anesthetic problems and emergency
TRANSCRIPT

1Copyright © 2011, 2003, 2000, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Every anesthetic procedure has the potential to cause the death of the animal
Anesthetic Problems and Emergencies
Chapter 12

2Copyright © 2011, 2003, 2000, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Anesthetic Problems and Emergencies: Human Error
Failure to get an adequate history and do a physical examination
Lack of attention to the anesthetic machine and patient
Inability to recognize early signs of trouble Incorrect administration of drugs or
administration of incorrect drugs Lack of knowledge of pharmacology and
improper calculations Fatigue and inattentiveness
3Copyright © 2011, 2003, 2000, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Anesthetic Problems and Emergencies: Equipment Issues
Equipment failure Carbon dioxide absorbent exhaustion
(rebreathing system) Empty oxygen tank Incorrect assembly of the anesthetic machine Endotracheal tube (ET) blockage
4Copyright © 2011, 2003, 2000, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Anesthetic Problems and Emergencies: Equipment Issues (Cont’d)
Vaporizer problems Using the wrong anesthetic agent Tipping the vaporizer Vaporizer dial becomes stuck or jammed Vaporizer is overfilled Two vaporizers used at the same time
Pop-off valve problems Failure to open the pop-off valve

5Copyright © 2011, 2003, 2000, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Reduce the Adverse Effects of Anesthetic Agents
Choose a protocol suitable for the condition or needs of the patient
Be familiar with side effects and contraindications for preanesthetic and general anesthesia agents
Multidrug protocols are safer than single drug protocols

6Copyright © 2011, 2003, 2000, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Anesthetic Problems and Emergencies: Patient Factors
Geriatric animals Have reached 75% of life expectancy Decreased heart, lung, and liver function Presence of degenerative disorders Poor response to stress Reduced anesthetic requirements Prolonged recovery Tendency for hypothermia

7Copyright © 2011, 2003, 2000, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Anesthetic Problems and Emergencies: Patient Factors (Cont’d)
Neonates and pediatric animals are less than 3 months old Preoperative fasting IV 5% dextrose in lactated Ringers during
anesthesia Use pediatric microdrip administration set Use pediatric or gram scale to weigh animals <5 kg Injectable agents may require dilution
8Copyright © 2011, 2003, 2000, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Anesthetic Problems and Emergencies: Patient Factors (Cont’d)
Neonates and pediatric animals Have reduced anesthetic requirements Neonates have reduced liver and kidney function Induction with inhalant agents Intubation and catheterization are difficult Prone to hypothermia

9Copyright © 2011, 2003, 2000, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Anesthetic Problems and Emergencies: Patient Factors (Cont’d)
Brachycephalic animals Anatomic characteristics Avoid agents that depress respiration or relax
muscles of the pharynx/larynx Prone to bradycardia Difficult induction period
• Preoxygenate if possible Difficult to intubate
• Use laryngoscope and smaller diameter tube

10Copyright © 2011, 2003, 2000, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Anesthetic Problems and Emergencies: Patient Factors (Cont’d)
Brachycephalic animals (Cont’d) Use agents that allow rapid recovery Monitor closely during recovery for dyspnea Recover in an excitement-free or stress-free
environment Postoperative tranquilizers may be needed

11Copyright © 2011, 2003, 2000, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Anesthetic Problems and Emergencies: Patient Factors (Cont’d)
Sighthounds Increased sensitivity to some anesthetic agents
Obese animals Require lower doses of drugs on a per-kilogram
basis Anesthetic agents are poorly distributed to fat Possible respiratory difficulty; preoxygenate Shallow, rapid respirations during anesthesia
12Copyright © 2011, 2003, 2000, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Anesthetic Problems and Emergencies: Patient Factors (Cont’d)
Cesarean delivery Most often an emergency surgical procedure Patient is in compromised condition due to
advanced pregnancy Patient is not properly prepared for surgery (e.g.,
not fasted) Most anesthetic agents will cross the placenta and
affect fetuses Patient is at risk for going into shock during
surgery

13Copyright © 2011, 2003, 2000, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Cesarean Anesthetic Protocols
Epidural with tranquilizers or neuroleptanalgesic IV fluids and oxygen also administered Monitor blood pressure
General anesthesia with injectable or inhalant agents Preoxygenation is helpful Propofol or ketamine
Opioid agents Reversible in both mother and neonate

14Copyright © 2011, 2003, 2000, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Anesthetic Concerns for Cesarean Patients
Hypoxemia Hypercarbia Hypotension Physiological anemia Acid/base imbalance Tissue trauma Cardiac arrhythmias

15Copyright © 2011, 2003, 2000, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Care of Puppies and Kittens Delivered by Cesarean Section
Respiratory function Deliver oxygen by facemask Intubate with 16- or 18-gauge IV catheter and
gently bag every 5 seconds Aspirate fluid from the mouth and nose with
eyedropper or bulb syringe Administer reversal agents, doxapram, and/or
dilute atropine as needed

16Copyright © 2011, 2003, 2000, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Care of Puppies and Kittens Delivered by Cesarean Section (Cont’d)
Cardiac function Gentle cardiac massage Deliver oxygen by facemask
Allow to nurse as soon as mother is recovered Watch neonates if mother is still groggy Anesthetic agents secreted in milk don’t affect
neonates
17Copyright © 2011, 2003, 2000, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Anesthetic Problems and Emergencies: Patient Factors
Recent trauma that requires emergency attention Trauma ailments increase anesthetic risk
Respiratory difficulties May result from pneumothorax, pulmonary
contusions, hemorrhage, or diaphragmatic hernia Decreases the VT of the patient leading to
decreased oxygenation Increased CO2 levels leading to acid/base
imbalance and cardiac arrhythmias Loss of blood or fluid sequestration changes blood
pressure

18Copyright © 2011, 2003, 2000, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Anesthetic Problems and Emergencies: Patient Factors (Cont’d)
Change in blood pressure Resulting from a change in cardiac output or
vascular tone Anesthetic depth will affect both parameters Hypotension → decreased tissue perfusion →
tissue hypoxia/anoxia → anaerobic glycolysis → lactic acid production → acid/base imbalance
Monitor blood pressure closely• Doppler or oscillometric methods • Digital pulse palpation • Capillary refill time

19Copyright © 2011, 2003, 2000, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Fluid Therapy for Hypotension
Crystalloid fluid administration May have to deliver small boluses for rapid
therapy Crystalloid fluids stay in intravascular space
<2 hours Watch for fluid overload, especially in cats Monitor heart rate, blood pressure, mucous
membrane color, and capillary refill time

20Copyright © 2011, 2003, 2000, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Fluid Therapy for Hypotension (Cont’d)
Colloid fluid administration Helpful if blood pressure can’t be maintained Remain in the intravascular space longer than
crystalloids Will increase colloidal osmotic pressure and help
stabilize blood pressure Given in smaller volume in conjunction with
crystalloids
21Copyright © 2011, 2003, 2000, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Anesthetic Problems and Emergencies: Patient Factors
Respiratory problems in the trauma patient Direct trauma to the chest leading to lung collapse
or failure of alveolar gas exchange Must remove air/fluid from chest cavity prior to
anesthesia Deliver supplemental oxygen
Oxygen delivery methods Flow-by-oxygen Nasal catheters Oxygen collars

22Copyright © 2011, 2003, 2000, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Oxygen Delivery Methods

23Copyright © 2011, 2003, 2000, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Thoracocentesis (Chest Tap)
To relieve pneumothorax or pleural effusion from chest cavity
Performed by veterinarian Prepped by veterinary technician Temporary bandage over chest wound Place animal in sternal recumbency or standing
position Shave lateral chest wall between the 7th and 9th
intercostal spaces caudal to point of the elbow Aseptically prepare 4 cm × 4 cm area Prepare a 20- to 22-gauge, 1- to 1½-inch catheter
with a three-way stopcock and large syringe

24Copyright © 2011, 2003, 2000, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Other Considerations for the Trauma Patient
Cardiac arrhythmias Common 12-72 hours after trauma Electrocardiograms
Shock: especially where hemorrhage is significant Internal injuries: fractures or ruptured organs Anesthesia
Best to delay it until the animal is stabilized Delay allows more thorough patient workup
including thoracic radiographs

25Copyright © 2011, 2003, 2000, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Anesthetic Problems and Emergencies: Patient Factors
Preexisting cardiovascular disease Anemia Shock Cardiomyopathy (primary or secondary) Congestive heart disease (mitral valve
insufficiency) Heartworm disease Coexisting imbalances (e.g., hypoxia,
hypercapnia, electrolyte imbalances)

26Copyright © 2011, 2003, 2000, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Anesthetic Problems and Emergencies: Patient Factors (Cont’d)
Bradycardia Most common cardiac anesthetic problem Caused by preanesthetic or anesthetic drugs Force of cardiac contraction may also be
decreased Blood return to the heart may be decreased
(preload) Treat with drugs or adjustment of anesthetic depth

27Copyright © 2011, 2003, 2000, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Anesthetic Problems and Emergencies: Patient Factors (Cont’d)
Cardiac arrhythmias Caused by anoxia/hypercarbia, poor tissue
perfusion, acid/base imbalance, myocardial damage
Difficult to detect on physical examination; may find dropped beats
Diagnose with ECG and report immediately to veterinarian who will determine the treatment required
Concurrent pulmonary disease is sometimes seen
28Copyright © 2011, 2003, 2000, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Anesthetic Problems and Emergencies: Patient Factors (Cont’d)
Anesthetic considerations Stabilize patient as per veterinarian’s instructions Preoxygenate with facemask 5 minutes prior to
induction Increased risk of overhydration with IV fluid
• Monitor for pulmonary edema

29Copyright © 2011, 2003, 2000, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Anesthetic Problems and Emergencies: Patient Factors (Cont’d)
Respiratory disease Caused by:
Pleural effusion Diaphragmatic herniaPneumothorax PneumoniaTracheal collapse Pulmonary edema
Clinical signs • Tachypnea• Dyspnea• Cyanosis
30Copyright © 2011, 2003, 2000, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Anesthetic considerations VT is reduced and respiratory rate is decreased in
most anesthetized animals A decrease in VT will result in a decreased alveolar
gas exchange Lighten anesthesia as much as possible in a
patient with respiratory disease Provide intermittent ventilation Evaluate oxygen-carrying capacity with PCV or
pulse oximeter Preoxygenation is necessary prior to induction
Anesthetic Problems and Emergencies: Patient Factors (Cont’d)
31Copyright © 2011, 2003, 2000, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Respiratory Problems During Anesthesia
Clinical signs: dyspnea or cyanosis Assessment
Respiratory character and volume Depth of anesthesia Associated with pain Proper ET tube placement ET tube blockage Oxygen saturation Arterial or end-tidal CO2
32Copyright © 2011, 2003, 2000, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Respiratory Problems During Anesthesia (Cont’d)
Actions Intermittent positive-pressure ventilation Reintubate if necessary Radiographs and thoracocentesis

33Copyright © 2011, 2003, 2000, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Anesthetic Problems and Emergencies: Patient Factors
Diaphragmatic hernia Preoxygenate for 5-10 minutes prior to induction Avoid head-down patient positions before and
during anesthesia Rapid intubation Ventilatory assistance or ventilator if necessary Postoperative observation for signs of respiratory
distress
34Copyright © 2011, 2003, 2000, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Anesthetic Problems and Emergencies: Patient Factors (Cont’d) Hepatic disease
Liver necessary for drug metabolism, blood clotting factors, plasma proteins, carbohydrate metabolism
Preanesthetic agents must be chosen with care

35Copyright © 2011, 2003, 2000, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Anesthetic Problems and Emergencies: Patient Factors (Cont’d) Renal disease
Kidneys maintain volume and electrolyte composition of body fluids
Renal excretion removes anesthetic agents and metabolites from the body
General anesthesia is associated with decreased blood flow to the kidneys
Diagnosis: urine specific gravity, BUN, creatinine Offer water up to 1 hour prior to premedication Correct dehydration prior to anesthesia
36Copyright © 2011, 2003, 2000, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Anesthetic Problems and Emergencies: Patient Factors (Cont’d)
Urinary blockage Clinical signs
• Depression• Dehydration• Uremia• Acidosis• Hyperkalemia (can lead to cardiac arrest)
Inhalation agents are less hazardous for the patient
37Copyright © 2011, 2003, 2000, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Anesthetic Problems and Emergencies
Animals won’t stay anesthetized Check vaporizer setting Check level of anesthetic in the vaporizer Proper ET tube placement or air leakage around it Patient apnea Shallow respirations Proper assembly of anesthetic machine with tight
connections Adequate oxygen flow Anesthetic machine/vaporizer is working properly Agonal breathing vs. light plane breathing
38Copyright © 2011, 2003, 2000, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Anesthetic Problems and Emergencies (Cont’d)
Animals are too deeply anesthetized <6 bpm; shallow respirations, dyspnea Pale/cyanotic mucous membranes Capillary refill time >2 seconds Bradycardia Weak pulse; systolic blood pressure <80 mm Hg Cardiac arrhythmias; irregular QRS complexes or
VPCs Hypothermia Absent reflexes Flaccid muscle tone Dilated pupils
39Copyright © 2011, 2003, 2000, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Anesthetic Problems and Emergencies (Cont’d)
Pale mucous membranes Preexisting conditions Blood loss during surgery Anesthetic agent that causes vasodilation and
hypotension Hypothermia Pain

40Copyright © 2011, 2003, 2000, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Anesthetic Problems and Emergencies (Cont’d)
Prolonged capillary refill time (>2 seconds) Blood pressure cannot adequately perfuse
superficial tissues May result from conditions present prior to
induction May be secondary to blood loss during surgery May be seen in animals in deep anesthesia

41Copyright © 2011, 2003, 2000, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Anesthetic Problems and Emergencies (Cont’d)
Respiratory distress Dyspnea
• Patient is unable to obtain sufficient oxygen or remove adequate CO2
Cyanosis• Oxygenation is inadequate
42Copyright © 2011, 2003, 2000, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Anesthetic Problems and Emergencies (Cont’d)
Sources of respiratory distress during anesthesia Empty oxygen tank Flowmeter is turned off Anesthetic circuit or ET tube is blocked Airway obstruction or respiratory pathology Deep anesthesia
43Copyright © 2011, 2003, 2000, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Anesthetic Problems and Emergencies (Cont’d)
Tachypnea Rapid respirations as opposed to dyspnea Commonly seen with opioid use Associated with light anesthesia accompanied by
tachycardia and spontaneous movement May be seen in hyperthermic animals

44Copyright © 2011, 2003, 2000, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Anesthetic Problems and Emergencies (Cont’d)
Abnormalities in cardiac rate and rhythm seen in anesthetized animals Tachypnea
• May result from drugs, preexisting conditions, or surgical stimulation
• May not require treatment • Check vaporizer setting and anesthetic depth

45Copyright © 2011, 2003, 2000, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Anesthetic Problems and Emergencies (Cont’d)
Abnormalities in cardiac rate and rhythm are seen in anesthetized animals Bradycardia
• May be secondary to drug administration, vagal stimulation, deep anesthesia, or physiologic imbalances
• May not require treatment• Check vaporizer setting, bag with 100% oxygen, or
administer reversal drugs Cardiac arrhythmias
• May result from drugs and will have a short duration• May be a problem in geriatric patients or patients with
preexisting conditions• Common during induction and light anesthesia
46Copyright © 2011, 2003, 2000, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Anesthetic Problems and Emergencies (Cont’d)
Respiratory arrest Cessation of respiratory efforts Can lead to cardiac arrest Temporary arrest
• May follow injection of respiratory depressants or following a period of prolonged bagging
• Check other vital signs for abnormalities
47Copyright © 2011, 2003, 2000, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Anesthetic Problems and Emergencies (Cont’d)
Respiratory arrest (Cont’d) True arrest
• Requires immediate action• Can result from anesthetic overdose, cessation of
oxygen flow, or preexisting respiratory disease• May be preceded by dyspnea or cyanosis and abnormal
vital signs• May use Ambu bag, mouth-to-ET tube, or mouth-to-
muzzle resuscitation

48Copyright © 2011, 2003, 2000, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Use of an Ambu Bag
49Copyright © 2011, 2003, 2000, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Anesthetic Problems and Emergencies (Cont’d)
Cardiac arrest No heartbeat is auscultated or palpated Normal QRS complexes are absent No arterial pulse and blood pressure <25 mm Hg Gray or cyanotic mucous membranes Widely dilated pupils, no corneal reflex Agonal breathing
Some prior warning is usually present Respiratory distress or arrest, cyanosis/dyspnea,
prolonged capillary refill time, arrhythmia

50Copyright © 2011, 2003, 2000, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Anesthetic Problems and Emergencies (Cont’d)
Cardiopulmonary cerebrovascular resuscitation (CPCR) started immediately after cardiac arrest Five people (ideal) involved
• 1 performs chest compressions• 2 bags the animal • 3 assesses the pulse during compressions and checks
the pulse or ECG when compressions are stopped• 4 draws up and administers drugs as per the
veterinarian’s instructions • 5 maintains a record of the patient’s status and
resuscitative treatment

51Copyright © 2011, 2003, 2000, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Anesthetic Problems and Emergencies (Cont’d)
Cardiac arrest with CPCR A = airway B = breathing C = circulation D = drugs E = ECG
Circulation is the most important step so the correct order is CABDE

52Copyright © 2011, 2003, 2000, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Cardiopulmonary Cerebrovascular Resuscitation (CPCR)
Circulation Most important factor is return of spontaneous
circulation (ROSC) Cardiac compressions
• Method depends on the size of the animal• Compress chest about 1/3 the diameter of the chest wall • 1-2 compressions/second generates 100 bpm heart rate • Compressions manually force blood through the heart
and into tissues• Each compression should produce a palpable femoral
pulse

53Copyright © 2011, 2003, 2000, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Cardiopulmonary Cerebrovascular Resuscitation (CPCR) (Cont’d)
Circulation (Cont’d) Bag the patient every 10-12 seconds
• Simultaneously with compressions Some results should be seen within 2 minutes Internal compressions may be necessary Resuscitation is unlikely to be successful after
15 minutes Once spontaneous cardiac contractions are
established, continue bagging until spontaneous breathing is established (several hours)

54Copyright © 2011, 2003, 2000, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Cardiac Compressions

55Copyright © 2011, 2003, 2000, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Cardiopulmonary Cerebrovascular Resuscitation (CPCR) (Cont’d)
Airway and breathing Intubate immediately if not already intubated Turn off vaporizer and nitrous oxide
• Animal should breathe 100% oxygen One breath every 10-12 seconds Chest should rise slightly during bagging

56Copyright © 2011, 2003, 2000, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Cardiopulmonary Cerebrovascular Resuscitation (CPCR) (Cont’d)
Drugs Veterinarian authorizes dosage, route, and nature
of drugs Catheterized animals
• Drugs administered IV followed by rapid fluid administration
• Be careful of overhydration Injections into the base of the tongue or by the
intratracheal route are the second choice Intracardiac injections should be avoided
57Copyright © 2011, 2003, 2000, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Cardiopulmonary Cerebrovascular Resuscitation (CPCR) (Cont’d)
Commonly used drugs Epinephrine
• Cardiac arrest Vasopressin
• In place of or alternated with epinephrine Atropine
• Anesthesia-related cardiac arrest Dopamine or dobutamine
• Increase force and rate of cardiac contractions

58Copyright © 2011, 2003, 2000, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Cardiopulmonary Cerebrovascular Resuscitation (CPCR) (Cont’d)
ECG Don’t use alcohol if a defibrillator is present Asystole
• No electrical activity Ventricular fibrillation
• Coarse vertical zig-zag lines resulting from disorganized muscular heart activity
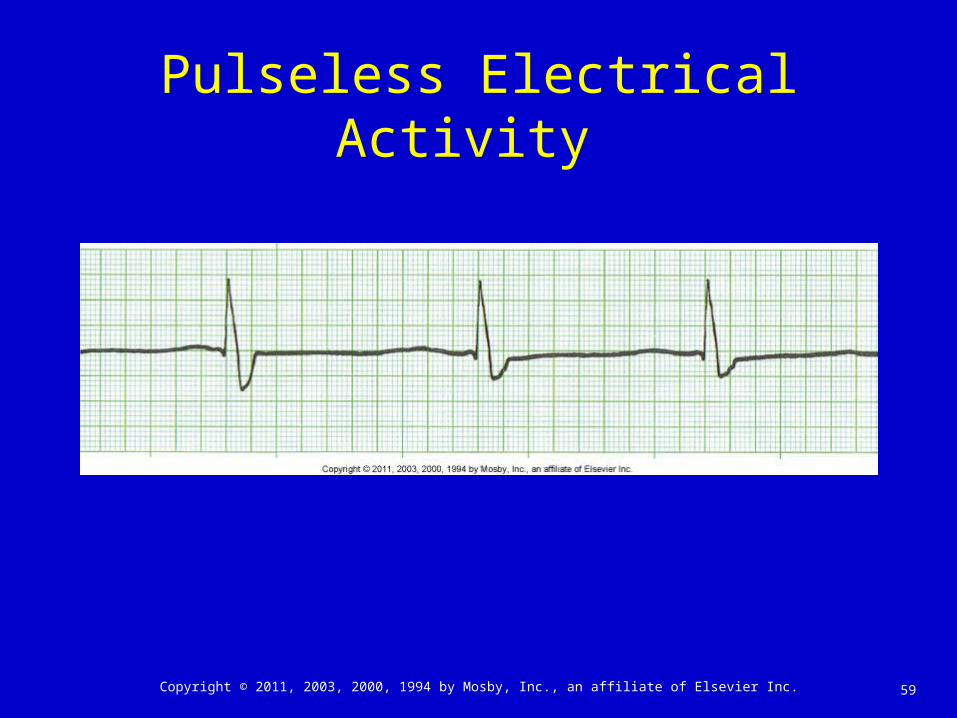
Pulseless electrical activity (electromechanical dissociation, EMD)
• Normal or near-normal complexes
59Copyright © 2011, 2003, 2000, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Pulseless Electrical Activity

60Copyright © 2011, 2003, 2000, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
ROSC Aftercare
Monitor cardiovascular and respiratory function Blood pressure, blood gases, pulse oximetry,
ECG, capnography Drug and fluid therapy varies Assess brain function Repeat arrest within 24 hours is common Following successful ROSC, other conditions
may arise Pulmonary or cerebral edema

61Copyright © 2011, 2003, 2000, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Potential Problems During the Recovery Period
Regurgitation during anesthesia A passive process under anesthesia
• No retching, just fluid draining from animal’s mouth or nose
Stomach contents may be aspirated into respiratory tract
Most common occurrence in head-down surgical positions and in ruminants
Treatment• Immediate placement of cuffed ET tube• Clean out regurgitated material with suction

62Copyright © 2011, 2003, 2000, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Potential Problems During the Recovery Period (Cont’d)
Vomiting during or after anesthesia Common in brachycephalic dogs or nonfasted
animals An active process usually accompanied by
retching Usually occurs as the animal is losing or regaining
consciousness Signs
• Airway obstruction leading to dyspnea/cyanosis, bronchospasm
Treatment• Intubation and suction if unconscious• Lower head and clean oral cavity if conscious

63Copyright © 2011, 2003, 2000, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Potential Problems During the Recovery Period (Cont’d) Seizures
Seen with ketamine administration, after diagnostic procedures (myelography), or preexisting conditions
Signs• Spontaneous twitching; uncontrolled movements of
head, neck, and limbs; opisthotonus; triggered by a stimulus
Treatment• Reduce stimuli, postoperative analgesia, diazepam or
propofol, monitor for hyperthermia
64Copyright © 2011, 2003, 2000, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Potential Problems During the Recovery Period (Cont’d)
Excitement Seen after barbiturate anesthesia or high opioid
doses, as spontaneous paddling and vocalization Treatment may not be necessary
• Sedatives may help• Naloxone can reverse opioids
Seizures should be differentiated from excitement
65Copyright © 2011, 2003, 2000, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Potential Problems During the Recovery Period (Cont’d)
Dyspnea in cats Dyspnea is usually caused by laryngospasm
sometimes triggered by removal of the ET tube Laryngeal edema may result from repeated
intubation attempts May breathe with an audible stertor (wheeze)
during inspiration Differentiate from growling during expiration May resolve itself or may need oxygen
administration via facemask, intubation, or a tracheotomy
Is easier to prevent than treat

66Copyright © 2011, 2003, 2000, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Potential Problems During the Recovery Period (Cont’d)
Dyspnea in dogs Breed-related
• Brachycephalic dogs Airway obstruction
• Anatomy, foreign objects, postsurgical tissue swelling Humidified oxygen can be delivered to an awake
animal• By facemask, nasal cannula, E-collar, or oxygen
cage/tent

67Copyright © 2011, 2003, 2000, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Potential Problems During the Recovery Period (Cont’d)
Causes of prolonged recovery Impaired renal or hepatic function Hypothermia Patient susceptibility to anesthetic agent Breed variation Coexisting disorder Prolonged anesthesia or deep anesthesia