and impaired glucose regulation undergo metabolic surgery? · and impaired glucose regulation...
TRANSCRIPT

(Who and) When should patients with obesity and impaired glucose regulation undergo
metabolic surgery?
Alex Miras
Senior Clinical Lecturer in Endocrinology

Disclosures
• Fractyl
• Novo Nordisk
• Astra Zeneka

Edmonton Obesity Staging System (EOSS)
Stage 0
Sharma AM & Kushner RF, Int J Obes 2009
Stage 1
Stage 2
Stage 3
Stage 4
co-morbidity
moderate
moderate
Obesity

EOSS Predicts Mortality in NHANES III
Padwal R, Sharma AM et al. CMAJ 2011

King’s Obesity Staging Score
Aasheim E et al, Clinical Obesity 2011

Diagrams of the four bariatric/metabolic operations currently in common clinical use.
Francesco Rubino et al. Dia Care 2016;39:861-877

Current situation
• Operate on <1% of eligible patients
• Constantly use BMI to base treatment decisions
• First come first served
• Treat healthy obese
• Treat patients with end-stage disease

London underground newspaper

NICE guidelines for the surgical therapy of obesity
Revised 2014
• BMI > 40
• BMI > 35 + “significant comorbidities”
• BMI 30-34.9 + T2DM for < 10 years

Weight loss
Sjostrom L et al, JAMA 2014;311(22)

Bariatric Surgery and Long-term Cardiovascular Events

Bariatric Surgery and Long-term Cardiovascular Events

NBSR - 5 year effects of surgery
Miras and Welbourn et al, unpublished data

Suggestions
• Stop using BMI cut offs - keep 30 (or even lower)
• Define what is a significant comorbidity
• Establish which comorbidity is improved by surgery in a cost effective manner
• Compare the cost effectiveness of treating comorbidities
• Establish predictive markers of comorbidity resolution
• Healthy obese will have to go to the back of the queue

Moving from weigh to sugar
Dixon 2008 JAMA
Mingrone 2012 NEJM
Schauer 2012, 2014 NEJM
NICE guidelines for the surgical therapy of obesity
Revised 2014
• BMI > 40
• BMI > 35 + “significant comorbidities”
• BMI 30-34.9 + T2DM for < 10 years

NICE guidelines for the therapy of T2DM
Type 2 diabetes in adults: management’, NICE guideline NG28 (December 2015)

HbA1c after metabolic surgery compared with medical treatments in published RCTs
Philip R. Schauer et al. Dia Care 2016;39:902-911
Among the RCTs, the most common predictors of diabetes remission
included:
• duration of diabetes
• requirement for insulin
• disease status (HbA1c)

Forest plots from a systematic review and meta-analysis of all published articles reporting T2DM remission rates following bariatric/metabolic surgery.
David E. Cummings, and Ricardo V. Cohen Dia Care 2016;39:924-933
Remission 72%
Remission 71%
BMI<35
BMI≥35

Algorithm for the treatment of T2DM, as recommended by DSS-II voting delegates
Francesco Rubino et al. Dia Care 2016;39:861-877

Diabetes Remission in the SOS
Sjostrom L et al, JAMA 2014;311(22)

Predictors of remission in the SOS
• Duration of diabetes
• Weight change at 2 years
• Not BMI
Sjostrom L et al, JAMA 2014;311(22)

Microvascular complications
Sjostrom L et al, JAMA 2014;311(22)

Macrovascular complications
Sjostrom L et al, JAMA 2014;311(22)

Predictors of micro and macro-vascular complications
Sjostrom L et al, JAMA 2014;311(22)
Diabetes < 1 year Diabetes ≥ 4 years
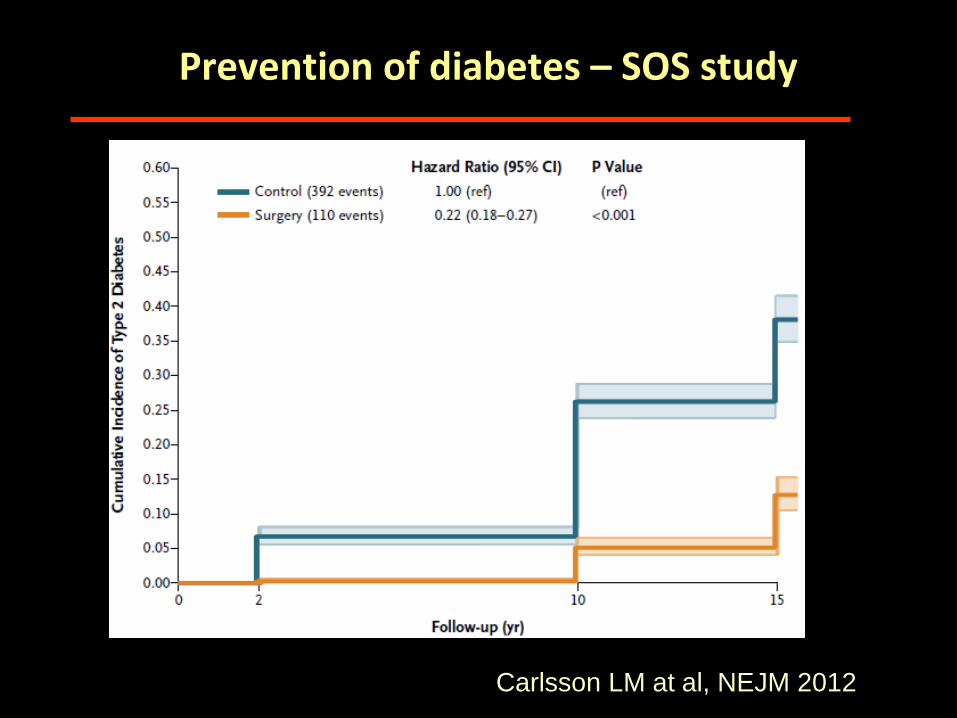
Prevention of diabetes – SOS study
Carlsson LM at al, NEJM 2012

Reduction in microvascular complications
Mingrone 2012 NEJM
A: normal glycaemia B: Prediabetes C: New T2DM D: Established T2DM
Carlsson et al, Lancet D&E 2017

Conclusion so far
• Data say: We should be operating on patients with pre-diabetes or as early as possible in their diagnosis of T2DM
• In practice: Really?
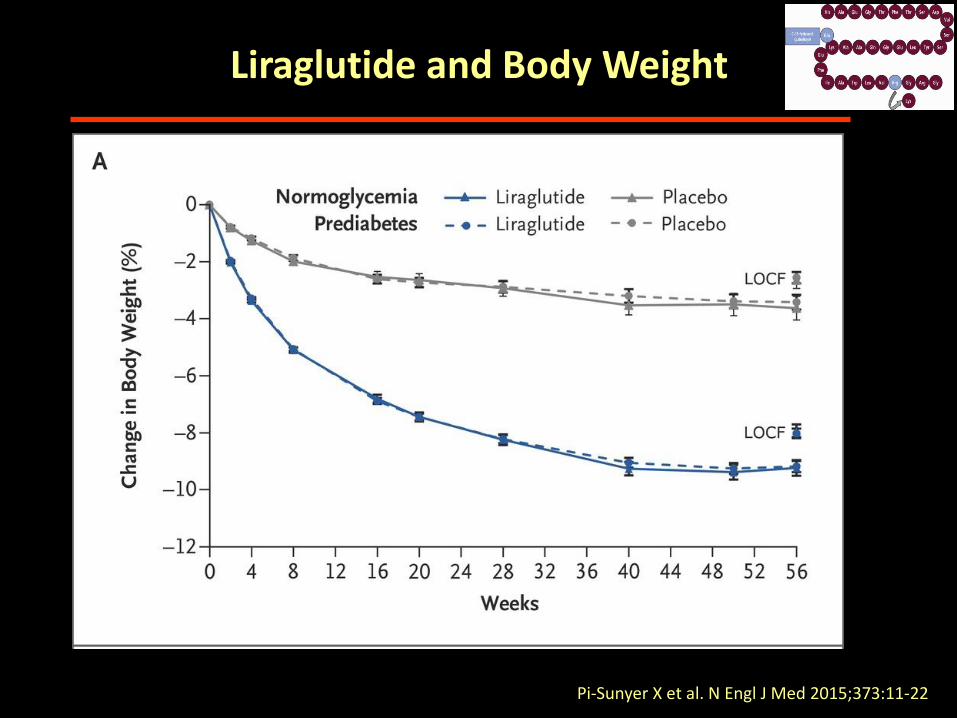
Liraglutide and Body Weight
Pi-Sunyer X et al. N Engl J Med 2015;373:11-22
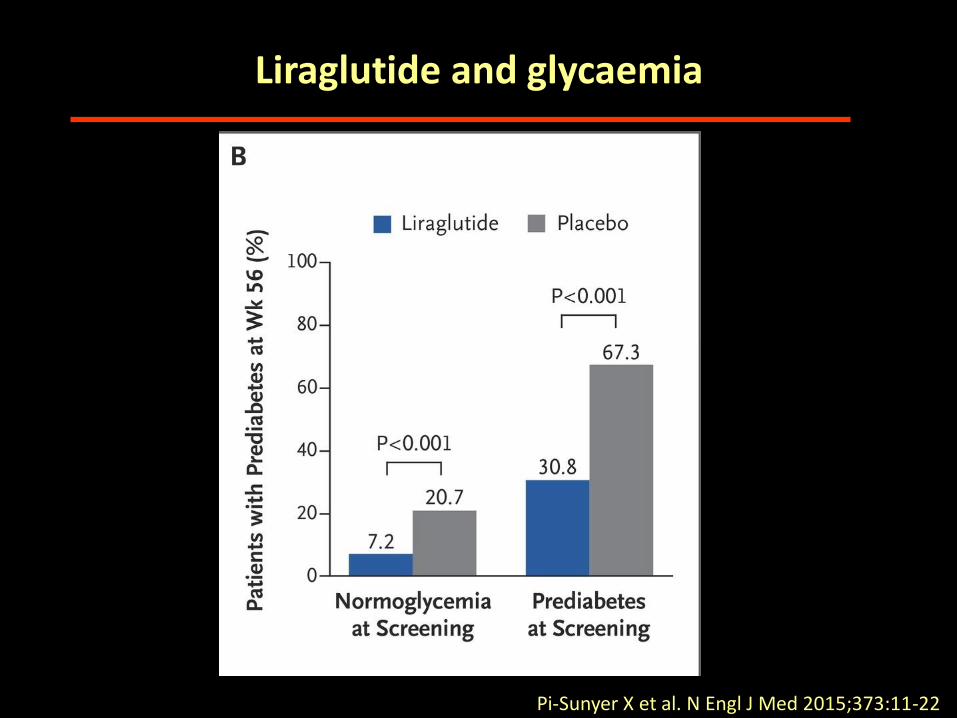
Liraglutide and glycaemia
Pi-Sunyer X et al. N Engl J Med 2015;373:11-22

Marso SP et al. N Engl J Med 2016.
Liraglutide for CV events in diabetes

Zinman B et al. N Engl J Med 2015. DOI: 10.1056/NEJMoa1504720
Empagliflozin: Cardiovascular Outcomes and Death

Wanner C et al. N Engl J Med 2016;375:323-334
Empagliflozin and kidneys

Suggestions
• If the patient has multiple comorbidities and also happen to have pre-diabetes or early diabetes - operate (obesity surgery)
• If the patient just has T2DM - work with non-surgical treatments
• When you see insulin coming - operate, prioritise (metabolic surgery)
• In advanced T2DM (when you are stuck) - still operate but expect less; do not prioritise

Imperial College London Steve Bloom Tricia Tan Anna Kamocka Belen Pevida Madawi Aldhwayan Harvinder Chahal Samantha Scholtz Ahmed Ahmed Sanjay Purkayastha Krishna Moorthy Julian Teare University of Dublin Carel W le Roux Neil Docherty University of Surrey Margot Umpleby Barbara Fielding Fariba Shojaee-Moradie Nicola Jackson
Acknowledgements Florida State University Alan C Spector King’s College London Francesco Rubino Ameet Patel Simon Aylwin Royce Vincent King Saud University, Saudi Arabia Ghalia Abdeen University of Zurich Marco Bueter University of Wurzburg Florian Seyfried
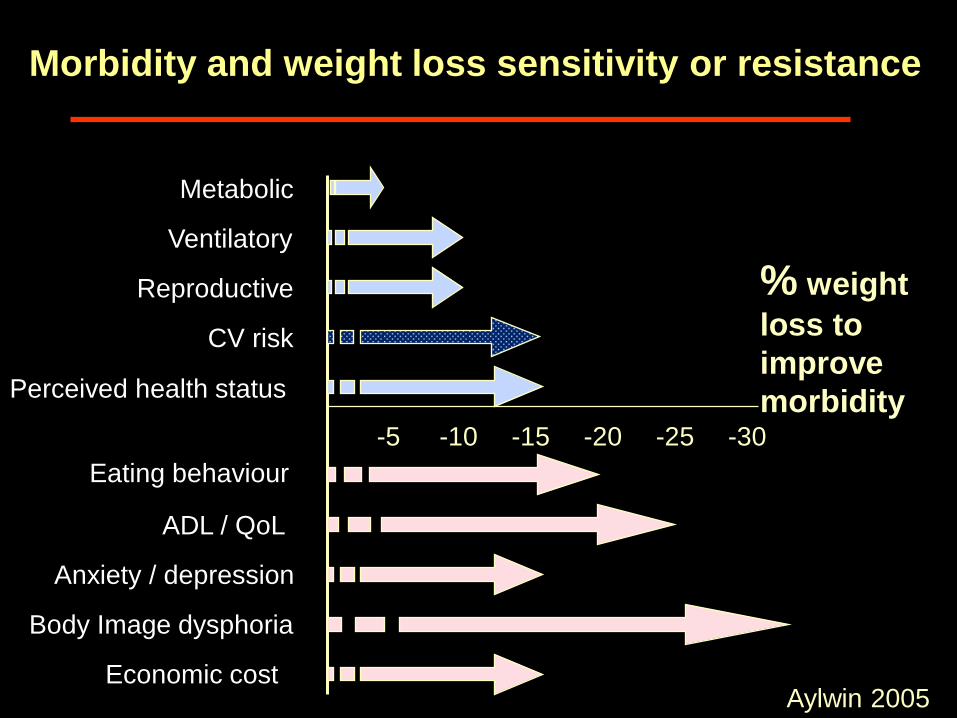
Morbidity and weight loss sensitivity or resistance
Metabolic
Ventilatory
Reproductive
CV risk
Perceived health status
ADL / QoL
Eating behaviour
Anxiety / depression
Body Image dysphoria
Economic cost
-5 -10 -15 -20 -25 -30
% weight
loss to
improve
morbidity
Aylwin 2005

Armstrong et al, Lancet D&E 2016
Liraglutide and the liver

Chao EC, et al. Nat Rev Drug Discovery. 2010;9:551-559.
Targeting the Kidney