anaesthesia news - aagbi july web.pdffunding of research into anaesthesia and perioperative care....
TRANSCRIPT

ISSN 0959-2962 No. 324
JULY 2014
The NewsleTTer of The
AssociATioN of ANAesTheTisTs of GreAT BriTAiN
ANd irelANd NEWSANAESTHESIA
INSIDE THIS ISSUE: The James Lind Alliance & setting research priorities
Jury summons: an anaesthetist’s reflection on the legal system
Old, new, borrowed and blue: tranexamic acid
Photograph: W
ellcome Library London

Anaesthesia News July 2014 • Issue 324 3
contents03 editorial 05 The James lind Alliance & National institute of Academic Anaesthesia - Anaesthesia and Perioperative care Priority setting Partnership 06 Jury summons: an anaesthetist’s reflection on the legal system 09 old, new, borrowed and blue: tranexamic acid 11 independent Practice committee report 12 creating a south west simulation network through hiec 15 A novel approach to exam preparation 16 Teaching sAfe obstetrics in Ghana
19 2015 AAGBi innovation in Anaesthesia, critical care and Pain Award 20 less Than full Time training demystified 23 Anaesthesia digested 25 Your letters 28 Particles
12
05
06
16
20
The Association of Anaesthetists of Great Britain and Ireland21 Portland Place, London W1B 1PYTelephone: 020 7631 1650Fax: 020 7631 4352Email: [email protected]: www.aagbi.org
Anaesthesia NewsChair Editorial Board: Nancy RedfernEditors: Nicholas Love and Caroline Wilson (GAT), Nancy Redfern, Richard Griffiths, Sean Tighe, Tom Woodcock, Mike Nathanson, Rachel Collis and Upma MisraAddress for all correspondence, advertising or submissions: Email: [email protected]: www.aagbi.org/publications/anaesthesia-news
Editorial Assistant: Rona GloagEmail: [email protected]
Design: Chris SteerAAGBI Website & Publications Officer Telephone: 020 7631 8803Email: [email protected]: Portland Print
Copyright 2014 The Association of Anaesthetists of Great Britain and Ireland
The Association cannot be responsible for the statements or views of the contributors. No part of this newsletter may be reproduced without prior permission.
Advertisements are accepted in good faith. Readers are reminded that Anaesthesia News cannot be held responsible in any way for the quality or correctness of products or services offered in advertisements. 3
Editorial
The aim of Anaesthesia News is to inform and entertain; preferably at the same time. How? By providing Association members with news, views, and a forum for discussion and, perhaps, challenge. Members submit many articles (and all the letters) and the most interesting news comes from members. So budding authors, get writing and tell us what you are doing and want to share with others and send it to [email protected]. We can't promise to accept every article and letter we receive, but we’ll do our best. We have appointed an Editorial Assistant (Rona Gloag - [email protected]) who works alongside Chris Steer, our Publications and Website Officer; between them they run the submission, review and production processes, while the editors decide which articles to accept.
In this month’s issue there are contributions about international work, jury service, and a report from a trainee in a project management post about his work to create a simulation network in the South West. We receive many articles on overseas work, reflecting the importance the Association’s members place on supporting healthcare in the developing world. Dr Ahmed’s article on jury service reminds us that we are not the only ones working in a bureaucratic, state-run enterprise. As I write, there is an article on the BBC News website that a major trial has been halted due to the defence finding it impossible to find barristers prepared to work at new (reduced) legal aid rates. At a time when the BMA are enduring difficult times as they try to negotiate a new consultant contract, I wonder whether we will read similar stories about the NHS in the future?
There is also an article on a new research priorities setting development run by the James Lind Alliance and the NIAA. The Association is a major funder of the NIAA and of this particular project, which is noticeably different in that as well as professionals, it includes carers and patients. This will be your chance to contribute to guiding the funding of research into anaesthesia and perioperative care.
Finally, summertime is bracketed by AAGBI conferences – GAT in June and Annual Congress in September. I’m looking forward to the Annual Congress in Harrogate. As ever, the scientific programme looks great, and there is the added attraction of Betty’s Tea Rooms. Just don’t tell Mrs N what happens to my diet that week! Following the success of the Charity Bike Ride to Dublin last year, there will be another ride to this year’s venue. Please watch out for details in an e-newsletter very soon. You can either support the riders by donating or, better still, you can join them. The Association’s conferences continue to grow and grow; WSM London 2014 had a record attendance. We assume this is because we are providing what delegates want – good scientific content in a convivial atmosphere and at an attractive location? See you there.
Mike NathansonCouncil member
1939 04/14
2014 Course Dates Location Organisers14-15 July Brighton (A) Dr Susanne Krone25–26 September Liverpool Dr Steve Roberts28–29 November Nottingham (A) Dr Nigel Bedforth
Faculty will vary depending on location
10% Discount for ESRA members – 15% Discount for RA-UK (FULL) members. Cost: £400 / £500 (A) including a CD with presentations and course notes.
Pre-course material can be downloaded once registered on the course – including US physics, anatomy of the brachial / lumbar plexus, current articles of interest and MCQ’s. A pre course questionnaire will be sent 30 days before each course.
For further information and to register logon to www.sonositeeducation.co.uk
PROGRAMMEDay 1• Ultrasound a ppearance of the nerves• Machine characteristics and set-up• Imaging and needling techniques• Common approaches to the brachial plexus / upper /
lower limb• Workshops – using phantoms / models / cadaveric
prosections (A)
Day 2• Consent / training and image storage• Upper / lower limb techniques• Abdominal / thoracic techniques • Cervical plexus / spinal / epidural / pain procedures• Workshops – using phantoms / models / cadaveric
prosections (A)
(A) – Anatomy based courses / with cadaveric prosections
ULTRASOUND GUIDED REGIONAL ANAESTHESIA – BEYOND INTRODUCTORYThese courses are organised by Regional Anaesthesia UK (RA-UK) in conjunction with SonoSite Ltd for training in ultrasound guided regional anaesthetic techniques. Previous experience in regional anaesthesia is essential.
FUJIFILM SonoSite, Inc,. the SonoSite logo and other trademarks not owned by third parties are registered and unregistered trademarks of FUJIFILM SonoSite, Inc. in various jurisdictions. All other trademarks are the property of their respective owners. ©2014 FUJIFILM SonoSite, Inc. All rights reserved.
2014 COURSE DATES:Introductory Ultrasound Guided Regional Anaesthesia29-30 April 6-7 October
Ultrasound Guided Venous Access5 June 23 October
Ultrasound Guided Paediatric Venous Access28 July
All courses qualify for CPD Accreditation.
Venue: SonoSite Education Centre, 240 The Village, Butterfield, Great Marlings, Luton, Bedfordshire LU2 8DL
Contact: Louise Smith Tel: +44 (0) 7593 614034 Email: [email protected]
For the full listing of SonoSite training and education courses, dates and to register go to: www.sonositeeducation.co.uk
SonoSite, the world leader and specialist in hand-carried ultrasound, has teamed up with some of the leading specialists in the medical industry to design a series of courses, for both novice and experienced users, focusing on point-of-care ultrasound.
INTRODUCTORY ULTRASOUND GUIDED REGIONAL ANAESTHESIA The two-day introductory course is designed to teach those who have little or no experience in the use of ultrasound in their normal daily practice. The course comprises of didactic lectures on the physics of ultrasound, ultrasound anatomy and regional anaesthesia techniques. The lectures and hands-on sessions will concentrate on the brachial plexus, upper and lower limb blocks.
ULTRASOUND GUIDED VENOUS ACCESSThis one-day course is aimed at physicians and nurses involved with line placement and comprises didactic lectures, ultrasound of the neck, hands-on training with live models, in-vitro training in ultrasound guided puncture and demonstration of ultrasound guided central venous access. The emphasis is on jugular venous access, but femoral, subclavian and arm vein access will also be discussed.
ULTRASOUND GUIDED PAEDIATRIC VENOUS ACCESSThis one-day course is designed to teach delegates the technique of ultrasound-guided venous access in children. The course is aimed at physicians, nurses and healthcare professionals and comprises didactic lectures, hands-on ultrasound of the neck, in-vitro training in ultrasound guided puncture and demonstration of ultrasound guided central venous access. Areas covered will include jugular, femoral, subclavian venous access and arm vein access will also be discussed.
Fees: £375 (two-day courses) includes VAT, lunch, refreshments and course materials. £260 (one-day courses) includes VAT, lunch, refreshments and course materials.
ULTRASOUND TRAINING COURSES

Anaesthesia News July 2014 • Issue 324 5
Fifth National Audit Project from The Royal College of Anaesthetists and The Association of Anaesthetists of Great Britain and Ireland Accidental Awareness during General Anaesthesia
NAP5 Professional Launch Wednesday 10 September 2014
The Royal Society of Medicine, London
A full-‐day’s educational meeting, presenting the Fifth National Audit Project from The Royal College of Anaesthetists and The Association of Anaesthetists of Great Britain and Ireland. The day will present the largest ever study of Accidental Awareness during General Anaesthesia. Open to all anaesthetists and others with an interest. NAP5 Local Co-‐ordinators are especially invited to attend. The presentations will be delivered by the NAP5 Steering Panel: anaesthetists, psychologists and patient representatives Organisers: Professor Jaideep J Pandit & Professor Tim M Cook Fee: £150 CPD Credits anticipated: 5 Topics to be covered will include -‐
Overview of findings Baseline survey results Activity survey results Incidence(s) of awareness Depth of anaesthesia monitoring Patient experiences Consequences of awareness Awareness during induction, maintenance
and emergence Awareness and anaesthetic techniques -‐
TIVA, muscle relaxation etc.
Awareness and sub-‐specialties -‐ Obstetrics, Cardiac, Airway, ICU, Paediatrics etc.
Reports of awareness following sedation Depth of anaesthesia monitoring and NAP5 Medico-‐legal and consent issues The Irish experience Case presentations Question and answer session Recommendations Future steps
James Lind was an 18th century Scottish naval surgeon who discovered by careful analysis and exclusion of other factors, and against contemporary medical wisdom, the cause of scurvy in sailors. His methodology is reported to have included the first ever clinical trial. He campaigned for better ventilation and improved personal cleanliness on naval vessels and his MD thesis was on venereal disease. He spent part of his career as Chief Physician at the Royal Hospital at Haslar, where his son John succeeded him. The James Lind Alliance (JLA) (www.lindalliance.org) is a not-for-profit organisation created in 2004 and now part of the National Institute for Health Research’s NIHR Evaluation, Trials and Studies Coordinating Centre (NETSCC). The JLA facilitates partnerships of patients, carers and clinicians to develop a list of possible treatment uncertainties, discover which are truly unanswered, and then prioritise into a top 10. There are currently 19 completed partnerships listed on the JLA website and others are in progress. The completed top 10s include stroke, asthma and dementia. While some uncertainties are (perhaps) clear, others, for example ‘What are the benefits of breathing exercises as a form of physical therapy for asthma?’, might not be so obvious to clinicians.
The NIAA undertook a research priority setting exercise in 2009.1 A list, generated by clinicians, of research topics was published and some have gone on to be the subject of research projects. The difference between that exercise and the current JLA-guided project is the addition of carers and patient groups in both the survey and the project steering group. The output (expected in 2015) will be used to guide the awarding of research grants by the funding partners and may be used by other funders when deciding how to prioritise research in our areas of interest. For example, it might be helpful to colleagues who apply for a grant from one of the larger funders such as the Wellcome Trust or the MRC.
As I write this piece, the exact question and survey are being finalised, and by the time this article in published the survey should be live and responses will have been invited. You know what comes next - please take part! This is a great opportunity to raise awareness of your ideas and your own priorities.
The AAGBI and Anaesthesia are already major sponsors of UK and Irish research into anaesthesia, intensive care and pain management (approx. £180,000 in 2013-14; most of which was awarded via the NIAA to allow studies to be eligible for NIHR portfolio funding, which can help offset NHS costs of research). The AAGBI has research aims (see Box 1), based on the views of its members. It is very likely that the output of this project will be added into our ‘menu’, so please do participate in the survey.
Mike NathansonCouncil Member
Reference1. Howell SJ, Pandit JJ, Rowbotham DJ, for the Research Council of the
National Institute of Academic Anaesthesia. National Institute of Academic Anaesthesia research priority setting exercise. British Journal of Anaesthesia 2012; 108: 42-52.
The James Lind Alliance & National Institute of Academic Anaesthesia - Anaesthesia and Perioperative Care Priority Setting Partnership
This project (which may well have the longest title in the history of the AAGBI) is an initiative of the major funders of the National Institute of Academic Anaesthesia (NIAA) who have commissioned the James Lind Alliance to discover and prioritise treatment uncertainties in anaesthesia and perioperative care, as nominated by members of the profession, patients and their carers.
Photograph: W
ellcome Library London
Box 1
current AAGBi research priorities
• Patient safety
• Innovation
• Clinical outcomes
• Education and training
• Professional issues (e.g. standards and guidelines, working conditions, medico-legal issues)
• The environment

6 Anaesthesia News July 2014 • Issue 324 Anaesthesia News July 2014 • Issue 324 7
Jury summons: an anaesthetist’s reflection on the legal systemIt was my first weekend off after nights, and I was perusing my mail: papers, ads, bills, magazines... and a letter from HM Courts and Tribunal Service. The Jury Central Summoning Bureau computer randomly selects jurors from the electoral register. I was 1 of 200,000 people randomly chosen that year. Previously, people performing an important service, such as doctors, were exempted but since 2004 this is no longer so. Exempted professions are restricted to those associated with law enforcement - police, magistrates and lawyers. Also exempt are people who have had to spend time in a mental facility or been detained at Her Majesty's Pleasure. As no employed doctor would fall in either category I had to accept the fact that I belonged to the Court for two weeks.
The date on which I was required was during the ESRA congress in Glasgow which I had booked in advance. So I asked for a deferral, listed the dates when I could attend and hoped the Bureau would forget all about me. No such luck. A fortnight later I received another letter informing me that because I had deferred once I couldn’t defer again and was now required to attend.
I was relieved to find I did not have to do any on-call swaps and broke the news to the department. It was agreed that, although inconvenient, it really could have been a lot worse! With no rota problem, I now had to tackle how two weeks away was going to impact on my training. I was supported by the College Tutor and rota coordinator to maximise training opportunities and thus facilitate a 'sign off' at the end of the module.
Safety and trust induction
Similar to trust and department inductions we trainee doctors endure on a regular basis, there was a court induction. I went through a metal detector, had my handbag searched and was led to the Jury Lounge (a process repeated every time I entered the Court), a large hall that held over 150 would-be jurors. Loss of earnings certificates were submitted, travel expense forms were completed and we were issued with meal allowance cards. A 20 minute video was played giving information on who's who in Court and what their jobs are.
The waiting game
Not unlike the NHS there is a lot of waiting, and it is possible for a juror to be summoned but not get called for Court. You can read, play, watch the television or work, but you can't get out. When you are called, you are one of 15 people who get marched into a Court room where one or more jurors may be rejected because of familiarity with the stakeholders. Twelve names are picked randomly and the rest make their way back to the lounge where they can enjoy overpriced coffee. After taking an oath to assess the defendant based on the evidence, the trial begins.
Data protection
The judge explains our duty, and how it differs to his, and lays down the ground rules. It's simple really - discuss the particulars of the case with anyone or discuss the deliberations with anyone and you get slammed with contempt of court. Foolish jurors have been fined or even imprisoned when they tested the court.
Procedure, consent and evidence based practice
A lot of time is spent explaining the minutiae of procedures, akin to consent. In the same way as a missing consent form results in delays in operating theatres, the courts also suffer with missing documents causing delays. These documents also have typos and incorrect grammar although I envy the fact that documents submitted in evidence were handwritten in full. I wish we could do that in the NHS - how much time is wasted trying to decipher the codes left to us by our colleagues?
Quality control
In their own way the courts are as obsessed with quality as we are. The judge plays a major part in that, but so do jurors. The judge deals with legal matters and makes notes as we go along. This is very much a rate limiting factor; we can go as quickly as it takes the judge to write or type the notes he needs. Colleagues working with particularly slow surgeons will share the pain.
Life and drama
Disappointingly there were no tear jerking closing speeches. Nor was there any sudden unplanned evidence or surprise witnesses that would blow the case wide open. And no - there were no constant calls of 'Objection!' from anyone; no one dared upset the judge. Sad to say there was no Tom Cruise or Richard Gere, with or without wigs. But then I imagine our patients are equally disappointed to find that George Clooney does not work in ED, and Patrick Dempsey does not grace our operating theatres. We were assured many times by the judges that this is not at all like it is portrayed on television. There is no denying that the slow pace and controlled manner in which the process was run inspired confidence.
Leadership in practice
After the witnesses have given their statements, been cross-examined, re-examined and the counsellors have given their closing speeches, it is down to the judge to round proceedings up. He gives a summary, reminds us of our duties and sends us away to deliberate under the care of a sworn bailiff. After making sure we are free of tablets and smartphones, we are locked in a
room with only a buzzer as a means of communication. First we had to elect a foreman who chairs the discussions and declares the verdict at the end. Then we need to agree. To come back with a verdict of guilty we must all be sure that this is the case, based on the evidence. Nothing less will suffice.
As in medical meetings, it is difficult to agree on a course of action. As Madame Foreman, it was helpful to get people to verbalise their thoughts and concerns, and also to suggest ways to view the evidence put before us in terms of relevance and reliability. In this way, rather than influence jurors one way or another, we all participated in discussing and analysing the data. Every now and again I would count those who stated ‘guilty’, ‘not guilty’ and ‘unsure’, to mark our progress. Eventually we were sent home and although I could not discuss the case I could not stop thinking about it. I believed that a few of my fellow jurors would do the same, and so when we continued deliberations next morning, a count revealed we had a unanimous verdict. Some things can't be rushed - the same is true in medicine.
Court efficiency
Just as we try and improve theatre efficiency by decreasing turnover time, the courts improve their efficiency by juggling more than one case at a time. No one can rush the jury into making a verdict so during deliberations the judge presides over another case. Once we reach a verdict and have called the bailiff, a message is sent to the judge and a break is made in the other case, whose jurors are discharged back to the lounge while we are marched back in to deliver our verdict.
Cost
Healthcare is not cheap, politicians tell us, but neither is justice. It costs the taxpayer anything from £7,000–£10,000 per court per day, hence their need to juggle cases.
Pros and cons
The high cost of catering is not just an NHS theme, the courts are affected too. Although the catering was expensive, and the meal allowance minimal, there was at least an allowance and lunchtime was never less than an hour. But there is one strong advantage that we miss in the NHS; there was never any pressure, or emotional blackmail to come earlier or stay later than we should.
inas Ahmed ST7 Northwest Deanery
Conclusion
Although I was unimpressed with the calibre of cases presented to us by the CPS, it was an interesting experience that gave me insight to the judicial system. I was, however, glad to go back to the friendly banter in theatre where I am much more at home.
Anaesthesia News July 2014 • Issue 324 9
Winner of the Wylie Undergraduate Essay Prize 2014
Old, new, borrowed and blue: tranexamic acidNot all weddings will end with happiness forever after. Every day in the UK and worldwide, countless unsuitable weddings are taking place; asphalt with bare skin, cold metal with blood vessels, and glass with taut muscle. What gift would a wise doctor bring to such traumatic marriages, to ensure the best chance of a happy outcome following these ill-fated pairings? Superstition dictates brides wear something old, something new, something borrowed and something blue to avoid misfortune. One gift springs to mind which, it can be argued, satisfies all criteria at once: tranexamic acid.
Tranexamic acid is an old drug indeed, discovered (appropriately) by married couple Utako and Shosuke Okamoto over 50 years ago.1 An analogue of lysine, it reduces bleeding by inhibiting fibrinolysis.2 Through reversible antagonism of the lysine binding sites of plasminogen, tranexamic acid prevents the activation of plasminogen to plasmin and the subsequent degradation of fibrin polymers. It therefore reduces bleeding by slowing thrombus breakdown, rather than promoting thrombus formation. Tranexamic acid also has anti-inflammatory properties, since plasminogen receptors on many cells activate pro-inflammatory signalling pathways.3
New enthusiasm for using this old drug in trauma follows several large trials showing it reduces mortality; CRASH-2; MATTERs; and, MATTERs II.4-6 CRASH-2 was a randomised placebo-controlled trial of 20 211 patients worldwide, showing that tranexamic acid slightly reduced overall mortality in adult trauma patients with actual or suspected bleeding without increasing vascular events. Later subgroup analysis showed 7.7% of patients given placebo died from bleeding versus 5.3% of patients given tranexamic acid within 3 hr, while later administration decreased survival.7 Importantly, the mortality reduction wasn’t just in the most severely injured patients, but in all groups.8 MATTERs, a retrospective non-randomised trial in one military hospital in Afghanistan, showed tranexamic acid improved survival and reduced coagulopathy (MATTERs II showed this benefit was additive to that of giving cryoprecipitate). This was an interesting finding mechanistically as, following major trauma, hypovolaemic shock rapidly leads to multiple derangements of coagulation. This is known as acute traumatic coagulopathy.9,10 Widespread simultaneous coagulation and fibrinolysis ensues, with the degree of fibrinolysis linked to the risk of death.11 Tranexamic acid may therefore reduce mortality through inhibiting acute traumatic coagulopathy.
The rationale for tranexamic acid in trauma was borrowed from existing evidence showing a reduction in blood transfusions during elective surgery. This in turn was borrowed from the drug’s oldest established use – for menorrhagia.12 It has been used in cardiac surgery13 and orthopaedics to reduce blood loss,14 with no apparent increase in thrombotic complications. A recent meta-analysis showed decreased transfusion requirements across a wide range of surgical procedures.15 This may be a
compelling argument for routine use in surgery, once safety is assured. Aside from reducing transfusion-related complications, in a post-‘Nicholson Challenge’ NHS there is an economic argument; one unit of blood costs £125,15 while 2 g of tranexamic acid costs £6.20.16
Blue is the mood of many asking why this cheap effective drug isn’t more widely and readily available. The CRASH-2 authors estimated over 100 000 lives could be saved yearly worldwide,17 calling on medical professionals to promise to use it to full effect.18 Tranexamic acid is perhaps the first drug promoted by a comic,19 and even the Daily Mail has commented in typical measured tone, asking ‘Why are hospitals ignoring a drug that can stop patients bleeding to death?’.20 While it may well be underutilised, some caution may be warranted as unanswered questions exist. Many are outlined in an excellent recent review,11 so only the most important are considered here. Firstly, the relevance of a study largely conducted in developing countries was queried in patients who receive rapid access to treatments like fixed ratio transfusion.21 MATTERs and MATTERs II, based in well-resourced military hospitals, perhaps answered this point. The mechanism of action was unclear in CRASH-2, as there was no reduction in transfusions. However, transfusion decisions may often have been made before the decision to give tranexamic acid, and survivors bias could mean patients surviving longer received more transfusions. The most serious issue with antifibrinolytics is the potential for vascular occlusive events. Some argue the extremely low rate of thrombo-embolic events overall in CRASH-2 could be due to varying protocols for screening;21 others counter that myocardial infarctions would be a more sensitive measure, which decreased in the treatment group.22 The MATTERs treatment group had nine times as many pulmonary embolisms as placebo.5 However, the MATTERs authors argue that its retrospective nature means this could be due to more severe injury in treated patients, in addition to survivors bias, and that mortality decreased overall. A current Australian trial, PATCH, aims to fill some of these ‘knowledge gaps’,22 and provide definitive evidence tranexamic acid is safe and effective in developed countries. These blue notes may seem overly cautious, but history should be considered. Recombinant factor VIIa has also been used to reduce traumatic bleeding; evidence accumulated that it wasn’t as safe or effective as initially thought,23,24 and it is becoming less popular.
Join usgoanesthesiology.org
14-102
Members of the Association of Anaesthetists of Great Britain and Ireland will receive a discount to attend the ANESTHESIOLOGY™ 2014 annual meeting. Enter promo code: GBI14
THE
ANNUAL MEETING
OCTOBER 11-15, 2014NEW ORLEANS, LA
OCTOBER 24-28, 2015SAN DIEGO, CA
OCTOBER 22-26, 2016CHICAGO, IL
OCTOBER 21-25, 2017BOSTON, MA
OCTOBER 13-17, 2018SAN FRANCISCO, CA
OCTOBER 19-23, 2019ORLANDO, FL
Register now for the ANESTHESIOLOGY™ 2014 annual meeting, the premier educational event in anesthesiology:
• More than 15,000 attendees from 90 countries• Presenters from around the world as well as dedicated international sessions• Participation from national and international societies representing every
anesthesiology specialty• Networking opportunities at the International Connection Center• Largest exhibit hall featuring the latest products and services in the industry
Join usgoanesthesiology.org
14-102
Members of the Association of Anaesthetists of Great Britain and Ireland will receive a discount to attend the ANESTHESIOLOGY™ 2014 annual meeting. Enter promo code: GBI14
THE
ANNUAL MEETING
OCTOBER 11-15, 2014NEW ORLEANS, LA
OCTOBER 24-28, 2015SAN DIEGO, CA
OCTOBER 22-26, 2016CHICAGO, IL
OCTOBER 21-25, 2017BOSTON, MA
OCTOBER 13-17, 2018SAN FRANCISCO, CA
OCTOBER 19-23, 2019ORLANDO, FL
Register now for the ANESTHESIOLOGY™ 2014 annual meeting, the premier educational event in anesthesiology:
• More than 15,000 attendees from 90 countries• Presenters from around the world as well as dedicated international sessions• Participation from national and international societies representing every
anesthesiology specialty• Networking opportunities at the International Connection Center• Largest exhibit hall featuring the latest products and services in the industry
Anaesthesia News July 2014 • Issue 324 11
Tranexamic acid is a gift steadily becoming more fashionable; often initiated by UK paramedics pre-hospital, subject of the first NICE off-label evidence summary, part of UK military ballistic trauma protocols25 and a WHO ‘essential drug’.26 Before its adoption into many UK trauma protocols, hospital surveys showed it was probably underutilised –auditing current practice may well be useful.27 As with any new drug or off-label use, unanswered questions remain following the first trials. Despite this, there is enough evidence to suggest it can become an important part of trauma management. It’s not a heroic intervention – the benefit will be seen through widespread use rather than saving the most severely injured. It’s not an expensive or ostentatious gift – there certainly isn’t much commercial interest in promoting it. Unlike an expensive and dazzling white gown, tranexamic acid may be the quiet, unassuming wedding present which surprises over the years with its usefulness. Hopefully this old, new, borrowed and blue drug will bring luck as the old wives’ tale says, and keep more victims of traumatic weddings around each year to live happily ever after.
References1. Okamoto S, Okamoto U. Amino-methyl-cyclohexane-carbolic acid: AMCHA. A new potent
inhibitor of fibrinolysis. Keio Journal of Medicine 1962; 11: 105-15.2. Ortmann E, Besser MW, Klein AA. Antifibrinolytic agents in current anaesthetic practice. British
Journal of Anaesthesia 2013; 111: 549-63.3. Godier A, Roberts I, Hunt J. Tranexamic acid: less bleeding and less thrombosis? Critical Care
2012; 16: 135.4. The CRASH-2 Collaborators. Effects of tranexamic acid on death, vascular occlusive events, and
blood transfusion in trauma patients with significant haemorrhage (CRASH-2): a randomised, placebo-controlled trial. Lancet 2010; 376: 23-32.
5. Morrison JJ, Dubose JJ, Rasmussen TE, Midwinter MJ. Military Application of Tranexamic Acid in Trauma Emergency Resuscitation (MATTERs) Study. Archives of Surgery 2012; 147: 113-9.
6. Morrison JJ, Ross JD, Dubose JJ, et al. Association of cryoprecipitate and tranexamic acid with improved survival following wartime injury: findings from the MATTERs II study. JAMA Surgery 2013; 148: 218-25.
7. The CRASH-2 Collaborators. The importance of early treatment with tranexamic acid in bleeding trauma patients: an exploratory analysis of the CRASH-2 randomised controlled trial. Lancet 2011; 377: 1096-101.
8. Roberts I, Perel P, Prieto-Marino D, et al. Effect of tranexamic acid on mortality in patients with traumatic bleeding: prespecified analysis of data from randomised controlled trial. British Medical Journal 2012; 345: 16.
9. Brohi K, Singh J, Heron M, and Coats T. Acute traumatic coagulopathy. Journal of Trauma 2003; 54: 1127-30.
10. Davenport R. Pathogenesis of acute traumatic coagulopathy. Transfusion 2013; 53 (suppl 1): 23S-7S.
11. Napolitano LM, Cohen MJ, Cotton BA, et al. Tranexamic acid in trauma: how should we use it? Journal of Trauma and Acute Care Surgery 2013; 74: 1575-86.
12. Nilsson L, Goran R. Treatment of menorrhagia with an antifibrinolytic agent, tranexamic acid. Acta Obstetrica et Gynecologica Scandinavica 1967; 46: 572-80.
13. Brown RS, Thwaites BK, Mongan PD. Tranexamic acid is effective in decreasing postoperative bleeding and transfusions in primary coronary bypass operations: a double-blind, randomised, placebo-controlled trial. Anesthesia & Analgesia 1997; 85: 963-70.
14. Ho KM, Ismail H. Use of intravenous tranexamic acid to reduce allogeneic blood transfusion in total hip and knee arthroplasty: a meta-analysis. Anaesthesia and Intensive Care 2003; 31: 529-37.
15. Ker K, Edwards P, Perel P, et al. Effect of tranexamic acid on surgical bleeding: systematic review and cumulative meta-analysis. British Medical Journal 2012; 344: 15.
16. Joint Formulary Committee. British National Formulary, 2013. http://www.medicinescomplete.com (accessed 23/12/13)
17. Ker K, Edwards P, Perel P, et al. Avoidable mortality from giving tranexamic acid to bleeding trauma patients: an estimation based on WHO mortality data, a systematic literature review and data from the CRASH-2 trial. BMC Emergency Medicine 2012; 12: 1-7.
18. Shakur H, Roberts I, Piot P, et al. A promise to save 100,000 trauma patients. Lancet 2012; 380: 2062-3.
19. Roberts I, Vieceli E, Duffield P. TXA Comic strip, 2012. http://researchonline.lshtm.ac.uk/333704/1/TXA.pdf (accessed 28/12/13)
20. Lavender C. Why are hospitals ignoring a drug that can stop patients bleeding to death? 2012. http://www.dailymail.co.uk/health/article-2214884/Why-hospitals-ignoring-drug-stop-patients-bleeding-death.html (accessed 28/12/13)
21. Gruen RL, Jacobs IG, Reade MC. Trauma and tranexamic acid. Medical Journal of Australia 2013; 199: 310-1.
22. Cap AP, Baer DG, Orman JA, et al. Tranexamic acid for trauma patients: a critical review of the literature. Journal of Trauma 2011; 71: S9-S14.
23. Levi M, Levy JH, Andersen HF. Truloff D. Safety of recombinant activated factor VII in randomized clinical trials. New England Journal of Medicine 2010; 363: 1791-800.
24. Mamtani R, Nascimento B, Rizoli S, et al. The utility of recombinant factor VIIa as a last resort in trauma. World Journal of Emergency Surgery 2012; 7 (suppl 1): S1-S6.
25. Doughty HA, Woolley T, Thomas GOR. Massive transfusion. Journal of the Royal Army Med Corps 2011; 157: S277-S83.
26. World Health Organisation. Summary of the report of the 18th meeting of the WHO Expert Committee on the Selection and Use of Essential Medicines, 2011. http://www.who.int/selection_medicines/committees/TRS_web_summary.pdf (accessed 24/12/13)
27. Bozzette A, Aeron-Thomas A. Reducing trauma deaths in the UK. Lancet 2013; 382: 208.
Jamie l McPhersonUniversity of Newcastle
NATIONAL HONOURS
FOR ANAESTHESIA, CRITICAL CARE AND PAIN MEDICINE(MBE, OBE, CBE, KNIGHT/DAME)
Do you know someone who you believe should receive national recognition for their contribution to anaesthesia, critical care or pain medicine? Someone who has really made a difference to others’ lives, often in a quiet and unsung way, perhaps working in a voluntary capacity or for a charity linked to anaesthesia?
The AAGBI is always pleased to receive names of suitable individuals whom it can consider for nomination via the specialty’s National Honours Committee.
Please contact [email protected] for further details and guidance
Medical students in Great Britain and Ireland are eligible to apply to the AAGBI Foundation for funding towards a medical student elective period taking place between October 2014 and March 2015. A further round of funding will be advertised in the Autumn for electives taking place from April 2015 onwards.
Preference will be given to those applicants who can show the relevance of their intended elective to anaesthesia, intensive care or pain relief. Applicants may wish to note that a key focus of the AAGBI is support for projects in the developing world.
For further information and to apply please visit our website: www.aagbi.org/undergraduate-awards email [email protected] or telephone 020 7631 1650 (option 3)
Closing date: 18 July 2014 for consideration at the September 2014 Research & Grants Committee meeting
UNDERGRADUATE ELECTIVE FUNDINGUP TO £750
Q&A
Anaesthesia News July 2014 • Issue 324 11
Independent practIce commIttee report
What were the IPC’s three biggest achievements from last year?
1. The CMA found that anaesthetic groups do not cause an adverse effect on competition as originally suggested by the Office of Fair Trading and by several PMIs. This conclusion resulted mainly as a result of the evidence submitted by the AAGBI. It is our legal advisor’s view that it is unlikely that this issue will be addressed again and, therefore, the growing number of Independent Departments of Anaesthesia (IDAs) are secure from future accusation of anti-competitive behaviour.
2. The CMA has recognised that differential NHS earnings in the private sector can be regarded as incentives. This provides a major opportunity to advance the cause of pay parity for anaesthetists in the private sector. As NHS activity in the private sector is planned to increase substantially, it is likely that an increasing number of our members will be advantaged by this decision, even when they have no interest in private practice.
3. The CMA has quoted AAGBI evidence on several occasions. In particular, our ‘Voluntary Code of Practice for Billing Private Patients’2 was commended as an example of good practice.
What current challenges are independent practices facing?
We are preparing for a judicial review on the CMA information remedies. While we support the remedies in principle, they are disproportionate if fees continue
to be constrained by PMI recognition agreements and ‘top-ups’ by patients are not facilitated. As a result, patients will not be able to ‘shop around on the basis of quality and cost’.1 The Federation of Independent Practitioner Organisations (FIPO) has obtained expert legal opinion that there is ‘a better than even’ chance of success on these grounds and therefore, the AAGBI has contributed to the legal costs on behalf of members. FIPO has to raise £100,000 and is currently asking individual consultants to make a donation. Please support this. Instructions can be obtained from [email protected]
What are the IPC’s priorities for the coming year?
1. To actively engage with FIPO to mount a successful appeal against the CMA findings.
2. To revise the AAGBI guideline ‘Voluntary Code of Practice for Billing Private Patients’.
3. To organise a seminar on Private Practice Issues in late 2014 or early 2015.
References1. https://assets.digital.cabinet-office.gov.uk/
media/533af065e5274a5660000023/Private_healthcare_main_report.pdf (accessed 23/04/2014).
2. http://www.aagbi.org/sites/default/files/code_of_practice_08.pdf (accessed 23/04/2014).
dr sean Tighe Chair of the Independent Practice Committee
what does your committee focus on?
The independent Practice committee discusses all issues relating to anaesthetic practice in the private sector. This year our activity has been concentrated on responding to the Competition Commission’s Investigation into the private healthcare market. The final report was published by the Competition and Markets Authority (CMA) in April 2014.1

12 Anaesthesia News July 2014 • Issue 324 Anaesthesia News July 2014 • Issue 324 13
Creating a South West simulation network through HIEC
‘what is hiec? what are you up to?’ i forget the number of times these questions were asked over the course of my secondment. The first was easy enough to answer; you just Google the description, but you’re not really left any the wiser with what it actually does. The second is somewhat more difficult and i’m still trying to bring it all into focus.
According to the HIEC website, Health Innovation and Education Clusters are ‘collaborative partnerships between NHS organisations, academia and industry’. There is mention of transforming healthcare, driving up quality, developing the workforce. The mantra of progressive, innovative thinking no doubt, but what does it all mean?
Putting this into context, I’m an anaesthetic registrar with two years training to go. On a normal day I head to work, I am given a list of patients to anaesthetise, patients are provided, a team is present, the surgeon operates, patients are woken up and I go home. By 8.30am I’ve planned my day and follow it as long as the patients and staff behave themselves. Ideal for creatures of habit who enjoy the comfort of routine.
The next year would be very different. The offer of a project management post from the South West HIEC director was unexpected. I had registered interest in management experience over 18 months previously but nothing had materialised. The initial proposition left me somewhat bewildered, with an uncomfortable lack of specificity. I had to propose a project and run with it. I had to be ‘innovative’. A few initiatives were mooted and I was strongly in favour of developing simulation in the region. I had experience with simulation training, understood its limitations and some of its potential. The timing was fortuitous as there had been a large Deanery capital investment in equipment and there were fears of under-utilisation. The Chief Medical Officer’s 2008 report had emphasised the importance of building simulation into future workforce training.1 The Framework for Technology Enhanced Learning was in draft and would raise the bar for workforce skills education.2 This was a ‘hot potato’.
Building a network
Following a successful competitive application process, the proposal was to scope regional simulation provision and build a functional network between the Severn and Peninsula Deaneries. I immediately hijacked Kipling’s six honest and serving men: What, Why, When, How, Where and Who, as these highlighted the sheer scale of the venture.3
Defining simulation was the first problem; it means different things to different people. Was I really going to achieve collaboration in simulation ranging from actors undertaking role playing and part task (body part) trainers, to high fidelity simulation? How could I possibly engage everyone from HCAs to Trust Boards and the Strategic Health Authority (SHA) in this process? Covering the geographical expanse of the Deaneries from Lands End to Swindon seemed a little adventurous. It was not as though I had huge team for support, it was just me with some guidance from an overburdened director.
Making progress
The next few months were spent touring the simulation centres, the Deaneries and the SHA. I spent time talking to providers, commissioners, managers and learners to understand the level of provision, the challenges faced and proposals for future delivery of care. Themes emerged and through the use of qualitative research methodology - grounded theory - these ideas were coded and distilled.4 This formed the backbone to a South West simulation strategy.
Simulation provision within the region was entrenched, there were large pockets of expertise, enthusiasm was palpable, and some had been using it for years. The existing Peninsula Simulation Network provided an excellent forum for idea sharing amongst providers and hosted a number of regional simulation programmes. The Bristol Medical Simulation Centre was internationally renowned, providing an array of multidisciplinary educational initiatives. Despite this there was a palpable lack of structure, cohesion and accountability. Many providers lacked financial and technical support to provide sustainable future training programmes.
The main purpose of the strategy was to provide a vision for the future. We wanted to build high quality simulation training, fully integrated into the workforce and to promote safe and excellent clinical care. Effective collaboration across the region was a key element. The Peninsula and Severn Deaneries were brought together, formal and informal meetings were held to discuss joint
figure 1 The interdependence of individual and team training is central to providing a high quality service
ventures in education and research, share best practice, and widen the participation of simulation and faculty development. Raising and maintaining standards of simulation were essential to drive up quality. A formal quality assurance framework was devised with benchmarks for organisational structure, courses, resources and faculty.
We formed a steering group to take the newly coined ‘South West Technology Enhanced Education and Research’ (STEER) strategy forward. This group was fundamental to successful implementation. As a trainee in anaesthetics, I felt I neither had the necessary credibility or indeed wisdom to make this project work alone. The STEER committee comprised providers including doctors, nurses, midwives, the Deaneries and the SHA/LETB (Local Education & Training Board). The purpose was not only to drive forward implementation of the STEER strategy but also to provide a vital link between providers and commissioners. It remains the only truly multidisciplinary networked organisation within the new LETBs.
Depending on your view, the timing of this project was either fortunate or poor. Poor, in terms of the pending demise of the SHA meant that financial commitment was absent. Fortunate, in that the evolution of the LETB provided an opportunity to reframe the relationship between commissioners and trusts or educational providers. We took the opportunity to influence the content of the Learning and Development Agreements with trusts to raise the profile of simulation in the region.
Targeted training
Implementing the strategy has been most challenging. It soon became apparent that achieving all the strategic work streams would be impossible in the short term. We had to maximise the impact and target the widest part of the workforce in closest proximity to patients to improve care and outcomes. Historically, the link between education provision and service improvement had been missing, with education provided in uniprofessional silos at a distance from actual patient care. This was inefficient and often missed the point of what we are training for. The perception of education by many trusts was also unhelpful, where releasing staff and faculty was felt to have a detrimental impact on service provision. Only the more forward thinking could see that improved team performance through education enhanced productivity and promoted safer care.
We strongly supported multidisciplinary point-of-care training with robust learning outcomes. Knowledge, technical and non-technical skills must all be addressed with an integrated approach using appropriate educational modalities such as simulation. Team-based training should be part of the fabric of healthcare delivery. The STEER challenge was to work with commissioners and providers to make this happen.
Through integrated education, human factor elements to patient safety can be addressed and taught. Both system and personal errors can be identified and rectified. In February 2013, a collaboration of STEER with the Safety Patient Initiative in the LETB and other human factors experts ran a South West Human Factors conference. Representatives from 27 organisations ranging from primary care and mental health to acute healthcare trusts collaborated to create a regional human factors strategy. With greater personal clarity it seems that innovation, simulation and human factors are necessary ingredients to improving safer patient care.
Conclusion
While the natural life of HIEC is coming to an end, it has spawned a number of initiatives of which STEER is one. The new Academic Health Science Networks must be embraced and help to ensure that these initiatives are sustained for the future.
In terms of lessons learned there are many, but a few key ones are:i Develop clear and achievable outcomes from the outset, even if you don’t know how to get there. Though these may evolve with time, time may have been used more effectively.ii Undertake early project management training (e.g. Prince2). These tools would have been invaluable at the start. I completed an Open University certificate in management but this was too late to make a real diiference.iii Early commitment planning is vital. Find out who the movers and the shakers are early on and get them on board.iv Building the need is essential. If people can’t understand what you want to achieve and why it’s important they won’t support it.v Understanding people, insight and reflection is important. If you want people to change their practice and their behaviour, understand why they don’t want to and why they think their way of doing things is better than yours.
The South West simulation strategy can be found at http://workforce.southwest.nhs.uk/simulation/
Alex MillsSpecialist Registrar, Derriford Hospital, Plymouth
References1. Safer Medical Practice: Machines, Manikins and Polo Mints.
CMO annual report 2008-2009. http://www.bmsc.co.uk/pdf/DH-096227.pdf (accessed 25/03/2014)
2. A Framework for Technology Enhanced Learning. London: Department of Health, 2011. https://www.gov.uk/government/publications/a-framework-for-technology-enhanced-learning (accessed 25/03/2014).
3. Kipling R. Selected poem from “The Elephant’s Child” The Ladies Home Journal, April 1900.
4. Glaser BG, Strauss AL. The Discovery of Grounded Theory: Strategies for Qualitative Research. Mill Valley, CA: Sociology Press, 1967.

Anaesthesia News July 2014 • Issue 324 15
A novel approach to exam preparation
E-learning and improved technology such as video calling from smartphones and tablets presents another option for examination practice. Video calling using such applications as Skype and FaceTime provide ideal mediums for this. Outlined below is one method that has been employed to prepare a candidate for the examination, which may encourage a more widespread use of the technique.
Pros
SOE practice via the internet may sound like an easier option than remaining behind after a long day at work and, providing you own the required technology, is cheaper than attending a course. However, this method requires as much dedication as the traditional route. Ground rules must be in place to ensure maximum benefit and minimise non-work chat! If done effectively the online viva sessions can be productive for both involved.
set-up and format
Both parties require access to an internet connection and video calling technology. Transmitted images must include the candidate’s upper body to allow assessment of both verbal and non-verbal communication. For example, fidgeting hands are as much as a distraction during online practice as they are in real life.
The technique requires an agreed format. An example would be breaking the session into sections, separating the clinical and science aspects of the exam.
There are a few hurdles compared to a face-to-face technique. For the clinical part of the exam, information (including clinical material) needs to be emailed to the candidate at the start of the session and 10 minutes allocated for its assimilation. After this assimilation time, questioning can begin in the same format as in the exam (20 minutes of clinical material questions followed by 20 minutes of clinical anaesthesia questions unrelated to the material provided). The examiner must be prepared. Questions are pre-printed with the answers included. This enables marking whilst the candidate speaks, maintenance of eye contact during questioning and evaluation of non-verbal communication. The clinical science portion is divided into two sections of 15 minutes. Each section covers two questions on the application of basic science to anaesthesia, intensive care medicine and pain management. Again pre-printed question sheets containing the answer points are invaluable here.
A feedback debriefing session is taken at the end of each component rather than ploughing on through all questions,
as ability to retain suggestions and tips diminishes if delivered in one large chunk at the end of the session.
limitations
One limitation is the reliability of internet connectivity but the advent of more capable broadband will alleviate this. Candidates may wish to draw diagrams to illustrate a point and time can be lost holding these up to the camera. This can be overcome by using diagrams annotated with letters, which are part of the prior information emailed to the candidate. This then allows demonstration of understanding by identification of parts of the diagram, without the time-consuming process of drawing and then attempting to show to the examiner.
This technique will not suit everyone, but it presents another option for preparation and is preferable to no practice at all. It can be adapted to fit the formats of other postgraduate bodies, both within the UK and beyond, and may ultimately lead to a faculty of virtual world remote examiners assisting in exam preparation.
rex Kinnear-MellorST5 Anaesthesia, Nottingham City Hospital
The Fellowship of The Royal College of Anaesthetists Final examination has a structured oral examination (SOE) component. Success at this examination requires extensive practice of oral examination technique. Traditionally the preparation for this is done face to face within the hospital or at a specifically designed course.

16 Anaesthesia News July 2014 • Issue 324 Anaesthesia News July 2014 • Issue 324 17
In 2012 two groups of volunteers comprising anaesthetic consultants, trainees and resuscitation officers from Southampton University Hospital travelled to northern Ghana to run the Safe Anaesthesia From Education (SAFE) Obstetric Course. Here we outline the motivation, value and challenges in delivering such a programme.
Ghana has a population of over 24 million and a life expectancy of 57 yrs for males and 64 yrs for females.1 Since independence from colonial rule in 1957, Ghana has demonstrated relatively strong political stability and minimal corruption, making it an excellent environment for exploring how best to improve the general ‘health of a nation’ by addressing healthcare needs. If successful this could provide a model for development in other poor areas of the world.
Whilst Ghana is the third richest African country, northern areas of Ghana remain as impoverished as the poorest areas in the world with 70% of people living on the equivalent of less than $1 per day.2 One of the problems faced by the northern Ghana health service is recruitment and retention of medical staff to these poor areas. Putting this in perspective, the UK has roughly one doctor for every 250 people, compared to one per 27,000 in northern Ghana.3 One of the reasons behind this poor staffing provision lies in the fact that, despite Ghanaian medical graduates being instructed to work for a minimum number of years in pre-selected areas around
the country, the reality differs when these newly qualified doctors find reasons to stay in the more prosperous southern areas. The long-term aspiration is to set up a self-sustaining healthcare training programme which will both improve the health of the local population and act as a strong incentive to those Ghanaian doctors who may have originally come from these regions, but previously have not seen the long-term attraction of staying there.
Currently there is only one anaesthetic doctor in this region, Dr Thomas Anabah (who joined us teaching on the courses), with anaesthetics in the regional hospitals being delivered by nurse anaesthetists. After their initial training these nurse anaesthetists often work completely on their own in isolated areas with few resources in terms of drugs and equipment. Further training is infrequent and, to attend, they usually have to travel 600 km south to the capital Accra, where they will be taught in a lecture theatre with over 400 other students. The SAFE course aims to provide up-to-date learning in small groups with a more hands-on approach.
June 2012 saw the first faculty of anaesthetists from Southampton go out to the northern region to deliver the SAFE course. Lessons learnt from this were put to good use when the second faculty went out 3 months later to run the course again.
The G.A.S. Partnership
The trips were organised in conjunction with the G.A.S. Partnership. This is a collaboration between the Ghana Health Service, Afrikids (a children’s rights NGO charity working with communities across northern Ghana) and staff volunteers from Southampton University Hospital. The G.A.S. Partnership aims to improve medical skills in northern Ghana to provide a lasting impact on health in the region.
SAFE course
The SAFE Obstetric Course has been designed by the AAGBI with support from the World Federation of Societies of Anaesthesiologists and it is hoped it will be delivered by UK healthcare volunteers throughout sub-Saharan Africa and south Asia; prior to our work in Ghana it has already been run in Liberia and Uganda.4 It comprises a generic guide to the teaching methods used and comes ready made with lectures, workshops, discussion groups and teaching sessions for the teaching faculty to run. This follows a similar framework to the Resuscitation Council life support courses which medical staff from the UK will be familiar with. The course covers basic and advanced airway techniques, general and spinal anaesthesia, how to approach setting up an HDU, and management of specific conditions such as pre-eclampsia, haemorrhage and sepsis.
The courses
The faculty set out from Southampton carrying an assortment of adult and neonatal manikins, kindly loaned by Southampton Hospital’s resuscitation department, and a collection of teaching aids ranging from laryngoscopes to bougies and IV fluid bags. After arriving in Accra for a brief overnight stop we flew north to Tamale, a city in the northern region with a rapidly expanding population of over 500,000.
On the first course, 23 nurse anaesthetists from the upper east, upper west and northern regions of Ghana attended, some of whom had travelled incredibly long distances to attend the course, and a further 16 attended in September. The reason for the lower number on the second course was due to transport logistics across water-logged terrain during the rainy season, emphasising some of the difficulties local staff have to contend with on a regular basis.
The courses were taught in the local complex of the nursing and midwifery council. The first evening was spent registering candidates, handing out copies of Obstetric Anaesthesia for Developing Countries,5 which all candidates received, and completing pre-course MCQs. A sub-group undertook a skill station assessment which was repeated at the end of the course. Once this had been completed and the candidates left we continued to set up our teaching rooms ready for the next day. Over the next three days we delivered a series of lectures, small group teaching sessions and discussion groups, and
ran scenarios with manikins. This was a new style of teaching for many of the students but, once the course started, each candidate was immersed in the programme and turned up to each teaching session with impressive enthusiasm; although keeping to schedule with candidates more used to running on ‘Ghanaian time’ was challenging! Teaching was complemented by several videos prepared by AAGBI members, including Dr Ollie Ross from Southampton who joined the second faculty teaching in September. These videos demonstrated how to perform spinal anaesthesia, rapid sequence inductions and how to approach common complications such as a high spinal. On the final day we ran an essay competition with the title ‘What inspired you to be a nurse anaesthetist?’. Many of the stories were deeply moving and showed how tough it is to work in such poorly resourced and demanding environments.
To finish, each candidate repeated the MCQs and a post-course skill station assessment. Almost without exception scores rose significantly. It is hoped that we will be able to evaluate retention of knowledge and skills during subsequent trips to the area. At the end of the course, a few candidates who were felt to have shown the greatest enthusiasm and potential to go back to their respective hospitals and pass on the skills they had learned were offered the opportunity to stay and attend a ‘Training the Trainers’ course following on from SAFE. Here candidates were taught how to prepare and deliver a lecture, demonstrate and teach a skill and run a scenario using a manikin.
The course was very enjoyable and rewarding to teach on and we have rarely seen such eager, enthusiastic and grateful students. Days were often long, with early starts preparing teaching rooms and learning how to cope with challenges such as frequent power cuts leaving us bereft of projection facilities, lighting and much-needed air conditioning. Each evening ended with a faculty meeting (supplemented by an ice cold beer). We were well looked after by the local team and well fed with Ghanaian dishes.
Benefits of teaching on SAFE
We would highly recommend teaching on the SAFE course to other trainees. It is a very different experience to teaching in the UK and you feel like you are really teaching skills and knowledge which will be put to use to save lives and improve care. It’s a great way to get overseas experience with just a week away from the UK and add something a bit different to your CV. We all learnt how to be much more flexible and prepare for any eventuality while running the course and all of the faculty found their teaching skills were
Teaching SAFE
obstetrics in Ghana
Anaesthesia News July 2014 • Issue 324 17

Anaesthesia News July 2014 • Issue 324 19
The Association of Anaesthetists of Great Britain and Ireland invites applications for the 2015 AAGBI Prize for Innovation in Anaesthesia, Critical Care and Pain. This prize is open to all anaesthetists, intensivists and pain specialists based in Great Britain and Ireland. The emphasis is on new ideas contributing to patient safety, high quality clinical care and improvements in the working environment. The entries will be judged by a panel of experts in respective fields.
Applicants should complete the application form that can be found on the AAGBI website www.aagbi.org/research/innovation.
The closing date for applications is Tuesday 30 September 2014.
Three prizes will be awarded and the winners will be invited to present their work and collect their prizes at the Winter Scientific Meeting in London on 16 January 2015.
INNOVATIONAAGBI
The Annual AAGBI Prize for Innovation in Anaesthesia, Critical Care and Pain
www.aagbi.org/research/innovation Kindly sponsored by:
C
M
Y
CM
MY
CY
CMY
K
InnovationHalf2014.pdf 1 05/06/2014 14:41
tested as we learnt to adapt and overcome the various problems associated with running a course in a new environment. And never underestimate the value of a bag of sweets in ensuring your candidates turn up to your teaching session on time!
We were very fortunate and grateful to benefit from funding from the AAGBI, the Tropical Health and Education Trust and the G.A.S. Partnership, which kept costs relatively low. We are also indebted to Dr Alison Carling from Newport who joined us and prepared us well for our first course having previously taught SAFE in Uganda and Liberia. It is hoped that staff from Southampton will return to Ghana to deliver the SAFE course again and improve training for more nurse anaesthetists in the region.
dr Paul stevens dr laura Tarry Specialist Registrars, University Hospital Southampton
dr Malvena stuart-TaylorConsultant Anaesthetist, University Hospital Southampton
References1. http://www.who.int/countries/gha/en/2. http://www.oxfam.org/en/ghana3. http://www.gaspartnership.org/4. http://www.aagbi.org/sites/default/files/Report%20of%20
Uganda%20Safe%20Course%20June-%20July%202011.pdf5. Clyburn P, Collis R, Harries S, eds. Obstetric Anaesthesia
for Developing Countries. Oxford: OUP, 2010. Also available at http://oxfordmedicine.com/view/10.1093/med/9780199572144.001.0001/med-9780199572144 (accessed 3/4/2014).
SAFIRA is a new device for regional anaesthesia, invented by Dr Emad Fawzy, Dr Peter Young and Dr John Gibson (Consultant Anaesthetists, Queen Elizabeth Hospital, Kings Lynn) and Dr Joseph Carter (Consultant Anaesthetist, York Teaching Hospital, York).
SAFIRA is a new device allowing anaesthetists to safely perform nerve blockade single-handed. It is a safe single user regional anaesthetic injection system controlled by buttons attached to the hub of the regional anaesthetic needle. SAFIRA enables precise speed, time, pressure and volume control of the injectate and is designed to minimise the risk of intraneural injection and so nerve injury, and allows you to record the whole anaesthetic injection procedure.
Due to confidentiality, only basic features can be disclosed; however there are five intellectual property applications so far.
SAFIRA has been developed as a NHS innovation device and is managed by Health Enterprise East (NHS innovation agency) and was awarded the NHS Innovation Award for Best Medical Technology 2013 by Health Enterprise East, and also the AAGBI Innovation Award 2014 at WSM London 2014.
Winning the AAGBI award was invaluable for the SAFIRA project as it added huge value and credit to SAFIRA. After winning such a prestigious award we received huge interest from different groups of investors and major companies in the field of regional anaesthesia. The AAGBI award represents the recognition of the potential of SAFIRA from a panel of world experts acknowledged as one of the most prestigious organisations in the field of anaesthesia and this was fully appreciated by the various investment groups who approached us.
Winning this award has raised awareness among anaesthetists about the importance of inventions and promoting the culture of innovation. Following on from WSM 2014, I received many calls from anaesthetists across the UK who had bright ideas but required guidance on how to take their ideas forward. After winning the
AAGBI Innovation Award, we received an offer from an investment group to fund the SAFIRA project over the next two years and build a prototype up to the required standards. We have built three prototypes so far, and are currently planning to build a prototype up to the standard of FDA and CE marking. We expect to have this prototype ready by the end of this year, when we will start our first animal and cadaveric studies.
We aim to start out first patient study in early 2015 and, by the end of 2015, SAFIRA should be ready to be marketed.
dr emad fawzyConsultant Anaesthetists, Queen Elizabeth Hospital, Kings Lynn
SAFIRA – Safe Injection System for Regional Anaesthesia
It is with great excitement and anticipation that we launch our fourth annual AAGBI Innovation in Anaesthesia, Critical Care and Pain Award. We are looking forward to receiving new entries in this ever more popular competition.
The previous winners were: a new, safe intravenous fluids drip chamber; a universal, portable EtCO2 monitor and an infusion pump to aid performance of ultrasound guided regional anaesthesia. All these winning entries will potentially enhance patient safety.
Throughout our medical careers we are all inventors and innovators to some degree, sometimes we do not even notice it. The old cliché, ‘necessity is the mother of invention’, still stands and you can try to apply it in your everyday hospital setting. It is often something that repeatedly does not function or perform as it should, as far as equipment or techniques are concerned and you may find new, better solutions. The same applies to our everyday IT issues. The road to success with a new idea is not easy: as part of the AAGBI
innovation initiative we hope to be able to offer useful advice to help new innovators, for instance through sessions at the main conferences and future seminars at the AAGBI.
Apart from well established, already on the market products, well described techniques and well known IT solutions, we welcome new innovations at various stages of development where winning the award can financially and otherwise enhance progress of the project. Please make sure that you have the necessary intellectual property protection, if applicable, before you enter the competition.
So please fill in your award application form today! We are looking forward to receiving your entry!
For more information visit www.aagbi.org/research/innovation
dr J Bernard libanAAGBI Innovation Lead
2015 AAGBI Innovation in Anaesthesia, Critical Care and Pain Award
10TH NOVEMBER 2014LONDON
Association
The Preoperative
NATIONAL CONFERENCE
ROYA
L COL
LEGE
OF PH
YSICI
ANS
ACCREDITED WITH 5 CEPD POINTS
Fit-4-Surgery: Exercise Interventions & Patient Outcome / Assessment of Patients with Neurological Conditions / Training Standards for Nurses / Preoperative Scoring Systems / Prevention of Thromboembolism / Enhanced Recovery 5 Years On / Latest Guidelines on Anaemia
Open to all healthcare professionals involved in the preoperative assessment of the surgical patient. For full details and to book your place, please contact us:
TOPICS TO INCLUDE:
ABSTRACT FOR PRESENTATIONS OR POSTERS TO BE SUBMITTED BY 30TH SEPTEMBER 2014
W: WWW.PRE-OP.ORG / T: 020 7631 8896

20 Anaesthesia News July 2014 • Issue 324 Anaesthesia News July 2014 • Issue 324 21
less Than full Time (lTfT) training, part-time, flexible training: call it what you will, but training lTfT, and part-time working generally, is becoming increasingly common as work-life balance expectations increase.
Anaesthesia has a strong track record in supporting lTfT training and the royal college of Anaesthetists (rcoA), supported by the AAGBi, is hosting a second National lTfT day, ’Making Part-Time work’, on 9th october 2014. This meeting will address the practical issues encountered by lTfT trainees and those involved with administering it. here we debunk some of the myths, and explain how to negotiate some of the pitfalls.
Less Than Full Time training demystified
Anaesthesia News July 2014 • Issue 324 21 20 Anaesthesia News July 2014 • Issue 324
Less Than Full Time (LTFT) training: even the title feels something of a mouthful. However, it’s nothing compared with actually navigating the complexity of training LTFT. The way it’s administered varies between regions; there are multiple different models; no two trainees work the same pattern of hours; and the scope for wrangles over pay, ‘days off’, on-call cover, and indeed almost any other aspect of working life seems endless.
There is no doubt that LTFT training, badly managed, can cause headaches for all concerned. However, like any employer, the NHS has a clear interest in retaining employees; furthermore, the NHS has an obligation to taxpayers, whose taxes fund medical school and postgraduate training, to get value for money from its investment in medical training. Offering flexible employment allows several trainees, who might be unable or unwilling to work full-time, to continue their training and subsequent careers. This is clearly preferable to losing a proportion of trainees who might otherwise provide decades of service.
The key to making LTFT work, for employee and employer, is communication, understanding and flexibility. The overall goal is twofold: for the trainee, to allow them to fulfil commitments outside work without compromising their training; for the employing trust, to fulfil their obligations to provide rigorous training and an adequately staffed anaesthesia service. A successful arrangement relies on a reasonable degree of cooperation and flexibility on both sides, while also being clear about any stipulations that are effectively non-negotiable (such as needing to look after your children on a set day every week).
If all this sounds scary and confusing, fret not – most LTFT arrangements work satisfactorily for both parties in the end – and rest assured that the whole purpose of October’s ‘Making Part-Time Work’ symposium is to address the challenges encountered when organising LTFT training. Until then we offer some general tips from the viewpoint of both trainee and ‘trainer’ (employing trust, Educational Supervisor, Training Programme Director) for ensuring a successful LTFT working arrangement and avoiding potential difficulties.
Tips for trainees
Organisation and communication are vital. It is important that you apply for LTFT training as far in advance as possible as approval may take up to three months. The application process involves several steps but there will be many people who can help to guide you through it. LTFT colleagues will be very knowledgeable around arrangements locally and an excellent resource having already negotiated the process. Many schools will also have a LTFT advisor who can support you. Speak to your Training Programme Director about your plans early to make sure they’re in agreement; then get the paperwork signed by the right people (medical HR and finance director at your employing trust), and finally return it to your deanery.
If your reasons for wishing to train LTFT are health-related it may be that this process can be expedited. Occupational Health, as well as providing support and advice, will be able to make recommendations to support your application for a change to your working pattern. In addition some schools have a Training Programme Director whose role is specifically to support trainees with differing needs.
You should also contact the relevant people (the anaesthetics secretary, the rota writer, the College Tutor) in advance at the hospital where you’ll be working to let them know your specific LTFT requirements and make sure they can accommodate them. You don’t want to discover a week before you start that they can’t let you have every Friday off for childcare, and you won’t win friends by presuming that your specific LTFT needs are common knowledge.
In addition to local support, the AAGBI,1 the RCoA2 and the British Medical Association3 all have LTFT resources available online and the RCoA has a Bernard Johnson Advisor with responsibility for LTFT training who can be contacted for advice. The GAT Handbook 2013-144 has chapters on ‘LTFT Training’, ‘Returning to Practice’ and ‘The Pregnant Anaesthetist’, while the GAT (and RCoA) websites host an A to Z Guide to LTFT Training in Anaesthesia.5 These explain more about the practicalities and logistics of training part-time such as eligibility criteria, pay and banding and working patterns and include a comprehensive list of useful references.
Finally, once you’ve started LTFT, be vigilant about keeping on top of workplace-based assessments (WPBAs), the requirements of the curriculum and what you need to get signed off. Annual review of competency progressions are generally untidy affairs because you’ll often be part-way through (rather than at the end of) a specific ‘ST’ year. However they’ll be a whole lot less tidy if you discover belatedly that you haven’t got the requisite documentary evidence to get signed off for the competencies or completed stages of training that you were expecting.
Tips for trainers
Find out about any LTFT trainees rotating through your hospital well in advance. This is particularly important for rota writers, who clearly need to know what percentage of whole-time equivalent trainees are expecting to work and which days they can’t. It’s also important for College Tutors to ensure that LTFT trainees are actually working the correct number of hours for the proportion of whole-time equivalent training they’ve had approved. This may need some planning if your department hasn’t had LTFT trainees before (or if you’ve got more LTFT trainees than usual, or two trainees wanting the same day off, etc.)
For Educational Supervisors, College Tutors and others with responsibility for achievement of training objectives, be aware that arranging meetings with LTFT trainees may require considerable forward planning, for the simple reason that they’re at work less often. Try to meet your LTFT trainee as early in their placement as possible to agree educational objectives; then try to touch base regularly to check that they’re managing to complete the requisite WPBAs, getting the lists they need, and making progress with any other objectives you agreed on (exams, audits etc.). LTFT trainees will need longer training blocks to achieve equivalent training and this should be factored in when planning rotations.
Also, do bear in mind that LTFT trainees may be slower to find their feet in a new department. Longer rotational placements, e.g. a year rather than 6 months, will allow them time to orientate themselves and then make the most of all the opportunities a department has to offer. They may be less confident in their practical skills, or more likely to be overwhelmed by stressors outside the workplace, especially when returning from a period of absence. Both the Academy of Medical Royal Colleges6 and the RCoA7 have issued updated guidance on how to manage a successful return to work and these should be used to develop a personalised return to practice plan
for each trainee. As with all trainees, any effort on behalf of the department and its permanent staff to make new trainees feel welcome and help them settle in is usually greatly appreciated.
Making the most of LTFT training
If this appears more like a scrutiny of the things that can go wrong with LTFT training than a celebration of the opportunities and advantages it can bring, we sincerely apologise and let us reiterate that, in the vast majority of cases, it works to the mutual benefit of all. To find out more on how to make the most of LTFT join us at the ‘Making Part-Time Work’ symposium. As well as sessions on the practicalities of training part-time there will be a series of workshops, tailored to both trainees and trainers, exploring the opportunities LTFT presents and what to do when things aren’t going quite as expected. The General Medical Council has recommended that doctors seek out a trained mentor at times of change8 and one of the workshops will focus on the role of mentoring in helping you make the most of the opportunities, and negotiate the dilemmas, that part-time training presents.
You can find the meeting programme and registration details at http://www.rcoa.ac.uk/education-and-events/making-part-time-work-2014-%E2%80%93-the-2nd-national-ltft-day. We look forward to seeing you there.
dr oliver Boney ST5, London Deanery
dr sarah GibbSpR5, Northern Deanery
References1. Association of Anaesthetists of Great Britain and Ireland. Less Than
Full Time (LTFT) Training. www.aagbi.org/professionals/trainees/training-issues/ltft-training
2. Royal College of Anaesthetists. Less than Fulltime training (LTFT). www.rcoa.ac.uk/training-and-the-training-programme/less-fulltime-training-ltft
3. British Medical Association. Guide to flexible training. bma.org.uk/developing-your-career/foundation-training/flexible-training
4. Association of Anaesthetists of Great Britain and Ireland. The GAT Handbook 2013-2014. www.aagbi.org/sites/default/files/GAT%20Handbook%20Web.pdf
5. Gibb S, Carey S. Less than Full Time Training in Anaesthesia: An A to Z Guide, March 2013. www.aagbi.org/sites/default/files/A%20to%20Z%20Guide%20to%20LTFT%20%20Anaesthetic%20Training%20March%202013%20%282%29.pdf
6. Academy of the Medical Royal Colleges. Return to Practice Guidance, April 2012. www.aomrc.org.uk/doc_details/9486-return-to-practice-guidance
7. Royal College of Anaesthetists. Returning to Work After a Period of Absence, May 2012. www.rcoa.ac.uk/system/files/PUB-ReturnToWork2012.pdf
8. General Medical Council. Good Medical Practice, March 2013. http://www.gmc-uk.org/static/documents/content/Good_medical_practice_-_English_0414.pdf

Anaesthesia News July 2014 • Issue 324 23
July 2014
Digested
N.B. the articles referred to can be found either in a print issue or on Early View (ePub ahead of print)
A prospective randomised comparison of two insertion methods for i-gelTM placement in anaesthetised paralysed patients: standard vs rotational techniqueKim HC, Yoo DH, Kim HJ, Jeon YT, Hwang JW, Park HP
A randomised comparison of free-handed vs air-QTM assisted fibreoptic-guided tracheal intubation in children <2 years of ageSohn LE, Jagannathan N, Sequera-Ramos L, Sawardekar A, Schaldenbrand K, De Oliveira GS
The July edition of Anaesthesia includes a number of articles regarding the airway. Two of these specifically explore insertion techniques of airway devices. Anaesthetics is often described as a ‘craft’ specialty. Occasionally the choice of anaesthetic technique is based on personal experience, an ‘it is safe in my hands’ approach. These two articles help suggest how an evidence base could be used to influence the choices made in performing specific tasks, whilst acknowledging a study only gives us part of the answer to this difficult question.
Helen Laycock Editor, Anaesthesia
To rotate or not to rotate, that is the question? The i-gel is a commonly used supraglottic airway device. Unfortunately multiple insertion attempts can lead to airway trauma and the incidence of failure with insertion on first attempt is reported as anywhere between 7% and 22%. This failure is mostly a consequence of impaction at the back of the mouth by tongue folding. Previous work from this group showed a higher success rate for first insertion with ProSealTM laryngeal mask airways when using a rotational technique. Here the authors evaluate the efficacy of this technique for i-gel insertion.
One hundred and eighty-one paralysed patients were randomly allocated to receive i-gel insertion by either the standard or rotational technique following induction of general anaesthesia. The rotational technique showed a higher success rate and shorter time of insertion on first attempt. In addition it was associated with a better airway seal and less airway trauma to the patient. In this regard the evidence suggests the rotation technique for i-gel placement may improve specific insertion outcomes.
The second paper on airway insertion techniques investigates whether using a specific supraglottic airway device, the Air-Q, as a conduit shortens the time to fibreoptic-guided tracheal intubation compared with the traditional free-hand fibreoptic technique in both experienced and inexperienced operators. Whilst fibreoptic-guided tracheal intubation is an important skill, some practising anaesthetists report limited experience and it is likely that this proportion is increased in those confident using this technique in the paediatric population. Therefore any method to improve success, especially in the inexperienced, seems useful to evaluate.
This prospective randomised study looked at 80 healthy children with normal airways, aged between 1 month and 24 months, undergoing elective surgery that required tracheal intubation. They were randomised into four groups depending on operator experience and whether a free-handed or Air-Q assisted fibreoptic-guided tracheal intubation occurred. No
differences were observed between groups for time to tracheal intubation, number of attempts, manoeuvres required for tracheal tube passage or complication rates. The Air-Q group did require fewer manoeuvres to obtain an adequate laryngeal view. Fibreoptic-guided tracheal intubation times were similar with or without the Air-Q, irrespective of the operator’s experience. Therefore, based on this study, should everyone use a free-hand approach? The authors suggest that, in deciding on insertion technique, there may be possible advantages with the Air-Q that were not evaluated, such as help with scope positioning, relieving upper airway obstruction and allowing continuous oxygenation during fibreoptic-guided tracheal intubation. In this regard the evidence of no difference is useful; however, when considering individual patients, certain circumstances exist where it seems likely the Air-Q would appear to be helpful.
ACTA SHEFFIELD Association of Cardiothoracic Anaesthetists
Core Topics Day andAutumn MeetingMercure Sheffield St Paul’s Hotel and Spa13th - 14th November 2014www.actasheffield2014.co.ukAbstracts for oral/poster presentationto be submitted by 5th September 2014
Confirmed Faculty includes:
Dr Conn Russell, Belfast
Prof Justiaan Swanevelder, Cape Town
Lt Col Michael Butler, TruroDr Jean-Pierre van Besouw, London
Prof Martin Cowie, LondonDr Tomas Drabek, Pittsburgh
Prof Gebrine El Khoury, BrusselsDr Michel van Dyck, Brussels
For all enquiries please contact Jane Heppenstall on 0114 2455423 or email [email protected] Early bird registration closes 10th October 2014
Topics include:Teams and conflict: lessons from the militaryThe 'NICE' way to manage rib fracturesExtracorporeal CPR in traumatic cardiac arrestTTE in ICU: friend or foe?New frontiers in heart failure managementExercise and the heartReversal of old and new anticoagulantsMinimal access mitral valve repair
@actasheffield
Second announcement_Layout 1 12/03/2014 13:24 Page 1
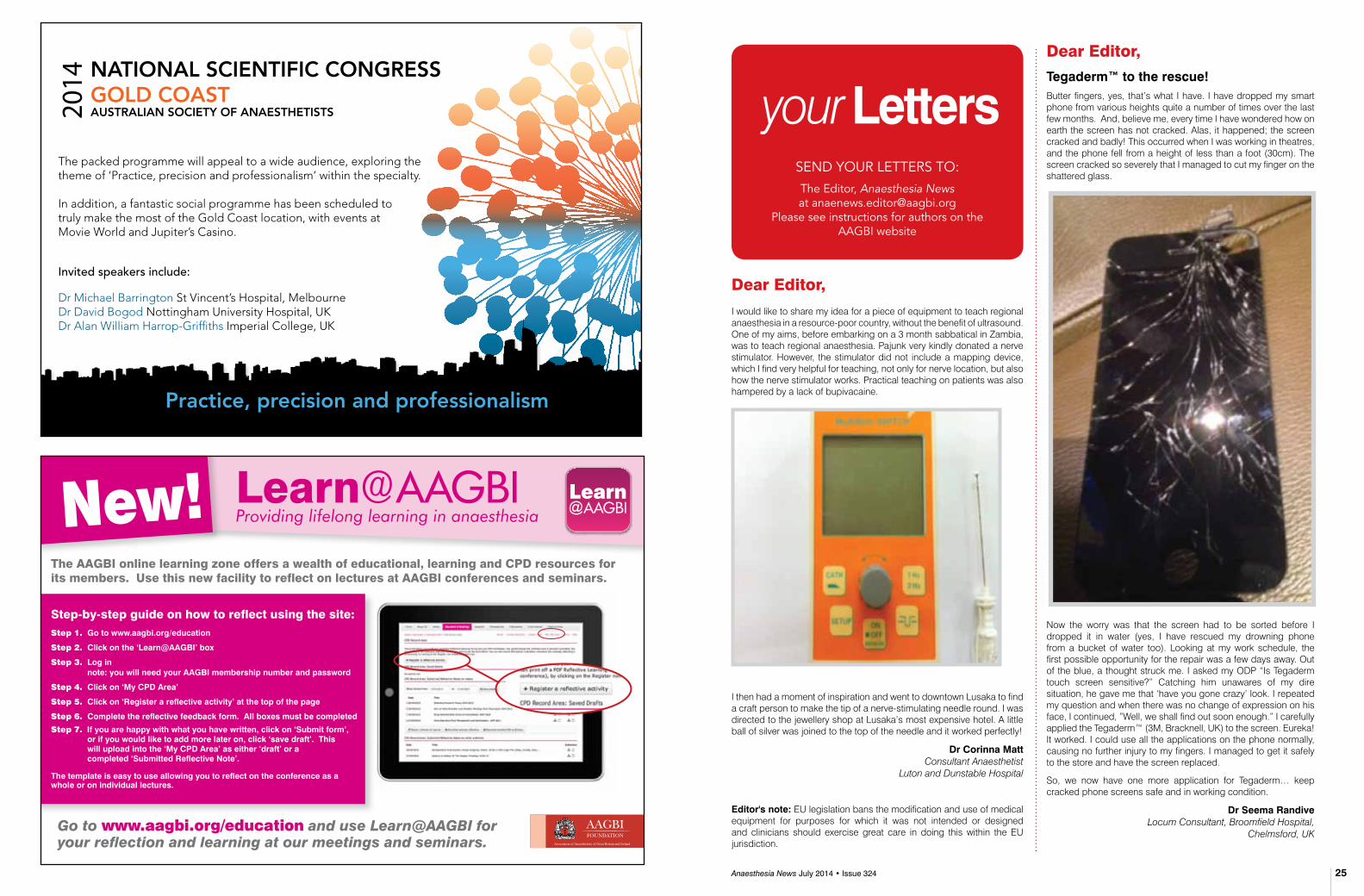
Anaesthesia News July 2014 • Issue 324 25
Learn@AAGBI The AAGBI online learning zone offers a wealth of educational, learning and CPD resources for its members. Use this new facility to reflect on lectures at AAGBI conferences and seminars.
New!
Step-by-step guide on how to reflect using the site:Step 1. Go to www.aagbi.org/education
Step 2. click on the ‘learn@AAGBi’ box
Step 3. log in note: you will need your AAGBi membership number and password
Step 4. click on ‘My cPd Area’
Step 5. click on ‘register a reflective activity’ at the top of the page
Step 6. complete the reflective feedback form. All boxes must be completed
Step 7. if you are happy with what you have written, click on ‘submit form’, or if you would like to add more later on, click ‘save draft’. This will upload into the ‘My cPd Area’ as either ‘draft’ or a completed ‘submitted reflective Note’.
The template is easy to use allowing you to reflect on the conference as a whole or on individual lectures.
Go to www.aagbi.org/education and use Learn@AAGBI for your reflection and learning at our meetings and seminars.
your lettersSEND YOUR LETTERS TO:
The Editor, Anaesthesia News at [email protected]
Please see instructions for authors on the AAGBI website
Dear Editor,
Tegaderm™ to the rescue!Butter fingers, yes, that’s what I have. I have dropped my smart phone from various heights quite a number of times over the last few months. And, believe me, every time I have wondered how on earth the screen has not cracked. Alas, it happened; the screen cracked and badly! This occurred when I was working in theatres, and the phone fell from a height of less than a foot (30cm). The screen cracked so severely that I managed to cut my finger on the shattered glass.
Now the worry was that the screen had to be sorted before I dropped it in water (yes, I have rescued my drowning phone from a bucket of water too). Looking at my work schedule, the first possible opportunity for the repair was a few days away. Out of the blue, a thought struck me. I asked my ODP “Is Tegaderm touch screen sensitive?” Catching him unawares of my dire situation, he gave me that ‘have you gone crazy’ look. I repeated my question and when there was no change of expression on his face, I continued, ”Well, we shall find out soon enough.” I carefully applied the Tegaderm™ (3M, Bracknell, UK) to the screen. Eureka! It worked. I could use all the applications on the phone normally, causing no further injury to my fingers. I managed to get it safely to the store and have the screen replaced.
So, we now have one more application for Tegaderm… keep cracked phone screens safe and in working condition.
dr seema randive Locum Consultant, Broomfield Hospital,
Chelmsford, UK
Dear Editor,
I would like to share my idea for a piece of equipment to teach regional anaesthesia in a resource-poor country, without the benefit of ultrasound. One of my aims, before embarking on a 3 month sabbatical in Zambia, was to teach regional anaesthesia. Pajunk very kindly donated a nerve stimulator. However, the stimulator did not include a mapping device, which I find very helpful for teaching, not only for nerve location, but also how the nerve stimulator works. Practical teaching on patients was also hampered by a lack of bupivacaine.
I then had a moment of inspiration and went to downtown Lusaka to find a craft person to make the tip of a nerve-stimulating needle round. I was directed to the jewellery shop at Lusaka’s most expensive hotel. A little ball of silver was joined to the top of the needle and it worked perfectly!
dr corinna Matt Consultant Anaesthetist
Luton and Dunstable Hospital
editor's note: EU legislation bans the modification and use of medical equipment for purposes for which it was not intended or designed and clinicians should exercise great care in doing this within the EU jurisdiction.
The packed programme will appeal to a wide audience, exploring the theme of ‘Practice, precision and professionalism’ within the specialty.
In addition, a fantastic social programme has been scheduled to truly make the most of the Gold Coast location, with events at Movie World and Jupiter’s Casino.
Invited speakers include:
Dr Michael Barrington St Vincent’s Hospital, Melbourne Dr David Bogod Nottingham University Hospital, UK Dr Alan William Harrop-Griffiths Imperial College, UK
Practice, precision and professionalism
NATIONAL SCIENTIFIC CONGRESSGOLD COASTAUSTRALIAN SOCIETY OF ANAESTHETISTS

You are invited to submit an abstract for poster presentation at WSM London in January 2015. The deadline for submission is 23:59 on Monday 01 September 2014 and further instructions and information can be found on our WSM microsite: www.wsmlondon.org
After the deadline, a preliminary review of the abstracts received will determine which ones are accepted for poster presentation.
All accepted abstracts will be published in Anaesthesia in the form of a fully referenceable online supplement (NB Editor-in-Chief reserves the right to refuse publication, e.g. where there are major concerns over ethics and/or content).
Authors of the best poster(s) will be awarded ‘Editors’ Prizes’.
If you have any queries, please contact the AAGBI Secretariat on 020 7631 1650 (option 3) or [email protected]
ABSTRACTS FOR PRESENTATION AT AAGBI WSM LONDON 2015
South West
Regional Anaesth
esia Course
31st October
- 1st November 2011
Royal Devon
& Exeter Hospita
l, Exeter
• P
opular 2 day course with experienced f
South West Regional Anaesthesia Course
31st October - 1st November 2011 Royal Devon & Exeter Hospital, Exeter
• Popular 2 day course with experienced faculty
• Upper, lower limb and abdominal blocks
• Ultrasound & landmark techniques
• Scanning and needling practice
• Video demonstrations
• Lectures and workshops
• Aimed at anaesthetists in training
Cost: £205 Register early – strictly limited to 30 participants For details & online registration visit: www.sowra.org.uk Or email: [email protected]
• Popular2daycoursewithexperiencedfaculty
• Ultrasoundguidanceforupper&lowerlimb,abdominalandneuroaxialblocks
• Sonoanatomyandscanningpracticeonlivemodels
• Lecturesandworkshops
• Needlingpracticeandcompetencyassessment
• Suitableforallgrades
SouthWestRegionalAnaesthesia
Registration Fee: £280 (10% Discount ESRA members)
Register early – strictly limited to 24 participants to ensure ratios
10 CPD points applied for – counts towards ESRA Diploma
For details & online registration visit: www.sowra.org.uk Or email: [email protected]
6th&7thNovember2014DerrifordHospital,Plymouth
EVELYN BAKER MEDAL
The Evelyn Baker award was instigated by Dr Margaret Branthwaite in 1998, dedicated to the memory of one of her former patients at the Royal Brompton Hospital. The award is made for outstanding clinical competence, recognising the ‘unsung heroes’ of clinical anaesthesia and related practice. The defining characteristics of clinical competence are deemed to be technical proficiency, consistently reliable clinical judgement and wisdom and skill in communicating with patients, their relatives and colleagues. The ability to train and enthuse trainee colleagues is seen as an integral part of communication skill, extending beyond formal teaching of academic presentation. Nominees should normally still be in clinical practice.
Dr John Cole (Sheffield) was the first winner of the Evelyn Baker medal in 1998, followed by Dr Meena Choksi (Pontypridd) in 1999, Dr Neil Schofield (Oxford) in 2000, Dr Brian Steer (Eastbourne) in 2001, Dr Mark Crosse (Southampton) in 2002, Dr Paul Monks (London) in 2003, Dr Margo Lewis (Birmingham) in 2004, Dr Douglas Turner (Leicester) in 2005, Dr Martin Coates (Plymouth) in 2006, Dr Gareth Charlton (Southampton) in 2007, Dr Neville Robinson (London) in 2008, Dr Fred Roberts (Exeter) in 2009, Dr Sudheer Medakkar (Torquay) in 2010, Dr Keith Clayton (Coventry) in 2011, Dr John Windsor (London) in 2012, and Drs Amanda Blackburn (Rotherham), Michael Donaldson (Hull), Andrew Kilner (Newcastle) and Chris Vallis (Newcastle) in 2013.
Nominations are now invited for the award, which will be presented at WSM London in January 2015. Members of the AAGBI can nominate any practising anaesthetist who is also a member of the Association. Examples of successful previous nominations are available on request. Nominations should include an indication that the nominee has broad support within their department.
The nomination, accompanied by a citation of up to 1000 words, should be sent to the Honorary Secretary at [email protected] by 17:00 on Monday 22 September 2014
AN AWARD FOR OUTSTANDING CLINICAL COMPETENCE
17th Anaesthesia, Critical Care and Pain Forum
www.doctorsupdates.com
Da Balaia, The AlgarvePortugal
29 September -2 October 2014

Par
ticl
es
Anaesthesia News July 2014 • Issue 324 29 28 Anaesthesia News July 2014 • Issue 324
Botto on behalf of the Vascular events In noncardiac Surgery patIents cOhort evaluatioN (VISION) Writing Group
Myocardial injury after noncardiac surgery: a large, international, prospective cohort study establishing diagnostic criteria, characteristics, predictors, and 30-day outcomesAnesthesiology 2014; 120: 564-578
BackgroundMyocardial ischaemia is a frequent cause of death within 30 days of non-cardiac surgery.1 Minor postoperative increases in serum troponin levels have, in the past, been dismissed as less relevant cases of supply/demand mismatch. Emerging evidence2,3 suggests many patients sustain myocardial injury in the peri-operative period, which does not satisfy the diagnostic criteria for myocardial infarction.4 This shows that a new diagnosis of myocardial injury after non-cardiac surgery (MINS) may be useful to clinicians. MINS was defined in this paper as prognostically relevant myocardial injury due to ischaemia (that may or may not result in necrosis), which occurs during or within 30 days after non-cardiac surgery.
MethodsInvestigators prospectively looked at a cohort of 15,065 patients aged 45 or older who underwent inpatient (elective and emergency) non-cardiac surgery (under GA and/or RA) and had troponin T measured during the first 3 postoperative days. Patients with a troponin T level of ≥0.04ng/ml (elevated ‘abnormal’ laboratory threshold) were assessed for ischaemic features i.e. ischaemic symptoms and ECG findings. Patients not requiring an overnight stay, lacking postoperative troponin T measurement or judged as having a non-ischaemic cause for the troponin elevation (e.g. sepsis, pulmonary embolus, cardioversion) were excluded. The authors used regression analysis to validate a cut-off value for TnT of ≥0.03ng/ml to define myocardial injury after non-cardiac surgery. The primary outcome measure was 30 day mortality after surgery.
resultMINS (irrespective of the presence of an ischaemic feature) was an independent predictor of 30-day mortality (adjusted hazard ratio 3.87; 95% CI 2.96–5.08). It also had the highest population attributable risk (34.0%, 95% CI 26.6-41.5) of the peri-operative complications. A total of 1,200 patients (8.0%; 95% CI 7.5-8.4) suffered MINS, and 58.2% of these patients would not have fulfilled the universal definition of myocardial infarction, 1 in 13 died within 30 days. Only 15.8% of patients with MINS experienced an ischaemic symptom.
discussionFour peri-operative complications - MINS, sepsis, stroke, and pulmonary embolus - were independent predictors of 30-day mortality. Failure to monitor troponin measurements after non-cardiac surgery will result in missing more than 80% of MINS events. Age ≥75, cardiovascular risk factors, known cardiovascular disease and surgical factors (urgent/emergency surgery) were all independent predictors of MINS. Patients with MINS were at higher risk of nonfatal cardiac arrest, congestive heart failure and stroke compared with patients who did not suffer MINS. An estimated 8 million adults worldwide may suffer MINS annually, which highlights the need to prevent and treat this important condition.
Marcin PachuckiST4 Bristol School of Anaesthesia
References1. Pearse RM Moreno RP, Bauer P, et al. Mortality after surgery in Europe: a
7 day cohort study. Lancet 2012; 380: 1059-65.2. Ali ZA, Callaghan CJ, Ali AA, et al. Perioperative myocardial injury after
elective open abdominal aortic aneurysm repair predicts outcome. Eur J Vasc Endovasc Surg 2008; 35: 413-9.
3. VISION Study Investigators, Devereaux PJ, Chan MT, et al. Association between postoperative troponin levels and 30-day mortality among patients undergoing noncardiac surgery. JAMA 2012; 307: 2295-304.
4. Thygesen K. Alpert JS, Jaffe AS, et al. Third universal definition of myocardial infarction. Circulation 2012; 126: 2020-35.
Hillyard S, Cowman S, Ramasundaram R, Seed PT, O’Sullivan G
does adding milk to tea delay gastric emptying?British Journal of Anaesthesia 2014; 112: 66-71
BackgroundTo minimise the risk of aspiration of gastric contents during anaesthesia, patients are fasted prior to surgery.1 Standard guidelines suggest clear liquids are permitted until 2 hours pre-operatively but that milk should be regarded as similar to solid foods, obeying a 6 hour interval.2 However there is very little evidence to support this. This study attempts to establish whether the addition of a modest volume of milk to tea results in delayed gastric emptying.
MethodsTen healthy volunteers were entered into this randomised controlled crossover trial. Participants with a predisposition to delayed gastric emptying such as diabetes were excluded. Gastric emptying was determined by the paracetamol absorption technique and by serial real time ultrasound measurements of the gastric antral cross-sectional area.
Participants were fasted prior to the study. Each participant then took part in both arms of the trial, and drank black tea with milk (250ml tea with 50ml full fat milk) or without milk (300ml black tea), followed by 1.5g of dispersible paracetamol dissolved in 30ml of water. Paracetamol is absorbed almost exclusively from the small intestine and its rate of appearance in the systemic circulation is accepted as being indicative of the rate of gastric emptying.
Venous blood sampling and ultrasound measurements were performed at baseline, every 10 minutes for the first 60 minutes and then every 30 minutes until 150 minutes.
resultsMean plasma paracetamol concentrations plotted against time showed little difference in gastric emptying regardless of whether milk was added. In fact the study showed the mean difference in time to reach peak paracetamol concentration (tmax) was -8 min (95% confidence interval -23.1 to 7), in favour of tea with milk.
The difference in gastric emptying times as assessed using ultrasound was not significant either. The geometric mean T1/2 after drinking tea with and without milk was 23.6 minutes and 22.7 minutes respectively. In addition, at 60 minutes, measurements show the stomach had returned to a pre-drink size.
discussionThe study showed that a moderate volume of milk in tea or coffee does not delay gastric emptying. Its limitations are that it is a very small study and involves only healthy volunteers. Further studies are required to investigate this in surgical patients. The results of this study suggest that current fasting guidelines could be modified to allow the addition of milk to tea and coffee. This would improve cancellation rates and increase patient comfort.
dr N Patel and dr K shelleyGloucestershire Hospitals' NHS Foundation Trust
References1. Mendelson CL. The aspiration of stomach contents into the lungs during
obstetric anaesthesia. Am J Obstet Gynecol 1946; 52; 191-205.2. American Society of Anesthesiologists Committee. Practice guidelines
for preoperative fasting and the use of pharmacologic agents to reduce the risk of pulmonary aspiration: application to healthy patients undergoing elective procedures: an updated report by the American Society of Anesthesiologists Committee on Standards and Practice Parameters. Anesthesiology 2011; 114: 495–511.
Garry DA, McKechnie SR, Culliford DJ et al.
A prospective multi-centre observational study of adverse iatrogenic events and substandard care preceding intensive care unit admission (PreVeNT)Anaesthesia 2014; 16: 137-142
introductionIatrogenic events are those adverse clinical events caused by medical professionals and not related to underlying pathology. They are one of the factors contributing to intensive care unit (ICU) admissions and can cause severe harm to the patient. Importantly, they are potentially avoidable. Previous studies in the UK have found high levels of sub-optimal care prior to admission to ICU.1 International studies within the last 20 years have had varied results, showing that between 1 and 20% of ICU admissions were associated with iatrogenic events.2-5 This study aimed to assess the incidence of iatrogenic events associated with ICU admission in five hospitals in the UK.
MethodsAll unscheduled adult admissions to ICU in a six-week period in 2011 were included. The notes were reviewed for the seven days prior to admission using a modified Global Trigger Tool. The cause of the admission was categorised as an ‘anaesthetic event’, ‘medical event’ or ‘iatrogenic event’. Iatrogenic events included potentially harmful acts of commission or omission as confirmed by the investigators answering ‘no’ to the question “would this standard of care be acceptable for a relative”. Cases were then reviewed by four consultants and recorded as iatrogenic if consensus was reached. Further meetings were held to review the case with specialist input (e.g. radiology) as required. If there was still no consensus the case was discarded. Events were graded by severity of harm caused between A (no harm) to E (contributed to patients death).
resultsThe notes of 280 patients were reviewed. In 95/28 patients, 149 potential iatrogenic events were identified. On review it was agreed that 76/280 patients had experienced 104 (27%) events. Eighty-three events either directly caused (28) or contributed (55) to the ICU admission. Of the excluded events, five caused or contributed to prolonged ICU stay and none caused or contributed to permanent harm or death.
discussionThe study found that a high proportion of ICU admissions were associated with iatrogenic events (27%), which is higher then the current literature (1–20%). These events were deemed largely preventable (77%). The nature of the events included delays seeking advice, inadequate resuscitation and misapplication of the early warning score. The authors suggest a new approach may be required in critically ill patient identification, such as continuous telemetry to detect those at risk of acute deterioration. Further studies are required to identify and prevent adverse events in all patients, including those not admitted to ICU.
dr emil hodzovicCT1 Weston General Hospital
References1. McQuillan P, Pilkington S, Allan A, et al. Confidential inquiry into quality of
care before admission to intensive care. BMJ 1998; 316: 1853–8. 2. Mercier E, Giraudeau B, Giniés G, Perrotin D, Dequin PF. Iatrogenic
events contributing to ICU admission: a prospective study. Intensive Care Medicine 2010; 36: 1033–7.
3. Trunet P, Le Gall JR, Lhoste F, et al. The role of iatrogenic disease in admissions to intensive care. JAMA 1980; 244: 2617–20.
4. Darchy B, Le Miére E, Figuérédo B, Bavoux E, Domart Y. Iatrogenic diseases as a reason for admission to the intensive care unit: incidence, causes, and consequences. Archives of Internal Medicine 1999; 159: 71–8.
5. Lehmann LS, Puopolo AL, Shaykevich S, Brennan TA. Iatrogenic events resulting in intensive care admission: frequency, cause, and disclosure to patients and institutions. American Journal of Medicine 2005; 118: 409–13.

19th ANNUAL SCIENTIFIC MEETING Friday 7th November 2014
Nottingham Conference Centre
£2000 Prize fund
Consultant/SAS £100 BSOA Member £70 Trainee/PA £35 BSOA Member £20
www.bsoa.org.uk or www.nuh.nhs.uk/pgec
Contact: Sue on 0115 840 2608 Email: [email protected]
10 years of conflict: Lessons learnt in pain management Dr Dominic Aldington
Surgeons & Anaesthetists talking: Damage limitation & timing of polytrauma surgery
Professor Chris Moran
Anaesthesia for the bigger boned: Obesity & orthopaedic anaesthesia
Dr Nick Reynolds
Orthopaedic Enhanced Recovery: What’s new & what works?
David McDonald
Orthopaedic Enhanced Recovery: Fine tuning the process
Tom Wainwright
Comprehensive Geriatric Assessment in Orthopaedics: Panacea or Pandora’s Box
Dr Adam Gordon
Hip Fracture Anaesthesia: Art or Science Dr Iain Moppett
(Abstract closing date Wednesday 17th September)
Approved by the Royal College of Anaesthetists
for 5 CPD credits
The AAGBI has partnered with Heartweb
to offer AAGBI members a discount on
distance learning online echocardiography
and clinical ultrasound courses.
CliniCal UltrasoUnd
EducAtIon ProGrAmmE
For more information on the course,
please visit www.aagbi.org/ultrascan
New AAGBI Member Benefit Discounted rates and a special introductory offer
UltrasCanTM
TM
The Association of Anaesthetists of Great Britain & Ireland and Anaesthesia will be awarding new research grants in September 2014.
Priority will be given to proposals that support the Associations’ research aims:
• Patient safety• Innovation• Clinical outcomes• Education and training• Related professional issues (e.g. standards
and guidelines, working conditions, medico-legal issues)
• The environment
Applications must describe how the proposed project meets the above aims. Suitable projects may be large research studies, small clinical/benchtop projects, idea (innovation) development, observational studies/data collection, quality improvements or clinical audits (although the latter are unlikely to receive AAGBI funding if they are small, ‘routine’ local audits). Any amount of funding may be sought, but applications will be judged on ‘value-for money’ as well as scientific credibility. Awards will be made via the NIAA and, if appropriate, will be eligible for NIHR portfolio status.
The deadline for applications is 5pm Friday 08 August 2014
For further information and to apply please visit the NIAA website http://www.niaa.org.uk
ASSOCIATION OF ANAESTHETISTS OF GREAT BRITAIN & IRELAND/ANAESTHESIA
RESEARCH GRANTS

17-19 SeptemBer 2014
Discounted rates for AAGBI members
Book now!
Keynote Lectures
how much has Nhs productivity changed over time?Prof Andrew Street, Centre of Health Economics, University of York
organisational culture and its impact on patient careMr Peter Lees, Medical Director, Faculty of Medical Leadership and Management, London
Sessional Highlights
The varied scientific programme includes local, national and international speakers.
Topics include:
• critical care obstetrics
• state of the art regional anaesthesia
• Quality improvement
• safety
• The airway – latest concepts
• intensive care medicine – update for the generalist
• Transplant medicine
• Medico-legal
• Pre-operative patient care
• Military medicine
• revalidation
We look forward to seeing you there!
Register on or before 21/07/2014 to qualify for the early member rates