an approach to the immigrant disclosures patient wheeler.keller...an approach to the immigrant...
TRANSCRIPT

2/23/2017
1
An Approach to the Immigrant Patient
Margaret Wheeler MD and Devora Keller MD
Disclosures
• We have benefitted directly and indirectly from having recent immigrants in our community– Indirectly through taxation, cultural vibrancy,
research, agriculture, construction, restaurant work etc.
– Directly through adoption, friendships, colleagues, personal health care; health care for family members; child care; home repair and cleaning; laundry and the list goes on….
Objectives
• Review recent trends in US immigration
• Introduce an approach to immigrant health
• Review legal issues important caring for undocumented patients
World Wide Era of Unprecedented Migration
• Growing numbers of migrants world-wide
• More refugees now than at end of WWII
• US country with highest # of immigrants– California state with highest # immigrants/
and highest # undocumented immigrants
2/23/2017
2
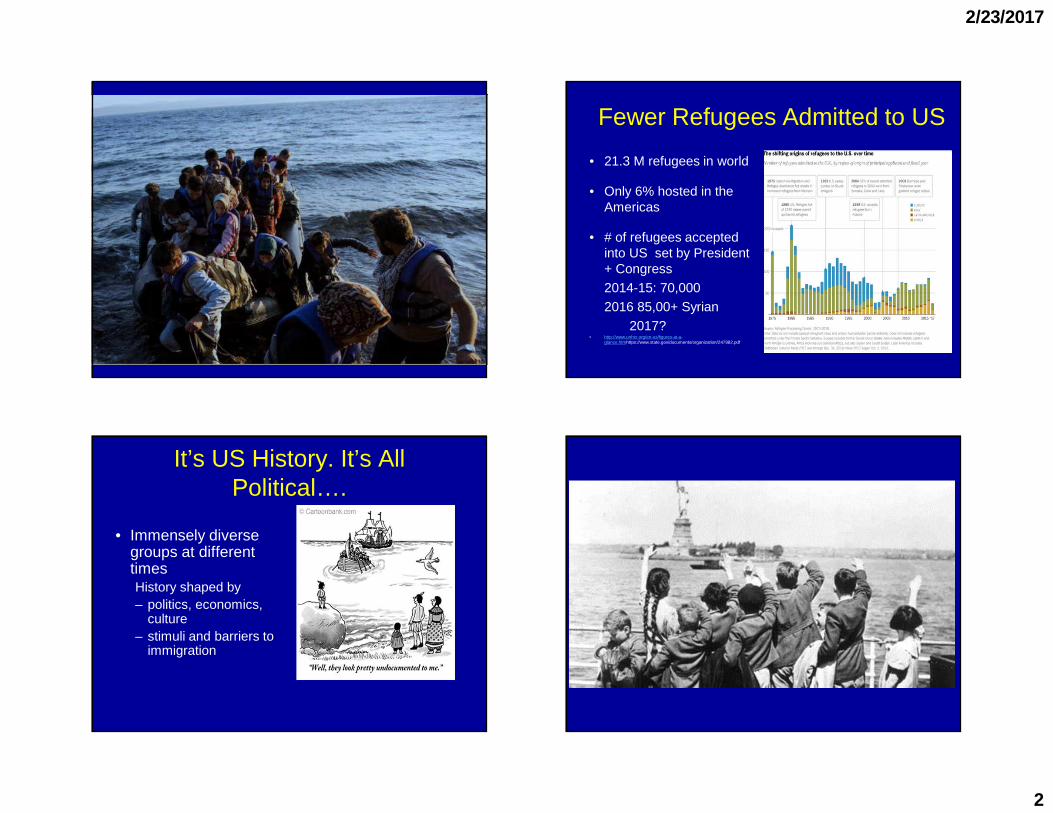
Fewer Refugees Admitted to US
• 21.3 M refugees in world
• Only 6% hosted in the Americas
• # of refugees accepted into US set by President + Congress2014-15: 70,000 2016 85,00+ Syrian
2017?• http://www.unhcr.org/en-us/figures-at-a-
glance.htmhttps://www.state.gov/documents/organization/247982.pdf
It’s US History. It’s All Political….
• Immensely diverse groups at different timesHistory shaped by– politics, economics,
culture – stimuli and barriers to
immigration

2/23/2017
3
US Immigration Over Time
Immigration Since 1860• Today 13.3% (42.4 million) of US population foreign born (FB) • ½ citizens
• ¼ here legally; ¼ without documentation
» Pew, 2016
• 26% FB or children of FB• ¼ US children have at
least 1 FB parent
Shift from Europe to LA and Asia
The Immigrant SES Hourglass
• 20% of low wage workers are immigrants– 70% farmworkers– 75% home-healthcare aides
• 25% of physicians are FB• 22% of STEM workers FB
• More FB with advanced degrees than NB• More FB with low education
– Pew, 2013
American Community Survey

2/23/2017
4
Undocumented Immigration• Decrease since 2008• Half Mexico; Asia/LA
• Net benefit to economy$12 billion in payroll/SSA taxes
» Goss, 2013 https://www.ssa.gov
State and local taxes–$10.5 billion in 2010
Institute on Taxation and Economic policy, 2013 http://www.itep.org
Mixed Status Families
• Nearly 2/3 of undocumented in US for over decade
• 4 million US born children have one UD parent
• 6-10% of K-12 students have at least one UD parent
An Approach to Immigrant Patients:Three Considerations
• Health risks of native country
• Health risks of travel– both initial and recurrent
• Health risks of adopted country
Risks of Native Country
• Epidemiology of diseases– Higher risk exposure to infectious diseases, environmental
exposures, geography of genetic disorders
– High rate of chronic disease in developing world
• Epidemiology of stressors – Politics/economics/natural disasters– Keeping up current events as important as med updates
• Health care access and practices - Vaccinations, chronic disease care, medication use

2/23/2017
5
An Approach to Immigrant Health
• Health risks of native country
• Health Risks of Travel–Initial and Recurrent
• Health risks of adopted country
Risks of Initial Travel
• When—age, health, who left behind
• Travel itself—refugee camp, border crossing, debt, jet lag?
• Recurrent travel vs permanent break with home
Migration is Stressful• forced separation • dangers of the migratory
journey, • social isolation, difficulty
communicating • absence/gain opportunities • possible failure of the
migratory goals • drop/gain in social status• remittances/family
expectations • attitudes in the receiving
country.
Migratory GriefSupport/goodConditions-SIMPLE GRIEF
Poor ConditonsCOMPLICATED GRIEF
Ulysses SyndromeDepression/anxiety/ somatic sx
Individual factors
Pre-migration Stress—work,war…
Post-migration factors Migratory Grief
VALERO-GARCES,2014
Ulysses Syndrome• “Ulysses spent his days sitting on
the rocks by the sea, being consumed by tears, sighs and sadness...”
• Odyssey, Song V.
• “… mere mortals have to behave like heroes in order to survive. ....”
• Syndrome of prolonged grief with symptoms that include headaches, insomnia, abdominal discomfort and symptoms of depression and anxiety
• Dr. Joseba Achotegui (2010)

2/23/2017
6
Stress vs. Mental Health
• Rates of mental illness vary with different groups
• High rates of PTSD, anxiety, depression in refugees/immigrants exposed to violence/IPV as reason for immigrating
• For California Latinos– Central Am: high rates of political violence 1980s, 1990s; gangs– Mexico: IPV, gang, political violence
• Don’t ask, don’t tell – .
High Risk Travel Medicine
• ½ of US residents traveling abroad are FB visiting home
• Higher risk of getting sick while traveling
• Riskier behavior – Visit when pregnant, sick or with children– Stay for longer, eat like hosts. – More often sex, rural areas, contact sick relatives– Travel for health care or use health care– dentistry etc
• But less often vaccinated/prophylaxed• Recs for FB travelers same all travelers
Implications for Care• Awareness of migratory stresses
– Mitigate: language/communication/resources/ culturally competent systems/changes legal status
– Encourage English class, library,
• Practice travel medicine!– Ask about healthcare bridge–
treatments/meds from home– Recognize potential for travel/return home for
treatment and severe illness
An Approach to Immigrant
• Health risks of native country
• Health risks of travel–initial and recurrent
• Health risks of adopted country

2/23/2017
7
Risks of US Life• Epidemiology of Disease
– More chronic illness, lifestyle changes– Environmental risks:
• Latinos highest workplace fatalities; pesticides, sexual harassment
– https://www.bls.gov/news.release/pdf/cfoi.pdf, Loh
• Epidemiology of Stressors Minority StatusLegal statusLanguage marginalizationDiscrimination/FearAbsent family
• Health Care Access and Practices
Immigrant Health: Summary
• Native country• Screen for infectious diseases, mental illness,
violence/torture, missed screening (PAP), vaccinations
• Traveler• Immigrants are diverse, understand the immigration history• Immigrants are high risk travelers• Take repeated travel history
• Health risks of adopted country• Chronic illnesses, exposures• Remember barriers to care– communication and legal issues• Develop culturally competent systems
Legal Issues and Health Care for Undocumented Immigrants
Tanforan Japanese Internment, Executive 0rder, 1 942
Undocumented and Access to Care
• Highly variable by state, county, city policies• Can range from excellent to none• Undocumented children covered in many states• Undocumented adults covered in NYC, SF, LA,
others• Some undocumented adults have private
insurance via employers

2/23/2017
8
Policies Matter• Undocumented in Sanctuary Cities with good
access do well:– No difference btwn
undocumented/documented/citizens Mexican-Americans in diabetes outcomes
Iten/Fernandez 2014
– Undocumented present with more advanced HIV do equally well once in care
» Poon, 2012
• Expanding coverage to undocumented children results in high enrollments and better outcomes
» Howell, 2010
Policies Matter: ESRD and Undocumented
• Near universal coverage for ESRD with exception of undocumented
• Two strategies depending on state– Emergent dialysis (only when emergent
conditions exist)• more costly; 5x the mortality
– Chronic dialysis– Rodriguez, 2015; Cervantes, 2017;Fernandez 2017
Policies Matter: US Citizen Children
• In 2012 about 150,000 US children had an undocumented parent deported
» http://www.humanimpact.org/
• 75% undocumented parents report their US citizen children have sx of PTSD
• US citizen children of undocumented parents: – fewer health care visits
– worse health – more food insecurity
» http://www.familyunityfamilyhealth.org 2013 Report
Fear as Barrier
• 1/8 undocumented immigrants fear deportation when accessing care
» Maldonado, 2013
• Patients forgo care for fear of ICE
» Hacker, 2012
• Patients forgo care when immigration policies become more stringent
» Rhodes, 2015

2/23/2017
9
Asking About Legal Status
• Immigrant rights organizations advise against
• Pts may fear– Denial of care or lower standard of care– Immigration service involvement– Risking future legal/citizen standing– Discrimination
• Documenting in chart: Do Not
• If need, to know or remember “can you travel?”
If Patient Reveals Undocumented Status
Reassure
• Confidentiality, especially from ICE
• Current federal policies keep ICE out of hospitals/clinics
• Will not lead to differential care or abandonment/repatriation
• Consider legal referralshttps://www.immigrationlawhelp.org
Advocating for Undocumented Patients
• Know basic immigration policies and processes
• Refer for forensic examinations, legal assistance and rights education
• Support the immigration process with medical documentation
• Establish clinic policies to support undocumented
• Strengthen partnerships with community groups
Achieving ‘Legal Status’ in the U.S.
• Citizenship through birth• Citizenship through Naturalization
– Permanent resident > 5 years– Married to citizen >3 years– Served >1 year in armed forces
• Citizenship through acquisition (born to US parent)• Citizenship through Derivation (naturalization of
one’s parents)

2/23/2017
10
Paths to Permanent Status
• Family Sponsorship Green Card
• Employment Related Green Card (EB1-5)
• Asylum/refugee
• Victims of crime ( U-visa/T-visa/VAWA)
• Lottery (Diversity Green Card)
Refugees Apply for Legal Status in via Specific Process
https://www.theguardian.com/world/2016/aug/18/boy-i n-the-ambulance-image-emerges-syrian-child-aleppo-r ubble
Fear of Persecution
Must have faced persecution or have a well-founded fear of persecution on protected grounds:
• Race• Religion• Nationality• Political Opinion• Membership in a Particular Social Group
Women (FGM, domestic abuse)LGBT
Home government must have been involved in persecution or unable to protect
Refugee vetting process

2/23/2017
11
Asylum Process in US
Affirmative Asylum Process•Applies for asylum
– After arrival on valid visa– Within one year of the date of their last arrival in the US
Defensive Asylum Process• Requests asylum
– as a defense against removal while undergoing removal proceedings
– after being denied an affirmative asylum application
Factors Improving Asylum Approval Rates
• Having Legal Representation
• Having a medical affidavit from a physician or mental health provider
• Applying Affirmatively
• Country of origin• Location and assignment of immigration
Judge
Forensic Medical Evaluation: Refer
• Completed by specially trained providerworking with lawyers
• History focusing on trauma and torture
• Assessment of sequela of past abuse
• PE and MS exam documenting trauma
• Written documentation (affidavit) of trauma using guidelines from Istanbul Protocol
Often no treatment or therapies are offered
A forensic affidavit helps
• Helps build a case of ‘credible fear of persecution’
• Documents physical or psychological trauma
• In asylum cases: explains why 1 year bar not met (due to depression/PTSD or other medical concerns)

2/23/2017
12
Visas for victims of crime perpetrated in the US
Created as part of the Victims of Trafficking and Violence Protection Act (October 2000)
U-Visa•Visa for victims of violent crimes
•Limit to 10,000/year.
•Multiple year backlog.
•Applicants eligible for deferred action while application is pending.
VAWA
•Visa for spouse/child/ parent victim of abuse by American citizen/ green card holder
•Available to all genders
T-Visa
•Visa for victims of human trafficking
•Limit to 5,000/year
•Cap rarely if ever met
How do I screen my patient?
• Take an immigration history
• Screen for domestic violence and community violence
• Ask open ended questions
• Screen for victims of trafficking– Do you live and work in the same place– Do you have access to your own documents– Have you been denied access to
care/food/clothes
If You Are Asked for a Letter
• Contact the lawyer to determine the scope/focus needed for letter
• Refer to legal assistance if your patient does not have legal counsel. (Ideally no letter without lawyer).
Refer Your Undocumented Patients for Legal Advice
• Naturalization
• Asylum
• Specialty visas• Deportation issues
• Advice for DACA
• Anticipatory guidance

2/23/2017
13
Anticipatory Guidance- Legal • Rights of Habeus Corpus
– Remain silent
– Insist on warrant/don’t open the door
– Right to legal counsel
• Carry a lawyer’s #• Don’t sign anything• Have an emergency plan,
especially with children– Backup childcare– Designate POA
– Contact consulate
https://www.ilrc.org/know-your-rights-and-what-immigrant-families-should-do-now
Red Cardshttps://www.ilrc.org/red-cards
Clinic Policies
• Staff training on asking demographics
• On documentation of undocumented status
• Pro-active “signal safety” --- posters, cards
• Strengthen partnership with community groups
• Easy access to referral information for immigration services

2/23/2017
14
Watch for these possible changes
• Threat to sanctuary cities?
• Rescind DACA( Deferred Action on Child-hood Arrivals)?
• New EO:– Shifts emphasis of deportation– Emphasizes issue of “public charge”– May challenge some privacy issues
Approach to Immigrant HealthSummary: Legal
• Stay up to date on basic national and local immigration policies and processes
• Support the immigration process with medical documentation
• Refer for legal assistance and rights education and planning, now more than ever
• Consult a lawyer!
Immigrant Health: Think Globally, Act Locally Legal Referrals SF
www.projectlegallink.org

2/23/2017
15
More resources• Public Health Actions for Immigrant Rights
(https://docs.google.com/document/d/1MXecn5b_IZPZ5r6LA3U4Ggz2gSMqxMONGBlCngsXHEU)
• National Immigrant Law Center (https://www.nilc.org)
• The Fair Immigration Reform Movement (FIRM; http://fairimmigration.org/)
• United We Dream (http://unitedwedream.org/)• We Belong Together (https://www.domesticworkers.org/we-
belong-together)• National Council of La Raza (NCLR; http://www.nclr.org/)• Check for potential partners on local college campuses,
which may have groups already formed around immigration.• Human Impact Partners
([email protected])• Immigrant Legal Resource Center (https://www.ilrc.org)• ACLU (aclu.org)
More Resources
• Minnesota Department of Public Health: A Call to Action, Immigrant Health
http://www.health.state.mn.us/divs/idepc/refugee/topics/immhealthrpt.pdf
• Examining asylum seekers: A clinician’s guide to physical and psychological evaluations of torture and ill treatment; 2012 Dec [cited 2015 Sept 1]. 191 . Available from: http://physiciansforhumanrights.org/library/reports/examining-asylum-seekers-manual-2012.html
• United Nations. The Manual on Effective Investigation and Documentation of Torture and Other Cruel, Inhuman, or Degrading Treatment or Punishment: Istanbul Protocol. Geneva, Switzerland: United Nations, November 1999.
http://www.ohchr.org/Documents/Publications/training8Rev1en.pdf