annex 3: common challenge & functional specifications · annex 3: common challenge &...
TRANSCRIPT

Annex 3: Common Challenge & Functional Specifications European Commission Horizon 2020 Pre-commercial Procurement: Project number 727534 www.nightingale-h2020.eu Five Academic Hospitals seek innovative partners to deliver cutting edge health care solutions for wireless monitoring and identification of high-risk patients, both in hospital and at home.
Executive Summary
Clinical need Patients die because signs of deterioration are missed. There is a huge unfulfilled need for better monitoring of vital signs and other data to identify high-risk patients who are on general hospital wards or at home. Patient deterioration is often overlooked or not detected at all. One of the reasons is the intensity in nursing and frequency of vital signs monitoring which decreases from the Intensive Care via ward towards home. Early detection of physiological instability is crucial to prevent death and disability. Pre-commercial Procurement (PCP) Five leading European academic hospitals (Utrecht, the Netherlands; Stockholm, Sweden; London, United Kingdom; Leuven, Belgium and Aachen, Germany) uses the European commission’s Pre-commercial Procurement (PCP) funding scheme to challenge and stimulate European industry to develop a system to connect patients and carers to wirelessly monitor patients’ vital signs and identify high risk individuals. The available budget for the development of this innovative solution is 5.3 million euro, consisting of 3.75 million euro in the form of innovation subsidies to the industry. Finding a solution The solution should consist of one or more unobtrusive wireless sensors that do not interfere with the patient’s daily activities or rehabilitation. Intelligent analysis software is a key feature of the requested system, as the false alarm rate must be extremely low to be acceptable to the users. It should be well-integrated into the hospital’s electronic medical record system. The sensors should involve a mechanism that allows patients and informal carers to communicate with their healthcare team, and allow entry of qualitative data (e.g., pain and well-being scores). Vital signs such as respiratory rate, pulse, blood pressure and level of consciousness are key predictors of deterioration 1., 2., but prediction will be much enhanced with analysis of various data from the medical record. This includes demographic data such as patient age and also biochemistry and haematology data, e.g., serum creatinine (as an indicator of acute kidney injury); urea, white blood cell count, etc1. Patient inputs are critical for several reasons, not least because respiration, blood pressure and consciousness are probably the three most important parameters 2. - and standard monitoring devices cannot measure
1

consciousness. However, patients’ response(s) to questions or instructions can tell us how their brain is working - and also allow patients to say if they are thirsty (perhaps dehydrated), light-headed or faint (altered neurological or cardiovascular function), nauseous (neurological or gastrointestinal dysfunction), in pain, or simply “feeling well”/”not well”. We expect that successful implementation of such a system will empower patients and carers. It will have the potential to transform healthcare by reducing death and disability from undetected deterioration, and can provide a ‘safety net’ to high-risk patients after discharge home. We invite industry to solve this huge unfilled need for better patient monitoring!
2
Nightingale - Connecting Patients and Carers using wireless technology:
The Common Challenge
The Clinical Need
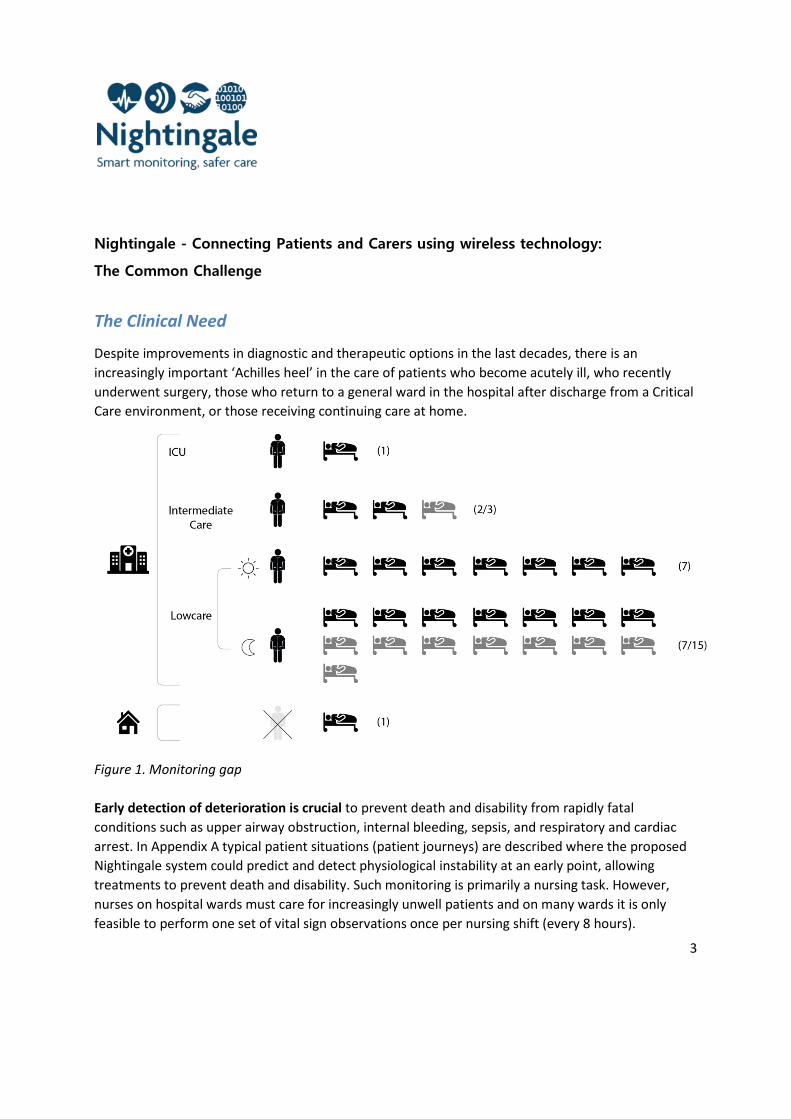
Despite improvements in diagnostic and therapeutic options in the last decades, there is an increasingly important ‘Achilles heel’ in the care of patients who become acutely ill, who recently underwent surgery, those who return to a general ward in the hospital after discharge from a Critical Care environment, or those receiving continuing care at home.
Figure 1. Monitoring gap Early detection of deterioration is crucial to prevent death and disability from rapidly fatal conditions such as upper airway obstruction, internal bleeding, sepsis, and respiratory and cardiac arrest. In Appendix A typical patient situations (patient journeys) are described where the proposed Nightingale system could predict and detect physiological instability at an early point, allowing treatments to prevent death and disability. Such monitoring is primarily a nursing task. However, nurses on hospital wards must care for increasingly unwell patients and on many wards it is only feasible to perform one set of vital sign observations once per nursing shift (every 8 hours).
3

Increasing the intensity of patient observation and vital sign monitoring by more frequent nurse rounds is severely limited by the availability of sufficient numbers of trained nurses and budget constraints. Once discharged home, patients’ vital signs are no longer monitored at all. While this may seem acceptable for patients who are stable and nearly completely recovered from their illness, the reality today is different in many cases. A sizeable proportion of mortality occurs in the first week after discharge; on the other hand, patients are now discharged home earlier than ever before. Note that while enhanced early recovery after surgery is associated with better outcomes, early discharge also means that some major complications will become first manifested in the home setting. A system that connects the high-risk patient at home with the healthcare team, and generates alerts when vital signs deteriorate will allow early recognition of any problems and early treatment, with rapid rehospitalisation where needed. Objective and Key Performance Indicators of the Nightingale solution The objective of Nightingale is: ‘prediction and detection of physiological instability to prevent death and disability, by wearable smart monitoring leading to safer care’. In the end, after successful (commercial) implementation in the healthcare market, Nightingale’s long term performance can be described in the following ‘performance indicators’:
● Safe reduction of Length of Stay (LOS) in the hospital ● Reduced number of avoidable re-admissions to Intensive Care Unit (ICU) ● Faster re-admission to ICU for patients who do need escalation of care ● Reduction of mortality ● Reduction of additional costs of care
To assess the performance of Nightingale systems clinical trials are needed with large patient populations. In the short term, during the research & development phase of Nightingale, system performance can be described in the following ‘performance indicators’:
● Ease of use and acceptance by the users; both the patient as the nurses ● Technical validity of both hardware and software components
Scope The Nightingale solution should be supportive both in the hospital and in the home setting. For in-hospital use we are currently focussing on high risk patients admitted for both serious medical problems and for surgery. For the home setting, we expect Nightingale solutions to be of added value for post-surgery patients and patients sent home after emergency room visits for acute medical problems (who would otherwise need to be admitted ‘for observation’). Nightingale may be used to monitor patients in three different situations:
1. to highlight and communicate information about high risk patients, based on analysis of both acute
4

physiology (primarily vital signs and blood profile) and factors related to age, chronic disease, frailty, functional status); and to ensure that they are monitored when subject to acute insults or any procedures.
2. to allow early detection of physiological deterioration, which then allows early treatment and improved outcomes. In some situations monitoring and rapid treatment will prevent re-admission to the ICU, while in others necessary (re)admission to the ICU will not be delayed by late recognition of deterioration.
3. to provide assurance about patient status and continuing recovery when discharged from higher levels of care in the hospital (e.g., from the ICU or operating theatre recovery area to the ward; or, in some cases, from the Emergency Department to home).
Figure 2. Hospital and home application Market search (as of November 15th 2016) The consortium partners have performed an extensive search to discover possible solutions that are currently available. We identified several ‘wearable’ devices that are designed to measure one or more vital signs and transmit these data wirelessly to another device such as a smartphone or network-attached ‘bridge’ (and from there to a server and the patient record). Currently the majority of wearable sensor devices appear to be geared towards lifestyle and sports. We identified only a handful of companies that produce a ‘medical grade’ wearable sensor that can measure and wirelessly transmit vital signs such as heart rate, respiratory rate and temperature. None of these companies currently has a user front end for the care giver that intelligently interprets the various signals to avoid repeated triggering of false alarms. Most systems that present data on a central terminal use traditional user-selectable alarm ‘threshold’ functionality. None of the currently available systems is sufficiently developed to allow remote monitoring of patients’ vital signs in the home situation. Moreover, there is also a need to add in information from the medical record and from patient inputs as described above; i.e., demographic data, laboratory data, patient responses to questions or instructions.
5

Nightingale - Connecting Patients and Carers using wireless technology:
The Common Challenge
The Business Case
The business case for our requested solution is very strong. Avoidable adverse events (including death) are extremely costly; for example, most major surgical complications result in excessive Length of Stay and added costs for additional drugs and interventions (total cost up to more than twice the cost of admission without complications). For example, it is estimated that if the number of [cases of] sepsis were reduced by 10%, 20% or 30% …the potential annual cost savings to the UK NHS would be £148 million, £296 million or £444 million respectively3.. Moreover, patients with complications have a higher likelihood of being readmitted to hospital after discharge home. For hospitals and third-party payers, unplanned readmissions are an increasing cause for concern. Even complications that cannot be avoided by improved patient monitoring will benefit from rapid recognition and timely treatment. The partners have initiated formal Health Technology Assessment (HTA) studies to help define the business case and cost effectiveness ratio of the envisioned solution.
An example: If Nightingale is able to reduce:
● Length of Stay with 5% (assumed costs of one day extra LoS is €600) ● Mortality by 5% (relative risk reduction) and assumed societal cost of one avoidable death is
€200.000) ● Readmission rate by 5% (assumed costs of readmission is €6.000)
The potential savings in healthcare are calculated at €7,3 million per year per hospital with a capacity of 30.000 patients per year, based on the mentioned assumptions. This is based on the following rationale: - If we assume that with using Nightingale the average Length of Stay can be reduced by 5% from an average of 6.1 days of stay per patient and assuming a hospital with 30.000 clinical admissions per year, this results in potential annual cost savings of €5,5 million. - If we assume that the absolute number of avoidable deaths (hospital mortality rate of 2% with a potentially avoidable fraction of 4%) can be reduced with 0.25 by applying monitoring on vital signs
6

and detecting early deterioration and assuming a hospital has 30.000 patients a year this results in potential avoided costs of death of €1,2 million per year. - If we assume a modest reduction of the readmission rate by 5% (from a current readmission rate of 6.2% to 5.9%) this results in potential cost savings of €560.000 per year. In these potential cost savings we have not taken into account the costs of applying the Nightingale solution. Assuming a cost level of €100 per patient, the net potential savings are €4,3 million per year for this type of hospital (30.000 patients per year). Assuming a purchase price of €50 per patient, the net potential savings are €5,8 million per year; while at a € 200 price point the savings would be €1,3 million per year.
7

Nightingale - Connecting Patients and Carers using wireless technology:
The Common Challenge
Nightingale minimum technical requirements
As mentioned in the PCP Request for Tenders document (section 4.5), there are a few minimum technical requirements for the Nightingale solution, shown below:
Nightingale system
Final solution must be at least a sophistication level 3 system (Details in common challenge document)
Final solution must be compliant with all applicable law & standards of the participating buyer hospitals for use in a clinical environment
Final solution must correspond to at least Technology Readiness Level1 7 at the end of Phase 3
Sensing system
The final sensor(s) must be able to perform continuous monitoring for at least 5 days
The final sensor(s) must measure at least the following parameters:
1. Heart rate
2. respiratory rate
3. temperature
4. motion and 3 axis position
Data Transmission
Data transmission of the final solution must be compliant with the HL7 standard
Data transmission of the final solution must be compliant with the Fast Healthcare Interoperability Resources (FHIR) standard
All sensors and integrated wireless signal transmission systems must be compliant with all applicable (National and European) safety regulations
(Wireless) data transmission must be encrypted
Please be aware that proposals for solutions that do not meet these requirement will be excluded. All solutions that meet these minimum requirements will be evaluated for awarding to Phase 1. This evaluation will be done by assessing the award criteria as described in the PCP Request for Tenders document (section 4.6). The main basis for the awarding criteria are the functional specifications as described in the pages below. These functional specifications in the pages below are not minimum requirements, but the better a solution meets these specifications, the higher the score per criterion will be.
1 https://en.wikipedia.org/wiki/Technology_readiness_level 8

The Functional specifications for a system to wirelessly connect patients, carers and the healthcare team The Nightingale system is used by healthcare workers, patients, and informal caregivers. In the low care ward the Nightingale system notifies healthcare workers in case of deterioration of the patient’s condition when deterioration (or increased deterioration risk) is detected from the monitored patient’s vital signs, patient-entered subjective data and updates in the patient’s medical record and lab result data. In the home environment the informal caregiver can also receive a notification if applicable. Additionally, the Nightingale system provides a means of communication between healthcare workers, patients, and informal caregivers.
Figure 3. The Nightingale system and its users both in hospital and home application
9

The system will consist of five building blocks, creating all together the solution for safe patient monitoring. Per building block the different functional specs that Nightingale is aiming for are described. Also the link to the specific award criteria is shown.
Figure 4. Functional components of Nightingale (building blocks) The Nightingale solution should consist of a few simple sensors (and preferably one), referred to as the Nightingale sensor, and an Intelligent information analysis information system. The wireless Nightingale sensor continuously monitors vital signs without interfering with the patient’s daily activities or mobilization/rehabilitation. The Nightingale system notifies healthcare workers of the deterioration of patient’s conditions in case deterioration (or increased deterioration risk) is detected from the monitored patient’s vital signs, patient-entered subjective data, patient demographic data and updates in the patient’s medical record and lab result data.
10

Figure 5. The Nightingale solution consists of a sensor and an intelligent information analysis information system Sensing system (linked to award criteria I1.1 & Q4.1)
● The ideal multi-parameter sensor is small, light-weight and can be worn on an area of the body without the patient being aware of its presence
● The sensor can be continuously used for uninterrupted vital signs monitoring for at least 5 days Please note: for practical reasons, we define ‘continuous’ here as: at least one full set of vital signs measurements every 2 min; In the home setting this update rate may be reduced.
o this requires that it either uses very little battery power for its sensing functions and data transmission, or:
11

o that it can extract its required energy from the patient ● robustness: the sensor can withstand a daily shower. Preferably the sensor can also remain attached
during imaging studies (with MRI studies as a possible unavoidable exception) ● A sensor that can measure oxygen saturation is highly desirable
o the consortium partners are aware of the fairly high energy requirements of the current generation pulse oximeters
o Intermittent readings of oxygen saturation to preserve battery life (at fixed intervals or triggered by abnormalities in any continuous parameter) might be acceptable
● A sensor that gives an approximation of the patient’s current global hemodynamic status, in particular, blood pressure or pulse pressure, is highly desirable. This does not need to be a conventional arm or finger cuff-based ‘exact’ blood pressure measurement, but must be able to reliably track changes over time in perfusion pressure.
● A sensor system that appraises the consciousness level of the patient is highly desirable (e.g. evidence of spontaneous, appropriate movements or responses to verbal or tactile stimuli).
● Other sensors measuring stress, distress, relevant blood parameters (lactate, pH, other) are potentially very valuable.
● Sustainability of the sensor (for example: is it designed for reuse?) Current experiences with vital signs monitoring and minimal accuracy levels The minimal accuracy levels of vital sign measurements are described in table 1, however emphasizing that accuracy of trend measurements (ability to detect deterioration over time) is far more important than just an accurate single measurement at one specific point in time. In addition, experiences with current wireless sensors for vital sign monitoring within patients and the consequences regarding false positive alarms are further explored in more detail. The solution should be capable of recognizing vital instability and as such, able to measure vital sign trends accurately and reliable. In the subsequent table we have tried to set minimal requirements for measuring different vital signs. In terms of accuracy of vital sign measurements, there are two aspects which need elaboration first:
1. Ideally, we want to measure every vital sign accurately, but this is not in every situation as important. Normal rates of for example respiratory rate vary between 10 to 20 breaths per minute. However, the challenge lies in the abnormal range. Measuring both high (>21/min) and lower respiratory rates (0-10 breaths per minute) is far more important, as in those regions small measurement deviations may have implications for treatment (e.g. reversal of opioids in case of bradypnea).
2. Secondly, it is even more important to pick up vital sign trends over time rather than the ability to accurately measure a single parameter at one point in time only. For example, detecting a decreasing respiratory rate over time (e.g. a slowly changing RR starting at 10 brpm to 4 brpm) could be an important indicator of vital instability. Likewise a slowly changing trend pattern of RR measurements from 18 to 10 brpm which is still within the normal range is important to detect. Table 1: minimal accuracy levels of vital signs
Parameter Range Minimal accuracy Remarks
12

Heart Rate 30 - 200 beats per minute (bpm)
≤5 or 10% bpm, whichever is greater
Heart Rate Variability (variation in time interval between heartbeats) is a very interesting parameter to measure as well
Respiration Rate
0 - 40 breaths per minute (brpm)
≤5 brpm See remarks below
Temperature 35 °C - 41 °C ≤ 0.3 between 36.0 and 39.0 °C
Cut-offs for hypothermia, normal, fever, (or hyperyrexia) could be used as well?
Oxygen saturation
70 - 100 % ≤ 3%
A sensor that can measure oxygen saturation is highly desirable. We are aware of the fairly high energy requirements of the current generation pulse oximeters. Intermittent readings to preserve battery life (at fixed intervals or triggered by abnormalities) might be acceptable.* See remarks below
Blood pressure
Systolic: 80-220 mmHg. Diastolic: 40-100 mmHg
≤ 15 mmHg
A sensor that gives an approximation of the patient’s current global hemodynamic status, in particular blood pressure or pulse pressure is highly desirable. This does not need to be a conventional arm or finger cuff-based ‘exact’ blood pressure measurement, but must be able to reliably track changes over time in perfusion pressure*
Activity rate / motion
TBD (gravity/second)
The consortium partners suggest active monitoring of patient motion. Not only will this greatly facilitate flagging of motion artefacts, we also believe that motion itself (or lack thereof) might prove to be an important vital sign that is worthy of tracking alongside the more traditional vital signs *
Posture detection
TBD >70% accuracy compared to visual
Lying down, upright, walking (or running).
Remarks Respiration rate
• We have experienced that the current medical-grade wireless sensors for continuous respiratory rate monitoring do not measure respiration rates lower than 4 brpm, either because it is technically too difficult, or due to other safety issues and/ or liability restrictions. However, we want to be able to detect life threatening conditions, such as apnea (cessation of respiratory air flow due to a morphine overdose for example), which is probably preceded by severe bradypnea (RR < 9 brpm). If a sensor may somehow not be able to measure RR < 4, a slowly changing RR pattern starting at 10 to 4 brpm for example, could still be identified and used as important indicator of vital instability. In addition, the activity level of a patient with apnea is probably (almost) zero. See also aspect nr 2 as mentioned above.
• It is technically more difficult to accurately measure respiration continuously, especially during spontaneous breathing in patients who are moving and talking. However, movement detection by an accelerometer not only provides additional information about the patient’s activity level, but can also distinguish between physiological abnormalities and movement artefacts. An elevated heart rate while a patient is very active will be interpreted differently compared to a rapidly increasing heart rate while the activity level is almost zero. Also, artifacts casued by active moving patients may imply
13

that the patient is alive and breathing, which makes the chance of an apnea very unlikely. Using all this information ‘smart’ could be helpful to reduce the number of false alarms. Remarks oxygen saturation
• We have experienced that measuring continuously measuring saturation levels with a wired pulse oximeter doesn’t always detect the level of saturation accurately when patients are moving their fingers intensively. Distinguishing these technical artefacts from actual (accurate) saturations levels during rest may be helpful to reduce the number of false alarms. Data transmission protocol and interference rejection (linked to award criteria I1.2 & Q4.2)
● the consortium expects safe and reliable data transmission with a minimum of dropouts, but does not wish to prescribe any specific protocols for data transmission
o the transmission protocol can therefore be either an industry standard (e.g., WiFi, Bluetooth LE, etc.) or a proprietary protocol
o however, ‘open standards’ are highly desirable from an interoperability perspective o any sensor and integrated wireless signal transmission system must be compliant with all applicable
safety regulations, both regarding patient harm (electrical safety, EM radiation) and potentially unsafe RF interference causing malfunction of other medical devices
● Data transmission needs to be compliant with HL7/Fast Healthcare Interoperability Resources (FHIR) international standards for transfer of clinical data (https://www.hl7.org/fhir/summary.html).
● The sensor (whether or not via a relay device) is able to cover an entire home; e.g., the sensor worn by the patient can transmit from any room in the patient’s home without the necessity to be in close vicinity of a relay device.
● Wireless data security requires the use of robust encryption, in particular while wireless vital signs data are in transit
● patient acceptance of the system will be highly dependent on the convenience of using the entire system.
o for example: a system using a number of fixed ‘wired’ receivers (bridges) in many rooms to connect the patient to the health care worker over the network will have dead zones in some areas of the hospital.
o using such a system for home monitoring means that the patient effectively has ‘house arrest’. ● when there are two wireless transmission protocols active at the same time to sequentially and
wirelessly relay the vital signs data streams (first from sensor to mobile device and then from mobile device to a hospital server), this might theoretically increase the likelihood of data loss caused by electromagnetic interference or other network issues. Artefact rejection system (linked to award criteria I1.3 & Q4.3)
● a high quality artefact rejection system is necessary to prevent false alarms, ‘alarm fatigue’ in caregivers (from the need to check the patient repeatedly on spurious readings) and unnecessary anxiety in patients
● many artefacts in vital signs monitoring are caused by motion artefact. In contrast to anaesthetised patients and patients on intensive care units, most patients in the targeted groups are mobile and
14

may be actively exercising several times a day. ● The consortium partners suggest active monitoring of patient motion. Not only will this greatly
facilitate flagging of motion artefacts, we also believe that in the future motion itself (or lack thereof) might prove to be an important vital sign that is worthy of tracking alongside the more traditional vital signs Analysis system (linked to award criteria I1.4 & Q4.4) A sophisticated analysis and alarm generation system is paramount. Unlike operating rooms and intensive care units where ‘one on one’ nursing is the rule, on general hospital wards many patients will be simultaneously monitored. In case of abnormal signals, the nurse can immediately check the patient to see if there is any real deterioration of vital status or that the alarm was caused by technical problems with the sensor or data transmission. In contrast, when telemonitoring is applied in the home care situation there is no easy way to perform such ‘cross-checks’ for sensor dislodgment, strange movements, etc. Therefore we request that the solution design contains:
• intelligent analysis of the incoming vital signs data streams • analysis of trends and rates of change • pattern analysis in multiple simultaneous data streams • generation of probabilistic alarms
The consortium partners realize that this might require the use of machine learning and artificial intelligence. There are several possible levels of sophistication with clinical decision support based on such intelligent alarms (see below). Usability (linked to award criteria I1.5 & Q4.5) The usability of Nightingale will be assessed based on the following functional specifications:
• The sensor is small, extremely lightweight, easy to clean/disinfect (waterproof). • The sensor device can be worn on an area of the body without the patient being aware of its
presence. • The sensor is externally placed, not damaging/pulling the skin and biocompatible. • The sensor cannot interfere the patient while sleeping. • The sensor will stay correctly in place in case of sweating. • The sensor ideally can withstand a daily shower. Preferably the sensor can also remain
attached during imaging studies (with MRI studies as a possible unavoidable exception) • The sensor must have characteristics such that the application of the sensor (properly
connecting it to the body of the patient) and its operation is learnable by medical professionals (hospital situation) and is learnable by an instructed patient or instructed informal caregiver home situation).
• The system must indicate to the user whether the sensor is properly applied. • The sensor must identifiably be part of the Nightingale system and clearly distinguishable
15

from other non-Nightingale devices, sensors or instruments applied to the patient. • The sensor must comply to all applicable safety standards. • The user interface shall be easy to use, intuitive and human-centered. • The system has the option to display ‘actionable’ recommendations. • The system can signal and deliver the notification to the user by different modalities (eg.
visually, aurally, by vibration) of its user’s choice.
Note that solution designers should carefully balance security and usability. The system must be usable for patients with limited e-health literacy (for example, frail elderly still living independently at home). Demanding password protection means that some device in the system needs a (virtual) keyboard to enter passwords. However entering passwords on a disposable sensor will not make sense. Password or biometric security should not be a problem for caregiver notification devices. Value Sensitive Design The use of the Nightingale solution is influenced by the needs and competencies of the (end-) users. Lack of understanding of human factors is key to failure of innovation. Stakeholders such as patients, informal carers, nurses and physicians have a direct relation with the solution, but also indirect stakeholders as industry, engineers, and insurers are related to the solution. By identifying these stakeholders we are able to translate values into benefits and risks during the design process. The insights of the various stakeholders will support different design choices in different phases of development. As a methodological feature, Nightingale will involve (end-)users in the design process by using a ‘value sensitive design’ (VSD) approach. The approach involves investigation of patient values and concerns, as well as those of caregivers and informal carers throughout the development. We will elicit these values and concerns via focus group sessions with patients, informal carers and health care workers. Patients who have participated in the validation studies will be explicitly asked for their attitudes, values, concerns and experiences with the test system. The following (main) values are distinguished and are key for the system development and the solution. During the different phase we will test how the solution meets the requirements ao with help of the values as mentioned below :
• Health • Trust • Accessibility • Reliability • Autonomy
See Appendix C for a detailed description of the Nightingale values per stakeholder, comparing benefits and risks per subcategory.
16

Nightingale - Connecting Patients and Carers using wireless technology:
The Common Challenge
Levels of sophistication with clinical decision support based on intelligent alarms
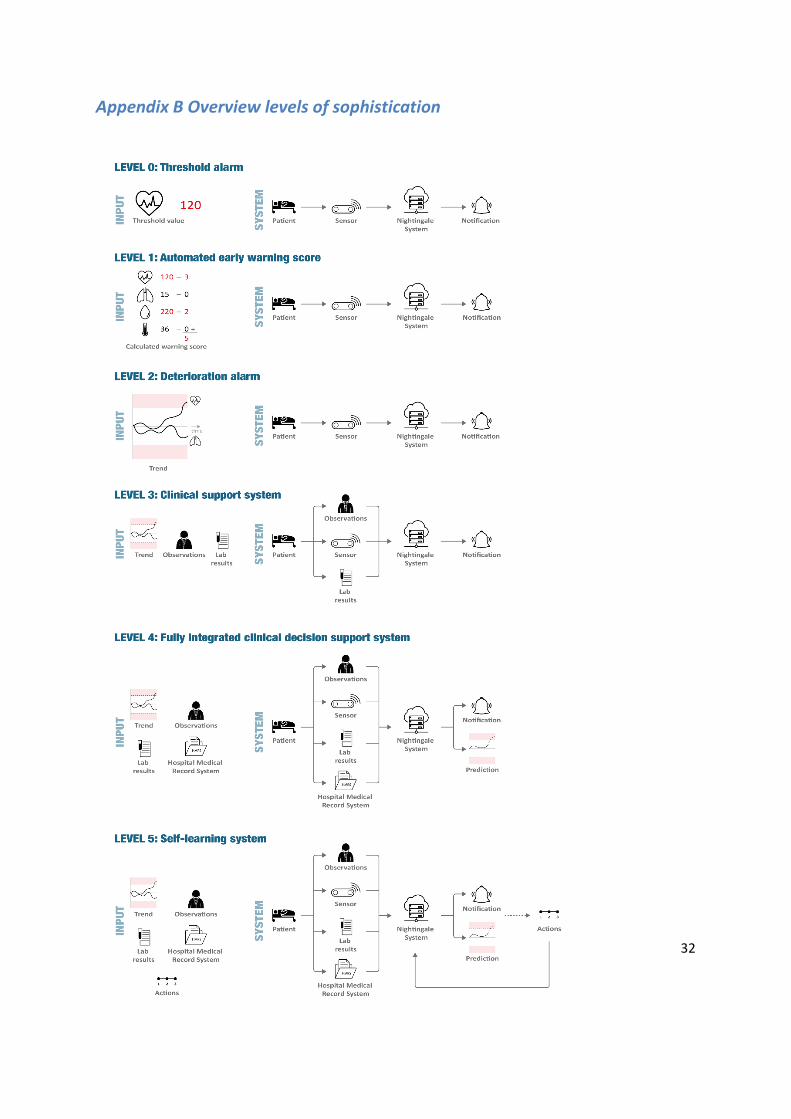
Different levels of sophistication can be distinguished. Starting with the early warning systems as we have today ending with a level based on artificial intelligence that is self-learning and self-optimizing. Nightingale is aiming for the best solution possible, with at least level 3.
Figure 5. Levels of sophistication
17

Level 0: Threshold alarm No artificial intelligence, simple threshold alarms only (the user must set the lower limit and the upper limit for each measured variable). For example: <alarm> IF (heart rate > 100/min OR heart rate < 40/min). A slightly more sophisticated alternative simple alarm scenario: < ‘orange’ alarm> IF (heart rate > 90/min OR heart rate < 50/min); <‘red’ alarm> IF (heart rate > 110/min OR heart rate < 40/min). Or a ‘no data’ alert, when the patient moves to far from a relay device. Such systems may also attempt to avoid triggering of false alarms by applying median filtering (or some other method of averaging the signal over longer periods of time) to remove brief movement-induced artefact transients or by simply delaying the alarm for a predefined time period, as currently used in some monitor systems.
Level 1: Automated early warning score As described above for ‘level 0’, but with simple integration of multiple data sources: for example an ‘automated early warning score’. Early warning scores (EWS) are simple sum scores calculated by adding points for each vital sign that is ‘out of range’. For example: the National EWS (NEWS, United Kingdom)
18

Figure 3 Example of physiological parameters
Level 2: Deterioration alarm An advanced system to track vital signs that does not only track changes in single parameters, but also considers the relationship between changes in various vital signs. For example, a combination of progressive tachycardia (high heart rate, increasing over time), progressive tachypnea (high respiratory rate, increasing over time) combined with fever, suggests early sepsis which may necessitate measurement of blood lactate and intensive care expert consultation. Alternatively: a pattern of reduced motion, decreasing respiratory rate followed by progressive hypoxemia (low blood oxygen saturation) in a patient who recently had surgery and is receiving opioid pain medication suggests the possibility of opioid overdose. The latter constellation requires the nurse to check on the patient immediately and discuss the need for an opioid antagonist such a naloxone with the attending doctor.
19

Level 3: Clinical Decision Support system – minimum requirement for the Nightingale solution! A clinical decision support system that incorporates more than only the intelligent analysis of vital signs data. Such a system may also take existing or new abnormal laboratory results into account, e.g., a new observation of hyperkalaemia (high blood potassium level), or an increase in blood creatinine (an indicator of acute kidney injury) that becomes available in the laboratory tab of the EMR). A level 3 system may also take environmental information and important diagnostic information into account, including structured nursing observations such as restlessness, sleepiness/sedation, dyspnea, sweating, etc. In the home setting, such information can be entered directly by the patient or informal carer.
Level 4: fully-integrated hospital-wide clinical decision support system A fully-integrated hospital-wide clinical decision support system that monitors the patient’s status in real-time and constantly updates the risk of death and severe complications each time a new data element becomes available. It may be even optimized to detect several specific rare but lethal conditions. For example, a life-threatening disturbance of ventricular rhythm (‘torsade des pointes’ caused by ‘long QT-syndrome’ – please see use case ‘Henrik’) as a result of inadvertent drug-drug interactions. Such a highly sophisticated system takes as its inputs clinical data (current diagnoses, recent procedures, prior history, structured nurse observations (including a sense of ‘worry’ regarding the condition of the patient), doctors observations and clinical notes, data entered by the patient or informal carer, on-line continuous vital signs data, laboratory data, new imaging results, and updates its predictions every time a new data element reaches the system.
20

Level 5: Self-learning system an artificial intelligence integrated self-optimising system. The most obvious application of artificial intelligence in healthcare is data management. Nightingale is collecting many data, storing it, normalizing it, tracing its lineage – it is the first step in revolutionizing the existing healthcare system. With artificial integrated in Nightingale it should be possible to optimise the dedicated patient specific decision support.
The consortium partners require a solution with at least ‘level 3’ sophistication. In appendix B of this common challenge an overview of the levels of sophistication can be found.
21

Nightingale - Connecting Patients and Carers using wireless technology:
The Common Challenge
A brief introduction to Pre-commercial Procurement (PCP)
Several years ago the European Commission designed a new scheme / demand-side instrument called ‘Pre-Commercial Procurement’ that enables the public sector to stimulate European Innovation by engaging with innovative businesses and other interested parties to deliver cutting-edge, innovative solutions , , in situations where there is currently no existing solution in the market. The European Commission funded Nightingale project is an implementation of Pre-Commercial Procurement (PCP). Rather than directly subsidizing European industry, the prospective users of the new technology assist in guiding the development process using a ‘funnel-shaped’ procurement model, which entails the use of competitive development in phases (as several technology vendors will be selected to enter the first phase of the PCP), risk-benefit sharing under market conditions, and a clear separation between the procurement of R&D services and the potential public procurements of innovative solutions focusing on deployment of commercial volumes of end-products (Public Procurement of Innovative Solutions - PPI). This innovative process presents an opportunity for suppliers to develop new solutions and to introduce new, beyond state-of-the-art technologies and products, in direct cooperation with the healthcare institutes and their employees. The PCP process is exempted from the EU procurement directives, is flexible and allows an early dialogue between potential suppliers and the healthcare institutes in order to optimize the solution. The aforementioned exclusion from the application of the European public procurement framework is also justified by the fact that the procurer does not reserve all the benefits of the R&D exclusively for himself. Accordingly, Intellectual Property Rights (IPR) of the developed solution will be shared between the Nightingale procurers and the supplier in the sense that each R&D provider participating in the PCP retains the ownership of the IPRs it generates in the PCP, provided the Nightingale procurers receive a ‘free use’ license in return, as well as a right to license or to request the R&D provider to license the IPR to third parties on non-exclusive, fair and reasonable market-based terms and conditions. The development work will be co-financed by Nightingale project funding, within the Horizon 2020 programme of the European Union. The PCP process will start with an extensive preparation phase (‘Phase zero’; below leftmost panel) and is followed by three development phases, as visualized below:
22

*This is an example of the PCP process. In Nightingale PCP, we will select a minimum of 8 suppliers for phase 1, 4 suppliers for phase 2, and 2 suppliers for phase 3. Phase 0 - The preparation of the Nightingale PCP started with the publication of a Public Information Notice (PIN) and then entered an Open Market Consultation, which consisted of the following sequential components: I) Market Sounding, II) Market Sounding Review, and III) Market Consultation. In the Market Sounding, through different channels, the Nightingale procurers widely announced the project and raised the interest of possible developers/suppliers. All interested companies in the EU have been invited to fill in an online questionnaire that is aimed to help the procurers gain more insight into the market and the scope. In the Market Sounding Review, a summary/conclusion of the questionnaires has been made. In the Market Consultation, the Nightingale procurers invited all those interested companies for a face to face workshop & dialogue, with the aim of further explain the Nightingale and obtain more insight in the feasibility and technical developments & possibilities. Partly based on the results of this Market Consultation, the Nightingale procurers further fine-tuned the scope and criteria that are used in the PCP. The Market Consultation is followed by this formal PCP Call for Tender. Interested companies (or consortia) are invited to submit their proposals on paper. These submitted proposals will be further evaluated according to the criteria and the selection guidelines described in the PCP Call for Tender. The Nightingale procurers aim to select the eight companies with the most promising proposals which will be invited to participate in the first phase Nightingale PCP process (Phase 1). A framework agreement and a Phase 1 contract between the Nightingale consortium and every individual company will be signed. The Nightingale PCP process will include three phases of solution development. In Phase 1, which will last 3 months, the selected companies (min. of 8) will each develop their proposal, including feasibility studies. The Nightingale consortium partners will evaluate the tenders with respect to their technical, economical and organizational viability. Four companies will be invited to proceed to the second phase, in which actual prototype systems will be developed and tested.
23

In Phase 2, two interim evaluations are foreseen to assist in continuously improving the prototypes under development. After critical evaluation of these early prototypes at the end of the second phase, two companies will be invited to develop and test a pre-production model within the hospitals during the last, third phase of the PCP process. Phase 3: in this phase the prototype system will be refined to a pre-production model. Three interim evaluations and feedback sessions are foreseen, based on field tests with actual patients and care givers using the system. During the entire PCP process, selection of companies/consortia to enter the next phase will be based on transparent and objective evaluation criteria. After this phased process, the PCP process ends.
Public Procurement of Innovation (PPI) In order to help the companies with such new highly innovative technology to overcome market inertia, the European Commission also facilitates the uptake of innovative solutions by the intended end-users. The EU can subsidize the purchase of large quantities of the new devices or solutions using the Public Procurement of Innovation (PPI) model. The Nightingale Consortium intends to conduct a PPI after the completion of the PCP if the PCP is successful (i.e., at least one ‘market-ready’ solution has been generated). For more information about PCP, please visit the EU website by clicking on the links below: https://ec.europa.eu/digital-single-market/en/innovation-procurement See also: https://ec.europa.eu/digital-single-market/en/news/frequently-asked-questions-about-pcp-and-ppi
24

References
1. Churpek MM, et al. Multicenter Comparison of Machine Learning Methods and Conventional
Regression for Predicting Clinical Deterioration on the Wards. Crit Care Med. 2016 ;44(2):368-74. doi: 10.1097/CCM.0000000000001571.
2. Singer M, et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3).
JAMA. 2016;315(8):801-10. doi: 10.1001/jama.2016.0287. 3. York Health Economics Consortium. The Cost of Sepsis Care in the UK. 17 February 2017 (downloaded
from http://sepsistrust.org/wp-content/uploads/2017/02/YHEC-Sepsis-Report-17.02.17-FINAL.pdf).
25

Appendix A Nightingale Patient journeys
Four patient journeys will be shown in this appendix. At this moment the Steering Committee is working on the final versions:
1. Just one loose stitch – at home situation
2. When a patient stops breathing – hospital situation
3. If everything starts failing – hospital situation
4. Deterioration can go slow – at home situation
5. It is all in the detail - hospital situation
26

27

28

29

30

31
Appendix B Overview levels of sophistication
32

Appendix C Value Sensitive Design – Stakeholder values
Table 1: Values and their interpretations for the Nightingale solution IN-HOSPITAL
Value Subcategory Benefit Risk Stakeholder (direct/indirect)
Health Patient safety
Timely detection of patient deterioration on the ward
Harm caused by the system: too many false positives (alarm fatigue)
Technical failure (sensing, transmission) Adverse reaction to (sensor) solution
Patient Nurse Physician Industry/engineer (indirect)
Optimal care Personalized care Additional information about the
patient’s condition and vital signs
New knowledge may generate questions that cannot be answered
Problems with availability of healthcare professionals to respond to alarms
Nurse Physician Patient
Health Related Quality of Life
Survival & freedom from disability as much as possible
Reduced risk to suffer from avoidable consequences of a severe complication
Earlier hospital discharge to own home (or low-care facility)
Potential burden of (sensor) solution Earlier hospital discharge to own home does
not fit the patient’s needs and expectations
Patient Informal carer
Trust Reassurance Assurance of response of caregivers in case of patient deterioration
Skipping patient rounds, longer periods without direct nurse-patient contact
Management may be tempted to reduce nurse staffing
Patient Informal carer Nurse
33

Technical failure (sensing, transmission)
Confidence Healthcare professional is confident to be able to monitor all patients
Availability of appropriate patient (trend) information
Skipping patient rounds New knowledge on trend information
(rather than single measurements) may impede decision making by healthcare professional
Nurse
Quality of Life Sense of trust and relaxation Potential burden for informal carer at home Earlier hospital discharge does not fit
patients’ needs and expectations
Patient Informal carer
Accessibility Usability Ease of use (Technical) support Personalised care
Technical failure (sensing, transmission) Problems with availability of trained
healthcare professionals to respond to alarms
Nurse Physician Patient
Availability Easy access to data of patient’s condition
Costs of solution Acceptance of insurance Not all patients will be equipped with
solution: risk of ‘missed patients’
Patient Nurse Insurer (indirect) Industry (indirect)
Reliability Accuracy Accurate vital sign measurements (scientific validity)
Ability to detect ‘trend’ changes Low number of false positives/false
negatives
Unacceptable number of false positive alarms
Alarm fatigue Interpretation of vital sign ‘trends’ remains
difficult
Physician Nurse Industry/engineer (indirect)
Technical functioning
Sustainability Continuous, real time information
Inadequate technical support Interference with other systems
Industry/engineer (indirect)
34

Remote control Nurse Physician
Autonomy Privacy More privacy in case of earlier discharge from hospital to home
Inadequate security: Patient identity information (with patient data) is being used elsewhere
Inadequate security/legal framework: patient data is being used for other (commercial) purposes
Industry/engineer (indirect) Patient
Responsibility More patient information to ensure more optimal conditions for responsible care
Potential burden of responsibility to healthcare professional
Unclear ‘overriding authority’ leads to safety issues
Problems with availability of trained healthcare professionals to respond to alarms
Nurse Physician
35

Table 2: Values and their interpretations for the Nightingale solution in the HOME situation
Value Subcategory Benefit Risk Stakeholder (direct/indirect)
Health Patient safety
Timely detection of patient deterioration at home
Alarm fatigue: having to react on a multitude of false positive alarms at home will make the system unfeasible to use and unacceptable to users
Unrecognized deterioration: solely interpreting vital signs without actively taking into account the patient’s or informal carer’s subjective complaints, appearance, etc.
Technical failure (sensing, transmission) Adverse reaction to (sensor) solution
Patient Nurse Physician Industry/engineer (indirect)
Optimal care Providing timely & tailored treatment New information about patient’s
condition and vital signs at home Patients who need to be readmitted
to the hospital are in a less serious state (due to early recognition of patient deterioration)
New knowledge may generate questions that cannot be answered
Problems with availability of healthcare professionals to timely respond to alarms remotely
Nurse Physician
Health related Quality of Life
Survival & freedom from disability as much as possible
Reduced risk to suffer from consequences of a severe complication
Potential burden of (sensor) solution when no caregiver is around directly
Potential burden to informal carer to feel the need to check their relative’s condition
Responsibility of home caregiver to respond
Patient Informal carer
36

Trust Reassurance Pleasant feeling that someone is looking over their shoulder to check their condition
Pleasant feeling to be able to communicate with the healthcare professional if the patient feels worried
Assurance of response of caregivers in case of patient deterioration at home
Not able to communicate with healthcare professional due to failure or unavailability of healthcare professional
Patient Informal carer Nurse
Confidence Healthcare professional is equipped with appropriate patient (trend) information
Healthcare professional is confident to be able to monitor patients, even when they’re at home
Skipping patient check-ups (remotely) Skipping communication with patient New knowledge on trend information
(rather than single measurements) may impede decision making by healthcare professional
Nurse Physician
Quality of Life Sense of trust and relaxation Technical failure (sensing, transmission) Potential burden for informal carer at home
Patient Informal carer
Accessibility Usability Ease of use Personalized care (Technical) support Allows bi-directional communication
Technical failure (sensing, transmission) Patients with low health literacy cannot cope
with solution at home Problems with availability of trained
healthcare professionals to respond to alarms remotely
Bi-directional communication forces structural availability of healthcare professional
Nurse Physician Patient
Availability Easy access to data of patient’s Costs of solution Patient
37

condition
Acceptance of insurance Not all patients will be equipped with
solution: risk of ‘missed patients’ Not all patients that may benefit from home
monitoring will be happy to participate
Nurse Insurer (indirect) Industry (indirect)
Reliability Accuracy Accurate vital sign measurements (scientific validity)
Ability to detect ‘trend’ changes Low number of false positives/false
negatives
High number of false positive alarms Alarm fatigue Interpretation of vital sign ‘trends’ remains
difficult
Physician Nurse Industry/engineer (indirect)
Technical functioning
Sustainability Continuous, real time information Remote control
Unseen patient deterioration due to absence of technical support remotely
Interference with other systems at home
Industry/engineer (indirect) Nurse, Physician
Autonomy Privacy Patient surveillance Restriction of freedom, feeling that someone is keeping an eye on you continuously
Transmitted patient identity information (with patient data) is being used elsewhere
Patient data is being used for other (commercial) purposes
Industry/engineer (indirect) Patient
Self-management
More patient empowerment Self-management skills increase
Difficult to estimate self-management skills of a patient remotely and to rely on this
Patient or informal carer will ‘judge’ their feeling on measurements they follow
Patient Informal carer Nurse
Responsibility More patient information ensure more optimal conditions for responsible care
Unclear ‘overriding authority’ leads to patient safety issues
Potential burden of responsibility
Nurse Physician
38