an interesting case of cardiac amyloidosis initially ... · elevated creatine kinase (cpk), 435...
TRANSCRIPT

552 • HJC (Hellenic Journal of Cardiology)
Hellenic J Cardiol 2010; 51: 552-557
Case ReportCase Report
Manuscript received:April 2, 2009;Accepted:February 9, 2010.
Address:Lilian Mantziari
First Cardiology Dept.AHEPA University Hospital1 Kiriakidi St.Thessaloniki, Greecee-mail: lmantziari@
yahoo.com
Key words: Amyloid, cardiac involvement, endomyocardial biopsy, ECG findings, echocardiography.
An Interesting Case of Cardiac Amyloidosis Initially Diagnosed as Hypertrophic CardiomyopathyAmAliA Boufidou1, liliAn mAntziAri1, StelioS PArASkevAidiS1, HArAlAmBoS kArvouniS1, eleni nenoPoulou2, mAriA-eleni mAntHou2, ioAnniS H. StyliAdiS1, GeorGioS PArcHAridiS1
1First Cardiology Department, AHEPA University Hospital, 2General Pathology Laboratory, Aristotle University of Thessaloniki, Greece
Cardiac involvement occurs frequently in primary amyloidosis and is associated with heart failure hospital-izations and poor survival. The initial presentation of the disease may be misleading, resulting in under-diag-nosis of cardiac amyloidosis and late initiation of treatment. We present a case of cardiac amyloidosis initial-ly misdiagnosed as hypertrophic cardiomyopathy and we discuss the key findings of the disease along with the latest evidence regarding the management and prognosis of cardiac amyloidosis.
A myloidosis refers to a rare group of disorders caused by the extra-cellular deposition of insoluble
abnormal fibrils, called amyloid, which are composed of a variety of serum proteins. Cardiac involvement may occur, with or without clinical manifestations, as a part of systemic amyloidosis or as a localized phenomenon, and is associated with poor prognosis.1,2 We present a case of biopsy-proven cardiac amyloidosis in a woman with symptoms of congestive heart failure who was referred to our hospital with the diagnosis of hypertrophic cardiomyopathy, and we discuss the key ECG and echocar-diographic findings that a clinician should evaluate in order to eliminate under-di-agnosis of cardiac amyloidosis, along with the current data concerning prognosis and treatment.
Case presentation
A 48-year-old woman was admitted to our clinic with dyspnea on exertion, fatigue, anorexia and lower limb edema. She al-
so mentioned exertional chest pain. The patient was free of any personal history until three months before presentation, when peripheral edema and ascites first occurred. The diagnosis by her cardiol-ogist was hypertrophic cardiomyopathy, based on asymmetrical hypertrophy of the left ventricle on echocardiography. She had no family history of cardiovascular disease, sudden cardiac death or syncope.
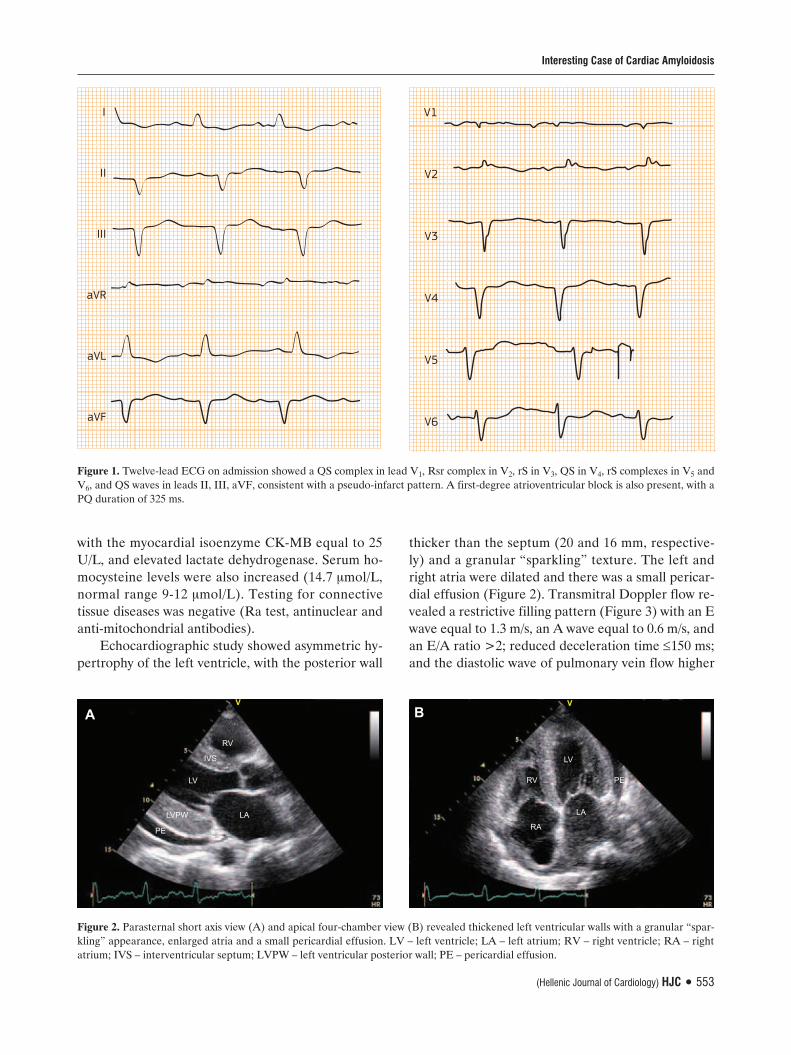
On physical examination she had blood pressure 90/70 mmHg, heart rate 66 beats/min, a second heart sound with an in-creased intensity of the pulmonic com-ponent, a 2/6 apical systolic murmur and normal lung auscultation. Jugular vein dil-atation and a palpable liver with positive hepatojugular reflux were present, along with signs of ascites. There was a first de-gree atrioventricular block on the ECG and a pseudo-infarct pattern without signs of left ventricular hypertrophy (Figure 1). The chest X-ray on admission showed car-diomegaly. Blood count was normal. Se-rum biochemistry was normal except for elevated creatine kinase (CPK), 435 U/L,
(Hellenic Journal of Cardiology) HJC • 553
Interesting Case of Cardiac Amyloidosis
with the myocardial isoenzyme CK-MB equal to 25 U/L, and elevated lactate dehydrogenase. Serum ho-mocysteine levels were also increased (14.7 μmol/L, normal range 9-12 μmol/L). Testing for connective tissue diseases was negative (Ra test, antinuclear and anti-mitochondrial antibodies).
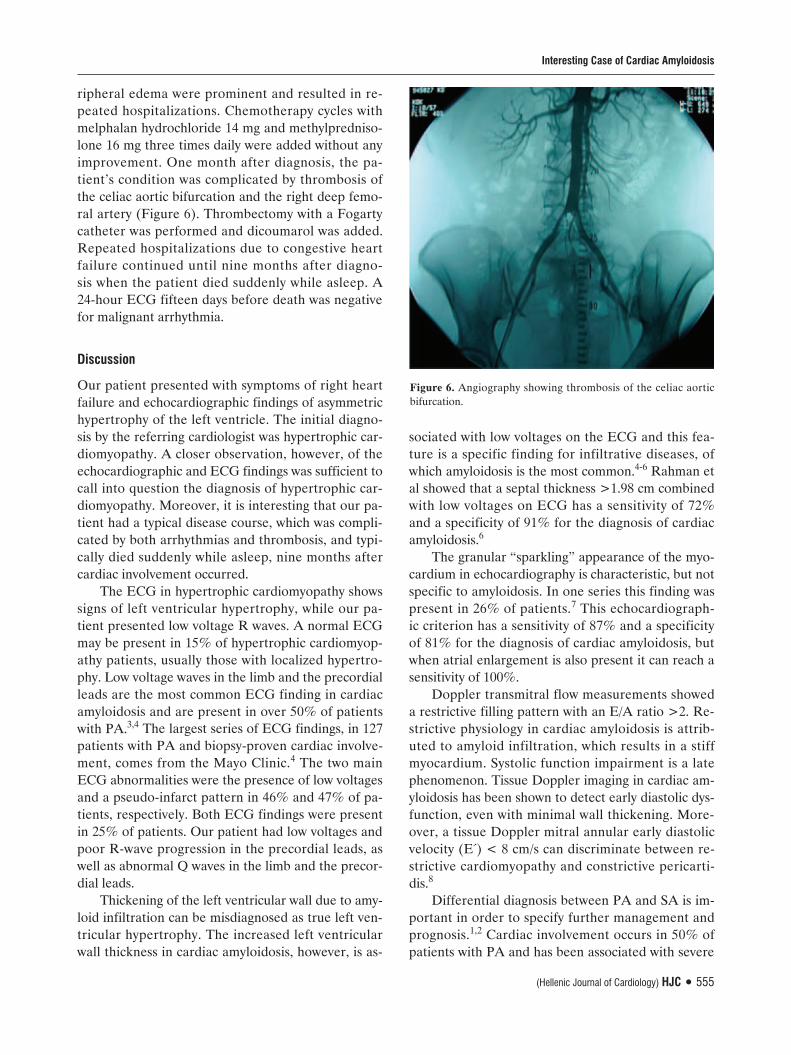
Echocardiographic study showed asymmetric hy-pertrophy of the left ventricle, with the posterior wall
thicker than the septum (20 and 16 mm, respective-ly) and a granular “sparkling” texture. The left and right atria were dilated and there was a small pericar-dial effusion (Figure 2). Transmitral Doppler flow re-vealed a restrictive filling pattern (Figure 3) with an E wave equal to 1.3 m/s, an A wave equal to 0.6 m/s, and an E/A ratio >2; reduced deceleration time ≤150 ms; and the diastolic wave of pulmonary vein flow higher
RV
LV
IVS
LA
V
PE
LVPW
RV
LV
LA
V
PE
RA
Figure 2. Parasternal short axis view (A) and apical four-chamber view (B) revealed thickened left ventricular walls with a granular “spar-kling” appearance, enlarged atria and a small pericardial effusion. LV – left ventricle; LA – left atrium; RV – right ventricle; RA – right atrium; IVS – interventricular septum; LVPW – left ventricular posterior wall; PE – pericardial effusion.
I
II
III
aVR
aVL
aVF
A Β
V1
V2
V3
V4
V5
V6
Figure 1. Twelve-lead ECG on admission showed a QS complex in lead V1, Rsr complex in V2, rS in V3, QS in V4, rS complexes in V5 and V6, and QS waves in leads II, III, aVF, consistent with a pseudo-infarct pattern. A first-degree atrioventricular block is also present, with a PQ duration of 325 ms.

554 • HJC (Hellenic Journal of Cardiology)
A. Boufidou et al
than the systolic. Tissue Doppler imaging revealed re-duced systolic and diastolic mitral annular velocities. There was mild mitral and tricuspid regurgitation and the estimated right ventricular systolic pressure was 34 mmHg.
The patient was on atenolol 50 mg/day and a hy-drochlorothiazide-amiloride combination (25/2.5 mg). Amiodarone 200 mg twice daily was added be-cause of multifocal ventricular premature beats and an episode of non-sustained ventricular tachycardia on the 24-hour ECG. On the fifth day of treatment with amiodarone the patient experienced a presyn-copal episode with nausea, dizziness, hypotension (systolic arterial pressure equal to 65 mmHg) and a
slow junctional rhythm of 38 bpm. A temporary pace-maker was implanted while atenolol and amiodarone were withdrawn. The pacemaker was removed three days later when sinus rhythm was restored and amio-darone was started again in a smaller dose of 200 mg once daily.
Coronary angiography showed normal coronary arteries. Ventriculography revealed a reduced ejec-tion fraction and mild to moderate mitral regurgita-tion. Right heart catheterization had the following findings: mean right atrial pressure 9 mmHg, right ventricular pressures 35/0-10 mmHg (systolic/diastol-ic-mean), pulmonary artery pressure 36/12-24, mean capillary wedge pressure 18 mmHg and increased left ventricular end-diastolic pressure of 19 mmHg (sys-tolic 105 mmHg). An endomyocardial biopsy was tak-en, which revealed severe lesions consistent with car-diac amyloidosis with muscle cell necrosis (Figures 4 & 5).
Once the diagnosis of amyloidosis was established by echocardiographic and biopsy findings, methyl-prednisolone 16 mg daily was added and we sought to differentiate between primary amyloidosis (PA) and secondary amyloidosis (SA). PA is often associated with multiple myeloma, which was ruled out using ap-propriate tests. Urine protein immunoblotting indi-cated a lambda light monoclonal chain, which is diag-nostic for PA.
The patient was treated with amiodarone 200 mg daily, furosemide 40-80 mg, spironolactone 50-100 mg and folic acid. During six months of follow up, symptoms of right heart failure with ascites and pe-
Figure 3. Transmitral Doppler flow showed a restrictive filling pattern with E/A >2, reduced deceleration time and reduced isovolumic relaxation time. E – early diastolic velocity; A – late diastolic velocity.
Figure 4. Extended degeneration of the myocardium, vacuoliza-tion and disruption of the cardiac myocytes. Focal necrosis and interstitial fibrosis are also seen.
Figure 5. Amyloid (black arrows) was identified on immunohisto-chemical testing with the use of monoclonal antibodies.
(Hellenic Journal of Cardiology) HJC • 555
Interesting Case of Cardiac Amyloidosis
ripheral edema were prominent and resulted in re-peated hospitalizations. Chemotherapy cycles with melphalan hydrochloride 14 mg and methylpredniso-lone 16 mg three times daily were added without any improvement. One month after diagnosis, the pa-tient’s condition was complicated by thrombosis of the celiac aortic bifurcation and the right deep femo-ral artery (Figure 6). Thrombectomy with a Fogarty catheter was performed and dicoumarol was added. Repeated hospitalizations due to congestive heart failure continued until nine months after diagno-sis when the patient died suddenly while asleep. A 24-hour ECG fifteen days before death was negative for malignant arrhythmia.
Discussion
Our patient presented with symptoms of right heart failure and echocardiographic findings of asymmetric hypertrophy of the left ventricle. The initial diagno-sis by the referring cardiologist was hypertrophic car-diomyopathy. A closer observation, however, of the echocardiographic and ECG findings was sufficient to call into question the diagnosis of hypertrophic car-diomyopathy. Moreover, it is interesting that our pa-tient had a typical disease course, which was compli-cated by both arrhythmias and thrombosis, and typi-cally died suddenly while asleep, nine months after cardiac involvement occurred.
The ECG in hypertrophic cardiomyopathy shows signs of left ventricular hypertrophy, while our pa-tient presented low voltage R waves. A normal ECG may be present in 15% of hypertrophic cardiomyop-athy patients, usually those with localized hypertro-phy. Low voltage waves in the limb and the precordial leads are the most common ECG finding in cardiac amyloidosis and are present in over 50% of patients with PA.3,4 The largest series of ECG findings, in 127 patients with PA and biopsy-proven cardiac involve-ment, comes from the Mayo Clinic.4 The two main ECG abnormalities were the presence of low voltages and a pseudo-infarct pattern in 46% and 47% of pa-tients, respectively. Both ECG findings were present in 25% of patients. Our patient had low voltages and poor R-wave progression in the precordial leads, as well as abnormal Q waves in the limb and the precor-dial leads.
Thickening of the left ventricular wall due to amy-loid infiltration can be misdiagnosed as true left ven-tricular hypertrophy. The increased left ventricular wall thickness in cardiac amyloidosis, however, is as-
sociated with low voltages on the ECG and this fea-ture is a specific finding for infiltrative diseases, of which amyloidosis is the most common.4-6 Rahman et al showed that a septal thickness >1.98 cm combined with low voltages on ECG has a sensitivity of 72% and a specificity of 91% for the diagnosis of cardiac amyloidosis.6
The granular “sparkling” appearance of the myo-cardium in echocardiography is characteristic, but not specific to amyloidosis. In one series this finding was present in 26% of patients.7 This echocardiograph-ic criterion has a sensitivity of 87% and a specificity of 81% for the diagnosis of cardiac amyloidosis, but when atrial enlargement is also present it can reach a sensitivity of 100%.
Doppler transmitral flow measurements showed a restrictive filling pattern with an E/A ratio >2. Re-strictive physiology in cardiac amyloidosis is attrib-uted to amyloid infiltration, which results in a stiff myocardium. Systolic function impairment is a late phenomenon. Tissue Doppler imaging in cardiac am-yloidosis has been shown to detect early diastolic dys-function, even with minimal wall thickening. More-over, a tissue Doppler mitral annular early diastolic velocity (E΄) < 8 cm/s can discriminate between re-strictive cardiomyopathy and constrictive pericarti-dis.8
Differential diagnosis between PA and SA is im-portant in order to specify further management and prognosis.1,2 Cardiac involvement occurs in 50% of patients with PA and has been associated with severe
Figure 6. Angiography showing thrombosis of the celiac aortic bifurcation.

556 • HJC (Hellenic Journal of Cardiology)
A. Boufidou et al
cardiac impairment and a worse prognosis than cardi-ac involvement due to SA; the median survival is 1.08 years and is shorter in the presence of heart failure.9
PA involves extracellular tissue and cardiac de-position of fibrils, called amyloid, that are composed of light chain immunoglobulin (AL) produced by monoclonal plasma cells.10 Multiple myeloma and Waldestrom macroglobulinemia are the two main dis-eases associated with PA.1 Multiple myeloma and am-yloidosis may coexist, or the diagnosis of multiple my-eloma may come before or after the presentation of amyloidosis or cardiac amyloidosis. Amyloid deposi-tion in the heart may involve the myocardium and the conductive system. Other sites where amyloid can be found are the intima, media and adventitial layers of the epicardial11 and endomyocardial coronary arter-ies, the cardiac valves and the pericardium. Extensive amyloid deposition in coronary arteries may result in typical anginal symptoms with normal coronary angi-ography.12
Amyloid deposition in the conductive tissue may cause atrioventricular conduction abnormalities, main-ly second- and third-degree atrioventricular block. Pa-tients with cardiac amyloidosis are sensitive to digital-is, nifedipine and verapamil. It is possible that this in-creased sensitivity to antiarrhythmics was the substrate for the manifestation of junctional rhythm in our pa-tient, as a response to treatment with the combination of atenolol and amiodarone, while a reduced dosage of amiodarone alone was well tolerated.
Our case was complicated by thrombosis of the celiac aortic bifurcation and the right deep femoral artery. Even though amyloidosis may be associated with hemorrhagic diathesis, the occurrence of throm-boembolic episodes is common even in sinus rhythm. In one series of patients with PA, 9 out of 15 patients who were not receiving anticoagulation therapy had arterial thromboembolic events involving ischemic stroke, multiple peripheral emboli and mesenteric ischemia. All 9 patients were in sinus rhythm and only one had a visible thrombus on echocardiography.13 It is generally believed that amyloid deposition in atrial walls results in a mechanic atrial standstill, which fa-vors thrombus formation. This is the rationale behind the recommendation of dicoumarol prescription in patients with severe cardiac amyloidosis and abnor-mal atrial function.
The prognosis of PA is poor, with a mean survival of 13 months without treatment, which may be pro-longed to 17 months after cyclic melphalan and methyl-prednisolone treatment.14 Cardiac involvement is as-
sociated with an even worse prognosis. Mean survival from onset of heart failure symptoms is no more than 6 months and predisposes to sudden death.15
Heart transplantation remains controversial be-cause of the potential for amyloid deposition in the graft, or for multiple myeloma occurrence during fol-low up. There are a few patients who have received a cardiac transplant and shown variable survival. Early postoperative results do not differ from other heart transplantation patients, but survival rates drop 30 months after transplantation in amyloidosis patients.1 The survival of 7 patients with PA treated with heart transplantation and chemotherapy in the United King-dom was 71% at 1 and 2 years, but 36% at 5 years.16 High-dose intravenous melphalan in combination with stem cell autologous transplantation is currently used for systemic PA, but its efficacy has not yet been proved. The overall survival of 92 patients who re-ceived this treatment in the United Kingdom was 5.3 years and survival among those who survived beyond day 100 was 8.5 years.17 Alternatively, a more aggres-sive treatment with sequential heart and stem cell transplantation has been applied in selected patients; after a median of 95 months follow up, 3 out of 5 pa-tients were asymptomatic, without evidence of cardi-ac or extra-cardiac amyloid accumulation.18 Recent-ly, new chemotherapy regimens have been developed and various specific anti-amyloid drugs have shown very promising results.19
In conclusion, cardiac amyloidosis is a severe dis-ease with a poor prognosis. The clinical cardiolo-gist should suspect cardiac amyloidosis in a patient with right heart failure symptoms and thickened left ventricular walls, with a restrictive filling pattern of the left ventricle combined with low voltages on the ECG. In addition, anticoagulation treatment with dicoumarol is recommended in patients with severe cardiac amyloidosis, even those in sinus rhythm, in or-der to avoid thromboembolic events.
References
1. Hassan W, Al-Sergani H, Mourad W, Tabbaa R. Amyloid heart disease. New frontiers and insights in pathophysiology, di-agnosis, and management. Tex Heart Inst J. 2005; 32: 178-184.
2. Selvanayagam JB, Hawkins PN, Paul B, Myerson SG, Neu-bauer S. Evaluation and management of the cardiac amyloi-dosis. J Am Coll Cardiol. 2007; 50: 2101-2110.
3. Murtagh B, Hammill SC, Gertz MA, Kyle RA, Tajik AJ, Grogan M. Electrocardiographic findings in primary system-ic amyloidosis and biopsy-proven cardiac involvement. Am J Cardiol. 2005; 95: 535-537.

(Hellenic Journal of Cardiology) HJC • 557
Interesting Case of Cardiac Amyloidosis
4. Rahman JE, Helou EF, Gelzer-Bell R, et al. Noninvasive di-agnosis of biopsy-proven cardiac amyloidosis. J Am Coll Car-diol. 2004; 43: 410-415.
5. Carroll JD, Gaasch WH, McAdam KP. Amyloid cardiomyop-athy: characterization by a distinctive voltage/mass relation. Am J Cardiol. 1982; 49: 9-13.
6. Simons M, Isner JM. Assessment of relative sensitivities of noninvasive tests for cardiac amyloidosis in documented car-diac amyloidosis. Am J Cardiol. 1992; 69: 425-427.
7. Falk RH, Plehn JF, Deering T, et al. Sensitivity and specific-ity of the echocardiographic features of cardiac amyloidosis. Am J Cardiol. 1987; 59: 418-422.
8. Ha J-W, Ommen SR, Tajik AJ, et al. Differentiation of con-strictive pericarditis from restrictive cardiomyopathy using mitral annular velocity by tissue Doppler echocardiography. Am J Cardiol. 2004; 94: 316-319.
9. Dubrey SW, Cha K, Anderson J, et al. The clinical features of immunoglobulin light-chain (AL) amyloidosis with heart in-volvement. QJM. 1998; 91: 141-157.
10. Glenner GG. Amyloid deposits and amyloidosis. The beta-fibrilloses (first of two parts). N Engl J Med. 1980; 302: 1283-1292.
11. Wittich CM, Neben-Wittich MA, Mueller PS, Gertz MA, Ed-wards WD. Deposition of amyloid proteins in the epicardial coronary arteries of 58 patients with primary systemic amyloi-dosis. Cardiovasc Pathol. 2007; 16: 75-78.
12. Yagishita A, Tanimoto S, Tanabe K, et al. Cardiac amyloido-
sis presumptively diagnosed as cardiac syndrome X. Circ J. 2009; 73: 1349-1351.
13. Hausfater P, Costedoat-Chalumeau N, Amoura Z, et al. AL cardiac amyloidosis and arterial thromboembolic events. Scand J Rheumatol. 2005; 34: 315-319.
14. Kyle RA, Gertz MA, Greipp PR, et al. A trial of three regi-mens for primary amyloidosis: colchicine alone, melphalan and prednisone, and melphalan, prednisone, and colchicine. N Engl J Med. 1997; 336: 1202-1207.
15. Grogan M, Gertz MA, Kyle RA, Tajik AJ. Five or more years of survival in patients with primary systemic amyloidosis and biopsy-proven cardiac involvement. Am J Cardiol. 2000; 85: 664-5, A11.
16. Dubrey SW, Burke MM, Hawkins PN, Banner NR. Cardiac transplantation for amyloid heart disease: the United King-dom experience. J Heart Lung Transplant. 2004; 23: 1142-1153.
17. Goodman HJB, Gillmore JD, Lachmann HJ, Wechalek-ar AD, Bradwell AR, Hawkins PN. Outcome of autologous stem cell transplantation for AL amyloidosis in the UK. Br J Haematol. 2006; 134: 417-425.
18. Gillmore JD, Goodman HJ, Lachmann HJ, et al. Sequential heart and autologous stem cell transplantation for systemic AL amyloidosis. Blood. 2006; 107: 1227-1229.
19. Wechalekar AD, Hawkins PN, Gillmore JD. Perspectives in treatment of AL amyloidosis. Br J Haematol. 2008; 140: 365-377.