amputations - a procedure no body wants or likes
TRANSCRIPT
AMPUTATIONS
Dr R S DhaliwalMBBS,MS,DNB(Surgery),M.Ch,DNB(CTVS),
FACS,FCCP,FICA,FNCCP,FIACS Former Prof & HOD , CTV
Surgery,PGIMER,Chandigarh

Amputation is one of the meanest yet one of the greatest operations
in surgery,i.e. mean- when resorted to where better may be done,
Great – as the only step to give comfort to patient and prolong life
- Sir William Ferguson
Amputation
• Amputation is the removal of a body part or an extremity (or its part) by surgery or by trauma or prolonged constriction . It is used to control pain or a disease process in the affected limb, such as malignancy or gangrene. In some cases, it is carried out on individuals as a preventative surgery for such problems

Amputation: the surgical removal of a part of the body, a limb or part of a limb for gangrene, tumours severe trauma or infection for saving life of patient

Etiology
• Land mine injuries
• War & Terroism injuries
• Road side accidents
• Industrial trauma
• Criminal activity
• Punishment for crimes
• Surgical for dieases
Statistics Lower limb amputations are 4 times more common than upper limb
(infection) .
While over 90% of amputations caused by vascular disease involve the lower limb, nearly 70% of amputations caused by trauma involve the upper limb For both males and females, risk of traumatic amputations increased steadily with age, reaching its highest level among people age 85 or older
Limb amputations resulting from cancer most commonly involved the lower limb; above-knee and below-knee amputations alone accounted for more than a third (36 percent) of all cancer-related amputations.
There were no notable differences by sex or race in the age-specific risk of cancer-related amputations, though rates of limb loss due to cancer were generally higher among individuals other than African Americans.
In all age groups, the risk of dysfunctional vascular related amputation was highest among males and individuals who are African American
Indications for Amputation
• Dead limb - Gangrene
• Deadly limb - Wet gangrene- Spreading cellulitis
- Multiple or huge AV fistula- Bone or soft tissue tumour
. Dead loss limb – Severe rest pain - Sever contracture or paralysis making it impossible to use and it is a hinderance-Major unrecoverable traumatic damage

Indications
• Gangrene due to atherosclerosis,embolism, diabetes,Beurger’s disease , ergots poisoning
• Trauma – Massive crush injury ,to save life
• Tumours – Bone and soft tissue tumours(osteosarcoma, chonderosarcoma,melanoma, Sq cell carcinoma(Marjolin’s ulcer)
• Gas gangrene . Severe sepsis
• Dead,dying, devitalised tissue
• Severe defformity –congenital or acquired
Causative Factors of Amputations
Peripheral arterial disease
Diabetes Mellitus
Gangrene (due to the complication of fracture
or tight plaster cast ) .
Trauma (crushing, frost bite, burns)
Congenital deformities
Chronic Osteomyelitis
Malignant Tumors


General • Amputation is considered as treatment when a
limb or its part is dead , deadly or is dead loss
• Dead limb – Occurs due to severe arterial occlusive disease causing death of tissues i.e. gangerene. The occlusion may be in major vessels (atherosclerosis or embolic) or in small peripheral vessels (diabetes,Buerger’s disease, Raynaud’sdisease or accidental intra arterial injection.If the obstuction can not be reversed and symptoms are severe, amputation is required.

General• Deadly limb- Limb becomes deadly when
putrefaction and infection of moist gangrene spreads to surrounding viable tissues leading to cellulitis and severe toxaemia.It is dangerous to life of patient .Massive broad spectrum antibiotic cover is a must
• Dead loss limb – A limb may seem dead loss when there is relentless, severe rest pain with out gangrene, here amputation will improve quality of life. When a limb is impossible to use and becomes a hinderance in daily activity as in paralysis or severe contracture or major traumatic damage amputation is done to improve quality of life
Pre-operative Assessment
Neurovascular and functional status of extremity
Function and Condition of residual limb (in case of
traumatic amputation)
Circulatory status and function of unaffected limb
Signs & Symptoms of infection (culture required)
Nutritional Status
Concurrent medical problems
Current medications
Evaluation of Patients for amputation
• Check for anemia – correct it by blood or packed cells transfusion
• Control of infection using antibiotics and dressings
• Informed consent for operation from patient or his close family members (v.imp)
• Decide level of amputation by skin temp. and arterial doppler study
• Psychological counciling of patient-very important
• Plan for prosthesis and rehabilitation by physiotherapist and rehabilitation team

Psychological Support
Emotional reaction to amputation
Circumstances surrounding amputation
(ie. Traumatic versus surgical)
Occupational and social Rehabilitation
Types of Amputations• Major amputations-
- Transcondylar femoral level (GrittiStokes amputation )
- Above knee, below knee or through knee amputation
- Syme’s ampuatation – below ankle
• Minor amputations -Distal and transmetacarpal and metatarsal
amputations

Types
• Weight bearing• Non weight bearing
It can be : • Non- end bearing/ side bearing- Wt is taken up by
the joint • End bearing/ cone bearing- Wt is taken up by the
body of patient It can be - Provisional amputation with flap, later finial formal amputation may be done
. Guillotine amputation- It always requires revision formal amputation
. Formal amputation – It is deffinitive procedure

Amputations• Types of Flaps-
-Long posterior flap in B/ K amputation- Equal flaps in A/K amputation
• Ideal Stump--Should heal adequately by 1st intention - Should have rounded gentle contour with
adequate muscle padding
• Should have sufficient length to bear prosthesis> For B/K amputation 7.5 to 12.5 cms from tibial tuberosity> For A/K 23cms from greater trochanter> For above and below elbow 20 cms stump
Different Amputations
• Ray amputation- Amputation of toe with head of metatarsal or metacarpal
• Gillies ( Transmetatarsal ) –Amputation proximal to neck ,distal to base of metatarsal
• Lisfranc’s( Tarsometatarsal) – The tarso meta tarsal joint is disarticulated
• Chopart’s ( Mid tarsal)- Talonavicular and calcaneo cuboid joints are disarticulated
• Syme’s –Tibia and fibula are cut just above ankle joint to remove foot

Different Amputations• Burgess (below –knee amputation) – Long
posterior flap is made so that scar is anterior Stump length is 14-17 cms, minimum 8cms
• Peg- leg amputation - It is done 5 cms below knee joint, anterior flap is rotated postly. Like a hood. Pt kneels and bears wt on this.It is only done when patient can not afford or bear prosthesis limb.Uncommon
• Gritti- Stokes (transcondylar)- It is done through knee joint, patella is anchored to divided femur.Not done these days
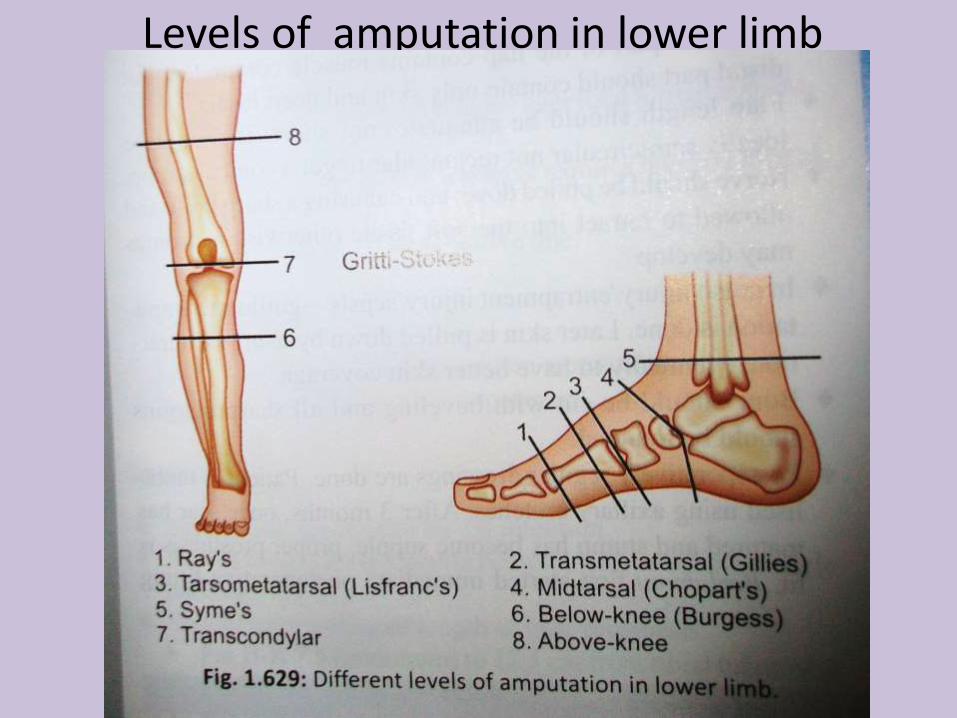
Levels of amputation in lower limb
Different amputations• Above knee A/K amputation- Equal anterior and
posterior flaps, ideal femur stump should be 25 cmslong.Not done in children as growing epiphysis of femur is in lower end. Minimum stump should be 10cms long. It is technically easy, healing chances are better and faster. Cosmetic results poor, prosthesis fitting is not proper, pt limps while walking and need support
• Hip disarticulation- It is done when minimum 10cms stump is not possible in A/K amputation. Single posterior flap –Solcum approach(better) or anterior racquet incision –Boyd’s approach
• Hind quarter amputation or Hemipelvectomy-( Sir Gordon Taylor’s amputation) One side pelvis with iliac bone, pubis muscles and vessels along with lower limb are removed. Internal and external vessels are ligated.Internal hemipelvectomy is new method where lower limb is saved
Different amputations
• Krukenberg’s amputation- Done in upper limb through forearm. A claw like gap is left between radius and ulna which is used for a grip or holding some thing
• Forequarter amputation ( Interscapulothoracicamputation)-It is removal of upper limb with scapula and lateral 2/3rd of clavicle and muscles .It is done for tumours of scapula,upper part of humerus and near shoulder joint It can be done through Littlewood’s posterior approach or Berger’s anterior approach.
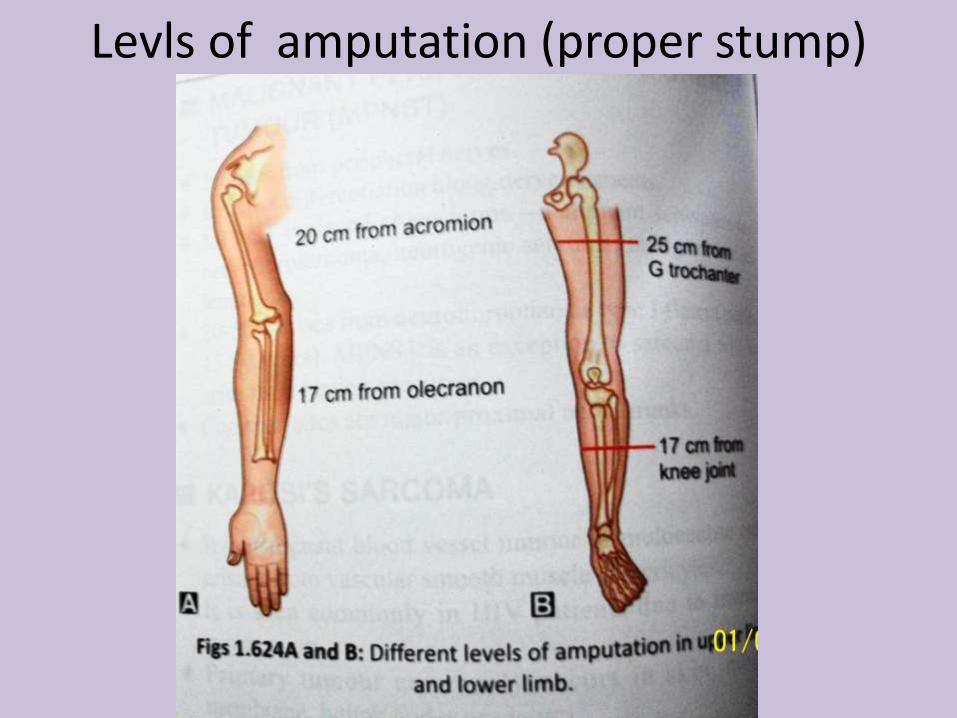
Levls of amputation (proper stump)
Post operative period & Complications
• Regular dressings are done
• Physiotherapy is started as early as possible
• Pt uses crutches for walking, Prosthesis is fitted after 3 months
• Rehablitation is started
• Complications-Early - Haemorrhage, hematoma, Infection Late- Pain, Ulceration at stump, Flap
necrosis, Painful scar, Phantom limb – feeling of amputated part partially or in toto with pain over it.
Prosthesis or Artificial limbs
• A prosthesis a is an artificial device that replaces a missing body part or a limb ( or its part ) lost due to trauma, disease, or congenital conditions.
• These are devices to make shape and function of the residual limb and help patient readapt to his job and life style

Prosthesis or Artificial limbs
• In Lower Limb-1 Syme’s amputation-Elephant boot,CanadianSyme’s prosthesis 2. Below Knee amputation- Patellar tendon bearing (PTB) prosthesis and solid ankle cushion heel (SACH)3.Above Knee amputation- Suction type prosthesis, it is placed above the stump.It is better and well tolerated4.Nonsuction type prosthesis- It is placed at the end.It requires additional support 5.Hind quarter amputation- Tilting table prosthesis or Canadian prosthesis is used
Prosthesis• Upper Extremity prosthesis-
a.Partial hand amputation- Cosmetic glove b.Wrist disarticulation- Plastic laminate socket
with triceps cuff and wrist unit with terminal devicec.Below elbow amputation- Same as wrist disarticulation but with different socket confg.
d.Elbow disarticulation- cosmetically undesirable as outside locking elbow hinge is bulky e.Above elbow amputation- The unit has internal locking system and turn table which permits passive control of rotation. Elbow joint lock is controlled by shoulder depression and terminal device is operated by scapular abduction or shoulder flexion
Prosthesis
• Myoelectric prosthesis ( Externally powered prosthesis)- It is self suspending unit with electrodes embeded in the prosthetic socket. Electrodes detect muscle action potential form contracting muscles in residual limb.The signals are amplified,rectified,modulated to run an electric motor to do desired function. These prosthesis are costly, weigh more and not reliable. They provide only coarse movements with out sensory feedback which is most important function of hand
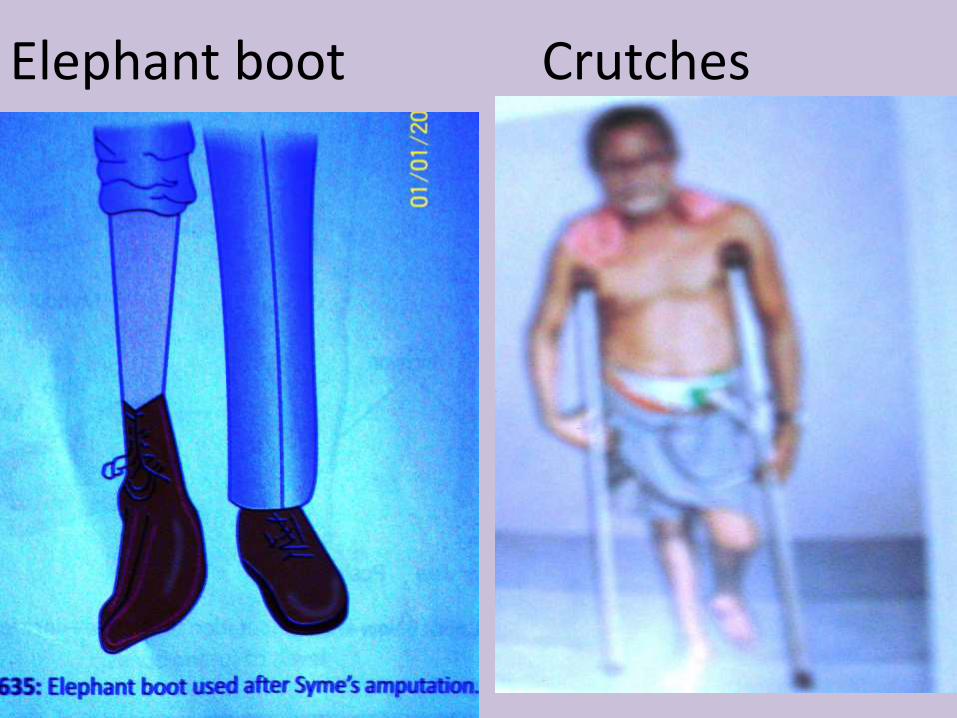
Elephant boot Crutches
Lower limb prosthesis• Toe amputation- Shoe with filler
• Partial foot amputation- Moulded plastic foot support with toe filler and rigid extension in the shoe
• Syme’s amputation- Prosthesis similar to B/K amputation prosthesis( PTB)
• Below Knee B/K amputation- Patellar tendon bearing (PTB) prosthesis made up of socket, shin piece and SACH foot. It has a thigh corset for suspension along with side knee joints
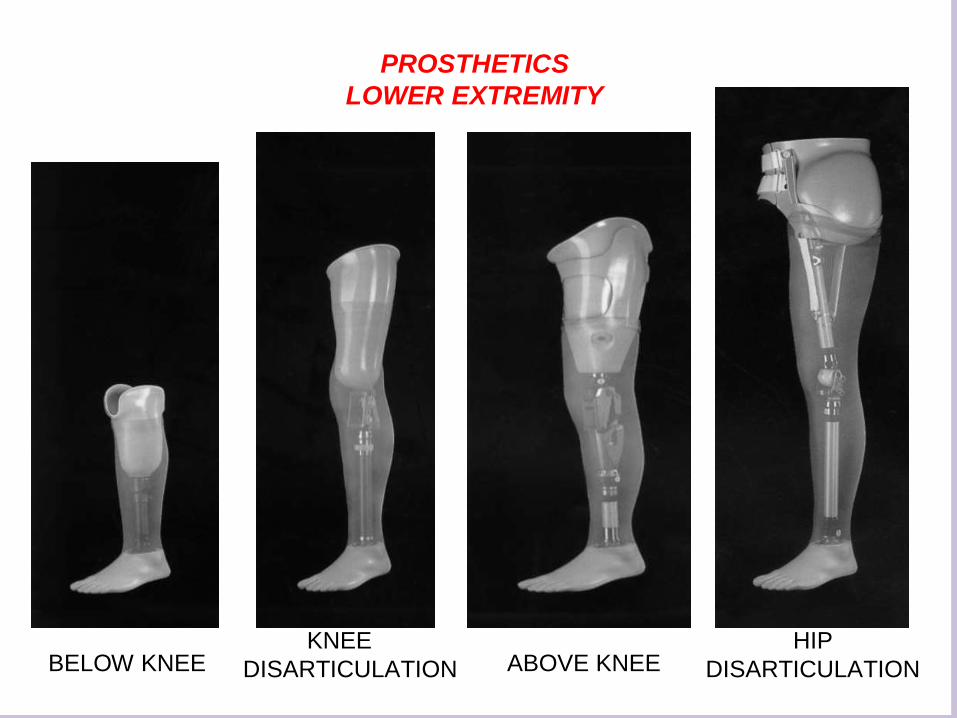
Types of Prosthesis
BELOW KNEEKNEE
DISARTICULATION ABOVE KNEEHIP
DISARTICULATION
PROSTHETICS
LOWER EXTREMITY
Lower limb prosthesis• Jaipur foot- It is Indian modification for bare foot walking
made of vulcanized rubber and shaped like normal foot.Itis flexible and is helpful in walking on uneven surfaces
• SACH foot( Solid Ankle Cushioned Heel)- It is most commonly used foot.It has no mechanicle ankle joint .The cushioned heel stimulates the plantar flexion motion.
• Endoskeletal prosthesis- It uses aluminium, titanium, graphite and tubular material to form central supporting structure and have modular or interchange able connectors and components like knee and feet.Thestructural strength is derived from central skelton like components.It is covered by foam material like skin.
• Exoskeletal prosthesis- there is outer plastic laminated skin or shell with wood or poly urethane foam interiors.Herestrength is provided by outer lamination and shape is an integral part of prosthesis
Lower limb prosthesis
• Above Knee prosthesis- It has four major parts the socket, the knee system,the shank and foot ankle system.A variety of sockets (quadri lateral, ischial containment, CAD-CAM designed) knee joints(constant friction, hydraulic, polycentric etc) shanks( wood, metal ,composite),foot ankle assembly(SACH,Jaipur foot,energing storing foot,Madras foot etc).These can be combined to make custom made.It does not permit squat or sit cross legged on ground. AIIMS modification allows these movements to patient.
Prosthesis or Artificial limb• Patellar tendon bearing prostheiss (PTB
Prosthesis)- All the wt bearing is done below knee, movement is controlled by his own knee joint.Patellar tendon is main wt bearing area within the socket.
• CAD –CAM made socket – It is an automated processing method to make prosthesis.It is more comfortable ,made of thermoplastic or laminated plastic with polyethylene foam
• Suspension for B/K amputation prostheis is leather cuff strap above femoral condyles.Exo or endoskeleton is used.Endo skelton is preferred in athletics
• SACH (Solid Ankle Cushion Heel) foot- Needs minimal maintenance,preferred in old people


Upper limb prosthesis
• Above elbow prosthesis is a high technology prosthesis with harness, socket, elbow joint unit ,control cable, forearm and wrist device.
• Below elbow prosthesis- Krukenberg’samputation does not require any prosthesis Advantages of Prosthesis--Cosmetic - Function of the part is
gained to some extent - Ambulation in lower limb prosthesis
Prosthesis or Artificial limb
• Disadvantages-- Infection - Pressure ulcers
- Joint disability
• Prosthesis Types-- Exoskeletal prosthesis-fixed with belts and
brces to remaining limb or stump- Endoskeletal prosthesis with
modular system Internal prosthesis are used inside body ,placed by open surgery.These are non reactive long durable materials.e.g hip prosthesis for hip replacement
There are 5 Stages of Rehabilitation:
1. Healing and Starting Physiotherapy
2. Visiting the Prosthetist
3. Choosing an Artificial Limb
4. Learning to Use your Artificial Limb
5. Life as a New Amputee
THANK YOU