antibiotic stewardship indicators. diamantis plachouras (ecdc)
TRANSCRIPT
Integration of the ESAC-Net data collection / protocol at the ARHAI networks level
Diamantis Plachouras Surveillance and response support unit - ECDC
3rd Joint Meeting of the Antimicrobial Resistance and Healthcare-Associated Infections (ARHAI) Networks – Stockholm, 11-13 February 2015
Integration of the ESAC-Net data collection / protocol at the ARHAI networks level - ESAC-Net Meeting 3rd Joint Meeting of the Antimicrobial Resistance and Healthcare-Associated Infections (ARHAI) Networks – Stockholm, 11-13 February 2015
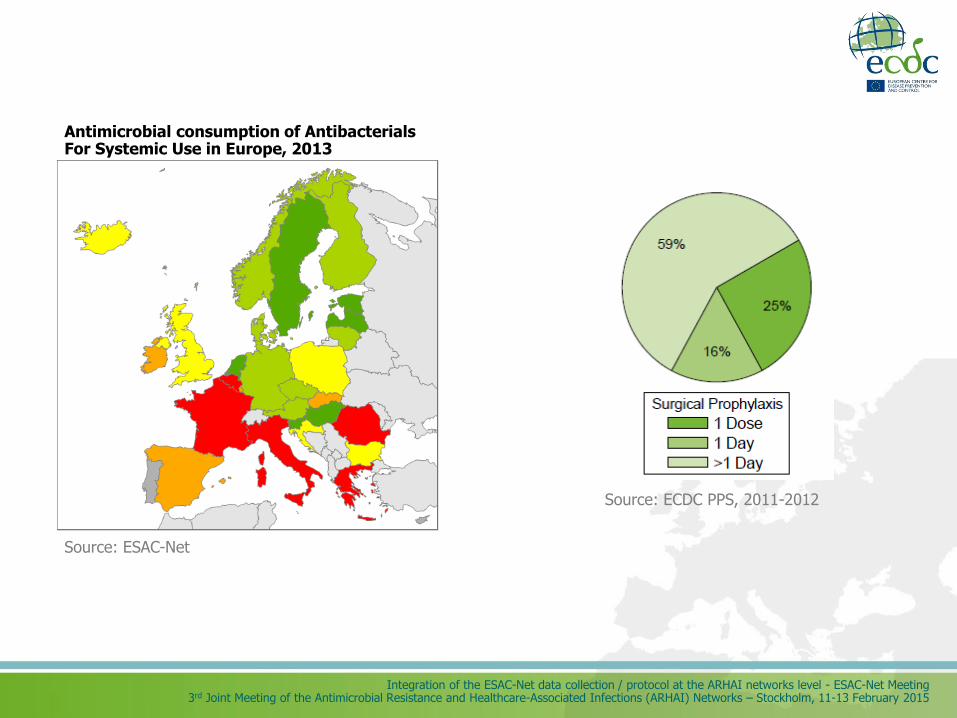
Source: ECDC PPS, 2011-2012
Antimicrobial consumption of Antibacterials For Systemic Use in Europe, 2013
Source: ESAC-Net
Integration of the ESAC-Net data collection / protocol at the ARHAI networks level - ESAC-Net Meeting 3rd Joint Meeting of the Antimicrobial Resistance and Healthcare-Associated Infections (ARHAI) Networks – Stockholm, 11-13 February 2015
Outline
• Need for indicators
• Overview of indicators in HAI-Net
• HAI-Net Point Prevalence Survey
• HAI-Net ICU
• HAI-Net SSI
• The TATFAR indicators of hospital antimicrobial stewardship programmes
Integration of the ESAC-Net data collection / protocol at the ARHAI networks level - ESAC-Net Meeting 3rd Joint Meeting of the Antimicrobial Resistance and Healthcare-Associated Infections (ARHAI) Networks – Stockholm, 11-13 February 2015
Need for monitoring and evaluation
Second report from the commission on the implementation of the council recommendation (2002/77/ec) on the prudent use of antimicrobial agents in human medicine.
• Develop and use indicators to monitor the implementation of the Council Recommendation and assess the impact of national action plans and the efficiency of measures.
• Develop mechanisms and indicators to assess the impact of national guidelines
Communication from the commission to the European parliament and the council: Action plan against the rising threats from Antimicrobial Resistance, 2011
• Better assessment and monitoring at national level of the implementation and efficiency of the national strategies and control measures.
Integration of the ESAC-Net data collection / protocol at the ARHAI networks level - ESAC-Net Meeting 3rd Joint Meeting of the Antimicrobial Resistance and Healthcare-Associated Infections (ARHAI) Networks – Stockholm, 11-13 February 2015
Quality indicators
• Assessment of quality of care is increasingly important element of the healthcare systems
• This is especially true for infections associated with healthcare and caused by pathogens resistant to antimicrobials
• Indicators allow the assessment of the quality of care
Mainz J. International Journal for Quality in Health Care 2003.15;6:523–530
Indicators are measures to assess a particular structure, process or outcome
Integration of the ESAC-Net data collection / protocol at the ARHAI networks level - ESAC-Net Meeting 3rd Joint Meeting of the Antimicrobial Resistance and Healthcare-Associated Infections (ARHAI) Networks – Stockholm, 11-13 February 2015
Types of indicators
• Structure
• Attributes of care settings
– Material resources
– Human resources
– Organisational structure
• e.g. presence of antimicrobial stewardship team
• Process
• Actual activity during care provision
• e.g. proportion of perioperative prophylaxis prescriptions reviewed
• Outcome
• Accomplishment of desired outcomes
• e.g. number of antibiotic prescriptions or incidence of infections by resistant pathogens
Integration of the ESAC-Net data collection / protocol at the ARHAI networks level - ESAC-Net Meeting 3rd Joint Meeting of the Antimicrobial Resistance and Healthcare-Associated Infections (ARHAI) Networks – Stockholm, 11-13 February 2015
The ideal indicator should be
• Clearly defined
• Evidence-based
• Specific and sensitive
• Accurate and reproducible
• Valid
• Feasible
• Allow discrimination and comparison
• Action-focused
Integration of the ESAC-Net data collection / protocol at the ARHAI networks level - ESAC-Net Meeting 3rd Joint Meeting of the Antimicrobial Resistance and Healthcare-Associated Infections (ARHAI) Networks – Stockholm, 11-13 February 2015
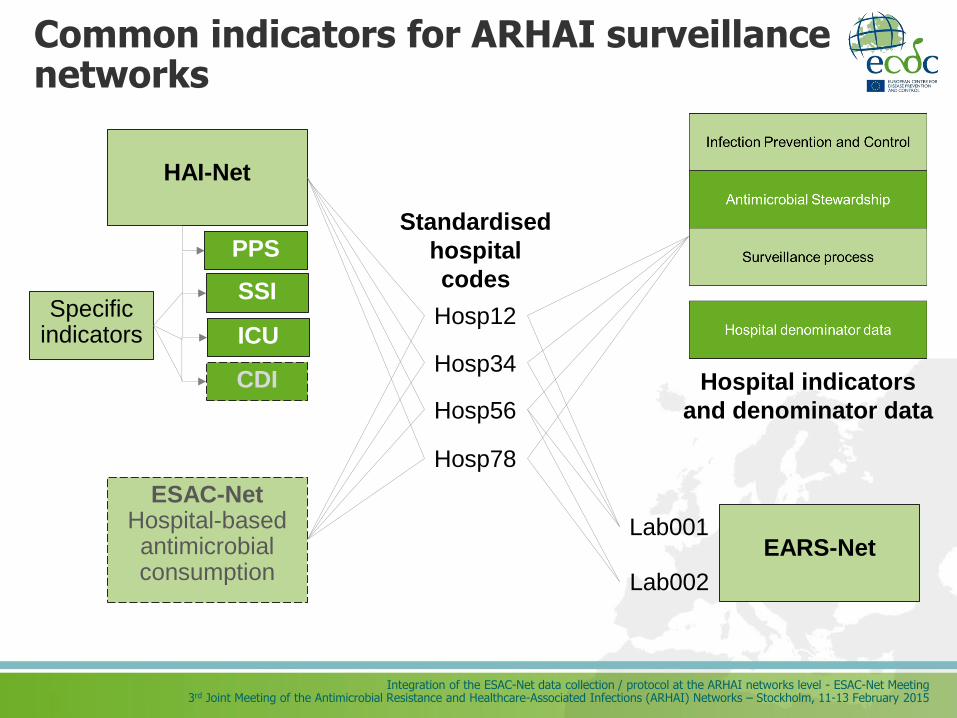
Common indicators for ARHAI surveillance networks
EARS-Net
HAI-Net
Lab001
Lab002
ESAC-Net Hospital-based antimicrobial consumption
PPS
ICU
SSI
CDI
Specific indicators
Hosp12
Hosp34
Hosp56
Hosp78
Standardised
hospital
codes
Hospital indicators
and denominator data

HAI-Net indicators
Integration of the ESAC-Net data collection / protocol at the ARHAI networks level - ESAC-Net Meeting 3rd Joint Meeting of the Antimicrobial Resistance and Healthcare-Associated Infections (ARHAI) Networks – Stockholm, 11-13 February 2015
Objectives
Increase awareness for HAI/AMR prevention
Add local value to surveillance by inter-hospital comparison and follow-up of key preventive measures
Inter-country comparison and follow-up of implementation of key preventive measures in EU/EEA countries
Follow-up of implementation of ECDC guidance and Council Recommendation 2009/C 151/01
At the longer term: linking evolution of prevention indicators with outcome indicators trends
Integration of the ESAC-Net data collection / protocol at the ARHAI networks level - ESAC-Net Meeting 3rd Joint Meeting of the Antimicrobial Resistance and Healthcare-Associated Infections (ARHAI) Networks – Stockholm, 11-13 February 2015
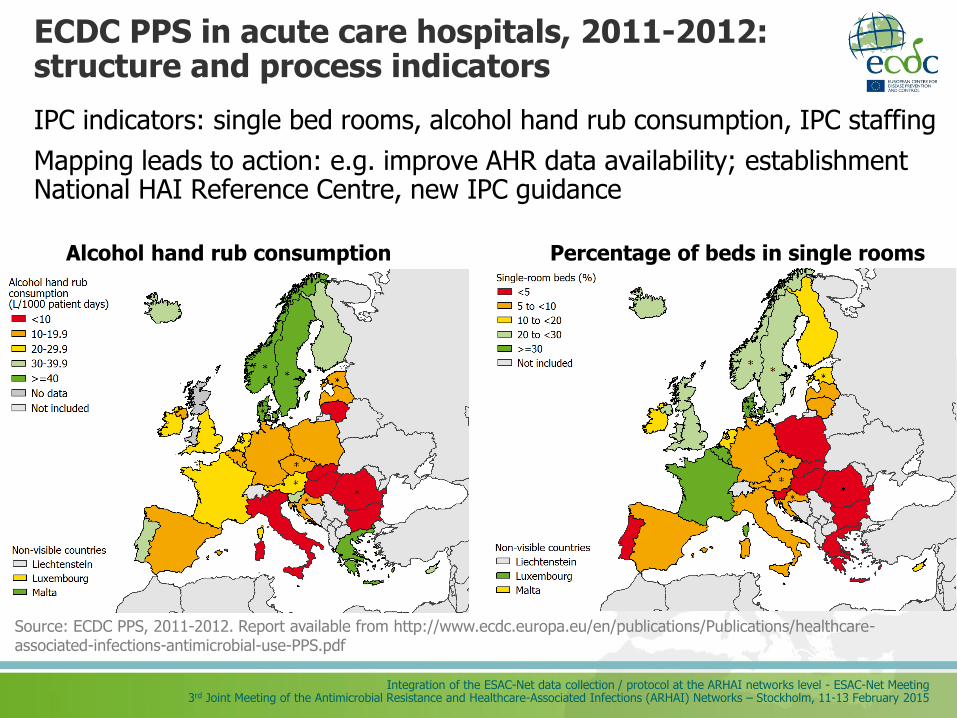
ECDC PPS in acute care hospitals, 2011-2012: structure and process indicators
IPC indicators: single bed rooms, alcohol hand rub consumption, IPC staffing
Mapping leads to action: e.g. improve AHR data availability; establishment National HAI Reference Centre, new IPC guidance
Percentage of beds in single rooms Alcohol hand rub consumption
Source: ECDC PPS, 2011-2012. Report available from http://www.ecdc.europa.eu/en/publications/Publications/healthcare-associated-infections-antimicrobial-use-PPS.pdf
Integration of the ESAC-Net data collection / protocol at the ARHAI networks level - ESAC-Net Meeting 3rd Joint Meeting of the Antimicrobial Resistance and Healthcare-Associated Infections (ARHAI) Networks – Stockholm, 11-13 February 2015
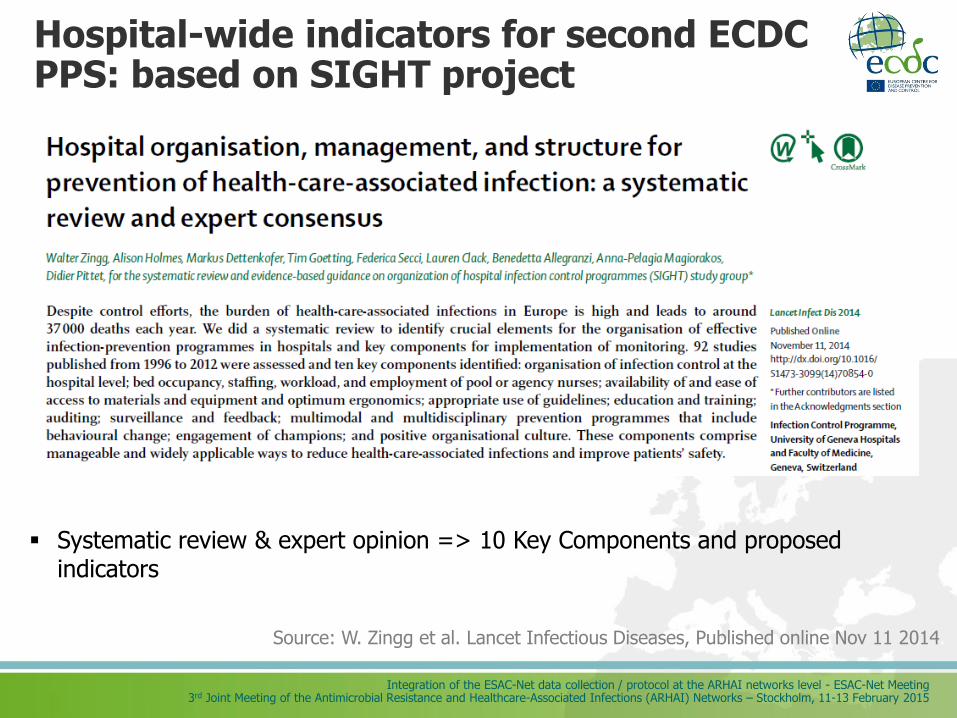
Hospital-wide indicators for second ECDC PPS: based on SIGHT project
Source: W. Zingg et al. Lancet Infectious Diseases, Published online Nov 11 2014.
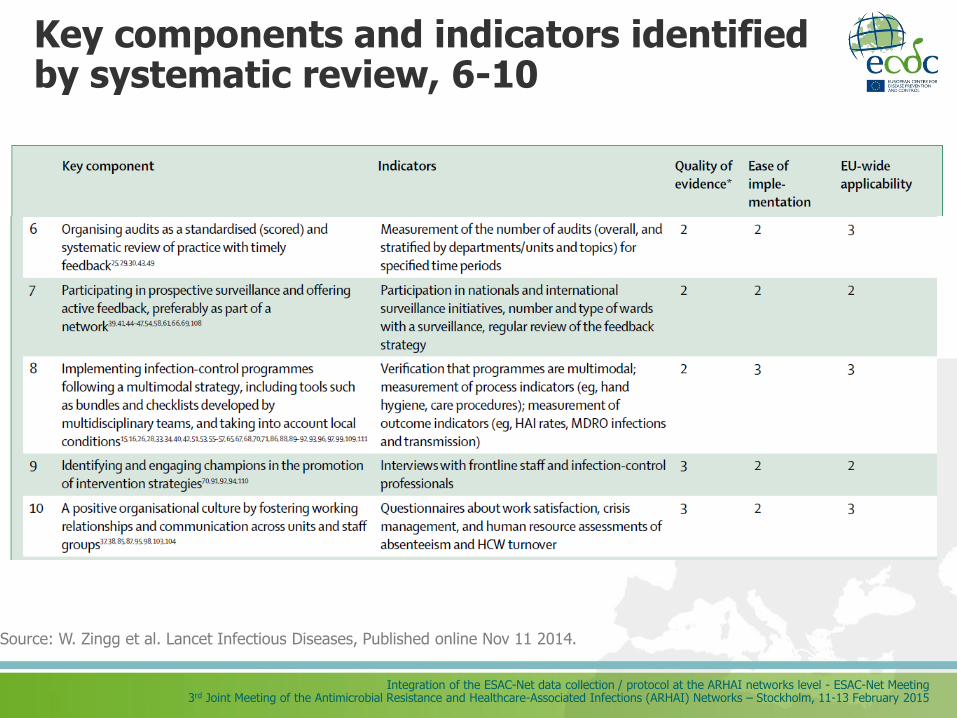
Systematic review & expert opinion => 10 Key Components and proposed indicators
Integration of the ESAC-Net data collection / protocol at the ARHAI networks level - ESAC-Net Meeting 3rd Joint Meeting of the Antimicrobial Resistance and Healthcare-Associated Infections (ARHAI) Networks – Stockholm, 11-13 February 2015
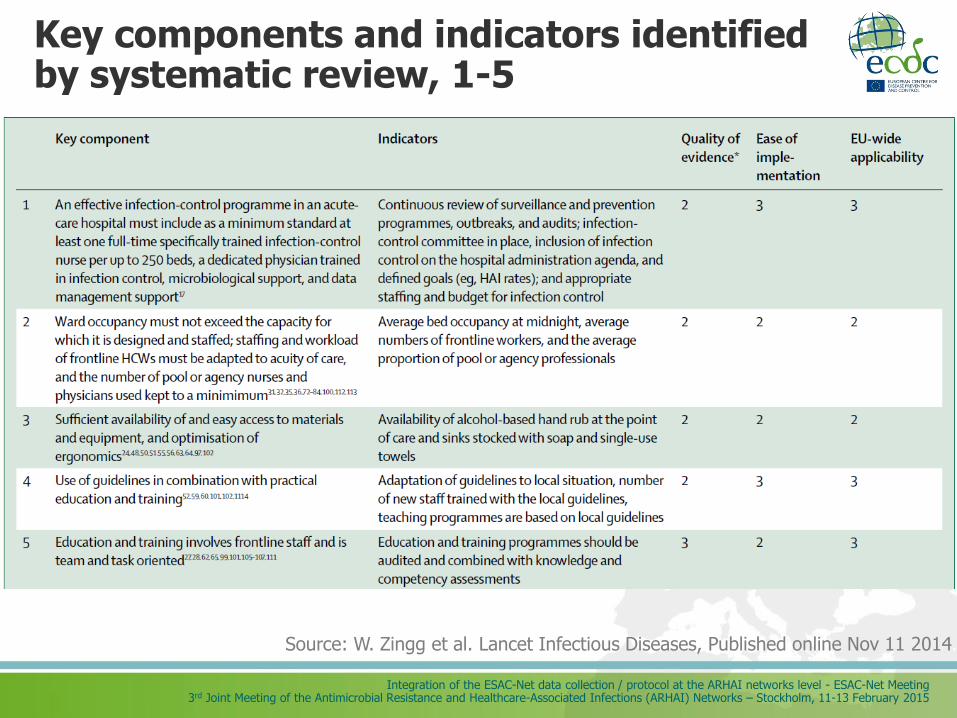
Key components and indicators identified by systematic review, 1-5
Source: W. Zingg et al. Lancet Infectious Diseases, Published online Nov 11 2014.
Integration of the ESAC-Net data collection / protocol at the ARHAI networks level - ESAC-Net Meeting 3rd Joint Meeting of the Antimicrobial Resistance and Healthcare-Associated Infections (ARHAI) Networks – Stockholm, 11-13 February 2015
Key components and indicators identified by systematic review, 6-10
Source: W. Zingg et al. Lancet Infectious Diseases, Published online Nov 11 2014.
Integration of the ESAC-Net data collection / protocol at the ARHAI networks level - ESAC-Net Meeting 3rd Joint Meeting of the Antimicrobial Resistance and Healthcare-Associated Infections (ARHAI) Networks – Stockholm, 11-13 February 2015
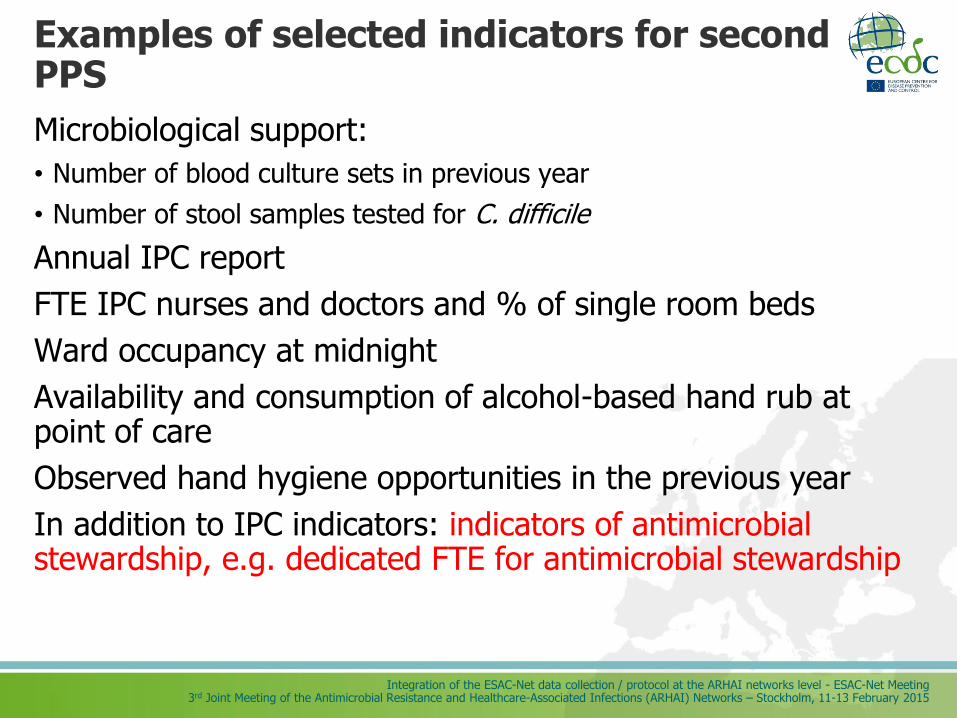
Examples of selected indicators for second PPS
Microbiological support:
• Number of blood culture sets in previous year
• Number of stool samples tested for C. difficile
Annual IPC report
FTE IPC nurses and doctors and % of single room beds
Ward occupancy at midnight
Availability and consumption of alcohol-based hand rub at point of care
Observed hand hygiene opportunities in the previous year
In addition to IPC indicators: indicators of antimicrobial stewardship, e.g. dedicated FTE for antimicrobial stewardship
Integration of the ESAC-Net data collection / protocol at the ARHAI networks level - ESAC-Net Meeting 3rd Joint Meeting of the Antimicrobial Resistance and Healthcare-Associated Infections (ARHAI) Networks – Stockholm, 11-13 February 2015
0
5
10
15
20
25
20
08
20
09
20
10
20
11
20
12
20
08
20
09
20
10
20
11
20
12
20
10
20
11
20
12
20
08
20
09
20
10
20
11
20
12
20
08
20
09
20
10
20
11
20
12
20
08
20
09
20
10
20
11
20
12
20
08
20
09
20
10
20
11
20
12
20
08
20
09
20
10
20
11
20
12
20
08
20
09
20
10
20
11
20
12
20
08
20
09
20
10
20
11
20
12
Austria Belgium Estonia France Italy Lithuania Luxembourg Portugal Slovakia Spain
N o
f IA
P /
1 0
00
intu
bat
ion
day
s
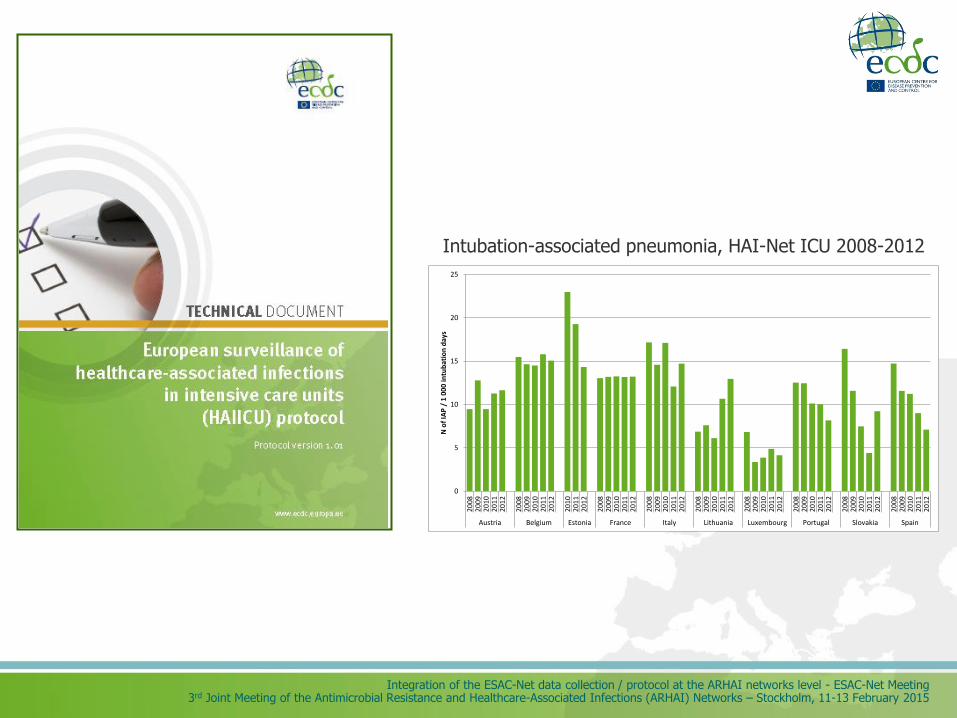
Intubation-associated pneumonia, HAI-Net ICU 2008-2012
Integration of the ESAC-Net data collection / protocol at the ARHAI networks level - ESAC-Net Meeting 3rd Joint Meeting of the Antimicrobial Resistance and Healthcare-Associated Infections (ARHAI) Networks – Stockholm, 11-13 February 2015
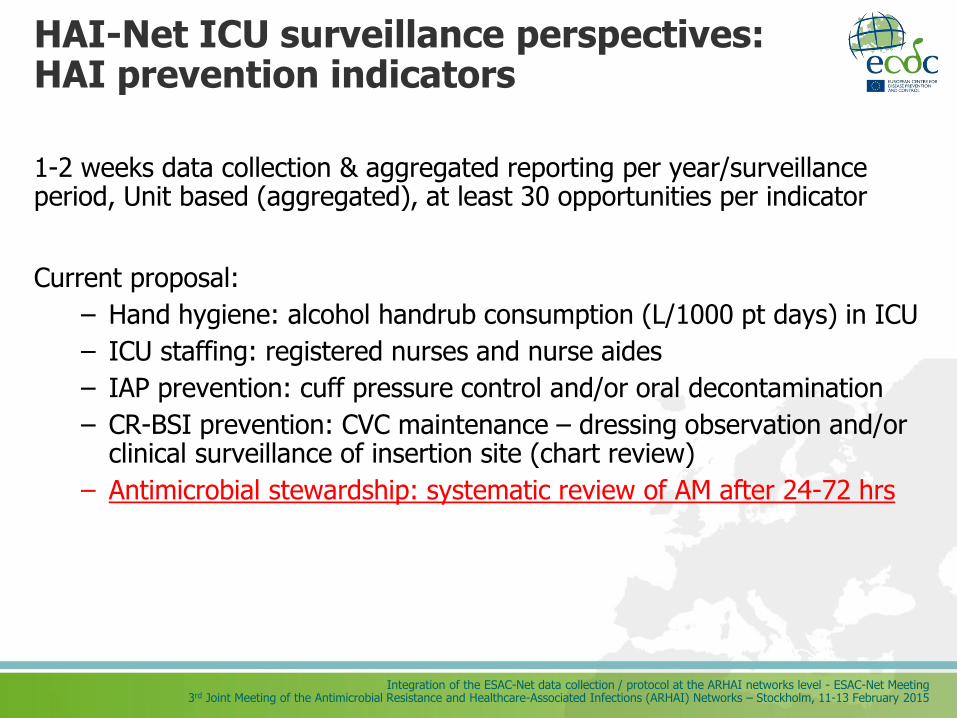
HAI-Net ICU surveillance perspectives: HAI prevention indicators
1-2 weeks data collection & aggregated reporting per year/surveillance period, Unit based (aggregated), at least 30 opportunities per indicator
Current proposal:
– Hand hygiene: alcohol handrub consumption (L/1000 pt days) in ICU
– ICU staffing: registered nurses and nurse aides
– IAP prevention: cuff pressure control and/or oral decontamination
– CR-BSI prevention: CVC maintenance – dressing observation and/or clinical surveillance of insertion site (chart review)
– Antimicrobial stewardship: systematic review of AM after 24-72 hrs
Integration of the ESAC-Net data collection / protocol at the ARHAI networks level - ESAC-Net Meeting 3rd Joint Meeting of the Antimicrobial Resistance and Healthcare-Associated Infections (ARHAI) Networks – Stockholm, 11-13 February 2015
Indicators for perioperative antibiotic prophylaxis
• to identify the effectiveness of key modalities of perioperative antibiotic prophylaxis from a systematic review
• to develop five key PAP modalities and process indicators for monitoring their implementation on the basis of scientific evidence and expert opinion.
ECDC, 2013
Integration of the ESAC-Net data collection / protocol at the ARHAI networks level - ESAC-Net Meeting 3rd Joint Meeting of the Antimicrobial Resistance and Healthcare-Associated Infections (ARHAI) Networks – Stockholm, 11-13 February 2015
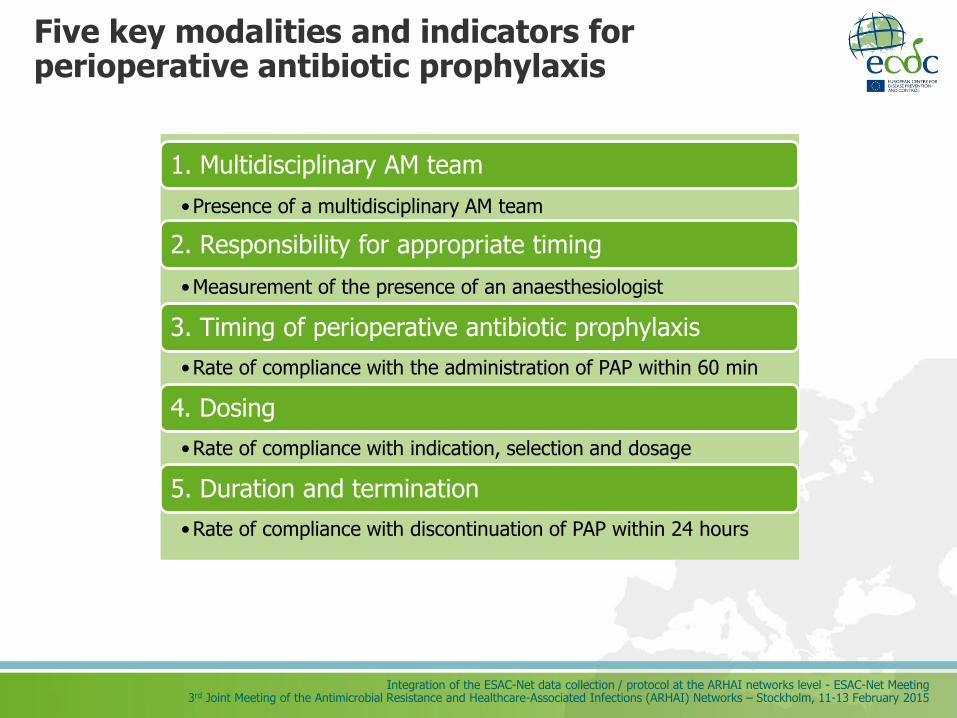
Five key modalities and indicators for perioperative antibiotic prophylaxis
1. Multidisciplinary AM team
•Presence of a multidisciplinary AM team
2. Responsibility for appropriate timing
•Measurement of the presence of an anaesthesiologist
3. Timing of perioperative antibiotic prophylaxis
•Rate of compliance with the administration of PAP within 60 min
4. Dosing
•Rate of compliance with indication, selection and dosage
5. Duration and termination
•Rate of compliance with discontinuation of PAP within 24 hours
Integration of the ESAC-Net data collection / protocol at the ARHAI networks level - ESAC-Net Meeting 3rd Joint Meeting of the Antimicrobial Resistance and Healthcare-Associated Infections (ARHAI) Networks – Stockholm, 11-13 February 2015
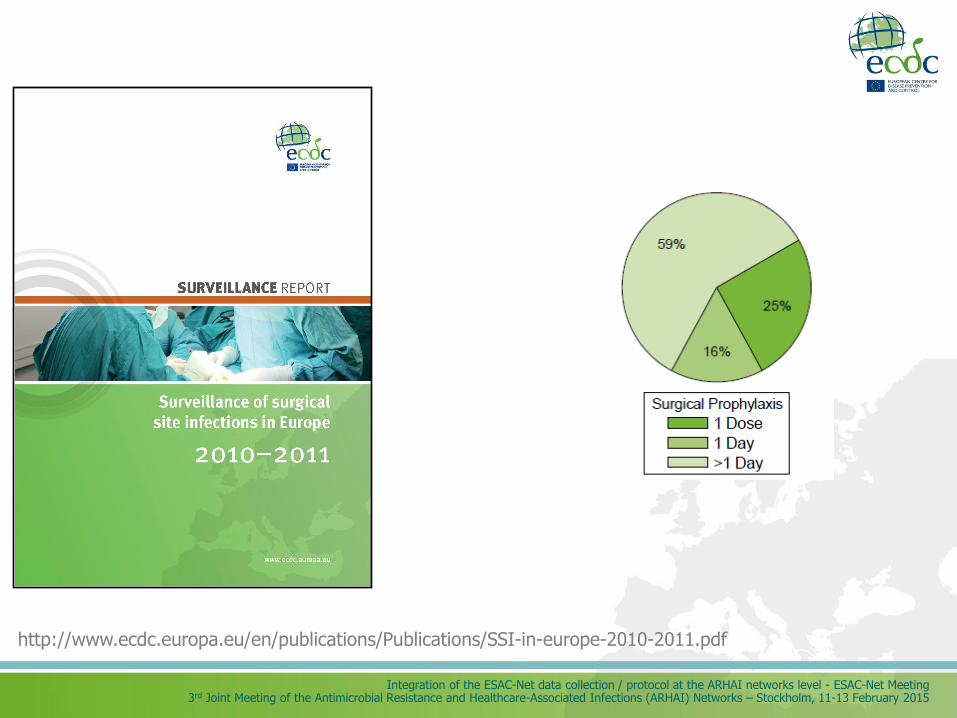
http://www.ecdc.europa.eu/en/publications/Publications/SSI-in-europe-2010-2011.pdf
Integration of the ESAC-Net data collection / protocol at the ARHAI networks level - ESAC-Net Meeting 3rd Joint Meeting of the Antimicrobial Resistance and Healthcare-Associated Infections (ARHAI) Networks – Stockholm, 11-13 February 2015
Proposed indicators in HAI-Net SSI surveillance
Peri-operative prophylaxis (PAP): two indicators from ECDC guidance:
–% compliance with the administration of PAP within 60 minutes
–% compliance with discontinuation of PAP within 24 hours after initiation of surgery
SSI prevention, other:
–Pre-operative skin preparation: % no hair removal or clipping
–Peri-operative normothermia (pilot)
–OR discipline ? (door opening based on Dutch PREZIES experience, inclusion in pilot)
–Possibly others in pilot, e.g. alcohol-based skin antisepsis
Modified Delphi Process for common structure and process indicators for hospital antimicrobial stewardship programmes Transatlantic Taskforce on Antimicrobial Resistance (TATFAR)
Integration of the ESAC-Net data collection / protocol at the ARHAI networks level - ESAC-Net Meeting 3rd Joint Meeting of the Antimicrobial Resistance and Healthcare-Associated Infections (ARHAI) Networks – Stockholm, 11-13 February 2015
TATFAR was created in 2009 with the goal of improving cooperation between the U.S. and the EU in three key areas 1. appropriate therapeutic use of antimicrobial drugs in
medical and veterinary communities 2. prevention of healthcare and community-associated drug-
resistant infections and 3. strategies for improving the pipeline of new antimicrobial
drugs
Integration of the ESAC-Net data collection / protocol at the ARHAI networks level - ESAC-Net Meeting 3rd Joint Meeting of the Antimicrobial Resistance and Healthcare-Associated Infections (ARHAI) Networks – Stockholm, 11-13 February 2015
Objective
TATFAR Recommendation #1: Develop a set of structure and process indicators for hospital antimicrobial stewardship programs
• Key elements of successful stewardship programmes and interventions
• Common strategy for the use, monitoring, and interpretation
• Meaningful comparisons between the US and EU Member States, as well as among institutions and regions.
Integration of the ESAC-Net data collection / protocol at the ARHAI networks level - ESAC-Net Meeting 3rd Joint Meeting of the Antimicrobial Resistance and Healthcare-Associated Infections (ARHAI) Networks – Stockholm, 11-13 February 2015
Antimicrobial stewardship programme
a coordinated programme that implements interventions to ensure appropriate antimicrobial prescribing in order to
• improve clinical efficacy of antimicrobial treatment
• limit antimicrobial resistance
• prevent Clostridium difficile infections
Integration of the ESAC-Net data collection / protocol at the ARHAI networks level - ESAC-Net Meeting 3rd Joint Meeting of the Antimicrobial Resistance and Healthcare-Associated Infections (ARHAI) Networks – Stockholm, 11-13 February 2015
Development of initial list of indicators
Integration of the ESAC-Net data collection / protocol at the ARHAI networks level - ESAC-Net Meeting 3rd Joint Meeting of the Antimicrobial Resistance and Healthcare-Associated Infections (ARHAI) Networks – Stockholm, 11-13 February 2015
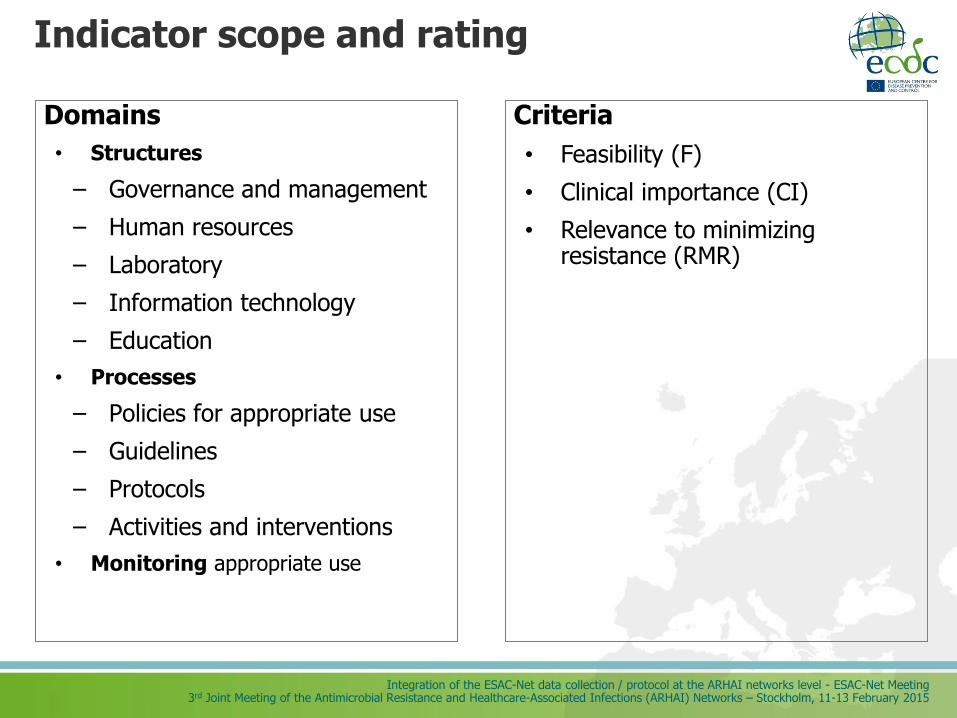
Indicator scope and rating
Domains
• Structures
– Governance and management
– Human resources
– Laboratory
– Information technology
– Education
• Processes
– Policies for appropriate use
– Guidelines
– Protocols
– Activities and interventions
• Monitoring appropriate use
Criteria
• Feasibility (F)
• Clinical importance (CI)
• Relevance to minimizing resistance (RMR)

Integration of the ESAC-Net data collection / protocol at the ARHAI networks level - ESAC-Net Meeting 3rd Joint Meeting of the Antimicrobial Resistance and Healthcare-Associated Infections (ARHAI) Networks – Stockholm, 11-13 February 2015
Level of evidence
Code Quality of Evidence Definition
A High
Further research is very unlikely to change our confidence in the estimate of effect.
Several high-quality studies with consistent results
In special cases: one large, high-quality multi-centre trial
B Moderate
Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate.
One high-quality study Several studies with some limitations
C Low
Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate.
One or more studies with severe limitations
D Very Low Any estimate of effect is very uncertain.
Expert opinion No direct research evidence One or more studies with very severe
limitations
Grading of Recommendations Assessment, Development and Evaluation (GRADE)
Integration of the ESAC-Net data collection / protocol at the ARHAI networks level - ESAC-Net Meeting 3rd Joint Meeting of the Antimicrobial Resistance and Healthcare-Associated Infections (ARHAI) Networks – Stockholm, 11-13 February 2015
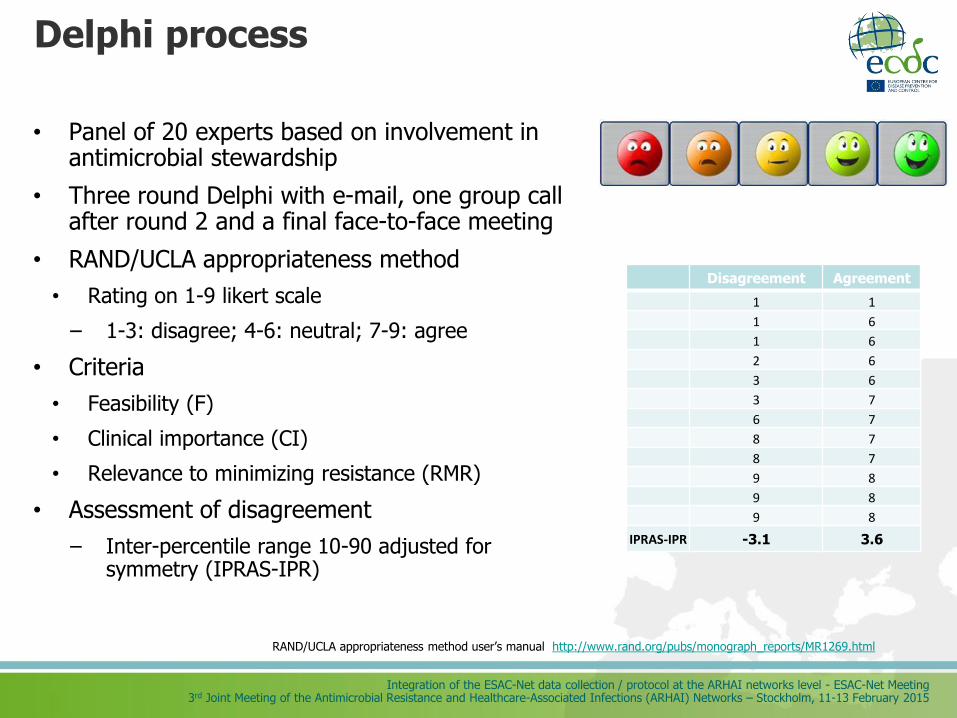
Delphi process
• Panel of 20 experts based on involvement in antimicrobial stewardship
• Three round Delphi with e-mail, one group call after round 2 and a final face-to-face meeting
• RAND/UCLA appropriateness method
• Rating on 1-9 likert scale
– 1-3: disagree; 4-6: neutral; 7-9: agree
• Criteria
• Feasibility (F)
• Clinical importance (CI)
• Relevance to minimizing resistance (RMR)
• Assessment of disagreement
– Inter-percentile range 10-90 adjusted for symmetry (IPRAS-IPR)
RAND/UCLA appropriateness method user’s manual http://www.rand.org/pubs/monograph_reports/MR1269.html
Disagreement Agreement
1 1
1 6
1 6
2 6
3 6
3 7
6 7
8 7
8 7
9 8
9 8
9 8
IPRAS-IPR -3.1 3.6
Integration of the ESAC-Net data collection / protocol at the ARHAI networks level - ESAC-Net Meeting 3rd Joint Meeting of the Antimicrobial Resistance and Healthcare-Associated Infections (ARHAI) Networks – Stockholm, 11-13 February 2015
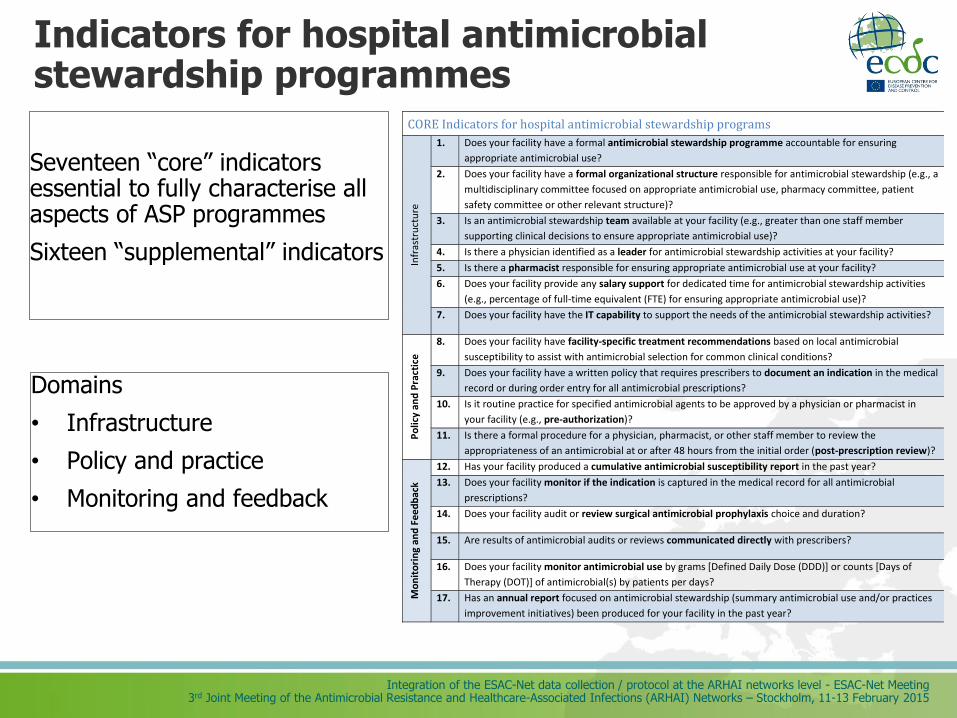
Indicators for hospital antimicrobial stewardship programmes Seventeen “core” indicators essential to fully characterise all aspects of ASP programmes
Sixteen “supplemental” indicators
CORE Indicators for hospital antimicrobial stewardship programs
Infr
astr
uct
ure
1. Does your facility have a formal antimicrobial stewardship programme accountable for ensuring
appropriate antimicrobial use?
2. Does your facility have a formal organizational structure responsible for antimicrobial stewardship (e.g., a
multidisciplinary committee focused on appropriate antimicrobial use, pharmacy committee, patient
safety committee or other relevant structure)?
3. Is an antimicrobial stewardship team available at your facility (e.g., greater than one staff member
supporting clinical decisions to ensure appropriate antimicrobial use)?
4. Is there a physician identified as a leader for antimicrobial stewardship activities at your facility?
5. Is there a pharmacist responsible for ensuring appropriate antimicrobial use at your facility?
6. Does your facility provide any salary support for dedicated time for antimicrobial stewardship activities
(e.g., percentage of full-time equivalent (FTE) for ensuring appropriate antimicrobial use)?
7. Does your facility have the IT capability to support the needs of the antimicrobial stewardship activities?
Po
licy
and
Pra
ctic
e
8. Does your facility have facility-specific treatment recommendations based on local antimicrobial
susceptibility to assist with antimicrobial selection for common clinical conditions?
9. Does your facility have a written policy that requires prescribers to document an indication in the medical
record or during order entry for all antimicrobial prescriptions?
10. Is it routine practice for specified antimicrobial agents to be approved by a physician or pharmacist in
your facility (e.g., pre-authorization)?
11. Is there a formal procedure for a physician, pharmacist, or other staff member to review the
appropriateness of an antimicrobial at or after 48 hours from the initial order (post-prescription review)?
Mo
nit
ori
ng
and
Fee
db
ack
12. Has your facility produced a cumulative antimicrobial susceptibility report in the past year?
13. Does your facility monitor if the indication is captured in the medical record for all antimicrobial
prescriptions?
14. Does your facility audit or review surgical antimicrobial prophylaxis choice and duration?
15. Are results of antimicrobial audits or reviews communicated directly with prescribers?
16. Does your facility monitor antimicrobial use by grams [Defined Daily Dose (DDD)] or counts [Days of
Therapy (DOT)] of antimicrobial(s) by patients per days?
17. Has an annual report focused on antimicrobial stewardship (summary antimicrobial use and/or practices
improvement initiatives) been produced for your facility in the past year?
Domains
• Infrastructure
• Policy and practice
• Monitoring and feedback
Integration of the ESAC-Net data collection / protocol at the ARHAI networks level - ESAC-Net Meeting 3rd Joint Meeting of the Antimicrobial Resistance and Healthcare-Associated Infections (ARHAI) Networks – Stockholm, 11-13 February 2015
Core indicators - Infrastructure
1. Does your facility have a formal antimicrobial stewardship programme accountable for
ensuring appropriate antimicrobial use?
2. Does your facility have a formal organizational structure responsible for antimicrobial
stewardship (e.g., a multidisciplinary committee focused on appropriate antimicrobial use, pharmacy
committee, patient safety committee or other relevant structure)?
3. Is an antimicrobial stewardship team available at your facility (e.g., greater than one staff
member supporting clinical decisions to ensure appropriate antimicrobial use)?
4. Is there a physician identified as a leader for antimicrobial stewardship activities at your
facility?
5. Is there a pharmacist responsible for ensuring appropriate antimicrobial use at your facility?
6. Does your facility provide any salary support for dedicated time for antimicrobial stewardship
activities (e.g., percentage of full-time equivalent (FTE) for ensuring appropriate antimicrobial use)?
7. Does your facility have the IT capability to support the needs of the antimicrobial stewardship
activities?
Integration of the ESAC-Net data collection / protocol at the ARHAI networks level - ESAC-Net Meeting 3rd Joint Meeting of the Antimicrobial Resistance and Healthcare-Associated Infections (ARHAI) Networks – Stockholm, 11-13 February 2015
Core indicators - Policy and practice
8. Does your facility have facility-specific treatment recommendations based on local antimicrobial
susceptibility to assist with antimicrobial selection for common clinical conditions?
9. Does your facility have a written policy that requires prescribers to document an indication in the
medical record or during order entry for all antimicrobial prescriptions?
10. Is it routine practice for specified antimicrobial agents to be approved by a physician or pharmacist in
your facility (e.g., pre-authorization)?
11. Is there a formal procedure for a physician, pharmacist, or other staff member to review the
appropriateness of an antimicrobial at or after 48 hours from the initial order (post-prescription
review)?
Integration of the ESAC-Net data collection / protocol at the ARHAI networks level - ESAC-Net Meeting 3rd Joint Meeting of the Antimicrobial Resistance and Healthcare-Associated Infections (ARHAI) Networks – Stockholm, 11-13 February 2015
Core indicators - Monitoring and feedback
12. Has your facility produced a cumulative antimicrobial susceptibility report in the past year?
13. Does your facility monitor if the indication is captured in the medical record for all antimicrobial
prescriptions?
14. Does your facility audit or review surgical antimicrobial prophylaxis choice and duration?
15. Are results of antimicrobial audits or reviews communicated directly with prescribers?
16. Does your facility monitor antimicrobial use by grams [Defined Daily Dose (DDD)] or counts [Days
of Therapy (DOT)] of antimicrobial(s) by patients per days?
17. Has an annual report focused on antimicrobial stewardship (summary antimicrobial use and/or
practices improvement initiatives) been produced for your facility in the past year?
Integration of the ESAC-Net data collection / protocol at the ARHAI networks level - ESAC-Net Meeting 3rd Joint Meeting of the Antimicrobial Resistance and Healthcare-Associated Infections (ARHAI) Networks – Stockholm, 11-13 February 2015
Potential for comparison
• 15 questions based on the indicators are currently being asked to nearly 4000 US facilities reporting to NHSN
• acute care,
• long-term acute care,
• inpatient rehabilitation facilities
National Healthcare Safety Network (NHSN) annual hospital survey. Courtesy of L. Pollack, CDC
Integration of the ESAC-Net data collection / protocol at the ARHAI networks level - ESAC-Net Meeting 3rd Joint Meeting of the Antimicrobial Resistance and Healthcare-Associated Infections (ARHAI) Networks – Stockholm, 11-13 February 2015
Outcome measures
• Antimicrobial consumption measures
• Antimicrobial resistance measures
• Incidence of infections by antimicrobial resistant organisms
• Patient outcome measures
• Mortality associated with antimicrobial resistant organisms
• Incidence of infection by C. difficile
• Length of hospitalisation
Morris AM et al. Infect Control Hosp Epidemiol. 2012 Apr;33(4):374-80
• Challenges
• Specificity of association
• Interpretation of quantitative information
• Variability of systems
Integration of the ESAC-Net data collection / protocol at the ARHAI networks level - ESAC-Net Meeting 3rd Joint Meeting of the Antimicrobial Resistance and Healthcare-Associated Infections (ARHAI) Networks – Stockholm, 11-13 February 2015
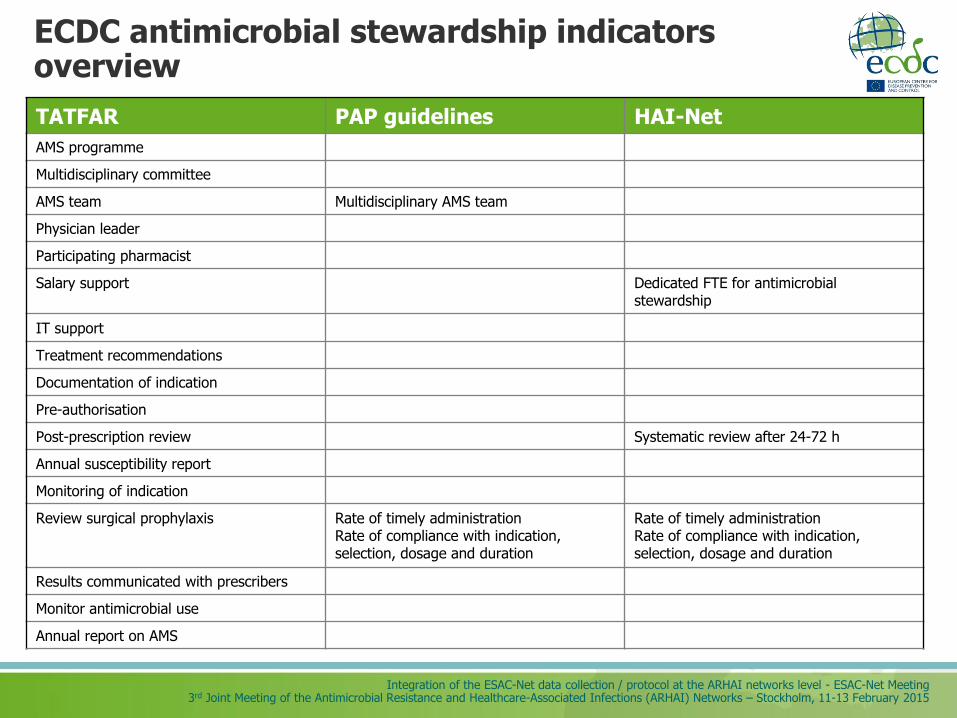
ECDC antimicrobial stewardship indicators overview
TATFAR PAP guidelines HAI-Net
AMS programme
Multidisciplinary committee
AMS team Multidisciplinary AMS team
Physician leader
Participating pharmacist
Salary support Dedicated FTE for antimicrobial stewardship
IT support
Treatment recommendations
Documentation of indication
Pre-authorisation
Post-prescription review Systematic review after 24-72 h
Annual susceptibility report
Monitoring of indication
Review surgical prophylaxis Rate of timely administration Rate of compliance with indication, selection, dosage and duration
Rate of timely administration Rate of compliance with indication, selection, dosage and duration
Results communicated with prescribers
Monitor antimicrobial use
Annual report on AMS
Integration of the ESAC-Net data collection / protocol at the ARHAI networks level - ESAC-Net Meeting 3rd Joint Meeting of the Antimicrobial Resistance and Healthcare-Associated Infections (ARHAI) Networks – Stockholm, 11-13 February 2015
Conclusions and future steps
Harmonised indicators
• Enable
• Monitoring of activities related to antimicrobial use
• Inter-hospital comparisons
• Inter-country comparisons
• Global comparisons
• Set common targets for quality improvement
• Support the optimal use of antimicrobials
Integration of the ESAC-Net data collection / protocol at the ARHAI networks level - ESAC-Net Meeting 3rd Joint Meeting of the Antimicrobial Resistance and Healthcare-Associated Infections (ARHAI) Networks – Stockholm, 11-13 February 2015
Acknowledgements
• Centers for Disease Prevention and Control: Heidi Gruhler, Ronda Sinkowitz-Cochran, J. Todd Weber
• ECDC ARHAI Disease Programme: Klaus Weist, Carl Suetens, Anna-Pelagia Magiorakos, Marc Struelens, Dominique Monnet
• TATFAR Indicators for Hospital Antimicrobial Stewardship Programmes Expert Group: Anastasia Antoniadou, Bojana Beovic, Franky Buyle, Sara Cosgrove, Peter Davey, Elizabeth S. Dodds Ashley, Catherine Dumartin, Alison Holmes, Winfried Kern, Maria Luisa Moro, Dilip Nathwani, Jeanne Negley, Melinda Neuhauser, Christopher A. Ohl, Jeroen Schouten, Ed Septimus, Agnes Wechsler- Fördös

Integration of the ESAC-Net data collection / protocol at the ARHAI networks level - ESAC-Net Meeting 3rd Joint Meeting of the Antimicrobial Resistance and Healthcare-Associated Infections (ARHAI) Networks – Stockholm, 11-13 February 2015
Website: http://antibiotic.ecdc.europa.eu Facebook: EAAD.EU Twitter: @EAAD_EU (#EAAD)
18 November

Integration of the ESAC-Net data collection / protocol at the ARHAI networks level - ESAC-Net Meeting 3rd Joint Meeting of the Antimicrobial Resistance and Healthcare-Associated Infections (ARHAI) Networks – Stockholm, 11-13 February 2015
Integration of the ESAC-Net data collection / protocol at the ARHAI networks level - ESAC-Net Meeting 3rd Joint Meeting of the Antimicrobial Resistance and Healthcare-Associated Infections (ARHAI) Networks – Stockholm, 11-13 February 2015
Core indicators using strict criteria
1. Does your facility have a formally defined antimicrobial stewardship programme for assuring appropriate antimicrobial use? (78.9%)
2. Is an antimicrobial stewardship team available at your facility? (83.3%)
3. Is there a physician identified as a leader for stewardship activities at your facility (88.9%)
4. Is there a pharmacist responsible for working to improve antimicrobial use at your facility? (76.5%)
5. Does your facility produce a cumulative antimicrobial susceptibility report at least annually? (73.7%)
6. Is there a formal procedure for a physician, pharmacist, or other staff member to review the appropriateness of an antimicrobial after 48 hours from the initial order (post-prescription review)? (72.2%)
7. Does your facility monitor antimicrobial use by grams [Defined Daily Dose (DDD)] or counts [Days of Therapy (DOT)] of antimicrobial(s) by patients per day? (89.5%)
Integration of the ESAC-Net data collection / protocol at the ARHAI networks level - ESAC-Net Meeting 3rd Joint Meeting of the Antimicrobial Resistance and Healthcare-Associated Infections (ARHAI) Networks – Stockholm, 11-13 February 2015
Features of ideal TATFAR indicators
Characterize and differentiate among programmes
Capture current and expansion activities
Able to integrate with other assessment tools
Comparable
Manageable number of indicators
Integration of the ESAC-Net data collection / protocol at the ARHAI networks level - ESAC-Net Meeting 3rd Joint Meeting of the Antimicrobial Resistance and Healthcare-Associated Infections (ARHAI) Networks – Stockholm, 11-13 February 2015
Challenges
Differences in public health and health care systems
• CDC is a health agency for one country, with no national healthcare system
• ECDC is a health agency for many countries, some with national healthcare systems
Link to outcomes
• What are the best outcomes?
• Do they impact resistance?
Integration of the ESAC-Net data collection / protocol at the ARHAI networks level - ESAC-Net Meeting 3rd Joint Meeting of the Antimicrobial Resistance and Healthcare-Associated Infections (ARHAI) Networks – Stockholm, 11-13 February 2015
Why Delphi?
• Structured communication technique based on panel of experts for:
• synthesising information
• building of expert consensus
• avoiding domination of the process by one or few experts
Boulkedid R et al. Using and reporting the Delphi method for selecting healthcare quality indicators: a systematic review. PLoS One. 2011;6(6):e20476.
Integration of the ESAC-Net data collection / protocol at the ARHAI networks level - ESAC-Net Meeting 3rd Joint Meeting of the Antimicrobial Resistance and Healthcare-Associated Infections (ARHAI) Networks – Stockholm, 11-13 February 2015
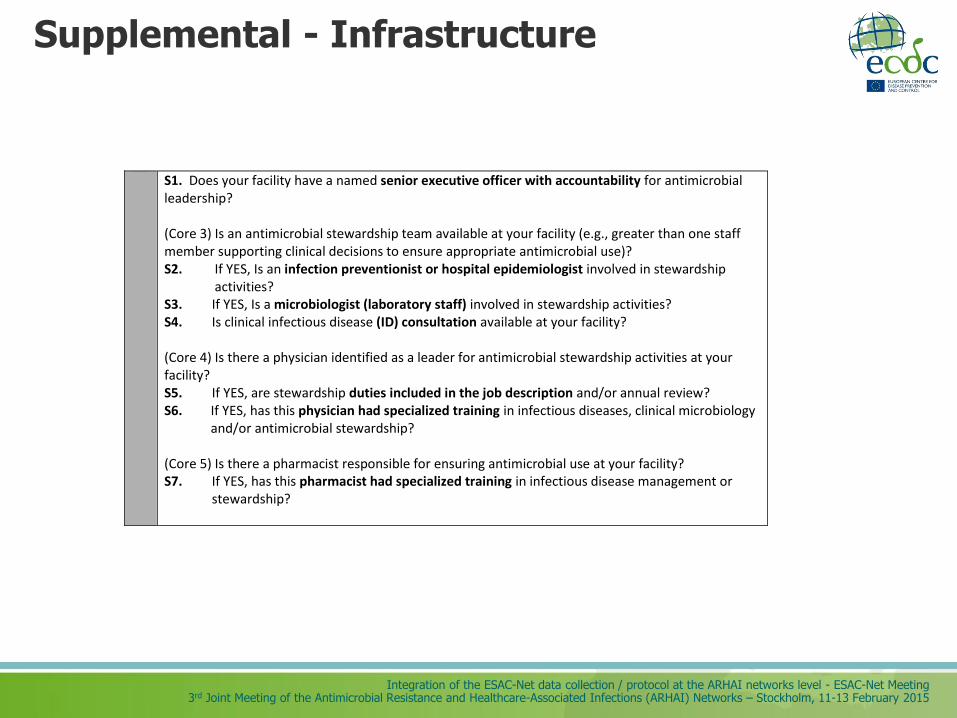
Supplemental - Infrastructure
S1. Does your facility have a named senior executive officer with accountability for antimicrobial leadership? (Core 3) Is an antimicrobial stewardship team available at your facility (e.g., greater than one staff member supporting clinical decisions to ensure appropriate antimicrobial use)? S2. If YES, Is an infection preventionist or hospital epidemiologist involved in stewardship
activities? S3. If YES, Is a microbiologist (laboratory staff) involved in stewardship activities? S4. Is clinical infectious disease (ID) consultation available at your facility? (Core 4) Is there a physician identified as a leader for antimicrobial stewardship activities at your facility? S5. If YES, are stewardship duties included in the job description and/or annual review? S6. If YES, has this physician had specialized training in infectious diseases, clinical microbiology
and/or antimicrobial stewardship? (Core 5) Is there a pharmacist responsible for ensuring antimicrobial use at your facility? S7. If YES, has this pharmacist had specialized training in infectious disease management or stewardship?
Integration of the ESAC-Net data collection / protocol at the ARHAI networks level - ESAC-Net Meeting 3rd Joint Meeting of the Antimicrobial Resistance and Healthcare-Associated Infections (ARHAI) Networks – Stockholm, 11-13 February 2015
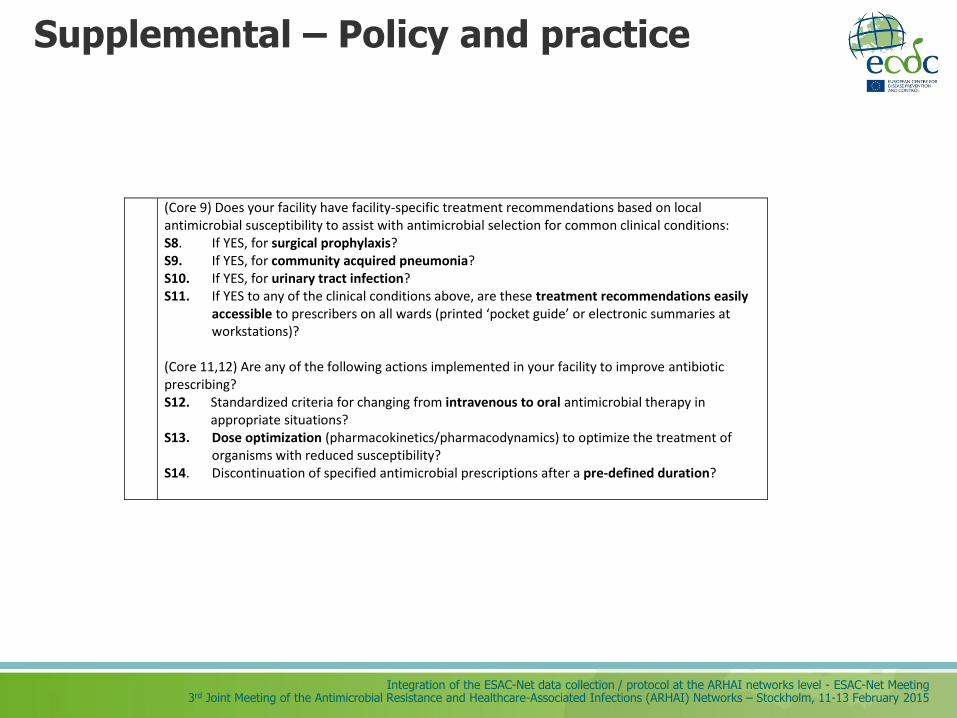
Supplemental – Policy and practice
(Core 9) Does your facility have facility-specific treatment recommendations based on local antimicrobial susceptibility to assist with antimicrobial selection for common clinical conditions: S8. If YES, for surgical prophylaxis? S9. If YES, for community acquired pneumonia? S10. If YES, for urinary tract infection? S11. If YES to any of the clinical conditions above, are these treatment recommendations easily accessible to prescribers on all wards (printed ‘pocket guide’ or electronic summaries at workstations)? (Core 11,12) Are any of the following actions implemented in your facility to improve antibiotic prescribing? S12. Standardized criteria for changing from intravenous to oral antimicrobial therapy in
appropriate situations? S13. Dose optimization (pharmacokinetics/pharmacodynamics) to optimize the treatment of organisms with reduced susceptibility? S14. Discontinuation of specified antimicrobial prescriptions after a pre-defined duration?
Integration of the ESAC-Net data collection / protocol at the ARHAI networks level - ESAC-Net Meeting 3rd Joint Meeting of the Antimicrobial Resistance and Healthcare-Associated Infections (ARHAI) Networks – Stockholm, 11-13 February 2015
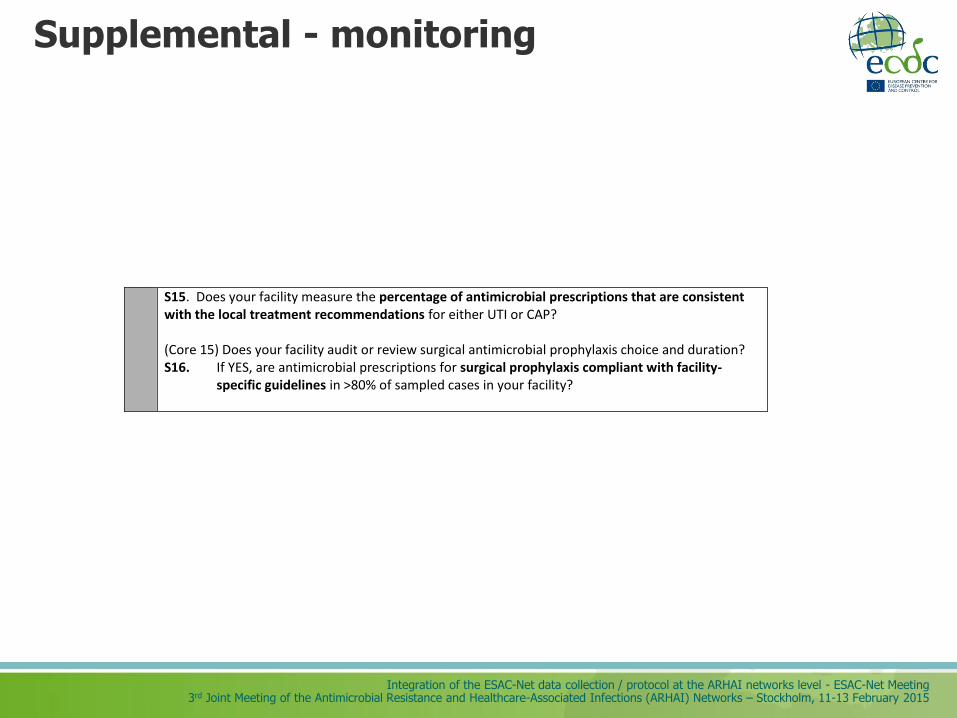
Supplemental - monitoring
S15. Does your facility measure the percentage of antimicrobial prescriptions that are consistent with the local treatment recommendations for either UTI or CAP? (Core 15) Does your facility audit or review surgical antimicrobial prophylaxis choice and duration? S16. If YES, are antimicrobial prescriptions for surgical prophylaxis compliant with facility-
specific guidelines in >80% of sampled cases in your facility?