antiangiogenici e tev - reteoncologica.it · precedente controllo con aumento della componente...
TRANSCRIPT

ANTIANGIOGENICIe
TEV
Roberta Buosi
Torino, 10 novembre 2016
Caso Clinico
COMORBILITA'
Ipertensione arteriosa
FA persistente
Artrite reumatoide
Diabete mellito in terapia orale
Obesità
Maschio 74 anni
Ex fumatore : stop da 12 aa (in precedenza 20 sigarette die per 45 aa)
Anamnesi familiare : negativa

07/02/2014 TC del torace senza mdc: al segmento postero basale del
LIsx in sede subpleurica nodulo di 35 mm in aumento rispetto al
precedente controllo con aumento della componente centrale aerea.
20/02/2014 Agoaspirato lesione LIS
cellule neoplastiche da adenocarcinoma scarsamente differenziato
EGFR wild type, ALK non traslocato, BRaf: negativo
DIAGNOSI

02/04/2014 Ecocardiogramma: FE 65% ventricolo sx moderatamente
ipertrofico, di normali dimensioni e funzione sistolica conservata.
Diastole monofasica da FA.
17/04/2014 Tc cerebrale con mdc: negativa
10/04/2014 Biopsia omero dx
Istologico 14-I-04113: metastasi ossea di
carcinoma
21/03/2014 PET:
-neoformazione al LIS
iperaccumulo SUV max 15.16
- focale accumulo di FDG al
terzo prossimale della diafisi
omerale dx sospetta per
componente produttiva.
27/03/2014 Tc arto superiore: nella
midollare ossea del III prossimale
dell'omero una formazione solida, con
estensione trasversale di circa 2 cm e
cranio-caudale di 2 cm: Nel contesto
del tessuto adiposo tra deltoide e
periostio tessuto di analoghe
caratteristiche di 2,4 cm, con evidenza
di reazione periostale limitrofa.
STADIAZIONE

Scelta terapeutica
- Coaprovel 150 mg/12,5 mg 1 cpr ore 8
- Lanoxin 0,25 mg 1/2 compressa ore 16
- Cardicor 2,5 mg 1 cpr ore 8 + ore 20
- Metformina 500 mg 1 cpr pranzo + 1/2 compressa cena
- Di Base 30 gtt ogni giovedì
- Paracetamolo 500 mg 1 cpr ore 8 + ore 20
- Duphalac sciroppo 3 cucchiai al giorno
-Fentanyl Spray Nasale 1 puff in ogni narice (tot 200
mcg) se dolore ingravescente
-- Desametasone 4 mg in F100 tre volte al giorno
- Omeprazolo 1 fiala in F100 al giorno
- Clexane 4000 U x 2 volte/die sc
Anticoagulante orale

Percorso terapeutico
I linea secondo schema
Carboplatino AUC6 + Paclitaxel 175 mg/mq +
Bevacizumab 7.5 mg/kg g1 q21
Inizia a maggio e termina nel settembre 2014
Luglio 2014 TC di restaging dopo 3 cicli
SD
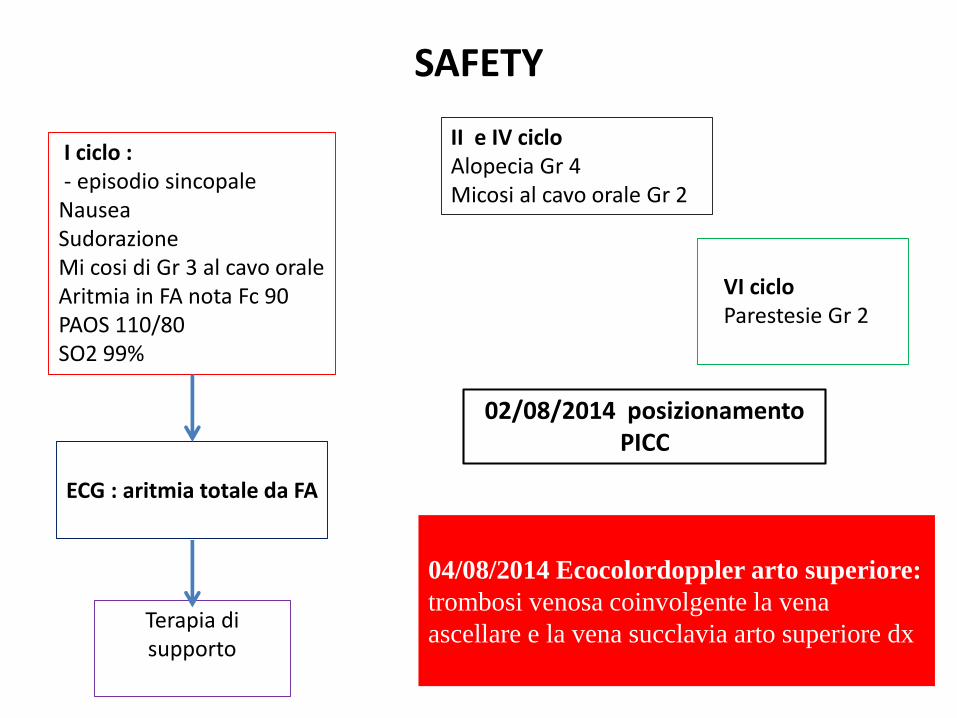
SAFETY
I ciclo :- episodio sincopale
NauseaSudorazioneMi cosi di Gr 3 al cavo oraleAritmia in FA nota Fc 90 PAOS 110/80SO2 99%
II e IV ciclo Alopecia Gr 4Micosi al cavo orale Gr 2
VI cicloParestesie Gr 2
ECG : aritmia totale da FA
Terapia di supporto
02/08/2014 posizionamento PICC
04/08/2014 Ecocolordoppler arto superiore:
trombosi venosa coinvolgente la vena
ascellare e la vena succlavia arto superiore dx
trattamento
Incremento della dose di EBPM a 8.000 UI x 2 volte/die sc
28/08/2014 Ecocolordoppler art superiori: parziale ricanalizzazione vena ascellare e succlavia ma non completa comprimibilità ed evidenzia di trombosi parietale.
PICC non viene rimosso
Continua con lo stesso schema terapeutico fino a settembre 2014Seguito da Bevacizumab di mantenimento

Deep vein thrombosis and pulmonary embolism are the most important manifestations of
thromboembolic disease in cancer patients

Incidenza TEV nei Tumori del polmone
retrsospective analysis of a lung cancer cohort of patienst
venous thromboembolic complications in 78 %, deep venous thrombosis in 55 % cases
arterial thromboembolic complications in 27 % casespulmonary embolism in 66 %
cases
autore TVE Ca polmone %
Connolly,6732 pts
13.9
Crolow,1940 pts
9.8
Zhang673 pts
13.2
Kadlec950 pts
8.4
Alexander 10.8

• Cancer patients with VTE have a two-fold or greater increased mortality compared with those without thrombosis
• Maybe due to development of fatal PEs or by with those cancers complicated by VTE (Sorensen 2000).
•VTE in cancer patients may behard to recognise due to aspecific symptoms which may overlap and be confused with symptoms caused by the underlying cancer disease process or cancer treatments.
• VTE carries significant morbidity due to the need for hospitalisation and an increased risk of recurrent VTE or bleeding complications while on anticoagulation (Hutten 2000; Prandoni 2002).
•The occurrence of (unrecognised) VTE may delay the delivery of cancer treatments such as chemotherapy with a further negative impacton morbidity and potentially mortality.
• venous thromboembolic events brings further emotional strain for patients and their families, which negatively impacts their QoL
• the costs related to the management of VTE may be considerable

Tramite TC
Conclusion Our findings suggest that oncology patients diagnosed with and treatedfor incidental PE, have similar high rates of recurrent VTE, bleeding complications,and mortality, as compared with oncology patients who develop symptomatic PE.

Fattori di rischio
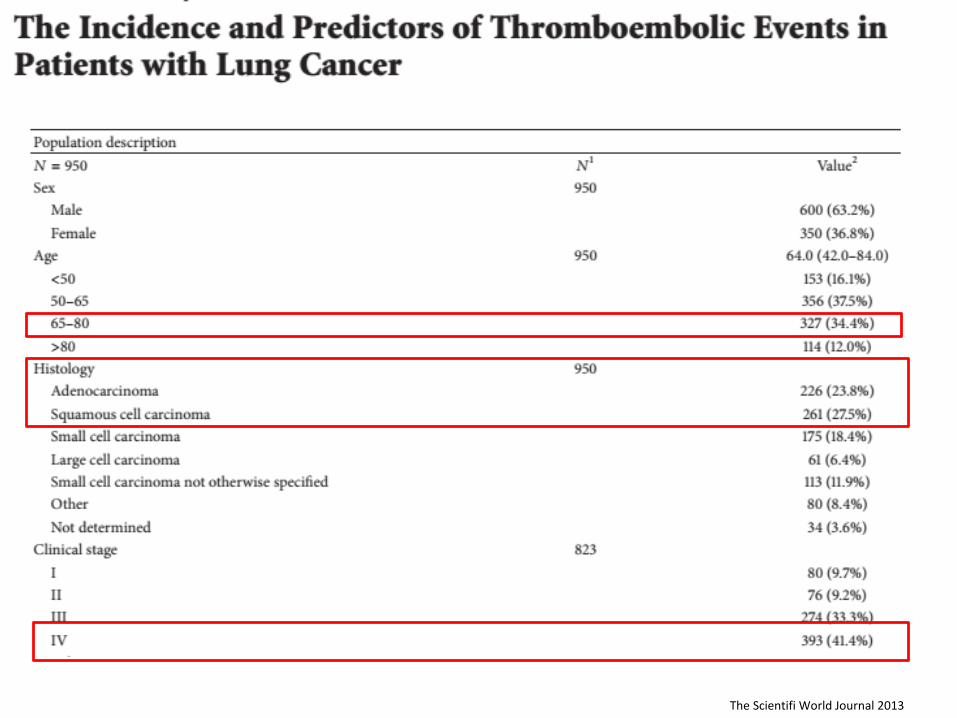
The Scientifi World Journal 2013


TEV e CHEMIOTERAPIA
• il rischio di TEV varia dal 15-20% a seconda del tipo di chemioterapia
• Chemioterapia determina effetti trombogeni attraverso:
- attivazione aggregazione piastrinica
- tossicità endoteliale
- espressione di TF da parte monociti/macrofagi, cellule endoteliali
- riduce attività fibrinolitica
- aumenta apoptosi cellule endoteliali
Agnelli G. Thrombosis Research 2007, 120 (Suppl 2); S128-S132

• antracicline: effetti non ancora completamente chiariti
• cancro del polmone non a piccole cellule: cisplatino + gemcitabina 16.7%
(Numico, Cancer 2015)
• cancro ovaio: cisplatino, epirubicina, ciclofosfamide 10.6%
Agnelli G. Thrombosis Research 2007, 120
0
2
4
6
8
10
12
14
16
18
20
8
CDDP2
5 FU
CDDP+Gem
Epi,MTX,platino
8-18%
15-17%
16.7%
10.6%
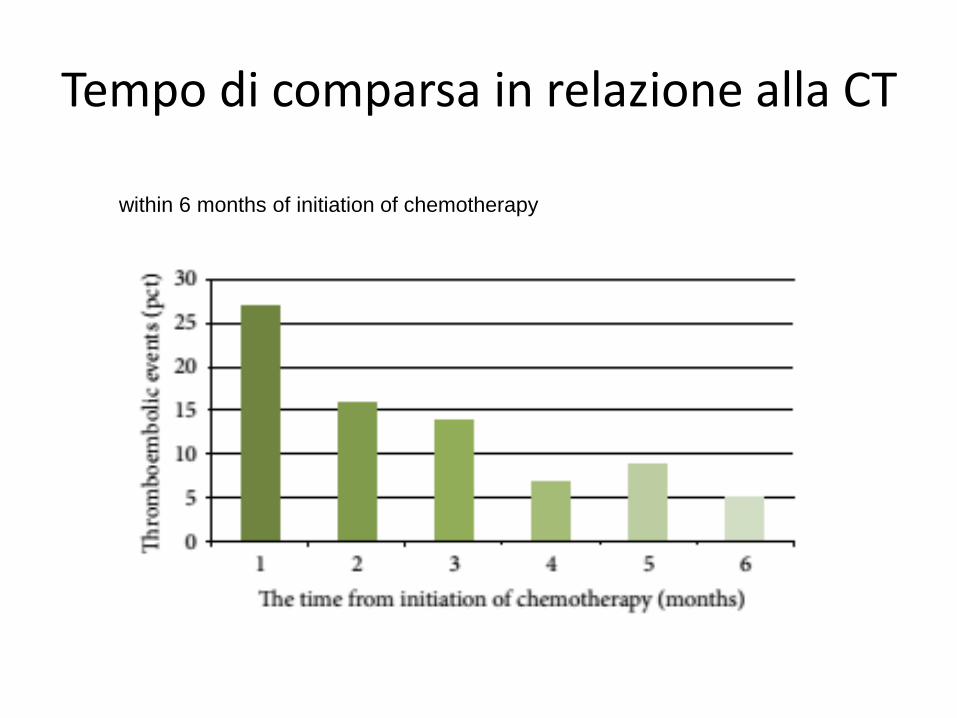
Tempo di comparsa in relazione alla CT
within 6 months of initiation of chemotherapy

Perplessità dell’oncologo sull’uso degli antiangiogenici
• Selezione dei pazienti
• Dati di efficacia
• Profilo di tossicità
• Gestione clinica degli eventi avversi
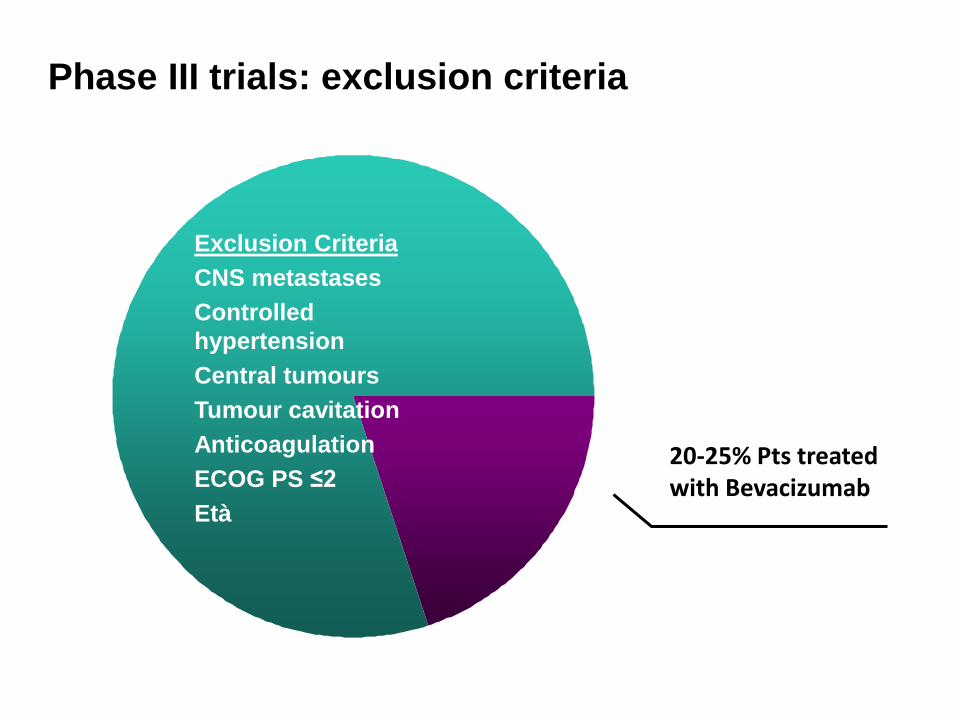
Current
exclusions
Exclusion Criteria
CNS metastases
Controlled
hypertension
Central tumours
Tumour cavitation
Anticoagulation
ECOG PS ≤2
Età
Phase III trials: exclusion criteria
20-25% Pts treatedwith Bevacizumab

25/08/2009 Lobectomia superiore dx + adenectomia ilo-mediastinicaIstologico Adenocarcinoma, G3, del polmone. pT2 N1. Analisi molecolare: EGFR wild type - Profilo genetico: TS high level
01/10/2009-10/12/2009 4 cicli CT adiuvante CDDP + Gemcitabina13/06/2011 TC total body con mdc: PD cerebrale19/08/2011-05/09/2011 RT panencefalica 30 Gy + RT lesione frontale sx 40Gy/fr 4Gy21/10/2011- 26/01/2012 5 cicli CT I linea: CBCA AUC 6 + Paclitaxel + Beva 10 mg/Kg 16/02/2012 - 08/01/2013: 14 somministrazioni Bevacizumab di mantenimento

Patients with CNS metastasescan receive bevacizumab-based therapy
Dataset1
No. of enrolled patients
No. of patients with CNS metastases
Rate of CNS bleeding (%)
Bevacizumab arm
Non-bevacizumabarm
A: 13 phase II/III trials 8,443 Bevacizumab: n=91Non-bevacizumab: n=96
3.3 1.0
B: 2 open-label trials (ATHENA and SAiL)
4,382 Bevacizumab: n=321 0.9 –
C: 2 prospective studies (ATLAS & PASSPORT)
845 Bevacizumab: n=131 0.8 –
25 March 2009: EMA removed label restriction to allow patientswith untreated CNS metastases to receive bevacizumab2
1. Besse, et al. Clin Cancer Res. 2010 ;16:269-78
2. http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Assessment_Report_-_Variation/human/000582/WC500029270.pdf
Low risk of CNS bleeding across tumour types (>13,000 patients)
Graphical elaboration from text data

Perplessità dell’oncologo
• Profilo di tossicità
• Gestione clinica degli eventi avversi
Crinò L, ASCO 2009
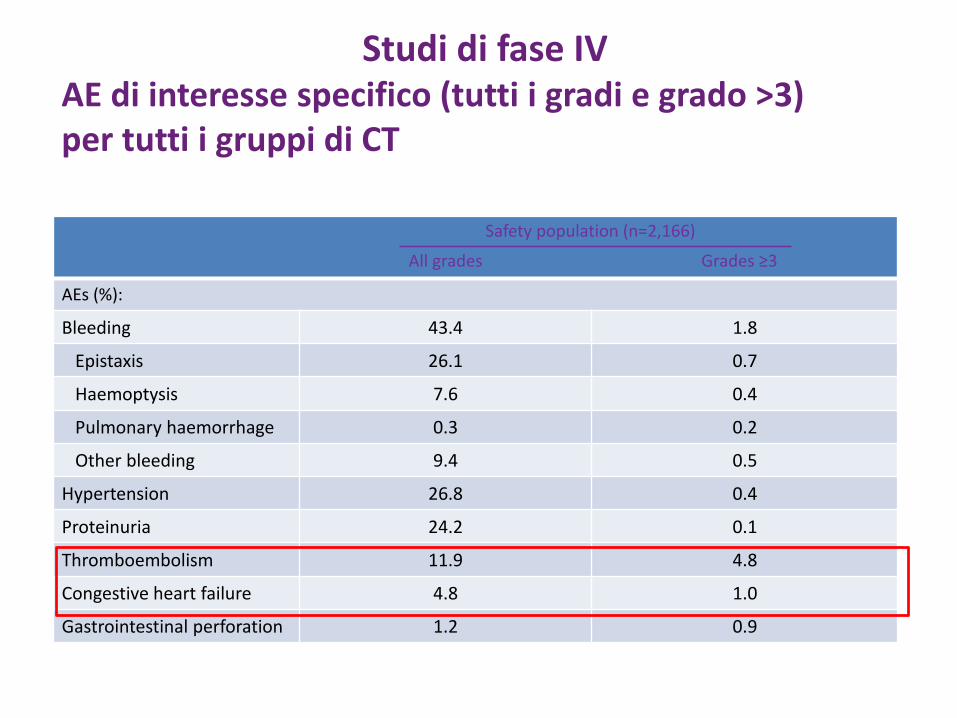
Studi di fase IVAE di interesse specifico (tutti i gradi e grado >3) per tutti i gruppi di CT
AEs (%):
Bleeding 43.4 1.8
Epistaxis 26.1 0.7
Haemoptysis 7.6 0.4
Pulmonary haemorrhage 0.3 0.2
Other bleeding 9.4 0.5
Hypertension 26.8 0.4
Proteinuria 24.2 0.1
Thromboembolism 11.9 4.8
Congestive heart failure 4.8 1.0
Gastrointestinal perforation 1.2 0.9
Safety population (n=2,166)
All grades Grades ≥3

Crinò L, ASCO 2009
BEVACIZUMABOutcome per AE specifici (n=2.166
AEs (%) Resolved ImprovedLeadingto death
Permanentdiscontinuationof bevacizumab
Temporaryinterruption
of bevacizumab
AEs of special interest 53.3 8.9 2.4 14.3 6.8
Bleeding 31.5 1.5 0.7 4.3 1.1
Hypertension 19.7 3.0 0 1.6 2.9
Proteinuria 16.9 2.8 0 1.2 1.2
Thromboembolism 5.9 2.2 1.1 6.2 1.6
Congestive heart failure 3.0 0.2 0.2 0.2 0.2
Gastrointestinalperforation
0.7 0.1 0.4 1.2 -

Antiangiogenici e rischio di Tromboembolismo
RCTs were included in the meta-analysis (n=7,956 patients)
Nalluri SR, 2008
summary incidence of high-grade VTE(13 RCTs, n=3795) was 6.3% (95% CI, 4.8,8.3)
The summary RR 1.33 of VTE (15 RCTs, n=7,956) for bevacizumab vs control
The summary RR 1.29 of all-grade VTE (6 RCTs, n=2,279) for bevacizumab vs control
The summary RR 1.38 of high-grade VTE(13 RCTs, n=3,795)
Both high dose (5mg/kg) and low dose (2.5mg/kg per week) bevacizumabwere associated with a statistically significant increase in the risk of VTE, RR, 1.31

Garon et al. Lancet 2014;384(9944):665-73.
REVEL: Adverse Events of Special Interest
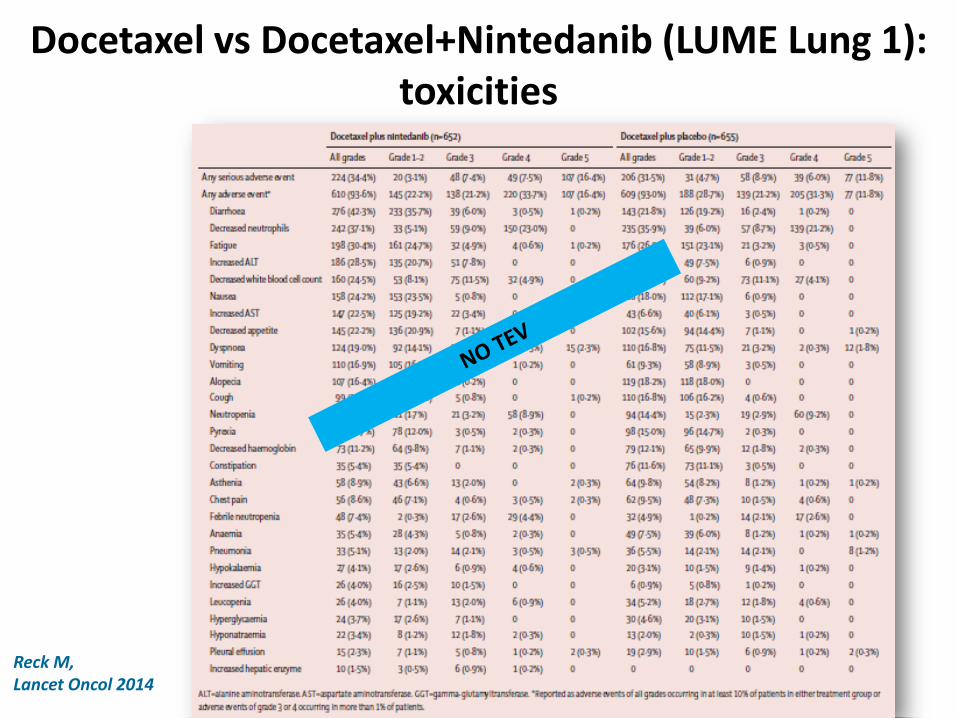
Docetaxel vs Docetaxel+Nintedanib (LUME Lung 1): toxicities
Reck M, Lancet Oncol 2014
Catheter related Central Venous Thrombosis: The Development of a Nationwide Consensus
Paper in ItalyNo trials randomizzati di confronto su tecnica di posizionamento
Fattori di rischio : - neoplasia
- Disturbi della coagulazione (mutazF V di Leiden/ bassi livelli di AT III)-Posizione del CVC-Monolume vs bilume- materiale del CVC ( basso rischio quelli in silicone o poliuretano 2-3 generazione)
Non differenza di outcome tra mantenere o rimuovere il CVC
7 trial retrospettivi: preservazione del CVC 45 – 96%
Elevato rischio di tEPA durante o subito dopo la rimozione del CVC in presenza di TVP del catetere
Rimozione solo in caso: infezione del CVC - malposizionamento- irreversibile occlusione del lume
Costantino Campisi, JAVA 2007
Incidenza : 0.3- 28% sintomatiche 27- 66% con metodiche strumentali

Esiste una profilassi?
Profilassi con anticoagulanti orali a basse dosi o EBPM 100 UI/kg
no evidenza scientifica di efficacia (trials randomizzati in doppio cieco)
PTS oncologici la scelta della profilassi
Non supportata dall’evidenza (Agnelli JCO 2005; Reichardt Prom ASCO 2002)
GAV eCELT considerano profilassi solo nell’alto rischio (familiarità o precedenti eventi TEV)
Trattamento di TVP del CVC
NO differenze
anticoagulanti orali vs EBPM

30 90 120 15060
0
2.5
5.0
7.5
days
Nadroparin
Placebo
Rate
of t
hro
mboem
bolic
events
Thromboembolic events: cumulative event rate
Protecht Study, Agnelli2009)

This study proofs the concept that thromboembolic events can be prevented in ambulatory cancer patients receiving chemotherapy
Nadroparin reduces by 50% the rate of thromboembolic
events in patients receiving chemotherapy for cancer
Future studies should focus on patients at high
thromboembolic risk such as those with lung cancer
Conclusion

Rischio di sanguinamento
Attenti a

Incidence of grade 3/4 AEs across trials
Planchard D., Expert Rev. Anticancer Ther. 11(8), 1163–1179 (2011)
Bevacizumab has a safe and tolerable profile1

Localizzazione Centrale
9% PH nei tumori centrali,con cavitazione e istologiasquamosa
Analisi retrospettiva degli studi di fase III non confermano il dato
AVAiL: 40.0% patients with severe
PH had tumours described as central
Tecniche di imaging
definizione di localizzazione centrale??
ARIES49% of patients ( n = 1489)central tumours were defined as
those showing a distance of <2.0
cm between central-most tumour
edge and the trachea, main
bronchi and lobular bronchi.
was not defined prospectively in the Phase III protocol
The methodology to define a mediastinal involvement by the tumor is not clear and suffers from the lack of specific recommendations
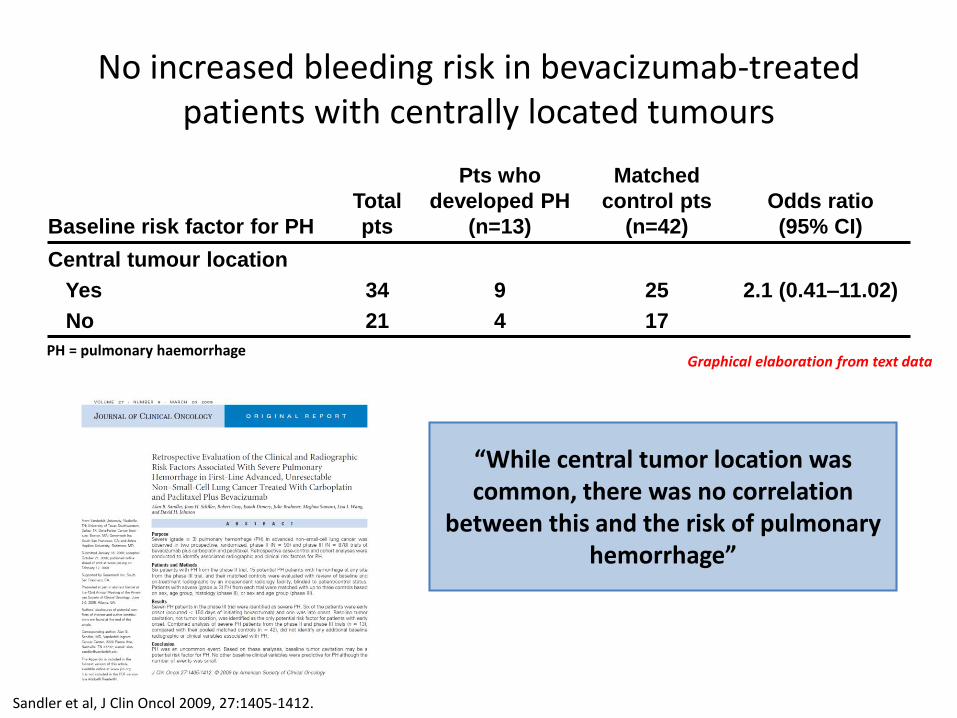
No increased bleeding risk in bevacizumab-treated patients with centrally located tumours
Baseline risk factor for PH
Total
pts
Pts who
developed PH
(n=13)
Matched
control pts
(n=42)
Odds ratio
(95% CI)
Central tumour location
Yes
No
34
21
9
4
25
17
2.1 (0.41–11.02)
“While central tumor location was common, there was no correlation
between this and the risk of pulmonary hemorrhage”
PH = pulmonary haemorrhage
Sandler et al, J Clin Oncol 2009, 27:1405-1412.
Graphical elaboration from text data

Anticoagulanti
analisi retrospettiva di tre studi randomizzati, placebo-controllati,che hanno coinvolto pazienti con tumore del colon-retto e delpolmone
terapia anticoagulante a dose terapeutica per unacomplicanza tromboembolica venosa durante la terapiacon bevacizumab.
rischio globale di emorragie gravi
bevacizumab 4,1% vs 4,2% placebo

SAiL: No increased bleeding risk with concomitant bevacizumab and anticoagulation
Dansin et al, Lung Cancer 2012; 76:373-379 Reck et al, Annals of Oncology 23: 1111–1120, 2012
The incidence of bleeding events, including grade ≥3 PH, was similar in patients receiving anticoagulants versus those not receiving anticoagulation therapy
CNS, central nervous system.a Pulmonary hemorrhage/hemoptysis.b Cerebral hemorrhage/hematoma.c Percentages are based on number of patients in each subgroup
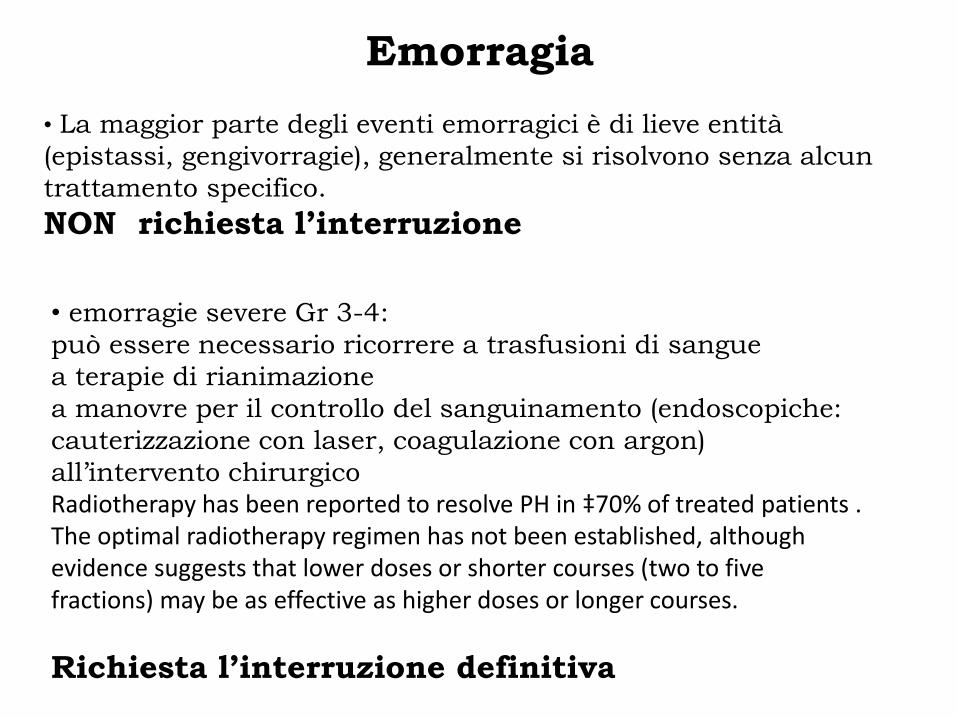
Emorragia
• La maggior parte degli eventi emorragici è di lieve entità
(epistassi, gengivorragie), generalmente si risolvono senza alcun
trattamento specifico.
NON richiesta l’interruzione
• emorragie severe Gr 3-4:
può essere necessario ricorrere a trasfusioni di sangue
a terapie di rianimazione
a manovre per il controllo del sanguinamento (endoscopiche:
cauterizzazione con laser, coagulazione con argon)
all’intervento chirurgico
Radiotherapy has been reported to resolve PH in ‡70% of treated patients . The optimal radiotherapy regimen has not been established, althoughevidence suggests that lower doses or shorter courses (two to fivefractions) may be as effective as higher doses or longer courses.
Richiesta l’interruzione definitiva
TROMBOEMBOLISMO
Nel caso di un TVP evento grave, di grado 3 o 4, la
terapia con bevacizumab dovrebbe essere interrotta per
due settimane e poi ripresa proseguendo la terapia
anticoagulante.
evento trombotico arterioso di qualsiasi grado, il
trattamento con bevacizumab dovrebbe essere interrotto
definitivamente

Nuovi farmaci
PROFILASSI SI O NO?