amr hassan mostafa, md, fscai a. professor of cardiology cairo university cairo, egypt egypt combat...
TRANSCRIPT
Amr Hassan Mostafa, MD, FSCAI
A. Professor of Cardiology
Cairo University
Cairo, Egypt
Egypt Combat MI, March 24-25, Cairo Sheraton
Definitions – Acute coronary syndrome
Any constellation of clinical symptoms that are compatible with acute myocardial ischemia.
It encompasses a spectrum from
AMI NSTEMI UA NSTEMI – acute process of myocardial
ischemia resulting in myocardial necrosis.The initial ECG does not show ST elevation
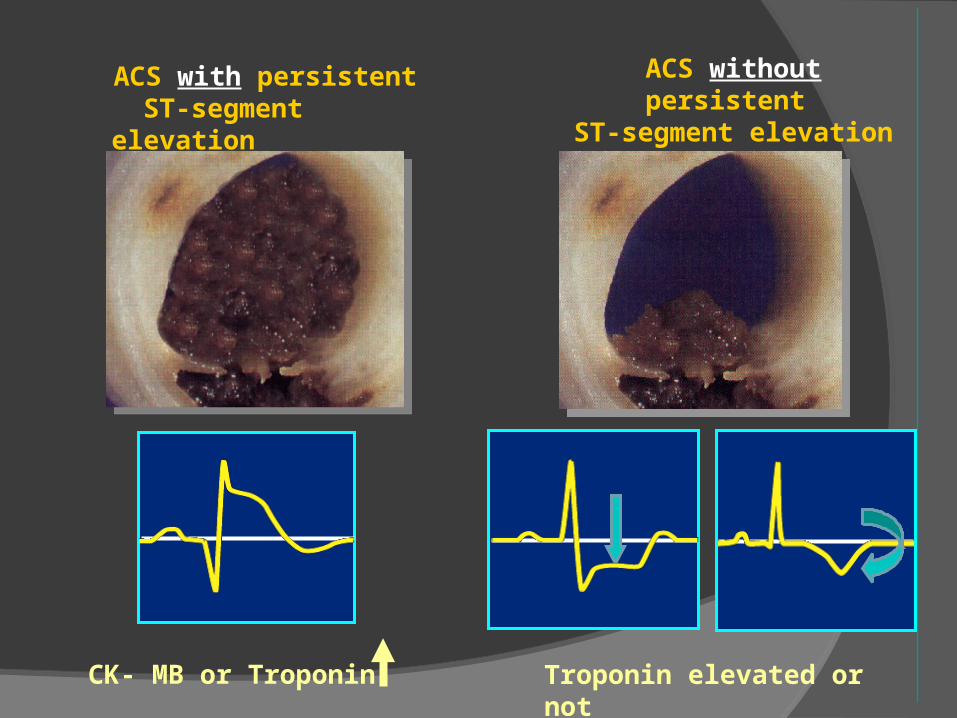
CK- MB or Troponin Troponin elevated or not
ACS without persistent
ST-segment elevation
ACS with persistent ST-segment elevation
Non ST Elevation Acute Coronary Syndrome
A heterogeneous population Varying risks of early and long-term
adverse events Early risk stratification at admission is
essential for a tailored therapeutic strategy
Various ACS risk scores are
available
Why be concerned re risk stratification………
Are the symptoms a manifestation of ACS?
Therapy/ site of care will vary dependent on diagnosis
To determine prognosis/short term survival
To determine need for early revascularization
ACS Risk Scores
TIMI: Thrombolysis In Myocardial Infarction
PURSUIT: Platelet glycoprotein IIb/IIIa in Unstable agina: Receptor Suppression Using Integrilin
GRACE: Global Registry of Acute Coronary Events
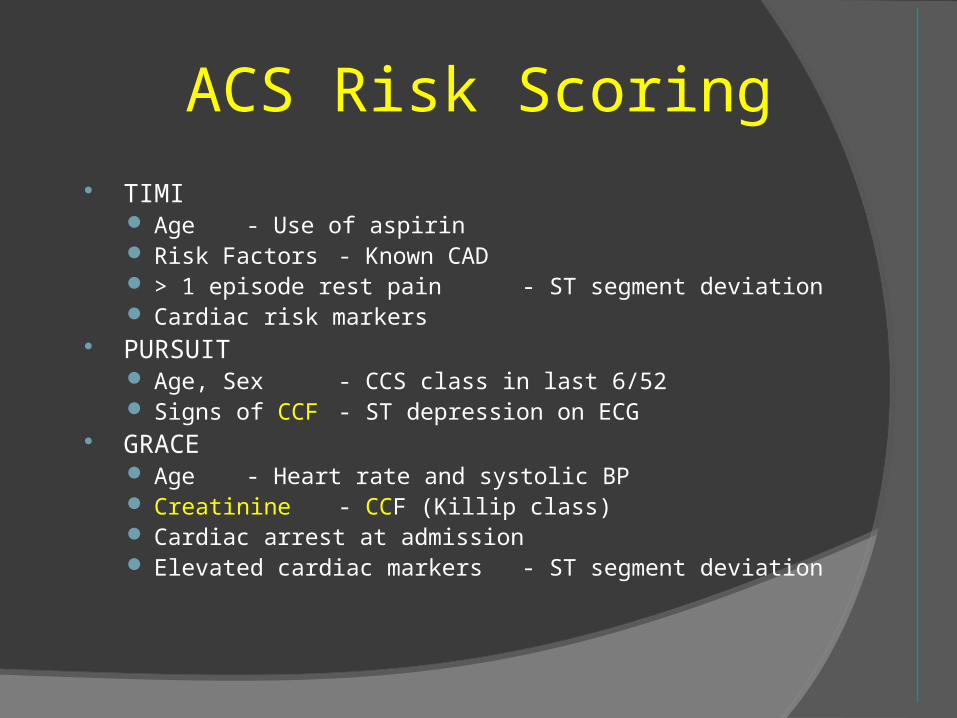
ACS Risk Scoring TIMI
Age - Use of aspirin Risk Factors - Known CAD > 1 episode rest pain - ST segment deviation Cardiac risk markers
PURSUIT Age, Sex - CCS class in last 6/52 Signs of CCF - ST depression on ECG
GRACE Age - Heart rate and systolic BP Creatinine - CCF (Killip class) Cardiac arrest at admission Elevated cardiac markers - ST segment deviation
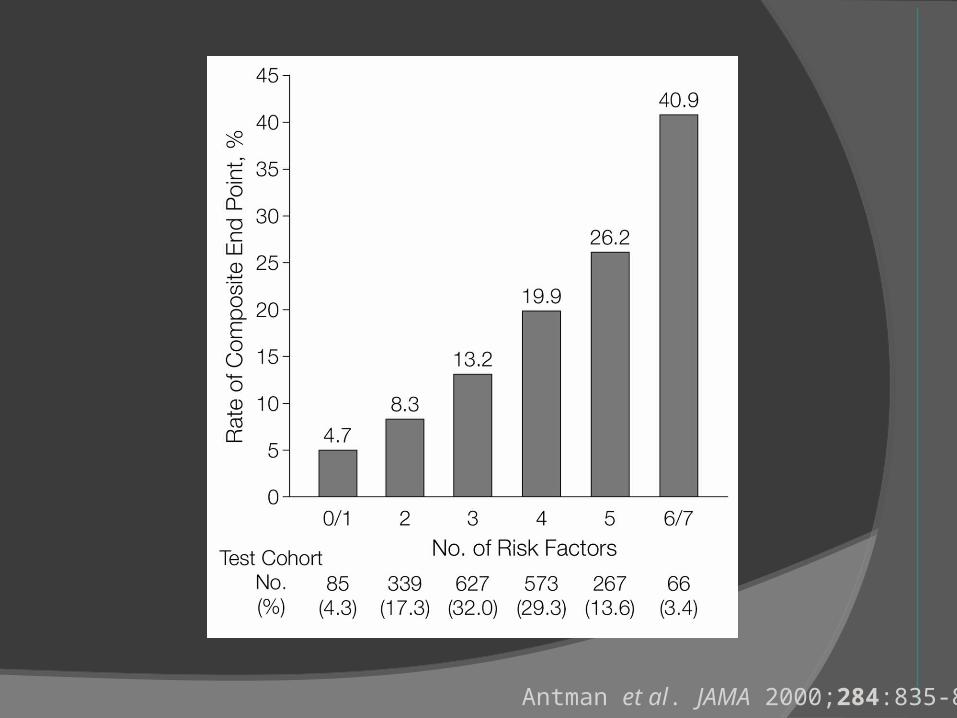
TIMI Risk Score
Age ≥ 65 years ≥3 Risk factors for coronary artery disease Significant coronary stenosis ST Segment deviation Severe anginal symptoms (≥2 anginal events
in last 24 hours) Prior aspirin use (within last 7 days) Elevated serum cardiac markers
Antman et al. JAMA 2000;284:835-842
ACC/AHA/SCAI 2007 PCI Guidelines Focused Update
9
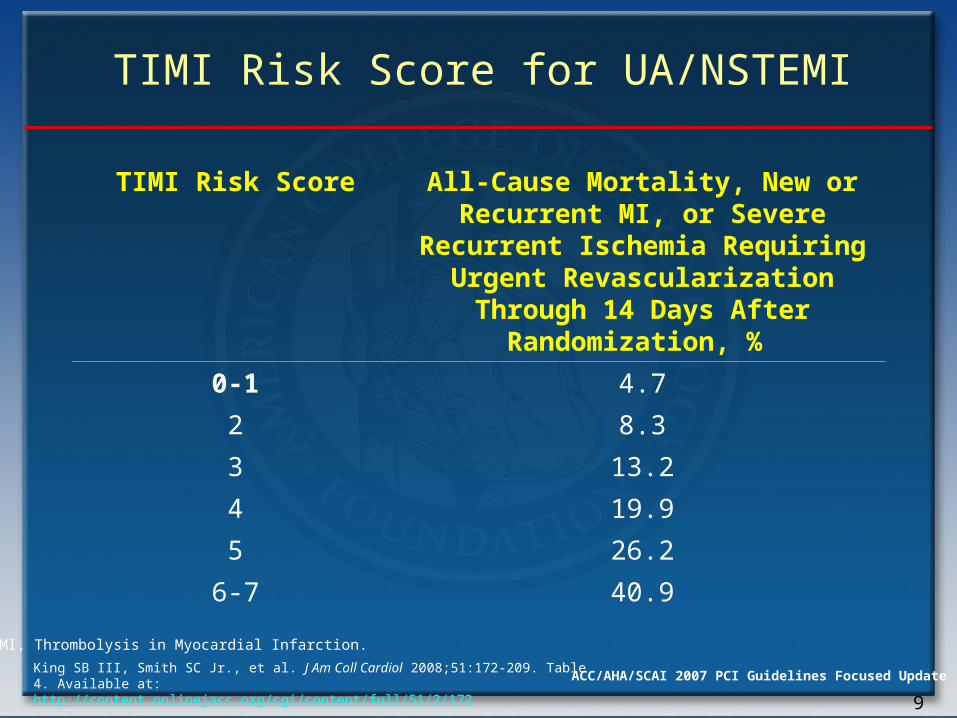
TIMI Risk Score for UA/NSTEMI
TIMI Risk Score All-Cause Mortality, New or Recurrent MI, or Severe
Recurrent Ischemia Requiring Urgent Revascularization
Through 14 Days After Randomization, %
0-1 4.7
2 8.3
3 13.2
4 19.9
5 26.2
6-7 40.9
TIMI, Thrombolysis in Myocardial Infarction.
King SB III, Smith SC Jr., et al. J Am Coll Cardiol 2008;51:172-209. Table 4. Available at: http://content.onlinejacc.org/cgi/content/full/51/2/172
Antman et al. JAMA 2000;284:835-842
ACS Risk Scoring TIMI
Age - Use of aspirin Risk Factors - Known CAD > 1 episode rest pain - ST segment deviation Cardiac risk markers
PURSUIT Age, Sex - CCS class in last 6/52 Signs of CCF - ST depression on ECG
GRACE Age - Heart rate and systolic BP Creatinine - CCF (Killip class) Cardiac arrest at admission Elevated cardiac markers - ST segment deviation
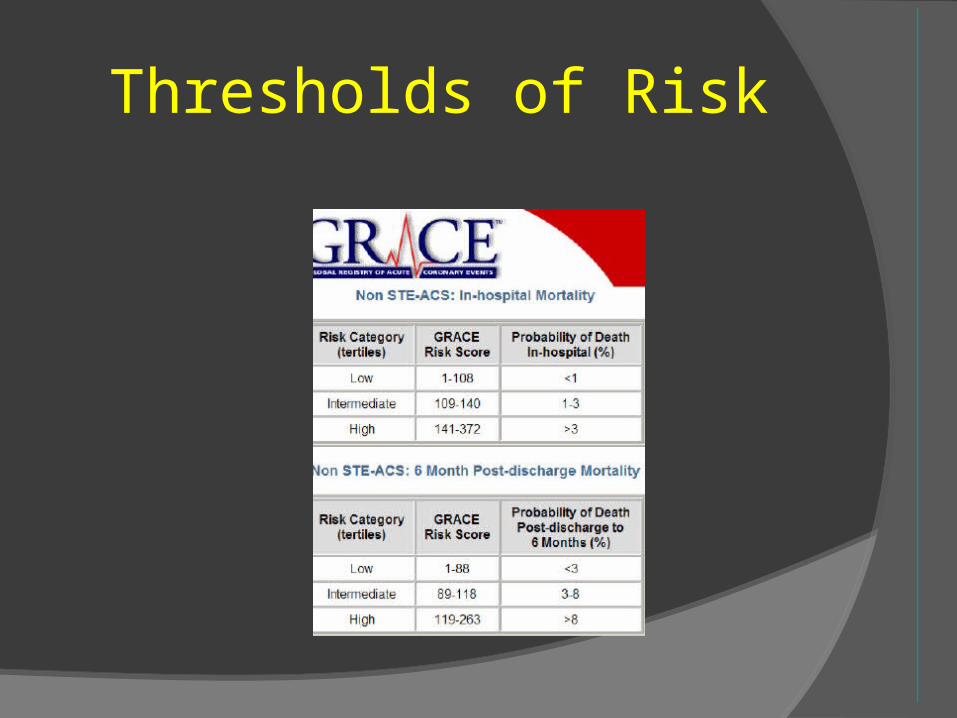
Thresholds of Risk
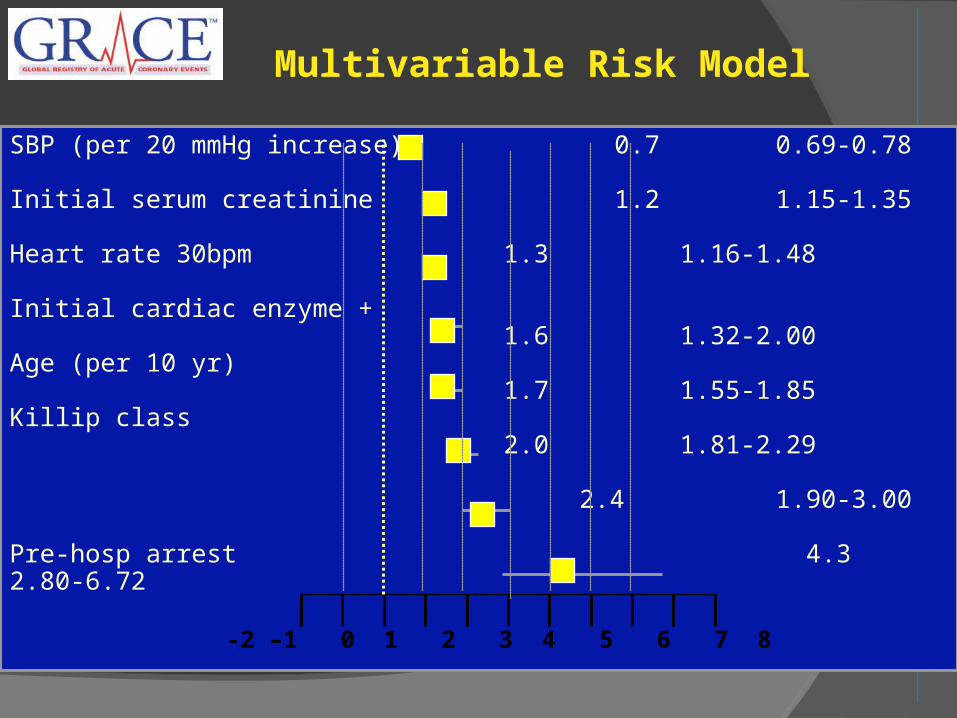
SBP (per 20 mmHg increase) 0.7 0.69-0.78
Initial serum creatinine 1.2 1.15-1.35
Heart rate 30bpm 1.3 1.16-1.48
Initial cardiac enzyme + 1.6 1.32-2.00
Age (per 10 yr) 1.7 1.55-1.85
Killip class 2.0 1.81-2.29
2.4 1.90-3.00
Pre-hosp arrest 4.3 2.80-6.72
-2 –1 0 1 2 3 4 5 6 7 8
Multivariable Risk Model
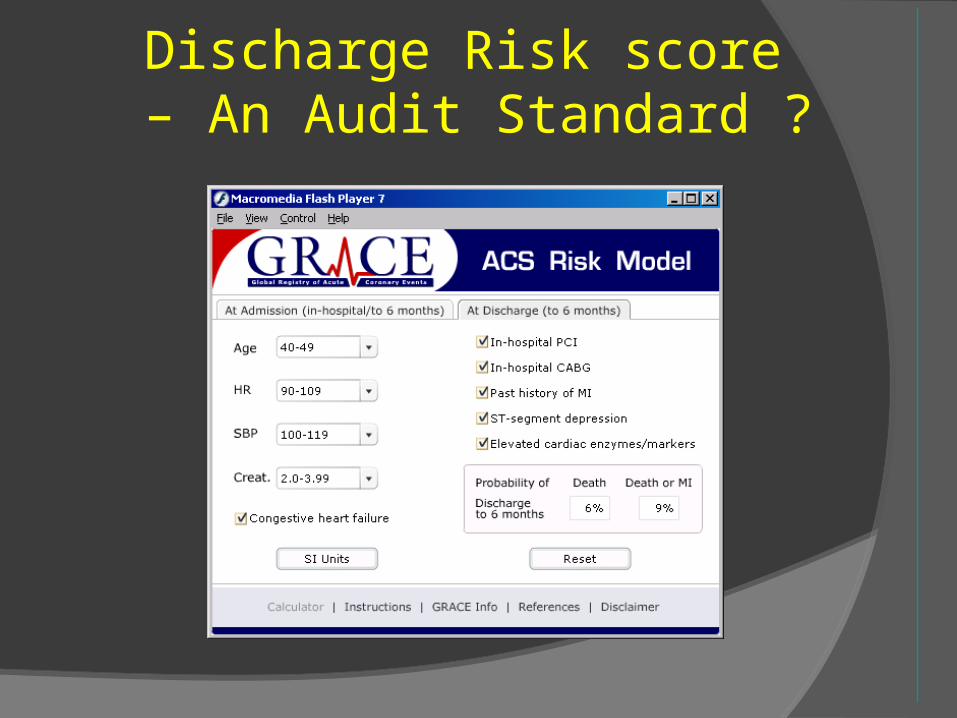
Discharge Risk score – An Audit Standard ?
Unique Features of GRACE
Multi-national perspective Full spectrum of coronary syndromes Increased data on demographics,
presentation, management and outcome Regular audits of data quality Feedback to participating sites 6-month follow-up
ACS Risk Scoring TIMI
Age - Use of aspirin Risk Factors - Known CAD > 1 episode rest pain - ST segment deviation Cardiac risk markers
PURSUIT Age, Sex - CCS class in last 6/52 Signs of CCF - ST depression on ECG
GRACE Age - Heart rate and systolic BP Creatinine - CCF (Killip class) Cardiac arrest at admission Elevated cardiac markers - ST segment deviation
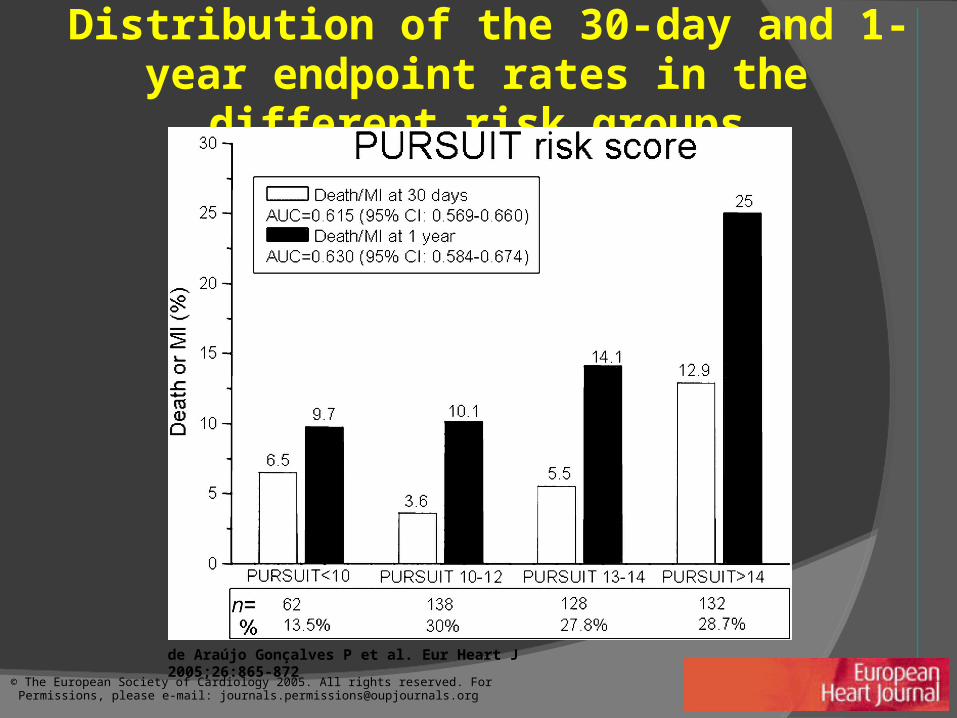
Distribution of the 30-day and 1-year endpoint rates in the different risk groups
de Araújo Gonçalves P et al. Eur Heart J 2005;26:865-872
© The European Society of Cardiology 2005. All rights reserved. For Permissions, please e-mail: [email protected]
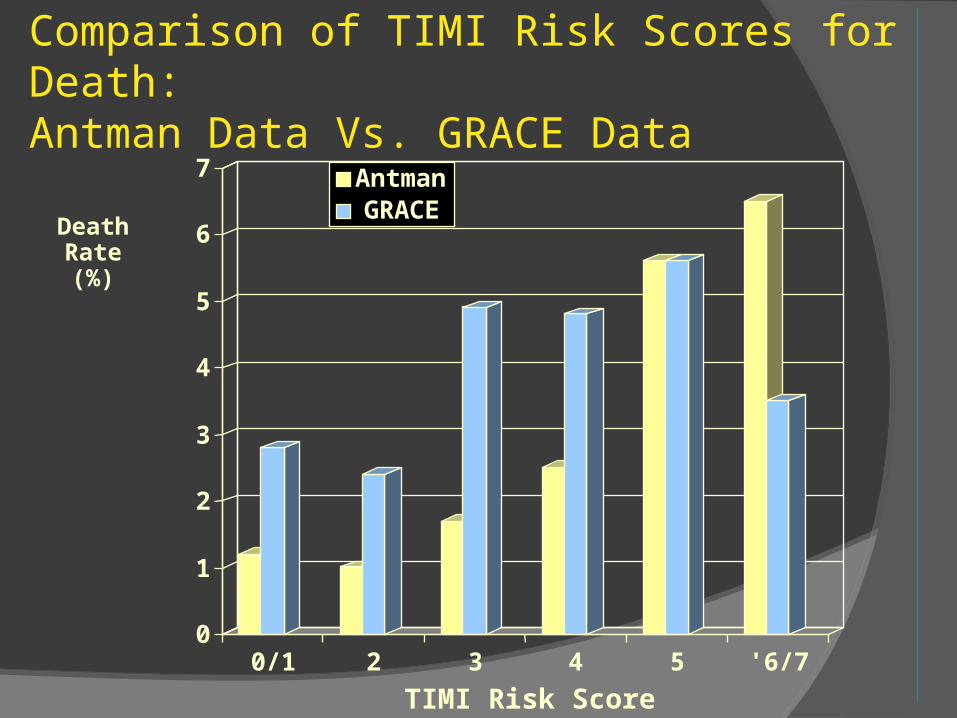
Comparison of TIMI Risk Scores for Death: Antman Data Vs. GRACE Data
0
1
2
3
4
5
6
7
0/1 2 3 4 5 '6/7
TIMI Risk Score
AntmanGRACE
DeathRate(%)
ACC/AHA/SCAI 2007 PCI Guidelines Focused Update
Confounding Factors Risk scores are largely developed from
registries & not CRT’s High risk pts usually receive more
aggressive antithrombotics & early revascularisation
Risk scores can only predict short term prognosis as they do not include important coronary anatomic or physiologic information
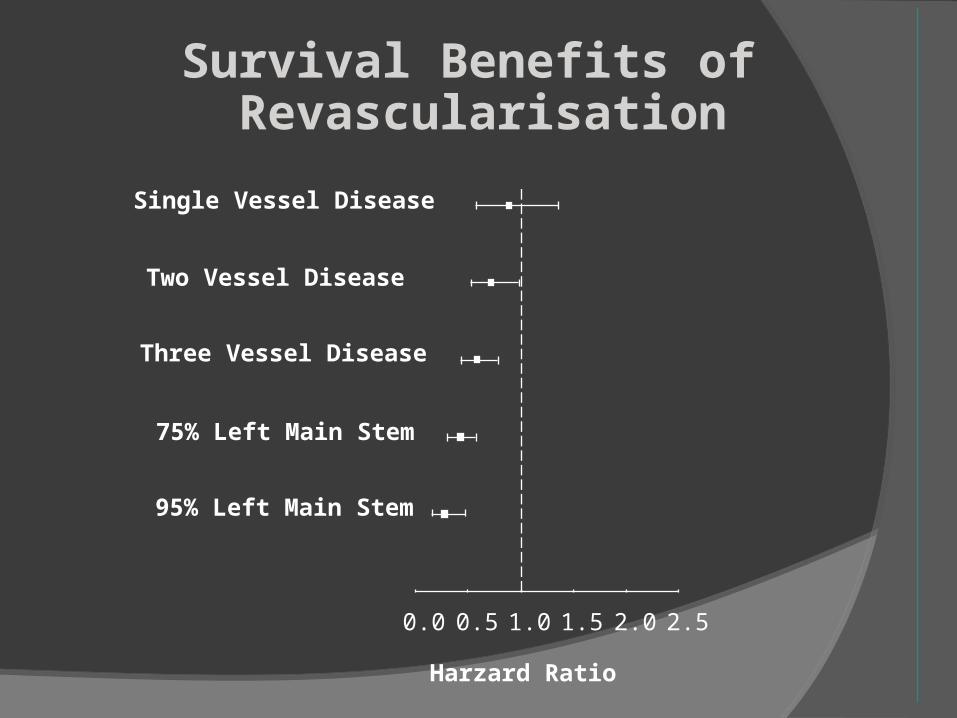
Single Vessel Disease
Two Vessel Disease
Three Vessel Disease
75% Left Main Stem
95% Left Main Stem
0.0 0.5 1.0 1.5 2.0 2.5
Harzard Ratio
Survival Benefits of Revascularisation
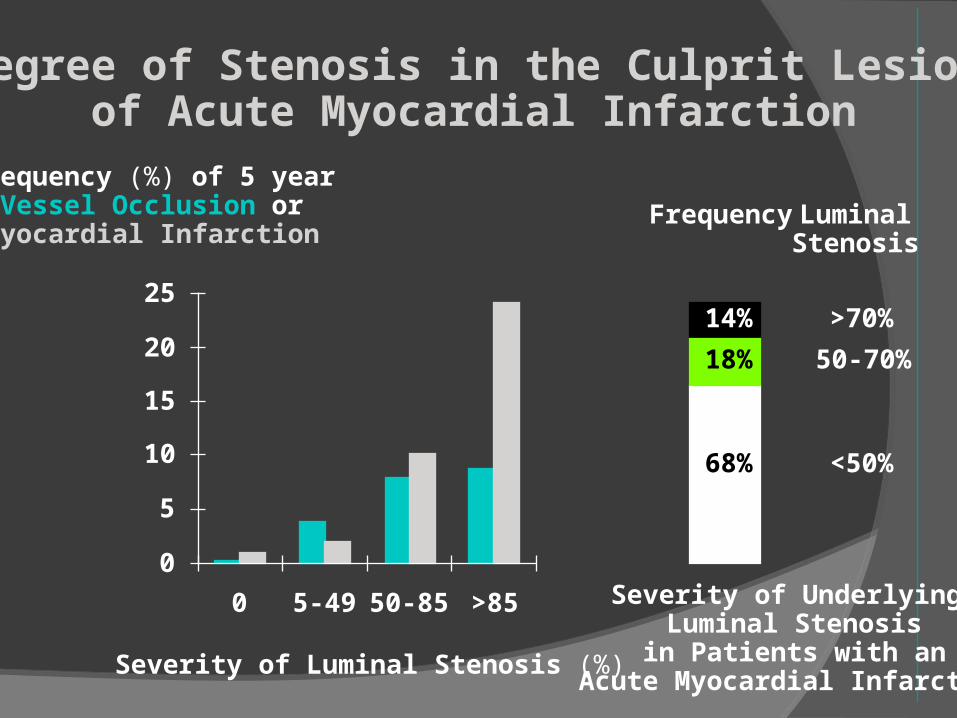
25
20
15
10
5
0
0 5-49 50-85 >85
Severity of Luminal Stenosis (%)
Frequency (%) of 5 yearVessel Occlusion or
Myocardial Infarction
<50%
50-70%
>70%
68%
18%
14%
Severity of Underlying Luminal Stenosis
in Patients with anAcute Myocardial Infarction
LuminalStenosis
Frequency
Degree of Stenosis in the Culprit Lesionof Acute Myocardial Infarction

ACS Risk Scoring
TIMI Age - Use of aspirin Risk Factors - Known CAD > 1 episode rest pain - ST segment deviation Cardiac risk markers
PURSUIT Age, Sex - CCS class in last 6/52 Signs of CCF - ST depression on ECG
GRACE Age - Heart rate and systolic BP Creatinine - CCF (Killip class) Cardiac arrest at admission Elevated cardiac markers - ST segment deviation
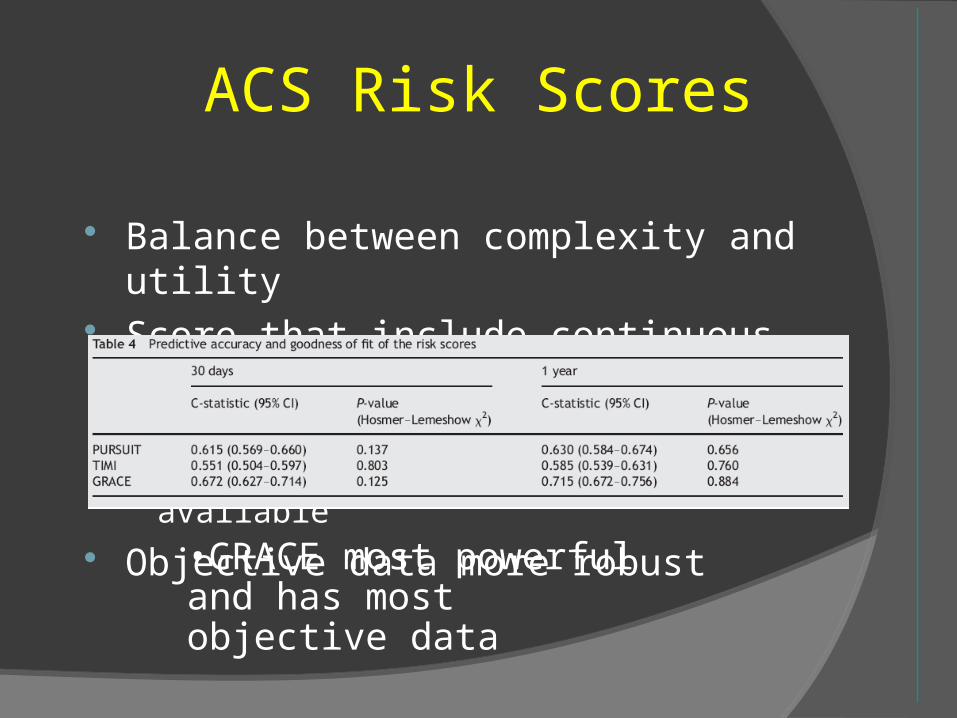
ACS Risk Scores
Balance between complexity and utility Score that include continuous variables
more powerful but more complex to computeSimple PC/PDA programmes now available
Objective data more robust
•GRACE most powerful and has most objective data

Risk AssessmentIn
Acute Coronary Syndromes
Evaluation of Treatment BenefitIn
Acute Coronary Syndromes
Take Home Message
• All risk scores were developed to predict short term prognosis
• GRACE risk scoring appears the most predictive of short & intermediate term prognosis
• GRACE risk scoring includes CHF & renal dysfunction at the time of presentation with ACS

Take Home Message
• Risk scores need to be carefully applied
• Risk scores may be population dependent and not reflect ‘true life’ populations
• Low risk is not no risk• High risk does not equate to most
benefit from intervention