anxiety presentation
TRANSCRIPT
Anxiety Management
PresenterDr. Anusa A MFirst year MD PG
Prepared by Prof. Rooban T,
Oral & Maxillofacial Pathologist
What is anxiety ?
Physical and emotional distress which interfere with normal life.
Physiological Anxiety
I have a presentation I have a tough exam I have an important interview
Should I be anxious ?
“Anxiety is an emotional state, unpleasant in nature, associated with uneasiness, discomfort and concern or fear about some defined or undefined future threat”
Pathological Anxiety
Some degree of anxiety is a part of normal life; but psychotics exhibit pathological anxiety, therefore, treatment is required.
Common Symptoms of Anxiety
EMOTIONAL SYMPTOMS
Irrational & excessive
fear, worry
Irritability
Restlessness
Trouble concentrating
Feeling tense
PHYSICAL SYMPTOMS
Sweating
Tachycardia
Stomach upset
Shortness of breath
Frequent urination or diarrhea
Sleep disturbances (Insomnia)
Fatigue
Types of Anxiety
Primary/Situational
Panic disorder
Generalized anxiety disorder
Obsessive-compulsive disorder
Post traumatic stress disorder
Phobic disorders
Secondary/Non-situational
Medical conditions
Substance abuse
Psychiatric conditions
Psychosocial stress
DSM IV-TR. Washington, DC: American Psychiatric Association. 2000.
Generalized Anxiety Disorder
Excessive anxiety and worry about a number of events for the majority of days over 6 months
Difficulty in controlling the worry
Associated with at least 3 physical and psychological symptoms
Causes significant distress or impairment
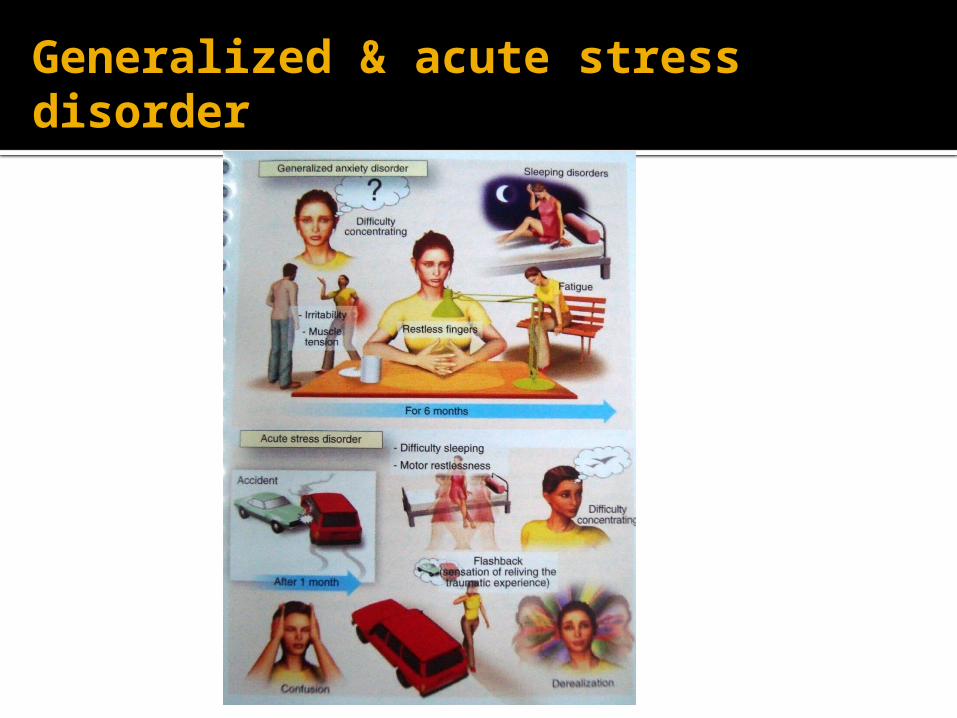
Generalized & acute stress disorder
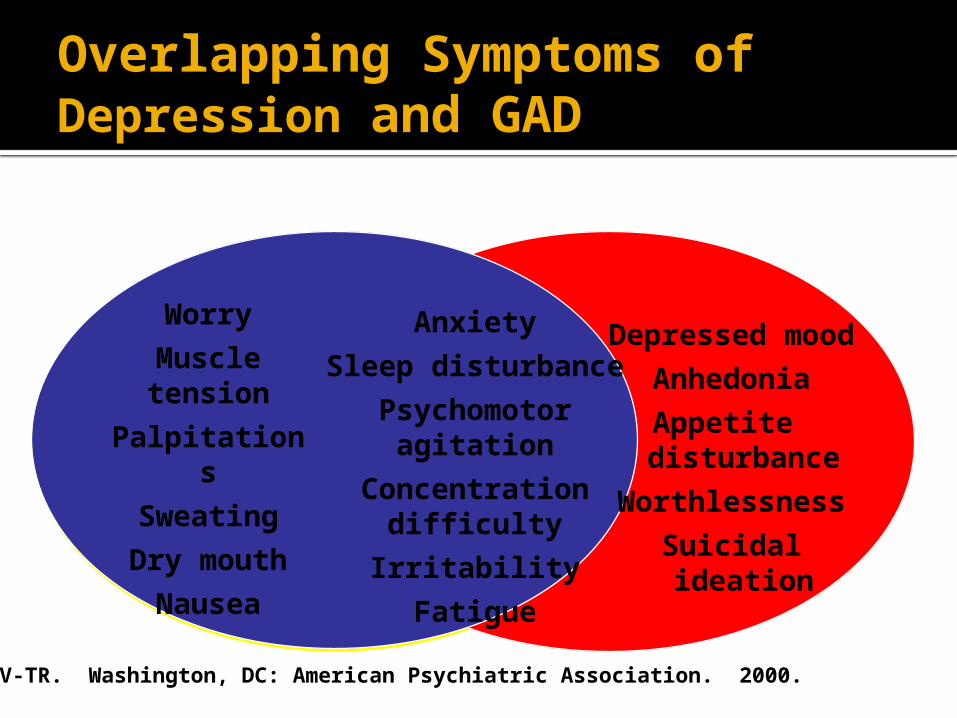
Depressed mood
Anhedonia
Appetite disturbance
Worthlessness
Suicidal ideation
Anxiety
Sleep disturbance
Psychomotor agitation
Concentration difficulty
Irritability
Fatigue
Worry
Muscle tension
Palpitations
Sweating
Dry mouth
Nausea
Overlapping Symptoms of Depression and GAD
DSM-IV-TR. Washington, DC: American Psychiatric Association. 2000.
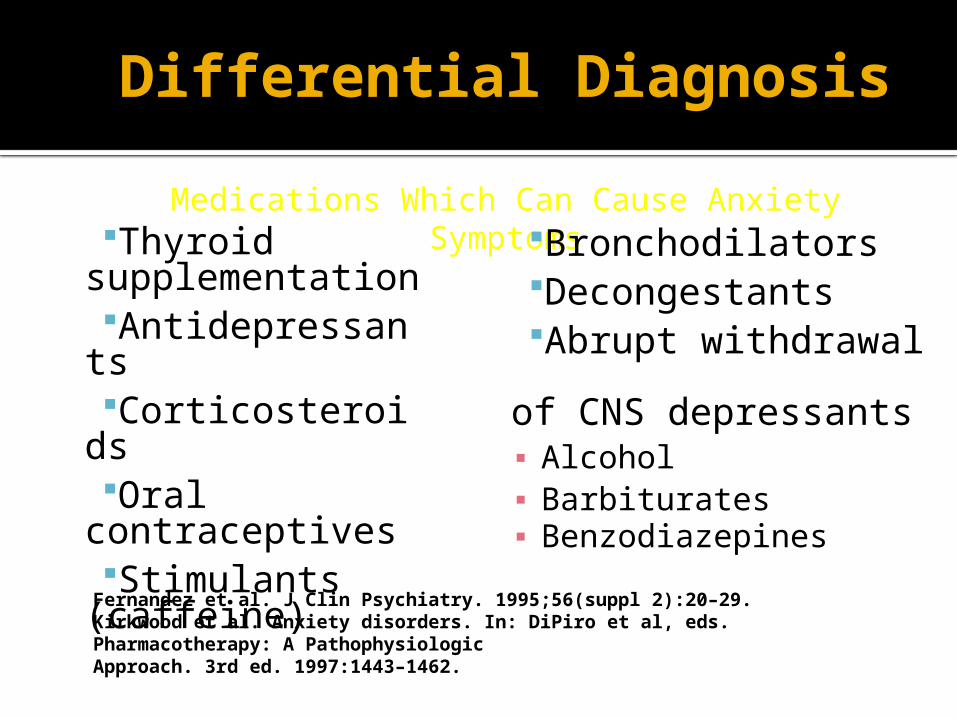
Fernandez et al. J Clin Psychiatry. 1995;56(suppl 2):20–29.Kirkwood et al. Anxiety disorders. In: DiPiro et al, eds. Pharmacotherapy: A Pathophysiologic Approach. 3rd ed. 1997:1443–1462.
Differential Diagnosis Medications Which Can Cause Anxiety Symptoms
Thyroid supplementationAntidepressants CorticosteroidsOral
contraceptivesStimulants
(caffeine)
BronchodilatorsDecongestantsAbrupt withdrawal
of CNS depressants▪ Alcohol ▪ Barbiturates▪ Benzodiazepines
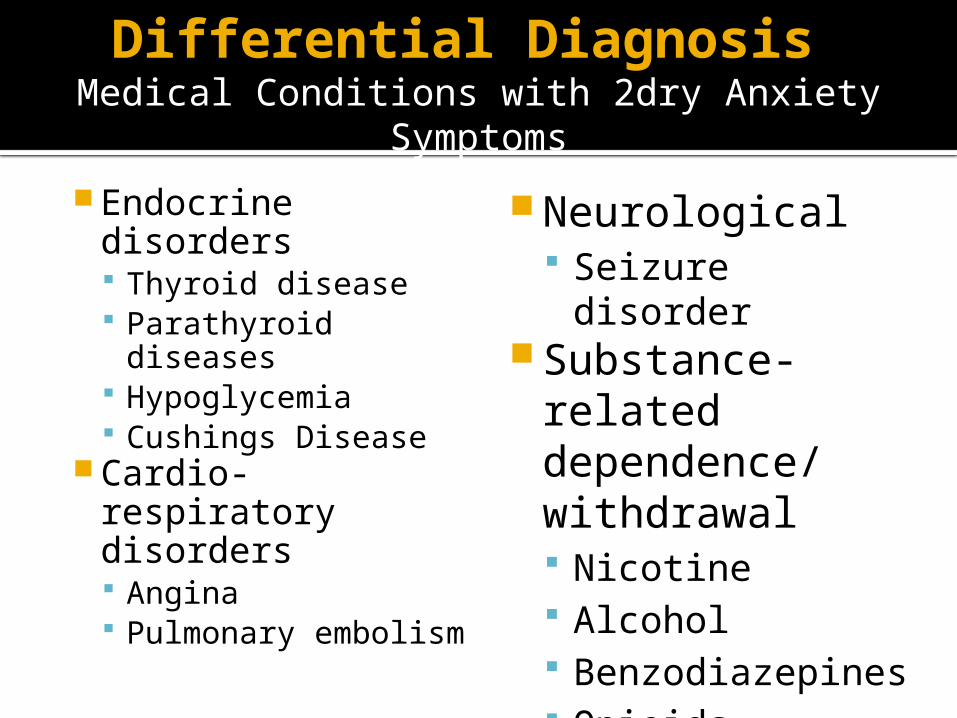
Differential Diagnosis Medical Conditions with 2dry Anxiety Symptoms
Endocrine disorders Thyroid disease Parathyroid
diseases Hypoglycemia Cushings Disease
Cardio-respiratory disorders Angina Pulmonary
embolism
Neurological Seizure disorder
Substance-related dependence/ withdrawal Nicotine Alcohol Benzodiazepines Opioids
Obsessive-Compulsive Disorder (OCD)
An anxiety disorder in which people cannot prevent themselves from unwanted thoughts or behaviors that seem impossible to stop as washing their hands
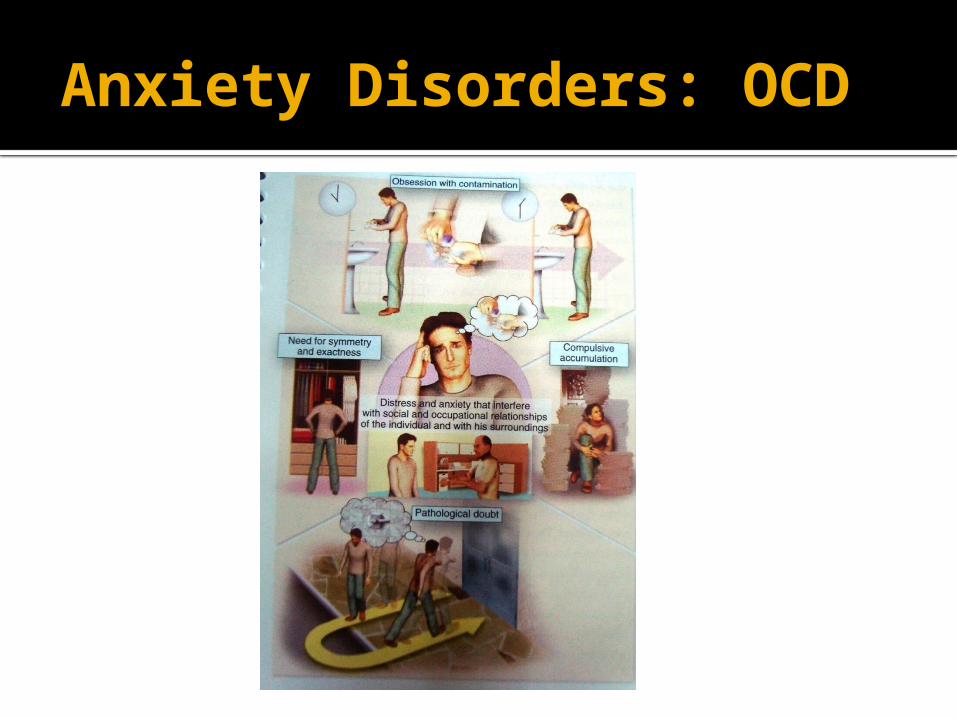
Anxiety Disorders: OCD
Obsessive-Compulsive Disorder
Obsessions:
1) recurrent or persistent thoughts, impulses, or images are
experienced as intrusive or inappropriate and cause distress
2) not simply excessive worries about real-life problems
3) person attempts to ignore or suppress thoughts or
neutralize them with another thought or action
4) person recognizes that obsessions are product of his/her
mind, not imposed from without
DSM IV-TR. Washington, DC: American Psychiatric Association. 2000. 15
Obsessive-Compulsive Disorder
Compulsions:1) repetitive behaviors or mental acts
performed in response to an obsession or according to certain rules
2) designed to neutralize or prevent discomfort or some dreaded event or situation
DSM IV-TR. Washington, DC: American Psychiatric Association. 2000. 16
Obsessive-Compulsive Disorder
Obsessions and compulsions:
cause marked distress
time-consuming
Significantly interfere with normal routine,
occupational functioning
Usual social activities or relationships with others
DSM IV-TR. Washington, DC: American Psychiatric Association. 2000. 17
Rasmussen & Eisen (1992a) Zetin & Kramer (1992)
Common obsessions in OCD
Contamination
Pathological doubt
Aggressive impulse
Somatic concerns
Need for symmetry
Sexual impulse
Rasmussen & Eisen (1992a) Zetin & Kramer (1992)
Common Compulsions in OCD
Washing
Checking
Counting
Symmetry and precision
Need to ask or confess
Hoarding
19
OCD Treatments
Behavior Therapy (Exposure and
Response Prevention)
Pharmacotherapy (SSRI)
Combination
20
Behavior Therapy for OCDExposure and Response Prevention
Systematic and intensive treatment
Stimuli for rituals and avoidance identified
and assigned a place in a hierarchy of
anxiety provocation
Intensive exposure to stimuli is done both
with therapist and as homework
Exposure is graded from easiest to most difficult
Rituals omitted or, if not possible, delayed21
Steiner et al. Presented at the American Psychiatric Association Annual Meeting, May, 1995.
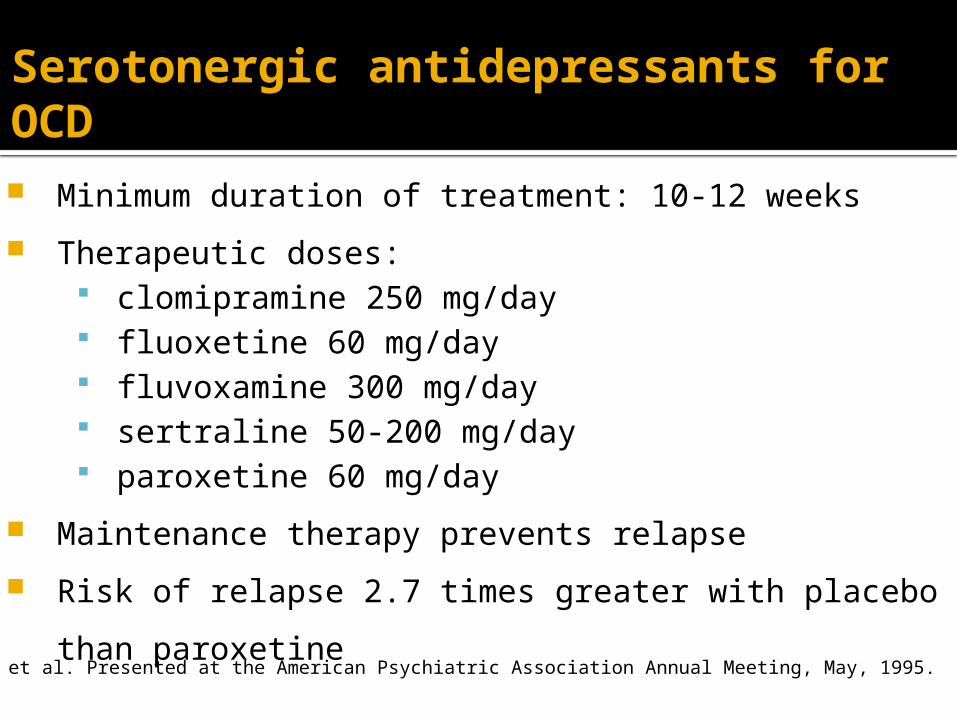
Serotonergic antidepressants for OCD Minimum duration of treatment: 10-12 weeks
Therapeutic doses: clomipramine 250 mg/day fluoxetine 60 mg/day fluvoxamine 300 mg/day sertraline 50-200 mg/day paroxetine 60 mg/day
Maintenance therapy prevents relapse
Risk of relapse 2.7 times greater with placebo than
paroxetine
Panic Disorder
An disorder in which people have sudden and intense attacks of anxiety in certain situations.
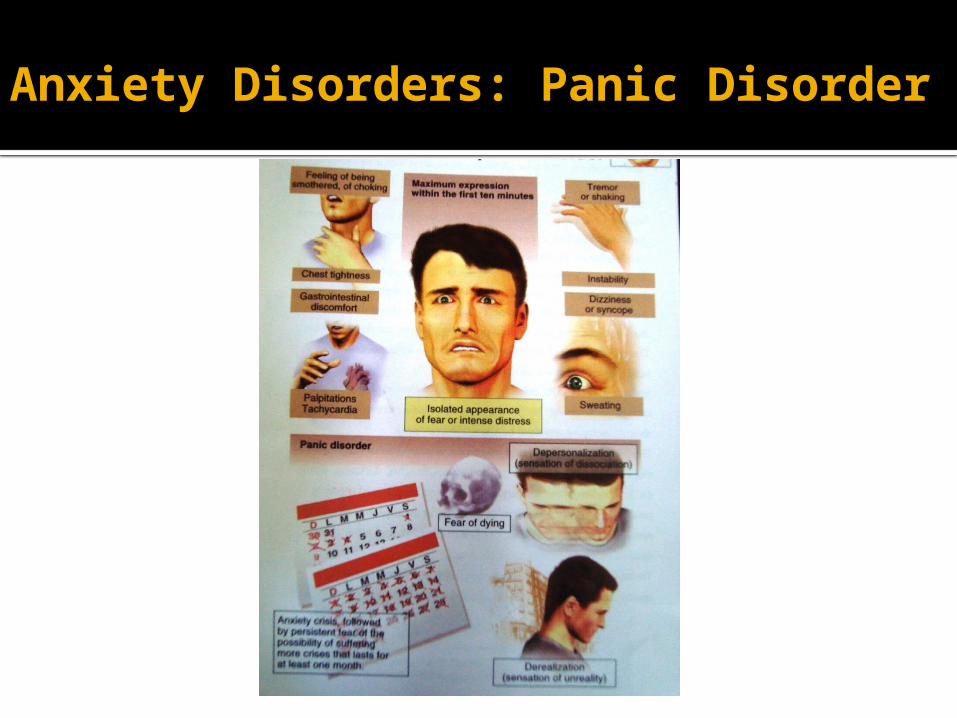
Anxiety Disorders: Panic Disorder
Panic Disorder Treatment:General Principles
Pharmacotherapy
Cognitive-Behavior Therapy (CBT)
Manual-driven CBT treatment to
normalize “catastrophic thinking”
Exposure to panic symptoms and other
feared situations
Panic Disorder Treatment:General Principles
Pharmacotherapy Selective serotonin reuptake inhibitors first line
due to favorable side effect profile
Other antidepressant classes work also
Venlafaxine (Effexor) is effective
Nefazodone(Serzone) no longer on US market due to liver
toxicity
Benzodiazepines and Beta-blockers useful
adjunctive treatments for residual symptoms
SSRI’s -PRACTICAL USAGE IN PANIC DISORDER
Sertraline• 1st week : 5mg/day for 2-3 days & if no side effects
50mg days 4-7• 2nd week-:75mg/day-days 8-10 & if no side effects
100mg days 11-14 • 3rd week-----------------------125 mg/day----if no response• 4-6 week-----------------------150mg/day ----if no response• 6 weeks & beyond-----------200mg/day & if partial
response consider up to 250-300mg day• With sertraline might need a benzodiazepine (Xanax or
Ativan-0.25-0.5mg bid-tid for breakthrough anxiety)
Paroxetine • 1st week-------------------------10mg/day for 2-4 days & if no side effects 20mg days 4-7• 2-3 weeks-----------------------30mg/day--if no response• 4-6 weeks-----------------------40mg/day-- if no response• 6 weeks & beyond-------------50-60mg/day as needed• With paroxetine less of a need for a benzodiazepine
Escitalopram• 1st week------------------------ -5 mg/day for 2 days then 10mg days 3-7• 2nd week------------------------ 10mg/day--if no response• 3rd thru 5thweek--------------15mg/day ----if no response• 6 weeks & beyond--------------20 mg/day as needed• Though 20mg is PDR recommended maximum, often 25-30 may be given to patients with partial
responses at 20mg and no side effects
SSRI’s -PRACTICAL USAGE IN PANIC DISORDER
Post-traumatic stress disorder
An anxiety disorder that affects people who have experienced a severe emotional trauma, such as rape or dramatic car accident, or even war.
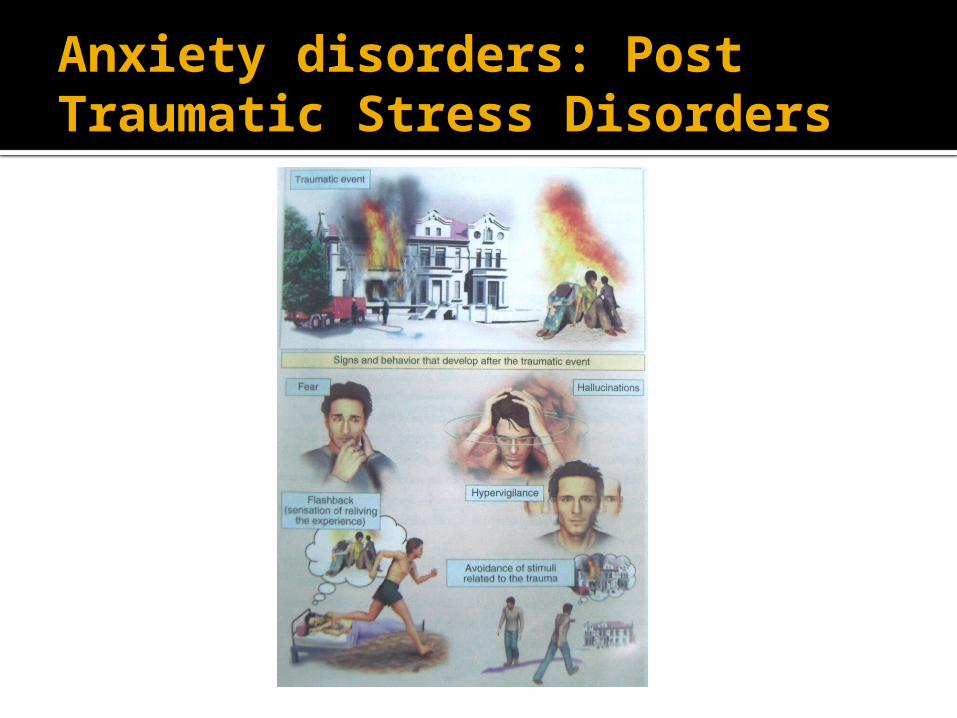
Anxiety disorders: Post Traumatic Stress Disorders
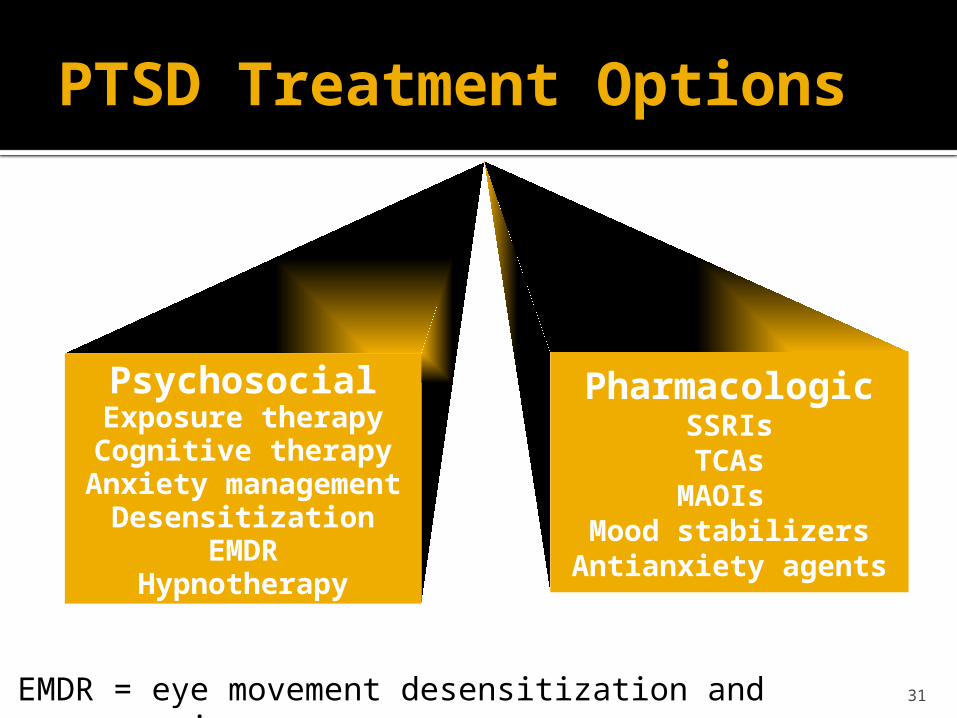
PsychosocialExposure therapyCognitive therapy
Anxiety managementDesensitization
EMDRHypnotherapy
PTSD Treatment Options
PharmacologicSSRIsTCAs
MAOIs Mood stabilizers
Antianxiety agents
EMDR = eye movement desensitization and reprocessing. 31
An intense, uncontrolled fear of a specific situation such as open spaces & heights
Anxiety Disorder: Phobias
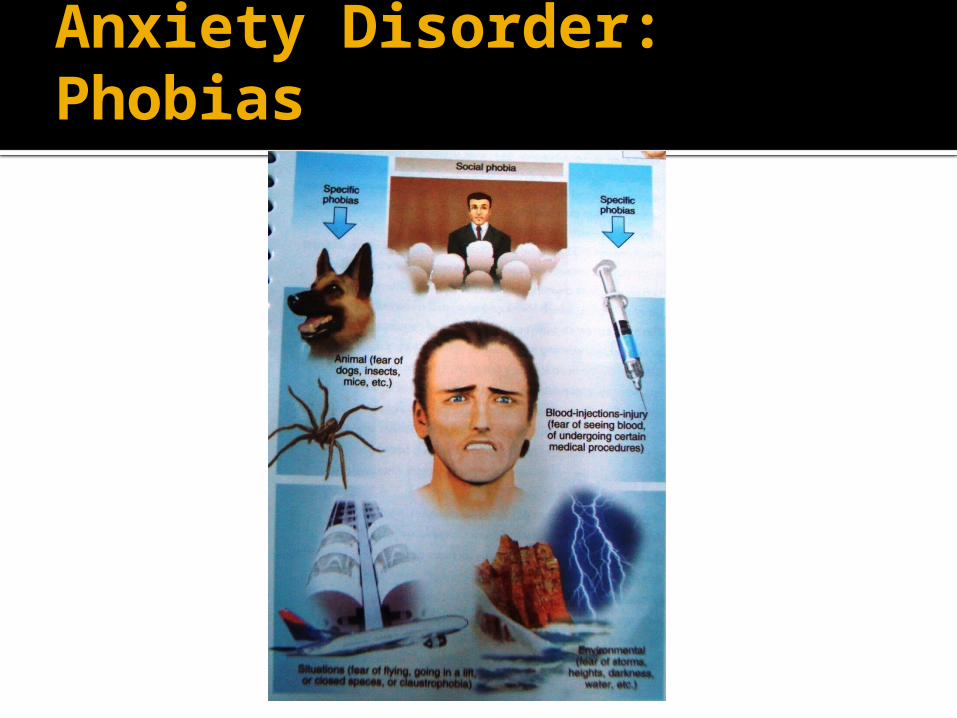
Anxiety Disorder: Phobias
Symptoms of social anxiety disorderFeared situations
Social Attending parties,
weddings etc Conversing in a group Speaking on
telephone Interacting with
authority figure (eg teacher or boss)
Making eye contact Ordering food in a
restaurant
Performance Public speaking Eating in public Writing a check Using public toilet Taking a test Trying on clothes in a
store Speaking up at a
meeting
34
Social anxiety disorder
CombinationCBT + pharmacotherapy
MAOIs
Benzodiazepines CBT
SSRIs
Social anxiety disorderTreatment options
35
Social anxiety disorder Treatment goals
Control anxiety and phobic avoidance Reduce associated disability Treat depression / other comorbid
disorders Tolerability over long term Eventual medication-free status
36
Pharmacological management of social anxiety disorder
Consider initial choice of an SSRI Initial dose for 2-4 weeks, then increase if
necessary example sertraline: 100mg/day with increase to
200mg/day Some benefit evident by 2-4 weeks If no response by 6-8 weeks, switch to drug
of another class or augment Consider psychosocial treatments Continue pharmacotherapy for at least 1 year
37
Social Anxiety Disorder: Pharmacological Treatments
Monoamine oxidase inhibitors
(standard/RIMAs)
Benzodiazepines
SSRIs--leading choice as sertraline
and paroxetine are FDA approved for
this disorder38
Treatment of anxiety
Psychotherapy (cognitive behavioral therapy).
Anxiolytics
Classification of anxiolytic drugs:
1. Benzodiazepines ( BDZ ).
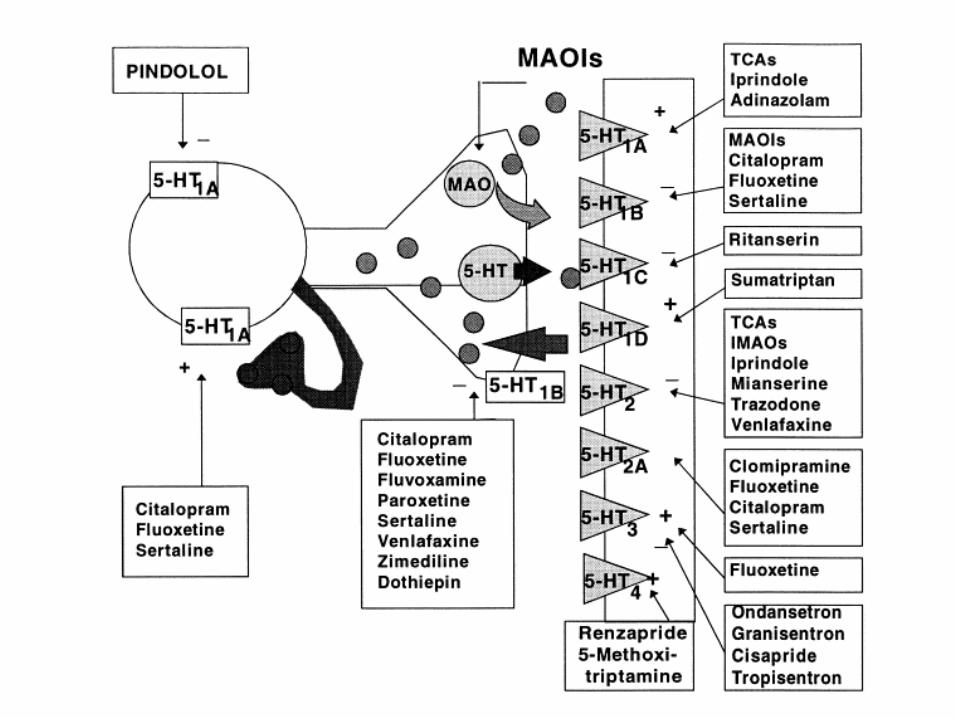
2. 5HT1A agonists.
3. 5HT reuptake inhibitors.4. Antidepressants5. Beta adrenergic blockers6. MAO inhibitors 7. Mood Stabilizers (?)
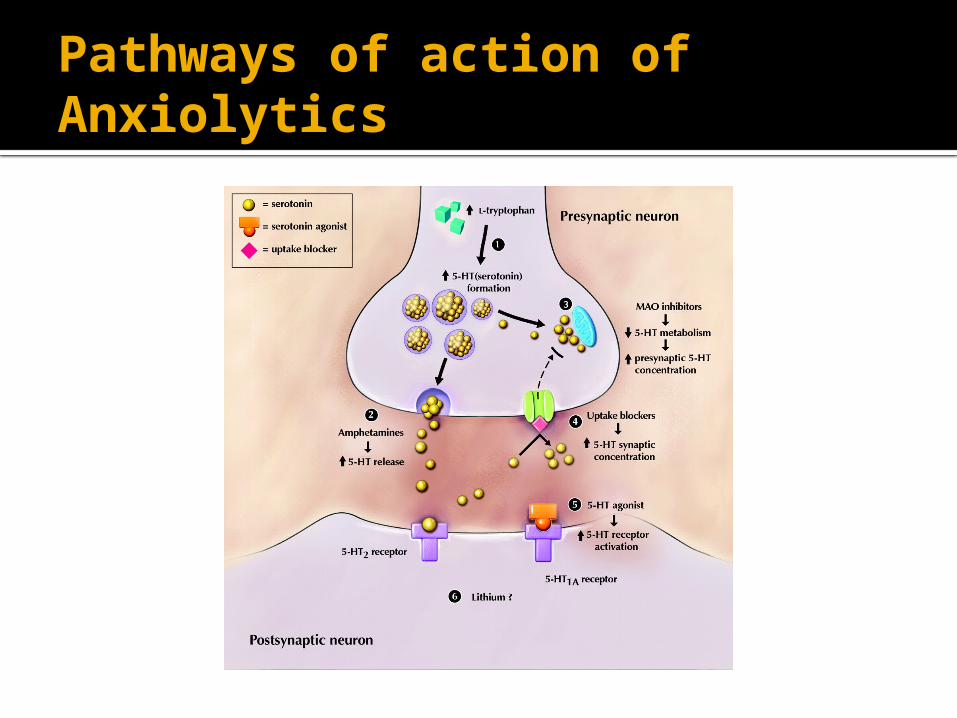
Pathways of action of Anxiolytics
Classifications of Benzodiazepines
- Short acting: (3-5 hours): triazolam
- Intermediate: (6-24 hours)
Alprazolam
Lorazepam
Oxazepam
Estazolam
Temazepam
Classifications of Benzodiazepines
- Long acting: ( 24-72 hours) Clonazepam Chlordiazepoxide Diazepam Flurazepam
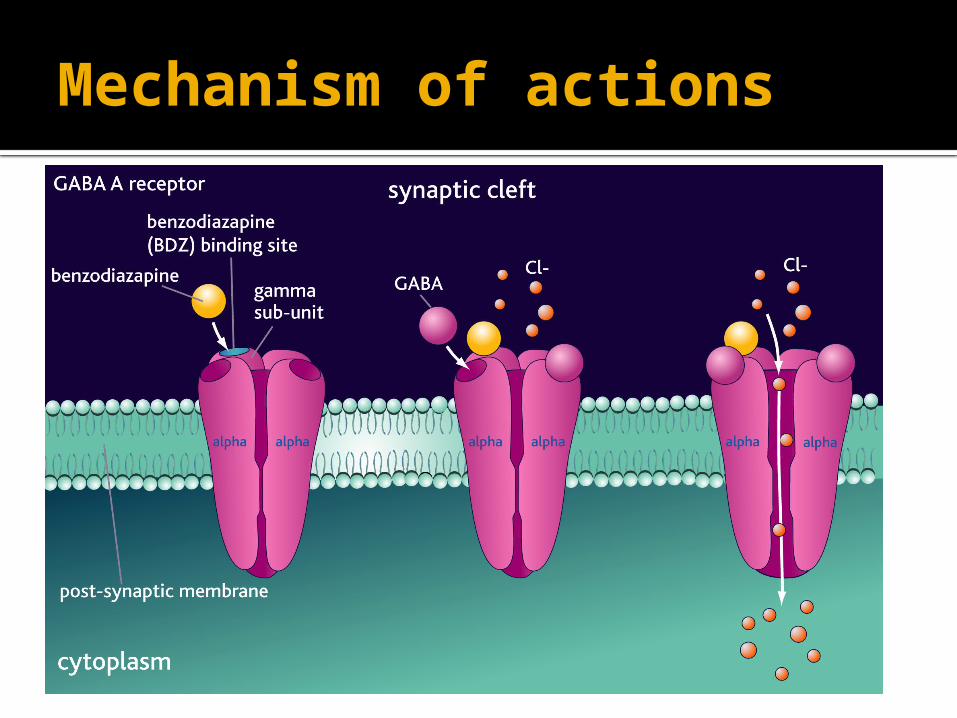
Mechanism of actions
Pharmacokinetics
are lipid soluble
well absorbed orally,
can be given parenterally
Chlordiazepoxide- Diazepam (IV only NOT IM)
widely distributed.
cross placental barrier (Fetal depression).
excreted in milk (neonatal depression).
Pharmacokinetics
metabolized in the liver to active metabolites (long duration of action- cumulative effect).
Redistribution from CNS to skeletal muscles, adipose tissue) (termination of action).
Pharmacological Actions
Anxiolytic action.
Depression of cognitive & psychomotor
function
Sedative & hypnotic actions
Anterograde amnesia.
Pharmacological Actions
Minimal depressant effects on
Cardiovascular system
Respiratory system
Some have anticonvulsant effect:
clonazepam, diazepam.
Adverse effects
• Ataxia (motor in coordination)
• Cognitive impairment.
• Hangover: (drowsiness, confusion)
• Tolerance & dependence
• Risk of withdrawal symptoms
Rebound Insomnia, anorexia, anxiety,
agitation, tremors and convulsion.
Adverse effects
Toxic effects:
Respiratory Depression
cardiovascular depression in large doses.

Drug interactions
Examples
CNS depressants Alcohol & Antihistaminics of effect of benzodiazepines
Cytochrome P450 (CYT P450) inhibitors
Cimetidine & Erythromycin
t ½ of benzodiazepines
CYT P450 inducers Phenytoin & Rifampicint 1/2 of benzodiazepines
Drug interactions
Dose should be reduced in
o Liver diseaseo Old people.
Precaution Should not used in pregnant women or breast-feeding. People over 65.
5HT1A agonists - Buspirone
acts as agonist at brain 5HT1A receptors
rapidly absorbed orally.
Slow onset of action (delayed effect)
T½ : (2 – 4 hrs).
liver dysfunction its clearance.
Drug Interactions with CYT P450 inducers
and inhibitors.
Buspirone
Only anxiolytic
No hypnotic effect.
Not muscle relaxant.
Not anticonvulsant.
No potentiation of other CNS depressants.
Minimal psychomotor and cognitive dysfunctions.
Does not affect driving skills.
Minimal risk of dependence.
No withdrawal signs.
Uses of buspirone
As anxiolytic in mild anxiety & generalized
anxiety disorders.
Not effective in severe anxiety/panic disorder.
Beta Blockers
Propranolol – atenolol
act by blocking peripheral sympathetic
system.
Reduce somatic symptoms of anxiety.
Decrease BP & slow HR.
Used in social phobia.
are less effective for other forms of anxiety
Tricyclic Antidepressants
Doxepin- imipramine
act by reducing uptake of 5HT & NA.
Used for anxiety associated with depression.
Effective for panic attacks.
Delayed onset of action (weeks).
dry mouth, postural hypotension, sexual
dysfunction, weight gain.
Selective serotonin reuptake inhibitors (SSRIs)
Fluoxetine
acts by blocking uptake of 5HT
Orally
Delayed onset of action (weeks).
Used for panic disorder – OCD depression-
Generalized anxiety disorders - phobia.
Side Effects:
Weight gain, sexual dysfunction, dry mouth
MONOAMINE OXIDASE INHIBITORS
Phenelzine Acts by blocking MAO enzymes. Used for panic attacks and phobia. Require dietary restriction Avoid wine, beer, fermented foods as
old cheese that contain tyramine. Side effects - Dry mouth, constipation,
diarrhea, restlessness, dizziness
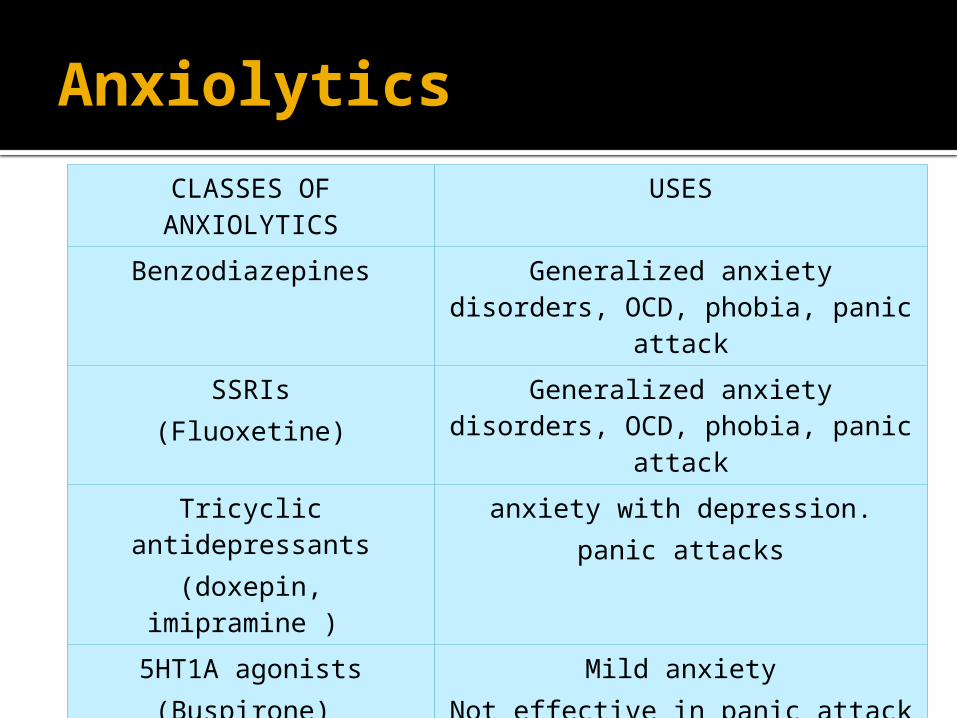
Anxiolytics
CLASSES OF ANXIOLYTICS USES
Benzodiazepines Generalized anxiety disorders, OCD, phobia, panic attack
SSRIs(Fluoxetine)
Generalized anxiety disorders, OCD, phobia, panic attack
Tricyclic antidepressants(doxepin, imipramine )
anxiety with depression.panic attacks
5HT1A agonists(Buspirone)
Mild anxietyNot effective in panic attack
Beta blockers (propranolol, atenolol)
Phobia (social Phobia)
MAO inhibitorsPhenelzine
Panic attack, phobia
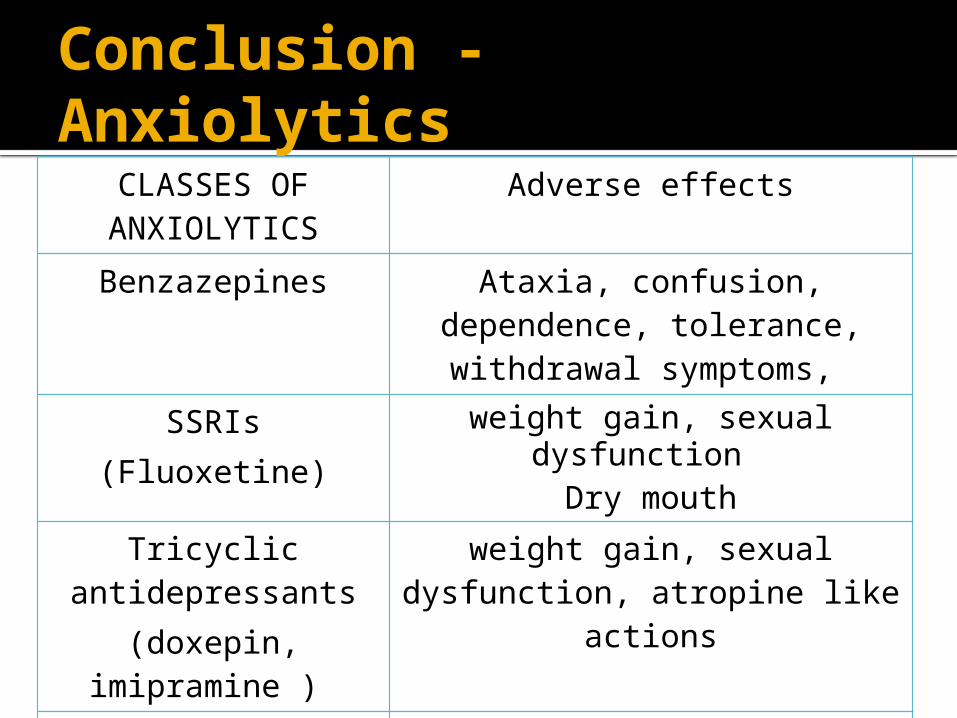
Conclusion - AnxiolyticsCLASSES OF ANXIOLYTICS
Adverse effects
Benzazepines Ataxia, confusion, dependence, tolerance, withdrawal
symptoms,
SSRIs(Fluoxetine)
weight gain, sexual dysfunction Dry mouth
Tricyclic antidepressants
(doxepin, imipramine )
weight gain, sexual dysfunction, atropine like
actions
5HT1A agonists(Buspirone)
Minimal adverse effects
Beta blockers (propranolol, atenolol)
Hypotension
Thank You