anaemia; transfusion cases therapeutics sahd
DESCRIPTION
Anaemia; transfusion cases Therapeutics SAHD. Medical Students (Dr N Jackson) January 2011. Case 1. A 60-year old woman is noted to be pale and an FBC is performed: Hb 5.5g/dL; MCV 51.4fL WBC 6.9x10 9 /L; Plts 521x10 9 /L What is the likely diagnosis? - PowerPoint PPT PresentationTRANSCRIPT
Anaemia; transfusion Anaemia; transfusion cases Therapeutics cases Therapeutics SAHDSAHD
Medical StudentsMedical Students(Dr N Jackson) January 2011(Dr N Jackson) January 2011

Case 1Case 1
A 60-year old woman is noted to be A 60-year old woman is noted to be pale and an FBC is performed:pale and an FBC is performed:– Hb 5.5g/dL; MCV 51.4fLHb 5.5g/dL; MCV 51.4fL
WBC 6.9x10WBC 6.9x1099/L; Plts 521x10/L; Plts 521x1099/L/L What is the likely diagnosis?What is the likely diagnosis? On what points will you major in the On what points will you major in the
history?history? What will you look for on examination?What will you look for on examination? What further tests will you request?What further tests will you request? What treatments will you consider?What treatments will you consider?
Case 1: Microcytic Case 1: Microcytic anaemia in a 60-year old anaemia in a 60-year old womanwoman Likely diagnosis: Likely diagnosis: Fe deficiencyFe deficiency History:History:
Intake Intake (diet: …)(diet: …) Blood loss Blood loss (sites: …)(sites: …) Malabsorption Malabsorption (history? test …)(history? test …)
Examination: Examination: GIGI Further tests:Further tests: (Ferritin); film; GI; (Ferritin); film; GI;
TTGTTG
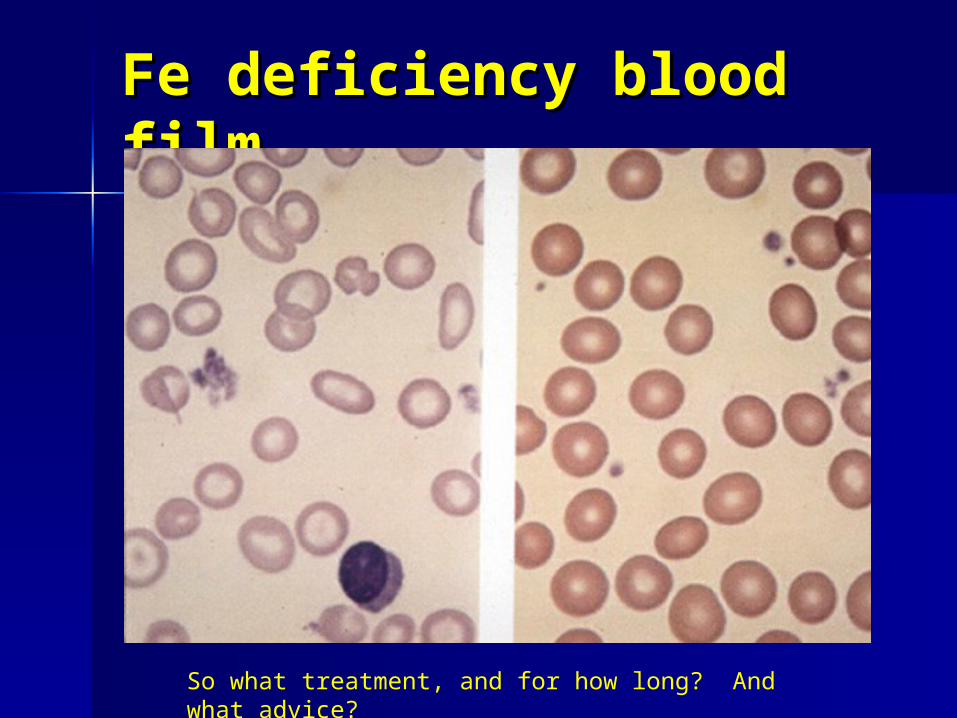
Fe deficiency blood Fe deficiency blood filmfilm
So what treatment, and for how long? And what advice?

Case 1: Microcytic anaemiaCase 1: Microcytic anaemia(Hb 5.5) in a 60-year old (Hb 5.5) in a 60-year old womanwoman Treatment (of Fe deficiency)Treatment (of Fe deficiency)
– FeSOFeSO44 200mg OD 200mg OD TDSTDS
– Add vit C ?Add vit C ?– 6/52 to restore Hb; 3/12 to replete6/52 to restore Hb; 3/12 to replete– Dietary adviceDietary advice
What side effects to expect and What side effects to expect and how to avoid?how to avoid?
Iron therapy: side Iron therapy: side effectseffects GI – nausea, vomiting, epigastric GI – nausea, vomiting, epigastric
pain, diarrhoea, constipation.pain, diarrhoea, constipation. (Care in inflamm bowel dis, (Care in inflamm bowel dis,
strictures, diverticular dis)strictures, diverticular dis) Black stools.Black stools. ?Take with food; build up dose ?Take with food; build up dose
slowlyslowly Use lower Fe content preparations:Use lower Fe content preparations:
– e.g. Ferrous gluconate 300mg TDSe.g. Ferrous gluconate 300mg TDS

No response to oral No response to oral Fe?Fe? Hb 6.5g/dL after 4 weeks Hb 6.5g/dL after 4 weeks
treatmenttreatment
What reasons can you think of?What reasons can you think of?
No response to oral No response to oral Fe?Fe? Hb 6.5g/dL after 4 weeks Hb 6.5g/dL after 4 weeks
treatment.treatment. What reasons can you think of?What reasons can you think of?
– Non complianceNon compliance– Non absorption (e.g. coeliac, small Non absorption (e.g. coeliac, small
bowel resection)bowel resection)– Loss > absorption (i.e. bleeding ++)Loss > absorption (i.e. bleeding ++)
What other treatment could you What other treatment could you consider?consider?

Parenteral FeParenteral Fe
Intramuscular:Intramuscular:– Fe dextranFe dextran
Intravenous:Intravenous:– Fe dextran = Cosmofer (TDI)Fe dextran = Cosmofer (TDI)– Fe sucrose = Venofer (x3/wk)Fe sucrose = Venofer (x3/wk)– Fe carboxymaltose = Ferinject (TDI)Fe carboxymaltose = Ferinject (TDI)– Fe isomaltoside = Monofer (TDI)Fe isomaltoside = Monofer (TDI)
What are problems with this approach?What are problems with this approach?
Parenteral Fe: side Parenteral Fe: side effectseffects IV infusion – ward, nurse time, IV infusion – ward, nurse time,
costcost Allergic/anaphylactic reactionsAllergic/anaphylactic reactions
– Test dose may be requiredTest dose may be required Other infusion reactions (flushing)Other infusion reactions (flushing) GI symptomsGI symptoms HeadacheHeadache Taste disturbanceTaste disturbance
Any questions on Fe therapy?Any questions on Fe therapy?

Case 2Case 2
A 50-year old single man presents with A 50-year old single man presents with fatigue. He admits to disliking fatigue. He admits to disliking vegetables. O/E: pallor; tinge vegetables. O/E: pallor; tinge jaundice; spleen tip palpable.jaundice; spleen tip palpable.– Hb 5.6g/dL; MCV 125fLHb 5.6g/dL; MCV 125fL
WBC 3.0x10WBC 3.0x1099/L; Plts 80x10/L; Plts 80x1099/L/L Describe the abnormalities in the FBC.Describe the abnormalities in the FBC. List your provisional and differential List your provisional and differential
diagnoses.diagnoses. State the investigations you would State the investigations you would
request.request. What treatment would you give while What treatment would you give while
waiting for results?waiting for results?

Case 2Case 2
Pancytopenia with macrocytosis:Pancytopenia with macrocytosis:– Megaloblastic anaemia (B12/Megaloblastic anaemia (B12/FolateFolate))– MyelodysplasiaMyelodysplasia– Acute leukaemiaAcute leukaemia– Aplastic anaemiaAplastic anaemia– EtOH/liver diseaseEtOH/liver disease
Which of these would you favour?Which of these would you favour?(NB dislikes vegetables)(NB dislikes vegetables)
Which investigations? Which investigations? (and expected (and expected results)results)
Case 2: Pancytopenia Case 2: Pancytopenia with macrocytosiswith macrocytosis Most likely megaloblastic anaemia Most likely megaloblastic anaemia
due to folate deficiency.due to folate deficiency. Investigations:Investigations:
– Blood filmBlood film: oval macrocytes, : oval macrocytes, aniso/poikilo hypersegmented aniso/poikilo hypersegmented neutrophils.neutrophils.(dysplastic features, blasts)(dysplastic features, blasts)
– B12 & FolateB12 & Folate (serum or RBC?)(serum or RBC?)
– ?Bone marrow: ?Bone marrow: megaloblastic changemegaloblastic change

Megaloblastic Anaemia: Megaloblastic Anaemia: blood filmblood film
Before B12/Folate levels known, what treatment(s) would you give?

Case 2: Pancytopenia Case 2: Pancytopenia with macrocytosiswith macrocytosis Treatments:Treatments:
– B12: Hydroxycobalamin 1000µg x5 B12: Hydroxycobalamin 1000µg x5 ….….
– Folic acid: 5mg ODFolic acid: 5mg OD Would you give Fe as well?Would you give Fe as well?
If so, why?If so, why? If the results showed very low If the results showed very low
folate and normal B12; any folate and normal B12; any further investigations?further investigations?

Case 2: (cont’d)Case 2: (cont’d)
The patient receives a course of The patient receives a course of treatment and soon feels much better, treatment and soon feels much better, but his blood count is then:but his blood count is then:– Hb 9.0g/dL; MCV 64fLHb 9.0g/dL; MCV 64fL
WBC 8.0x10WBC 8.0x1099/L; Plts 180x10/L; Plts 180x1099/L/L What complication has arisen, What complication has arisen,
and why?and why?
Case 2: (cont’d)Case 2: (cont’d)
Complication?Complication?– Fe deficiencyFe deficiency
Why?Why?– Response to B12/Folate outstrips Fe Response to B12/Folate outstrips Fe
storesstores– Many causes of B12/Fol deficiency Many causes of B12/Fol deficiency
also cause Fe deficiency.also cause Fe deficiency. What investigation & treatment?What investigation & treatment?
– No investigation – just give Fe.No investigation – just give Fe.

Treating Folate Treating Folate deficiencydeficiency Do not use folates alone in unsorted Do not use folates alone in unsorted
megaloblastic anaemia:megaloblastic anaemia:– In B12 def, may precipitate neurological problemsIn B12 def, may precipitate neurological problems– Use B12/Folate (+Fe) together in megaloblastic Use B12/Folate (+Fe) together in megaloblastic
anaemiaanaemia Folic acid: 5mg/dayFolic acid: 5mg/day ( ( if malabsorption present) if malabsorption present) Prevention of neural tube defects:Prevention of neural tube defects: 400 400μμg/day g/day
(low risk); 5mg/day (high risk)(low risk); 5mg/day (high risk) Diet:Diet: beans, citrus fruits, dark green leafy beans, citrus fruits, dark green leafy
vegetables, whole grains, poultry, pork, shellfish vegetables, whole grains, poultry, pork, shellfish and liverand liver
Think of cause:Think of cause: diet, malasorption (TTG) diet, malasorption (TTG) Side effects:Side effects: very rare. very rare.
Case 3Case 3
A 49-year old man complained of lethargy and A 49-year old man complained of lethargy and leg pain. He had undergone several blood leg pain. He had undergone several blood transfusions but had become anaemic again.transfusions but had become anaemic again.PMH: HypothyroidismPMH: HypothyroidismO/E: very pale; no organomegaly; no CCFO/E: very pale; no organomegaly; no CCF– Hb 2.1g/dL; MCV 114fLHb 2.1g/dL; MCV 114fL
WBC 1.5x10WBC 1.5x1099/L; Plts 35x10/L; Plts 35x1099/L/L List your differential diagnosis.List your differential diagnosis. What will you look for in the blood film What will you look for in the blood film
(report)?(report)? What further tests will you request?What further tests will you request? What is your immediate treatment?What is your immediate treatment?
Case 3Case 3
Differential diagnosis?Differential diagnosis?(from the abnormalities in the (from the abnormalities in the FBC?)FBC?)

Case 3Case 3
Severe pancytopenia with Severe pancytopenia with macrocytosis (order re-arranged):macrocytosis (order re-arranged):– Acute leukaemiaAcute leukaemia– MyelodysplasiaMyelodysplasia– Megaloblastic anaemia (B12/FolateMegaloblastic anaemia (B12/Folate))– Aplastic anaemiaAplastic anaemia– EtOH/liver diseaseEtOH/liver disease
What will you look for in the blood What will you look for in the blood film? And what other tests will you film? And what other tests will you request?request?
Case 3: Pancytopenia Case 3: Pancytopenia with macrocytosis with macrocytosis (severe)(severe) Blood Film:Blood Film:
– Leucoerythroblastic change ( diff ….)Leucoerythroblastic change ( diff ….)– BlastsBlasts– Dysplastic features (e.g. …..)Dysplastic features (e.g. …..)– Oval macrocytes; hyperseg neutsOval macrocytes; hyperseg neuts
Other tests:Other tests:– Bone marrowBone marrow– B12, FolateB12, Folate
What will be your treatment while What will be your treatment while awaiting test results? awaiting test results? Remember:Remember: Hb Hb 2.1g/dL; MCV 114fL, WBC 1.5x102.1g/dL; MCV 114fL, WBC 1.5x1099/L; Plts /L; Plts 35x1035x1099/L/L

Case 3: Pancytopenia Case 3: Pancytopenia with macrocytosis with macrocytosis (severe)(severe) Treatment while waiting tests:Treatment while waiting tests:
– Red cell transfusionRed cell transfusion Bone marrow again turned out to Bone marrow again turned out to
be megaloblastic, with very low be megaloblastic, with very low B12:B12:– What neurological signs would you What neurological signs would you
look for in the legs?look for in the legs? B12 <60ng/LB12 <60ng/L. What further tests?. What further tests?

Subacute combined degeneration of spinal cord due to B12 deficiency

B12 deficiencyB12 deficiency
Main cause:Main cause: pernicious anaemia pernicious anaemia– GPC or IF auto-ab. (Schilling test: no longer)GPC or IF auto-ab. (Schilling test: no longer)
Rare:Rare: strict vegan diet, gastrX, terminal strict vegan diet, gastrX, terminal ileum removal, other malabsorptionileum removal, other malabsorption
Treatment = B12Treatment = B12– Hydroxycobalamin 1000µg IM x5 over 2/52, Hydroxycobalamin 1000µg IM x5 over 2/52,
then 1000µg IM every 3/12then 1000µg IM every 3/12– Cyanocobalamin PO (if dietary cause) Cyanocobalamin PO (if dietary cause)
50µg/day50µg/day– Side effects rareSide effects rare : allergy; : allergy; K K++ initially initially
Part II:Part II:
Transfusion casesTransfusion cases
Case 1: Pre-op Case 1: Pre-op assessmentassessment
A 45-year old woman with fibroids A 45-year old woman with fibroids has menorrhagia and is has menorrhagia and is scheduled for a hysterectomyscheduled for a hysterectomy
In the pre-anaesthetic In the pre-anaesthetic assessment clinic (PAAC):assessment clinic (PAAC):– Hb 8.9g/dL, MCV 73fL (WBC, plts Hb 8.9g/dL, MCV 73fL (WBC, plts
normal)normal) Regarding Regarding her blood transfusion her blood transfusion
requirementsrequirements, what action(s) will , what action(s) will you take?you take?

Case 1: Pre-op Case 1: Pre-op assessment: Microcytic assessment: Microcytic anaemiaanaemia Hb optimisationHb optimisation ; oral Fe pre-op and ; oral Fe pre-op and
recheck Hb/MCV. Diet, medical recheck Hb/MCV. Diet, medical treat?treat?
Transfusion Transfusion information/consentinformation/consent
Blood ordering: Blood ordering: MSBOSMSBOS
Consider use ofConsider use of Cell salvage Cell salvage if if predicted peri-op blood losspredicted peri-op blood loss >1 L>1 L

Patient informationPatient information

MSBOSMSBOS

Cell Salvage

Case 1. Peri-op Case 1. Peri-op transfusiontransfusion
Hb 11.5g/dL pre-op as a result of Hb 11.5g/dL pre-op as a result of FeFe
‘‘Group & Screen’ requested.Group & Screen’ requested. Patient Group: A Pos.Patient Group: A Pos.
Antibody screen: NegativeAntibody screen: Negative Patient said to be:Patient said to be:
‘suitable for electronic issue’.‘suitable for electronic issue’. What does this mean?What does this mean?

Electronic issueElectronic issue
Two transfusion samples at different Two transfusion samples at different times; both showing same ABO/Rh times; both showing same ABO/Rh group and negative Ab screengroup and negative Ab screen
ABO-compatible can be issued off ABO-compatible can be issued off the shelf without a crossmatch (10 the shelf without a crossmatch (10 mins).mins).
More efficient use of blood.More efficient use of blood.
Case 1Case 1
Quite a lot of bleeding peri-opQuite a lot of bleeding peri-op Post-op Hb 7.8g/dL; patient feels Post-op Hb 7.8g/dL; patient feels
well.well. Will you prescribe blood Will you prescribe blood
transfusion?transfusion? If so, how will you do it?If so, how will you do it?

Case 1.Case 1.
If patient well and progressing post-If patient well and progressing post-op OK, then no need to transfuse.op OK, then no need to transfuse.
(Indication is Hb<8 (Indication is Hb<8 ANDAND symptoms) symptoms) If prescribe blood:If prescribe blood:
– Ring Blood Bank to order (from G&S)Ring Blood Bank to order (from G&S)– Give in the day time (Give in the day time (notnot after 10pm) after 10pm)– 1.5 hours per unit1.5 hours per unit– No need diuretic in fit 45-yr old No need diuretic in fit 45-yr old
womanwoman


Case 2. Liver biopsyCase 2. Liver biopsy
45-year old woman with abnormal liver 45-year old woman with abnormal liver function (?cirrhosis) is due a liver biopsyfunction (?cirrhosis) is due a liver biopsy
Blood count:Blood count:– Hb 12.0g/dL, WBC 3.4x10Hb 12.0g/dL, WBC 3.4x1099/L, Plts 80x10/L, Plts 80x1099/L/L
Coagulation screen:Coagulation screen:– PT 17 (control 14, INR 1.5), aPTTR 1.4PT 17 (control 14, INR 1.5), aPTTR 1.4
Your SpR asks you to order appropriate Your SpR asks you to order appropriate blood products to cover the procedure.blood products to cover the procedure.
What do you request?What do you request?(Where would you look for advice?)(Where would you look for advice?)

‘Policy for the transfusion of platelets, fresh frozen plasma and cryoprecipitate’
Answer: ensure vitamin K has been given.How should it be given? How long does it take to act?What are the side effects of vitamin K?
The side effects of vitamin K Vitamin K-dependent clotting factors Vitamin K-dependent clotting factors
will take 18-24 hours to normalisewill take 18-24 hours to normalise Minimal S/E.Minimal S/E. Should be given slow Should be given slow
IV.IV. Occasional irritation at injection siteOccasional irritation at injection site Oxidant drug – care in G6PD Oxidant drug – care in G6PD
deficiency (-> haemolysis)deficiency (-> haemolysis) Oral vitamin K currently not Oral vitamin K currently not
available (use IV prep orally)available (use IV prep orally)
Case 2. Liver biopsyCase 2. Liver biopsy
Despite this, your registrar insists Despite this, your registrar insists on giving 2 units of Fresh Frozen on giving 2 units of Fresh Frozen Plasma (FFP) immediately pre-Plasma (FFP) immediately pre-biopsy.biopsy.
The biopsy is carried outThe biopsy is carried out Two hours later: Severe SOB and Two hours later: Severe SOB and
hypoxaemia (SaO2 78% on air)hypoxaemia (SaO2 78% on air) CXRCXR

Post Liver Bx / FFP: Post Liver Bx / FFP: CXRCXR
Post liver biopsy (SOB) one week earlier
What are the possible causes of this lady’s dyspnoea?

Case 2. Dyspnoea & CXR Case 2. Dyspnoea & CXR white-out post white-out post transfusiontransfusion Fluid overloadFluid overload SepsisSepsis (infected blood) with (infected blood) with ARDSARDS TRALITRALI: : transfusion-related lung injurytransfusion-related lung injury
– Donor Ab (esp HLA or neut) react with Donor Ab (esp HLA or neut) react with recipient WBC’s -> lung infiltraterecipient WBC’s -> lung infiltrate
– 1-6 hours post transfusion1-6 hours post transfusion– Other features: fever, chills, low/normal Other features: fever, chills, low/normal
CVP,CVP, BP, (neutropenia, monocytopenia) BP, (neutropenia, monocytopenia)
– Good prognosis for recovery if supportedGood prognosis for recovery if supported(e.g. ventilate)(e.g. ventilate)
– Test donors: ?dangerous donor -> exclude.Test donors: ?dangerous donor -> exclude.

Case 3.Case 3.
A woman has just given birthA woman has just given birth
Suddenly she bleeds torrentially Suddenly she bleeds torrentially from the vagina and begins to from the vagina and begins to ooze from mouth, nose and ooze from mouth, nose and previous venepuncture sitesprevious venepuncture sites
In terms of blood product support, In terms of blood product support, What are your immediate actions?What are your immediate actions?

Case 3. Post-partum Case 3. Post-partum haemorrhagehaemorrhage(& generalised bleeding (& generalised bleeding tendency)tendency) PPH protocolPPH protocol – senior help, obstetric – senior help, obstetric
procedures/drugs etcprocedures/drugs etc Blood samples:Blood samples:
– FBC, PT/aPTT, Fibrinogen, D-DimerFBC, PT/aPTT, Fibrinogen, D-Dimer– Crossmatch/order at least Crossmatch/order at least 4 units RBC4 units RBC
(Consider use of O Neg flyers in LW fridge)(Consider use of O Neg flyers in LW fridge)
““Activate massive transfusion protocol Activate massive transfusion protocol (Obstetric)”:(Obstetric)”: includes immediate release includes immediate release ofof2 units of FFP2 units of FFP
Case 3. Post-partum Case 3. Post-partum haemorrhagehaemorrhage(& generalised bleeding (& generalised bleeding tendency)tendency) Hb 7.4g/dL, WBC 15x10Hb 7.4g/dL, WBC 15x1099/L, plts /L, plts
22x1022x1099/L/L
PT >60 secs (INR >12)PT >60 secs (INR >12)aPTTR >12aPTTR >12Fibrinogen 0.2g/L (n.r. 1.5-4.5)Fibrinogen 0.2g/L (n.r. 1.5-4.5)D-Dimer 25.4 D-Dimer 25.4 mg/L FEU (n.r. <0.45)mg/L FEU (n.r. <0.45)
Interpret these results.Interpret these results.

Case 3. Post-partum Case 3. Post-partum haemorrhagehaemorrhage(& generalised bleeding (& generalised bleeding tendency)tendency) AnaemiaAnaemia (bleeding) (bleeding) Virtually Virtually unclottable bloodunclottable blood
– Low plateletsLow platelets– Consumption of all clotting factorsConsumption of all clotting factors– Very low Fibrinogen & high D-DimerVery low Fibrinogen & high D-Dimer
Diagnosis:Diagnosis:Disseminated Intravascular coagulationDisseminated Intravascular coagulation
What blood product(s) will you prescribe What blood product(s) will you prescribe now?now?Where will you look for advice?Where will you look for advice?

‘Policy for the transfusion of platelets, fresh frozen plasma and cryoprecipitate’

Case 3. D.I.C.Case 3. D.I.C.
FFP 15ml/kgFFP 15ml/kg = 4 units for typical adult. = 4 units for typical adult. Approx 1000mL – over 30-60minsApprox 1000mL – over 30-60mins
Platelets 1-2 ‘adult doses’Platelets 1-2 ‘adult doses’ (1 unit = plts (1 unit = plts from 5 donations or one apheresis)from 5 donations or one apheresis)Each unit over 15-20 minsEach unit over 15-20 mins
Cryoprecipitate 2 adult dosesCryoprecipitate 2 adult doses (1 unit = (1 unit = Cryo from 5 donations), when Cryo from 5 donations), when Fibrinogen <1g/LFibrinogen <1g/L
RBC’sRBC’s obviously needed. obviously needed. Diagnose and Diagnose and treat underlying causetreat underlying cause
(e.g. amniotic fluid embolism, IUD) (e.g. amniotic fluid embolism, IUD)

Case 4. Case 4.
A 25-year old man has acute A 25-year old man has acute leukaemia. He has received leukaemia. He has received chemo, but is well with no chemo, but is well with no bleeding other than mild petechiae bleeding other than mild petechiae on legson legs
Hb 10.5g/dL, WBC 0.4x10Hb 10.5g/dL, WBC 0.4x1099/L,/L,Plts 15x10Plts 15x1099/L/L
What blood product(s) would you What blood product(s) would you prescribe?prescribe?Where will you look for advice?Where will you look for advice?

Case 4. Acute Leukaemia, well.Case 4. Acute Leukaemia, well. Hb 10.5g/dL, WBC 0.4x10Hb 10.5g/dL, WBC 0.4x1099/L, Plts /L, Plts 15x1015x1099/L/L
‘Blood Products for Ward 34 patients’
Platelet Transfusions:
For majority of patients give prophylactic platelets when Plt < 10
For patients with additional risk factors aim to maintain Plt > 20• Sepsis – when acutely septic• Concurrent use of antifungals (when acutely unwell)• Other abnormalities of coagulation (eg in those with APML)
Procedures (eg LP, line insertions, biopsies, urethral catheterisation, others) usually require Plt>50
When a thrombocytopenic patient bleeds: 1 adult dose for mild bleed.2 adult doses for serious bleeding – and discuss with Consultant.
So does he need any platelets?

Case 5.Case 5.
A 70-year old man with A 70-year old man with myelodysplasia is receiving his myelodysplasia is receiving his monthly red cell top up on the monthly red cell top up on the haematology day unit.haematology day unit.
Halfway through 2Halfway through 2ndnd unit, he complains unit, he complains of an itchy rash, and tempof an itchy rash, and temp to to 38.4°C. BP dropped to 90/50 mmHg38.4°C. BP dropped to 90/50 mmHg
The nurse calls you. The nurse calls you. What do you do?What do you do?Where do you look for advice?Where do you look for advice?

Itchy rash & Fever Itchy rash & Fever during blood during blood transfusiontransfusion E-library (& blood transfusion folder):
‘Trust wide policy for the transfusion of blood and its components to adults’
Appendix 5:‘POSSIBLE ACUTE COMPLICATIONS OF
TRANSFUSION’This table provides some guidance for
possible actions in the event of transfusion reactions.
HOWEVER: SEEK MEDICAL ADVICE IN EVERY CASE
So what do you think this reaction is?So what do you think this reaction is?

Unlikely to be acute Unlikely to be acute Haemolytic reaction =Haemolytic reaction = Early in transfusionEarly in transfusion Pain at infusion sitePain at infusion site Agitation, chest pain, back/loin pain, Agitation, chest pain, back/loin pain,
‘sense of impending doom’‘sense of impending doom’ Chills, rigors (high temperature, Chills, rigors (high temperature, BP)BP) Red urineRed urine Acute renal failure, DIC. 10% dieAcute renal failure, DIC. 10% die But still check that this is right blood for But still check that this is right blood for
this patient & a compatible ABO group !this patient & a compatible ABO group !

Most likely: febrile Most likely: febrile non-haemolytic non-haemolytic reactionreaction Allergic – usually to WBC Ag (HLA)Allergic – usually to WBC Ag (HLA) Usually in multi-transfused pts or Usually in multi-transfused pts or
multiparous womenmultiparous women Allergic-type manifestations:Allergic-type manifestations:
Urticarial rash, angioedema, itch, Urticarial rash, angioedema, itch, BPBP
How would you treat?How would you treat?

Febrile non-haemolytic Febrile non-haemolytic reactionreaction
Stop transfusionStop transfusion pro temps. pro temps. Give:Give:– Hydrocortisone 100mg IVHydrocortisone 100mg IV– Chlorpheniramine 10mg IVChlorpheniramine 10mg IV– Paracetamol 1g POParacetamol 1g PO– IV N/Saline if hypotensiveIV N/Saline if hypotensive
Consider restartingConsider restarting after 15 mins after 15 minsIf recurs: abandon that bag - ?try If recurs: abandon that bag - ?try another?another?
Blood Transfusion; Blood Transfusion; summarysummary
Consider ways to Consider ways to avoid/minimiseavoid/minimise Give Give rationally & safelyrationally & safely::
– The right productThe right product– At the right timeAt the right time– To the right patientTo the right patient
Pt Pt informationinformation and verbal and verbal consentconsent Understand blood is scarce, expensive Understand blood is scarce, expensive
and dangerous, & occasionally life-and dangerous, & occasionally life-saving!saving!