an initiative of - calrightmeds...2019/12/02 · laba/ics or laba/lama/ics, chronic bronchitis, and...
TRANSCRIPT

An initiative of

OVERVIEW OF DRUGS
FOR ASTHMA/COPD

Asthma Medications
• Reliever Medications
• Controller Medications
• Add-On Controller Medications

Asthma Medications
• Reliever Medications
• Short-Acting Beta2-Agonist bronchodilators (SABA)
• Low-dose ICS-formoterol
• Short-Acting Muscarinic Antagonists (SAMA)
• Controller Medications
• Add-On Controller Medications
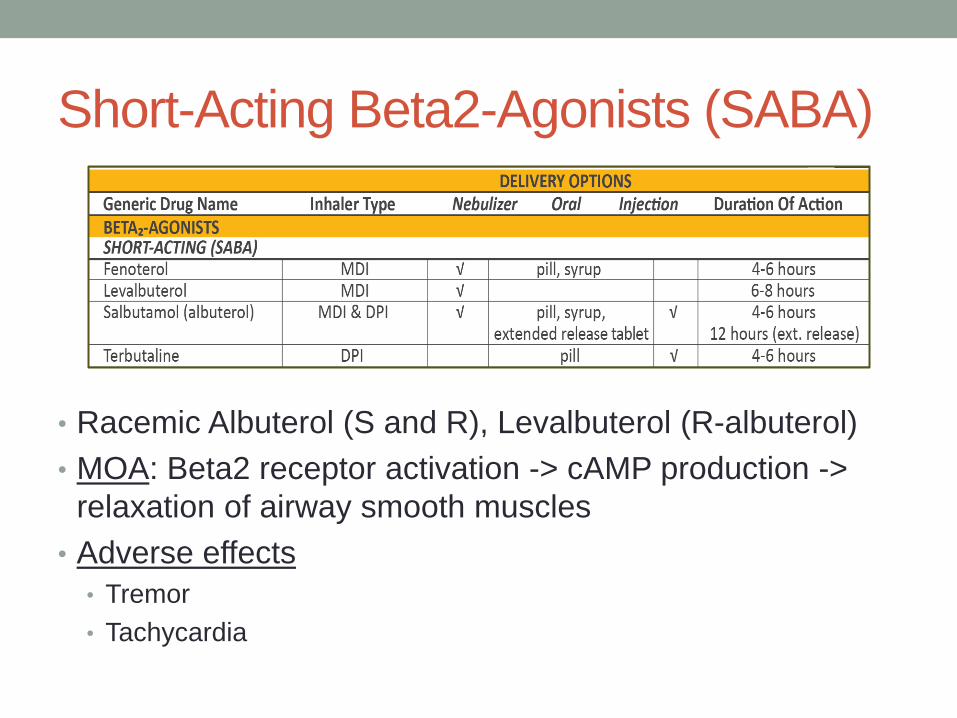
Short-Acting Beta2-Agonists (SABA)
• Racemic Albuterol (S and R), Levalbuterol (R-albuterol)
• MOA: Beta2 receptor activation -> cAMP production ->
relaxation of airway smooth muscles
• Adverse effects
• Tremor
• Tachycardia
Short-Acting Beta2-Agonists (SABA)
• Inhaled SABAs provide quick relief of asthma
symptoms and bronchoconstriction including in
acute exacerbations
• Pre-treatment of exercise-induced
bronchoconstriction
• Use only as-needed and at the lowest
dose/frequency required
• Tolerance develops rapidly with regular use due
to reduced number of beta-2 receptors in lung
Asthma Medications
• Reliever Medications
• Short-Acting Beta2-Agonist bronchodilators (SABA)
• Low-dose ICS-formoterol
• Short-Acting Antimuscarinics (SAMA)
• Controller Medications
• Add-On Controller Medications

Low-dose ICS-formoterol
• ICS MOA: anti-inflammatory – block late-phase reaction
to allergens, reduce airway hyperresponsiveness, inhibit
inflammatory mediators
• LABA MOA: bronchodilator that increases cAMP->
decreases intracellular calcium -> produces smooth
muscle relaxation

Low-dose ICS-formoterol
• Low dose Beclometasone-formoterol or
Budesonide-formoterol
• Reliever for patients prescribed as-needed
controller therapy for mild asthma
• Substantially reduces the risk of severe
exacerbations compared with SABA-only
treatment
Low-dose ICS-formoterol
• Low dose Beclometasone-formoterol or
Budesonide-formoterol
• Reliever for patients with moderate-severe
asthma prescribed maintenance and reliever
treatment
• Reduces risk of exacerbations compared with
using as-needed SABA treatment, with similar
symptom control
Asthma Medications
• Reliever Medications
• Short-Acting Beta2-Agonist bronchodilators (SABA)
• Low-dose ICS-formoterol
• Short-Acting Muscarinic Antagonist (SAMA)
• Controller Medications
• Add-On Controller Medications

Short Acting Muscarinic Antagonist
(SAMA)
Short Acting Muscarinic Antagonist
(SAMA)• MOA: inhibits bronchoconstriction by blockage of
muscarinic cholinergic receptors
• Adverse effects:
Dryness of mouth, bitter taste
• DOC for:
• Beta2 agonist intolerance
• Beta-blocker induced bronchospasm

Short Acting Muscarinic Antagonist
(SAMA)• Long-term use:
less effective reliever than SABAs
• Short-term use in acute asthma:
added to SABA reduces risk of hospital admission

Asthma Medications
• Reliever Medications
• Controller Medications
• Inhaled Corticosteroids (ICS)
• ICS and Long-acting beta2-agonist bronchodilatory combinations
(ICS-LABA)
• Leukotriene modifiers
• Add-On Controller Medications

Inhaled Corticosteroids
• Most effective anti-inflammatory medication
• Reduce symptoms
• Increase lung function
• Improve qualify of life
• Reduce risk of exacerbations and asthma-related
hospitalizations and death

Inhaled Corticosteroids
• Low dose ICS provides most of the clinical benefit for
most patients
• Some patients may need medium dose ICS if asthma
uncontrolled despite good adherence/technique with low
dose ICS
• High dose ICS needed by very few patients
• Long-term use: increased risk of local/systemic side effects

Inhaled Corticosteroids
• Adverse effects:
• Inhaled, Local: oropharyngeal candidiasis, dysphonia
• Use spacer device; rinse and spit after use
• Oral, Systemic: osteoporosis, cataract, glaucoma,
adrenal suppression, dermal thinning
• Less common vs oral steroids
• Risk increased with long-term high dose ICS

ICS Bioavailability
• ~10-50% of MDI dose delivered to the lungs
• Nearly all of the amount delivered to the lungs is bioavailable.
• ~50-80% of MDI dose without a spacer is swallowed
• High first-pass metabolism or use of space can ↓oral bioavailability
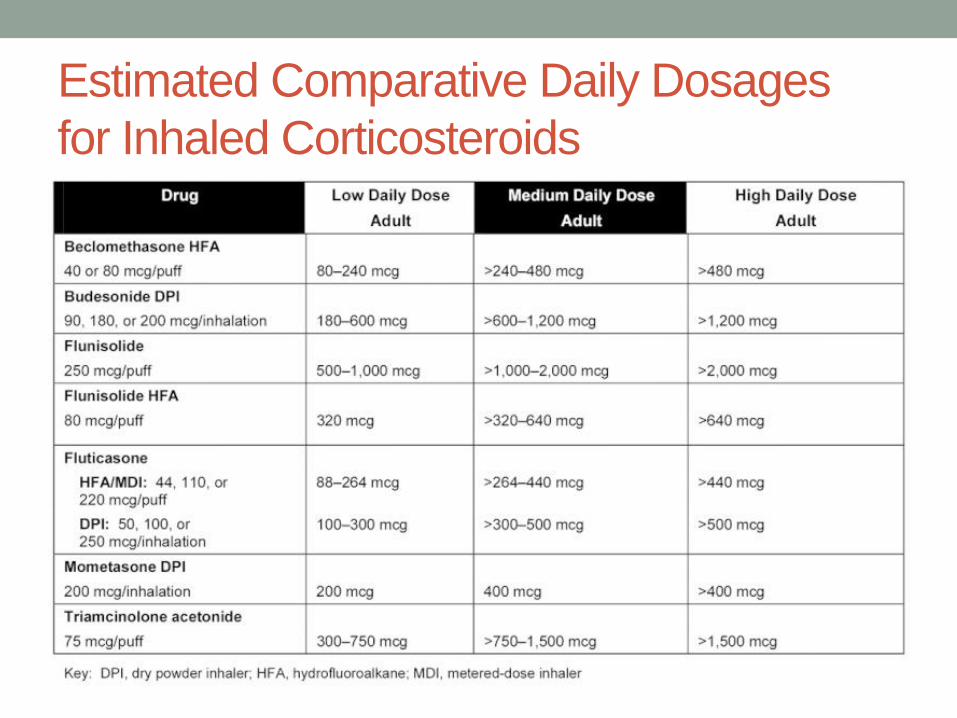
Estimated Comparative Daily Dosages
for Inhaled Corticosteroids
Asthma Medications
• Reliever Medications
• Controller Medications
• Inhaled Corticosteroids (ICS)
• ICS and Long-acting beta2-agonist bronchodilatory
combinations (ICS-LABA)
• Leukotriene modifiers
• Add-On Controller Medications

ICS-LABA
• LABA Adverse effect: tachycardia, headache, cramps
• ICS-LABA is safe for asthma when used in combination
• LABA monotherapy should not be used in asthma:
increased risk of asthma-related death
ICS-LABA
• Addition of LABA to ICS
• Improves symptoms, lung function, and reduces
exacerbations in more patients, more rapidly, than
doubling the dose of ICS
• Maintenance and reliever treatment with low dose ICS-
formoterol reduces exacerbations compared with
maintenance therapy with SABA as reliever
Asthma Medications
• Reliever Medications
• Controller Medications
• Inhaled Corticosteroids (ICS)
• ICS and Long-acting beta2-agonist bronchodilatory combinations
(ICS-LABA)
• Leukotriene modifiers
• Add-On Controller Medications
Leukotriene Modifiers
• Montelukast, Pranlukast, Zafirlukast, Zilueton (tablets)
• MOA: inhibits leukotriene activity -> anti-inflammatory
effects
• Leukotrienes 100-1000x more potent bronchoconstrictor than
histamine
• Attracts inflammatory cells -> more mucus production
• Adverse effects: Few side effects except elevated liver
function test with zileuton and zafirlukast
Leukotriene Modifiers
• Used as an option for controller therapy, particularly in
children
• Used alone: less effective than low dose ICS
• Added to ICS: less effective than ICS-LABA

Asthma Medications
• Reliever Medications
• Controller Medications
• Add-On Controller Medications
• Long-acting Muscarinic Antagonist
• Anti-IgE
• Antil-IL5 and anti-IL5R
• Anti-IL4R
• Systemic corticosteroids
Long-Acting Muscarinic Antagonist
(LAMA)
Tiotropium bromide 1.25mcg (soft mist inhaler)
2 puffs once daily
• Adverse effects: dry mouth
• Add-on option at Step 4 or 5 for patients with history of
exacerbations despite ICS ± LABA

Asthma Medications
• Reliever Medications
• Controller Medications
• Add-On Controller Medications
• Long-acting anticholinergic
• Anti-IgE
• Antil-IL5 and anti-IL5R
• Anti-IL4R
• Systemic corticosteroids

Anti-IgE
• Omalizumab (subcutaneous)
• Add-on option for patients with severe allergic asthma uncontrolled
on high dose ICS
• Serum IgE: 30-700IU/ml
• MOA: inhibits the binding of IgE to the surface of mast
cells and basophils -> limits release of mediators of the
allergic response (histamines, leukotrienes, etc)
• Adverse effect: injection site reactions are common but
minor. Anaphylaxis is rare.

Antil-IL5 and Anti-IL5R
• Anti-IL5:
• Mepolizumab (subcutaneous)
• Reslizumab (IV)
• Anti-IL5 Receptor
• Benralizumab (subcutaneous)
• Add-on options for patients
with severe eosinophilic asthma
uncontrolled on high dose
ICS-LABA
• Adverse effect: injection site reactions are common but minor.

Anti-IL4R
• Dupilumab (subcutaneous)
• Add-on option for patients with severe eosinophilic or Type 2
asthma uncontrolled on high dose ICS-LABA, or requiring
maintenance OCS
• Adverse effect: injection site reactions are common but
minor.

Asthma Medications
• Reliever Medications
• Controller Medications
• Add-On Controller Medications
• Long-acting anticholinergic
• Anti-IgE
• Antil-IL5 and anti-IL5R
• Anti-IL4R
• Systemic corticosteroids

Systemic Corticosteroids
• Prednisone, Prednisolone, Methylprednisolone,
Hydrocortisone
• Oral corticosteroid (OCS) therapy preferred
• Short-term treatment (5-7days): for severe acute
exacerbations, with main effects seen after 4-6 hours
• Long-term: may be required for patients with severe
asthma
Systemic Corticosteroids
• Adverse effects:
• Short-term: hyperglycemia, fluid retention sleep
disturbance, reflux, appetite increase, mood changes
• Long-term: cataract, glaucoma, hypertension, diabetes,
adrenal suppression, osteoporosis, dermal thinning
COPD Medications
• Bronchodilators
• Beta2-Agonists
• Antimuscarinics
• Methylxanthines
• Combination bronchodilator therapy
• Anti-inflammatory Agents
• Inhaled Corticosteroids
• Phosphodiesterase-4 (PDE4) Inhibitors
• Oral Glucocorticoids
• Antibiotics
Bronchodilators
• Central to symptom management and commonly given on
a regular basis to prevent/reduce symptoms
• Inhaled bronchodilators recommended over oral
bronchodilators
• Regular and as-needed use of SABAs or SAMAs improve
FEV1 and symptoms.
• Combinations of SABA/SAMA are superior compared to
either alone in improving FEV1 and symptoms.

COPD Medications
• Bronchodilators
• Beta2-Agonists
• Antimuscarinics
• Methylxanthines
• Combination bronchodilator therapy
• Anti-inflammatory Agents
• Inhaled Corticosteroids
• Phosphodiesterase-4 (PDE4) Inhibitors
• Oral Glucocorticoids
• Antibiotics

Short-Acting Beta2 Agonists (SABA)
• MOA: stimulates beta2-adrenergic receptors->↑ cyclic
AMP and produces functional antagonism to
bronchoconstriction -> relax airway smooth muscle
• Adverse effects: resting sinus tachycardia, potential to
precipitate cardiac rhythm disturbances in susceptible
patients

Long-Acting Beta2 Agonists (LABA)

Long-Acting Beta2 Agonists (LABA)

Antimuscarinic Agents
• MOA: blocks the bronchoconstrictor effects of
acetylcholine on M3 muscarinic receptors expressed in
airway smooth muscle
• Adverse effects: dry mouth. *Inhaled antimuscarinics are
poorly absorbed which limits systemic effects
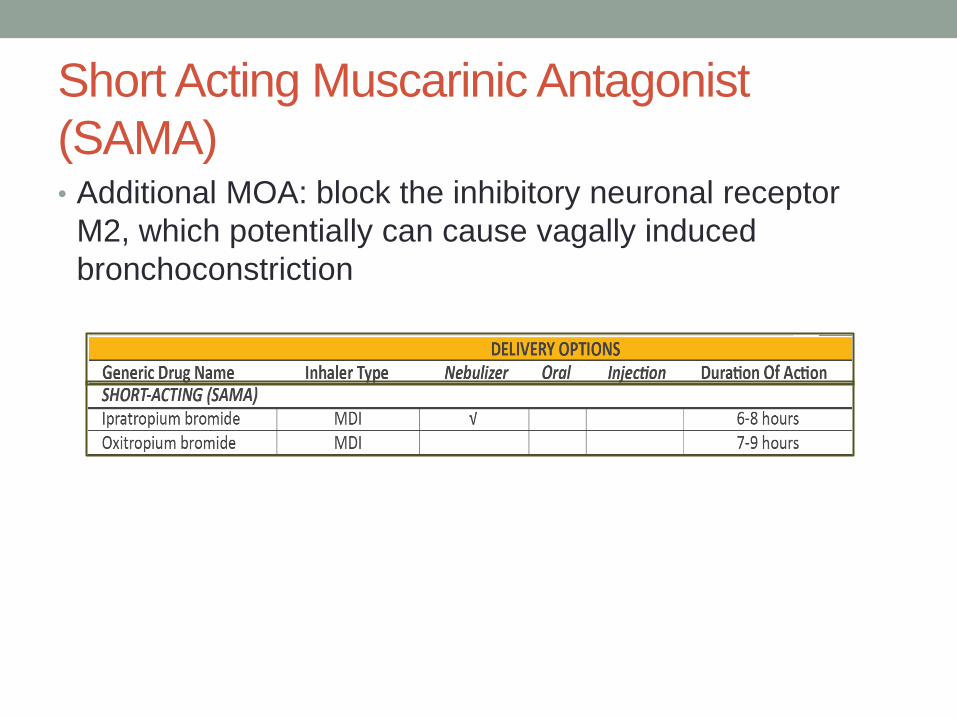
Short Acting Muscarinic Antagonist
(SAMA)• Additional MOA: block the inhibitory neuronal receptor
M2, which potentially can cause vagally induced
bronchoconstriction

Long-Acting Muscarinic Antagonist
(LAMA)• Additional MOA: prolonged binding to M3 muscarinic
receptors, with faster dissociation from M2 muscarinic
receptors -> prolonged duration of bronchodilator effect
• Clinical trials have shown a greater effect on exacerbation
rates for LAMA treatment (tiotropium) versus LABA
treatment.

Methylxanthines
• MOA:
• PDE Inhibition: smooth muscle relaxation (ie, bronchodilation)
• Suppression of the response of the airways to stimuli
• Enhanced calcium uptake in muscle cells: increases diaphragmatic
muscles contractility
• Adverse effects:
• Normal (10-15mcg/ml): N/V, tremor, tachycardia, HA, insomnia
• >20mcg/ml: arrhythmias, seizures

Methylxanthines
• Patients can be adequately treated with serum levels in
the 8-12 mcg/mL
• Theophylline addition to salmeterol produces greater
FEV1 improvement than salmeterol alone
• Evidence for modest bronchodilator effect compared to
placebo in stable COPD
• Data do not support a role for low-dose theophylline in
reducing the frequency of COPD exacerbations
• Theophylline not recommended unless other long
acting bronchodilators are unavailable or
unaffordable

Combination LABA/LAMA
• LABA/LAMA combination treatment increases FEV1 and
reduces symptoms and exacerbations compared to
monotherapy

COPD Medications
• Bronchodilators
• Beta2-Agonists
• Antimuscarinics
• Methylxanthines
• Combination bronchodilator therapy
• Anti-inflammatory Agents
• Inhaled Corticosteroids
• Phosphodiesterase-4 (PDE4) Inhibitors
• Oral Glucocorticoids
• Antibiotics
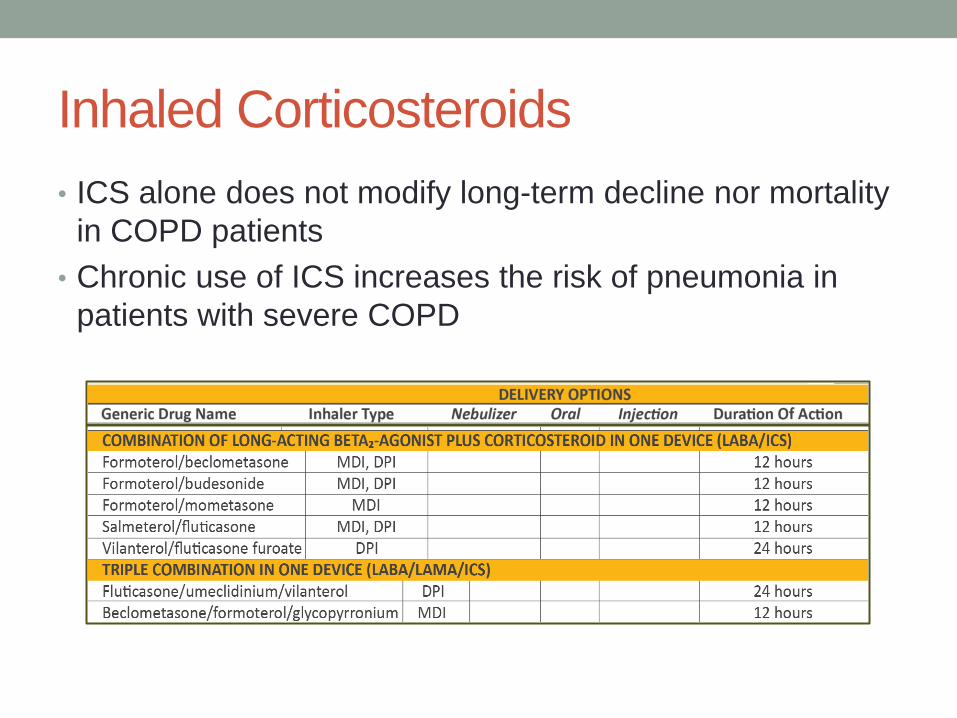
Inhaled Corticosteroids
• ICS alone does not modify long-term decline nor mortality
in COPD patients
• Chronic use of ICS increases the risk of pneumonia in
patients with severe COPD
Combination LABA/ICS
• Consider when exacerbations continue despite
appropriate long-acting bronchodilator therapy.
• Patients with blood eosinophil counts ≥ 100 cells/mcL
shown to have benefit with the addition of an ICS.
• May be used first-line in patients with blood eosinophil
counts ≥ 300 cells/mcL, or in patients who also have
asthma. Can combine with LAMA.

Triple Inhaled Therapy
• Adding a LAMA to existing LABA/ICS improves lung
function and patient reported outcomes – exacerbation
risk.

PDE4 Inhibitors
Roflumilast 250-500mcg PO daily
• MOA: PDE4 inhibitors prevents breakdown of cAMP ->
decreases inflammation and may promote airway smooth
muscle relaxation
• Consider use in patients with exacerbations despite
LABA/ICS or LABA/LAMA/ICS, chronic bronchitis, and
severe to very severe COPD (FEV1<50%)
• Beneficial effects report to be greater in patients with prior
history of hospitalization due to exacerbation

Oral Glucocorticoids
• MOA: inhibits multiple inflammatory cytokines, reduces
airway inflammation
• Benefit in COPD is less pronounced than in asthma
• Utilized in acute management of exacerbations
• Chronic daily treatment not recommended – lack of
benefit vs systemic complications

Antibiotics
• Macrolides for 1 year in patients prone to exacerbations
reduced exacerbation risk compared to usual care
• Azithromycin 250mg/day or 500mg 3x/week
• Erythromycin 500mg bid
• Preferentially for former smokers
• Azithromycin: increased incidence of bacterial resistance
and hearing test impairments

Drugs used in Both Asthma/COPD
• Bronchodilators
• Beta2-Agonists
• Long-Acting Anticholinergic: Tiotropium
• Inhaled Corticosteroids
• Combination ICS/LABA
• Oral Corticosteroids

An initiative of