anatomic pathology checklistwebapps.cap.org/apps/docs/laboratory_accreditation/... · sections:...
TRANSCRIPT
Revised: 09/27/2007
COMMISSION ON LABORATORY ACCREDITATION
Laboratory Accreditation Program
ANATOMIC PATHOLOGY CHECKLIST
Disclaimer and Copyright Notice The College of American Pathologists (CAP) Checklists are posted on the CAP's Web site for information only. If you are enrolled in the CAP's Laboratory Accreditation Program and are preparing for an inspection, you must use the Checklists that were mailed in your application or reapplication packet, not those posted on the Web site. The Checklists undergo regular revision and Checklists may be revised after you receive your packet. If a Checklist has been updated since receiving your packet, you will be inspected based upon the Checklists that were mailed. If you have any questions about the use of Checklists in the inspection process, please e-mail the CAP ([email protected]), or call (800) 323-4040, ext. 6065. All Checklists are ©2007. College of American Pathologists. All rights reserved.
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 2 of 95
ANATOMIC PATHOLOGY
OUTLINE
SUMMARY OF CHANGES ...............................................................................................................................................3 INSPECTION TECHNIQUES – KEY POINTS..................................................................................................................5
GENERAL ANATOMIC PATHOLOGY ................................................................................................................................6 INTERLABORATORY COMPARISONS..........................................................................................................................7 PROCEDURE MANUAL....................................................................................................................................................7 SAFETY.............................................................................................................................................................................11
SURGICAL PATHOLOGY ...................................................................................................................................................12 QUALITY MANAGEMENT ............................................................................................................................................12 QUALITY CONTROL ......................................................................................................................................................18
SURGICAL SPECIMEN EXAMINATION .................................................................................................................18 INTRAOPERATIVE CONSULTATION (RAPID DIAGNOSIS OR FROZEN SECTION).......................................25 SURGICAL PATHOLOGY REPORTS .......................................................................................................................29
HISTOLOGY LABORATORY..............................................................................................................................................35 QUALITY CONTROL/HISTOLOGIC PREPARATIONS ..........................................................................................36 SPECIAL STAINS (HISTOCHEMISTRY)..................................................................................................................37
IMMUNOLOGIC AND MOLECULAR METHODS .......................................................................................................40 IMMUNOFLUORESCENCE MICROSCOPY.............................................................................................................40 IMMUNOHISTOCHEMISTRY ...................................................................................................................................41 FLUORESCENCE AND NON-FLUORESCENCE IN SITU HYBRIDIZATION (FISH, ISH) .................................48 PREDICTIVE MARKERS............................................................................................................................................51 INSTRUMENTS AND EQUIPMENT..........................................................................................................................57
Equipment Maintenance ...........................................................................................................................................57 Pipettes and Thermometers.......................................................................................................................................58 Tissue Processor .......................................................................................................................................................60 Paraffin Dispenser.....................................................................................................................................................60 Flotation Baths..........................................................................................................................................................61 Microtomes ...............................................................................................................................................................62
PHYSICAL FACILITIES ..................................................................................................................................................62 STORAGE AND SUPPLY ...........................................................................................................................................63
HISTOLOGY LABORATORY SAFETY.........................................................................................................................64 AUTOPSY PATHOLOGY.....................................................................................................................................................68
QUALITY MANAGEMENT ............................................................................................................................................68 DEATH PROCEDURES....................................................................................................................................................71 AUTOPSY ROOM.............................................................................................................................................................73 AUTOPSY PERFORMANCE AND DOCUMENTATION..............................................................................................78 AUTOPSY SAFETY .........................................................................................................................................................83
ELECTRON MICROSCOPY.................................................................................................................................................86 QUALITY CONTROL ......................................................................................................................................................86
SPECIMEN COLLECTION .........................................................................................................................................86 ELECTRON MICROSCOPY SAMPLE PREPARATION...........................................................................................87 INSTRUMENTS AND EQUIPMENT..........................................................................................................................89 REPORTS......................................................................................................................................................................90 RECORDS, FILES AND PHOTOGRAPHS.................................................................................................................91
LABORATORY SAFETY.................................................................................................................................................93
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 3 of 95
SUMMARY OF CHANGES ANATOMIC PATHOLOGY Checklist
9/27/2007 Edition
The following questions have been added, revised, or deleted in this edition of the checklist, or in the two editions immediately previous to this one. If this checklist was created for a reapplication, on-site inspection or self-evaluation it has been customized based on the laboratory's activity menu. The listing below is comprehensive; therefore some of the questions included may not appear in the customized checklist. Such questions are not applicable to the testing performed by the laboratory. Note: For revised checklist questions, a comparison of the previous and current text may be found on the CAP website. Click on Laboratory Accreditation, Checklists, and then click the column marked Changes for the particular checklist of interest. NEW Checklist Questions Question Effective Date ANP.22989 09/27/2007 ANP.22990 09/27/2007 ANP.22993 09/27/2007 ANP.22994 09/27/2007 ANP.22996 09/27/2007 ANP.22997 09/27/2007 ANP.22998 09/27/2007 ANP.22999 09/27/2007 ANP.23005 09/27/2007 ANP.11665 12/12/2006 ANP.22982 12/12/2006 ANP.22984 12/12/2006 ANP.27170 12/12/2006 REVISED Checklist Questions Question Effective Date ANP.02888 12/12/2006 ANP.11600 12/12/2006 ANP.11605 12/12/2006 ANP.12350 12/12/2006 ANP.12500 12/12/2006 ANP.21150 12/12/2006 ANP.22550 12/12/2006 ANP.22570 12/12/2006 ANP.22660 12/12/2006
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 4 of 95
ANP.22980 12/12/2006 ANP.28290 12/12/2006 ANP.28860 12/12/2006 DELETED Checklist Questions Question Effective Date ANP.22991 09/27/2007 ANP.22995 09/27/2007 ANP.21200 12/12/2006 ANP.22950 12/12/2006 ANP.27720 12/12/2006
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 5 of 95
The checklists used in connection with the inspection of laboratories by the Commission on Laboratory Accreditation (“CLA”) of the College of American Pathologists have been created by the College and are copyrighted works of the College. The College has authorized copying and use of the checklists by College inspectors in conducting laboratory inspections for the CLA and by laboratories that are preparing for such inspections. Except as permitted by section 107 of the Copyright Act, 17 U.S.C. sec. 107, any other use of the checklists constitutes infringement of the College’s copyrights in the checklists. The College will take appropriate legal action to protect these copyrights.
CONTINUING EDUCATION INFORMATION Beginning January 2008, you may earn continuing education credits (CME/CE) by completing an online Inspection Preparation activity that includes review of this checklist. Prior to reviewing the checklist, log on to the CAP Web site at <www.cap.org <http://www.cap.org>>, click the Education Programs tab, then select Laboratory Accreditation Program (LAP) Education Activities, and Inspection Preparation for complete instructions and enrollment information. __________________________________________________________________________________ IMPORTANT: The contents of the Laboratory General Checklist are applicable to the Anatomic Pathology section of the laboratory.
****************************************************************
INSPECTION TECHNIQUES – KEY POINTS
**************************************************************** I. READ – OBSERVE – ASK – the three methods of eliciting information during the inspection process. These three methods may be used throughout the day in no particular order. Plan the inspection in a way that allows adequate time for all three components. READ = Review of Records and Documents Document review verifies that procedures and manuals are complete, current, available to staff, accurate and reviewed, and describe good laboratory practice. Make notes of any questions you may have, or processes you would like to observe as you read the documentation. In reviewing records of quality control, instrument maintenance, cases sent for consultation, and other activities, select records from various times during the two-year interval since the previous on-site inspection. A sufficient sample of surgical pathology reports (and other records, as appropriate) should be reviewed to assure that consultations, special notification of unexpected diagnoses (e.g., by phone), and corrections are well documented. OBSERVE – ASK = Direct Observation and Asking Questions Observing and asking questions accomplish the following:
1. Verifies that the actual practice matches the written policy or procedure
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 6 of 95
2. Ensures that the laboratory processes are appropriate for the testing performed 3. Ensures that outcomes for any problem areas, such as issues/problems identified through the
quality management process, have been adequately investigated and resolved 4. Ensures that previous deficiencies have been corrected
Use the following techniques: Observe laboratory practices – look at what the laboratory is actually doing. Compare the
written policy/procedure to what you actually observe in the laboratory to ensure the written policy/procedure accurately reflects laboratory practice. Note if practice deviates from the documented policies/procedures. Observe activities in the gross dissection and histology areas, to determine whether specimen identity is maintained throughout all the processing steps that result in the preparation of microscopic slides, and to determine if personnel follow written procedures.
Ask open ended, probing questions – these are starting points that will allow you to obtain large
amounts of information, and help you clarify your understanding of the documentation you’ve seen and observations you’ve made. This eliminates the need to ask every single checklist question, as the dialogue between you and the laboratory may address multiple checklist questions.
Ask open-ended questions that start with phrases such as “show me how…” or “tell me about
…” or “what would you do if…”. By asking questions that are open-ended, or by posing a hypothetical problem, you will avoid “cookbook” answers. For example, ask “Could you show me the specimen labeling policy and how it ensures accurate identification of the specimen throughout processing and reporting?” This will help you to determine how well the technical staff is trained, whether or not they are adhering to the laboratory’s procedures and policies, and give you a feel for the general level of performance of the laboratory.
Ask follow-up questions for clarification. Generally, it is best not to ask the checklist questions verbatim. For example, instead of asking the checklist question “Is there documentation of corrective action when an unlabeled specimen is received?” ask, “What would you do if an unlabeled specimen is received?” A follow-up probing question could be, “What would you do if there were repeated instances of unlabeled specimens from the same source?”
II. Review correction of previous deficiencies: Review the list of deficiencies from the previous on-site inspection provided in the inspector’s packet. Ensure that they have been appropriately addressed.
#############################################################################
GENERAL ANATOMIC PATHOLOGY
############################################################################# Do NOT use this Checklist if: 1. The laboratory does NOT perform any on-site preparation or examination of anatomic
pathology specimens, but refers all submitted material to an outside laboratory 2. The laboratory's involvement in anatomic pathology is limited to filing of reports and/or slides
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 7 of 95
This Checklist covers several areas of anatomic pathology services, and is divided into the following sections: Surgical Pathology, Histology Laboratory, Autopsy Pathology, and Electron Microscopy. Cytopathology (both gynecologic and non-gynecologic) is covered in a separate Checklist. The sequence for inspection of the anatomic pathology service is at the discretion of the inspection team. The sequence herein is consistent with that used for all other sections of the laboratory, but is not restrictive.
****************************************************************************
INTERLABORATORY COMPARISONS
**************************************************************************** ANP.02000 Phase I N/A YES NO As applicable, does the laboratory participate in a peer educational program in anatomic pathology (e.g., CAP Educational Anatomic Pathology Programs)? NOTE: The laboratory should consider participation in programs appropriate to its scope of service. Such programs provide valuable educational opportunities for peer performance comparisons in both technical and diagnostic arenas. While none of these completely emulates the precise clinical setting involving anatomic pathology preparations and rendering of anatomic or clinical diagnoses, they can be a useful benchmark of peer-based performance in a national database. COMMENTARY: N/A
*****************************************************************
PROCEDURE MANUAL
***************************************************************** The anatomic pathology laboratory must have a procedure manual that addresses pre-analytic, analytic, and post-analytic processes. The manual should include procedures for accessioning and maintaining the identity of specimens; reporting diagnostic results; safety issues relevant to anatomic pathology; and procedures for tests performed in the histology, immunohistochemistry, and electron microscopy laboratories. Procedures must include, as applicable, principle, clinical significance, specimen type, required reagents, calibration, quality control, procedural steps, calculations, reference intervals, and interpretation. The specific style and format of procedure manuals are at the discretion of the laboratory director.
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 8 of 95
The inspection team should review the procedure manual in detail to understand the laboratory's standard operating procedures, ensure that all significant information and instructions are included, and that actual practice matches the contents of the procedure manuals. **REVISED** 12/12/2006 ANP.02888 Phase II N/A YES NO Is a complete procedure manual available at the workbench or in the work area?
NOTE 1: The use of inserts provided by manufacturers is not acceptable in place of a procedure manual. However, such inserts may be used as part of a procedure description, if the insert accurately and precisely describes the procedure as performed in the laboratory. Any variation from this printed or electronic procedure must be detailed in the procedure manual. In all cases, appropriate reviews must occur.
NOTE 2: A manufacturer's procedure manual for an instrument/reagent system may be acceptable as a component of the overall departmental procedures. Any modification to or deviation from the procedure manual must be clearly documented. NOTE 3: Card files or similar systems that summarize key information are acceptable for use as quick reference at the workbench provided that:
a. A complete manual is available for reference b. The card file or similar system corresponds to the complete manual and is subject to
document control
NOTE 4: Electronic (computerized) manuals are fully acceptable. There is no requirement for paper copies to be available for the routine operation of the laboratory, so long as the electronic versions are readily available to all personnel. However, procedures must be available to laboratory personnel when the electronic versions are inaccessible (e.g., during laboratory information system or network downtime); thus, the laboratory must maintain either paper copies or electronic copies on CD or other media that can be accessed via designated computers. All procedures, in either electronic or paper form, must be readily available for review by the inspector at the time of the CAP inspection. Electronic versions of procedures must be subjected to proper document control (i.e., only authorized persons may make changes, changes are dated/signed (manual or electronic), and there is documentation of annual review). Documentation of review of electronic procedures may be accomplished by including statements such as “reviewed by [name of reviewer] on [date of review]” in the electronic record. Alternatively, paper review sheets may be used to document review of electronic procedures. Documentation of review by a secure electronic signature is NOT required.
COMMENTARY:
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 9 of 95
N/A REFERENCES: 1) Department of Health and Human Services, Centers for Medicare and Medicaid Services. Clinical laboratory improvement amendments of 1988; final rule. Fed Register. 2003(Jan 24):7164 [42CFR493.1251]; 2) Check W. Immunostains making the difference. Northfield, IL: College of American Pathologists CAP Today. 1997;11(10):1; 3) van Leeuwen AM. 6 Steps to building an efficiency tool. Advance/Lab. 1999:8(6):88-91; 4) Werner M, et al. Effect of formalin tissue fixation and processing on immunohistochemistry. Am J Surg Pathol. 2000;24:1016-1019; 5) Borkowski A, et al. Intranet-based quality improvement documentation at the Veterans Affairs Maryland health care system. Mod. Pathol. 2001;14:1-5; 6) Clinical and Laboratory Standards Institute (CLSI). Laboratory Documents: Development and Control; Approved Guideline—Fifth Edition. CLSI document GP2-A5 (ISBN 1-56238-600-X). Clinical and Laboratory Standards Institute, 940 West Valley Road, Suite 1400, Wayne, Pennsylvania 19087-1898 USA, 2006. ANP.03776 Phase II N/A YES NO Is there documentation of at least annual review of all policies and procedures in the anatomic pathology section by the current laboratory director or designee? NOTE: The director must ensure that the collection of policies and procedures is complete, current, and has been thoroughly reviewed by a knowledgeable person. Technical approaches must be scientifically valid and clinically relevant. To minimize the burden on the laboratory and reviewer(s), it is suggested that a schedule be developed whereby roughly 1/12 of all procedures are reviewed monthly. Paper/electronic signature review must be at the level of each procedure, or as multiple signatures on a listing of named procedures. A single signature on a Title Page or Index of all procedures is not sufficient documentation that each procedure has been carefully reviewed. Signature or initials on each page of a procedure is not required. COMMENTARY: N/A REFERENCES: 1) Department of Health and Human Services, Centers for Medicare and Medicaid Services. Clinical laboratory improvement amendments of 1988; final rule. Fed Register. 1992(Feb 28):7173 [42CFR493.1407(e)(13)]; 2) Borkowski A, et al. Intranet-based quality improvement documentation at the Veterans Affairs Maryland health care system. Mod. Pathol. 2001;14:1-5. ANP.04664 Phase II N/A YES NO If there is a change in directorship, does the new director ensure (over a reasonable period of time) that laboratory procedures are well-documented and undergo at least annual review? COMMENTARY:
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 10 of 95
N/A REFERENCE: Department of Health and Human Services, Centers for Medicare and Medicaid Services. Clinical laboratory improvement amendments of 1988; final rule. Fed Register. 2003(Jan 24):7164 [42CFR493.1251(d)]. ANP.05552 Phase II N/A YES NO When a procedure is discontinued, is a paper or electronic copy maintained for at least 2 years, recording initial date of use and retirement date? COMMENTARY: N/A REFERENCE: Department of Health and Human Services, Centers for Medicare and Medicaid Services. Clinical laboratory improvement amendments of 1988; final rule. Fed Register. 2003(Jan 24):7164 [42CFR493. 1105(a)(2); 493.1251(e)]. ANP.06440 Phase II N/A YES NO Does the laboratory have a system documenting that all personnel are knowledgeable about the contents of procedure manuals relevant to the scope of their testing activities? NOTE: This does not specifically require annual procedure sign-off by testing personnel. The form of this system is at the discretion of the laboratory director. COMMENTARY: N/A REFERENCES: 1) NCCLS. A Quality Management System Model for Health Care; Approved Guideline—Second Edition. NCCLS document HS1-A2 (ISBN 1-56238-554-2). NCCLS, 940 West Valley Road, Suite 1400, Wayne, Pennsylvania 19087-1898 USA, 2004.; 2) NCCLS. Application of a Quality Management System Model for Laboratory Services; Approved Guideline—Third Edition. NCCLS document GP26-A3 (ISBN 1-56238-553-4). NCCLS, 940 West Valley Road, Suite 1400, Wayne, Pennsylvania 19087-1898 USA, 2004. ANP.07328 Phase II N/A YES NO Is there a policy defining the handling of original slides/blocks for consultation and legal proceedings?
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 11 of 95
NOTE: This must include appropriate handling and documentation of the use, circulation, referral, transfer, and receipt of original slides and blocks. The laboratory must have a record of the location of original slides and blocks that have been referred for consultation or legal proceedings. COMMENTARY: N/A
*****************************************************************
SAFETY
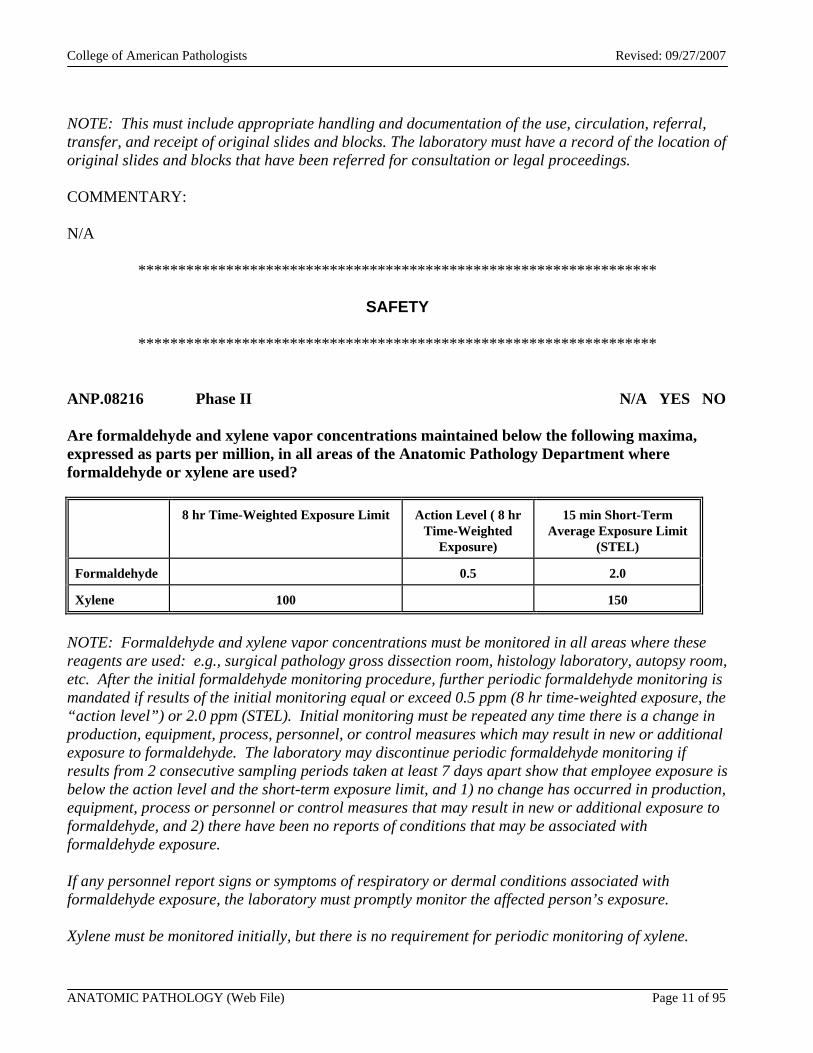
***************************************************************** ANP.08216 Phase II N/A YES NO Are formaldehyde and xylene vapor concentrations maintained below the following maxima, expressed as parts per million, in all areas of the Anatomic Pathology Department where formaldehyde or xylene are used?
8 hr Time-Weighted Exposure Limit Action Level ( 8 hr Time-Weighted
Exposure)
15 min Short-Term Average Exposure Limit
(STEL)
Formaldehyde 0.5 2.0
Xylene 100 150
NOTE: Formaldehyde and xylene vapor concentrations must be monitored in all areas where these reagents are used: e.g., surgical pathology gross dissection room, histology laboratory, autopsy room, etc. After the initial formaldehyde monitoring procedure, further periodic formaldehyde monitoring is mandated if results of the initial monitoring equal or exceed 0.5 ppm (8 hr time-weighted exposure, the “action level”) or 2.0 ppm (STEL). Initial monitoring must be repeated any time there is a change in production, equipment, process, personnel, or control measures which may result in new or additional exposure to formaldehyde. The laboratory may discontinue periodic formaldehyde monitoring if results from 2 consecutive sampling periods taken at least 7 days apart show that employee exposure is below the action level and the short-term exposure limit, and 1) no change has occurred in production, equipment, process or personnel or control measures that may result in new or additional exposure to formaldehyde, and 2) there have been no reports of conditions that may be associated with formaldehyde exposure. If any personnel report signs or symptoms of respiratory or dermal conditions associated with formaldehyde exposure, the laboratory must promptly monitor the affected person’s exposure. Xylene must be monitored initially, but there is no requirement for periodic monitoring of xylene.
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 12 of 95
COMMENTARY: N/A REFERENCES: 1) Montanaro A. Formaldehyde in the workplace and in the home. Exploring its clinical toxicology. Lab Med. 1996;27:752-757; 2) Goris JA. Minimizing the toxic effects of formaldehyde. Lab Med. 1997;29:39-42; 3) Wenk PA. Disposal of histology stains. Lab Med. 1998;29:337-338; 4) Occupational Safety and Health Administration. 29CFR1910.1048 and 1450, revised July 1, 1998. ANP.09104 Phase II N/A YES NO Is sufficient space available so that there is no compromise of the quality of work, (including quality control activities) or safety of personnel? NOTE: This checklist item applies to all areas of anatomic pathology. COMMENTARY: N/A REFERENCES: 1) NCCLS. A Quality Management System Model for Health Care; Approved Guideline—Second Edition. NCCLS document HS1-A2 (ISBN 1-56238-554-2). NCCLS, 940 West Valley Road, Suite 1400, Wayne, Pennsylvania 19087-1898 USA, 2004.; 2) NCCLS. Application of a Quality Management System Model for Laboratory Services; Approved Guideline—Third Edition. NCCLS document GP26-A3 (ISBN 1-56238-553-4). NCCLS, 940 West Valley Road, Suite 1400, Wayne, Pennsylvania 19087-1898 USA, 2004.
############################################################################
SURGICAL PATHOLOGY
############################################################################
****************************************************************************
QUALITY MANAGEMENT
**************************************************************************** Many technical and procedural quality control items are covered elsewhere in this Checklist. They are integral components of comprehensive quality management and should be included within the defined program. This section determines if there is an active program of surveillance of the quality of surgical pathology activities, particularly the diagnostic reports. How this is accomplished depends
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 13 of 95
upon the number of departmental staff, as well as the volume and type of diagnostic material. Such a program must include appropriate combinations of activities such as the use of intra- and extra-departmental consultations, circulation of diagnostic material (random or by case type), periodic review of completed surgical pathology reports, and participation in self-assessment and performance improvement programs. ANP.10000 Phase II N/A YES NO Is the quality management program defined and documented for surgical pathology? NOTE: The type of program may vary depending upon factors such as number of staff and workload. COMMENTARY: N/A REFERENCES: 1) Kempson RL. The time is now. Checklists for surgical pathology reports. Arch Pathol Lab Med. 1992;116:1107-1108; 2) Zarbo RJ. Interinstitutional assessment of colorectal carcinoma surgical pathology report adequacy. A College of American Pathologists Q-Probes study of practice patterns from 532 laboratories and 15 940 reports. Arch Pathol Lab Med. 1992;116:1113-1119; 3) Shaw PA. Launching quality improvement in histology. Med Lab Observ. 1993(Mar):45-49; 4) Abt AB, et al. The effect of interinstitution anatomic pathology consultation on patient care. Arch Pathol Lab Med. 1995;119:514-517; 5) Scully RE, et al. Practice protocol for the examination of specimens removed from patients with ovarian tumors. A basis for checklists. Arch Pathol Lab Med. 1995;119:1012-1022; 6) Gephardt GN, Zarbo RJ. Interinstitutional comparison of frozen section consultations. A College of American Pathologists Q-Probes study of 90538 cases in 461 institutions. Arch Pathol Lab Med. 1996;120:804-809; 7) Zarbo RJ. Quality assessment in anatomic pathology in the cost-conscious era. Am J Clin Pathol. 1996;106(Suppl 1):s3-s10; 8) Novis DA, et al. Interinstitutional comparison of frozen section consultation in small hospitals. A College of American Pathologists Q-Probes study of 18 532 frozen section consultation diagnoses in 233 small hospitals. Arch Pathol Lab Med. 1996;120:1087-1093; 9) Hammond EH, et al. Practice protocol for the examination of specimens removed from patients with carcinoma of the urinary bladder, ureter, renal pelvis, and urethra. Arch Pathol Lab Med. 1996;120:1103-1110; 10) Novis DA, Zarbo RJ. Interinstitutional comparison of frozen section turnaround time. A College of American Pathologists Q-Probes of 32 868 frozen sections in 700 hospitals. Arch Pathol Lab Med. 1997;121:559-567; 11) Lee RG, et al. Protocol for the examination of specimens removed from patients with esophageal carcinoma. A basis for checklists. Arch Pathol Lab Med. 1997;121:925-929; 12) Novis DA, et al. Interinstitutional comparison of surgical biopsy diagnosis turnaround time. A College of American Pathologists Q-Probes study of 5384 surgical biopsies in 157 small hospitals. Arch Pathol Lab Med. 1998;122:951-956; 13) Compton CC, et al. Updated protocol for the examination of specimens from patients with carcinomas of the colon and rectum, excluding carcinoid tumors, lymphomas, sarcomas, and tumors of the vermiform appendix: a basis for checklists. Arch Pathol Lab Med. 2000;124:1016-1025; 14) Cruz DC, et al. Digital image documentation for quality assessment. Arch Pathol Lab Med. 2001;125:1430-1435; 15) Cooper K, et al. Institutional consultations in surgical pathology. How should diagnostic disagreements be handled? Arch Pathol Lab Med. 2002;126:650-651; 16) Nakhleh
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 14 of 95
RE, Fitzgibbons PL, editors. College of American Pathologists. Quality improvement manual in anatomic pathology, second edition. Northfield, IL: CAP, 2002; 17) Renshaw AA, et al. Blinded review as a method of quality improvement in surgical pathology. Arch Pathol Lab Med. 2002;126:961-963; 18) Rüdiger T, et al. Quality assurance in immunohistochemistry: results of an interlaboratory trial involving 172 pathologists. Am J Surg Pathol. 2002;26:873-882. ANP.10016 Phase I N/A YES NO Is there a policy that lists types of specimens (if any) that an institution may choose to exclude from routine submission to the pathology department for examination, and for recording their disposition? NOTE: Specimens removed during surgery are ordinarily sent to a pathologist for evaluation, but there may be policy exceptions. Such a policy is neither mandatory nor a requirement for CAP accreditation. If all specimens are sent to the pathologist, this question is "N/A". If there is a policy, it should be made in conjunction with the hospital administration and appropriate medical staff departments. The laboratory director must have participated in or been consulted by the medical staff in deciding which surgical specimens are to be sent to the laboratory for examination. If certain types of specimens (e.g., dental appliances, pacemakers, bone donated to the bone bank, neonatal foreskins) are not routinely submitted for pathologist examination, there must be an alternative procedure for documenting the removal and disposition of such specimens. COMMENTARY: N/A REFERENCES: 1) Kassan MA, et al. Value of routine pathology in herniorrhaphy performed upon adults. Surg Gynecol Obstet. 1986;163:518-522; 2) Netser JC, et al. Value-based pathology: a cost-benefit analysis of the examination of routine and non-routine tonsil and adenoid specimens. Am J Clin Pathol. 1997;108:158-165; 3) Zarbo RJ, Nakleh RE. Surgical pathology specimens for gross examination only and exempt from submission. A College of American Pathologists Q-Probes study of current policies in 413 institutions. Arch Pathol Lab Med. 1999;123:133-139; 4) College of American Pathologists. Policies and guidelines manual. Surgical specimens to be submitted to pathology for examination. Northfield, IL: CAP, 1999:Appendix M; 5) Nakhleh RE, Fitzgibbons PL, editors. College of American Pathologists. Quality improvement manual in anatomic pathology, second edition. Northfield, IL: CAP, 2002. ANP.10032 Phase I N/A YES NO Is there a policy regarding what types of surgical specimens (if any) may be exempt from microscopic examination? NOTE: Such a policy is recommended as good laboratory practice but is not a requirement for CAP accreditation. Irrespective of any exemptions, microscopic examination should be performed
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 15 of 95
whenever there is a request by the attending physician, or at the discretion of the pathologist when indicated by the clinical history or gross findings. If there is such a policy, it should be approved by the medical staff or appropriate committee. Typical exempt specimens include foreskins in children, prosthetic cardiac valves without attached tissue, torn meniscus, varicose veins, tonsils in children below a certain age, etc. COMMENTARY: N/A REFERENCES: 1) Weibel E. Pathological findings of clinical value in tonsils and adenoids. Acta Otolaryngol. 1965;60:331-338; 2) Wolkomir AF, et al. Selective microscopic examination of gallbladders, hernia sacs and appendices. Am Surg. 1991:57:289-292; 3) Boutin P, Hogshead H. Surgical pathology of the intervertebral disc: is routine examination necessary? Spine. 1992;17:1236-1238; 4) Cornell WB, Levin HS. The inguinal hernia sac: trash or treasure? Anatomic pathology II check sample, APII-9. Chicago, IL: American Society of Clinical Pathology, 1993:17(4); 5) Delong WH, Grignon DJ. Pathologic findings in ribs removed at the time of radical nephrectomy for renal cell carcinoma. Int J Surg Pathol. 1994;1:177-180; 6) Raab SS. The cost-effectiveness of routine histologic examination. Am J Clin Pathol. 1998;110:391-396; 7) Zarbo RJ, Nakleh RE. Surgical pathology specimens for gross examination only and exempt from submission. A College of American Pathologists Q-Probes study of current policies in 413 institutions. Arch Pathol Lab Med. 1999;123:133-139; 8) College of American Pathologists. Policies and guidelines manual. Surgical specimens to be submitted to pathology for examination. Northfield, IL: CAP, 1999:Appendix M. ANP.10050 Phase II N/A YES NO Whenever possible, is pertinent previous cytologic and/or histologic material from the patient reviewed with current material being examined? NOTE: Because sequential analysis of cytologic and histologic specimens may be critical in patient management and follow-up, efforts must be made to routinely review pertinent previous material. COMMENTARY: N/A REFERENCE: Bozzo P. Implementing quality assurance. Chicago, IL: American Society of Clinical Pathology, 1991:72-74. ANP.10100 Phase II N/A YES NO When significant disparities exist between initial intraoperative consultation (e.g., frozen section, cytology, gross evaluation) and final pathology diagnosis, are these reconciled and documented either in the surgical pathology report or in the departmental quality management file?
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 16 of 95
COMMENTARY: N/A REFERENCES: 1) Gephardt GN, Zarbo RJ. Interinstitutional comparison of frozen section consultations. A College of American Pathologists Q-Probes study of 90 538 cases in 461 institutions. Arch Pathol Lab Med. 1996;120:804-809; 2) Nakhleh RE, Zarbo RJ. Amended reports in surgical pathology and implications for diagnostic error detection and avoidance. A College of American Pathologists Q-Probes study of 1 667 547 accessioned cases in 359 laboratories. Arch Pathol Lab Med. 1998;122:303-309; 3) Firlik KS, et al. Use of cytological preparations for the intraoperative diagnosis of stereotactically obtained brain biopsies: a 19-year experience and survey of neuropathologists. J Neurosurg. 1999;91:454-458. ANP.10150 Phase II N/A YES NO Does the laboratory have a policy for inclusion of INTRA-departmental consultations in the patient's final report? NOTE: Intradepartmental consultations may be included in the patient’s final report, or filed separately. The pathologist in charge of the surgical pathology case must decide whether the results of intra-departmental consultations provide relevant information for inclusion in some manner in the patient's report. COMMENTARY: N/A REFERENCES: 1) Leslie KO, et al. Second opinions in surgical pathology. Am J Clin Pathol. 1996;106(suppl 1):S58-S64; 2) Tomaszewski JE, et al. Consensus conference on second opinions in diagnostic anatomic pathology. Who, what, and when. Am J Clin Pathol. 2000;114:329-335; 3) Hahm GK, et al. Quality assurance of second opinion in gastrointestinal and liver pathology. Am J Clin Pathol. 2000;114:631; 4) Renshaw AA, et al. Blinded review as a method of quality improvement in surgical pathology. Arch Pathol Lab Med. 2002;126:961-963. ANP.10200 Phase II N/A YES NO Are EXTRA-departmental consultations documented, and are records of these consultations maintained in a systematic manner within the pathology department? NOTE: Documentation of extra-departmental consultations must be readily accessible within the pathology department. The method used to satisfy this requirement is at the discretion of the laboratory director, and can be expected to vary according to the organization of the department.
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 17 of 95
These consultations can be maintained with the official surgical pathology reports or kept separately, so long as they can be readily linked. COMMENTARY: N/A REFERENCES: 1) Leslie KO, et al. Second opinions in surgical pathology. Am J Clin Pathol. 1996;106(suppl 1):S58-S64; 2) Tomaszewski JE, et al. Consensus conference on second opinions in diagnostic anatomic pathology. Who, what, and when. Am J Clin Pathol. 2000;114:329-335; 3) Hahm GK, et al. Quality assurance of second opinion in gastrointestinal and liver pathology. Am J Clin Pathol. 2000;114:631; 4) Azam M, Nakhleh RE. Surgical pathology extradepartmental consultation practices. A College of American Pathologists Q-probes study of 2746 consultations from 180 laboratories. Arch Pathol Lab Med. 2002;126:405-412; 5) Cooper K, et al. Institutional consultations in surgical pathology. How should diagnostic disagreements be handled? Arch Pathol Lab Med. 2002;126:650-651. ANP.10250 Phase I N/A YES NO When extra-departmental cases are submitted to the laboratory for consultation, are they accessioned according to the standard practices of the laboratory, and is a documented report prepared, with a copy sent to the original pathologist? NOTE: Extra-departmental cases submitted for consultation should be accessioned according to the standard practices of the laboratory, and a report issued. A copy of this report should be sent to the original pathologist. In most cases, original materials including slides and blocks should be promptly returned to the original institution. However, in some situations (for example, when the patient is receiving ongoing care at the referral institution pending tumor resection, etc.) it may be appropriate for the referral laboratory to retain slides/blocks for a period of time. In such situations, a letter should be sent to the original pathologist along with the consultation report, requesting permission to retain the slides/blocks and accepting transfer of stewardship of the patient materials from the original laboratory to the referral institution. COMMENTARY: N/A REFERENCE: Stewardship of Pathologic Specimens. Policy Statement. College of American Pathologists, Waukegan, IL. Adopted February 1997. Reaffirmed May 2000. http://www.cap.org/apps/docs/policies/policy_appF.htm.
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 18 of 95
****************************************************************************
QUALITY CONTROL
**************************************************************************** ----------------------------------------------------------------- SURGICAL SPECIMEN EXAMINATION ----------------------------------------------------------------- Inspectors and laboratories are reminded that questions relating to collection and accessioning of specimens are covered in the Laboratory General Checklist. During the on-site inspection, the handling of surgical specimens must be evaluated. ANP.11200 Phase I N/A YES NO Is there sufficient space and are utilities (water, drainage, electrical power) adequate for collection, gross examination, and storage of specimens? COMMENTARY: N/A REFERENCES: 1) NCCLS. A Quality Management System Model for Health Care; Approved Guideline—Second Edition. NCCLS document HS1-A2 (ISBN 1-56238-554-2). NCCLS, 940 West Valley Road, Suite 1400, Wayne, Pennsylvania 19087-1898 USA, 2004.; 2) NCCLS. Application of a Quality Management System Model for Laboratory Services; Approved Guideline—Third Edition. NCCLS document GP26-A3 (ISBN 1-56238-553-4). NCCLS, 940 West Valley Road, Suite 1400, Wayne, Pennsylvania 19087-1898 USA, 2004. ANP.11250 Phase I N/A YES NO Is refrigerated storage available for large or unfixed specimens? COMMENTARY: N/A ANP.11275 Phase II N/A YES NO Are there specific policies and procedures for the safe handling of tissues that may contain radioactive material (e.g., sentinel lymph nodes, breast biopsies, prostate "seeds", etc.)?
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 19 of 95
NOTE: These procedures should be developed in conjunction with the institutional radiation safety officer, and must comply with any state regulations for the safe handling of tissues containing radionuclides. The policy should distinguish between low radioactivity specimens such as sentinel lymphadenectomy and implant devices with higher radiation levels. The pathology department may wish to monitor these specimens for radioactivity, with safe storage of specimens until sufficient decaying has occurred, before proceeding with processing in the histology laboratory. COMMENTARY: N/A REFERENCES: 1) Glass EC, et al. Editorial: radiation safety considerations for sentinel node techniques. Ann Surg Oncol. 1999:6:10; 2) Miner TJ, et al. Guideline for the safe use of radioactive materials during localization and resection of sentinel lymph nodes. Ann Surg Oncol. 1999;6:75-82; 3) Cibull ML. Handling sentinel lymph node biopsy specimens. A work in progress. Arch Pathol Lab Med. 1999;123:620-621; 4) Pfeifer JD. Sentinel lymph node biopsy. Am J Clin Pathol. 1999;112:599-602; 5) Barnes CA. False-negative frozen section results. Am J Clin Pathol. 2000;113:900; 6) Fitzgibbons PL, et al. Recommendations for handling radioactive specimens obtained by sentinel lymphadenectomy. Am J Surg Pathol. 2000;24:1549-1551. ANP.11300 Phase I N/A YES NO Is the lighting satisfactory? NOTE: Direct sunlight should be avoided because of its extreme variability and the need for low light levels necessary to observe various computer consoles, etc. Lighting control should be sectionalized so general levels of illumination can be controlled in areas of the room if desired. COMMENTARY: N/A ANP.11350 Phase II N/A YES NO Are the examination and storage areas adequately ventilated by an exhaust fan or fume hood to remove noxious fumes and odors? COMMENTARY: N/A
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 20 of 95
ANP.11400 Phase I N/A YES NO Are dictating facilities available and convenient to use? COMMENTARY: N/A ANP.11450 Phase I N/A YES NO Are photographic facilities available and convenient? NOTE: In addition to providing material for a teaching collection, such photographs can serve as valuable documentation for the report. COMMENTARY: N/A ANP.11475 Phase I N/A YES NO Are there documented procedures for handling sub-optimal specimens (e.g., specimens that are unlabeled, unaccompanied by adequate requisition information, left unfixed or unrefrigerated for an extended period, received in a container/bag with a contaminated outside surface)? COMMENTARY: N/A ANP.11500 Phase II N/A YES NO Is the identity of every specimen maintained at all times during the processing and examination steps? COMMENTARY: N/A
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 21 of 95
ANP.11550 Phase I N/A YES NO Are all gross specimens retained until at least 2 weeks after the final reports are signed and results reported to the referring physician? COMMENTARY: N/A REFERENCES: 1) Travers H. Q&A Section. Northfield, IL: College of American Pathologists CAP Today, March 1992:63; 2) Travers H. Q&A Section. Savage RA, editor. CAP Today, November 1993:86-87; 3) Tracey ME. Hospital takes closer look at specimen returns. CAP Today, July 1992:81; 4) Lester SC. Manual of surgical pathology. New York, NY: Churchill Livingstone, 2001:18-20; 5) Nakhleh RE, Fitzgibbons PL. Quality improvement manual in anatomic pathology, second edition. Northfield, IL: CAP; 2002:14. **REVISED** 12/12/2006 ANP.11600 Phase II N/A YES NO Are all macroscopic tissue examinations performed by a pathologist or pathology resident, or under the supervision of a qualified pathologist? NOTE: Two levels of complexity of macroscopic tissue examination are defined, as follows: 1) Processing is defined as a tissue examination limited to description, inking and cutting of the specimen (if applicable), and submission of the entire specimen to histology. Tissue processing can be performed according to standardized protocols. Processing is generally limited to small specimens (skin ellipses, small biopsies, curettings, etc.) and does not require knowledge of anatomy. 2) Grossing (or gross examination) is defined as a tissue examination requiring a greater exercise of judgment and a knowledge of anatomy. Dissection of the specimen and selection of tissue samples for submission to histology are generally required. The specimen description is not necessarily standardized. Specific requirements for supervision of non-pathologists who process specimens, or assist in grossing specimens, are given below. COMMENTARY: N/A
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 22 of 95
**REVISED** 12/12/2006 ANP.11605 Phase II N/A YES NO When individuals other than a pathologist or pathology resident process specimens, or assist in gross examinations, is the extent of their activities (including the types of specimens examined) defined in a documented protocol? NOTE: This protocol must list the specific types of specimens that non-pathologists are permitted to process, and for which non-pathologists are permitted to assist in the gross examination. The laboratory director is responsible for this protocol. COMMENTARY: N/A REFERENCES: 1) Department of Health and Human Services, Centers for Medicare and Medicaid Services. Clinical laboratory improvement amendments of 1988; final rule. Fed Register. 1992(Feb 28):7183 [42CFR493.1489(b)(6)]; 2) Cibull ML. Q&A. Northfield, IL: College of American Pathologists CAP Today. 1997;11(7):112; 3) Grzybicki DM, et al. National practice characteristics and utilization of pathologists’ assistants. Arch Pathol Lab Med. 2001;125:905-912. ANP.11610 Phase II N/A YES NO If individuals other than a pathologist or pathology resident assist in gross examinations, do such individuals qualify as high complexity testing personnel under CLIA-88 regulations? NOTE: The laboratory director may delegate the dissection of specimens to non-pathologist individuals; these individuals must be qualified as high complexity testing personnel under CLIA-88 regulations. The minimum training/experience required of such personnel is:
1. An earned associate degree in a laboratory science or medical laboratory technology, obtained from an accredited institution, OR
2. Education/training equivalent to the above that includes at least 60 semester hours or equivalent from an accredited institution. This education must include 24 semester hours of medical laboratory technology courses, OR 24 semester hours of science courses that includes 6 semester hours of chemistry, 6 semester hours of biology, and 12 semester hours of chemistry, biology or medical laboratory technology in any combination. In addition, the individual must have laboratory training including either completion of a clinical laboratory training program approved or accredited by the ABHES, NAACLA, or other organization approved by HHS (note that this training may be included in the 60 semester hours listed above), OR at least 3 months documented laboratory training in each specialty in which the individual performs high complexity testing.
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 23 of 95
The CLIA-88 regulations on high complexity testing personnel may be found at http://ecfr.gpoaccess.gov/cgi/t/text/text-idx?c=ecfr&sid=9fcc70f1174dc1686ebba1e853afc7b5&rgn=div8&view=text&node=42:4.0.1.5.29.13.223.42&idno=42
In addition, the CLIA-88 regulations include exceptions for grandfathered individuals; these regulations (42CFR493.1489 and 1491) may be found at the above Web address and at http://ecfr.gpoaccess.gov/cgi/t/text/text-idx?c=ecfr&sid=c9d60c9da737b7fbbc6f43fc4d3485c9&rgn=div8&view=text&node=42:4.0.1.5.29.13.223.43&idno=42 It is the responsibility of the laboratory director to determine whether an individual’s education, training and experience satisfies the requirements of this checklist question. This checklist question applies only to laboratories subject to CLIA-88. COMMENTARY: N/A REFERENCES: 1) Department of Health and Human Services, Centers for Medicare and Medicaid Services. Clinical laboratory improvement amendments of 1988; final rule. Fed Register. 2003(Oct 1):1070-1071 [42CFR493.1489], 1071-1072 [42CFR493.1491]; 2) http://www.naacls.org/news/naacls-news/archives.asp?article_id=599. ANP.11630 Phase II N/A YES NO When individuals other than pathologists or pathology residents process specimens or assist in gross examinations, is the nature of the pathologist supervision (direct vs. indirect) clearly documented for each type of specimen? NOTE: The laboratory director must determine the nature of supervision for each specimen type. The nature of the supervision must be established individually, for each non-pathologist. COMMENTARY: N/A REFERENCES: 1) Department of Health and Human Services, Centers for Medicare and Medicaid Services. Clinical laboratory improvement amendments of 1988; final rule. Fed Register. 1992(Feb 28):7183 [42CFR493.1489(b)(6)]; 2) Cibull ML. Q&A. Northfield, IL: College of American Pathologists CAP Today. 1997;11(7):112; 3) Grzybicki DM, et al. The usefulness of pathologists' assistants. Am J Clin Pathol. 1999;112:619-626.
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 24 of 95
ANP.11640 Phase II N/A YES NO Is the performance of non-pathologist(s) who process specimens and assist in the performance of gross tissue examinations evaluated by the pathologist on a regular, periodic basis? COMMENTARY: N/A REFERENCES: 1) Cibull ML. Q&A. Northfield, IL: College of American Pathologists CAP Today. 1997;11(7):112; 2) Grzybicki DM, et al. The usefulness of pathologists' assistants. Am J Clin Pathol. 1999;112:619-626; 3) Galvis CO, et al. Pathologists’ assistants practice. A measurement of performance. Am J Clin Pathol. 2001;116:816-822. ANP.11660 Phase II N/A YES NO Are all surgical tissue diagnoses made by a pathologist? COMMENTARY: N/A REFERENCE: Cibull ML. Q&A. Northfield, IL: College of American Pathologists CAP Today. 1997;11(7):112. **NEW** 12/12/2006 ANP.11665 Phase I N/A YES NO Are there written procedures for processing specimens? NOTE: This question refers to processing as defined in ANP.11600, and applies only to processing of specimens by non-pathologist individuals who are not qualified as high complexity testing personnel under CLIA-88. COMMENTARY: N/A
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 25 of 95
ANP.11670 Phase I N/A YES NO Are documented instructions or guidelines available for the proper dissection, description, and histologic sampling of various specimen types (e.g., mastectomy, colectomy, hysterectomy, renal biopsy, etc.)? NOTE: The guidelines should address large or complicated specimen types and smaller specimens requiring special handling, such as muscle biopsies, renal biopsies, and rectal suction biopsies for Hirschsprung's disease. Guidelines serve an important educational function in departments with postgraduate (residency) programs. However, they also are useful in providing consistency in the handling of similar specimen types in departments without such training programs. COMMENTARY: N/A ANP.11713 Phase II N/A YES NO Is there documented evidence of daily review of the technical quality of histologic preparations by the pathologist? NOTE: If specimens are referred to an outside laboratory for histologic processing, there must be a procedure for providing feedback on slide quality to the outside laboratory. This checklist question is intended to apply to routine histology slides. Specific quality control requirements for special stains, immunohistochemistry, and other special studies are found elsewhere in this checklist. COMMENTARY: N/A ----------------------------------------------------------------- INTRAOPERATIVE CONSULTATION (RAPID DIAGNOSIS OR FROZEN SECTION) ----------------------------------------------------------------- ANP.11756 Phase II N/A YES NO Are all working solutions and stains properly labeled? NOTE: Working solutions and stains must be properly labeled with the contents, and, if applicable, date they are changed/filtered, and expiration date.
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 26 of 95
COMMENTARY: N/A ANP.11800 Phase II N/A YES NO Is each slide labeled with patient's name and/or accession number? COMMENTARY: N/A ANP.11810 Phase II N/A YES NO Are frozen section preparations adequate for intraoperative diagnosis? NOTE: The inspector should evaluate several cases for quality of histological sectioning and staining. COMMENTARY: N/A ANP.11820 Phase I N/A YES NO Does the laboratory periodically evaluate turnaround time for intraoperative frozen sections? NOTE: If 90% of frozen sections are not completed within 20 minutes, the laboratory must document evaluation of the reason(s) for the delay. This turnaround time is intended to apply to the typical single frozen section. In cases where there are multiple sequential frozen sections required on a single specimen (e.g., resection margins), or in cases where additional studies such as radiographic correlation are required, longer turnaround times may be expected. COMMENTARY: N/A REFERENCE: Novis DA, Zarbo RJ. Interinstitutional comparison of frozen section turnaround time. A College of American Pathologists Q-Probes study of 32 868 frozen sections in 700 hospitals. Arch Pathol Lab Med. 1997;121:559-567.
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 27 of 95
ANP.11850 Phase II N/A YES NO Are the results of surgical consultations documented and signed by the pathologist who made the diagnosis? NOTE: The intent of this question is for the laboratory to maintain a contemporaneous report of the surgical consultation. This may be a handwritten, signed report or a computer-generated report with electronic signature. COMMENTARY: N/A ANP.11900 Phase II N/A YES NO If verbal reports are given, is the pathologist able to speak directly with the surgeon? COMMENTARY: N/A ANP.11950 Phase II N/A YES NO Is the patient's identification checked and confirmed before delivery of any verbal report? COMMENTARY: N/A ANP.12000 Phase II N/A YES NO Are all intraoperative consultation reports made a part of the final surgical pathology report? COMMENTARY: N/A ANP.12050 Phase II N/A YES NO Are all frozen section slides permanently stained, mounted, properly labeled, and retained with the rest of the slides from the case?
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 28 of 95
COMMENTARY: N/A REFERENCE: Nakhleh RE, Fitzgibbons PL, editors. College of American Pathologists. Quality improvement manual in anatomic pathology, second edition. Northfield, IL: CAP, 2002. ANP.12075 Phase I N/A YES NO Following frozen section examination, is the residual frozen tissue routinely processed and a paraffin section prepared for comparison with the intraoperative interpretation? NOTE: Correlation of frozen section findings with a permanent section prepared from routinely fixed and processed residual frozen tissue is an important quality assurance and improvement mechanism. Evaluation of such permanent sections improves recognition of specific frozen section morphologic alterations and provides important feedback regarding diagnostic accuracy. For some evaluations (e.g., margin assessment), the findings on deeper permanent sections from residual frozen material may not be as clinically relevant as the original frozen section. Also, in some cases, the frozen tissue may be required for specialized studies. For these situations, the laboratory should have a policy specifying the types of specimens for which permanent section follow-up is not performed. COMMENTARY: N/A REFERENCES: 1) Rickert RR. Quality assurance goals in surgical pathology. Arch Pathol Lab Med. 1990;114:1157-1162; 2) Association of Directors of Anatomic and Surgical Pathology. Recommendations on quality control and quality assurance in anatomic pathology. Am J Surg Pathol. 1991;15:1007-1009; 3) Gephardt GN, et al. Interinstitutional comparison of frozen section consultations. A College of American Pathologists Q-probes study of 90 538 cases in 461 institutions. Arch Pathol Lab Med. 1996;120:804-809; 4) Novis DA, et al. Interinstitutional comparison of frozen section consultation in small hospitals. Arch Pathol Lab Med. 1996;120:1087-1093; 5) Nakhleh RE, Fitzgibbons PL, editors. College of American Pathologists. Quality improvement manual in anatomic pathology, second edition. Northfield, IL: CAP, 2002. ANP.12087 Phase II N/A YES NO Is there a documented procedure for the routine decontamination of the cryostat at defined intervals, and are decontamination records evident? NOTE: Decontamination of the interior of cryostats may be accomplished with 70% ethanol. Trimmings and sections of tissue that accumulate inside the cryostat should be removed during decontamination. In addition to this decontamination process, the cryostat should be defrosted and
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 29 of 95
decontaminated with a tuberculocidal disinfectant at an interval appropriate for the institution; this should be weekly for instruments used daily. Although not a requirement, steel mesh gloves should be worn when changing knife blades. COMMENTARY: N/A REFERENCE: NCCLS. Protection of laboratory workers from instrument biohazards and infectious disease transmitted by blood, body fluids, and tissue; approved guideline M29-A. Wayne, PA: NCCLS, 1997. ----------------------------------------------------------------- SURGICAL PATHOLOGY REPORTS ----------------------------------------------------------------- ANP.12100 Phase II N/A YES NO Are all reports reviewed and signed by the pathologist? NOTE: The inspector must review 15-20 recent surgical pathology reports. When diagnostic reports are generated by computer or telecommunications equipment, the actual signature or initials of the pathologist may not appear on the report. It is nevertheless essential that the laboratory have a procedure that ensures and documents that the responsible pathologist has reviewed and approved the completed report before its release. In the occasional situation when the diagnosing pathologist is not available for timely review and approval of the completed report, the laboratory may have a policy and procedure for review and approval of that report by another pathologist. In that circumstance, the names and responsibilities of both the pathologist who made the diagnosis and the pathologist who performs final verification must appear on the report . COMMENTARY: N/A REFERENCE: http://www.cap.org/apps/docs/laboratory_accreditation/RetentionGuidelines010405.pdf. ANP.12150 Phase II N/A YES NO Are reports on routine cases completed within 2 working days? NOTE: Unusual, complex or special specimens may require prolonged fixation before dissecting and selecting tissue samples, additional time for special stains, etc., and the reporting time may extend
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 30 of 95
beyond 2 working days of receipt by the laboratory conducting the surgical pathology examination. This question is primarily concerned with routine specimens, and applies to all laboratories. COMMENTARY: N/A REFERENCES: 1) Zarbo RJ, et al. Intralaboratory timeliness of surgical pathology reports. Results of two College of American Pathologists Q-Probes studies of biopsies and complex specimens. Arch Pathol Lab Med. 1996;120:234-244; 2) Smith MT, Garvin AJ. Anatomic pathology turnaround times. Use and abuse. Am J Clin Pathol. 1996;106(suppl 1):S70-S73; 3) Novis DA, et al. Interinstitutional comparison of surgical biopsy diagnosis turnaround time. A College of American Pathologists Q-Probes study of 5384 surgical biopsies in 157 small hospitals. Arch Pathol Lab Med. 1998;122:951-956. ANP.12175 Phase I N/A YES NO Is there a policy regarding the timely communication, and documentation thereof, of significant or unexpected surgical pathology findings? NOTE: Certain surgical pathology diagnoses may be considered particularly significant or unexpected. Such diagnoses may include: malignancy in an uncommon location or specimen type (e.g., hernia sac, intervertebral disk material, tonsil, etc.), absence of chorionic villi when clinically expected (potential ectopic pregnancy), change of a frozen section diagnosis after review of permanent sections, and/or mycobacterial, fungal or other significant infectious organisms identified on special stains. Diagnoses to be defined as “significant” or “unexpected,” if any, should be determined by the pathology department, in cooperation with local clinical medical staff. Consideration should be given to assuring, with reasonable effort, prompt communication of such results, by telephone, pager, or other system. There should be documentation of date and time of such special notification (which may be included in the pathology report or in laboratory files). COMMENTARY: N/A REFERENCES: 1) Rosai J, Bonfiglio TA, Corson JM, et al. Standardization of the surgical pathology report. Mod Pathol.1992 Mar;5(2):197-9; 2) Zarbo RJ, Nakhleh RE, Walsh M; Quality Practices Committee, College of American Pathologists. Customer satisfaction in anatomic pathology. A College of American Pathologists Q-Probes study of 3065 physician surveys from 94 laboratories. Arch Pathol Lab Med. 2003 Jan;127(1):23-9.
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 31 of 95
ANP.12200 Phase II N/A YES NO Do all surgical pathology reports include gross descriptions that contain adequate information regarding type, number, dimensions and/or weight of specimens, measurements and extent of gross lesions, and other information essential to the diagnosis and patient care? NOTE: Annotated drawings and photographs are valuable tools for documenting gross findings, but are not adequate replacements for a text description. COMMENTARY: N/A REFERENCES: 1) Association of Directors of Anatomic and Surgical Pathology. Recommendations for the reporting of resected large intestinal carcinomas. Am J Clin Pathol. 1996;106:12-15; 2) Imperato PJ, et al. Radical prostatectomy specimens among Medicare patients in New York State. A review of pathologists' reports. Arch Pathol Lab Med. 1998;122:966-971; 3) Cochran AJ, et al. Recommendations for the reporting of tissues removed as part of the surgical treatment of cutaneous melanoma. Am J Clin Pathol. 1998;110:719-722; 4) Ruby SG. Clinician interpretation of pathology reports. Confusion or comprehension? Arch Pathol Lab Med. 2000;124:943-944; 5) Powsner SM, et al. Clinicians are from Mars and pathologists are from Venus. Clinician interpretation of pathology reports. Arch Pathol Lab Med. 2000;124:104-1046. ANP.12250 Phase II N/A YES NO When appropriate, do gross descriptions include a key or summary noting block and slide designations for special sections (e.g., margins of resection, deepest penetration of tumor, breast quadrants, lymph node levels, etc.)? COMMENTARY: N/A REFERENCE: Imperato PJ, et al. Radical prostatectomy specimens among Medicare patients in New York State. A review of pathologists' reports. Arch Pathol Lab Med. 1998;122:966-971. ANP.12300 Phase II N/A YES NO Do gross descriptions and microscopic findings (if included) support the pathologic diagnosis? COMMENTARY: N/A
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 32 of 95
REFERENCE: Rickert RR. Quality Assurance in Surgical Pathology. Arch Pathol Lab Med 1990;114:1157-1162. **REVISED** 12/12/2006 ANP.12350 Phase II N/A YES NO For specimens from definitive cancer resections, and in specific biopsies as outlined in the CAP Cancer Protocols, are all scientifically validated data elements needed for standard systems of grading, staging and prognostication included in the pathology report? NOTE: The pathology report must provide data that, within the confines of information available to the pathologist, is sufficient to allow appropriate grading and staging of neoplasms according to standard classification schemes. Lists of the scientifically validated data elements may be found in the CAP Cancer Protocols and Checklists. The use of these checklists is encouraged, but not required, providing that the required data elements are present in the report. The use of synoptic diagnostic reports is recommended, to ensure that all information relevant to staging and grading is included, and to facilitate interpretation of pathology reports by clinicians. COMMENTARY: N/A REFERENCE: College of American Pathologists. Practicing Pathology: Cancer Protocols. http://www.cap.org/cancerprotocols/protocols/intro.html. ANP.12400 Phase II N/A YES NO Is there a mechanism to correlate the results of specialized studies (e.g., immunohistochemistry, nucleic acid probes, cytogenetics, flow cytometry, electron microscopy) with the morphologic diagnosis? NOTE: It is not in the best interests of the patient to have potentially conflicting diagnoses or interpretations rendered by different sections of the laboratory. The pathologist should issue a report reconciling potentially conflicting data, when appropriate. COMMENTARY: N/A REFERENCES: 1) Editorial. Incorporation of immunostaining data in anatomic pathology reports. Am J Clin Pathol. 1993;99:1; 2) Putti T, et al. Cost-effectiveness of immunohistochemistry in surgical pathology. Am J Clin Pathol. 1998;110:51; 3) Raab SS. The cost-effectiveness of immunohistochemistry. Arch Pathol Lab Med. 2000;124:1185-1191.
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 33 of 95
ANP.12425 Phase II N/A YES NO If patient testing is performed using Class I analyte-specific reagents (ASR’s) obtained or purchased from an outside vendor, does the patient report include the disclaimer required by federal regulations? NOTE: ASR’s are antibodies, both polyclonal and monoclonal, specific receptor proteins, ligands, nucleic acid sequences, and similar reagents which, through specific binding or chemical reaction with substances in a specimen, are intended for use in a diagnostic application for identification and quantification of an individual chemical substance or ligand in biological specimens. By definition, an ASR is the active ingredient of a laboratory-developed test system. ASR’s may be obtained from outside vendors or synthesized in-house. ASR’s from outside vendors are supplied individually. They are not bundled with other materials in kit form, and the accompanying product literature does not include any claims with respect to use or performance of the reagent. Class I ASR’s in use in the anatomic pathology laboratory include some antibodies for immunohistochemistry and nucleic acid probes for FISH and ISH. Class I ASR’s are not subject to preclearance by the U.S. Food and Drug Administration or to special controls by FDA. Thus, if the laboratory performs patient testing using Class I ASR’s obtained or purchased from an outside vendor, federal regulations require that the following disclaimer accompany the test result on the patient report:
"This test was developed and its performance characteristics determined by (laboratory name). It has not been cleared or approved by the U.S. Food and Drug Administration."
The CAP recommends additional language, such as "The FDA has determined that such clearance or approval is not necessary. This test is used for clinical purposes. It should not be regarded as investigational or for research. This laboratory is certified under the Clinical Laboratory Improvement Amendments of 1988 (CLIA-88) as qualified to perform high complexity clinical laboratory testing." The above disclaimer is not required when using reagents that are sold in kit form with other materials and/or an instrument, and/or with instructions for use, and/or when labeled by the manufacturer as Class I for in vitro diagnostic use (IVD), Class II IVD, or Class III IVD. Most antibodies used in immunohistochemistry are labeled “for in vitro diagnostic use” and thus do NOT require the disclaimer. Antibodies, nucleic acid sequences, etc., labeled “Research Use Only” (RUO) purchased from commercial sources may be used in laboratory-developed tests only if the laboratory has made a reasonable effort to search for IVD or ASR class reagents. The results of that failed search should be documented by the laboratory director.
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 34 of 95
The laboratory must establish or verify the performance characteristics of tests using Class I ASR’s and RUO’s in accordance with the Method Performance Specifications section of the Laboratory General checklist. The laboratory may put an ASR disclaimer on the pathology report for all immunostains, FISH and ISH studies collectively used in a particular case. Separately tracking each reagent used for a case and selectively applying the disclaimer to only the class I ASR’s is unnecessary. COMMENTARY: N/A REFERENCES: 1) Department of Health and Human Services, Food and Drug Administration. Medical devices; classification/reclassification; restricted devices; analyte specific reagents. Final rule. Fed Register. 1997(Nov 21);62243-45 [21CFR809, 21CFR864]; 2) Caldwell CW. Analyte-specific reagents in the flow cytometry laboratory. Arch Pathol Lab Med. 1998;122:861-864; 3) Graziano. Disclaimer now needed for analyte-specific reagents. Northfield, IL: College of American Pathologists CAP Today. 1998;12(11):5-11; 4) Analyte Specific Reagents; Small Entity Compliance Guidance. http://www.fda.gov/cdrh/oivd/guidance/1205.html, February 26, 2003; 5) Shapiro JD and Prebula RJ. FDA’s Regulation of Analyte-Specific Reagents. Medical Devicelink, February 2003. http://www.devicelink.com/mddi/archive/03/02/018.html; 6) U.S. Department of Health and Human Services, Food and Drug Administration. www.fda.gov/cdrh/ode/immuno.html; 7) U.S. Department of Health and Human Services, Food and Drug Administration. http://www.fda.gov/cdrh/oivd/index.html. ANP.12450 Phase II N/A YES NO Can surgical pathology report information be retrieved by patient identifier (e.g., name, medical record number, etc.)? NOTE: For computerized surgical pathology systems, software tools typically permit text-based searches for any element of the report, such as name and diagnosis. Or, these data elements may already be stored in an electronic database. For paper-based manual systems, it is acceptable to store reports by name. COMMENTARY: N/A **REVISED** 12/12/2006 ANP.12500 Phase II N/A YES NO Are surgical pathology records and materials retained for an appropriate period?
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 35 of 95
NOTE: Minimum requirements for surgical pathology, providing these are not less stringent than state and federal regulations, are:
1. Accession log records - 2 years 2. Wet tissue (stock bottle) - 2 weeks after final report 3. Paraffin blocks - 10 years 4. Glass slides (including control slides) and reports - 10 years 5. Fluorochrome-stained slides – at the discretion of the laboratory director
The retention period should be extended, when appropriate, to provide documentation for adequate quality control and medical care. Pathology reports may be retained in either paper* or electronic format. If retained in electronic format alone, however, the electronic reports must include a secure pathologist electronic signature. There must be a documented policy for protecting and preserving the integrity and retrieval of surgical pathology materials and records. *Images of paper reports—such as microfiche or PDF files—are acceptable. COMMENTARY: N/A REFERENCE: College of American Pathologists. http://www.cap.org/apps/docs/laboratory_accreditation/RetentionGuidelines010405.pdf.
############################################################################
HISTOLOGY LABORATORY
############################################################################ If the histology laboratory is a separate and distinct laboratory in the Anatomic Pathology section, the inspector may find it more convenient to use an additional copy of the Anatomic Pathology Checklist for the inspection, answering all applicable questions. The questions on procedure manuals in the General Anatomic Pathology section of the checklist apply to the histology laboratory.
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 36 of 95
----------------------------------------------------------------- QUALITY CONTROL/HISTOLOGIC PREPARATIONS ----------------------------------------------------------------- ANP.21050 Phase II N/A YES NO Is the identity of every specimen maintained through each step of processing and slide preparation? NOTE: An unambiguous system of specimen identification coupled with a legible, sequential cassette and slide labeling system that withstands reagents and stains are essential to fulfill this requirement. The number of blocks processed and the number of slides prepared for each case must be recorded. COMMENTARY: N/A ANP.21100 Phase II N/A YES NO Are blocks identified adequately? NOTE: Each block of tissue must be identified by the entire accession number assigned to the case and by any descriptive letter(s)/number(s) added by the prosector during the dissection. If additional blocks are prepared later, all lists and logs must reflect these additions. Identification number and letter(s)/numbers(s) must be affixed to all blocks in a manner that remains legible. COMMENTARY: N/A **REVISED** 12/12/2006 ANP.21150 Phase II N/A YES NO Are slides identified permanently with adequate, legible information? NOTE: Each slide must be identified by the entire accession number and descriptive letters unique to the block from which it is cut. Other appropriate identifiers should be included as applicable (e.g., levels of sectioning). Automated prelabeling systems are acceptable. Regardless of whether the identifying information is on the slide or on a label, the information must be indelible, legible and able to withstand all stages of processing and conditions of storage.
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 37 of 95
The laboratory director is responsible for ensuring that slides are adequately, permanently identified. COMMENTARY: N/A REFERENCE: O'Briain DS, et al. Sorting out mix-ups. The provenance of tissue sections may be confirmed by PCR using microsatellite markers. Am J Clin Pathol. 1996;106:758-764. ANP.21250 Phase II N/A YES NO Examine several prepared slides. Are they of sufficient quality for diagnosis? NOTE: Histopathology slides must be of adequate technical quality to be diagnostically useful. Criteria to evaluate include adequate tissue fixation, thickness of sections, absence of interfering tissue folds and tears, and good staining technique. For hematoxylin and eosin and other routine stains, the patient slide serves as the internal control to ensure adequate staining technique. The sections must be cut from sufficient depth in the block to include the entire tissue plane. COMMENTARY: N/A ANP.21350 Phase I N/A YES NO Does the histology laboratory maintain records of the number of blocks, slides, and stains prepared? COMMENTARY: N/A ----------------------------------------------------------------- SPECIAL STAINS (HISTOCHEMISTRY) ----------------------------------------------------------------- The inspector must examine and evaluate sample case(s) of all special stains (with controls) routinely prepared by the histology laboratory. The histochemical stains listed below are neither compulsory for every laboratory nor all-inclusive, but simply intended to represent some common stains.
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 38 of 95
ANP.21366 Phase II N/A YES NO Are reagents and solutions properly labeled, as applicable and appropriate, with the following elements?
1. Content and quantity, concentration or titer 2. Storage requirements 3. Date prepared or reconstituted by laboratory 4. Expiration date
NOTE: The above elements may be recorded in a log (paper or electronic), rather than on the containers themselves, providing that all containers are identified so as to be traceable to the appropriate data in the log. While useful for inventory management, labeling with "date received" is not routinely required. There is no requirement to routinely label individual containers with "date opened"; however, a new expiration date must be recorded if opening the container changes the expiration date, storage requirement, etc. The inspector will describe specific issues of non-compliance in the Inspector's Summation Report. COMMENTARY: N/A REFERENCES: 1) Department of Health and Human Services, Centers for Medicare and Medicaid Services. Clinical laboratory improvement amendments of 1988; final rule. Fed Register. 2003(Jan 24):7164 [42CFR493.1252(c)]; 2) Clinical and Laboratory Standards Institute (CLSI). Laboratory Documents: Development and Control; Approved Guideline—Fifth Edition. CLSI document GP2-A5 (ISBN 1-56238-600-X). Clinical and Laboratory Standards Institute, 940 West Valley Road, Suite 1400, Wayne, Pennsylvania 19087-1898 USA, 2006. ANP.21382 Phase II N/A YES NO Are all histological/histochemical reagents used within their indicated expiration dates? NOTE: The acceptable performance of tissue stains, used before their expiration date, is determined by technical assessment on actual case material, use of suitable control sections, and as part of the pathologist's diagnostic evaluation of a surgical pathology or autopsy pathology case. COMMENTARY: N/A
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 39 of 95
ANP.21400 Phase II N/A YES NO Are positive controls run routinely on all special stains, with reactivity results documented, and are they verified for acceptability before reporting results? NOTE: A positive control slide must be run at the same time as any single or group of slides stained with the same special stain. The tissue chosen for the special stain control slide must be appropriate in type and amount. Both the control slide and the test tissue slide must be judged technically acceptable before the results of the special stains are reported. COMMENTARY: N/A REFERENCE: Sundblad AS. A simplified multitissue block. Am J Clin Pathol. 1994;102:192-193. ANP.21450 Phase II N/A YES NO Are the following special stains of high quality, and do they satisfactorily demonstrate (on each day of use), the tissue characteristics for which they were designed?
1. Acid fast organisms 2. Iron 3. Bacteria 4. Elastic tissues 5. Fungi or pneumocystis 6. Mucin 7. Connective tissue 8. Myelin 9. Nerve fibers 10. Periodic acid Schiff (PAS) 11. Glycogen 12. Reticulin fibers 13. Amyloid 14. Methyl green-pyronine (MGP)
NOTE: This list is neither all-inclusive nor exclusive of other "special stains" used in a given histopathology laboratory. For Gram stains, control slides must demonstrate both Gram-positive and Gram-negative organisms. With the mucicarmine method, the stain must be sufficiently carminophilic. If the myelin stain is luxol fast blue, the tissue must be properly differentiated, i.e., myelin must be turquoise and clearly distinguishable from unmyelinated structures. For nerve fiber stains, axons must be distinct and black with a Bodian or related stain. With MGP, the control slide must demonstrate sufficient pyroninophilia.
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 40 of 95
The Inspector must provide specific details of which stains (this list or others) are deficient in Part B (Deficiency Summary) of the Inspector's Summation Report. COMMENTARY: N/A REFERENCES: 1) Department of Health and Human Services, Centers for Medicare and Medicaid Services. Clinical laboratory improvement amendments of 1988; final rule. Fed Register. 2003(Jan 24):7166 [42CFR493.1256(e)(2)]; 2) Thaxton PH. Recipes for rapid special stains. Advance/Lab. 1999(Oct);8(10):57-58.
****************************************************************************
IMMUNOLOGIC AND MOLECULAR METHODS
**************************************************************************** ----------------------------------------------------------------- IMMUNOFLUORESCENCE MICROSCOPY ----------------------------------------------------------------- ANP.21850 Phase II N/A YES NO Are appropriate positive and negative controls performed with each case tested using immunofluorescence? NOTE: Internal antigens serve as positive controls (e.g., IgA in tubular casts, IgG in protein droplets, and C3 in blood vessels). Non-reactive elements in the patient specimen may serve as a negative tissue control. A negative reagent control in which the patient tissue is processed in an identical manner to the test specimen but with the primary antibody omitted must be performed for each patient test specimen. COMMENTARY: N/A REFERENCE: Walker PD, et al. Practice guidelines for the renal biopsy. Mod. Pathol. 2004;17:1555-1563.
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 41 of 95
----------------------------------------------------------------- IMMUNOHISTOCHEMISTRY ----------------------------------------------------------------- If there is an immunohistochemistry laboratory that is separate and distinct from the histology laboratory, the inspector may find it more convenient to use an additional copy of the Anatomic Pathology Checklist for that purpose, answering all applicable questions. The questions on procedure manuals in the General Anatomic Pathology section of the checklist apply to the immunohistochemistry laboratory. ANP.22250 Phase II N/A YES NO Does the procedure manual address all methods and antibodies currently in use? COMMENTARY: N/A REFERENCES: 1) Varma M, et al. Effect of formalin fixation and epitope retrieval techniques of antibody 34ßE12 immunostaining of prostatic tissues. Mod Pathol. 1999;12:472-478; 2) Vis AN, et al. Quantitative analysis of the decay of immunoreactivity in stored prostate needle biopsy sections. Am J Clin Pathol. 2000;113:369-373; 3) Taylor CR. The total test approach to standardization of immunohistochemistry. Arch Pathol Lab Med. 2000;124:945-951; 4) Werner M, et al. Effect of formalin tissue fixation and processing on immunohistochemistry. Am J Surg Pathol. 2000;24:1016-1019; 5) Rhodes A, et al. Study of interlaboratory reliability and reproducibility of estrogen and progesterone receptor assays in Europe. Documentation of poor reliability and identification of insufficient microwave antigen retrieval time as a major contributory element of unreliable assays. Am J Clin Pathol. 2001;115:44-58; 6) Rohr LR, et al. A comparison of routine and rapid microwave tissue processing in a surgical pathology laboratory. Quality of histologic sections and advantages of microwave processing. Am J Clin Pathol. 2001;115:703-708; 7) Rhodes A, et al. A formalin-fixed, paraffin-processed cell line standard for quality control of immunohistochemical assay of HER2/neu expression in breast cancer. Am J Clin Pathol. 2002;117:81-89; 8) Hsi ED, Yegappan S. Lymphoma immunophenotyping: a new era in paraffin-section immunohistochemistry. Adv Anat Pathol. 2001;8:218-39; 9) Dabbs DJ. Diagnostic Immunohistochemistry. New York: Churchill Livingstone; 2002; 10) NCCLS. Quality Assurance for Immunocytochemistry; Approved Guideline. NCCLS document MM4-AC (ISBN 1-56238-396-5). NCCLS, 940 West Valley Road, Suite 1400, Wayne, Pennsylvania 19087-1898 USA, 1999..
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 42 of 95
ANP.22300 Phase II N/A YES NO If the laboratory performs immunohistochemical staining on specimens other than formalin-fixed, paraffin-embedded tissue, does the procedure manual include appropriate modifications to address such specimens? NOTE: Such specimens include frozen sections, air-dried imprints, cytocentrifuge or other liquid-based preparations, decalcified tissue, and tissues fixed in alcohol blends or other fixatives. COMMENTARY: N/A REFERENCE: Perkins SL, Kjeldsberg CR. Immunophenotyping of lymphomas and leukemias in paraffin-embedded tissues. Am J Clin Pathol 1993:99(4):362-373. ANP.22366 Phase II N/A YES NO Are reagents and solutions properly labeled, as applicable and appropriate, with the following elements?
1. Content and quantity, concentration or titer 2. Storage requirements 3. Date prepared or reconstituted by laboratory 4. Expiration date
NOTE: The above elements may be recorded in a log (paper or electronic), rather than on the containers themselves, providing that all containers are identified so as to be traceable to the appropriate data in the log. While useful for inventory management, labeling with "date received" is not routinely required. There is no requirement to routinely label individual containers with "date opened"; however, a new expiration date must be recorded if opening the container changes the expiration date, storage requirement, etc. The inspector will describe specific issues of non-compliance in the Inspector's Summation Report. Labeling of concentration or titer is not applicable to prediluted reagents. COMMENTARY: N/A REFERENCES: 1) Department of Health and Human Services, Centers for Medicare and Medicaid Services. Clinical laboratory improvement amendments of 1988; final rule. Fed Register. 2003(Jan 24):7164 [42CFR493.1252(c)]; 2) Clinical and Laboratory Standards Institute (CLSI). Laboratory Documents: Development and Control; Approved Guideline—Fifth Edition. CLSI document GP2-A5 (ISBN 1-56238-600-X). Clinical and Laboratory Standards Institute, 940 West Valley Road, Suite 1400, Wayne, Pennsylvania 19087-1898 USA, 2006.
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 43 of 95
ANP.22432 Phase II N/A YES NO Are all immunohistochemical reagents used within their indicated expiration dates? COMMENTARY: N/A REFERENCE: Department of Health and Human Services, Centers for Medicare and Medicaid Services. Clinical laboratory improvement amendments of 1988; final rule. Fed Register. 2003(Jan 24):7164 [42CFR493.1252(c)]. ANP.22500 Phase II N/A YES NO Is the pH of the buffers used in immunohistochemistry routinely monitored? NOTE: pH should be tested when a new batch is prepared or received, and periodically thereafter. COMMENTARY: N/A **REVISED** 12/12/2006 ANP.22550 Phase II N/A YES NO Are positive tissue controls used for each antibody? NOTE: Positive controls assess the performance of the primary antibody. They are performed on sections of tissue known to contain the target antigen, using the same epitope retrieval and immunostaining protocols as the patient tissue. Ideally, the positive control tissue would be the same specimen type as the patient test specimen (e.g., small biopsy, large tissue section, cell block), and would be processed and fixed in the same manner (e.g., formalin-fixed, alcohol-fixed, decalcified) as the patient specimen. However, for most laboratories, it is not practical to maintain separate positive control samples to cover every possible combination of fixation, processing and specimen type. Thus, it is reasonable for a laboratory to maintain a bank of formalin-fixed tissue samples as its positive controls; these controls can be used for patient specimens that are of different type, or fixed/processed differently, providing that the laboratory can show that these patient specimens exhibit equivalent immunoreactivity. This can be accomplished by parallel testing a small panel of common markers to show that specimens of different

College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 44 of 95
type, or processed in a different way (e.g., alcohol-fixed cytology specimens, decalcified tissue) have equivalent immunoreactivity to routinely processed, formalin-fixed tissue. A separate tissue section may be used as a positive control, but test sections often contain normal elements that express the antigen of interest (internal controls). Internal positive controls are acceptable for these antigens, but the laboratory manual must clearly state the manner in which internal positive controls are used on a case-by-case basis. A positive control section included on the same slide as the patient tissue is optimal practice because it helps identify failure to apply primary antibody or other critical reagent to the patient test slide; however, one separate positive control per staining run for each antibody in the run (batch control) may be sufficient provided that the control slide is closely scrutinized by a qualified reviewer. Ideally, positive control tissues possess low levels of antigen expression, as is often seen in neoplasms. Exclusive use of normal tissues that have high levels of antigen expression may result in antibody titers of insufficient sensitivity, leading to false-negative results. COMMENTARY: N/A REFERENCES: 1) O’Leary TJ. Standardization in immunohistochemistry. Appl Immunohistochem Molecul Morphol 2001;9:3-8; 2) NCCLS. Quality Assurance for Immunocytochemistry; Approved Guideline. NCCLS document MM4-AC (ISBN 1-56238-396-5). NCCLS, 940 West Valley Road, Suite 1400, Wayne, Pennsylvania 19087-1898 USA, 1999.. **REVISED** 12/12/2006 ANP.22570 Phase II N/A YES NO Are appropriate negative controls used? NOTE: Negative controls must assess the presence of nonspecific staining in patient tissue as well as the specificity of each antibody. A negative reagent control is used to assess nonspecific or aberrant staining in patient tissue related to the antigen retrieval conditions and/or detection system used. A separate section of patient tissue is processed using the same reagent and epitope retrieval protocol as the patient test slide, except that the primary antibody is omitted, and replaced by any one of the following:
• An unrelated antibody of the same isotype as the primary antibody (for monoclonal primary antibodies)
• An unrelated antibody from the same animal species as the primary antibody (for polyclonal primary antibodies)
• The negative control reagent included in the staining kit
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 45 of 95
• The diluent/buffer solution in which the primary antibody is diluted In general, a separate negative reagent control should be run for each block of patient tissue being immunostained; however, for cases in which there is simultaneous staining of multiple blocks from the same specimen with the same antibody (e.g., cytokeratin staining of multiple axillary sentinel lymph nodes), performing a single negative control on one of the blocks may be sufficient provided that all such blocks are fixed and processed identically. This exception does not apply to stains on different types of tissues or those using different antigen retrieval protocols or antibody detection systems. The laboratory director must determine which cases will have only one negative reagent control, and this must be specified in the department's procedure manual. The negative reagent control would ideally control for each reagent protocol and antibody retrieval condition; however, large antibody panels often employ multiple antigen retrieval procedures. In such cases, a reasonable minimum control would be to perform the negative reagent control using the most aggressive retrieval procedure in the particular antibody panel. Aggressiveness of antigen retrieval (in decreasing order) is as follows: pressure cooker; enzyme digestion, boiling; microwave; steamer; water bath. High pH retrieval should be considered more aggressive than comparable retrieval in citrate buffer at pH 6.0. It is also important to assess the specificity of each antibody by a negative tissue control, which must show no staining of tissues known to lack the antigen. The negative tissue control is processed using the same fixation, epitope retrieval and immunostaining protocols as the patient tissue. Unexpected positive staining of such tissues indicates that the test has lost specificity, perhaps because of improper antibody concentration or excessive antigen retrieval. Intrinsic properties of the test tissue may also be the cause of "non-specific" staining. For example, tissues with high endogenous biotin activity such as liver or renal tubules may simulate positive staining when using a detection method based on biotin labeling. A negative tissue control must be processed for each antibody in a given run. Any of the following can serve as a negative tissue control:
1. Multitissue blocks. These can provide simultaneous positive and negative tissue controls, and are considered “best practice” (see below).
2. The positive control slide or patient test slides, if these slides contain tissue elements that should not react with the antibody.
3. A separate negative tissue control slide. The type of negative tissue control used (i.e., separate sections, internal controls or multitissue blocks) should be specified in the laboratory manual (refer to ANP.22250). Multitissue blocks may be considered best practice and can have a major role in maintaining quality. When used as a combined positive and negative tissue control as mentioned above, they can serve as a permanent record documenting the sensitivity and specificity of every stain, particularly when mounted on the same slide as the patient tissue. When the components are chosen appropriately, multitissue blocks may be used for many different primary antibodies, decreasing the number of different control blocks needed by the laboratory. Multitissue blocks are also ideal for determining optimal titers of
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 46 of 95
primary antibodies since they allow simultaneous evaluation of many different pieces of tissue. Finally, they are a useful and efficient means to screen new antibodies for sensitivity and specificity or new lots of antibody for consistency, which should be done before putting any antibody into diagnostic use. COMMENTARY: N/A REFERENCES: 1) Leong AS-Y, Cooper K, Leong FJW-M. Manual of Diagnostic Antibodies for Immunohistology. 2nd ed. London: Greenwich Medical Media; 2003; 2) Dabbs DJ. Diagnostic Immunohistochemistry. New York: Churchill Livingstone; 2002; 3) Burry RW. Specificity controls for immunocytochemical methods. J Histochem Cytochem 2000;48:163-166; 4) Weirauch M. Multitissue control block for immunohistochemistry. Lab Med. 1999;30:448-449; 5) Miller RT. Multitumor “sandwich” blocks in immunohistochemistry. Simplified method and preparation and practical uses. Appl Immunohistochem 1993;1: 156-159; 6) Chan JKC, Wong CSC, Ku WT, Kwan MY. Reflections on the use of controls in immunohistochemistry and proposal for application of a multitissue spring-roll control block. Ann Diagn Pathol 2000;4: 329-336; 7) NCCLS. Quality Assurance for Immunocytochemistry; Approved Guideline. NCCLS document MM4-AC (ISBN 1-56238-396-5). NCCLS, 940 West Valley Road, Suite 1400, Wayne, Pennsylvania 19087-1898 USA, 1999.. ANP.22615 Phase I N/A YES NO If the laboratory uses an avidin-biotin complex (ABC) detection system (or a related system such as streptavidin-biotin or neutravidin-biotin), is there a policy that addresses nonspecific false positive staining from endogenous biotin? NOTE: Biotin is a coenzyme present in mitochondria, and cells that have abundant mitochondria such as hepatocytes, kidney tubules and many tumors (particularly carcinomas) are rich in endogenous biotin. Biotin-rich intranuclear inclusions are also seen in gestational endometrium and in some tumors that form morules. If steps are not included in the immunostaining method to block endogenous biotin before applying the ABC detection complex, nonspecific false-positive staining may occur, particularly when using heat-induced epitope retrieval (which markedly increases the detectability of endogenous biotin). This artifact is often exquisitely localized to tumor cells and may be easily misinterpreted as true immunoreactivity. Blocking endogenous biotin involves incubating the slides with a solution of free avidin (which binds to endogenous biotin), followed by incubation with a biotin solution (which saturates any empty biotin-binding sites remaining on the avidin). Biotin-blocking steps should be performed immediately after epitope retrieval and before incubation with primary antibody. A number of vendors offer reagent kits for this purpose, but since avidin is expensive, an economical option available to laboratories involves using dilute egg whites as a source of avidin (2 egg whites in 200 mL of distilled water). Slides are incubated in the avidin solution at room temperature for 15 minutes. A distilled water rinse should then be used to prevent precipitation of egg white proteins by salts present in rinsing buffers. Slides
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 47 of 95
are then placed in a 0.2% solution of biotin in rinsing buffer for 15 minutes at room temperature. Biotin is inexpensive, but if desired, reconstituted dried nonfat milk may be used as a source of biotin (5 gm dried milk in 100 mL of rinsing buffer). Following a buffer rinse, the primary antibody is then applied. COMMENTARY: N/A REFERENCES: 1) Miller RT, Kubier P. Blocking of endogenous avidin-binding activity in immunohistochemistry: the use of egg whites. Appl Immunohistochem 1997; 5: 63-66; 2) Miller RT, Kubier P, Reynolds B, Henry T. Blocking of endogenous avidin-binding activity in immunohistochemistry: the use of skim milk as an economical and effective substitute for commercial biotin solutions. Appl Immunohistochem & Molec Morphol 1999;7:63-65. **REVISED** 12/12/2006 ANP.22660 Phase II N/A YES NO When batch controls are run, does the laboratory director or designee review all control slides each day of patient testing? NOTE: Records of this daily review must be maintained and should clearly document that positive and negative controls for all antibodies stain appropriately. Batch control records must be retained for 2 years. The batch control slides must be readily available to pathologists who are signing out cases. The location of the slides should be stated in the procedure manual. COMMENTARY: N/A REFERENCE: Shellhorn N. IHC troubleshooting tips. Advance/Lab. 2000;9(1):33-37. ANP.22750 Phase II N/A YES NO Has the laboratory documented evaluation of new antibody lots and new antibodies, prior to use in patient diagnosis? NOTE: For newly introduced antibodies, staining conditions should be evaluated in cases expected to be positive and negative for the antigen of interest. Ideally, a series of sufficient size should be run to give the laboratory an idea of the sensitivity and specificity of the test. This is particularly important for antibodies with little available data in the literature. When sensitivity and specificity data are well-
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 48 of 95
established in the literature, the laboratory's studies should give similar results. Studies may not be feasible for antigens such as ALK that are only seen in rare tumors. Defining optimum conditions for such factors as antibody titer, antigen retrieval, as well as types and concentration of other processing reagents should be a part of this evaluation. New lots of primary antibody or commercial detection reagent should be compared to the previous lot using an appropriate panel of control tissues. COMMENTARY: N/A REFERENCES: 1) Hsi ED. A practical approach for evaluating new antibodies in the clinical immunohistochemistry laboratory. Arch Pathol Lab Med. 2001;125:289-294; 2) NCCLS. Quality Assurance for Immunocytochemistry; Approved Guideline. NCCLS document MM4-AC (ISBN 1-56238-396-5). NCCLS, 940 West Valley Road, Suite 1400, Wayne, Pennsylvania 19087-1898 USA, 1999.. ANP.22800 Phase II N/A YES NO If automatic immunohistochemistry staining equipment is used, are records kept of recommended maintenance? COMMENTARY: N/A ANP.22900 Phase II N/A YES NO Are the immunohistochemical stains produced of acceptable technical quality? NOTE: The inspector must examine examples of the immunohistochemical preparations offered by the laboratory. A reasonable sample might include 5-10 diagnostic antibody panels. COMMENTARY: N/A REFERENCE: Shellhorn N. IHC troubleshooting tips. Advance/Lab. 2000;9(1):33-37. ----------------------------------------------------------------- FLUORESCENCE AND NON-FLUORESCENCE IN SITU HYBRIDIZATION (FISH, ISH) -----------------------------------------------------------------
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 49 of 95
This section is intended for the application of FISH (e.g., HER2) and ISH (e.g., HPV, HBV) techniques in histologic sections. ANP.22956 Phase II N/A YES NO Is there documentation of validation of commercially available ISH and FISH probes used? COMMENTARY: N/A REFERENCES: 1) American College of Medical Genetics Laboratory. Standards and guidelines for clinical genetics laboratories, 2nd ed. Bethesda, MD: ACMG, 1999; 2) NCCLS. Fluorescence In Situ Hybridization (FISH) Methods for Medical Genetics; Approved Guideline. NCCLS document MM7-A (ISBN 1-56238-524-0). NCCLS, 940 West Valley Road, Suite 1400, Wayne, Pennsylvania 1908-1898 USA, 2004. ANP.22962 Phase II N/A YES NO Is there documentation of validation of probes that are developed in-house (including those using class I analyte-specific reagents)? COMMENTARY: N/A REFERENCES: 1) American College of Medical Genetics Laboratory. Standards and guidelines for clinical genetics laboratories, 2nd ed. Bethesda, MD: ACMG, 1999; 2) NCCLS. Fluorescence In Situ Hybridization (FISH) Methods for Medical Genetics; Approved Guideline. NCCLS document MM7-A (ISBN 1-56238-524-0). NCCLS, 940 West Valley Road, Suite 1400, Wayne, Pennsylvania 1908-1898 USA, 2004. ANP.22974 Phase I N/A YES NO Are there documented procedures for scoring results, including the number of cells scored, and are all analyses scored according to these procedures? COMMENTARY: N/A REFERENCES: 1) American College of Medical Genetics Laboratory. Standards and guidelines for clinical genetics laboratories, 2nd ed. Bethesda, MD: ACMG, 1999; 2) NCCLS. Fluorescence In Situ
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 50 of 95
Hybridization (FISH) Methods for Medical Genetics; Approved Guideline. NCCLS document MM7-A (ISBN 1-56238-524-0). NCCLS, 940 West Valley Road, Suite 1400, Wayne, Pennsylvania 1908-1898 USA, 2004. **REVISED** 12/12/2006 ANP.22980 Phase II N/A YES NO Are control loci (internal or external) used with and documented for each FISH analysis? NOTE: When normal chromosome targets are expected to be present within a sample, an internal control for that target should be used during each hybridization (i.e., a locus specific probe at a different site on the same chromosome and/or a normal locus on the abnormal homolog). If a probe is used that does not produce an internal control signal (e.g., a Y chromosome probe in a female), another sample that is known to have the probe target should be run in parallel with the patient sample. COMMENTARY: N/A REFERENCES: 1) American College of Medical Genetics Laboratory. Standards and Guidelines for Clinical Genetics Laboratories, 3rd ed. Bethesda, MD: ACMG, 2003. Available at: http://www.acmg.net Accessed 2006 ; 2) NCCLS. Fluorescence In Situ Hybridization (FISH) Methods for Medical Genetics; Approved Guideline. NCCLS document MM7-A (ISBN 1-56238-524-0). NCCLS, 940 West Valley Road, Suite 1400, Wayne, Pennsylvania 1908-1898 USA, 2004. **NEW** 12/12/2006 ANP.22982 Phase I N/A YES NO Are photographic or digitized images retained for documentation of all FISH assays (at least one cell for assays with normal results, and at least two cells for assays with abnormal results)? NOTE: For assays where multiple chromosomal loci (>2) are targets in part of a single test, an image of at least one cell must be retained for documentation of each target. Images of at least two cells are required to document all abnormalities. COMMENTARY: N/A
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 51 of 95
**NEW** 12/12/2006 ANP.22984 Phase II N/A YES NO For in situ hybridization studies, are the morphologic interpretation and correlation of results performed by a qualified pathologist as appropriate? COMMENTARY: N/A ANP.22986 Phase I N/A YES NO Is appropriate interpretation of in situ hybridization results provided in the report? COMMENTARY: N/A REFERENCE: NCCLS. Fluorescence In Situ Hybridization (FISH) Methods for Medical Genetics; Approved Guideline. NCCLS document MM7-A (ISBN 1-56238-524-0). NCCLS, 940 West Valley Road, Suite 1400, Wayne, Pennsylvania 1908-1898 USA, 2004. ----------------------------------------------------------------- PREDICTIVE MARKERS ----------------------------------------------------------------- ANP.22988 Phase I N/A YES NO For immunohistochemistry tests that provide independent predictive information, does the patient report include information on specimen processing, the antibody clone, and the scoring method used? NOTE: For immunohistochemical studies used to provide diagnostic predictive information independent of other histopathologic findings (e.g., hormone receptors in breast carcinoma, HER2, EGFR), the laboratory should include the following information in the patient report:
1. The type of specimen fixation and processing (e.g., formalin-fixed paraffin-embedded sections, air-dried imprints, etc.)
2. The antibody clone and general form of detection system used (e.g., LSAB, polymer, proprietary kit, etc.; information on the vendor name or type of equipment used is not necessary)
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 52 of 95
3. Criteria used to determine a positive vs. negative result, and/or scoring system (e.g., percent of stained cells, staining pattern, etc.)
The laboratory should periodically compare its patient results with published benchmarks, and also evaluate interobserver variability among the pathologists in the laboratory. COMMENTARY: N/A REFERENCES: 1) Fisher ER, et al. Solving the dilemma of the immunohistochemical and other methods used for scoring ER and PR receptors in patients with invasive breast cancer. Cancer. 2005;103:164-73; 2) Collins LC, et al. Bimodal frequency distribution of estrogen receptor immunohistochemical staining results in breast cancer: an analysis of 825 cases. Am J Clin Pathol. 2005;123:16-20; 3) Allred DC, et al. ER expression is not bimodal in breast cancer. Am J Clin Pathol. 2005;124:474-5. **NEW** 09/27/2007 ANP.22989 Phase II N/A YES NO Is the laboratory enrolled in the appropriate CAP Surveys, or CAP-accepted other proficiency testing (PT) program, for HER2 testing? NOTE: HER2 PT is method specific, and laboratories performing HER2 testing by multiple methods must participate in PT for each method. Details are available on the CAP website www.cap.org. Satisfactory performance requires correct responses on at least 90% of graded challenges in each testing event (mailing). If the laboratory interprets HER2 test results from stains prepared at another facility, the laboratory must (1) enroll in an appropriate PT survey, (2) send PT materials to the staining facility for preparation, and (3) interpret the resulting stains using the same procedures that are used for patient specimens. COMMENTARY: N/A REFERENCE: Wolff AC, Hammond ME, Schwartz JN, et al. American Society of Clinical Oncology/College of American Pathologists guideline recommendations for human epidermal growth factor receptor 2 testing in breast cancer. Arch Pathol Lab Med 2007;131:18-43.
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 53 of 95
**NEW** 09/27/2007 ANP.22990 Phase II N/A YES NO Does the laboratory integrate all proficiency testing samples within the routine workload, and are those samples analyzed by personnel who routinely test patient/client samples, using the same primary method systems as for patient/client samples? NOTE: Replicate analysis of any proficiency sample is acceptable only if patient/client specimens are routinely analyzed in the same manner. With respect to morphologic examinations (identification of cell types and microorganisms; review of electrophoretic patterns, etc.), group review and consensus identifications are permitted only for unknown samples that would ordinarily be reviewed by more than one person in an actual patient sample. COMMENTARY: N/A REFERENCES: 1) Department of Health and Human Services, Centers for Medicare and Medicaid Services. Clinical laboratory improvement amendments of 1988; final rule. Fed Register. 1992(Feb 28):7146 [42CFR493.801(b)]; 2) Shahangian S, et al. Toward optimal PT use. Med Lab Observ. 2000;32(4):32-43; 3) Parsons PJ. Evaluation of blood lead proficiency testing: comparison of open and blind paradigms. Clin Chem. 2001;47:322-330. **NEW** 09/27/2007 ANP.22993 Phase II N/A YES NO Is there ongoing evaluation of PT results, with prompt corrective action taken for unacceptable results? NOTE: Compliance with this item can be examined by selecting a sample of PT evaluation results. Special attention should be devoted to unacceptable results. Compliance requires that all of the following are true:
1. There is documented evidence of ongoing review of all PT reports by the laboratory director or the director’s designee. Reviews should be completed within one month of the date reports and results become available to the laboratory.
2. All “unacceptable” PT results have been investigated. 3. Corrective action has been initiated for all unacceptable PT results. 4. Primary records related to PT are retained for two years. These include all instrument
tapes, work cards, computer printouts, evaluation reports, evidence of review, and documentation of follow-up/corrective action.
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 54 of 95
COMMENTARY: N/A REFERENCES: 1) Ehrmeyer SS, et al. Use of alternative rules (other than the 1-2s) for evaluating interlaboratory performance data. Clin Chem. 1988:34:250-256; 2) Klee GG, Forsman RW. A user's classification of problems identified by proficiency testing surveys. Arch Pathol Lab Med. 1988;112:371-373; 3) Department of Health and Human Services, Centers for Medicare and Medicaid Services. Clinical laboratory improvement amendments of 1988; final rule. Fed Register. 1992(Feb 28):7173 [42CFR493.1407(e)(4)(iv)]; 4) Steindel SJ, et al. Reasons for proficiency testing failures in clinical chemistry and blood gas analysis. A College of American Pathologists Q-Probes study in 655 laboratories. Arch Pathol Lab Med. 1996;120:1094-1101; 5) NCCLS. Using proficiency testing (PT) to improve the clinical laboratory; approved guideline. NCCLS Document GP27-A. [ISBN 1-56238-381-7]. NCCLS, 940 West Valley Road, Suite 1400, Wayne, PA: NCCLS, 1998 19087-1898, USA, 1999; 6) Shahangian S, et al. Toward optimal PT use. Med Lab Observ. 2000;32(4):32-43; 7) Zaki Z, et al. Self-improvement by participant interpretation of proficiency testing data from events with 2 to 5 samples. Clin Chem. 2000;46:A70. **NEW** 09/27/2007 ANP.22994 Phase II N/A YES NO Is there a policy that prohibits interlaboratory communication about proficiency testing samples until after the deadline for submission of data to the proficiency testing provider? COMMENTARY: N/A REFERENCES: 1) Department of Health and Human Services, Centers for Medicare and Medicaid Services. Clinical laboratory improvement amendments of 1988; final rule. Fed Register. 1992(Feb 28):7146 [42CFR493.801(b)(3)]; 2) Bierig JR. Comparing PT results can put a lab’s CLIA license on the line. Northfield, IL: College of American Pathologists CAP Today. 2002;16(2):84-87. **NEW** 09/27/2007 ANP.22996 Phase II N/A YES NO Is there a policy that prohibits referral of proficiency testing specimens to another laboratory? NOTE: Under CLIA-88 regulations, there is a strict prohibition against referring proficiency testing specimens to another laboratory. In other words, the laboratory may not refer a proficiency testing
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 55 of 95
specimen to a laboratory with a different CLIA number (even if the second laboratory is in the same health care system). COMMENTARY: N/A REFERENCE: Department of Health and Human Services, Centers for Medicare & Medicaid Services. Clinical laboratory improvement amendments of 1988; final rule. Fed Register. 1992(Feb 28): [42CFR493.801(b)(4)]. **NEW** 09/27/2007 ANP.22997 Phase I N/A YES NO If the laboratory assesses HER2 protein over-expression by immunohistochemistry (IHC) or HER2 gene amplification by fluorescence in situ hybridization (FISH), has the laboratory documented appropriate validation for the assay(s)? NOTE: Initial test validation must be performed on a minimum of 25 cases (recommended 25-100). Validation may be performed by comparing the results of testing with a validated alternative method (i.e., IHC vs. FISH) either in the same laboratory or another laboratory, or with the same validated method performed in another laboratory; validation testing must be done using the same set of cases in both labs. If specimens are fixed in a medium other than 10% neutral buffered formalin, the validation study must show that results are concordant with results from formalin-fixed tissues. If significant changes are made in testing methods (e.g., antibody clone, antigen retrieval protocol or detection system), revalidation is required. COMMENTARY: N/A **NEW** 09/27/2007 ANP.22998 Phase I N/A YES NO If the laboratory assesses HER2 protein over-expression by immunohistochemistry (IHC) or HER2 gene amplification by fluorescence in situ hybridization (FISH), does the laboratory have a documented procedure for ensuring appropriate length of fixation of specimens tested?
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 56 of 95
NOTE: Specimens subject to HER2 testing should be fixed in 10% neutral buffered formalin for at least 6 hours and no longer than 48 hours. While core biopsies must not be fixed for less than 1 hour, it is recommended that such specimens have the same fixation as larger specimens (i.e., 6 hours minimum). It is recommended that time of fixation be recorded and included in the report if available. While the maximum fixation time of 48 hours is not an exclusion criterion for HER2 testing, laboratories should qualify any negative results for specimens fixed longer than 48 hours. For cases with negative results by IHC, consideration should be given to performing confirmatory analysis by FISH. Laboratories testing specimens obtained from another institution should have a policy that addresses time of fixation. Information on time of fixation may be obtained by appropriate questions on the laboratory’s requisition form. The time of fixation should be recorded in the final report. COMMENTARY: N/A **NEW** 09/27/2007 ANP.22999 Phase I N/A YES NO If the laboratory assesses HER2 protein over-expression by immunohistochemistry (IHC), does the laboratory report the results using the ASCO/CAP scoring criteria? NOTE: For IHC stained slides, positive cases are those with strong and complete membrane staining in greater than 30% of invasive cancer cells (Score 3). Negative cases are defined as those with no staining (Score 0) or weak, incomplete membrane staining in any proportion of cells (Score 1). Equivocal or indeterminate cases are those cases with strong staining in less than or equal to 30% of cells, or less than strong but complete membrane staining in any proportion of cells. These scoring criteria used must be stated in the pathology report, along with the clone of antibody and details of the method used (see also ANP.22988). Careful attention should be paid to the recommended exclusion criteria for performing or interpreting HER2 assays (e.g., artifactual distortion of tissue; strong membrane staining of normal ducts; see table 5 in reference 1, below). COMMENTARY: N/A REFERENCE: Wolff AC, Hammond ME, Schwartz JN, et al. American Society of Clinical Oncology/College of American Pathologists guideline recommendations for human epidermal growth factor receptor 2 testing in breast cancer. Arch Pathol Lab Med 2007;131:18-43.
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 57 of 95
**NEW** 09/27/2007 ANP.23005 Phase I N/A YES NO If the laboratory assesses HER2 gene amplification by fluorescence in situ hybridization (FISH), does the laboratory report the results using the ASCO/CAP scoring criteria? NOTE: For HER2 gene status determined by FISH, positive (amplified) cases are those with ratios of HER2 to CEP17 of > 2.2. Negative cases are defined as those with FISH ratios of < 1.8. Equivocal cases are those with a FISH ratio of 1.8 – 2.2. For test systems without an internal control probe, positive (amplified) cases are those with an average HER2 gene copy number > six signals/nucleus, negative cases are those with < four signals/nucleus, and equivocal cases are those with an average HER2 gene copy number of four to six signals/nucleus. Careful attention should be paid to the recommended exclusion criteria for performing or interpreting FISH for HER2 (e.g., signal obscured by background; difficulty in defining areas of invasive carcinoma under UV light; see table 6 in reference 1, below). COMMENTARY: N/A REFERENCE: Wolff AC, Hammond ME, Schwartz JN, et al. American Society of Clinical Oncology/College of American Pathologists guideline recommendations for human epidermal growth factor receptor 2 testing in breast cancer. Arch Pathol Lab Med 2007;131:18-43. ----------------------------------------------------------------- INSTRUMENTS AND EQUIPMENT ----------------------------------------------------------------- ................................................................. Equipment Maintenance ................................................................. A variety of instruments and equipment are used to support the performance of analytical procedures. All instruments and equipment should be properly operated, maintained, serviced, and monitored to ensure that malfunctions of these instruments and equipment do not adversely affect the analytical results. The inspection team should review the procedures for instrument/equipment operations, maintenance, and monitoring records to ensure that these devices are properly used. The procedures and schedules for instrument maintenance must be as thorough and as frequent as specified by the manufacturer.
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 58 of 95
ANP.23010 Phase II N/A YES NO Is there a schedule for checking, servicing, and maintenance of all instruments? COMMENTARY: N/A ANP.23050 Phase II N/A YES NO Are instrument maintenance, service and repair records (or copies) promptly available to, and usable by, the technical staff operating the equipment? NOTE: Effective utilization of instruments by the technical staff depends upon the prompt availability of maintenance, repair, and service documentation (copies are acceptable). Laboratory personnel are responsible for the reliability and proper function of their instruments and must have access to this information. Off-site storage, such as with centralized medical maintenance or computer files, is not precluded if the inspector is satisfied that the records can be promptly retrieved. COMMENTARY: N/A ANP.23075 Phase II N/A YES NO Is there evidence of ongoing evaluation of results of instrument maintenance and function for all devices? COMMENTARY: N/A ................................................................. Pipettes and Thermometers ................................................................. NOTE TO THE INSPECTOR: This section applies if the laboratory uses volumetric pipettes, or procedures requiring precise temperatures. Mark questions N/A that do not apply to the laboratory being inspected.
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 59 of 95
ANP.23085 Phase II N/A YES NO Are pipettes that are used for quantitative dispensing of material checked for accuracy and reproducibility at specified intervals, and results documented? NOTE: Such checks are most simply done gravimetrically. This consists of transferring a number of measured samples of water from the pipette to a balance. Each weight is recorded, the weights are converted to volumes, and then means (for accuracy), and SD/CV (for imprecision) are calculated. Alternative approaches include spectrophotometry or (less frequently) the use of radioactive isotopes, and commercial kits are available from a number of vendors. Computer software is useful where there are many pipettes, and provides convenient documentation. This checklist question does not apply to Class A volumetric pipettes that meet the American Society for Testing and Materials calibration (accuracy) specifications. COMMENTARY: N/A REFERENCES: 1) Curtis RH. Performance verification of manual action pipets. Part I. Am Clin Lab. 1994;12(7):8-9; 2) Curtis RH. Performance verification of manual action pipets. Part II. Am Clin Lab. 1994;12(9):16-17; 3) Perrier S, et al. Micro-pipette calibration using a ratiometric photometer-reagent system as compared to the gravimetric method. Clin Chem. 1995;41:S183; 4) Bray W. Software for the gravimetric calibration testing of pipets. Am Clin Lab. Oct 1995 (available on the internet at http://www.labtronics.com/pt_art.htm); 5) Kroll MH, et al (eds). Laboratory instrument evaluation, verification & maintenance manual, 5th edition. Northfield, IL: College of American Pathologists, 1999:126-127; 6) Johnson B. Calibration to dye for: Artel's new pipette calibration system. Scientist. 1999;13(12):14; 7) Connors M, Curtis R. Pipetting error: a real problem with a simple solution. Parts I and II. Am Lab News. 1999;31(13):20-22; 8) Skeen GA, Ashwood ER. Using spectrophotometry to evaluate volumetric devices. Lab Med. 2000;31:478-479; 9) American Society for Testing and Materials. Standard specification for glass volumetric (transfer) pipets, designation E 969-95. Philadelphia, PA: ASTM, 1995. ANP.23090 Phase II N/A YES NO Is an appropriate thermometric standard device of known accuracy (NIST-certified or guaranteed by manufacturer to meet NIST Standards) available? NOTE: Thermometers should be present on all temperature-controlled instruments and environments and checked daily. Thermometric standard devices should be recalibrated or recertified prior to the date of expiration of the guarantee of calibration. COMMENTARY: N/A
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 60 of 95
ANP.23095 Phase II N/A YES NO Are all non-certified thermometers in use checked against an appropriate thermometric standard device before initial use? COMMENTARY: N/A ................................................................. Tissue Processor ................................................................. ANP.23100 Phase II N/A YES NO Are solutions changed as needed? NOTE: Tissue processor solutions must be changed at intervals appropriate for workload. COMMENTARY: N/A REFERENCE: Baunoch DA, et al. Troubleshooting problems in processing, staining. Advance/Lab. 1999(Oct));8(10):59-64. ANP.23150 Phase II N/A YES NO Is the temperature of the paraffin baths checked regularly and recorded? COMMENTARY: N/A ................................................................. Paraffin Dispenser .................................................................
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 61 of 95
ANP.23200 Phase I N/A YES NO Is the instrument clean and well-maintained? COMMENTARY: N/A ANP.23250 Phase II N/A YES NO Is the temperature checked regularly and recorded? COMMENTARY: N/A ANP.23300 Phase II N/A YES NO Is the temperature adjusted properly for the type of paraffin used? COMMENTARY: N/A ................................................................ Flotation Baths ................................................................. ANP.23350 Phase II N/A YES NO Are flotation baths clean and well-maintained, and is there a procedure for preventing cross-contamination of paraffin sections in the bath? NOTE: Of particular importance are periodic water changes or blotting of the water surface so that sections from one patient block are not inadvertently carried over to another case (so-called "floaters" or "extraneous tissue"). COMMENTARY: N/A
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 62 of 95
REFERENCE: Gephardt GN, Zarbo RJ. Extraneous tissue in surgical pathology. A College of American Pathologists Q-Probes study of 275 laboratories. Arch Pathol Lab Med. 1996;120:1009-1014. ................................................................. Microtomes ................................................................. ANP.23400 Phase I N/A YES NO Are microtomes clean, well-maintained, properly lubricated and without excessive play in the advance mechanism? COMMENTARY: N/A ANP.23450 Phase I N/A YES NO Are microtome knives sharp and free of nicks? COMMENTARY: N/A
****************************************************************************
PHYSICAL FACILITIES
**************************************************************************** ANP.23500 Phase I N/A YES NO Is there adequate space for technical and clerical work? COMMENTARY: N/A
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 63 of 95
ANP.23550 Phase I N/A YES NO Is the lighting satisfactory? NOTE: Direct sunlight should be avoided because of its extreme variability and the need for low light levels necessary to observe various computer consoles, etc. Lighting control should be sectionalized so general levels of illumination can be controlled in areas of the room if desired. COMMENTARY: N/A ANP.23600 Phase I N/A YES NO Are work areas clean and well-maintained? COMMENTARY: N/A ---------------------------------------------------------------- STORAGE AND SUPPLY ----------------------------------------------------------------- ANP.23650 Phase I N/A YES NO Is the working storage area sufficient for routine supplies? COMMENTARY: N/A ANP.23700 Phase I N/A YES NO Are slides and paraffin blocks properly stored in an organized manner (i.e., accessible for retrieval, and properly identified)? NOTE: Slides and blocks should be stored in a manner to prevent contamination from blood or other fluids or tissues. The storage area for blocks should be cool to prevent blocks from melting together. COMMENTARY:
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 64 of 95
N/A
***************************************************************************
HISTOLOGY LABORATORY SAFETY
*************************************************************************** NOTE TO THE INSPECTOR: The inspector should review relevant questions from the Safety section of the Laboratory General checklist, to assure that the histology laboratory is in compliance. Please elaborate upon the location and the details of each deficiency in the Inspector's Summation Report. The following questions pertain specifically to the histology laboratory. ANP.24050 Phase II N/A YES NO Is each open (i.e., generative of flammable vapors into the ambient workspace) automated tissue processor operated at least 5 feet from the storage of combustible materials and from the paraffin dispenser? NOTE: Each open (i.e., generative of flammable vapors into the ambient workspace) automated tissue processor must be located at least 5 feet from the storage of combustible materials unless separated by one-hour fire-resistive construction (NFPA 99-10-4.2.1 (1993)). Flammable and combustible liquids, such as in a paraffin dispenser, must not be positioned near sources of heat or ignition (NFPA 99-10.7.2.4 (1993)). At least 5 feet must separate each open system tissue processor from the paraffin dispenser. Tissue processors that operate as a closed system confine ignitable vapor hazards within the processor and thus do not pose a hazard requiring a 1.52 m (5 ft) separation. COMMENTARY: N/A REFERENCE: A.11.4.2.1 (NFPA 99-2002). ANP.24100 Phase I N/A YES NO Are microtome knives stored in original containers or by some other means to avoid personnel injury or equipment damage? COMMENTARY: N/A
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 65 of 95
ANP.24200 Phase II N/A YES NO Are infectious tissues and other contaminated materials disposed of with minimum danger to professional, technical, and custodial personnel? NOTE: Waste disposal must be in accord with all regulations and disposed of with minimum danger to professional, technical, and custodial personnel. COMMENTARY: N/A REFERENCES: 1) Clinical and Laboratory Standards Institute (CLSI). Protection of Laboratory Workers From Occupationally Acquired Infections; Approved Guideline—Third Edition. CLSI document M29-A3 (ISBN 1-56238-567-4). Clinical and Laboratory Standards Institute, 940 West Valley Road, Suite 1400, Wayne, Pennsylvania 19087-1898 USA, 2005; 2) NCCLS. Clinical Laboratory Waste Management; Approved Guideline—Second Edition. NCCLS document GP5-A2 (ISBN 1-56238-457-0). NCCLS, 940 West Valley Road, Suite 1400, Wayne, Pennsylvania 19087-1898, USA 2002.. ANP.24300 Phase II N/A YES NO Are there documented procedures for the special handling of tissues in the histology laboratory from cases in which Creutzfeldt-Jakob disease is suspected? NOTE: Neuropathology tissues from cases of Creutzfelt-Jakob disease should be treated with formic acid. Paraffin blocks and slides prepared from formic-acid-treated tissue may be handled routinely. If tissue has not been treated with formic acid, it must be hand-processed and treated as containing potentially transmissible prions. Double gloves must be worn at all times when handling such tissue. All solutions, including water washes, must be collected and treated with equal volumes of fresh undiluted household bleach for 60 minutes before disposal. Disposables, glassware tools, etc. must be handled according to the procedures employed in the autopsy room described elsewhere in this checklist. All scraps of paraffin and unused sections should be collected on a disposable sheet. The microtome may be wiped with bleach or NaOH solution. No special precautions are needed in handling intact glass slides once they have been coverslipped. Broken slides should be decontaminated and discarded. Paraffin blocks should be stored in a bag or box and labeled as infectious. Alternatively, the laboratory may reseal the cut surface of the blocks with paraffin. COMMENTARY: N/A
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 66 of 95
REFERENCES: 1) Brown W, et al. A simple and effective method for inactivating virus activity in formalin-fixed tissue samples from patients with Creutzfeldt-Jakob disease. Neurology. 1990;40:887-890; 2) Brown P. Guidelines for high risk autopsy cases: special precautions for Creutzfeldt-Jakob disease. In: Hutchins G, ed. Autopsy performance and reporting. Northfield, IL: College of American Pathologists, 1990:68-74; 3) Greenblatt, M. Q&A. Northfield, IL: College of American Pathologists, CAP Today 1993(March);7(3):69-70; 4) Crain BJ. Safety tips for anatomic studies of possible CJD. Northfield, IL: College of American Pathologists, CAP Today. 1996(Jan);10(1):56; 5) Rank JP. How can histotechnologists protect themselves from Creutzfeldt-Jakob disease. Lab Med. 1999;30:305; 6) Nixon RR. Prions and prion diseases. Lab Med. 1999;30:335-338. ANP.27150 Phase I N/A YES NO Are there documented procedures for safe disposal of used glass slides and paraffin blocks? NOTE: The laboratory must follow CAP retention requirements for slides and blocks (refer to checklist question in the “Surgical Pathology Reports” section of this checklist). COMMENTARY: N/A REFERENCE: NCCLS. Clinical Laboratory Waste Management; Approved Guideline - Second Edition GP5-A2. Wayne, PA: NCCLS, 2002. NOTE: The following four questions apply to microwave devices used in the histology laboratory. **NEW** 12/12/2006 ANP.27170 Phase I N/A YES NO Are microwave devices used in accordance with manufacturer’s instructions? NOTE: Microwave devices should be used in accordance with manufacturer’s instructions, unless CAP requirements are more stringent. COMMENTARY: N/A
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 67 of 95
**REVISED** 12/12/2006 ANP.28290 Phase I N/A YES NO Are microwave devices periodically monitored for reproducibility? NOTE: “Reproducibility” is defined as consistency in diagnostic quality obtained from microwave equipment and procedures. For some devices, reproducibility may be evaluated by monitoring the temperatures of identical samples after microwave processing. For those microwave devices (particularly those incorporated into histology processing equipment) that use temperature-independent methods to evaluate reproducibility, the laboratory should have a written procedure for monitoring reproducibility that follows instrument manufacturer’s instructions. Information on such procedures is given in the reference to this checklist question (see below). The microwave device should be tested for radiation leakage if there is visible damage to the device. COMMENTARY: N/A REFERENCE: Clinical and Laboratory Standards Institute. Microwave Device Use in the Histology Laboratory; Approved Guideline. CLSI document GP28-A [ISBN 1-56238-563-1]. Clinical and Laboratory Standards Institute, 940 West Valley Road, Suite 1400, Wayne, Pennsylvania 19087-1898 USA, 2005. **REVISED** 12/12/2006 ANP.28860 Phase I N/A YES NO Are all containers used in microwave devices vented? NOTE: Venting of containers is necessary so that processing occurs at atmospheric pressure, to prevent explosion. For procedures using pressure above that of the atmosphere, specialized containers must be used, with strict adherence to manufacturer instructions. COMMENTARY: N/A REFERENCE: Clinical and Laboratory Standards Institute. Microwave Device Use in the Histology Laboratory; Approved Guideline. CLSI document GP28-A [ISBN 1-56238-563-1]. Clinical and Laboratory Standards Institute, 940 West Valley Road, Suite 1400, Wayne, Pennsylvania 19087-1898 USA, 2005.
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 68 of 95
ANP.29430 Phase I N/A YES NO Are microwave devices properly vented? NOTE: Microwave devices should be placed in an appropriate ventilation hood to contain airborne chemical contaminants and potentially infectious agents. Before operation of the microwave device, flammable and corrosive reagents should be removed from the hood, to prevent fire or chemical damage to the electronic components of the device. Microwave devices used outside a fume hood should have an integral fume extractor that is certified by the manufacturer for use in a clinical laboratory. The effectiveness of ventilation should be monitored at least annually. This checklist question does not apply if only non-hazardous reagents (and non-infectious specimens) are used in the device (e.g., water, certain biological stains, paraffin sections). The laboratory should consult the MSDS sheets received with reagents and stains to assist in determining proper handling requirements and safe use. COMMENTARY: N/A REFERENCE: Clinical and Laboratory Standards Institute. Microwave Device Use in the Histology Laboratory; Approved Guideline. CLSI document GP28-A [ISBN 1-56238-563-1]. Clinical and Laboratory Standards Institute, 940 West Valley Road, Suite 1400, Wayne, Pennsylvania 19087-1898 USA, 2005.
###########################################################################
AUTOPSY PATHOLOGY
###########################################################################
****************************************************************************
QUALITY MANAGEMENT
**************************************************************************** The purpose of this section is to determine if there is an active program of surveillance of the quality of autopsy diagnostic reports and utilization of the information obtained to enhance the quality of patient care.
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 69 of 95
ANP.30000 Phase II N/A YES NO Is the quality management program defined and documented? COMMENTARY: N/A REFERENCES: 1) McManus BM, et al. A decade of acceptable autopsy rates. Does concordance of clinician and pathologist views explain relative success? Arch Pathol Lab Med. 1992;116:1128-1136; 2) Young NA, Naryshkin S. An implementation plan for autopsy quality control and quality assurance. Arch Pathol Lab Med. 1993;117:531-534; 3) Hunt LW Jr, et al. Accuracy of the death certificate in a population-based study of asthmatic patients. JAMA. 1993;269:1947-1952; 4) Haque AK, et al. High autopsy rates at a university medical center. What has gone right? Arch Pathol Lab Med. 1996;120:727-732; 5) Pellegrino ED. The autopsy. Some ethical reflections on the obligations of pathologists, hospitals, families, and society. Arch Pathol Lab Med. 1996;120:739-742; 6) Baker PB, et al. Quality assurance of autopsy face sheet reporting, final autopsy report turnaround time, and autopsy rates. A College of American Pathologists Q-Probes study of 10 003 autopsies from 418 institutions. Arch Pathol Lab Med. 1996;120:1003-1008; 7) Nemetz PN, et al. Determinants of the autopsy decision. A statistical analysis. Am J Clin Pathol. 1997;108:175-183; 8) Schwartz DA, Herman CJ. The importance of the autopsy in emerging and reemerging infectious diseases. Clin Inf Dis. 1996;23:248-254; 9) Nichols L, et al. Are autopsies obsolete? Am J Clin Pathol. 1998;110:210-218; 10) Zarbo RJ, et al. The autopsy as a performance measurement tool - diagnostic discrepancies and unresolved clinical questions. Arch Pathol Lab Med. 1999;123:191-198; 11) Nakhleh RE, et al. Autopsy result utilization. A College of American Pathologists Q-Probes study of 256 laboratories. Arch Pathol Lab Med. 1999;123:290-295; 12) Hutchins GM, et al. Practice guidelines for autopsy pathology. Autopsy reporting. Arch Pathol Lab Med. 1999;123:1085-1092; 13) Chariot P, et al. Declining autopsy rate in a French hospital. Physicians' attitudes to the autopsy and use of autopsy material in research publications. Arch Pathol Lab Med. 2000;124:739-745; 14) Sinard JH, et al. Quality improvement on an academic autopsy service. Arch Pathol Lab Med. 2001;125:237-245; 15) Bove KE, et al. The role of the autopsy in medical malpractice cases, I. A review of 99 appeals court decisions. Arch Pathol Lab Med. 2002;126:1023-1031; 16) Sens MA, et al. Quality assurance in autopsy pathology. In: Collins KA, et al, eds. Autopsy Performance and Reporting. 2nd ed. Northfield, IL: College of American Pathologists: 2003; chap 37. ANP.30050 Phase II N/A YES NO Are formal intra- and extra-departmental consultations documented and the reports maintained with the patient's autopsy report? NOTE: When formal intra- and extra-departmental consultations are obtained, they must be documented and the reports kept with the patient autopsy report. COMMENTARY:
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 70 of 95
N/A REFERENCE: Tomaszewski JE, et al. Consensus conference on second opinions in diagnostic anatomic pathology. Who, what, and when. Am J Clin Pathol. 2000;114:329-335.. ANP.30100 Phase II N/A YES NO Are the findings of the postmortem examination used for correlative clinicopathological teaching purposes designed to enhance the quality of patient care? NOTE: The autopsy has an important role in medical education and quality improvement. The value of the final autopsy report is enhanced when the findings are used for teaching that emphasizes clinicopathological correlations. This teaching activity should be documented and may take any of several forms, including a correlative note in the autopsy report, interdepartmental note or summary, or a clinical teaching conference. COMMENTARY: N/A REFERENCES: 1) McPhee SJ. Maximizing the benefits of autopsy for clinicians and families. What needs to be done. Arch Pathol Lab Med. 1996;120:743-748; 2) Feinstein AR. Epidemiologic and clinical challenges in reviving the necropsy. Arch Pathol Lab Med. 1996;120:749-752; 3) Baker PB, et al. Quality assurance of autopsy face sheet reporting, final autopsy report turnaround time, and autopsy rates. A College of American Pathologists Q-Probes study of 10 003 autopsies from 418 institutions. Arch Pathol Lab Med. 1996;120:1003-1008; 4) Nakhleh RE, et al. Autopsy result utilization. A College of American pathologists Q-Probes study of 256 laboratories. Arch Pathol Lab Med. 1999;123:290-295; 5) Hutchins GM, et al. Practice guidelines for autopsy pathology. Autopsy reporting. Arch Pathol Lab Med. 1999;123:1085-1092; 6) Hanzlick RL. The autopsy lexicon. Suggested headings for the autopsy report. Arch Pathol Lab Med. 2000;124:594-603; 7) Bayer-Garner IB, et al. Pathologists in a teaching institution assess the value of the autopsy. Arch Pathol Lab Med. 2002;126:442-447; 8) Baker PB. Communication of autopsy results. In: Collins KA, et al, eds. Autopsy Performance and Reporting. 2nd ed. Northfield, IL: College of American Pathologists: 2003; chap 33; 9) Davis GJ, et al. The autopsy in medical education. In: Collins KA, et al, eds. Autopsy Performance and Reporting. 2nd ed. Northfield, IL: College of American Pathologists: 2003; chap 34; 10) Hutchins GM, et al. Autopsy reporting. In: Collins KA, et al, eds. Autopsy Performance and Reporting. 2nd ed. Northfield, IL: College of American Pathologists: 2003; chap 28. ANP.30150 Phase I N/A YES NO Are the findings from autopsies incorporated into the institutional quality management program? COMMENTARY:
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 71 of 95
N/A REFERENCES: 1) Suchii-Bernal L, et al. Application of an autopsy report specifically designed for cardiovascular diseases. Arch Pathol Lab Med. 1994;118:71-78; 2) O'Leary DS. Relating autopsy requirements to the contemporary accreditation process. Arch Pathol Lab Med. 1996;120:763-766; 3) Nakhleh RE, et al. Autopsy result utilization. A College of American Pathologists Q-Probes study of 256 laboratories. Arch Pathol Lab Med. 1999;123:290-295; 4) Sens MA, et al. Quality assurance in autopsy pathology. In: Collins KA, et al, eds. Autopsy Performance and Reporting. 2nd ed. Northfield, IL: College of American Pathologists: 2003; chap 37. ANP.30575 Phase II N/A YES NO Are autopsy findings that were clinically inapparent but important specifically documented and communicated interdepartmentally? NOTE: The form in which this is accomplished is at the discretion of the laboratory director. For example, presentation at a clinical conference or specifically highlighting these findings in the discussion/case summary of the autopsy report would meet this requirement. The goal is to enhance the quality of patient care by documenting findings that were not detected antemortem. COMMENTARY: N/A REFERENCES: 1) Anderson RE, et al. A model for autopsy based quality assessment of medical diagnostics. Hum Pathol.1990;21:174-181; 2) Hill RB, et al. Autopsy-based quality assessment program for improvement of diagnostic accuracy. Qual Assur Health Care. 1993;5: 351-359; 3) Nakhleh RE, et al. Autopsy result utilization. a College of American Pathologists Q-Probes study of 256 laboratories. Arch Pathol Lab Med. 1999;123:290-295; 4) Sinard J, Blood D. Quality Improvement on an academic autopsy service. Arch Pathol Lab Med. 2001;125:237-245; 5) Baker PB. Communication of autopsy results. In: Collins KA, et al, eds. Autopsy Performance and Reporting. 2nd ed. Northfield, IL: College of American Pathologists: 2003; chap 33; 6) Hutchins GM, et al. Autopsy reporting. In: Collins KA, et al, eds. Autopsy Performance and Reporting. 2nd ed. Northfield, IL: College of American Pathologists: 2003; chap 28.
****************************************************************************
DEATH PROCEDURES
****************************************************************************
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 72 of 95
ANP.31000 Phase II N/A YES NO Are there documented instructions covering such items as receipt, storage, and release of bodies? NOTE: In some institutions, such policies and procedures may reside in the Nursing or Security manuals. In such cases, the laboratory should have copies of such manuals available at the time of inspection. COMMENTARY: N/A ANP.31050 Phase II N/A YES NO Are the instructions for body handling available at the nursing stations, admitting office, administration, and/or other appropriate places? COMMENTARY: N/A ANP.31070 Phase II N/A YES NO Is there a documented procedure for obtaining autopsy consent, including who may give consent? COMMENTARY: N/A REFERENCES: 1) Warren JW, et al. Organ-limited autopsies. Obtaining permission for postmortem examination of the urinary tract. Arch Pathol Lab Med. 1995;119:440-443; 2) Saqi A, Hoda S. Limitations on autopsy by next-of-kin: a significant hindrance to pathologic evaluation? Am J Clin Pathol. 1998;110:512-513; 3) Chariot P, et al. Declining autopsy rate in a French hospital. Physicians' attitudes to the autopsy and use of autopsy material in research publications. Arch Pathol Lab Med. 2000;124:739-745; 4) Bierig JR. Informed consent in the practice of pathology. Arch Pathol Lab Med. 2001;125:1425-1429; 5) College of American Pathologists documents pertaining to the autopsy. In: Collins KA, et al, eds. Autopsy Performance and Reporting. 2nd ed. Northfield, IL: College of American Pathologists: 2003; chap 5.
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 73 of 95
ANP.31100 Phase II N/A YES NO Are there instructions covering possible medical examiner or coroner jurisdiction over hospital deaths to assess the appropriateness of performing a hospital autopsy? NOTE: To assess the appropriateness of performing a hospital autopsy, the department must be familiar with applicable statutes and/or regulations that identify hospital deaths subject to medical examiner or coroner jurisdiction. The department should maintain a copy of applicable statute(s) and/or regulation(s) that identify those deaths that are in the jurisdiction of the medical examiner and/or coroner. COMMENTARY: N/A REFERENCE: Randall BB, et al. Forensic pathology. In: Collins KA, et al, eds. Autopsy Performance and Reporting. 2nd ed. Northfield, IL: College of American Pathologists: 2003; chap 7.
****************************************************************************
AUTOPSY ROOM
**************************************************************************** ANP.32100 Phase I N/A YES NO Is there an autopsy room located within the institution or a contract/agreement with a CAP-accredited facility to provide the service? NOTE: If feasible, the autopsy room should be located within the institution. Requirements relating to the physical facility, dissection, and handling of organs and tissues apply only to those cases that are performed at the site under CAP accreditation. The pathologist should encourage off-site facilities where autopsies are performed (e.g., funeral homes) to meet the standards expected for on-site autopsy rooms. COMMENTARY: N/A REFERENCE: Hanzlick RL, et al. Autopsy facility design. In: Collins KA, et al, eds. Autopsy Performance and Reporting. 2nd ed. Northfield, IL: College of American Pathologists: 2003; chap 14.
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 74 of 95
ANP.32150 Phase II N/A YES NO Are instruments clean, sharp and well-maintained? COMMENTARY: N/A REFERENCE: Hanzlick RL, et al. Autopsy facility design. In: Collins KA, et al, eds. Autopsy Performance and Reporting. 2nd ed. Northfield, IL: College of American Pathologists: 2003; chap 14. ANP.32200 Phase I N/A YES NO Is there sufficient space? NOTE: The space should be sufficient for the workload requirements of the service. COMMENTARY: N/A REFERENCES: 1) Hazlett SO. Perspectives in pathology. The newly designed morgue. Advance/Lab. 2000;9(1):10-11; 2) Hanzlick RL, et al. Autopsy facility design. In: Collins KA, et al, eds. Autopsy Performance and Reporting. 2nd ed. Northfield, IL: College of American Pathologists: 2003; chap 14. ANP.32250 Phase I N/A YES NO Is the autopsy room clean and well-maintained? COMMENTARY: N/A REFERENCES: 1) Hazlett SO. Perspectives in pathology. The newly designed morgue. Advance/Lab. 2000;9(1):10-11; 2) Baker PB. Autopsy safety. In: Collins KA, et al, eds. Autopsy Performance and Reporting. 2nd ed. Northfield, IL: College of American Pathologists: 2003; chap 11; 3) Hanzlick RL, et al. Autopsy facility design. In: Collins KA, et al, eds. Autopsy Performance and Reporting. 2nd ed. Northfield, IL: College of American Pathologists: 2003; chap 14. ANP.32300 Phase I N/A YES NO Is the location of the autopsy room convenient in relation to other pathology and institutional services?
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 75 of 95
COMMENTARY: N/A REFERENCE: Hanzlick RL, et al. Autopsy facility design. In: Collins KA, et al, eds. Autopsy Performance and Reporting. 2nd ed. Northfield, IL: College of American Pathologists: 2003; chap 14. ANP.32350 Phase I N/A YES NO Is the lighting satisfactory? NOTE: Direct sunlight should be avoided because of its extreme variability and the need for low light levels necessary to observe various computer consoles, etc. Lighting control should be sectionalized so general levels of illumination can be controlled in areas of the room if desired. Lighting should be adequate for the dissection and examination of organs and tissue and the safety of the prosector. Either bright, general room lights or spot lights may be used. COMMENTARY: N/A REFERENCE: Hanzlick RL, et al. Autopsy facility design. In: Collins KA, et al, eds. Autopsy Performance and Reporting. 2nd ed. Northfield, IL: College of American Pathologists: 2003; chap 14. ANP.32400 Phase II N/A YES NO Are provisions available for satisfactory storage of bodies (refrigeration or embalming)? NOTE: For refrigeration, the temperature should be in the range of 34-40º F. (1.1-4.4º C). COMMENTARY: N/A REFERENCES: 1) Hanzlick RL, et al. Autopsy facility design. In: Collins KA, et al, eds. Autopsy Performance and Reporting. 2nd ed. Northfield, IL: College of American Pathologists: 2003; chap 14; 2) Cooperation between pathologists and funeral directors. In: Collins KA, et al, eds. Autopsy Performance and Reporting. 2nd ed. Northfield, IL: College of American Pathologists: 2003; chap 16. ANP.32450 Phase II N/A YES NO Is a scale and/or balance provided for reliable weighing of organs?
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 76 of 95
NOTE: If infants or fetuses are autopsied at the institution, accuracy of balances to 1.0 gm for infants and 0.1 gm for fetuses must be documented by periodic calibration. COMMENTARY: N/A REFERENCES: 1) Hutchins GM. Autopsy performance. In: Collins KA, et al, eds. Autopsy Performance and Reporting. 2nd ed. Northfield, IL: College of American Pathologists: 2003; chap 15; 2) Hanzlick RL, et al. Autopsy facility design. In: Collins KA, et al, eds. Autopsy Performance and Reporting. 2nd ed. Northfield, IL: College of American Pathologists: 2003; chap 14; 3) Bove KE, et al. The Perinatal and Pediatric Autopsy. In: Collins KA, et al, eds. Autopsy Performance and Reporting. 2nd ed. Northfield, IL: College of American Pathologists: 2003; chap 18. ANP.32500 Phase I N/A YES NO Are ambient temperature and ventilation control adequate? COMMENTARY: N/A REFERENCES: 1) Montanaro A. Formaldehyde in the workplace and in the home. Exploring its clinical toxicology. Lab Med. 1996;27:752-757; 2) Hazlett SO. Perspectives in pathology. The newly designed morgue. Advance/Lab. 2000;9(1):10-11; 3) Hanzlick RL, et al. Autopsy facility design. In: Collins KA, et al, eds. Autopsy Performance and Reporting. 2nd ed. Northfield, IL: College of American Pathologists: 2003; chap 14. ANP.32550 Phase I N/A YES NO Are photographic facilities available and convenient? COMMENTARY: N/A REFERENCES: 1) Belanger AJ, et al. Implementation of a practical digital imaging system for routine gross photography in an autopsy environment. Arch Pathol Lab Med. 2000;124:160-165; 2) Lantz PE, et al. Photography in autopsy pathology. In: Collins KA, et al, eds. Autopsy Performance and Reporting. 2nd ed. Northfield, IL: College of American Pathologists: 2003; chap 26; 3) Hanzlick RL, et al. Autopsy facility design. In: Collins KA, et al, eds. Autopsy Performance and Reporting. 2nd ed. Northfield, IL: College of American Pathologists: 2003; chap 14.
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 77 of 95
ANP.32600 Phase I N/A YES NO Is there a conveniently located locker and shower available for personnel participating in autopsies? COMMENTARY: N/A REFERENCE: Hanzlick RL, et al. Autopsy facility design. In: Collins KA, et al, eds. Autopsy Performance and Reporting. 2nd ed. Northfield, IL: College of American Pathologists: 2003; chap 14. ANP.32650 Phase II N/A YES NO Are appropriate equipment and reagents available and maintained in accordance with laboratory standards for performance of special studies (e.g., toxicologic, microbiologic)? NOTE: Reagents and solutions must be properly labeled, as applicable and appropriate with the following information:
1. Content and quantity, concentration or titer 2. Storage requirements 3. Date prepared or reconstituted by laboratory 4. Expiration date
The above elements may be recorded in a log (paper or electronic), rather than on the containers themselves, providing that all containers are identified so as to be traceable to the appropriate data in the log. While useful for inventory management, labeling with "date received" is not routinely required. There is no requirement to routinely label individual containers with "date opened"; however, a new expiration date must be recorded if opening the container changes the expiration date, storage requirement, etc. COMMENTARY: N/A REFERENCE: Collins KA, et al. Ancillary studies for autopsy pathology. In: Collins KA, et al, eds. Autopsy Performance and Reporting. 2nd ed. Northfield, IL: College of American Pathologists: 2003; chap 24.
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 78 of 95
****************************************************************************
AUTOPSY PERFORMANCE AND DOCUMENTATION
**************************************************************************** ANP.33000 Phase II N/A YES NO Are available clinical records reviewed and/or clinical information discussed with the attending physician before conducting the autopsy? COMMENTARY: N/A REFERENCES: 1) Hutchins GM et al. Autopsy reporting. In: Collins KA, et al, eds. Autopsy Performance and Reporting. 2nd ed. Northfield, IL: College of American Pathologists: 2003; chap 28; 2) Hanzlick RL. The autopsy: its impact on clinical medicine, health care, and research. In: Collins KA, et al, eds. Autopsy Performance and Reporting. 2nd ed. Northfield, IL: College of American Pathologists: 2003; chap 31; 3) Baker PB. Communication of autopsy results. In: Collins KA, et al, eds. Autopsy Performance and Reporting. 2nd ed. Northfield, IL: College of American Pathologists: 2003; chap 33. ANP.33050 Phase II N/A YES NO Are all autopsies performed, or directly supervised, by a pathologist qualified in anatomic pathology? COMMENTARY: N/A ANP.33100 Phase II N/A YES NO Is a documented preliminary report of the gross pathologic diagnoses submitted to the attending physician and the institutional record within a reasonable time (2 working days)? COMMENTARY: N/A REFERENCES: 1) Zarbo RJ, et al. Quality assurance of autopsy permit form information, timeliness of performance, and issuance of preliminary report. Arch Pathol Lab Med. 1996;120:346-352; 2)
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 79 of 95
Adickes ED, Sims KL. Enhancing autopsy performance and reporting. A system for a 5-day completion time. Arch Pathol Lab Med. 1996;120:249-253; 3) Smith MT, Garvin AJ. Anatomic pathology turnaround times. Use and abuse. Am J Clin Pathol 1996;106(Suppl 1):S70-S73; 4) Baker PB, et al. Quality assurance of autopsy face sheet reporting, final autopsy report turnaround time, and autopsy rates. A College of American Pathologists Q-Probes study of 10 003 autopsies from 418 institutions. Arch Pathol Lab Med. 1996;120:1003-1008; 5) Hanzlick RL. The autopsy lexicon. Suggested headings for the autopsy report. Arch Pathol Lab Med. 2000;124:594-603; 6) Hutchins GM, et al. Autopsy reporting. In: Collins KA, et al, eds. Autopsy Performance and Reporting. 2nd ed. Northfield, IL: College of American Pathologists: 2003; chap 28; 7) Baker PB. Communication of autopsy results. In: Collins KA, et al, eds. Autopsy Performance and Reporting. 2nd ed. Northfield, IL: College of American Pathologists: 2003; chap 33. ANP.33125 Phase I N/A YES NO Are the majority of autopsy final reports produced within 30 working days? NOTE: The clinical and quality management value of the autopsy is enhanced by prompt reporting of results to the referring physician and the institutional record. COMMENTARY: N/A REFERENCES: 1) Adickes ED, Sims KL. Enhancing autopsy performance and reporting. A system for a 5-day completion time. Arch Pathol Lab Med. 1996;120:249-253; 2) Smith MT, Garvin AJ. Anatomic pathology turnaround times. Use and abuse. Am J Clin Pathol 1996;106(Suppl 1):S70-S73; 3) Baker PB, et al. Quality assurance of autopsy face sheet reporting, final autopsy report turnaround time, and autopsy rates. A College of American Pathologists Q-Probes study of 10 003 autopsies from 418 institutions. Arch Pathol Lab Med. 1996;120:1003-1008; 4) Hanzlick RL. The autopsy lexicon. Suggested headings for the autopsy report. Arch Pathol Lab Med. 2000;124:594-603; 5) Bove KE, et al. The role of the autopsy in medical malpractice cases, II. Controversy related to autopsy performance and reporting. Arch Pathol Lab Med. 2002;126:1032-1035; 6) Hutchins GM, et al. Autopsy reporting. In: Collins KA, et al, eds. Autopsy Performance and Reporting. 2nd ed. Northfield, IL: College of American Pathologists: 2003; chap 28; 7) Baker PB. Communication of autopsy results. In: Collins KA, et al, eds. Autopsy Performance and Reporting. 2nd ed. Northfield, IL: College of American Pathologists: 2003; chap 33. ANP.33150 Phase II N/A YES NO For all cases, is the final autopsy report produced within 60 working days? NOTE: Allowance may be needed if portions of a case are referred for external consultation, and completion of the case is dependent upon information from such consultations (e.g., complex
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 80 of 95
neuropathology). If cases exceed 60 days, there should be documentation of the reason for the delay and of ongoing review of this information by the director of the service. COMMENTARY: N/A REFERENCES: 1) Adickes ED, Sims KL. Enhancing autopsy performance and reporting. A system for a 5-day completion time. Arch Pathol Lab Med. 1996;120:249-253; 2) Smith MT, Garvin AJ. Anatomic pathology turnaround times. Use and abuse. Am J Clin Pathol 1996;106(Suppl 1):S70-S73; 3) Baker PB, et al. Quality assurance of autopsy face sheet reporting, final autopsy report turnaround time, and autopsy rates. A College of American Pathologists Q-Probes study of 10 003 autopsies from 418 institutions. Arch Pathol Lab Med. 1996;120:1003-1008; 4) Hanzlick RL. The autopsy lexicon. Suggested headings for the autopsy report. Arch Pathol Lab Med. 2000;124:594-603; 5) Bove KE, et al. The role of the autopsy in medical malpractice cases, II. Controversy related to autopsy performance and reporting. Arch Pathol Lab Med. 2002;126:1032-1035; 6) Hutchins GM, et al. Autopsy reporting. In: Collins KA, et al, eds. Autopsy Performance and Reporting. 2nd ed. Northfield, IL: College of American Pathologists: 2003; chap 28; 7) Baker PB. Communication of autopsy results. In: Collins KA, et al, eds. Autopsy Performance and Reporting. 2nd ed. Northfield, IL: College of American Pathologists: 2003; chap 33. ANP.33200 Phase II N/A YES NO Are gross descriptions clear and concise, are all pertinent findings adequately described and do the descriptions support the diagnosis? NOTE: Annotated drawings and photographs are valuable tools for documenting the autopsy findings, but are not adequate replacements for a text description. COMMENTARY: N/A REFERENCES: 1) Hutchins GM, et al. Autopsy reporting. In: Collins KA, et al, eds. Autopsy Performance and Reporting. 2nd ed. Northfield, IL: College of American Pathologists: 2003; chap 28; 2) Hanzlick RL, et al. The autopsy lexicon: suggested headings for the autopsy report. In: Collins KA, et al, eds. Autopsy Performance and Reporting. 2nd ed. Northfield, IL: College of American Pathologists: 2003; chap 29. ANP.33250 Phase II N/A YES NO If microscopic descriptions are included in the report, are they clear and concise, and do they support the diagnosis?
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 81 of 95
COMMENTARY: N/A ANP.33300 Phase II N/A YES NO When appropriate, does the report include a key or summary noting block and slide designations to allow identification of the source of specific microscopic sections? NOTE: At a minimum, the key should include information on laterality and on specific lesions sampled. COMMENTARY: N/A REFERENCES: 1) Hutchins GM, et al. Autopsy reporting. In: Collins KA, et al, eds. Autopsy Performance and Reporting. 2nd ed. Northfield, IL: College of American Pathologists: 2003; chap 28; 2) Hanzlick RL, et al. The autopsy lexicon: suggested headings for the autopsy report. In: Collins KA, et al, eds. Autopsy Performance and Reporting. 2nd ed. Northfield, IL: College of American Pathologists: 2003; chap 29. ANP.33350 Phase II N/A YES NO Does the final autopsy report contain sufficient information in an appropriate format so that a physician may ascertain the patient's major disease processes and probable cause of death? COMMENTARY: N/A REFERENCES: 1) Hutchins GM, et al. Autopsy reporting. In: Collins KA, et al, eds. Autopsy Performance and Reporting. 2nd ed. Northfield, IL: College of American Pathologists: 2003; chap 28; 2) Hanzlick RL, et al. The autopsy lexicon: suggested headings for the autopsy report. In: Collins KA, et al, eds. Autopsy Performance and Reporting. 2nd ed. Northfield, IL: College of American Pathologists: 2003; chap 29; 3) Hanzlick RL. Medical certification of death and cause-of-death statements. In: Collins KA, et al, eds. Autopsy Performance and Reporting. 2nd ed. Northfield, IL: College of American Pathologists: 2003; chap 30. ANP.33400 Phase I N/A YES NO Are autopsy records organized and readily available for review?
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 82 of 95
COMMENTARY: N/A REFERENCE: Moore GW. Computer-based indexing. In: Collins KA, et al, eds. Autopsy Performance and Reporting. 2nd ed. Northfield, IL: College of American Pathologists: 2003; chap 32. ANP.33450 Phase I N/A YES NO Are major diagnoses entered into a database that allows prompt retrieval? NOTE: At the facility’s discretion, this could be accomplished through the use of an electronic database, card file, or log book, depending on the size of the database. COMMENTARY: N/A REFERENCES: 1) Moore GW. Computer-based indexing. In: Collins KA, et al, eds. Autopsy Performance and Reporting. 2nd ed. Northfield, IL: College of American Pathologists: 2003; chap 32; 2) Hutchins GM, et al. Autopsy reporting. In: Collins KA, et al, eds. Autopsy Performance and Reporting. 2nd ed. Northfield, IL: College of American Pathologists: 2003; chap 28. ANP.33500 Phase II N/A YES NO Are autopsy pathology records and materials retained for an appropriate period? NOTE: There must be a documented policy for preserving the integrity of retained autopsy service materials. The laboratory must define the period of time that such materials are retained. The retention period shall provide for adequate quality control and potential medical care of other individuals. In establishing retention requirements, care should be taken to comply with state and federal regulations. Minimum requirements for autopsy pathology, providing these are not less stringent than state and federal regulations, are:
1. Accession log records - 2 years 2. Wet tissue (stock bottle) - 3 months after final report 3. Paraffin blocks - 10 years 4. Glass slides and reports - 10 years
COMMENTARY: N/A
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 83 of 95
REFERENCES: 1) College of American Pathologists. Guidelines for the retention of laboratory records and materials. Northfield, IL: CAP, current edition; 2) College of American Pathologists documents pertaining to the autopsy. In: Collins KA, et al, eds. Autopsy Performance and Reporting. 2nd ed. Northfield, IL: College of American Pathologists: 2003; chap 5.
****************************************************************************
AUTOPSY SAFETY
**************************************************************************** NOTE TO THE INSPECTOR: The inspector should review relevant questions from the safety section of the Laboratory General checklist, to assure that the autopsy laboratory is in compliance. Please elaborate upon the location and the details of each deficiency in the Inspector's Summation Report. The following questions pertain specifically to the autopsy laboratory. ANP.33650 Phase II N/A YES NO Are appropriate facilities, equipment and instruments available to meet safety policies and procedures? NOTE: Containers must be available for contaminated waste and hazardous chemicals and policies in place for their disposal. Equipment and apparel must be available to provide protection to eyes, hands, and skin surfaces from direct and aerosolized exposures during autopsy performance. Procedures must be in place for the disposition or cleaning of these items for re-use upon completion of the autopsy. COMMENTARY: N/A REFERENCES: 1) Baker PB. Autopsy safety. In: Collins KA, et al, eds. Autopsy Performance and Reporting. 2nd ed. Northfield, IL: College of American Pathologists: 2003; chap 1; 2) Hanzlick RL, et al. Autopsy facility design. In: Collins KA, et al, eds. Autopsy Performance and Reporting. 2nd ed. Northfield, IL: College of American Pathologists: 2003; chap 14; 3) Bull AD, et al. Should eye protection be worn when performing necropsies? J Clin Pathol. 1991;44:782-; 4) Towfighi J, et al. A protective device for performing cranial autopsies. Hum Pathol. 1989;20:288-289; 5) Kembach-Wighton G, et al. Bone-dust in autopsies: reduction of spreading. Forensic Sci Intl. 1996;83:95-103; 6) Wetli CV. Autopsy safety. Lab Med. 2001;32:451-453.
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 84 of 95
ANP.34000 Phase II N/A YES NO Are safety policies and procedures for contaminated cases/specimens, hazardous chemicals, etc. written and posted in the autopsy suite? NOTE: The responsibility for safety of employees under OSHA regulations is clear: "the employer must provide a job free of recognized hazards and provide warning of hazards and protective equipment." COMMENTARY: N/A REFERENCES: 1) Johnson MD, et al. Autopsy risk and acquisition of human immunodeficiency virus infection. A case report and reappraisal. Arch Pathol Lab Med. 1997;121:64-66; 2) The implantable cardioverter-defibrillator. A potential hazard for autopsy pathologists. Arch Pathol Lab Med. 1997;121:1076-1080; 3) Wetli CV. Autopsy safety. Lab Med. 2001;32:451-453; 4) Baker PB. Autopsy safety. In: Collins KA, et al, eds. Autopsy Performance and Reporting. 2nd ed. Northfield, IL: College of American Pathologists: 2003; chap 11. ANP.34050 Phase II N/A YES NO Do the safety policies and procedures provide instructions for daily cleaning, cleaning after an autopsy, proper handling of highly infectious cases, and disposal of tissues? NOTE: The safety policies and procedures must include measures to reduce or eliminate hazards, both chemical and infectious. COMMENTARY: N/A REFERENCES: 1) Baker PB. Autopsy safety. In: Collins KA, et al, eds. Autopsy Performance and Reporting. 2nd ed. Northfield, IL: College of American Pathologists: 2003; chap 1; 2) Nichols WS, et al. High risk autopsy cases. In: Collins KA, et al, eds. Autopsy Performance and Reporting. 2nd ed. Northfield, IL: College of American Pathologists: 2003; chap 12. ANP.34100 Phase II N/A YES NO Are tables and reusable instruments and aprons adequately disinfected after use? NOTE: The safety manual must specify the procedures used. Either autoclaving or chemical disinfection is acceptable, but the method chosen must be adequate to inactivate the hepatitis B virus.
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 85 of 95
COMMENTARY: N/A REFERENCES: 1) Baker PB. Autopsy safety. In: Collins KA, et al, eds. Autopsy Performance and Reporting. 2nd ed. Northfield, IL: College of American Pathologists: 2003; chap 11; 2) Nichols WS, et al. High risk autopsy cases. In: Collins KA, et al, eds. Autopsy Performance and Reporting. 2nd ed. Northfield, IL: College of American Pathologists: 2003; chap 12. ANP.34150 Phase II N/A YES NO Are there documented procedures for the special handling of cases in which Creutzfeldt-Jakob disease is suspected? NOTE: In addition to practicing universal precautions during the autopsy, procedures must be written for the special precautions to be taken for autopsies on patients in whom the diagnosis of Creutzfeldt-Jakob disease is suspected. Pathologists should consider taking these special precautions as well in cases of (a) rapidly progressive dementia, (b) dementia with seizures, especially myoclonic seizures, and (c) dementia associated with cerebellar or lower motor neuron signs. The recommended method for handling these brains to reduce infectivity is immersion of tissue blocks in 95% formic acid. Aerosol formation must be avoided during removal of the brain. If there is any suspicion of Creutzfeldt-Jakob disease, the autopsy should be limited to the brain, and the tissue treated as outlined below. There should be very few exceptions to this rule. Autopsy brain tissues should be handled as follows: The intact brain is fixed in formalin for 1-2 weeks before cutting. Tissue blocks (representative regions of neocortex, basal ganglia, and cerebellum) are taken, agitated in at least 50-100 mL of 95-100% formic acid for 1 hour, and then returned to formalin for 2 days before embedding. Alternatively, one may take the necessary diagnostic sections from the fresh brain, fix them in formalin for 2-7 days, treat with formic acid for 1 hour, fix again in formalin for 2 days, and then embed in paraffin. This method significantly reduces infectivity. At the conclusion of the autopsy, the area of incision and other contaminated skin surfaces are washed with freshly opened undiluted commercial household bleach (sodium hypochlorite). As sodium hypochlorite deteriorates after several months, a newly opened container should be used for each autopsy. After 10 minutes, the skin may be washed with water. All gowns, gloves, plastic sheets, and other disposable supplies are placed in a red or orange biohazard bag and incinerated. Alternatively, they may be autoclaved (132ºC steam) and discarded. Hard surfaces are decontaminated with freshly opened undiluted bleach or NaOH. 1N NaOH is adequate unless there will be dilution by surface liquid, in which case 2N NaOH should be used. Bleach and NaOH are equally effective, but NaOH is preferred for steel instruments and surfaces because it is less corrosive than bleach. The disinfectant should remain in contact with the surface for at least 15 and preferably 60 minutes. Autopsy
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 86 of 95
instruments should have any visible blood removed, then decontaminated with undiluted bleach or 1-2N NaOH as above. Alternatively, they may be autoclaved for 1 hour at 132ºC and 20 psi. For information on handling slides and blocks, refer to the checklist question in the Histology Laboratory Safety section of this checklist. COMMENTARY: N/A REFERENCES: 1) Brown PW, et al. A simple and effective method for inactivating virus activity in formalin-fixed tissue samples from patients with Creutzfeldt-Jakob disease. Neurology. 1990;40:887-890; 2) Greenblatt, M. Q&A. In: CAP Today. 1993(March);7(3):69-70. Northfield, IL: College of American Pathologists; 3) Brown P. Special precautions for autopsies of patients with Creutzfeldt-Jakob disease. In: Collins KA, et al. . Autopsy Performance and Reporting. 2nd ed. Northfield, IL: College of American Pathologists;2003:chap 1; 4) Johnson MD, et al. Autopsy risk and acquisition of human immunodeficiency virus infection: a case report and reappraisal. Arch Pathol Lab Med. 1997;121:64-66.
############################################################################
ELECTRON MICROSCOPY
############################################################################ If the electron microscopy service is a separate and distinct laboratory in the Anatomic Pathology section, the inspector may find it more convenient to use an additional copy of the Anatomic Pathology Checklist for the inspection, answering all applicable questions.
****************************************************************************
QUALITY CONTROL
**************************************************************************** The questions on procedure manuals in the General Anatomic Pathology section of the checklist apply to the electron microscopy service. ----------------------------------------------------------------- SPECIMEN COLLECTION -----------------------------------------------------------------
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 87 of 95
ANP.51000 Phase II N/A YES NO Are written instructions provided for persons collecting specimens for electron microscopic study? COMMENTARY: N/A ANP.51050 Phase II N/A YES NO Do requisitions include sources of tissue and appropriate clinical data? COMMENTARY: N/A ANP.51100 Phase II N/A YES NO Are fixatives suitable for electron microscopy easily accessible to collection areas (such as operating room, outpatient area(s), and autopsy room)? COMMENTARY: N/A ----------------------------------------------------------------- ELECTRON MICROSCOPY SAMPLE PREPARATION ----------------------------------------------------------------- ANP.52000 Phase II N/A YES NO Is the identity of every specimen maintained through each step in processing? COMMENTARY: N/A ANP.52050 Phase II N/A YES NO Are blocks identified adequately?
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 88 of 95
NOTE: Each Epon® block of tissue must be individually labeled with unique patient identifier(s), e.g., accession number etched onto the block or embedded into it. Storage of unlabeled blocks in separate containers that are labeled with patient number or name does not meet this requirement. COMMENTARY: N/A ANP.52100 Phase II N/A YES NO Are sections of embedded tissue (face sections) reviewed by the pathologist to ensure that appropriate areas are selected for electron microscopic examination? COMMENTARY: N/A ANP.52150 Phase I N/A YES NO Where appropriate, are one micron sections (prepared after trimming or ultra thin sectioning) also reviewed by the pathologist to ensure that appropriate areas have been selected? NOTE: An example might be a mesenchymal neoplasm where confusion between tumor cells and admixed stromal elements could occur. COMMENTARY: N/A ANP.52200 Phase II N/A YES NO Are slides of face (semithin) and one micron sections labeled adequately? COMMENTARY: N/A ANP.52250 Phase II N/A YES NO Are the electron micrographs identified adequately?
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 89 of 95
NOTE: Each electron micrograph must be individually labeled with unique patient identifier(s). Unlabeled micrographs should not be stored in separate envelopes that are identified with a patient number or name. The original magnification should be recorded on each electron micrograph. COMMENTARY: N/A ANP.52300 Phase II N/A YES NO Examine several slides and electron photomicrographs. Are they of sufficient quality for proper interpretation of ultrastructural changes? COMMENTARY: N/A ----------------------------------------------------------------- INSTRUMENTS AND EQUIPMENT ----------------------------------------------------------------- ANP.53000 Phase II N/A YES NO Are ultramicrotomes adequate and in good repair? COMMENTARY: N/A ANP.53100 Phase II N/A YES NO Is the electron microscope under a regular maintenance and repair system? COMMENTARY: N/A ANP.53150 Phase I N/A YES NO Is the magnification calibrated after major maintenance, as appropriate?
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 90 of 95
COMMENTARY: N/A ANP.53200 Phase II N/A YES NO Is all unscheduled service and routine maintenance documented? COMMENTARY: N/A ANP.53250 Phase II N/A YES NO Are instrument maintenance, service, and repair records (or copies) promptly available to, and usable by, the technical staff operating the equipment? NOTE: Effective utilization of instruments by the technical staff depends upon the prompt availability of maintenance, repair, and service documentation. Laboratory personnel are responsible for the reliability and proper function of their instruments and must have access to this information. . Off-site storage, such as with centralized medical maintenance or computer files, is not precluded if the inspector is satisfied that the records can be promptly retrieved.. COMMENTARY: N/A ----------------------------------------------------------------- REPORTS ----------------------------------------------------------------- ANP.54000 Phase II N/A YES NO Does the report format provide for correlation with routine light microscope and other (e.g., immunohistochemical and immunofluorescent) studies? COMMENTARY: N/A
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 91 of 95
ANP.54050 Phase II N/A YES NO Are all reports signed by the pathologist? NOTE: Where diagnostic reports are generated by computer or telecommunications equipment, the actual signature or initials of the pathologist may not appear. It is nevertheless essential that the laboratory have a procedure that ensures and documents that the responsible pathologist has reviewed and approved the completed report before its release. COMMENTARY: N/A ANP.54100 Phase II N/A YES NO Are copies of all reports retained by the laboratory? COMMENTARY: N/A ----------------------------------------------------------------- RECORDS, FILES AND PHOTOGRAPHS ----------------------------------------------------------------- ANP.55000 Phase I N/A YES NO Are specimen records organized and readily available for review? COMMENTARY: N/A ANP.55050 Phase I N/A YES NO Are photographs properly indexed and filed in a usable manner? COMMENTARY: N/A
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 92 of 95
ANP.55100 Phase I N/A YES NO Are wet/fixed tissues retained for at least 2 weeks after the final report is released? COMMENTARY: N/A ANP.55150 Phase I N/A YES NO Are one micron sections retained by the laboratory? COMMENTARY: N/A
***************************************************************************
PHYSICAL FACILITIES
************************************************************************** Sufficient space and utilities need to be provided for the workload of the department, and to meet all safety requirements. ANP.56000 Phase I N/A YES NO Is there adequate space for preparation of sections? COMMENTARY: N/A ANP.56050 Phase I N/A YES NO Is there adequate space for the electron microscope instrument working area? COMMENTARY: N/A
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 93 of 95
ANP.56100 Phase I N/A YES NO Is there adequate space for photographic processing? COMMENTARY: N/A ANP.56150 Phase I N/A YES NO Is there adequate space for supply storage? COMMENTARY: N/A ANP.56200 Phase I N/A YES NO Is there adequate space for filing of records, reports and photographs? COMMENTARY: N/A
****************************************************************************
LABORATORY SAFETY
**************************************************************************** NOTE TO THE INSPECTOR: The inspector should review relevant questions from the Safety section of the Laboratory General checklist, to assure that the electron microscopy laboratory is in compliance. Please elaborate upon the location and the details of each deficiency in the Inspector's Summation Report. The following questions pertain specifically to the electron microscopy laboratory. ANP.57000 Phase II N/A YES NO Are safety policies and procedures established for electron microscopy sample preparations and instrument operation? COMMENTARY:
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 94 of 95
N/A ANP.57050 Phase II N/A YES NO Is a safety hood used when handling osmium tetroxide and other volatile and hazardous material? NOTE: OSHA 29CFR1910, subpart A, has established permissible limits for osmium tetroxide (0.006 mg/m3). Exposure to hazardous material can reasonably be controlled by a proper functioning hood. NFPA 99 and NFPA 45 have defined fire and safety requirements for fume hoods. Additional information can be found in the CDC/NIH "Biosafety in Microbiological and Biomedical Laboratories” (GPO stock # 017-040-00523-7). COMMENTARY: N/A ANP.57070 Phase II N/A YES NO Are procedures adequate for the safe handling and disposal of osmium tetroxide, epoxy resins, and other hazardous chemicals? NOTE: Osmium tetroxide is volatile and toxic. Exposure to its vapor can lead to blindness and serious respiratory complications. There must be a clearly stated and posted policy as to what should be done if there is accidental spillage. Material for dealing with such a spill should be readily available, e.g., corn oil and an absorbent such as saw dust. For U.S. laboratories, disposal of osmium tetroxide should be according to OSHA regulations for toxic compounds. Epoxy resins are highly allergenic, and direct contact should be avoided. The laboratory should have documentation that personnel have been trained in the handling of these materials. COMMENTARY: N/A REFERENCES: 1) Cooper K. Neutralization of osmium tetroxide in case of accidental spillage and for disposal. Micros Soc Canada Bull. 1988;8(3):24-28; 2) Wenk PA. Disposal of histology stains. Lab Med. 1998;29:337-338. ANP.57100 Phase II N/A YES NO Has the electron microscope been checked for x-ray leakage at the time of installation and after major repair?
College of American Pathologists Revised: 09/27/2007
ANATOMIC PATHOLOGY (Web File) Page 95 of 95
NOTE: Periodic monitoring is also required for devices operating at 70,000 volts or above. Records of radiation leakage checks must be maintained. COMMENTARY: N/A