ankle fracture post- operative rehabilitation · ankle fracture post-operative rehabilitation ....
TRANSCRIPT

Ankle Fracture Post-Operative Rehabilitation
BioMed Central
Open Access
Page 1 of 11(page number not for citation purposes)
BMC Musculoskeletal Disorders
Research articleEffects of a training program after surgically treated ankle fracture: a prospective randomised controlled trialGertrud M Nilsson*1, Kjell Jonsson2, Charlotte S Ekdahl1 and Magnus Eneroth3
Address: 1Department of Health Sciences, Division of Physical Therapy, Lund University, Lund, Sweden, 2Department of Radiology, Lund University Hospital, Lund, Sweden and 3Department of Orthopaedics, Malmö University Hospital, Malmö, Sweden
Email: Gertrud M Nilsson* - [email protected]; Kjell Jonsson - [email protected]; Charlotte S Ekdahl - [email protected]; Magnus Eneroth - [email protected]
* Corresponding author
AbstractBackground: Despite conflicting results after surgically treated ankle fractures few studies have evaluatedthe effects of different types of training programs performed after plaster removal. The aim of this studywas to evaluate the effects of a 12-week standardised but individually suited training program (traininggroup) versus usual care (control group) after plaster removal in adults with surgically treated anklefractures.
Methods: In total, 110 men and women, 18-64 years of age, with surgically treated ankle fracture wereincluded and randomised to either a 12-week training program or to a control group. Six and twelvemonths after the injury the subjects were examined by the same physiotherapist who was blinded to thetreatment group. The main outcome measure was the Olerud-Molander Ankle Score (OMAS) which ratessymptoms and subjectively scored function. Secondary outcome measures were: quality of life (SF-36),timed walking tests, ankle mobility tests, muscle strength tests and radiological status.
Results: 52 patients were randomised to the training group and 58 to the control group. Five patientsdropped out before the six-month follow-up resulting in 50 patients in the training group and 55 in thecontrol group. Nine patients dropped out between the six- and twelve-month follow-up resulting in 48patients in both groups. When analysing the results in a mixed model analysis on repeated measuresincluding interaction between age-group and treatment effect the training group demonstrated significantlyimproved results compared to the control group in subjects younger than 40 years of age regarding OMAS(p = 0.028), muscle strength in the plantar flexors (p = 0.029) and dorsiflexors (p = 0.030).
Conclusion: The results of this study suggest that when adjusting for interaction between age-group andtreatment effect the training model employed in this study was superior to usual care in patients underthe age of 40. However, as only three out of nine outcome measures showed a difference, the beneficialeffect from an additional standardised individually suited training program can be expected to be limited.There is need for further studies to elucidate how a training program should be designed to increase andoptimise function in patients middle-aged or older.
Trial Registration: Current Controlled Trials ACTRN12609000327280
Published: 25 September 2009
BMC Musculoskeletal Disorders 2009, 10:118 doi:10.1186/1471-2474-10-118
Received: 15 April 2009Accepted: 25 September 2009
This article is available from: http://www.biomedcentral.com/1471-2474/10/118
© 2009 Nilsson et al; licensee BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Effects of a Training Program After Surgically Treated Ankle Fracture: A Prospective Randomized Controlled Trial
Part 1:

BMC Musculoskeletal Disorders 2009, 10:118 http://www.biomedcentral.com/1471-2474/10/118
Page 2 of 11(page number not for citation purposes)
BackgroundAnkle fractures are among the most common fractures inthe lower extremity [1,2]. In younger ages the incidence ishigher among men but at the age of 50 the gender ratioreverses [1,3]. The incidence rate has been reported to bebetween 101/105 person years [2] to 107/105 [3]. Dislo-cated fractures and fractures resulting in instability of theankle mortise are surgically treated with internal fixationusing screws and plates and/or cerclage, staples and pins[4,5]. Most fractures are immobilised in a plaster cast forbetween six and eight weeks [6-9].
The results after surgically treated ankle fractures are con-flicting. Evaluating subjective recovery using the Olerud-Molander Ankle Score (OMAS) some studies havereported only slight disability [7,10-12] whereas morerecent reports have shown poorer results [13,14]. Usingthe OMAS Nilsson et al. showed in subjects over the ageof 40 years a risk of subjectively scored poor function [15].Similar results were found by Egol et al. using the ShortMuscular Function Assessment (SMFA) [16]. Regardingphysical outcomes, decreased balance capacity and anklejoint mobility were found to be independently associatedwith symptoms and poorly scored function one year afterinjury [17].
Neuromuscular training programs are commonly used inclinical practice for lower extremity rehabilitation. Theseprograms are mainly applied in rehabilitation after kneeinjuries [18] and after ankle ligament injuries [19-21].There are a limited number of studies that have evaluatedthe results of a rehabilitation program after surgicallytreated ankle fracture [8,22]. Shaffer et al. showed normal-ised muscle performance, functional ability and fatigueresistance following ten weeks of physical therapy focus-ing on strengthening and ambulation. The study includedten patients mean 35 years and the results were comparedto an age-and gender matched control group [8]. Stevenset al. found similar results in a group of nine individualsmean 21 years [22]. To our knowledge no randomisedcontrolled trials have been performed evaluating the effectof a standardised training program after plaster removal.
The aim of this randomised controlled study was to eval-uate if a standardised but individually suited training pro-gram, supervised by a physiotherapist, starting within oneweek after plaster removal, focusing on regained anklejoint mobility, muscle strength, balance and functionaltraining could improve symptoms, subjectively scoredand physical outcome in patients 18-64 years of age com-pared to usual care.
MethodsStudy design and settingThis is a prospective, randomised controlled trial per-formed at the Department of Orthopaedics, University
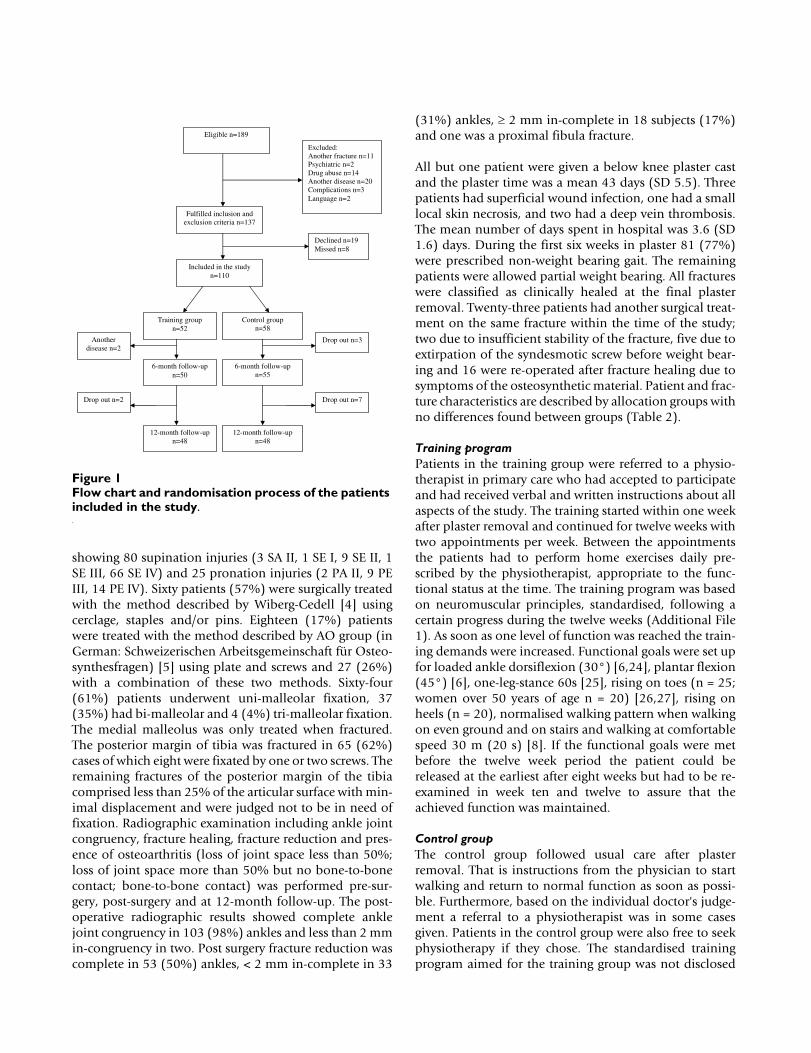
Hospital, Lund, Sweden in collaboration with physiother-apists in primary health care. During January 2003 untilOctober 2005, consecutive patients with a surgicallytreated ankle fracture, 18-64 years of age and living withinan area of 50 kilometres from the University Hospital,Lund, Sweden were eligible for inclusion. One hundred-eighty-nine patients fulfilled these criteria. Exclusion crite-ria were diseases that might influence the physical func-tion of the lower extremity or adherence to therandomisation process: co-existing fracture on the otherleg or another fracture on the same leg (n = 11), psychiat-ric diagnosis (n = 2), drug abuse (n = 14), symptomaticosteoarthritis in the lower extremity, rheumatic or othersystemic diseases (n = 20) delayed surgery due to compli-cations (n = 3) and persons not proficient in the Swedishlanguage (n = 2). Thus 137 fulfilled the inclusion criteriafor this study. Of these, 19 declined participation andeight were missed for inclusion during their hospital stay(14 men aged (median) 32 and 13 women aged (median)52) resulting in 110 participants. Of these 52 were allo-cated to the training group and 58 to the control group.Before the first follow-up at six months after the injurytwo patients allocated to the training group were excludedsecondary to a new injury in the same ankle (n = 1) and acerebral haemorrhage (n = 1) and additionally threepatients allocated to the control group dropped out(declined to participate) resulting in 105 subjects left forthe study (Figure 1).
The day after surgery patients were given written and ver-bal information about the study and were asked to partic-ipate in the study. After written informed consent, thepatients were randomised by sealed envelopes allocatingthem either to a standardised rehabilitation program(training group) or to usual care (control group). All sub-jects had to complete a questionnaire at six and 12months after injury and were examined by the same phys-iotherapist (GN) who was blinded to the allocationgroup. At the 12-month follow-up the patients were alsoexamined by a doctor for a medical check up and radio-logical examination. The Research Ethics Committee atthe Lund University approved the study (LU297-02)
Patients and fracture characteristicsStudy data are presented for the 105 patients. The meanage for men was 37 (SD 13) years and for women 48 (SD12) years (p < 0.001). Age, height, weight and BMI did notdiffer between the two random groups (Table 1). The leftankle was injured in 60 (57%) patients, 96 injuries (91%)were falls on level ground or in on stairs, four were bicycleaccidents, two were motorbike accidents and three werefalls from a height. Twenty-two patients had been injuredduring sport/leisure time activities.
The same radiologist (KJ) examined all the images and thefractures were classified according to Lauge-Hansen [23]
BMC Musculoskeletal Disorders 2009, 10:118 http://www.biomedcentral.com/1471-2474/10/118
Page 3 of 11(page number not for citation purposes)
showing 80 supination injuries (3 SA II, 1 SE I, 9 SE II, 1SE III, 66 SE IV) and 25 pronation injuries (2 PA II, 9 PEIII, 14 PE IV). Sixty patients (57%) were surgically treatedwith the method described by Wiberg-Cedell [4] usingcerclage, staples and/or pins. Eighteen (17%) patientswere treated with the method described by AO group (inGerman: Schweizerischen Arbeitsgemeinschaft für Osteo-synthesfragen) [5] using plate and screws and 27 (26%)with a combination of these two methods. Sixty-four(61%) patients underwent uni-malleolar fixation, 37(35%) had bi-malleolar and 4 (4%) tri-malleolar fixation.The medial malleolus was only treated when fractured.The posterior margin of tibia was fractured in 65 (62%)cases of which eight were fixated by one or two screws. Theremaining fractures of the posterior margin of the tibiacomprised less than 25% of the articular surface with min-imal displacement and were judged not to be in need offixation. Radiographic examination including ankle jointcongruency, fracture healing, fracture reduction and pres-ence of osteoarthritis (loss of joint space less than 50%;loss of joint space more than 50% but no bone-to-bonecontact; bone-to-bone contact) was performed pre-sur-gery, post-surgery and at 12-month follow-up. The post-operative radiographic results showed complete anklejoint congruency in 103 (98%) ankles and less than 2 mmin-congruency in two. Post surgery fracture reduction wascomplete in 53 (50%) ankles, < 2 mm in-complete in 33
(31%) ankles, ≥ 2 mm in-complete in 18 subjects (17%)and one was a proximal fibula fracture.
All but one patient were given a below knee plaster castand the plaster time was a mean 43 days (SD 5.5). Threepatients had superficial wound infection, one had a smalllocal skin necrosis, and two had a deep vein thrombosis.The mean number of days spent in hospital was 3.6 (SD1.6) days. During the first six weeks in plaster 81 (77%)were prescribed non-weight bearing gait. The remainingpatients were allowed partial weight bearing. All fractureswere classified as clinically healed at the final plasterremoval. Twenty-three patients had another surgical treat-ment on the same fracture within the time of the study;two due to insufficient stability of the fracture, five due toextirpation of the syndesmotic screw before weight bear-ing and 16 were re-operated after fracture healing due tosymptoms of the osteosynthetic material. Patient and frac-ture characteristics are described by allocation groups withno differences found between groups (Table 2).
Training programPatients in the training group were referred to a physio-therapist in primary care who had accepted to participateand had received verbal and written instructions about allaspects of the study. The training started within one weekafter plaster removal and continued for twelve weeks withtwo appointments per week. Between the appointmentsthe patients had to perform home exercises daily pre-scribed by the physiotherapist, appropriate to the func-tional status at the time. The training program was basedon neuromuscular principles, standardised, following acertain progress during the twelve weeks (Additional File1). As soon as one level of function was reached the train-ing demands were increased. Functional goals were set upfor loaded ankle dorsiflexion (30°) [6,24], plantar flexion(45°) [6], one-leg-stance 60s [25], rising on toes (n = 25;women over 50 years of age n = 20) [26,27], rising onheels (n = 20), normalised walking pattern when walkingon even ground and on stairs and walking at comfortablespeed 30 m (20 s) [8]. If the functional goals were metbefore the twelve week period the patient could bereleased at the earliest after eight weeks but had to be re-examined in week ten and twelve to assure that theachieved function was maintained.
Control groupThe control group followed usual care after plasterremoval. That is instructions from the physician to startwalking and return to normal function as soon as possi-ble. Furthermore, based on the individual doctor's judge-ment a referral to a physiotherapist was in some casesgiven. Patients in the control group were also free to seekphysiotherapy if they chose. The standardised trainingprogram aimed for the training group was not disclosed
Flow chart and randomisation process of the patients included in the studyFigure 1Flow chart and randomisation process of the patients included in the study.
Control group n=58
Included in the study n=110
6-month follow-up n=50
Training group n=52
6-month follow-up n=55
Another disease n=2
Drop out n=7 Drop out n=2
12-month follow-upn=48
12-month follow-upn=48
Drop out n=3
Fulfilled inclusion and exclusion criteria n=137
Declined n=19 Missed n=8
Eligible n=189
Excluded: Another fracture n=11 Psychiatric n=2 Drug abuse n=14 Another disease n=20 Complications n=3 Language n=2
BMC Musculoskeletal Disorders 2009, 10:118 http://www.biomedcentral.com/1471-2474/10/118
Page 4 of 11(page number not for citation purposes)
for the usual care group. That is as soon as a physiothera-pist was included in the study and had taken part of thespecific training program a written consent had to bereturned to the project leader (GN) that no other patientswith surgically treated ankle fractures than those includedin the study and directed to her were trained by her untilthe study was finished. The physiotherapist was alsoinstructed not to inform colleagues, who might treatpatients in the usual care group, about the program.
Age-groupsForty individuals were younger than 40 years of age, 20 ofthese were randomised to the training group and 20 to thecontrol group. Sixty-five were over 40 years of age, 30 ofthese were randomised to the training group and 35 to thecontrol group (p = 0.53).
OutcomesOlerud-Molander Ankle ScoreThe Olerud-Molander Ankle Score (OMAS) [28] was theprimary outcome measure and is a self-administeredpatient questionnaire. The scale is a rating scale from 0(totally impaired) to 100 (completely unimpaired) and isbased on nine items: pain, stiffness, swelling, stair climb-ing, running, jumping, squatting, supports and work/activities of daily living. The OMAS has been frequentlyused to evaluate symptoms and subjectively scored func-tion after ankle fracture [10,12,28,29]. The score is vali-dated against (a) linear analogue scale (LAS) measuringsubjective recovery, (b) range of motion in loaded dorsi-flexion, (c) presence of osteoarthritis and (d) presence ofdislocations on radiographs, and it has been found to cor-relate well with these four parameters [28]. No floor orceiling effect has been reported [30].
Short-form SF-36The Short-form 36 (SF-36) is a self-administered genericquestionnaire designed to evaluate health-related qualityof life. The instrument measures eight health domainsusing eight scales assessing physical function (PF), rolelimitation due to physical problems (RP), bodily pain(BP), general health (GH), vitality (VT), social function(SF), role limitation due to emotional problems (RE), andmental health (MH). Low score implies poor health statushigh score implies good health status [31]. The SF-36 hasbeen validated for use in Sweden and normative data onhealthy people have been reported [32]. No studies eval-uating reliability and validity of SF-36 for use in anklefractures have been found. However, the SF-36 has beenemployed in some studies concerning patients with anklefractures [12,33-36]. The summary scales of PhysicalHealth (PCS) and Mental Health (MCS) were analysed.
Functional measuresAmbulation was assessed using the timed 9-meters walk-ing test performed at the maximum speed [8]. Further-more, the timed stair-climbing test was performed, that isthe time to ascend a flight of stairs (12 steps) using a self-selected technique. If possible the test should be per-formed without using a handrail [8].
Physical examinationLower limb muscle strength was evaluated using rising ontoes and heels. Ankle mobility was examined in loadeddorsiflexion and plantar flexion [17]. Loaded dorsiflexionwas measured with the technique described by Lindsjö etal. [24]. The head of the fibula was marked. The patientstood with the examined foot placed on a stool about 30cm high. With the sole of the foot flat on the stool the
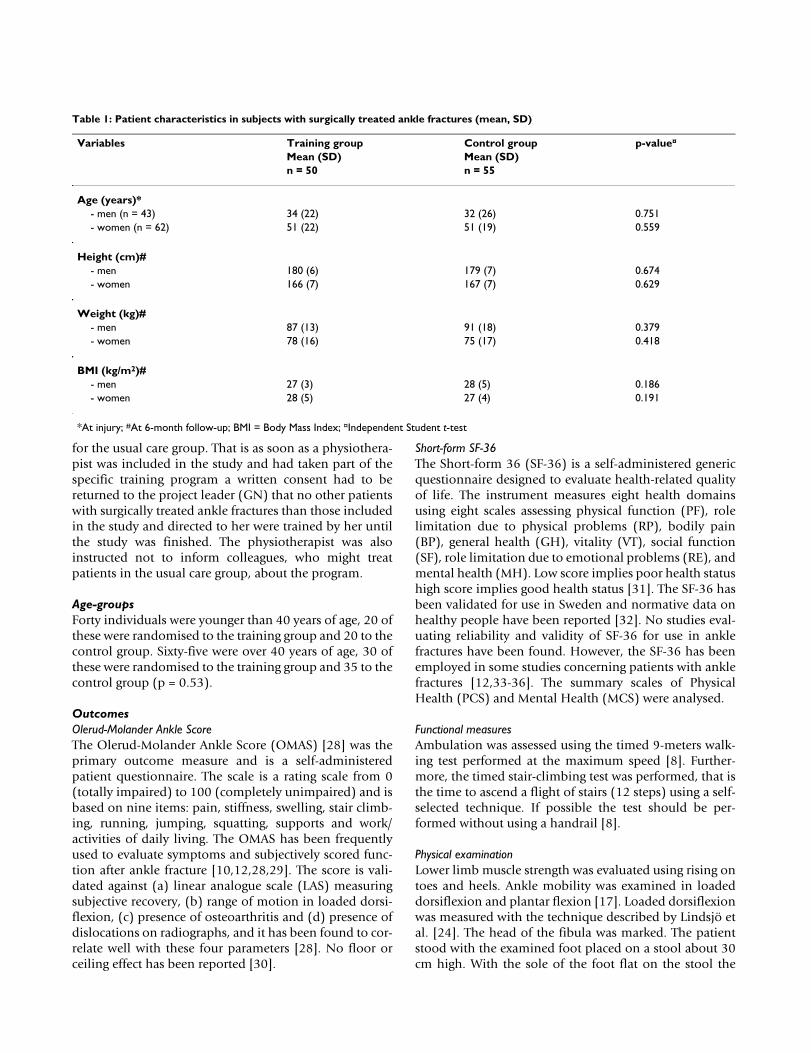
Table 1: Patient characteristics in subjects with surgically treated ankle fractures (mean, SD)
Variables Training group Control group p-value¤
Mean (SD) Mean (SD)n = 50 n = 55
Age (years)*- men (n = 43) 34 (22) 32 (26) 0.751- women (n = 62) 51 (22) 51 (19) 0.559
Height (cm)#- men 180 (6) 179 (7) 0.674- women 166 (7) 167 (7) 0.629
Weight (kg)#- men 87 (13) 91 (18) 0.379- women 78 (16) 75 (17) 0.418
BMI (kg/m2)#- men 27 (3) 28 (5) 0.186- women 28 (5) 27 (4) 0.191
*At injury; #At 6-month follow-up; BMI = Body Mass Index; ¤Independent Student t-test
BMC Musculoskeletal Disorders 2009, 10:118 http://www.biomedcentral.com/1471-2474/10/118
Page 5 of 11(page number not for citation purposes)
patient leaned forward with the greater part of the bodyweight on the examined foot to the point where the heelwas just in contact with the stool surface. The anglebetween the stool surface and a line going through the tipof the lateral malleolus and the mark at the head of thefibula was measured using a standard goniometer. The
normal value for dorsal extension was stated as 30° [37].To measure plantar flexion the patient sat on the edge ofa stool. The leg investigated was stretched forwards withthe whole sole of the foot on the floor to the point wherethe medial part of the forefoot was just in contact with thefloor. The angle between the floor and a line going
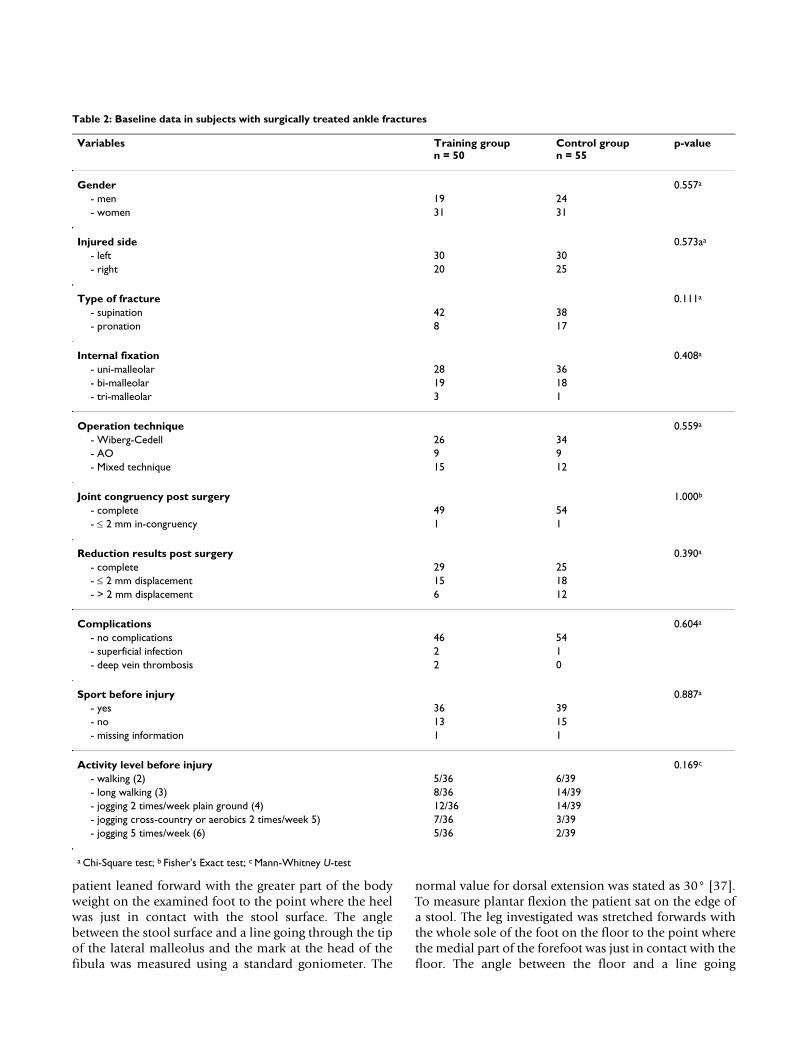
Table 2: Baseline data in subjects with surgically treated ankle fractures
Variables Training groupn = 50
Control groupn = 55
p-value
Gender 0.557a
- men 19 24- women 31 31
Injured side 0.573aa
- left 30 30- right 20 25
Type of fracture 0.111a
- supination 42 38- pronation 8 17
Internal fixation 0.408a
- uni-malleolar 28 36- bi-malleolar 19 18- tri-malleolar 3 1
Operation technique 0.559a
- Wiberg-Cedell 26 34- AO 9 9- Mixed technique 15 12
Joint congruency post surgery 1.000b
- complete 49 54- ≤ 2 mm in-congruency 1 1
Reduction results post surgery 0.390a
- complete 29 25- ≤ 2 mm displacement 15 18- > 2 mm displacement 6 12
Complications 0.604a
- no complications 46 54- superficial infection 2 1- deep vein thrombosis 2 0
Sport before injury 0.887a
- yes 36 39- no 13 15- missing information 1 1
Activity level before injury 0.169c
- walking (2) 5/36 6/39- long walking (3) 8/36 14/39- jogging 2 times/week plain ground (4) 12/36 14/39- jogging cross-country or aerobics 2 times/week 5) 7/36 3/39- jogging 5 times/week (6) 5/36 2/39
a Chi-Square test; b Fisher's Exact test; c Mann-Whitney U-test

BMC Musculoskeletal Disorders 2009, 10:118 http://www.biomedcentral.com/1471-2474/10/118
Page 6 of 11(page number not for citation purposes)
through the tip of the lateral malleolus and a mark at thehead of the fibula was measured using a standard goniom-eter. Measurements were carried out on both sides.
Statistical analysisThe statistical tests were performed according to the inten-tion to treat principles. Sample size calculation regardingthe main outcome measure OMAS showed that a samplesize of 51 individuals per group was needed to detect a dif-ference of 10 points between groups with an alfa level of0.05 and 80% power. We performed mixed model analy-sis on repeated measures of OMAS, the sub-scores PCSand MCS of SF-36, the muscle strength tests and the timedwalking tests as dependant variables, and treatmentgroup, gender, age-group, follow-up time as fixed factorsand the subjects as random factors. Analyses were per-formed both with and without interaction between age-group and treatment effect. The correlation between resid-uals within individuals was modelled as autoregressive(AR (1)). As an age younger than 40 years has been foundas a predictor of recovery after surgically treated ankle frac-tures the patients were divided in two groups over oryounger than forty years of age [16]. When analysing dif-ferences between groups regarding baseline characteris-tics, baseline data and radiological results the Student t-test, Mann-Whitney U-test and Chi-square tests wereemployed. An alpha level of 0.05 was regarded as statisti-cally significant.
ResultsAdherence to the programAll subjects remained in their allocation group through-out the study. The training group had a mean of 17 (SD 6)appointments with the physiotherapist and the controlgroup had a mean of 7 (SD 8) (p < 0.001). Thirteenpatients in the control group did not visit a physiothera-pist. Out of these all but two patients described differentactivities that they had performed on their own in order toregain function such as increased daily walking, move-ments of the ankle regularly, dancing, aerobics, balancetraining, strength training and stretching.
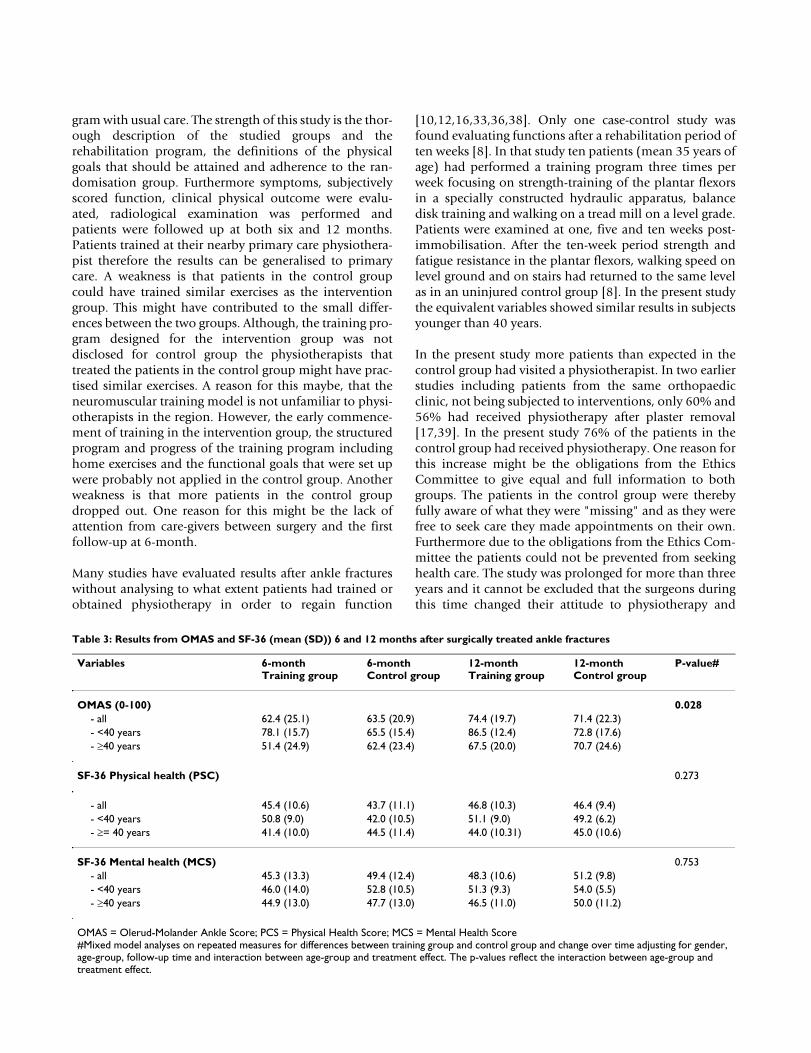
Olerud-Molander Ankle ScoreSubjects younger than 40 years in the training groupscored higher OMAS than those who were over 40 at bothfollow-ups. When including the variables age-group, gen-der, treatment group and follow-up time in the mixedmodel analysis no differences were found between groups(p = 0.310). When also including the interaction betweenage-group and treatment effect in the model a significantdifference was found in favour of the training group insubjects younger than 40 (p = 0.028) (Table 3).
Short-form SF-36The Summary Scale of Physical Health (PCS) showedhigher scores at 6-month in the training group in patients
younger than 40 years. However, when including the var-iables age-group, gender, treatment group and follow-uptime in the mixed model analysis no differences werefound between groups (p = 0.554). Neither when includ-ing the interaction of age-group and treatment effect inthe model was any significant difference found (p =0.273) (Table 3). Neither in the Summary Scale of MCSwas any difference found between the groups regardingtreatment effects. When performing the equivalent analy-sis regarding MCS no differences between groups werefound (p = 0.136) vs (p = 0.753) (Table 3).
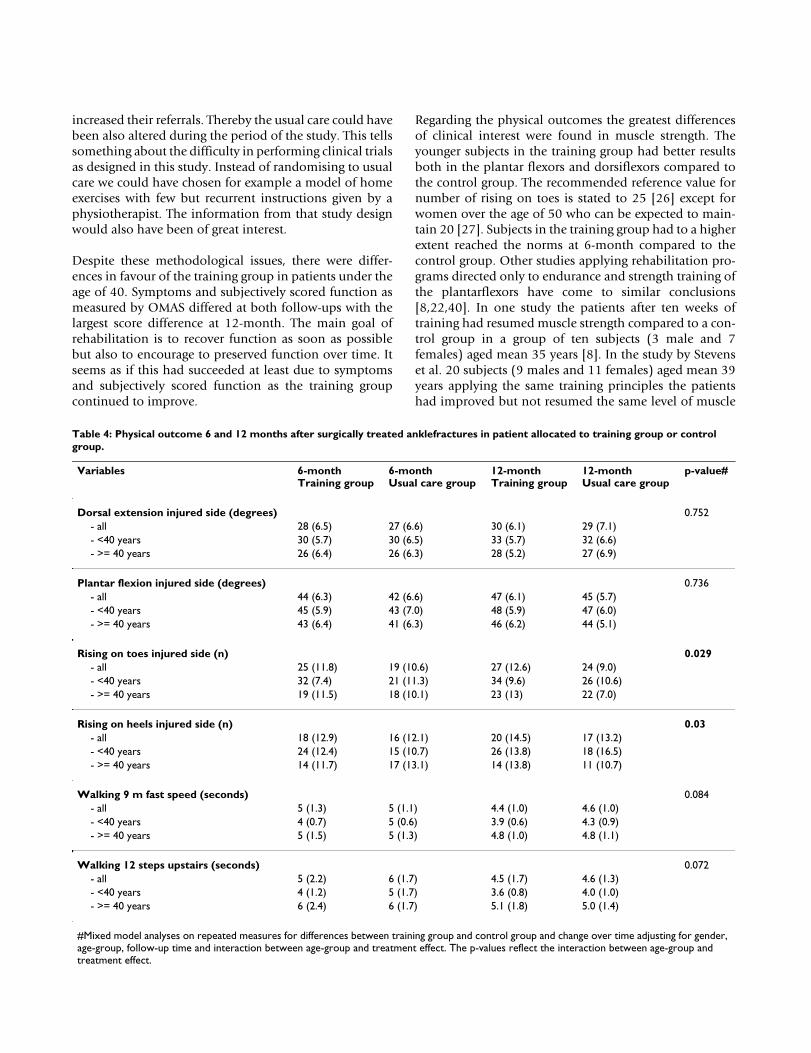
Physical examinationSubjects younger than 40 years of age in the traininggroup showed improved muscle strength both in theplantar flexors and dorsiflexors at both follow-ups com-pared to the control group. When including the variablesage-group, gender, treatment group and follow-up time inthe mixed model analysis there was a significant differ-ence regarding treatment effect in favour of the traininggroup in the plantar flexors (p = 0.007). When alsoincluding the interaction of age-group and treatmenteffect there was a significant difference in favour of thetraining group in subjects younger than 40 years of age (p= 0.029). After performing the equivalent analyses regard-ing muscle strength in the dorsiflexors significant differ-ences were found only when interaction of age-group andtreatment effect were included in the model (p = 0.030) vsnot included (p = 0.145). The timed walking test on evenground and on stairs did not show any significant differ-ences between groups (Table 4).
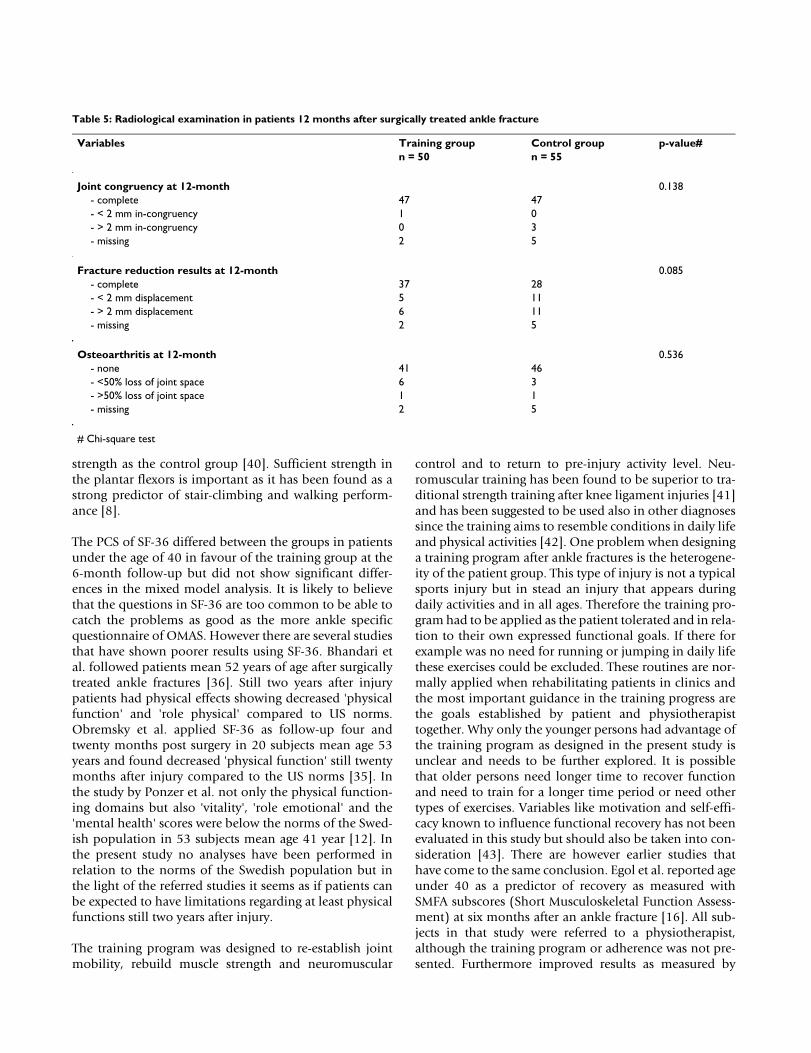
Radiographic examination at 12-month follow-upIn all, 98 patients attended at the radiological examina-tion at 12-month. All fractures were healed and 94/98showed complete joint congruency, < 2 mm in-congru-ency in one and > 2 mm in-congruency in three cases.Fracture reduction was complete in 65/98 ankles, < 2 mmin-complete in 16/98 ankles and > 2 mm in-complete in17/98. Nine patients had discrete signs of osteoarthritis (aloss of joint space less than 50%) and two had moderateosteoarthritis (a loss of joint space of more than 50% butno bone-to-bone contact). The results are presented intable by allocation groups (Table 5).
DiscussionThe standardised supervised training program employedin this study showed improved results for the exercisegroup compared to usual care when adjusting for theinteraction between age-group and treatment effect. Theseresults concerned both subjectively scored function andclinical physical outcome.
To our knowledge, this is the first randomised controlledtrial in patients with surgically treated ankle fracturescomparing a standardised and supervised training pro-
BMC Musculoskeletal Disorders 2009, 10:118 http://www.biomedcentral.com/1471-2474/10/118
Page 7 of 11(page number not for citation purposes)
gram with usual care. The strength of this study is the thor-ough description of the studied groups and therehabilitation program, the definitions of the physicalgoals that should be attained and adherence to the ran-domisation group. Furthermore symptoms, subjectivelyscored function, clinical physical outcome were evalu-ated, radiological examination was performed andpatients were followed up at both six and 12 months.Patients trained at their nearby primary care physiothera-pist therefore the results can be generalised to primarycare. A weakness is that patients in the control groupcould have trained similar exercises as the interventiongroup. This might have contributed to the small differ-ences between the two groups. Although, the training pro-gram designed for the intervention group was notdisclosed for control group the physiotherapists thattreated the patients in the control group might have prac-tised similar exercises. A reason for this maybe, that theneuromuscular training model is not unfamiliar to physi-otherapists in the region. However, the early commence-ment of training in the intervention group, the structuredprogram and progress of the training program includinghome exercises and the functional goals that were set upwere probably not applied in the control group. Anotherweakness is that more patients in the control groupdropped out. One reason for this might be the lack ofattention from care-givers between surgery and the firstfollow-up at 6-month.
Many studies have evaluated results after ankle fractureswithout analysing to what extent patients had trained orobtained physiotherapy in order to regain function
[10,12,16,33,36,38]. Only one case-control study wasfound evaluating functions after a rehabilitation period often weeks [8]. In that study ten patients (mean 35 years ofage) had performed a training program three times perweek focusing on strength-training of the plantar flexorsin a specially constructed hydraulic apparatus, balancedisk training and walking on a tread mill on a level grade.Patients were examined at one, five and ten weeks post-immobilisation. After the ten-week period strength andfatigue resistance in the plantar flexors, walking speed onlevel ground and on stairs had returned to the same levelas in an uninjured control group [8]. In the present studythe equivalent variables showed similar results in subjectsyounger than 40 years.
In the present study more patients than expected in thecontrol group had visited a physiotherapist. In two earlierstudies including patients from the same orthopaedicclinic, not being subjected to interventions, only 60% and56% had received physiotherapy after plaster removal[17,39]. In the present study 76% of the patients in thecontrol group had received physiotherapy. One reason forthis increase might be the obligations from the EthicsCommittee to give equal and full information to bothgroups. The patients in the control group were therebyfully aware of what they were "missing" and as they werefree to seek care they made appointments on their own.Furthermore due to the obligations from the Ethics Com-mittee the patients could not be prevented from seekinghealth care. The study was prolonged for more than threeyears and it cannot be excluded that the surgeons duringthis time changed their attitude to physiotherapy and
Table 3: Results from OMAS and SF-36 (mean (SD)) 6 and 12 months after surgically treated ankle fractures
Variables 6-monthTraining group
6-monthControl group
12-monthTraining group
12-monthControl group
P-value#
OMAS (0-100) 0.028- all 62.4 (25.1) 63.5 (20.9) 74.4 (19.7) 71.4 (22.3)- <40 years 78.1 (15.7) 65.5 (15.4) 86.5 (12.4) 72.8 (17.6)- ≥40 years 51.4 (24.9) 62.4 (23.4) 67.5 (20.0) 70.7 (24.6)
SF-36 Physical health (PSC) 0.273
- all 45.4 (10.6) 43.7 (11.1) 46.8 (10.3) 46.4 (9.4)- <40 years 50.8 (9.0) 42.0 (10.5) 51.1 (9.0) 49.2 (6.2)- ≥= 40 years 41.4 (10.0) 44.5 (11.4) 44.0 (10.31) 45.0 (10.6)
SF-36 Mental health (MCS) 0.753- all 45.3 (13.3) 49.4 (12.4) 48.3 (10.6) 51.2 (9.8)- <40 years 46.0 (14.0) 52.8 (10.5) 51.3 (9.3) 54.0 (5.5)- ≥40 years 44.9 (13.0) 47.7 (13.0) 46.5 (11.0) 50.0 (11.2)
OMAS = Olerud-Molander Ankle Score; PCS = Physical Health Score; MCS = Mental Health Score#Mixed model analyses on repeated measures for differences between training group and control group and change over time adjusting for gender, age-group, follow-up time and interaction between age-group and treatment effect. The p-values reflect the interaction between age-group and treatment effect.
BMC Musculoskeletal Disorders 2009, 10:118 http://www.biomedcentral.com/1471-2474/10/118
Page 8 of 11(page number not for citation purposes)
increased their referrals. Thereby the usual care could havebeen also altered during the period of the study. This tellssomething about the difficulty in performing clinical trialsas designed in this study. Instead of randomising to usualcare we could have chosen for example a model of homeexercises with few but recurrent instructions given by aphysiotherapist. The information from that study designwould also have been of great interest.
Despite these methodological issues, there were differ-ences in favour of the training group in patients under theage of 40. Symptoms and subjectively scored function asmeasured by OMAS differed at both follow-ups with thelargest score difference at 12-month. The main goal ofrehabilitation is to recover function as soon as possiblebut also to encourage to preserved function over time. Itseems as if this had succeeded at least due to symptomsand subjectively scored function as the training groupcontinued to improve.
Regarding the physical outcomes the greatest differencesof clinical interest were found in muscle strength. Theyounger subjects in the training group had better resultsboth in the plantar flexors and dorsiflexors compared tothe control group. The recommended reference value fornumber of rising on toes is stated to 25 [26] except forwomen over the age of 50 who can be expected to main-tain 20 [27]. Subjects in the training group had to a higherextent reached the norms at 6-month compared to thecontrol group. Other studies applying rehabilitation pro-grams directed only to endurance and strength training ofthe plantarflexors have come to similar conclusions[8,22,40]. In one study the patients after ten weeks oftraining had resumed muscle strength compared to a con-trol group in a group of ten subjects (3 male and 7females) aged mean 35 years [8]. In the study by Stevenset al. 20 subjects (9 males and 11 females) aged mean 39years applying the same training principles the patientshad improved but not resumed the same level of muscle
Table 4: Physical outcome 6 and 12 months after surgically treated anklefractures in patient allocated to training group or control group.
Variables 6-monthTraining group
6-monthUsual care group
12-monthTraining group
12-monthUsual care group
p-value#
Dorsal extension injured side (degrees) 0.752- all 28 (6.5) 27 (6.6) 30 (6.1) 29 (7.1)- <40 years 30 (5.7) 30 (6.5) 33 (5.7) 32 (6.6)- >= 40 years 26 (6.4) 26 (6.3) 28 (5.2) 27 (6.9)
Plantar flexion injured side (degrees) 0.736- all 44 (6.3) 42 (6.6) 47 (6.1) 45 (5.7)- <40 years 45 (5.9) 43 (7.0) 48 (5.9) 47 (6.0)- >= 40 years 43 (6.4) 41 (6.3) 46 (6.2) 44 (5.1)
Rising on toes injured side (n) 0.029- all 25 (11.8) 19 (10.6) 27 (12.6) 24 (9.0)- <40 years 32 (7.4) 21 (11.3) 34 (9.6) 26 (10.6)- >= 40 years 19 (11.5) 18 (10.1) 23 (13) 22 (7.0)
Rising on heels injured side (n) 0.03- all 18 (12.9) 16 (12.1) 20 (14.5) 17 (13.2)- <40 years 24 (12.4) 15 (10.7) 26 (13.8) 18 (16.5)- >= 40 years 14 (11.7) 17 (13.1) 14 (13.8) 11 (10.7)
Walking 9 m fast speed (seconds) 0.084- all 5 (1.3) 5 (1.1) 4.4 (1.0) 4.6 (1.0)- <40 years 4 (0.7) 5 (0.6) 3.9 (0.6) 4.3 (0.9)- >= 40 years 5 (1.5) 5 (1.3) 4.8 (1.0) 4.8 (1.1)
Walking 12 steps upstairs (seconds) 0.072- all 5 (2.2) 6 (1.7) 4.5 (1.7) 4.6 (1.3)- <40 years 4 (1.2) 5 (1.7) 3.6 (0.8) 4.0 (1.0)- >= 40 years 6 (2.4) 6 (1.7) 5.1 (1.8) 5.0 (1.4)
#Mixed model analyses on repeated measures for differences between training group and control group and change over time adjusting for gender, age-group, follow-up time and interaction between age-group and treatment effect. The p-values reflect the interaction between age-group and treatment effect.
BMC Musculoskeletal Disorders 2009, 10:118 http://www.biomedcentral.com/1471-2474/10/118
Page 9 of 11(page number not for citation purposes)
strength as the control group [40]. Sufficient strength inthe plantar flexors is important as it has been found as astrong predictor of stair-climbing and walking perform-ance [8].
The PCS of SF-36 differed between the groups in patientsunder the age of 40 in favour of the training group at the6-month follow-up but did not show significant differ-ences in the mixed model analysis. It is likely to believethat the questions in SF-36 are too common to be able tocatch the problems as good as the more ankle specificquestionnaire of OMAS. However there are several studiesthat have shown poorer results using SF-36. Bhandari etal. followed patients mean 52 years of age after surgicallytreated ankle fractures [36]. Still two years after injurypatients had physical effects showing decreased 'physicalfunction' and 'role physical' compared to US norms.Obremsky et al. applied SF-36 as follow-up four andtwenty months post surgery in 20 subjects mean age 53years and found decreased 'physical function' still twentymonths after injury compared to the US norms [35]. Inthe study by Ponzer et al. not only the physical function-ing domains but also 'vitality', 'role emotional' and the'mental health' scores were below the norms of the Swed-ish population in 53 subjects mean age 41 year [12]. Inthe present study no analyses have been performed inrelation to the norms of the Swedish population but inthe light of the referred studies it seems as if patients canbe expected to have limitations regarding at least physicalfunctions still two years after injury.
The training program was designed to re-establish jointmobility, rebuild muscle strength and neuromuscular
control and to return to pre-injury activity level. Neu-romuscular training has been found to be superior to tra-ditional strength training after knee ligament injuries [41]and has been suggested to be used also in other diagnosessince the training aims to resemble conditions in daily lifeand physical activities [42]. One problem when designinga training program after ankle fractures is the heterogene-ity of the patient group. This type of injury is not a typicalsports injury but in stead an injury that appears duringdaily activities and in all ages. Therefore the training pro-gram had to be applied as the patient tolerated and in rela-tion to their own expressed functional goals. If there forexample was no need for running or jumping in daily lifethese exercises could be excluded. These routines are nor-mally applied when rehabilitating patients in clinics andthe most important guidance in the training progress arethe goals established by patient and physiotherapisttogether. Why only the younger persons had advantage ofthe training program as designed in the present study isunclear and needs to be further explored. It is possiblethat older persons need longer time to recover functionand need to train for a longer time period or need othertypes of exercises. Variables like motivation and self-effi-cacy known to influence functional recovery has not beenevaluated in this study but should also be taken into con-sideration [43]. There are however earlier studies thathave come to the same conclusion. Egol et al. reported ageunder 40 as a predictor of recovery as measured withSMFA subscores (Short Musculoskeletal Function Assess-ment) at six months after an ankle fracture [16]. All sub-jects in that study were referred to a physiotherapist,although the training program or adherence was not pre-sented. Furthermore improved results as measured by
Table 5: Radiological examination in patients 12 months after surgically treated ankle fracture
Variables Training group Control group p-value#n = 50 n = 55
Joint congruency at 12-month 0.138- complete 47 47- < 2 mm in-congruency 1 0- > 2 mm in-congruency 0 3- missing 2 5
Fracture reduction results at 12-month 0.085- complete 37 28- < 2 mm displacement 5 11- > 2 mm displacement 6 11- missing 2 5
Osteoarthritis at 12-month 0.536- none 41 46- <50% loss of joint space 6 3- >50% loss of joint space 1 1- missing 2 5
# Chi-square test
BMC Musculoskeletal Disorders 2009, 10:118 http://www.biomedcentral.com/1471-2474/10/118
Page 10 of 11(page number not for citation purposes)
OMAS have been reported in patients under the age of 40compared to those over 40 at both one and three yearsafter injury. In that study 60% of the patients had visiteda physiotherapist [15].
ConclusionThe training model used in this study showed superiorresults compared to usual care regarding subjectivelyscored function and muscle strength in the plantar flexorsand dorsiflexors in patients under the age of 40. However,as only three out of nine outcome measures showed a dif-ference, the beneficial effect from an additional standard-ised individually suited training program can be expectedto be limited. There is need for further studies to elucidatehow a training program should be designed to increaseand optimise function in patients middle-aged or older.
Competing interestsThe authors declare that they have no competing interests.
Authors' contributionsGN participated in the design of the study, participated incollecting the data, performed the statistical analyses, anddrafted the manuscript. KJ examined all the radiographs.CE participated in the design of the study, and in theprogress and revision of the manuscript. ME was respon-sible for the identifying and including the patients, andparticipated in the progress and revision of the manu-script. All authors read and approved the final manu-script.
Additional material
AcknowledgementsWe would like to thank all the subjects who volunteered for this study, Per Nyberg at the Primary Healthcare Research Department, Skane County Council for statistical advice, the Faculty of Medicine at Lund University and the Skane County Council, Primary Healthcare Research for financial sup-port.
References1. van Staa TP, Dennison EM, Leufkens HG, Cooper C: Epidemiology
of fractures in England and Wales. Bone 2001, 29:517-522.2. Court-Brown C, Caesar B: Epidemiology of adult fractures: A
review. Injury 2006, 37:691-697.3. Jensen S, Andresen B, Mencke S, Nielsen P: Epidemiology of ankle
fractures. A propspective population-based study of 212cases in Aalborg, Denmark. Acta Orthop Scand 1998, 69:48-50.
4. Cedell C-A: Supination-outward rotation injuries of the ankle.In Acta Orthop Scand, Suppl No110 Munksgaard Copenhagen; 1967.
5. Müller ME, Allgöver M, Schneider R: Manual of internal fixation:Technique recommended by the AO-group. 2nd edition. Ber-lin, Germany, Springer-Verlag; 1979.
6. Lindsjö U: Operativ behandling av fotledsfrakturer. In PhD the-sis Uppsala Univerity, Uppsala, Sweden; 1980.
7. Tropp H, Norlin R: Ankle performance after ankle fracture: arandomized study of early mobilisation. Foot Ankle Int 1995,16:79-83.
8. Shaffer M, Okereke E, Esterhai J, Elliott M, Walter G, Yim S: Effectsof immobilization on plantar-flexion torque, fatigue resist-ance, and functional ability following an ankle fracture. PhysTher 2000, 80:769-780.
9. Lehtonen H, Jarvinen TL, Honkonen S, Nyman M, Vihtonen K,Jarvinen M: Use of a cast compared with a functional anklebrace after operative treatment of an ankle fracture. A pro-spective, randomized study. J Bone Joint Surg Am 2003, 85-A:205-11.
10. Hedström M, Ahl T, Dalen N: Early postoperative ankle exer-cise. A study of postoperative lateral malleolar fractures.Clinical Orthop Relate Res 1994, 300:193-196.
11. Low CK, Pang HY, Wong HP: A retrospective evaluation ofoperative treatment of ankle fractures. Ann Cad Med Singapore1997, 26:172-173.
12. Ponzer S, Nåsell H, Bergman B, Törnkvist H: Functional outcomeand quality of life patients with Type B ankle fractures: atwo-year follow up study. J Orthop Trauma 1999, 13:363-368.
13. Day G, Swanson C, Hulcombe B: Operative treatment of anklefractures: A minimum ten-year follow-up. Foot Ankle 2001,2:102-106.
14. Lash N, Horne G, Fielden J, Devane P: Ankle fractures: Functionaland lifestyle outcomes at 2 years. ANZ J Surg 2002, 72:724-730.
15. Nilsson GM, Jonsson K, Ekdahl CS, Eneroth M: Unsatisfactory out-come following surgical intervention of ankle fractures. FootAnkle Surg 2005, 11:11-16.
16. Egol KA, Tejwani NC, Walsh MG, Capla EL, Koval KJ: Predictors ofshort-term functional outcome following ankle fracture sur-gery. J Bone Joint Surg Am 2006, 88:974-979.
17. Nilsson G, Nyberg P, Ekdahl C, Eneroth M: Performance after sur-gical treatment of patients with ankle fractures 14-monthfollow up. Phys Res Int 2003, 8:69-82.
18. Risberg MA, Mörk H, Jenssen HK, Holm I: Design and implemen-tation of a neuromuscular training program following ante-rior cruciate ligament reconstruction. J Orthop Sports Phys Ther2001, 31:620-31.
19. Uh BS, Beynnon BD, Helie BV, Alosa PM, Renström PA: The benefitof a single-leg strength training program for the musclesaround the untrained ankle. Am J Sports Med 2000, 28:568-573.
20. Eils E, Rosenbaum D: A multi-station proprioceptive exerciseprogram in patients with ankle instability. Med Sci Sports Exerc2001, 33:1991-1998.
21. Matsusaka N, Yokoyama S, Tsurusaki T, Inokuchi S, Okita M: Effectof ankle disk training combined with tactile stimulation tothe leg and foot on functional instability of the ankle. Am JSports Med 2001, 29:25-30.
22. Stevens JE, Pathare NC, Tillman SM, Scarborough MT, Gibbs CP, ShahP, Jayaraman A, Walter GA, Vandenborne K: Relative contribu-tions of muscle activation and muscle size to plantarflexortorque during rehabilitation after immobilization. J OrthopRes 2006, 24:1729-1736.
23. Lauge-Hansen N: Combined experimental-surgical and exper-imental-roentgenological investigations. Arch Surg 1950,60:957-985.
24. Lindsjö U: Operative treatment of ankle fracture-dislocations:a follow-up of 306/321 consecutive cases. Clin Orthop 1985,199:28-38.
25. Kaikkonen A, Kannus P, Järvinen M: A performance test protocoland scoring scale for evaluation of ankle injuries. Am J SportsMed 1994, 4:462-469.
26. Lunsford B, Perry J: The standing heel-rise test for ankleplantar flexion: criterion for normal. Phys Ther 1995,75:694-698.
27. Stibrant-Sunnerhagen K, Hedberg M, Henning G-B, Cider Å, Svantes-son U: Muscle performance in an urban population sample of
Additional file 1Description of the rehabilitation program. Training program in patients with surgically treated ankle fractures starting within one week after plas-ter removal.Click here for file[http://www.biomedcentral.com/content/supplementary/1471-2474-10-118-S1.DOC]
RESEARCH ARTICLE
Weight-Bearing and Mobilization in thePostoperative Care of Ankle Fractures: ASystematic Review and Meta-Analysis ofRandomized Controlled Trials and CohortStudiesDiederik P. J. Smeeing1*, Roderick M. Houwert2, Jan Paul Briet3, Johannes C. Kelder4,Michiel J. M. Segers5, Egbert Jan M. M. Verleisdonk3, Luke P. H. Leenen1, Falco Hietbrink1
1 Department of Surgery, University Medical Center Utrecht, Utrecht, The Netherlands, 2 TraumacenterUniversity Medical Center Utrecht, Utrecht, The Netherlands, 3 Department of Surgery, DiakonessenhuisUtrecht, Utrecht, The Netherlands, 4 Department of Epidemiology, St Antonius Hospital Nieuwegein,Nieuwegein, The Netherlands, 5 Department of Surgery, St Antonius Hospital Nieuwegein, Nieuwegein, TheNetherlands
Abstract
Purpose
To determine the effectiveness and safety of interventions used for rehabilitation after open
reduction and internal fixation of ankle fractures.
Methods
A systematic review and meta-analysis was performed using both randomized trials and co-
hort studies. The effect of mobilization, weight-bearing, and unprotected weight-bearing as
tolerated on postoperative recovery was compared using the Olerud Molander score, return
to work/daily activities, and the rate of complications.
Results
A total of 25 articles were included. Ankle exercises resulted in earlier return to work and/or
daily activities compared to immobilization (mean difference (MD) -20.76 days; 95% confi-
dence interval (CI) -40.02 to -1.50). There was no difference in the rate of complications be-
tween exercises and immobilization (risk ratio (RR) 1.22; 95% CI 0.60 to 2.45) or between
early and late weight-bearing (RR 1.26; 95%CI 0.56 to 2.85).
Interpretation
Results of this meta-analysis show that following ankle surgery, 1) active exercises acceler-
ate return to work and daily activities compared to immobilization, 2) early weight-bearing
PLOSONE | DOI:10.1371/journal.pone.0118320 February 19, 2015 1 / 12
OPEN ACCESS
Citation: Smeeing DPJ, Houwert RM, Briet JP,Kelder JC, Segers MJM, Verleisdonk EJMM, et al.(2015) Weight-Bearing and Mobilization in thePostoperative Care of Ankle Fractures: A SystematicReview and Meta-Analysis of Randomized ControlledTrials and Cohort Studies. PLoS ONE 10(2):e0118320. doi:10.1371/journal.pone.0118320
Academic Editor: Stanislaw Stepkowski, Universityof Toledo, UNITED STATES
Received: September 25, 2014
Accepted: January 13, 2015
Published: February 19, 2015
Copyright: © 2015 Smeeing et al. This is an openaccess article distributed under the terms of theCreative Commons Attribution License, which permitsunrestricted use, distribution, and reproduction in anymedium, provided the original author and source arecredited.
Data Availability Statement: All relevant data arewithin the Supporting Information file Table S1(characteristics of all included studies). References ofall included studies are stated in the paper. If needed,full-text articles can be supplied by the correspondingauthor.
Funding: These authors have no support or fundingto report.
Competing Interests: The authors have declaredthat no competing interests exist.
Part 2:
tends to accelerate return to work and daily activities compared to late weight-bearing. Ac-
tive exercises in combination with immediate weight-bearing may be a safe option.
IntroductionAnkle fractures are the most common type of lower extremity fracture and among the mostcommon types of fractures worldwide [1]. The incidence of ankle fractures is between 100 and150 per 100,000 person-years and rising [2,3]. More than half of ankle fractures occur duringsports activities, which is indicative of a healthy patient population [4].
Ankle fractures are associated with high costs for both the affected individual and society.These costs are related not only to the operation and subsequent hospitalization, but also to theduration of occupational disability [5–8]. To reduce these latter costs, early functional return iscrucial [9].
While various classification systems exist to describe ankle fractures, the indication for sur-gery depends on the congruency of the ankle joint [10–12]. When an incongruent joint is pres-ent, fractures are often treated by open reduction and internal fixation to stabilize the anklejoint. The postoperative care regimens vary widely, e.g. from immobilization in a plaster castwithout weight-bearing for multiple weeks to immediate post-operative protected mobiliza-tion. Even direct post-operative unprotected weight-bearing as tolerated has been suggested[13].
Several systematic reviews have been published on various aspects of postoperative care reg-imens [14–17]. However, none of these reviews could provide clear advice for the postoperativecare of ankle fractures since the regimens differ in terms of protection, ankle movements, andweight-bearing. In this systematic review and meta-analysis, non-randomized studies were in-cluded to potentially assist in showing effectiveness. Furthermore, specific aspects of the post-operative care regimen were compared.
The aim of this study was to determine the effectiveness and safety of interventions that areused for rehabilitation after open reduction and internal fixation of ankle fractures.
MethodsA published review protocol does not exist.
Search strategy and selection criteriaRandomized controlled trials (RCT’s) and cohort studies evaluating postoperative care regimenof ankle fractures were included in this systematic review and meta-analysis (Weber, AO orLauge Hansen classifications) [10,11]. Two reviewers (DS and FH) independently searched theMEDLINE and EMBASE electronic databases in January 2014. No language or publication re-strictions were applied to the search, and disagreements were resolved by discussion (DS, FHand RH). The search was conducted using the following specific broad search string: [anklefracture OR Lauge Hansen ORWeber] AND [cast OR orthosis OR weight-bearing] AND[Olerud Molander OR follow-up].
Quality assessmentThe methodological quality of all included studies was assessed by three reviewers (DS, FH andRH) using the ‘risk of bias’ assessment tool provided by The Cochrane Collaboration [18].
The Postoperative Care of Ankle Fractures
PLOS ONE | DOI:10.1371/journal.pone.0118320 February 19, 2015 2 / 12

Outcome measuresThe effectiveness and safety of the postoperative care regimens were evaluated using the follow-ing outcome measures: the Olerud Molander score for functional objective outcome (short-term and long-term) [19], return to work and/or daily activities in days for functional subjec-tive outcome, and rate of complications, which is a direct result of the postoperative care regi-men, for safety outcome.
Data extractionTwo reviewers (DS and FH) independently extracted the following data: authors, year of publi-cation, study design, treatment groups, outcome, results between 6 and 12 weeks (short-term),results after 6 months (long-term), confidence interval (CI) or P value, and complications. Thecomplications were defined as reported in the studies. Author contact was attempted for stud-ies with missing data.
Data analysisStudies were included in the short-term analysis for the Olerud Molander score if results be-tween 6 and 12 weeks were reported. If more short-term results were reported, the resultsclosest to 6 weeks were used. Studies were included in the long-term analysis if results after6 months were reported. If more results were reported on the long-term, the Olerud Molanderscores from the final survey were used.
Review Manager ((RevMan) [Computer program]. Version 5.2. Copenhagen: The NordicCochrane Centre, The Cochrane Collaboration, 2012.) was used for the meta-analysis. A meandifference (MD) was calculated for continuous outcomes. The Inverse Variance (IV) with fixedeffect (Fixed) or with random effect (Random) method was used to construct a 95%CI. If astudy did not report standard deviation (SD), the value was not estimated. Available case analy-sis was performed with missing data. A risk ratio (RR) was calculated for complications, whichwas the only dichotomous outcome. The Mantel-Haenszel (M-H) with fixed effect (Fixed) orrandom effect (Random) method was used to compute a 95%CI for the dichotomous outcome.The assessment of statistical heterogeneity was done by visual inspection of the forest plots, theTau2 test, the Chi2 test, the degrees of freedom (df), the I2 value and the overall effect Z-test. Ifthe I2 value was below 25%, fixed effects were used. If the I2 value was 25% or greater, randomeffects were used. After the primary analyses, sensitivity analyses were performed. In the sensi-tivity analyses on bias, all studies with less than 5 high risk factors for bias were included. Stud-ies with 5 or more high risk factors for bias were excluded. In the sensitivity analysis on studydesign, only RCT’s were included. In the sensitivity analyses on time, all studies published after2000 were included.
Results
SearchTheMEDLINE and EMBASE search identified 259 and 87 studies, respectively. The 14 relevantstudies from the initial search were checked for related citations, resulting in 28 relevant studies.
In Kimmel et al. mobilization started with a difference of one day between the two groupsand in Starkweather et al. with a difference of seven days [20,21]. Partenheimer et al. only ana-lysed one group of patients [22]. Therefore, these studies were not included. Ultimately, a totalof 25 studies met the inclusion criteria (Fig. 1) [13,23–46].
The Postoperative Care of Ankle Fractures
PLOS ONE | DOI:10.1371/journal.pone.0118320 February 19, 2015 3 / 12
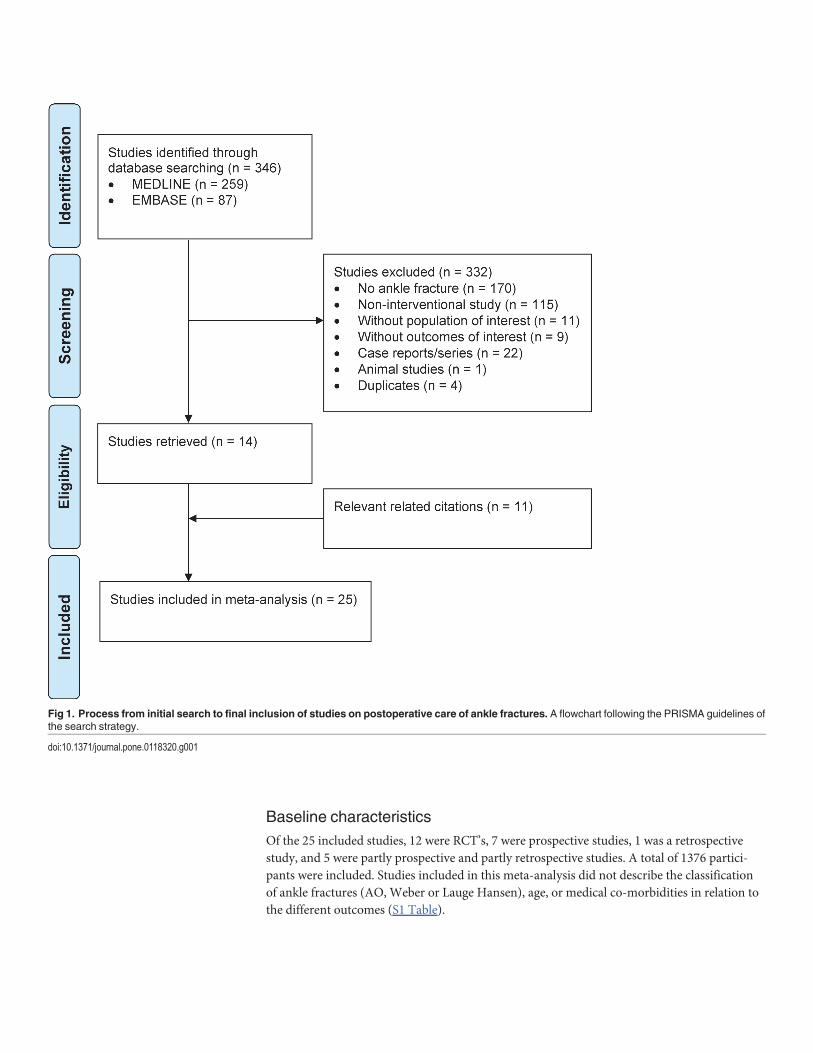
Baseline characteristicsOf the 25 included studies, 12 were RCT’s, 7 were prospective studies, 1 was a retrospectivestudy, and 5 were partly prospective and partly retrospective studies. A total of 1376 partici-pants were included. Studies included in this meta-analysis did not describe the classificationof ankle fractures (AO, Weber or Lauge Hansen), age, or medical co-morbidities in relation tothe different outcomes (S1 Table).
Fig 1. Process from initial search to final inclusion of studies on postoperative care of ankle fractures. A flowchart following the PRISMA guidelines ofthe search strategy.
doi:10.1371/journal.pone.0118320.g001
The Postoperative Care of Ankle Fractures
PLOS ONE | DOI:10.1371/journal.pone.0118320 February 19, 2015 4 / 12
BiasNearly all studies had a high risk of bias, both cohort studies and RCT’s (Fig. 2). More thanhalf of the studies had a high risk on random sequence generation (52%), on allocation con-cealment (80%), and on blinding of outcome assessment (80%). Since treatment was visible,the participants and personnel of all studies, cohort studies and RCT’s, were not blinded. In11 (44%) studies, a high risk of other bias was found. In 7 of these studies, patients with aWeber A fracture who had undergone surgery were included [13,27,33,36,38,39,43]. However,further specifications of these fractures were not presented.
Effect of mobilizationA total of 19 studies investigated the effect of mobilization (ankle exercises) on recovery[13,27–33,35–38,40–46]. Honigmann et al. and Laarhoven van et al. only reported the medianresults and Wetzler et al. did not describe enough data for analysis [36,37,46]. Therefore, thesethree studies were excluded from the analysis. Tropp et al. used a modified Olerud Molanderscore [44]. Finsen et al. compared 3 groups with each other; only groups A and B with a non-weight-bearing treatment were analysed [32].
The Olerud Molander score was reported in 9 studies. No statistically significant resultswere found with the short-term (MD -6.88; 95%CI -17.66 to 3.91) or long-term Olerud Molan-der score (MD -1.05; 95%CI -4.11 to 2.00).
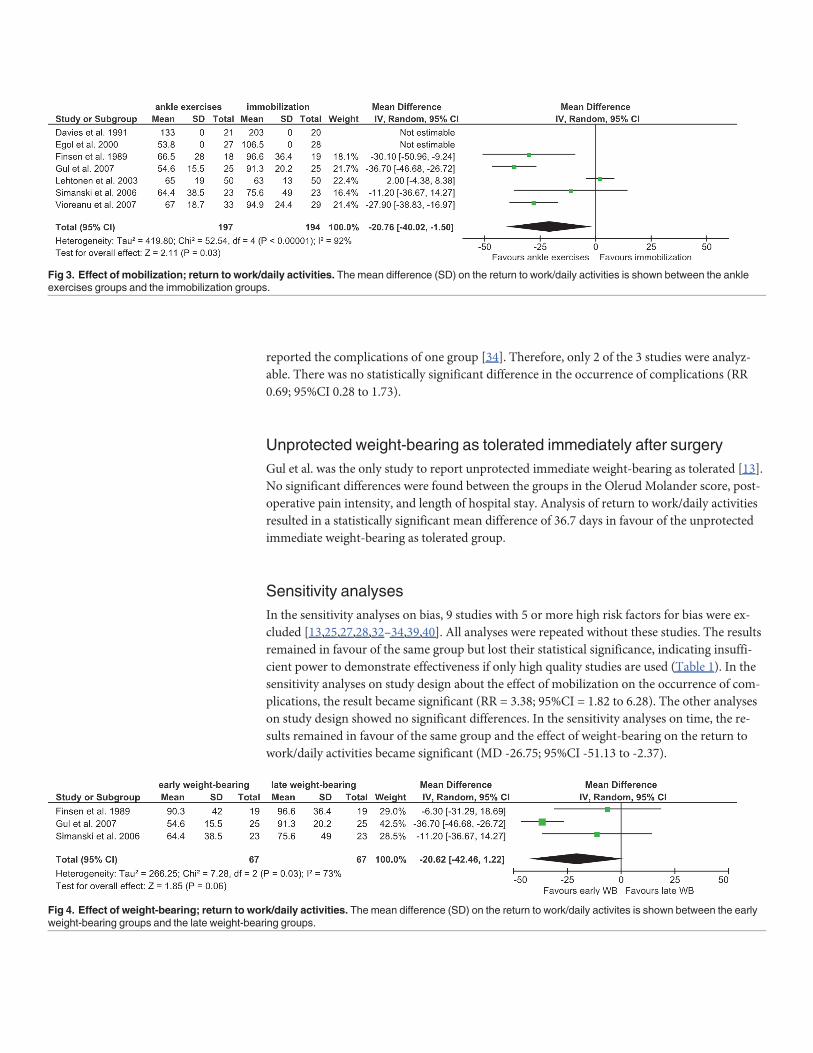
The return to work and/or daily activities was reported in 7 of the active mobilization stud-ies (Fig. 3). The total mean difference was -20.76 days in favour of the ankle exercises group(95%CI -40.02 to -1.50).
Complications were reported entirely (and attributed to a group) in 12 studies. The natureand definition of the complications differed, but they were comparable in terms of severity. Nostatistically significant difference was found in the occurrence of complications (RR 1.22; 95%CI0.60 to 2.45). Lehtonen’s data skewed the results [38].
Unprotected mobilization was described in 7 studies [13,32,36,37,39,41,43]. With theexception of Gul et al., these studies used unprotected mobilization in combination with lateweight-bearing (3–6 weeks post-operatively) [13]. Finsen et al. and Lund-Kristensen et al. didnot report the groups in which complications occurred [32,39]. Siddique et al. did not reportthe complications [41]. No statistically significant difference was found in the occurrence ofcomplications (RR 1.03; 95%CI 0.42 to 2.50).
Effect of weight-bearingThe effect of weight-bearing on postoperative recovery was reported in 11 studies that com-pared early versus late weight-bearing [13,23–26,32,34,36,37,42,46]. Honigmann et al. andLaarhoven van et al. reported only the median scores, and Wetzler et al. did not describeenough data for analysis. Therefore, these three studies were excluded from analyses[36,37,46].
Analysis of the short-term Olerud Molander score was not possible. Although the long-term Olerud Molander score was reported in three studies, only Simanski et al. reported the SDvalues, so analysis of the long-term score also was not possible [42].
Of the 11 studies, only 3 reported the mean results of return to work and/or daily activities(Fig. 4). In Finsen et al., the two groups without ankle exercises (groups B and C) were used inthe analysis [32]. The total mean difference was -20.62 days in favour of the early weight-bear-ing group (95%CI -42.46 to 1.22). For analysis of complications, 8 of the 11 studies were used.No statistically significant difference was found (RR 1.26; 95%CI 0.56 to 2.85). Weight-bearingas tolerated began immediately after surgery in 3 studies [13,27,34]. Harager et al. only
The Postoperative Care of Ankle Fractures
PLOS ONE | DOI:10.1371/journal.pone.0118320 February 19, 2015 5 / 12
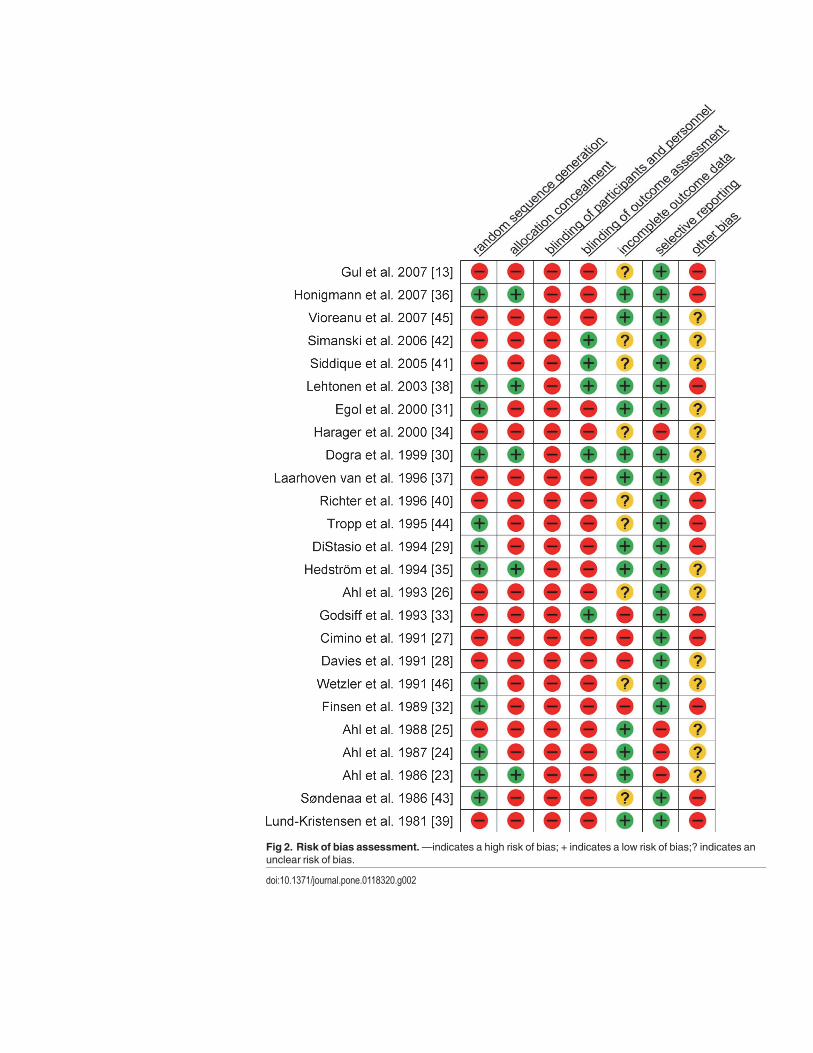
Fig 2. Risk of bias assessment.—indicates a high risk of bias; + indicates a low risk of bias;? indicates anunclear risk of bias.
doi:10.1371/journal.pone.0118320.g002
The Postoperative Care of Ankle Fractures
PLOS ONE | DOI:10.1371/journal.pone.0118320 February 19, 2015 6 / 12
reported the complications of one group [34]. Therefore, only 2 of the 3 studies were analyz-able. There was no statistically significant difference in the occurrence of complications (RR0.69; 95%CI 0.28 to 1.73).
Unprotected weight-bearing as tolerated immediately after surgeryGul et al. was the only study to report unprotected immediate weight-bearing as tolerated [13].No significant differences were found between the groups in the Olerud Molander score, post-operative pain intensity, and length of hospital stay. Analysis of return to work/daily activitiesresulted in a statistically significant mean difference of 36.7 days in favour of the unprotectedimmediate weight-bearing as tolerated group.
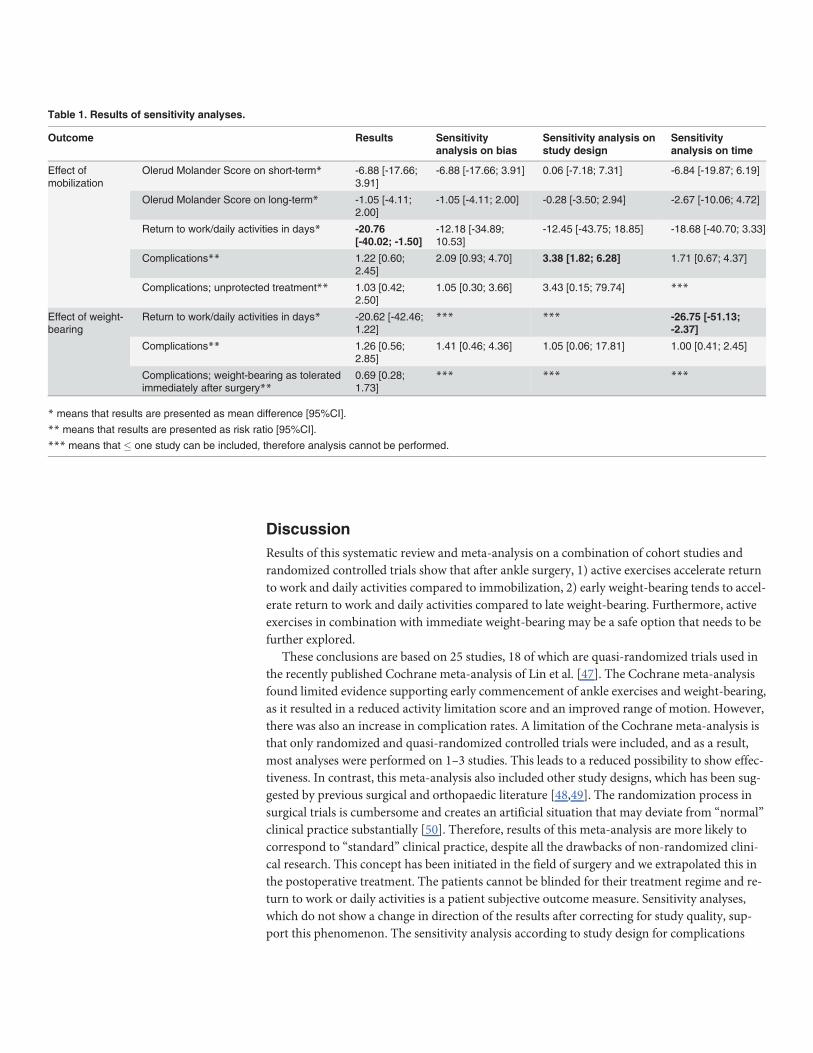
Sensitivity analysesIn the sensitivity analyses on bias, 9 studies with 5 or more high risk factors for bias were ex-cluded [13,25,27,28,32–34,39,40]. All analyses were repeated without these studies. The resultsremained in favour of the same group but lost their statistical significance, indicating insuffi-cient power to demonstrate effectiveness if only high quality studies are used (Table 1). In thesensitivity analyses on study design about the effect of mobilization on the occurrence of com-plications, the result became significant (RR = 3.38; 95%CI = 1.82 to 6.28). The other analyseson study design showed no significant differences. In the sensitivity analyses on time, the re-sults remained in favour of the same group and the effect of weight-bearing on the return towork/daily activities became significant (MD -26.75; 95%CI -51.13 to -2.37).
Fig 3. Effect of mobilization; return to work/daily activities. The mean difference (SD) on the return to work/daily activities is shown between the ankleexercises groups and the immobilization groups.
doi:10.1371/journal.pone.0118320.g003
Fig 4. Effect of weight-bearing; return to work/daily activities. The mean difference (SD) on the return to work/daily activites is shown between the earlyweight-bearing groups and the late weight-bearing groups.
doi:10.1371/journal.pone.0118320.g004
The Postoperative Care of Ankle Fractures
PLOS ONE | DOI:10.1371/journal.pone.0118320 February 19, 2015 7 / 12
DiscussionResults of this systematic review and meta-analysis on a combination of cohort studies andrandomized controlled trials show that after ankle surgery, 1) active exercises accelerate returnto work and daily activities compared to immobilization, 2) early weight-bearing tends to accel-erate return to work and daily activities compared to late weight-bearing. Furthermore, activeexercises in combination with immediate weight-bearing may be a safe option that needs to befurther explored.
These conclusions are based on 25 studies, 18 of which are quasi-randomized trials used inthe recently published Cochrane meta-analysis of Lin et al. [47]. The Cochrane meta-analysisfound limited evidence supporting early commencement of ankle exercises and weight-bearing,as it resulted in a reduced activity limitation score and an improved range of motion. However,there was also an increase in complication rates. A limitation of the Cochrane meta-analysis isthat only randomized and quasi-randomized controlled trials were included, and as a result,most analyses were performed on 1–3 studies. This leads to a reduced possibility to show effec-tiveness. In contrast, this meta-analysis also included other study designs, which has been sug-gested by previous surgical and orthopaedic literature [48,49]. The randomization process insurgical trials is cumbersome and creates an artificial situation that may deviate from “normal”clinical practice substantially [50]. Therefore, results of this meta-analysis are more likely tocorrespond to “standard” clinical practice, despite all the drawbacks of non-randomized clini-cal research. This concept has been initiated in the field of surgery and we extrapolated this inthe postoperative treatment. The patients cannot be blinded for their treatment regime and re-turn to work or daily activities is a patient subjective outcome measure. Sensitivity analyses,which do not show a change in direction of the results after correcting for study quality, sup-port this phenomenon. The sensitivity analysis according to study design for complications
Table 1. Results of sensitivity analyses.
Outcome Results Sensitivityanalysis on bias
Sensitivity analysis onstudy design
Sensitivityanalysis on time
Effect ofmobilization
Olerud Molander Score on short-term* -6.88 [-17.66;3.91]
-6.88 [-17.66; 3.91] 0.06 [-7.18; 7.31] -6.84 [-19.87; 6.19]
Olerud Molander Score on long-term* -1.05 [-4.11;2.00]
-1.05 [-4.11; 2.00] -0.28 [-3.50; 2.94] -2.67 [-10.06; 4.72]
Return to work/daily activities in days* -20.76[-40.02; -1.50]
-12.18 [-34.89;10.53]
-12.45 [-43.75; 18.85] -18.68 [-40.70; 3.33]
Complications** 1.22 [0.60;2.45]
2.09 [0.93; 4.70] 3.38 [1.82; 6.28] 1.71 [0.67; 4.37]
Complications; unprotected treatment** 1.03 [0.42;2.50]
1.05 [0.30; 3.66] 3.43 [0.15; 79.74] ***
Effect of weight-bearing
Return to work/daily activities in days* -20.62 [-42.46;1.22]
*** *** -26.75 [-51.13;-2.37]
Complications** 1.26 [0.56;2.85]
1.41 [0.46; 4.36] 1.05 [0.06; 17.81] 1.00 [0.41; 2.45]
Complications; weight-bearing as toleratedimmediately after surgery**
0.69 [0.28;1.73]
*** *** ***
* means that results are presented as mean difference [95%CI].
** means that results are presented as risk ratio [95%CI].
*** means that � one study can be included, therefore analysis cannot be performed.
doi:10.1371/journal.pone.0118320.t001
The Postoperative Care of Ankle Fractures
PLOS ONE | DOI:10.1371/journal.pone.0118320 February 19, 2015 8 / 12
changed into statistical significance in favour of immobilization. These results are heavily influ-enced by the study of Lehtonen et al. [38].
This study provides data about return to work, which is becoming increasingly importantfor health care providers in current practice. We found that active mobilization results in earli-er return to work and/or daily activities of 21 days. This result might lead to a cost reduction insocial security payments and lost wages [5,7,51].
Other reviews have been published on various aspects of postoperative care regimens[14–17]. Nash et al. concluded that immobilization provides no benefit, and Thomas et al. con-cluded that it is difficult to determine whether early motion is overall better or worse than castimmobilization [15,17]. Black et al. suggested that early weight-bearing might allow for fasterrehabilitation and earlier return to work [14]. Smith et al. concluded that because of the littledifference in outcome, the optimum time to commence weight-bearing cannot be determined[16]. These reviews focused on whole postoperative care regimens rather than specific aspectsof postoperative care and could not give a differentiated clinical advice. In this review, we ana-lyzed separate aspects of the postoperative care regimen: effect of ankle exercises, weight-bear-ing, and unprotected treatment in order to tailor clinical advice accordingly.
Nilsson et al. suggested that a difference of 4.4 points in the Olerud Molander score is ofclinical interest for a group of patients [52]. This meta-analysis shows an even greater differ-ence in the Olerud Molander score of 6.88 points on short-term in favour of active mobiliza-tion and 8.00 points on long-term in favour of early weight-bearing. Both outcomes fail toreach statistical significance but are in concordance with previous analyses [15,17,47].
Due to the inclusion of all relevant study designs without language restrictions, a large num-ber of studies were evaluated in this meta-analysis. Three independent reviewers systematicallyevaluated the studies for risk of bias. In this quality assessment, a great deal of bias was foundin the published studies, which rendered the results of these studies less reliable. The differentvariables used in this meta-analysis could cause heterogeneity because of poor definitions ofthese variables in some of the included studies. This meta-analysis describes the complicationsas defined in the studies, which allowed the severity of complications to be compared. Howev-er, definitions vary and thus may result in bias.
Direct active mobilization after surgery is advantageous compared to immobilization, andweight-bearing shows a similar trend. This meta-analysis shows no increased risk for complica-tions with active mobilization after early weight-bearing. Therefore, the combination of activemobilization and early weight-bearing might be a promising strategy. Gul et al. published en-couraging results on direct unprotected weight-bearing as tolerated in a retrospective study de-sign [13]. Currently, there are two trials being conducted on the postoperative care of anklefractures (NCT01196338 and NTR3727).
ConclusionActive mobilization results in an earlier return to work. Both active mobilization and immedi-ate protected weight-bearing may be safe postoperative care strategies after ankle surgery, sothe regimen choice should be based on patient demands with an emphasis on active mobiliza-tion. Unprotected weight-bearing as tolerated after ankle surgery may also be a safe and prom-ising choice. As such, future research should address this option.
Supporting InformationS1 Table. Characteristics of included studies. Results which are not used in analyses arewritten in italics. Complications that are not directly related to the post-operative treatmentregimen and the complications with an unknown group are also written in italics. + means
The Postoperative Care of Ankle Fractures
PLOS ONE | DOI:10.1371/journal.pone.0118320 February 19, 2015 9 / 12
yes/present; - means no/not present.(PDF)
S2 Table. PRISMA Checklist.(PDF)
Author ContributionsConceived and designed the experiments: DS RH FH. Performed the experiments: DS RH FH.Analyzed the data: DS RH FH. Contributed reagents/materials/analysis tools: DS RH JK FH.Wrote the paper: DS RH JB JK MS EV LL FH.
References1. Court-Brown CM, Caesar B (2006) Epidemiology of adult fractures: A review. Injury. 37: 691–697.
S0020-1383(06)00323-8 [pii]; doi: 10.1016/j.injury.2006.04.130 PMID: 16814787
2. Jensen SL, Andresen BK, Mencke S, Nielsen PT (1998) Epidemiology of ankle fractures. A prospectivepopulation-based study of 212 cases in Aalborg, Denmark. Acta Orthop Scand. 69: 48–50. PMID:9524518
3. Daly PJ, Fitzgerald RH Jr, Melton LJ, Ilstrup DM (1987) Epidemiology of ankle fractures in Rochester,Minnesota. Acta Orthop Scand. 58: 539–544. PMID: 3425285
4. Reiner M, Niermann C, Jekauc D, Woll A (2013) Long-term health benefits of physical activity—a sys-tematic review of longitudinal studies. BMC Public Health. 13: 813. 1471-2458-13-813 [pii]; doi: 10.1186/1471-2458-13-813 PMID: 24010994
5. Bhandari M, Sprague S, Ayeni OR, Hanson BP, Moro JK (2004) A prospective cost analysis followingoperative treatment of unstable ankle fractures: 30 patients followed for 1 year. Acta Orthop Scand. 75:100–105. doi: 10.1080/00016470410001708200 PMID: 15022817
6. Jain N, Symes T, Doorgakant A, DawsonM (2008) Clinical audit of the management of stable anklefractures. Ann R Coll Surg Engl. 90: 483–487. doi: 10.1308/003588408X301145 PMID: 18765028
7. Lin CW, Haas M, Moseley AM, Herbert RD, Refshauge KM (2008) Cost and utilisation of healthcare re-sources during rehabilitation after ankle fracture are not linked to health insurance, income, gender, orpain: an observational study. Aust J Physiother. 54: 201–208. PMID: 18721124
8. Murray AM, McDonald SE, Archbold P, Crealey GE (2011) Cost description of inpatient treatment forankle fracture. Injury. 42: 1226–1229. S0020-1383(10)00635-2 [pii]; doi: 10.1016/j.injury.2010.08.023PMID: 20869055
9. DelBuono A, Smith R, Coco M, Woolley L, Denaro V, et al. (2013) Return to sports after ankle fractures:a systematic review. Br Med Bull. 106: 179–191. lds039 [pii]; doi: 10.1093/bmb/lds039 PMID:23258924
10. Hughes JL, Weber H, Willenegger H, Kuner EH (1979) Evaluation of ankle fractures: non-operative andoperative treatment. Clin Orthop Relat Res. 111–119.
11. Lauge-Hansen N (1942) Ankelbrud I. Genetisk diagnose og reposition. Copenhagen, M.D. thesis.Munksgaard. [dissertation].
12. Olerud C, Molander H, Olsson T, Hagstedt B (1986) Ankle fractures treated with non-rigid internal fixa-tion. Injury. 17: 23–27. PMID: 3770880
13. Gul A, Batra S, Mehmood S, Gillham N (2007) Immediate unprotected weight-bearing of operativelytreated ankle fractures. Acta Orthop Belg. 73: 360–365. PMID: 17715727
14. Black JD, Bhavikatti M, Al-Hadithy N, Hakmi A, Kitson J (2013) Early weight-bearing in operatively fixedankle fractures: A systematic review. Foot (Edinb). S0958-2592(13)00022-9 [pii];10.1016/j.foot.2013.05.002 [doi].
15. Nash CE, Mickan SM, Del Mar CB, Glasziou PP (2004) Resting injured limbs delays recovery: a sys-tematic review. J Fam Pract. 53: 706–712. jfp_0904_5309i [pii]. PMID: 15353159
16. Smith T, Davies L (2008) When Should Open Reduction and Internal Fixation Ankle Fractures BeginWeight Bearing? A Systematic Review. Eur J Trauma Emerg Surg. 34: 69–76.
17. Thomas G, Whalley H, Modi C (2009) Early mobilization of operatively fixed ankle fractures: a system-atic review. Foot Ankle Int. 30: 666–674. 50026187 [pii]; doi: 10.3113/FAI.2009.0666 PMID: 19589314
The Postoperative Care of Ankle Fractures
PLOS ONE | DOI:10.1371/journal.pone.0118320 February 19, 2015 10 / 12
18. Higgins JP, Altman DG, Gotzsche PC, Juni P, Moher D, et al. (2011) The Cochrane Collaboration's toolfor assessing risk of bias in randomised trials. BMJ. 343: d5928. doi: 10.1136/bmj.d5928 PMID:22008217
19. Olerud C, Molander H (1984) A scoring scale for symptom evaluation after ankle fracture. Arch OrthopTrauma Surg. 103: 190–194. PMID: 6437370
20. Kimmel LA, Edwards ER, Liew SM, Oldmeadow LB, Webb MJ, et al. (2012) Rest easy? Is bed rest real-ly necessary after surgical repair of an ankle fracture? Injury. 43: 766–771. S0020-1383(11)00422-0[pii]; doi: 10.1016/j.injury.2011.08.031 PMID: 21962296
21. Starkweather MP, Collman DR, Schuberth JM (2012) Early protected weightbearing after open reduc-tion internal fixation of ankle fractures. J Foot Ankle Surg. 51: 575–578. S1067-2516(12)00213-X [pii];doi: 10.1053/j.jfas.2012.05.022 PMID: 22819002
22. Partenheimer A, Geerling J, Voigt C, Lill H (2010) [Early functional treatment and full weight-bearing ofsurgically treated isolated ankle fractures in the elderly]. Unfallchirurg. 113: 308–312. doi: 10.1007/s00113-009-1724-9 PMID: 20195841
23. Ahl T, Dalen N, Holmberg S, Selvik G (1986) Early weight bearing of malleolar fractures. Acta OrthopScand. 57: 526–529. PMID: 3577722
24. Ahl T, Dalen N, Holmberg S, Selvik G (1987) Early weight bearing of displaced ankle fractures. ActaOrthop Scand. 58: 535–538. PMID: 3425284
25. Ahl T, Dalen N, Selvik G (1988) Mobilization after operation of ankle fractures. Good results of early mo-tion and weight bearing. Acta Orthop Scand. 59: 302–306. PMID: 3132812
26. Ahl T, Dalen N, Lundberg A, Bylund C (1993) Early mobilization of operated on ankle fractures. Pro-spective, controlled study of 40 bimalleolar cases. Acta Orthop Scand. 64: 95–99. PMID: 8451961
27. CiminoW, Ichtertz D, Slabaugh P (1991) Early mobilization of ankle fractures after open reduction andinternal fixation. Clin Orthop Relat Res. 152–156. PMID: 1934726
28. Davies S (1991) Effects of Continuous Passive Movement and Plaster of Paris after Internal Fixation ofAnkle Fractures. Physiotherapy. 77: 516–520.
29. DiStasio AJ, Jaggears FR, DePasquale LV, Frassica FJ, Turen CH (1994) Protected early motion ver-sus cast immobilization in postoperative management of ankle fractures. Contemp Orthop. 29: 273–277. PMID: 10150249
30. Dogra AS, Rangan A (1999) Early mobilisation versus immobilisation of surgically treated ankle frac-tures. Prospective randomised control trial. Injury. 30: 417–419. S0020138399001102 [pii]. PMID:10645355
31. Egol KA, Dolan R, Koval KJ (2000) Functional outcome of surgery for fractures of the ankle. A prospec-tive, randomised comparison of management in a cast or a functional brace. J Bone Joint Surg Br. 82:246–249. PMID: 10755435
32. Finsen V, Saetermo R, Kibsgaard L, Farran K, Engebretsen L, et al. (1989) Early postoperative weight-bearing and muscle activity in patients who have a fracture of the ankle. J Bone Joint Surg Am. 71: 23–27. PMID: 2492286
33. Godsiff SP, Trakru S, Kefer G, Maniar RN, Flanagan JP, et al. (1993) A comparative study of early mo-tion and immediate plaster splintage after internal fixation of unstable fractures of the ankle. Injury. 24:529–530. PMID: 8244545
34. Harager K, Hviid K, Jensen CM, Schantz K (2000) Successful immediate weight-bearing of internal fix-ated ankle fractures in a general population. J Orthop Sci. 5: 552–554. PMID: 11180917
35. HedstromM, Ahl T, Dalen N (1994) Early postoperative ankle exercise. A study of postoperative lateralmalleolar fractures. Clin Orthop Relat Res. 193–196.
36. Honigmann P, Goldhahn S, Rosenkranz J, Audige L, Geissmann D, et al. (2007) Aftertreatment of mal-leolar fractures following ORIF—functional compared to protected functional in a vacuum-stabilizedorthesis: a randomized controlled trial. Arch Orthop Trauma Surg.; 127: 195–203. doi: 10.1007/s00402-006-0255-x PMID: 17195934
37. Laarhoven van CJ, Meeuwis JD, van der Werken C (1996) Postoperative treatment of internally fixedankle fractures: a prospective randomised study. J Bone Joint Surg Br. 78: 395–399. PMID: 8636173
38. Lehtonen H, Jarvinen TL, Honkonen S, NymanM, Vihtonen K, et al. (2003) Use of a cast comparedwith a functional ankle brace after operative treatment of an ankle fracture. A prospective, randomizedstudy. J Bone Joint Surg Am. 85-A: 205–211. PMID: 12571295
39. Lund-Kristensen J, Greiff J, Riegels-Nielsen P (1981) Malleolar fractures treated with rigid internal fixa-tion and immediate mobilization. Injury. 13: 191–195. 0020-1383(81)90237-0 [pii]. PMID: 6799402
40. Richter J, Langer C, Hahn MP, Josten C, Muhr G. Ist die funktionell konservative Behandlung stabilerAussenknöchelfrakturen gerechtfertigt? Chirurg. 1996; 67: 1255–1260. PMID: 9081789
The Postoperative Care of Ankle Fractures
PLOS ONE | DOI:10.1371/journal.pone.0118320 February 19, 2015 11 / 12
41. Siddique A, Prasad C, O'Connor D (2005) Early Active Mobilization Versus Cast Immobilization in Op-eratively Treated Ankle Fractures. Eur J Trauma. 31: 398–400.
42. Simanski CJ, Maegele MG, Lefering R, Lehnen DM, Kawel N, et al. (2006) Functional treatment andearly weightbearing after an ankle fracture: a prospective study. J Orthop Trauma. 20: 108–114. doi:10.1097/01.bot.0000197701.96954.8c 00005131-200602000-00005 [pii]. PMID: 16462563
43. Sondenaa K, Hoigaard U, Smith D, Alho A (1986) Immobilization of operated ankle fractures. ActaOrthop Scand. 57: 59–61. PMID: 3083644
44. Tropp H, Norlin R (1995) Ankle performance after ankle fracture: a randomized study of early mobiliza-tion. Foot Ankle Int. 16: 79–83. PMID: 7767451
45. Vioreanu M, Dudeney S, Hurson B, Kelly E, O'Rourke K, et al. (2007) Early mobilization in a removablecast compared with immobilization in a cast after operative treatment of ankle fractures: a prospectiverandomized study. Foot Ankle Int. 28: 13–19. 952667 [pii]; doi: 10.3113/FAI.2007.0003 PMID:17257532
46. Wetzler M, Whitelaw G, Lee P (1991) The post-operative management of ankle fractures with pneumat-ic braces versus short leg cast. Orthop Trans, Abstract only. 15: 719.
47. Lin CW, Donkers NA, Refshauge KM, Beckenkamp PR, Khera K, et al. (2012) Rehabilitation for anklefractures in adults. Cochrane Database Syst Rev. 11: CD005595. doi: 10.1002/14651858.CD005595.pub3 PMID: 23152232
48. JacobsWC, Kruyt MC, Verbout AJ, Oner FC (2012) Effect of methodological quality measures in spinalsurgery research: a metaepidemiological study. Spine J. 12: 339–348. S1529-9430(12)00082-4 [pii];doi: 10.1016/j.spinee.2012.01.015 PMID: 22381574
49. Antonopoulos CN, Kakisis JD, Sergentanis TN, Liapis CD (2011) Eversion versus conventional carotidendarterectomy: a meta-analysis of randomised and non-randomised studies. Eur J Vasc EndovascSurg. 42: 751–765. S1078–5884(11)00531–4 [pii]; doi: 10.1016/j.ejvs.2011.08.012 PMID: 21903425
50. JacobsWC, Kruyt MC, Verbout AJ, Oner FC (2012) Spine surgery research: on and beyond currentstrategies. Spine J. 12: 706–713. S1529-9430(12)00986-2 [pii]; doi: 10.1016/j.spinee.2012.08.424PMID: 23021034
51. Toivanen JAK (2003) (ii) The management of closed tibial shaft fractures. Current Orthopaedics. 17:167–175.
52. Nilsson GM, Eneroth M, Ekdahl CS (2013) The Swedish version of OMAS is a reliable and valid out-come measure for patients with ankle fractures. BMCMusculoskelet Disord. 14: 109. 1471-2474-14-109 [pii]; doi: 10.1186/1471-2474-14-109 PMID: 23522388
The Postoperative Care of Ankle Fractures
PLOS ONE | DOI:10.1371/journal.pone.0118320 February 19, 2015 12 / 12
“This course was developed and edited from the document: Effects of a Training Program after
Surgically Treated Ankle Fracture: A Prospective Randomized Controlled Trial - Gertrud M Nilsson et al.
BMC Musculoskeletal Disorders 2009, 10:118 doi:10.1186/1471-2474-10-118Eneroth, used under the
Creative Commons Attribution License."
“This course was developed and edited from the document: Weight-Bearing and Mobilization in
the Postoperative Care of Ankle Fractures: A Systematic Review and Meta-Analysis of Randomized
Controlled Trials and Cohort Studies – Smeeing DPJ, Houwert RM, Briet JP, Kelder JC, Segers MJM,
Verleisdonk EJMM, et al. (2015) PLoS ONE 10(2):e0118320. doi:10.1371/journal.pone.0118320, used under
the Creative Commons Attribution License."