antibody responses and viral load in patients with crimean-congo hemorrhagic fever: a comprehensive...
TRANSCRIPT

�������� ����� ��
Antibody Responses and Viral Load in Patients with with Crimean-CongoHemorrhagic Fever: A Comprehensive Analysis During the Early Stages ofthe Infection
Koray Ergunay, Zeliha Kocak Tufan, Cemal Bulut, Sami Kinikli, AliPekcan Demiroz, Aykut Ozkul
PII: S0732-8893(14)00005-4DOI: doi: 10.1016/j.diagmicrobio.2013.12.015Reference: DMB 13506
To appear in: Diagnostic Microbiology and Infectious Disease
Received date: 7 October 2013Revised date: 23 December 2013Accepted date: 26 December 2013
Please cite this article as: Ergunay Koray, Tufan Zeliha Kocak, Bulut Cemal, KinikliSami, Demiroz Ali Pekcan, Ozkul Aykut, Antibody Responses and Viral Load in Patientswith with Crimean-Congo Hemorrhagic Fever: A Comprehensive Analysis During theEarly Stages of the Infection, Diagnostic Microbiology and Infectious Disease (2014), doi:10.1016/j.diagmicrobio.2013.12.015
This is a PDF file of an unedited manuscript that has been accepted for publication.As a service to our customers we are providing this early version of the manuscript.The manuscript will undergo copyediting, typesetting, and review of the resulting proofbefore it is published in its final form. Please note that during the production processerrors may be discovered which could affect the content, and all legal disclaimers thatapply to the journal pertain.

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT 1
Antibody Responses and Viral Load in Patients with with Crimean-Congo Hemorrhagic Fever:
A Comprehensive Analysis During the Early Stages of the Infection
Running Title: Antibody response and viral load in CCHF
Koray Ergunay1 , Zeliha Kocak Tufan2, Cemal Bulut3, Sami Kinikli3, Ali Pekcan Demiroz3, Aykut Ozkul4
1Hacettepe University; Faculty of Medicine, Department of Medical Microbiology, Virology Unit, Ankara, TURKEY
2Yıldırım Beyazıt University, Ankara Ataturk Training and Research
Hospital, Infectious Diseases and Clinical Microbiology Department, Ankara, TURKEY
3 MOH Ankara Training and Research Hospital, Infectious
Diseases and Clinical Microbiology Department, Ankara, TURKEY 4 Ankara University; Faculty of Veterinary Medicine, Department of
Virology, Ankara, TURKEY
Author for Correspondence:
Koray Ergunay MD PhD
Hacettepe University Faculty of Medicine Department of Medical Microbiology, Virology Unit
Morphology Building 3rd floor 06100 Sihhiye Ankara TURKEY Phone: 90 312 305 15 60-131
Fax: 90 312 311 52 50 Email:[email protected]
The findings of this study have been submitted as an abstract to the
24th ECCMID Congress to be held in 10-13th May, 2014 in Barcelona, Spain.

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT 2
Abstract
This study was performed to assess viral load, viral nucleocapsid (N) and
glycoprotein precursor (GPC) antibodies in consecutive samples obtained
from Crimean Congo hemorrhagic fever (CCHF) patients to reveal viral
replication kinetics and antiviral immune responses during the early stages of
the infection. Among 116 samples from 20 individuals, 43.9% and 76.7% were
positive for viral RNA and IgM/IgG antibodies, respectively, whereas both
markers could be detected in 22.4%. Mean duration of viremia was 3 days
(range:1-6 days). N-IgM antibodies were identified as the initial serological
marker during the infection, becoming detectable in a median of 2-3 days after
disease onset, followed by GPC-IgM (4-6 days) and IgG antibodies (5-6
days). Clearance of viremia followed or coincided N-IgM response. Partial S
gene sequences amplified in viremic patients were identical or closely-related
to previously-characterized strains and grouped within European Lineage I
group II viruses via neighbor-joining analysis without significant aminoacid
substitutions.
Keywords: Crimean Congo Hemorrhagic Fever, CCHF, antibody, viral load,
immune response
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT 3
1.Introduction
Crimean Congo hemorrhagic fever (CCHF) is a severe human
infection, characterized by a febrile disease with headache, myalgia/arthralgia
and petechial rash, which may be followed by signs of hemorrhagic diathesis,
disseminated intravascular coagulation and circulatory shock due to
microvascular instability and impaired hemostasis (Akıncı et al, 2013). The
case fatality rates in CCHF demonstrate a notable geographical variation but
can be as high as 50% (Whitehouse, 2004; Ergonul, 2012). The causative
agent, Crimean Congo hemorrhagic fever virus (CCHFV), classified in the
Nairovirus genus of Bunyaviridae family, is an enveloped virus with a
segmented negative sense RNA genome, encoding the viral nucleocapsid,
envelope glycoproteins and replicase, along with accessory proteins (Plyusnin
et al, 2011). In nature, CCHFV circulates in an enzootic tick-vertebrate-tick
cycle. The major transmission route of CCHFV to susceptible vertebrates is
via bites of infected ticks, usually belonging to the Hyalomma genus.
Moreover, infections may occur by contact with blood, blood-containing body
fluids or tissues of viremic livestock or humans during the acute phase of the
infection (Whitehouse, 2004; Ergonul, 2012). CCHF is the most widespread
infection among medically-important tick-borne viral infections and cases as
well as outbreaks have been described in parts of Africa, Asia, Eastern
Europe and Middle East; in accordance with the distribution of tick species
acting as vectors (Ergonul, 2012). Although viremia with subsequent
seroconversion can be detected in animals, there is no evidence that the
infection manifests with clinical disease in vertebrates other than humans.
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT 4
Subclinical infections are also common in humans and may constitute over
80% of the virus exposures in endemic regions (Bodur et al, 2012)
A rapid diagnosis of CCHF is essential to initiate the appropriate
treatment protocol and employ management precautions including patient
isolation, which is especially pertinent as CCHF virus has a propensity to
cause severe nosocomial outbreaks (van Eeden et al, 1985; Mardani et al,
2009). Like in many viral infections, virus isolation is considered as the gold
standard diagnostic method in CCHF (Ergonul, 2012; Vanhomwegen et al,
2012). However, the requirement of a high-containment biosafety level 4
facility often renders this approach unpractical for routine use. Moreover, a
high level of viremia, usually encountered during the first 5 days of infection,
required for a successful cell culture or suckling mice inoculation further
restricts the use of virus isolation techniques (Vanhomwegen et al, 2012).
Therefore, detection viral nucleic acids or immune response is often employed
for the specific diagnosis of CCHV. The methods include conventional and
real-time quantitative reverse transcription PCR (RT-PCR and qRT-PCR) for
detection of the viral genome (Drosten et al, 2003; Cevik et al, 2007; Duh et
al, 2007) and indirect immunofluorescence assays (IFAs) or enzyme-linked
immonusorbent assays (ELISAs) for detection of antibodies (Saijo et al, 2002;
Emmerich et al, 2010; Dowall et al, 2012). In this study, viral load and IgM-IgG
antibodies were investigated in consecutive samples obtained from CCHF
patients with acute CCHF infection to reveal viral replication dynamics and
antiviral immune responses during the early stages of the infection.
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT 5
2. Materials and Methods
2.1. Setting and Clinical Samples:
The study was conducted in the Ankara Training and Research
Hospital, a 670-bed tertiary care teaching hospital which serves as one of the
reference centers for CCHF patients in Central Anatolia. The study protocol
was approved by the local ethics board (13.07.11/0426).
During May-August 2012, individuals referred to the institution with a
preliminary diagnosis of CCHF were evaluated for the study. All patients
originated from different locations of Kelkit valley, established as a CCHF
endemic region in Turkey (Karti et al, 2004). Criteria for inclusion were the
presence of epidemiological risk factors for CCHF, which comprise recent
history of tick bites, tick contact and/or working in animal husbandry or farm,
or a recent travel to the endemic region, plus clinical and laboratory findings
suggestive of CCHF including fever, headache, myalgia/arthralgia, lethargy,
nausea/vomiting, abdominal pain/diarrhea, and/or hemorrhages along with
thrombocytopenia, leucopenia, elevated liver enzymes (mainly alanine
aminotransferase and aspartate aminotransferase), elevated alkaline
phospatase, gamma glutamyl transferase and/or creatinine kinase. Individuals
suffering from peripheral or cerebral vascular disease, hematological
disorders, cirrhosis, portal hypertension, and malignancies were excluded.
A total of 20 adult patients (10 males and 10 females) with enrolled in
the study with informed consent. The individuals were admitted to the hospital
within 1-10 days of the tick bite and 24-72 hours of disease onset. Starting
with hospital admission, daily serum samples were obtained each day from
the patients, aliquoted and stored in -80ºC for future analyses.
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT 6
2.2. Detection of CCHFV RNA and Viral Load
All samples were subjected to nucleic acid purification and reverse
transcription using random hexamers via commercial assays (High Pure Viral
Nucleic Acid Kit, Roche Diagnostics, Germany; RevertAid First Strand cDNA
Synthesis Kit, Thermo Scientific, Japan) as directed by the manufacturers. For
the quantitative determination of CCHFV RNA, a previously-described
TaqMan-based single-step qRT-PCR was employed with minor modifications
(Yapar et al. 2005). Briefly, sense and antisense primers (50-TCT TYG CHG
ATG AYT CHT TYC-30 and 50-GGG ATK GTY CCR AAG CA-30) and
labeled probe (50-FAM-ACA SRA TCT AYA TGC AYC CTG C-TAMRA-30)
(H: A/C/T, K: G/T, R: A/G, S: G/C, Y: C/T), targeting the S segment of the viral
genome were used for reaction mixture containing 5 l extracted RNA, 5 pmol
of each primer, 4 pmol of labeled probe, 0.2 mM of each deoxyribonucleotide
triphosphate, 6 mM MgCl2 and a mixture of reverse transcriptase (Fermentas,
Vilnius, Lithuania) plus hot start Taq polymerase (Bioron GmBH, Munchen,
Germany) in a total volume of 25 l. Cycling conditions were set as follows: a
single cycle of 30 min at 42 C for reverse transcription followed by 5 min. at
95 C and 45 cycles of 15 s at 95 C and 60 s at 60 C, performed in a Rotor-
Gene 6000 instrument (Corbett Research, Australia) for a 103 bp amplicon.
In each run, plasmid standards with 4x102 to 4x109 copies/ml per reaction
were included for quantitation.
For the characterization of CCHFV partial S gene sequences in
patients, an in house PCR was performed as described previously (Rodriguez
et al. 1997), using a PTC-200 Thermal Cycler (MJ Research, Massachusetts,
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT 7
USA). Amplicons of approximately 520 basepairs from the first PCR round
were visualized by ethidium bromide staining after 1.5% agarose gel
electrophoresis and further characterized by sequencing. For this purpose,
PCR products were cleaned up via High Pure PCR Product Purification Kit
(Roche Diagnostics, Mannheim, Germany), and sequenced using forward and
reverse primers in an ABI Prism 310 Genetic Analyzer (Applied Biosystems,
CA, USA). Obtained sequences were aligned and analyzed using CLC Main
Workbench v5.5 (CLCBio, Aarhus, Denmark).
2.3. Detection of CCHFV Antibodies
Samples were tested for anti-CCHFV IgM and IgG antibodies by a
commercial IFA (Crimean-Congo fever virus mosaic 2, IgM and IgG,
Euroimmun, Luebeck, Germany), performed according to the manufacturer's
recommendations. The IFAs utilize EU90 cells transfected with CCHFV
nucleocapsid (N) and glycoprotein precursor (GPC) separately, as well as
non-transfected cells to differentiate non-specific reactions. For the IgM
detection, interfence in the assay was prevented using IgG-rheumatoid factor
absorbant in the sample dilution buffer as directed by the manufacturer. The
assays were performed at the serum dilution of 1:10 for IgM, 1:100 for IgG
and interpreted via fluorescence microscopy. The positive results were
evaluated as equivalent (+), moderate (++) and strong (+++), according to
visual intensity of fluorescence compared to control sera. The sensitivity and
specificity of the IgM assay is reported as 97.2% and 97.5%, respectively
whereas they are 89.5% and 100% for IgG, respectively. An independent
comparison of various assays have also revealed an overall sensitivity and
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT 8
specificity of 93.9% and 98.9% for IgM and 86.1% and 100% for IgG assays,
respectively (Vanhomwegen et al, 2012).
2.4. Statistical Analysis
Descriptive parameters of the study group, viral load levels,
fluorescence intensities and seroconversion times were assessed via
statistical tests. Student's t, Mann-Whitney U and Fisher's Exact tests were
employed for univariate comparisons whereever appropriate. Statistical
significance was considered as p<0.05 level. All statistical analyses were
performed by SPSS package version 15.0 (SPSS Inc.,USA).
3. Results
3.1. Samples and CCHFV Laboratory Follow-Up
A total of 116 samples from 20 patients (samples per patient:
mean:5.8, median:5, range:3-13) were evaluated in the study. Among the 116
samples tested, 51(43.9%) were positive for viral RNA, 89 (76.7%) were
positive for antibodies, whereas in 26 (26/116, 22.4%), both markers were
reactive (Table 1).
In 9 patients (45%), seroconversion of CCHFV antibodies and
simultaneous or subsequent elimination of viremia could be observed (Figure
1, patients 1-9). In two patients (10%), precise timing of seroconversion and
control of viral replication could not be determined due to missing days of
sampling (Figure 1, patients 10-11). In 6 patients (30%), antibodies were
present in all samples studied, with or without detectable viremia (Figure 1,
patients 12-17). All samples from 3 patients (15%) remained CCHFV RNA
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT 9
negative despite seroconversion in 2 (Figure 1, patients 18 and 19) and
IgM+IgG seroreactivity in 1(Figure 1, patient 20). All patients except patient 2
survived the disease and discharged from the hospital (19/20, 95%).
3.2. CCHFV Viral Loads and S Segment Sequences
Detectable viremia was present in 17 cases (17/20, 85%), which lasted
for a mean of 3 days (median:3, range:1-6). In patients with more than one
viremic sample, mean viral loads on the day of hospital admission and on the
last viral RNA-detectable sample were 2.4 x108 copies/ml and 6.3 x106
copies/ml, respectively (standard deviation: 1.008-1.01 log). The differences
in viral loads were statistically significant (p:0.005).
CCHFV partial S segment sequences were amplified and sequenced
in 11 cases (patients 1-11); from samples acquired on the day of hospital
admission. All samples used for sequence characterization were negative for
CCHFV antibodies. The alignment of the nucleotide sequences demonstrated
similarities ranging from 60.69% to 99.24% among isolates. All sequences
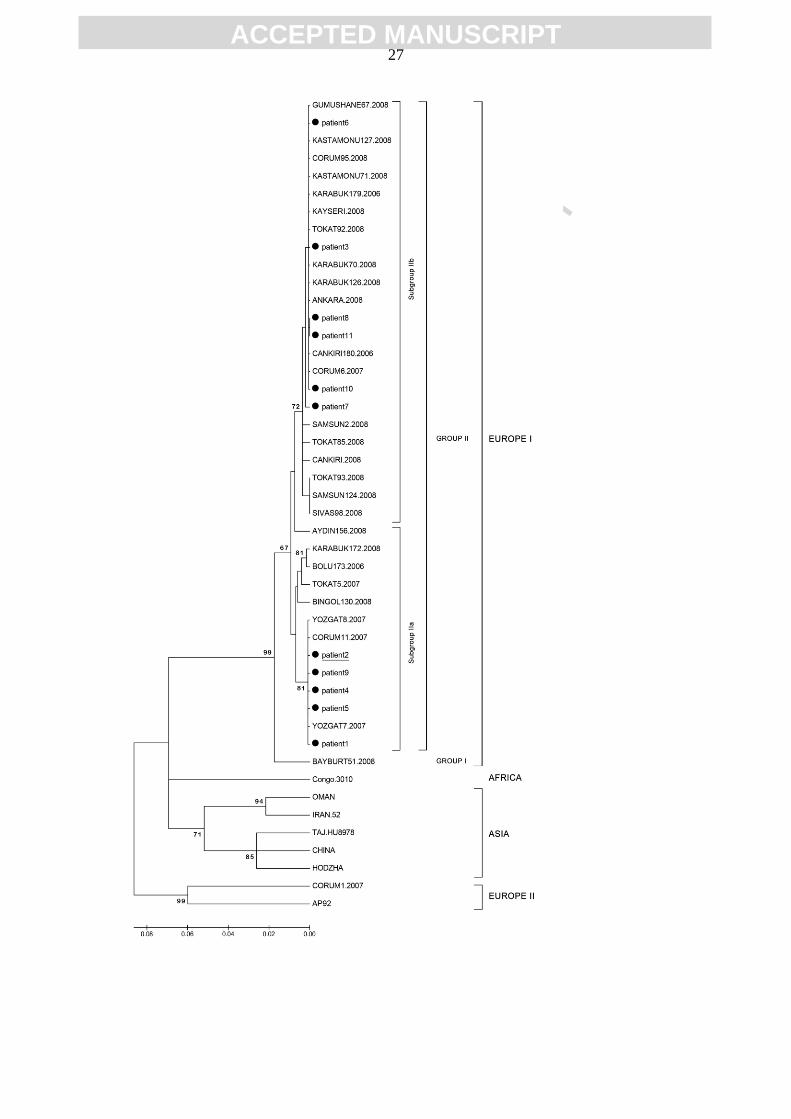
were grouped with CCHFV European Lineage I group II viruses via neighbor-
joining analysis (Figure 3). Comparison of S segment sequences identified in
various provinces of Turkey during 2006-2008 revealed identical or similar
nucleotide compositions and distribution of current sequences in subgroup 2a
and 2b within group I CCHFV strains (Figure 3). Comparison of aminoacid
sequences deduced from the nucleotide sequence demonstrated identical
sequences without aminoacid variations in 10 cases. However, two aminoacid
substitutions in the S segment (R146K and S165T) were identified in patient
6.
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT 10
3.2. Dynamics of CCHFV GPC and N Antibody Responses
Detectable immune responses to CCHFV could be observed in 89
samples (76.7%), originating from all patients studied. IgM antibodies were
present in 26 samples (26/89, 29.2%) that include N-specific responses in 20
and GPC+N responses in 6 samples. In 63 samples (70.8%), IgM and IgG
antibodies were detected simultaneously.
In patients with observed IgM and/or IgG seroconversion, average
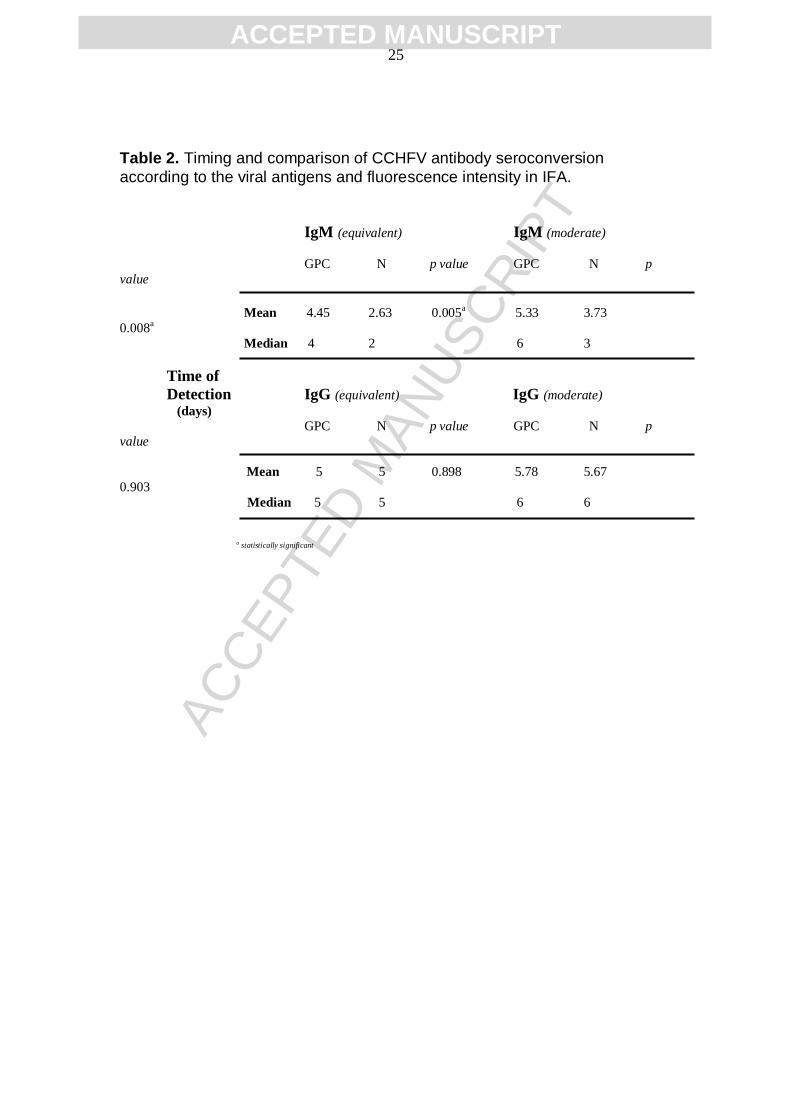
times required for reactivity were calculated (Table 2). Overall, IgM
seroconversion was followed by IgG seroconversion in 1-2 days (mean:1.73,
median:2). Detection of N-IgM was significantly earlier than GPC-IgM,
regardless of the interpreted fluorescence intensity (Table 2). When evaluated
separately as equivalent or moderate IFA results, a statistically-significant
difference in days required for seroconversion was observed for N IgM
(p:0.013), but not for GPC (p:0.170). N-IgM response preceded or coincided
with the clearance of viremia as determined by undetectable CCHFV RNA
levels (Figure 1). For IgG detection, no differences related to viral proteins
(Table 2) or for fluorescence intensities could be revealed (p:0.261 and 0.195,
data not given).
4. Discussion
Emergence or reemergence of CCHF poses a serious public health
threat due to being a highly contagious and potentially lethal infection that is
difficult to treat, prevent, and control, with the potential to cause nosocomial
spread (Ergonul, 2012; Vanhomwegen et al, 2012). Access to early, sensitive,
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT 11
and specific laboratory diagnosis is of paramount importance for increasing
preparedness in countries at risk, as well as for enhanced surveillance and
development of therapeutics (Maltezou et al, 2010). Various in house and
commercial assays have been developed for the detection and/or quantitation
CCHFV RNA and antibodies. However, consensus on the most efficient
molecular and serologic testing method is yet to be reached and early events
during the initial phases of the human infection are relatively less known
(Vanhomwegen et al, 2012, Akinci et al, 2013). This study was performed to
elucidate viral replication kinetics associated with the patterns of antibody
responses to different viral antigens in individuals with CCHFV infection
during the early stages of the disease.
Twenty patients with the history of tick bites and the clinical diagnosis
of CCHF were enrolled in the study during 2012. A total of 116 samples from
the patients were investigated via a well-characterized single-step qRT-PCR
for viral RNA quantitation and a commercial IFA to detect IgM-IgG antibodies
against viral GPC and N proteins. Samples from selected cases were further
amplified via an in house PCR assay for partial characterization of S segment
of the viral genome. Various phases of the disease were observed in the
patients. Detectable viremia with relatively high viral loads and subsequent
elimination of circulating viruses via specific immune response were identified
in the majority of the cases (Figure 1). Mean duration of the viremia was 3
days and statistically-significant declines in viral load levels were
demonstrated between the initial and last viremic samples. In two patients,
viral RNA could not be demonstrated despite early sampling and subsequent
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT 12
seroconversion (patients 18 and 19, Figure 1). Initial samples from these
patients might have suffered from PCR inhibitors.
In the study, clearance of viremia was associated with IgM response to
N protein, which frequently became reactive prior to the reduction of the viral
load to undetectable levels (Figure 1). Moreover, N-IgM antibodies were
identified as the initial serological marker during the infection, appearing in a
median of 2-3 days in IFA, significantly earlier than GPC-IgM antibodies. This
observation is further supported by the comparison of the results of various
fluorescence intensities (Table 2). Evidence for a robust N-IgM response is
indirectly provided by the significant increase for the time required for a
detectable elevation in fluorescence (2.63 versus 3.73 days, Table 2). IgG
seroconversion emerged after 1-2 days following the IgM responses. No
significant variations in GPC or N-IgG antibodies according to fluorescence
intensity were demonstrated. A relatively later phase of the infection were
observed in 6 patients, where IgG and/or IgM antibodies were reactive in all
evaluated samples (Figure 1). However, similar dynamics for IgG
seroconversion were noted.
Previous reports indicate that IgM and IgG antibodies are detectable in
CCHFV infection from about 7-9 days after the onset of disease (Shepherd et
al, 1989). However, IgM antibodies are reported to be present as early as day
5 and when viremia is also evident (Tang et al, 2003; Saijo et al, 2005).
Maximum antibody titers were usually attained in the 2nd to 3rd week of
illness. Specific IgM declines to undetectable levels by 4 months post-
infection, and IgG remains detectable for at least 5 years (Shepherd et al,
1989; Ergonul, 2006). Our findings demonstrate that seroconversion can be
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT 13
detected during 2nd to 6th day of hospital admission using currently-
developed assays, depending on the antigens used. Emergence of IgG also
follows a rapid course and both antibodies could be identified during the 2nd
week. In this study, a highly-sensitive and specific commercial IFA was
employed. Generally, IFA is considered to be relatively more labor-intensive
due to the requirement of the individual examination of all samples under the
fluorescent microscope and the interpretation can vary according to the
microscopist. However, it enables the interpretation of fluorescence patterns
that may be useful to differentiate positive from cross-reactive samples, a
clear advantage over ELISA (Vanhomwegen et al, 2012).
The fatality rates in individuals with CCHF range between 5% and 30%,
depending on geographic region and route of entry (Jamil et al. 2005, Akinci
et al, 2013). The outcome of the disease has been shown to be correlated
with viral load as well as certain laboratory and clinical parameters such as
platelet count, hepatic enzyme and fibrinogen levels, presence of
somnolence, gastrointestinal bleeding and others (Akinci et al, 2013). The
fatality rate in this study was 1/20 (5%), comparable to the rates reported from
Turkey during 2003-2009 (4.5-6.2%) (Ergunay et al, 2011). The fatal case
observed in the study had the highest initial viral load (2.36 x 109 copies/ml)
which remained within 108-109 range during follow-up (Figure 1A, Patient 2).
Previous studies have indicated viral load as a strong predictor of clinical
outcome in CCHF patients (Cevik et al, 2007; Duh et al, 2007). However,
suggested viral load thresholds vary according to the rRT-PCR set-up,
probably due to the variations of sensitivity and the lack of consensus
quantitation standards. Nevertheless, a viral load exceeding 109 copies/ml is
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT 14
widely considered as a severe infection with impending mortality (Cevik et al,
2007; Duh et al, 2007). Interestingly, in the patient with the fatal outcome,
GPC-IgM and IgG responses could be mounted during the disease course,
but viral replication could not be limited (Figure 1, Patient 2). These findings
further support the impact of N-IgM response in controlling viral replication.
Generally, antibodies against viral glycoproteins demonstrate a neutralizing
effect, preventing viral attachment and entry into uninfected cells and further
promoting immune clearance. Neverheless, data from various phleboviruses
suggest that in Bunyaviruses, neutralization is a complex phenomenon
involving a number antigenic epitopes. Even the majority of the exposed
persons develop antibodies against linear epitopes of N protein, the immune
response against viral glycoproteins, which directly affects virus neutralization
in vitro, display considerable variations (Besselaar and Blackburn 1991, Di
Bonito et al, 2002). This is consistent with the previous data that most of the
CCHF patients developed relatively low levels of neutralizing antibodies
(1:8 to 1:32 by fluorescent-focus reduction tests), while titers of 1:256 to
1:512 could be observed in some individuals (Shepherd et al, 1989).
The main limitation of this study is that relatively mild or non-fatal cases of
CCHF constitute the majority in the study group. Although this enabled
precise detection of antiviral immune responses suppressing viral replication,
GPC and N responses and their relation to viremia could not be evaluated in
cases with viral loads over 109 copies/ml. For a comprehensive understanding
of in vivo CCHFV neutralization, which will potentially influence the
therapeutic use of convescelent sera in patients, neutralizing antibody titers
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT 15
for viral glycoprotein and nucleocapsid antigens must be evaluated in cases
with higher viral loads in future efforts.
Seven lineages of CCHFV, distributed according to distinct
geographical locations exist (Deyde et al. 2006). Previous analyses of partial
CCHFV sequences in ticks and affected individuals demonstrated that the
majority of the virus strains in Turkey are closely-related and belonged to the
European lineage I (Ozkaya et al, 2010; Kalaycioglu et al, 2012). The S-
segment sequences were observed to be suitable for assessments of
genomic variations. Moreover, local viruses could be grouped in two main
clusters in which two subgroups were also distinguishable (Ozkaya et al.
2010). In Central Anatolia, both subgroups were observed to be prevalent,
regardless of the location (Ozkaya et al. 2010). Partial sequences
characterized in this study are also consistent with these findings, as
sequences identical or similar to subgroup IIa and IIb were distributed in the
cases (Figure 2). In Turkey, AP92-like strains, grouped within European
lineage II viruses, have also been identified in the Thrace region as well as
Corum province in Central Anatolia (Midilli et al, 2009; Ozkaya et al, 2010).
Originally characterized in Greece and associated with low pathogenicity,
AP92 and closely-related CCHFV strains have not been detected in Central
Anatolia during 2009-2010 (Kalaycioglu et al, 2012), as well as in this study
(Figure 2). In CCHFV, variations in the S segment of the viral genome, that
codes for the nucleocapsid protein, may affect individual immune response as
well diagnostic assays targeting the nucleocapsid (Dowall et al, 2012).
Although sequence diversity in CCHFV isolates in this study have been
observed, aminoacid substitutions (R146K and S165T) were only detected in

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT 16
one CCHFV case, with indistinguishable antibody/viral load kinetics and
clinical presentation (Figure 1, patient 6). Remarkable variations have
previously been revealed among the CCHFV isolates in Turkey and low-rate
homologous recombination events have been proposed to affect amino acids
155-200 of the S segment, according to yearly analysis of corresponding
peptide regions (Ozkaya et al, 2010). It is likely that the aminoacid
substitutions identified in this study in a single case without any impact on
diagnostics or prognosis reflect the occurance of such events.
In conclusion, N-IgM antibodies appear as the initial serological marker
and become detectable earlier than GPC-IgM during the course of CCHF
infection. N-IgM response also correlates with the control of viral replication.
IgM antibodies are rapidly followed by IgG responses to GPC and N. In the
single fatal case, an initial viral load exceeding 109 copies/ml and GPC-
IgM/IgG were noted, lacking N responses. Further data are required to assess
the impact of GPC/N responses during in vivo virus neutralization and in
patients with very high viral loads.
Acknowledgements
The CCHFV IFA employed in this study were kindly provided by
EuroImmun, Turkey. The company and the representatives had no
involvement in study design, performance or evaluation of the assays and
interpretation of the results. The authors declare no competing interests and
are grateful to N.Emin Guven for graphics.
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT 17
References
Akıncı E, Bodur H, Leblebicioglu H (2013) Pathogenesis of Crimean-Congo
hemorrhagic fever. Vector Borne Zoonotic Dis. 13:429-437.
Besselaar TG, Blackburn NK (1991) Topological mapping of antigenic sites on
the Rift Valley fever virus envelope glycoproteins using monoclonal
antibodies. Arch Virol. 121:111-124.
Bodur H, Akinci E, Ascioglu S, Öngürü P, Uyar Y (2012) Subclinical infections
with Crimean-Congo hemorrhagic fever virus, Turkey. Emerg Infect Dis.
18:640-642.
Cevik MA, Erbay A, Bodur H, Eren SS, Akinci E, Sener K, Ongürü P, Kubar A
(2007) Viral load as a predictor of outcome in Crimean-Congo hemorrhagic
fever. Clin Infect Dis. 45:E96-100.
Deyde VM, Khristova ML, Rollin PE, Ksiazek TG, Nichol ST (2006). Crimean-
Congo hemorrhagic fever virus genomics and global diversity. J Virol.
80:8834-8842.
Di Bonito P, Bosco S, Mochi S, Accardi L, Ciufolini MG, Nicoletti L et al.
(2002) Human antibody response to Toscana virus glycoproteins expressed
by recombinant baculovirus. J Med Virol. 68:615-619.
Dowall SD, Richards KS, Graham VA, Chamberlain J, Hewson R (2012)
Development of an indirect ELISA method for the parallel measurement of
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT 18
IgG and IgM antibodies against Crimean-Congo haemorrhagic fever (CCHF)
virus using recombinant nucleoprotein as antigen. J Virol Methods. 179:335-
341.
Drosten C, Kümmerer BM, Schmitz H, Günther S (2003) Molecular
diagnostics of viral hemorrhagic fevers. Antiviral Res. 57:61-87.
Duh D, Saksida A, Petrovec M, Ahmeti S, Dedushaj I, Panning M, et al. Viral
load as predictor of Crimean-Congo hemorrhagic fever outcome. Emerg Infect
Dis. 2007;13:1769–72.
Emmerich P, Avsic-Zupanc T, Chinikar S, Saksida A, Thome-Bolduan C,
Parczany-Hartmann A, et al. Early serodiagnosis of acute human Crimean-
Congo hemorrhagic fever virus infections by novel capture assays. J Clin
Virol. 2010;48:294-295.
Ergonul O (2006). Crimean-Congo haemorrhagic fever. Lancet Infect Dis.
6:203-214.
Ergonul O (2012) Crimean-Congo hemorrhagic fever virus: new outbreaks,
new discoveries. Curr Op Virol 2:215-220.
Ergunay K, Whitehouse CA, Ozkul A (2011) Current status of human arboviral
diseases in Turkey. Vector Borne Zoonotic Dis. 11:731-741.

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT 19
Jamil B, Hasan RS, Sarwari AR, Burton J, Hewson R, Clegg C (2005)
Crimean-Congo hemorrhagic fever: Experience at a tertiary care hospital in
Karachi, Pakistan. Trans R Soc Trop Med Hyg. 99:577-584.
Kalaycioglu AT, Durmaz R, Uyar Y, Unaldi O, Aksekili E, Ozkul A et al.
(2012). Lack of genetic diversity in Crimean-Congo hemorrhagic fever viruses
in Turkey: assessment of present and future patterns of disease. J Med Virol.
84:471-478.
Karti SS, Odabasi Z, Korten V, Yilmaz M, Sonmez M, Caylan R et al. (2004).
Crimean-Congo hemorrhagic fever in Turkey. Emerg Infect Dis. 10:1379-
1384.
Maltezou HC, Andonova L, Andraghetti R, Bouloy M, Ergonul O, Jongejan F,
et al. (2010) Crimean-Congo hemorrhagic fever in Europe: current situation
calls for preparedness. Euro Surveill. 15:19504.
Mardani M, Keshtkar-Jahromi M, Ataie B, Adibi P (2009) Crimean-Congo
hemorrhagic fever virus as a nosocomial pathogen in Iran. Am J Trop Med
Hyg. 81:675–678.
Midilli K, Gargili A, Ergonul O, Elevli M, Ergin S, Turan N et al (2009).The first
clinical case due to AP92 like strain of Crimean-Congo Hemorrhagic Fever
virus and a field survey. BMC Infect Dis. 9:90.
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT 20
Plyusnin A, Beaty BJ, Elliott RM, Goldbach R, Kormelink R, Lundkvist A,
Schmaljohn CS, Tesh RB. Bunyaviridae. In: King AMQ, Lefkowitz E, Adams
MJ, Carstens EB, editors. Virus taxonomy: classification and nomenclature of
viruses. Ninth Report of the International Committee on Taxonomy of Viruses.
San Diego: Elsevier. 2011. p. 693–709.
Ozkaya E, Dincer E, Carhan A, Uyar Y, Ertek M, Whitehouse CA et al. (2010)
Molecular epidemiology of Crimean-Congo haemorrhagic fever virus in
Turkey: occurence of local topotype. Virus Res. 149:64-70.
Rodriguez LL, Maupin GO, Ksiazek TG, Rollin PE, Khan AS, Schwarz TF et
al. (1997) Molecular investigation of a multisource outbreak of Crimean-
Congo hemorrhagic fever in the United Arab Emirates. Am J Trop Med Hyg
57:512–518.
Saijo M, Qing T, Niikura M, Maeda A, Ikegami T, Sakai K, et al. Immunofl
uorescence technique using HeLa cells expressing recombinant nucleoprotein
for detection of immunoglobulin G antibodies to Crimean-Congo hemorrhagic
fever virus. J Clin Microbiol. 2002;40:372-375.
Saijo M, Tang Q, Shimayi B, Han L, Zhang Y, Asiguma M et al (2005)
Recombinant nucleoprotein-based serological diagnosis of Crimean-Congo
hemorrhagic fever virus infections. J Med Virol. 75:295-299.
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT 21
Shepherd AJ, Swanepoel R, Leman PA (1989) Antibody response in
Crimean-Congo hemorrhagic fever. Rev Infect Dis. 11:S801-S806.
Tang Q, Saijo M, Zhang Y, Asiguma M, Tianshu D, Han L et al. (2003) A
patient with Crimean-Congo hemorrhagic fever serologically diagnosed by
recombinant nucleoprotein-based antibody detection systems. Clin Diagn Lab
Immunol. 10:489-491.
Vanhomwegen J, Alves MJ, Zupanc TA, Bino S, Chinikar S, Karlberg H, et al
.(2012) Diagnostic assays for Crimean-Congo hemorrhagic fever. Emerg
Infect Dis. 18:1958-1965.
van Eeden PJ, van Eeden SF, Joubert JR, King JB, van de Wal BW, Michell
WL (1985) A nosocomial outbreak of Crimean-Congo haemorrhagic fever at
Tygerberg Hospital. Part II. Management of patients. S. Afr. Med. J. 68, 718-
721.
Whitehouse CA (2004) Crimean-Congo hemorrhagic fever. Antiviral Res.
64:145-160.
Yapar M, Aydogan H, Pahsa A, Besirbellioglu BA, Bodur H, Basustaoglu AC,
Guney C, Avci IY, Sener K, Setteh MH, Kubar A (2005) Rapid and
quantitative detection of Crimean-Congo hemorrhagic fever virus by one-step
real-time reverse transcriptase-PCR. Jpn J Infect Dis. 58:358-362.
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT 22
Table and Figure Legends:
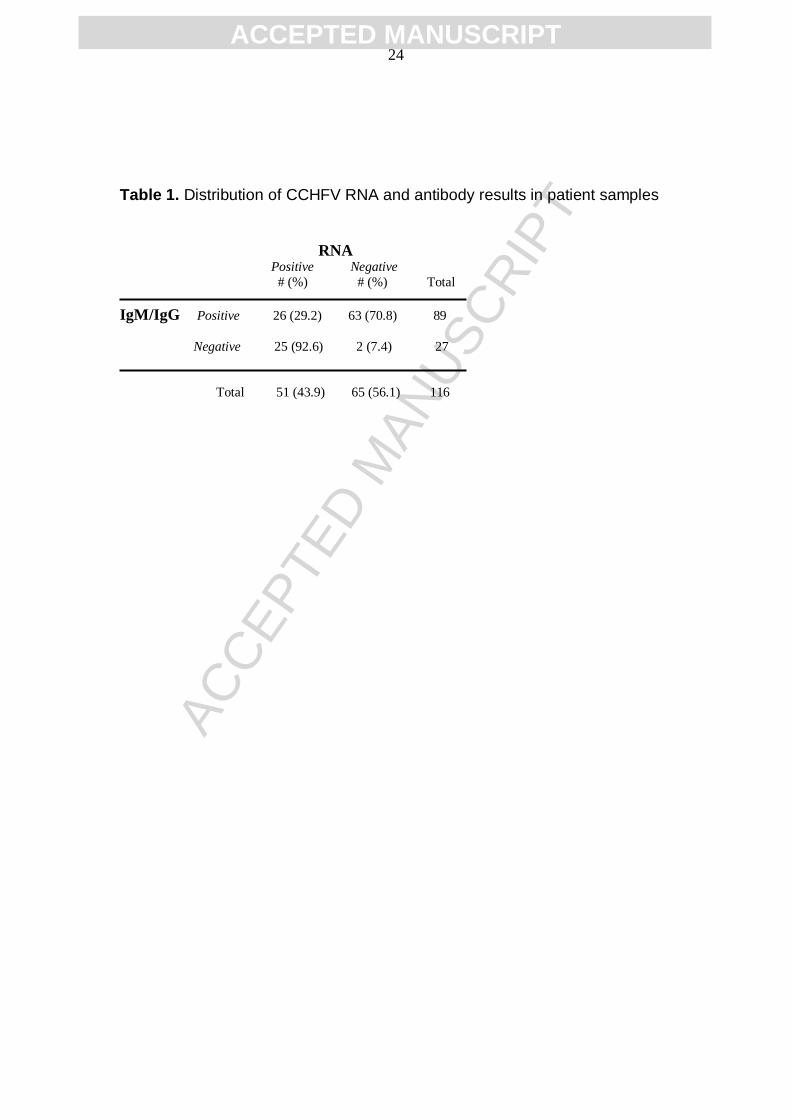
Table 1. Distribution of CCHFV RNA and antibody results in patient samples
Table 2. Timing and comparison of CCHFV antibody seroconversion
according to the viral antigens and fluorescence intensity in IFA.
Figure 1: CCHFV viral load and GPC-N antibody responses according to the
sampling times. Viral loads were given as copies/ml and antibody titers in IFA
were interpreted as equivalent:+, moderate:++, strong:+++/++++) (N/A:not
available). Patient with the fatal outcome is underlined (Patient 2).
Figure 2: Phylogenetic analysis of the partial S segment sequences identified
in the study (●) with related local and global sequences. Numbers at the
nodes indicate bootstrapping values. Bars represent nucleotide substitutions
per position. Local sequences are represented with location, strain number
and year of isolation. GeneBank accession numbers of the isolates are:
OMAN: DQ211645, IRAN-52: DQ446212, CHINA: AF358784, HODZHA:
AY223475, TAJ.Hu8978: AY297691, CONGO.3010: DQ144418,
AP92:DQ211638, CORUM1.2007: FJ601872, GUMUSHANE67.2008:
FJ601848, KASTAMONU127.2008: FJ601855, CORUM95.2008: FJ601884,
KASTAMONU71.2008: FJ601850, KARABUK179.2006: FJ601866,
KAYSERI.2008: FJ601891, TOKAT92.2008: FJ601882, KARABUK70.2008:
FJ601866, KARABUK126.2008: FJ601854, ANKARA.2008: FJ601893,
CANKIRI180.2006: FJ601867, CORUM6.2007: FJ601876, SAMSUN2.2008:
FJ601861, TOKAT85.2008: FJ601880, CANKIRI.2008: FJ601890,
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT 23
TOKAT93.2008: FJ601883, SAMSUN124.2008: FJ601894, SIVAS98.2008:
FJ601885, AYDIN156.2008: FJ601896, KARABUK172.2008: FJ601860,
BOLU173.2006: FJ601863, TOKAT5.2007: FJ601878, BINGOL130.2008:
FJ601856, YOZGAT8.2007: FJ601870, CORUM11.2007: FJ601873,
YOZGAT7.2007: FJ601871, BAYBURT51.2008: FJ601847, Patient1:
KF705528, Patient2: KF705527, Patient3: KF705529, Patient4: KF705535,
Patient5: KF705531, Patient6: KF705536, Patient7: KF705533, Patient8:
KF705526, Patient9: KF705532, Patient10: KF705534, Patient11: KF705530)
Sequence from the patient with the fatal outcome is underlined (Patient 2).
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT 24
Table 1. Distribution of CCHFV RNA and antibody results in patient samples
RNA Positive Negative
# (%) # (%) Total
IgM/IgG Positive 26 (29.2) 63 (70.8) 89
Negative 25 (92.6) 2 (7.4) 27
Total 51 (43.9) 65 (56.1) 116
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT 25
Table 2. Timing and comparison of CCHFV antibody seroconversion
according to the viral antigens and fluorescence intensity in IFA.
IgM (equivalent) IgM (moderate)
GPC N p value GPC N p
value
Mean 4.45 2.63 0.005a 5.33 3.73
0.008a
Median 4 2 6 3
Time of
Detection IgG (equivalent) IgG (moderate)
(days)
GPC N p value GPC N p
value
Mean 5 5 0.898 5.78 5.67
0.903
Median 5 5 6 6
a statistically significant

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT 26
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT 27