anatomic double-bundle anterior cruciate ligament...
TRANSCRIPT

F
rtr
tot
Anatomic Double-BundleAnterior Cruciate Ligament ReconstructionMarcus Hofbauer, MD,*,† Bart Muller, MD,*,‡ Megan Wolf, BS,* Brian Forsythe, MD,§ andreddie H. Fu, MD*
Over the past decade, intense research of the function of the 2 distinct bundles, theanteromedial and posterolateral, of the anterior cruciate ligament (ACL) has led to pro-nounced changes in the technical concepts of ACL reconstruction. Recently, the renewedfocus of ACL reconstruction has been to restore the anatomy of the ACL to its nativedimensions, collagen orientation, and insertion sites. The goal of ACL reconstruction is torestore normal knee kinematics, to enable patients to return to their preinjury level ofactivity, and to prevent further degenerative changes of the articular knee cartilage.Anatomic double-bundle ACL reconstruction has recently gained popularity as a conceptthat can be used to achieve these goals. This article provides an overview of the anatomyand function of the ACL. Furthermore, we highlight individual anatomic considerations asthey pertain to ACL reconstruction and describe the technique for anatomical ACLreconstruction.Oper Tech Sports Med 21:47-54 © 2013 Elsevier Inc. All rights reserved.
KEYWORDS ACL, anatomic, anterior cruciate ligament, double-bundle concept, sports medi-
cinehssnw
ot
c(b“bsptin
Tears of the anterior cruciate ligament (ACL) are amongthe most common ligamentous knee injuries, with
�200,000 ACL tears occurring annually in the United Statesalone.1 Traditionally, conventional single-bundle (SB) ACLeconstruction was the treatment of choice for complete ACLears; this technique improved knee stability and allowed aeturn to sports at short-term follow-up.2 However, several
prospective series and meta-analyses have shown that asignificant number of patients have persistent knee insta-bility, which prevents them from returning to sport andtheir previous level of activity.3,4 After SB ACL reconstruc-ion, good to excellent results were achieved in only 60%f patients, and �50% of patients returned to athletics atheir preinjury level. Furthermore, long-term evaluation
*Department of Orthopaedic Surgery, University of Pittsburgh, Pittsburgh,PA.
†Department of Trauma Surgery, Medical University Vienna, Vienna, Aus-tria.
‡Department of Orthopaedic Surgery, Academic Medical Center, Amster-dam, the Netherlands.
§Division of Sports Medicine, Rush University Medical Center, Chicago, IL.Address reprint requests to Freddie H. Fu, MD, Department of Orthopedic
Surgery, University of Pittsburgh Medical Center, Kaufman BuildingSuite 1011, 3471 Fifth Ave, Pittsburgh, PA 15213. E-mail:
1060-1872/13/$-see front matter © 2013 Elsevier Inc. All rights reserved.http://dx.doi.org/10.1053/j.otsm.2012.10.006
as revealed rates of osteoarthritis after SB ACL recon-truction that are similar to those in the nonoperated knee,uggesting that conventional SB ACL reconstruction doesot protect the knee from degenerative changes associatedith the initial ACL injury.5
Traditional SB ACL reconstruction techniques have fo-cused on recreating the ACL as 1 ligament. Furthermore, SBreconstructions have often resulted in nonanatomic tunnelplacement; the most common scenario being a tibial postero-lateral (PL) position to a femoral “‘high antero-medial’” tun-nel position.6,7 Recent focus on recreating the native anatomyf the ACL has changed our approach away from the tradi-ional ACL reconstruction technique.
Since 1938, anatomical studies have shown that the ACLonsists of 2 distinct functional bundles: the anteromedialAM) and the PL bundle8 (Fig. 1). Reconstruction of bothundles for ACL reconstruction led to the use of the termdouble-bundle” when describing this technique. “Double-undle” (DB) means that the ACL is reconstructed using 2eparate bundles but does not specify the location of tunnellacement. However, the term “anatomic” differs from theerm “double-bundle,” implying that the ACL graft is placedn the anatomic position with the tunnels drilled into theative ACL insertion site, regardless of the reconstruction
echnique (SB vs DB).47

scpt
leh
48 M. Hofbauer et al
The goal of ACL reconstruction is to restore normal kneekinematics, to enable patients to return to their preinjurylevel of activity, and to prevent further degeneration of artic-ular knee cartilage. Anatomic DB ACL reconstruction hasrecently gained popularity as a technique that can be used toachieve these goals.
Anatomy andBiomechanical ConsiderationsAnatomy is the basis of orthopedic surgery. The approach toACL reconstruction should be governed by this concept, aimingto reproduce the native anatomy and physiological function ofthe knee. The ACL consists of 2 functional bundles, namedaccording to the relative position of their tibial insertions: theAM bundle and the PL bundle. On the femoral side, the bundlesare vertically aligned with the knee in full extension, with theAM insertion superior to the PL insertion. When the knee isflexed to 90° during surgery, however, the bundles are horizon-tally aligned, with the AM insertion site relatively deeper in theknee joint than the PL insertion site. Both bundles have a syn-ergistic but distinct biomechanical function throughout therange of motion of the knee. In full extension, the PL bundle istaut, and the AM bundle is more lax. During knee flexion, thefemoral insertion site becomes horizontal, resulting in the tight-ening of the AM bundle and loosening of the PL bundle. Theindependent kinematic function of each bundle has importantclinical implications. Biomechanical studies have shown that DBACL reconstruction restores the knee function closer to prein-jury levels, particularly with internal and external rotation, thanthe conventional SB reconstruction procedure.9 Each bundleerves an integral purpose to prevent abnormal knee biome-hanics as a function of knee flexion angle. The AM bundle is therimary restraint against anterior–posterior translation, whereashe PL bundle is primarily responsible for rotational stability.10
Figure 1 Cadaveric dissection showing the 2 distinct bundles ofthe anterior cruciate ligament (ACL). AM, anteromedial; PL,posterolateral.
Therefore, by recreating the native anatomy, the concept of an-
atomic DB ACL reconstruction may restore preinjury kinemat-ics.
To reconstruct the ACL anatomically, detailed knowledgeof the anatomical bony landmarks of the femoral and tibialinsertion sites is essential. On the femoral side, 2 bony land-marks on the lateral wall of the intercondylar notch are themost important. The lateral intercondylar ridge, or “resi-dent’s ridge,” represents the anterior border of the femoralAM and PL bundle insertion sites when the knee is flexed to90°. The second ridge, the lateral bifurcate ridge, which ispresent in 80% of all cases, separates the origins of the AMand PL bundle insertion sites and runs perpendicular to thelateral intercondylar ridge11 (Fig. 2). Knowledge of theseandmarks is crucial to anatomical restoration of the ACL,specially in chronic cases where the bundle remnants mayave completely resorbed.
The Concept andIndications of AnatomicDB ACL ReconstructionAnatomic DB ACL reconstruction is not merely a techniquebut rather a concept based on the following 4 principles. Thefirst concept involves restoration of both the AM and PLbundles. Second, the tibial and femoral tunnels should beplaced anatomically within their native ACL insertion sites.Third, each bundle is tensioned in accordance with its nativetensioning pattern from full knee extension through flexion.The fourth and final principle is to customize the surgery foreach patient by taking into account their respective ACL in-sertion anatomy and activity level.
Figure 2 Arthroscopic view of a left knee through the centralportal. After ACL remnant debridement, the 2 bony landmarkson the medial wall of the lateral condyle, the lateral intercondylarridge, or “resident’s ridge” (black arrows), and the lateral bifur-cate ridge (white arrows) can be visualized. AM, anteromedial;
PL, posterolateral.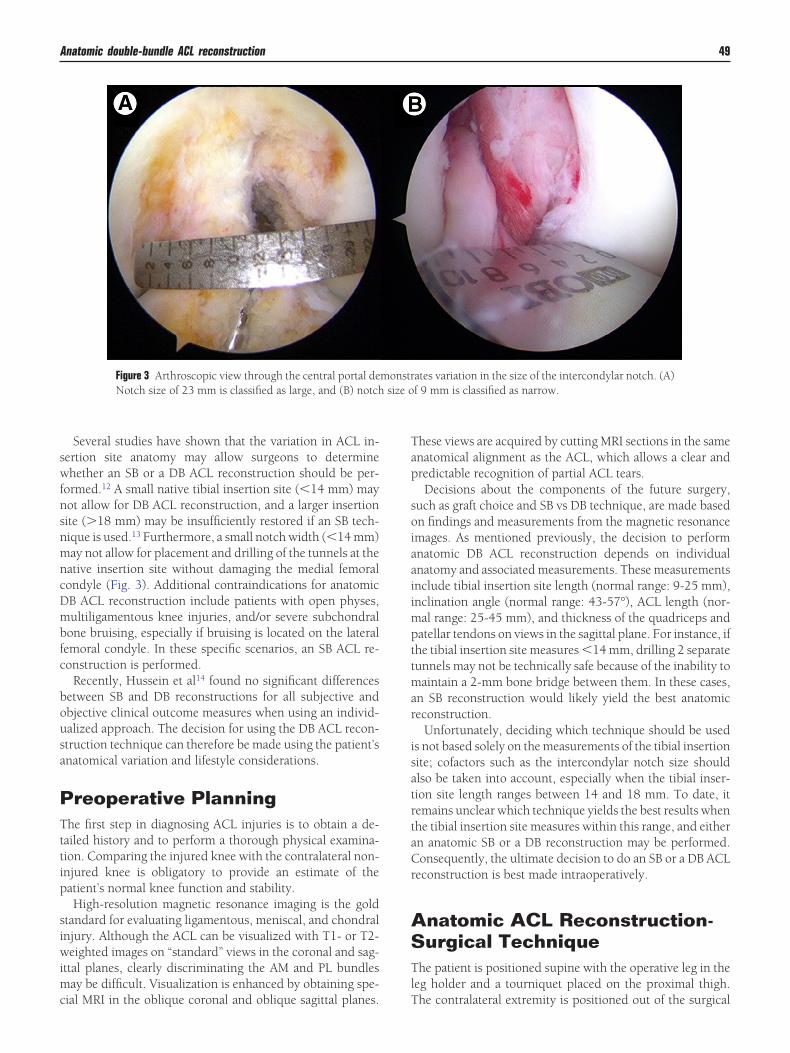
mncDmbfc
bousa
size o
Anatomic double-bundle ACL reconstruction 49
Several studies have shown that the variation in ACL in-sertion site anatomy may allow surgeons to determinewhether an SB or a DB ACL reconstruction should be per-formed.12 A small native tibial insertion site (�14 mm) maynot allow for DB ACL reconstruction, and a larger insertionsite (�18 mm) may be insufficiently restored if an SB tech-nique is used.13 Furthermore, a small notch width (�14 mm)
ay not allow for placement and drilling of the tunnels at theative insertion site without damaging the medial femoralondyle (Fig. 3). Additional contraindications for anatomicB ACL reconstruction include patients with open physes,ultiligamentous knee injuries, and/or severe subchondral
one bruising, especially if bruising is located on the lateralemoral condyle. In these specific scenarios, an SB ACL re-onstruction is performed.
Recently, Hussein et al14 found no significant differencesetween SB and DB reconstructions for all subjective andbjective clinical outcome measures when using an individ-alized approach. The decision for using the DB ACL recon-truction technique can therefore be made using the patient’snatomical variation and lifestyle considerations.
Preoperative PlanningThe first step in diagnosing ACL injuries is to obtain a de-tailed history and to perform a thorough physical examina-tion. Comparing the injured knee with the contralateral non-injured knee is obligatory to provide an estimate of thepatient’s normal knee function and stability.
High-resolution magnetic resonance imaging is the goldstandard for evaluating ligamentous, meniscal, and chondralinjury. Although the ACL can be visualized with T1- or T2-weighted images on “standard” views in the coronal and sag-ittal planes, clearly discriminating the AM and PL bundlesmay be difficult. Visualization is enhanced by obtaining spe-
Figure 3 Arthroscopic view through the central portal deNotch size of 23 mm is classified as large, and (B) notch
cial MRI in the oblique coronal and oblique sagittal planes.
These views are acquired by cutting MRI sections in the sameanatomical alignment as the ACL, which allows a clear andpredictable recognition of partial ACL tears.
Decisions about the components of the future surgery,such as graft choice and SB vs DB technique, are made basedon findings and measurements from the magnetic resonanceimages. As mentioned previously, the decision to performanatomic DB ACL reconstruction depends on individualanatomy and associated measurements. These measurementsinclude tibial insertion site length (normal range: 9-25 mm),inclination angle (normal range: 43-57°), ACL length (nor-mal range: 25-45 mm), and thickness of the quadriceps andpatellar tendons on views in the sagittal plane. For instance, ifthe tibial insertion site measures �14 mm, drilling 2 separatetunnels may not be technically safe because of the inability tomaintain a 2-mm bone bridge between them. In these cases,an SB reconstruction would likely yield the best anatomicreconstruction.
Unfortunately, deciding which technique should be usedis not based solely on the measurements of the tibial insertionsite; cofactors such as the intercondylar notch size shouldalso be taken into account, especially when the tibial inser-tion site length ranges between 14 and 18 mm. To date, itremains unclear which technique yields the best results whenthe tibial insertion site measures within this range, and eitheran anatomic SB or a DB reconstruction may be performed.Consequently, the ultimate decision to do an SB or a DB ACLreconstruction is best made intraoperatively.
Anatomic ACL Reconstruction-Surgical TechniqueThe patient is positioned supine with the operative leg in theleg holder and a tourniquet placed on the proximal thigh.
ates variation in the size of the intercondylar notch. (A)f 9 mm is classified as narrow.
monstr
The contralateral extremity is positioned out of the surgical
50 M. Hofbauer et al
field in the lithotomy position. Positioning of the operativeextremity is carefully performed to allow for �120° of kneeflexion.
First, an examination under anesthesia is performed toevaluate for associated ligamentous laxity: Lachman, anteriordrawer, posterior drawer, AM and PL drawer, and dial testexaminations at 30 and 90° of knee flexion are performed onthe affected and contralateral sides. If the patient has a knownunstable meniscus tear (ie, bucket handle tear) in associationwith an ACL tear, the pivot shift should be deferred.
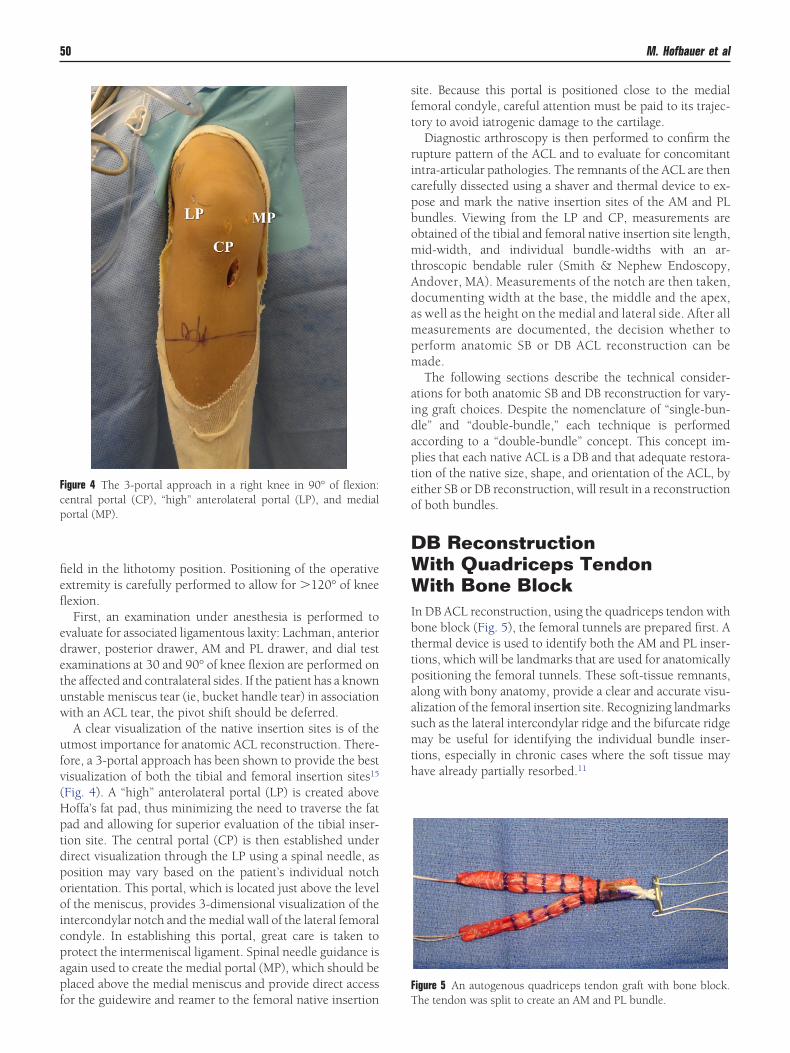
A clear visualization of the native insertion sites is of theutmost importance for anatomic ACL reconstruction. There-fore, a 3-portal approach has been shown to provide the bestvisualization of both the tibial and femoral insertion sites15
(Fig. 4). A “high” anterolateral portal (LP) is created aboveHoffa’s fat pad, thus minimizing the need to traverse the fatpad and allowing for superior evaluation of the tibial inser-tion site. The central portal (CP) is then established underdirect visualization through the LP using a spinal needle, asposition may vary based on the patient’s individual notchorientation. This portal, which is located just above the levelof the meniscus, provides 3-dimensional visualization of theintercondylar notch and the medial wall of the lateral femoralcondyle. In establishing this portal, great care is taken toprotect the intermeniscal ligament. Spinal needle guidance isagain used to create the medial portal (MP), which should beplaced above the medial meniscus and provide direct access
Figure 4 The 3-portal approach in a right knee in 90° of flexion:central portal (CP), “high” anterolateral portal (LP), and medialportal (MP).
for the guidewire and reamer to the femoral native insertion
site. Because this portal is positioned close to the medialfemoral condyle, careful attention must be paid to its trajec-tory to avoid iatrogenic damage to the cartilage.
Diagnostic arthroscopy is then performed to confirm therupture pattern of the ACL and to evaluate for concomitantintra-articular pathologies. The remnants of the ACL are thencarefully dissected using a shaver and thermal device to ex-pose and mark the native insertion sites of the AM and PLbundles. Viewing from the LP and CP, measurements areobtained of the tibial and femoral native insertion site length,mid-width, and individual bundle-widths with an ar-throscopic bendable ruler (Smith & Nephew Endoscopy,Andover, MA). Measurements of the notch are then taken,documenting width at the base, the middle and the apex,as well as the height on the medial and lateral side. After allmeasurements are documented, the decision whether toperform anatomic SB or DB ACL reconstruction can bemade.
The following sections describe the technical consider-ations for both anatomic SB and DB reconstruction for vary-ing graft choices. Despite the nomenclature of “single-bun-dle” and “double-bundle,” each technique is performedaccording to a “double-bundle” concept. This concept im-plies that each native ACL is a DB and that adequate restora-tion of the native size, shape, and orientation of the ACL, byeither SB or DB reconstruction, will result in a reconstructionof both bundles.
DB ReconstructionWith Quadriceps TendonWith Bone BlockIn DB ACL reconstruction, using the quadriceps tendon withbone block (Fig. 5), the femoral tunnels are prepared first. Athermal device is used to identify both the AM and PL inser-tions, which will be landmarks that are used for anatomicallypositioning the femoral tunnels. These soft-tissue remnants,along with bony anatomy, provide a clear and accurate visu-alization of the femoral insertion site. Recognizing landmarkssuch as the lateral intercondylar ridge and the bifurcate ridgemay be useful for identifying the individual bundle inser-tions, especially in chronic cases where the soft tissue mayhave already partially resorbed.11
Figure 5 An autogenous quadriceps tendon graft with bone block.
The tendon was split to create an AM and PL bundle.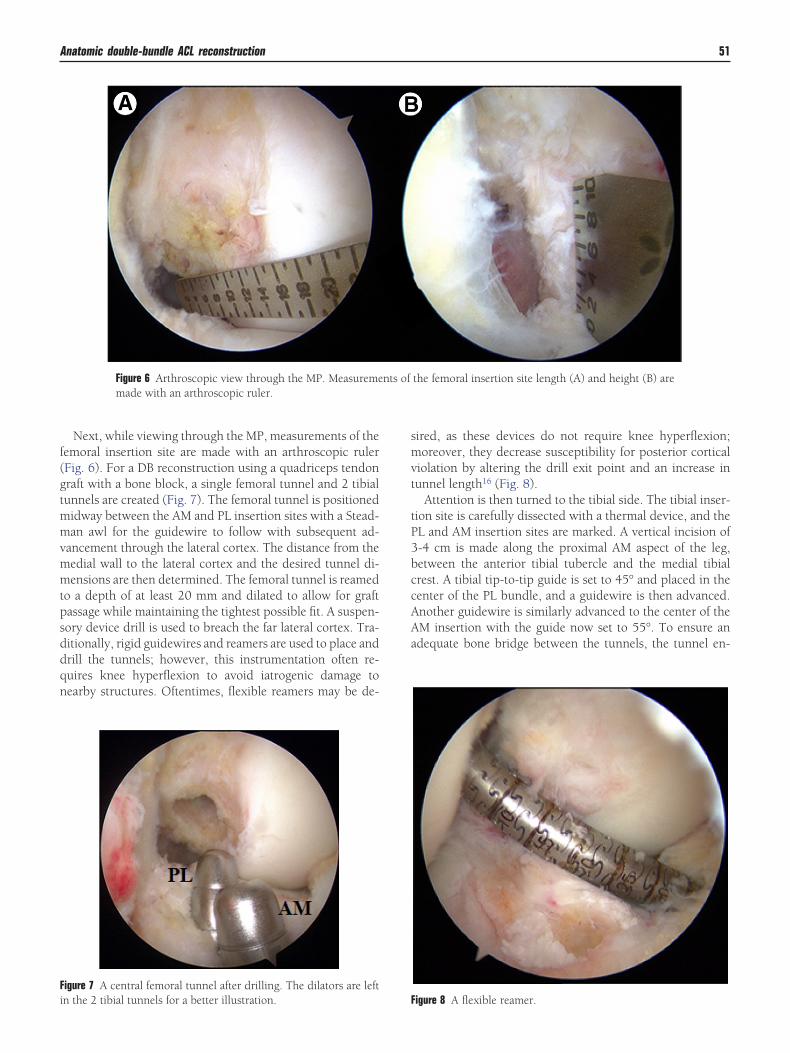
Anatomic double-bundle ACL reconstruction 51
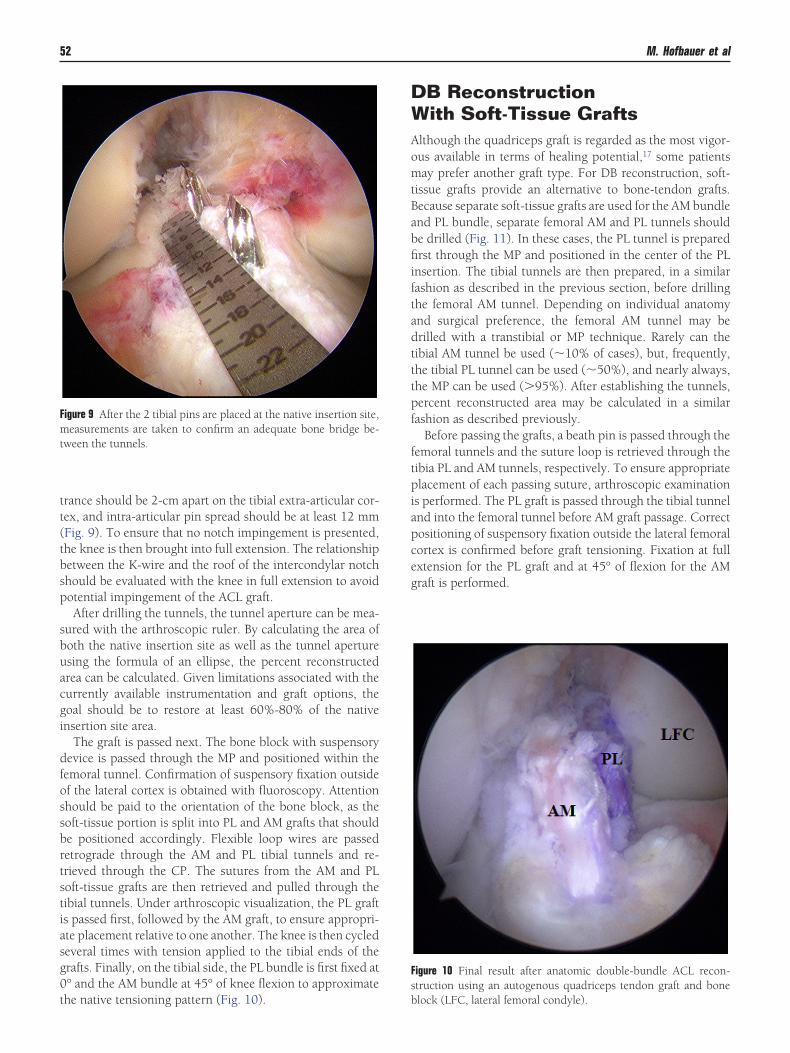
Next, while viewing through the MP, measurements of thefemoral insertion site are made with an arthroscopic ruler(Fig. 6). For a DB reconstruction using a quadriceps tendongraft with a bone block, a single femoral tunnel and 2 tibialtunnels are created (Fig. 7). The femoral tunnel is positionedmidway between the AM and PL insertion sites with a Stead-man awl for the guidewire to follow with subsequent ad-vancement through the lateral cortex. The distance from themedial wall to the lateral cortex and the desired tunnel di-mensions are then determined. The femoral tunnel is reamedto a depth of at least 20 mm and dilated to allow for graftpassage while maintaining the tightest possible fit. A suspen-sory device drill is used to breach the far lateral cortex. Tra-ditionally, rigid guidewires and reamers are used to place anddrill the tunnels; however, this instrumentation often re-quires knee hyperflexion to avoid iatrogenic damage tonearby structures. Oftentimes, flexible reamers may be de-
Figure 6 Arthroscopic view through the MP. Measurememade with an arthroscopic ruler.
Figure 7 A central femoral tunnel after drilling. The dilators are left
in the 2 tibial tunnels for a better illustration.sired, as these devices do not require knee hyperflexion;moreover, they decrease susceptibility for posterior corticalviolation by altering the drill exit point and an increase intunnel length16 (Fig. 8).
Attention is then turned to the tibial side. The tibial inser-tion site is carefully dissected with a thermal device, and thePL and AM insertion sites are marked. A vertical incision of3-4 cm is made along the proximal AM aspect of the leg,between the anterior tibial tubercle and the medial tibialcrest. A tibial tip-to-tip guide is set to 45° and placed in thecenter of the PL bundle, and a guidewire is then advanced.Another guidewire is similarly advanced to the center of theAM insertion with the guide now set to 55°. To ensure anadequate bone bridge between the tunnels, the tunnel en-
the femoral insertion site length (A) and height (B) are
nts ofFigure 8 A flexible reamer.
mtBabfiiftadtttpf
ftpiapceg
52 M. Hofbauer et al
trance should be 2-cm apart on the tibial extra-articular cor-tex, and intra-articular pin spread should be at least 12 mm(Fig. 9). To ensure that no notch impingement is presented,the knee is then brought into full extension. The relationshipbetween the K-wire and the roof of the intercondylar notchshould be evaluated with the knee in full extension to avoidpotential impingement of the ACL graft.
After drilling the tunnels, the tunnel aperture can be mea-sured with the arthroscopic ruler. By calculating the area ofboth the native insertion site as well as the tunnel apertureusing the formula of an ellipse, the percent reconstructedarea can be calculated. Given limitations associated with thecurrently available instrumentation and graft options, thegoal should be to restore at least 60%-80% of the nativeinsertion site area.
The graft is passed next. The bone block with suspensorydevice is passed through the MP and positioned within thefemoral tunnel. Confirmation of suspensory fixation outsideof the lateral cortex is obtained with fluoroscopy. Attentionshould be paid to the orientation of the bone block, as thesoft-tissue portion is split into PL and AM grafts that shouldbe positioned accordingly. Flexible loop wires are passedretrograde through the AM and PL tibial tunnels and re-trieved through the CP. The sutures from the AM and PLsoft-tissue grafts are then retrieved and pulled through thetibial tunnels. Under arthroscopic visualization, the PL graftis passed first, followed by the AM graft, to ensure appropri-ate placement relative to one another. The knee is then cycledseveral times with tension applied to the tibial ends of thegrafts. Finally, on the tibial side, the PL bundle is first fixed at0° and the AM bundle at 45° of knee flexion to approximate
Figure 9 After the 2 tibial pins are placed at the native insertion site,measurements are taken to confirm an adequate bone bridge be-tween the tunnels.
the native tensioning pattern (Fig. 10).
DB ReconstructionWith Soft-Tissue GraftsAlthough the quadriceps graft is regarded as the most vigor-ous available in terms of healing potential,17 some patients
ay prefer another graft type. For DB reconstruction, soft-issue grafts provide an alternative to bone-tendon grafts.ecause separate soft-tissue grafts are used for the AM bundlend PL bundle, separate femoral AM and PL tunnels shoulde drilled (Fig. 11). In these cases, the PL tunnel is preparedrst through the MP and positioned in the center of the PL
nsertion. The tibial tunnels are then prepared, in a similarashion as described in the previous section, before drillinghe femoral AM tunnel. Depending on individual anatomynd surgical preference, the femoral AM tunnel may berilled with a transtibial or MP technique. Rarely can theibial AM tunnel be used (�10% of cases), but, frequently,he tibial PL tunnel can be used (�50%), and nearly always,he MP can be used (�95%). After establishing the tunnels,ercent reconstructed area may be calculated in a similarashion as described previously.
Before passing the grafts, a beath pin is passed through theemoral tunnels and the suture loop is retrieved through theibia PL and AM tunnels, respectively. To ensure appropriatelacement of each passing suture, arthroscopic examination
s performed. The PL graft is passed through the tibial tunnelnd into the femoral tunnel before AM graft passage. Correctositioning of suspensory fixation outside the lateral femoralortex is confirmed before graft tensioning. Fixation at fullxtension for the PL graft and at 45° of flexion for the AMraft is performed.
Figure 10 Final result after anatomic double-bundle ACL recon-struction using an autogenous quadriceps tendon graft and bone
block (LFC, lateral femoral condyle).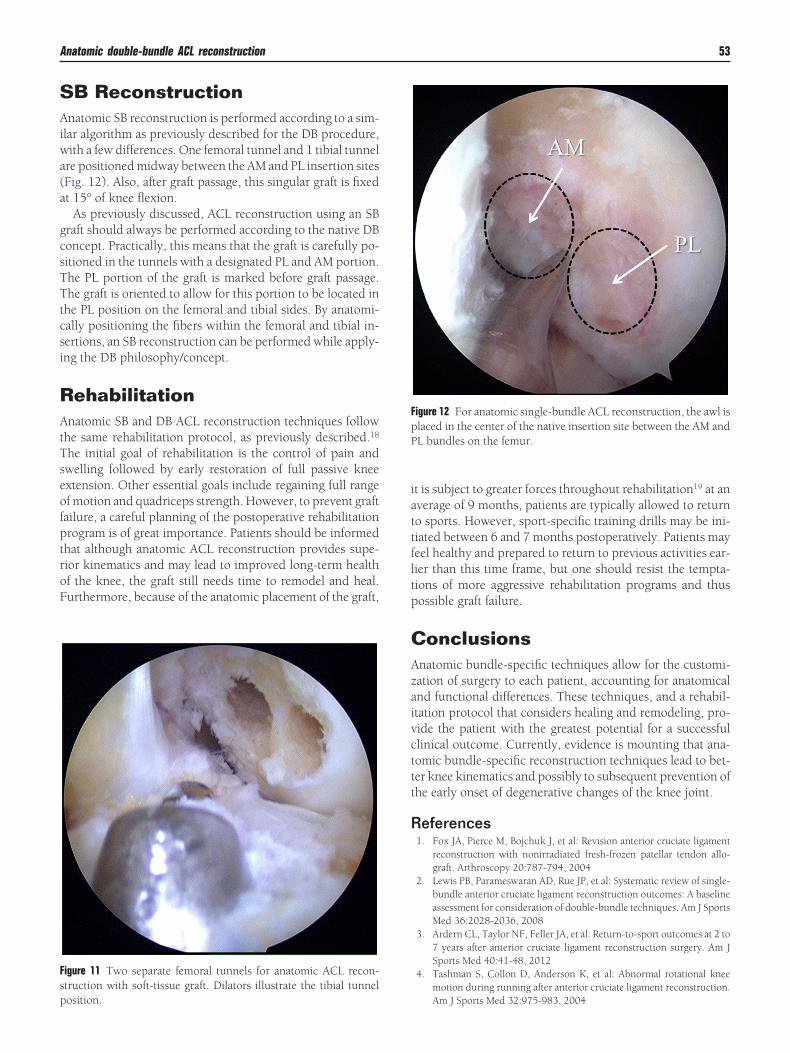
attfltp
sp
Anatomic double-bundle ACL reconstruction 53
SB ReconstructionAnatomic SB reconstruction is performed according to a sim-ilar algorithm as previously described for the DB procedure,with a few differences. One femoral tunnel and 1 tibial tunnelare positioned midway between the AM and PL insertion sites(Fig. 12). Also, after graft passage, this singular graft is fixedat 15° of knee flexion.
As previously discussed, ACL reconstruction using an SBgraft should always be performed according to the native DBconcept. Practically, this means that the graft is carefully po-sitioned in the tunnels with a designated PL and AM portion.The PL portion of the graft is marked before graft passage.The graft is oriented to allow for this portion to be located inthe PL position on the femoral and tibial sides. By anatomi-cally positioning the fibers within the femoral and tibial in-sertions, an SB reconstruction can be performed while apply-ing the DB philosophy/concept.
RehabilitationAnatomic SB and DB ACL reconstruction techniques followthe same rehabilitation protocol, as previously described.18
The initial goal of rehabilitation is the control of pain andswelling followed by early restoration of full passive kneeextension. Other essential goals include regaining full rangeof motion and quadriceps strength. However, to prevent graftfailure, a careful planning of the postoperative rehabilitationprogram is of great importance. Patients should be informedthat although anatomic ACL reconstruction provides supe-rior kinematics and may lead to improved long-term healthof the knee, the graft still needs time to remodel and heal.Furthermore, because of the anatomic placement of the graft,
Figure 11 Two separate femoral tunnels for anatomic ACL recon-truction with soft-tissue graft. Dilators illustrate the tibial tunnel
osition.it is subject to greater forces throughout rehabilitation19 at anverage of 9 months, patients are typically allowed to returno sports. However, sport-specific training drills may be ini-iated between 6 and 7 months postoperatively. Patients mayeel healthy and prepared to return to previous activities ear-ier than this time frame, but one should resist the tempta-ions of more aggressive rehabilitation programs and thusossible graft failure.
ConclusionsAnatomic bundle-specific techniques allow for the customi-zation of surgery to each patient, accounting for anatomicaland functional differences. These techniques, and a rehabil-itation protocol that considers healing and remodeling, pro-vide the patient with the greatest potential for a successfulclinical outcome. Currently, evidence is mounting that ana-tomic bundle-specific reconstruction techniques lead to bet-ter knee kinematics and possibly to subsequent prevention ofthe early onset of degenerative changes of the knee joint.
References1. Fox JA, Pierce M, Bojchuk J, et al: Revision anterior cruciate ligament
reconstruction with nonirradiated fresh-frozen patellar tendon allo-graft. Arthroscopy 20:787-794, 2004
2. Lewis PB, Parameswaran AD, Rue JP, et al: Systematic review of single-bundle anterior cruciate ligament reconstruction outcomes: A baselineassessment for consideration of double-bundle techniques. Am J SportsMed 36:2028-2036, 2008
3. Ardern CL, Taylor NF, Feller JA, et al: Return-to-sport outcomes at 2 to7 years after anterior cruciate ligament reconstruction surgery. Am JSports Med 40:41-48, 2012
4. Tashman S, Collon D, Anderson K, et al: Abnormal rotational kneemotion during running after anterior cruciate ligament reconstruction.
Figure 12 For anatomic single-bundle ACL reconstruction, the awl isplaced in the center of the native insertion site between the AM andPL bundles on the femur.
Am J Sports Med 32:975-983, 2004

54 M. Hofbauer et al
5. Lohmander LS, Ostenberg A, Englund M, et al: High prevalence of kneeosteoarthritis, pain, and functional limitations in female soccer playerstwelve years after anterior cruciate ligament injury. Arthritis Rheum50:3145-3152, 2004
6. Woo SL, Kanamori A, Zeminski J, et al: The effectiveness of reconstruc-tion of the anterior cruciate ligament with hamstrings and patellartendon. A cadaveric study comparing anterior tibial and rotationalloads. J Bone Joint Surg Am 84-A:907-914, 2002
7. Kopf S, Forsythe B, Wong AK, et al: Nonanatomic tunnel position intraditional transtibial single-bundle anterior cruciate ligament recon-struction evaluated by three-dimensional computed tomography.J Bone Joint Surg Am 92:1427-1431, 2010
8. Girgis FG, Marshall JL, Monajem A: The cruciate ligaments of the kneejoint. Anatomical, functional and experimental analysis. Clin OrthopRelat Res 106:216-231, 1975
9. Yagi M, Wong EK, Kanamori A, et al: Biomechanical analysis of ananatomic anterior cruciate ligament reconstruction. Am J Sports Med30:660-666, 2002
10. Zantop T, Herbort M, Raschke MJ, et al: The role of the anteromedialand posterolateral bundles of the anterior cruciate ligament in anteriortibial translation and internal rotation. Am J Sports Med 35:223-227,2007
11. Ferretti M, Ekdahl M, Shen W, et al: Osseous landmarks of the femoralattachment of the anterior cruciate ligament: An anatomic study. Ar-
throscopy 23:1218-1225, 200712. Kopf S, Pombo MW, Szczodry M, et al: Size variability of the humananterior cruciate ligament insertion sites. Am J Sports Med 39:108-113,2011
13. Karlsson J, Irrgang JJ, van Eck CF, et al: Anatomic single- and double-bundle anterior cruciate ligament reconstruction, part 2: Clinical ap-plication of surgical technique. Am J Sports Med 39:2016-2026, 2011
14. Hussein M, van Eck CF, Cretnik A, et al: Prospective randomizedclinical evaluation of conventional single-bundle, anatomic single-bun-dle, and anatomic double-bundle anterior cruciate ligament recon-struction: 281 cases with 3- to 5-year follow-up. Am J Sports Med40:512-520, 2012
15. Araujo PH, van Eck CF, Macalena JA, et al: Advances in the three-portaltechnique for anatomical single- or double-bundle ACL reconstruction.Knee Surg Sports Traumatol Arthrosc 19:1239-1242, 2011
16. Steiner ME, Smart LR: Flexible instruments outperform rigid instru-ments to place anatomic anterior cruciate ligament femoral tunnelswithout hyperflexion. Arthroscopy 28:835-843, 2012
17. Geib TM, Shelton WR, Phelps RA, et al: Anterior cruciate ligamentreconstruction using quadriceps tendon autograft: Intermediate-termoutcome. Arthroscopy 25:1408-1414, 2009
18. Hensler D, Van Eck CF, Fu FH, et al: Anatomic anterior cruciate liga-ment reconstruction utilizing the double-bundle technique. J OrthopSports Phys Ther 42:184-195, 2012
19. Kato Y, Ingham SJ, Kramer S, et al: Effect of tunnel position for ana-tomic single-bundle ACL reconstruction on knee biomechanics in a
porcine model. Knee Surg Sports Traumatol Arthrosc 18:2-10, 2010