anesthesia acls-online friendly
TRANSCRIPT

ANESTHESIA ACLSfor WRHA Anesthesiology staff
!

OUTLINE
• TRADITIONAL ACLS - Review
• Anesthesia-Specific ACLS
• Quiz

ACLS• Systematic approach to assessment and management of
cardiopulmonary emergencies
!
• Continuation of Basic Life Support - ACLS builds on good BLS (C - A - B). Emphasis on compressions and maintenance of circulation
!
• Resuscitation efforts aimed at restoring spontaneous circulation and retaining intact neurologic function

ACLS
• As Anesthesia lifelong learners, we are up to date with literature. However, current ACLS certification courses focus to paramedic and primary care scenarios.
• In the OR setting, ACLS is a real entity; however, the ddx and specific management is unique and not part of current ACLS courses
Review of Traditional ACLS• very simple algorithms for a number of cardiac
situations
• communication and the Team Approach is very important
• someone acts as Team Leader, but all members can contribute
• the debrief at the end is a useful tool to strengthen and improve the response for the next code

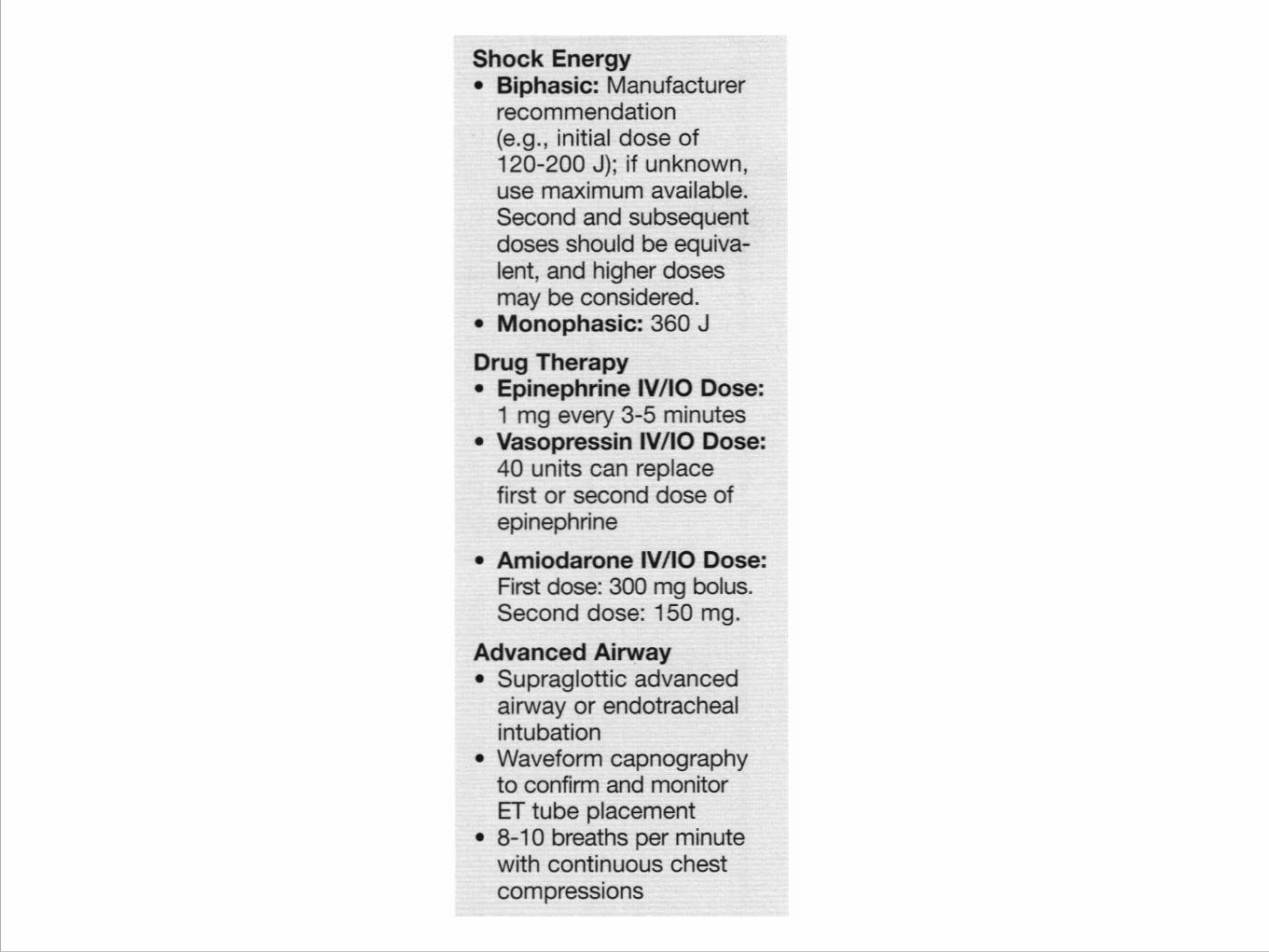
Drug Administration■ Peripheral IV – easiest to insert during CPR
!
■ Central IV – fast onset of action
!
■ Endo-trachealy (down an ET tube) (NAVEL)
■ Narcan, Atropine, Ventolin, Epinepherine, Lidocaine
■ Need 2-2.5x the IV dose, unpredictable response
■ Intraosseous – with no IV access - Useful in paediatrics

Algorithms

CPR
• The cornerstone of good ACLS
• Push hard, Push fast (100 compressions per minute)
• Goal is to minimize interruptions in compressions



ACS



STROKE



Fibrinolytic Checklist

Bradycardia


PACING• Always appropriate
• Doesn’t always work (trans-thoracic)
• Technique
–Attach pacer pads
–Set a rate to 80 bpm
–Turn up the juice (amps) until you get capture
• Painful – may need sedation / analgesia
• Disposition becomes important
Tachycardia

V-fib/V-tach/Asystole/PEA


The Basic H’s and T’s do not always include what we think about
DDX - the traditional approach

ROSC - Return of Spontaneous Circulation
• extremely important time
• disposition important
• cause may still need to be treated (stenting, sx)
• if non responsive, cooling may be appropriate


Anesthesia Specific ACLS• Most often witnessed pre-arrest and arrest events
• Almost pre-emptive or immediate interventions
• The ddx is widened as certain events specific to peri-operative period
• Often the arrest is short lived, and we choose to use lower doses of drugs that traditional ACLS would otherwise suggest.

Anesthesia ACLS
• More often than not, the sequence of events is different than following the basic ACLS approach ex. cardiac arrest during thoracotomy ex. managing hypotension/bradycardia in a patient with a new vascular graft.
Common Arrest-Anesthesia Situations


Intubation during CPR Algorithm


As we can see, the Ddx is more inclusive
DDX - H’s and T’s

Hypotension - common Pre arrest


Tachycardia


Know when to stop• return of spontaneous circulation (but work’s not
done)
• no ROSC after prolonged efforts (situation dependant)
• DNR orders presented
• Obvious signs of irreversible death

Post event• Be sure to debrief with the team
• Anesthesia, Surgery, Nursing, Aids
• All play important roles and it i very important to acknowledge what went well and review what could be done better
• Debriefing also helps cope with the stress of the situation

QuizRead the following questions and pick the best answer. The
answer key is at the end.

1. You find an unresponsive patient, not breathing. After calling EMS, you determine there is no pulse. What is your next action?
• A. Open the airway with a head tilt, chin lift
• B. Administer Epinepherine at a dose of 1mg/kg
• C. Deliver 2 rescue breaths each over 1 second
• D. Start chest compressions at a rate of at least 100/min

2. You are assessing a 58 yr old with chest pain. BP is 92/50, HR 92, RR 14, non laboured.
pulse ox 97%. Which assessment is best?
• A. PET C02
• B. CXR
• C. Lab testing
• D. 12 lead EKG

3. What is a common but sometimes fatal mistake in cardiac arrest management?
• A. failure to obtain vascular access
• B. prolonged periods of no ventilations
• C. failure to perform endotracheal intubation
• D. prolonged interruptions in chest compressions

4. Which action increases the chance of successful conversion of v-fib?
• A. pausing chest compressions immediately after a defibrillation attempt.
• B. administering 4 quick ventilations immediately before a defibrillation attempt
• C. using manual defibrillation pads pressed lightly on the chest
• D. providing quality compressions immediately before a defibrillation attempt.
5. 3 minutes after a witnessed cardiac arrest, a team member intubates during compressions. Waveform
capnography reads 8 mmHg. What is significance of this finding?
• A. chest compressions may not be effective
• B. The ET tube is no longer in the tracy
• C. The patient meets criteria to discontinue efforts
• D. The team is hyperventilating the patient
6. Which is a safe and effective practice within the defibrillation sequence?
• A. stop chest compressions during defibrillator charge
• B. be sure oxygen is not blowing over patient’s chest during shock
• C. Assess for the presence of a pule immediately after the shock
• D. commandingly announce “clear” after you deliver the shock

7. Which drug and dose is recommended for the management of a patient in
refractory v-fib?
• A. Atropine 2mg
• B. Amiodarone 300 mg
• C. Vasopressin 1mg/kg
• D. Dopamine 2 mg/kg/min

8. Which of the following is a sign of effective CPR?
• A. PET C02 greater than 10 mmHg
• B. measured urine output of 1 ml/kg/hr
• C. patient temp greater than 32 degrees Celsius
• D. diastolic intra-arterial pressure less than 20 mmHg

9. A patient presents the the ER with dizziness and fatigue. HR 35, BP 70/50, RR 22, Sats 95%.
What is best first medication to administer?
• A. Atropine 0.5 mg
• B. Oxygen 12-15 lpm
• C. Epinepherine 0.5 mg
• D. Aspirin 160 mg chewed

10. A patient presents to the ER with dizziness and SOB with a HR of 40. Initial atropine dose was ineffective. Monitor does not have pacing capability. What’s the
appropriate dose of dopamine?
• A. 2-10 mg/min
• B. 2-10 mcg/kg/min
• C. 10-15 mg/min
• D. 10-15 mcg/kg/min

11. EMS is transporting a patient with a positive prehospital stroke assessment. In the ER, BP 138/78, HR 80, RR 12, Sats 95%, EKG sinus, glucose N. What should
you do next?
• A. Head CT
• B. transfer to stroke unit
• C. immediate rTPA administration
• D. administer 100% 02

12. What is the initial priority for an unconscious patient with any tachycardia
on the monitor?
• A. review the patient’s home meds
• B. evaluate the breath sounds
• C. determine wether pulses are present
• D. administer selective drugs
13. Which rhythm requires synchronized cardioverison?
• A. unstable supraventricular tachycardia
• B. Atrial Fibrillation
• C. Sinus Tachycardia
• D. NSR on monitor, but no pulse

14. Which condition is a contraindication to therapeutic hypothermia during the post-cardiac
arrest period for patients who achieve ROSC?
• A. initial rhythm of asystole
• B. responding to verbal commands
• C. patient age greater than 60
• D. desire to provide coronary repercussion (ex. PCI)
15. What is the minimum SBP one should attempt to achieve with fluid, inotropic, or vasopressor administration in a hypotensive post cardiac arrest patient who achieves
ROSC (return of spontaneous circulation)?
• A. 90 mmHg
• B. 85 mmHg
• C. 80 mmHg
• D. 75 mmHg

ANSWER KEY• 1 - D 2 - D 3 - D
• 4 - D 5 - A 6 - B
• 7 - B 8 - A 9 - A
• 10 - B 11 - A 12 - C
• 13 - A 14 - B 15 - A
Congrats.
• Print off the next slide as proof you completed the didactic portion of the program.

! ! !!!!!!!This is to certify that !!!!!_________________________________________________________________________ !!Has successfully completed the didactic portion of the Anesthesia ACLS course (approx 2 hours). !Having completed the didactic portion, the person mentioned above can now participate in the hands-on session in the Sim Lab. !!!!
Department of Anesthesia 2nd Floor, Harry Medovy House 671 William Avenue Winnipeg, Manitoba R3E 0Z2 Phone: (204) 787-2261 Fax #: (204) 787-4291