anaesthetic trainees- the trauma call at smh anaesthetic
TRANSCRIPT

Imperial College NHS Trust
Dr Sabeena Qureshi May 2012
Anaesthetic Trainees- The Trauma Call at SMH
Anaesthetic staff at a trauma call Bleep Grade Times
Consultant 08:00 – 18:00 1201 SpR on-call for theatres 18:00 – 08:00 Extra SpR 08:00 – 17:00 6348 Obstetric SpR (only if not busy) 17:00 – 08:00
1213 SHO 24 hours 6345 Trauma ODP 24 hours
ICU SpR (bleep 1212) does not routinely come to trauma calls unless requested by the anaesthetic team.
The Bleep “Adult” or “Paediatric Trauma Team to A&E Resus, 1st floor QEQM” +/- “Code Red”
• Major haemorrhage protocol will be activated by the Trauma Team Leader (TTL)
• Inform the Anaesthetic Consultant on-call if not present • Consider calling for a second ODP (bleep 1651) • Ensure an ODP has switched on the TEG machine in theatres
If the voice over does not work change the batteries.
People on the Trauma Team
Patient
Anaes ODP
Anaesthetic machine and monitor
A+E SpR
Radiol
Nurse 2
TTL
Defib
Routine IV access trolley, blood
bottles, blood gas syringes
resus minijets
Nurse 1
A+E SHO
Neurosurg Fellow
Surg SpR & SHO
Radiographer Ortho SHO
Scribe
Imperial College NHS Trust
Dr Sabeena Qureshi May 2012
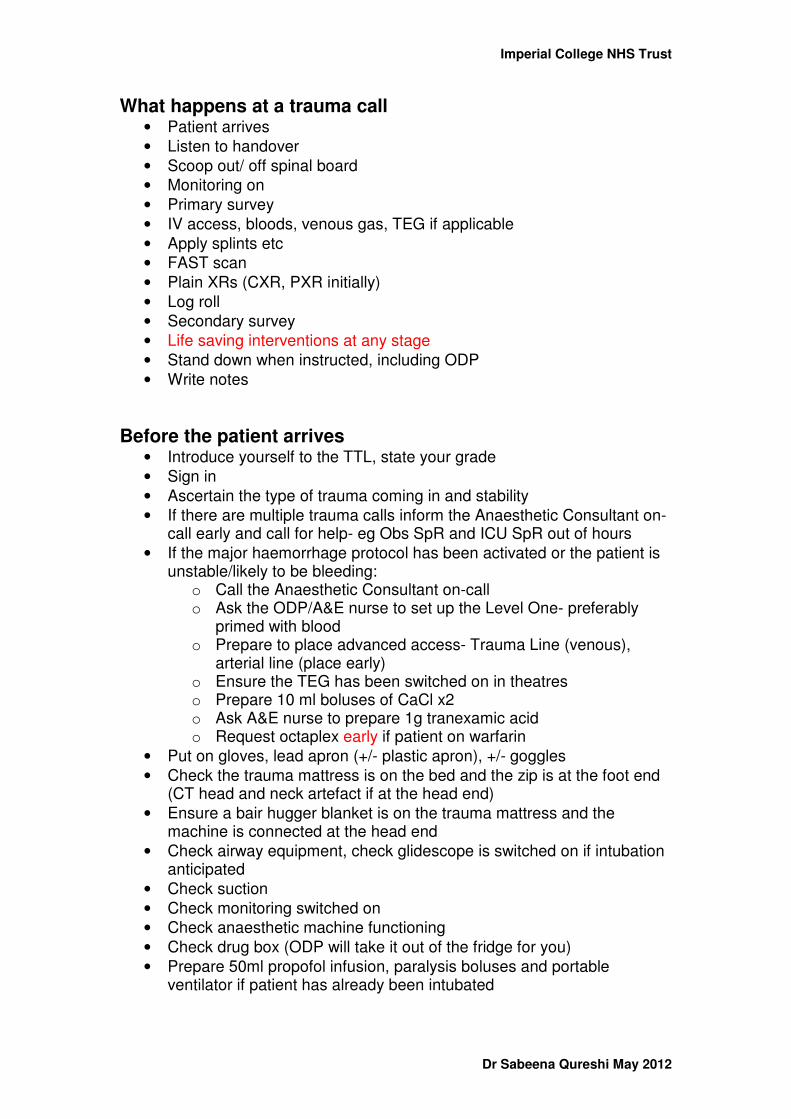
What happens at a trauma call • Patient arrives • Listen to handover • Scoop out/ off spinal board • Monitoring on • Primary survey • IV access, bloods, venous gas, TEG if applicable • Apply splints etc • FAST scan • Plain XRs (CXR, PXR initially) • Log roll • Secondary survey • Life saving interventions at any stage • Stand down when instructed, including ODP • Write notes
Before the patient arrives • Introduce yourself to the TTL, state your grade • Sign in • Ascertain the type of trauma coming in and stability • If there are multiple trauma calls inform the Anaesthetic Consultant on-
call early and call for help- eg Obs SpR and ICU SpR out of hours • If the major haemorrhage protocol has been activated or the patient is
unstable/likely to be bleeding: o Call the Anaesthetic Consultant on-call o Ask the ODP/A&E nurse to set up the Level One- preferably
primed with blood o Prepare to place advanced access- Trauma Line (venous),
arterial line (place early) o Ensure the TEG has been switched on in theatres o Prepare 10 ml boluses of CaCl x2 o Ask A&E nurse to prepare 1g tranexamic acid o Request octaplex early if patient on warfarin
• Put on gloves, lead apron (+/- plastic apron), +/- goggles • Check the trauma mattress is on the bed and the zip is at the foot end
(CT head and neck artefact if at the head end) • Ensure a bair hugger blanket is on the trauma mattress and the
machine is connected at the head end • Check airway equipment, check glidescope is switched on if intubation
anticipated • Check suction • Check monitoring switched on • Check anaesthetic machine functioning • Check drug box (ODP will take it out of the fridge for you) • Prepare 50ml propofol infusion, paralysis boluses and portable
ventilator if patient has already been intubated

Imperial College NHS Trust
Dr Sabeena Qureshi May 2012
Role of the anaesthetist at the trauma call • Airway and breathing • Switch on the bair hugger • In-line immobilisation, apply and remove collar and blocks as
necessary (ensure the tapes are re-applied to top blue trauma mattress only). Please always carry a full role of transpore tape with you if you are 6348 or 1201.
• Lead the log rolls • Assist with applying monitoring and appropriate NIBP intervals • Communicate observations regularly to the TTL and scribe • Look at the head in detail, comment on any external signs of head
injury, look for facial fractures and airway bleeding (often under-estimated), comment on any scalp lacerations (bleeding often under-estimated), assist applying head bandages including Celox
• Pupils, GCS • Talk to patient, reassure them, ascertain if in any pain and where, Hx of
event, PMH, DH (especially warfarin and anti-platelet therapy), allergies, last meal, anaesthetic history
• Assist with IV access, bloods, venous gas and TEG if requested • Gain large bore central venous access if necessary
o 8F trauma line subclavian or femoral vein (avoid femoral if pelvic injury likely)
o subclavian line should be sited on the side of any likely chest injury or side thoracostomy/chest drain in situ
o 14G or 16G long abbocaths in femoral vein o connect to Level One or fluid warmer (if rapid blood products not
required) • Site an arterial line but do not delay transfer. • Do not give any fluids unless instructed to do so by the TTL. • Colloid should not be used at all. • Inotropes/ vasoconstrictors should not be used routinely for
hypotension. • You may be asked to be a blood monitor if the Major Haemorrhage
Protocol has been activated. Accept the role if you understand what it involves and if you are not primarily responsible for the airway or other life-saving manoeuvres.
• Administer analgesia (IV paracetamol +/- opiates), anti-emetics (ondansetron 1st line)
• Administer procedural sedation, eg IV ketamine for fracture reduction • Consider large bore NGT/OGT. Always insert and leave on free
drainage if intubated. • Package for transfer to CT/theatres/angiography/ICU/PICU (transfer
checklist time allowing) o Oxygen, ambubag, suction o Ventilator if intubated o Full monitoring, ETCO2 if ventilated o Airway equipment o Fluids/blood/blood products o Anaesthetic drugs, resus drugs

Imperial College NHS Trust
Dr Sabeena Qureshi May 2012
o Transfer bag • If stood down by TTL ensure full documentation in the anaesthetic
section of the trauma notes and the time stood down on the signing-in sheet.
• Complete any relevant trauma audit forms.
In CT
• NB Time to CT very important, especially for head injuries (aim within 30 minutes of decision made to go to CT)
• No latex gloves please • Intubate before CT if concerned about airway protection • Give anti-emetics prior to CT if not intubated. • The patient can be transferred onto the CT table on the trauma
mattress (scoop or patslide not required). • Connect the monitoring block to the mobile monitor in CT • In a self-ventilating patient connect and tape the end of the oxygen
tubing to the long green oxygen tubing connected to the wall oxygen. • In a ventilated patient on a mobile ventilator connect the oxygen to the
oxygen pipeline hanging from the ceiling. • Remove the blocks and re-tape the head in order to reduce CT
artefact. • Do not stay in the CT scanner during scanning if at all possible. Ensure
the monitor is visible from the control room. • CT head (+/- facial bones) and neck first • CT chest to below pelvis is done with contrast so that active bleeding
can be assessed (arterial phase, portal venous phase +/- delayed phase). This should be done with the arms above the head and via large bore IV access with no 3-way taps connected. Help the radiographer with this process.
• Take the patient off the table and follow the TTL’s instruction of where to go (usually back to A&E Resus)
Decision to go to theatre • This may happen straight from A&E if the patient is unstable +/-
following a FAST scan, or after definitive diagnosis in CT. • Bleep 1655 (theatre nurse in charge) to let theatres know:
• When you are going up • What operation you think needs to be done • Confirm which theatre you can go to- usually Th 8 (no
anaesthetic room) • Ask the ODP to bleep 1651 to ensure a second ODP is setting up
theatre. Remember to ask for what you require, eg: • Drugs • Intubation equipment +/- glidescope • NG tube • Temp probe

Imperial College NHS Trust
Dr Sabeena Qureshi May 2012
• Bair hugger(s) • Blood warmer +/- Level One • Switch on TEG machine • Large bore peripheral IV access • Art line, CVP line, trauma line (swan sheath or vascath) • Table set up for neurosurgery if craniotomy planned • Armboards to connect to table once patient transferred • Cell saver if applicable
• Inform the Consultant on call • The TTL should accompany you • In theatre keep the cordless phone near you • Start the anaesthetic chart • Continue the blood monitor role: liase with the lab, follow the major
haemorrhage protocol, store blood and FFP that is not needed immediately in the theatre fridge (scan in and out properly), liase with theatre porters to continually collect products, send samples to the lab hourly, regular TEGS, and blood gases
• Early discussion with ICU if you think a bed is required
Decision to go to angiography • The same applies as for going to theatre, except it is not immediately
necessary to let bleep 1655 (theatre nurse in charge) know. • The patient may need to go to theatre first and then angiography
depending on the injury and the stability of the patient • Patients may not need to be intubated for angiography but you must be
prepared to anaesthetise at short notice if they become unstable. • You are relatively isolated. A Consultant Anaesthetist should be
present as these are high risk cases and angiography with embolisation/coiling can be a protracted process. Senior input is required to avoid excessive time and instability in angiography. The TTL should also be present. It may be appropriate to abandon the procedure and go to theatre.
• The blood monitor role should continue as above if applicable.

Imperial College NHS Trust
Dr Sabeena Qureshi May 2012

Imperial College NHS Trust
Dr Sabeena Qureshi May 2012

Imperial College NHS Trust
Dr Sabeena Qureshi May 2012

Imperial College NHS Trust
Dr Sabeena Qureshi May 2012

Imperial College NHS Trust
Dr Sabeena Qureshi May 2012
Imperial College NHS Trust
Dr Sabeena Qureshi May 2012
Imperial College NHS Trust
Dr Sabeena Qureshi May 2012

Imperial College NHS Trust
Dr Sabeena Qureshi May 2012

Imperial College NHS Trust
Dr Sabeena Qureshi May 2012