antimicrobial stewardship program: pearls for … · antimicrobial stewardship program: pearls for...
TRANSCRIPT
Antimicrobial Stewardship Program: Pearls for Hospital and
Long-Term Care Jason D. North, PharmD, MBA
System Director of Pharmacy
SageWest Health Care,
Lander and Riverton, WY
Disclosure / Acknowledgement
• There are no potential conflicts of interest to disclose.
• This review was facilitated by SageWest Health Care; however, the material is the sole responsibility of the presenter.
Objectives
• Explain CMS/CDC expectations for antimicrobial stewardship programs (ASP)
• Examine evidence-based practices for ASP
• Describe process applications in hospital and long-term care settings
• Define metrics for sustained optimization of antimicrobial use
Antibiotic History
• 1909 Organoarsenic
• 1928 Fleming’s Penicillium mold
• 1935 Sulfanilamide derivatives
• 1945 Penicillin–“weapon to save lives”
• 1950s – 1970s Semisynthetic penicillins, aminoglycosides, tetracyclines, macrolides, vancomycin, cephalosporins, carbapenems, quinolones
• 1990s – Novel anti-MRSA, anti-GNB
Life magazine, August 1944
Mechanisms of Resistance
• Resistance genes
– Degrading enzymes, Efflux pumps, Binding targets
• Vertical gene transfer
– Spontaneous mutations
• Horizontal gene transfer
– Conjugation – pilus bridge for plasmid transfer
– Transduction – bacteriophage virus transfers gene
– Transformation – active uptake of free DNA
History of Resistance
• 1930s – Sulfonamide resistance
• 1940s – Streptomycin resistance by TB
• 1950s – Genetically transferable resistance
• 1961 – First MRSA isolated, 3 years after Methicillin introduced; acronym now refers to “Multi-drug Resistant S. aureus”
• 1990s – Quinolone resistance
• Exponential genetic mutations
Epidemiologically Important Pathogens
• Propensity for transmission (2 or more patients)
– VRE, MRSA, C. difficile, Enterobacter spp, Serratia spp, group A streptococcus
• Antimicrobial resistance
– VRE, MRSA, ESBL-producing, CRE
– First isolates, ie Burkholderia cepacia, quinolone-resistant Pseudomonas
– Innately resistant, ie Acinetobacter, S. maltophilia
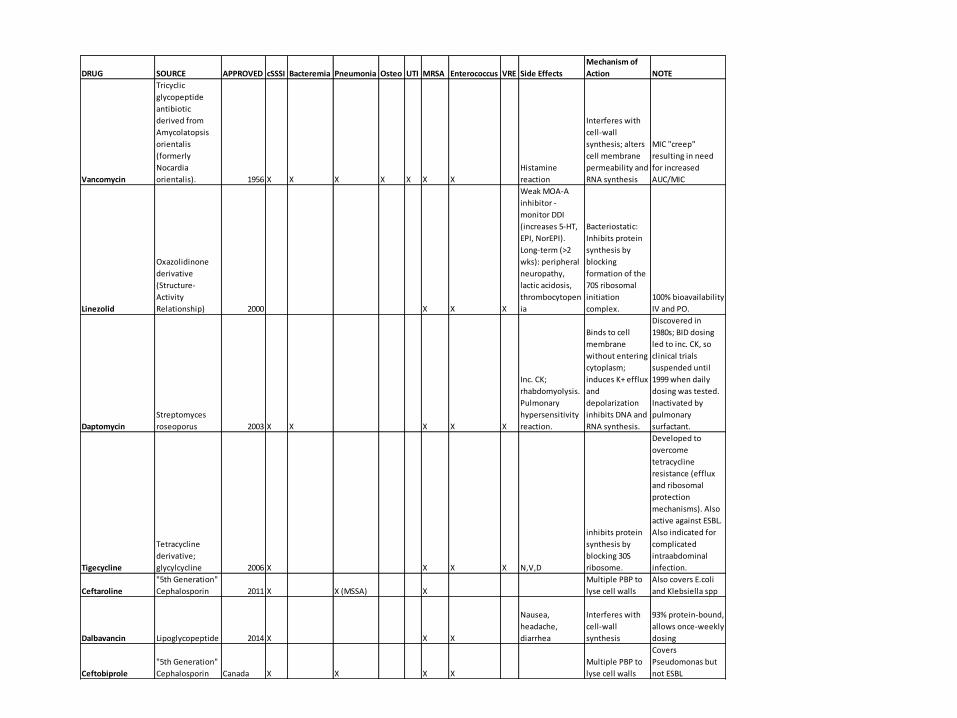
DRUG SOURCE APPROVED cSSSI Bacteremia Pneumonia Osteo UTI MRSA Enterococcus VRE Side Effects
Mechanism of
Action NOTE
Vancomycin
Tricyclic
glycopeptide
antibiotic
derived from
Amycolatopsis
orientalis
(formerly
Nocardia
orientalis). 1956 X X X X X X X
Histamine
reaction
Interferes with
cell-wall
synthesis; alters
cell membrane
permeability and
RNA synthesis
MIC "creep"
resulting in need
for increased
AUC/MIC
Linezolid
Oxazolidinone
derivative
(Structure-
Activity
Relationship) 2000 X X X
Weak MOA-A
inhibitor -
monitor DDI
(increases 5-HT,
EPI, NorEPI).
Long-term (>2
wks): peripheral
neuropathy,
lactic acidosis,
thrombocytopen
ia
Bacteriostatic:
Inhibits protein
synthesis by
blocking
formation of the
70S ribosomal
initiation
complex.
100% bioavailability
IV and PO.
Daptomycin
Streptomyces
roseoporus 2003 X X X X X
Inc. CK;
rhabdomyolysis.
Pulmonary
hypersensitivity
reaction.
Binds to cell
membrane
without entering
cytoplasm;
induces K+ efflux
and
depolarization
inhibits DNA and
RNA synthesis.
Discovered in
1980s; BID dosing
led to inc. CK, so
clinical trials
suspended until
1999 when daily
dosing was tested.
Inactivated by
pulmonary
surfactant.
Tigecycline
Tetracycline
derivative;
glycylcycline 2006 X X X X N,V,D
inhibits protein
synthesis by
blocking 30S
ribosome.
Developed to
overcome
tetracycline
resistance (efflux
and ribosomal
protection
mechanisms). Also
active against ESBL.
Also indicated for
complicated
intraabdominal
infection.
Ceftaroline
"5th Generation"
Cephalosporin 2011 X X (MSSA) X
Multiple PBP to
lyse cell walls
Also covers E.coli
and Klebsiella spp
Dalbavancin Lipoglycopeptide 2014 X X X
Nausea,
headache,
diarrhea
Interferes with
cell-wall
synthesis
93% protein-bound,
allows once-weekly
dosing
Ceftobiprole
"5th Generation"
Cephalosporin Canada X X X X
Multiple PBP to
lyse cell walls
Covers
Pseudomonas but
not ESBL
Concept of “Stewardship”
“Optimize antimicrobial use to achieve the best clinical outcomes while minimizing adverse events and limiting selective pressures that drive the emergence of resistance and may also reduce excessive costs attributable to suboptimal antimicrobial use.”
– Society for Healthcare Epidemiology of America (SHEA), the Infectious Diseases Society of America (IDSA), and the Pediatric Infectious Diseases Society of America (PIDSA)

Combating Antibiotic Resistance Report to the President
• “CMS should use reimbursement incentives to drive antibiotic stewardship.”
• End of 2017: Conditions of Participation for hospitals, critical access hospitals, long-term care and nursing home facilities, then phase in long-term acute care hospitals, ambulatory surgery centers, and dialysis centers
• Implement robust antibiotic stewardship programs that adhere to best practices
CDC / CMS Expectations
• Ensure optimal antibiotic prescribing and limit overuse and misuse of antibiotics
– Leadership
– Accountability
– Drug Expertise
– Specific Interventions
– Tracking / Reporting: Prescribing, Use, and Resistance
– Education
• CDC recommends / CMS enforces
CDC Checklist
• Antibiotic time out / review after 48 hours
• Pre-authorization of selected agents
• Prospective audit for specified antibiotics
• Protocols: CAP, UTI, SSTI, PRE-OP, MRSA
• Monitor: protocol adherence, interventions, C. difficile rate, cumulative susceptibility (antibiogram), antibiotic consumption
Proposed TJC Standard
• Proposed Standard for Antimicrobial Stewardship in AHC, CAH, HAP, NCC, and OBS
• Standard MM.09.01.01,
with 8 Elements of Performance
Standard MM.09.01.01
• EP 1: Leaders establish antimicrobial stewardship as an organizational priority.
• EP 2: Educate staff and licensed independent practitioners involved in antimicrobial ordering, dispensing, administration, and monitoring about antimicrobial resistance and antimicrobial stewardship practices. Education occurs upon hire and annually thereafter.
Standard MM.09.01.01
• EP 3: Educate patients, and their families as needed, regarding the appropriate use of antimicrobial medications, including antibiotics.
Standard MM.09.01.01
• EP 4: The organization has an antimicrobial stewardship multidisciplinary team that includes the following members, when available in the setting: Pharmacist(s), Infection disease physician, Infection preventionist(s). Note: Part-time or consultant staff are acceptable as members of the antimicrobial stewardship multidisciplinary team.
Standard MM.09.01.01
• EP 5: The organization’s antimicrobial stewardship program includes the following core elements:
– Leadership commitment
– Accountability
– Drug expertise
– Action
– Tracking
– Reporting
– Education
Standard MM.09.01.01
• EP 6: The organization’s antimicrobial stewardship program uses organization-approved multidisciplinary protocols.
• Note: Examples of protocols are as follows: • Plan for Parenteral to Oral Antibiotic Conversion
• Guidelines for Antimicrobial Use in Adults, Peds
• Formulary Restriction, Preauthorization Requirements
• Treatment Guidelines for Common Infections
• "Wait-and-See" Antibiotic Protocol
Standard MM.09.01.01
• EP 7: The organization collects and analyzes data on its antimicrobial stewardship program, including antimicrobial prescribing and resistance patterns.
• EP 8: The organization takes action on improvement opportunities identified in its antimicrobial stewardship program.
IDSA Response to TJC Standard
• IDSA agrees that antimicrobial stewardship programs should contain the core elements indicated by the CDC.
• Successful programs should demonstrate how accountability, training and education efforts are shaped from other core elements (Drug Expertise, Action, Tracking, Reporting) and these efforts should be assessed through the accreditation process
SHEA Response to TJC
• Society for Healthcare Epidemiology of America recommends TJC move forward with finalizing this standard, with recommended revisions, for the CAH, HAP, and NCC settings.
• SHEA recommends suspending the finalization of a standard for the ABH and OBS settings until more research and work can be done to identify the most effective approach to ASP implementation.
Evidence-Based Practices
• Antibiotic time out / review after 48 hours
• Pre-authorization of selected agents
• Prospective audit for specified antibiotics
• Protocols: CAP, UTI, SSTI, PRE-OP, MRSA
Antibiotic Time-Out
• VA study: 145 vancomycin, 105 pip/tazo
• Orders allowed to expire at 72 hours:
– Vanco 53.1%, Pip/Tazo 49.5%
• Time-Out Template Completed by Prescriber:
– D/C: Vanco 9%, Pip/Tazo 16.2%
– Oral Alternate: Vanco 2.1%, Pip/Tazo 1.9%
• Inappropriate continuation: Vanco 4.8%, Pip/Tazo 8.6%
• Appropriate continuation: Vanco 26.8%, Pip/Tazo 24.8%
Time-Out Template
• Time-Out / Renewal Progress Note Template
– Is a bacterial infection present?
– Has the site of infection been determined?
– Has the bacterial pathogen(s) been identified?
– Is the patient clinically stable?
• Information links to antibiogram, empiric recommendations, dosing algorithms
Antibiotic Pre-authorization
• Tools: formulary, utilization checklist, approval
• Ohio State University Wexner Medical Center
• Doripenem required prescriber to obtain approval code from on-call ASP team member
• Approval time approx 6 min; 91% approved
• Mean doripenem use lower than previous imipenem use (11 ABX days/1,000 PD vs 27)
Antibiotic Pre-authorization
• Potential limitations:
– Delays in therapy; availability of personnel
– Prescriber pushback
– Unintended increases in use of un-restricted antimicrobials
• Potential benefits:
– Apply only to a few select antimicrobials
– Improve appropriate prescribing
– Preserve utility
Prospective Audit
• Prospective audit and feedback interventions are probably the most widely practiced of all antimicrobial stewardship strategies. Although labor-intensive, they are more easily accepted by physicians compared with formulary restriction and preauthorization strategies and have a higher potential for educational opportunities.
• Pharmacist interventions in real-time
Prospective Audit
• Potential limitations:
– Competency and availability of personnel
– Acceptance of recommendations is voluntary
• Potential benefits:
– Improved adherence to empiric protocols
– Options due to allergies, organ function
– Improve appropriate prescribing / education
– Preserve utility / de-escalation
Empiric Protocols
• Treatment Guidelines for Common Infections
• Sepsis, CAP, UTI, SSTI, PRE-OP, MRSA
• Based on incidence data from historic C&S
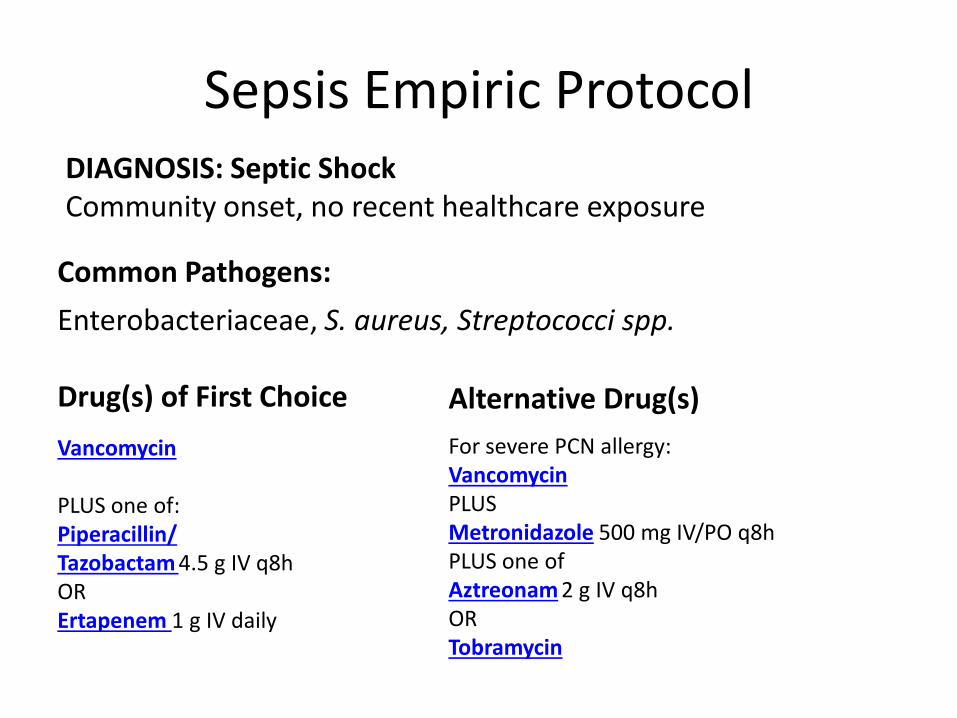
Sepsis Empiric Protocol DIAGNOSIS: Septic Shock Community onset, no recent healthcare exposure
Common Pathogens:
Enterobacteriaceae, S. aureus, Streptococci spp.
Drug(s) of First Choice
Vancomycin
PLUS one of: Piperacillin/ Tazobactam 4.5 g IV q8h OR Ertapenem 1 g IV daily
Alternative Drug(s)
For severe PCN allergy: Vancomycin
PLUS Metronidazole 500 mg IV/PO q8h PLUS one of Aztreonam 2 g IV q8h OR Tobramycin
Hospital ASP Applications
• Form ASP team
• Review proposed TJC standard
• Complete CDC Checklist (gap analysis)
• Baseline chart reviews (common / complex)
• Antibiogram
• Action Plan (measurable outcomes)
Drug Usage Evaluation
• Daptomycin usage
• N=14 in 5-month period
• 5 inpatients (3 continued OP); 9 OP
• Impact of ID consult on duration of therapy
• Inpatient therapy (1.7 vs 2 days)
• Outpatient therapy (9.5 vs 2.5 days)
• No ID consult: cellulitis, DM foot, osteomyelitis
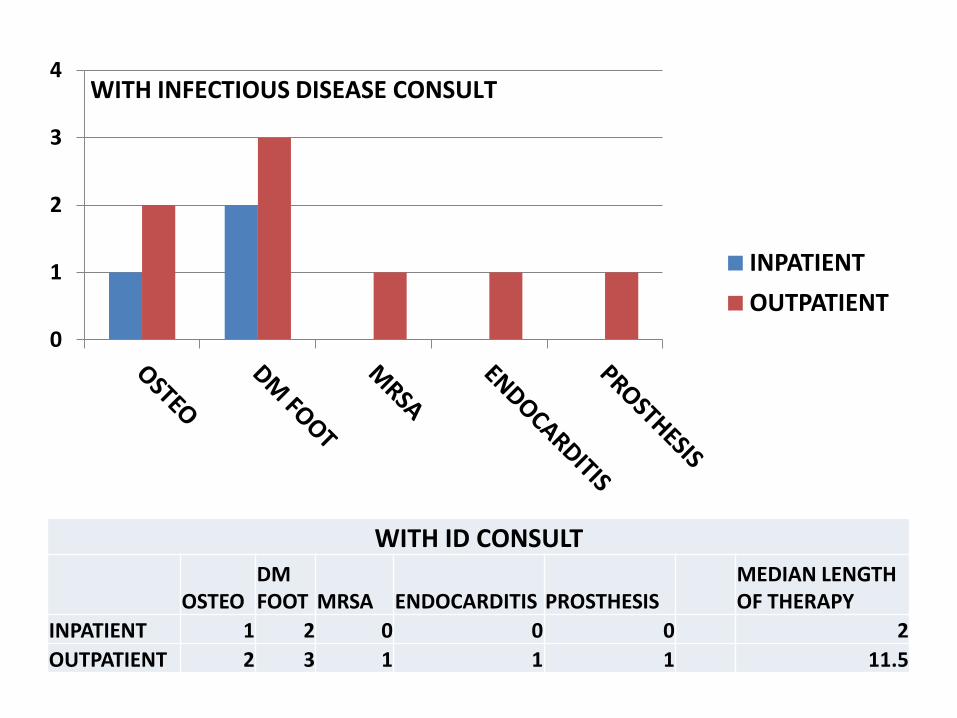
WITH ID CONSULT
OSTEO DM FOOT MRSA ENDOCARDITIS PROSTHESIS
MEDIAN LENGTH OF THERAPY
INPATIENT 1 2 0 0 0 2
OUTPATIENT 2 3 1 1 1 11.5
0
1
2
3
4
INPATIENT
OUTPATIENT
WITH INFECTIOUS DISEASE CONSULT
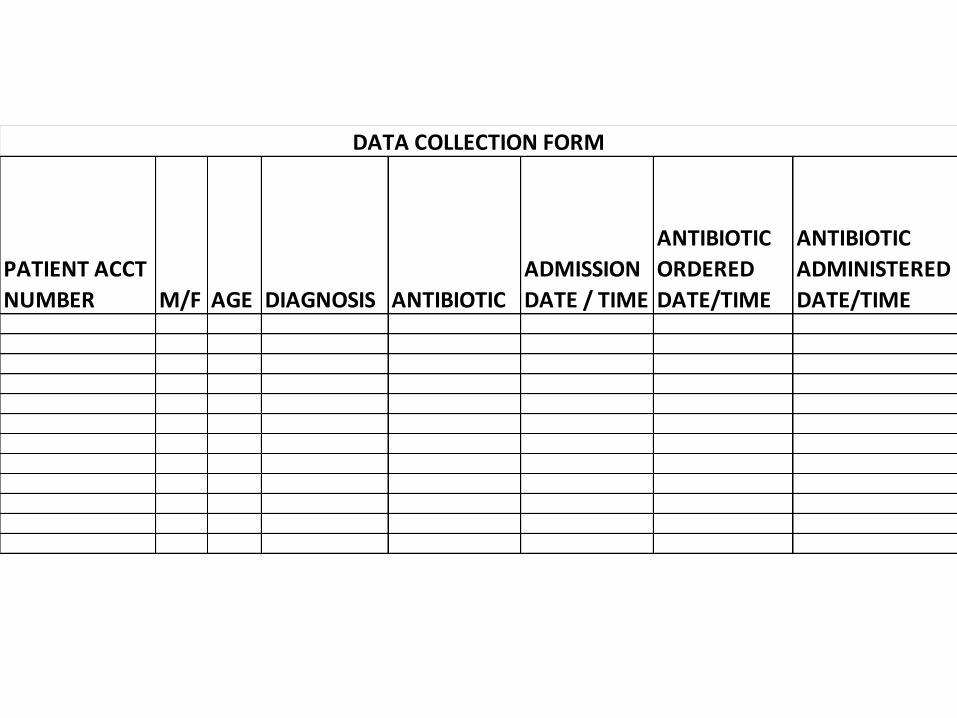
PATIENT ACCT
NUMBER M/F AGE DIAGNOSIS ANTIBIOTIC
ADMISSION
DATE / TIME
ANTIBIOTIC
ORDERED
DATE/TIME
ANTIBIOTIC
ADMINISTERED
DATE/TIME
DATA COLLECTION FORM

Hospital ASP: Action Plan
• Hospital –
– Antibiogram (susceptibility AND incidence rate)
– Timely C&S final results
– Protocols (sepsis, CAP, etc)
– IV to PO (bioavailability considerations)
– Renal adjustment
– 48-hour Time Out
– ID consult / restrictions / rotation
Long-Term Care ASP
• 4.1 million Americans in nursing homes
• 70 percent receive at least 1 round of antibiotics per year
• Up to 75 percent are unnecessary or wrong antibiotic / dose / duration
http://www.cdc.gov/media/releases/2015/p0915-nursing-home-antibiotics.html
Long-Term Care ASP
• Nursing leadership
• “Emergency Drug Box” access
• Intermittent Pharmacist presence
• Prophylactic therapy

Long-Term Care ASP Applications
• Form ASP team
• Review proposed TJC standard
• Complete CDC Checklist (gap analysis)
• Baseline chart reviews (common / complex)
• Antibiogram
• Action Plan (measurable outcomes)
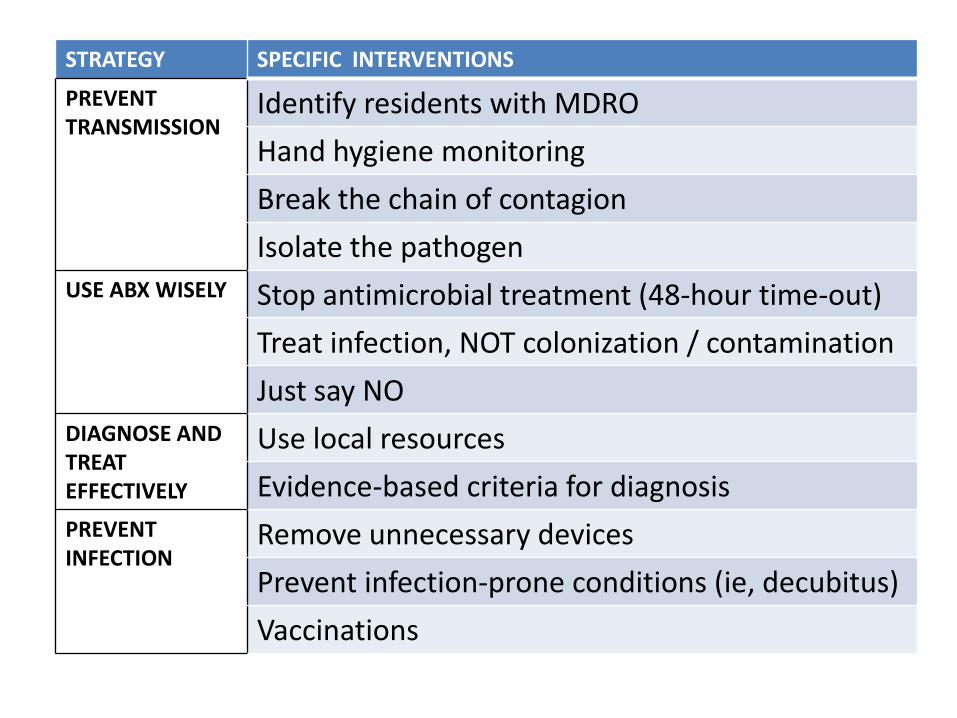
STRATEGY SPECIFIC INTERVENTIONS
PREVENT TRANSMISSION
Identify residents with MDRO
Hand hygiene monitoring
Break the chain of contagion
Isolate the pathogen
USE ABX WISELY Stop antimicrobial treatment (48-hour time-out)
Treat infection, NOT colonization / contamination
Just say NO
DIAGNOSE AND TREAT EFFECTIVELY
Use local resources
Evidence-based criteria for diagnosis
PREVENT INFECTION
Remove unnecessary devices
Prevent infection-prone conditions (ie, decubitus)
Vaccinations
Long-Term Care ASP: Action Plan
• Long-term care
– Consultant pharmacist
– 48-hour time out
– Prevent outbreaks
– Competency training for Rapid Response
– PPE / Isolation precautions for MDRO
– Viral vs bacterial
– Length of therapy
– C diff risk factors
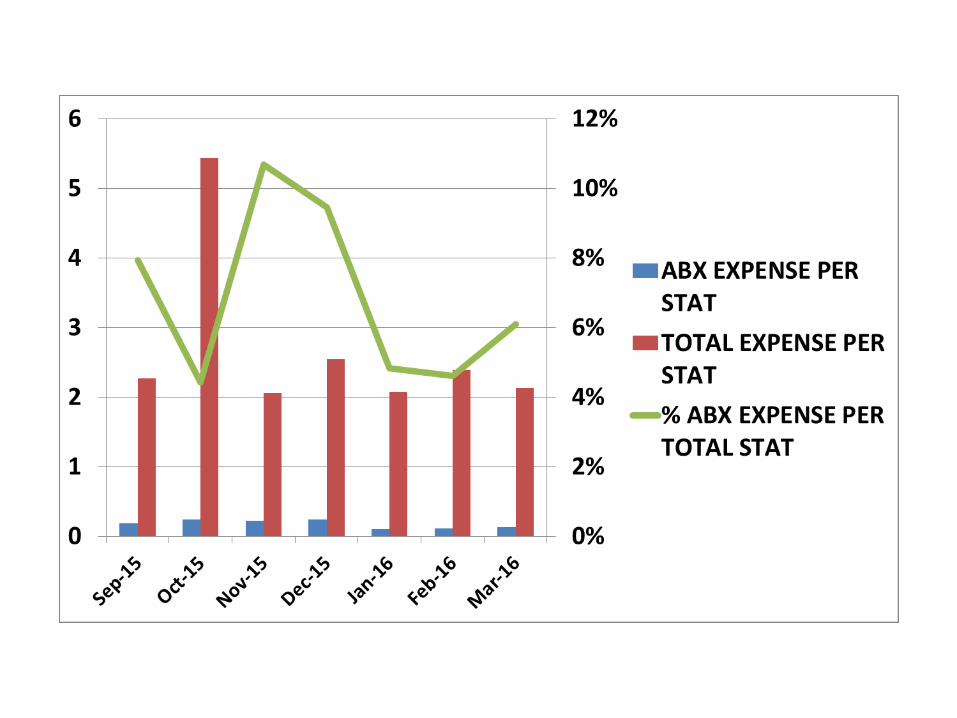
Current Key Metrics (ROI?)
• Affects reimbursement: – VBP: Readmission rates
– VBP: Patient satisfaction / HCAHPS
– VBP: HAI, not documented on admission “HARM”
– VBP: Core measures – time to 1st dose; pre-op
– Transparency, Public perception
• Affects costs: – Antibiotic costs (per: stat, APD, admission; total $)
– LOS, LOTx, Days on Vent, Catheter Days
PDSA
• PLAN – Baseline key metrics to identify problem areas
• DO – Implement prioritized interventions
• STUDY – Measure direct / indirect metrics for impact
• ACT – Hardwire successful interventions

Stewardship
• The sensitivity of bacteria to antibiotics should be managed as a finite natural resource
• Unsustainable use of antibiotics, combined with a dearth of new drugs, threatens to usher us back to an era when common infections were incurable or very costly to treat.
• A name change to ‘antimicrobial safety’ can accelerate acceptance of the importance of antimicrobial stewardship