anatomy - mtitx.com · web viewanatomy. ligaments cervical spine. atlanto occipital joint...
TRANSCRIPT

ADVANCED CERVICAL SPINE I
© The Manual Therapy Institute PLLC 1998-2019
1

CONTENT
Anatomy 3
Biomechanics and arthrokinematics 9
Pre manipulative testing 11
Joint manipulations 29
Muscle imbalance 35
ANATOMY
2

Ligaments cervical spine
Atlanto occipital joint ligamentsJoint capsuleThin and loose. Surrounds the condyles of the occipital bones, connects them with the articular processes of the atlas.
Anterior atlanto occipital membraneConnects the anterior part of the foramen magnum to the anterior arch of C1. It is thought to be a continuation of the ALL. May provide some A-P stability when both anterior and posterior A-O membranes are intact.
Posterior atlanto occipital membraneConnects the posterior ring of C1 to the occiput at the foramen magnum. Broad and thin.The anterior and posterior membranes prevent anterior and vertical displacement of C1.
Ligaments connecting C2 with occiputTectorial membraneContinuation of PLL. Runs from the body of C2 up over the posterior portion of the dens and then makes a 45-degree angle in the anterior direction as it attaches to the anterior edge of the foramen magnum. It limits flexion, extension and vertical translation. Unable to prevent any anterior dislocation.
Alar ligamentA pair of ligaments attached to the dorsolateral surfaces of the tip of the dens. Each runs obliquely to the medial surfaces of the occipital condyles. The function of the alar ligament is to resist flexion, sidebending and rotation. Combined flexion and rotation puts the most stress on the ligament.
Apical ligamentConnects the apex of the dens to the anterior edge of the foramen magnum. It is a fairly strong structure of elastic consistency. It contributes little to upper cervical spine stability.
Ligaments of the atlanto axial jointAnterior atlanto axial membraneConnects C1 to C2 anteriorly. Strengthened at mid line by a rounded cord
Posterior atlanto axial ligamentBroad thin membrane. It attaches to the posterior ring of the atlas and the axis. The posterior A- O and A-A membrane are anatomically analogous to the yellow ligament. However they are considerably different in physical properties. The yellow ligament is first present between C2-3. If present higher up, the highly elastic but still rather stiff
3

yellow ligament would never allow the considerable amount of rotation currently present in the upper cervical spine (80 degrees). So stability is sacrificed for ROM.
Cruciate ligamentThe major portion of this ligament is the transverse ligament, which is the most important ligament in the upper cervical spine. It attaches to the 2 condyles of the atlas. There is an ascending and a descending part, which is triangular shaped. The ascending portion attaches to the anterior edge of the foramen magnum, the descending part attaches to the body of C2. They are 3-4 mm thick. The ascending and descending part have little importance in controlling physiological motion, but they do check inferior/superior displacement of the transverse ligament.
Transverse ligamentMost important ligament in upper cervical spine, it is the number one stabilizer. It’s 7-8 mm thick. It attaches on the medial surface of the lateral mass of the atlas. It keeps the dens in contact with the anterior arch of C1. Anterior dislocation of C1 on C2 can only occur with insufficiency of the transverse ligament. The transverse ligament is almost twice as strong as the alar ligaments, with a tensile strength of 330 N. Injuries to the transverse ligament are classified as follows:Type I: disruption of the substance of the ligament, without osseous componentType II: fractures or avulsions involving the insertion of the ligament on the lateral mass, without disruption of the ligamentType I injuries are incapable of healing without surgery for internal fixation, but most type II injuries heal when treated with an orthosis.
Remaining cervical spine ligamentsNuchal ligamentDistinct band that runs from the posterior border of the occiput to the SP of C7. Anteriorly it attaches to the SP’s of the cervical vertebrae and the interspinous ligaments. Its precise role has not been identified yet. It may play an important role in the clinical biomechanics of the neck. One hypothesis is that it plays a major proprioceptive role in the functioning of the erector spinae muscles. Another hypothesis is that it provides A-P stability at C1-4 due to specific fiber attachment.
Anterior longitudinal ligamentContinuation of the ligament that runs the entire length of the spine. Well developed in the thoracic and lumbar regions. Described as a thin, translucent structure in the cervical spine. Little is known about the mechanical properties of this structure in this region of the spine.
4

Musculature cervical spine
Sub occipital musculatureRectus capitis posterior major. Runs from the C2 spinous process to the inferior nuchal line on the occiput.
Rectus capitis posterior minorRuns from the C1 posterior tubercle to the inferior nuchal line on the occiput.
Oblique capitis superiorRuns from the C1 transverse process to the lateral part of the inferior nuchal line on the occiput. The direction of the muscle is perpendicular to the oblique capitis inferior.
Oblique capitis inferiorRuns superior, lateral and anterior from the C2 spinous process to the C1 transverse process.
The main function of the sub occipital musculature is fine-tuning of position changes of the head. The oblique capitis inferior also acts as an active stabilizer of C1-2. Bilateral contraction of the sub occipital muscles extends the neck at O-A. Unilateral contraction of the sub occipital muscles side bends and rotates the upper cervical spine. The rotation at O-A is conjunct.
Trigger points of the sub occipital musculature are activated by sustained positions of the head. Referred pain from these muscles is “ghostly”. The definition is poor, but usually radiates from occiput to the orbit.
SternocleidomastoidLies immediately under the platysma. It has a sternal and a clavicular origin and inserts at the mastoid process. It is one of the prime movers of the head and neck
Longus colliDeepest anterior cervical muscle. It is multi layered and covers the entire anterior cervical spine from the anterior arch of the atlas to the vertebral body of T3. Contraction of the longus colli decreases the cervical lordosis and flexes the cervical spine. It plays an important role in stabilizing the cervical spine.
Longus capitis, rectus capitis anterior and lateralisLie in front of the longus colli. Main function is to provide upper cervical flexion
The hyoid musclesLie anterior of the cervical spine and due to their long lever arm are able to contribute significantly to neck flexion and stability of the cervical spine. They also open the mouth. They connect the hyoid to the mandible superior and to the thorax inferior.
5

ScaleniRun on the anterior lateral side of the cervical spine, connecting the cervical vertebrae with the 1st and 2nd rib. They function much like the mainstays on a sailboat. It consists of 3 muscles: The scalenus anterior runs from the C3-6 anterior TP’s to the superior anterior part of the1st rib.The scalenus medius lies behind the anterior, running from the C2-7 TP’s to the 1st rib where it attaches right behind the groove of the subclavian artery.The scalenus posterior lies behind the 2 previous muscles. It runs from the posterior C4-6 TP’s to the lateral part of the 2nd ribBetween the anterior and medial scalenus run the brachial plexus and the subclavian artery, which are both palpable in this region.Unilateral contraction of the scaleni causes the cervical spine to rotate and side bend to the same side. Bilateral contraction increases the cervical lordosis. They also function as primary muscles of inspiration.
On the posterior side of the cervical spine are 4 layers of muscles. The deepest layer consists of the small intrinsic muscles (transversospinal and interspinous muscles).
The second layer consists of the semispinalis capitis and the longissimus capitis. Lateral of these muscles are the iliocostalis cervicis and the longissimus cervicis and thoracis.
The third layer consists of the levator scapulae and the splenius capitis and cervicis.
The fourth superficial layer consists of the trapezius and the posterior lateral part of the sternocleidomastoid.
Splenius capitisRuns from the T1-3 spinous processes and nuchal ligament at C5-7 to the lateral part of the superior nuchal line and the mastoid process. It is a so-called spino-transverse muscle, which means that it causes rotation to the same side upon contraction. This allows us to differentiate it from the semispinalis capitis, which muscle rotates the head to the opposite side on contraction.
Semispinalis capitisAttaches to the C4-T6 TP’s and the C7-T1 SP’s. On the occiput it attaches just lateral of the external occipital protuberance. Vertical muscle belly, which fills up the gutter between the spinous and transverse processes. The left and right muscle belly are separated by the nuchal ligament. Bilateral contraction increases the cervical lordosis and extends the head.
Levator scapulaeFrom the C1-4 transverse processes to the superior angle of the scapula. Palpation is facilitated by active medial rotation of the scapula (place arm on back in full internal rotation, then move arm posterior). The muscle runs more ventrally than what we might
6
expect. The distal part of the muscle is harder to palpate, but lateral of C7 spinous process it’s possible to feel a rolling string. The insertion on the superior angle of the scapula is often very point tender.
PlatysmaMost superficial muscle of the anterior cervical region. Palpable and visible when opening the mouth as wide (lateral) as possible.
HyoidPalpate the mandible left and right with thumb and index finger. Follow the contour of the neck and slide caudally. The hyoid is then easily palpable. It’s horseshoe shaped and moves up and down with swallowing. The hyoid is at the level of C3. Palpate for mobility.
Thyroid cartilageOne fingers width under the hyoid the cartilage of the thyroid is palpable. The sharp edge where the cartilage plates meet is the Adam’s apple.
CricoidCaudally of the thyroid you can palpate a ring of cartilage: the cricoid. Caudally of the cricoid is the trachea. The cricoid is used for orientation purposes in the anterior cervical region. It lies at the level of C6. Here the vertebral artery enters the transverse foramen of C6. Lateral of the cricoid you can palpate the thyroid gland. Palpate the cricoid between thumb and indexfinger and have the patient swallow. The larynx and thyroid should move up and down. Size and consistency of the thyroid can then be evaluated.
The menisci of the cervical synovial jointsThree types of intra-articular inclusions are found in the synovial joints: capsular rims, intra-articular fat pads and fibro adipose meniscoid structures. At least one type of structure is found in each synovial joint.
Intra-articular fat padsArticular fat pads occupy the space bounded by the joint capsule and the perimeter of the articular cartilage and therefore remain outside the joint space. They are composed primarily of adipose tissue. They occur most frequently at O-A, where they are located medial or lateral of the facet of the atlas. At lower levels of the cervical spine their presence is rare and their disposition irregular.
Fibro-adipose meniscoidsThey are the most commonly found inclusion in joints at all levels of the cervical spine, except at O-A where the fat pads predominate. The fibro-adipose meniscoid has a thick base attached to the joint capsule, which tapers to a thin fibrous end, which protrudes into the joint for 2-5 mm.
7

Capsular rimsThey are stiff, wedge shaped intrusions of the joint capsule. They occur around the margin of the articular surface and do not enter the joint space, occupying the space between the joint capsule and the facet margin. The presence of the articular rims at each level is rare, most likely to occur at O-A. They appear to be internal thickenings of the joint capsule.
FunctionAt O-A the predominant structures were the articular fat pads. Their site suggests that they could be acting as displaceable space fillers. For this purpose neither synovial fluid nor fibrous tissue would serve as well as fat. Synovial fluid is not designed to fill cavities but rather to act as a lubricant while fibrous tissue would cause the joint to be stiff.The fibro adipose meniscoids, being located along the articular surfaces and attached to the capsule, would protect the exposed cartilage during joint motion by maintaining a film of synovial fluid between themselves and the cartilage.Capsular rims are rarely present, but their highest incidence is at O-A, where they fill the space around the rim and so help distribute forces.Because of their size and presence in such small joints, imaging of these structures is difficult so that discussion of their role in joint pathology must be speculative. The presence of meniscoids within the joint cavity provides an ideal site for tissue proliferation, which could develop into adhesions between the articular cartilage. Stiffness of cervical joints could be accounted for by fibrous tissue proliferation and such adhesions. Intra articular inclusion of the fibro adipose meniscus has also been implicated in acute locked necks. It is suggested that menisci slide into the joint, become trapped and so apply tension to the joint capsule resulting in pain and motion restriction. The mid cervical spine appears to be the most common clinical site of pain associated with acute locked necks.
8

Biomechanics
C0-C1The articular surfaces of the occipital condyles are bi-convex. The articular surfaces of the superior articular facets of C1 are bi-concave. The long axes of the superior facets converge anteriorly.
There are 2 degrees of movement:Sagital plane Flexion, extension
Frontal plane Sidebending (with conjunct rotation to opposite side)
Range of motionFlexion 5 degreesExtension 10 degreesSidebending 5 degrees to each sideRotation Minimal, conjunct
C1-C2The inferior articular surfaces of C1 are bi-convex.The superior articular surfaces of C2 are bi-convex. Although the actual bony configuration is concave, the configuration of the cartilage is such that the articular surface is convex.
A synovial joint is also present between the posterior surface of the anterior arch of the C1 and the anterior surface of the dens. There is also a synovial joint present between the posterior surface of the dens and the anterior surface of the transverse ligament.
The joint has 2 degrees of freedom:Transverse plane: rotationSagittal plane: flexion/extension
Range of motionRotation 35-40 degrees Flexion 5 degreesExtension 10 degrees
Arthrokinematics
Flexion of the upper cervical spine The convex occipital condyles glide backward on the concave facets of C1 The occiput moves upwards and away from the posterior arch of C1 C1 glides forward 2-3mm until the transverse ligament checks its motion
9

The posterior ligaments between occiput and C1 tighten and pull the posterior arch up while the anterior arch drops 2-4 mm.
When the slack in the posterior ligaments of C1-2 has been taken up, the spinous process of C2 goes up, and C2 flexes on C3
Extension of the upper cervical spine The occipital condyles glide forward on C1 The occiput moves caudally, approximating the posterior arch of C1 C1 is squeezed backwards 2-3 mm until its anterior arch butts up against the dens C1 tilts 12 degrees on C2. The anterior arch of C1 raises 2-4 mm while the posterior arch of C1 drops down The anterior ligaments at C1-2 tighten and pull up on C2, while the occiput and
posterior arch of C1 push down on C2, causing the inferior facets of C2 to glide down and back on the superior facets of C3
Rotation C0-C1 (left) Occiput rotates on C1 and its rotation is secondary to C1-2 rotation As rotation continues, the right alar ligament tightens The tension in the alar ligament pulls the right occipital condyle to the left, producing
right sidebending
Sidebending C0-C1 (right)During right sidebending of C0-C1, the right occipital condyle glides medial, inferior and anterior, while the left condyle glides lateral, posterior and superior.The right condyle, by moving anterior, now rests on the lower portion of the surface of C1, while the left has moved to the higher, posterior portion of C1. The inferior movement on the right, coupled with the superior movement on the left produces the sidebending of the occiput. During right sidebending, the left alar ligament will tighten up, causing right rotation of C2.
Rotation C1-C2 (left)C1 osteoligamentous ring moves around the dens in a counter clockwise fashion.This relaxes the left C1-2 capsule and stretches the C1-2 capsule on the right.C1 is pulled into a slight glide to the left so that the right lateral mass moves closer to the dens.The right lateral mass moves forward and its inferior articular surface drops down on C2 while the left lateral mass moves posteriorly and drops down on C2 on the left. This causes C1 to move 2-3 mm. caudally. There is also a momentary rotation of C2 to the right due to the pressure of C1 screwing down on it. As C1 continues to rotate to the left, motion is taken up at C1-2 and C2 eventually “pulls out” of its momentary right rotation and follows C1 to the left, producing left rotation atC2-3.
10

Premanipulative screening17
Before attempting to manipulate the cervical spine, two factors need to be taken into consideration. Ruling out the presence of cardinal signs and symptoms is a priority. They are considered to be extremely important as they suggest either vertebral/basilar artery insufficiency, or cervical cord compression. If such symptoms can be initiated, reproduced or aggravated by stressing the vertebral artery or by passive linear motions to the craniovertebral joints, then it’s reasonable to assume that there is possible insufficiency of the vertebral artery or that instability exists within the craniovertebral joint complex.
Risk factors upper cervical instabilityThe following risk factors are associated with the potential for bony or ligamentous compromise of the upper cervical spine:
History of trauma (e.g. whiplash, football neck injury) Congenital collagenous compromise (e.g. syndromes: Down’s, Ehlers-Danlos) Inflammatory arthritides (e.g. rheumatoid arthritis, ankylosing spondylitis) Recent neck/head/dental surgery.
Early presentation: Neck and head pain Feeling of instability Cervical muscle hyperactivity Constant support needed for head Worsening symptoms
Late presentation Bilateral or quadrilateral limb paresthesiae, either constantly or
reproduced/aggravated by head or neck movements. Hyperreflexia Clonus Positive Babinski or Hoffman’s Arm and leg weakness Lack of coordination bilaterally
Reproduction of pain is of questionable importance when stress testing for instability. Ask the patient: “tell me if you feel anything other than pain”. If a stress test produces no reaction from the patient other then pain, the test can be considered negative. If a cardinal sign or symptom is produced, the test is positive.
Keep in mind that the inert tissues being stressed are heavily innervated by the trigeminal nucleus (adjacent to C2-3), which in turn is being joined by a branch of the vagus nerve. Therefore, “obscure” or “bizarre” complaints may occur during stress testing of the upper cervical spine.
11
These are not cardinal symptoms, but definitely warrant caution: headaches, reluctance to move the head, difficulty lying down or lifting head from the pillow, vomiting, dizziness, disorientation, nausea, anxiety and a feeling of “a lump in the throat”.
When treating the upper cervical spine, stress tests should be done routinely, much like stress tests for knee ligaments are done routinely in a knee examination. The original discovery of life threatening complications due to high velocity trauma is rare. Even as rare as it is, if there exists even the suspicion of a life threatening instability, then the appropriate stress tests should obviously be performed.
Stability testing upper cervical spine
Assessment of ligament stability involves systematically working through a series of active/patient generated, passive/therapist generated and passive accessory motion testing, in order to feel the degree of movement at each joint (and therefore ligament integrity), as well as to produce the patient’s symptoms.
Active/patient generated testsPerformed with patient seated, minimal hands on required. This reduces the chance of significantly exacerbating patient’s status. Cervical rotation. Unable to move in presence of dens fracture Upper cervical sidebending Active upper cervical flexion. If the neck is unstable due to dens fracture and/or
transverse ligament tear, the patient will be unable to flex the neck and will substitute with chin protrusion. Local symptoms are ignored for the purpose of evaluating the test. If cardinal signs/symptoms are provoked the assumption can be made that they are caused by excessive translation of the atlas. So if a patient is able to flex the neck, a cervical fracture or transverse ligament tear can be ruled out.
Active upper cervical extension
Passive/therapist generated tests Distraction O-A, C1-2. Feel for separation. Patient seated Alar ligament stress test Compression lateral masses C1 to rule out Jefferson fracture Posterior shear occiput on C1. Patient supine. Therapist cups the head with both
hands, the pads of the indexfingers over the each posterior arch of C1. Translate C1 anterior on occiput.
Anterior shear occiput on C1, 2 Patient supine. Cradle occiput. Pads of index- and middlefingers placed on anterolateral aspect of the transverse masses of C1 and C2. Posterior glide both C1 and C2 on occiput.
Transverse ligament - modified Sharp Purser testPatient seated, with the head slightly flexed. Assess resting symptoms. Grasp the C2 spinous process with a pincer grasp. Gently at first, apply a posterior translation force from the palm of the hand on the patient’s forehead in a posterior direction. Assess amount of linear displacement. A positive test is identified either by reproduction of
12

myelopathic symptoms during forward flexion, or a decrease in symptoms during an anterior to posterior movement, or excess displacement during the AP movement.The specificity of this test is high. It differs from the original Sharp Purser, which was poorly defined and only consisted of upper cervical flexion. Specificity: 96 Sensitivity: 69
Upper motor neuron tests Babinski Hoffman’s. Flick patient’s middle finger. Positive if there is a flexion pattern of
indexfinger and thumb Dynamic Hoffman’s Flex/extend cervical spine a few times, flick middle
patient’s finger DTR’s Clonus Shimizu’s or ScapuloHumeral Reflex
Shimizu et al (Spine 1993) identified the ScapuloHumeral Reflex as and additional upper motor neuron test. The SHR is elicited by tapping the tip of the spine of the spine of the scapula and acromion in a caudal direction. It is classified as hyperactive when elevation of the scapula or abduction of the humerus occurs. The reflex center of the SHR is presumed to be located between C1-3. A hyperactive SHR provides useful information about dysfunctions of the upper motor neurons cranial to C3
Risk factors Cervical Arterial DysfunctionThe following risk factors are associated with an increased risk of either internal carotid or vertebrobasilar arterial pathology and should be thoroughly assessed during the patient history:
History of trauma to cervical spine / cervical vessels History of migraine-type headache Hypertension Hypercholesterolemia / hyperlipidemia Cardiac disease, vascular disease, previous cerebrovascular accident or transient
ischaemic attack Diabetes mellitus Blood clotting disorders Anticoagulant therapy Long-term use of steroids History of smoking Recent infection Immediately post partum Trivial head or neck trauma Absence of a plausible mechanical explanation for the patient’s symptoms.
13

Early presentation: Mid-upper cervical pain Pain around ear and jaw Head pain (front- temporo- parietal) Occipital headache Acute onset of pain described as "unlike any other”
Late presentation: Drop attacks Dizziness Dysphagia (difficulty swallowing) Dysarthria (speech change, either slurred or slowed) Diplopia (double vision) Nausea Nystagmus Facial lip paresthesiae/ facial numbness Cranial nerve dysfunction
Clinical Reasoning
The estimated risk of serious complications resulting from HVT of the cervical spine has been reported to range between 1 in 4500 (Dunne et al., 2000) to 6 in10 million (Hurwitz et al., 1996). The precise risk of injury is indeterminable due to the unknown number of unreported cases (Ernst, 2004; Carlesso et al. 2010) and the paucity of methodologically sound research studies (Kerry et al., 2008). Although the number of patients experiencing minor to moderate adverse events following manual therapy may be as high as 50%, the risk of major adverse events with manual therapy is reported to be low (Carlesso et al., 2010). Nevertheless, given the limitations of known prevalence and the serious nature of the adverse event, manipulation of the upper cervical spine remains a contentious issue
A case control study by Thomas et al looked at 21 patients < 55 years with radiologically confirmed vertebral or carotid artery dissection. They were interviewed about risk factors, preceding events and clinical features of their stroke24
Headache and neck pain, speech disturbance, limb weakness, and to a lesser extent balance disturbance and ptosis were the primary presenting features of CAD.
Importantly, a high proportion of participants (67%) with CAD reported antecedent transient ischemic features prior to their admission to hospital. This is considerably higher than rates reported prior to general stroke, which range between 3.8% and 15.7%.
14

These antecedent transient ischemic features have not been identified in previous studies and should prompt physical therapists to question patients carefully for such features.
Risk Factors TraumaRecent prior minor mechanical trauma or strain to the neck is an important feature in CAD. This may include cervical manipulation, but less vigorous manual techniques or exercises should also be considered.
The finding that recent minor mechanical trauma or strain to the neck was associated with CAD is consistent with the findings of other reports. There was no frank or extreme trauma described by participants with CAD, also consistent with data from previous reports
Trauma identified by participants fit into 3 main categories: abrupt or jerky head movements, particularly into extension or lateral flexion; intense or unusual physical effort, such as Valsalva-type maneuvers or high-intensity gym exercise; and activities involving sustained extended positions of the neck. It is recommended that clinicians question patients with recent-onset neck pain or headache about exposure to these types of activity within the last month.
15

SmokingTwenty-one percent of participants with CAD were smokers, reflecting the percentage of smokers for this age group in the general population. Smoking is associated with higher blood levels of inflammatory mediators, which may have implications for vessel-wall friability. However, no participant had elevated blood levels of any particular clinical inflammatory markers.
Infection21% of participants reported a recent infection prior to CADDespite the low incidence in this current study, and in respect to the higher incidence found in other studies, we recommend that clinicians specifically question patients presenting with recent-onset neck pain or headache about recent infection prior to manual therapy to the neck
Blood pressureHypertension is considered a risk factor for carotid and vertebral artery disease. An increase in blood pressure may be related to acute arterial trauma, including of the internal carotid and vertebral arteries. Evaluation of blood pressure as part of the physical examination may therefore be a valuable test to inform clinical reasoning. Normal range for a non-diabetic adult is 120-140 mmHg systolic / 70-90 mmHg diastolic. Although hypertension is an undoubtedly strong predictor of cardiovascular disease, interpretation of readings must be in the context of other findings, and sound clinical reasoning
Cardiovascular Risk FactorsGeneral cardiovascular risk factors, with the exception of diagnosed migraine, were not strongly represented in the CAD group, suggesting that they may not be useful indicators of risk of dissection. This is inconsistent with current recommendations for general cardiovascular screening prior to any cervical manual treatment.In summary, in regard to cardiovascular risk factors, a history of diagnosed migraine may be a potential risk factor for dissection; however, it may be difficult to distinguish the clinical presentation of migraine headache from a dissection in progress.
Cervical manipulationCervical manipulation was not a statistically significant factor in this study. Of concern is that any manual treatment could potentially be implicated if a patient with CAD were to seek treatment for neck pain or headache.
This study suggests that examination for joint hypermobility or skin elasticity is probably not useful in premanipulative screening prior to manual treatment of the cervical spine. Keep in mind though that this only pertains to assessing vertebral artery involvement. Assessing the upper cervical spine for ligamentous laxity is a must, and cannot be omitted from your evaluation of the cervical spine.
16

The major vascular complication after cervical manipulation occurred predominantly in young adults. This finding suggests that cervical osteoarthritic changes would not be the pathogenesis in the majority of these cases.
A study by Cassidy et al investigated the risk of vertebrobasilar stroke and chiropractic care3. In this case control study they found an association between chiropractic care and vertebral artery dissection and VBA stroke. However, they also found strong associations between PCP visits and subsequent VBA stroke. They found no evidence of excess risk of VBA stroke associated with chiropractic care compared to primary care. A plausible explanation for this is that patients with head and neck pain due to vertebral artery dissections seek care for these symptoms, which precede more than 80% of VBA strokes. Since it is unlikely that PCP’s cause stroke while caring for these patients, we can assume that the observed association between recent PCP care and VBA stroke represents the background risk associated with patients seeking care for dissection related symptoms leading to VBA stroke. Since the association between chiropractic visits and VBA stroke is not greater that the association between PCP visits and VBA stroke, there appears to be no excess risk of VBA stroke from chiropractic care. These results need to be interpreted cautiously though. Cervical manipulations as a potential cause of some VBA strokes have not been ruled out. On the other hand, it is unlikely to be a major cause of these rare events. The results suggest that the association between cervical manipulation and VBA stroke found in previous studies is likely explained by presenting symptoms attributable to vertebral artery dissection. To account for this uncertainty, it is probably prudent not to use manipulation in the initial few sessions for patients with acute onset of neck pain. It may be unclear if these patients are experiencing a rare VBI incident or more common mechanical neck pain.
It is very difficult however, to ignore the close temporal association between trauma and the number of cases of VA dissection, whether it is from manipulation, trivial trauma, MVA’s, or strenuous activity. Significantly, at times symptoms of VA dissection are acute neck pain and headache, which are exactly the symptoms for which patients seek treatment and for which they not uncommonly receive manipulation.
Provocative positional testing is frequently used in practice. It is intended to provide a challenge to the vascular supply to the brain, and the presence of signs or symptoms of cerebrovascular ischaemia during or immediately post testing is interpreted as a positive test. Sustained end-range rotation has been advocated, and has been described as the most provocative and reliable test. The sustained pre-manipulative test position has also been advocated.
Despite endorsement by guidelines and common clinical usage, current research does not support the contention that provocative positional testing can accurately identify patients at risk for cervical artery disease. Vertebral artery testing procedures have a sensitivity and specificity that approximates zero. This indicates a high likelihood of false negative findings.
17

Test procedures for the vertebral artery also hold a certain risk, and screening tests will not identify all patients at risk of suffering adverse reaction to cervical manipulation. There is also disagreement on what constitutes a clinically meaningful change in blood flow on cervical movement. It should be reiterated that there is no known method for testing the intrinsic anatomy of the vertebral artery. Doppler studies have shown that only full range cervical rotation and a pre-manipulative hold at C1-2 stresses the vertebral artery sufficiently to demonstrate reduction of bloodflow. Therefore the Clinical Guidelines of the Australian Physiotherapy Association recommend that only rotation be used to test for VBI1,57.
Biomechanically, cranio-cervical rotation is the movement most likely to be associated with arterial damage20,21,22. The part of the vertebral artery that extends from the point of exit from the axis to its entry into the spinal canal is reported to be the structure most vulnerable to mechanical insult and injury 25, 19
One underlying concern is that manipulation involving rotation may, at least momentarily, alter the velocity of blood flow in one or both of the vertebral arteries22. However, this argument seems to be dispelled by a study by Erhardt et al18. In this study they tried to quantify changes in blood flow velocity in the VA during manipulation of C1-2. The findings of this study indicate that in normal subjects, blood flow velocity of vertebral artery is not affected by manipulation of C1-2. Therefore, in apparently healthy vessels, manipulation of C1-2 does not appear to increase mechanical stress on the vertebral artery. It remains unknown whether adverse haemodynamic responses would be recorded in the presence of vessel hypoplasia, vessel wall pathology or inherent weakness.
As such this study indirectly supports a stance taken by IFOMPT that careful subjective and objective risk assessment combined with prudent clinical reasoning may be the way to progress for clinicians17.
Although a definitive sensitive exam has not been identified, continued manipulative intervention should be guided by patient’s response to treatment.In many reported cases where death or serious neurological events have been attributed to manipulation, practitioners ignored patient’s progressive symptoms of vertebrobasilar ischemia and continued manipulative treatment.
If there is a strong likelihood of vertebral artery disease, provocative pre-manipulative testing should not be performed, and the patient must be referred appropriately.
Although the risk of injury associated with manipulation of the upper cervical spine appears to be small, this type of therapy has the potential to expose patients to vertebral artery damage. Procedures that involved a rotational thrust had the largest representation. The occurrence of injury following manipulation of the upper cervical spine in patients without known systemic or vascular pathology and the absence of serious neurovascular accident during the first exposures to manipulation might provide indirect support for the
18

theory that cumulative sub clinical damage to the vertebral arteries occurs following upper cervical manipulation.
It is important to remember that in the early stages, vertebral artery pathology can commonly present as neuromusculoskeletal symptoms. It is often isolated to neck and head pain without commonly described VBI symptoms and can therefore be easily misdiagnosed as a strict mechanical problem. So despite a temporal relationship between an ischemic event and manual therapy intervention, the ischemic event may have already been in progress and thus not directly attributable to manipulative intervention.
Recent evidence also suggest that the amount of strain on the vertebral arteries during manipulation is similar to, or lower than, the strain recorded during ROM testing and other diagnostic testing procedures. Serious complications have also occurred following lower grade mobilization procedures, suggesting that the speed and amplitude of the technique used (i.e. manipulation vs. mobilization) may not be the only consideration necessary for prudent decision-making. End range movements are known to stress the cervical arteries and potentially neural structures. Thus avoidance of these positions is recommended during cervical manipulation48. Although evidence is limited, this principle also logically applies to techniques performed in end range neck positions during cervical mobilization and exercise interventions. Do not challenge the C spine beyond what it would encounter during exam and treatment.
A review by Puentedura et al of 134 cases describing patients who experienced severe adverse events after cervical manipulation showed that, if all contraindications and red flags were ruled out, there was potential for a clinician to prevent 44.8% of adverse events. Additionally, 10.4% of the events were unpreventable, suggesting some inherent risk associated with cervical manipulation even after thorough exam and proper clinical reasoning16.
Importance of observation throughout history takingSigns and symptoms of serious pathology and contraindications / precautions to treatment may manifest during the patient history stage of assessment. This is an opportunity to observe and recognize possible red flag indicators such as gait disturbances, subtle signs of disequilibrium, upper motor neuron signs, cranial nerve dysfunction, and behavior suggestive of upper cervical instability (e.g. anxiety, supporting head/neck) early in the clinical encounter.
Alternative approaches to direct cervical treatmentEmerging pain sciences suggests that the effects of mobilization/manipulation on pain may be largely neurological in nature and not limited to the direct influence of a particular spinal motion segment. Furthermore, clinical trials have reported that thoracic spine manipulation results in improvements in perceived levels of cervical pain, ranges of motion, and disability in patients with mechanical neck pain, although the mechanism by which this occurs is not known34, 43,71. A RCT by Young et al71 showed that 1 session of thoracic manipulation to patients with cervical radiculopathy resulted in improved pain, disability, cervical ROM, and deep neck flexor endurance compared to those patients
19

treated with sham manipulation. Patients treated with manipulation were also more likely to report at least moderate change in their neck and upper extremity symptoms up to 48 to 72 hours following treatment
Given the concern regarding the risks associated with cervical spine manipulation, thoracic spine manipulation provides an alternative, or supplement to, cervical manipulation and mobilization to maximize the patient’s outcome with an extremely low level of risk. The current evidence suggests that during the initial treatment sessions there is a large likelihood of improved patient outcomes when thoracic manipulation is coupled with cervical active range of movement exercises. Subsequent sessions can then introduce more direct manual cervical treatments if warranted.
SummaryUpper cervical manipulations should be used with caution. Use of this technique should be based upon sound clinical reasoning: a thorough physical therapy examination, an evidence-based interpretation of the clinical state and circumstances, patient preferences and actions, and the research literature. Stay away from endrange techniques, especially extension and rotation. Incorporate T spine manipulation in the treatment of C spine disorders.
Patients may present for treatment of acute-onset headache or neck pain arising from a dissection in progress. Individuals with CAD may have transient ischemic signs and symptoms as warning signs in the preceding few weeks. General cardio- vascular risk factors do not appear to be associated with dissection, with the exception of diagnosed migraine.
Clinicians should carefully question patients presenting with recent onset, moderate to severe, or unusual neck pain or headache about minor trauma and any signs of visual disturbance, dizziness and balance deficits, arm paresthesia, or speech deficits.
Events and presentations of cervical artery dysfunction are rare, but are an important consideration as part of your assessment. Arterial dissection and other vascular presentations are fairly recognizable if the appropriate questions are asked during the patient history, if interpretation of elicited data enables recognition of this potential, and if the physical exam can be adapted to explore any vasculogenic hypothesis further.
Based on the current evidence, there is no strong foundation for the claim that there is a causal relationship between cervical manipulation and vertebral artery dissection or stroke. There is no strong empirical evidence to support the notion that upper cervical manipulation carries any greater risk of injury than middle or lower cervical manipulation, or that non thrust mobilization to any region of the cervical spine carries any less risk than manipulation to the same region.
20
The exact mechanism and risk factors for vertebral artery dissection must be considered no more than speculation at this time. The occurrence of stroke following manipulation appears to be a rare and unpredictable event. It is very difficult to definitely determine exactly which patients are at serious risk. Do not further examine or treat a patient with signs and symptoms of cervical artery disease. You cannot ignore the presence of cardinal signs and symptoms. A patient with cardinal signs and symptoms warrants a referral to a medical specialist for appropriate management.
Develop a high index of suspicion for cervical vascular pathology, particularly in cases of cervical trauma. Be aware of the limitations of current objective tests. Reliance on objective testing alone represents incomplete clinical reasoning. In cases of acute onset headache “unlike any other”, conservative treatment techniques are recommended in the early stages.
21

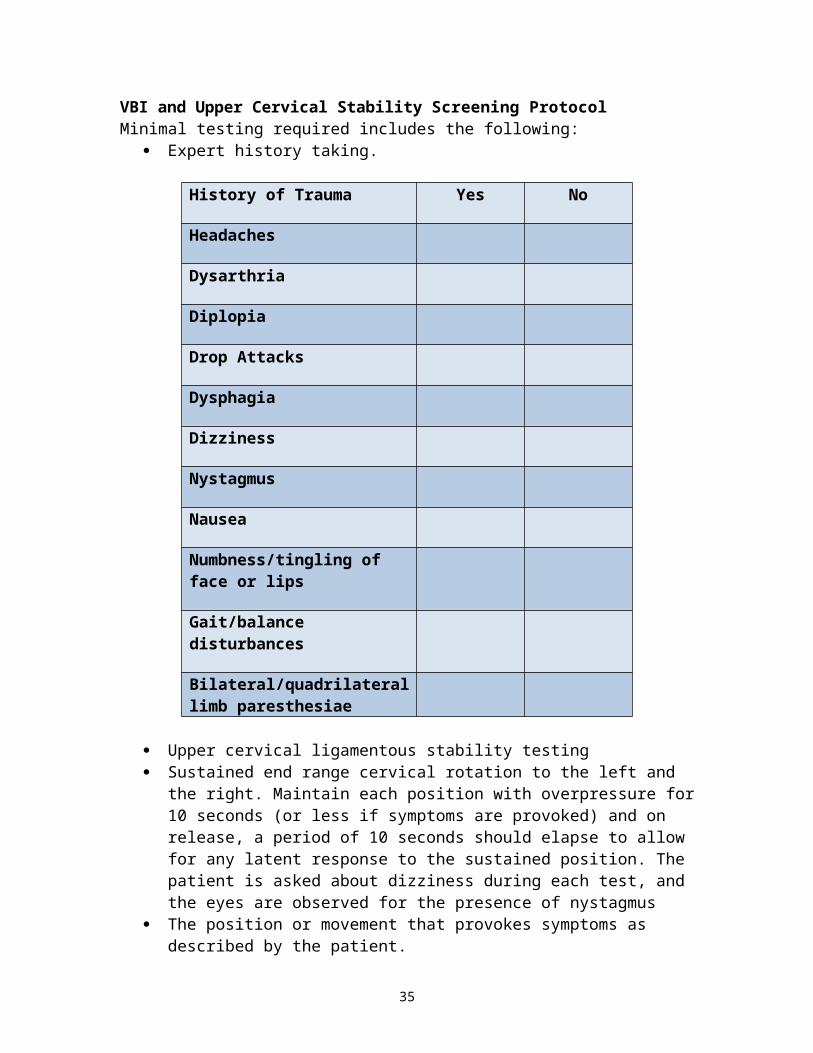
VBI and Upper Cervical Stability Screening ProtocolMinimal testing required includes the following:
Expert history taking.
History of Trauma Yes No
Headaches
Dysarthria
Diplopia
Drop Attacks
Dysphagia
Dizziness
Nystagmus
Nausea
Numbness/tingling of face or lips
Gait/balance disturbances
Bilateral/quadrilateral limb paresthesiae
Upper cervical ligamentous stability testing Sustained end range cervical rotation to the left and the right. Maintain each
position with overpressure for 10 seconds (or less if symptoms are provoked) and on release, a period of 10 seconds should elapse to allow for any latent response to the sustained position. The patient is asked about dizziness during each test, and the eyes are observed for the presence of nystagmus
The position or movement that provokes symptoms as described by the patient. Sustained mobilization position
Specific questioning regarding reproduction of symptoms suggestive of VBI is essential and should be included:
Immediately before and after a cervical manipulation During and immediately after a technique involving endrange rotation
22

Informed consentLast, but not least, you have to obtain informed consent26,39. We recommend you obtain verbal consent and document it as such in your notes. Since specific requirement for informed consent differ from country to country and more importantly for us, from state to state, it is difficult to specify how this needs to be worded. We recommend something along the following lines:
"I would like to perform a "quick stretch" on your neck to improve range of motion of a particular joint. This is likely to improve and/or eliminate your neck, shoulder symptoms (also could refer to arm or headache). You may sense a "popping" of the joint and may experience some local soreness due to the stretching procedure. Is it ok to perform this quick stretch?"
The use of the term “quick stretch” circumvents the use of the word manipulation, which in many states can give rise to problems.
23

Typical case histories of vascular dysfunction
Common vertebral artery dissection
Case:A 46 year-old female supermarket worker presented to physical therapy with left-sided head (occipital) and neck pain described as “unusual”. She reported a 6 day history of the symptoms following a road traffic accident. The symptoms were progressively worsening. The pain was eased by rest. She reported a history of previous road traffic accidents. Past medical history included hypertension, high cholesterol, and a maternal family history of heart disease and stroke. Cranial nerve tests for VIII, IX, and X were positive and resting blood pressure was 170/110. Two days after assessment, the patient reported an onset of new symptoms including “feels like might be sick”, “throaty” and “feels faint” – especially after performing prescribed neck exercises. Two days after this, she reported a stronger feeling of nausea, loss of balance, swallowing difficulties, speech difficulties and acute loss of memory. Magnetic resonance arteriography revealed an acute hindbrain stroke related to a left vertebral (extra-cranial) artery dissection.Synopsis:A typical background of vascular risk factors and trauma, together with a classic pain distribution for vertebral arterial somatic pain which was worsening. Positive signs (blood pressure and cranial nerve dysfunction) were suggestive of cervical vascular pathology. Signs of hindbrain ischaemia developed in a typical time period post-trauma.
Vertebral artery with pain as the only clinical feature
Case:A friend presents to a physical therapist with a sore neck and unremitting headache. The individual complains that they “think” their “neck is out”. They ask if they can have their neck manipulated to “put it back in”. The headache has been present for 3-4 days and is getting worse. They note that the pain has been unrelieved by medication (paracetamol) and it appears to be of a mechanical presentation. Without taking a full history and carrying out a physical examination, the physical therapist goes ahead and manipulates the neck. The result was the individual experiencing numbness and paralysis to their left arm and hand.Synopsis:Investigation post incident identified an intimal tear of the vertebral artery. The key issue in this case is that the presentation was not fully assessed through a detailed history and physical examination. The warning feature from the history of worsening pain, unrelieved by medication, combined with an inadequate physical examination and limited clinical reasoning, all contributed to an unfortunate and probably avoidable outcome.
24

Internal carotid artery dissection
Case:A 42 year-old accountant presents to physical therapy with a 5 day history of unilateral neck and jaw pain, as well as temporal headache, following a rear-end motor vehicle collision. There is a movement restriction of the neck and the physical therapist begins to treat with gentle passive joint mobilisations, and advises range of movement exercises. The following day, the patient’s pain is worse, and he has developed an ipsilateral ptosis. The patient’s blood pressure is unusually high.Synopsis:On medical investigation, an extra-cranial dissection of the internal carotid artery was found. The patient had underlying risk factors for arterial disease, and the presentation was typical of internal carotid artery dissection, with a key differentiator being the ptosis. A dramatic systemic blood pressure response was a result of this vascular insult.
References
1. Arnold, C. et al. Doppler studies evaluating the effect of a physical therapy screening protocol on vertebral artery blood flow. Man. Ther. 2004:9:13-21
2. Baracchini C, Tonello S, Meneghetti G, Ballotta E. Neurosonographic monitoring of 105 spontaneous cervical artery dissections A prospective study. Neurology. 2010;75:1864e70.
3. Cassidy, J. et al. Risk of vertebrobasilar stroke and chiropractic care: results of a population based case control and case cross over study. Spine.2008
4. Childs, J. et al. Screening for vertebrobasilar insufficiency in patients with neck pain: manual therapy decision making in the presence of uncertainty. JOSPT.2005:5(5)
5. Childs, J. et al.(2002) Physical Therapy for the cervical spine and TMJ. APTA Home Study Course 13.3.1,
6. DiFabio, R. Manipulation of the cervical spine: risks and benefits. Phys Ther.1999; 79(1)7. Grant R. Premanipulative testing of the cervical spine - reappraisal and update. Physical
Therapy of the Cervical and Thoracic Spine, 3rd edition. Elsevier 2002 8. Haldeman S, Kohlbeck FJ, McGregor M (1999) Risk factors and precipitating neck
movements causing vertebrobasilar artery dissection after cervical trauma and spinal manipulation, Spine1999;24(8): 785
9. Mitchell, Changes in vertebral artery blood flow following normal rotation of the cervical spine. J Man Phys Ther.2003
10. Thiel, H. and Rix, G. Is it time to stop functional pre-manipulation testing of the cervical spine? Man Ther.2005
11. Cassidy J et al. Risk of vertebrobasilar stroke and chiropractic care. Results of a population based case control and case crossover study. Spine. 2009;33(45)
12. Kerry, R. and Taylor, A. Cervical Artery dysfunction: knowledge and reasoning for manual physical therapists. JOSPT. 2008;39(5)
13. Haldeman, S and Kohlbeck, F. Unpredicability of cerebrovascular ischemia associated with cervical spine manipulation therapy: a case review of 64 cases after spinal manipulation. Spine. 2002;27(1):49-55
14. Dunning, J et al. Upper Cervical and Upper Thoracic Thrust Manipulation Versus Nonthrust Mobilization in Patients With Mechanical Neck Pain: A Multicenter Randomized Clinical Trial. JOSPT .2012;(42):1
15. Dunning, J and Cleland, J.(2012) Cervical and thoracic mobilization versus manipulation for mechanical neck pain. Letters to the editor-response. JOSPT .2012;42(4)
16. Puentedura E et al. Safety of cervical spine manipulation: are adverse events preventable and are manipulations being performed appropriately. A review of 134 case reports. JMMT.2012;20 (2)
25

17. Rushton A, Rivett D, Carlesso L, Flynn T, Hing W, and Kerry R. International Framework for Examination of the Cervical Region for potential of Cervical Arterial Dysfunction prior to Orthopaedic Manual Therapy Intervention. IFOMPT consensus document 2012
18. Erhardt JW et al. The immediate effect of atlanto axial high velocity thrust techniques on bloodflow in the vertebral artery. A randomized controlled trial. Man Ther. 2015 http://dx.doi.org/10/1016
19. Macchi C, Giannelli F, Cecchi F, Gulisano M, Pacini P, Corcos L, et al. The inner diameter of human intracranial vertebral artery by color Doppler method. Italian J Anat Embryol 1996; 1⁄4 Archivio Italiano di Anatomia ed Embriologia ;101:81e7.
20. Malo-Urries M, Tricas-Moreno M, Lucha-Lopez O, Estebanez-de-Miguel E, Hidalgo- Garcia C, Perez-Guillen S. Vertebral and internal carotid artery flow during vascular premanipulative testing using duplex Doppler ultrasound measurements: a systematic review. Int J Osteopath Med 2012.15:103e10
21. Mitchell J. Vertebral artery blood flow velocity changes associated with cervical spine rotation: a meta-analysis of the evidence with implications for professional practice. J Man Manip Ther. 2009;17:46e57
22. Mitchell J, Keene D, Dyson C, Harvey L, Pruvey C, Phillips R. Is cervical spine rotation, as used in the standard vertebrobasilar insufficiency test, associated with a measureable change in intracranial vertebral artery blood flow? Man Ther .2004;9:220e7
23. Sturzenegger M, Mattle HP, Rivoir A, Rihs F, Schmid C. Ultrasound findings in spontaneous extracranial vertebral artery dissection. Stroke. 1993;24:1910e21.
24. Thomas L, Rivett D, Attia H and Levi C. Risk factors and clinical presence of cervical arterial dissection: preliminary results of a prospective case control study. JOSPT. 2015;45 (7)
25. Kuether TA, Nesbit GM, Clark WM, Barnwell SL. Rotational vertebral artery occlu- sion: a mechanism of vertebrobasilar insufficiency. Neurosurgery . 1997;41: 427e32. discussion 32.
26. Appelbaum PS, Lidz CW, Meisel A (1987). Informed Consent: Legal theory and clinical practice. Oxford University Press, New York.
27. Asavasopon S, Jankoski J, Godges JJ (2005). Clinical diagnosis of vertebrobasilar insufficiency: resident’s case problem. Journal of Orthopaedic and Sports Physical Therapy 35:645-650.
28. Atallah PC, Atallah P, Kashyap V (2010). Internal carotid artery aneurysm discovered by palpation of asymmetric pulses. The American Journal of Medicine 123(7):e1-e2.
29. Caplan LR, Biousse V (2004). Cervicocranial arterial dissections. Journal of Neuroophthalmology 24:299-305.
30. Carlesso LC, Gross AR, Santaguida PL, et al (2010). Adverse events associated with the use of cervical manipulation and mobilization for the treatment of neck pain in adults: A systematic review. Manual Therapy 15(5):434-44.
31. Carlesso L, Rivett D (2011). Manipulative practice in the cervical spine: a survey of IFOMPT member countries. Journal of Manual and Manipulative Therapy 19(2):66-70.
32. Cattrysse E, Swinkels R, Oostendorp R, et al (1997). Upper cervical instability: are clinical tests reliable? Manual Therapy 2(2):91-97.
33. Chan CCK, Paine M, O'Day J (2001). Carotid dissection: a common cause of Horner's syndrome. Clinical and Experimental Ophthalmology 29:411-415.
34. Cleland JA, Childs JD, Fritz JM, et al (2007a). Development of a clinical prediction rule for guiding treatment of a subgroup of patients with neck pain: use of thoracic spine manipulation, exercise, and patient education. Physical Therapy 87:9-23.
35. Cleland JA, Glynn P, Whitman JM, et al (2007b). Short-term effects of thrust versus nonthrust mobilization/manipulation directed at the thoracic spine in patients with neck pain: a randomized clinical trial. Physical Therapy 87:431-440.
36. Cook C, Brismee JM, Fleming R, et al (2005). Identifiers suggestive of clinical cervical spine instability: a Delphi study of physical therapists. Physical Therapy 85(9):895-906.
26

37. Crum B, Mokri B, Fulgham J (2000). Spinal manifestations of vertebral artery dissection. Neurology 55:302-306.
38. Debette S, Leys D (2009). Cervical-artery dissections: predisposing factors, diagnosis, and outcome. Lancet Neurology 8(7):668-78.
39. Delany C (2005). Respecting patient autonomy and obtaining their informed consent: ethical theory - missing in action. Physiotherapy 91:197-203.
40. Ernst E (2004). Cerebrovascular complications associated with spinal manipulation. Physical Therapy Reviews 9(1):5-15.
41. Fenety A, Harman K, Hoens A, et al (2009). Informed consent practices of physiotherapists in the treatment of low back pain. Manual Therapy 14(6):654-60.
42. Flynn TW, Wainner RS, Fritz JM (2006). Spinal manipulation in physical therapist professional degree education: A model for teaching and integration into clinical practice. J Orthop Sports Phys Ther 36(8):577-587.
43. Gonzalez-Iglesias J, Fernandez-de-las-Penas C, Cleland JA, et al (2009). Thoracic spine manipulation on the management of patients with neck pain: A randomized clinical trial. Journal of Orthopaedic and Sports Physical Therapy 39(1):20-27.
44. Greenman PE (1996). Principles of Manual Medicine, 2nd edn. Wilkins and Wilkins, Baltimore.
45. Gross A, Goldsmith C, Hoving JL, et al (2007). Conservative management of mechanical neck disorders: a systematic review. Journal of Rheumatology 34(5):1083-1102.
46. Haneline M, Lewkovich G (2004). Identification of internal carotid artery dissection in chiropractic practice. J Can Chiropr Assoc 48(3):206-10.
47. Hartman L (1997). Handbook of OsteopathicTechnique, 3rd edn. Chapman & Hall, London.48. Hing WA, Reid DA, Monaghan M (2003). Manipulation of the cervical spine. Manual
Therapy 8(1):2-9.49. Hurwitz EL, Aker PD, Adams AH, Meeker WC, Shekelle PG. (1996). Manipulation and
mobilization of the cervical spine. A systematic review of the literature. Spine 21(15):1746e59. Discussion 1759e60
50. Kaale BR, Krakenes J, Albrektsen G, et al (2008). Clinical assessment techniques for detecting ligament and membrane injuries in the upper cervical spine region: a comparison with MRI results. Manual Therapy 13(5):397-403.
51. Kerry R, Taylor AJ, Mitchell J, et al (2007). Manipulation Association of Chartered Physiotherapists, Cervical Arterial Dysfunction and Manipulative Physiotherapy: information document. Available at: http://www.macpweb.org/home/index.php?p=170
52. Kerry R, Taylor AJ, Mitchell JM, et al (2008). Cervical arterial dysfunction and manual therapy: A critical literature review to inform professional practice. Manual Therapy 13(4):278-288.
53. Krauss J, Creighton D, Ely JD, et al (2008). The immediate effects of upper thoracic translatoric spinal manipulation on cervical pain and range of motion: a randomized clinical trial. J Man Manip Ther 16(2):93-99.
54. Mintken PE, Metrick L, Flynn TW (2008a). Upper cervical ligament testing in a patient with os odontoideum presenting with headaches. J Orthop Sports Phys Ther 38(8):465-475.
55. Mintken PE, DeRosa C, Little T, et al (2008b). AAOMPT clinical guidelines: A model for standardizing manipulation terminology in physical therapy practice. J Orthop Sports Phys Ther 38(3):A1-A6.
56. Mitchell J, Keene D, Dyson C, et al (2004). Is cervical spine rotation, as used in the standard vertebrobasilar insufficiency test, associated with a measureable change in intracranial vertebral artery blood flow? Manual Therapy 9(4):220-7.
57. Moore A, Jackson A, Jordan J, et al (2005). Clinical guidelines for the physiotherapy management of whiplash associated disorder. Chartered Society of Physiotherapy, London.
58. Murphy DR (2010). Current understanding of the relationship between cervical manipulation and stroke: what does it mean for the chiropractic profession? Chiropractic and Osteopathy 18:22.
59. Panjabi MM, White AA (1990). Physical properties and functional biomechanics of the spine. In: Clinical Biomechanics of the Spine, 2nd edn, Chapter 1. Philadelphia, J. B. Lippincott. P33.
27

60. Rao R (2002). Neck pain, cervical radiculopathy, and cervical myelopathy. The Journal of Bone and Joint Surgery 84A(10):1872-1881.
61. Rivett DA (2004). Adverse effects of cervical manipulative therapy. In J.D. Boyling and G.A. Jull (eds.), Grieve’s Modern Manual Therapy of the Vertebral Column (3rd ed). Churchill Livingstone: Edinburgh 533-549.
62. Rivett DA, Shirley D, Magarey M, et al (2006). Clinical Guidelines for Assessing Vertebrobasilar Insufficiency in the Management of Cervical Spine Disorders. Australian Physiotherapy Association: Melbourne.
63. Rogalewski A, Evers S (2005). Symptomatic hemicrania continua after internal carotid artery dissection. Headache 45:167-169.
64. Rubinstien SM, Saskia M. Peerdeman SM, et al (2005). A systematic review of risk factors for cervical artery dissection. Stroke 36: 1575-80.
65. Savitz S, Caplan L (2005). Vertebrobasilar Disease. The New England Journal of Medicine 352:2618-2626.
66. Taylor AJ, Kerry R (2005). Neck pain and headache as a result of internal carotid artery dissection: implications for manual therapists - case report. Manual Therapy 10:73-77
67. Taylor AJ, Kerry R (2010). A ‘system based’ approach to risk assessment of the cervical spine prior to manual therapy. International Journal of Osteopathic Medicine 13:85-93
68. Thanvi B, Munshi SK, Dawson SL, et al (2005). Carotid and vertebral artery dissection syndromes. Postgraduate Medical Journal 81(956):383-8.
69. Thomas LC, Rivett DA, Attia JR, et al (2011). Risk factors and clinical features of craniocervical arterial dissection. Manual Therapy 16(4):351-356.
70. Walker MJ, Boyles RE, Young BA, et al (2008). The effectiveness of manual physical therapy and exercise for mechanical neck pain: a randomized clinical trial. Spine 33(22):2371-2378.
71. Young I, et al (2019) Immediate and short term effects of thoracic spine manipulation in patients with cervical radiculopathy: a randomized controlled trial. JOSPT 49(5):299-309
28

Manipulations
Critical rules for cervical manipulations Don’t overlock No follow through on the thrust Low amplitude
Additional good advice to follow when manipulating the cervical spine: Use minimal leverage Use non torsional techniques There should be no pain Use multiple components so the main thrust can be minimal Excessive force conceals weakness
O - A distraction, supinePatient supine. Occiput in slight right rotation and left sidebending and slight extensionContact; under left mastoid process. Thrust occiput cranially.
O-A distraction, sidelyingPatient in right side lying. Occiput in slight rotation, sidebending and slight extension. Contact under left mastoid process. Thrust cranially.
29

O-A seatedFor the left side. Patient seated. Fingertip of the middle finger of the left hand contacts anterior left C1 TP. Turban grip around head. Slight right rotation, compression, sideshift towards you, sidebend away. Pull back on C1 and at the same time compress the head and thrust in rotation (posterior direction with left hand, anterior direction with the right hand)
C1-2, supineFor restriction in right rotation. Rotate the head 30 degrees. Main component is rotation. Sidebend left, sideglide right, a bit of extension. This should bring you to the barrier. The thrust is performed with a quick supination thrust with the right hand.
u
30

C1-2 distraction, supine Patient supine. Cradle the head with the right arm. Contact: posterior arch of C1, behind the TP with the left arm. Thrust C1 cranially on C2.
C1-2 distraction, sidelyingPatient in right side lying. Occiput/atlas in left side bending and left rotation. C2 in mid position. Contact the posterior arch of C1, behind the TP. Thrust C1 (and occiput) cranially - on the left side.
31

C2 - 3 distraction, supinePatient supine. Occiput/atlas/axis: slight left sidebending and right rotation. Contract: left inferior facet of C 2. Thrust C 2 cranially.
Mid cervical seatedStand slightly behind the patient. Your feet are pointed in an anterior direction. Wrap the middlefinger of the left hand around the SP. Cup the right hand over the ear. Primary component: rotation. Secondary components: sidebend, sideshift to the left, mild extension, compression. Then move the C spine in small circles to locate the barrier. Keep your touch very light in this technique.
32

Mid cervical supineFor restriction in left rotation. The main component is left rotation. Additional components: sidebend right, sidehift left by moving your hips to the left, compress both thumbs down on pt’s cheekbones, a little distraction pull of the left hand, then abduct the right indexfinger. Don’t necessarily extend the patient’s neck. Rotate the head three times to fine tune the barrier, thrust
Distraction CT - sittingPatient seated on plinth, hands clasped behind neck. Therapist stands behind patient, holds patient in “full nelson”. Thrust cranial. Make sure not to flex patient’s head during manipulation.
33

Chin pivot thrustPatient prone while resting on chin. Therapist stands at head end. Sidebend the head away, then rotate the head towards the restriction. Stabilize head with one hand. The other hand crosses over, and engages the opposite TP with the pisiform. Thrust in anterior, somewhat inferior direction.
34
Muscle imbalance upper quarter
Cervical extension/rotation syndromeInsufficient scapular upward rotation syndrome
Most common upper quarter syndrome. Frequently seen in this combination. Many patients sit prolonged working with computer and poor ergonomic seating.
Symptoms
Typically unilateral but not always. Pain with overhead work. Predisposed to joint locking. Impingement. Problems lying on either side. Associated with mid, lower and especially upper trapezius strain. Headaches.
Signs Compensatory cervical extension with movements of upper extremity Hypermobility often seen. Forward head and rounded shoulders. Crease or hinge point lower cervical spine Hyperextension upper cervical spine Clavicle horizontal or lower; depressed shoulder. One arm may appear longer than the other. Long neck. Heavy arms. Keyboard, arm rests too low. Wears bifocals. Cervical hyperextension when raise arms overhead. Raise one arm overhead and palpate spinous processes. Vertebrae will rotate to
opposite side with this syndrome. Superior angle of scapula lower than spinous process of T 2. Position of scapulae Weak neck flexors. Short pectoralis minor, major and latissimus dorsi. Quadruped rock back, head and neck go into extension. Quadruped and neck flex, see “cogwheel” motion.
35

Key tests
Cervical Rotation
With patient seated have them rotate head. Notice range of motion and quality (is the head and neck rotating on vertical axis). Therapist then goes behind patient and elevates scapulae to their normal position (between T-2 and T-9 vertebrae). Grasp the lateral border of scapulae to achieve this elevation. Now have patient rotate head again noticing ROM, quality and if this eliminates or reduces the patient’s symptoms/pain.
Cervical FlexionPatient seated and have patient flex head and neck. Notice ROM and quality. Notice if patient does not flex any part of the neck , typically lower cervical. Make sure not shearing at certain level. Axis of movement should be through the ears. A good verbal cue is to have them bring chin towards their Adam’s apple instead of chin to chest. Using verbal and/or manual cues, have patient correct this movement fault. Repeat and notice if reduces or eliminates patient’s symptoms/pain. There ROM may not be full but stop movement before shearing/extension occurs.
36

Single Arm ElevationPatient typically standing but could do this seated. Raise one arm overhead. Palpate inferior angle of scapula of arm being raised, this angle should get to the mid axillary line. If this causes the patent’s symptoms/pain, manually assist scapula into upward rotation and see if this reduces or eliminates pain.
Bilateral Arm ElevationHave patient raise arms overhead. Notice if neck goes into extension and/or shears. Verbally and/or manually correct movement impairment and notice if decreases/eliminates symptoms.
Scapular PalpationScapula should be between T-2 and T-7Vertebral border of scapula should be 3 inches from spinous processesThe root of the spine of the scapula should be in a vertical line with the inferior angleThe inferior angle and vertebral border of the scapula should be flat against rig cageThe scapula should be 35 degrees internal rotation from vertical plane through AC joint
37

Dominant RhomboidPatient’s elbow flexed 90 degrees and in medial rotation, forearm resting on abdomen. PT palpates vertebral border of scapula. Patient then lateral rotates arm. Vertebral border should not move with in the first 50% of movement.
Arm Elevation/Cervical RotationPatient seated or standing. Patient actively elevates/flexes arm, while PT palpates mid cervical spinous processes. If the spinous process rotates towards the side of the arm being elevated, the upper trapezius is insufficient and dominating the intrinsic cervical muscles. If the spinous processes rotated away, then the levator scapulae is dominant.
38

Manual Muscle Tests
Upper trapeziusPatient seated or standing. Patient actively elevates shoulders with arms overhead to isolate the upper trapezius from levator scapulae. Therapist then fully elevates the patient’s shouldergirdle. Hold it for 5 seconds to see if there is any give in the shoulder. If not, can add some manual resistance in inferior direction.
Serratus anteriorPatient seated. Check for the ability of the serratus to stabilize the scapula in a position of abduction and lateral rotation with the arm in approximately 120-130 degrees of flexion. When bringing the arm in flexion, the scapula is also brought in abduction. Rest the patient’s arm on the therapist’s shoulder and have the patient relax the arm. The PT monitors the inferior angle of the scapula. The PT then steps away from under the patient’s arm so the patient is holding the arm at 120 degrees flexion just against gravity. If the inferior angle of the scapula moves medially i.e. into adduction/downward rotation, then the test is already over and the serratus anterior is at least less than 3/5. If the scapula does not move then the PT applies pressure with one hand against the dorsal surface of the arm just above the elbow. The PT at this time grades the serratus.
Middle trapezius
39

Patient prone. Head and neck in neutral position, may need to use towel roll. Therapist horizontally abducts the arm at 90 degrees with external rotation and passively adducts the scapula. Patient then actively holds the arm against gravity while therapist monitors the inferior angle and medial border of the scapula for any movement. If patient is able to stabilize the scapula against gravity, therapist can add manual resistance to the arm. Also watch for anterior glide of humerus.
Lower trapeziusPatient prone. Head and neck in neutral position, may use a towel roll under the forehead. Therapist adducts, depresses, and slightly upwardly rotates the scapula along with arm flexion and external rotation. Patient then holds the UE against gravity while therapist monitors the scapula for movement, particularly elevation or tilting forward. If patient can stabilize the scapula against gravity, you can add manual resistance against the UE.
Rhomboids
40

Patient prone, head in midline. Therapist places one hand on the superior portion of the shoulder, the other hand on the elbow. Adduct the scapula with downward rotation and elevation of the shoulder girdle. First see if patient can hold the scapular position against gravity. If so, add resistance by depressing and derotating (in this picture my left hand is trying to pull the distal humerus into abduction) the scapula. Use the arm as a lever
SubscapularisPatient supine. Humerus abducted 90 degrees and elbow flexed 90 degrees. Place the humerus in neutral position. Typically the humeral head is forward so re-position with towel roll if necessary. Apply resistance to internal rotation.
Deep Neck Flexors (DNF)Patient seated with good posture. PT places one hand on patient’s forehead and the other on patient’s upper back. Force is A-P, resisting flexion. Patient should be able to hold this without cervical extension/shearing. To compare, place head on back of patient’s head and resist P-A, resisting extension.
41

Treatment
The primary objectives of treatment are to limit the degree of cervical extension during daily activities, to improve the control, strength, and performance of the intrinsic neck flexor muscles (longus colli, longus capitis, rectus capitis anterior and lateralis). With the scapula depressed and downwardly rotated it does not elevate and upwardly rotate with upper extremity elevation. Muscle impairments may include dominance, stiffness or shortness of depressor muscles (latissimus dorsi, pectoralis minor and major) and insufficient activity or lengthened upward rotators and elevators (upper trapezius, lower trapezius and serratus anterior).
Anterior cervical spine- A-P mobilizationPerform with gentle handling skills. Passively flex patient’s head and neck ,while performing a sustained A-P mobilization.
Functional Movement Pattern to improve cervical rotation
42

Functional Movement Pattern and STM to improve cervical flexion
Deep cervical flexion strengthening.
Correct Incorrect
It is often observed that patients with neck pain have problems with upper cervical flexion. The patient must be able to perform this correctly before any further training is undertaken. The pressure biofeedback is used to guide training. The feedback is motivational and allows the therapist to gain some quantification of improvement to guide progression of the exercise. Training is started at 22 mmHg. The movement is facilitated with eye movement into the flexion direction and emphasis is always on precision and control. Fast movements are discouraged as they often mask inadequacies in the deep neck flexors. The emphasis needs to be on craniocervical flexion. Shearing in the cervical spine should be avoided. Training should be short of fatigue so that incorrect movement patterns do not occur. For each pressure level the holding time is 10 seconds, and 10 repetitions are performed. At this point the exercise is progressed to the next level. The goal is to get to 10 repetitions of 10 second holds at 30 mmHG. Once this is accomplished correctly, begin single arm flexion while maintaining 30 mmHG. It is helpful to put a pillow on the patient’s chest while holding the cuff monitor to relax the arms and neck. Posture Drill
43

Seated or standing. Have patient make themselves tall. Make sure they do not go into cervical and/or lumbar extension. Then have them take a deep breath and hold it. Have elbows at sides and 90 degrees flexed, have them gently externally rotate. Make sure this is pure external rotation of humerus and not scapular adduction. Then they can let their air out but keep their shoulders where they were with the deep breath. This is close to their ideal posture.
Wiggles Gently and effortlessly wiggle fingers and float upwards, extending the elbows. Gently shrug shoulders with arms overhead. Take a deep breath, thinking lifting lateral rib cage. Externally rotate and posteriorly tilt the scapulae (flatten scapulae against rib
cage) Finally, lower arms making sure to “lead” with the elbows and not downward
rotation of scapulae.This is a difficult exercise!
44

Pitfalls to watch for with each action: Make sure posture drill done correctly and maintained correctly. When arms put to chest with full elbow flexion, make sure forearms are vertical,
thumbs pointing backwards. When raising arms overhead effortlessly, make sure neck does not go into
extension or shear. When perform gently shoulder shrug, make sure again neck does not go into
extension or shear. Also make sure scapulae do not adduct but elevate and upwardly rotate.
With deep breath, again look for cervical extension and shear. Also, make sure rib cage is being elevated.
With external rotation and posterior tilt of scapulae, make sure scapulae get flat to rib cage and avoid cervical and lumbar extension.
When lowering arms, must lead with elbows and not downward rotation of scapulae as this causes impingement.
Intrinsic cervical muscle performance training
Flexion and extensionStarting position on knees and forearms with forehead on table/floor. Maintaining weight bearing on forehead, roll head and neck into flexion. As this is done, look between legs. Then roll head into extension and roll eyes up as if looking up. Maintain forehead weight bearing pressure.
45

RotationLean weight to one arm as you look and rotate head to the opposite side. Rotate left and right
Side bending with flexion/extensionRotate head to one side and keep it there with eyes looking to that side. Then in this position, flex and extend head looking down with flexion then up for extension.
Quadruped rock back. Keep head and neck neutral. Chin towards adams apple. Do not allow neck extension. This is to train serratus anterior and intrinsic cervical muscles. If patient does not have internal rotated scapula then may arch thoracic spine before rock back.
46

Robot: Start with patient in supine, short lying. Flatten back, thumbs point to ceiling, flex elbows 90 degrees, touch finger tips to table and slide superior to tension keeping elbows in and back flat, hold 5-10 seconds. Progress to seated then standing back against wall. Stretches latissimus dorsi, trains serratus, intrinsic cervical and lumbar muscles and thoracic extensors.
Wall Slides: Back against wall in pivot prone starting position. Pinkies/back of hands touching wall in “stick up” position. Flatten low back to wall and slight chin tuck. Slowly slide arms overhead attempting to straighten elbows. Stop when feel tension so that neck does not extend, elbows and pinkies/back of hands stay touching wall and back stays flat against wall. Do one inch wiggles. Then bring elbows as if going to back pockets and do one inch wiggles. Stretches pectoralis major, minor, latissimus dorsi, cervical and low back extensors. Trains serratus, intrinsic cervical and lumbar muscles and thoracic extensors.
47
Lower and middle trapezius strengthening.Prone with thumbs up and arms overhead in a “Y” position. Raise arms up by squeezing scapulae and hold 5-10 seconds . Can also do standing facing wall. Do not shrug shoulders.
Touchdown: Stand facing wall , elbows flexed with ulnar side of hands touching wall. Head and neck in neutral position Slide arms up into full shoulder flexion and shrug shoulders. May do 3-5 reps. Isolated upper trapezius strengthening and abduction of scapulae.
48

Horizontal adduction with internal rotationSame starting position as wall slide. Maintain scapulae flat against rib cage while horizontally adducting arms without allowing scapulae to abduct. Then perform internal rotation on involved arm while not allowing scapula to move.
Arm elevation with scapular upward rotationThis exercise is designed to facilitate serratus contraction during arm elevation. Protract the arm maximally, and while maintaining the protraction, upwardly rotate the scapula (as if a string is attached from inferior angle to elbow). Raise arm slowly. You may manually assist .
Assisted cervical flexion: Lie supine in neutral position. Use hands to grasp side and back of head. Assist head into flexion trying to do this segmentally. When lowering head make sure to “uncoil” the neck segmentally.Seated cervical flexion-segmentallySeated cervical rotation-on axis
49

Patient Instructions
Exercises should ideally be done many times per day. Pay attention to correct depression of shoulders. Raise armrests. Typically even adjustable armrests do not get high enough. Pay attention to arm rests in car. If possible, lower chair so arms rest on desk but be careful that hips do not get
much lower than knees. Make sure screen level with eyes AFTER patient assumes excellent position Use pillows when watching TV or reading. Sleep with 1-2 pillows while on side between legs as well as hugging pillows to
chest. Do not put hands in pockets Hook hands in belt loop, pocket, or belt, or hold elbow with opposite hand. Wear sports bra or tape bra straps together from behind. Get straps away from
distal clavicle area. Carry purse or briefcase or book bag on opposite uninvolved shoulder by crossing
strap over head. Sit ideally with hips higher than knees, legs apart and one leg in front and other
back. Use lumbar back support. May use wedge under ischial tuberosities and back of buttocks to tilt into more
neutral spine. Use headset for phone.
50