antimicrobial stewardship in the er - horizon health...
TRANSCRIPT
Dr. Michael ArmitageMaritime Trauma and EM Conference
April 5, 2014
Antimicrobial Stewardship in the ER
Declaration of Conflict of Interest
I DO NOT have an affiliation(financial or otherwise) with a pharmaceutical, medical device, or communications organization .
Outline
Describe antimicrobial stewardship and resistance
Review Treatment Guidelines for UTI, Cellulitis and CAP (New Brunswick Anti‐infective Stewardship Committee [ASC] and ASC Working Group, 2013)
What is Antimicrobial Stewardship?
• “…the limitation of inappropriate antimicrobial use while optimizing antimicrobial selection, dosing, route, and duration of therapy to maximize clinical cure or prevention of infection; while limiting unintended consequences, such as the emergence of resistance, adverse drug events, the selection of pathogenic organisms, and cost…”
(Vancouver Coastal Health Antimicrobial Stewardship Treatment Guidelines for Common Infections, March 2011)
Why Stewardship?• Widespread and suboptimal use of antibiotics has promoted the emergence of bacterial resistance resulting in infection related morbidity/mortality; also predisposition to secondary infections
• Factors that contribute to resistance propagation: inadequate hygiene, proximity of hospitalized patients, international travel.
• Must consider individual and public health consequences when writing a prescription for an antibiotic

Effective Stewardship Prescribing Is an antibiotic indicated? Suspected pathogen? Spectrum of activity of antimicrobial? Local resistance patterns? Risk of resistance?Medical history? Pregnancy Others

UTI: Guidelines for Treatment
Classic Signs and Symptoms
Dysuria, frequency, urgency, suprapubic/abdominal pain, gross hematuria
F/S/C, N/V, flank pain, CVA tenderness Gross hematuria ‐ not a sign of complicated UTI, needing different empiric/prolonged Rx
Variations in UTI Presentation
Isolated dysuria or frequency or urgency or abdominal/suprapubic pain or flank pain, or gross hematuria.
Elderly or those with CNS or Spinal Cord Disease
Urinalysis (dip stick and microscope)
Leukocyte esterase
Nitrite
Pyuria

Prevalence of Pyuria, IDSA GuidelinesPyuria?
Pyuria : >10Lkc on microscopy
Pyuria : presence or absence does not differentiate symptomatic from asymptomatic bactreiuria
Pyuria :not an indication for antimicrobial therapy
Pyuria: absence with symptoms ‐ consider alternate diagnoses
Prevalence 32% of young women 30‐70% of pregnant women 70% of diabetic women 90% of LTC men and women 90% of hemodialysis patient 30‐75% ST catheters 50‐100% LT catheters
(Nicolle, LE, et al, CID 2005)

Urine Culture
Resistance surveillance Atypical symptoms Persistent symptoms Recurrence Complicated infections Catheter in‐situ ≥ 2wk Not necessary post treat except in pregnancy and recurrences

Asymptomatic Bacteriuria (ASB)“Isolation of a specified quantity of bacteriuria in an appropriately collected urine specimen obtained from a person without symptoms or signs referable to urinary infection”
Women – 2 specimens same species ≥10⁵Men – 1 specimen single species ≥10⁵Catheter – 1 specimen single species ≥10
(Nicolle,LE, et al CID 2005)
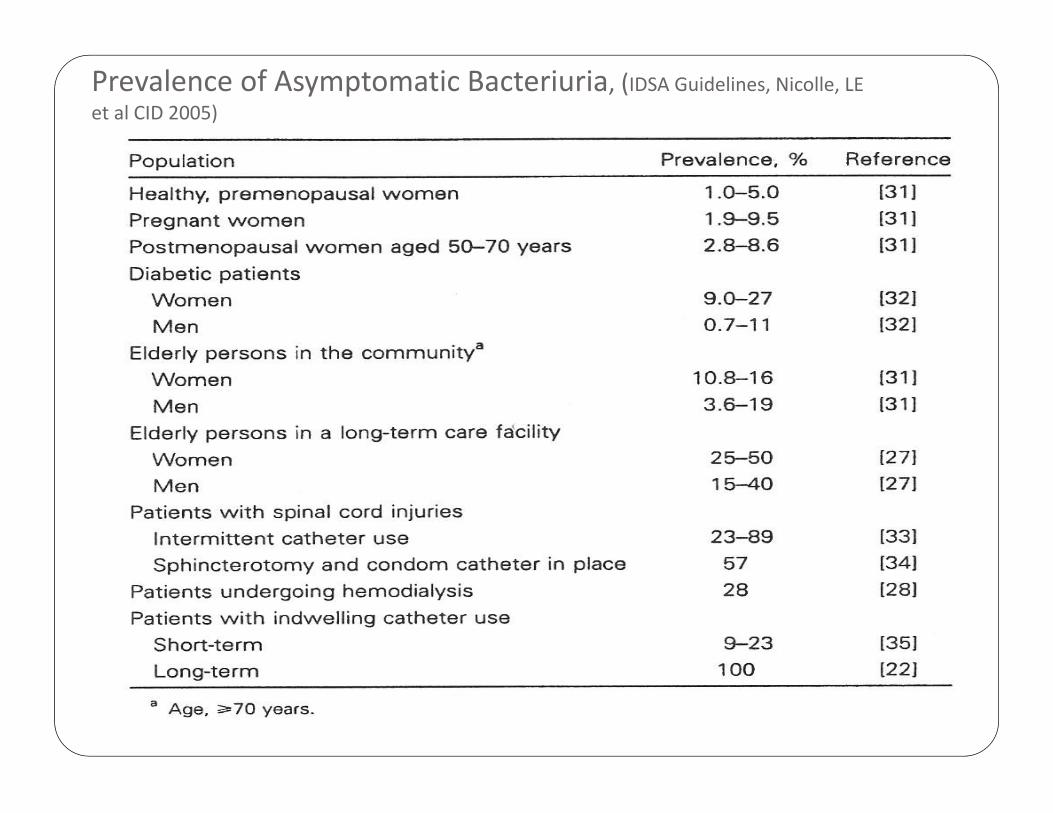
Prevalence of Asymptomatic Bacteriuria, (IDSA Guidelines, Nicolle, LE et al CID 2005)

Screening for and Treatment of ASB
Not Recommended RecommendedPremenopausal, nonpregnant womenDiabetic womenOlder persons living in the communityElderly LTCFPersons with spinal cord injuriesCatheterized patients, short or long term, while catheter is in‐situ
Pregnant women, at least once early
Before TURP or other urological procedures causing mucosal bleeding
Asymptomatic women with catheter‐acquired bacteriuria 48h post catheter removal

Empiric Antimicrobial Therapy – UTI
Uncomplicated Cystitis (Lower UTI)
E.coli Other Enterobacteria CoNS, particularly S.saprophyticus
First‐Line Options NitrofurantoinMacrocrystals 5 days
Alternatives TMP‐SMX 3days Amoxicillin/clavulanate 7days Fosfomycin
Pregnancy Nitrofurantoin (avoid near term, i.e. 36 – 42 weeks)
Cephalexin 7days Cefixime 7days

Therapy for UTI Acute Uncomplicated
Pyelonephritis
E.coli, other Enterobacteria, CoNS
Complicated UTI
structural abnormality, obstruction, recent urogenital procedure, male, immunosuppression, poorly controlled diabetes, spinal cord injury, catheterization/urologic apparatus, or S+S ≥ 7 days)
Above plus Ps., Enterococci, Grp B Strep

Empiric Therapy for UTI Systemically Well: Cefixime Ciprofloxacin TMP‐SMX Amoxicillin/clavulanate
Systemically Unwell: Ceftriaxone Ampicillin + Gentamicin Piperacillin/tazobactam(if at risk of MDR organisms)
Pregnant: Ceftriaxone Ampicillin + Gentamicin
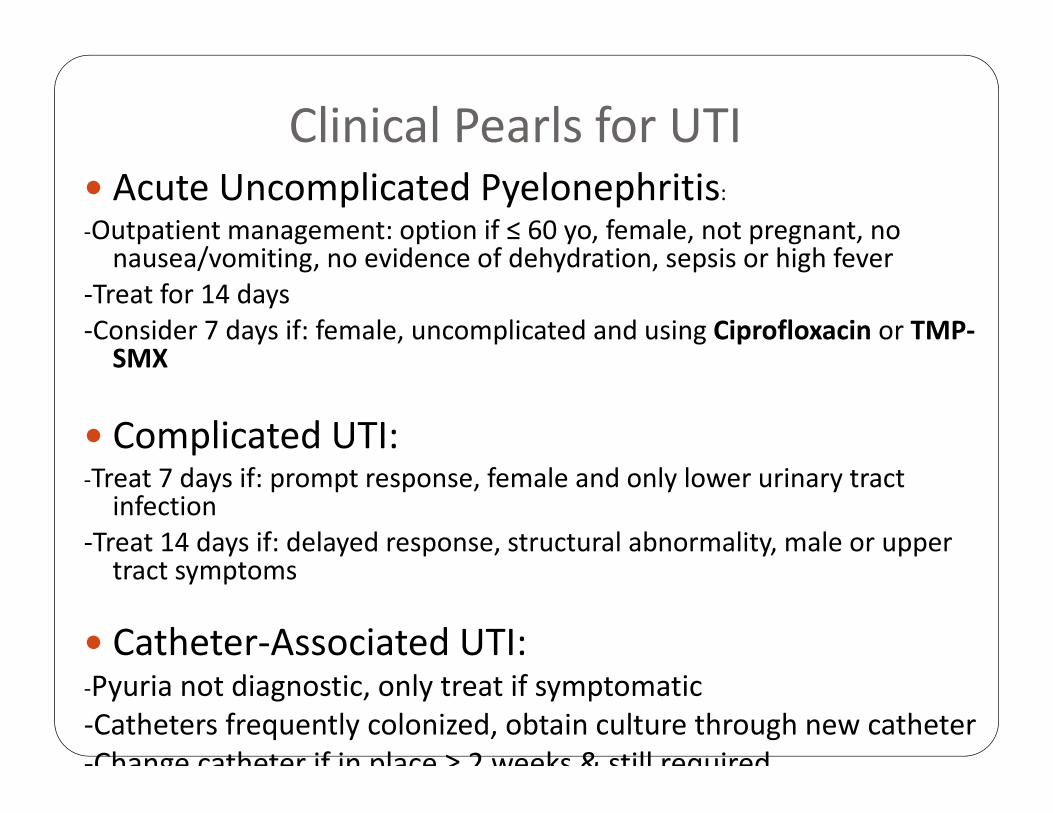
Clinical Pearls for UTI Acute Uncomplicated Pyelonephritis: ‐Outpatient management: option if ≤ 60 yo, female, not pregnant, no nausea/vomiting, no evidence of dehydration, sepsis or high fever
‐Treat for 14 days ‐Consider 7 days if: female, uncomplicated and using Ciprofloxacin or TMP‐SMX
Complicated UTI: ‐Treat 7 days if: prompt response, female and only lower urinary tract infection
‐Treat 14 days if: delayed response, structural abnormality, male or upper tract symptoms
Catheter‐Associated UTI: ‐Pyuria not diagnostic, only treat if symptomatic ‐Catheters frequently colonized, obtain culture through new catheter ‐Change catheter if in place ≥ 2 weeks & still required

Clinical Pearls for Empiric SSTI Therapy
Basic Skin Infections Only:
Any complicating features on history may require alternative management (specific but not exclusive examples include:, diabetic foot infections, cellulitis associated with a surgical site, penetrating trauma or animal/human bites, immunocompromised patients)
Look for predisposing feature (e.g. Tinea pedis, trauma, eczema, lymphedema)

Purulent vs Non‐purulent Cellulitis
Simple abscess without cellulitis – no antibiotic coverage
NON PURULENT ‐ β‐Hemolytic Strep/MSSA
PURULENT ‐MRSA/MSSA
C&S ‐ if purulent and using an antibiotic, not responding, severe local infection, systemically unwell
(IDSA CPG for MRSA: Liu K, et al CID 2011)
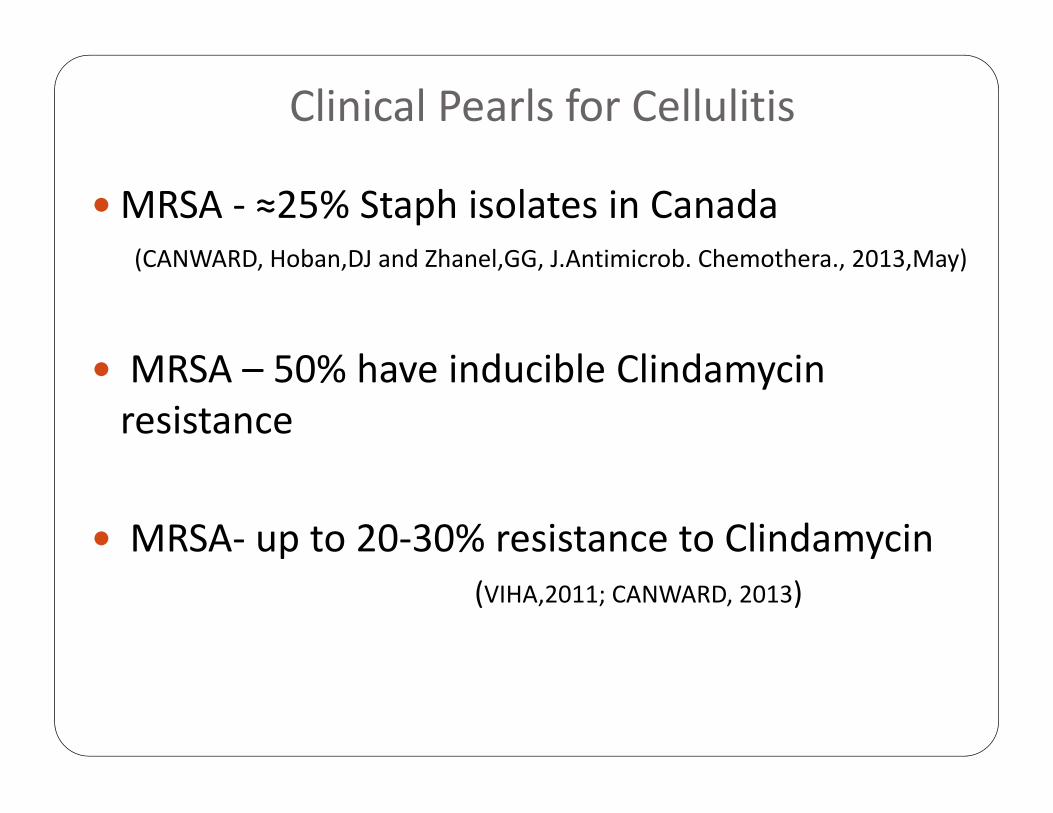
Clinical Pearls for Cellulitis
MRSA ‐ ≈25% Staph isolates in Canada(CANWARD, Hoban,DJ and Zhanel,GG, J.Antimicrob. Chemothera., 2013,May)
MRSA – 50% have inducible Clindamycinresistance
MRSA‐ up to 20‐30% resistance to Clindamycin(VIHA,2011; CANWARD, 2013)

MRSA Risk Factors (Baddour,LM, UpToDate 2014)
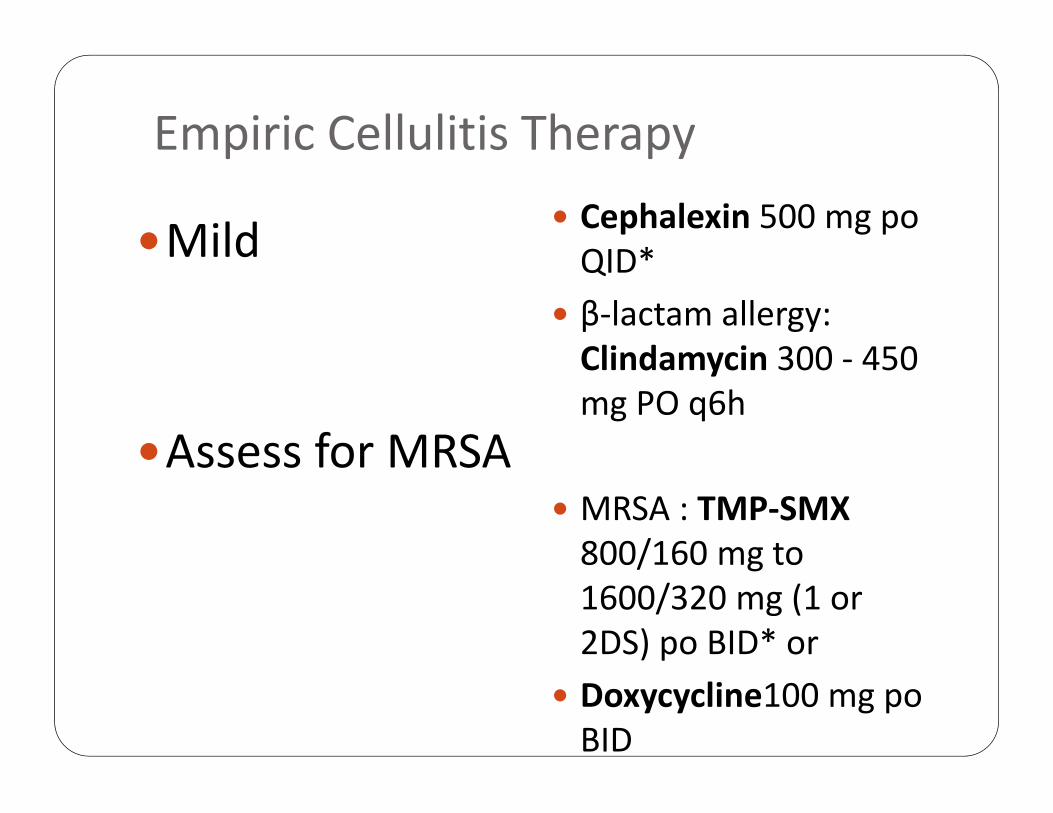
Empiric Cellulitis Therapy
Mild
Assess for MRSA
Cephalexin 500 mg poQID*
β‐lactam allergy: Clindamycin 300 ‐ 450 mg PO q6h
MRSA : TMP‐SMX 800/160 mg to 1600/320 mg (1 or 2DS) po BID* or
Doxycycline100 mg poBID

Empiric Cellulitis Therapy
Moderate
Assess for MRSA
Cefazolin 2 g IV q8h* Alternative for outpatient management ( when outpt. use Cefazolin not possible): Ceftriaxone 1 g IV q24h*
β‐lactam allergy: Clindamycin 600 mg IV q8h
MRSA suspected: Vancomycin 15 mg/kg IV q12h*

Empiric Cellulitis Therapy
Severe Sepsis/Septic Shock/ Necrotizing Fasciitis .
Pipericillin‐Tazobactam 3.375 g IV q6h* + Clindamycin600 mg IV q8h

CAP Diagnosis and Treatment Considerations
Diagnostic Triad 1) S+S of infection2) S+S referable to Respiratory Tract 3) New/Changed infiltrate on CXR
Treatment Triad 1) Choice of Antimicrobial 2) Extent of testing for etiology3) Location of treatment

CAP Risk for HAP/MDR Wunderwink RG, et al ,NEJM, Feb.6,2014
()

Clinical Pearls for CAP
CURB65 calculator:
1) new Confusion2) BUN >7mmol/L3)RR >304)BP < 90mmHG systolic or <60mmHg diastolic 5)Age ≥65
Each criterion scores 0 or 1
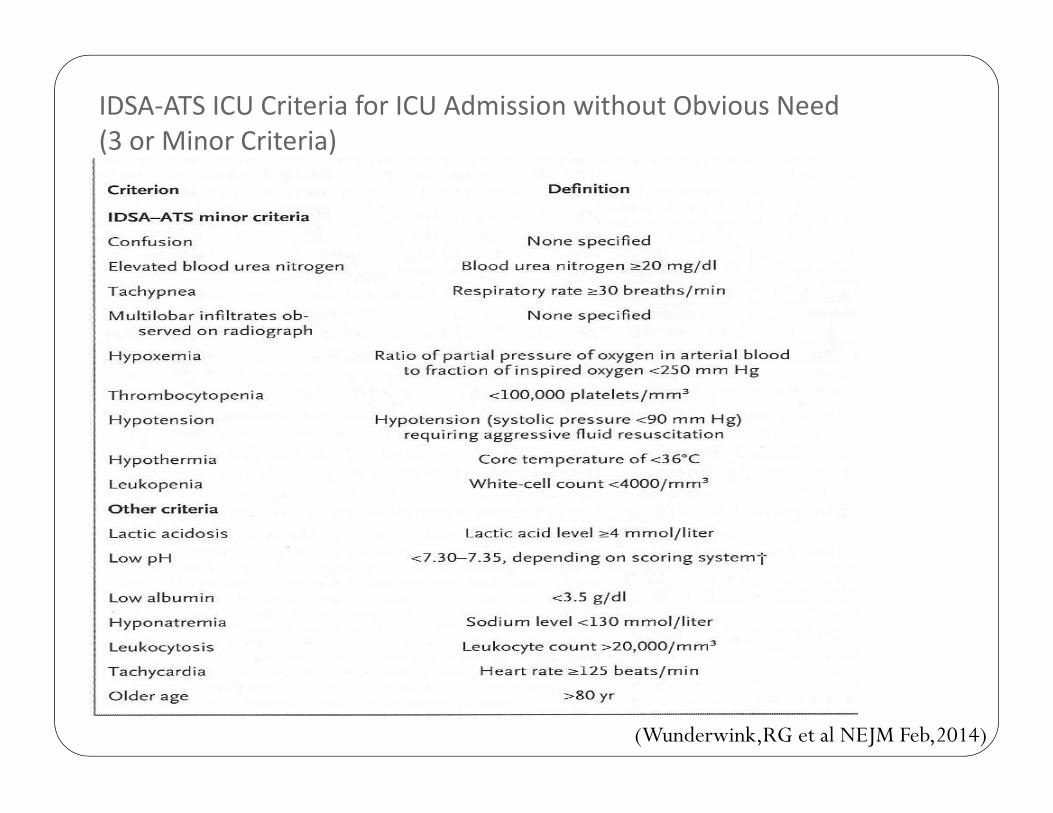
IDSA‐ATS ICU Criteria for ICU Admission without Obvious Need(3 or Minor Criteria)
(Wunderwink,RG et al NEJM Feb,2014)

Empiric Therapy for Community Acquired Pneumonia
CURB65: 0‐1 Low severity, mortality <3%, treatment at home or hospital (for reason other pneumonia)
Amoxicillin 500 mg – 1000 mg PO TID*
Doxycycline 100 mg PO BID
Macrolide: (Clarithromycin 500 mg PO BID or Azithromycin 500 mg PO first day followed by 250 mg once daily on days 2‐5)*
*Renal dose adjustment

Empiric Therapy for Community Acquired Pneumonia
CURB65: 2
Moderate Severity, mortality risk 9%,treatment site: hospital
Amoxicillin 1000 mg po TID*+ Macrolide*
Ampicillin 2 g IV q6h* + Macrolide or Doxycycline100mg po BID
*renal dose adjustment

Empiric Therapy for CommunityAcquired Pneumonia
CURB 65: ≥ 3High severity, mortality risk 15‐40%, treatment site: hospital, consider ICU
Cefuroxime 1.5 g IV q8h* + (Macrolide or Doxycycline) Ceftriaxone 2 g IV once daily + (Macrolide or Doxycycline) Levofloxacin 750 mg IV once daily* + ampicillin 2 g IV q6h* If Legionellosis strongly suspected, consider using Levofloxacin
*Renal dose adjustment
Simply Put……..
• “Right drug at the right time at the right dose for the right duration”
(Dryden M et al. J Antimicrob Chemother 20011; 66:2441)
• “Making sure patients get the right antibiotics when they need them (and only when they need them)”
(Dr Andrew Morris. Antimicrobial Stewardship: a New ROP for Acute Care Hospitals. Sept 20, 2012)
Parting Words “Antimicrobials are a limited, nonrenewableresource.”
(Carlet, et al, 2011)
“Every antibiotic expected by a patient, every unnecessary prescription written by a doctor, every uncompleted course of antibiotic, and every inappropriate or unnecessary use in animals or agricultureis potentially signing a death warrant for a future patient”
(Dryden et al, 2009)
Questions…
Intra‐abdominal Infections (IAI) CATEGORIAZATION: Community vs Hospital Acquired Mild/Moderate vs Severe Uncomplicated vs Complicated
CORE PATHOGENS: Enterobacteria esp. E.coli Anaerobes esp. GNB eg Bacteroides Enterococci
Empiric Therapy for IAI’s(Mild, Moderate, Severe)
1. Cipro/Flagyl2. Cipro/Flagyl3. Cipro/Flagyl
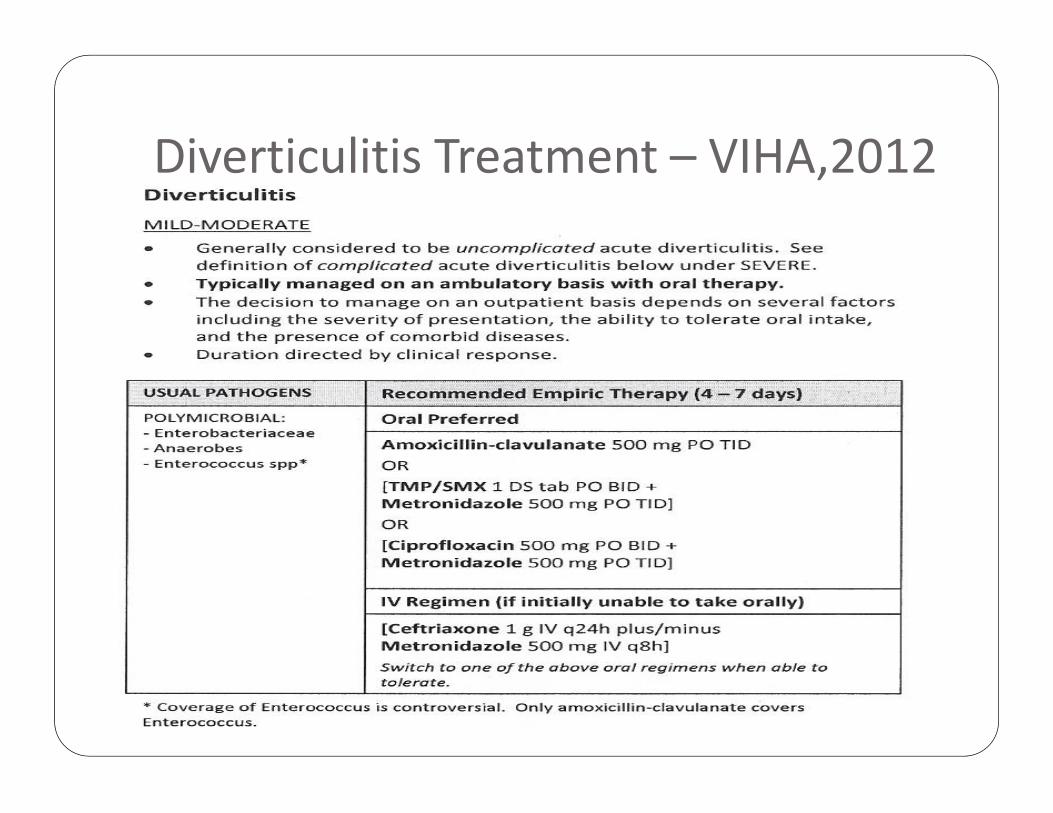
Diverticulitis Treatment – VIHA,2012
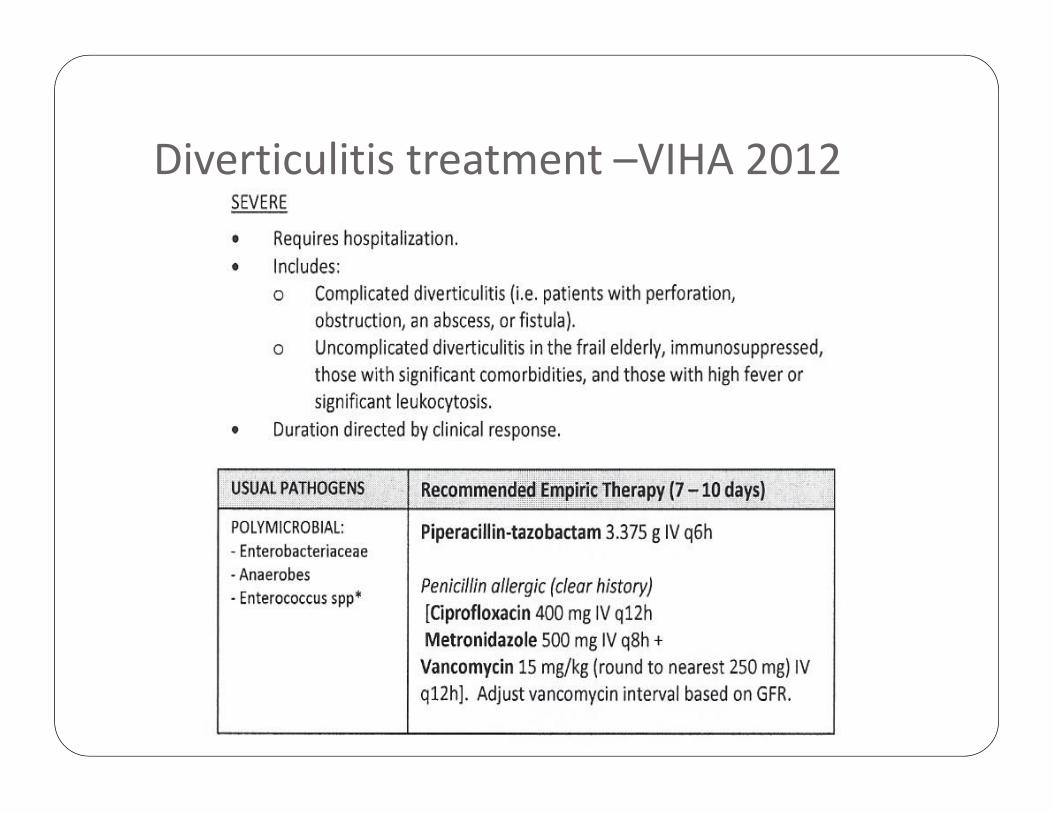
Diverticulitis treatment –VIHA 2012
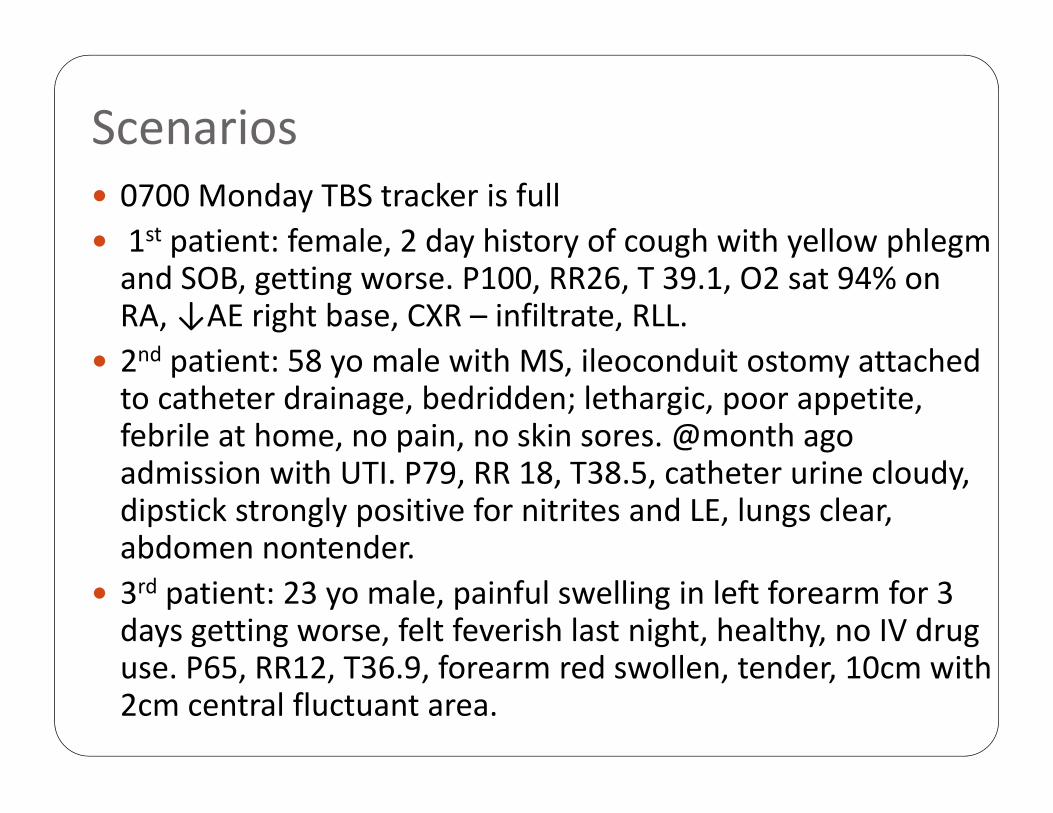
Scenarios 0700 Monday TBS tracker is full 1st patient: female, 2 day history of cough with yellow phlegm and SOB, getting worse. P100, RR26, T 39.1, O2 sat 94% on RA, ↓AE right base, CXR – infiltrate, RLL.
2nd patient: 58 yo male with MS, ileoconduit ostomy attached to catheter drainage, bedridden; lethargic, poor appetite, febrile at home, no pain, no skin sores. @month ago admission with UTI. P79, RR 18, T38.5, catheter urine cloudy, dipstick strongly positive for nitrites and LE, lungs clear, abdomen nontender.
3rd patient: 23 yo male, painful swelling in left forearm for 3 days getting worse, felt feverish last night, healthy, no IV drug use. P65, RR12, T36.9, forearm red swollen, tender, 10cm with 2cm central fluctuant area.

Terminology‐ Bacteria
Gram Negative Bacilli(GNB) – E.coli, Klebsiella, Proteus, Serratia, Morganella, Citrobactero, Enterobacter, Pseudomonas, Acinetobacter
Enterobacteriacea – Above except Ps., Acineto. Coagulase‐Negative Staph.(CoNS) – S. Epidermidis, S. saprophyticus
Enterococcus(GPC) – species(urine), feacalis, feacium
Anaerobic– GNB: Bacteroides, Fusibacterium; GPC: Peptostreptococci; GPS – Clostridium
Gram Negative Cocci(GNC) – H.flu, Nisseria, Legionella