anticholinergic, antidepressant, antipsychotic drug toxicity4_anticholinergic... · block, and...
TRANSCRIPT
Dr.Bushra H. MaroufUniversity of Sulaimani-College of Pharmacy
Anticholinergic, Antidepressant, Antipsychotic drug Toxicity
November 14, 2018 Clinical Toxicology 5th year -Lec 3,4 1
34
Overview
l Anticholinergics l Antidepressants (Tricyclic, Newer non cyclic) l Antipsychotics , Neuroleptics (Typical..,Atypical..)
November 14, 2018 Clinical Toxicology 5th year -Lec 3,4 2
Introduction
l Anticholinergic (Antimuscarinic, cholinergic-blocking) activity is one of the most common adverse actions associated with numerous drugs including TCA and APD
l Anticholinergics competitively inhibit action of the neurotransmitter Ach at central and peripheral receptor sites (both muscarinic and nicotinic)
l Quaternary derivatives do not enter CNS, thus their action is directed more toward peripheral rather than central.
l Today, poisoning by these drugs are less common because these drugs are not used as frequently in drug therapy.
November 14, 2018 Clinical Toxicology 5th year -Lec 3,4 3
Drugs that have anticholinergic properties
l Despite the decline in popularity of classic anticholinergic, many poisonings from drugs that have a potent anticholinergic properties continue to be reported ,these drugs include:
l Antihistamines, l Phenothiazines, l TCA, l Gastrointestinal anticholinergic , l Antiparkinson drugs.
November 14, 2018 Clinical Toxicology 5th year -Lec 3,4 4
November 14, 2018 Clinical Toxicology 5th year -Lec 3,4 5
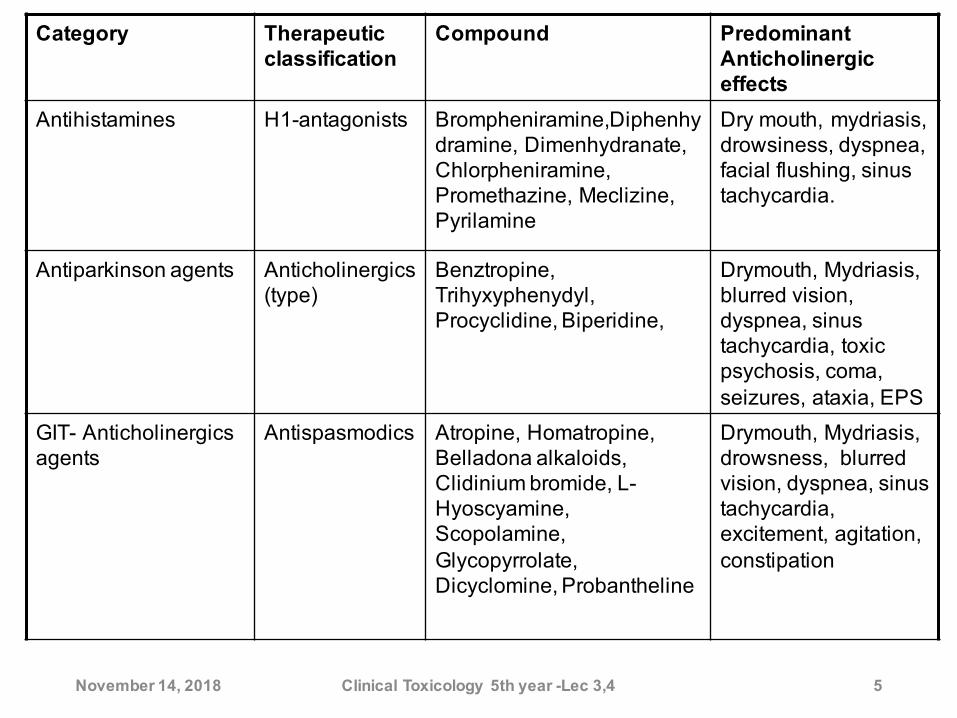
Predominant Anticholinergic effects
CompoundTherapeutic classification
Category
Dry mouth, mydriasis, drowsiness, dyspnea, facial flushing, sinus tachycardia.
Brompheniramine,Diphenhydramine, Dimenhydranate, Chlorpheniramine, Promethazine, Meclizine, Pyrilamine
H1-antagonists Antihistamines
Drymouth, Mydriasis, blurred vision, dyspnea, sinus tachycardia, toxic psychosis, coma, seizures, ataxia, EPS
Benztropine, Trihyxyphenydyl, Procyclidine, Biperidine,
Anticholinergics (type)
Antiparkinson agents
Drymouth, Mydriasis, drowsness, blurred vision, dyspnea, sinus tachycardia, excitement, agitation, constipation
Atropine, Homatropine, Belladona alkaloids, Clidinium bromide, L-Hyoscyamine, Scopolamine, Glycopyrrolate, Dicyclomine, Probantheline
Antispasmodics GIT- Anticholinergics agents
November 14, 2018 Clinical Toxicology 5th year -Lec 3,4 6
Antidepressants
Tricyclicantidepressant (TCA)
Selective reuptake inhibitors
TCA
l These agents used in the treatment of depression.
l The name derived from their structure, since it consist of three rings except maprotline which consist of four rings, but, still all known as tricyclic antidepressants (TCAs).
l This group posses anticholinergic activity, and a greater degree of CNS sedative activity.
November 14, 2018 Clinical Toxicology 5th year -Lec 3,4 7
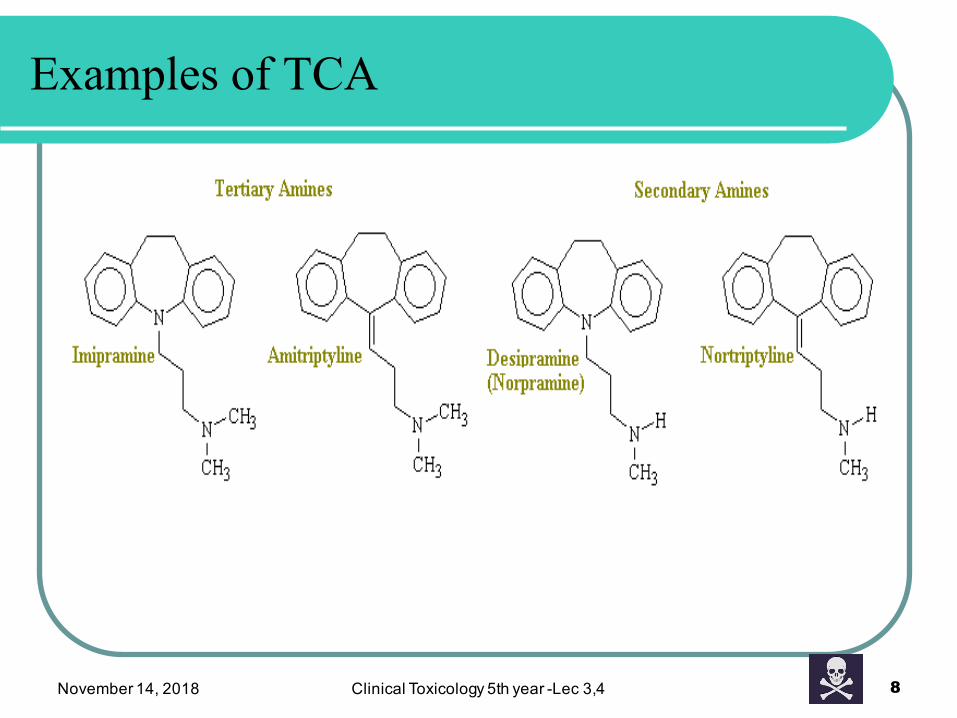
Examples of TCA
November 14, 2018 Clinical Toxicology 5th year -Lec 3,4 8
• Toxicitiesresultfrombothaccidentalorintentional.
• TCAarecommonlyprescribedassecond-lineagentandforotherindicationslikechronicpain
• Amitriptylineisthemajoragentthatproducetoxicity.Thisisfollowedbydoxepinthenimipraminethendesipramine.
• MostcasesoftoxicitymainlyduetoconcomitantadministrationofTCAsandotherCNSdepressants.
November 14, 2018 Clinical Toxicology 5th year -Lec 3,4 9
TCA
ToxicitywithTCAsislifethreatening
l TCAs have low margin of safety.l Patients taking TCAs medication have a high risk for
suicide.l Most Poisoning involve multiple ingestion with other
drugs (ethanol, diazepam, propoxyphen, codeine)l TCAs are rapidly absorbed, tightly bind to plasma protein
and tissues, and undergo enterohepatic recycling l Children are sensitive to cardiovascular complication and
seizure activities.
November 14, 2018 Clinical Toxicology 5th year -Lec 3,4 10
November 14, 2018 Clinical Toxicology 5th year -Lec 3,4 11
Toxic dose ?
l Large Variations exist in adult toxic doses?
November 14, 2018 Clinical Toxicology 5th year -Lec 3,4 12
Toxic dose?
l Most of TCAs have a narrow therapeutic index. so that doses of less than 10 times the therapeutic daily dose may produce severe intoxication.
l In general ingestion of 10-20mg/kg is potentially life-threatening.
November 14, 2018 Clinical Toxicology 5th year -Lec 3,4 13
Toxicokinetics
l Tricyclic antidepressant drugs are rapidly absorbed with quick onset.
l Highly lipophilicl Readily crosses blood-brain barrierl Peak levels occur 2-6 hours post ingestion l They possess high protein binding l They possess high volume of distribution (Vd) properties,
providing for a prolonged duration of action.
November 14, 2018 Clinical Toxicology 5th year -Lec 3,4 14
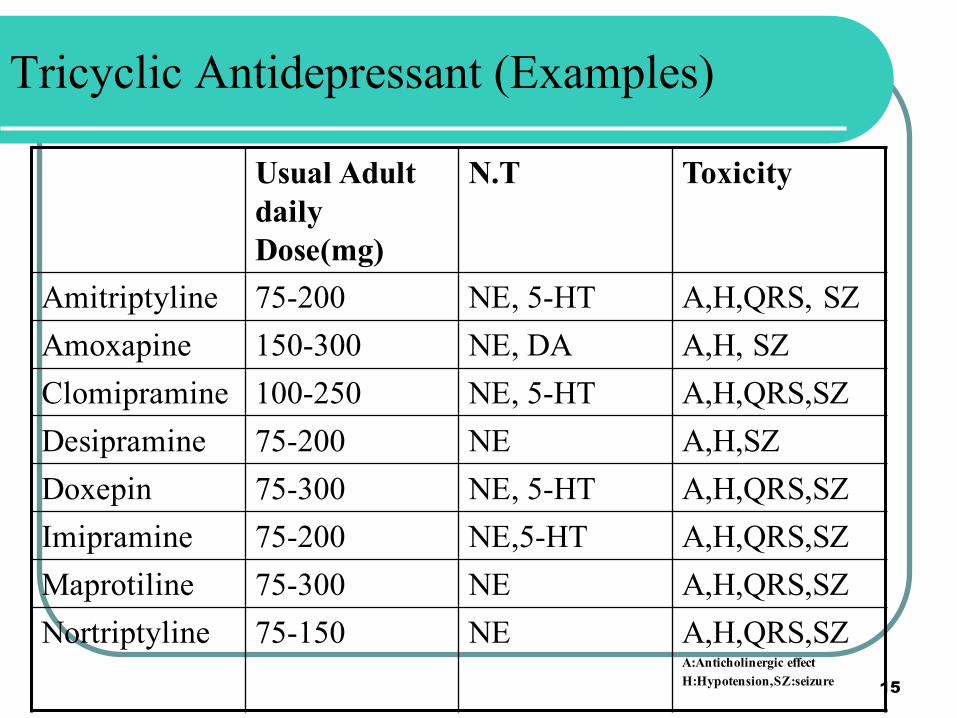
Tricyclic Antidepressant (Examples)
Toxicity N.T Usual Adult daily Dose(mg)
A,H,QRS, SZNE, 5-HT75-200Amitriptyline A,H, SZNE, DA 150-300AmoxapineA,H,QRS,SZNE, 5-HT100-250ClomipramineA,H,SZNE75-200DesipramineA,H,QRS,SZNE, 5-HT75-300DoxepinA,H,QRS,SZNE,5-HT75-200ImipramineA,H,QRS,SZNE75-300MaprotilineA,H,QRS,SZA:Anticholinergic effect H:Hypotension,SZ:seizure
NE75-150Nortriptyline15
Anticholinergics CNS(Seizure)
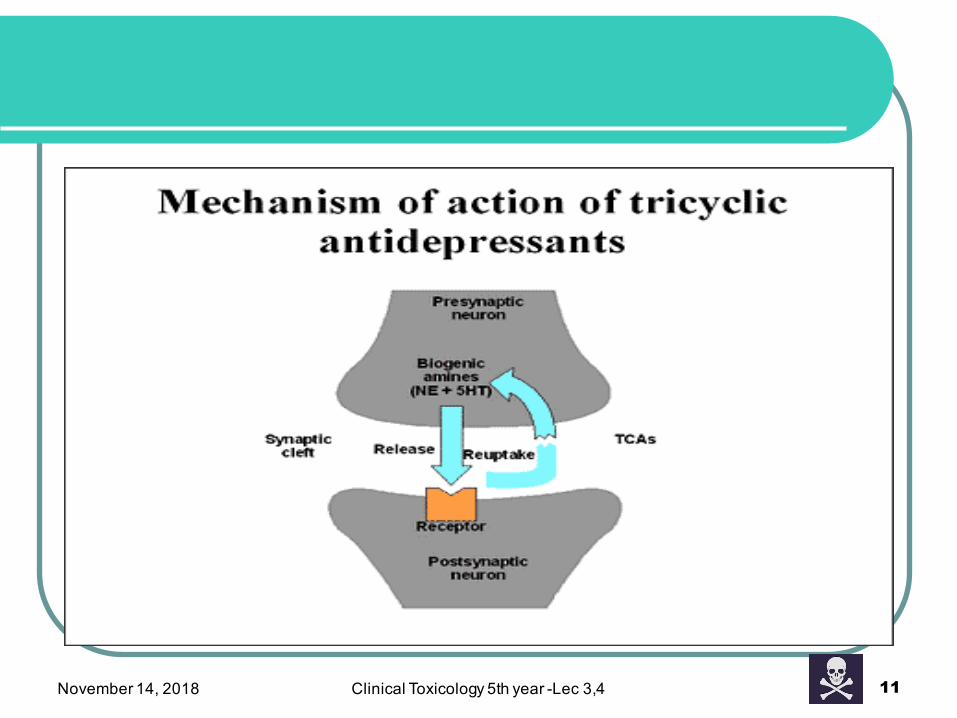
Mechanism of toxicity and Clinical presentation
Cardiovascular
TCA affect primarily the cardiovascular and CNS
November 14, 2018 Clinical Toxicology 5th year -Lec 3,4 16
Mechanism of Toxicity-CV effect
A: Cardiovascular (CV)effects: several mechanisms contribute to cardiovascular toxicity:
1. Anticholinergic effects (tachyarrhythmia due to blockade of vagus nerve), atrial tachycardia, fibrillation, and flutter; AV block, and ventricular tachycardia which lead to decreased cardiac output and hypotension.
2. Inhibition of neuronal reuptake of catecholamines result in tachycardia and mild hypertension.
3. Direct Peripheral alpha-adrenergic blockade causes vasodilation and contributes to secondary hypotension
November 14, 2018 Clinical Toxicology 5th year -Lec 3,4 17
4. Membrane-depressant or membrane stabilizing (quinidine-like) effects cause myocardial depression and cardiac conduction disturbances (delay conduction velocity) by blockade of sodium influx channel resulting in QRS prolongation and arrythmia and possibly convulsion.
l The binding of TCAs to the sodium channel is PH-dependent and acidosis increase the degree of blockade. This explain why arrhythmias become more frequent in the presence of acidosis.
l Metabolic or respiratory acidosis may contribute to cardiotoxicity by further inhibiting the fast sodium channel .
Hypotension: predominant
Mechanism of toxicity-CV effect
November 14, 2018 Clinical Toxicology 5th year -Lec 3,4 18
B. Central nervous system effects: these effects result from:1. Anticholinergic toxicity (e.g sedation and coma) Depression
and coma may occur because it is believed that a cholinergic component in the reticular activating system (RAS) is responsible for maintaining arousal.
2. Antihistaminergic and anticholinergic effects cause sedation which may be severe enough to cause respiratory depression and acidosis.
3. Inhibition of reuptake of norepinephrine or serotonin in the brain or other central effects (e.g seizures)
Mechanism of toxicity-CNS effect
November 14, 2018 Clinical Toxicology 5th year -Lec 3,4 19
November 14, 2018 Clinical Toxicology 5th year -Lec 3,4 20
Clinical presentation
A. Anticholinergic (Amitriptyline has the greatest anticholinergic activity)
l Agitation, sedation, delirium, coma l Red, hot, dry skinl Tachycardia,l Dilated pupilsl No bowel soundsl Urinary retentionl Mild hyperthermial Mild hyperreflexial Myoclonal muscle jerking
November 14, 2018 Clinical Toxicology 5th year -Lec 3,4 21
Clinical presentation
B. Cardiovascular toxicity manifest as1. Abnormal cardiac conduction, arrhythmias, typical ECG
finding is sinus tachycardia with prolongation of the QRS〉100msec , and PR/QT intervals .
2. Hypotension: caused by venodilation, in severe cases hypotension results from myocardial depression and may be refractory to treatment.
ü Some patients die with progressive cardiogenic shock ü Pulmonary edema is common in severe poisoning.
November 14, 2018 Clinical Toxicology 5th year -Lec 3,4 22
Clinical presentation
C. CNS: pyramidal signs, brisk reflexes, coma, convulsions, respiratory depression. Seizures are common with TCA toxicity and may be recurrent or persistent. The muscular hyperactivity from seizures and myoclonic jerking, combined with diminished sweating can lead to severe hyperthermia, resulting in rhabdomyolysis, brain damage, multisystem failure and death.
November 14, 2018 Clinical Toxicology 5th year -Lec 3,4 23
Other ?
l Respiratory dysfunction result from direct action of TCAs on the respiratory center in the medulla.
l Disturbance in body temperature occur as a result of direct action on the thermoregulatory site in the hypothalamus in addition to decreased sweating (anticholinergic effect).
l Depression and coma may occur (Anticholinergic effect on RAS).
November 14, 2018 Clinical Toxicology 5th year -Lec 3,4 24
Other CNS Characteristics of poisoning ?
l Hallucination, loss of short term memory, ataxia, respiratory difficulties, hypothermia (Amitriptyline) or hyperthermia (with imipramine), tonic- clonic seizures (maprotiline).
November 14, 2018 Clinical Toxicology 5th year -Lec 3,4 25
Cause of Death
Death occurs within a few hours of admission and may result from ventricular fibrillation, intractable cardiogenic shock or status epilepticus with hyperthermia.
November 14, 2018 Clinical Toxicology 5th year -Lec 3,4 26
Management of TCAs Poisoning
l Management is determined by the clinical features, active treatment of complications such as arrhythmia and convulsions is mandatory.
l Observation in an ICU is critical.l Activated charcoal is used to adsorb the drug and to decrease
enterohepatic recycling of TCAs, so it administered in multiple doses.
l Gastric lavage is potentially hazardous and may wash the tricyclic into the duodenum leading to more rapid drug absorption and increased toxicity.(2014)
November 14, 2018 Clinical Toxicology 5th year -Lec 3,4 27
Management of TCAs Poisoning
l Arrhythmia: prolongation of the QRS interval >120ms is an indication for prophylactic NaHCO3 aiming to achieve a pH of 7.5.
l Note: Anti-arrhythmic drugs are not used because they have negative inotropic and membrane effects which may aggravate toxic myocardial effects.
l Bicarbonates 1-2mEq/kg I.V is used and repeat as needed to maintain arterial PH 7.45-7.55
l Alkalinization decrease the chance for arrhythmia, it also promotes movement of potassium into cardiac muscle. Potassium narrows the width of the QRS complex of the ECG.
November 14, 2018 Clinical Toxicology 5th year -Lec 3,4 28
Management of TCAs Poisoning
l TCA may prolong the QT interval, a risk factor for torsade de points , use Magnesium sulfate (I.V) when there is QT prolongation.
l Patients with hypotension treated with vasoconstrictors such as phenylephrine(2014).
l Syrup of ipecac ? controversy ? with any TCA ingestion due to the possibility of rapid neurological deterioration and high incidence of seizures.
l Hemoperfusion may be attempted in severe intoxication.l Hyperthermia and fever can be treated with ice-water
sponging or immersion in cooled water.
November 14, 2018 Clinical Toxicology 5th year -Lec 3,4 29
l Convulsions should be controlled with I.V diazepam or lorazepam
l Acidosis and hypoxia should be corrected after seizure to reduce the risk of arrhythmia.
l For severe clomipramine overdose, the use of I.V lipid emulsion therapy has been reported ( decrease free conc. of the drug)
l Physostigmin no longer recommended for routine TCA poisoning why?
l To treat hypotension, direct sympathomimetic amine is used e.g. Dobutamine or dopamine(why?) Dihydroergotamine also used.
November 14, 2018 Clinical Toxicology 5th year -Lec 3,4 30
Management of TCAs Poisoning
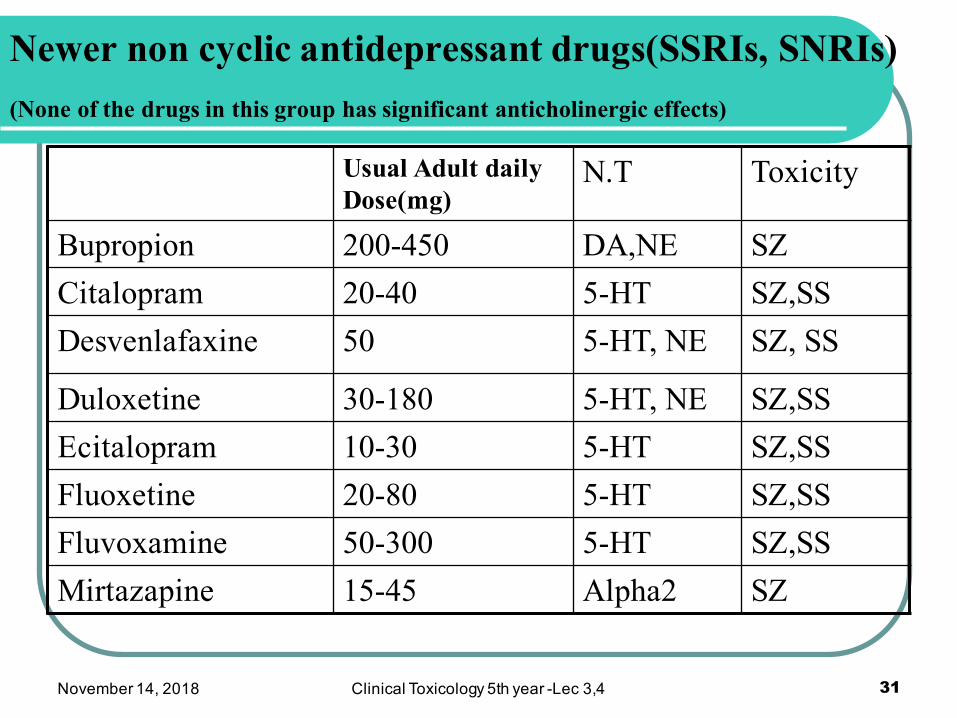
Newer non cyclic antidepressant drugs(SSRIs, SNRIs) (None of the drugs in this group has significant anticholinergic effects)
Toxicity N.T Usual Adult daily Dose(mg)
SZDA,NE200-450Bupropion SZ,SS5-HT20-40Citalopram SZ, SS5-HT, NE50Desvenlafaxine
SZ,SS5-HT, NE30-180DuloxetineSZ,SS5-HT10-30Ecitalopram SZ,SS5-HT20-80Fluoxetine SZ,SS5-HT50-300Fluvoxamine SZAlpha2 15-45Mirtazapine
November 14, 2018 Clinical Toxicology 5th year -Lec 3,4 31
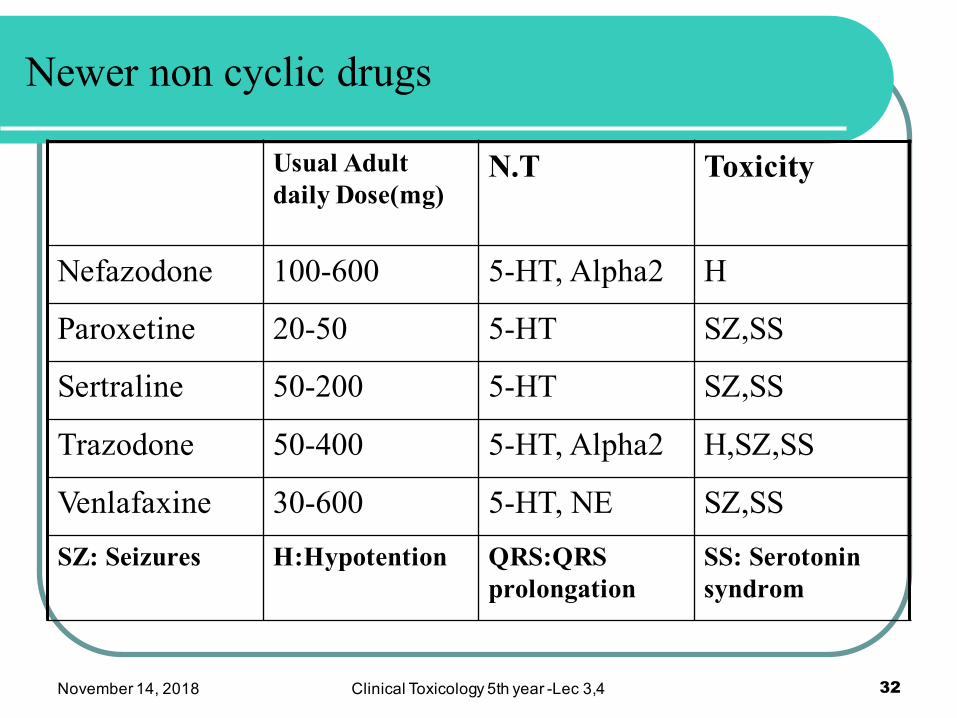
Newer non cyclic drugs
Toxicity N.T Usual Adult daily Dose(mg)
H5-HT, Alpha2 100-600Nefazodone
SZ,SS5-HT20-50Paroxetine
SZ,SS5-HT50-200Sertraline
H,SZ,SS5-HT, Alpha250-400Trazodone
SZ,SS5-HT, NE30-600Venlafaxine
SS: Serotonin syndrom
QRS:QRS prolongation
H:HypotentionSZ: Seizures
November 14, 2018 Clinical Toxicology 5th year -Lec 3,4 32
Toxic dose?
l SSRIs toxicity is considerably less than TCAs.l The non cyclic antidepressants generally have a wide
therapeutic index , with doses in excess of 10 times the usual therapeutic dose tolerated without serious toxicity.
l Bupropion can cause seizures in some patients with moderate overdoses or even in therapeutic doses, particularly in people with a history of seizure disorders.
l None of the drugs in this group has significant anticholinergic effects.
November 14, 2018 Clinical Toxicology 5th year -Lec 3,4 33
Mechanism of Toxicity:
l They are potent inhibitors of neuronal serotonin reuptake and toxicity arises from serotonergic effects such as agitation and increased muscle activity which may progress to serotonin syndrome.
l At high dose some SSRIs has a direct effects on myocardial and central ion channels causing ventricular intraconduction abnormalities, prolongation of QRS, QT intervals, convulsion and arrhythmia.
November 14, 2018 Clinical Toxicology 5th year -Lec 3,4 34
Clinical features:
l Most patients will have only mild serotoninergic features including: Nausea , vomiting, agitation, tachycardia.
l Sedation, convulsion and coma may develop after large overdoses >1.5g.
l More severe cardiac effects include hypertension and ECG change
l In large single overdose there is a risk of serotonin syndrome (restlessness, hyperpyrexia, rhabdomyolysis and renal failure).
November 14, 2018 Clinical Toxicology 5th year -Lec 3,4 35
Treatment (newer non cyclic antidepressant)
l Emergency and supportive measures l Maintain an open airway + Oxygen l Treat coma, hypotension, hypertension, and seizurel Decontamination; oral activated charcoal may be valuable if
administered within 1-2 hrs of ingestion. l For Mild serotonin syndrome use benzodiazepine for
control of agitation and tremor.l I.V fluid for vomiting , pyrexia or serotonin syndrome. l Severe serotonin syndrome with hyperthermia required
hospitalization+ aggressive cooling measure including neuromuscular paralysis and endotracheal intubation.
November 14, 2018 Clinical Toxicology 5th year -Lec 3,4 36
Treatment (newer non cyclic antidepressant)
l Treat convulsion with I.V diazepam , or lorazepam l Prolongation of QRS or QT intervals on ECG should be managed as
described for TCAS?l Benzodiazepines may be helpful for severe myoclonic jerking.l Specific drugs and antidote: for suspected serotonin syndrome,
anecdotal reports and case series claim benefit from cyproheptadine12mg orally or by NG-tube, followed by 4 mg every hour for 3-4 doses,
l Chlorpromazine (5HT2A antagonist) may be used for severe serotonin syndrome although clinical evidence of benefit is lacking.
l Dantrolene may also be considered. l Enhanced elimination; due to extensive protein binding and large Vd,
dialysis, hemoperfusion peritonial dialysis and repeated dose of charcoal are not effective.
37
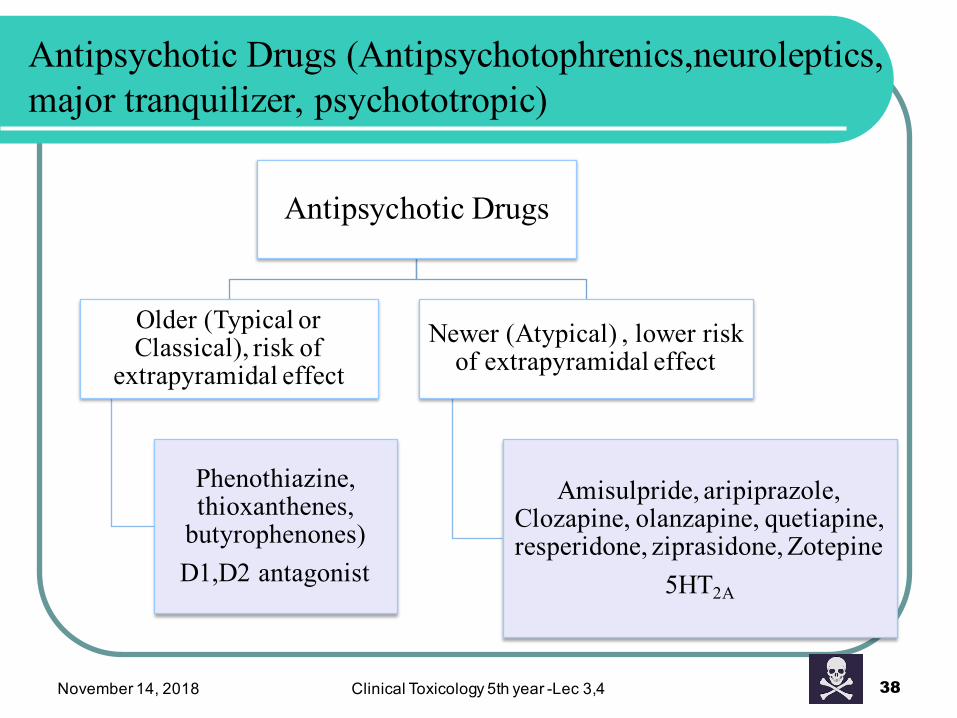
Antipsychotic Drugs (Antipsychotophrenics,neuroleptics, major tranquilizer, psychototropic)
Antipsychotic Drugs
Older (Typical or Classical), risk of
extrapyramidal effect
Phenothiazine,thioxanthenes,
butyrophenones)D1,D2 antagonist
Newer (Atypical) , lower risk of extrapyramidal effect
Amisulpride, aripiprazole, Clozapine, olanzapine, quetiapine, resperidone, ziprasidone, Zotepine
5HT2A
November 14, 2018 Clinical Toxicology 5th year -Lec 3,4 38
APD Poisonig
Mixed poisoning
Suicideoverdose
Other indications
November 14, 2018 Clinical Toxicology 5th year -Lec 3,4 39
Antipsychotic Drugs (Antipsychotophrenics,neuroleptics, major tranquilizer,psychototropic)
l Several drugs used to treat severe psychotic disorders. In addition to their use in mental diseases, they are also used as antiemetic, tranquilizers and cough suppressants
l Serious morbidity and mortality to pure antipsychotic overdose are low. However, many antipsychotic drug poisonings represent mixed poisonings (a combination of different drugs).
l Suicidal overdoses are common but because of the high toxic/therapeutic ratio acute overdose seldom results in death.
November 14, 2018 Clinical Toxicology 5th year -Lec 3,4 40
Reasons for presence of large number of poisoning:
1. Antipsychotic drugs (APDs) are widely prescribed.2. Mental patients receive these drugs as outpatients,
therefore antipsychotic drugs are widely available.3. Psychotic patients are at greater risk than the general
population for suicidal.4. Many of the tablet preparations resemble smooth-coated
candy confections and therefore are attractive to children (increase accidental poisoning among them) .
November 14, 2018 Clinical Toxicology 5th year -Lec 3,4 41
Toxicokinetics
l Most APD are lipid-soluble. They have large Vd (Vd=10-30L)
l Long elimination t1/2 (e.g chlorpromazin t1/2 = 18-30hr)l Elimination by hepatic metabolism
November 14, 2018 Clinical Toxicology 5th year -Lec 3,4 42
Toxic dose?
l Antipsychotic drugs have a relatively wide therapeutic margin.
l The toxic dose after acute ingestion is highly variable, e.g serious CNS depression and hypotension may occur after ingestion of 200 –1000 mg of chlorpromazine in children or of 3-5g in adult.
l Extrapyramidal reaction, anticholinergic side effects, and orthostatic hypotension are often seen with therapeutic doses.
November 14, 2018 Clinical Toxicology 5th year -Lec 3,4 43
Mechanism of Toxicity & Characteristics of poisoning
l A variety of pharmacological effects are responsible for toxicity involving the cardiovascular and CNS .
1. Cardiovascular System: l Anticholinergic effect especially chlorpromazine, clozapine,
Olanzapine resulting in sedation, tachycardia, hypotension, dry mouth, urinary retention.
l Alpha-adrenergic blockade may cause orthostatic hypotension, reflex tachycardia.
l Myocardial ion channel effect : Quinidine-like membrane depressant effects on heart may occur.
l Many of these agents can cause QRS, QT prolongation.
November 14, 2018 Clinical Toxicology 5th year -Lec 3,4 44
2. Central nervous system (CNS): l Sedation and anticholinergic effects contribute to CNS
depression.l Extrapyramidal dystonic reaction are common with
therapeutic doses which caused by central dopamine receptor blockade(receptors in the limbic system and basal ganglia)
l Acute dystonic reaction (e.g oculogyric) l Convulsion may occur and may be more common with
typical agents and with clozapine. l Temperature regulation is disturbed resulting in
poikilothermia.
November 14, 2018 Clinical Toxicology 5th year -Lec 3,4 45
Mechanism of Toxicity & Characteristics of poisoning
l All levels of the CNS affected by APD overdose particularly:l limbic system (amygdala which is part of limbic system) may
be stimulated by large doses of APD→lowering of the seizure threshold , EEG recording resembles epilepsy, the response is most prominent with aliphatic phenothiazines and least with others.
November 14, 2018 Clinical Toxicology 5th year -Lec 3,4 46
Characteristics of poisoning (CNS):
Characteristics of poisoning
l Hypothalamus: APD inhibit vasomotor and temperature regulating centers resulting in vasodilation and orthostatic hypotension. Either hypo-or hyperthermia may result and can be fatal.
November 14, 2018 Clinical Toxicology 5th year -Lec 3,4 47
l RAS: APD overdose depress the RAS resulting in sedation usually occurring within an hour of ingestion.
l Coma is common in acute overdose in children but rarely in adults which is characterized by restlessness, tremors, spasms and dystonic reaction
l Respiration rate depressed by APD overdose due to RAS depression.
November 14, 2018 Clinical Toxicology 5th year -Lec 3,4 48
Characteristics of poisoning
l APD block dopaminergic receptors in the striatum within the basal ganglia → extrapyramidal side effects
l 10% of all APD intoxicated patients will experience these effects
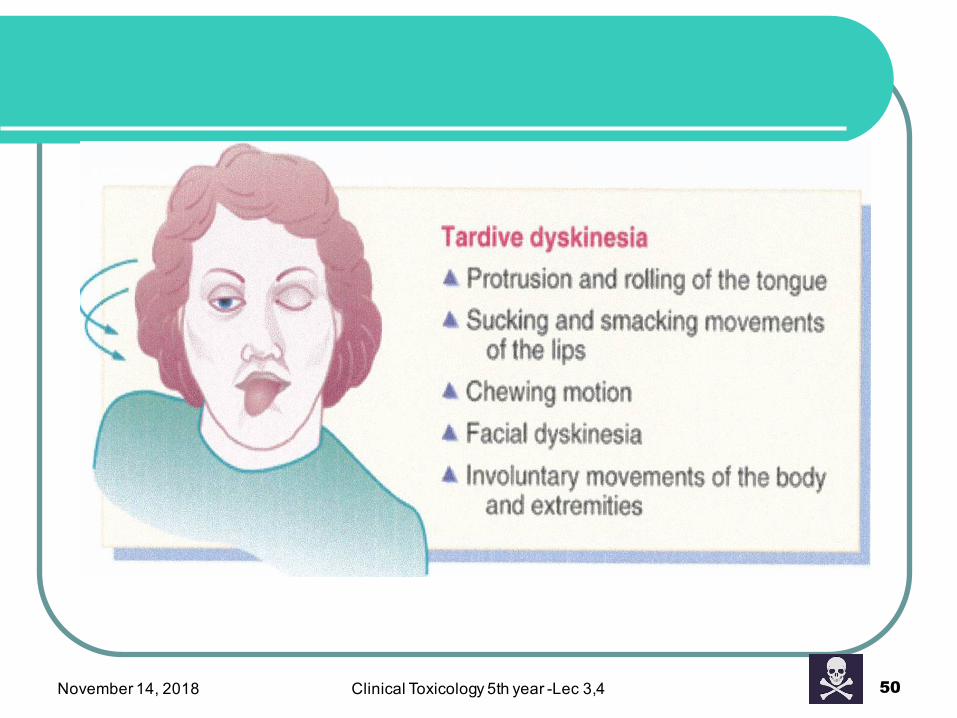
l Extrapyramidal effects includel Involuntary movements such as ;Tremor, Tics, Athetosisl Impairment of voluntary movement or akinesia l Change in muscle tone including muscle rigidity and dystonia l acute dystonia and tardive dyskinesia (involuntary movement
of face and tongue, trunk and limbs)
November 14, 2018 Clinical Toxicology 5th year -Lec 3,4 49
Extrapyramidal system effect of APD
November 14, 2018 Clinical Toxicology 5th year -Lec 3,4 50
November 14, 2018 Clinical Toxicology 5th year -Lec 3,4 51

November 14, 2018 Clinical Toxicology 5th year -Lec 3,4 52
l Patients on chronic antipsychotic medication may develop the neuroleptic malignant syndrome which is characterized by
l Rigidityl Hyperthermia l Sweatingl Lactic acidosis l Rhabdomyolysis
November 14, 2018 Clinical Toxicology 5th year -Lec 3,4 53
Neuroleptic malignant syndrome
l APDs have potent cholinergic and alpha-adrenergic blocking actions.
l Thus APD overdose produce atropine-like signs( dry mouth, constipation, blurred vision….etc) and alpha-adrenergic blocking side effects such as orthostatic hypotension with reflex tachycardia.
l Anticholinergic and alpha-adrenergic blocking potencies of APD are variable among the individual drugs
November 14, 2018 Clinical Toxicology 5th year -Lec 3,4 54
Autonomic nervous system-APD
The CV-effects of APD overdose are related to peripheral and central mechanism } Orthostatic hypotension result from blockade of the vasomotor center as well as from inhibition of alpha-adrenergic receptors.}Quinidin-like action, There is decreased AV nodal conduction→heart block and ventricular arrhythmia, ECG shows prolonged PR and QT interval, blunted T wave and depressed ST segment}Children patients with hypokalemia and/or preexisting CV disease are more susceptible to cardiotoxic effects of antipsychotics.}Most death are attributed to VF or cardiac arrest
November 14, 2018 Clinical Toxicology 5th year -Lec 3,4 55
Cardiovascular System-APD
Management of APD poisoning
} Emergency and supportive measures
} Stabilization of vital signs is the first priority as severe hypotension may produce shock
} Hypotension should be corrected by; I.V fluid then norepinephrine and dopamine assist in maintaining adequate cardiac output (Dopamine is preferred).
November 14, 2018 Clinical Toxicology 5th year -Lec 3,4 56
Management of APD poisoning
} Phenytoin or lidocaine control phenothiazine-induced arrythmias because they decrease automaticity and increase conduction velocity (Quinidine and procainamide are C.I).
} QRS-interval prolongation , treat quinidine like cardiotoxic effects with bicarbonate, 1-2meq/kg I.V
} If seizures are not controlled by phenytoin, diazepam should be added.
} Physostigmine is a drug of choice for treating anticholinergic toxicity (not routinely) but may be used in patients with hemodynamically unstable supraventricular tachycardia.it is also useful in ventricular dysarrythmias unresponsive to phenytoin, lidocaine
} For Dystonic reaction give diphenhydramine 0.5-1mg/kg I.M or I.V , or benztropine or procyclidine 5-10g I.V or I.M or diazepam.
November 14, 2018 Clinical Toxicology 5th year -Lec 3,4 57
} Decontamination by activated charcoal if appropriate
} Reduce further drug absorption by both emesis and lavage (not necessary after small to moderate ingestion)
} APD are not rapidly absorbed from stomach (the drugs are not water soluble and their anticholinergic action delay gastric emptying
} Saline cathartics will hasten elimination from intestine.
} After emesis or lavage, activated charcoal should be given to adsorb remaining traces of drug.
November 14, 2018 Clinical Toxicology 5th year -Lec 3,4 58
Management of APD poisoning
Review Questions:
l 10% of all APD intoxicated patients will experience extrapyramidal side effects, describe these effects briefly?
l Forced diuresis is not successful for increasing elimination of APD Why?
l Patients with APD toxicity are not significantly benefit from dialysis and hemoperfusion Why?
November 14, 2018 Clinical Toxicology 5th year -Lec 3,4 59