGF-
Anti-inflammatory drugs 1. NSAID (aspirin or ibuprofen)2. Biologics (anti-TNF)
Subtopics are numbered, and examples are indicated by round bullets ( ). Advanced subtopics are indicated by square bullets ( ).
454 UNDERGRADUATE IMMUNOLOGY COURSE RECOMMENDATIONS ImmunoHorizons
https://doi.org/10.4049/immunohorizons.2100030
by guest on Decem
ber 10, 2021http://w
ww
.imm
unohorizons.org/D
ownloaded from
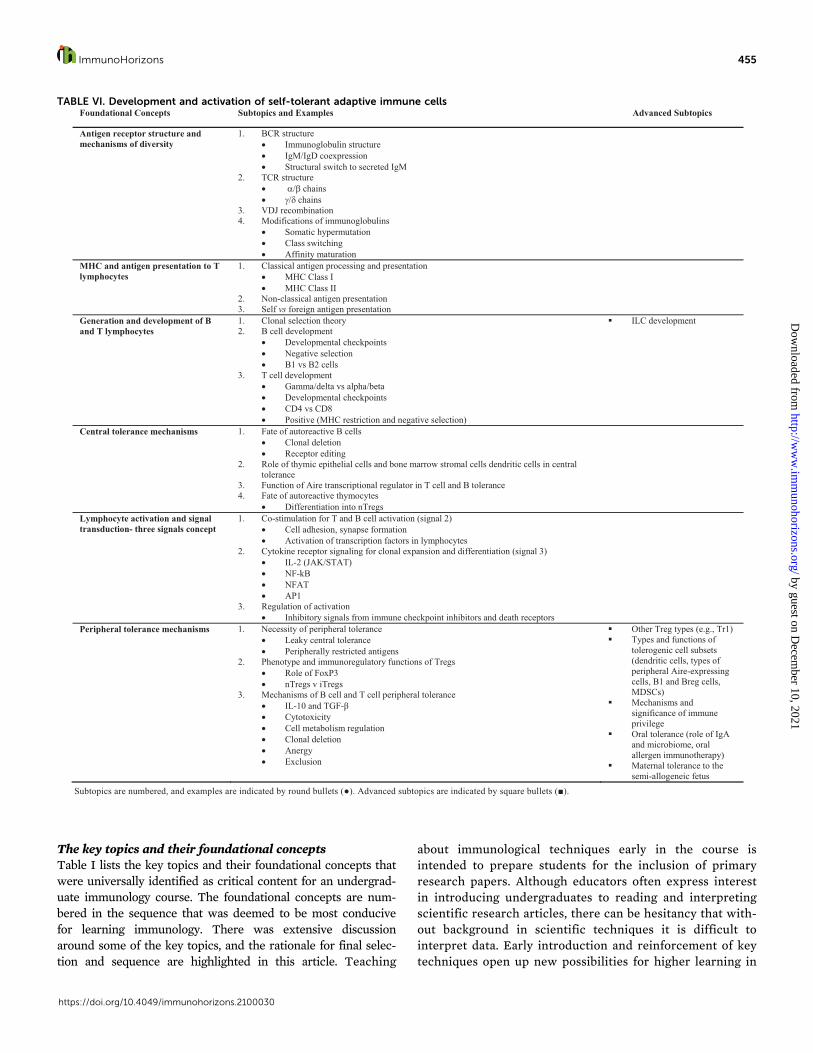
The key topics and their foundational conceptsTable I lists the key topics and their foundational concepts thatwere universally identified as critical content for an undergrad-uate immunology course. The foundational concepts are num-bered in the sequence that was deemed to be most conducivefor learning immunology. There was extensive discussionaround some of the key topics, and the rationale for final selec-tion and sequence are highlighted in this article. Teaching
about immunological techniques early in the course isintended to prepare students for the inclusion of primaryresearch papers. Although educators often express interestin introducing undergraduates to reading and interpretingscientific research articles, there can be hesitancy that with-out background in scientific techniques it is difficult tointerpret data. Early introduction and reinforcement of keytechniques open up new possibilities for higher learning in
TABLE VI. Development and activation of self-tolerant adaptive immune cellsFoundational Concepts Subtopics and Examples Advanced Subtopics
Antigen receptor structure and mechanisms of diversity
1. BCR structure• Immunoglobulin structure• IgM/IgD coexpression• Structural switch to secreted IgM
2. TCR structure• α/β chains• γ/δ chains
3. VDJ recombination4. Modifications of immunoglobulins
• Somatic hypermutation• Class switching• Affinity maturation
MHC and antigen presentation to T lymphocytes
1. Classical antigen processing and presentation• MHC Class I • MHC Class II
2. Non-classical antigen presentation3. Self vs foreign antigen presentation
Generation and development of B and T lymphocytes
1. Clonal selection theory2. B cell development
• Developmental checkpoints• Negative selection• B1 vs B2 cells
3. T cell development• Gamma/delta vs alpha/beta• Developmental checkpoints• CD4 vs CD8• Positive (MHC restriction and negative selection)
� ILC development
Central tolerance mechanisms 1. Fate of autoreactive B cells • Clonal deletion• Receptor editing
2. Role of thymic epithelial cells and bone marrow stromal cells dendritic cells in central tolerance
3. Function of Aire transcriptional regulator in T cell and B tolerance4. Fate of autoreactive thymocytes
• Differentiation into nTregsLymphocyte activation and signal transduction- three signals concept
1. Co-stimulation for T and B cell activation (signal 2)• Cell adhesion, synapse formation• Activation of transcription factors in lymphocytes
2. Cytokine receptor signaling for clonal expansion and differentiation (signal 3)• IL-2 (JAK/STAT)• NF-kB• NFAT • AP1
3. Regulation of activation• Inhibitory signals from immune checkpoint inhibitors and death receptors
Peripheral tolerance mechanisms 1. Necessity of peripheral tolerance• Leaky central tolerance• Peripherally restricted antigens
2. Phenotype and immunoregulatory functions of Tregs • Role of FoxP3• nTregs v iTregs
3. Mechanisms of B cell and T cell peripheral tolerance • IL-10 and TGF-β• Cytotoxicity• Cell metabolism regulation• Clonal deletion• Anergy• Exclusion
� Other Treg types (e.g., Tr1)� Types and functions of
tolerogenic cell subsets (dendritic cells, types of peripheral Aire-expressing cells, B1 and Breg cells, MDSCs)
� Mechanisms and significance of immune privilege
� Oral tolerance (role of IgA and microbiome, oral allergen immunotherapy)
� Maternal tolerance to the semi-allogeneic fetus
Subtopics are numbered, and examples are indicated by round bullets (●). Advanced subtopics are indicated by square bullets (■).
ImmunoHorizons 455
https://doi.org/10.4049/immunohorizons.2100030
by guest on Decem
ber 10, 2021http://w
ww
.imm
unohorizons.org/D
ownloaded from
the undergraduate classroom. Tolerance, which is oftenintroduced later in an immunology course when autoim-mune diseases are discussed, was merged with the develop-ment of adaptive immune cells as development is tightlylinked to selection of self-tolerant cells. This connectionwill allow students to gain a clinical context for develop-ment of adaptive immune cells early on.
The topic, integrated immune response, is intended to allowstudents to construct an understanding of the entire immuneresponse as a dynamic and interdependent system. It is
important for students to put together all of the informationthey have learned up to that point before delving more in depthinto the more-complex, clinically relevant topics. Understand-ing the mucosal immune response provides a foundation forimmunizations and, therefore, the topic mucosal immunity wasplaced before the topic on active and passive immunizations.Tumor immunology follows active and passive immunizationsbecause of the common principles applicable to generation oftumor immune response and the significance of tumor vaccines.In medical school, allergies and hypersensitivities are often
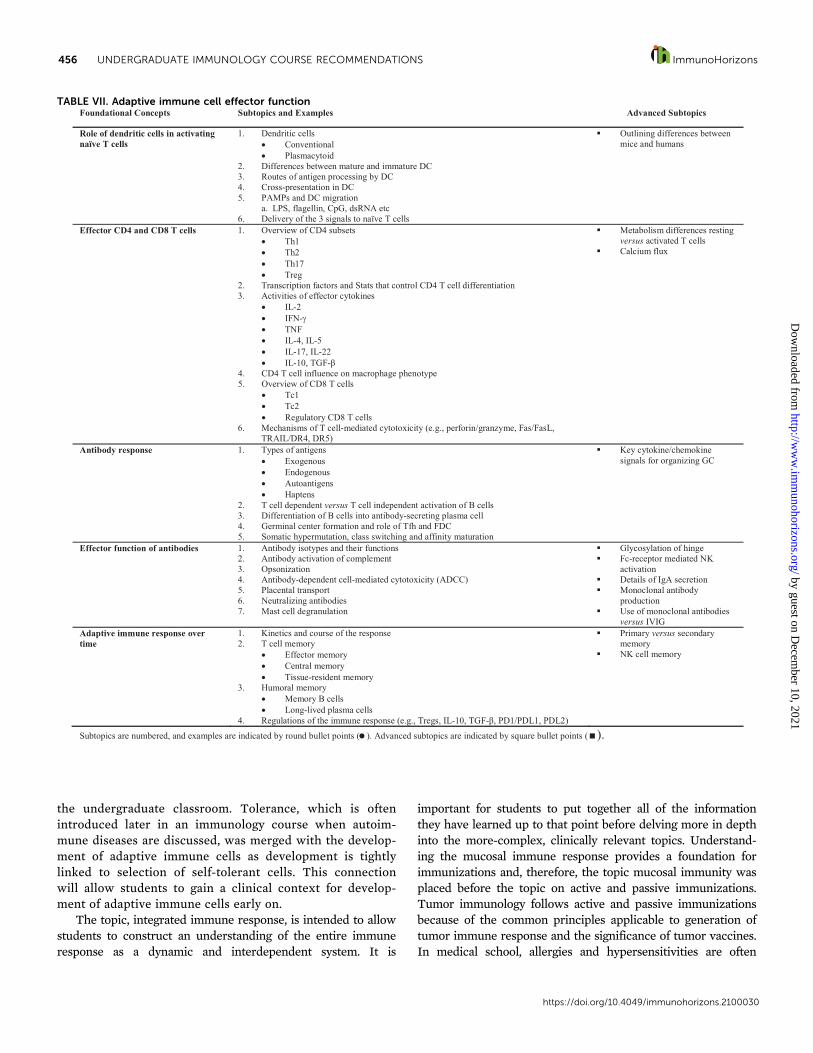
TABLE VII. Adaptive immune cell effector functionFoundational Concepts Subtopics and Examples Advanced Subtopics
Role of dendritic cells in activating naïve T cells
1. Dendritic cellsConventionalPlasmacytoid
2. Differences between mature and immature DC3. Routes of antigen processing by DC4. Cross-presentation in DC5. PAMPs and DC migration
a. LPS, flagellin, CpG, dsRNA etc6. Delivery of the 3 signals to naïve T cells
Outlining differences betweenmice and humans
Effector CD4 and CD8 T cells 1. Overview of CD4 subsetsTh1Th2Th17Treg
2. Transcription factors and Stats that control CD4 T cell differentiation3. Activities of effector cytokines
IL-2IFN-TNFIL-4, IL-5IL-17, IL-22IL-10, TGF-
4. CD4 T cell influence on macrophage phenotype5. Overview of CD8 T cells
Tc1Tc2Regulatory CD8 T cells
6. Mechanisms of T cell-mediated cytotoxicity (e.g., perforin/granzyme, Fas/FasL, TRAIL/DR4, DR5)
Metabolism differences resting versus activated T cellsCalcium flux
Antibody response 1. Types of antigens ExogenousEndogenousAutoantigensHaptens
2. T cell dependent versus T cell independent activation of B cells3. Differentiation of B cells into antibody-secreting plasma cell4. Germinal center formation and role of Tfh and FDC5. Somatic hypermutation, class switching and affinity maturation
Key cytokine/chemokine signals for organizing GC
Effector function of antibodies 1. Antibody isotypes and their functions2. Antibody activation of complement 3. Opsonization4. Antibody-dependent cell-mediated cytotoxicity (ADCC)5. Placental transport6. Neutralizing antibodies7. Mast cell degranulation
Glycosylation of hingeFc-receptor mediated NK activationDetails of IgA secretionMonoclonal antibody productionUse of monoclonal antibodies versus IVIG
Adaptive immune response over time
1. Kinetics and course of the response2. T cell memory
Effector memoryCentral memoryTissue-resident memory
3. Humoral memoryMemory B cellsLong-lived plasma cells
4. Regulations of the immune response (e.g., Tregs, IL-10, TGF- , PD1/PDL1, PDL2)
Primary versus secondary memoryNK cell memory
Subtopics are numbered, and examples are indicated by round bullet points ( ). Advanced subtopics are indicated by square bullet points ( ).
456 UNDERGRADUATE IMMUNOLOGY COURSE RECOMMENDATIONS ImmunoHorizons
https://doi.org/10.4049/immunohorizons.2100030
by guest on Decem
ber 10, 2021http://w
ww
.imm
unohorizons.org/D
ownloaded from
taught along with autoimmune diseases in a combinedapproach reflecting the pathophysiological similarities. How-ever, it was felt that for an undergraduate curriculum, autoim-mune diseases should be covered as a separate topic becauseundergraduate students are still building their knowledge andare not exposed to the depth of clinical experience more typicalfor medical students. To highlight the importance of turning offthe immune response after Ag removal, downregulatory mecha-nisms are taught across the topics. Finally, instead of creating aseparate key topic for the therapy of diseases involving theimmune system, therapies are embedded where the diseases ofthe immune system are discussed to reinforce the underlyingpathophysiological mechanisms and frequently used to engagethe students who are typically genuinely interested in howimmunology is applied to treat diseases.
The subtopics with examples and advanced subtopics forthe foundational concepts for each key topicWe have created tables for each key topic to list the associatedfoundational concepts with subtopics and examples and
advanced subtopics. The subtopics are numbered to show thesequence deemed to best advance student understanding andlearning. Bullets identify subtopics, advanced subtopics, andspecific examples. The advanced subtopics were contributed byIGIT members according to their in-depth knowledge in agiven area, and instructors are encouraged to use advanced sub-topics from their own specialized area.
Table II summarizes the key topic overview and terminologyof the immune system, which primarily serves the goal to estab-lish vocabulary and a common ground for all students. Here, stu-dents are introduced to critical components of the immuneresponse at the molecular, cellular, and tissue level and therespective terminology. Because immunology is notable for itssubstantial, and often intimidating, nomenclature, establishingthe terminology early is critical for establishing a working�language� for the remainder of the course. Table III summa-rizes important immunological techniques from molecular andcellular in vitro approaches to animal models. Ab-based techni-ques are extensively covered because of their applications inresearch, diagnostics, and therapeutics. Flow cytometry is
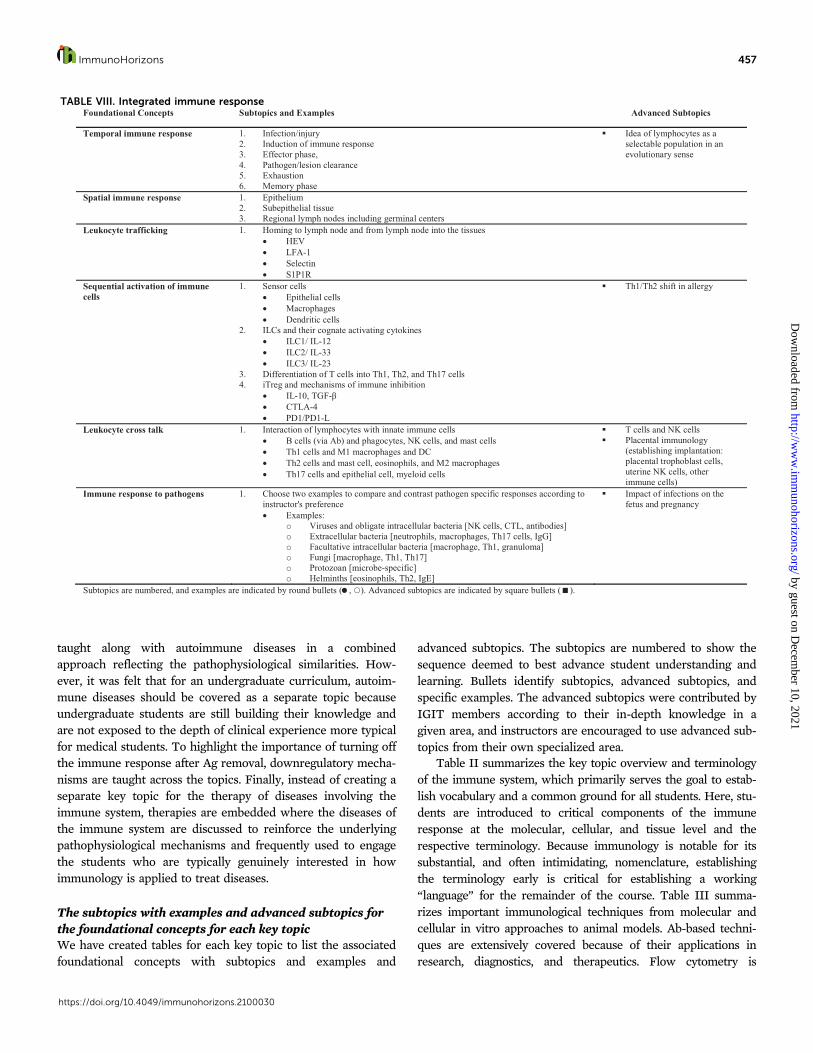
TABLE VIII. Integrated immune responseFoundational Concepts Subtopics and Examples Advanced Subtopics
Temporal immune response 1. Infection/injury2. Induction of immune response3. Effector phase,4. Pathogen/lesion clearance5. Exhaustion6. Memory phase
Idea of lymphocytes as a selectable population in an evolutionary sense
Spatial immune response 1. Epithelium2. Subepithelial tissue3. Regional lymph nodes including germinal centers
Leukocyte trafficking 1. Homing to lymph node and from lymph node into the tissuesHEVLFA-1SelectinS1P1R
Sequential activation of immune cells
1. Sensor cellsEpithelial cellsMacrophagesDendritic cells
2. ILCs and their cognate activating cytokinesILC1/ IL-12ILC2/ IL-33ILC3/ IL-23
3. Differentiation of T cells into Th1, Th2, and Th17 cells4. iTreg and mechanisms of immune inhibition
IL-10, TGF-CTLA-4PD1/PD1-L
Th1/Th2 shift in allergy
Leukocyte cross talk 1. Interaction of lymphocytes with innate immune cellsB cells (via Ab) and phagocytes, NK cells, and mast cellsTh1 cells and M1 macrophages and DCTh2 cells and mast cell, eosinophils, and M2 macrophagesTh17 cells and epithelial cell, myeloid cells
T cells and NK cellsPlacental immunology (establishing implantation: placental trophoblast cells, uterine NK cells, other immune cells)
Immune response to pathogens 1. Choose two examples to compare and contrast pathogen specific responses according to instructor's preference
Examples: o Viruses and obligate intracellular bacteria [NK cells, CTL, antibodies]o Extracellular bacteria [neutrophils, macrophages, Th17 cells, IgG]o Facultative intracellular bacteria [macrophage, Th1, granuloma]o Fungi [macrophage, Th1, Th17]o Protozoan [microbe-specific]o Helminths [eosinophils, Th2, IgE]
Impact of infections on the fetus and pregnancy
Subtopics are numbered, and examples are indicated by round bullets ( , ). Advanced subtopics are indicated by square bullets ( ).
ImmunoHorizons 457
https://doi.org/10.4049/immunohorizons.2100030
by guest on Decem
ber 10, 2021http://w
ww
.imm
unohorizons.org/D
ownloaded from

included because it is a commonly used technique that is centralto immunology findings described throughout each topic. Therewas strong consensus to introduce immunological techniques asa dedicated key topic early in the course to provide studentswith a robust basis for understanding primary immunologyresearch papers throughout the course.
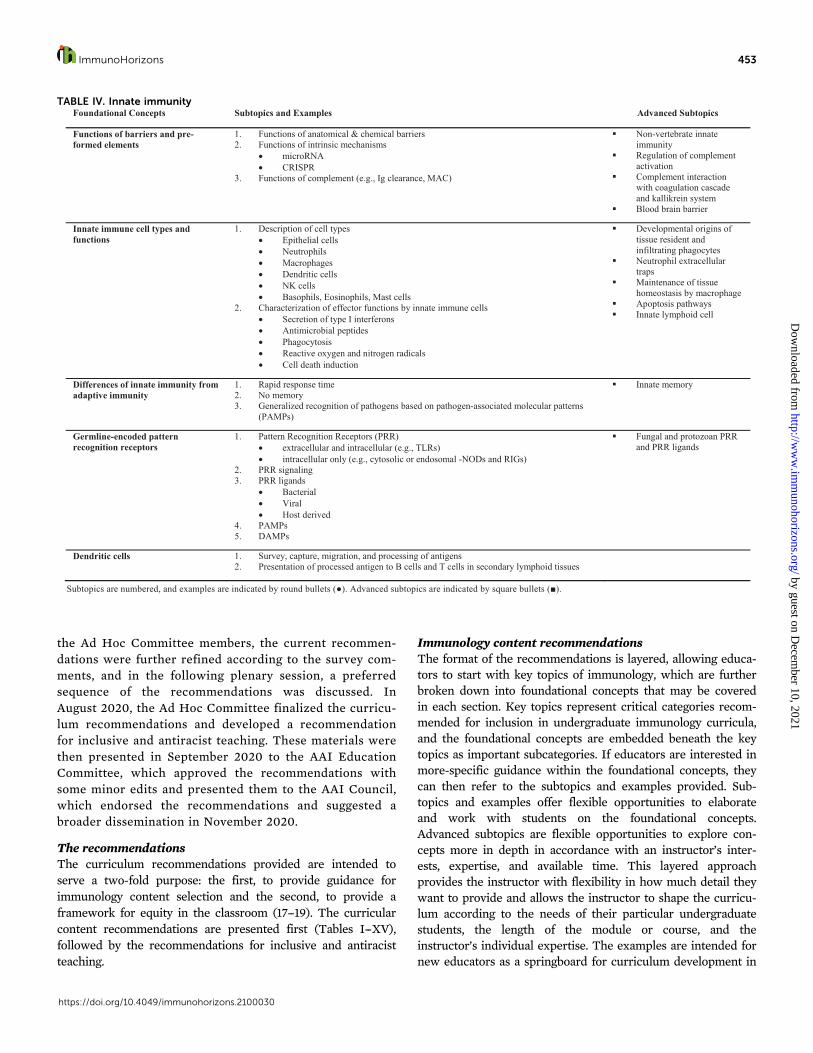
Table IV summarizes the key topic innate immunity. As oneof the major conceptual �arms� of the immune system, this keytopic helps frame an understanding of how the organs and cel-lular systems first recognize and combat potentially dangerousmicrobial or environmental encounters. This key topic was
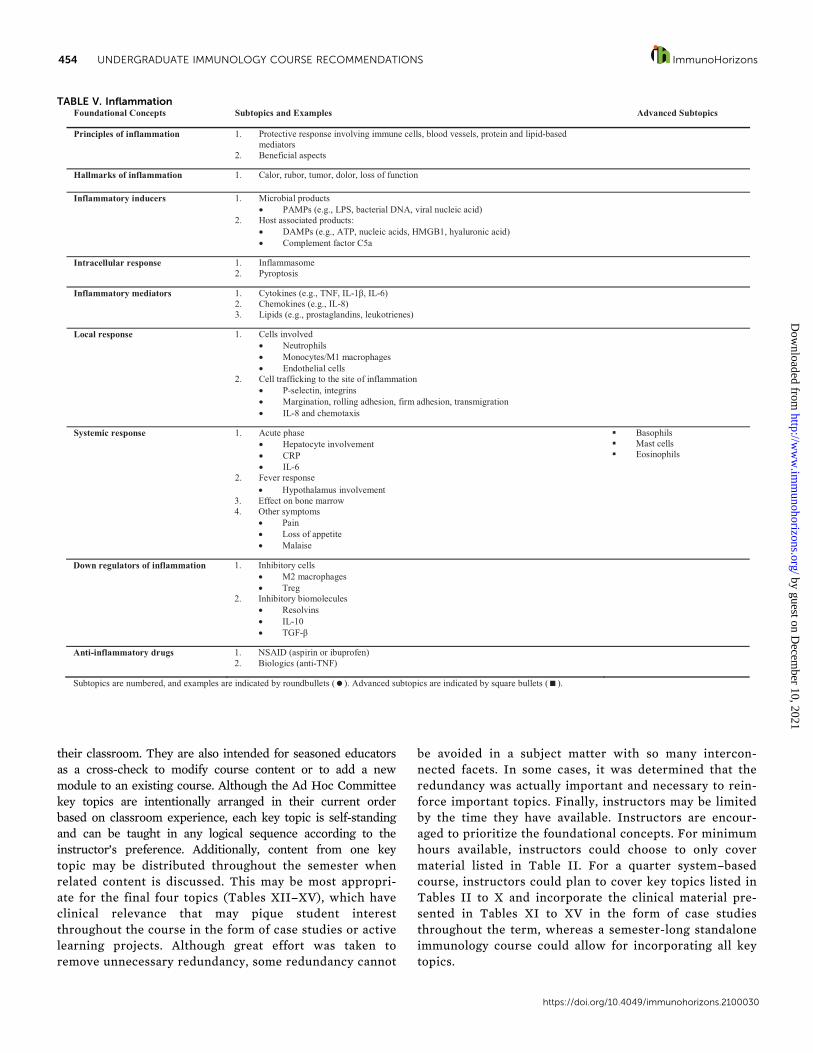
created with primarily bacterial and viral infections in mind;thus, innate responses to fungal and protozoan microbes arelisted as advanced subtopics, reflecting instructional directionsthat are traditionally less common in curricula. In addition tocomplement, phagocytic cells, and NK cells, epithelial cells areincluded as effector cells in the innate immune response asthey exemplify how different cell types and tissues, not tradi-tionally considered part of the immune system, can play keyroles in immunity. Table V summarizes the key topic inflamma-tion. It is recommended that instructors also highlight the ben-eficial aspects of inflammation and begin this key topic with a
TABLE IX. Mucosal immunityFoundational Concepts Subtopics and Examples Advanced Subtopics
Organization of the mucosal immune system
1. Overview of anatomic compartmentsBALT, NALT, GALT, GUWaldeyer’s ring with adenoids, palatine, and lingual tonsilsIsolated lymphoid folliclesLamina propria crypts
2. Mucus componentsMucinsAntimicrobial peptides and proteinsIgA
3. Difference between systemic and mucosal lymph nodesPeyer’s PatchesMesenteric lymph nodesCryptopatchesAppendixCecum
4. High endothelial venules
Specialized immune cells located at mucosal sites
1. Activation state of lymphoid cells in the area2. Mast cells and other innate cells present3. / T cells 4. Plasma cells (IgA secreting)
Activation markers on residentB and T lymphoid cellsInnate lymphoid cells (ILC)MAITIntraepithelial lymphocytes (CD8)CD8 + T cellsActivities of / T cells
Unique APC populations and uptake of antigen at mucosal sites
1. Overview of APC presentLack of inflammatory receptors
o TLR, FcR, CD14Lack of inflammatory cytokines
o IL-1 , TNF2. Role of M cells3. Antigen transport across epithelium 4. Lumenal access of DCs
CD103+ DCs
Role of IgA in protection at mucosal sites
1. IgA secretion by plasma cell on basolateral side of epithelial surface2. Transcytosis of IgA to apical face of epithelial cell via poly-Ig receptor3. IgA’s role in the mucosa/with mucin
IgA deficiency and transport of IgMRole of secretory IgA component
Induction and regulation of the immune response at mucosal sites
1. Initiation of the response in mucosal sites2. Reasons for limited inflammation3. Role of Tregs
Tregs control T cells with inflammatory potential4. Tolerance to non-pathogenic substances (e.g.. food)5. Tolerance to normal microbiota
Differences between gut and lung mucosal immune responsesPathology at mucosal sites, examples:
Inflammatory bowel diseaseAntibiotic use and C. difficileDefense against helminthsAsthmaFood allergyIgA deficiencyBacterial vaginosis
Subtopics are numbered, and examples are indicated by round bullets ( , ). Advanced subtopics and their examples are indicated by closed square bullets ( ) and open square bullets ( ), respectively.
458 UNDERGRADUATE IMMUNOLOGY COURSE RECOMMENDATIONS ImmunoHorizons
https://doi.org/10.4049/immunohorizons.2100030
by guest on Decem
ber 10, 2021http://w
ww
.imm
unohorizons.org/D
ownloaded from

discussion of the protective aspects of acute inflammation.Inflammation leads to initiation of the adaptive immuneresponse, and thus, this key topic is followed by the key topicdevelopment and activation of self-tolerant adaptive immunecells, which is summarized in Table VI. The concept of toler-ance is introduced under this key topic because the develop-ment of lymphocytes is tightly linked to tolerance. Theimportance of self-tolerance for lymphocyte development isalso reflected in the title of this key topic. Instructors whowant to highlight oral tolerance or tolerance in pregnancy maywish to introduce these advanced topics here.
Table VII summarizes the key topic adaptive immune celleffector function. Dendritic cells, effector CD4 and effectorCD8 T cells, Ab response, and Ab function are first examined,and then the adaptive immune response over time is described.Germinal centers and NK cell functioning can be explored asadvanced subtopics. Table VIII summarizes the key topic inte-grated immune response, which aims to provide students witha general understanding of how the innate and adaptiveimmune responses interweave over time. This section alsodefines the locations where the interactions between Ag, innate,and adaptive immune cells take place throughout the course of
TABLE X. Active and passive immunizationsFoundational Concepts Subtopics and Examples Advanced Subtopics
Historical aspects of immunization 1. Variolation2. Jenner’s Experiments with smallpox3. Development of the polio vaccine
Implications of von Behring’s discovery of diphtheria anti-toxinSmallpox eradication campaignCutter labs
Why vaccines work and concept of herd immunity
1. Statistics of safety versus morbidity/mortality of infectious diseaseAny example would work
2. R0 and herd immunity thresholdsMeasles
3. Rationale for targeting specific vaccines to particular populationsAge dependencyPregnant mothersCareer associated exposure (e.g., veterinarians, military)Prevalence of a disease in regards to global vaccination
Types of vaccines 1. Whole killed organism vaccines2. Live-attenuated organism vaccines3. Toxoid vaccines4. Subunit vaccines5. Recombinant vaccines6. Polysaccharide vaccines7. Nucleic acid-based vaccines
Important aspects of vaccines 1. Advantages and Disadvantages of the vaccines listed above2. Type of immune response initiated for each vaccine listed above
Humoral immunityHumoral and cell mediated immunity
3. Example of different flu vaccine types can initiate different types of immunity (live attenuated influenza vaccine versus the quadrivalent flu vaccine)
Vaccine production, adjuvants and preservatives
1. Vaccines preparation2. Route of administration3. Common vaccine adjuvants (e.g. thimerosal, aluminum)
Purpose (depot effect, inflammasome activation)Toxicities Mechanism of action
4. Vaccine preservativesChallenges of vaccine success 1. Technological difficulties associated with vaccine development
Example: influenza vaccines and seasonal variability2. Microbial limitations for making vaccines
Example: HIV vaccine and high mutation rate3. Societal and global challenges to achieve R0 levels required to generate herd immunity
Anti-vaccine movementExample: Polio and global challenges for eradications
Passive immunization 1. Use of pre-formed antibodies versus active immunizationAdvantages/disadvantagesHalf-life of preparationsMechanism of action
2. Polyclonal and monoclonal antibody preparationsMedical examples of how passive immunization is used (e.g., tetanol)
3. Differences of immune globulin, specific immune globulin, and intravenous IG 4. Natural examples of passive immunization (e.g., maternal antibodies via crossing the
placenta or breast feeding)Subtopics are numbered, and examples are indicated by round bullets ( ). Advanced subtopics are indicated by square bullets ( ).
ImmunoHorizons 459
https://doi.org/10.4049/immunohorizons.2100030
by guest on Decem
ber 10, 2021http://w
ww
.imm
unohorizons.org/D
ownloaded from

the immune response. To highlight that the immune responseto pathogens is tailored to the specific type of pathogens, theimmune responses to two different pathogens could be com-pared and contrasted according to the instructor�s expertise. Itis highly recommended that instructors choose pathogens thatare relevant or well-known to the students.
Table IX summarizes the key topic mucosal immunity,which examines the immune response in the mucosa with spe-cial attention paid to the gut mucosa. Here, examples for patho-logical conditions affecting the mucosa can be introduced asadvanced subtopics. Many types of immunizations target themucosal immune system. Thus, the key topic active and passiveimmunizations, summarized in Table X, follows the key topicmucosal immunity. A brief historical overview and a descrip-tion of parameters for vaccine success have been included as afoundational concept to increase awareness of the complexityand difficulty of developing a protective vaccine. Passive immu-nization is focused on Ab-related subtopics. Table XI summa-rizes the key topic tumor immunology. This key topicfollows the key topic active and passive immunizations
because many novel approaches of cancer immunotherapyemploy mechanisms of active and passive immunization.The key topic tumor immunology first explores mechanismsof tumor surveillance, then investigates tumor escape fromthe immune response, and concludes with subtopics on can-cer immunotherapy.
The remaining four key topics are dedicated to pathologyassociated with the immune system, and each include therapeu-tic interventions as a foundational concept. Table XII summa-rizes the key topic allergies and hypersensitivities. With areference to the medical school curriculum, hypersensitivitiesare first introduced as pathological responses to Ag that can beclassified as allergies, autoimmunity, and transplant rejection.Thereafter, hypersensitivities are classified based on the under-lying mechanism according to the Gell--Coombs classificationmore consistent with the undergraduate immunology curricu-lum, and the remainder of the key topic follows this classifica-tion. Table XIII summarizes the key topic autoimmunediseases. The foundational concepts include causes and epide-miology of autoimmune diseases and a classification based on
TABLE XI. Tumor immunologyFoundational Concepts Subtopics and Examples Advanced Subtopics
Tumor immunosurveillance 1. Examples of tumor antigensAberrant or overexpression of normal proteinsDifferentiation antigensViral antigensAntigens expressed by mutated passenger/driver mutations
2. Anti-tumor immune mechanismsTumor killing by cytotoxic CD8 T cellsCross-presentation of tumor antigens to CD8 T cells by dendritic cellsHumoral antitumor responsesNK-mediated killing of tumor cellsRole of activated macrophages in tumor suppression
Role of immune cells in promotingtumor -chronic inflammationModifiable host factors affectingtumor immunity (e.g., diet,microbiota)
Immune escape by tumors 1. The three Es of immunoeditingEliminationEquilibriumEscape
2. Escape mechanismsLoss of tumor antigens
Immunosuppressive tumor microenvironmento Abnormal vasculature and hypoxiao Role of immune check points on CD8 and regulatory T cells (PD-
1/CTLA-4)o Tumor secreted immunosuppressive cytokines/growth factors
(TGF- /VEGFo Suppressive myeloid cells (M2 macrophages, myeloid-derived
suppressor cells, tolerogenic dendritic cells)
Clinical evidence of the presence of immune cells in the tumor microenvironment (tumor biopsies) and the relevance of ‘immunoscore’ to assess prognosis (hot vs cold tumors)Co-opting of immune cells by tumors, especially tolerogenic mechanisms like recruitment of Tregs and changing the orientation of macrophages to wound-healing modeCo-opting of stromal cells including the cancer-associated fibroblasts by tumor cells
Cancer immunotherapy 1. Brief history of cancer immunotherapy1854 – Virchow1883 – Fehleisen1891 – Coley1909 – Ehrlich
2. Classes of cancer immunotherapyTumor-targeting monoclonal antibodies (e.g., anti-CD20, anti-Her2)Cytokine therapy (e.g., high dose IL-2 and IFN-Tumor vaccines (e.g., dendritic cell-based vaccine in prostate cancer)
3. T-cell based agentsT cell checkpoint inhibitors (anti-PD1 and anti-CTLA4)Adoptive cell therapies (CAR-TNK cell therapy
4. The rationale for combinatorial therapies
Example of one of the successful clinical trials of PD-1/CTLA-4 or CAR-T
Subtopics are numbered, and examples are indicated by round bullets ( , ). Advanced subtopics are indicated by square bullets ( ).
460 UNDERGRADUATE IMMUNOLOGY COURSE RECOMMENDATIONS ImmunoHorizons
https://doi.org/10.4049/immunohorizons.2100030
by guest on Decem
ber 10, 2021http://w
ww
.imm
unohorizons.org/D
ownloaded from

their underlying mechanism. It is strongly recommendedthat instructors choose clinical examples for autoimmunediseases based on student interest. Table XIV summarizesthe key topic transplant rejection and includes referencesto both organ transplants and blood transfusions. Finally,Table XV summarizes the key topic immunodeficiencies,which are presented as primary and secondary immunode-ficiencies. As time permits and according to instructorexpertise, one or more examples for each type of immuno-deficiency can be presented. Diagnostic assessments usedfor both primary and secondary immunodeficiencies areincluded here and may be a tool to reinforce immunologictechniques described earlier in Table III.
Recommendations for inclusive and antiracist teachingOur society is undergoing transformative changes in the aware-ness of institutional racism and structural inequality that limitthe participation of all. It is imperative to recognize the need toinclude different perspectives in solving scientific problems.Yet it is not enough to enable all to come to the table wheredecisions are made; rather, it is time to reconstruct this table,collaboratively informed by all participants� vision in our soci-ety. We, as educators, have an opportunity to take part in
eliminating institutional racism and structural inequality (19).Inclusivity in science education means expanding access toeducational and professional opportunities to underrepresentedgroups and crafting our teaching in a way that specificallyacknowledges and engages all learners and validates their indi-vidual and collective experiences. Our teaching practices mustbe informed by not only our students� personal histories butalso the history and dynamics of how their world is and wasshaped before their arrival into our classroom.
As educators, we hope to empower the next generationthrough knowledge and agency. As educators in the scien-ces, we have a responsibility to ensure that all of our schol-ars from diverse backgrounds�representing individualswho differ in racial, cultural, and ethnic identity; genderidentity; sexual orientation; age; physical and intellectualdisability; spiritual beliefs; and socioeconomic status�willhave an opportunity to contribute to the scientific enter-prise. Students in an immunology course typically comeacademically prepared by having completed prerequisitecourses in general biology and general and organic chemis-try. However, their life stories and their living circumstan-ces at the time they take your immunology course will varywidely. Some students might be caregivers or breadwinners,live in crowded quarters, and may have grown up doubting
TABLE XII. Allergies and hypersensitivitiesFoundational Concepts Subtopics and Examples Advanced Subtopics
Immunological hypersensitivities, definition and classification
1. General definition of immunological hypersensitivities and contrast to non-immunological hypersensitivities
Role of sensitization2. Classification of immunological hypersensitivities based on antigen types
Allergies (pathological responses to harmless environmental antigens)Autoimmunity (pathological responses to self-antigens)Graft rejection/transfusion reactions (pathological responses to alloantigens)
3. Classification of immunological HS based on mechanism (Gell-Coombs classification)Primarily antibody-mediated via IgE (Type 1) and IgG/IgM (Types 2 and 3)T cell-mediated via inflammatory and cytotoxic T cells (Type 4)
Main allergic reaction types according to the Gell-Coombs classification
1. “Classical” allergies (Type 1 HS, IgE-mediated)Role of mast cells, histamine, eicosanoids“Immediate”, biphasic pattern (early and late phase)AnaphylaxisAtopy definition: genetic predisposition to IgE hyper-responsivenessExamples (based on student interest):o Hay fevero Acute asthmao Eczemao Food and drug allergieso Insect bites
2. T cell-mediated allergies (Type 4 hypersensitivity reactions): Delayed-type reactionsInflammatory (Th1, Th2, Th17-mediated) and/or cytotoxic reactionsExamples:o Contact dermatitiso Chronic asthmao Stevens-Johnson syndrome
Recognizing anaphylactic reactionsHygiene hypothesisRole of early exposure to allergens The skin-prick test and serum IgE testing for diagnosis of allergy diagnosis
IgG-mediated allergies (Type 2 and 3 hypersensitivities): cytotoxic and cytolytic effects, inflammation with examples (typically drug-induced):
Penicillin (hemolytic disease)Biologicals (serum sickness)
Principles of therapy of allergic reactions
1. Drugs used to treat allergic reactionsAnti-histaminesCorticosteroidsBronchodilators (rescue inhalers)
2. Allergen immunotherapy (desensitization strategies)
Epinephrine and use of Epi pens
Allergen desensitization protocols
Subtopics are numbered, and examples are indicated by closed round bullets ( ). Advanced subtopics are indicated by square bullets ( ). Examples for specific diseases and drugs are indicated by open bullets ( , ).
ImmunoHorizons 461
https://doi.org/10.4049/immunohorizons.2100030
by guest on Decem
ber 10, 2021http://w
ww
.imm
unohorizons.org/D
ownloaded from

their qualifications to be in your class and/or not realizingthat immunology also applies to them. It is paramount thatwe create a culturally responsive learning environment thataccommodates our students� diverse backgrounds and fos-ters an authentic sense of belonging. There are changes weshould make in curriculum and pedagogy to embrace differ-ences without compromising standards.
We can start without delay working toward this goal. Wecan engage in implicit bias training and make small changes inour teaching with great impact. Examples include initiatingactivities that bring personal lived experiences (including cul-ture) into the classroom, rebranding �office hours� as �studenthours,� offering low-bandwidth options in remote learning(e.g., using real-time chat rather than video/audio conferencingor discussion boards for asynchronous online courses), provid-ing flexible dates for assignment submissions that accommodateoutside responsibilities, including curriculum materials that areauthored by researchers from diverse backgrounds, sharing
success stories of former students and inviting them as panel-ists, including images of people from diverse backgrounds incase studies, and tapping into the experiences of our studentsin class projects. In addition, we can include group work as apedagogical tool to support the social and emotional needs ofboth underrepresented and majority students (20). We canimplement the question formulation technique to foster self-confidence and use various types of formative and summativeassessments (21).
Furthermore, we can actively promote equity, diversity, andinclusion among our faculty by participating in search commit-tees and creating a welcoming and inclusive environment forour new colleagues. We can reach out to members across allidentity groups on our campuses to become fully aware ofdiverse cultures, lifestyles, and interests and become allies whoinfuse inclusive pedagogy. Moreover, we can enroll in institu-tional programs that target faculty training in equity, diversity,and inclusion, such as those offered by the Association of
TABLE XIII. Autoimmune diseasesFoundational Concepts Subtopics and Examples Advanced Subtopics
Causes, epidemiology, genetics 1. Autoimmunity as failure of immunological self-tolerance 2. Epidemiological and clinical features of common autoimmune diseases
PrevalenceRanges of age of onsetSex EthnicitySystemic vs Organ-specific
3. Genetic predisposition to autoimmunity:Monogenic autoimmune syndromes, examples:o APECEDo IPEX syndromesRole of HLA association, example:o HLA-B27 and ankylosing spondylitis
4. Self-tolerance breakdown during immune responses, examples:o Molecular mimicry (rheumatic fever)o Bystander activationo Epitope spreading
Definitions of and compare/ contrast: autoreactivity, autoimmunity, autoimmune diseaseSmoking and citrullinatedpeptides in RASympathetic ophthalmia
Mechanisms of autoimmune disease
1. Autoantibody-mediated immune reactionsCytotoxic and cytolytic reactions (Type 2 hypersensitivity), examples:o Thrombocytopenia purpurao Autoimmune hemolytic anemiaReceptor-mediated cell dysfunction (Type 2 hypersensitivity), examples:o Myasthenia graviso Graves diseaseo PemphigusImmune complex-mediated/ complement activation (Type 3 hypersensitivity), example:o Lupus (note that this could be mixed-type)
2. T cell-mediatedInflammatory (Th1, Th2, Th17-mediated) and/or cytotoxic reactions, examples:o Type 1 diabeteso Psoriasis
3. Diseases caused by mixed HS reactions, example:o Rheumatoid arthritis
Autoantibodies as diagnostic tools, examples:
Rheumatoid factorAnti-citrullinated peptide antibodiesAntinuclear autoantibodies and the ANA assayAnti-islet autoantibodies
Additional examples of autoimmune diseases for discussion based on student interest:Multiple sclerosis
SarcoidosisCeliac diseaseIBDHashimoto’s thyroiditis
Principles of therapy ofautoimmune disease
1. Drugs used to treat autoimmune disease:CorticosteroidsImmunosuppressive drugs (e.g., methotrexate)Biologics (e.g., TNF inhibitors)JAK inhibitors
Mycophenolate mofetilAdditional biologics, examples:
Anti-CD52Anti-CD20Anti-IL-12/IL-23Anti-integrinsAnti-IL-6
Subtopics are numbered, and examples are indicated by round bullets ( ). Advanced subtopics are indicated by square bullets ( ). Examples for specific diseases and drugs are indicated by open bullets ( , ).
462 UNDERGRADUATE IMMUNOLOGY COURSE RECOMMENDATIONS ImmunoHorizons
https://doi.org/10.4049/immunohorizons.2100030
by guest on Decem
ber 10, 2021http://w
ww
.imm
unohorizons.org/D
ownloaded from

American Colleges and Universities and The Leadership Alli-ance. If these opportunities are not available on campuses,we can begin a conversation to institute new antiracist orallyship programs, whereby additional resources on antira-cism for the biomedical research training community areavailable on the Diversity Program Consortium Web site(funded by the National Institutes of Health). Finally, yetimportantly, through the AAI Teaching Interest group, wecan exchange ideas with like-minded faculty striving toeliminate race-based, socioeconomic, and other barriers tolearning. We are keenly aware that the writing above doesnot do justice to this enormous topic, but there is an abso-lute urgency to begin moving our educational practicestoward inclusive and antiracist teaching, and we considerthe suggested steps as important possible first steps.
CONCLUSIONS
The final product of the AAI Ad Hoc Committee and ITIG is aliving document that will be reexamined by the AAI EducationCommittee over time to make sure the content stays up to date,topical, and cutting-edge. This work is a powerful testamentthat the combined efforts of a dedicated group of educatorswith a common purpose can provide a novel tool to improvecourse content and delivery in the field of immunology. Thiswork comes on the back of other successful efforts to provideconsensus on topics such as chemistry, physics, and microbiol-ogy. The guidance document published in this article canbe easily paired with pedagogy strategies for immunolo-gists, which are provided in the AAI Newsletter through-out the year. Future work is necessary to provide examplelearning outcomes for educators employing the new AAIcurriculum recommendations.
Additional resourcesTo meet the needs of different learning styles, it is paramountto enrich the curriculum with varied tools. To gather supple-mentary teaching resources, including sources for case studies,primary literature, and visual tools, members of the AAI ITIGwere surveyed for their recommendations for teaching sources.Their compiled recommendations are listed below. They reflectcurrent teaching practices and do not represent a comprehen-sive evaluation of teaching resources.
1) Basic Immunology: Functions and Disorders of the ImmuneSystem, 6th Edition, by Abul K. Abbas, Andrew H. Lichtman,Shiv Pillai; ISBN-13: 978-0323549431; ISBN-10: 0323549438.
2) Immunology: A Short Course, 7th Edition, by RichardCoico, Geoffrey Sunshine; ISBN-13: 978-1118396919; ISBN-10:111839691X.
3) How the Immune System Works (The How it WorksSeries), 6th Edition, by Lauren M. Sompayrac; ISBN-13: 978-1119542124; ISBN-10: 111954212X.
4) Case Studies in Immunology: A Clinical Companion, Sev-enth Edition, by Raif S. Geha, Luigi Notarangelo; ISBN-13: 978-0815345121; ISBN-10: 9780815345121.
5) National Center for Case Study Teaching in Science atthe University at Buffalo (https://sciencecases.lib.buffalo.edu/collection/).
6) Primary literature: AAI collection of Pillars of Immunol-ogy articles (https://www.jimmunol.org/pillarsofimmunology).
7) YouTube channels such as Armando Hasudungan�s chan-nel (https://www.youtube.com/user/armandohasudungan/search?query=immunology).
8) Lumen Learning (https://lumenlearning.com/courses/).9) InQuizitive learning tool from Norton�s, accompanying
their textbooks (Janeway�s and Parham�s).10) Immunopaedia.org (https://www.immunopaedia.org.za/),
a nonprofit educational Web site.
TABLE XIV. Transplant rejectionFoundational Concepts Subtopics and Examples Advanced Subtopics
Transplant immunology 1. Definition of alloreactivityThe mixed lymphocyte reactionRole of allorecognition in transplant rejection and blood transfusion reactionsMHC as the major determinant of graft rejection
2. Basic immunological mechanism of alloreactivityRecognition of allogeneic MHC by TCRRecognition of allo-peptidesAlloantibodies
3. Difference between transplant rejection and graft-vs-host disease4. Blood types (ABO and Rh) as alloantigens:
Transfusion reactionsHemolytic disease of the newborn
Types of transplants based on graft donor genetics (autologous, syngeneic, allogeneic, xenogeneic)Types and mechanisms of transplant rejection reactions (hyperacute, acute, chronic)Role of passenger APCs and lymphocytesHLA matching and transplant lists (role of donor registries in transplant, criteria for matching)Blood banking
Principles of immunosuppressive therapy for transplant rejection
1. Drugs used to treat transplant rejection:CorticosteroidsImmunosuppressives, examples:o Cyclosporineo Methotrexateo Mycophenolate mofetil
Other calcineurin inhibitors
Biologics, examples:OKT3ThymoglobulinAnti-CD20Anti-C5a
Subtopics are numbered, and examples are indicated by round bullets ( ). Advanced subtopics are indicated by square bullets ( ). Examples for specific diseases and drugs are indicated by open bullets ( , ).
ImmunoHorizons 463
https://doi.org/10.4049/immunohorizons.2100030
by guest on Decem
ber 10, 2021http://w
ww
.imm
unohorizons.org/D
ownloaded from
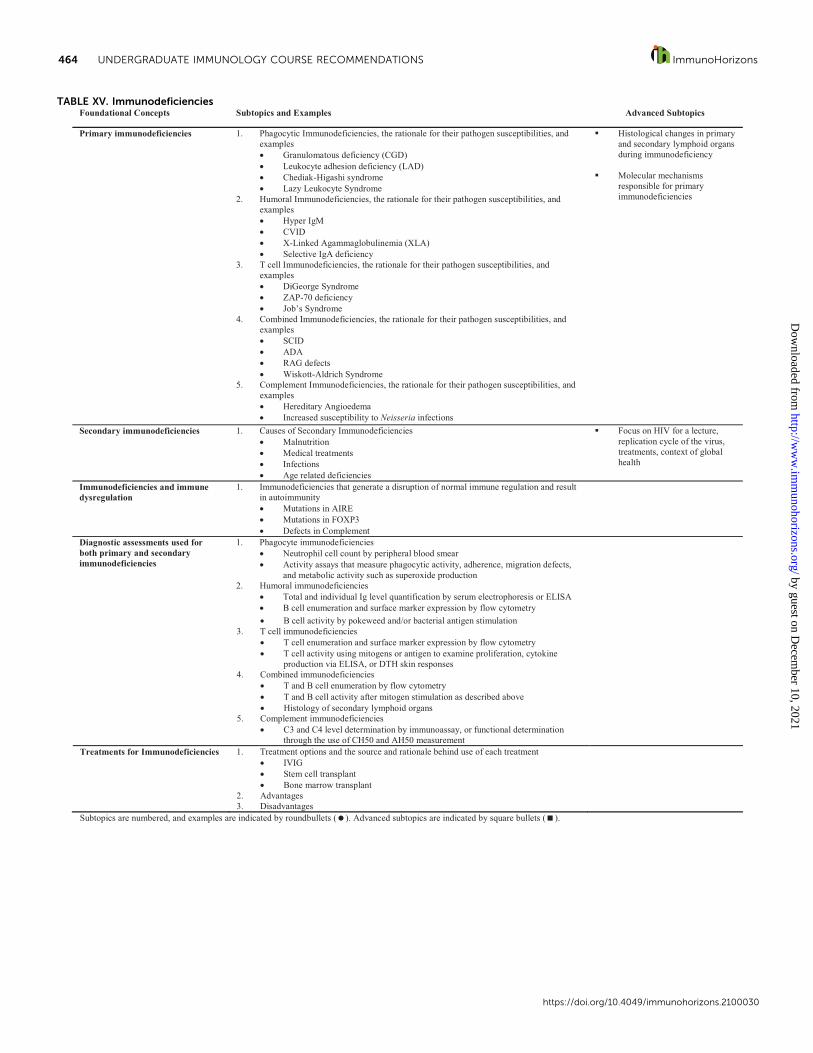
TABLE XV. ImmunodeficienciesFoundational Concepts Subtopics and Examples Advanced Subtopics
Primary immunodeficiencies 1. Phagocytic Immunodeficiencies, the rationale for their pathogen susceptibilities, and examples
Granulomatous deficiency (CGD)Leukocyte adhesion deficiency (LAD)Chediak-Higashi syndromeLazy Leukocyte Syndrome
2. Humoral Immunodeficiencies, the rationale for their pathogen susceptibilities, and examples
Hyper IgMCVIDX-Linked Agammaglobulinemia (XLA)Selective IgA deficiency
3. T cell Immunodeficiencies, the rationale for their pathogen susceptibilities, and examples
DiGeorge SyndromeZAP-70 deficiencyJob’s Syndrome
4. Combined Immunodeficiencies, the rationale for their pathogen susceptibilities, and examples
SCIDADARAG defectsWiskott-Aldrich Syndrome
5. Complement Immunodeficiencies, the rationale for their pathogen susceptibilities, and examples
Hereditary AngioedemaIncreased susceptibility to Neisseria infections
Histological changes in primary and secondary lymphoid organs during immunodeficiency
Molecular mechanisms responsible for primary immunodeficiencies
Secondary immunodeficiencies 1. Causes of Secondary ImmunodeficienciesMalnutrition Medical treatmentsInfectionsAge related deficiencies
Focus on HIV for a lecture, replication cycle of the virus, treatments, context of global health
Immunodeficiencies and immune dysregulation
1. Immunodeficiencies that generate a disruption of normal immune regulation and result in autoimmunity
Mutations in AIREMutations in FOXP3Defects in Complement
Diagnostic assessments used for both primary and secondary immunodeficiencies
1. Phagocyte immunodeficienciesNeutrophil cell count by peripheral blood smearActivity assays that measure phagocytic activity, adherence, migration defects,and metabolic activity such as superoxide production
2. Humoral immunodeficienciesTotal and individual Ig level quantification by serum electrophoresis or ELISAB cell enumeration and surface marker expression by flow cytometryB cell activity by pokeweed and/or bacterial antigen stimulation
3. T cell immunodeficienciesT cell enumeration and surface marker expression by flow cytometryT cell activity using mitogens or antigen to examine proliferation, cytokineproduction via ELISA, or DTH skin responses
4. Combined immunodeficienciesT and B cell enumeration by flow cytometryT and B cell activity after mitogen stimulation as described aboveHistology of secondary lymphoid organs
5. Complement immunodeficienciesC3 and C4 level determination by immunoassay, or functional determination through the use of CH50 and AH50 measurement
Treatments for Immunodeficiencies 1. Treatment options and the source and rationale behind use of each treatmentIVIGStem cell transplantBone marrow transplant
2. Advantages3. Disadvantages
Subtopics are numbered, and examples are indicated by round bullets ( ). Advanced subtopics are indicated by square bullets ( ).
464 UNDERGRADUATE IMMUNOLOGY COURSE RECOMMENDATIONS ImmunoHorizons
https://doi.org/10.4049/immunohorizons.2100030
by guest on Decem
ber 10, 2021http://w
ww
.imm
unohorizons.org/D
ownloaded from

DISCLOSURES
The authors have no financial conflicts of interest.
ACKNOWLEDGMENTS
These recommendations could not have been developed without thededication and contributions of the following teaching-invested individ-uals: Carla J. Aldrich, Tzvia Abramson, Pierette Appasamy, Anil K.Bamezai, Tatiana Barichello, Fabian Benencia, Aimee Bernard, AlexBoyden, Deborah Brown, Catherine Brennan, Jack Bui, Gerald Buldak,Althea Campuzano, Benjamin Christmann, Sarah Collier, Maurizio Cos-tabile, Beckley K. Davis, Brittney Dinkel, Kerry Empey, Diana L. Flana-gan, Sherry Fleming, Fabiani Gai Frantz, John Frelinger, VitalyGanusov, Keith Garrison, Abby Geis, Jennifer Grier, Melanie GubbelsBupp, Jeniffer Hernandez, Katrina Hoyer, Gentaro Izumi, StephanieJames, Hans-Martin J€ack, Paula Kavathas, Brian Knoll, Ashwini Kuck-noor, Cynthia Anne Leifer, Kara Lukin, Lydia Lynch, Charitha Madir-aju, Jennifer Manilay, Clinton Mathias, Michelle Messmer, FernandoMonroy, Jeff Novack, Steve O�Barr, Kirstin Parkin, Todd Pearson, Nich-olas Pullen, Parameswaran Ramakrishnan, Jason Rawlings, Sarah BethRedmond, Sophia Sarafova, Jean L Scholz, Anil Shanker, Penny Shock-ett, Laurie Shornick, Keri Csencsits Smith, Doreen Szollosi, Steven Taf-fet, Rebekah Taylor, Yanet Valdez, Hector Valenzuela, MichaelViolin, Crystal Walline, Tim Wilson, and Heather Minges Wols. Wealso thank Krishna Foster, Andre Ellis, and Marla Parker for help-ful discussions on the statement on inclusive and antiracistteaching.
REFERENCES
1. Gregory, E., C. Lending, A. N. Orenstein, and J. P. Ellis. 2011. Redesigningintroductory biology: a proposal. J. Microbiol. Biol. Educ. 12: 13--17.
2. Cheesman, K., D. French, I. Cheesman, N. Swails, and J. Thomas.2007. Is there any common curriculum for undergraduate biologymajors in the 21st century? Bioscience 57: 516--522.
3. Bruns, H. A., J. Deaver, and L. B. Justement. 2019. Out of the curric-ular shadows: revolutionizing undergraduate immunology educa-tion. Front. Immunol. 10: 2446.
4. Justement, L. B., and H. A. Bruns. 2020. The future of undergradu-ate immunology education: can a comprehensive four-year immu-nology curriculum answer calls for reform in undergraduate biologyeducation? Immunohorizons 4: 745--753.
5. Bruns, H. A., B. D. Wisenden, T. Vanniasinkam, R. T. Taylor, S. L.Elliott, R. L. Sparks-Thissen, L. B. Justement, and S. Pandey. 2021.
Inside the undergraduate immunology classroom: current practicesthat provide a framework for curriculum consensus. J. Microbiol.Biol. Educ. 22: 22.1.8.
6. Anderson, T. R., and J. M. Rogan. 2011. Bridging the educationalresearch-teaching practice gap. Curriculum development, part 1:components of the curriculum and influences on the process of cur-riculum design. Biochem. Mol. Biol. Educ. 39: 68--76.
7. Horak, R. E., S. Merkel, and A. Chang. 2015. The ASM curriculum guide-lines for undergraduate microbiology: a case study of the advocacy roleof societies in reform efforts. J. Microbiol. Biol. Educ. 16: 100--104.
8. Seitz, H. M., R. E. A. Horak, M. W. Howard, L. W. KluckhohnJones, T. Muth, C. Parker, A. P. Rediske, and M. M. Whitehurst.2017. Development and validation of the microbiology for healthsciences concept inventory. J. Microbiol. Biol. Educ. 18: 18.3.54.
9. Kabelitz, D., M. Letarte, and C. M. Gray. 2019. Immunology educa-tion without borders. Front. Immunol. 10: 2012.
10. Di Rosa, F. 2020. Editorial: Serafino Zappacosta and the CeppelliniSchool: a pioneer model for nurturing education in immunology.[Published erratum appears in 2020 Front. Immunol. 11: 600832.]Front. Immunol. 11: 1524.
11. Parham, P. 2014. The Immune System, 4th Ed. W. W. Norton & Com-pany, Inc., New York.
12. Delves, P. J., S. J. Martin, D. R. Burton, and I. M. Roitt. 2017. Roitt�s Essen-tial Immunology, 13th Ed. JohnWiley & Sons, Inc., Bridgewater, NJ.
13. Punt, J., S. Stranford, P. Jones, and J. Owen. 2019. Kuby Immunol-ogy, 8th Ed. WH Freeman, Macmillan Learning, New York.
14. Murphy, K., and C. Weaver. 2017. Janeway�s Immunobiology, 9th Ed.Garland Science, Taylor & Francis Group, LLC, New York.
15. Ratcliffe, M. J. 2016. Encyclopedia of Immunobiology, 1st Ed. Aca-demic Press, Elsevier Ltd., Cambridge, MA.
16. Abbas, A. K., A. H. Lichtman, and S. Pillai. 2017. Cellular and Molecu-lar Immunology, 9th Ed. Elsevier Helath Sciences, Philadelphia, PA.
17. Jackson, A., M. A. Parker, L. T. DeVera, I. G. Zambrana, T. Holmes,E. Shiau, and C. Medina. 2018. Moving the needle: early findings onfaculty approaches to integrating culturally competent pedagogyinto educational spaces. J. Public Aff. 7: 119--145.
18. Slovacek, S., K. Soto, and K. Foster. 2019. Traditional vs. affilia-tion paths model for science student success. Adv. Soc. Sci. Res. J.6: 420--429.
19. Adams, M., and L. A. Bell, eds. 2016. Teaching for Diversity and SocialJustice, 3rd Ed. Routledge, New York.
20. Hilts, A., R. Part, and M. L. Bernacki. 2018. The roles of social influ-ences on student competence, relatedness, achievement, and reten-tion in STEM. Sci. Educ. 102: 744--770.
21. Rothstein, D., and L. Santana. 2011. Make Just One Change: TeachStudents to Ask Their Own Questions. Harvard Education Press,Cambridge, MA.
ImmunoHorizons 465
https://doi.org/10.4049/immunohorizons.2100030
by guest on Decem
ber 10, 2021http://w
ww
.imm
unohorizons.org/D
ownloaded from