“intelligence is the ability to adapt to change…” “if there´s a will, … › bitstream ›...
TRANSCRIPT

“Intelligence is the ability to adapt to change…”
“If there´s a will, there´s a way…”
Stephen Hawking
Patient with Amyotrophic Lateral Sclerosis and a ventilator user. English theoretical physicist and cosmologist, was the Lucasian Professor of Mathematics at the University of Cambridge for thirty years, taking up the post in 1979 and retiring on 1 October 2009, year he was awarded the Presidential Medal of Freedom, the highest civilian award in the United States.


Research work and line of investigation developed as
part of a PhD Thesis in Biomedicine presented at the
Faculty of Medicine of the University of Porto
PhD Tutors:
• Professor João Carlos Winck Fernandes Cruz
Faculty of Medicine, University of Porto
• Professor John Robert Bach
University of Medicine and Dentistry of New Jersey Medical School


Official Jury:
• President –Professor José Agostinho Marques
Director of the Faculty of Medicine, University of Porto
• Professor Dominique Robert
Faculty of Medicine, University of Lyon, France
• Professor Massimo Antonelli
Faculty of Medicine, Policlinico Universitario A. Gemelli, Universitá Cattolica del Sacro Cuore, Rome Italy
• Professor João Carlos Winck Fernandes Cruz
Faculty of Medicine, University of Porto
• Professor Maria Isabel Amorim de Azevedo
Faculty of Medicine, University of Porto
• Professor Henrique José Correia Queiroga
Faculty of Medicine, University of Porto
• Professor Marta Susana Monteiro Drummond de Freitas
Faculty of Medicine, University of Porto


CONTENTS
Introduction ___________________________________________________________________ 1
Historical perspective of mechanical ventilation and respiratory muscle aids _____________ 5
Equipments and techniques for noninvasive positive pressure ventilation _______________ 21
Characteristics of different modes of ventilation _____________________________ 21
Pressure cycled ventilation __________________________________________ 22
Volume cycled ventilation ___________________________________________ 25
Ventilators with mixed pressure and volume target modes __________________ 27
Interfaces for the delivery of NPPV ________________________________________ 28
Humidification during NPPV _____________________________________________ 31
Noninvasive ventilation in the acute care setting ____________________________________ 32
Rationale ______________________________________________________________ 32
Chronic obstructive pulmonary disease with acute exacerbation ________________ 35
Acute Cardiogenic Pulmonary Edema ______________________________________ 37
Hypoxemic Respiratory Failure ___________________________________________ 38
Imunocompromised patients ______________________________________________ 39
Weaning from Invasive ventilation and post extubation failure _________________ 40
Acute Respiratory Failure in Restrictive Disorders ___________________________ 41
Chest wall disorders _______________________________________________ 42
Neuromuscular Disorders ___________________________________________ 43
Amyotrophic Lateral Sclerosis _______________________________________ 44
Gullian-Barré syndrome and Myastenia Gravis __________________________ 49
Spinal Cord Injury _________________________________________________ 49
Critical- illness myoneuropathy _______________________________________ 51
Contraindications to NPPV in acute care ___________________________________ 51
Noninvasive ventilation in the chronic care setting __________________________________ 53
Rationale ______________________________________________________________ 53
Indications of Noninvasive ventilatory support _______________________________ 54
Disease categories _________________________________________________ 54
Patient selection ___________________________________________________ 55
Physiologic evaluations _____________________________________________ 56
Muscle strength ___________________________________________________ 57

Blood Gases ______________________________________________________ 58
Noninvasive ventilation in stable COPD ____________________________________ 59
Noninvasive ventilation in Restrictive Disorders ______________________________ 62
Chest wall disorders _______________________________________________ 62
Amyotrophic Lateral Sclerosis _______________________________________ 63
Duchenne muscular dystrophy _______________________________________ 65
Manual and Mechanical techniques for secretion management ________________________ 68
Rationale ______________________________________________________________ 68
Patient evaluation and monitoring _________________________________________ 71
Pulmonary function and cough tests ________________________________________ 72
Control of Mucus and Airway Clearance Techniques _________________________ 74
Chest physical therapy techniques _____________________________________ 75
Manual Assisted Cough techniques ____________________________________ 76
Mechanical Respiratory Muscle Aids for Secretion Management _______________ 78
Intrapulmonary Percussive Ventilation (IPV) ____________________________ 79
High Frequency Chest Wall Oscillation (HFCWO) _______________________ 80
Mechanical Insufflation-Exsufflation __________________________________ 82
Purpose of the Thesis __________________________________________________________ 86
Acute Respiratory Failure ________________________________________________________ 87
Chronic Respiratory Failure ______________________________________________________ 93
Home mechanical ventilation ____________________________________________________ 101
Studies and Publications _______________________________________________________ 109
Study 1- Extubation of Patients with Neuromuscular Weakness: A New
Management Paradigm _________________________________________________________ 109
Study 2- Noninvasive ventilation associated with mechanical assisted cough for
extubation and decannulation in high spinal cord injury patients ________________________ 121
Study 3- Effects of mechanical insuffaltion-exsufflation in preventing respiratory failure after
extubation: a randomized controlled trial __________________________________________ 147
Study 4- A Ventilator Requirement Index ___________________________________________ 169
Study 5- Expiratory Flow Maneuvers of Patients with Neuromuscular Disease _____________ 179
Study 6- Lung Insufflation Capacity in Neuromuscular Disease. ________________________ 189
Study 7- Indications and Compliance of Home Mechanical Insufflation-Exsufflation in Patients
with Neuromuscular Diseases ____________________________________________________ 197

Study 8- At Home and On Demand Mechanical Cough Assistance Program for Patients with
Amyotrophic Lateral Sclerosis ___________________________________________________ 205
Study 9- Home mechanical cough assistance for acute exacerbations in neuromuscular
disease ______________________________________________________________________ 213
Study 10- Evolution of Noninvasive Management of End-Stage Respiratory Muscle Failure in
Neuromuscular disease. ________________________________________________________ 231
General Discussion ___________________________________________________________ 265
Acute Respiratory Failure ________________________________________________ 265
Chronic Respiratory Failure _______________________________________________ 277
Home mechanical ventilation ______________________________________________ 285
Conclusions _________________________________________________________________ 299
Resumo _____________________________________________________________________ 301
Objectivos _____________________________________________________________ 302
Resultados ____________________________________________________________ 303
Conclusões ____________________________________________________________ 306
Summary (Abstract) __________________________________________________________ 308
Purpose _______________________________________________________________ 309
Results _______________________________________________________________ 310
Conclusions ___________________________________________________________ 313
References __________________________________________________________________ 314


Acknowledgments
� To Professor John Bach for all the guidance, mentorship and lessons throughout my clinical and academic career. It has been my greatest honor to be taught and trained by who i consider to be the most brilliant mind in the field of noninvasive ventilation. It is a privilege to be his friend and his personal and professional influence will be eternal in my life.
� To Professor João Carlos Winck for always believing in my work and always being there as a mentor and a very special friend. His teachings and advices were the support of this thesis and made me a better academic and clinical professional. It has been a great privilege to share with him the “challenge” of changing the paradigms and improving respiratory care in our country.
� To Professor Agostinho Marques for always making me believe in my potential to achieve this PhD degree. I will always be thankful to him for this opportunity and for his contribution to make this dream possible.
� To all the staff of the Pulmonology Department, Hospital S. João for the motivation and support throughout this thesis. It is a privilege for me to work in this department where a fantastic multidisciplinary “team work” spirit was crucial to perform this line of research. A special thanks to my colleague Tiago Pinto, Professor Marta Drummond, Dr João Almeida, Dr João Bento and Dr Anabela Marinho that gave me great support and actively contributed to this thesis line of research.
� To all the medical and nursing staff of the Intensive Care and Emergency Department, Hospital S. João for the motivation and both clinical and technical support in the critical care studies of this thesis. It has been an overwhelming experience to share knowledge and learn new concepts in this department. A special thanks to Dr Teresa Honrado, Dr Teresa Oliveira, Dr Celeste Dias, Dr Ana Maria Mota and Professor José Artur Paiva for trusting and believing in my research as well as in my daily clinical work.

� To all the private home care professionals that take good care of our home mechanical ventilated patients. Their dedication and competence in this field have improved significantly the quality of life of these patients and their availability and “team work” were crucial to achieve the results of the home care studies of this thesis. A special thanks to Nuno Silva (clinical Nurse) and all the Linde
home care team that gave me great support and actively contributed to this thesis line of research.
� To Dr. Michele Vitacca and his Respiratory Rehabilitation multidisciplinary team of Fondazione Salvatore Maugeri IRCCS,
Lumezzane (BS) Italy, for his kind friendship and for sharing with us all his knowledge and experience in home mechancial ventilation and telemedicine. It has been a great honor to perform a line of research together with this reference center.
� To Hugo Casais, long time and forever best friend, for his professional competence and outstanding creativity in developing all the thesis and presentation template design.
� To Paulo Abreu, Luísa Morais and Ana Menezes, my main influences in Respiratory Physiotherapy. Their teachings motivated me, still as a student, to dedicate my professional life to this field. Their words and advices still and always motivate me to continue my path.
� To all my old friends (that the number does not permit me to individualize) and all the new friends that i had the opportunity to meet during my journeys throughout the world teaching and learning about Noninvasive ventilation and Respiratory Care. I have had the privilege to meet fantastic people from USA, South America (Brazil, Argentina, Ecuador, Cuba, Mexico, Columbia, Chile), Europe (Spain, Italy, France, Belgium, United Kingdom, Germany, Switzerland, Greece, Sweden, Norway, Denmark), Japan, Middle East, Australia etc.. Each one of these international friends represent special moments that i will never forget
� To my Family, especially to my Mother, the main responsible for my educational and ethical principles. She is always an example for me and was a “solid anchor” that allowed me to grow as a professional as well as a human being. A special dedication to my grandfather Antonio Ramalho, that since i was a child always believed in my dreams but let his own dreams be prematurely ended by cancer. I know he would be proud of this “dream” thesis.

� To Luana, for all the Love and Support that where important to maintain the necessary emotional balance to finish this work. I thank her for all her patience, understanding and for always being there with a “kiss” when I needed.
� Last, but not the least, TO ALL THE VENTILATOR DEPENDENT PATIENTS that trusted me and gave me the responsibility to help them breathe better. They are, and always will be, my greatest source of inspiration and the main responsables for all this work.
With them i learned the most important lessons and to them I DEDICATE THIS THESIS.


INTRODUCTION
Most patients with impairment of pulmonary function can be differentiated into those
who have primarily oxygenation impairment due to predominantly intrinsic lung
disease, and those with lung ventilation impairment on the basis of respiratory muscle
weakness (1). This distinction is important because, although many patients in the
former category have been described to benefit from noninvasive ventilation in the
acute care setting (2-3), long term use is more controversial (4-8). Patients with
primarily ventilatory impairment, on the other hand, can benefit from the use of both
inspiratory and expiratory muscle aids and have excellent prognoses with long term
home mechanical ventilation (9-17).
One of the most important developments in the field of mechanical ventilation over the
past 15 years has been the emergence of noninvasive ventilation (NIV) as an increasing
part of the critical care armamentarium (18). Noninvasive positive-pressure ventilation
(NPPV) is the delivery of mechanical ventilation to patients with respiratory failure
without the requirement of an artificial airway. Although NPPV is often used for long-
term nocturnal or continuous support of patients with forms of chronic respiratory
failure (19), its use is increasingly popular in varied clinical situations in the intensive
care unit (ICU) setting as high level evidence supporting its use continues to accumulate
(2, 20-21).
The attraction for NPPV relates primarily to its advantages over invasive mechanical
ventilation. It has been shown to comparatively decrease resource utilization and
circumvents the myriad of complications associated with invasive mechanical
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 1

ventilation such as upper airway trauma, ventilator associated pneumonia, and
compromise of speech and swallowing (22-23). NPPV should, however, be considered
in some cases an alternative to invasive mechanical ventilation rather than its
replacement (24-28). Keys to the success of NPPV and to improving clinical outcomes
of patients with acute respiratory failure are careful patient selection and a well
designed clinical protocol because failure of NPPV only delays potentially more
definitive therapy with invasive ventilation (29). For patients with secretion
accumulation or a weak cough reflex, adequate secretion management with manual or
mechanical techniques might be advisable before non-invasive ventilation is declared
failed or contraindicated (2, 30).
Noninvasive ventilation has been proposed for several other applications, including
facilitation of weaning and extubation. One major determinant of weaning failure is an
excessive load on the respiratory muscles after disconnection from the ventilator (31-
32). In patients who fail a T-piece trial, invasive and noninvasive ventilation are equally
effective in reducing inspiratory effort and improving gas exchange, although
noninvasive ventilation results in better patient comfort (33). By allowing effective
ventilator assistance, while eliminating the risks associated with endotracheal
intubation, noninvasive ventilation may be a valuable alternative to the conventional
weaning techniques (20). Considering that difficult to wean patients have higher
morbidity and mortality and consume a substantial amount of health care resources(34),
these results could lead many of those who have so far considered noninvasive
ventilation ineffective or unsafe (35) to change their mind and reevaluate its potential.
Although a relatively straightforward technique, noninvasive ventilation has several
specific features that must be taken into account to avoid negative and disappointing
results (36).
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
2 Miguel Ramalho do Souto Gonçalves

In the intensive care setting very often patients have impaired airway clearance.
Endotracheal intubation prevents the patient from closing the glottis, which is necessary
for effective coughing (37). Care of the intubated patient includes direct suction applied
to the endotracheal tube which clears a small portion of the airway, is ineffective for
clearing secretions in the peripheral airways, and the patient is left dependent upon
mucociliary clearance rather than cough clearance (38). Conventional techniques for
augmenting the normal mucociliary clearance and cough efficacy have been used for
many years to treat patients with respiratory disorders from different etiologies. In
recent years, new technologies and more advanced techniques have been developed to
be more effective in acute respiratory failure These techniques involve mechanical
application of forces to the chest wall (39) or intermittent pressure changes to the airway
to assist airway mucus clearance (40-41).
Mechanical insufflation-exsufflation (MI-E) acts directly on the airway to assist or
substitute for expiratory muscle function in the elimination of airway secretions. The
effective elimination of airway mucus and other debris is one of the most important
factor that permits successful use of chronic and acute ventilation support (noninvasive
and invasive) for patients with either ventilatory or oxygenation impairment.
Decades of experience during the polio epidemics (42-43) and subsequently (13, 44-45)
established that long-term nocturnal noninvasive ventilation stabilizes gas exchange and
improves symptoms in patients with chronic respiratory failure. For home mechanical
ventilation, noninvasive ventilation has a number of advantages over invasive
mechanical ventilation, including greater ease of administration, reduced need for
skilled caregivers, elimination of tracheostomy-related complications, enhanced patient
comfort, and lower cost (46-47). However, as is the case in the acute setting, not all
patients with chronic respiratory failure are good candidates for noninvasive ventilation.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 3

Long term mechanical ventilation at home now incorporate both ventilator dependent
(>16 h per day ventilatory support) and ventilator assisted (primarily nocturnal only)
individuals, using a variety of devices and interfaces including invasive ventilation and
NIV techniques(48). The diversity of conditions and variability in level of care needed
by these individuals means that introducing and maintaining long-term ventilation in the
home requires skill and experience on the part of the prescribing centre, particularly if
the patient is using ventilatory support on a near continuous basis or has a tracheostomy
in place for the delivery of ventilation (49-51). Additionally, introducing medical
technology into the home raises a number of issues for the patient and caregivers, as
well as local health services, which need to be identified on an individual basis (52-53).
Although no controlled trials have evaluated the efficacy of MI-E, significant amount of
evidence suggests that it enhances removal of secretions in patients with impaired
cough (54-62). It has been particularly useful in patients’ homes to treat episodes of
acute bronchitis, permitting avoidance of hospitalization (63). Clinicians caring for
patients with severe cough impairment should be familiar with the various techniques
available to assist expectoration. These are particularly important with noninvasive
ventilation, because there is no direct access to the airway, and secretion retention is a
frequent complication and common cause for failure. Although controlled data are
lacking, these techniques appear to be helpful in maintaining airway patency in patients
with cough impairment during use of noninvasive ventilation in both acute and chronic
settings.
Research on a continuum strategy of care, that include NIV therapy coupled with MI-E
from acute care to chronic settings in patients with muscle weakness is warranted to
support the application of specific protocols that may improve survival in this patient
population.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
4 Miguel Ramalho do Souto Gonçalves

HISTORICAL PERSPECTIVE OF MECHANCIAL
VENTILATION AND RESPIRATORY MUSCLE AIDS
NIV was first described in Genesis Chapter 2 when the Lord God “breathed into his
(Adam’s) nostrils a breath of life”(64). Around 800 BC, mouth to mouth NIV was
provided by Elisha to resuscitate a child as he "...went up, and lay upon the child, and
put his mouth upon his mouth, and his eyes upon his eyes, and his hands upon his
hands; and he stretched himself upon the child; and the flesh of the child waxed warm.
Mechanical ventilatory assistance may have first been attempted by Theophrastus
Paracelsus in1530. Paracelsus used his chimney bellows to ventilate patients' lungs via
the mouth (Figure 1). This technique of respiratory resuscitation continued to be used
in Europe through the 1830s (65).
Figure 1- Description of mouth ventilation through a chimney bellows as described by Paracelsus in
1530
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 5

Thereafter, John Fathergill, and others used pumps and bellows to insufflate patients via
upper airway canulas (66). Successful mouth-to-mouth resuscitation was reported in
1744 (67). In 1767, the Dutch Humane Society published guidelines resuscitating
drowning victims. A memo from Louis D’Etiolles to the French Academy of Sciences
reported that death from drowning was markedly decreased from 1774 to 1829 by
mouth-to-mouth and orolaryngeal intubation resuscitation methods (68).
Orolaryngeal intubation actually dates to Hippocrates in the 4th century BC but was
apparently dropped until 1800 (69). For the next 30 years 10 to 20 others in France,
Germany, England, and Italy developed manual pumps to ventilate via translaryngeal
tubes as well as via noninvasive oral and nasal interfaces, and were “strong advocates of
insufflation of the lungs for asphyxia, believing this the best method to restore the
victims of asphyxia, no matter what the cause (69).
Then in 1893 Dr. George H. Fell of Buffalo, New York presented a hand-operated
bellows to deliver air via translarngeal or tracheotomy tubes at an International
Congress in Washington in 1893. He then substituted an oronasal interface for the
invasive tubes to ventilate CO2 narcosis patients(not surgical), using a finger as an
“exhalation valve (69). Ignez von Hauke of Austria was probably the first person to use
NIV via an oronasal interface in the 1870s (70). In 1896 the Fell-O’Dwyer foot operated
manual resuscitator bellows made at Columbia Presbyterian Hospital in New York
provide ventilation via orolaryngeal tubes to treat CO2 narcosis due to opium (71). In
1898 Matas used these ideas to provide both anesthesia and ventilatory support via an
orolaryngeal tube for thoracic surgery. However, the idea of supporting ventilation
rather than just providing anesthesia via airway tubes during surgery did not catch on.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
6 Miguel Ramalho do Souto Gonçalves

Until around 1830, mouth-to-mouth and tranlaryngeal positive pressure methods were
used for resuscitation but gradually the paradigm shifted from applying pressures via
airways to pressures to the body. In the “Inversion Method” of the 1770s the body was
turned upside down and the chest intermittently compressed. In the “Barrel Method,”
(1773) the victim was hoisted onto a wine barrel and rolled back and forth to compress
the chest. In 1812 Lifeguards hoisted drowning victims onto horses that trotted to
bounce the chest. This was banned in 1815 by "Citizens for Clean Beaches". In 1856,
Marshall Hall rolled drowning victims 16 times a minute and applied pressure to the
back during exhalation when prone and achieved tidal volumes of 300 ml to 500 ml
(72).
The first tank ventilator was described by the Scottish physician, John Dalziel, in 1838.
The negative pressure was created in the tank by a pair of bellows worked from outside
the tank by manually operating a piston rod (73).
In 1931 John Emerson of Cambridge, Massachusetts built a simplified, inexpensive, and
more convenient iron lung that operated quietly, permitted speed changes, and could be
operated by hand if electricity failed (Figure 2)(74). Then, in 1936 Fred Snite Jr., age
25, son of Colonel Frederick Snite, a prominent Chicago financier, was stricken with
poliomyelitis while traveling with his family in Beijing. The Drinker iron lung, one of
only 222 iron lungs in the world in 1936, was used by Mr. Snite for 1 year. He then
returned to the United States via truck, ocean liner, and train along with a physician, 7
Chinese nurses, a Chinese physiotherapist, two American nurses, and his family(75).
The fanfare, including the fact that he married and fathered 3 daughters, stimulated
public awareness and resulted in mass production of Emerson iron lungs in time for the
poliomyelitis epidemics that were to come (Figure 3) (76). Mr. Snite lived using the
iron lung continuously until 1954 when he died from cor pulmonale.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 7

Figure 2- Emerson™ Iron Lung opened for nursing care, while the patient was ventilated through a
dome that covered their heads.
Figure 3- Iron lung wards that managed hundreds of patients during the poliomyelitis epidemics
In 1947 Emerson placed transparent glass domes that enclosed the users' heads and
sealed at the iron lung's neck collar. The iron lung bellows could create both negative
and positive pressure in the cylinder, and after 1947, the bellows could create positive
pressure under the dome. Just as the negative tank pressure insufflated the lungs, the
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
8 Miguel Ramalho do Souto Gonçalves

subsequent positive pressure forcibly exsufflated the patient, increasing tidal volumes.
When iron lungs had to be opened to permit nurses access to the body, patients with no
breathing tolerance received IPPV via the dome (Figure 2) (43, 76).
The Fairchild-Huxley chest respirator (77) and Monaghan Portable (chest shell)
Respirator(78) were introduced in 1949 and became the first mass produced chest
shells. Emerson came out with a negative pressure cycling generator for chest shells in
1950. Although the shells were portable, the negative pressure generators used for them
were not. These devices were built by hand and so were very expensive. There were no
filters so that patients inhaled a great deal of dust and particles from the ventilator itself.
Figure 4- Chest shells for daytime ventilatory support
Chest shells were used long-term for daytime ventilatory support with the user sitting
(Figure 4) as well as for nocturnal support with the user supine. Similar chest shells are
manufactured today and are used predominately for nocturnal ventilatory assistance(68).
After successfully resuscitating drowned cats with a negative pressure body jacket,
Alexander Graham Bell developed a similar negative pressure jacket to assist
ventilation in premature infants in 1881. However, Bell's invention was not picked up
by the medical community until the British Tunnicliffe breathing jacket was described
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 9

in 1955 and Jack Emerson put the Poncho "wrap" style ventilator on the market in 1957
(79). These ventilators, and the wrap ventilators that followed them, consist of a firm
grid covering at least the thorax and upper abdomen. The grid and the body under it are
covered by a wind-proof jacket that is sealed around the neck and extremities. As
negative pressure is cycled under the wrap and grid, air enters the upper airway to
ventilate the lungs. The only significant changes in modern wrap ventilators from the
original designs are the plastics used to fabricate the jacket and grid, and the length and
form of the extremity sleeves (Figure 5).
Figure 5- The pneumowrap ventilator used by a patient with late-onset chronic ventilatory failure.
Figure 6- The rocking bed ventilator (J. H. Emerson Company, Cambridge, MA)
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
10 Miguel Ramalho do Souto Gonçalves

The Rocking Bed Ventilator (J. H. Emerson Company, Cambridge, MA) has been used
for ventilatory assistance since 1932 (Figure 6). It rocks the patient 15o to 30o, thereby
using gravity to cyclically displace abdominal contents for diaphragmatic
excursion(80). It was used until the late 1950s by predominantly poliomyelitis and
muscular dystrophy patients and is still occasionally used today. This device is
generally less effective than other body ventilators but can be adequate for some
patients.
The intermittent abdominal pressure ventilator (IAPV) was developed by Alvin Barach
in the United States in 1955 where he used a pump made by the Gast Rotary Pump
Company to pump air from an air reservoir into the sac inside the belt that was attached
to the abdomen (68).
In 1946, after anesthesiologist James Elam had read about mouth-to-mouth NIV in a
historical article on resuscitation, a child became apneic on his ward and he “went into
total reflex behavior.”.. .I stepped out in the middle of the corridor, stopped the gurney,
grabbed the sheet, wiped the copious mucous off his mouth and face, sealed my lips
around his nose and inflated his lungs. In four breaths he was pink..." In 1951, Elam
demonstrated that his expired air blown into an endotracheal tube maintained normal
oxygen saturation on postoperative patients before ether anesthesia wore off. This was
exactly what Elsberg had done in 1910, Paracelsus in 1530, and even Hippocrates.
Elam then recruited 31 physicians and medical students, and one nurse to observe
ventilation in anaesthetised and curarized patients most of them for several hours each.
Blood O2 and CO2 were analyzed. He demonstrated the method to over 100 lay persons
who were then asked to perform the method. These dramatic demonstrations along with
the lack of iron lungs during a polio epidemic in Denmark in 1952 resulted in a
paradigm shift from body ventilator to tracheostomy tubes for ventilatory support (81)
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 11

Galen reported using tracheostomies to ventilate animals in the 2nd century.
Trendelenburg was the first to describe the use of a tracheostomy tube with an inflated
cuff for manual application of positive pressure ventilatory assistance during anesthesia
of a human in 1869(43).Tracheostomy was also used for drowning victims from the 17th
century through the mid-19th century and tubes were placed into polio iron lung users
with severe bulbar-innervated muscle impairment to suction out airway secretions.
Noninvasive IPPV had not yet been reported and mechanical forced exsufflation
devices to assist cough were not widely available until after 1953(82-84).
Furthermore, during the Danish epidemic the mortality rate was 94% for patients with
respiratory paralysis and concomitant bulbar muscle involvement and 28% for those
without bulbar involvement. Lassen reported that mortality figures for ventilator
supported patients decreased from 80% to 41%, or to about 7% for the entire Danish
acute paralytic poliomyelitis population overall(85). This was in part due to more
frequent use of tracheostomy, particularly for those with severe bulbar involvement.
In the meantime, specialized centers in the United States were also reporting equally
impressive decreases in mortality by "individualizing" patient care. From 1948 to 1952,
3500 patients were treated at Los Angeles General Hospital. Fifteen to 20% required
ventilatory support. Acute poliomyelitis mortality decreased from about 15% in 1948 to
2% in 1952 without the use of tracheostomy for ventilatory support(86). Better nursing
care and attention to managing airway secretions including the use of devices to help
eliminate them were factors in decreasing mortality rates.
A long debate ensued as to whether tracheostomy IPPV or body ventilators were
preferable for ventilatory support. In 1955, an International Consensus Symposium
defined the indications for tracheostomy as the combination of respiratory insufficiency
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
12 Miguel Ramalho do Souto Gonçalves

with swallowing insufficiency and disturbance in consciousness or vascular
disturbances (86).
Tracheostomy ventilation facilitated mobility by permitting patients to leave iron lungs
for wheelchairs with positive pressure ventilators rolled behind them, an obvious
advantage considering that the iron lungs were very heavy to transport. The switching to
tracheostomy spread across the United States where, in 1956, the small, portable,
pressure-limited Bantam ventilator came onto the market for positive pressure through
the tube. Tracheostomy also provided for a closed system of ventilatory support that
was amenable to precise monitoring of ventilatory volumes and pressures, oxygen
delivery, and the use of the high technology respirators and alarm systems that were to
come (68).
As the use of endotracheal methods became widespread, manually assisted coughing
was no longer taught in medical, nursing, and respiratory therapy curricula and
clinicians lost familiarity with body ventilators. Noninvasive IPPV methods were not to
be described until 1969 and 1973 (43) and their 24 hour use was not reported for a large
population until 1993 (87). Further, the only studies of the use of MI-E devices had
been for acute poliomyelitis patients and patients with severe intrinsic pulmonary
disease (84). The former was felt to be a transient population, and the latter a population
for which the use of noninvasive respiratory muscle aids was not ideal. Although MI-E
devices went off the market in the 1950s or early 1960s they continued to be used by
patients who had access to them. Meanwhile, with widespread use of translaryngeal
intubation and tracheostomy, numerous reports of complications appeared.
Ironically, what may now seem like the simplest solution to the problem of providing
ventilatory support, that of delivering positive pressure ventilation via a simple mouth
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 13

piece, continues to be the last to be considered. In 1953, Dr. John E. Affeldt of Rancho
Los Amigos Hospital in Los Angeles reported in a post-poliomyelitis respiratory
equipment conference that the positive pressure attachment used to deliver the IPPV
was the simple mouth piece used for pulmonary function testing. Patients would
intermittently block the mouth piece to cycle adequate tidal volumes into their lungs
(42).
The ventilator unit of Goldwater Memorial Hospital in New York City was opened in
1955. In a short period of time the 80 bed unit was filled with mostly post-poliomyelitis
body ventilator users. Most of the patients had been recumbent in iron lungs in their
local hospitals since having poliomyelitis. At Goldwater Hospital these patients, often
with no breathing tolerance, were encouraged to leave their iron lungs during daytime
hours and use the chest shell ventilator or IAPV when sitting. These patients could now
be placed in wheelchairs using chest shells, IAPVs, or IPPV via mouth pieces and the
"portable" negative-positive pressure ventilators were rolled behind them until the
smaller portable machines like the Bantam became available in 1957(68).
Because mouth piece IPPV can provide much greater air volumes directly to the lungs
than can IAPV or chest shell use, it became the mode of ventilatory support that the
patients used during intercurrent chest infections and other times of stress. Although in
centers other than Goldwater Hospital the great majority of ventilator users were
switched to tracheostomy IPPV, isolated patients around the country refused
tracheotomy and some reported that they themselves had the idea to ventilate their lungs
via mouthpieces.
Dr. Augusta Alba took charge of the Goldwater Memorial Hospital ventilator unit in
1956. She encouraged patients to use mouthpiece IPPV for daytime ventilatory support.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
14 Miguel Ramalho do Souto Gonçalves

Like Dr. Affeldt before her, she soon discovered that mouthpiece IPPV users would nap
during the daytime without the mouthpieces falling out of their mouths. This was
remarkable because many of these patients had little or no autonomous breathing
ability; their ventilators did not have alarms; there was nothing to hold the mouthpiece
in the mouth other than the patient's own oropharyngeal muscles and these muscles are
not thought to function during REM sleep; and they had little or no extremity function
so they could not have put the mouthpieces back into their mouths if they had fallen out.
In 1964 she permitted a number of patients to use mouthpiece IPPV overnight rather
than return to body ventilators (88). It is remarkable that few if any patients died by
losing their mouthpieces during sleep.
No patients were admitted to or managed with tracheostomy tubes on the Goldwater
Memorial Hospital ventilator unit until 1968. From the mid-1960s until nocturnal nasal
IPPV was described in 1987 (89), simple mouthpiece IPPV was the only method of
daytime or nocturnal noninvasive IPPV. It was not until oximeters became widely
available in the early 1980s that it was discovered that these patients experienced
frequent, and at times, severe SpO2 desaturation associated with periods of leakage of
ventilator delivered air (insufflation leakage) during sleep (90).
The Bennett mouth piece with lipseal retention (Mallincrodt, Pleasanton, CA) came
onto the market in 1968. It was designed to be used for pulmonary function testing. To
prevent the mouthpieces from falling out of the mouths of her IPPV users during sleep,
Dr. Alba convinced many of her patients to use mouthpiece IPPV with lipseal retention.
Besides mouthpiece retention, by sealing the lips it greatly reduced insufflation leakage
out of the mouth (90).
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 15

In 1981, as a technical advisor to Professor Yves Rideau of the University of Poitiers,
France, Dr. John R. Bach introduced mouthpiece and lipseal IPPV into France. It was
in the Winter of 1981-82 that Dr. Rideau suggested to Drs. Delaubier and Bach that
ventilation should be tried via nasal access (13). He felt that humidification would be
facilitated and the nasal route would prove more physiologic for IPPV. Drs. Bach and
Delaubier first used urinary drainage catheters with the cuffs inflated in each nostril to
deliver nasal IPPV to themselves and then to French muscular dystrophy patients for
daytime and nocturnal ventilatory assistance (91). Nasal IPPV was first used as an
alternative to airway intubation for 24 hour ventilatory support in 1984 and it was first
reported in 1987 (92).It was in 1984 that nasal CPAP masks became commercially
available and could be used as IPPV interfaces (93). This permitted rapidly expanding
application of nasal ventilation.
Excessive nasal bridge pressure and insufflation leakage into the eyes were common
complaints when using nasal IPPV with the first commercial CPAP "masks". Attempts
at customizing nasal interfaces for IPPV were first described in 1987 (92). Custom
molded nasal interfaces eventually became available both commercially and
individually (94).
In the late 1980s Dr. Adolphe Ratza, a Swedish post- poliomyelitis survivor,
experimented with the construction of strap-retained custom nasal and oral-nasal
interfaces. His oral-nasal interfaces, with strap retention systems much like those used
for lipseal and nasal IPPV, were described for long-term supported ventilation in 1989.
Over the last 15 years, strap-retained oral-nasal interfaces have been marketed by
several ventilatory companies both for chronic and acute care (68).
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
16 Miguel Ramalho do Souto Gonçalves

By 1949 there were over 400 respiratory polio survivors using ventilators in the United
States in custodial care at over a hundred hospitals scattered around the country. They
were funded by the National Foundation for Infantile Paralysis (March of Dimes) which
President Franklin Roosevelt had founded. The hospital charges were so high that the
March of Dimes funded a study to find ways to reduce the cost. The study showed that
it would be far more economical to move the patients to regional centers with
multidisciplinary professional teams. Thus, 16 polio respiratory and rehabilitation
centers with 15 to 160 patients were created at the teaching hospitals of 16 medical
schools. The March of Dimes paid for the centers' professional staff, patient care,
equipment, research, and ultimately for home care, home modifications, and personal
care attendants (95). Interestingly, there were no pulmonologists and respiratory therapy
did not exist at that time. The patients' and their families were taught how to ventilate
lungs and to facilitate airway secretion elimination and were made key participants in
the rehabilitation team.
In 1953 a home care plan was developed at Rancho Los Amigos Hospital in California
to save money when it was shown that de-institutionalization with home care by
attendants could result in 75% cost savings. The first attendants were trained by the
centers but ultimately attendants were hired and trained by the patients and families
themselves. In 1953 it was estimated that 1800 post-poliomyelitis patients had been
respirator (iron lung) supported for one month or more and that 20% of these patients
had already been discharged home. Forty-four percent of the home mechanical
ventilation users were cared for solely by their families, and 15% of these patients were
under 9 years of age. Over 50% of the patients required ventilatory support over 16
hours per day. By 1956, 92% of permanently ventilator dependent individuals had been
discharged to their homes (68).
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 17

In 1952, Barach and Beck, began applying negative pressure to patient airways via a
face mask(84). In May of 1953 Dr. John Affeldt of Rancho Los Amigos noted that he
had had his patients try many methods of assisted coughing including Barach's
mechanical cough chamber, the suction of vacuum cleaners, manual chest and
abdominal compression, and providing maximal insufflation in an iron lung then
closing the glottis until positive pressure peaks in the tank to maximize cough flows.
He reported being disappointed that he was unable to clear atelectasis in a number of
patients with these methods. Mr. Emerson, however, noted that it made much more
sense to apply positive and then negative pressure to a face mask to increase cough
flows than it did to place patients into the mechanical cough chamber(42). Five months
later, Fagin and Barach's brother Edward's company OEM put the
Exsufflation-with-Negative Pressure device called a "Cof-flator" (Figure 8) on the
market.
Figure 7 - The OEM™ Exsufflation-with-Negative Pressure device called the "Cof-flator®"
In 1954 Beck and Alvin Barach wrote of the Cof-flator, "The life-saving value of
exsufflation with negative pressure was made clear through the relief of obstructive
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
18 Miguel Ramalho do Souto Gonçalves

dyspnea as a result of immediate elimination of large amounts of purulent sputum, and,
in a second episode, by the substantial clearing of pulmonary atelectasis after 12 hours'
treatment” (83). Although many studies demonstrated its efficacy and no major
untoward effects were described with its use, the Cof-flator was abandoned with the
increasing resort to tracheostomy. However, patients who had access to the original
Cof-flators kept them and used them effectively as needed. Occasional medical
publications continued to refer to its effective use even though it was no longer on the
market (81, 88, 96-98).
In February of 1993, a new mechanical insufflator-exsufflator (In-Exsufflator, J. H.
Emerson Co., Cambridge, MA) was released onto the market. The In-exsufflator
operated like the Cof-flator except that cycling between positive and negative pressure
had to be done manually. The manual cycling feature facilitated care giver-patient
coordination of inspiration and expiration with insufflation and exsufflation but it
required that an additional hand be available to deliver an abdominal thrust (99). Then,
in 1995, an automatically cycling device became available. In 2001 it was renamed the
"Cough-AssistTM".
The creation of the medical specialty of respiratory therapy in 1961 and the training of
respiratory therapists has become of paramount importance for the noninvasive
management of patients with ventilatory impairment(94). Respiratory therapists have
been and continue to be essential for evaluating and training patients in the use of
noninvasive ventilation and expiratory muscle aids.
Although NPPV first made its mark in the home environment, as confidence grew,
criticall ill patients with acute ventilatory failure were ventilated in hospital, and now
the noninvasive approach is considered by some to be the treatment of choice for acute
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 19

ventilatory failure of whatever etiology (2). Because ventilation can be assisted without
the need for paralysing and sedating drugs, patients do not need continuous one-to-one
nursing care and assisted ventilation for acute ventilatory failure outside the intensive
care unit (ICU) has become a feasible option (19). There is now an ever-growing body
of prospective randomized control data to inform medical practice, and it is likely that,
just as NPPV has been described as "a new standard of care" in patients admitted to
hospital with an acute exacerbation of COPD (18, 100-101), it will assume a still greater
role in the management of acutely ill patients with respiratory disease from other
etiologies (102-106).
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
20 Miguel Ramalho do Souto Gonçalves

EQUIPMENT AND TECHNIQUES FOR NON INVASIVE
POSITIVE PRESSURE VENTILATION
Successful assisted ventilation depends critically upon adapting mechanical ventilation
to the patient needs. This is particularly true when the noninvasive mode is used
because the patient is conscious and if ventilation is ineffective or uncomfortable the
patient may reject it. An understanding of the technical equipment, in particular the
modes of ventilation and the potential problems with each, is crucial, as is the selection
of an appropriate interface(101)
Characteristics of different modes of ventilation
During noninvasive positive pressure ventilation (NPPV) positive- end expiratory
pressure (PEEP) is combined with positive inspiratory pressure. The delivery of positive
inspiratory pressure is triggered by the patient’s inspiratory effort, and usually titrated to
produce either constant volume (assist volume control; AVC) or constant pressure
(pressure-support ventilation; PSV)(107).
Pressure-cycled machines deliver a predetermined pressure and the volume delivered
will depend upon the impedance to inflation. If there is a leak in the circuit, flow will
increase to compensate, but if there is airway obstruction, tidal volume will be
reduced(108). Volume cycled machines deliver a fixed tidal or minute volume and will
generate a pressure sufficient to achieve this. If the impedance to inflation is high,
pressure will be increased and the targeted tidal volume will be delivered. However, if
there is a leak, there will be no increase in flow rate to compensate, a lower pressure
will be generated, and the delivered tidal volume will fall(107). Triggering into
inspiration and cycling into expiration can be timed by the machine or on the basis of
detection of patient initiated changes in flow or pressure(109). Mechanical ventilation
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 21

can be "controlled" (i.e. the machine determines respiratory frequency), "assisted" (i.e.
the machine augments the patient´s spontaneous breaths), or a combination of the two,
"assist/control" (A/C) mode, which is called "spontaneous-timed" (S/T) mode in
pressure targeted ventilators. The backup rate is usually set at slightly below the
spontaneous breathing rate (110).
In chronic respiratory failure (CRF), timed modes alone may be used in patients with
unreliable respiratory effort, unstable ventilatory drive or mechanics, apnoea or
hypopneas, massively overloaded respiratory muscles or in patients where the assist
mode fails to augment spontaneous breathing. In practice, however, the A/C or S/T has
the advantages of the timed mode but allows augmentation of extra spontaneous efforts
that may occur with irregular breathing patterns that may be seen at sleep onset or
during rapid eye movement (REM) sleep. The proportion of breaths which are assisted
and those which are controlled will depend upon the backup rate that is set (111).
Pressure cycled ventilation.
In this mode, inspiratory pressure delivered by the ventilator is constant to the preset
pressure level, regardless of the magnitude of the patient’s inspiratory effort. It also
unloads the fatigued inspiratory muscles by decreasing their inspiratory work of
breathing and oxygen consumption(112). For these reasons, it has gained widespread
acceptance as a mode of delivering NPPV in both the acute and chronic setting(113).
Pressure cycled modes are available on most ventilators designed for use on intubated
patients in critical care units. Most such “critical care ventilators” provide pressure
support ventilation (PSV) that delivers a preset inspiratory pressure to assist
spontaneous breathing efforts and has attained popularity in recent years as a weaning
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
22 Miguel Ramalho do Souto Gonçalves

mode(114). Most such modes also permit patient-triggering with selection of a backup
rate. Nomenclature for these modes varies between manufacturers, causing confusion.
For the pressure support mode, some ventilators require selection of a pressure support
level that is the amount of inspiratory assistance added to the preset expiratory pressure
and is not affected by adjustments in PEEP. Bi-level pressure ventilation requires the
selection of inspiratory and expiratory positive airway pressures (IPAP and EPAP) and
the difference between the two determines the level of pressure support. It is important
to recall that with the latter configuration, alterations in EPAP without parallel changes
in IPAP will alter the pressure support level(115).
What distinguishes PSV from other currently available ventilator modes is the ability to
vary inspiratory time breath by breath, permitting close matching with the patient’s
spontaneous breathing pattern. A sensitive patient-initiated trigger signals the delivery
of inspiratory pressure support, and a reduction in inspiratory flow causes the ventilator
to cycle into expiration. In this way, PSV allows the patient to control not only
breathing rate but also inspiratory duration(116). As shown in patients undergoing
weaning from invasive mechanical ventilation, PSV offers the potential of excellent
patient-ventilator synchrony, reduced diaphragmatic work, and improved patient
comfort. However, PSV may also contribute to patient- ventilator asynchrony,
particularly in patients with COPD as brief rapid inhalations that may be seen in these
patients with may not permit adequate time for the PSV mode to cycle into expiration,
so that the patient’s expiratory effort begins while the ventilator is still delivering
inspiratory pressure(117). During NPPV these forms of asynchrony are exacerbated in
the presence of air leaks.
Although noninvasive PSV is often administered using standard critical care ventilators,
portable devices that deliver pressure- limited ventilation (Figure 8) have also seen
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 23

increasing use for both acute and chronic applications. These devices, sometimes
referred to as “bi-level” devices because they cycle between two different positive
pressures, are lighter and more compact than critical care ventilators, offering greater
portability at lower expense.
Figure 8 – Bi-level portable devices
Some offer not only a spontaneously triggered pressure support mode but also pressure-
limited, time-cycled, and assist modes. Some also offer adjustable trigger sensitivities,
“rise time” (the time required to reach peak pressure), and inspiratory duration, all
features that may enhance patient-ventilator synchrony and comfort(118). Further, the
performance characteristics of these ventilators compare favorably with those of critical
care ventilators (119). On the other hand, unlike the critical care ventilators, the bi-level
are not currently recommended for patients who require high oxygen concentrations or
inflation pressures, or are dependent on continuous mechanical ventilation unless
appropriate alarm and monitoring systems can be added. Recently, however, new
versions of bi-level ventilators (Figure 9) have been introduced that have more
sophisticated alarm and monitoring capabilities, graphic displays, and oxygen blenders
and are quite suitable for use in the acute care and ICU setting.
Because of their portability, convenience, and low cost, the bi-level devices have proven
ideal for home use in patients with chronic respiratory failure requiring only nocturnal
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
24 Miguel Ramalho do Souto Gonçalves

ventilatory assistance. In addition, unlike volume-limited ventilators, they are able to
vary and sustain inspiratory airflow to compensate for air leaks, thereby potentially
providing better support of gas exchange during leaking(120)
Figure 9 – V60 acute care bi-level ventilator (Philips Respironics, Inc)
Volume cycled ventilation
In this mode, inspiratory pressure delivered by the ventilator is titrated in order to
achieve a preset constant volume target. Most critical care ventilators offer both
pressure- and volume-limited modes, either of which can be used for administration of
noninvasive ventilation. However, the expiratory volume alarm of intensive care
volume ventilators makes them almost impractical to use to deliver NPPV and they are
usually not sufficiently portable for home use(121). Portable volume-cycled ventilators,
however, are most often conventionally used for providing long-term tracheostomy
rather than NPPV, using standard tubing with exhalation valves and humidification as
necessary(122). Compared with the portable pressure-limited ventilators described
above, the volume-limited portable ventilators are more expensive and heavier.
However, they also have more sophisticated alarm systems, the capability to generate
higher positive pressures, and built-in backup batteries that power the ventilator for at
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 25

least a few hours in the event of power failure(123). These ventilators are usually set in
the assist/control mode to allow for spontaneous patient triggering, and backup rate is
usually set at slightly below the spontaneous patient breathing rate. The only important
difference relative to invasive ventilation is that tidal volume is usually set higher (10 to
15 ml/kg) to compensate for air leaking. Volume cycled ventilators can generally
deliver up to 2500 ml volumes and are well suited for patients in need of continuous
ventilatory support or those with severe chest wall deformity or obesity who need high
inflation pressures(124-125).
The minimum inspiratory effort required by the patient is to trigger the ventilator. The
volumes delivered to the lungs correlate with ventilator gauge pressures. Thus, the
pressures indicated on the volume ventilator pressure gauge vary depending on
ventilator delivered volumes, insufflation leakage, and lung impedance. There are also
low and high pressure alarms, sensitivity controls that permit the patient to trigger
ventilator delivered breaths, and flow rate adjustments. Alternatively, when the patient
increases their inspiratory effort, due to increased ventilatory needs, the inspiratory
pressure delivered by the ventilator will decrease in order to keep the constant volume
target(126). The greater the patient’s inspiratory effort, the lesser the ventilator’s
assistance. The ventilator might even deliver negative inspiratory pressure (i.e. pull air
back), when the patient makes an adequately strong inspiratory effort, in order not to
exceed the preset volume target(125). Additionally, it has been shown that some home
ventilators are inaccurate in delivering the preset VT, especially when faced with
deteriorating structural properties of the lung(107). For this reason, this mode has been
disfavored for use as NPPV in the acute setting(18) and, currently, is used merely for
home NIMV for patients with chronic respiratory failure due to neuromuscular
disease(1, 127).
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
26 Miguel Ramalho do Souto Gonçalves

Ventilators with mixed pressure and volume -targeted modes.
In order to make the most of the advantages of pressure and volume ventilators, new
machines which combine the two modes have recently been released (Figure 10). These
respirators are similar to critical care ventilators and may be useful for difficult-to-adapt
patients and those with rapidly changing breathing patterns and mechanics(119). The
clinical impact of these "dual mode ventilators" has not been well evaluated and
therefore it is not known if they offer important advantages to other respirators in
routine practice. In an effort to combine the advantages of pressure- and volume-
targeted modes into one ventilation mode, new hybrid modes such as average volume-
assured pressure support(128) and adaptive servo ventilation(129-130) have recently
been introduced in the NPPV setting.
Figure 10 – Elysée 150 for both pressure and volume targeted ventilation (ResMed, Inc)
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 27

Interfaces for the delivery of NPPV
The major difference between invasive and NPPV is that with the latter, gas is delivered
to the airway via a mask or “interface” rather than via an invasive conduit. The open
breathing circuit of NPPV permits air leaks around the mask or through the mouth,
rendering the success of NPPV critically dependent on ventilator systems designed to
deal effectively with air leaks and to optimize patient comfort and acceptance.
Apart from the choice of ventilator type, mode and setting, another crucial issue when
starting NIV is to find an optimal interface(131). However, despite a broad variety, until
now only little attention has been focused on the choice of interface and no generally
accepted consensus has been reached concerning the management of interfaces(21). In
general, six different types of interface exist: total face masks, oronasal masks, nasal
masks, nasal pillows or plugs, mouthpieces and helmets. Advantages and disadvantages
of each interface is listed in figure 11.
Early studies dealing with NIV in ARF used nasal masks(132). The nasal mask adds
less dead space, causes less claustrophobia and allows expectoration and oral intake. In
order to reduce mouth leaks while wearing a nose mask a chin strap is sometimes
required but is rarely effective (119). The improvement in arterial blood gas tensions
appear to be slower in some studies using nasal masks compared to face masks (133).
Compared to nasal masks, the more common application of full face masks in ARF is
also a reflection of better quality of ventilation (at least during the initial phase of the
intervention) in terms of minute ventilation and improved blood gases (134). Compared
to nasal masks, face masks are generally more claustrophobic, impede communication,
limit oral intake and increase the dead space which may cause CO2 rebreathing (135).
However, based on practical experience, dead space does not seem to reduce the
effectiveness of NIV in ARF. In addition, further types of full face masks both for open
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
28 Miguel Ramalho do Souto Gonçalves

and closed circuits are available. Some of these masks have addressed the issue of dead
space and have increased leak rates, which may improve the quality of NIV(136-137).
Reducing the risk of skin damage is one of the major goals. The most common sites of
friction and skin damage are the bridge of the nose, the upper lip, the nasal mucosa, and
the axillae (with the helmet) (136). The most important strategy to prevent skin damage
is to avoid an excessively tight fit. Masks that have angle adjustments between the
forehead support and the interface can help prevent pressure and friction against the
bridge of the nose (119). Rotating interfaces might reduce the risk of skin damage, by
changing the distribution of pressure and friction, especially on the bridge of the nose
(138-139).
Air leaks may reduce the efficiency of NIV, reduce patient tolerance, increase patient-
ventilator asynchrony (through loss of triggering sensitivity), and cause awakenings and
sleep fragmentation (140). During pressure-support ventilation (PSV) leaks can hinder
achievement of the inspiration- termination criterion (136). In patients with
neuromuscular disorders receiving nocturnal NIV, leaks are associated with daytime
hypercapnia (141). In order to compensate for a significant leak a ventilator needs high
flows. Pressure-targeted ventilators have leak compensating abilities with peak
inspiratory flow rates of 120–180 L/min (142). Modern pressure ventilators can
compensate for very large leaks, but if they are allowed, sleep quality may be sacrificed.
Recently, respiratory system model studies have been published which investigated
mask mechanics and leak dynamics during simulated NIV (143). Leak compensation is
much more limited in volume-targeted ventilators; adding a leak to the circuit of these
ventilators caused a fall in tidal volume of 50% (125). However, moderate leaks can be
compensated for by increasing the tidal volume (124).
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 29

Figure 11 – Advantages and disadvantages of different types of interfaces (Adapted from
Nava and Hill (2)
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
30 Miguel Ramalho do Souto Gonçalves

Humidification during NPPV
Humidification and warming of the inspired gas may be needed to prevent the adverse
effects of cool, dry gases on the airway epithelium. Unidirectional inspiratory nasal
airflow, which can worsened by mouth air-leak, can dry the nasal mucosa, because the
nasal mucosa receives little or none of the moisture it would receive from the exhaled
gas(136).
If the gas delivered from the ventilator is not humidified, it will have lower than the
ambient air, and this is particularly true as the level of inspiratory support
increases(140) Humidification can prevent these adverse effects. The 2 types of
humidification device, heated humidifier, and heat-and-moisture exchanger (HME), are
used both for both short-term and long-term NIV(144). Heat and moisture exchangers
(HMEs) are widely used in intubated patients, because HMEs are easy to use and may
be less expensive than heated humidifiers(136). However, an HME, which is usually
placed between the Y-piece and the interface, can add an important amount of dead-
space, compared to a heated humidifier, which is placed in the inspiratory limb(145).
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 31

NON INVASIVE VENTILATION IN THE ACUTE CARE
SETTING
Rationale
Non-invasive ventilation refers to the delivery of mechanical ventilation with techniques
that do not need an invasive endotracheal airway(146). It should not, therefore, be used
when patients cannot protect their airway. It is not appropriate for all, and the selection
of candidates is important Compared with invasive mechanical ventilation, this type of
ventilation achieves the same physiological benefits of reduced work of breathing and
improved gas exchange(22, 33). Furthermore, it avoids the complications of intubation
and the increased risks of ventilator-associated pneumonia and sinusitis(103), especially
in patients who are immunosuppressed or with co-morbidities(147).
Studies published in the 1990s (132, 148) that evaluated the efficacy of noninvasive
positive-pressure ventilation for treatment of diseases such as chronic obstructive
pulmonary disease, congestive heart failure and acute respiratory failure have
generalized its use in recent years and made a major advance in the management of
acute respiratory failure(21). Over the past decade alone, it has been the subject of over
1,500 scientific papers, including 14 meta-analyses(2).
The use of non-invasive ventilation varies greatly between hospitals and geographical
regions, and has changed over time. Investigators of a worldwide prospective survey of
mechanical ventilation noted that use rose from 4% of all ventilators started in 2001, to
11% in 2004(149).It is increasingly being used in many countries, but frequency of use
is highly variable(2)
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
32 Miguel Ramalho do Souto Gonçalves

In 1996, Meduri et al(150). reported their experience with NPPV in 158 patients with
various diagnoses, of whom 65% avoided intubation with NPPV. They suggested that
NPPV be first-line therapy for patients with acute hypercapnic and hypoxemic
respiratory failure. In parallel with the evolving evidence supporting the use of NPPV
for acute respiratory failure, technical advances have increased the variety of interfaces
and ventilators for NPPV and facilitated wider application. Surveys have reported the
utilization of NPPV in several settings. Carlucci et al.(151) conducted a 3-week
observational survey in 42 French intensive care units (ICUs) to evaluate the use of
NPPV and to assess its efficacy in everyday practice. NPPV was used in 35% of the
patients who were not intubated on admission. This included 14% of patients with
hypoxemic respiratory failure, 27% with pulmonary edema, and half of those with
hypercapnic respiratory failure, but never in patients with coma.
In a follow-up survey, Demoule et al.(152) reported that NPPV use significantly
increased in French ICUs from 1997 to 2002 (up to 24% overall and 52% of patients
admitted without prior intubation), and the success rate remained unchanged (47% vs
48%, respectively).
Non-invasive ventilation in acute setting is used mainly for exacerbations of chronic
obstructive pulmonary disease (COPD) and for cardiogenic pulmonary oedema(18).
Use for hypoxic respiratory failure and facilitation of weaning is still infrequent and is
mainly done in specialised centres (153-156).
In patients with ARF due to restrictive disorders the evidence is lower, although
published studies demonstrate positive results (157). In fact, randomized clinical trials
(RCT) of NIV in ARF tend to exclude patients with restrictive disorders (153-155, 158-
161).
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 33

Despite these limitations, this technique is increasingly being used outside the
traditional and respiratory intensive care units(19), including in emergency
departments(29); postsurgical recovery rooms(104); cardiology(162), neurology(163),
oncology(164-165) wards; and palliative care units(166-167) Noninvasive ventilation
for acute respiratory failure has the potential of reducing hospital morbidity, facilitating
the weaning process from mechanical ventilation, shortening length of hospitalization
and thereby costs, and improving patient comfort(2). However, patients must be
selected carefully (Panel 1) because the risk of complications could be increased if
noninvasive ventilation is used inappropriately(156).
Panel 1: Recommendations for NIV to treat acute respiratory failure Recommendations based on levels of evidence
Level 1 Systematic reviews (with homogeneity) of RCTs
Evidence of use (favourable)
• COPD exacerbations • Facilitation of weaning/extubation in patients with COPD • Cardiogenic pulmonary oedema • Immunosuppressed patients Evidence of use (caution)
• None Level 2 Systematic reviews (with homogeneity) of cohort studies (including low quality RCTs; eg, <80% follow-up) Evidence of use (favourable)
• Do-not-intubate status • End-stage patients as palliative measure • Extubation failure (COPD or congestive heart failure) (prevention) • Community-acquired pneumonia in COPD • Postoperative respiratory failure (prevention and treatment) • Prevention of acute respiratory failure in asthma Evidence of use (caution)
• Severe community acquired pneumonia • Extubation failure (prevention)
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
34 Miguel Ramalho do Souto Gonçalves

Level 3 Systematic reviews (with homogeneity) of case–control studies, individual case-control study Evidence of use (favourable) • Neuromuscular disease/kyphoscoliosis • Upper airway obstruction (partial) • Thoracic trauma • Treatment of acute respiratory failure in asthma Evidence of use (caution)
• Severe acute respiratory syndrome Level 4 Case series (and poor quality cohort and case-control studies) Evidence of use (favourable) • Very old age, older than age 75 years • Cystic fibrosis • Obesity hypoventilation Evidence of use (caution) • Idiopathic pulmonary fibrosis
Chronic Obstructive Pulmonary Disease with acute exacerbation
Patients with acute respiratory acidosis caused by an exacerbation of COPD are the
group that benefits most from non-invasive ventilation(21). These benefits are because
NIPPV is able to decrease work of breathing (WOB) and eliminate diaphragmatic work
by unloading the respiratory muscles, lessening diaphragmatic pressure swings,
decreasing respiratory rate and counteracting the threshold loading effects of auto-
PEEP(168).
In an early study using historically matched control subjects, Brochard and colleagues
reported that only 1 of 13 patients with acute exacerbations of COPD treated with face
mask NPPV required endotracheal intubation, compared with 11 of 13 control subjects.
In addition, patients treated with NPPV were weaned from the ventilator faster and
spent less time in the intensive care unit than did the control subjects(169). Individual
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 35

trials and meta analyses have confirmed the benefit of NPPV for patients with COPD
exacerbation.
Lightowler et al.(170) conducted a meta-analysis of 8 studies restricted to the use of
NPPV for COPD exacerbation. NPPV significantly lowered the risk of treatment failure
risk of mortality, the risk of endotracheal intubation, complications of treatment, and
hospital stay. NPPV significantly improved pH, PaCO2 and respiratory rate within 1
hour of initiation. Keenan et al.(171) also conducted an updated systematic review and
meta-analysis of 15 randomized trials limited to COPD exacerbation. NPPV was
associated with significantly lower in-hospital mortality and a significantly lower rate of
endotracheal intubation.
Early use in patients with COPD who have with mild respiratory acidosis (as low as pH
7·30) and mild-to-moderate respiratory distress prevents further deterioration, and thus
avoids endotracheal intubation and improves survival compared with standard medical
therapy. In a large multicentre trial in patients with mild-to-moderate acidotic COPD
who were admitted to a respiratory ward, Plant and colleagues noted that intubation and
mortality rates were lower with non-invasive ventilation than with standard therapy
alone, but subgroup analysis showed that these rates did not differ when pH at
enrolment was less than 7.30(172). The investigators surmised that these patients with
low pHs might have fared better in an intensive care unit than in the respiratory ward.
Strong evidence of efficacy (from randomised controlled trials and meta-analyses) and
low risk of failure (10–20%) means that use of noninvasive ventilation to avoid
intubation in patients with mild-to-moderate COPD and acute respiratory failure (pH
7·30–7·34) is regarded as the ventilatory therapy of first choice and can be safely
administered in appropriately monitored and staffed areas outside intensive care(173).
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
36 Miguel Ramalho do Souto Gonçalves

Patients with a low pH are still candidates for this technique but transfer to a closely
monitored location is strongly advisable(174).
Acute Cardiogenic Pulmonary Edema
Non-invasive ventilation has been used to treat acute respiratory failure in patients with
cardiogenic pulmonary edema, mainly in emergency departments(175). Investigators of
several meta-analyses concluded that this technique, including CPAP, is better than is
standard medical therapy for reduction of intubation rate(176-177). This conclusion was
not supported in a multicentre trial that compared oxygen therapy alone, CPAP, and
non-invasive pressure support ventilation. The physiological improvements were faster
with non-invasive ventilation than with oxygen alone but without a statistically
significant effect on intubation or mortality rates(178). However, the very low
intubation rate (<3%) raises questions as to whether the patients’ population was similar
to that of other studies. Studies that compared non-invasive ventilation with CPAP alone
in patients with Cardiogenic pulmonary edema showed that intubation and mortality
rates did not differ, although investigators of some studies noted more rapid
improvements in dyspnea scores, oxygenation, and arterial partial pressure of carbon
dioxide (PaCO2) with non-invasive ventilation than with CPAP (179-181). Nonetheless,
because of ease of use, some clinicians regard CPAP as first-line treatment for
cardiogenic pulmonary oedema. In another meta-analysis, Winck et al.(177) also
concluded that robust evidence supports the use of CPAP and NPPV in acute
cardiogenic pulmonary edema, and that both techniques decrease the need for
endotracheal intubation but only CPAP decreases mortality, compared to standard
medical therapy.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 37

Hypoxemic Respiratory Failure
Studies have investigated the use of NPPV in patients with acute hypoxemic respiratory
failure (defined as those with a PaO2/FIO2 ratio of < 200, respiratory rate> 35/min from
more generalized causes). Antonelli et al.(182) conducted a randomized controlled trial
of NPPV in patients with a variety of diagnoses associated with acute hypoxemic
respiratory failure. Patients received NPPV or immediate intubation and invasive
ventilation. Only 31% of the patients who received NPPV required endotracheal
intubation, and more patients in the conventional ventilation group had serious
complications (66% vs 38%) and had pneumonia or sinusitis (31% vs 3%,). Among the
survivors, patients in the NPPV group had shorter periods of ventilation and shorter
ICU stays.
Ferrer et al.(154) conducted a randomized controlled trial of NPPV with patients with
acute hypoxemic respiratory failure from a variety of diagnoses. NPPV was associated
with less need for intubation, lower incidence of septic shock, and lower ICU mortality.
The improvement in hypoxemia and tachypnea was more rapid in the NPPV group.
Moreover, NPPV was associated with better cumulative 90-day survival.
Keenan et al(183). conducted a meta-analysis of randomized controlled trials of patients
who had acute hypoxemic respiratory failure not due to cardiogenic pulmonary edema.
The trials compared NPPV plus standard therapy to standard therapy alone, and
outcomes included need for endotracheal intubation, ICU and hospital stay, and ICU
and hospital survival. They concluded that patients with acute hypoxemic respiratory
failure are less likely to require endotracheal intubation when NPPV is added to
standard therapy. However, the effect on mortality is less clear, and the heterogeneity
found among studies suggests that the effectiveness differs among different settings,
patient populations, and diagnostic groups.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
38 Miguel Ramalho do Souto Gonçalves

Thus, although some studies suggest benefit of NPPV in hypoxemic respiratory failure,
its use in acute respiratory distress syndrome or severe community-acquired pneumonia
is controversial and not recommended routinely(156). Results of a survey in three
intensive care units(184), with staff highly skilled in this technique, showed that only
30% of patients with a diagnosis of acute respiratory distress syndrome met criteria for
a trial of this type of ventilation. Of these patients, intubation was avoided in 54%,
which was associated with much lowered morbidity (by about 40%) and mortality rates
(roughly 30%). This finding suggests that in real-life situations and in expert hands only
about 15% of such patients can be treated successfully with this technique; mainly those
with a low severity of illness, not in shock, and rapid improvement in oxygenation after
therapy is started.
Immunocompromised Patients
Acute respiratory failure in patients who are immunocompromised often signals a
terminal phase of the underlying disease, with short survival time and high costs of
admission to intensive care(105). Early use of non-invasive ventilation could be very
helpful, as shown by randomised studies in intensive care units that compared this
technique with standard treatment. In patients receiving a solid-organ transplant and
who had hypoxaemic acute respiratory failure, such ventilation reduced intubation rate,
complications, mortality, and duration of stay in intensive care(185).
In a second study this technique lowered intubation, complication, and mortality rates
compared with standard therapy in patients with hypoxaemia and bilateral pulmonary
infiltrates and immunosuppression secondary to hematological malignancies(24).
Hilbert et al. (186)conducted a randomized controlled study to compare NPPV with
standard medical treatment in 52 patients with immunosuppression from various causes
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 39

and acute hypoxemic respiratory failure. In the NPPV group, periods of NPPV of at
least 45 min delivered via face mask were alternated with 3-hour periods of spontaneous
breathing with supplemental oxygen. Fewer patients in the NPPV group than in the
standard treatment group required endotracheal intubation, had serious complications or
died in the ICU.
These results support use of NPPV in immunocompromised patients who develop acute
hypoxemic respiratory failure. One reason for the better survival in immunosuppressed
patients treated with NPPV is their lower likelihood of developing ventilator- associated
pneumonia(103, 187)
Weaning From Invasive Ventilation and Post Extubation Failure
NPPV may allow earlier extubation and thereby reduce the duration of mechanical
ventilation. Several randomized trials showed that non-invasive ventilation can be
safely and successfully used to enable weaning from mechanical ventilation in stable
patients recovering from an episode of hypercapnic acute respiratory failure (ie, COPD
exacerbations)(114, 161) and even in those who previously had an unsuccessful
spontaneous breathing trials(153, 188).
This application has been investigated in a meta-analysis. that compared traditional
weaning to early extubation with immediate application of NPPV, Burns et al found that
extubation to NPPV resulted in favorable outcomes, including lower mortality, lower
rate of ventilator-associated pneumonia, and shorter total mechanical ventilation. Burns
et al concluded that early extubation to NPPV decreased mortality, and that the use of
NPPV to facilitate early extubation is promising(20).
Another related potential application of NPPV in the weaning process is to avoid
reintubation in patients who fail extubation. Epstein and colleagues(189) have observed
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
40 Miguel Ramalho do Souto Gonçalves

that such patients have much higher morbidity and mortality rates than do those who are
extubated successfully.
Although controversial, accumulating evidence suggests that NIV may have a role in
treatment of extubation failure, but mainly in patients with hypercapnic and congestive
heart failure who are at high risk for extubation failure(155, 190). Furthermore, patients
should be monitored closely to avoid delays in intubation.
Acute Respiratory Failure in Restrictive Disorders
International surveys performed in ICU’s around the world in 1996 and 1998, showed
that neuromuscular patients correspond to 1.8-10% of patients receiving mechanical
ventilation (191-192). An Italian survey of Respiratory Intensive Care Units during
1997-1998 showed that chest wall and neuromuscular disorders accounted for 9% of
patients admitted (193).
Restrictive disorders are the most frequent indication for Long-term Home Mechanical
Ventilation, with thoracic cage and neuromuscular patients accounting for 65% of
patients ventilated at home in Europe (194).
NIV has been shown to be the first line intervention for ARF due to COPD (195). In
patients with ARF due to restrictive disorders the evidence is lower, although published
studies demonstrate positive results (157). In fact, randomized clinical trials (RCT) of
NIV in ARF tend to exclude patients with restrictive disorders. In the only RCT of NIV
in ARF that included patients with NMD (n=6) the authors did not discuss those
patients because the group was too small for analysis (196).
While Portier et al (197) in a prospective multicentre study of patients with acute-on-
chronic respiratory failure (including 16.7% with restrictive disorders) suggested that
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 41

the underlying disorder did not influence prognosis, Robino et al (198) in a
retrospective study with the larger sample of restrictive patients published to date
(mainly with CWD), suggested that effectiveness of NIV was less in this group of
patients.
Recently Banfi et al (199) successfully managed at home 7 Kyphoscoliotic patients with
infection-related respiratory failure. In fact by increasing daily duration of mechanical
ventilation to > 20h, they corrected respiratory acidosis and returned the patients to their
baseline condition in 4 weeks.
It seems that Respiratory Failure due to these disorders needs a different approach from
the more common obstructive pulmonary diseases (198, 200).
Acute Respiratory Failure in Chest Wall Disorders
Patients with severe Kyphoscoliosis (KS) and acute decompensation of respiratory
failure, exhibit marked decrease of pulmonary compliance but, contrary to COPD,
increase in airway resistance and intrinsic PEEP seem to play only a secondary role
(201). Because cough is not impaired like in NMD, secretion management is not so
critical in this context, and management of ARF may be easier.
Some case series have shown that ARF occurring in KS can be managed non-
invasively, either through negative (202) or positive pressure ventilation (157, 203).
Recently Banfi et al (199) have shown reversal of respiratory acidosis in KS patients
with ARF, by increasing duration of home mechanical ventilation up to > 20h, both
with volume and pressure-cycled ventilators.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
42 Miguel Ramalho do Souto Gonçalves

Acute Respiratory Failure in Neuromuscular Disorders
In neuromuscular disorders, the normality of the respiratory function requires the
integrity of three main respiratory muscles: 1) inspiratory muscles, responsible for
ventilation; 2) expiratory muscles, involved in the ability to cough and 3) Bulbar
muscles, that protect against the risk of aspiration (204). Laryngeal weakness and
swallowing dysfunction can lead to aspiration which is the main reason for failure of
non-invasive respiratory aids during ARF in NMD (27).
In patients with previous NMD, respiratory failure is commonly triggered by upper
respiratory tract infections (205). These can impair the three muscle components (200,
205). Those patients normally present with rapid shallow breathing, tachycardia,
accessory-muscle use, thoraco-abdominal asynchrony, and orthopnea. Blood gases, vital
capacity, maximum inspiratory and expiratory pressures and peak cough flow should be
evaluated and give useful information about the integrity of the respiratory muscle
system. According with the disease and objective parameters need for mechanical
ventilation can be predicted. Hypercapnia is a late finding of impending ventilatory
failure whereas hypoxemia may suggest atelectasis and secretion encumbrance or
pneumonia.
To avoid NMD to be admitted to hospital with ARF, a regular follow-up of all chronic
NMD patients with lung function evaluation in order to establish domiciliary non-
invasive respiratory aids is fundamental (206). Moreover a pro-active intervention with
intensification of home mechanical assisted cough and NIV guided by oxygen
saturation has been proposed by some authors (207). In fact this protocol reduces
hospitalization in NMD followed in specific outpatient clinics.
However there will always be cases where ARF will be the presentation for NMD,
especially those with a rapid evolution like ALS (208-209); apart from those patients,
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 43

acute neuromuscular disorders (like Guillain-Barré Syndrome) together with the ICU-
acquired neuromuscular disorders are the most frequent NMD associated with ARF (see
Table I).
Table I- Major NMD Diseases associated with ARF
Motor Nerves Neuromuscular
Junction
Myopathies Spinal Cord Acquired NMD
Amyotrophic
Lateral Sclerosis
Myasthenia
Gravis
Myotonic
dystrophy
Trauma Criticall ill
myoneuropathy
Guillain-Barré
syndrome
Duchennne
Muscular
Dystrophy
Transverse
myelitis
Acute Respiratory Failure in Amyotrophic Lateral Sclerosis
Analysing a large US database, Lechtzin N et al (210), report that in hospitalized ALS
patients mortality is 15%. According with conventional protocols, patients with ALS
who present acutely in respiratory failure and require endotracheal intubation and
invasive ventilation are rarely weaned and rarely return home (211).
If the cause of ARF is secretions encumbrance, and assisted mucus clearance techniques
were unavailable at home, a strict protocol of mechanical in-exsufflation (MI-E) should
be implemented (sometimes with a 5 min frequency) together with continuous NIV
until blood gases are normalized (212). It should be noted that patients with NMD and
excessive secretions/atelectasis may need very frequent assisted cough techniques
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
44 Miguel Ramalho do Souto Gonçalves

requiring time-consuming care from the nursing and respiratory therapists staffs,
making the help of family caregivers essential (213). This will reverse the majority of
cases (214); however some patients can be intubated for 24/48 hours to rest and
optimize secretion clearance with MI-E through the endotracheal tube (212).
Subsequently it might be possible to extubate them directly continuous NIV.
There are not so many studies analysing the role of NIV in ARF due to ALS. In 2000
Vianello et al (215) published the first paper, prospectively comparing the efficacy of
NIV combined with cricothyroid «mini-tracheostomy» and conventional mechanical
ventilation via endotracheal tube in 14 patients with ARF and NMD (including 3 ALS).
Mean pH was 7.29 in both groups, mortality was lower and ICU stay was shorter in the
NIV group compared with controls suggesting their «non-invasive ventilatory
approach» could be a first line intervention in this setting.
Five years later Vianello et al. (216) evaluated the short-term outcomes of 11 NMD
patients (including 2 ALS), not so severely acidotic (mean pH 7.36), with acute upper
respiratory tract infections and tracheobronchial mucous encumbrance. Apart from NIV,
they were submitted to MI-E treatment in addition to standard physical therapy. The
outcomes were compared with 16 historical matched controls who had received chest
physical therapy alone. The treatment failure (defined as the need for cricothiroid
“minitracheostomy” or endotracheal intubation, despite treatment) was significantly
lower in the MI-E group that in the conventional chest physical treatments group (2/11
vs 10/16 cases). No side effects were related to the use of MI-E alone, while the need of
bronchoscopy assisted suctioning was similar in the two groups (5/11 vs 6/16).
As noted by Gonçalves and Bach in the commentary accompanying the paper (213),
some mistakes concerning the use of the MI-E probably compromised the final results.
Setting the machine at a very low insufflation and exsufflation pressures (less than 30
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 45

cmH20), and forgetting the abdominal thrust during the exsufflation phase were reasons
for sub-optimal results. These low pressures have been shown not to be effective in lung
models (217) as well as in clinical studies (218-219) and accordingly did not effectively
avert bronchoscopy-assisted aspiration. Moreover, using the MI-E 2.7 times a day as
described in this paper may be insufficient. In fact as mentioned before, during an acute
episode of respiratory tract infection, MI-E may have to be applied very frequently and
the only way to solve this problem is allowing the primary care providers or relatives to
stay at the bedside to use it anytime is required (220).
Servera et al (27) in a non-intensive care setting prospectively evaluated the efficacy of
continuous NIV together with coughing aids (including MI-E) to avoid endotracheal
intubation for 17 patients with NMD during ARF. The studied group had a mean pH of
7.38 and included 11 patients with ALS (5 of which with Bulbar dysfunction). There
was treatment failure in 20.8% and mortality in 8.3% cases, significantly related with
patients with severe bulbar impairment. Those patients (in which NIV and assisted
coughing may be unsuccessful) and those who cannot cooperate, may have a more
invasive approach: endotracheal intubation and mechanical ventilation followed by
tracheostomy (221) or as Vianello (222) proposes minitracheostomy.
However, even in Bulbar ALS patients, MI-E should be tried, since Hanayama et al
(223) described an ALS woman with immeasurable CPF, already with a gastrostomy, in
which MI-E was able to clear bronchial secretions and reverse ARF.
In our experience with 11 consecutive non bulbar ALS with ARF, non invasive
respiratory aids (continuous NIV and high-intensity mechanical assisted cough) had a
success rate of 100%, with resolution of respiratory failure and discharge after 8 days
(214) (Figure12). With this protocol, MI-E resolved atelectasis and none of those
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
46 Miguel Ramalho do Souto Gonçalves

patients needed endotracheal intubation or fiberoptic bronchoscopy-assisted aspiration
(Figure 13).
Figure 12-Outcomes of 11 patients with non-bulbar ALS and ARF
LOS 7.9 ± 8.9 days
pH 7.37 ± 1.3
PaO2 57.8 ± 8.4 mmHg
PaCO2 64.7 ± 26.1 mmHg
Tt Failure 0
Legend: LOS-Length of stay; Tt Failure-Treatment Failure; CPF-Peak Cough Flow (L/min)
Figure 13-Resolution of Left lower lobe atelectasis in one patient ALS with MI-E (Left before;
right After MI-E)
33
57,8 64,7
242
76,7
40,6
0
50
100
150
200
250
Baseline Discharge
PCF
PaO2
PaCO2
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 47

Concerning the mode of non-invasive ventilation, it is preferable to use volume-cycled
ventilators in assist control with high tidal volumes, for sufficient lung expansion and to
allow air-stacking for coughing (27, 214). This can be done during the day through
mouthpiece and at night with a nasal or oral interface. As soon as the patient learns to
air-stack and can autonomously produce CPF above 160L/min, assisted coughing can
be reduced in frequency, provided that oxygen saturation levels on the ventilator are
above 95% (224). In the beginning the patient will need continuous NIV but at
discharge will return to the previous duration of home NIV (27, 214).
When patients with ALS under home mechanical ventilation need to be hospitalized due
to ARF there are some technical as well some ethical aspects that need to be considered.
We need to confirm if all non-invasive respiratory aids were optimized at home, if the
patient has refused tracheostomy, if bulbar impairment is severe and the risk of
aspiration is high. Lung function status previous to the decompensation can help in the
decision making. Discussions about aggressiveness of resuscitation should have been
carried out with the family and patient in a stable state (225).
Another different issue is when patients with non-bulbar NMD are intubated because of
failure of NIV or due to a more conventional approach. In this context, it is a common
attitude to gradually reduce the support of the ventilator until the patient is weaned.
Unfortunately NMD patients with a pre-existing respiratory dysfunction often fail to
wean from invasive ventilation and almost invariably are tracheostomized. MI-E in
these cases can be really successful to help clearing secretions first via the tube, and
then, after the tube is removed, via an oronasal mask while the ventilation in delivered
through non-invasive interfaces. MI-E, applied in this circumstance, avoid mucus
encumbrance, the need of blind suctioning through the nose and definitely
tracheostomy, also for patients 24 hours ventilator dependent.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
48 Miguel Ramalho do Souto Gonçalves

Acute Respiratory Failure in Guillain-Barré Syndrome and in Myasthenia Gravis
In the developed world Guillain-Barré Syndrome (GBS) and Myasthenia Gravis (MG)
account for the majority of cases of respiratory failure associated with NMD.
Although the use of NIV in this setting has not been extensively evaluated (226-228), it
should be always tried unless there is significant bulbar dysfunction. In fact, GBS and
MG are not so different diseases from other NMD where a non-invasive respiratory aids
protocol has avoided endotracheal intubation (27, 214, 216). The only difference is that
contrary to the majority of ALS and DMD patients with ARF, those patients are naïve
to NIV.
According with the literature, between 25-50% of GBS patients and 15-27% MG gravis
patients require mechanical ventilation (229-230). A practical rule (the «20/30/40 rule»)
proposed by Lawn et al (231) in which a VC<20ml/kg, Pimax<-30cmH20,
Pemax<40cmH20 were associated with progression to respiratory failure, may be useful
in deciding to initiate ventilatory support. These simple bed-side tests of respiratory
function may be clinically generalizable to other neuromuscular conditions.
Acute Respiratory Failure in Spinal Cord Injury
Demographic data form the US Spinal Cord Injury (SCI) data base between 1973 and
2003 show a significant increase in the percentage of cervical injuries and of ventilator-
dependent cases, with 6.8% of SCI patients requiring ventilation on discharge between
2000 and 2003 (232). Most SCI patients who require ventilatory support undergo
tracheostomy during their acute hospitalization (233). Despite improvements in SCI
medical management, re-hospitalization rates remain high, associated with respiratory
complications (234). Cervical spine injuries can be separated into higher cervical cord
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 49
injuries (levels C1 and C2) and mid and lower cervical cord injuries (C3 to C8). The
former produce almost total respiratory muscle paralysis, while the latter have limited
expiratory function. Lesions from C3-C5 cause also significant compromise of
inspiration (233).
During the 80’s, survival for ventilatory dependent tetraplegic patients ranged from
63% at 3 years (235) to 33% at 5 years (236). In those times, only 51% of SCI patients
with C3 injury levels were able to be weaned (236). Life expectancy was considerably
improved in those successfully weaned (237).
Because of their youth, intact mental status and bulbar musculature, high level
tetraplegic patients are perfect candidates for non invasive ventilatory assistance (238).
In fact, Bach et al suggest that patients with lesions under C1 level, can be managed by
using noninvasive respiratory aids (up to continuous noninvasive IPPV and manually
and mechanically assisted coughing) provided that they are able to generate assisted
peak cough flow >160 L/min (239).
It is recommended that all patients with acute SCI have their Vital Capacity measured
every 6h during the first few days of admission. If symptoms or signs of impending
ventilatory failure develop or VC decreases < 1500ml, the patient should be placed on
continuous oximetry monitoring and trained in using MIV and Manually and
mechanically assisted coughing (240).
When patients with SCI are tracheostomized, there will always be the potential for
decannulation. Although this topic his beyond the scope of this chapter, it must be
emphasized that even in patients with little ventilator-free breathing ability, switch to
NIV and «aggressive» mechanical insufflation-exsufflation can lead to successful
decannulation (241).
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
50 Miguel Ramalho do Souto Gonçalves

Critical-illness myoneuropathy
ICU-acquired NMD is reported in 25% of patients who have been ventilated for ≥ 7
days (242). This figure increases in patients with sepsis and severe acute asthma (243).
Normally patients present with diffuse skeletal-muscle weakness and difficult weaning.
ICU-acquired NMD is associated with longer duration of mechanical ventilation, longer
ICU stay and increased mortality (243). Cough inefficacy and reduction in maximal
respiratory pressures have been reported in these patients (244), suggesting the
implementation of secretion clearance techniques together with non invasive ventilatory
support can have a role (200). Although studies reporting application of Non-invasive
Respiratory aids in this context are lacking, in the authors’ experience, application of
this protocol in ICU-acquired NMD has allowed decannulation and weaning in a
significant number of patients (data not published).
Critical-illness myoneuropathy have been also implicated in respiratory failure that
develops after discharge from the ICU (244). Recovery of peripheral and respiratory
muscle function is highly variable, with some patients having persisting weakness at 2
years of follow-up.
Contraindications to Noninvasive Positive Pressure Ventilation in
acute care
There are few absolute contraindications to NPPV, the majority of which assume that
endotracheal intubation (ETI) is an immediate option(174). The need for a secure
airway contraindicates use of NPPV, as do severe facial trauma or burns and an ongoing
need to clear airway secretions that cannot be cleared by noninvasive means (including
mechanical assisted cough)(245-246). Altered mental status not due to CO2 retention is
a commonly cited contraindication, as are nausea and vomiting,Most studies have
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 51

excluded patients with significant hypotension and/or recent gastric surgery (within one
week). An uncooperative or combative patient is unlikely to benefit from NPPV(36).
Light sedation or analgesia may aid in the control of the latter type of patient. The
exclusion of patients with acute apnea, active cardiac ischemia, or ongoing arrhythmia
seems reasonable.
Panel II: Contraindications for NPPV in ARF:
The contraindications to NIPPV include (18, 21):
• severe hypoxemia (PaO2/FiO2 < 75mmHg)
• severe acidemia
• multi-organ failure or slowly reversible disease
• upper airway obstruction
• anatomic abnormalities that interfere with gas delivery (i.e., facial burns,
trauma)
• respiratory arrest/apnea
• cardiac arrest and hemodynamic or cardiac instability
• unconscious / uncooperative patient
• encephalopathy with the inability to protect the airway
• increased risk of aspiration (copious secretions, vomiting)
• severe Gastro-intestinal(GI) bleeding
• recent airway or GI surgery
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
52 Miguel Ramalho do Souto Gonçalves

NON INVASIVE VENTILATION IN THE CHRONIC
CARE SETTING
Rationale
Noninvasive ventilation (NIV) constitutes one of the major advances in pulmonary
medicine in recent times, having assumed an important role in the therapy of respiratory
failure in chronic settings(46). Long term NIV in the chronic setting refers to the
provision of NIV mainly at night during sleep, usually for 12 to 24 h, although some
NMD patients gradually extend hours of use to continuous as their disease
progresses(1).
From the 1950s through to the early 1990s, home mechanical ventilation (HMV) was
limited to a relatively small number of individuals using negative pressure devices or
receiving positive pressure ventilation through a tracheostomy(247). More recently,
noninvasive ventilation (NIV) has emerged as an effective and acceptable approach to
managing chronic respiratory failure (CRF) patients outside of the hospital setting(48).
The significant benefits of this therapy have been widely documented, and include relief
of symptoms, improved quality of life, reduced need for unplanned hospitalisation and
improved survival. Consequently, over the past 20 years a dramatic increase in the
number of individuals using HMV has occurred(248).
Before starting respiratory support, it is essential to ask three main questions: 1) Does
the patient have a disease known to cause ventilatory failure? 2) Does the patient have
symptoms suggesting hypoventilation? 3) Does the patient have physiological
abnormalities confirming hypoventilation? Sometimes, due to disease progression,
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 53

ventilatory dependency can increase and ventilatory support must be adapted
accordingly(249).
Indications of Noninvasive ventilatory support
Disease categories (table 1)
A large number of conditions can result in chronic ventilatory failure and benefit from
home ventilation. Typically, patients with restrictive disorders have decreased
compliance of the chest wall, resulting from thoracic cage deformity or respiratory
muscles involvement (250). In patients with severe Obstructive Pulmonary Disorders,
respiratory muscle fatigue and sleep hypoventilation are thought to contribute to
respiratory failure (251-252).
It is useful to define disease category in order to predict natural history and specific
intervention. It is well known that patients with primarily restrictive disorders can have
both inspiratory and expiratory muscle weakness and so apart from non-invasive
ventilatory support they also need cough assistance (207, 219). On the other hand,
patients with obstructive disorders rarely need mechanical expiratory aids except for
severe acute infectious exacerbations when difficulties in clearing copious secretions
can ensure (219, 253-254).
Some neuromuscular diseases, for example Guillain-Barre syndrome, may only require
temporary ventilatory support(255) while other, such as post-polio syndrome requires
lifelong noninvasive ventilatory support (45). Amyotrophic lateral sclerosis, an example
of a rapidly evolving disease, needs a specific approach particularly for the bulbar
involvement which may render noninvasive ventilatory support less effective (221).
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
54 Miguel Ramalho do Souto Gonçalves

Table II- Indications for Non-invasive ventilatory support
Restrictive disorders
Chest wall disorders
Kyphoscoliosis
Thoracoplasty
Fibrothorax
Obesity-hypoventilation syndrome
Stable Neuromuscular Disorders
Old polyomyelitis
Myopathies
Progressive Neuromuscular Disorders
Amyotrophic Lateral Sclerosis
Duchenne Muscular Dystrophy
Other Neurological Disorders
Cervical Spinal Cord Injury
Phrenic nerve lesions
Obstructive disorders
Chronic Obstructive Pulmonary Disease
Bronchiectasis and Cystic Fibrosis
Patient selection
Symptoms of nocturnal hypoventilation
Every consensus statement reinforces the importance of detecting symptoms of
nocturnal hypoventilation(252, 256-259). However, symptoms may be subtle due to the
variability of patient sensitivity and sometimes it is difficult for the patient to establish
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 55

differences between fatigue, dyspnea, and sleepiness. So, carefully designed
questionnaires that assess symptoms systematically may be very useful. Jackson et al
(260) have described a pulmonary symptom scale consisting of 14 questions, answered
on a scale from 1-7. Others evaluated by simple questionnaires the positive and negative
effects of ventilation(261). Although symptom questionnaire are insensitive in
identifying patients with SDB and nocturnal hypercapnic hypoventilation (260, 262)
their systematic evaluation is useful in evaluating response to NIV, as compliance to it
is strongly correlated with patients symptoms (263).
Using rating scales for different symptoms has been also recommended. Dougan et al
(264) developed a useful tool (the MND dyspnoea rating scale) consisting of 16
questions each rated on a five-point likert scale that allows the patients with ALS to
quantify how dyspnea affects their daily life. This specific questionnaire may be more
appropriate to quantify dyspnea in neuromuscular patients compared with other existing
measures such as the Medical Research Council (MRC) dyspnea scale (265).
Moreover, one of the most common used sleepiness scales, the Epworth Sleepiness
scale, may not be as reliable in NMD like Myotonic Dystrophy (266).
Physiologic evaluations
Together with the careful evaluation of symptoms, monitoring of respiratory function
should be evaluated routinely. Vital Capacity (VC) is one of the most reproducible tests
of lung function. Although it may not fall below normal limits until there is a 50%
reduction in muscle strength (267), its rate of decline has been shown to predict survival
(268). Although no consensus exist as to how often pulmonary function should be
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
56 Miguel Ramalho do Souto Gonçalves

evaluated, some authors propose that if VC is > 60% predicted it should be performed
every 6 months while if under 60% every 3-4 months (269)
Measurement of the VC in the supine position gives and index of weakness of the
diaphragm. A fall of more than 15% indicates diaphragmatic dysfunction and correlates
with complaints of orthopnea (270) and a supine FVC under 75% was highly sensitive
and specific of low transdiaphragmatic pressure (271).
Muscle strength
Like VC, testing for respiratory muscle strength should be obtained periodically.
Maximal inspiratory mouth pressure (MIP) values > 80cmH20 exclude clinically
relevant respiratory muscle weakness(267). A low MIP with a normal MEP suggests
isolated diaphragmatic weakness. Sniff nasal inspiratory pressure (SNIP) is a more
natural and easier to perform manoeuvre than MIP (272). Values greater than -
70cmH20 (for males) and -60cmH2O (for females) exclude significant inspiratory
muscle weakness(273). Moreover a SNIP < 40cmH20 was associated with nocturnal
hypoxemia and predicted median survival at 6 months(273). Chaudri et al (274) also
recommend that patients with SNIP<30 % of predicted are at risk of developing
hypercapnia and should have their ABG measured. Some authors advise that in patients
with moderate to severe restrictive defect MIP is higher than SNIP so suggesting that
the latter may overestimate the level of inspiratory weakness in this context(275).
Transdiaphragmatic pressures and nonvolitional tests of respiratory muscle strength are
more accurate and may be indicated when others tests are difficult to interpret or in the
context of clinical trials (268).
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 57

Blood Gases
Once the VC drops below 50% of predicted or MIP (or SNIP) below 30% predicted,
daytime arterial blood gases (ABG) should be checked (276). However, performance of
ABG analysis at every clinic attendance is uncomfortable for patients. Accurate devices
for measuring PaO2/PaCO2 non-invasively are becoming available and will become
standard practice in the future.
Daytime oxygen saturation (SpO2) measurement by pulse oximetry can be routinely
used as screening tool. If SpO2 is under 95% it can either be caused by inspiratory,
expiratory of bulbar dysfunction (221). In ALS, when SpO2 can not be normalized by
NIV and mechanical assisted cough tracheostomy needs to be considered due to severe
bulbar dysfunction (221).
Capnography as been recommended as ideal for measuring carbon dioxide
tensions(277). It measures end-tidal CO2 and can be performed during daytime
evaluations and continuously during sleep (278-279). According to recent data,
measuring ETCO2 by a VC maneuver provides a more accurate estimate of PaCO2 and
can be very useful for check-point determinations in hospital or at home (278).
Transcutaneous CO2 (TcCO2) has been widely used for long-term measurement during
sleep and after NIV (280-282). TcCO2 measurements require more time and its levels
are normally 3-12 mmHg higher and more accurate than ETCO2 (283-284). However
some authors advise that the accuracy of TcCO2 seems to be restricted to patients with
PaCO2 values <56mmHg (285).
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
58 Miguel Ramalho do Souto Gonçalves

Noninvasive methods of CO2 monitoring normally tend to give a slightly higher PaCO2
level, so a normal reading can exclude hypercapnia (267).
More recently combined TcCO2-SpO2 single sensors have been investigated, and seem
valid in various settings (286-288).
Noninvasive ventilation support in stable COPD
Long term NIV in COPD remains an area of controversy. The central conundrum is that
while there are have been no randomised trials which demonstrate a major impact on
survival or quality of life, the use of home NIV in COPD is a major growth area. A
European survey (194) has shown that in some countries far more obstructive lung
disease patients then restrictive patients are long term NIV recipients, even adjusted for
prevalence.
It is interesting to observe that early studies showed very mixed results. Case series (8,
289) from the early 1990s indicated that a possible target group for home NIV might be
those COPD patients that developed hypercapnia on long term oxygen therapy (LTOT).
Several uncontrolled (290) or retrospective studies (291) suggested significant
improvement in arterial blood gas tensions, and a possible reduction in hospital
admissions and General Practitioner consultation rates (292). In a cross over study of
LTOT v. NIV plus LTOT Meecham Jones and colleagues (293) demonstrated
improvements in nocturnal and arterial blood gas tensions on NIV and enhanced sleep
quality and improvement in quality of life. These results are offset by another
crossover study (294) that showed worse sleep quality using NIV v.LTOT, and two
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 59

small randomised trials (295-296) which showed no significant improvement in
physiological measures. In the RCT by Gay et al (296) bilevel pressure support was
compared to sham NIV. Poor tolerance of NIV was noted in both RCTs. A number of
messages emerge from this early work – firstly a suggestion that more hypercapnic
subgroups of patients may be more likely to benefit, and secondly in some studies
relatively low level of inspiratory positive pressure support were applied which may not
have been effective.
Finally is seems that acclimatisation to NIV may be slower in some COPD patients than
in those with restrictive disorders, therefore trials lasting only a few weeks may be
insufficient to gauge the impact of the intervention, even on physiological endpoints.
Clearly, longer trials are also required to investigate effects on the key outcomes of
frequency of exacerbations, quality of life and survival. More recently there have been
two longer term randomised controlled trials. Casanova et al in a one year study (297)
randomised 52 COPD patients to standard care or standard care plus NIV. Outcomes
included rate of acute exacerbations, hospital admissions, need for intubation and
mortality at 3, 6 and 12 months. For the NIV group, ventilation was initiated as an
inpatient using a bilevel positive pressure system in spontaneous mode. The authors
targeted an expiratory positive airway pressure (EPAP) level of 4 cmH2O and an
inspiratory positive airway pressure (IPAP) level of at least 12 cmH2O. Pressures were
adjusted to decrease perception of dyspnoea and accessory muscle use, and oxygen
delivered to the mask to achieve a SaO2 > 90%. Five of the NIV group (total n=26) did
not tolerate NIV. Average ventilation in the remainder was 6.2 hours per 24 hours and
marginally decreased to 5.9 hours/24 hours at 9 months. Eleven percent used NIV for
less than 3 hrs/day.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
60 Miguel Ramalho do Souto Gonçalves

One year survival was similar in both groups. The number of acute exacerbations did
not differ between standard and NIV groups at all time points. However, the frequency
of admissions was decreased at 3 months in the NIV group (5% versus 15%, p<0.05),
although this difference was not sustained at 6 months. Borg breathlessness scores
decreased in the NIV group, but only one psychomotor test improved. The authors
carried out a subgroup analysis to see if any clinical or functional variables were
predictive of benefit, but in this study there was no evidence that more hypercapnic
patients (PaCO2 >7.3 kPa versus PaCO2< 7.3Kpa), or those that used NIV for >5 hours
per 24 hours did better than standard group.
In an Italian multicentre trial (298) which has furthered the debate, 122 stable
hypercapnic COPD patients on LTOT for > 6 months were randomised to continue
LTOT alone, or LTOT plus NIV using a bilevel positive pressure device over a 2 year
period. The study was powered to assess reduction in daytime PaCO2 rather than
mortality. Drop out rates were similar in both groups, and compliance with NIV was
impressive at 9 hours/24 hours.
The authors showed no significant difference in hospital or ICU admissions, although
there was a trend to fewer admissions in the NIV group (compared to the previous year
admissions decreased by 45% in NIV group and increased by 27% in LTOT group).
Mortality did not differ. PaCO2 was slightly reduced in NIV patients using LTOT and
there was also a reduction in dyspnoea and increase in heath related quality of life
scores in NIV group. Potential criticisms of the study are that the IPAP levels used
were low, it is difficult to know whether nocturnal hypoventilation was corrected by
nighttime NIV, and it is possible that some quality of life and symptomatic
improvements might be related to a placebo effect. A reasonable riposte to this last
point is that although short term trials using sham CPAP and sham NIV have been
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 61

perfomed, it would be difficult practically and ethically to carry out a randomised trial
of NV over several years with a sham NIV limb.
It is evident therefore that widespread use of longterm NIV across the board in COPD
patient cannot be justified on the evidence presented above. The studies do however
suggest that primary end points of number of acute exacerbations and hospital
admissions may be a more sensitive measure than mortality. The frequency of acute
exacerbations of course has economic implications. On that point Tuggey et al (299)
examined the economic impact of home NIV in a selected group of COPD with
recurrent exacerbations who had responded well to NIV during these acute episodes. In
this group, preselected because of good tolerance, provision of home NIV resulted in a
mean cost saving of 11720 euros (5698-17,743 euros) per patient year. The number of
hospital admissions in the year on NIV compared to the year pre NIV was reduced from
5 to 3, mean hospital days decreased from a mean (SD) of 78 (51) to 25 (25) p=0.004,
and ICU days fell from 25 to 4 (p=0.24). Outpatient visits also decreased.
Noninvasive ventilation support in restrictive disorders
Chest wall disorders
Patients with untreated scoliosis have an increased risk of developing respiratory failure
(300) . The larger the scoliotic angle, the lower the vital capacity and the younger the
age of scoliosis onset, the greater is the risk (301). Patients who have reached skeletal
maturity and have a vital capacity below 45% of predicted value the risk of developing
respiratory failure increases with age (301). Symptoms of cardio-respiratory failure
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
62 Miguel Ramalho do Souto Gonçalves

generally appear between the fourth and sixth decade of life, however some patients
survive into the seventh decade without experiencing cardio-respiratory problems (302).
It is well known that severe kyphoscoliosis may induce sleep-related respiratory
abnormalities (303) and retrospective long-term studies of nocturnal NIV have shown a
better prognosis of those patients compared with neuromuscular and obstructive
disorders (8, 289). In fact, in prospective studies, NIV improves hypoventilation-based
symptoms, muscle function and nocturnal oxygenation in patients with daytime
hypercapnia and FVC< 50% (304-305). In patients with less severe respiratory
impairment, nocturnal NIV improves significantly exercise capacity and there is a trend
for an increase in daytime PaO2 (306). Data from a large French observatory (307) and
a recent prospective study (308) clearly show that kyphoscoliotic patients treated by
home mechanical ventilation experience a better survival than those treated by oxygen
therapy alone. Moreover, Masa et al have shown that NIV but not oxygen improved
nocturnal hypoventilation in 7 patients with Kyphoscoliosis and normal daytime ABG
(309). So, in symptomatic patients with daytime normocapnia but significant nocturnal
desaturation (according with Masa (309) > 10% of Total sleep time with <90% SpO2 or
mean REM SpO2 <90% and minimum SpO2<90% and according with the consensus
conference (252) SpO2≤ 88% for 5 consecutive minutes) NIV is warranted (252).
Amyotrophic Lateral Sclerosis
Although initially regarded as controversial because of fear that it would simply delay
death without improving quality of life, NIV has become the standard of care for
patients with symptoms and evidence of respiratory involvement (310). In fact, NIV
improves symptoms, quality of life (260, 311) and survival (312).
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 63

Because ALS patients eventually become quadriplegic, they require a high level of
assistance from caregivers (313). In one study, one of the best predictors of success of
NIV was a good caregiver support (314).
Although there is no clear evidence regarding timing for NIV, it seems reasonable to
start in symptomatic patients (table II) with signs of respiratory muscle weakness
(FVC<80% or SNIP<40cmH20) and evidence of significant nocturnal desaturation or
PaCO2> 49mmHg (310). Bourke et al suggest that ortopnea was the most useful
criterion for benefit and compliance with NIV (311) , and Sivak (315) that there was a
lack of correlation between VC at the institution of NIV and the duration of its
successful use.
In a small prospective study Jackson et al (260) suggest that early intervention, based on
nocturnal oximetry criteria (SpO2<90% form 1 cumulative minute), may result in
improved quality of life with NIV.
For most patients, NIV begins at night but may rapidly develop 24h ventilator
dependence (316). If bulbar function is well preserved, continuous NIV (daytime
mouth-piece and nocturnal oro-nasal NIV) may manage up to 20% of ALS patients
safely for long years (221, 239, 316), avoiding tracheostomy.
Unlike patients with Duchenne Muscle Dystrophy, Post-Poliomyelitis Syndrome, and
most other NMD, ALS may have bulbar muscle dysfunction, carrying a high risk of
aspirating saliva and not being able to clear airways secretions (316).
Bulbar muscles involvement carries a worse prognosis (317) and in those patients, NIV
may be less tolerated (318-319). However the recent RCT found that patients with
moderate to severe bulbar impairment gained a smaller, although clinically significant
quality of life benefit from NIV (312).
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
64 Miguel Ramalho do Souto Gonçalves

Bulbar muscle dysfunction should be evaluated in patients with ALS. Apart from rating
scales like the ALSFRS (320) one of the best ways to measure it objectively is by
comparing the MIC with the VC and the PEF with the CPF. The wider the gradient, the
better the bulbar function (321-322). Bach has shown that in ALS, that the ability to
generate assisted CPF>180L/min and to have an high MIC VC difference is associated
with the capacity to use continuous NIV (224). However, when strictly tailored NIV
and Mechanical Assisted Cough does not prevent oxygen desaturation below 95%,
saliva aspiration is likely and tracheostomy should be offered (221).
Care should also be put into secretion management since Mechanical Assisted Cough to
prevent airway encumbrance is an essential complement to NIV and a key to successful
full-time NIV (316)
Duchenne muscular dystrophy
Duchenne Muscular dystrophy (DMD) has an X-linked recessive pattern of inheritance
and affects up to 1 in 3300 live male births. (323) Affected patients typically become
wheel chair dependent by the age 10-12 years at which VC plateaus. With the
development of respiratory muscle weakness and skeletal deformity, VC starts to fall
(324). The patients usually remain asymptomatic until VC decreases below 450ml and
begin daytime hypercapnia (212). Hukins et al suggest that once FEV1 falls below 40%
predicted, arterial blood gases should be performed (325) and Hahn et al report that
hypercapnia appears in patients with MIP lower than 30cmH2O or 30% of predicted
normal (326).
The first signs of respiratory involvement occur during sleep. Obstructive sleep apnea is
very frequent in DMD, with some authors reporting a prevalence of 57% (327), and
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 65

occurring more commonly in younger children (328). Hypoventilation was the major
abnormality in older children (early second decade) (328).
By the time patients become hypercapnic, nocturnal NIV is clearly indicated. Vianello
et al (329) have shown that life expectancy is <1 year once diurnal hypercapnia
develops and compared with a non-ventilated control group, NIV significantly
prolonged survival in DMD patients with symptomatic daytime hypercapnia. In fact the
majority of published studies using NIV in DMD included patients with symptoms and
diurnal hypercapnia (17, 324, 330). In a UK study that followed a cohort of 23 severely
hypercapnic patients with DMD, the use of NIV has increased median survival, with a 5
year survival of 73% (17).
In a randomised controlled trial, including normocapnic, essentially asymptomatic
patients with VC between 20-50%, Raphael et al did not show any improvement in
survival (331). However this study should not be viewed as definitive as their findings
may have been caused by a lack of standardized ventilator and mask use between
investigators (332). In addition it may be argued that for NIV to be effective longterm,
the implementation of assisted cough techniques are critical a intervention that was not
considered in this trial, in which the main causes of death in the NIV group were due to
infection with retention of tracheobronchial secretions.
Although some authors suggest that once the VC is <1L the 5 year survival rate is 8%
(333) with inspiratory and expiratory non-invasive respiratory aids, 10 year survival can
be up to 93.3% (212). In fact, compared with a conventional approach before 1993, with
a proactive protocol that included NIV (up to full time) together with Mechanical In-
Exsufflation guided by home oximetry, the New Jersey University Hospital has
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
66 Miguel Ramalho do Souto Gonçalves

managed to significantly extend survival and avoid respiratory mortality in patients with
DMD(63).
More recently several groups in Europe have shown that once nocturnal hypercapnia
(measured by transcutaneous CO2) is present treatment with NIV should be
implemented (334-336). Others, in the absence of nocturnal CO2 measurements,
suggest that symptomatic patients with mean nocturnal SpO2 below 94% should be
encouraged to use NIV, especially if they had symptomatic relieve or correction of
nocturnal desaturation (207).
According with the ATS consensus statement daytime ventilation should be considered
when measured waking PaCO2 exceeds 50mmHg or when haemoglobin saturation
remains <92% while awake (277). The most commonly used noinvasive technique is
mouth-piece intermittent positive pressure ventilation (M-IPPV), which was first
reported in 1969 (337). Since then the New Jersey University Hospital has extensively
reported their experience with M-IPPV for continuous NIV as an alternative to
tracheostomy (338-340). Others centers from the US have also described their
successful experience (330, 341-344). In Europe, although an expert group report
recommended its use in 1993 (345), it was not until very recently that diurnal
ventilation via mouthpiece was described in end-stage DMD patients (335). In this
prospective study, Toussaint et al have shown that a simple angled mouthpiece held
stable near the mouth could confortably deliver volume cycled ventilation during the
daytime, stabilising VC, decreasing symptoms, daytime hypercapnia and extending
survival up to 7 years in 51% of 42 M-IPPV users(335).
Death from cardiomyopathy is significant in patients with DMD, so regular cardiac
assessment and adequate medication should be implemented (346)
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 67

A recent study has shown that although patients with DMD are severely disabled they
still perceive a high quality of life, not correlated with physical impairment nor the need
of NIV (347).
MANUAL AND MECHANICAL TECHNIQUES FOR
SECRETION MANAGEMENT
Rational
In healthy individuals, mucociliary clearance and cough mechanisms are normally
effective and efficient for defence on secretion encumbrance, but may become
ineffective if these systems malfunction and in the presence of excessive bronchial
secretions. Mucus secretion and clearance are extremely important for airway integrity
and pulmonary defence. It has been estimated that mucus secretion volume is between
10 and 100ml per day in healthy subjects (348).
Mucus is transported from the lower respiratory tract into the pharynx by airflow and
mucociliary clearance. Overload of normal secretion or mucociliary clearance impairs
pulmonary function and increases risk of infection. When there is extensive ciliary
damage and secretion encumbrance, coughing becomes critically important for airway
hygiene (349). Airflow dependent clearance can also be increased by moving secretions
from the periphery of the lung to the more proximal airways, were greater secretion
depth and higher expiratory air flow can improve expectoration. This is why cough is
generally incorporated into most chest physical therapy techniques (350).
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
68 Miguel Ramalho do Souto Gonçalves

Cough and expectoration of mucus are the best-known symptoms in patients with
pulmonary impairment disorders. Airway clearance may be impaired in disorders
associated with abnormal cough mechanics, altered mucus rheology, altered
mucociliary clearance, or structural airway defects. A variety of interventions are used
to enhance airway clearance with the goal of improving lung mechanics and gas
exchange, and preventing atelectasis and infection (351).
Techniques for augmenting the normal mucociliary clearance and cough efficacy have
been used for many years to treat patients with respiratory disorders from different
etiologies. In recent years, new technologies and more advanced techniques have been
developed to be more comfortable and effective for the majority of patients. Postural
drainage with manual chest percussion and shaking has, in most parts of the world, been
replaced by more independent and effective techniques such as the active cycle of
breathing, autogenic drainage, R-C Cornet®, Flutter®, positive expiratory pressure
mask, high frequency chest wall oscillation, intrapulmonary percussive ventilation and
mechanical insufflation-exsufflation (349). The evidence in support of these techniques
is variable and the literature is confusing and sometimes conflicting, regarding the
clinical indication for each technique. This fact may be related to the intensity, duration
and frequency being different between physiotherapists in different parts of the world,
and have changed over the years (352). Moreover, it can be confusing for health care
professionals, patients and their caregivers when it comes to choosing and utilizing the
most appropriate airway clearance techniques and products.
Patients who require mechanical breathing assistance or pharmaceutical intervention,
often also need assistance to mobilize and clear secretions from their airways and lungs.
It is critically important for these patients to keep their airways clear of secretions to
avoid the risk of atelectasis caused by mucus plugs and infections, including
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 69

pneumonia, which can often lead to numerous hospitalizations and even premature
death. Patients with chronic lung disease, such as chronic obstructive pulmonary disease
(COPD) and Cystic Fibrosis (CF), those that have neuromuscular disorders such as
muscular dystrophy (MD), amyotrophic lateral sclerosis (ALS), spinal muscular atrophy
(SMA), post-polio syndrome, and those paralyzed due to Spinal Cord Injury (SCI), are
at the greatest risk of developing such infections.
The effective elimination of airway mucus and other debris is one of the most important
factor that permits successful use of chronic and acute ventilation support (noninvasive
and invasive) for patients with either ventilatory or oxygenation impairment. In
ventilatory dependent patients, the goals of intervention are to maintain lung
compliance and normal alveolar ventilation at all times and to maximize cough flows
for adequate bronchopulmonary secretion clearance (353).
In patients with primarily ventilatory impairment, such us neuromuscular disease, 90%
of episodes of respiratory failure are a result of inability to effectively clear airway
mucus during intercurrent chest colds (354). Although the use of respiratory muscle
aids is the single most important intervention for eliminating airway secretions for
patients with inspiratory and expiratory muscle weakness, as for normal coughing these
aids may not adequately expulse secretions from the very small peripheral airways more
than 6 divisions from the trachea, the flows they create may not be sufficient to
eliminate secretions that are obstructing the smaller airways (355). In these situations, it
is important to consider secretion mobilization techniques to gradually loosen and
mobilize secretions to assist mucociliary clearance from the lower airway into the upper
airway where they then need to be cleared by either assisted coughing techniques or the
patient’s natural cough.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
70 Miguel Ramalho do Souto Gonçalves
A great majority of episodes of secretion encumbrance develop in acute respiratory
failure and it has been demonstrated that in even in acute episodes of respiratory failure
morbidity and mortality can be avoided without hospitalisations with a correct and
effective secretion management protocol (356). Moreover, it has been reported that
conventional chest physical therapy for secretion management does not increase the
chances of weaning and extubation success in critical ill patients (357). However, some
of these patients may have normal mucociliary clearance but ineffective peak cough
flows (CPF) which itself has been associated with extubation failure (37, 358). A
protocol that includes assisting coughing techniques as adjunct to a efficient NIV
application may increase the success rates of extubation in difficult to wean patients.
Patient evaluation and monitoring
The respiratory patient evaluation includes a survey for symptoms of chronic and /or
acute alveolar hypoventilation, medical history, physical examination, cough evaluation
and simple pulmonary function tests. Measurement of mucous transport through the
bronchial tree by radiolabeled tracers is a technique that has been used above all to
study mucociliary clearance, as well as the measurement of the volume of expectorated
mucous (359).
Respiratory physiotherapy interventions can be evaluated using different outcome
variables, such as bronchial mucus transport measurement, measurement of the amount
of expectorated mucus, pulmonary function, medication use, frequency of acute
exacerbations and quality of life(349, 352, 360).
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 71

Pulmonary function and cough tests
Evaluation of respiratory physiotherapy interventions only with pulmonary function
tests appears to be inadequate for significant conclusions. However it is knowned that
mucus retention has a strong impact on pulmonary function and gas exchange. Severe
mucus retention can cause an acute decrease in vital capacity (VC), forced VC, flow
rates, as well as SpO2. Patients with severe airway obstruction have more difficulties
expectorating mucus. Patients with ineffective cough and low VC´s are in extreme
respiratory distress in the presence of secretion accumulation. A correct evaluation of
pulmonary function and cough parameters may predict a successful respiratory
physiotherapy treatment.
Poponick et al.(361) demonstrated that acute viral illness was associated with a
reduction in vital capacity (VC) due to a reduction in inspiratory and expiratory
respiratory muscle strength (by 10–15% of baseline values), which causes a decline in
CPF to the critical level of 160 L·min-1.
A spirometer is used to measure VC in sitting, recumbent, and sidelying positions. The
spirometer is also used to measure the maximal insufflation capacity (MIC) for patients
with VCs at least 30% less than predicted normal levels who are trained in air stacking
(362). Usually a manual resuscitator is used for the patient to air stack via a mouthpiece
for the MIC measurements (Figure 14).
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
72 Miguel Ramalho do Souto Gonçalves

Figure 14: Air stacking with manual resuscitator via a mouthpiece in a DMD patient with low
vital capacity and suboptimal peak cough flow.
An effective CPF requires a pulmonary inspiration or insufflations until 85-90% of the
vital capacity, and the generation of high intratoracic pressure so as to expel 2,3-2,5 L of
air at a CPF of 6-20 L/sec. In order for an effective cough to occur, the Peak Cough
Flow (CPF) must be higher than 270 L/min (363)
Unassisted cough peak flows (CPF) are measured by having the patient cough as hard
as possible through a peak flow meter to get a baseline value. Kang and Bach (364)
proved that the CPF value could be even higher if it is performed through the Maximum
Insufflation Capacity (MIC). The MIC is related to the pulmonary compliance and with
the pharyngeal and oropharingeal muscles function. After a deep inspiration the subject
makes an apnoea and receives an extra air volume of air (through a manual resuscitator
or volume ventilator) via a mouthpiece, nasal interface. This extra air volume will
produce the lung distension, allowing a cough at a higher volume, and therefore more
effective. The patient coughs via an oronasal interface if there is a tendency for
insufflated air to leak out of the nose.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 73

Finally, (fully) assisted CPF are measured from the MIC with an abdominal
thrust timed to glottic opening. The most important CPF measurement is usually the
latter because it is the manually assisted cough from the MIC that the patient must often
use to clear airway secretions to avoid respiratory failure. The inability to generate a
CPF greater than 2.7 L/s even when MIC exceeds 1 L, generally indicates the existence
of fixed upper airway obstruction or significant bulbar impairment, with
hypopharyngeal collapse during mechanical assistance to aid cough (60, 365-366).
Control of Mucus and Airway Clearance Techniques
Airway clearance refers to two separate, but connected, mechanisms: mucociliary
clearance and cough clearance. Techniques for controlling and assisting the
mobilization of secretions from the airways have long been advocated for use in the
patient with impairment in mucociliary clearance or an ineffective cough mechanism.
The goals of this therapy are to reduce airway obstruction, improve mucociliary
clearance and ventilation and optimise gas exchange.
Approaches to preventing airway secretion retention include pharmacotherapy to
reduce mucus hypersecretion or to liquefy secretions, and the application of chest
physiotherapy techniques. Chest physiotherapy (CPT) can be defined as the external
application of a combination of forces to increase mucus transport that include postural
drainage positions, special breathing exercises, manual chest vibration and percussion,
autonomous instrumental techniques and manual assisted coughing.
Research studding the results of airway clearance are often difficult to evaluate because
the components of a given treatment have not been standardized. Availability of
equipment or education about a technique as well cultural differences in its application
confounds the results. CPT does not appear to benefit patients during recovery from
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
74 Miguel Ramalho do Souto Gonçalves

acute exacerbations of COPD or pneumonia. These conditions are characterized by
interstitial pathology, which cannot be influenced by physical interventions in the
airways (367-369). Further studies are needed to identify the patients and more
circumstances, which are at risk from complications or adverse effects of chest
physiotherapy.
Chest physical therapy techniques
Approaches to preventing retention of airway secretions include the use of medication
to reduce mucus hypersecretion or to liquefy secretions and the facilitation of mucus
mobilization. To complement this objective, chest physiotherapy techniques (CPT) are
shown to be very effective in preventing pulmonary complications in infant and adult
patients with bronchopulmonary secretion accumulation. The principles of manual chest
physiotherapy techniques consists in the application of external forces in the thoracic
cage that have direct effect on mucus mobilization.
Manual chest percussion, sometimes referred to as chest clapping, is very well knowed
in the respiratory physiotherapy community. Some authors demonstrated an increase in
airflow obstruction when chest clapping was included in an airway clearance regimen
(370). Chest clapping has also been shown to cause an increase in hypoxemia, but when
short periods of chest clapping have been combined with three or four thoracic
expansion exercises, no fall in oxygen saturation has been seen(349). Some patients
with severe lung disease demonstrate oxygen desaturation with self-chest clapping. This
may be due to the work of the additional upper limb activity. On the basis of three
randomised, controlled trials of chest physiotherapy and one observational study,
manual chest percussion as applied by physical or respiratory therapists is ineffective
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 75

and perhaps even detrimental in the treatment of patients with acute exacerbations of
COPD(371).
Another manual chest physical therapy technique is vibration applied throughout
exhalation concurrently with mild compression of the patient’s chest wall. Vibration is
proposed to enhance mucociliary transport from the peripheral of the lungs fields to the
larger airways.
Manual thoracic techniques are effective in removing pulmonary secretions, facilitating
inspiration and improving alveolar ventilation. Guidebooks have been published that
demonstrates the hand placements and thrusting techniques in children and adults (372).
Manual assisted coughing techniques
Cough is the primary defense mechanism against foreign bodies in the lower airways.
Any stimulation of the pharyngeal, laryngeal, tracheal or bronchial receptors can create
a cough. When this mechanism is not functioning correctly mucus restrain will occur, as
bronchial obstruction. This problem may be due to the fact that the subject cannot make
a deep inspiration, or incapable of glottis closure, or incapable of rising intra abdominal
and intra thoracic pressure.
An effective cough is based of expiratory muscles force, capable of producing effective
CPF´s. The CPF is a routine measure in the evaluation of neuromuscular patients (373)
and clinical investigations such suggest that it should be used in spinal cord patients as
well (88, 97).
The patient with partial or complete abdominal muscle paralysis is unable to produce an
effective cough. Manually assisted cough is the external application of pressure to the
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
76 Miguel Ramalho do Souto Gonçalves

thoracic cage or epigastric area, coordinated with a forced exhalation. This action serves
to simulate the normal cough mechanism by generating an increase in the velocity of the
expired air and may be helpful in moving secretions toward the trachea, where they can
be removed by nasotracheal suctioning.
The abdominal thrust is an assisted coughing technique which consists of the
association of two techniques: the costo-phrenic compression and the Heimlich
manoeuvre. The combination of deep lung insufflations to the MIC followed by manual
assisted cough with abdominal thrust (Figure 15) has been shown to increase
significantly CPF´s values in restrictive patients (366, 374).
Although an optimal insufflation followed by an abdominal thrust provides the greatest
increase in CPF, it can also be significantly increased by providing only a maximal
insufflation or providing only an abdominal thrust without a preceding maximal
insufflation. Interestingly, CPF are increased significantly more by the maximal
insufflation than by the abdominal thrust (375-376).
Manually assisted coughing and MIC maneuver requires a cooperative patient, good
coordination between the patient and care giver), and adequate physical effort and often
frequent application by the family care giver (Figure 2). It is usually ineffective in the
presence of severe scoliosis because of a combination of restricted lung capacity and the
inability to effect diaphragm movement by abdominal thrusting because of severe rib
cage and diaphragm deformity.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 77

Figure 15: Air stacking and manual assisted cough in a patient with neuromuscular disease, performed by
the family care giver
Abdominal compressions should not be used for 1 to 1.5 hours following a meal,
however, chest compressions can be used to augment CPF. Chest thrusting techniques
must be performed with caution in the presence of an osteoporotic rib cage.
Unfortunately, since it is not widely taught to health care professionals manually
assisted coughing is under utilized (377).
Mechanical Respiratory Muscle Aids for Secretion Management
Respiratory muscle aids for secretion management are devices and techniques that
involve mechanical application of forces to the body or intermittent pressure changes to
the airway to assist expiratory muscle function and airway mucus clearance. The
devices that act on the body include high frequency chest wall oscillators that create
atmospheric pressure changes with oscillations around the thorax and abdomen,
intrapulmonary percussive ventilators that create a rapid frequency adjusted for internal
percussion for mucus progression to the large airways, and insufflation- exsufflation
devices that apply force and pressure changes directly to the airway to assist the
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
78 Miguel Ramalho do Souto Gonçalves

expiratory muscles for cough augmentation and the inspiratory muscles for lung
expansion.
Intrapulmonary Percussive Ventilation (IPV)
The intrapulmonary percussive ventilator is an airway clearance device that
simultaneously delivers aerosolized solution and intrathoracic percussion. This modified
method of intermittent positive-pressure breathing imposes high-frequency minibursts
of gas (at 50–550 cycles/min) on the patient’s own respiration. This creates a global
effect of internal percussion of the lungs, which could promote clearance of the
peripheral bronchial tree.
IPV devices include: Im®-F00012, IPV1C®-F00001-C, IPV2C®-F00002-C
(Percussionaire® Corporation, ID, USA); and IMP II (Breas Medical, Sweden). The
percussions (sub-tidal-volume) are delivered continuously through a sliding air-
entrainment device (called Phasitron) powered by compressed gas at 20–40 psi. The
high frequency gas pulses expand the lungs, vibrate and enlarge the airways, and deliver
gas into distal lung units, beyond accumulated mucus (378-380) . Treatment with IPV is
titrated for patient comfort and visible thoracic movement. The patient initiates the flow
of gas and during inspiration the pulsatile flow results in an internal percussion.
Interruption of the inspiratory flow allows for passive expiration.
This technique has been shown to be as effective as a standard chest physiotherapy and
to assist mucus clearance in patients with secretion encumbrance from different
etiologies, such as cystic fibrosis (381), acute exacerbations of COPD (41) and
Duchenne muscle dystrophy (378). In cystic fibrosis IPV was shown to be as effective
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 79

as the other methods of airway clearance in sputum mobilization, when the amount of
sputum produced was assessed by dry weight(382).
IPV can be delivered through a mouthpiece, a facial mask and also through a
endotraqueal and tracheostomy tube (383). The primary aims of this technique are to
reduce secretion viscosity, promote deep lung recruitment, improve gas exchange,
deliver a vascular “massage”, and protect the airway against barotrauma. The main
contraindication is the presence of diffuse alveolar haemorrhage with homodynamic
instability. Relative contraindications include active or recent gross hemoptysis,
pulmonary embolism, subcutaneous emphysema, bronchopleural fistula, esophageal
surgery, recent spinal infusion, spinal anesthesia or acute spinal injury, presence of a
transvenous or subcutaneous pacemaker, increased intracranial pressures, uncontrolled
hypertension, suspected or confirmed pulmonary tuberculosis, bronchospasm, empyema
or large pleural effusion and acute cardiogenic pulmonary edema(384).
High-frequency chest wall oscillation (HFCWO)
In 1939 it was recognized that alveolar ventilation and blood circulation could be
assisted by rapidly alternating negative and positive pressure under a chest shell. J. H.
Emerson developed the first high frequency chest wall oscillation jacket, the Ucyclist-B
Vest, to facilitate bronchial secretion clearance in the early 1950s but he provided
oscillation only during part of the breathing cycle. Barach described use of a similar unit
by patients with chronic bronchial asthma and emphysema in 1966 (385).
During HFCWO, positive pressure air pulses are applied to the chest wall. Oscillation
and vibration can be applied externally to the chest wall or abdomen by rapidly
oscillating pressure changes in a vest that include the SmartVest® (Electromed Inc,
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
80 Miguel Ramalho do Souto Gonçalves

MN, USA), The Vest® (Hill-Rom, MN, USA) and the ThAIRapy Vest™, (American
Biosystems, Inc., St. Paul, MN), or by cycling oscillating pressures under a chest shell
(Hayek™ oscillator, Breasy Medical Equipment Inc., Stanford, CN).
This technique provides oscillation at 5 to 25 Hz. Mechanical vibration is performed at
frequencies up to 40 Hz. Vibration is applied during the entire breathing cycle or during
expiration only. The adjustable I/E ratio permits asymmetric inspiratory and expiratory
pressure changes (for example +3 to -6 cm H20), which favor higher exsufflation flow
velocities to mobilize secretions. Baseline pressures can be set at negative,
atmospheric, or positive values thus commencing oscillation above, at, or below the
functional residual capacity (FRC) (39, 353). The average length of time spent in each
treatment session will vary according to patient tolerance, amount and consistency of
secretions, and the phase of the patient´s illness (acute or chronic)(380). Simultaneous
use of an aerosolized medication or saline is recommended throughout the treatment.
This humidifies the air to counteract the drying effect of the increased airflow (41).
HFCWO may act like a physical mucolytic, reducing both the spinability and
viscoelasticity of mucus and enhancing clearance by coughing (353, 379, 386). High
frequency chest wall oscillation (HFCWO) has demonstrated efficacy in assisting
mucus clearance in patients with disorders associated with mucus hyper-secretion but
preserved muscle function such as cystic fibrosis (CF) (386). HFCWO is an external
non-invasive respiratory modality proven effective in mobilizing airway secretions from
the small peripheral airways and improving mucus rheology in patients with CF and has
become an important modality in the airway clearance techniques of this group of
patients (387-389). High frequency oscillation to the airways has also been reported to
increase mucus transport in healthy subjects (390).
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 81

These beneficial effects upon both mucus clearance and clinical parameters are are not
so evident in other groups of patients such as COPD. Moreover, side effects of
percussion and vibration include increasing obstruction to airflow for patients with
COPD. (369, 391-392). The proven value of HFCWO in patients with relatively normal
mucus composition and characteristics but neuromuscular weakness is still under
investigation, especially as a long-term treatment modality. In one study, the addition of
HFCWO to randomly selected patients with ALS failed to achieve any significant
clinical benefits in relation to the time of death (survival days). In addition, HFCWO
failed to modify the rate of decline in FVC given the progressive nature of this chronic
neurodegenerative disease process. There were no significant differences concerning the
frequency of atelectasis, pneumonia and number of hospitalisations for a respiratory
related abnormality, or requirement for tracheostomy and mechanical ventilation (39).
On another hand, Lange et al (393) also compared lung function parameters in ALS
patients who were randomized to 12 weeks of HFCWO or no treatment. Results showed
maintenance of FVC and decreased fatigue and dyspnoea in HFCWO group compared
to the untreated group.
Contraindications for HFCWO are mostly the same as for IPV, plus head or neck injury
not yet stabilized, burns, open wounds, infection or recent thoracic skin grafts,
osteoporosis, osteomyelitis, coagulopathy, rib fracture, lung contusion, distended
abdomen, and chest wall pain (353, 388).
Mechanical Insufflation-Exsufflation (MI-E).
Mechanical insufflator-exsufflators (Cough Assisttm, Philips Respironics, Inc) deliver
deep insufflations (at positive pressures of 30 to 60cmH2O) followed immediately by
deep exsufflations (at negative pressures of -30 to -60cmH2O). The insufflation and
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
82 Miguel Ramalho do Souto Gonçalves

exsufflation pressures and delivery times are independently adjustable(55). With an
inspiratory time of 2 seconds and an expiratory time of 3 seconds, there exists a very
good correlation between the pressures used and the flows obtained(56) (394).
Except after a meal, an abdominal thrust is applied in conjunction with the exsufflation
(MAC) (376). Mechanical in-exsufflation can be provided via an oral-nasal mask a
simple mouthpiece, or via a translaryngeal or tracheostomy tube. When delivered via
the latter, the cuff, when present, should be inflated (395).
MI-E applied with an oronasal mask can generate CPFs greater than 2.7 L/s in motor
neuron disease patients, with the exception of those with very acute bulbar dysfunction
(396), in whom there exists great instability of the upper airways (60). If, in normal
subjects, the sudden application of negative pressure at this level produces reflex
activation of the genioglossus to maintain permeability, in those patients with
diminished strength and speed of the pharyngeal muscles there will be obstruction
during the expiratory phase (363).
The Cough AssistTM can be manually or automatically cycled. Manual cycling
facilitates care giver-patient coordination of inspiration and expiration with insufflation
and exsufflation, but it requires hands to deliver an abdominal thrust, to hold the mask
on the patient, and to cycle the machine. One treatment consists of about five cycles of
MI-E or MAC followed by a short period of normal breathing or ventilator use to avoid
hyperventilation(62). Insufflation and exsufflation pressures are almost always from
+35 to +60 cm H2O to -35 to -60 cm H2O. Most patients use 35 to 45 cm H2O
pressures for insufflations and exsufflations. In experimental models, +40 to -40 cm
H2O pressures have been shown to provide maximum forced deflation VCs and flows
(365, 375, 394). Multiple treatments are given in one sitting until no further secretions
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 83

are expulsed and any secretion or mucus induced dessaturations are reversed. Use can
be required as frequently as every few minutes around the clock during chest
infections(58). Although no medications are usually required for effective MI-E in
neuromuscular ventilator users, liquefaction of sputum using heated aerosol treatments
may facilitate exsufflation when secretions are inspissated.
The use of MI-E via the upper airway can be effective for children as young as 11
months of age. Patients this young can become accustomed to MI-E and permit its
effective use by not crying or closing their glottises. Between 2 1/2 and 5 years of age
most children become able to cooperate and cough on queue with MI-E. Exsufflation
timed abdominal thrusts are also used for infants (397-398).
Whether via the upper airway or via indwelling airway tubes, routine airway suctioning
misses the left main stem bronchus about 90% of the time. MI-E, on the other hand,
provides the same exsufflation flows in both left and right airways without the
discomfort or airway trauma of tracheal suctioning and it can be effective when
suctioning isn't. Patients almost invariably prefer MI-E to suctioning for comfort and
effectiveness and they find it less tiring (399-400).
When mucous plugs are eliminated in acute episodes in ventilated neuromuscular
patients, MI-E may attain 300% improvement in VC as well as normalization of oxygen
saturation (401). Contraindications of the technique include previous barotrauma, the
existence of bullae, emphysema, or bronchial hyperreactivity (402). There continue to
be no publications contradicting the reports of effectiveness or describing significant
complications of MI-E. Even when used following abdominal surgery and following
extensive chest wall surgery no disruption of recently sutured wounds was noted (403-
404). Secondary effects, such as pneumothorax, aspiration, or coughing up blood are
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
84 Miguel Ramalho do Souto Gonçalves

reduced considerably by treating the mentioned contraindications. On the other hand,
gurgling noises and abdominal distension are rare and can be eliminated by lowering the
insufflation pressure. The significant increase of forced expiratory flows in periods
immediately following post-exsufflation indicates that MI-E does not provoke
obstruction of the airways. As patients with spinal shock can present bradycardias, MIE
should be carried out with cautious in them, with gradual increase in pressures or
premedication with anticholinergics (405). In patients with very low VC who have not
previously received maximum insufflations, the use of high pressures may cause
thoracic muscle discomfort; thus, progressive increase is also indicated.
The use of MI-E has been demonstrated to be very important in extubating NMD
patients following general anesthesia despite their lack of any breathing tolerance, and
to manage them with noninvasive ventilation (355-356, 373). It has also permitted to
avoid intubation or to quickly extubate NMD patients in acute ventilatory failure with
no breathing tolerance and profuse airway secretions due to intercurrent chest infections
(27, 406-407). MI-E in a protocol with manually assisted coughing, oximetry feedback,
and home use of noninvasive IPPV was shown to effectively decrease hospitalizations
and respiratory complications and mortality for patients with NMD (354, 408).
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 85

PURPOSE OF THE THESIS
Inspiratory and expiratory muscle aids are devices and techniques that involve the
manual or mechanical application of forces to the body or intermittent pressure changes
to the airway to assist inspiratory or expiratory muscle function. Noninvasive
ventilation (NIV) and mechanical assisted cough (MAC) are techniques that may have a
role in different phases of both acute and chronic respiratory failure. In fact, there is
sufficient evidence that support the physiological benefits of these techniques in aiding
both inspiratory (NIV) and expiratory muscle function (MAC) in different patient
populations.
Patients with impaired respiratory muscle function from different etiologies may be at
risk of developing ventilatory failure during an acute exacerbation or during the primary
disease progression in a chronic setting. Protocols and timing of NIV and MAC
application have to be adjusted according to the different clinical scenarios and
treatment goals should be based on a continuous level of care from acute to long term
management. In this patient population, primary treatment goals in acute care are
reversion of the episode of acute respiratory failure (ARF), avoid (when possible) or
minimize the time on invasive ventilation, prevent and reduce complications of
treatment and promote a safe hospital discharge to the community. In the chronic care
setting, the main treatment goals are to prevent complications with close follow up,
reduce hospitalizations due to ARF, prolong survival and enhance quality of life.
The main purpose of this thesis is to describe the efficacy of NIV and MAC in the
different “windows of opportunity” set to achieve specific goals from acute to chronic
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
86 Miguel Ramalho do Souto Gonçalves

care, and present new management and evaluation paradigms in patients with muscle
weakness from different etiologies. Methodological design of the thesis goals is
presented in Figure 16.
Figure 16: Methodological design of the thesis studies (1 to 10) according to the
different settings.
Acute Respiratory Failure
Mechanical ventilation using an artificial airway is probably the most frequently life-
saving procedure used in the management of critically ill patients with severe
respiratory failure(35). However, it is associated with multiple complications, primarily
increased risk of pneumonia(409) with a high mortality rate, but also generalized
myopathy, possibly related to the sedation or curarization necessary for invasive
mechanical ventilation(410). In the majority of cases, mechanical ventilation can be
withdrawn after resolution or significant improvement of the underlying indication for
mechanical ventilation. However, it is estimated that 20 to 30% of patients require
gradual withdrawal of ventilatory support, namely weaning(411).
4 5
10
3 2
1 6 7 8
9
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 87

A distinction must be made between dependence on the ventilator and an ongoing need
for endotracheal intubation. When there is no need for an artificial airway ,conventional
extubation attempts follow successful “spontaneous breathing trials (SBTs) and the
passing of ventilator weaning parameters that include respiratory rate less than 38 per
minute and a rapid shallow breathing index below 100 breaths/min/L (412). This
presupposes that ventilator weaning is mandatory before a patient can be safely
extubated, otherwise patients are extubated only after tracheotomy. However, even for
patients who satisfy weaning criteria and pass ventilator weaning trials, there is an
extubation failure rate of 10 to 20% (413). The reasons given for extubation failure
include lack of improvement in work of breathing, hypoxemia, respiratory acidosis,
retained secretions, and decreased consciousness (414).
The process of discontinuing mechanical ventilation may be a major challenge,
especially in patients with chronic respiratory disorders, in whom weaning is
particularly difficult (415). Patients that develop acute respiratory failure that could
result in prolonged invasive ventilation include COPD, spinal cord injury,
neuromuscular disease (NMD), chest wall disease, and primary central nervous system
disease.
The process of weaning from mechanical ventilation must balance the risk of
complications due to unnecessary delays in extubation with the risk of complications
due to early discontinuation and the need of reintubation(411). Patients who require
reintubation have been noted to have a significantly higher mortality rate than those
who are successfully extubated on the first attempt(416).
While studies have reported that NIV has been used in the emergency setting to avert
intubation (21, 29, 417), and to facilitate extubation and weaning in the critical care
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
88 Miguel Ramalho do Souto Gonçalves

setting (114, 153, 158) in patients with lung/airways diseases (primarily oxygenation
impairment) (155, 161, 418), the studies either report very few patients with primarily
ventilatory impairment (unable to sustain spontaneous breathing) due to neuromuscular
weakness i.e. 18 of 162 (155), 17 of 900 (413)) or they completely exclude these
patients when weaning is considered unlikely (357) or the risk of post-extubation failure
is considered high (160). This is true despite the fact that neither adequate ventilator
settings for full continuous noninvasive ventilatory support nor mechanically assisted
coughing (MAC) were used in any of the studies on adult patients (419). Some studies
do not even report the NIV settings (413).
Patients with pre-existing NMD are relatively infrequently in critical care (420), about 4
to 12.5% of cases (34, 156) (up to 25% in weaning centers) (421), and are seldom
included in randomized critical care controlled trials of NIV (422). On the other hand,
acquired critical care NMD is common yet often unrecognized (410, 423). Controlled
invasive mechanical ventilation can induce diaphragmatic dysfunction (424) and
becomes part of a positive feedback loop leading to respiratory muscle failure (425). In
multicenter prospective studies 25.3% of patients who underwent invasive mechanical
ventilation for more than 7 days developed acquired NMD (410). Risk factors include
malnutrition (423), corticosteroids (424), neuromuscular blocking agents (426),
aminoglycosides, hyperglycemia, sepsis (425, 427), and “prolonged” invasive
mechanical ventilation (428-429). These patients commonly fail extubation by
conventional approaches and are considered “unweanable” (188, 430-431).
Ventilatory insufficiency and impaired airway secretion clearance are common acute
care complications of NMDs and high level spinal cord injury patients (SCI) and can
lead to prolonged ventilation(415) with very difficult weaning (429, 432). Since the
extubation failure risk is very high in this patient population, they are also considered
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 89

“unweanable”(411, 431, 433). Standard invasive ventilatory management options such
as early intubation and tracheostomy for long term care have been described as
alternatives to minimize respiratory complications in these patients (434-437).
Although it might be presumed that self-directed adult unweanable muscle weakness
patients who have failed multiple ventilator weaning trials can cooperate with the use of
NIV and MAC, there are no critical care publications that have reported the use of
those methods to extubate them. We hypothesized that, since there is no chronic lung
disease in these totally ventilator dependent patients, and if at extubation the lungs are
healthy with SpO2>95% in ambient air, ventilation could be fully maintained
noninvasively even with no ventilatory autonomy (Study nr 1).
It has also been described that decannulation and conversion to NIV can facilitate
weaning in patients with no ventilator-free breathing ability(438), and that MAC can be
used for effective secretion clearance as an alternative to bronchoscopy to relieve
atelectasis and normalize Spo2.(358) Further, patients almost invariably prefer
noninvasive aids over tracheostomy for safety, convenience, appearance, comfort,
facilitating effect on speech, sleep, and swallowing, and general acceptability (439).
However, respiratory complications are highly prevalent in ASIA A SCI patients with
84% of patients with C1-C4 and 60% of those with C5-C7 injury levels present severe
ventilatory failure(440). Such patients are conventionally managed by translaryngeal
intubation and mechanical ventilatory support(441) and the overall incidence of
tracheostomy in these cases was between 81 and 83% (442-443). The number of
respiratory complications during this acute phase contributes significantly to both
hospital length of stay and costs(444).
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
90 Miguel Ramalho do Souto Gonçalves

Following the line of research of this thesis, we hypothesized that noninvasive methods
of assisted ventilation and coughing may facilitate both extubation and decannulation
with significant improvement on ventilatory dependence and pulmonary function in
totally ventilator dependent patients with high level SCI. We also questioned if early
intervention in extubation can produce better outcomes than late decannulation (study
nr 2)
It has been reported that conventional chest physical therapy for secretion management
does not increase the chances of weaning and extubation success (357). However,
critically ill patients may have normal mucociliary clearance but ineffective cough peak
flows (CPF) which itself has been associated with extubation failure (37, 358) due to
airway secretion accumulation (37, 358) but very few studies reported CPF at
extubation. (37, 445)
Early extubation, coupled with the use of noninvasive ventilatory support has been used
effectively in several critical ill populations to facilitate weaning(20, 114, 155), improve
survival(161), decrease the incidence of ventilator-associated pneumonia(103, 153) and
reduce ICU length of stay(153, 161). However there is a higher risk of NIV failure
when applied in patients that develop ARF after extubation and the evidence that
supports its application is controversial (159-160, 446).
Despite a great interest in this field, it is still not clear the role of impaired airway
secretion clearance on the outcome of post-extubation respiratory failure in critical ill
ventilator dependent patient treated with non-invasive ventilation. Airway clearance
may be impaired in disorders associated with abnormal cough mechanics, altered mucus
rheology, altered mucociliary clearance, or structural airway defects. A variety of
interventions are used to enhance airway clearance with the goal of improving lung
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 91

mechanics and gas exchange, and preventing atelectasis and infection (351). We
hypothesized that the inclusion in a weaning protocol of mechanical insufflation-
exsufflation (MI-E) device for mechanical cough assistance may prevent the
development of respiratory failure after extubation in patients that successfully pass the
SBT and may reduce the incidence of NIV failure in those who develop ARF after
extubation. We also questioned if this technique has a role in reducing both re-
intubation rates and ICU length of stay (study nr 3).
Considering the incidence of mortality and respiratory morbidity in “high risk” critical
ill patients with severe inspiratory and expiratory muscle weakness managed by
standard ventilatory invasive techniques, we question if NIV coupled with MAC is
efficient in treating post-extubation respiratory failure and can facilitate both extubation
and decannulation in “unweanable” patients with significant improvement on
ventilatory dependence and pulmonary function
Questions:
- Question 1 – Is it possible to extubate and prevent post-extubation failure in
cooperative, totally ventilator dependent (unweanable) neuromuscular weakness
patients without tracheotomy using a protocol that include full, continuous NIV and
MAC? Answer described in study nr 1.
- Question 2 – Can totally ventilator dependent neuromuscular weakness patients
wean from ventilatory support, with significant improvement in Vital Capacity
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
92 Miguel Ramalho do Souto Gonçalves

(VC) and CPF after being submitted to an extubation protocol that include full,
continuous NIV and MAC. Answer described in study nr 1
- Question 3 – Is it possible to extubate and decanulate totally ventilator dependent
ASIA A SCI patients with a protocol that include full and continuous NIV and
MAC? Answer described in study nr 2
- Question 4- Does a protocol that include full and continuous NIV and MAC
produce better outcomes when applied during extubation rather than in
decannulation of ASIA A SCI patients ? Answer described in study nr 2
- Question 5 – Can totally ventilator dependent ASIA A SCI patients wean from
ventilatory support, with significant improvement in Vital Capacity (VC) and CPF
after being submitted to an extubation or a decannulation protocol that include full,
continuous NIV and MAC. Answer described in study nr 2
- Question 6 - Is the inclusion of MI-E in weaning protocol effective in reducing
NIV failure and re-intubation rates in patients that successfully pass SBT´s, but
develop respiratory failure after extubation? Does it have any impact on ICU length
of stay? Answer described in study nr 3
Chronic Respiratory Failure
Chronic respiratory patients with primarily ventilatory impairment such as NMD and
other restrictive syndromes benefit significantly with the use of long term noninvasive
ventilation (8, 15, 447-449). In this line of research, noninvasive ventilation (NIV)
refers only to devices aimed to assist inspiratory muscles (CPAP excluded) through bi-
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 93

level positive airway pressure ventilation or volume cycled intermittent positive
pressure ventilation.
Standardized protocols for managing and monitoring NIV at home are lacking, and
depend on organizational, administrative and funding structures not only between
countries but often within different regions of the same country (248). Before starting a
patient on long term NIV(450), it is essential to ask three main questions: 1) Does the
patient have a disease known to cause ventilatory failure? 2) Does the patient have
symptoms suggesting hypoventilation? 3) Does the patient have physiological
abnormalities confirming hypoventilation? (249).
Ventilatory insufficiency progresses insidiously in most of restrictive muscle weakness
patients and NIV typically relieves fatigue and other daytime symptoms of which
patients may have been unaware (309, 451-453). Every consensus statement reinforces
the importance of detecting symptoms of nocturnal hypoventilation (252, 256-259).
However, symptoms may be subtle due to the variability of patient sensitivity and
sometimes it is difficult for the patient to establish differences between fatigue,
dyspnea, and sleepiness. So, carefully designed questionnaires that assess symptoms
systematically may be very useful. Jackson et al (260) have described a pulmonary
symptom scale consisting of 14 questions, answered on a scale from 1-7. Others
evaluated by simple questionnaires the positive and negative effects of ventilation(261).
Although symptom questionnaire are insensitive in identifying patients with nocturnal
hypercapnic hypoventilation (260, 262) their systematic evaluation is useful in
evaluating response to NIV, as compliance to it is strongly correlated with patients
symptoms (263).
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
94 Miguel Ramalho do Souto Gonçalves

Since 1993, different consensus conferences and guidelines have proposed indications
for initiating ventilatory support in patients with chronic respiratory failure (252, 256-
259, 277, 345, 454). Initially, criteria for beginning ventilatory support have relied on
abnormal awake blood gases (PaO2< 60mmHg and PaCO2 ≥ 45mmHg) or significant
nocturnal desaturation (SpO2 below 90% for ≥ 20% recorded time) (345), then on
Forced Vital Capacity (FVC) impairment (under 50% of predicted (256) or under
1L(258)) or mouth pressures (maximum inspiratory pressure under 60cmH20(252)).
More recently more sensitive parameters have also being included and nocturnal
hypercapnia (transcutaneous CO2 of 50 mmHg for more than 50% of sleep time(258))
and Sniff nasal pressure (SNP under 40cmH20(259, 310)) may be better in assessing the
need for ventilatory support.
Vital Capacity (VC) is one of the most reproducible tests of lung function in restrictive
patients. Although it may not fall below normal limits until there is a 50% reduction in
muscle strength (267), its rate of decline has been shown to predict survival (268).
Although no consensus exist as to how often pulmonary function should be evaluated,
some authors propose that if VC is > 60% predicted it should be performed every 6
months while if under 60% every 3-4 months (269). Measurement of the VC in the
supine position gives and index of weakness of the diaphragm. A fall of more than 15%
indicates diaphragmatic dysfunction and correlates with complaints of orthopnea (270)
and a supine FVC under 75% was highly sensitive and specific of low
transdiaphragmatic pressure (271).
Bellemare and Grassino demonstrated a relationship between tension time index of the
diaphragm (TTIdi) and diaphragm endurance or limitation time (Tlim)(455). TTIdi
signals the extent to which diaphragm action can continue unabated or fail due to
muscular fatigue. However, because of its invasive nature and the difficulties in its
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 95

interpretation in seriously compromised patients, TTIdi is neither practical for the acute
care nor for outpatient settings.
The TTIdi is the product of the fraction of time that the diaphragm spends in contraction
(Ti/Ttot) and the ratio of the tension generated at each contraction (Pdi) to the maximal
Pdi that can be achieved voluntarily during a near isometric contraction (PdiMax).
Bellemare and Grassino reported that this index correlates significantly with extent of
respiratory impairment in lung disease patients(456).
We hypothesized that the ratio of tidal volume to vital capacity (Vt/VC) could substitute
for the Pdi/PdiMax in the Bellemare and Grassino equation. A validated noninvasive
measurement of TTIdi (457) in NMD patients could play a role in the decision to
initiate ventilator use (458). We realized if this index would probably better correlate
with symptomatic inspiratory muscle dysfunction if it reflects ongoing inspiratory
muscle action rather than effort over only one breath cycle. Thus we proposed a
Ventilator Requirment Index (VRI) were we multiplied the Ti/Ttot x Vt/VC x
respiratory rate (RR), to determine whether this index could distinguish patients with
NMDs with various levels of inspiratory muscle dysfunction and need for ventilator use
and if such an index could add to the diagnostic efficiency of simple VC measurement
in determining need for ventilator use (study nr 4).
The main cause of morbidity and mortality in patients with NMD is respiratory failure
and, in particular, cough dysfunction (447, 459-460). Inspiratory, expiratory, and bulbar
innervated musculature are required for effective coughing (461-462). Normal pre-
cough inspiration is to 85-90% of total lung capacity(463). Thus, cough flows are
diminished for patients who have VCs less than 1500 ml (460).
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
96 Miguel Ramalho do Souto Gonçalves

Both, peak expiratory flows (PEF) and cough peak flows (CPF) have been described as
useful clinical parameters of respiratory muscle function (364).“Dart flows” (DF) are
generated by creating pressure behind the lips and tongue with the mouth closed. As
the lips open in a maneuver like spitting or projecting a dart through a narrow tube, the
flows can also be measured by peak flow meter. These flows can be confused with PEF
and CPF and cause the latter to be overestimated. They are largely a function of the
ability to seal the lips and control the tongue and buccal muscles.
To optimize CPF for patients with low VCs, particularly for those with VCs below 1000
ml, coughing needs to be preceded by the delivery of maximal insufflations or
maximum air stacking(462). The delivered air should be to the maximum insufflation
capacity (MIC)(362) which, even when not greater than 1500 ml, can greatly increase
the pressure of the lung's recoil once the glottis is opened during the cough(364). This
can dramatically increase CPF even without applying an abdominal thrust to manually
augment the flows(464).
Expiratory muscles can be manually assisted by providing thoracoabdominal
thrusts(465). The combination of applying an abdominal thrust to a maximally inflated
lung is an assisted cough (54, 464, 466). While unassisted cough flows depend on
inspiratory, expiratory, and bulbar-innervated musculature, air stacking ability and,
therefore, assisted cough flows depend only on glottic control or on bulbar-innervated
muscle function alone. Thus, the greater the difference between the MIC and the VC
and the difference between assisted and unassisted cough peak flows (CPF), the greater
is bulbar-innervated muscle function by comparison to inspiratory muscle function(10,
396, 460). Patients who cannot close the glottis cannot air stack. They may “huff” but
cannot cough. CPF better reflect the capacity to expulse debris from the airways than do
peak expiratory flows (PEF) which occur without glottic closure (461).
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 97

There are no standard normal values for CPF or DF but PEF range from 500 to 700
L/min for men and from 380 to 500 L/min for women, and from 150 to 840 L/sec for
children and adolescents with variations due to age, race, gender, and height(467).
We proposed to describe and compare the CPF, PEF, and DF in NMD patients, whose
VCs were less than normal, and question if they correlate with VC or MIC, to consider
their use in the evaluation of the respiratory muscles and to justify the indication of
inspiratory and expiratory muscle aids (study nr 5).
As VC decreases markedly, the largest breath that one can take can only expand a small
portion of the lungs. Use of incentive spirometry or deep breathing can expand the
lungs no greater than the VC. Although possibly useful, manual chest wall stretching
and rocking the pelvis onto the chest to decrease costovertebral tightness has not been
shown to increase lung volumes. As has been recognized since at least 1952, this can
only be achieved by air stacking, by providing deep insufflations (via the upper airway
or by "sighs" for patients using invasive mechanical ventilation), or by nocturnal
noninvasive ventilation for patients who can not cooperate with air stacking or
insufflation therapy(468).
A patient's maximum insufflation capacity (MIC) is determined by measuring
spirometrically the largest volume of air that a patient can hold with a closed
glottis(362). The patient air stacks via a mouth piece consecutively delivered volumes
from a volume-cycled ventilator or a manual resuscitator. This is performed multiple
times three times daily. The patient stacks the consecutively delivered volumes with a
closed glottis until the lungs are maximally expanded(469). If the lips or cheeks are too
weak to permit air stacking, stacking is done via a nasal interface or lipseal.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
98 Miguel Ramalho do Souto Gonçalves

The extent to which the MIC is greater than the VC predicts the capacity of the patient
to be maintained by noninvasive rather than tracheostomy ventilatory support. This is
because the MIC /VC difference, like the extent of assisted CPF, is a function of bulbar
muscle integrity (470-471).
With complete loss of glottic closure, MIC no longer exceeds VC; the NMD patient can
no longer air stack or cough, and both the glottis, and many bulbar-innervated muscles,
are extremely impaired. In this case, lung insufflation can only be provided by
bypassing glottic function. This can be done by using a manual resuscitator with a
closed expiratory valve mimicking glottic closure and insufflate to the approached
predicted maximum insufflation.
We proposed that the maximum passive lung insufflation volume achieved in this
manner is defined as the lung insufflation capacity (LIC). We questioned if passively
insufflating the patient to the maximum LIC could be efficient for chest wall ROM
when bulbar muscle impairment is present We hypothesized that LIC could be
compared with MIC (lung inflation by air stacking) and with vital capacity (VC) and
that relationships between these variables could correlate with glottic function and CPF
(study nr 6).
Questions:
- Question 7 – Can the measurement of a new proposed ventilator requirement index
(VRI) distinguish patients with NMDs according to various levels of inspiratory
muscle dysfunction and need for ventilator use? Answer described in study nr 4
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 99

- Question 8 – Does the VRI add new findings to the diagnostic efficiency of simple
VC measurement for determining the need and the extent for ventilator use?
Answer described in study nr 4.
- Question 8 – Can a simulation expiratory flow maneuver like the DF overestimate
PEF and CPF in NMD patients? Answer described in study nr 5.
- Question 9 – Is there any correlation between CPF and PEF with VC or MIC, for
evaluation of bulbar muscle function and how can it influence the efficacy of
inspiratory and expiratory muscle aids? Answer described in study nr 5.
- Question 10 – Will lung volumes be significantly greater by passive insufflation
than by air stacking, especially in patients with severe bulbar innervated muscle
dysfunction, and will both LIC and MIC significantly exceed VC and increase
CPF? Answer described in study nr 6.
- Question 11 – Will LIC-MIC correlate inversely with MIC-VC and, therefore,
correlate inversely with glottic integrity? Answer described in study nr 6.
- Question 12 – Can LIC and MIC increase with practice were the greatest increases
will be for the most severely affected patients, that is, with the lowest VC? Answer
described in study nr 6.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
100 Miguel Ramalho do Souto Gonçalves

Home mechanical ventilation
Preparing the patient for discharge on home mechanical ventilation requires planning.
Most respiratory patients are discharged home with a simple bi-level device for
nocturnal use only. Those patients have normally sleep disorder breathing defined as
nocturnal hypoventilation during sleep due to several causes that include either
obstructive lung/airways disease or mild to moderate restrictive syndromes(472).
However there are an increasing number of individuals on HMV that are continuous
ventilator dependent through either noninvasive interfaces or tracheostomy. Those
patients normally have severe muscle weakness associated in the majority of cases to
NMD that may include patients with severe bulbar muscle dysfunction, such as ALS.
Training, organizing and funding appropriate equipment and resources for such
individuals is more complex and time consuming(49, 473-476).
In patients with neuromuscular disorders with severe ventilatory impairment, instigating
a secretion-management protocol is an essential component of any home management
programme(46), and this needs to be carried out on a regular basis. Approaches to
preventing peripheral airway secretion retention at home for patients with NMD include
the use of medications to liquefy secretions and manual techniques of mucus
mobilization to transport mucus from the peripheral to the central airways from where it
can more easily be eliminated. As already described in the line of research of this thesis,
an optimal insufflation to the MIC followed by an abdominal thrust provides the
greatest increase in CPF in NMD patients with intact bulbar function. When these
techniques alone are no longer effective, MAC defined as the use of mechanical
insufflation-exsufflation (MI-E) (62) with an exsufflation-timed abdominal thrust can be
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 101

applied at home both through a oronasal interface or through a tracheostomy tube with
cuff inflated(61).
An optimal home management of both ventilatory failure and profuse secretion
retention should be guided by an oximetry feedback protocol. Since supplemental
oxygen is avoided for NMD patients, once artifact is ruled out, SpO2 below 95% is due
to one of three causes: hypercapnia (hypoventilation), airway encumberment
(secretions), and if these are not managed properly, intrinsic lung disease, usually gross
atelectasis or pneumonia(127). This protocol consists of using an oximeter for feedback
to maintain SpO2 greater than 94% by maintaining effective alveolar ventilation and
airway secretion elimination. However, application of these techniques and protocols at
home require skill and coordination if they are to be performed effectively(63).
Therefore, not only do the techniques need to be taught initially, periodic assessment of
the caregivers skills in performing the technique is required.
Despite increasing experience and published results concerning this technique as a first-
line intervention for hospitalized patients with ALS and others with neuromuscular
diseases (58-59, 61, 127, 246, 401, 477-478), there are limited data related to its
indications for home care use. We aimed at describing the indications of home MAC
use with oximetry feedback and questioned its safety and compliance in NMD patients,
under continuous mechanical ventilation either through noninvasive or tracheostomy
ventilation, when centred in non-professional caregivers, with the support of a trained
health care professional in a home on-call regime (study nr 7).
Particularly in patients with Amyotrophic Lateral Sclerosis (ALS), secretion
encumbrance episodes often result in acute respiratory failure especially during acute
chest infections(401, 460, 479). Moreover, in case of severe bulbar-innervated muscle
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
102 Miguel Ramalho do Souto Gonçalves

dysfunction with inability to protect the airways both manual assisted coughing with
lung insufflation and MAC may be ineffective(10, 60, 480) and result in hospitalization
and need for tracheotomy(481).
Organization of home care programs that include the use of MAC in this population
with severe ventilatory impairment requires more study. While effective when
continuously available at home(63, 127), expense can be mitigated by on-demand rather
than continuous access of MAC if on-demand use can be demonstrated to be effective.
In Europe, home respiratory care is often inadequate because home care companies
provide only equipment, not assistance, instruction, or expertise for which the patient
must depend on emergency services(476), and there is great burden on caregivers(482).
Thus, hospitalization rates and lengths of stay in this patient population are high,
especially when ARF and intubation result in tracheotomy. It has been reported that the
mean acute hospitalization for patients undergoing tracheotomy is 72 days, mostly in
intensive care(483) at a very high cost per day.
To help reduce hospitalizations costs and establish an optimal MI-E provision regimen
at home, we studied a telephone accessed integrated care (TAIC)(53) program with
oximetry feedback, that provided equipment and professional home care services on an
“as needed basis” to treat clinical exacerbations due to secretion encumbrance and
related respiratory problems in ALS patients (study nr 8).
For the great majority of NMD patients, up to continuous use of noninvasive ventilation
(NIV) can maintain quality of life,(484) and markedly prolong a survival(10) that is,
nevertheless, punctuated by respiratory tract infections (RTIs). Intercurrent RTIs are the
main cause of morbidity, prolonged hospitalizations, acute respiratory failure (ARF),
intensive care admissions, and mortality (47, 63, 127, 460). When MAC is used for
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 103

airway secretion clearance, multiple treatments are given until no further secretions are
expulsed and any secretion or mucus induced O2 desaturations are reversed. Use can be
required as frequently as every few minutes around-the-clock during intercurrent
RTIs(58, 127, 485). Because respiratory muscles are weakened and bronchial secretions
are profuse during RTI´s patients often need to NIV continuously at these times both to
maintain alveolar ventilation and for air stacking to increase CPF (246, 363). If, when
using NIV at adequate delivered volumes the SpO2 is not above 94%, the desaturation is
not due to hypoventilation but to mucus accumulation especially during chest infections
and ARF(27, 47).
In hospital application, MAC has been described an effective first-line intervention for
NMD patients with ARF,(61, 246, 401, 478, 486-487). However, similar immediate
effects of this technique when applied at home during ARF have not been widely
explored. We hypothesized that MAC when applied at home, according to previous
protocols included in this thesis, can be efficient in treating NMD patients with acute
exacerbations due to secretion encumbrance. We questioned if MAC could normalize
SpO2 in time to avoid hospitalizations and reduce the number of deep airway suctions
in patients under continuous ventilatory support either by NIV or tracheostomy (study
nr 9).
Respiratory insufficiency appears in the course of NMD patients first during sleep and
then at a later stage during the day. Nocturnal only NIV produces 24-h effective blood-
gas improvement and symptom control for several years(15). However, in end-stage
respiratory muscle failure patients such as Duchenne muscular dystrophy (DMD),
amyotrophic lateral sclerosis (ALS) and spinal muscular atrophy type 1 (SMA 1),
nocturnal NIV needs to be progressively extended during the day as increasing
ventilatory dependency develops(11, 16, 447, 488-489). Mouthpiece intermittent
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
104 Miguel Ramalho do Souto Gonçalves

positive pressure ventilation (IPPV) is the most important method of daytime
ventilatory support for patients who need ventilatory support continuously since
continuous NIV with a nasal or oronasal mask may create skin breakdown or may even
interfere with the patient’s social activity (87, 490-491).
Although mouthpiece IPPV is being used for ventilatory support since 1953 (42) very
few studies reported its use for long-term management(1, 87, 90, 491-492). Since
ventilatory support delivered noninvasively is the single most import inspiratory muscle
aid in patients with NMD routine evaluations are recommended to predict its
application and monitor its efficacy both for nocturnal only and continuous use(9).
Although nocturnal only NIV can benefit mildly affected patients, instead of increasing
the spans or switching to the use of volume-cycled ventilators for daytime mouthpiece
IPPV, when low span pressure assistance is no longer adequate and ventilator
dependence progresses to daytime use, clinicians conventionally recommend
tracheotomy(15, 493-496).
For the final work of this thesis and to conclude this line of research, we proposed to
analyse the historical evolution of practice regarding the use of noninvasive mechanical
ventilation (NIV) and complementary interventions for long-term full-time noninvasive
ventilatory support of patients with neuromuscular diseases (NMDs) with primary focus
on the three most common and severe disorders, that is, Duchenne muscular dystrophy
(DMD), amyotrophic lateral sclerosis (ALS), and spinal muscular atrophy type 1 (SMA
1). To reinforce the argument that noninvasive alternatives for ventilatory support and
secretion management are feasible and efficient, we aimed to analyze data from
different international centers that provide continuous NIV for this patient population as
an alternative to tracheostomy to prolong survival and develop conclusions and
recommendations that may permit its widespread use (study nr 10).
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 105

.
Questions
- Question 13 – Is home based MAC with oximetry feedback effective and can it be
safely applied by trained non professional caregivers in continuous ventilator
dependent NMD patients, according to specific indications? Answer described in
study nr 7
- Question 14 – What is the frequency use of home MAC in NMD patients? Do
patients under tracheostomy ventilation used it more than patients under NIV?
Answer described in study nr 7
- Question 15 – Is a telephone accessed integrated care, that include on-demand
consult and MI-E device rapid access, efficient and feasible for ALS patients?
Answer described in study nr 8
- Question 16 – Is a home on-demand MAC program cost effective and can it
produce significant cost savings when compared to continuous home MAC
prescription in ALS patients? Answer described in study nr 8.
- Question 17 – Can home MAC with oximetry feed-back be efficient in reverting
O2 desaturations related to secretion encumbrance during an acute exacerbation in
NMD patients under continuous ventilatory support either by NIV or tracheostomy?
Answer described in study nr 9.
- Question 18 – Are the effects of home MAC sufficient to avoid hospitalizations for
ARF episodes related to secretion encumbrance in NMD patients under continuous
ventilatory support either by NIV or tracheostomy? Answer described in study nr
9.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
106 Miguel Ramalho do Souto Gonçalves

- Question 19 – During the last two decades, has there been an evolution of practice,
regarding the recommendations of continuous full time NIV and MAC for patients
with NMD? Answer described in study nr 10.
- Question 20 – What are the outcomes from international centers that provide
continuous full time NIV and MAC for patients with NMD? Answer described in
study nr 10.
Analyzing the body of works that support the line of research of this thesis, our main
goal was to achieve a continuum of care for patients with respiratory muscle weakness,
that, due to their severe ventilatory impairment, can benefit either in acute or chronic
settings, from specific evaluation protocols and management paradigms that include
NIV for ventilatory assistance and MAC for secretion management.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 107

Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
108 Miguel Ramalho do Souto Gonçalves

Study 1
Extubation of Patients with Neuromuscular Weakness:
A New Management Paradigm
John R. Bach, Miguel R. Gonçalves, Irram Hamandi, João Carlos Winck
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 109

Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
110 Miguel Ramalho do Souto Gonçalves

DOI 10.1378/chest.09-2144 2010;137;1033-1039; Prepublished online December 29, 2009;Chest
Carlos WinckJohn Robert Bach, Miguel R. Gonçalves, Irram Hamdani and Joao Weakness : A New Management ParadigmExtubation of Patients With Neuromuscular
http://chestjournal.chestpubs.org/content/137/5/1033.full.htmlservices can be found online on the World Wide Web at: The online version of this article, along with updated information and
ISSN:0012-3692)http://chestjournal.chestpubs.org/site/misc/reprints.xhtml(
of the copyright holder.may be reproduced or distributed without the prior written permission Northbrook, IL 60062. All rights reserved. No part of this article or PDFby the American College of Chest Physicians, 3300 Dundee Road,
2010Physicians. It has been published monthly since 1935. Copyright is the official journal of the American College of ChestCHEST
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 111

CHEST Original ResearchCRITICAL CARE MEDICINE
www.chestpubs.org CHEST / 137 / 5 / MAY, 2010 1033
Conventional extubation attempts follow successful “spontaneous breathing trials” (SBTs) and the
passing of ventilator weaning parameters, 1 otherwise patients undergo tracheotomy. Patients are often extubated to supplemental oxygen and bilevel positive airway pressure (PAP), but settings are infrequently reported,2 and extubation studies report very few if any patients with neuromuscular disease (NMD) (eg, 18 of 162, 3 17 of 900 4 ) and completely exclude unweanable patients. 5-7
Patients with preexisting NMD make up only 4% to 12.5% of cases in critical care, 8-10 but about 25%
in weaning centers. 11 While acquired critical care myopathy (CCM) is common, it is an often unrecog-nized12,13 cause of extubation failure by conventional approaches.14-16
There are no guidelines for extubating unweanable patients with NMD and CCM. Many are dependent on noninvasive mechanical ventilation (NIV) with no autonomous breathing ability for years before being intubated, and they refuse tracheotomy. 17-20 Further, these patients can have ineffective cough peak fl ows (CPFs), which can result in extubation failure due to airway secretion accumulation, 21-24 but very few studies
Background: Successful extubation conventionally necessitates the passing of spontaneous breath-ing trials (SBTs) and ventilator weaning parameters. We report successful extubation of patients with neuromuscular disease (NMD) and weakness who could not pass them . Methods: NMD-specifi c extubation criteria and a new extubation protocol were developed. Data were collected on 157 consecutive “unweanable” patients, including 83 transferred from other hospitals who refused tracheostomies. They could not pass the SBTs before or after extubation. Once the pulse oxyhemoglobin saturation (Sp o 2) was maintained at � 95% in ambient air, patients were extubated to full noninvasive mechanical ventilation (NIV) support and aggressive mechani-cally assisted coughing (MAC). Rather than oxygen, NIV and MAC were used to maintain or return the Sp o 2 to � 95%. Extubation success was defi ned as not requiring reintubation during the hospitalization and was considered as a function of diagnosis, preintubation NIV experience, and vital capacity and assisted cough peak fl ows (CPF) at extubation. Results: Before hospitalization 96 (61%) patients had no experience with NIV, 41 (26%) used it , 24 h per day, and 20 (13%) were continuously NIV dependent. The fi rst-attempt protocol extubation success rate was 95% (149 patients). All 98 extubation attempts on patients with assisted CPF� 160 L/m were successful. The dependence on continuous NIV and the duration of depen-dence prior to intubation correlated with extubation success ( P , .005). Six of eight patients who initially failed extubation succeeded on subsequent attempts, so only two with no measurable assisted CPF underwent tracheotomy. Conclusions: Continuous volume-cycled NIV via oral interfaces and masks and MAC with oxime-try feedback in ambient air can permit safe extubation of unweanable patients with NMD. CHEST 2010; 137(5):1033–1039
Abbreviations: ALS 5 amyotrophic lateral sclerosis; CCM 5 critical care myopathy; CPF 5 cough peak fl ows; IPPV 5
intermittent positive pressure ventilation; MAC 5 mechanically assisted coughing; NIV 5 noninvasive mechanical ventila-tion; NMD 5 neuromuscular disease; PAP 5 positive airway pressure; SBT 5 spontaneous breathing trial; SMA 1 5 spinal muscular atrophy type 1; S p o 2 5 pulse oxyhemoglobin saturation; VC 5 vital capacity
Extubation of Patients With Neuromuscular Weakness
A New Management Paradigm
John Robert Bach , MD ; Miguel R. Gonçalves , PT ; Irram Hamdani , MD ; and Joao Carlos Winck , MD , PhD
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
112 Miguel Ramalho do Souto Gonçalves

1034 Original Research
a CPF , 160 L/m were offered extubation if acknowledging that three extubation failures would necessitate tracheotomy. Other, at least temporary, exclusion criteria were medical instability, inadequate cooperation, and imminent surgery. 20,35
Protocol
While intubated, sufficient ventilatory support was used to maintain normocapnia and normal respiratory rates. MAC (CoughAssist; Respironics, Inc.; Murrysville, PA) was used at 40 to 2 40 cm H 2 O or greater to rapidly achieve clinically full chest expansion to clinically complete emptying of the lungs, with exsuffl ation-timed abdominal thrusts. The MAC sessions were up to every 20 min to maintain or return the pulse oxyhemoglobin saturation ( S p o
2 ) to � 95% in ambient air. Tracheotomy would
have been recommended if the Table 1 criteria could not be met within 2 weeks of transfer.
Once the Table 1 criteria were met, the orogastric or nasogas-tric tube was removed to facilitate postextubation nasal NIV. The patient was then extubated directly to NIV on assist/control of 800 to 1,500 mL, at a rate of 10 to 14 min in ambient air. Pressure control of at least 18 cm H 2 O was used if abdominal distension developed. The NIV was provided via a combination of nasal, oro-nasal, and mouthpiece interfaces. 36 Assisted CPF and CPF obtained by abdominal thrust following “air stacking” were measured within 3 h as the patient received full volume-cycled NIV support. Patients kept 15-mm angled mouthpieces accessible ( Fig 1 ), and weaned themselves, when possible, by taking fewer and fewer IPPVs as tolerated. Diurnal nasal IPPV was used for those who could not secure the mouthpiece. Patients took as much of the delivered vol-umes as desired. They used nasal or oronasal interfaces ( Figs 2, 3 ) for nighttime ventilation. For episodes of Sp o 2 , 95%, ventilator positive inspiratory pressure, interface or tubing air leakage, CO 2retention, ventilator settings, and MAC were considered.
Patients were taught to maximally expand their lungs by air stacking (retaining consecutive) ventilator delivered volumes to the largest volume the glottis could hold. 37 Once the lunges were air stacked, an abdominal thrust was provided to manually assist the cough, 29,37 and these assisted CPFs were measured. For patients using pressure-cycling, air stacking volumes were provided by manual resuscitator. The therapists, nurses, and in particular, the family and personal care attendants provided MAC via oro-nasal interfaces up to every 20 min until the Sp o 2 no longer dipped below 95% and the patients felt clear of secretions. In seven cases, the postextubation oral intake was considered unsafe, so open
have reported CPF 2,21 and none systematically used mechanically assisted coughing (mechanical insuffl ation-exsuffl ation with exsuffl ation-timed abdominal thrust) (MAC).4,24 There are no “ventilator weaning parameters” that address the ability to expel secretions. With success in decannulating unweanable patients with traumatic tetraplegia and others to continuous MAC and NIV, which includes noninvasive intermittent positive pressure ventilation (IPPV) and high-span bilevel PAP, 20,25-27 we used similar criteria to extubate unweanable patients with NMD and CCM and report the success rates.
Materials and Methods
The data were gathered in two centers, with 113 patients in New Jersey and 44 in Portugal, using the inclusion criteria described in Table 1 . The study was approved by the institutions’ review boards. All intubated patients were treated conventionally except for the use of MAC via the tube. Although virtually unknown in critical care, MAC has been instrumental in avoiding pneumonia, respiratory failure, and hospitalizations for NIV-dependent patients with NMD. 28-30 Vital capacities (VCs) (Wright Mark 3 spirometer; Ferraris Ltd; London, England) and unas-sisted and assisted CPFs (Access Peak Flowmeter; Health Scan Products Inc.; Cedar Grove, NJ) were measured within 12 months before intubation for the local patients (group 1). The other 83 intubated patients were transferred intubated from other hospitals after one to four failed extubation attempts (group 2) or after failing multiple SBTs (group 3).
VC was measured via the tube with the cuff infl ated following clearing of the airways by MAC just prior to extubation. Patients were ready for extubation and inclusion in this study only when all Table 1 criteria were satisfi ed and SBTs failed, as described. 31-33
Patients had to experience immediate distress, precipitous oxyhe-moglobin desaturation, and hypercapnia without stabilization before return to full ventilatory support both before and immediately postextubation. Local patients were considered to be group 1 because their greater experience with NIV and MAC could have affected outcomes. All transferred patients had been told that extubation and survival were not possible without tracheotomy.
We reported that the risk for extubation failure is high when assisted CPF cannot attain 160 L/m. 22 Considering that patients with advanced averbal bulbar amyotrophic lateral sclerosis (ALS) can rarely attain a CPF of 160 L/m 34,35 we generally did not accept such patients for transfer (exclusion criteria). Local patients with
Manuscript received September 11, 2009; revision accepted November 29, 2009. Affiliations: From the Department of Physical Medicine and Rehabilitation (Dr Bach ) and the Department of Medicine (Dr Hamdani), University of Medicine and Dentistry of New Jersey–the New Jersey Medical School, Newark, NJ; and the Lung Function and Ventilation Unit, Pulmonary Medicine Department, Intensive Care and Emergency Department (Mr Gonçalves ), and the Pulmonary Medicine Department (Dr Winck), Faculty of Medicine University, Hospital of S. João, Porto, Portugal. Correspondence to: John R. Bach, MD, Department of Physical Medicine and Rehabilitation, University Hospital B-403, 150 Bergen St, Newark, NJ 07103; e-mail: [email protected] © 2010 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians ( www.chestpubs.org/site/misc/reprints.xhtml ). DOI: 10.1378/chest.09-2144
Table 1— Extubation Criteria for Unweanable Ventilator-Dependent Patients
Afebrile and normal WBC countAged 4 y and olderNo ventilator-free breathing tolerance with 7-cm pressure support in ambient air on the basis of NMD or CCMVC, 20% of normalPaco2 � 40 mm Hg at peak inspiratory pressures , 35 cm H 2 O on full-setting assist/control mode at a rate of 10-13/minSpo2 � 95% for 12 h or more in ambient airAll oxyhemoglobin desaturations , 95% reversed by MAC and suctioning via translaryngeal tubeFully alert and cooperative, receiving no sedative medicationsChest radiograph abnormalities cleared or clearingAir leakage via upper airway suffi cient for vocalization upon cuff defl ation
CCM5 critical care myopathy; MAC 5 mechanically assisted coughing; NMD5 neuromuscular disease; S p o
25 pulse oxyhemoglobin saturation;
VC5 vital capacity.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 113

www.chestpubs.org CHEST / 137 / 5 / MAY, 2010 1035
in means were compared using the Wilcoxon rank test. A P value � .05 was considered signifi cant. Univariate comparisons of potential predictive factors for failure or success were run with the Fisher exact test for categorical variables and the Wilcoxon rank-sums test for continuous variables.
Results
The 157 patients, mean age 37 6 21 years, included 139 (89%) with NMD who were intubated for acute respiratory failure and compromise due to pneumo-nia and/or surgery and 18 patients with CCM (11%). The 74 local patients (group 1) were intubated at our institutions, and 83 others were intubated elsewhere. Demographic data are in Table 2 . VC and CPF data are in Table 3 . Twenty (13%) of the 157 patients had been continuously NIV dependent for 12.2 years (range5 1-47) before being intubated. Forty-one (26%) used NIV part-time ( , 24 h/d), and 96 (61%) used no NIV before intubation. All patients satisfi ed the Table 1 criteria in , 2 weeks.
Univariate comparisons of potential predictive fac-tors for extubation success yielded signifi cant differ-ences for continuous NIV use ( P , .0001) and for the duration of continuous NIV use and MAC use prior to intubation ( P5 .0038), indicating that experience with NIV and MAC was signifi cant in predicting suc-cess. Given only 15 failures in eight patients, it was not possible to run multivariable logistic regression models considering diagnosis, patient group, VC, and CPF.
Of 172 extubations on 157 patients, all 98 on patients with assisted CPF � 160 L/m were successful. Fifty-nine of 74 attempts (80%) on patients with CPF, 160 L/m were successful, including 52 of 60 (87%) at fi rst extubation. Six patients who initially failed, succeeded on second (four patients) and third (three patients) attempts. One with advanced bulbar ALS and one with facioscapulohumeral muscular dys-trophy, both with no measurable assisted CPF, failed a total of fi ve extubations and underwent tracheotomy. Only one of the eight who failed any extubation attempt had preintubation experience with NIV and MAC, but she and several others had suboptimal postextubation care provider support for aggressive MAC. She and eight patients with bulbar ALS with little residual bulbar-innervated muscle function required oro-nasal interfaces for a closed system of postextuba-tion NIV (Hybrid NE; Telefl ex Medical; Research Triangle Park, NC) ( Fig 2 ). All nine had gastrostomy tubes for total enteral nutrition. One lip-seal nocturnal NIV user for 28 years prior to intubation was extubated back to lip-seal NIV ( Fig 3 ). 36
Data on VC, CPF, and duration of NIV use as a function of postextubation weaning capacity are included in Table 4 . Weaning from full-time to part-time
modifi ed Stamm gastrostomies were performed under local anes-thesia using NIV, as in Figure 2, without complication. 38
Extubation was considered successful if the patient was dis-charged without reintubation. When reintubation was necessary, the patient was again extubated after achieving the Table 1 criteria. Multiple failures necessitated tracheotomy. Extubation success was considered as a function of diagnosis, patient group, VC, CPF, and preintubation NIV experience. VC was measured 3 to 6 months after extubation. The total days intubated were compared pre-transfer and posttransfer.
Statistical Analysis
Results are expressed as mean 6 SD. Statistical analyses were carried out using SPSS 12.0 (SPSS, Inc.; Chicago, IL). Differences
Figure 1. A 10-year-old girl with neurofi bromatosis status post-spinal cord tumor resection, extubated with a vital capacity (VC) of 180 mL and no ventilator-free breathing ability, using a 15-mm angled mouthpiece (Malincrodt-Puritan-Bennett; Pleasanton, CA) for ventilatory support. Current VC 380 mL and minimal ventilator-free breathing ability. The patient provided written consent for the use of this photograph.
Figure 2. A 20-year-old man with Duchenne muscular dystrophy transferred for extubation after failing three extubations over a 26-day period. He used a 15-mm angled mouthpiece, as in Figure 1 , for daytime ventilatory support and a lip-seal phalange with nasal prongs for nocturnal ventilatory support. His VC was 260 mL at extubation in October 2007 and 720 mL in July 2009. See Figure 1 legend for expansion of the abbreviation. The patient provided written consent for the use of this photograph.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
114 Miguel Ramalho do Souto Gonçalves

1036 Original Research
and 97 6 39 L/m (range 0-150), respectively. No clin-ically or radiographically apparent barotrauma was noted for any patients.
The 83 patients in groups 2 and 3 had been intu-bated for 11 6 9.1 days (range 5 1-80) before transfer and 2 6 1 days (range 5 1-11) on our units before extu-bation ( P , .005). Upon admission, on 21% fraction of inspired O 2 , 71 (85%) of the patients’ Sp o2 levels set-tled below 95%. Increased NIV support to normalize CO2 and especially MAC normalized Sp o2 generally within 24 to 48 h to satisfy a criterion for extubation.
The intensivists and respiratory therapists esti-mated that noninvasive treatment necessitated more time than invasive respiratory treatment. The extuba-tion itself required about 1.5 h for a specifi cally trained respiratory therapist to train the patients and care providers in NIV and MAC. In part because only one local nursing/rehabilitation facility would accept NIV users, all except one patient who had a tracheo-stomy were discharged home. One hundred thirty-one patients are alive using NIV ( Table 4 ). Nine patients (6%) died of cardiac failure, six (4%) from lung disease/respiratory failure, two (2%) with bulbar ALS died after tracheotomy from sepsis and decubiti, and nine (6%) died of unknown causes. Although offered, no patients accepted tracheotomy following successfulextubation.
Discussion
There are no extubation studies on continuously NIV-dependent patients with NMD. 6 A recent controlled
NIV took 3 to 21 days and was usually accomplished at home. As supine VC increased to approach 1,000 mL, we encouraged patients to sleep without NIV but with Sp o2 and end-tidal CO 2 monitoring, and when these remained stable for 2 weeks to discontinue NIV. The mean extubation VCs and assisted CPFs for the 29 patients � 18 years of age who were suc-cessfully extubated at fi rst attempt despite assisted CPF, 160 L/m were 245 6 114 mL (range 120-620)
Figure 3. A 59-year-old woman with spinal cord injury at birth and 31 years of dependence on a daytime mouthpiece and noctur-nal lip-seal (seen here) ventilation. She was extubated back to noninvasive mechanical ventilation despite a VC of 130 mL and no autonomous breathing ability and continued to use simple 15-mm angled-mouthpiece ventilation for daytime ventilatory support and lip-seal ventilation overnight with the nose clipped to prevent air leakage. Current VC is 340 mL. She is employed full-time as a psychologist. See Figure 1 legend for expansion of the abbreviation. The patient provided written consent for the use of this photograph.
Table 2— Demographic Data
Characteristics Group 1 a Group 2 b Group 3 c Total
Subjects, No. (%) 74 (47) 45 (29) 38 (24) 157 (100)Sex, No. (%) 52 male (70) 28 male (62) 17 male (45) 97 male (62)
22 female (30) 17 female (38) 21 female (55) 60 female (38)Diagnoses, No. (%) ICUMy, 15 (20) SMA, 10 (22) SMA, 10 (26) SMA, 25 (16)
SCI, 13 (18) MD, 9 (20) DMD, 9 (24) MD, 22 (14)ALS, 11 (15) DMD, 8 (18) MD, 5 (13) DMD, 20 (13)MG, 9 (12) MG, 6 (13) PPS, 5 (13) SCI, 17 (11)MD, 8 (11) PPS, 4 (9) oNMD, 4 (11) ALS, 16(10)
oNMD, 8 (11) oNMD, 4 (9) SCI, 3 (8) oNMD, 16 (10)SMA, 5 (7) ALS, 3 (7) ALS, 2 (5) ICUMy, 15 (10)DMD, 3 (4) SCI, 1 (2) . . . MG, 15 (10)PPS, 2 (3) . . . . . . PPS. 11 (7)
Use of NIV preintubation, No. (%) No NIV, 51 (69) No NIV, 24 (53) No NIV, 21 (55) No NIV, 96 (61)Cont, 10 (14) Cont, 7 (16) Cont, 3 (8) Cont, 20 (13)Noct, 13 (17) Noct, 14 (31) Noct, 14 (37) Noct, 41 (26)
ALS5 amyotrophic lateral sclerosis; Cont 5 continuous noninvasive ventilation; DMD 5 Duchenne muscular dystrophy; ICUMy 5 ICU-acquired neuromuscular disease; MD 5 muscular dystrophy; MG 5 myasthenia gravis; NIV 5 noninvasive ventilation; Noct 5 nocturnal noninvasive ventilation;oNMD5 other neuromuscular disease; PPS 5 postpolio syndrome; SCI 5 spinal cord injury; SMA 5 spinal muscular atrophy, including types 1, 2, and 3, and other neuromuscular disease.a Local patients.b Patients transferred after failing extubations in other institutions.c Patients transferred after failing multiple spontaneous breathing trials in other institutions.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 115

www.chestpubs.org CHEST / 137 / 5 / MAY, 2010 1037
acutely increase VC and Sp o2 .30,40,41 Our success stemmed not only from providing continuous full-setting NIV via a variety of interfaces but also from frequent and aggressive MAC to expel secretions and maintain or return Sp o2 . 95%.
In our earlier study of extubation/decannulation to NIV, considering the extent of need for NIV, age, VC, and maximum assisted CPF, only assisted CPF � 160 L/m predicted success in 62 extubation/decannulation attempts on 49 consecutive patients, including 34 with no ventilator-free breathing ability. 22 None of the 15 attempts on those with maximum CPF , 160 L/m succeeded, as opposed to an 87% fi rst-attempt extu-bation success rate in this study. The most likely rea-sons for the difference between then and now are: baseline Sp o2 criterion for extubation of 92% vs 95%, and thus the earlier patients had more residual airway secretions or lung disease at extubation; 5% vs 39% of patients with pre-extubation experience with NIV and MAC; less hospital staff experience with NIV and MAC; 50 of 62 patients were decanulated, not extu-bated; the patients were in various hospital locations; and MAC was used less often and without family involvement.22
The 87% fi rst-attempt extubation success rate on patients with maximum CPF , 160 L/m in this study is greater than the 82.4% (61 of 74) success rate reported for extubating NIV-dependent infants with spinal muscular atrophy type 1 (SMA 1), according to an almost identical protocol. 42 The difference may be the result of the ability of these patients, as opposed to babies, to cooperate with NIV and MAC. The SMA 1 infants may have also had more severe bulbar-innervatedmuscle dysfunction. Thus, while higher than those
postextubation respiratory failure study of 106 patients included only two with restrictive syndromes, but none with NMD, and all had passed SBTs. They were extubated to supplemental O 2 alone or in con-junction with bilevel PAP at spans up to 14 cm H 2 O, pressures inadequate for normal alveolar ventilation for our patients. 39 A metaanalysis of 12 extubation studies to bilevel PAP demonstrated decreased mortality, ventilator-associated pneumonia, length of stay, and resort to tracheotomy, but unweanable patients with NMD were uniformly excluded. 6 Eligi-bility for extubation was based on “readiness for weaning” and failure of SBTs after 30 min or more. 6
While this justifies extubation to NIV for patients who primarily have lung/airways disease with some autonomous breathing ability and for whom Spo2 . 90% may be acceptable with or without sup-plemental O 2 , our patients had no ability to sustain breathing before or after extubation with VCs as low as 0 mL. Thus, no control group extubation to O 2 or less than full NIV would be possible, ethical, or per-missible by any review board. While there are always limitations of uncontrolled studies when comparing two approaches, this was a study of only one approach to extubate patients not previously considered extu-batable. For our long-term NIV users, aspiration causing persistent Sp o2 , 95% despite continuous NIV and MAC in ambient air is the indication for tracheotomy.35
Besides hypoventilation, ineffective CPF have been associated with extubation failure. 21,22 MAC is essentially noninvasive suctioning via noninvasive or invasive interfaces. It can clear the left airways that are often not cleared by invasive suctioning and can
Table 3— Pulmonary Function
Characteristics Group 1 a Group 2 b Group 3 c Total
Subjects, n (%) 74 (47%) 45 (29) 37 (24%) 157Assisted CPF at extubation, L/min 1876 85 1626 86 1786 62 1776 77VC at extubation, mL 3556 171 2736 189 2956 155 3156 173VC 3-6 mo postextubation, mL 1,1216 748 7096 679 6176 412 8776 698
Intergroup differences were not statistically signifi cantly different except for postextubation VC, with that of group 1 being greater than for groups 2 and 3 ( P , .05). CPF 5 cough peak fl ows. See Table 1 for expansion of the other abbreviation.a Local patients.b Patients transferred after failing extubations in other institutions.c Patients transferred after failing multiple spontaneous breathing trials in other institutions.
Table 4— Postextubation Long-Term Noninvasive Ventilation Use for 155 Patients
Characteristics Weaned in 1 wk Weaned to Part-Time NIV Unweanable
Subjects, n 23 62 72VC at extubation, mL 4236 157 3446 152 2596 179CPF at extubation, L/min 2046 58 1796 73 1586 85VC 6 mo postextubation, mL 17976 683 8966 649 5026 353Duration ventilator use, mo (range) . . . 486 55 (1-204) 716 62 (1-228)
See Tables 1 and 3 for expansion of abbreviations.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
116 Miguel Ramalho do Souto Gonçalves

1038 Original Research
Dr Winck: oversaw the extubations on all of the Portuguese patients and added material to the introductory and “Discussion” sections of the manuscript. Financial /nonfi nancial disclosures: The authors have reported to CHEST the following confl icts of interest: Respironics, Inc, is the manufacturer of the CoughAssist, a device mentioned in this article. Dr Winck has been reimbursed by Respironics, Inc, for attending a sleep conference, received 4,500€ for organizing two postgraduate courses on noninvasive ventilation for Respironics, Inc, and received 500€ for lectures in a conference sponsored by Respironics, Inc. Mr Gonçalves received lecture honoraria of 4,000€ from Respironics, Inc, for two postgraduate courses on noninvasive ventilation. Drs Bach and Hamdani have reported no confl icts of interest exist with any companies/organizations whose products or services may be discussed in this article. Other contributions: We wish to thank Teresa Honrado, MD; Teresa Oliveira, MD; and Celeste Dias, MD, as well as the ICU medical, respiratory therapy, and nursing staffs of both institutions for their assistance and support in treating the patients.
References
1 . Boles JM , Bion J , Connors A , et al . Weaning from mechanical ventilation . Eur Respir J . 2007 ; 29 ( 5 ): 1033 - 1056 .
2 . Caples SM , Gay PC . Noninvasive positive pressure ventila-tion in the intensive care unit: a concise review . Crit Care Med . 2005 ; 33 ( 11 ): 2651 - 2658 .
3 . Ferrer M , Valencia M , Nicolas JM , Bernadich O , Badia JR , Torres A . Early noninvasive ventilation averts extubation fail-ure in patients at risk: a randomized trial. Am J Respir Crit Care Med. 2006 ;173(2):164-170.
4 . Frutos-Vivar F , Ferguson ND , Esteban A , et al . Risk factors for extubation failure in patients following a successful spon-taneous breathing trial . Chest . 2006 ; 130 ( 6 ): 1664 - 1671 .
5 . Templeton M , Palazzo MG . Chest physiotherapy prolongs duration of ventilation in the critically ill ventilated for more than 48 hours . Intensive Care Med . 2007 ; 33 ( 11 ): 1938 - 1945 .
6 . Burns KE , Adhikari NKJ , Keenan SP , Meade M . Use of non-invasive ventilation to wean critically ill adults off inva-sive ventilation: meta-analysis and systematic review . BMJ . 2009 ; 338 : 1574 - 1580 .
7 . Nava S , Ambrosino N , Clini E , et al . Noninvasive mechanical ventilation in the weaning of patients with respiratory failure due to chronic obstructive pulmonary disease. A randomized, controlled trial . Intern Med . 1998 ; 128 ( 9 ): 721 - 728 .
8 . Esteban A , Anzueto A , Frutos F , et al ; Mechanical Ventilation International Study Group . Characteristics and outcomes in adult patients receiving mechanical ventilation: a 28-day international study . JAMA . 2002 ; 287 ( 3 ): 345 - 355 .
9 . Antonelli M , Conti G , Moro ML , et al . Predictors of failure of noninvasive positive pressure ventilation in patients with acute hypoxemic respiratory failure: a multi-center study . Intensive Care Med . 2001 ; 27 ( 11 ): 1718 - 1728 .
10 . Ceriana P , Delmastro M , Rampulla C , Nava S . Demographics and clinical outcomes of patients admitted to a respiratory intensive care unit located in a rehabilitation center . RespirCare . 2003 ; 48 ( 7 ): 670 - 676 .
11 . Pilcher DV , Bailey MJ , Treacher DF , Hamid S , Williams AJ , Davidson AC . Outcomes, cost and long term survival of patients referred to a regional weaning centre . Thorax . 2005 ; 60 ( 3 ): 187 - 192 .
12 . De Jonghe B , Sharshar T , Lefaucheur JP , et al ; Groupe de Réfl exion et d’Etude des Neuromyopathies en Réanimation . Paresis acquired in the intensive care unit: a prospective mul-ticenter study . JAMA . 2002 ; 288 ( 22 ): 2859 - 2867 .
13 . Deem S , Lee CM , Curtis JR . Acquired neuromuscular dis-orders in the intensive care unit . Am J Respir Crit Care Med . 2003 ; 168 ( 7 ): 735 - 739 .
for a comparable infant population, the success rate was signifi cantly less (87% vs 100%) ( P , .05) than for patients with assisted CPF � 160 L/m. Unmeasur-able assisted CPFs indicate an inability to close the glottis and are associated with stridor, saliva aspira-tion, and less effective NIV and MAC.
An NIV/MAC protocol has been used to avoid over 100 hospitalizations for continuously ventilator-dependent (NIV) patients with NMD. 20,35 Here we considered unweanable patients with NMD for whom intubation could not be avoided. Upon extubation, most patients with a VC of 200 mL or more eventually were weaned from continuous to part-time NIV by taking fewer and fewer mouthpiece IPPVs. Thus, the paradigm of weaning then extubation can be changed to extubation to permit self-weaning for patients with NMD. The notion that early tracheotomy after intu-bation somehow facilitates ventilator weaning 43 should be reassessed for patients with NMD. NIV is also associated with over 75% fewer ventilator-associated pneumonias.6,44 Use of mouthpieces rather than “masks” interfaced in acute-care facilitated speech, oral intake, comfort, and glossopharyngeal breathing 45 ; elimi-nated the risk of skin pressure sores; and permitted air stacking to maintain pulmonary compliance, 37,45
diminish atelectasis, and facilitate manually assisted coughing.
The purpose here was not to facilitate ventilator weaning or to consider long-term outcomes, but to extubate unweanable patients. Benefi ts included no mortality, fewer days intubated, no tracheostomies, and return home. Decannulation, too, can facilitate ventilator weaning. 46 Avoidance of tracheostomy for continuous ventilator (NIV) users can also better maintain quality of life, 47-49 significantly diminish long-term pneumonia and respiratory hospitalization rates,50 maximize ventilator-free breathing, 46 and facilitate return home. 49
In conclusion, unweanable intubated patients with NMD who satisfy specifi c criteria can be successfully extubated to full NIV and MAC. Patients with mea-surable assisted cough fl ows should no longer be advised to refuse intubation for fear of extubation failure and tracheotomy. We no longer consider tracheotomy for any ventilator-dependent patients with NMD who satisfy Table 1 criteria, and now offer extubation to most with CPF , 160 L/m.
Acknowledgments
Author contributions: Dr Bach: wrote all drafts of the paper and, with Dr Hamdani, extubated all the patients in New Jersey. Mr Gonçalves: performed the extubations on all of the patients in Portugal, gathered data on the Portuguese patients, and added material to the text of the manuscript. Dr Hamdani: performed the extubations on some of the patients in New Jersey, gathered data on the New Jersey patients, and added material to the text of the manuscript.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 117

www.chestpubs.org CHEST / 137 / 5 / MAY, 2010 1039
14 . Simonds AK . Streamlining weaning: protocols and weaning units . Thorax . 2005 ; 60 ( 3 ): 175 - 182 .
15 . Winck JC , Gonçalves M . Muscles and lungs: fatal attrac-tion, but time for intervention . Monaldi Arch Chest Dis . 2005 ; 63 ( 3 ): 121 - 123 .
16 . Epstein SK . Weaning the “unweanable”: liberating patients from prolonged mechanical ventilation . Crit Care Med . 2007 ; 35 ( 11 ): 2640 - 2641 .
17 . Benditt JO , Boitano L . Respiratory treatment of amyotrophic lateral sclerosis . Phys Med Rehabil Clin N Am . 2008 ; 19 ( 3 ): 559 - 572 .
18 . Benditt JO . Full-time noninvasive ventilation: possible and desirable . Respir Care . 2006 ; 52 ( 9 ): 1012 - 1015 .
19 . Soudon P , Steens M , Toussaint M . A comparison of invasive ver-sus noninvasive full-time mechanical ventilation in Duchenne muscular dystrophy . Chron Respir Dis . 2008 ; 5 ( 2 ): 87 - 93 .
20 . Gomez-Merino E , Bach JR . Duchenne muscular dystrophy: prolongation of life by noninvasive ventilation and mechani-cally assisted coughing . Am J Phys Med Rehabil . 2002 ; 81 ( 6 ): 411 - 415 .
21 . Smina M , Salam A , Khamiees M , Gada P , Amoateng-Adjepong Y , Manthous CA . Cough peak fl ows and extubation outcomes . Chest . 2003 ; 124 ( 1 ): 262 - 268 .
22 . Bach JR , Saporito LR . Criteria for extubation and tracheos-tomy tube removal for patients with ventilatory failure. A dif-ferent approach to weaning . Chest . 1996 ; 110 ( 6 ): 1566 - 1571 .
23 . Salam A , Tilluckdharry L , Amoateng-Adjepong Y , Manthous CA . Neurologic status, cough, secretions and extubation out-comes . Intensive Care Med . 2004 ; 30 ( 7 ): 1334 - 1339 .
24 . Ferrer M , Esquinas A , Arancibia F , et al . Noninvasive venti-lation during persistent weaning failure: a randomized con-trolled trial . Am J Respir Crit Care Med . 2003 ; 168 ( 1 ): 70 - 76 .
25 . Bach JR , Alba AS . Noninvasive options for ventilatory sup-port of the traumatic high level quadriplegic patient . Chest . 1990 ; 98 ( 3 ): 613 - 619 .
26 . Bach JR . New approaches in the rehabilitation of the traumatic high level quadriplegic . Am J Phys Med Rehabil . 1991 ; 70 ( 1 ): 13 - 19 .
27 . Bach JR . Amyotrophic lateral sclerosis: prolongation of life by noninvasive respiratory AIDS . Chest . 2002 ; 122 ( 1 ): 92 - 98 .
28 . Tzeng AC , Bach JR . Prevention of pulmonary morbidity for patients with neuromuscular disease . Chest . 2000 ; 118 ( 5 ): 1390 - 1396 .
29 . Bach JR . Mechanical insuffl ation-exsuffl ation. Comparison of peak expiratory fl ows with manually assisted and unassisted coughing techniques . Chest . 1993 ; 104 ( 5 ): 1553 - 1562 .
30 . Winck JC , Gonçalves MR , Lourenço C , Viana P , Almeida J , Bach JR . Effects of mechanical insuffl ation-exsuffl ation on respiratory parameters for patients with chronic airway secre-tion encumbrance . Chest . 2004 ; 126 ( 3 ): 774 - 780 .
31 . Ely EW , Baker AM , Dunagan DP , et al . Effect on the dura-tion of mechanical ventilation of identifying patients capable of breathing spontaneously . N Engl J Med . 1996 ; 335 ( 25 ): 1864 - 1869 .
32 . Meade M , Guyatt G , Sinuff T , et al . Trials comparing alterna-tive weaning modes and discontinuation assessments . Chest . 2001 ; 120 ( 6 Suppl ): 425S - 437S .
33 . MacIntyre NR , Cook DJ , Ely EW Jr , et al ; American College of Chest Physicians ; American Association for Respiratory Care ; American College of Critical Care Medicine . Evidence-
based guidelines for weaning and discontinuing ventilatory support: a collective task force facilitated by the AmericanCollege of Chest Physicians; the American Association for Respiratory Care; and the American College of Critical Care Medicine . Chest . 2001 ; 120 ( 6 Suppl ): 375S - 395S .
34 . Sancho J , Servera E , Díaz J , Marín J . Predictors of ineffec-tive cough during a chest infection in patients with stable amyotrophic lateral sclerosis . Am J Respir Crit Care Med . 2007 ; 175 ( 12 ): 1266 - 1271 .
35 . Bach JR , Bianchi C , Aufi ero E . Oximetry and indications for tra-cheotomy for amyotrophic lateral sclerosis . Chest . 2004 ; 126 ( 5 ): 1502 - 1507 .
36 . Bach JR , Alba AS , Saporito LR . Intermittent positive pressure ventilation via the mouth as an alternative to tracheostomy for 257 ventilator users . Chest . 1993 ; 103 ( 1 ): 174 - 182 .
37 . Bach JR , Kang SW . Disorders of ventilation: weakness, stiff-ness, and mobilization . Chest . 2000 ; 117 ( 2 ): 301 - 303 .
38 . Bach JR , Gonzalez M , Sharma A , Swan K , Patel A . Open gas-trostomy for noninvasive ventilation users with neuromuscular disease . Am J Phys Med Rehabil . 2010 ; 87 ( 1 ): 1 - 6 .
39 . Ferrer M , Sellares J , Valencia M , et al. Non-invasive venti-lation after extubation in hypercapnic patients with chronic respiratory disorders: randomised controlled trial. Lancet. 2009 ; 374 (9695): 1044 - 1045 .
40 . Bach JR , Ishikawa Y , Kim H . Prevention of pulmonary mor-bidity for patients with Duchenne muscular dystrophy . Chest . 1997 ; 112 ( 4 ): 1024 - 1028 .
41 . Servera E , Sancho J , Zafra MJ , Catalá A , Vergara P , Marín J . Alternatives to endotracheal intubation for patients with neu-romuscular diseases . Am J Phys Med Rehabil . 2005 ; 84 ( 11 ): 851 - 857 .
42 . Bach JR , Niranjan V , Weaver B . Spinal muscular atrophy type 1: a noninvasive respiratory management approach . Chest . 2000 ; 117 ( 4 ): 1100 - 1105 .
43 . Blot F , Melot C ; Commission d’Epidémiologie et de Recherche Clinique . Indications, timing, and techniques of tracheostomy in 152 French ICUs . Chest . 2005 ; 127 ( 4 ): 1347 - 1352 .
44 . Kollef MH . Avoidance of tracheal intubation as a strategy to prevent ventilator-associated pneumonia . Intensive Care Med . 1999 ; 25 ( 6 ): 553 - 555 .
45 . Bach JR , Bianchi C , Vidigal-Lopes M , Turi S , Felisari G . Lung infl ation by glossopharyngeal breathing and “air stacking” in Duchenne muscular dystrophy . Am J Phys Med Rehabil . 2007 ; 86 ( 4 ): 295 - 300 .
46 . Bach JR , Goncalves M . Ventilator weaning by lung expan-sion and decannulation . Am J Phys Med Rehabil . 2004 ; 83 ( 7 ): 560 - 568 .
47 . Bourke SC , Bullock RE , Williams TL , Shaw PJ , Gibson GJ . Noninvasive ventilation in ALS: indications and effect on quality of life . Neurology . 2003 ; 61 ( 2 ): 171 - 177 .
48 . Viroslav J , Rosenblatt R , Tomazevic SM . Respiratory man-agement, survival, and quality of life for high-level traumatic tetraplegics . Respir Care Clin N Am . 1996 ; 2 ( 2 ): 313 - 322 .
49 . Bach JR , Intintola P , Alba AS , Holland IE . The ventilator-assisted individual. Cost analysis of institutionalization vs rehabil-itation and in-home management . Chest . 1992 ; 101 ( 1 ): 26 - 30 .
50 . Bach JR , Rajaraman R , Ballanger F , et al . Neuromuscular ventilatory insuffi ciency: effect of home mechanical ventilator use v oxygen therapy on pneumonia and hospitalization rates . Am J Phys Med Rehabil . 1998 ; 77 ( 1 ): 8 - 19 .
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
118 Miguel Ramalho do Souto Gonçalves

DOI 10.1378/chest.09-2144; Prepublished online December 29, 2009; 2010;137; 1033-1039Chest
WinckJohn Robert Bach, Miguel R. Gonçalves, Irram Hamdani and Joao Carlos
Management ParadigmExtubation of Patients With Neuromuscular Weakness : A New
May 5, 2010This information is current as of
& ServicesUpdated Information
3.full.htmlhttp://chestjournal.chestpubs.org/content/137/5/103Updated Information and services can be found at:
References
3.full.html#ref-list-1http://chestjournal.chestpubs.org/content/137/5/103accessed free at:This article cites 50 articles, 27 of which can be
Permissions & Licensing
http://www.chestpubs.org/site/misc/reprints.xhtml(figures, tables) or in its entirety can be found online at: Information about reproducing this article in parts
Reprintshttp://www.chestpubs.org/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
Citation Alerts
of the online article.article. To sign up, select the "Services" link to the right Receive free e-mail alerts when new articles cite this
formatImages in PowerPoint
format. See any online figure for directions. downloaded for teaching purposes in PowerPoint slide
articles can beCHESTFigures that appear in
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 119

Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
120 Miguel Ramalho do Souto Gonçalves
Study 2
Noninvasive ventilation associated with mechanical
assisted cough for extubation and decannulation in high
spinal cord injury patients
Miguel R. Gonçalves, Tiago Pinto, Teresa Honrado, Teresa Oliveira,
Celeste Dias, Ana Maria Mota and João Carlos Winck
(Critical Care Medicine, submitted)
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 121

Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
122 Miguel Ramalho do Souto Gonçalves

1
Noninvasive ventilation associated with mechanical
assisted cough for extubation and decannulation in
high spinal cord injury patients
Concise title: Extubation and decannulation in spinal cord injury
Authors: Miguel R. Gonçalves, Tiago Pinto, Teresa Honrado, Teresa Oliveira, Celeste
Dias, Ana Maria Mota and João Carlos Winck
Affiliation: Lung Function and Ventilation Unit, Pulmonology Department; Intensive
Care and Emergency Department;, Faculty of Medicine, University Hospital of S. João
Corresponding author:
Miguel R. Gonçalves Lung Function and Ventilation Unit – Pulmonary Medicine Department Intensive Care Unit – Emergency Department University Hospital of S. João Address: Av. Prof. Hernani Monteiro, Porto, Portugal Phone: 00351 225512100 (extension 1042); [email protected] [email protected]
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 123

2
Abstract
Purpose: to compare extubation vs. decannulation outcomes of continuously ventilator dependent (CVD) high level spinal cord injured (SCI) patients. Methods: 20 (3 females) CVD high level SCI patients with 44±16.3 years of age, were either extubated (n=13) or decannulated (n=7) to continuous noninvasive ventilation (NIV) and mechanically assisted coughing (MAC). Successful extubation/decannulation was defined by not requiring re-intubation/tracheotomy during hospitalization. Vital capacity (VC) and cough peak flows (CPF) were measured immediately (T1), at 48 hours (T2), and at 6 months (T3) after tube removal. Days using invasive ventilation, extubation/decannulation success rates, Intensive Care Unit (ICU) lengths of stay, days required for protocols and extent of ventilator dependence at discharge and after 6 months were analyzed. Readmissions and survival were evaluated at 1 year. Results: All extubations and decannulations were successful. Extubation required significantly fewer ICU days than decannulation. The VC, unassisted and assisted CPF at T1, T2 and T3 improved significantly more for the extubation than for the decannulation. Patients had comparable ASIA levels and VCs at T1 but the extubation group had significantly higher VC at T2 and unassisted and assisted CPF at T2 and T3. All patients were discharged home using either NIV or breathing autonomously. During the year follow-up, 1 extubated patient was hospitalized due to a respiratory tract infection (RTI) and 1 died. Two decanulated patients were hospitalized for a RTI and a stroke. None required critical care. Conclusions: Decannulation or avoidance of tracheostomy by extubation of CVD SCI patients can result in better respiratory outcomes.
Key-words: Noninvasive ventilation, Mechanical Insufflation-Exsufflation, Extubation,
Decannulation, Spinal Cord Injury.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
124 Miguel Ramalho do Souto Gonçalves

3
Introduction
Ventilatory insufficiency and impaired airway secretion clearance are common
complications of high level spinal cord injury (SCI) and can lead to respiratory failure
in both the acute and chronic stages. Standard invasive ventilatory management options
include early intubation and tracheostomy for long term care [1].
High level SCI, ascending cord edema, spinal shock, and perhaps other factors
can result in progressive ventilatory insufficiency usually shortly after hospital
admission for SCI. Following intubation, failure to pass “spontaneous breathing trials
(SBTs)” and ventilator weaning parameters [2] is common and often results in
intubation and tracheostomy [1]. It is presumed that ventilator weaning is necessary
before patients can be safely extubated/decanulated [3]. However, more recently, a
successful extubation protocol was described for 157 continuously ventilator dependent
(CVD) patients who could not pass SBTs before or after extubation [4]. Further, in 1990
Bach et al. reported the decannulation of “unweanable” CVD high level spinal cord
injured (SCI) patients and their transition to non-invasive mechanical ventilation (NIV)
and mechanically assisted coughing (MAC) [5].
Mechanical assisted cough is the use of mechanical insufflation-exsufflation
(CoughAssistTM, Phillips Respironics International Inc., Murrysville, Pa) via invasive
tube or oronasal interface to fully expand and then fully empty the lungs, thereby
expelling airway secretions. An abdominal thrust is applied simultaneously with
exsufflation. By expelling secretions MAC can return SpO2 to normal, avoiding
respiratory failure [6-7], and solving atelectasis [8-9].
Other than for occasional use of bi-level positive airway pressure at less than
ventilatory support levels [10], there has been no further research in this domain.
Despite the fact that cough impairment is one of the most common reasons for
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 125

4
extubation failure and respiratory complications long-term, there have been few studies
that considered its evaluation[11-12] and the use of assisted coughing to facilitate
extubation/decannulation of CVD SCI patients[4,13]
The role of NIV in the ICU continues to increase as evidence accumulates
regarding the prevention of post-extubation respiratory failure [14-15]. However, few
studies focus on the role of NIV in extubation and decannulation of high level SCI
patients [16-17]. Since the patients in our study were CVD, total ventilatory support was
necessary following tube removal. Our purpose is to report and compare extubation and
decannulation success rates and outcomes of self-directed, CVD SCI patients using a
management protocol that included continuous full setting NIV and MAC to maintain
SpO2≥95% in ambient air [4,16].
Patients and Methods
This study received approval from the department and institutional review
boards. Twenty (3 females) consecutively admitted, CVD high level SCI patients with
44±16.3 years of age, who failed multiple SBTs were studied between 2004 to 2009.
There were 13 intubated patients (Group 1 –G1) and seven with tracheostomies (Group
2- G2). Besides CVD and failing multiple SBTs, inclusion criteria included the ability
to cooperate, medical stability, and the resolution of surgical issues. Exclusion criteria
were age less than 18 years, lung disease, lack of cooperation, traumatic head injury or
otherwise impaired cognition, and chest trauma. Patients’ SCI levels were established
according to American Spinal Injury Association (ASIA) criteria[18].
Vital capacity (VC) (Wright Mark 8 spirometer, Ferraris Ltd., London),
unassisted and assisted CPF (Access Peak Flow Meter, Health Scan Products Inc.,
Cedar Grove, New Jersey) were measured immediately (T1), at 48 hours (T2), and 6
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
126 Miguel Ramalho do Souto Gonçalves

5
months after tube removal (T3) for both groups. Assisted CPF were measured by having
the patient air stack to the maximum lung volumes[19] that could be held by the glottis
then have an abdominal thrust applied as they cough into a peak flow meter[20].
Extubation and decannulation success was defined by not requiring re-intubation
or re-cannulation during the same hospitalisation. The days using invasive mechanical
ventilation (MV), VC and (unassisted and assisted) CPF at T1, T2, and T3, ICU lengths
of stay, days required for extubation/decannulation, and extent of ventilator dependence
at discharge and 6 months later were compared for the two groups. One year incidence
of readmissions and survival is reported.
Extubation protocol:
Criteria for extubation were: normal white blood cell count, chest radiograph
abnormalities cleared or clearing, oxyhemoglobin saturation greater than or equal to
95% in ambient air, and afebrile[4].Once these criteria were met the nasogastric tube
was removed if present to facilitate immediate post-extubation nasal NIV, and
measurement of CPF and VC.
The extubation protocol included maintaining normal alveolar ventilation by full
ventilator support settings and using MAC (pressures 40 to 60 cm H2O to -40 to -60 cm
H2O with exsufflation-timed abdominal thrust) via the translaryngeal tube every 30 to
120 minutes as needed until SpO2 remained ≥95% in ambient air.
Patients were then extubated directly to mouth piece or nasal NIV with a
portable ventilator on pressure control with 18-20 cm H2O or assist/control mode with
800 to 1500 ml delivered volumes and a back up rate of 10 to 12 per minute[21]. For
mouth piece NIV patients kept 15mm or 22mm angled mouth pieces accessible to their
mouths (Figure 1). Patients weaned themselves, when possible, by taking fewer and
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 127

6
fewer mouth piece intermittent positive pressure ventilations (IPPVs) as needed. For
night-time ventilation patients used nasal, oral or oronasal interfaces. No supplemental
oxygen was used.
Patients were taught how to maximally expand their lungs by “air stacking”
(retaining consecutive) ventilator delivered volumes to the largest volume the glottis
could hold[19].Once the patient maximally air stacked, an abdominal thrust was timed
to glottic opening to manually assist the cough[20,22]. The respiratory therapy and
nursing staff were trained in and provided MAC via oro-nasal interfaces (Figure 2) post-
extubation until airway secretion elimination was no longer a problem and the SpO2 no
longer dipped below 95%. Generally, pressures of 40 to -40 cm H2O were used with an
exsufflation-timed abdominal thrust. All clinical staff used this strategy with oximetry
as feedback to maintain SpO2≥ 95%. Re-intubation was indicated for acute distress and
irreversible oxyhemoglobin desaturation.
Decannulation protocol:
Our protocol is similar to one previously described[16,23]. Besides having to
satisfy the same criteria as for extubation, all patients from G2 had to be able to
verbalize when the tube cuff was deflated, have effective swallow and be medically
stable. Normal alveolar ventilation was maintained by adequate ventilator settings.
Supplemental oxygen therapy was discontinued and MAC used via tube (with
cuff inflated) until SpO2 remained ≥95% in ambient. Through the tube MAC was used
at gauge pressures of 50 to 60 cm H2O to -50 to -60 cm H2O. All of the patients were
placed on portable volume-cycled ventilators or, when preferred by the patient, portable
pressure-cycled ventilators. The cuffs were completely deflated for increasing periods,
hourly, until cuff deflation could be tolerated both throughout daytime hours and
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
128 Miguel Ramalho do Souto Gonçalves

7
overnight. When necessary, the patient's tracheostomy tube diameter was changed to
permit sufficient leakage for speech while maintaining adequate fit to permit effective
assisted ventilation with delivered ventilator volumes generally of 1 to 2 liters to
compensate leaks through the upper airway. Ventilator parameters were set on
assist/control mode, rate 10 to 12, and were titrated to maintain paCO2 levels between
35 to 40 mm Hg. Tracheal integrity, tracheostomy tube width, volitional glottic and
vocal cord movements were evaluated through upper airway fiberoptic examination.
Patients were advanced to the use of 24 hour tracheostomy ventilation with a
fenestrated tracheostomy tube with a deflated cuff, and after that period they were
trained in the use of mouthpiece IPPV for daytime ventilatory support with the
tracheostomy tube capped and ventilator settings adjusted. Each patient learned to close
off the nasopharynx with the soft palate to prevent nasal leakage. Once daytime
mouthpiece IPPV was mastered, effective NIV during sleep through a nasal or oronasal
mask was also implemented. When the efficacy of continuous NIV had been observed
and before definitive decannulation, the tracheostomy tube was replaced by a
tracheostomy button that allowed more accurate measurement of VC and CPF.
After 48 hours, patients maintained NIV, the tracheostomy button was removed
and a compressive silicon material was placed over an occlusive tracheostomy site
dressing that was fit to avoid leaks. Although the tracheostomy site usually closed in 24
to 72 hours, if not closed after 2 weeks it was usually sutured closed.
Statistical Analysis
Results are expressed as mean and standard deviation. Statistical analysis was
carried out using SPSS version 15.0 (SPSS, Inc, Chicago, IL). Differences between VC,
unassisted and assisted CPF, as well as ICU length of stay, days on invasive MV, days
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 129

8
on protocol and ventilatory dependence at discharge were compared using the Wilcoxon
rank test. A p value ≤ 0.05 was considered significant.
Results
Demographic data are in Table 1. There were no significant differences on age
and level of injury severity between groups and none of the patients had lung disease.
All patients failed multiple SBTs before the application of the protocols. Other than for
3 local patients, the tracheostomy patients were transferred to our ICU for
decannulation.
The patients required NIV for 43±8 and 45±7 of the first post-
extubation/decannulation 48 hours, respectively. Outcomes data are noted in Table 2.
Vital capacity, unassisted and assisted CPF over time are shown in Figures 3 and
4 respectively. Both patient groups had significant improvements in VC and unassisted
and assisted CPF from T1 to T2 and T2 to T3 (p<0,05). In addition, the extubated
patients had significantly higher VC at T2 (1.5±0.50L or 40±15% of predicted normal
vs. 0.9±0.4L or 24±8% of predicted normal, p<0.05), unassisted CPF (170±58L/min vs.
84±25L/min at T2, p<0.05; 247±60 L/min vs. 114±46 L/min at T3, p<0.05) and assisted
CPF (263±78L/min vs. 198±41L/min at T2, p<0.05; and 359±98 L/min vs. 226±74
L/min at T3, p<0.05) than the decanulated patients.
All patients were successfully extubated/decanulated with no respiratory
complications. Two decanulated patients’ stomas were sutured for final closure. All
were discharged home with caregivers proficient in providing NIV, manually assisted
cough and air-stacking, During the first post-discharge year, one extubated patient was
hospitalized for a RTI and 2 decanulated patients (one on nocturnal-only NIV) were
hospitalized, one for a RTI and the other for a stroke. None of the hospitalizations
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
130 Miguel Ramalho do Souto Gonçalves

9
resulted in intubation or critical care. One year post discharge, 1 extubated patient died
from non-respiratory causes and 2 were lost to follow up. All others were alive and
well.
Discussion
Seventy-four percent of ASIA A acute SCI patients above the C5 level have
been reported to require intubation[24]and the overall incidence of tracheostomy in
these cases was between 81 and 83%[3,25]. The number of respiratory complications in
SCI including ventilator associated pneumonia (VAP) during the acute phase
contributes significantly to both hospital length of stay and cost[26]. However, it is not
ventilator use that causes VAP but the invasive interface [27]. After the conversion to
NIV and MAC, none of the patients in this study developed pneumonia or other
respiratory complications during the hospitalization.
Guidelines for respiratory management after SCI were published in 2005[28].
However, the guidelines assumed the need for tracheostomy for unweanable CMV
patients. In 2006, Bach challenged the medical community to decanulate high level SCI
patients to NIV to avoid the complications of tracheostomy, to facilitate training in
glossopharyngeal breathing to increase autonomous breathing ability and security in the
event of ventilator failure, and to return home [13]This work is the first to accept this
challenge.
In this study, besides successful extubation and decannulation of CVD patients,
after the protocol, only 9 (45%) of the total population used NIV at discharge and all
others weaned to autonomous breathing. The use of high delivered NIV volumes has
been reported to facilitate the weaning process and lessen risk of respiratory
complications[29] as well as result in increased VC and CPF for patients who are
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 131

10
extubated[4] or decanulated[16,17,30] and our results are consistent with those studies.
Moreover, it is not expected that continuous NIV can be a successful alternative to
invasive ventilation, if patients use only mask ventilation[31]. Further, for both groups,
mouthpiece ventilation normalized speech, provided normal daytime ventilation,
permitted "air stacking" for lung expansion and assisted coughing, and
weaning[4,21,30].
Aggressive use of MAC via translaryngeal and tracheostomy tubes was the main
intervention that may have improved pulmonary function (VC and CPF) and normalized
SpO2 in ambient air to satisfy the most important criterion for
extubation/decannulation. Our findings are consistent with those of Bach et al.[16,32],
however our patients were all successfully extubated despite some having assisted CPF
below 160l/min at T1. This was possibly due to the more aggressive use of MAC up to
every 15 min to maintain normal SpO2. Pillastrini et al.[33], too reported that
mechanical in-exsufflation aided in clearance of bronchial secretions and increased
forced VC, forced expiratory volume in 1 second, and peak expiratory flows for
tracheostomized SCI subjects. Vital Capacity and CPF also improved in our patients
because of lung expansion and secretions removal.
Transition from tracheostomy to continuous NIV was progressive and implied a
specific protocol that included ventilation with a deflated cuff for increasing periods
until it could be tolerated throughout daytime hours and overnight.
This “open system” ventilation[34] permitted the patients to improve their vocal
cord function that was essential for successful NIV training with a capped cuffless
fenestrated tube. In 2004 we reported that decannulation and conversion to NIV and
MAC can facilitate ventilator weaning of CMV dependent patients[30]. It has also been
reported that decanulated patients invariably prefer NIV over return to tracheostomy
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
132 Miguel Ramalho do Souto Gonçalves

11
ventilation for safety, convenience, appearance, comfort, facilitating effect on speech,
sleep, and swallowing, and overall[35]. Despite this, until this study, no other has
described the systematic extubation/decannulation of CVD SCI patients to noninvasive
alternatives or the avoidance of tracheotomy for unweanable intubated patients.
In this study, both short –term and long term outcomes for the extubated patients
were better than for the decanulated patients. Thus, it appears preferable, in this patient
population, to prevent tracheotomy in the first place, whenever possible, rather than
decanulate later on. Certainly, patients with severe bulbar-innervated muscle
involvement, head injury, chest trauma, medical fragility, complicated courses including
the need for surgical procedures over a greater than 3 or 4 week period are best
managed by tracheotomy.
Our data show that the extubated SCI patients had significantly shorter ICU
stays, were more quickly extubated than the decanulated patients decanulated, had
higher VC at 48 hours after tube removal, higher unassisted and assisted CPF at 48
hours and at 6 months after tube removal than those decannulated. This can be due to
the fact that extubated patients had significant less time on invasive ventilation with
consequent less respiratory muscle deconditioning, were somehow less severely
affected despite comparable VCs and ASIA levels at T1, or had less risk of upper
airway instability and less secretion encumbrance or segmental atelectasis despite the
same CPF and normal SpO2. Moreover, the decanulated patients needed MAC to clear
airway secretions for longer periods of time as well as more time for NIV training and
tracheostomy site closure.
The higher values of VC at 48 hours after extubation explains the greater
number of extubated patients discharged to the community with no ventilatory support.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 133

12
Although tracheostomy may have physiologic benefits over endotracheal tubes
in terms of reduced work of breathing[36]and permitting more efficient suctioning, over
90% of the time suction catheters enter only the right mainstem bronchus resulting in
80% of pneumonias occurring on the left lungs of these patients[37] and work of
breathing is readily compensated by providing pressure support during SBTs. There are
no reports of better outcomes with tracheostomy ventilation when compared to the
NIV/MAC protocols.
This study has the limitations by its retrospective nature and small number of
participants suggesting caution when generalizing the importance of its outcomes.
Considering the incidence of mortality and respiratory morbidity in this
population of SCI patients managed by standard ventilatory invasive techniques, the
results of this study suggest that noninvasive methods of assisted ventilation and
coughing can facilitate both extubation and decannulation with significant improvement
on ventilatory dependence and pulmonary function and may facilitate return home
rather than prolonged institutionalization for weaning attempts. Randomized controlled
trials to evaluate these precepts may be unethical since noninvasive management is
clearly effective.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
134 Miguel Ramalho do Souto Gonçalves

13
Acknowledgments:
The authors wish to thank the medical, respiratory therapy and nursing staffs of
both ICU and Pulmonology departments for their assistance and support in managing
the patients.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 135

14
Figure 1- Forty nine year old man with C4 ASIA A spinal cord injury extubated with
no ventilator-free breathing ability, using volume cycled ventilation through a 15 mm
angled mouth piece for ventilatory support.
Figure 2- Twenty- one year old man with a C3 ASIA A spinal cord injury, using post-
extubation mechanically assisted coughing (MAC) with the CoughAssistTM (Philips
Respironics International Inc.) via an oronasal interface at pressures of 40 to -40
cmH2O.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
136 Miguel Ramalho do Souto Gonçalves

15
Figure 3 – Vital capacity at extubation (T1), after 48 hours (T2) and at 6months follow up (T3)
Legend: VC – Vital Capacity (Liters).
# - p<0,05; &- p<0,05; ¶ -p < 0.05
#
&
#
#
&
&
¶
¶
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 137

16
Figure 4- Unassisted and Assisted CPF data at extubation (T1), after 48 hours (T2) and at 6months follow up (T3)
Legend: CPF – Unassisted cough peak flow (L/min); AsCPF – Assisted cough peak flow (L/min). #1,#2,#3 – p <0,05; &1,&2,&3 – p <0,05 #2 and &2 – p <0,05; #3 and &3 – p <0,05
#1
#1
&1
#2
#2
#3
#3
&1
&2
&3
&2 &3
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
138 Miguel Ramalho do Souto Gonçalves

17
Table 1 – Demographic data
G1
G2
N 13 7
Age (years)
42±19
48±11
Sex, n (%)
FVC, Liters (%) *
male – 10 (77%)
female – 3 (23%)
0,5±0,6 (16±24)
male – 7 (100%)
0,2±0,3 (8±10)
FEV1/FVC (%) *
CPF (L/min) *
Level SCI, n (/%)
ASIA scale, n (/%)
88±5
64±64
C2-C3 – 4 (31%)
C4-C5 –8 (62%)
C6 -1 (7%)
A – 11 (85%)
B – 2 (15%)
78±5
23±29
C2-C3 – 2 (29%)
C4-C5 –5 (71%)
A- 6 (86%)
B- 1 (14%)
Legend: G1 – Extubated patients; G2 – Decannulated patients; N – number of patients; FVC –Forced Vital Capacity; FEV1 – Forced expiratory volume at 1
st second; CPF- (Unassited) Cough Peak Flow; SCI –
Spinal cord injury; ASIA – American Spinal Injury Association
* - measured at T1 (immediately after tube removal) Note – p value is non- significant in all items between the 2 groups
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 139

18
Table 2 – ICU and discharge outcomes:
G1
G2
Days on invasive mechanical
Ventilation
ICU length of stay (days)
15±12 &
22±16*
61±34 &
97±93*
Duration of protocol (days)
8±6 #
14±3 #
Ventilatory
dependence
at discharge, n (%)
Ventilatory
dependence
at 6 months, n (%)
SB – 8 (61%)
nNIV - 5 (39%)
SB – 11 (85%)
nNIV – 2 (15%)
SB – 3 (43%)
nNIV - 3 (43%)
cNIV – 1 (14%)
SB - 4 (57%)
nNIV - 2 (29%)
cNIV – 1 (14%)
Data presented as mean ± standard deviation Legend: : G1 – Extubated patients; G2 – Decannulated patients; ICU – Intensive Care Unit; Duration of
protocol - days required to finish the protocol; SB – Spontaneous breathing; nNIV – nocturnal noninvasive
ventilation; cNIV – continuous noninvasive ventilation
& - p<0,05
* - p < 0,05
# - p < 0,05
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
140 Miguel Ramalho do Souto Gonçalves

19
References
1. Berney S, Bragge P, Granger C, Opdam H, Denehy L (2010) The acute respiratory
management of cervical spinal cord injury in the first 6 weeks after injury: A systematic
review. Spinal Cord
2. Boles JM, Bion J, Connors A, Herridge M, Marsh B, Melot C, Pearl R, Silverman H,
Stanchina M, Vieillard-Baron A, Welte T (2007) Weaning from mechanical ventilation.
Eur Respir J 29 (5):1033-1056
3. Harrop JS, Sharan AD, Scheid EH, Jr., Vaccaro AR, Przybylski GJ (2004)
Tracheostomy placement in patients with complete cervical spinal cord injuries:
American spinal injury association grade a. J Neurosurg 100 (1 Suppl Spine):20-23
4. Bach JR, Goncalves MR, Hamdani I, Winck JC (2010) Extubation of patients with
neuromuscular weakness: A new management paradigm. Chest 137 (5):1033-1039
5. Bach JR, Alba AS (1990) Noninvasive options for ventilatory support of the
traumatic high level quadriplegic patient. Chest 98 (3):613-619
6. Tzeng AC, Bach JR (2000) Prevention of pulmonary morbidity for patients with
neuromuscular disease. Chest 118 (5):1390-1396
7. Gomez-Merino E, Bach JR (2002) Duchenne muscular dystrophy: Prolongation of
life by noninvasive ventilation and mechanically assisted coughing. Am J Phys Med
Rehabil 81 (6):411-415
8. Vianello A, Corrado A, Arcaro G, Gallan F, Ori C, Minuzzo M, Bevilacqua M (2005)
Mechanical insufflation-exsufflation improves outcomes for neuromuscular disease
patients with respiratory tract infections. Am J Phys Med Rehabil 84 (2):83-88;
discussion 89-91
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 141

20
9. Miske LJ, Hickey EM, Kolb SM, Weiner DJ, Panitch HB (2004) Use of the
mechanical in-exsufflator in pediatric patients with neuromuscular disease and impaired
cough. Chest 125 (4):1406-1412
10. Tromans AM, Mecci M, Barrett FH, Ward TA, Grundy DJ (1998) The use of the
bipap biphasic positive airway pressure system in acute spinal cord injury. Spinal Cord
36 (7):481-484
11. Smina M, Salam A, Khamiees M, Gada P, Amoateng-Adjepong Y, Manthous CA
(2003) Cough peak flows and extubation outcomes. Chest 124 (1):262-268
12. Salam A, Tilluckdharry L, Amoateng-Adjepong Y, Manthous CA (2004)
Neurologic status, cough, secretions and extubation outcomes. Intensive Care Med 30
(7):1334-1339
13. Bach JR (2006) Prevention of respiratory complications of spinal cord injury: A
challenge to "Model" Spinal cord injury units. J Spinal Cord Med 29 (1):3-4
14. Ferrer M, Valencia M, Nicolas JM, Bernadich O, Badia JR, Torres A (2006) Early
noninvasive ventilation averts extubation failure in patients at risk: A randomized trial.
Am J Respir Crit Care Med 173 (2):164-170
15. Burns KE, Adhikari NK, Meade MO (2003) Noninvasive positive pressure
ventilation as a weaning strategy for intubated adults with respiratory failure. Cochrane
Database Syst Rev (4):CD004127
16. Bach JR, Saporito LR (1996) Criteria for extubation and tracheostomy tube removal
for patients with ventilatory failure. A different approach to weaning. Chest 110
(6):1566-1571
17. Viroslav J, Rosenblatt R, Tomazevic SM (1996) Respiratory management, survival,
and quality of life for high-level traumatic tetraplegics. Respir Care Clin N Am 2
(2):313-322
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
142 Miguel Ramalho do Souto Gonçalves

21
18. International standards for neurologic and fuctional classification of spinal cord
injury (1996). Chicago, IL; American Spinal Injury Association
19. Kang SW, Bach JR (2000) Maximum insufflation capacity. Chest 118 (1):61-65
20. Bach JR (1993) Mechanical insufflation-exsufflation. Comparison of peak
expiratory flows with manually assisted and unassisted coughing techniques. Chest 104
(5):1553-1562
21. Bach JR, Alba AS, Saporito LR (1993) Intermittent positive pressure ventilation via
the mouth as an alternative to tracheostomy for 257 ventilator users. Chest 103 (1):174-
182
22. Bach JR (1994) Update and perspective on noninvasive respiratory muscle aids. Part
2: The expiratory aids. Chest 105 (5):1538-1544
23. Bach JR, Saporito LR (1994) Indications and criteria for decannulation and
transition from invasive to noninvasive long-term ventilatory support. Respir Care 39
(5):515-528; discussion 529-531
24. Velmahos GC, Toutouzas K, Chan L, Tillou A, Rhee P, Murray J, Demetriades D
(2003) Intubation after cervical spinal cord injury: To be done selectively or routinely?
Am Surg 69 (10):891-894
25. Romero J, Vari A, Gambarrutta C, Oliviero A (2009) Tracheostomy timing in
traumatic spinal cord injury. Eur Spine J 18 (10):1452-1457
26. Winslow C, Bode RK, Felton D, Chen D, Meyer PR, Jr. (2002) Impact of
respiratory complications on length of stay and hospital costs in acute cervical spine
injury. Chest 121 (5):1548-1554
27. Girou E, Schortgen F, Delclaux C, Brun-Buisson C, Blot F, Lefort Y, Lemaire F,
Brochard L (2000) Association of noninvasive ventilation with nosocomial infections
and survival in critically ill patients. Jama 284 (18):2361-2367
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 143

22
28. Consortium for spinal cord medicine. Respiratory management during the first five
days after spinal cord injury: A clinical practice guideline for health care professionals.
(2005). available from wwwguidelinegov/summary/pdfaspxdoc_id=spinal+AND+injury
29. Peterson WP, Barbalata L, Brooks CA, Gerhart KA, Mellick DC, Whiteneck GG
(1999) The effect of tidal volumes on the time to wean persons with high tetraplegia
from ventilators. Spinal Cord 37 (4):284-288
30. Bach JR, Goncalves M (2004) Ventilator weaning by lung expansion and
decannulation. Am J Phys Med Rehabil 83 (7):560-568
31. Bach JR (2003) Noninvasive ventilation is more than mask ventilation. Chest 123
(6):2156-2157; author reply 2157
32. Bach JR (1993) Inappropriate weaning and late onset ventilatory failure of
individuals with traumatic spinal cord injury. Paraplegia 31 (7):430-438
33. Pillastrini P, Bordini S, Bazzocchi G, Belloni G, Menarini M (2006) Study of the
effectiveness of bronchial clearance in subjects with upper spinal cord injuries:
Examination of a rehabilitation programme involving mechanical insufflation and
exsufflation. Spinal Cord 44 (10):614-616
34. Gregoretti C, Olivieri C, Navalesi P (2005) Physiologic comparison between
conventional mechanical ventilation and transtracheal open ventilation in acute
traumatic quadriplegic patients. Crit Care Med 33 (5):1114-1118
35. Bach JR (1993) A comparison of long-term ventilatory support alternatives from the
perspective of the patient and care giver. Chest 104 (6):1702-1706
36. Diehl JL, El Atrous S, Touchard D, Lemaire F, Brochard L (1999) Changes in the
work of breathing induced by tracheotomy in ventilator-dependent patients. Am J
Respir Crit Care Med 159 (2):383-388
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
144 Miguel Ramalho do Souto Gonçalves

23
37. Fishburn MJ, Marino RJ, Ditunno JF, Jr. (1990) Atelectasis and pneumonia in acute
spinal cord injury. Arch Phys Med Rehabil 71 (3):197-200
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 145

Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
146 Miguel Ramalho do Souto Gonçalves

Study 3
Effects of mechanical insufflation-exsufflation in
preventing respiratory failure after extubation:
A randomized controlled trial.
Miguel R. Gonçalves, Teresa Honrado, João Carlos Winck, José Artur Paiva
(Critical Care, submitted)
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 147

Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
148 Miguel Ramalho do Souto Gonçalves

Effects of mechanical insufflation-exsufflation in preventing
respiratory failure after extubation.
A randomized controlled trial.
Authors: Miguel R. Gonçalves, Teresa Honrado, João Carlos Winck, José Artur Paiva
Affiliation: Lung Function and Ventilation Unit, Pulmonology Department; Intensive
Care and Emergency Department;, Faculty of Medicine, University Hospital of S. João,
Porto, Portugal
Corresponding author:
Miguel R. Gonçalves Lung Function and Ventilation Unit – Pulmonary Medicine Department Intensive Care Unit – Emergency Department University Hospital of S. João Address: Av. Prof. Hernani Monteiro, Porto, Portugal Phone: 00351 225512100 (extension 1042); [email protected] [email protected]
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 149

Abstract:
(Word count 341)
Background: Weaning protocols that include the use of noninvasive ventilation (NIV),
decreases the incidence of re-intubation and ICU length of stay. However, the role of
NIV in post-extubation failure is still not clear. Impaired airway clearance is associated
with NIV failure. Mechanical Insufflation-Exsufflation (MI-E) is an assisted coughing
technique that has been proven to be very effective in patients under NIV.
Aims: To assess the efficacy of MI-E as part of a protocol for patients that develop
respiratory failure after extubation.
Methods: Patients under mechanical ventilation (MV) for more than 48 hours with
specific inclusion criteria, who successfully tolerated an spontaneous breathing trial
(SBT) were randomly allocated before extubation, either for (A) conventional
extubation protocol (control group) or (B) MI-E extubation protocol (study group). Re-
intubation rates, ICU length of stay and NIV failure rates were analyzed.
Results: Seventy five patients (26 females) with a mean age of 61.8±17.3 years old
were randomized to control group (n=40, mean SAPS II) and to study group (n=35,
mean SAPS II 45.0±15.0). MV time before enrollment for was 9.4 ±4.8 and
10.5±4.1days for control and study group respectively. In the 48 hours post extubation,
20 control patients (50%) and 14 study patients (40%) used NIV. Study group patients
had a significant lower re-intubation rate than controls; 6 patients (17%) vs 19 patients
(48%), p<0.05 respectively and a significant lower time under MV; 17.8±6.4 vs
11.7±3.5 days, p<0.05, respectively. Considering only the sub-group of patients that
used NIV, the re-intubation rates related to NIV failure were significantly lower in the
study group when compared to controls; 2 patients (6%) vs 13(33%), p<0.05,
respectively. Mean ICU length of stay pós - extubation was significantly lower in the
study group when compared to controls (3.1± 2.5 vs 9.8± 6.7 days, p<0.05). There were
no differences in the total ICU length of stay
Conclusions: Inclusion of MI-E in post-extubation failure may reduce re-intubation
rates with consequent reduction in post-extubation ICU length of stay. This technique
seems to b efficient in improving the efficacy of NIV in this patient population.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
150 Miguel Ramalho do Souto Gonçalves

(Word count 2977)
Introduction
The process of weaning from mechanical ventilation must balance the risk of
complications due to unnecessary delays in extubation with the risk of complications
due to early discontinuation and the need of reintubation[1]. Patients who require
reintubation have been noted to have a significantly higher mortality rate than those
who are successfully extubated on the first attempt[2].
Patients in the intensive care setting very often have impaired airway clearance.
Endotracheal intubation prevents the patient from closing the glottis, which is necessary
for effective coughing[3]. Care of the intubated patient includes direct suction applied
through the endotracheal tube which clears a small portion of the airway, is ineffective
for clearing secretions in the peripheral airways, and leaves the patient dependent upon
mucociliary clearance rather than cough clearance[4]. Deep insufflation with a self-
inflating ventilation bag can help, especially if accompanied by chest physiotherapy, but
it does not recreate a cough[5].
Ventilator-associated pneumonia is an exceedingly common problem in
intensive care units (ICUs), occurring in as many as 27% of patients [6]. The reasons for
this are complex, but a significant role is played by the aspiration of upper-airway
secretions and gastric contents[7]. In reality, “ventilator-associated” pneumonia is more
“interface-associated” pneumonia as pathogenic mechanisms are related to the
(invasive) interface used for mechanical ventilation rather than the ventilator itself [8],
Despite the many reports and reviews on ventilator-associated pneumonia, little
emphasis is placed on airway clearance[9].
Predictors for successful weaning include respiratory rate less than 38 per
minute and a rapid shallow breathing index below 100 breaths/min/L [10]. However,
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 151
even in patients who satisfy weaning criteria and pass ventilator weaning trials, there is
an extubation failure rate of 10 to 20% [11].
Post –extubation respiratory failure is defined as the presence of signs and
symptoms of respiratory distress in the first 48 hours after extubation. The reasons
given for extubation failure include lack of improvement in work of breathing,
hypoxemia, respiratory acidosis, retained secretions, and decreased consciousness [12].
However, if at extubation the lungs are healthy and ventilation can be fully maintained
noninvasively[13], then the only remaining concern is the effective expulsion of airway
secretions[14]. Despite the importance of this factor, no ventilator weaning parameter
addresses the ability to cough.
Early extubation, coupled with the use of noninvasive ventilatory support has
been used effectively to facilitate weaning[15-17], improve survival[18], decrease the
incidence of ventilator-associated pneumonia[8, 19] and reduce ICU length of stay[18-
19]. However there is a higher risk of NIV failure when applied in patients that develop
ARF after extubation and the evidence that supports its application is controversial [20-
22].
Despite a great interest in this field, the role of impaired airway secretion
clearance on the outcome of post-extubation respiratory failure in critically ill ventilator
dependent patient treated with non-invasive ventilation is still not clear. Airway
clearance may be impaired in disorders associated with abnormal cough mechanics,
altered mucus rheology, altered mucociliary clearance, or structural airway defects. A
variety of interventions are used to enhance airway clearance with the goal of improving
lung mechanics and gas exchange, and preventing atelectasis and infection [23].
Conventional techniques for augmenting the normal mucociliary clearance and
cough efficacy have been used for many years to treat patients with respiratory
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
152 Miguel Ramalho do Souto Gonçalves
disorders from different etiologies. In recent years, new technologies and more
advanced techniques have been developed to be more effective in acute respiratory
failure These techniques involve mechanical application of forces to the chest wall[24]
or intermittent pressure changes to the airway to assist airway mucus clearance[25-26].
Mechanical insufflation-exsufflation (MI-E) applies positive pressure followed
by negative pressure across the entire airway (both central and peripheral), in contrast to
direct tracheal suction, which applies negative pressure to a small, localized area[27].
This therapy is perhaps the most physiologic recreation of a natural cough.
The purpose of this study is to assess the efficacy of MI-E as part of a weaning
protocol for patients that develop acute respiratory failure after extubation.
Methods:
The data of this randomized control trial was gathered in a 12 bed general ICU
between 2007 and 2009. The study was approved by the ethical institutional committee
and review board.
Patients:
Patients older than 18 years and under mechanical ventilation, for more than 48
hours, for acute hypoxemic and/or hypercapnic respiratory failure from a specific
etiology were considered potentially eligible for the study. Exclusion criteria included
facial or cranial trauma, tracheostomy, active upper gastrointestinal bleeding, neurologic
instability (inability to respond to direct simple orders), hemodynamic instability, lack
of cooperation and confirmed diagnosis of neuromuscular disease.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 153

All patients included were evaluated for discontinuation of mechanical
ventilation through the application of a spontaneous breathing trial (SBT). The
application of a SBT trial was considered appropriate when all of the following criteria
were met : improvement of the condition that caused acute respiratory failure,
respiratory rate less than 38 per minute, rapid shallow breathing index below 100
breaths/min/L [10] suspension of sedative medications, ability to stay alert and
communicate, core temperature less than 38ºC throughout the last 24h, suspension of
vasoactive drugs, with the exception of dopamine at doses lower than 5ug per kilogram
of body weight per minute and partial pressure of oxygen greater than 60mmHg on an
inspired fraction of oxygen(FiO2) of 0.40 (PaO2/FiO2 >200) or less, with a positive
end-expiratory pressure (PEEP) of 5cmH2O
Discontinuation of mechanical ventilation was assessed by a trial of spontaneous
breathing with a T tube on a FiO2 of 50% for up to 60 to 120 minutes. The SBT was
considered successful when during the trial time none of the following symptoms were
found: Respiratory Rate > 35bpm, SpO2 < 90 %, 20% variation of Heart rate or Blood
pressure, respiratory distress, agitation and loss of conscience[28].
Patients who successfully tolerated the SBT were randomly allocated before
extubation, using a computer-generated table either for (A) conventional extubation
protocol (control group) or (B) MI-E extubation protocol (study group). During the first
48 hours after extubation, patients were observed for symptoms of acute respiratory
distress/insufficiency as defined by dyspnea and the presence of at least two of the
following: respiratory acidosis (pH < 7.35 with a PaCO2 >45mmHg), increased use of
accessory respiratory muscles, increased respiratory rate (>35 bpm), and decreasing
oxyhemoglobin saturation, i.e. Spo2 < 90% and PaO2 <80 mmHg with fiO2 > 50%.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
154 Miguel Ramalho do Souto Gonçalves

Group A patients received (post-extubation) standard medical treatment (SMT),
including NIV in case of specific indications, whereas Group B received the same post-
extubation approach plus mechanical in-exsufflation (MI-E).
Patients with persistent weaning failure who failed 3 or more SBTs in one week
were excluded.
Standard medical therapy:
All patients received post extubation standard medical therapy including
supplemental oxygen as needed, respiratory chest physiotherapy, bronchodilators,
antibiotics and any other therapies as directed by the attending physician.
Criteria for NIV were the same in the two groups. Patients were submitted to
NIV, if they met at least one of the following criteria, as judged after they had
undergone the assigned treatment: Respiratory Rate > 35bpm, SpO2 < 90 %, 20%
variation of Heart rate or Blood pressure, dyspnoea with respiratory distress, PaO2<
60mmHg, PaCO2 > 45mmHg, pH < 7,35.
Noninvasive ventilation was provided via an ICU ventilator with noninvasive
mode or via a portable pressure cycled ventilator through a oronasal mask as first
choice. Other interfaces such as nasal, total face, helmet and mouthpieces were used in
case of patient´s intolerance to the oronasal mask.
The fraction of inspired oxygen and the positive end-expiratory pressure were
titrated to maintain the arterial oxygen saturation above 90 percent ( or PaO2 >
60mmHg). The ventilator settings were subsequently adjusted as needed for the
patient’s comfort The facial skin was assessed every four hours to prevent damage from
the tightly fitting mask.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 155

The decision regarding when to discontinue noninvasive ventilation was left to
the attending physician.
Mechanical Insufflation-Exsufflation Protocol (study group):
After passing the SBT and randomized to the study group, before extubation, all
patients were submitted to a treatment of MI-E (3 sessions) with the Cough Assist™
(Philips Respironics, Inc) through the endotracheal tube with pressures set at 40 cm
H2O for insufflation and -40 cm H2O for exsufflation pressure. An
insufflation/exsufflation time ratio of 3secs/2 secs and a pause of 3 sec between each
cycle was used. Eight cycles were applied in every session with an abdominal thrust
timed to the exsufflation cycle.
On top of the standard medical therapy, during the first 48 hours post extubation,
each patient received 3 daily treatments by means of a light-weight, elastic oronasal
mask. Treatments (3 sessions each) were divided between morning, afternoon and night,
making a total of 9 daily sessions.
The daily treatment frequency and its outcomes were recorded in a diary by the
nursing staff. All MI-E treatments were administered by a trained respiratory therapist,
ICU physician or nurse.
Criteria for reintubation:
In both patient groups, the final decision to reintubate was left to and made by
the attending physician, who recorded the single most relevant reason for reintubation.
Reason to reintubate was the existence of at least one of the following, as judged after
they had undergone the assigned treatment: (a) respiratory or cardiac arrest, (b)
respiratory pauses with loss of consciousness, (c) respiratory distress despite 2 hour
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
156 Miguel Ramalho do Souto Gonçalves

treatment with SMT and NIV, (d) decreasing level of consciousness, (c) intolerance to
NIV; (f) hypotension, with a systolic blood pressure below 90 mm Hg for more than 30
minutes despite adequate volume challenge, the use of vasopressors, or both and (g)
copious secretions that could not be adequately cleared or that were associated with
severe hypoxemia. The final decision to reintubate was made by the attending
physician, who recorded the single most relevant reason for reintubation. Only re-
intubations required in the first 48 hours post-extubation was considered for this study.
Outcomes:
Reintubation rate was considered as primary endpoint. Total ICU length of stay,
post-extubation ICU length of stay and reasons for reintubation and NIV failure were
also analysed and compared between groups as secondary endpoints. A sub-group
analysis, both for primary and secondary outcomes, was performed in patients that were
submitted to post-extubation NIV
Statistical analysis:
Descriptive data are reported as mean± standard deviation (SD). Statistical analysis was
performed by SPSS software (Release 15.0 SPSS, Chicago, I1, USA).
Sample size calculation: The primary end-point variable was to decrease reintubation
rates defined by the necessity of mechanical positive pressure ventilation through
orotracheal intubation in the first 48 hours post-extubation in the treatment group.
Initial calculations revealed a required sample size of 33 subjects in each group
with reintubation rates to be reduced by 30%. One interim analysis was performed after
inclusion of 50% of the estimated patients using an α curtailment (p< 0.005) to correct
the analysis.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 157

Comparisons between groups: For all endpoints, differences between groups were
analyzed by using a paired Student’s t-test for the parametric variables and unpaired
Mann-Whitney for the non parametric ones, respectively. P-values were considered
significant if <0.05.
Results:
A total of 92 patients were considered for the study period, 17 of which did not
meet the inclusion criteria. Seventy five patients (26 females) with a mean age of
61,8±17,3 years old were randomized, 40 to control group and 35 to the study group.
Baseline characteristics at baseline were similar in both groups, as well as the reasons
for MV. Demographic data and patients characteristics at the entry of the study are
listed in Table 1.
In the 48 hours post- extubation, 20 controls (50%) and 14 study patients (40%)
used NIV. Considering this sub-group of patients, the re-intubation rates related to NIV
failure were significantly lower in the study group when compared to controls; 2
patients (6%) vs 13(33%), p<0.05, respectively.
Outcomes of both patients groups in the first 48 hours post-extubation and ICU
length of stay data are listed in Table 2. When compared to controls, both duration of
invasive mechanical ventilation and post – extubation ICU length of stay were shorter
by 6 days (p<0,05), and reintubation rate was lower (17% vs 48%) in the study group.
There were no significant differences in total ICU length of stay
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
158 Miguel Ramalho do Souto Gonçalves

Discussion:
The results found in this trial suggest that secretion management with MI-E may
work as a useful complement technique to treat patients who develop ARF in the first
48 hours post-extubation. The use of MI-E had a stronger impact in preventing re-
intubation in the group of patients that required NIV, as shown by the lower NIV failure
rates in the patients that were submitted to MI-E.
Significant debate still exists concerning the precise indications and efficacy of
NIV in this patient population[29] without any mention to the problem of impaired
airway secretion.
The randomized controlled studies performed by Esteban et al [21]. and Keenan
et al[20]. concluded that NIV is not efficient in reducing re-intubation rates, duration of
invasive mechanical ventilation and ICU and hospital length of stay. None of these
studies showed improvement in survival in patients that used NIV in addition to SMT.
On the contrary, the trials conducted by Nava et al.[30] and Ferrer et al.[15] showed that
NIV could prevent ARF after extubation. Several reasons may explain these differences.
First, whereas the studies by Keenan et al[20] and Esteban et al[21] applied NIV after
patients had developed symptoms of respiratory failure, the studies by Nava et al[30]
and Ferrer et al[15] previously identified the high-risk patients and applied NIV
immediately after extubation. As longer time from extubation to re-intubation is
associated with worse outcome[31], delay in re-intubation correlates with worse
survival rates in patients who received NIV for established post-extubation respiratory
failure[20-21]. Thus, the early application of NIV seems crucial to avoid respiratory
failure after extubation, and consequently re-intubation. Second, a significantly higher
proportion of patients with chronic respiratory disorders were included in the studies
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 159

that used early NIV in high risk patients, whereas the NIV post-extubation respiratory
failure trials enrolled only 10–11% of patients with chronic pulmonary disease and used
different definitions for post-extubation respiratory failure.
In our study, both study and control groups included 20% of patients with
chronic respiratory disorders, and all patients were closely monitored during the first 48
hours for early detection of signs and symptoms that indicated post-extubation
respiratory failure. Similarly Esteban et al.[21] and Keenan et al.[20] NIV was only
applied after the development of those symptoms according to specific criteria.
However, in our study NIV was applied in both study group patients and controls and
only MI-E application was considered an independent variable.
Secretion encumbrance with impaired airway clearance has been considered an
independent factor for extubation failure[32], and associated to NIV failure both in
persistent weaning[19] and in post-extubation failure[21] patients. While it is relatively
easy managing secretions through an endotracheal tube, it can be a serious problem
after extubation and specially during NIV. Deep airway suction suctioning through the
tube is a strategy most commonly used by nursing staff to manage secretions while
patients are on invasive MV, however it can be traumatic, difficult to perform and often
ineffective in the extubated patients since it must be performed blindly through the nose
or the mouth.
This study randomly used MI-E (CoughAssistTM, Phillips Respironics
International Inc., Murrysville, Pa) pre- extubation via invasive tube and post-
extubation through oronasal interface at sufficient inspiratory and expiratory pressures
(minimum of 40 to -40 cm H2O) to fully expand and then fully empty the adult lungs in
6-8 seconds, thereby expelling airway secretions while avoiding both hyper and
hypoventilation. The ability to use MI-E through the endotracheal tube immediately
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
160 Miguel Ramalho do Souto Gonçalves

before extubation was the main intervention that permitted the study group patients to
minimize the risk of post-extubation secretion encumbrance and, together with its 3
time daily noninvasively application, may have had influence on the reduction of re-
intubation and NIV failure rates.
Although MI-E has been described as a very efficient technique in the acute
setting for patients with neuromuscular disease (NMD), in the treatment of respiratory
failure due to upper respiratory tract infections[27], to avoid intubation[33] and to
facilitate extubation, decannulation and prevent post-extubation failure[34-36], the
evidence supporting the role of this technique in this other critical ill patient population
is lacking. Indeed, this study is the first randomized controlled trial focused on MI-E in
critical care.
The fact that there is strong evidence on the efficacy of MI-E in critically ill
patients with NMD, and the authors´ positive experience with this technique in this
patient population, was the ethical reasons to exclude them from the study. In fact, our
group recently reported a 97% extubation success to full-setting noninvasive ventilation
(NIV) and MI-E in 157 NMD patients who had previously failed extubations and/or
SBTs [37].
Potential limitations have to be taken into account when analyzing the
differences between the two groups. First, although there were no significant differences
in baseline characteristics at the entry of the study between the two groups hypoxemic
respiratory failure was slightly more frequent in group A and this may had impact on
the NIV failure rate in this patient group, since NIV is more likely to fail when severe
hypoxia is present[38]. Second, 6 controls and 4 study group patients were re-intubated
immediately with no indication for NIV. This fact was associated with causes that could
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 161

not be solved by MI-E, since cooperation with the technique is crucial in extubated
patients.
Another potential limitation of this type of open clinical trials is the difficulty for
a correct blinding of the investigators that might lead to possible bias. Despite the fact
that we predefined the criteria for all relevant interventions and clinical decisions to be
made by the attending physicians, as well as the outcome variables, this bias could not
be entirely controlled.
Thus, our results recommend that MI-E for secretion clearance should be
included in an extubation protocol in specific subgroups of patients that may require
post-extubation NIV. However, because of the paucity of data, and the fact that this is a
pilot study performed in a center highly experienced with MI-E, more studies are
required to settle the issue.
Acknowledgments:
The authors wish to thank all medical and nursing staffs of the emergency
department ICU of our institution, for their motivation, assistance and support in
managing the patients according to the trial.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
162 Miguel Ramalho do Souto Gonçalves

Table 1 – Baseline characteristics of patients at entry into the study Group A
(n = 40)
Group B (MI-E) (n=35)
p
Age (years) 62±19,2 61,4±15,1 NS
Sex (M/F) 21/19 28/7 NS
SAPS II 47,8±17,7 45±15 NS
Duration of MV (days) 9,4±4,8 10,5±4,1 NS
Patients with chronic pulmonary disorders (n,%)
9(23%) 7 (20%) NS
Patients with hypoxemic respiratory failure (n,%) Reasons of MV (n)
24 (60%) 18(52%) NS
COPD exacerbations 6 4
Congestive heart failure 5 4
Community – acquired pneumonia 11 6
Hospital – acquired pneumonia Postoperative respiratory failure Acute lung injury Thoracic trauma Sepsis Cardiac arrest
-- 5 --
6 7 --
2 8 1
3 4 3
Data is Data presented as mean ± standard deviation Legend- SAPS II - New Simplified Acute Physiology Score; MV – mechanical ventilation; COPD –chronic obstructive pulmonary disease; NS – Non significant
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 163

Table 2 – Post-extubation outcomes data Group A
(n = 40)
Group B (MI-E) (n=35)
NIV application, n (%) Reasons for NIV (n)
20 (50%) 14 (40%)
Respiratory Rate > 35bpm 5 (25%) 9 (64%)
SpO2 < 90% 4(20%) 1(7%)
20% variation of HR or BP 1(5%) -----
PaO2<60; PaCO2>45
10(50%) 4 (29%)
Total period of MV (days)
17,8±6,4* 11,7±3,5*
Patients re-intubated (n,%)
Causes of re-intubation (n)
19 (48%) * 6 (17%) *
Respiratory pauses with loss of consciousness --- 1
Respiratory distress after 2h NIV 6 2
Decreasing level of consciousness 2 --
Intolerance to NIV Hypotension (systolic BP< 90 mm Hg for more than 30 minutes) Secretion encumbrance associated with severe hypoxemia.. NIV failure rate, n (%) Total ICU length of stay Post-extubation ICU length of stay
2
---
9
13 (65%) *
19,3±8,1
9,8±6,7*
--
1
2
2 (14%) *
16,9±11,1
3,1±2,5*
Data is Data presented as mean ± standard deviation Legend- NIV – Noninvasive ventilation; APS II - New Simplified Acute Physiology Score; MV – mechanical ventilation; COPD –chronic obstructive pulmonary disease; NS – Non significant
*- p<0,05
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
164 Miguel Ramalho do Souto Gonçalves

References: 1. Boles JM, Bion J, Connors A, Herridge M, Marsh B, Melot C, Pearl R,
Silverman H, Stanchina M, Vieillard-Baron A, Welte T: Weaning from mechanical ventilation. Eur Respir J 2007, 29:1033-1056.
2. MacIntyre NR, Cook DJ, Ely EW, Jr., Epstein SK, Fink JB, Heffner JE, Hess D, Hubmayer RD, Scheinhorn DJ: Evidence-based guidelines for weaning and discontinuing ventilatory support: a collective task force facilitated by the American College of Chest Physicians; the American Association for Respiratory Care; and the American College of Critical Care Medicine. Chest 2001, 120:375S-395S.
3. Smina M, Salam A, Khamiees M, Gada P, Amoateng-Adjepong Y, Manthous CA: Cough peak flows and extubation outcomes. Chest 2003, 124:262-268.
4. Nakagawa NK, Franchini ML, Driusso P, de Oliveira LR, Saldiva PH, Lorenzi-Filho G: Mucociliary clearance is impaired in acutely ill patients. Chest 2005, 128:2772-2777.
5. Templeton M, Palazzo MG: Chest physiotherapy prolongs duration of ventilation in the critically ill ventilated for more than 48 hours. Intensive
Care Med 2007, 33:1938-1945. 6. Rello J, Paiva JA, Baraibar J, Barcenilla F, Bodi M, Castander D, Correa
H, Diaz E, Garnacho J, Llorio M, et al: International Conference for the Development of Consensus on the Diagnosis and Treatment of Ventilator-associated Pneumonia. Chest 2001, 120:955-970.
7. Isakow W, Kollef MH: Preventing ventilator-associated pneumonia: an evidence-based approach of modifiable risk factors. Semin Respir Crit Care
Med 2006, 27:5-17. 8. Girou E, Schortgen F, Delclaux C, Brun-Buisson C, Blot F, Lefort Y,
Lemaire F, Brochard L: Association of noninvasive ventilation with nosocomial infections and survival in critically ill patients. Jama 2000, 284:2361-2367.
9. Rello J, Ollendorf DA, Oster G, Vera-Llonch M, Bellm L, Redman R, Kollef MH: Epidemiology and outcomes of ventilator-associated pneumonia in a large US database. Chest 2002, 122:2115-2121.
10. Meade M, Guyatt G, Cook D, Griffith L, Sinuff T, Kergl C, Mancebo J, Esteban A, Epstein S: Predicting success in weaning from mechanical ventilation. Chest 2001, 120:400S-424S.
11. Frutos-Vivar F, Ferguson ND, Esteban A, Epstein SK, Arabi Y, Apezteguia C, Gonzalez M, Hill NS, Nava S, D'Empaire G, Anzueto A: Risk factors for extubation failure in patients following a successful spontaneous breathing trial. Chest 2006, 130:1664-1671.
12. Capdevila X, Perrigault PF, Ramonatxo M, Roustan JP, Peray P, d'Athis F, Prefaut C: Changes in breathing pattern and respiratory muscle performance parameters during difficult weaning. Crit Care Med 1998, 26:79-87.
13. Ferrer M, Bernadich O, Nava S, Torres A: Noninvasive ventilation after intubation and mechanical ventilation. Eur Respir J 2002, 19:959-965.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 165

14. Salam A, Tilluckdharry L, Amoateng-Adjepong Y, Manthous CA: Neurologic status, cough, secretions and extubation outcomes. Intensive
Care Med 2004, 30:1334-1339. 15. Ferrer M, Valencia M, Nicolas JM, Bernadich O, Badia JR, Torres A:
Early noninvasive ventilation averts extubation failure in patients at risk: a randomized trial. Am J Respir Crit Care Med 2006, 173:164-170.
16. Girault C, Daudenthun I, Chevron V, Tamion F, Leroy J, Bonmarchand G: Noninvasive ventilation as a systematic extubation and weaning technique in acute-on-chronic respiratory failure: a prospective, randomized controlled study. Am J Respir Crit Care Med 1999, 160:86-92.
17. Burns KE, Adhikari NK, Meade MO: Noninvasive positive pressure ventilation as a weaning strategy for intubated adults with respiratory failure. Cochrane Database Syst Rev 2003:CD004127.
18. Nava S, Ambrosino N, Clini E, Prato M, Orlando G, Vitacca M, Brigada P, Fracchia C, Rubini F: Noninvasive mechanical ventilation in the weaning of patients with respiratory failure due to chronic obstructive pulmonary disease. A randomized, controlled trial. Ann Intern Med 1998, 128:721-728.
19. Ferrer M, Esquinas A, Arancibia F, Bauer TT, Gonzalez G, Carrillo A, Rodriguez-Roisin R, Torres A: Noninvasive ventilation during persistent weaning failure: a randomized controlled trial. Am J Respir Crit Care Med
2003, 168:70-76. 20. Keenan SP, Powers C, McCormack DG, Block G: Noninvasive positive-
pressure ventilation for postextubation respiratory distress: a randomized controlled trial. Jama 2002, 287:3238-3244.
21. Esteban A, Frutos-Vivar F, Ferguson ND, Arabi Y, Apezteguia C, Gonzalez M, Epstein SK, Hill NS, Nava S, Soares MA, et al: Noninvasive positive-pressure ventilation for respiratory failure after extubation. N Engl J Med
2004, 350:2452-2460. 22. Hilbert G, Gruson D, Portel L, Gbikpi-Benissan G, Cardinaud JP:
Noninvasive pressure support ventilation in COPD patients with postextubation hypercapnic respiratory insufficiency. Eur Respir J 1998, 11:1349-1353.
23. McCool FD, Rosen MJ: Nonpharmacologic airway clearance therapies: ACCP evidence-based clinical practice guidelines. Chest 2006, 129:250S-259S.
24. Chaisson KM, Walsh S, Simmons Z, Vender RL: A clinical pilot study: high frequency chest wall oscillation airway clearance in patients with amyotrophic lateral sclerosis. Amyotroph Lateral Scler 2006, 7:107-111.
25. Bellone A, Spagnolatti L, Massobrio M, Bellei E, Vinciguerra R, Barbieri A, Iori E, Bendinelli S, Nava S: Short-term effects of expiration under positive pressure in patients with acute exacerbation of chronic obstructive pulmonary disease and mild acidosis requiring non-invasive positive pressure ventilation. Intensive Care Med 2002, 28:581-585.
26. Vargas F, Bui HN, Boyer A, Salmi LR, Gbikpi-Benissan G, Guenard H, Gruson D, Hilbert G: Intrapulmonary percussive ventilation in acute exacerbations of COPD patients with mild respiratory acidosis: a randomized controlled trial [ISRCTN17802078]. Crit Care 2005, 9:R382-389.
27. Vianello A, Corrado A, Arcaro G, Gallan F, Ori C, Minuzzo M, Bevilacqua M: Mechanical insufflation-exsufflation improves outcomes for
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
166 Miguel Ramalho do Souto Gonçalves

neuromuscular disease patients with respiratory tract infections. Am J Phys
Med Rehabil 2005, 84:83-88; discussion 89-91. 28. Esteban A, Alia I, Tobin MJ, Gil A, Gordo F, Vallverdu I, Blanch L, Bonet
A, Vazquez A, de Pablo R, et al: Effect of spontaneous breathing trial duration on outcome of attempts to discontinue mechanical ventilation. Spanish Lung Failure Collaborative Group. Am J Respir Crit Care Med
1999, 159:512-518. 29. Agarwal R, Aggarwal AN, Gupta D, Jindal SK: Role of noninvasive
positive-pressure ventilation in postextubation respiratory failure: a meta-analysis. Respir Care 2007, 52:1472-1479.
30. Nava S, Gregoretti C, Fanfulla F, Squadrone E, Grassi M, Carlucci A, Beltrame F, Navalesi P: Noninvasive ventilation to prevent respiratory failure after extubation in high-risk patients. Crit Care Med 2005, 33:2465-2470.
31. Epstein SK, Ciubotaru RL: Independent effects of etiology of failure and time to reintubation on outcome for patients failing extubation. Am J Respir
Crit Care Med 1998, 158:489-493. 32. Khamiees M, Raju P, DeGirolamo A, Amoateng-Adjepong Y, Manthous
CA: Predictors of extubation outcome in patients who have successfully completed a spontaneous breathing trial. Chest 2001, 120:1262-1270.
33. Servera E, Sancho J, Zafra MJ, Catala A, Vergara P, Marin J: Alternatives to endotracheal intubation for patients with neuromuscular diseases. Am J
Phys Med Rehabil 2005, 84:851-857. 34. Bach JR, Goncalves M: Ventilator weaning by lung expansion and
decannulation. Am J Phys Med Rehabil 2004, 83:560-568. 35. Bach JR, Saporito LR: Criteria for extubation and tracheostomy tube
removal for patients with ventilatory failure. A different approach to weaning. Chest 1996, 110:1566-1571.
36. Bach JR: Inappropriate weaning and late onset ventilatory failure of individuals with traumatic spinal cord injury. Paraplegia 1993, 31:430-438.
37. Bach JR, Goncalves MR, Hamdani I, Winck JC: Extubation of patients with neuromuscular weakness: a new management paradigm. Chest 2010, 137:1033-1039.
38. Antonelli M, Conti G, Moro ML, Esquinas A, Gonzalez-Diaz G, Confalonieri M, Pelaia P, Principi T, Gregoretti C, Beltrame F, et al: Predictors of failure of noninvasive positive pressure ventilation in patients with acute hypoxemic respiratory failure: a multi-center study. Intensive
Care Med 2001, 27:1718-1728.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 167

Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
168 Miguel Ramalho do Souto Gonçalves

Study 4
A Ventilator Requirement Index
John R. Bach, Miguel R. Gonçalves, Yuka Ishikawa, Michal Eisenberg, João Carlos Winck , Eric Altschuler
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 169

Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
170 Miguel Ramalho do Souto Gonçalves

Authors:
John R. Bach, MDMiguel Goncalves, RTMichal Eisenberg, MDYuka Ishikawa, MDEric Altschuler, MDJoao Carlos Winck, MD, PhDEugene Komaroff, PhD
Affiliations:
From the Department of PhysicalMedicine and Rehabilitation,UMDNJ–New Jersey Medical School,Newark, New Jersey (JRB, ME, EA,EK); Hospital Universitario de SanJoao, Porto, Portugal (MG, JCW); andDepartment of Pediatrics, YakumoByoin National Sanatorium,Hokkaido, Japan (YI).
Correspondence:
All correspondence and requests forreprints should be addressed to JohnR. Bach, MD, Department of PhysicalMedicine and Rehabilitation,University Hospital B-403, 150Bergen St., Newark, NJ 07103.
0894-9115/08/8703-0001/0
American Journal of Physical
Medicine & Rehabilitation
Copyright © 2008 by Lippincott
Williams & Wilkins
DOI: 10.1097/PHM.0b013e318164a96e
A Ventilator Requirement Index
ABSTRACT
Bach JR, Goncalves M, Eisenberg M, Ishikawa Y, Altschuler E, Winck JC,Komaroff E: A ventilator requirement index. Am J Phys Med Rehabil 2008;87:000–000.
Objective: To determine the efficacy of vital capacity (VC) and aproposed ventilator requirement index (VRI) for justifying ventilator pre-scription and use for patients with neuromuscular/chest wall diseases(NMD).
Design: Prospective observational study in which 319 patients withNMD, including 187 ventilator users, were separated into four groups:(1) asymptomatic, (2) abnormal specific screening factors and/or symp-tomatic, (3) ventilator use 8–20 hrs/day, and (4) �20 hrs/day ofventilator use. The VRI was defined as 60 � Ti/(Ttot)2
� (Vt/VC) � RR,where Ti � inspiratory time of one breath (secs), Ttot � total time of onebreath (secs), Vt � tidal volume (ml) at rest, VC � vital capacity (ml), andRR � respiratory rate.
Results: The overall analysis of variance F-tests and post hoc pairwisecontrasts were significant (P � 0.001) for differences in the VC and VRIacross groups. Thus, VC and VRI are independent predictors of groupmembership. Satisfying VC or VRI criteria signaled the highest number ofpatients benefiting from ventilator use.
Conclusions: The prescription of one or two ventilators can be justifiedby both VC and VRI, with the combination being most sensitive.
Key Words: Ventilator Requirement Index, Noninvasive Mechanical Ventilation, Respi-
ratory Insufficiency, Home Mechanical Ventilation, Neuromuscular Disease
When a patient is not able to fully sustain the muscular work of breathingto maintain normal alveolar ventilation in the presence of increasing ventilatoryload or decreasing work capacity, muscle fatigue can only be averted by symp-tomatic hypoventilation or by ventilatory assistance. Bellemare and Grassino1
examined the effects of the tension time index of the diaphragm (TTIdi) oninspiratory muscle endurance and fatigue. They define the point at which atarget tension could no longer be sustained as the Tlim. In the case of thediaphragm, there are two main factors influencing Tlim or muscle fatigue. They
March 2008 Ventilator Requirement Index 1
ORIGINAL RESEARCH ARTICLE
Pulmonary
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 171

are the product of the TTIdi or the product of thefraction of time that the inspiratory muscles spendin contraction (Ti/Ttot) (the duty cycle of the in-spiratory muscles), and the ratio of the tensiongenerated at each contraction (Pdi) to the maxi-mum Pdi that can be achieved during a near iso-metric contraction (PdiMax). Thus, TTIdi � (Ti/Ttot) � (Pdi/PdiMax). Tlim is the percentage ofTTIdi such that effective diaphragm contraction isnot sustainable. Because the diaphragm contractsmainly during inspiration, it should fatigue morerapidly at any given tension if Ti/Ttot is abnormallyincreased. It should also fatigue more rapidly at anygiven Ti/Ttot if the Pdi/PdiMax ratio increases withadvancing inspiratory muscle weakness/dysfunc-tion. Bellemare and Grassino1 report that the Tlimfor patients with chronic obstructive pulmonarydisease is (TTIdi equal to) 0.12. That is, with TTIdigreater than this, chronic obstructive pulmonarydisease patients’ respiratory muscles fatigue. TTIdi �
0.15–0.2 was reported as “the critical zone forfatigue” in that fatigue could occur in less than 1hr at this TTIdi level. Thus, diaphragm (inspiratorymuscle) endurance could be predicted by the TTIdi.However, determining TTIdi requires placement ofan esophageal balloon to measure Pdi and PdiMax.This makes it impractical for general use.
We have already demonstrated that tidal vol-ume (Vt)/vital capacity (VC) can substitute for Pdi/PdiMax, because the more Vt approaches VC, theless ability the inspiratory muscles have to sustainalveolar ventilation.1 Our previous data, on pre-dominantly chronic obstructive pulmonary diseasepatients, suggest that a breathing intolerance indexusing Vt/VC can supplement VC criteria to helpgauge the need for ventilator use by reflectingventilatory reserve.1 Subsequently, we hypothe-sized that the index might better correlate withsymptomatic inspiratory muscle dysfunction if itreflected ongoing inspiratory muscle action ratherthan effort over only one breath cycle. Thus, wemultiplied the index (Ti/Ttot � Vt/VC) by respira-tory rate, or 60 � Ti/(Ttot)2
� Vt/VC (an equivalentequation), to define a new ventilator requirementindex (VRI). The purpose of this study was to de-termine whether this VRI could distinguish pa-tients with neuromuscular diseases (NMD) withvarious levels of inspiratory muscle dysfunctionand need for ventilator use, and whether such anindex could add to the efficacy of simple VC mea-surement in indicating the extent of the need forventilator use.
MATERIALS AND METHODS
This was a prospective analysis of data gath-ered on 332 consecutively referred patients withNMDs. It was approved by our institutional reviewboards. Three hundred nineteen of the 332 could
achieve steady-state breathing sufficiently for sixbreaths to be averaged for data analysis, and 13 couldnot (were continuously ventilator dependent). Of the319, there were 187 males and 132 females, 36.8 �
19.1 yrs of age. They had the following diagnoses:Duchenne muscular dystrophy, 90 (mean age 22.7range 9–45); non-Duchenne myopathy, 83 (meanage 28.8, range 13–78); amyotrophic lateral sclerosis,64 (mean age 56.3, range 19–84); spinal muscularatrophy, 25 (mean age 25.3, range 16–53); postpolio-myelitis, 18 (mean age 60.9, range 44–77); myotonicdystrophy, 13 (mean age 38.3, range 29–48); spinalcord injury, 11 (mean age 28.8, range 18–52); myas-thenia gravis, 6 (mean age 42.8, range 31–58); mul-tiple sclerosis, 5 (mean age 48.1, range 34–59); Char-cot–Marie–Tooth disease, 2 (ages 57 and 42); andmiscellaneous, 15 (mean age 37, range 18–85).
All of the patients underwent evaluation forspecific ventilator need–screening factors, whichincluded symptoms of inspiratory muscle dysfunc-tion (chronic alveolar hypoventilation) as previ-ously published,2 recent or increasing fatigue, dys-pnea at rest (especially on waking), morningheadaches, nocturnal arousals associated with dys-pnea/tachycardia or urination, difficulty arousingin the morning, difficulty in getting to sleep, hy-persomnolence or need for multiple naps, impair-ment of concentration, nightmares, signs of right-heart failure, anxiety, depression, and weightchange. Dyspnea caused by walking or stair climb-ing was excluded because most patients werewheelchair dependent, because ambulation re-quires much greater minute ventilation than mostactivities from a wheelchair, and because nocturnalnoninvasive mechanical ventilation (NIV) has notbeen reported to relieve exertional dyspnea.
Other abnormal screening factors were derivedfrom spirometry (Wright spirometer, Mark 14, Fer-raris Development and Engineering Co., Ltd, Lon-don), end-tidal CO2 levels (Microspan 8090 capno-graph, Biochem International, Waukesha, WI), andpulse oximetry (SpO2) (Ohmeda Model #3760oximeter, Louisville, CO). They were VC measuredin a sitting position less than 50% of predictednormal (Medicare standard), VC sitting/VC supineratio greater than 1.2 (normal ratio �1.07), diur-nal end-tidal carbon dioxide (CO2) greater than 44mm Hg, diurnal pulse oxyhemoglobin saturation(SpO2) decreasing to less than 95%, and ventilator-free breathing ability �10 mins in any position.The VC was recorded as the maximum observed infive or more attempts. The American Academy ofRespiratory Care Clinical Practice Guidelines werefollowed.3 The VC percentage of predicted normalwas calculated as 100 times the VC (ml) divided bythe predicted normal VC (ml), using the Baldwinformula: males’ predicted VC (liters) � [27.63 �
0.112 � age] � height (cm)/1000; females’ pre-
2 Bach et al. Am. J. Phys. Med. Rehabil. ● Vol. 87, No. 3
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
172 Miguel Ramalho do Souto Gonçalves

dicted VC (liters) � [21.78 � 0.101 � age] �
height (cm)/1000.4 For patients with scoliosis, armspan was used rather than height.5 Some question-ably symptomatic patients, especially those using ac-cessory breathing muscles and not having clearsymptoms or other abnormal screening factors, un-derwent polysomnography (13%) or nocturnal oxim-etry and end-tidal CO2 monitoring (33%). Sleep end-tidal CO2 maximum �50 mm Hg, nocturnal SpO2
decreases � 95% at least four times per hour or 10mins or more total during the night, and apnea/hypopnea index �10/hr on polysomnography wereconsidered abnormal screening factors.
The VRI was determined by Meteor digitalspirometer with a liquid crystal diode monitor(Cardio-Pulmonary Technologies Inc.), usingcustom-prepared software to analyze flow andvolume signals on a Windows-based personalcomputer (FMV-660MC/W, A Fujitsu Corp., To-kyo, Japan). The computer selected the six mostconsistent consecutive Vt waveforms with thepatient sitting at rest, and it averaged them forthe Ti, Ttot, and Vt data.
Group 1 patients were asymptomatic and hadno abnormal specific screening factors. Group 2patients had one or more abnormal screening fac-tors. Forty-two of 97 patients were clearly and 55were questionably symptomatic for hypoventila-tion. Group 3 patients depended on ventilator use8–20 hrs/day for symptomatic relief (Fig. 1). Group4 patients required ventilatory assistance aroundthe clock (Fig. 2).
The four respiratory impairment categorieswere correlated with VRI and VC in the sittingposition, using Spearman correlation coefficients.The VC was transformed into natural logarithmbecause the standard deviations seemed to corre-late with means, and residuals from the analysis ofvariance model were obviously skewed. The Tukey–Kramer post hoc adjustment for multiple compar-isons was used to protect �. � 0.05 for statisticalsignificance. Data on 25 historical normals from a
previous study, age 33.9 � 8.5 yrs, were also mul-tiplied by their respiratory rates and were consid-ered for comparison.6
RESULTS
The VRI and VC of 25 historical normals(group 0) and our group 1–4 subjects are shown inTable 1 and 2. The overall analysis of varianceF-tests and post hoc pairwise contrasts were signif-icant (P � 0.001) for all intergroup pairwise com-parisons for both VC and VRI. Thus, VC and VRIwere both independent, significant predictors ofgroup membership (P � 0.001, P � 0.0016, respec-tively). On the basis of Spearman correlation coef-ficients, the four respiratory impairment categoriescorrelated significantly with VRI (rS � 0.05, P �
0.001) and VC (rS � �0.55, P � 0.001) in thesitting position.
The Medicare ventilator prescription criterionof VC �50% captured 82 of 97 (85%) group 2patients but also 12 of 35 (35%) group 1 members.Having a VRI index �1.2 captured 89 of 97 (92%)of group 2 and 16 of 35 (46%) group 1 members. AtVRI �1.3, these figures were 87/97 (90%) and11/35 (31%), respectively; at VRI �1.1, 91/97(94%) and 17/35 (49%), respectively; and at 0.9,93/97 (96%) and 23/35 (66%), respectively. Sensi-tivity is more important than specificity becauseventilator prescription indication parameters needto support ventilator use for patients who can ben-efit from it, whereas patients who do not benefitsufficiently to offset the inconvenience and dis-comfort of ventilator use are unlikely to useventilators, irrespective of parameter values.Thus, a VRI of 1–1.2 or greater may be useful tojustify initial ventilator prescription, whether byvolume-limited or pressure-limited ventilatorssuch as bilevel positive airway pressure devices.
FIGURE 1 Patient with Duchenne muscular dystro-
phy using nasal ventilation.
FIGURE 2 Patient with amyotrophic lateral sclerosis
dependent on continuous noninvasive
mechanical ventilation support uses a
15-mm angled mouthpiece for diurnal
ventilatory support (shown here) and a
nasal interface for nocturnal support.
March 2008 Ventilator Requirement Index 3
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 173

VRI �1.2 or VC �50% of predicted normal cap-tured 92 of 97 (95%) of group 2 members. Thisincluded 18 patients with initially questionablesymptoms who, after a trial of NIV, appreciatedsufficient benefit on fatigue and other mildsymptoms to go on using it.
Of the group 3 ventilator users, 91 were usingsleep-only NIV, and 54 were using NIV into daytimehours up to 20 hrs/day. Twenty-one patients hadVC greater than 50% in the sitting position but stillrequired nocturnal NIV. For all group 3 patients,except the 13 with myotonic dystrophy, symptomswere relieved, and normal daytime end-tidal CO2
and SpO2 were maintained early on with nocturnalventilator use. The myotonic dystrophy patientstended to use nocturnal NIV sporadically and rarelythroughout sleep. The NMD patients who eventu-ally required more than nocturnal-only NIV oftenspontaneously used it into daytime hours, usuallyvia 15-mm angled mouth pieces (Fig. 2), until theyrequired it around the clock (group 4). They oftenused oximetry as feedback to use diurnal NIV suf-ficiently to maintain sufficient alveolar ventilationto maintain SpO2 �95%.
Whereas all of the group 4 patients were es-sentially continuous NIV users, they had sufficientbreathing autonomy to establish six consistent Vtfor a 2-min period of ventilator-free breathing.Considering Figure 3 for group 4, for whom itcould be argued that a back-up (daytime use)ventilator is warranted, 37 of the 42 were cap-tured by the criterion of VC �1100 ml (88%),with 109 of 277 also meeting this criterion ingroups 1 through 3 (39%) (specificity 100 � 39,or 61%). At VC �1000, these figures were 34/42and 99/277 (39%), respectively; at VC �800 ml,they were 33/42 and 76/277 (27%), respectively;and at 1200 ml, they were 38/42 and 120/277(43%), respectively. Considering that sensitivityis more important than specificity when consid-ering the safety afforded by having a back-upventilator for around-the-clock users, and thatless severely affected (with higher VC and lowerVRI) continuous ventilator users can survivelonger breathing autonomously or using a manualresuscitator or glossopharyngeal breathing in the
event of ventilator failure than the more severelyaffected (lower VC and higher VRI) patients, itseems that a VC of 1100 ml (capturing 88% ofgroup 4 membership) as opposed to a VC of 1000(capturing 81% with slightly higher specificity)might be the more appropriate threshold to sup-port prescription of a second ventilator. Similarly,a VC of 700 ml (point at which the sensitivity andspecificity lines cross on Fig. 3) strongly supportsprescription of a second ventilator. Likewise, bysimilar analysis of Figure 4, a VRI of 2.4 captures34 of 42 (81%) group 4 members and 125 of 277(45%) group 1–3 patients. At a VRI of 2.2, sensi-tivity is unchanged (36/42) and specificity de-creases, with 145/277 meeting the criterion (57%).At VRI � 3.3, the point at which sensitivitytransects specificity in Figure 4, 31/42 (74%) group4 and only 63/277 (23%) group 1–3 patients meetthe criterion. This level might be considered tostrongly support prescription of a second ventila-tor. Having a VRI �2.4 or VC �1100 captured 39 ofthe 42 (93%) group 4 patients.
In addition to the group 4 patients, 13 othersrequired continuous ventilatory support but couldnot breathe long enough for the computer to es-tablish a VRI by analyzing six consistent breaths.These patients either could not complete the studyor, in three cases, had VRI �2.0 because Vt valueswere unsustainably low for steady-state analysis.
DISCUSSION
Third-party payors demand justification forthe prescription of both initial and secondary ven-tilators. Decisions about ventilator use have beenlargely based on the results of polysomnograms,pulmonary function testing, and arterial bloodgases. However, daytime arterial blood gases maybe normal despite symptomatic nocturnal hy-poventilation, and 30% of patients hyperventilatefrom the pain of arterial puncture, so normalPaCO2 may need to be corrected for pH for evi-dence of hypercapnia.7 Further, conventionalpulmonary function testing, including forced expi-ratory flows and volumes, is designed for patientswith lung and airway diseases, rather than muscleweakness and hypoventilation. The VC measured
TABLE 1 Spirometric and ventilator use data
Group n Age Mean vital capacity, ml Percent vital capacity Hvuse per day, hrs
0* 25 33.9 � 8.5 3680.4 � 860.5 106.6 � 13.7 01 35 37.7 � 17.5 2735.7 � 1174.5 79.3 � 17.9 02 97 31.5 � 20.0 1499.3 � 697.2 43.2 � 12.1 03 145 40.6 � 19.2 1184.1 � 799.7 38.1 � 13.0 9.65 � 4.34 42 35.2 � 15.1 550.3 � 547.8 15.8 � 9.1 23.3 � 1.1
Hvuse, home ventilator use in hours per day. * Historical controls.14
4 Bach et al. Am. J. Phys. Med. Rehabil. ● Vol. 87, No. 3
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
174 Miguel Ramalho do Souto Gonçalves

with the patient supine is not part of routine pul-monary function testing, but it reflects diaphragmweakness better than the VC measured in the sit-ting position. In a recent study, supine VC �75% ofpredicted normal was 100% sensitive and specificfor predicting an abnormally low Pdi.8 Patients canhave VC levels that approach normal when sittingbut that are less than 50% of normal, and thesepatients might have no ability to breathe whensupine. The inaccuracy of considering VC alone,especially in the sitting position, to indicate venti-lator use has already been reported.4 Accessorymuscle use and abdominal paradox were also bothsignificantly negatively associated with Pdi, and thepresence of accessory muscle use had a sensitivityof 84% and a specificity of 100% for detecting alow Pdi,8 but these signs are not quantitative indi-cations for ventilatory assistance. Numeric param-eters such as respiratory rate, rapid shallow breath-ing index, maximal inspiratory pressure, andPaCO2 have been offered as indicators for noctur-nal NIV, but they have been unreliable.9 CurrentMedicare guidelines for ventilator use mandate aVC �50% of predicted normal, yet there are pa-tients with NMDs who have 10% or less of pre-dicted normal VC who are eucapnic and whobreathe asymptomatically unaided, and there areothers with �70% of predicted normal VC whorequired continuous ventilatory support.10–12
Although polysomnography has become popu-lar in the assessment of NMD patients for sleep-disordered breathing,13 polysomnnograms are pro-grammed to interpret all hypopneas and apneas ascentral or obstructive in nature rather than frominspiratory muscle impairment. This often resultsin inappropriate treatment with continuous posi-tive airway pressure or low-span bilevel positiveairway pressure, methods that maintain airway pa-tency but give little or no assistance to inspiratorymuscles. Further, many asymptomatic NMD pa-tients fail to appreciate benefit and do not tolerateNIV despite polysomnographic abnormalities. Poly-somnography is also expensive and inconvenient.
Meeting VRI or VC criteria better indicatesextent of ventilator need by comparison with VC orVRI alone or with other measures. This requiresonly simple spirometry with specific software.Anyone with neuromuscular weakness and symp-toms of alveolar hypoventilation should be offereda trial of NIV. However, a VC �50% or a VRI �1.2supports the justification of a ventilator for noc-turnal use. Patients whose benefit from nocturnalNIV more than offsets the inconvenience of using itare likely to continue use, regardless of whetherthe ventilator is pressure cycled (bilevel positiveairway pressure) or volume cycled. Nasal or oralinterfaces can be used.14 –17 Once a patient re-quires ventilator use �20 hrs/day, a second ven-
TA
BLE
2V
entil
ator
requ
irem
ent
inde
xan
dot
her
pulm
onar
yda
ta
MIP
,cm
H20
RR
,bpm
SpO
2,
%E
tCO
2T
iTit
ot
VT
/VC
Mea
nV
RI
Gro
up
1(n
�35)
�64.1
�100
16.6
�4.5
96.6
�2.3
37.7
�4.4
0.4
2�
0.1
00.1
9�
0.1
61.3
7�
1.4
7G
rou
p2
(n�
97)
�34.9
�28.5
21.5
�5.7
95.7
�3.7
40.1
�6.4
0.4
3�
0.1
50.2
7�
0.1
72.3
6�
1.1
8G
rou
p3
(n�
145)
�20.3
�21.8
22.5
�6.9
94.7
�3.0
41.3
�7.3
0.4
1�
0.0
60.3
6�
2.9
23.6
1�
2.9
2G
rou
p4
(n�
42)
�7.4
�7.1
022.6
�5.4
94.6
�2.6
36.9
�9.1
0.4
3�
0.0
70.5
3�
0.2
35.4
1�
3.0
1
VC
,vi
tal
capac
ity;
MIP
,m
axim
um
insp
irat
ory
pre
ssu
re;
RR
,re
spir
ato
ryra
te;
Sp
O2,
per
cen
to
xyh
emo
glo
bin
satu
rati
on
;E
tCO
2,
end-t
idal
CO
2in
mm
Hg;
TiT
itot,
insp
irat
ory
tim
ediv
ided
by
tota
lbre
ath
tim
e;V
T/V
C,
tidal
volu
me
div
ided
by
VC
;V
RI,
ven
tila
tor
req
uir
emen
tin
dex
.
March 2008 Ventilator Requirement Index 5
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 175

tilator should be prescribed and might be justi-fied by having a VC �1100 ml or VRI �2.5.
A limitation of interpreting these outcomes isthe large number of diagnoses and age rangesstudied. It has been noted that with age, largerabsolute values and percentages of predicted nor-mal VC are needed for one to maintain normalPaCO2 levels.18 Thus, young patients with diag-noses like spinal muscular atrophy type 2 or Duch-enne muscular dystrophy might be expected tomaintain more normal alveolar ventilation at lowerVC levels than older patients with amyotrophiclateral sclerosis or spinal cord injury, for example.Nevertheless, satisfying VC or VRI criteria mayfacilitate ventilator prescription justification tothird-party payors.
REFERENCES
1. Bellemare F, Grassino A: Force reserve of the diaphragm inpatients with chronic obstructive pulmonary disease. J ApplPhysiol 1983;55:8–15
2. Bach JR, Alba AS: Management of chronic alveolar hypoven-tilation by nasal ventilation. Chest 1990;97:52–7
3. American Association for Respirtory Care: Clinical practiceguidelines: static lung volumes: 2001 revision & update.Respir Care 2001;46:531–9
4. Gelinas D: Nocturnal oximetry as an early indicator ofrespiratory involvement in ALS—correlation with FVC plussymptoms and response to NIPPV therapy. Amyotroph Lat-eral Scler Other Motor Neuron Disord 2000;1:38–9
5. Johnson BE, Westgate HD: Methods of predicting vitalcapacity in patients with thoracic scoliosis. J Bone JointSurg (Am) 1970;52A:1433–9
6. Koga T, Watanabe K, Sano M, Ishikawa Y, Bach JR: Thebreathing intolerance index for ventilator use. Am J PhysMed Rehabil 2006;85:24–30
FIGURE 3 The percentage of members of group 4 (sensitivity) vs. group 1, minus the percentage of members of
groups 1–3 (specificity) having vital capacities less than that indicated on the x-axis.
FIGURE 4 The percentage of members of group 4 (sensitivity) vs. 100%, minus the percentage of members of
groups 1–3 (specificity) having ventilator requirement index values (VRI) greater than that indicated
on the x-axis.
6 Bach et al. Am. J. Phys. Med. Rehabil. ● Vol. 87, No. 3
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
176 Miguel Ramalho do Souto Gonçalves

7. Cinel D, Markwell K, Lee R, Szidon P: Variability of therespiratory gas exchange ratio during arterial puncture. AmRev Respir Dis 1991;143:217–8
8. Lechtzin N, Wiener CM, Shade DM, Clawson L, Diette GB:Spirometry in the supine position improves the detection ofdiaphragmatic weakness in patients with amyotrophic lat-eral sclerosis. Chest 2002;121:436–42
9. Pierson DJ: Indication for mechanical ventilation in adultswith acute respiratory failure. Respir Care 2002;47:249–65
10. Wedzicha JA, Muir JF: Noninvasive ventilation in chronicobstructive pulmonary disease, bronchiectasis and cysticfibrosis. Eur Respir J 2002;20:777–84
11. AARC: Consensus statement. Noninvasive positive pressureventilation. Respir Care 1997;42:365–9
12. International Consensus Conferences in Intensive CareMedicine: Noninvasive positive pressure ventilation in acuterespiratory failure. Am J Respir Crit Care Med 2001;163:283–91
13. Chaudhry SS, Bach JR: Management approaches in muscu-lar dystrophy association clinics. Am J Phys Med Rehabil2000;79:193–6
14. Bach JR, Alba AS, Mosher R, Delaubier A: Intermittentpositive pressure ventilation via nasal access in the man-agement of respiratory insufficiency. Chest 1987;92:168–70
15. Ellis ER, Bye PTP, Bruderer JW, Sullivan CE: Treatment ofrespiratory failure during sleep in patients with neuromus-cular disease, positive-pressure ventilation through a nosemask. Am Rev Respir Dis 1987;135:148–52
16. Kerby GR, Mayer LS, Pingleton SK: Nocturnal positivepressure ventilation via nasal mask. Am Rev Respir Dis1987;135:738–40
17. Kirshblum SC, Bach JR: Walker modification for ventilatorassisted individuals. Am J Phys Med Rehabil 1992;71:304–6
18. Bach JR: Noninvasive ventilation: mechanisms for inspira-tory muscle substitution, in Bach JR (ed): NoninvasiveMechanical Ventilation. Philadelphia, Hanley & Belfus,2002, pp 83–102
March 2008 Ventilator Requirement Index 7
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 177

Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
178 Miguel Ramalho do Souto Gonçalves

Study 5
Expiratory Flow Maneuvers of Patients with
Neuromuscular Diseases
John R. Bach, Miguel R. Gonçalves, Sylvia Páez, João Carlos Winck, Sandra Leitão, Paulo Abreu
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 179

Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
180 Miguel Ramalho do Souto Gonçalves

Authors:
John R. Bach, MDMiguel R. Goncalves, BS, PTSylvia Paez, MDJoao Carlos Winck, MD, PhDSandra Leitao, BS, PTPaulo Abreu, BS, PT
Affiliations:
From the Department of PhysicalMedicine and Rehabilitation, UMDNJ–New Jersey Medical School, Newark,New Jersey (JRB); Pulmonology,Fundacion Neumologica Colombiana,Bogota, Colombia (SP); theDepartment of Pulmonary Medicine,Sao Joao University Hospital, Porto,Portugal (MRG, JCW); and thePhysiotherapy Department, Universityof Alcoitao, Estoril, Portugal (SL, PA).
Disclosures:
This work was performed atUniversity Hospital, Newark, NewJersey; Sao Joao University Hospital,Porto, Portugal; and AlcoitaoUniversity, Estoril, Portugal.
Correspondence:
All correspondence and requests forreprints should be addressed to JohnR. Bach, MD, Department of PhysicalMedicine and Rehabilitation,University Hospital B-403, 150Bergen Street, Newark, NJ 07871.
0894-9115/06/8502-0105/0
American Journal of Physical
Medicine & Rehabilitation
Copyright © 2006 by Lippincott
Williams & Wilkins
DOI: 10.1097/01.phm.0000197307.32537.40
Expiratory Flow Maneuvers inPatients with NeuromuscularDiseases
ABSTRACT
Bach JR, Goncalves MR, Paez S, Winck JC, Leitao S, Abreu P: Expiratory flowmaneuvers in patients with neuromuscular diseases. Am J Phys Med Rehabil2006;85:105–111.
Objectives: To compare cough peak flows (CPF), peak expiratoryflows (PEF), and potentially confounding flows obtained by lip and tonguepropulsion (dart flows, DF) for normal subjects and for patients withneuromuscular disease/restrictive pulmonary syndrome and to correlatethem with vital capacity and maximum insufflation capacity.
Design: A cross-sectional analytic study of 125 stable patients and 52normal subjects in which CPF, PEF, and DF were measured by peak flowmeter and vital capacity and maximum insufflation capacity by spirometer.
Results: In normal subjects and in patients, the DF significantly exceededPEF and CPF (P � 0.001). For normal subjects, PEF and CPF were notsignificantly different. For patients with neuromuscular disease/restrictive pul-monary syndrome, the CPF significantly exceeded PEF (P � 0.05). Nonormal subjects but 14 patients had DF lower than CPF. Thirteen of these14 had the ability to air stack (maximum insufflation capacity greater than vitalcapacity), indicating greater compromise of mouth and lip than of glotticmuscles. For 14 of 88 patients, maximum insufflation capacity values did notexceed vital capacity, mostly because of inability to close the glottis (inabilityto air stack). Nonetheless, for 11 of these 14 patients, the DF were withina standard deviation of the whole patient group; thus, bulbar-innervatedmuscle dysfunction was not uniform. CPF and PEF correlated with vitalcapacity (r � 0.85 and 0.86, respectively), and with maximum insufflationcapacity (r � 0.76 and 0.72, respectively).
Conclusions: Measurements of CPF, PEF, and DF are useful forassessing bulbar-innervated, inspiratory, and expiratory muscle function.Care must be taken to not confuse them.
Key Words: Amyotrophic Lateral Sclerosis, Duchenne Muscular Dystrophy, Neuro-
muscular Disease, Cough Peak Flows, Peak Expiratory Flows, Dart Flows, Vital Capacity,
Maximum Insufflation Capacity, Respiratory Muscles, Glottic Muscles
February 2006 Expiratory Flow Maneuvers 105
RESEARCH ARTICLE
Neuromuscular Disease
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 181

Both peak expiratory flows (PEF) and cough
peak flows (CPF) have been described as useful
clinical variables of respiratory muscle function.1
“Dart flows” (DF) are generated by creating pres-
sure behind the lips and tongue with the mouth
closed. As the lips open and tongue releases the air,
in a maneuver like spitting or projecting a dart
through a narrow tube, these flows can also be
measured by peak flow meter. These flows can be
confused with PEF and CPF and cause the latter to
be overestimated. They are largely a function of the
ability to seal the lips and control the tongue and
buccal muscles.
The main cause of morbidity and mortality in
patients with neuromuscular disease/restrictive
pulmonary syndrome (NMD) is respiratory muscle
dysfunction and, in particular, cough dysfunc-
tion.2–4 Inspiratory, expiratory, and bulbar-inner-
vated musculature are required for effective cough-
ing.5,6
Normal precough inspiration is to 85–90% of
total lung capacity.7 Thus, cough flows are dimin-
ished for patients who have decreased ability to
inflate the lungs, especially when vital capacity
(VC) is �1500 ml.8 After a deep breath, the glottis
is closed by intrinsic laryngeal (bulbar-innervated)
muscles. The expiratory muscles (abdominal and
intercostals) then contract, resulting in intrapleu-
ral pressures of 200 cm H2O.9 On full glottic open-
ing with hypopharyngeal patency maintained by
other bulbar-innervated musculature, there is an
explosive decompression that normally generates
flows of 300–1200 liters/min to expulse airway
secretions.
In patients with NMD, weak inspiratory mus-
cles can be assisted by providing deep lung insuf-
flations or by the stacking of consecutively deliv-
ered volumes of air held with a closed glottis to
approach a maximum insufflation capacity
(MIC).10–12 Expiratory muscles can be manually
assisted by providing thoracoabdominal thrusts.
The combination of applying an abdominal thrust
to a maximally inflated lung is an assisted
cough.1,10 Unassisted cough flows depend on in-
spiratory, expiratory, and bulbar-innervated mus-
culature. However, air stacking ability and, there-
fore, assisted cough flows depend only on glottic
control or on bulbar-innervated muscle function
alone. Thus, the greater the difference between the
MIC and the VC and between assisted and unas-
sisted CPF, the greater is bulbar-innervated muscle
function by comparison with inspiratory muscle
function. Patients who cannot close the glottis
cannot air stack. They may “huff” but cannot
cough. CPF better reflect the capacity to expulse
debris from the airways (cough efficacy) than do
PEFs. CPF not exceeding 160 liters/min are asso-ciated with extubation failure.13
There are no standard normal values for CPFor DF, but PEF range from 500 to 700 liters/minfor men and from 380 to 500 liters/min for women,and from 150 to 840 liters/min for children andadolescents, with variations due to age, race, sex,and height.14,15 For patients with asthma, theirdiminution generally indicates bronchospasm.16
The purpose of this study was to compare the CPF,PEF, and DF, to see if they correlate with VC orMIC, and to consider their use in the evaluation ofthe respiratory muscles.
METHODS
A cross-sectional study was conducted on allNMD patients entering an outpatient clinic be-tween August 2003 and May 2004. The charts of thepatients were reviewed for anthropometric data(age, sex) and for diagnosis. All cooperative NMDpatients whose VCs were �80% of predicted nor-mal were studied. No one meeting these criteriawas excluded. Normal subjects were recruited, in-formed about the purpose of the study, and signedconsent forms that were approved by the hospitals’ethics committee. The patients and controls re-ceived a written description of the maneuvers andhad a 3-min training period before the measure-ments were taken.
The following variables were measured: PEFaccording to the recommendations of the Ameri-can Thoracic Society,17 CPF, and DF, all via anAccess Peak Flow Meter (model 710, Health ScanProducts, Cedar Grove, NJ), and VC (sitting andsupine) and MIC via a spirometer (Mark 14, Fer-raris Development and Engineering, London, UK).All of these measurements were done by a specifi-cally trained respiratory therapist who was un-aware of the study and recorded the highest valueof four or more correctly performed efforts. Thepeak flow meter measured flows from 60 to 880liters/min. Flows of �60 liters/min were recordedas 0 and flows of �880 liters/min were recorded as881 liters/min. No patients had been hospitalizedduring the previous 30 days.
Statistical Analysis
Data for the categorical variables are expressedas number and percentage of patients. Data for thecontinuous variables are reported as median withdispersion of minimum, maximum, and interquar-tile range and range. The use of median valuesrather than mean values eliminated the effect ofimprecisely measured ceiling and floor data.
Normally distributed continuous variableswere compared using the unpaired and paired Stu-dent’s t test, as appropriate, and nonparametriccontinuous variables using Wilcoxon’s signed-
106 Bach et al. Am. J. Phys. Med. Rehabil. ● Vol. 85, No. 2
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
182 Miguel Ramalho do Souto Gonçalves

ranks test and Mann–Whitney U test, as appropri-ate. The statistical analyses were repeated assum-ing that all flows of �60 liters/sec were 59 liters/min, except for CPF, which occur without glotticclosure and which, by definition, could only be 0liters/min. PEF of �880 liters/min were estimatedas 881 and then re-estimated as 1008 liters/min,which is 20% greater than 840 liters/min or 2 SDgreater than maximum normal PEF. In addition, aunivariable linear regression analysis was con-ducted to compare expiratory flows with pulmo-nary capacities. All statistical tests were two tailed.A P value of �0.05 was considered to indicatestatistical significance. Statistical analysis was con-ducted with the use of Stata, version 7.0, and SPSS,version 12.0.
RESULTS
There were 125 patients with a mean age of 41� 21 (range, 7–82) yrs; 64% were men (n � 80)and 100 were �18 yrs old (80%). The patients’diagnoses are listed in Table 1. The 52 normalsubjects were 28.6 � 9.8 (range, 19–58) yrs of age,65.4 � 11.4 (range, 49–100) kg, and 165.8 � 8.4(range, 152–183) cm tall. CPF, PEF, and DF dataare presented in Table 2. Two patients were unableto attain any measurable flows, two had measur-able PEF and CPF but not DF, nine had measurableCPF and DF but no measurable PEF, six had mea-surable DF but not CPF or PEF, and one patienthad measurable PEF and DF but not CPF.
The DF were significantly greater than CPFand PEF (P � 0.001) for both the normal subjectsand the patient group. The CPF and PEF were notsignificantly different for the normal subjects. Forthe patient group, assuming unmeasurable flows tobe 0 liters/min, the CPF were significantly greaterthan PEF (P � 0.01) (Table 2). The differencesremained significant (P � 0.01) when considering
adults only but not children only. The patients’CPF remained significantly greater than PEF (P �
0.05) when the eight patients with unmeasurableCPF and PEF were eliminated and when PEF wereestimated to be 59 liters/min for the nine patientswith measurable CPF but not measurable PEF.
The flow data for the six patients (5.5%) withunmeasurable PEF and CPF but measurable DF arein Table 3. Thus, these patients had relatively well-preserved bulbar-innervated musculature, despitesevere inspiratory and expiratory muscle weakness.This was consistent with their diagnoses of post-poliomyelitis1 and congenital muscular dystrophy,5
conditions that, relatively speaking, spare bulbarmusculature.
There were two patients with unmeasurableDF who had severe bulbar amyotrophic lateral scle-rosis yet had mean CPF of 205 liters/min. In fact,the CPF exceeded the DF for 12 patients: two chil-dren with non-Duchenne muscular dystrophy andten adults, of whom seven had amyotrophic lateralsclerosis, two had fascioscapulohumeral dystrophy,and one had myotonic dystrophy. Only one wasunable to air stack. These 12 patients had a greatercapacity to air stack, as seen by a greater MIC–VCdifference, than in the general group (Table 4),suggesting less compromise of glottic musclesthan of the cheeks, lips, and tongue. The 16 pa-tients whose PEF exceeded CPF and, thus, whoseexpiratory muscles were relatively preserved bycomparison with bulbar-innervated muscles areconsidered in Table 5. The PEF of 11 normal sub-jects (21.1%) also exceeded their CPF.
The MIC was measured for 88 patients. For 14of the 88, the MIC did not exceed the VC because ofinability to firmly close the glottis or prevent airleakage out of the nose or mouth during the air-stacking process; their mean VC was 1518.6 �
764.8 ml, significantly lower than the mean VC ofthe whole population (2000 ml, P � 0.03), suggest-ing more advanced disease. Eight of these 14 hadCPF equal to or lower than PEF, confirming moresevere compromise of facial and glottic muscula-ture. In only three of these 14 cases were the DFlower than or equal to CPF, indicating that bulbarmusculature was variably involved with relativesparing of the tongue and lips.
Good correlation was found between CPF andMIC (r � 0.76) (Fig. 1) and between PEF and MIC(r � 0.72) (Fig. 2). Correlation was also foundbetween MIC and DF (r � 0.73). For the remaining37 patients, MIC was not measured because the VCwas too close to the normal range (3155 � 1091.7ml in 27 adults and 2861 � 997.9 ml for the tenchildren) and bulbar musculature was clinicallyintact. There was also a direct correlation betweenCPF and PEF with VC (r � 0.85 and 0.86, respec-tively) and with MIC (r � 0.76 and 0.72, respec-
TABLE 1 Diagnosis of neuromuscular patients
Diagnosis n %
Amyotrophic lateral sclerosis 41 32.8Duchenne–Becker muscular
dystrophy27 21.6
Other muscular dystrophies 18 14.4Postpoliomyelitis 12 9.6Myopathies (nonmuscular
dystrophy)8 6.4
Myasthenia gravis 6 4.8Spinal muscular atrophy 5 4.0Myotonic dystrophy 4 3.2Neuropathies 2 1.6Spinal cord injury 1 0.8Obesity hypoventilation syndrome 1 0.8Total 125 100
February 2006 Expiratory Flow Maneuvers 107
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 183

tively) for the entire patient group (Fig. 3). This isnot surprising because CPF and PEF are dependenton the ability to take a deep breath. DF also cor-related with VC (r � 0.79), indicating relative pres-ervation of tongue and lips in early disease.
DISCUSSION
Unlike in a previous report by Suarez et al.18,although CPF were greater than PEF for normalsubjects, we did not find the difference to be sta-tistically significant. However, our patient popula-tion may have been too small to observe a signifi-cant difference.18 As Suarez et al.18 reported for
patients with Duchenne muscular dystrophy, wedid observe significantly greater CPF than PEF forpatients with NMD.
The three flow maneuvers we studied are sim-ilar in that they are expiratory flows measured atthe mouth using a peak flow meter. However, eachmethod requires different respiratory musclegroup combinations. With glottic closure, thegreater transpulmonary pressures created bycoughing rather than by PEF maneuvers resultedin greater flows measured at the mouth for 88.2%of patients and 78.9% of normal subjects. However,cough efficacy is dependent on the peak flow ve-locity, which is greater as airways narrow during
TABLE 2 Expiratory maneuvers for normal subjects and patients with neuromuscular diseases
Measurement Variable
Group Statistics CPF PEF DF
Normal patients(n � 52)
Median, liters/min 455 445 881Minimum, liters/min 290 320 370Maximum, liters/min 880 720 881Interquartile range, liters/min 225 160 148Range, liters/min 590 400 510Measurement above reference
range of �880 liters/min, n (%)a0 0 34 (65.4)
Measurement below referencerange of �60 liters/min, n (%)b
0 0 0
Patients(n � 125)
Median, liters/min 250 220 335Minimum, liters/min 0 0 0Maximum, liters/min 710 635 881Interquartile range, liters/min 210 188 270Range, liters/min 650 575 820Measurement above reference
range of �880 liters/min, n (%)a0 0 5 (4.0)
Measurement below referencerange of �60 liters/min, n (%)b
9 (7.3) 17 (13.5) 5 (4.0)
�18 yrs of age (n � 100),mean � SD
280.1 � 167.6 225.6 � 159.9 395 � 260.3
�18 yrs of age (n � 25),mean � SD
248.4 � 108 234.6 � 98.5 332.8 � 158.7
CPF, cough peak flows; PEF, peak expiratory flows; DF, dart flows.a Flows of �880 liters/min were recorded as 881 liters/min.b Flows of �60 liters/min were recorded as 0 liters/min.
TABLE 3 Patients with unmeasurable cough and expiratory flows vs. group as a whole
Patients with Unmeasurable CPF and PEF (n � 6) All 125 Patients P
Age, yrs 29.5 � 14.6 41 � 21 0.06DF, liters/min 128.3 � 50.9 382.6 � 244.1 �0.01VC, ml 358.3 � 115.5 2000.0 � 1245.6 �0.01
CPF, cough peak flow; PEF, peak expiratory flow; DF, dart flows; VC, vital capacity. Data (except for significance) providedas mean � standard deviation.
108 Bach et al. Am. J. Phys. Med. Rehabil. ● Vol. 85, No. 2
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
184 Miguel Ramalho do Souto Gonçalves

coughing, making coughing more effective at ex-pulsing airway secretions than huffing, eventhough PEF and CPF may be comparable whenmeasured at the mouth.8 The reduction of thecross-sectional area of the airways during coughingis due to smooth muscle constriction mediated bya vagal reflex (presumably preserved in these dis-eases) and due to dynamic compression of theairways generated by the expiratory (transpulmo-nary) pressure.19,20 The reduction in the cross-sectional area of the airways increases five-fold thevelocity of gas and 25-fold the kinetic energy of theairstream. This explains why the subgroup of 16patients (12.8%) with CPF lower than PEF never-theless coughed rather than huffed to expel secre-
tions. Effective CPF and PEF share the need fordeep lung volumes, explaining their good correla-tion with VC and MIC.
The correlation of CPF with MIC or MIC–VCdifference is explained by their dependence on bul-bar-innervated muscle (glottic) function. CPF arealso dependent on hypopharyngeal patency beingmaintained by bulbar-innervated hypopharyngealmusculature. DF, on the other hand, are indepen-dent of laryngeal and hypopharyngeal dysfunctionand usually exceed CPF and PEF. However, DF donot emanate from the airways and require little orno inspiratory or expiratory muscle effort. We haveseveral patients who operate sip-and-puff motor-ized wheelchairs and generate high DF, despite
TABLE 4 Patients with cough peak flows (CPF) greater than dart flows (DF)
CPF > DF (n �12) All Group (n � 125) P
VC 1220.8 � 611.9 2000.0 � 1245.6 �0.01MIC 1974.0 � 643.3 2179.8 � 1097.9 NSMIC – VC 822.0 � 580.3 632.1 � 474.7 NSCPF 179.2 � 49 273.8 � 157.6 �0.01PEF 113.8 � 55.8 227.4 � 149.4 �0.01DF 107.9 � 75.1 382.6 � 244.1 �0.01
VC, vital capacity; MIC, maximum insufflation capacity; NS, not significant; PEF, peak expiratory flows. Data (except forsignificance) provided as mean � standard deviation.
TABLE 5 Patients with peak expiratory flows (PEF) greater than cough peak flows (CPF)
PEF > CPF (n �16) Entire Group (n � 125) P
VC 2042.3 � 899.8 2000 � 1245.6 NSMIC 2324.2 � 943.1 2179.8 � 1097.9 NSMIC – VC 588.5 � 580.5 632.1 � 474.7 NSCPF 213.4 � 103.2 273.8 � 157.6 0.04PEF 257.8 � 92.0 227.4 � 149.4 NSDF 387.8 � 168.4 382.6 � 244.1 NS
VC, vital capacity; NS, not significant; MIC, maximum insufflation capacity; DF, dart flow. Values (except for significance)provided as mean � standard deviation.
FIGURE 1 Correlation between cough peak flows
(CPF) and maximum insufflation capac-
ity (MIC).
FIGURE 2 Correlation between peak expiratory
flows (PEF) and maximum insufflation
capacity (MIC).
February 2006 Expiratory Flow Maneuvers 109
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 185
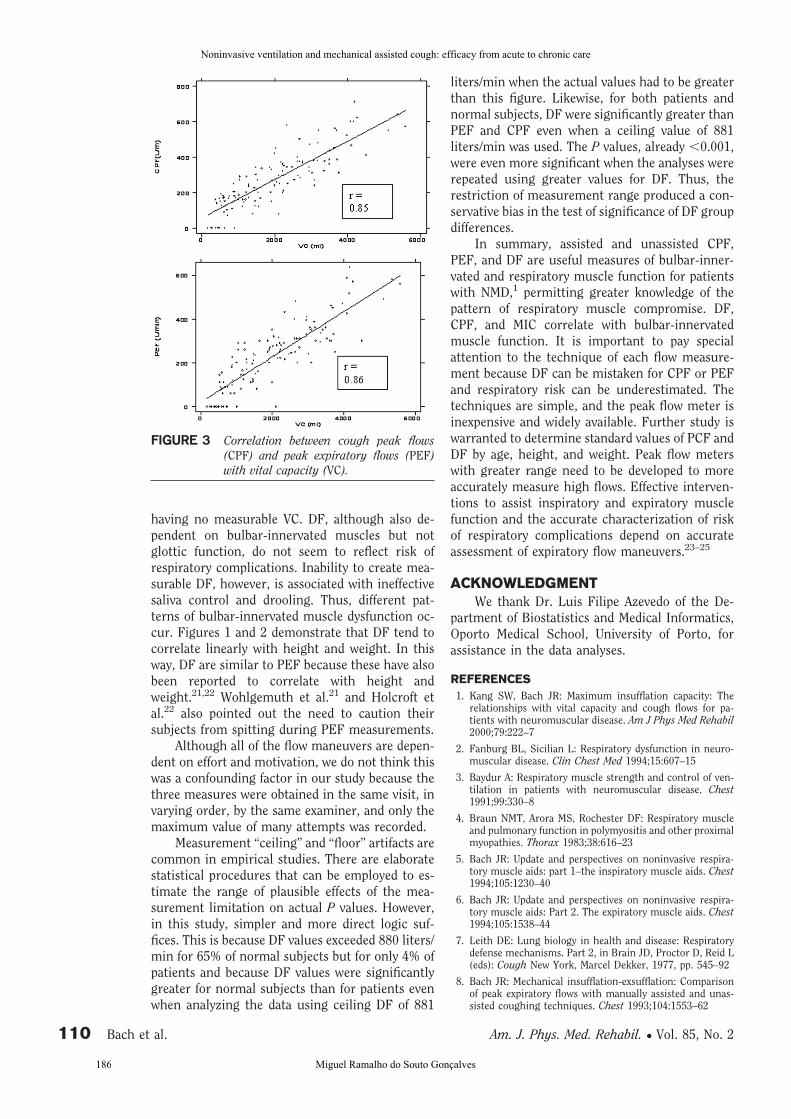
having no measurable VC. DF, although also de-pendent on bulbar-innervated muscles but notglottic function, do not seem to reflect risk ofrespiratory complications. Inability to create mea-surable DF, however, is associated with ineffectivesaliva control and drooling. Thus, different pat-terns of bulbar-innervated muscle dysfunction oc-cur. Figures 1 and 2 demonstrate that DF tend tocorrelate linearly with height and weight. In thisway, DF are similar to PEF because these have alsobeen reported to correlate with height andweight.21,22 Wohlgemuth et al.21 and Holcroft etal.22 also pointed out the need to caution theirsubjects from spitting during PEF measurements.
Although all of the flow maneuvers are depen-dent on effort and motivation, we do not think thiswas a confounding factor in our study because thethree measures were obtained in the same visit, invarying order, by the same examiner, and only themaximum value of many attempts was recorded.
Measurement “ceiling” and “floor” artifacts arecommon in empirical studies. There are elaboratestatistical procedures that can be employed to es-timate the range of plausible effects of the mea-surement limitation on actual P values. However,in this study, simpler and more direct logic suf-fices. This is because DF values exceeded 880 liters/min for 65% of normal subjects but for only 4% ofpatients and because DF values were significantlygreater for normal subjects than for patients evenwhen analyzing the data using ceiling DF of 881
liters/min when the actual values had to be greaterthan this figure. Likewise, for both patients andnormal subjects, DF were significantly greater thanPEF and CPF even when a ceiling value of 881liters/min was used. The P values, already �0.001,were even more significant when the analyses wererepeated using greater values for DF. Thus, therestriction of measurement range produced a con-servative bias in the test of significance of DF groupdifferences.
In summary, assisted and unassisted CPF,PEF, and DF are useful measures of bulbar-inner-vated and respiratory muscle function for patientswith NMD,1 permitting greater knowledge of thepattern of respiratory muscle compromise. DF,CPF, and MIC correlate with bulbar-innervatedmuscle function. It is important to pay specialattention to the technique of each flow measure-ment because DF can be mistaken for CPF or PEFand respiratory risk can be underestimated. Thetechniques are simple, and the peak flow meter isinexpensive and widely available. Further study iswarranted to determine standard values of PCF andDF by age, height, and weight. Peak flow meterswith greater range need to be developed to moreaccurately measure high flows. Effective interven-tions to assist inspiratory and expiratory musclefunction and the accurate characterization of riskof respiratory complications depend on accurateassessment of expiratory flow maneuvers.23–25
ACKNOWLEDGMENT
We thank Dr. Luis Filipe Azevedo of the De-partment of Biostatistics and Medical Informatics,Oporto Medical School, University of Porto, forassistance in the data analyses.
REFERENCES
1. Kang SW, Bach JR: Maximum insufflation capacity: Therelationships with vital capacity and cough flows for pa-tients with neuromuscular disease. Am J Phys Med Rehabil2000;79:222–7
2. Fanburg BL, Sicilian L: Respiratory dysfunction in neuro-muscular disease. Clin Chest Med 1994;15:607–15
3. Baydur A: Respiratory muscle strength and control of ven-tilation in patients with neuromuscular disease. Chest1991;99:330–8
4. Braun NMT, Arora MS, Rochester DF: Respiratory muscleand pulmonary function in polymyositis and other proximalmyopathies. Thorax 1983;38:616–23
5. Bach JR: Update and perspectives on noninvasive respira-tory muscle aids: part 1–the inspiratory muscle aids. Chest1994;105:1230–40
6. Bach JR: Update and perspectives on noninvasive respira-tory muscle aids: Part 2. The expiratory muscle aids. Chest1994;105:1538–44
7. Leith DE: Lung biology in health and disease: Respiratorydefense mechanisms. Part 2, in Brain JD, Proctor D, Reid L(eds): Cough New York, Marcel Dekker, 1977, pp. 545–92
8. Bach JR: Mechanical insufflation-exsufflation: Comparisonof peak expiratory flows with manually assisted and unas-sisted coughing techniques. Chest 1993;104:1553–62
FIGURE 3 Correlation between cough peak flows
(CPF) and peak expiratory flows (PEF)
with vital capacity (VC).
110 Bach et al. Am. J. Phys. Med. Rehabil. ● Vol. 85, No. 2
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
186 Miguel Ramalho do Souto Gonçalves

9. Evans JN, Jaeger MJ: Mechanical aspects of coughing. Pneu-monologie 1975;152:253–7
10. Chaudhry SS, Bach JR: Management approaches in muscu-lar dystrophy association clinics. Am J Phys Med Rehabil2002;79:193–6
11. Giggs RG, Donohoe KM, Utell MJ, et al: Evaluation ofpulmonary function in neuromuscular disease. Arch Neurol1981;38:9–12
12. Ishikawa Y, Minami R: The effect of nasal IPPV of patientswith respiratory failure during sleep due to Duchenne mus-cular dystrophy. Clin Neurol 1993;33:856–61
13. Bach JR, Saporito LR: Criteria for extubation and tracheos-tomy tube removal for patients with ventilatory failure: Adifferent approach to weaning. Chest 1996;110:1566–71
14. Nunn AJ, Gregg I: New regression equations for predictingpeak expiratory flow in adults. BMJ 1989;298:1068–70
15. Polgar G, Promadhat V: Pulmonary Function Testing inChildren: Techniques and Standards. Philadelphia, WBSaunders, 1971
16. Jain P, Kavuru MN, Emerman CL, et al: Utility of peakexpiratory flow monitoring. Chest 1998;114:861–76
17. Standardization of spirometry, 1994 Update: American Tho-racic Society. Am J Respir Crit Care Med 1995;152:1107–36
18. Suarez AA, Pessolano F, Monteiro SG, et al: Peak flow andpeak cough flow in the evaluation of expiratory muscleweakness and bulbar impairment of neuromuscular pa-tients. Am J Phys Med Rehabil 2002;81:506–11
19. Irwin RS, Boulet LP, Cloutier MM, et al: Managing cough asa defense mechanism and as a symptom: A consensus panelreport of the American College of Chest Physicians. Chest1998;114:133S–81S
20. McCool FD, Leith DE: Pathophysiology of cough. Clin ChestMed 1987;2:189–95
21. Wohlgemuth M, Van Der Kooi EL, Hendriks JC, et al: Facemask spirometry and respiratory pressures in normal sub-jects. Eur Respir J 2003;22:1001–6
22. Holcroft C, Eisen E, Sama S, et al: Measurement charac-teristics of peak expiratory flow. Chest 2003;124:501–509
23. Gomez-Merino E, Bach JR: Duchenne muscular dystrophy:Prolongation of life by noninvasive respiratory muscle aids.Am J Phys Med Rehabil 2002;81:411–5
24. Bach JR, Baird JS, Plosky D, et al: Spinal muscular atrophytype 1: Management and outcomes. Pediatr Pulmonol 2002;34:16–22
25. Bach JR: Amyotrophic lateral sclerosis: Prolongation of lifeby noninvasive respiratory aids. Chest 2002;122:92–8
February 2006 Expiratory Flow Maneuvers 111
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 187

Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
188 Miguel Ramalho do Souto Gonçalves
Study 6
Lung Insufflation Capacity in Neuromuscular Diseases
John R. Bach Kedar Mahajan Bethany Lipa, Lou Saporito, Miguel Goncalves, Eugene Komaroff,
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 189

Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
190 Miguel Ramalho do Souto Gonçalves

Authors:
John Robert Bach, MDKedar Mahajan, BSBethany Lipa, BSLou Saporito, BSMiguel Goncalves, BSEugene Komaroff, PhD
Affiliations:
From the Department of PhysicalMedicine and Rehabilitation,University of Medicine and Dentistryof New Jersey (UMDNJ)–New JerseyMedical School, Newark, New Jersey(JRB, KM, BL, LS, EK); andDepartment of Pulmonary Medicine,Sao Joao University Hospital, Porto,Portugal (MG).
Correspondence:
All correspondence and requests forreprints should be addressed to JohnR. Bach, MD, Professor of PhysicalMedicine and Rehabilitation,Professor of Neurosciences,Department of Physical Medicine andRehabilitation, University HospitalB-403, 150 Bergen Street, Newark, NJ07103.
Disclosures:
The authors have received nofinancial support from any companymentioned in this manuscript.
0894-9115/08/8709-0720/0
American Journal of Physical
Medicine & Rehabilitation
Copyright © 2008 by Lippincott
Williams & Wilkins
DOI: 10.1097/PHM.0b013e31817fb26f
Lung Insufflation Capacity inNeuromuscular Disease
ABSTRACT
Bach JR, Mahajan K, Lipa B, Saporito L, Goncalves M, Komaroff E: Lunginsufflation capacity in neuromuscular disease. Am J Phys Med Rehabil 2008;87:720–725.
Objective: To compare maximal passive lung insufflation capacity (LIC)with lung inflation by air stacking (to maximum insufflation capacity [MIC]) andwith vital capacity (VC); to explore relationships between these variables thatcorrelate with glottic function and cough peak flows (CPF); to demonstratethe effect of routine inflation therapy on LIC and MIC; and to determine therelative importance of lung inflation therapy as a function of disease severity.
Design: Case series of 282 consecutive neuromuscular disease(NMD) clinic patients 7 yrs and older with VC �70% of the predictednormal value. All cooperative patients meeting these criteria were pre-scribed thrice-daily air stacking and/or maximal passive lung insufflation topressures of 40–80 cm H2O, and they underwent measurements of VC,MIC, LIC, and unassisted and assisted CPF on every visit.
Results: Means � standard deviations for VC, MIC, and LIC were1131 � 744, 1712 � 926, and 2069 � 867 ml, respectively, and, forunassisted and assisted CPF, they were 2.5 � 2.0 and 4.3 � 2.2liters/sec, respectively, with all differences statistically significant (P �
0.001). MIC minus VC correlated inversely with LIC minus MIC (P �
0.01) and, therefore, with glottic function. Both MIC and LIC increasedwith practice (P � 0.001). Increases in LIC but not MIC over VC weregreatest for patients with the lowest VC (P � 0.05). There were nocomplications of lung mobilization therapy.
Conclusions: Passive lung insufflation can distend the lungs of pa-tients with NMD significantly greater than air stacking, particularly whenglottic and bulbar-innervated muscle dysfunction is severe. LIC, MIC, andVC measurements permit quantifiable assessment of glottic integrity and,therefore, bulbar-innervated muscle function for patients with NMD. Thepatients who benefit the most from insufflation therapy are those who havethe lowest VC.
Key Words: Neuromuscular Disease, Lung Insufflation Capacity, Pulmonary Compli-
ance, Cough Flows, Air Stacking
720 Am. J. Phys. Med. Rehabil. ● Vol. 87, No. 9
ORIGINAL RESEARCH ARTICLE
Pulmonary
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 191

Respiratory failure for patients with pediatricneuromuscular disease (NMD) is often caused byineffective coughing during otherwise benign chestinfections.1–3 Whereas a normal tidal volume canbe 500 ml, a normal cough volume is 2.3 � 0.5liters.4 Indeed, the lower the VC, the poorer arecough peak flows (CPF) independently of expira-tory (thoracoabdominal) muscle strength.5
Lung expansion to optimize lung recoil pres-sure and increase CPF can be achieved by maxi-mally “air stacking” consecutively delivered vol-umes of air held with a closed glottis. Themaximum volume that can be held in this manneris defined as the maximum insufflation capacity(MIC).6 The MIC can exceed predicted inspiratorycapacity (IC) in people with intact glottic func-tion,7–9 but it only approaches predicted IC in pa-tients with moderate to severe glottic dysfunction.6
With complete loss of glottic closure, MIC nolonger exceeds VC; the NMD patient can no longerair stack or cough, and the glottis, and many, if notall, bulbar-innervated muscles, are extremely im-paired. In this case, lung insufflation can only beprovided by bypassing glottic function. This can bedone by using a manual resuscitator with a closedexpiratory port mimicking glottic closure, or byusing a CoughAssist or volume-cycled ventilator atdelivered volumes/pressures that approach pre-dicted IC.6 The maximum passive lung insufflationvolume achieved in this manner is defined as thelung insufflation capacity (LIC).
The goal of conventional prescriptions for“range-of-motion” mobilization of extremity artic-ulations is to slow the development of musculo-skeletal contractures for patients with limb muscleweakness. However, the prevention of chest wallcontractures and lung restriction has only recentlybeen addressed. In 2006, Lechtzin et al.10 reportedthe use of short-term noninvasive intermittentpositive pressure ventilation (IPPV) to increase pul-monary compliance for patients with amyotrophiclateral sclerosis (ALS). In 2000, we demonstratedthat lung volumes could be increased significantlyover VC by air stacking to approach MIC for pa-tients with NMD.6 This resulted in significantlyincreased (assisted) CPF that can decrease the riskof pneumonia.11,12 For patients such as those withadvanced bulbar ALS whose MIC equals VC, as-sisted CPF cannot be increased by air stacking, andprognosis is poor.13
The purpose of this work was to explore thefollowing hypotheses: (1) lung volumes will be sig-nificantly greater by passive insufflation than by airstacking, especially in patients with severe bulbar-innervated muscle dysfunction, and both LIC andMIC will significantly exceed VC and increase CPF;(2) LIC-MIC will correlate inversely with MIC-VC
and, therefore, correlate inversely with glottic in-tegrity; (3) LIC and MIC can increase with practice;and (4) the greatest increases in MIC and LIC willbe for the most severely affected patients, that is,with the lowest VC.
METHODS
The institutional review board approved thisstudy. In 1979, we began to routinely prescribe airstacking and/or maximal (passive) lung insufflationat pressures of 40 cm H2O or more, three timesdaily, for all patients with VC less than 70–80% ofnormal. Beginning in 2005, we routinely measuredVC, MIC, and LIC in all 290 consecutive patients 7yrs and older whose VC were less than 70%. Ex-clusion criteria were inability to cooperate attrib-utable to severe cognitive impairment, medical in-stability, and primarily lung/airways rather thanventilatory pump insufficiency. Two with DMD,one with congenital myotonic dystrophy, and twoothers with poorly characterized NMD could notcooperate. Three patients were acutely ill and hos-pitalized. No NMD patients had signs of lung/air-ways disease sufficient to warrant evaluation forconcomitant chronic obstructive pulmonary dis-ease or reversible bronchospasm.
All lung volumes were measured by Wrightspirometer model Mark 14 (Ferraris Ltd., London,England) and recorded as the greatest observedvalue in five or more attempts. The MIC was ob-tained by the patient air stacking volumes deliveredvia an oronasal interface from a manual resuscita-tor with a directed expiratory port and with eitherno pressure-limitation device or with the pressurerelease value deactivated, or obtained by air stack-ing via a volume-cycled mechanical ventilator forpatients using daytime noninvasive ventilation.Once no more air could be held with a closedglottis, the patient exhaled into the spirometer toresidual volume (MIC).7
Cough peak flows, both unassisted and as-sisted, were measured by Access Peak Flow Meter(Health Scan Products Inc., Cedar Grove, NJ). Thelargest value of five or more attempts was recorded.Cough flows were assisted by air stacking to ap-proach MIC and an expiratory-timed abdominalthrust.
The LIC was obtained by using the same man-ual resuscitator connected to a spirometer. Thespirometer’s reset button was held and the expira-tory port of the spirometer was occluded duringinsufflation. After insufflation to maximal observedlung (chest wall) expansion with maximum toler-able resistance to further insufflation, the spirom-eter’s reset button and the expiratory port of thespirometer were simultaneously released, and thepatient exhaled to residual volume into the spirom-eter via a tightly held anesthesia (oronasal) inter-
September 2008 Lung Insufflation Capacity 721
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
192 Miguel Ramalho do Souto Gonçalves

face (Fig. 1). The maximum insufflation pressuretolerated by the patient, and the correspondingresistance felt by the therapist, were then repro-duced by insufflating the patient, using theCoughAssist. This was done to observe the pres-sures required for full insufflations to prescribeinsufflation therapy three times daily at home.Thus, glottic closure was unnecessary for the mea-surement of LIC.
Correlation analysis was done between LIC-MIC and MIC-VC using Spearman correlation co-efficients (rS) with P � 0.05 as the level of statis-tical significance (alpha). The same Spearmancorrelation analyses were done for ALS and DMDpatient subgroups. A categorical variable from VCwas based on quartiles, and the correlations wererun within each quartile. Wilcoxon signed rankstests were used to determine possible significance inthe differences between the means of the lung vol-ume variables and also the CPF variables. The differ-ences in the means of the lung volume variables(MIC � MIC, LIC � VC, and MIC � VC) by VC(sitting) levels were evaluated by analysis of variance.
RESULTS
The 290 patients had the following diagnoses:ALS/motor neuron disease 81, DMD 54, non-DMDmuscular dystrophy 38, other myopathies 23, post-
poliomyelitis 26, spinal muscular atrophy 32, and
other conditions 36. Two hundred eighty-two NMD
patients met the criteria. Seventy-eight of these
had had multiple visits and had been prescribed
maximal lung expansion therapy three times daily,
with 10–15 cycles of air stacking/passive insufflations
for a 6-mo to 24-yr period, before the most recent
clinic visit, during which data points were taken for
this study. Among the patients, 103, 116, and 69 were
using continuous NIV, nocturnal-only NIV, or no aid,
respectively.
The patient population had mean � standard
deviation values of 1131 � 744 ml for VC, 1712 �
926 ml for MIC (significantly greater than VC, P �
0.001), and 2069 � 867 ml for (passive) LIC (sig-
nificantly greater than MIC and VC at P � 0.001) at
the most recent evaluation. For 46 of the 78 pa-
tients with two or more measurements who were
prescribed daily air stacking/lung insufflation, the
MIC and LIC increased 462 � 260 and 365 � 289
ml, respectively, despite a decrease in VC of 209 �
97 ml. The increase in lung volumes by air stacking
to approach MIC combined with abdominal thrust
resulted in CPF of 4.3 � 1.7 liters/sec by compar-
ison with unassisted CPF of 2.5 � 2.0 liters/sec
(P � 0.001). Patients’ diagnoses, VC, MIC, LIC, CPF,
and extent of ventilator use are noted in Table 1.
Although they could not be measured, “cough” flows
FIGURE 1 Air is delivered via the manual resuscitator (bottom) to full lung expansion, with the exhalation port
of the spirometer manually covered so that the insufflated air does not exit the patient (or enter the
spirometer) until its exhalation port is uncovered at maximally tolerated lung inflation (top).
722 Bach et al. Am. J. Phys. Med. Rehabil. ● Vol. 87, No. 9
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 193

from the greater lung volumes at LIC can only exceedflows obtained from the necessarily smaller MIC.
For 15 patients, the LIC did not exceed theMIC; any insufflation beyond VC triggered cough-ing that was most likely attributable to airwayirritation or atelectasis from saliva aspiration be-cause no patients had lung/airways disease or highpressure resistance to insufflation. Deep breathsalso caused these patients to cough. These patientshad little or no ability to air stack, because of severebulbar-innervated muscle dysfunction. Eleven ofthe 15 patients had gastrostomy tubes, and 13 whohad had modified Barium swallow examinationshad faucial pooling of secretions with glottic pen-etration.
For the 282 patients, the Spearman correlationcoefficient revealed a negative association betweenLIC � MIC and MIC � VC (rS � �0.23, P � 0.01)(Fig. 2). Even stronger negative associations werefound for the ALS (rS � �0.30, P � 0.0085) andDMD (rS � �0.38, P � 0.0051) subpopulations.The LIC � MIC trended inversely with VC (sitting)(P � 0.001). The MIC � VC did not vary signifi-cantly as a function of VC (sitting). The LIC � VCtrended inversely with VC (sitting), with marginalstatistical significance (P � 0.048).
DISCUSSION
This work describes a simple technique forproviding deep lung insufflations and for quanti-tating them. Patients with NMD often lose VC tothe extent that they can expand their lungs to onlya small fraction of predicted volumes. For example,DMD patients’ VC decrease to approximately 10%of predicted normal by age 20,14 and typical SMAtype 1 patients’ VC have been reported to neverexceed 250 ml, which, by age 10, amounts to lessthan 10% of the predicted normal value.2 Incentivespirometry is, therefore, useless because such pa-tients’ tidal volumes approach their deepestbreaths, and these cannot exceed a small percent-age of their IC. Likewise, in reviews of studies inwhich inspiratory resistive exercise was performedby NMD patients, no effect on VC, lung volumes, ormaximum inspiratory or expiratory pressures wasreported.15,16 On the other hand, expanding thelungs well beyond IC by air stacking or by single,deep insufflations permits greater lung distension,voice volume, and CPF6 and can decrease atelecta-sis and loss of pulmonary compliance.10 Our re-sults show that the benefits can be greatest for themost advanced patients with the lowest VC. Thefact that lung expansion to LIC � VC trends in-versely with VC, whereas MIC � VC does not,indicates that, for the most advanced patients, it isincreasingly important to expand the lungs by pas-sive insufflation rather than by air stacking. Inaddition, MIC and LIC can increase with practice.
Tab
le1
Pat
ient
diag
nose
s
Maj
or
Dia
gn
ose
sN
o.
of
Pat
ien
tsM
ean
Age
Mea
nV
Csi
tM
ean
MIC
Mea
nL
ICM
ean
CP
FM
ean
AC
PF
>8
hrs
NIV
8h
rsN
on
e
DM
D53
26
(14–44)
�7
62
2(1
–2
71
0)
�5
95
12
52
(22
0–
32
80
)�
67
01
69
6(8
40
–3
40
0)
�5
48
1.5
8(0
.1–
5.7
)�
1.7
3.7
6(0
–6
.2)
�1
.43
31
65
Myo
ton
ic6
47
(36–53)
�7
20
38
(11
90
–3
58
0)
�8
64
22
80
(11
90
–3
72
0)
�8
74
24
47
(13
80
–3
85
0)
�8
51
4.0
3(2
.7–
4.7
)�
0.8
5.1
0(4
.4–
5.9
)�
0.6
02
4O
ther
myo
pat
hie
s55
39
(11–85)
�18
11
95
(27
0–
27
70
)�
64
21
74
1(4
20
–3
36
0)
�8
25
20
26
(50
0–
36
00
)�
79
13
.11
(0.1
–7
.5)
�1
.84
.64
(1.6
–7
.5)
�1
.41
62
31
3S
MA
31
19
(7–56)
�14
86
1(3
0–
21
60
)�
55
41
25
4(3
0–
27
80
)�
74
81
54
4(3
20
–3
10
0)
�6
70
1.7
6(0
.1–
4.6
)�
1.5
3.5
4(1
.7–
5.5
)�
1.1
11
18
12
AL
S76
57
(27–82)
�13
13
71
(20
–3
48
0)
�7
89
19
39
(15
0–
51
00
)�
10
80
24
09
(78
0–
54
00
)�
98
92
.55
(0.1
–7
.5)
�2
.14
.29
(0–
8.5
)�
1.9
21
33
22
Post
-poli
o25
64
(49–85)
�8
10
66
(0–
24
00
)�
57
41
87
7(9
00
–2
95
0)
�6
03
21
68
(12
20
–3
20
0)
�5
96
3.0
0(0
.1–
8.2
)�
2.2
4.9
5(2
–8
.2)
�1
.51
01
05
Mis
cell
aneo
us
36
44
(16–58)
�14
13
54
(35
0–
17
60
)�
70
01
98
4(3
80
–3
80
0)
�9
84
22
29
(45
0–
38
50
)�
98
53
.05
(0.1
–3
.8)
�2
.14
.57
(0–
7.7
)�
2.1
12
14
10
Tota
l282
42
(7–85)
�20
11
31
(0–
35
80
)�
74
41
71
2(3
0–
51
00
)�
92
62
06
9(3
20
–5
40
0)
�8
67
2.5
2(0
.1–
9.7
)�
2.0
4.2
8(0
–9
.7)
�2
.21
03
11
66
9
VC
,vi
tal
capac
ity;
MIC
,m
axim
um
insu
fflat
ion
cap
acit
y;L
IC,
lun
gin
suffl
atio
nca
pac
ity;
CP
F,
cou
gh
pea
kfl
ow
s;A
CP
F,
assi
sted
CP
F;
AL
S,
amyo
troph
icla
tera
lsc
lero
sis.
September 2008 Lung Insufflation Capacity 723
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
194 Miguel Ramalho do Souto Gonçalves

Inability to air stack no longer means that patientscannot simply and inexpensively expand theirlungs beyond IC.
This study demonstrates that like MIC minusVC17 and assisted minus unassisted CPF,12 LIC �
MIC, too, is an objective, quantifiable, reproduciblemeasure that (inversely) correlates with glottic in-tegrity. Glottic function is the most important as-pect of bulbar-innervated muscle function for NMDpatients6,12 because it is most important for airwayprotection and cough effectiveness and, therefore,permits the use of NIV to avoid otherwise inevitablerespiratory failure leading to death or tracheos-tomy with decreased quality of life.11 In fact, in arecent study, all decanulated/extubated patientswith sufficient glottic function for (assisted) CPFgreater than or equal to 160 liters/min were suc-cessfully extubated, whereas those with less than160 liters/min failed extubation within 48 hrs.18
Previously reported correlates of bulbar-innervatedmuscle function have been based on subjective-only assessments of speech and swallowing.19,20
Some patients were hypercapnic on presenta-tion and had lungs stiff to the extent that using amanual resuscitator to increase tidal volumes tonormalize CO2 failed to do so and resulted in highairway pressures and chest discomfort. With regu-lar lung mobilization therapy and nocturnal NIV,however, five such patients became able to renor-malize CO2 when breathing autonomously withoutchest discomfort. This is consistent with previousstudies in which passive lung insufflation volumeswere greatly diminished for patients who were ven-tilated at constant pressures/volumes without reg-ular deep insufflations.10,21 Patients supported byNIV at large delivered volumes (1100–1500 ml)11
physiologically vary tidal volumes, can air stack todeep lung volumes as a function of their bulbar-innervated muscle integrity, and can better retainlung distensibility. Thus, if pressure-cycled venti-
lators such as “BiPAP” units (with which air stack-ing is impossible) are used for nocturnal NIV, pa-tients with diminished VC should be equipped forair stacking/maximal insufflations. One DMD pa-tient who had been using continuous tracheostomyventilation at 250 ml delivered volumes for 9 yrs,had PaCO2 76 cm H2O, and could not tolerate a100-ml volume increase without chest pain. Bycontrast, our 53 DMD patients who practice dailyinsufflation, mean age 26 � 7 yrs, tolerated deliv-ered volumes that exceeded VC by 1074 � 406 ml.Eight of these patients with VC less than 200 ml(mean 101 ml) have MIC values of 874 � 548 mland LIC values of 1414 � 764 ml.
In conclusion, regular lung insufflation, eitherby air stacking (to approach MIC) or by passivelung insufflation (to approach LIC), is indicated forall NMD patients with diminishing VC. Because thegoal is to approach the predicted IC, passive insuf-flation is used when the patient obtains a deepervolume in this manner than by air stacking (i.e.,when bulbar musculature is very weak). It is oftenbeneficial to prescribe both methods.
REFERENCES
1. Bach JR, Rajaraman R, Ballanger F, et al: Neuromus-
cular ventilatory insufficiency: the effect of home
mechanical ventilator use vs. oxygen therapy on
pneumonia and hospitalization rates. Am J Phys Med
Rehabil 1998;77:8–19
2. Bach JR, Saltstein K, Sinquee D, Weaver B, Komaroff
E: Long term survival in Werdnig-Hoffmann disease.
Am J Phys Med Rehabil 2007;86:339–48
3. Finder JD, Birnkrant D, Carl J, et al: Respiratory care
of the patient with Duchenne muscular dystrophy:
American Thoracic Society consensus statement.
Am J Respir Crit Care Med 2004;170:456–65
4. Leith DE: Lung biology in health and desease: respi-
ratory defense mechanisms, part 2, in Brain JD,
Proctor D, Reid L (eds): Cough. New York, Marcel
Dekker, 1977, pp 545–92
FIGURE 2 Plot of LIC � MIC vs. MIC � VC in milliliters, where LIC is lung insufflation capacity, MIC is
maximum insufflation capacity, and VC is vital capacity.
724 Bach et al. Am. J. Phys. Med. Rehabil. ● Vol. 87, No. 9
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 195

5. Gauld LM, Boynton A: Relationship between peak
cough flow and spirometry in Duchenne muscular
dystrophy. Pediatr Pulmonol 2005;39:457–60
6. Kang SW, Bach JR: Maximum insufflation capacity:
vital capacity and cough flows in neuromuscular
disease. Am J Phys Med Rehabil 2000;79:222–7
7. Seccombe LM, Rogers PG, Mai N, et al: Features of
glossopharyngeal breathing in breath-hold divers.
J Appl Physiol 2006;101:799–801
8. Bach JR, Tewfik G: “Air doping”: an expose on “frog”
insufflation in competitive sports. Am J Phys Med
Rehabil 2007;86:301–3
9. Mygren-Bonnier M, Lindholm P, Markstrom A,
Skedinger M, Mattsson E, Klefbeck B: Effects of
glossopharyngeal pistoning for lung insufflation on
vital capacity in healthy women. Am J Phys Med
Rehabil 2007;86:290–4
10. Lechtzin N, Shade D, Clawson L, Wiener CM: Supra-
maximal inflation improves lung compliance in sub-
jects with amyotrophic lateral sclerosis. Chest 2006;
129:1322–9
11. Gomez-Merino E, Bach JR: Duchenne muscular
dystrophy: prolongation of life by noninvasive respi-
ratory muscle aids. Am J Phys Med Rehabil 2002;81:
411–5
12. Bach JR, Gonzalves M, Paez S: Expiratory flow ma-
neuvers of patients with neuromuscular diseases.
Am J Phys Med Rehabil 2006;85:105–11
13. Bach JR, Bianchi C, Aufiero E: Oximetry and indica-
tions for tracheotomy in amyotrophic lateral sclero-
sis. Chest 2004;126:1502–7
14. Bach J, Alba A, Pilkington LA, Lee M: Long-term
rehabilitation in advanced stage of childhood onset,
rapidly progressive muscular dystrophy. Arch Phys
Med Rehabil 1981;62:328–31
15. DiMarco AF, Kelling JS, DiMarco MS, Jacobs I,
Shields R, Altose MD: The effects of inspiratory re-
sistive training on respiratory muscle function in
patients with muscular dystrophy. Muscle Nerve
1985;8:284–90
16. Martin AJ, Stern L, Yeates J, Lepp D, Little J: Respi-
ratory muscle training in Duchenne muscular dys-
trophy. Dev Med Child Neurol 1986;28:314–8
17. Kang SW, Bach JR: Maximum insufflation capacity.
Chest 2000;118:61–5
18. Bach JR, Saporito LR: Criteria for extubation and
tracheostomy tube removal for patients with venti-
latory failure: a different approach to weaning. Chest
1996;110:1566–71
19. Gilardeau C: Troubles de la deglutition dans la dys-
trophie musculaire de Duchenne de Boulogne, in:
Gastro-Enterologie et Maladies Neuromusculaires.
Evry, Association Francaise Contre les Myopathies,
1991, pp 79–87
20. Norris FH, Calanchini PR, Fallat RJ, et al: The ad-
ministration of guanidine in amyotrophic lateral
sclerosis. Neurology 1974;24:721–8
21. Bach JR, Kang SW: Disorders of ventilation: weak-
ness, stiffness, and mobilization. Chest 2000;117:
301–3
September 2008 Lung Insufflation Capacity 725
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
196 Miguel Ramalho do Souto Gonçalves

Study 7
Indications and Compliance of Home Mechanical
Insufflation-Exsufflation in Patients with
Neuromuscular Diseases
João Bento, Miguel Gonçalves, Nuno Silva, Tiago Pinto Anabela Marinho João Carlos Winck
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 197

Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
198 Miguel Ramalho do Souto Gonçalves

Órgano Oficial de la Sociedad Española de Neumología y Cirugía Torácica (SEPAR),la Asociación Latinoamericana del Tórax (ALAT) y la Asociación Iberoamericana de Cirugía Torácica (AIACT)
Volumen 46, Número 7, Julio 2010
www.archbronconeumol.org
Originales
Auditoria clínica de los pacientes hospitalizados por
exacerbación de EPOC en España (estudio AUDIPOC):
método y organización del trabajo
Factores asociados con el control del asma en
pacientes de atención primaria en España:
el estudio CHAS
Valores pretratamiento e inducidos por el tratamiento
de enolasa específica de neurona en pacientes con
cáncer de pulmón microcítico: estudio prospectivo,
abierto
Relación del test de control del asma (ACT) con la
función pulmonar, niveles de óxido nítrico exhalado
y grados de control según la Iniciativa Global para
el Asma (GINA)
Revisión
Hipercapnia permisiva o no permisiva: mecanismos
de acción y consecuencias de altos niveles de
dióxido de carbono
Artículo especial
Archivo de Archivos: 2009
Archivos deBronconeumolog ía
ISSN: 0300-2896
www.archbronconeumol.org
0300-2896/$ - see front matter © 2009 SEPAR. Published by Elsevier España, S.L. All rights reserved.
Arch Bronconeumol. 2010;46(8):420-425
Original Article
Indications and Compliance of Home Mechanical Insufflation-Exsufflation in Patients with Neuromuscular Diseases
João Bento,a,* Miguel Gonçalves,a,b Nuno Silva,c Tiago Pinto,a Anabela Marinho,a and João Carlos Winck,a,b
a Pulmonology Department, HS João, Oporto, Portugalb Faculty of Medicine, University of Porto, Oporto, Portugalc Linde homecare, Oporto, Portugal
*Corresponding author.
E-mail address: [email protected] (J. Bento).
A R T I C L E I N F O
Article info:
Received October 20, 2009
Accepted April 22, 2010
Keywords:
Mechanical insufflation-exsufflation
Home
Safety
Efficacy
Neuromuscular disease
Palabras clave:
Insuflación-exuflación mecánica
Domicilio
Seguridad
Eficacia
Enfermedad neuromuscular
A B S T R A C T
Introduction: Neuromuscular disease (NMD) patients frequently have impaired cough. Mechanical
insufflation-exsufflation (MI-E) has proven efficacy in improving airway clearance, however data related to
its long-term home use is lacking. The purpose of this study was to describe indications, safety and
compliance of home MI-E in NMD patients.
Methods: Four years observational analysis of 21 NMD patients on home MI-E. Diagnosis included bulbar
and non-bulbar Amyotrophic Lateral Sclerosis (ALS) and other NMD. Median age was 58 years. Only
cooperative patients with unassisted baseline Peak Cough Flow (PCF) < 270 L/min were included. All
patients were under continuous mechanical ventilation (6 by tracheostomy). Pulmonary function before
initiation of MI-E (median): FVC = 0.81 L, MIP = 28 cmH2O, MEP = 22 cmH2O and PCF = 60 L/min. MI-E was
performed by previously trained non-professional caregivers, with an on-call support of a trained health
care professional. Patients had pulse oximetry monitorization and applied MI-E whenever SpO2 < 95 %.
Median follow-up was 12 months (3-41 months).
Results: Ten patients (9 ALS) used MI-E daily. Eleven patients used MI-E intermittently, during exacerbations,
and in 8 patients early application of MI-E (guided by oximetry feed-back) avoided hospitalization. All
tracheostomized patients used MI-E daily and more times a day than patients under NIV. Four patients
(3 bulbar ALS), were hospitalized due to secretion encumbrance. MI-E was well-tolerated and there were
no complications. In general, caregivers considered MI-E effective. During this period, 4 patients died,
related to disease progression.
Conclusions: Home MI-E is well tolerated, effective and safe if used by well trained caregivers. MI-E should
be considered as a complement to mechanical ventilation.
© 2009 SEPAR. Published by Elsevier España, S.L. All rights reserved.
Indicaciones y cumplimiento con la insuflación-exuflación mecánica domiciliaria en pacientes con enfermedades neuromusculares
R E S U M E N
Introducción: Con frecuencia, los pacientes con enfermedades neuromusculares (ENM) presentan un dete-
rioro del mecanismo de la tos. Se ha demostrado la eficacia de la insuflación-exuflación mecánica (IEM) en
la mejora del aclaramiento de las vías respiratorias aunque no se dispone de datos relacionados con su uti-
lización domiciliaria a largo plazo. El objetivo del presente estudio fue describir las indicaciones, tolerabili-
dad y cumplimiento con la IEM domiciliaria en pacientes con ENM.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 199

J. Bento et al / Arch Bronconeumol. 2010;46(8):420-425 421
Métodos: Análisis observacional de 4 años de duración de 21 pacientes ENM tratados con IEM domiciliaria.
El diagnóstico incluyó esclerosis lateral amiotrófica (ELA) bulbar y no bulbar y otras ENM. La edad mediana
fue de 58 años. Sólo se incluyeron pacientes cooperadores con valores de flujo pico de tos basal (FTM) no
asistido < 270 l/min. Todos los pacientes estaban sometidos a ventilación mecánica continua (seis mediante
traqueostomía). La función pulmonar previa al inicio de la IEM (mediana) era: FVC, 0,81 l, MIP, 28 cmH2O,
MEP = 22 cmH2O y PCF = 60 l/min. Cuidadores no profesionales adiestrados previamente con el apoyo per-
manente de un profesional sanitario experto efectuaron la IEM. En los pacientes se monitorizó la pulsioxi-
metría y se aplicó IEM siempre que la SpO2 fue < 95 %. El seguimiento mediano fue de 12 meses (3-41 me-
ses).
Resultados: Utilizaron diariamente IEM 10 pacientes (nueve con ELA). La utilizaron de forma intermitente
11 pacientes durante las exacerbaciones y en 8 la aplicación precoz de IEM (guiada por la información de la
oximetría) evitó la hospitalización. Todos los pacientes traqueostomizados utilizaron la IEM a diario y un
mayor número de veces al día que los pacientes sometidos a ventilación mecánica no invasiva (VNI). Requi-
rieron ingreso hospitalario 4 pacientes (3 ELA bulbar) debido a la acumulación de secreciones. La IEM fue
bien tolerada y no se asoció a complicaciones. En general, los cuidadores la consideraron eficaz. Durante
este período, 4 pacientes fallecieron, en relación con la progresión de la enfermedad.
Conclusiones: La IEM domiciliaria es bien tolerada, eficaz y segura cuando la utilizan cuidadores adiestrados
apropiadamente. Debe considerarse un complemento de la ventilación mecánica.
© 2009 SEPAR. Publicado por Elsevier España, S.L. Todos los derechos reservados.
Introduction
Patients with neuromuscular diseases (NMD) frequently have weak respiratory muscles and a deteriorated cough mechanism. Effective coughing depends on the capacity of the inspiratory muscles to achieve an inspiration of about 80 % of total pulmonary capacity, followed by closure of the glottis and a pause with an increase in pulmonary volume. 1 After the contraction of the expiratory muscles, intrathoracic pressure increases and, when the glottis opens, air is expelled and secretions are propelled to the central airways. 1 Therefore, deterioration of the cough reflex in patients with NMD is related to weakness of the respiratory muscles, bulbar dysfunction that causes disability to control the glottis or even a deformity of the chest wall due to scoliosis. 1-5 Deterioration of the cough reflex causes insufficient airway clearance, pneumonia, athelectasia, and respiratory failure related to the accumulation of secretions. 2,5 Based on basal function, a peak cough flow (PCF) < 160 l/min has been proposed as an indication of an ineffectual cough. 2,5-8 However, Even a basal PCF < 270 l/min has been associated with pulmonary complications, since, during acute disease, there are additional reductions of the force of the respiratory muscles with an even greater reduction of PCF. 2,9-11 As a result, management of airway secretions, especially during intercurrent airway infections, is a significant problem in patients with NMD and is the main cause of morbidity, prolonged hospitalisation, intensive care admissions and mortality. 2,5,9,12-15 The techniques to improve airway clearance can reduce complications related to the accumulation of secretions and hospitalisation rates to a minimum. 3,15,16 However, in patients with chest wall deformity, physiotherapy and manually assisted expectoration techniques can be ineffectual. 17 These techniques are also time-consuming and require an appropriately trained carer.
Mechanical Insufflation-exsufflation (MIE) is a mechanically assisted cough technique. It gradually applies positive pressure to the airways, followed by a rapid change due to negative pressure. It can be applied using a face mask or a tracheotomy tube. 2,5 In 1953, the first device for mechanical assistance of coughing was marketed. Since then, various studies have confirmed its efficacy. MIE is considered more effective than other reference techniques to increase the coughing mechanism. 4,5,7 In spite of ever greater experience and published results on this technique, only limited data is available on its indications for home use, as also on compliance and safety.
The aim of this study is to describe the indications for home treatment using MIE, as also to determine its safety and compliance in patients with NMD.
Material and Methods
Since 1989, the Pneumology Service of the Sant João Hospital has an ambulatory clinic for NMD in collaboration with the Neurology Service. This clinic offers respiratory care to many patients suffering from NMD.
IEM devices have been used for home care since February 2005. The device was prescribed for continuous daily rent. These devices are included in the respiratory material offered to patients according to specific clinical indications. This material includes instruments for ventilation, monitoring, and control of secretions and is hired by a home care private company that also provides regular home visits by health professionals. The MIE device and a portable oximeter have a daily rental cost of 10 Euros. All the expenses caused by this home treatment are the responsibility of the Hospital. All the strategies related to clinical assessment of patients, adaptation of devices and programs for carer training are carried out by professionals from the Pneumology Service of the NMD ambulatory clinic.
All the patients prescribed home MIE were included in this study. An observational analysis was carried out with a 4 year follow-up. The patients were recruited in the Pneumology Service from those on the multidisciplinary NMD clinic. The protocol was approved by the Investigation Committee of the Hospital and the study was carried out according to the ethical directives for investigation in humans and the principles of the Helsinki Declaration (1975, revised in 1983).
Patients
Patients were studied from February 2005 to February 2009. Home MIE was prescribed for 21 NMD patients (15 men) of a median age of 58 years (27-72 years). The diagnosis included bulbar and non-bulbar amyotrophic lateral sclerosis (ALS), Duchenne muscular dystrophy (DMD) and other NMD. The demographic data of the population studied are described at table 1. Inclusion criteria were as follows: diagnosis of NMD, basal assisted < 270 l/min and continuous dependence on mechanical ventilation (24 hours a day). For the prescription of home MIE the decisive criteria was insufficient assisted PCF, after a technique of air entrapment (in patients with non-bulbar ALS) in combination with abdominal thrust. All patients with NMD receiving mechanical ventilation through a tracheotomy were also included.
Patients who could not cooperate or did not receive dedicated care were excluded. All patients depended on continuous home
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
200 Miguel Ramalho do Souto Gonçalves

422 J. Bento et al / Arch Bronconeumol. 2010;46(8):420-425
mechanical ventilation through a volume limited time-cycled ventilator (mean current volume 1,000 ml). At the beginning of the study, 6 patients had tracheotomy tubes and 15 patients used continues VNI combining ventilation through a mouthpiece during the day and ventilation with a face-mask during the night.
Before entering the ambulatory MIE protocol, 20 patients had come to the emergency service due to respiratory complications related to the accumulation of secretions (median 3 hospitalisations per patient) and 12 patients had required hospitalisation due to respiratory infections (median 2 hospitalisations per patient).
Determinations
All patients underwent pulmonary function, respiratory muscle force and PCF screening. Pulmonary function was determined by spirometry (Vmax 229, Autobox, Sensormedics), registering the maximum expiratory volume during the first second of forced expiration (FEV1) and forced vital capacity (FVC). All lung function tests were carried out in a sitting position according to reference procedures defined by the ATS-ERS 2005work group. 18
Maximum inspiratory pressure (MIP) and maximum expiratory pressure (MEP) were determined with a portable pressure manometer with an occludable mouthpiece (Micro RPM, Micromedical Limited) during maximum inspiratory and expiratory manoeuvres through the mouthpiece starting with the residual volume (MIP) and from total lung capacity (MEP). These determinations were performed according to reference procedures defined by the ATS-ERS 2002 work group. 19 The manoeuvres were repeated until three determinations with a variability < 5 % were obtained.
The PCF was only determined in non-tracheotomised patients by requesting the patient in a sitting position to carry out a cough manoeuvre beginning by total lung capacity (TLC) by means of a standard (Assess Healthscan products, Inc.) flow-meter connected to a face-mask.
Maximum insufflation capacity (MIC) was assessed by spirometry requesting the patient to retain 2 consecutive air volumes supplied by a manual resuscitator bag (air entrapment technique). 20 Bulbar deterioration and glottic dysfunction were evaluated in non-tracheotomised patients by assessing the MIC/FVC ratio. It was considered that patients with a ratio # < 1 presented bulbar dysfunction. For patients with appropriate bulbar function assisted PCF is determined after the air entrapment test with synchronised manual abdominal compression synchronised with the cough effort.
Since the patients with bulbar dysfunction could not carry out the air entrapment test, assisted PCF was only determined by application of manual abdominal compression.
Protocol for Home MIE
Home MIE was carried out using the Cough-Assist® (Philips, Respironics, Inc) device using an oronasal mask or a non-fenestrated tracheotomy tube with an inflated cuff. Both patients and carers were trained in the use of a portable pulse-oximeter (Nonin 9500
oximeter Minneapolis Plymouth USA) and given information on the use of MIE in their homes, in which a MIE session was applied in each episode of SpO2 < 95 %, until a value > 95 % was obtained. 23 For better tolerance periods of rest with ventilation between sessions were applied. Before the prescription of home MIE, all the patients and carers in our service were convened to receive specific training on the technique with a specialized respiratory physiotherapist. Training included device management (adjustments and circuit connections) and a practical seminar with clinical simulations, and also detection of clinical signs necessary to determine efficacy. Each session consisted of 6-8 cycles of insufflation-exsufflation with mean pressures of 40 to -40 cmH2O. The duration of each cycle was 3 seconds for insufflation, 2 seconds for exsufflation and 4 seconds for the post-exsufflation pause. During the exsufflation phase, patients were trained to cough, at the same time a carer applied abdominal compression. The adaptation of the technique was gradual, pressure was increased progressively to obtain an adequate chest expansion at a comfortable level to eliminate secretions.
Home MIE was always administered y non-professional trained carers (family members or private assistants) with the support of a health care professional with experience from a home care private company (nurse or respiratory physiotherapist). In case of doubt, the carer called the health professional to resolve the problem or to help carry out the technique in difficult situations. Both patients and carers were trained to detect early signs of respiratory failure or respiratory infections and were instructed to contact service staff (pneumologist or respiratory physiotherapist) on appearance of the first sign. Whenever dyspnoea increased, secretions accumulated or a value of SpO2 < 95 % persisted, in spite of continuous use of the ventilator and an aggressive home technique (with the support of expert health carers), the patients were instructed to come in to the emergency service (ES) of the local hospital. The aim of the treatment
Diagnosis Amyotrophic lateral
sclerosis
Duchenne muscular
dystrophy
Other neuromuscular
diseases
Multiple sclerosis All
Patients, number 15 2 3 1 21
Age (onset of respiratory deterioration) 62 (46-72) 32 (30-34) 35 (27-36) 68 58 (27-72)
Duration of symptoms, months 26 (9-90) 83 (27-139) 38 (8-271) 7 29 (7-271)
FVC (l and predictable %) 0.99 (0.4-1.93) 0.4 (0.26-0.54) 0.6 (0.26-0.84) 0.7 0.81 (0.26-1.93)
32.5 % (15-48 %) 9.5 % (7-12 %) 14 % (7-20 %) 29 % 27.5 % (7-48 %)
FEV1 (l and predictable %) 0.95 (0.3-1.76) 0.37 (0.24-0.49) 0.57 (0.24-0.84) 0.67 0.72 (0.24-1.76)
34 % (7-56 %) 10 % (7-13 %) 16.5 % (7-23 %) 33 % 28 % (7-56 %)
MIP (cmH2O) 31 (0-45) 14 (0-28) 16 (0-28) ND 28 (0-45)
MEP (cmH2O) 27 (0-56) 15 (3-27) 21 (3-27) ND 22 (0-56)
Spontaneous PCF (l/min) 60 (0-250) 90 (80-100) 115 (80-150) 40 60 (0-250)
Assisted PCF (l/min) 160 (0-260) 170 (160-180) 192.5 (130-250) 80 160 (0-260)
NIV, No. of patients 10 2 2 1 15
Tracheotomy, No. of patients 5 0 1 0 6
Time undergoing continuous ventilation
support, months.
24.5 (9-51) 81.5 (24-139) 37 (7-271) 6 29 (7-271)
Table 1
Characteristics and prior lung function in patients before applying mechanical insufflation-exsufflation protocol
FEV1 indicates forced expiratory volume in first second; MEP, maximum expiratory pressure; MIP, maximum inspiratory pressure; NIV, non invasive ventilation; PCF, peak cough
flow.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 201

J. Bento et al / Arch Bronconeumol. 2010;46(8):420-425 423
was defined as satisfactory control of acute dyspnoea or secretion accumulation, confirmed by pulse-oximetry data (SpO2 > 95 %).
Variables Analysed
A descriptive statistical analysis was performed using the SPSS 14.0 database for Windows. Data presented are function on diagnosis, symptom duration, time on mechanical ventilation, spirometry, force of respiratory muscles and assisted and non-assisted PCF. Compliance, tolerance and efficacy were assessed based on daily frequency of MIE use, number of complications, number of visits to the ES due to episodes of secretion accumulation and number of hospitalisations related to airway infections. Clinical files were analysed to assess the number of visits to the ES and the number of hospitalizations prior to the MIE protocol.
Intolerance and adverse effects of the technique were also examined.
Results
A total of 21 patients with NMD undergoing continuous mechanical ventilation (6 with tracheotomies) and home MIE treatment were studied. The diagnoses were the following: Amyotrophic lateral sclerosis (ASL) (n = 5), Duchenne muscular dystrophy (DMD) (n = 2), other NMDs (n = 3) and multiple sclerosis (EM) (n = 1) (table 1). Other NMDs included a heterogeneous group of diseases: Myopathy due to cytoplasmic inclusion bodies, type 2 spinal muscular atrophy and non-classified myopathies. Lung function prior to MIE can be seen at table 1.
Median time of onset of respiratory deterioration of the patients were 29 months (7-271 months) and had been using home ventilation support treatment for a median of 29 months (7-271 months) before their inclusion in the protocol (table 1). As to the ALS patients, at the beginning of the program, there were 6 patients with severe bulbar dysfunction. During follow-up, there was disease progression, so that, at the end of treatment, 10 patients presented severe bulbar dysfunction, 5 of them had undergone tracheotomy (5 rejected it). There was also a patient with non-classified myopathy, ventilated through a tracheotomy, without bulbar dysfunction, that rejected decannulation to VNI.
Compliance with MIE is shown in table 2. This technique was used daily by 10 patients (7 with bulbar ALS and 1 with non-classified myopathy) (table 2). The 6 patients with tracheotomy (5 with bulbar ALS and 1 with non-classified myopathy) and 4 patients undergoing VNI (2 with bulbar ALS that rejected tracheotomy and 2 with non-bulbar ALS) used the technique daily. The data related to daily frequency of sessions in the groups of daily users are shown in table 3. In this group, the patients with tracheotomies used MIE more times a day than those with VNI (table 3).
The technique was used intermittently by 11 patients (table 2). These patients only used the device during acute exacerbations, such as infection of the airways or during individual episodes of secretion accumulation. When the exacerbation was resolved of the secretions reduced to the point of maintaining a SpO2 > 95 %, its use was interrupted.
In general, the carers considered the device was effective.In 8 patients the early application of MIE (guided by oximetry
data) prevented visits to the ES due to an accumulation of secretions
and the device inverted the episode of desaturations and normalized SpO2 without the need to administer supplementary oxygen. The 8 patients and their respective carers reported that, if they had not had access to the device, they would have had to come in to the emergency service.
In 4 patients (3 bulbar ALS and 1 non-bulbar ALS), home MIE was not sufficient to normalise oxygen saturation and required hospitalisations to treat accumulated secretions during acute respiratory airway infections (table 4). Of the 3 bulbar ALS patients, one of them had undergone a tracheotomy and the other 2 had constantly rejected it.
Home MIE was well tolerated and there were no complications related to treatment (table 4).
During the study period, 4 patients with bulbar ALS died due to disease progression (table 4).
Discussion
The efficacy of MIE to increase PCF and improve the efficacy of cough manoeuvre has already been demonstrated. 1-4,7,13,14,21,22 Chatwin et al compared different interventions (cough assisted by physiotherapy, cough assisted by VNI, cough assisted by exsufflation and MIE) with non-assisted cough and showed that MIE was the technique associated with the greatest increase in PCF. 4 Oximetry data has shown the usefulness of this technique since it makes it possible to detect a sudden decrease of oxygen saturation as a consequence of a mucous plug. 2,3,15,21 The patients described in this study suffered from severe ventilation failure and continuously depended on mechanical ventilation (24 hours a day). They had all used volume limited time-cycled ventilation for many years before inclusion in the study.
This study was based on the protocol proposed by Bach et al, that consists in home treatment with a VNI support, oximetry monitoring during 24 hours and the use of MIE guided by the data from this (SpO2 < 95 %). 3,7,15,23,24
In this study home MIE was carried out by non-professional carers of the patients with the support of health professionals trained in home care.
Few studies have described home respiratory treatment with MIE in patients with NMD, although many studies describe the efficacy of the combination of cough assistance techniques, manual and mechanical, in acute in-hospital situations. 8,9,21 Although MIE carried out by non-professional carers has been considered effective and well tolerated, it causes certain controversy and we still require more data on its home use in the long term. 15,21,23,24
In our strategy, the main condition for effective home care after hospital discharge was the presence of appropriately trained and
Diagnosis Bulbar amyotrophic
lateral sclerosis
Non-bulbar amyotrophic
lateral sclerosis
Duchenne muscular
dystrophy
Other myopathies Multiple sclerosis All
Daily users 7 2 0 1 0 10
Intermittent users 3 3 2 2 1 11
Table 2
Compliance with mechanical insufflation-exsufflation
Patients with ventilator support Median (min-max) No. of patients
Users of ventilations that
underwent tracheotomy
6 (3-6) times a day 6 (100 %)
Users of non-invasive ventilation 3 (1-4) times a day 4 (26.7 %)
All 4.5 (1-6) times a day 10 (47.6 %)
Table 3
Daily users of mechanical insufflation-exsufflation
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
202 Miguel Ramalho do Souto Gonçalves

424 J. Bento et al / Arch Bronconeumol. 2010;46(8):420-425
motivated carers. This study supports the importance of an appropriate early training phase, administered to both patients and carers in the hospital, as has also been proposed by Tzeng et al. 15 Furthermore, This study confirmed that carers with appropriate training and motivation can detect respiratory worsening and effectively use a home MIE protocol. Patients with neuromuscular diseases, especially ALS, can suffer progressive disease with early decrease of respiratory muscle force and cough deterioration, both associated with premature death. 3,9,14,25,26 The natural course of NMD does not make it possible to clarify the influence of home MIE on visits to the ES/hospitalizations. The number of episodes before and after the home MIE protocol is not comparable. Indeed, before beginning home treatment, the patients’ cough reflex was more powerful and therefore, they suffered fewer episodes of secretion accumulation. In contrast to other NMD, ALS also includes glottic muscle control. In general, in patients with non-bulbar NMD non-invasive support treatment may be used and they have a higher survival rate. 3,5,16 However, the almost inevitable progression to bulbar dysfunction is one of the more negative characteristics of this disease and the main reason due to which, in contrast to other NMDs, tracheotomy becomes necessary to prolong survival. 1,3,6-9,12,13,16,23,24,26,27 The MIC/FVC ratio has been widely used to assess bulbar function, due to the fact that appropriate glottic function is necessary to accumulate consecutive volumes of air to achieve MIC. 20 Furthermore, a severe bulbar dysfunction is also responsible for dysfunction of the higher respiratory airway muscles in this group of patients. 2,4,13,23,25 Sancho et al have identified 2 types of bulbar ALS patients: those that only suffer from failure of glottis closure that cannot entrap air but in which MIE can be effective and those that present a dynamic collapse of the upper respiratory airways in which MIE is not effective and can even cause risk. 25 In this study, ALS, the most usual diagnosis, is seen in a heterogeneous group: from a non-bulbar disease with inadequate PCF to a severe bulbar disease that requires tracheotomy. This in itself represents an additional problem concerning patient acceptance or associated problems (local inflammation, increase of secretions and infections). 2,3,12,15,26,28 Indeed, although it was offered to all patients with severe bulbar dysfunction, some continued to reject it and preferred to continue with VNI and the MIE protocol. Bach et al have also described the fact that patients with severe bulbar ALS can receive support treatment with the combined use of VNI and MIE, which delays tracheotomy, as long as they can maintain an oxygen saturation > 95 % with ambient air. 23 However, these patients required careful regular supervision to anticipate the failure of a non-invasive strategy, so that therapeutic options can be examined and analysed with patients and their families, so that decisions can be made beforehand and not at the time of a respiratory crisis. Farrero et al have suggested that a follow-up every 3 months or on patient demand makes it possible to opportunely recognise disease progression. 16
In this study, each MIE session consisted of 6-8 cycles of insufflations-exsufflations with mean pressures of 40 to –40 cm H2O, titrated according to patient tolerance. Chatwin and Sivasothy have considered that lower pressures are more comfortable and involve fewer risks. 4,17 However, the adjustments used in this study are widely preferred due to their effects on patient welfare and their efficacy and are also suggested by the manufacturers. 1,3,8,24,29 In general, they are well tolerated and have been considered the most effective means of obtaining higher values of PCF with practically no complications. 1,3,5,7,8,21,24 In spite of this, we paid special attention to careful individual titration of the MIE pressure, to obtain maximum chest expansion, respecting welfare, which can justify the tolerance and absence of complications seen in this study. The application of MIE was adjusted to the needs of each patient in as far as frequency of use, considering daily and intermittent users. With intermittent users it was not possible to register the number of MIE sessions per month or week because compliance was not regular and depended on the number and severity of respiratory exacerbations. In contrast, daily users reported that they used the device every day, independently of exacerbations, both for secretion control and for lung insufflation and to revert episodes of SpO2 < 95 %. This study also shows that patients that had undergone tracheotomy used MIE daily and more times a day than patients with VNI. This fact may be due to local inflammation and the increase of secretions related to tracheotomy. We also found that some patients with bulbar ALS, incapable of air entrapment, did not only use MIE as a technique for cough assistance, but also for lung insufflation.
According to this study, both patients and carers described greater efficacy in clearance of airway secretions with this home protocol. Its early application, guided by oximetry data with normalisation of oxygen saturation with ambient air, prevented visits to the Emergency Service due to secretion accumulation. Patients stated that, during these episodes, without MIE, they would have had to go to hospital due to their acute respiratory problems. Furthermore, there were very few episodes in which home MIE was not sufficient to resolve the problem of secretion accumulation and made it unnecessary to visit the ES or to require hospitalisation. None of these patients required intubation. Indeed, it would seem that the protocol reduces the risk of airway infection and prevents both visits to the ES and hospitalizations. Bach et al have reported that patients with NMD dependent on VNI that used MIE guided by oximetry data can be treated at home without risk or need of hospitalisation. 3,6,7,13,14,15
This study did not show any complications related to use of the device. Potential complications are very infrequent and include abdominal distension, increase of gastroesophageal reflux, haemoptysis, chest and abdominal discomfort, acute cardiovascular events, barotraumas and pneumothorax. 5 Bach et al have not described any complications in more than 500 batches of MIE. 7 Some simple but prudent measures to prevent complications are: brief
Diagnosis Bulbar amyotrophic
lateral sclerosis
Non-bulbar amyotrophic
lateral sclerosis
Duchenne muscular
dystrophy
Other
myopathies
Multiple
sclerosis
All
Patients, No. 10 5 2 3 1 21
Time undergoing MIE, months 6.5 (3-41) 19 (12-38) 7.5 (3-12) 16 (6-16) 4 12 (3-41)
Intolerance MIE 0 0 0 0 0 0
Complications due to MIE 0 0 0 0 0 0
Visits to the emergency service
(No. of patients/No. of events)
3/5 1/1 0/0 0/0 0/0 4/6
Hospitalisations
(No. of patients/No. of events)
3/3 1/1 0/0 0/0 0/0 4/4
Deaths, No. of patients 4 0 0 0 0 4
Table 4
Follow-up and results of mechanical insufflations-exsufflation
MIE indicates mechanical Insufflation-exsufflation.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 203

J. Bento et al / Arch Bronconeumol. 2010;46(8):420-425 425
pauses between applications (to avoid hyperventilation), avoiding applications after meals, appropriate treatment of gastroesophageal reflux and reduction of insufflation pressure according to tolerance. 5
During the study period, 4 patients with bulbar ALS died. The main cause of death was rapid progressive disease with severe bulbar dysfunction. These 4 patients had constantly rejected tracheotomy.
The main limitations of this study are the fact that it is observational, the reduced number of patients including the absence of a control group. However, shortly after beginning this protocol, the benefits of the treatment as far as efficacy in management of accumulated secretions, preventing visits to the Emergency Service and improvement of quality of life in these patients became evident As a result, we consider that it would not be ethical to deprive the patients of a treatment that has been shown to be effective.
Conclusion
The most important conclusion of this study is that it is possible to treat patients with severe NMD with sufficient clearance of the secretions of their respiratory airways with home MIE based on careful training of non-professional carers. This is valid for patients with VNI and those with tracheotomies. According to the patients, greater use of MIE during respiratory infections can prevent visiting the emergency service.
This technique can be considered a useful complement to ventilation support in these patients.
References
1. Gomez-Merino E, Sancho J, Martin J. Mechanical insufflaton-exsufflation: pressure, volume and flow relationships and the adequacy of manufacturer’s guidelines. Am J Phys Med Rehabil. 2002;81:579-83.
2. Servera E, Sancho J, Zafra MJ. Cough and neuromuscular diseases. Noninvasive airway secretion management. Arch Bronconeumol. 2003;39:418-27.
3. Bach JR. Amyotrophic lateral sclerosis: prolongation of life by non-invasive respiratory aids. Chest. 2002;122:92-8.
4. Chatwin M, Ross E, Hart N, Nickol AH, Polkey MI, Simonds AK. Cough augmentation with mechanical insufflation/exsufflation in patients with neuromuscular weakness. Eur Respir J. 2003;21:502-8.
5. Homnick DN. Mechanical insufflation-exsufflation for airways mucus clearance. Respir Care. 2007;52(10):1296-305.
6. Bach JR. Amyotrophic lateral sclerosis: predictors for prolongation of life by non-invasive respiratory aids. Arch Phys Med Rehabil. 1995;76:828-32.
7. Bach JR. Mechanical insufflation-exsufflation. Comparison of peak expiratory flows with manually assisted and unassisted coughing techniques. Chest. 1993;104:1553-62.
8. Bach JR, Saporito LR. Criteria for extubation and tracheostomy tube removal for patients with ventilatory failure: a different approach to weaning. Chest. 1996;110:1566-71.
9. Sancho J, Servera E, Diaz J, Marin J. Predictors of ineffective cough during a chest infection in patients with stable amyotrophic lateral sclerosis. Am J Respir Crit Care Med. 2007;175:1266-71.
10. Mier-Jedrezejowicz A, Brophy C, Green M. Respiratory muscle weakness during upper respiratory tract infections. Am Rev Respir Dis. 1988;138:5-7.
11. Poponick JM, Jacobs I, Supinski G, DiMarco AF. Effect of upper respiratory tract infection in patients with neuromuscular disease. Am J Respir Crit Care Med. 1997;156:659-64.
12. Bach JR, Rajaraman R, Ballanger F, Tzeng AC, Ishikawa Y, Kulessa R, et al. Neuromuscular ventilatory insufficiency: the effect of home mechanical ventilator use vs oxygen therapy on pneumonia and hospitalization rates. Am J Phys Med Rehabil. 1998;77:8-19.
13. Bach JR. Mechanical insufflation/exsufflation: has it come of age? A commentary. Eur Respir J. 2003;21:385-6.
14. Gomez-Merino E, Bach JR. Duchenne muscular dystrophy: prolongation of life by noninvasive ventilation and mechanically assisted coughing. Am J Phys Med Rehabil. 2002;81:411-5.
15. Tzeng AC, Bach JR. Prevention of pulmonary morbidity for patients with neuromuscular disease. Chest. 2000;118:1390-6.
16. Farrero E, Prats E, Povedano M, Martinez-Matos JA, Manresa F, Escarrabill J. Survival in amyotrophic lateral sclerosis with home mechanical ventilation: the impact of systematic respiratory assessment and bulbar involvement. Chest. 2005;127:2132-8.
17. Sivasothy P, Brown L, Smith IE. Effect of manually assisted cough and mechanical insufflation on cough flows of normal subjects, patients with chronic obstructive pulmonary disease (COPD) and patients with respiratory muscle weakness. Thorax. 2001;56:438-44.
18. Pellegrino R, Viegi G, Brusasco V, Crapo RO, Burgos F, Casaburi R, et al. Series “ATS/ERS task force: standardisation of lung function testing”. Eur Respir J. 2005;26:948-68.
19. American Thoracic Society/European Respiratory Society. ATS/ERS Statement on Respiratory Muscle Testing. Am J Respir Crit Care Med. 2002;166:518-624.
20. Bach JR, Kang SW. Disorders of ventilation. Chest. 2000;117:301-3.21. Vianello A, Corrado A, Arcaro G, Gallan F, Ori C, Minuzzo M, et al. Mechanical
insufflation-exsufflation improves outcomes for neuromuscular disease patients with respiratory tract infections. Am J Phys Med Rehabil. 2005;84:83-8.
22. Winck JC, Gonçalves MR, Lourenço C, Viana P, Almeida J, Bach JR. Effects of Mechanical Insufflation-Exsufflation on Respiratory Parameters for patients with chronic airway secretion encumbrance. Chest. 2004;126:774-80.
23. Bach JR, Bianchi C, Aufiero E. Oximetry and indications for tracheotomy for amyotrophic lateral sclerosis. Chest. 2004;126:1502-7.
24. Gonçalves MR, Bach JR. Mechanical insufflation-exsufflation improves outcomes for neuromuscular disease patients with respiratory tract infections. A step in the right direction. Am J Phys Med Rehabil. 2005;84:89-91.
25. Sancho J, Servera E, Díaz J, Marín J. Efficacy of Mechanical Insufflation-Exsufflation in Medically Stable Patients with Amyotrophic Lateral Sclerosis. Chest. 2004;125:1400-5.
26. Simonds AK. Recent advances in respiratory care for neuromuscular disease. Chest. 2006;130:1879-86.
27. Magnus T, Beck M, Giess R. Disease progression in amyotrophic lateral sclerosis: predictors of survival. Muscle Nerve. 2002;25:709-14.
28. Bach JR. A comparison of long-term ventilatory support alternatives from the perspective of the patient and the care giver. Chest. 1993;104:1702-6.
29. Bach JR. Noninvasive respiratory muscle aids: intervention goals and mechanism of action. In Management of patients with neuromuscular disease. Philadelphia, PA: Hanley & Belfus; 2004. p. 211-69.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
204 Miguel Ramalho do Souto Gonçalves

Study 8
At Home and on Demand Mechanical Cough Assistance
Program for Patients With Amyotrophic Lateral
Sclerosis
Michele Vitacca, Mara Paneroni, Debora Trainini, Luca Bianchi, Giuliano Assoni ND, Manuela Saleri RTD, Sonia Gilè PHD, João C. Winck and
Miguel R. Gonçalves
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 205

Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
206 Miguel Ramalho do Souto Gonçalves

Authors:
Michele Vitacca, PhDMara Paneroni, RTDDebora Trainini, RTDLuca Bianchi, PhDGiuliano Assoni, NDManuela Saleri, RTDSonia Gile, PhDJoao C. Winck, PhDMiguel R. Goncalves, RTD
Affiliations:
From the UO di PneumologiaRiabilitativa e Terapia IntensivaRespiratoria (MV, MP, DT, LB, MS,SG), Fondazione Salvatore MaugeriIRCCS, Lumezzane, Brescia, Italy;Servizio di Telemedicina FondazioneSalvatore Maugeri IRCCS (GA),Lumezzane, Brescia, Italy; and LungFunction and Ventilation Unit (JCW,MRG), Pulmonology Department andFaculty of Medicine, UniversityHospital S. Joao Porto, Portugal.
Correspondence:
All correspondence and requests forreprints should be addressed to:Michele Vitacca, PhD, FondazioneSalvatore Maugeri, IRCCS, Division ofPneumology, Via Giuseppe Mazzini,129, 25066 Lumezzane, Brescia, Italy.
Disclosures:
This study was supported, in part, bythe Associazione Italiana SclerosiLaterale Amiotrofica, grant no.060765. Financial disclosurestatements have been obtained, andno conflicts of interest have beenreported by the authors or by anyindividuals in control of the contentof this article.
0894-9115/10/8905-0401/0
American Journal of Physical
Medicine & Rehabilitation
Copyright © 2010 by Lippincott
Williams & Wilkins
DOI: 10.1097/PHM.0b013e3181d89760
At Home and on DemandMechanical Cough AssistanceProgram for Patients WithAmyotrophic Lateral Sclerosis
ABSTRACT
Vitacca M, Paneroni M, Trainini D, Bianchi L, Assoni G, Saleri M, Gile S, WinckJC, Goncalves MR: At Home and on Demand Mechanical Cough AssistanceProgram for Patients With Amyotrophic Lateral Sclerosis. Am J Phys MedRehabil 2010;89:401–406.
Objective: To establish a cost-effective telephone-accessed consultationand mechanical in-exsufflation (MI-E) and manually assisted coughing, oxim-etry feedback program for 39 patients with amyotrophic lateral sclerosis.
Design: Rapid access to healthcare consultation and to MI-E wasprovided to treat episodes of distress as a result of secretion encum-brance not reversed by suctioning and associated with a decrease inoxyhemoglobin saturation (SpO2) baseline. Avoided hospitalizations, de-fined by relief of respiratory distress and return of SpO2 baseline to�95% by continuous ventilator use and assisted coughing, were re-corded. Patient satisfaction was queried at 6 mos, and a cost analysis wasperformed of continuous vs. on demand MI-E use.
Results: Thirty-nine patients made a total of 1661 calls in 7.46 � 5.8mos of follow-up. Twenty-seven patients had 66 home care visits by arespiratory therapist for a total time commitment of 89.7 � 99.3 min/patient/mo. Twelve patients, all ventilator users, were also brought me-chanical in-exsufflators for mechanically assisted coughing for 47 respi-ratory episodes. Thirty hospitalizations were avoided. Seventy-five percentof the patients were extremely satisfied. Mean monthly cost per patient foron-demand telephone consultation, professional home healthcare visits,and MI-E as deemed necessary was €403 � €420 or 59% less than forcontinuous MI-E rental. Hospitalization costs were also spared.
Conclusions: An on-demand consult and MI-E access program canavoid hospitalizations for patients with amyotrophic lateral sclerosis withsignificant cost savings.
Key Words: Amyotrophic Lateral Sclerosis, Home Care, Acute Respiratory Failure,
Mechanically Assisted Coughing
www.ajpmr.com Cough Assistance in ALS 401
ORIGINAL RESEARCH ARTICLE
ALS
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 207

For patients with neuromuscular diseases, in-cluding amyotrophic lateral sclerosis (ALS), con-tinuous dependence on noninvasive intermittentpositive pressure ventilation (NIV) can markedlyprolong survival,1 maintain optimal quality-of-life,2 and along with mechanically assisted cough-ing (MAC)3–5 can be used in the home to avoidhospitalizations, acute respiratory failure with en-dotracheal intubation, and tracheotomy.4,6,7 MACis the use of mechanical in-exsufflation (MI-E)8
with an exsufflation-timed abdominal thrust. Al-though effective when continuously available, ex-pense can be mitigated by on-demand rather thancontinuous access if on-demand use can be dem-onstrated to be effective.
Severe bulbar-innervated muscle dysfunctionwith inability to protect the airways can renderMI-E ineffective, and even when effective, patientscan require considerable assistance and train-ing.1,7,9 In Europe, home respiratory care is ofteninadequate because home care companies provideonly equipment, not assistance, instruction, or ex-pertise for which the patient must depend on emer-gency services,10 and there is great burden oncaregivers.11 Thus, hospitalization rates andlengths of stay are high, especially when acuterespiratory failure and intubation result in trache-otomy. Even in the United States, it has beenreported that the mean hospitalization duration forpatients with neuromuscular disease undergoingtracheotomy is 72 days, most of which is spent inintensive care12,13 at great expense, and long andexpensive ventilator weaning unit stays often fol-low this.
To help reduce costs, avoid hospitalizations,and establish an optimal MI-E provision regimen athome, we studied a telephone-accessed integratedcare14 program with oximetry feedback that pro-vided equipment and professional home care ser-vices on an “as needed basis” to treat clinical exac-erbations and related respiratory problems.
METHODS
All 47 patients with a diagnosis of ALS accord-ing to El Escorial criteria15 referred to our reha-bilitation department for adaptation and trainingin some combination of cough assistance, mechan-ical ventilation, and tracheostomy managementwere analyzed. Our center has 145 beds for multi-disciplinary intermediate care. Reimbursement de-pended on diagnosis and comorbidities. Exclusioncriteria were death before enrollment, location�80 km from the center, and inadequate careproviders or cooperation. The protocol was ap-proved by the ethics committee, and the study wasconducted in accordance with the ethical standardsof the Declaration of Helsinki (1975, revised in
1983, clinical trials identifier #NCT00613899). Allpatients gave informed consent.
Hospital Phase: Training
All patients were offered the telephone-ac-cessed integrated care program that included tele-phone access to a triage nurse who directed thecalls to a pulmonologist, neurologist, psychologist,or physio-respiratory therapist (RT) for consulta-tion14 and possibly home visit. The patients wereeducated and trained in oximetry feedback (9500 byNonin, Minneapolis Plymouth) to maintain or re-turn SpO2 to �95% by manually assisted coughingor MAC or both as needed4,16,17 and in mechanicalventilation, including interface use, cleaning, hu-midification, safety, and tracheostomy care, as ap-propriate. Manually assisted coughing involved theapplication of deep lung insufflation followed byabdominal thrust. For MAC, the maximum toler-ated MI-E pressures (range, 35–60 cmH2O) wereused. The tube cuff was inflated for MI-E use viatracheostomy tubes.18
The patients were told to contact the call cen-ter for: dyspnea, 3% reduction in baseline SpO2,20% increase in need for deep airway suctioning,18
increased airway mucus congestion or changes insecretion properties,19 fever, headache, asthenia,sleepiness, or confusion, and consideration for an-tibiotic therapy.16
Before discharge, the patients underwent pul-monary function testing, including spirometry(VMAX 20, Sensor Medics, Yorba Linda, CA) andpeak cough flow measurement via a standard peakflow meter (MiniRight Peak Flow Meter, ClementClarke International, England, UK) connected to afacial interface.20
Home Phase
An RT called each patient every 7 days. Thecalls and home visits reinforced the oximetry/as-sisted coughing protocol. MI-E was brought topatients for whom, despite NIV or tracheostomyintermittent positive pressure ventilation (TIV) andmanually assisted coughing, the SpO2 would notremain �94%.3,4,16 All patients were instructed tocall the emergency service for hospitalization if theSpO2 remained �95% despite continuous ventila-tory support and assisted coughing, includingMAC.
Outcome Measurements
Mortality and the number of telephone callsfor assistance, respiratory exacerbations with SpO2
baseline �95%, RT home visits, home MAC rent-als, days of home MAC requirement, the percentageof SpO2 improvement with intervention, side ef-fects of MAC, avoided hospitalizations defined byrelief of dyspnea and return of SpO2 baseline to
402 Vitacca et al. Am. J. Phys. Med. Rehabil. ● Vol. 89, No. 5, May 2010
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
208 Miguel Ramalho do Souto Gonçalves

�95% by assisted coughing and continuous venti-latory support without hospitalization, and hospi-talizations were recorded. At 6 mos, patients werealso telephoned to question their satisfaction andestimate the efficacy of the program.
Costs
On-call telephone access costs have been al-ready reported by our group.14 The RT home visitsand rental costs for suction machine, manualresuscitator, and ventilator were additional. Perdiem MI-E rental costs were compared with con-tinuous rental costs in Italy and in the UnitedStates. The latter information was provided by anaccredited respiratory home care company (Mil-lennium Respiratory Services, Whippany, NJ) atMedicare reimbursement rates. Inpatient respi-ratory rehabilitation admission costs were €289per day, and critical care costs were €1600 perday. When applicable, costs were converted fromdollars to euros.
Statistical Analysis
Descriptive data are reported as mean � SD.Statistical analysis was performed by using SPSSsoftware (Release 12.0 SPSS, Chicago, IL). For allparameters, the differences between treatmenttimes were analyzed using a paired Student’s t testfor the parametric variables and an unpaired Wil-coxon-test for the nonparametric ones. P values�0.05 were considered significant.
RESULTS
Between October 2006 and September 2008,47 consecutive patients with ALS were screened.Eight were excluded: three died before enrollment,two refused to participate, one lived �80 km from
the referring center, one showed poor compliance,
and one had no caregiver. The remaining 39 re-
ceived riluzole and were followed up for 7.46 � 5.8
mos. Twenty-seven of the 39 were ventilator users.
Their baseline anthropometric, clinical, and func-
tional characteristics are shown in Table 1. All
tracheotomized patients (n � 12) required contin-
uous TIV, whereas the NIV patients (n � 15) used
NIV 8–16 hr/d.
Telephone-Accessed Integrated Care
Program
The total nurse/RT time commitment was
1.49 � 1.65 hr/patient/mo or the equivalent of a 0.4
full-time RT. During the 7.46 � 5.8-mo follow-up,
there were 1661 calls with a high interindividual
variability (6.65 � 6.45, range 1–138). All except
one call to a physician was triaged to an RT. Seven
and one-half percent of the calls triggered a home
RT visit. Sixty-seven home visits were required and
38 had MI-E delivered.
Outcomes and hospitalization data are listed in
Table 2. Overall, 10 NIV users (26%) died: two
suddenly and eight from respiratory causes and
refusing intubation. Only 1 of the 10 called the
center. No TIV user died.
All MAC deliveries were for TIV and NIV users
who were also followed up for a longer than aver-
age period of time. Table 3 shows outcomes of MAC
intervention performed during a 12.6 � 3.3-mo
period. The latency period for initiating home MAC
use was 3 � 3 mos for the tracheotomy patients
and 10 � 3 mos for the NIV users. The TIV users
required MI-E twice as many days per month as the
NIV users.
TABLE 1 Patient characteristics
Patients (n) 39Age, years � SD (range) 62 � 11 (39–83)Gender (M/F) 21/18Years of diseasea 3.47 � 3.21Distance from the referring center, Km (range) 34 � 18 (1–80)Bulbar/nonbulbar involvementb 23/16No ventilator use (n) 12NIV users (n) 15TIV users (n) 12VC, % predicted (n) Total population (24) 66 � 29
Tracheotomized patients (6) 50 � 20Nontracheotomized patients (30) 71 � 29
PCF, cmH2O (n � 27) no-T patients 186 � 113PEF, cmH2O (n � 12) 88 � 51
aFrom diagnosis.bFrom time of respiratory therapist evaluation.TIV, tracheostomy mechanical ventilation; NIV, noninvasive mechanical ventilation; VC, vital capacity; PCF, peak cough
flow; PEF, peak expiratory flow.
www.ajpmr.com Cough Assistance in ALS 403
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 209

Costs
Table 4 shows costs. One NIV and two nonven-tilator users underwent tracheotomy during thestudy. Comparing the costs of “on-demand” MI-Ewith standard continuous use for the 6660 days ofventilator use for the 27 patients, the cost savingswas €108,758.
The daily rental of MI-E in the United States is$10 per day for a monthly rental and Medicarereimbursement of $424 (€301). Rental for mechan-ical ventilation, MI-E, and supplies and on-call RTservices is about $1000 per month or about 30%greater than the cost of this rental program. Theavoidance of 34 hospitalizations added to the costsavings.
All 39 patients were satisfied with the project,and 86% of the MAC users considered it effective,whereas 14% considered it somewhat effective.There were no significant side effects of assistedcoughing, including MAC.
DISCUSSION
For patients with ALS, a program of tele-phone access and as needed home intervention,including manually assisted coughing and MAC,was shown to be feasible, well tolerated, and costeffective. A previous ALS study used continuousvideoconferencing and telephone consultationfor four patients with ALS, although it was lim-ited by the small number of subjects and by their
TABLE 3 Outcomes of the 12 users of mechanically assisted coughing
Patients Having RTVisits and Provision
of MI-E (n � 12)
TIV Users Having RTVisits and Provision
of MI-E (n � 9)
NIV Users Having RTVisits and Provision
of MI-E (n � 3)
Total home MI-E rentals,a n 30 27 3Mean change in SpO2 (%) with
intervention, all baselines werecorrected
�3.2 � 0.8 3.5 � 0.9 2.2 � 0.0
Total MI-E rental days, n 46.7 � 27.4 56.7 � 24 16.7 � 5.8Time to normalization of baseline SpO2
�20 days 33% 0 34%20 and 40 days 17% 34% 66%�40 days 50% 66% 0
Days of home MI-E rental, n 54.2 � 30.0 50 � 28.2 23.3 � 11.5
aHome respiratory therapist (RT) visit for reinforcement of instruction in manually assisted coughing and provision of amechanical insufflator-exsufflator for mechanically assisted coughing (MAC).
TIV, tracheostomy intermittent positive pressure ventilation; NIV, noninvasive intermittent positive pressure ventilation;MI-E, mechanical insufflation-exsufflation; SpO2, pulse oxyhemoglobin saturation.
TABLE 2 Outcomes of home care visits
Total PatientsHaving Home
Visits (n � 27)
Patients WithHome Visits
Only(n � 15)
Patients WithHome VisitsPlus MI-Ea
(n � 12)
TIV Users HavingHome Visits and
Provision of MI-E(n � 9)
NIV Users HavingHome Visits and
MIE (n � 3)
Total respiratoryexacerbations, n
67 20 47 40 7
Home visits withoutMI-E delivery, n
13 4 9 9 0
Home visits plusprovision of MI-E, n
21 0 21 18 3
Patients hospitalized, n 18 8 10 7 3Total hospitalizations, n 33 16 17 13 4Avoided
hospitalizations, n34/67 (51%) 4/20 (22%) 30/47 (64%) 27/40 (67%) 3/7 (42%)
Avoided hospitalizations are defined by the domiciliary need for continuous ventilatory support and correction of a persistentdecrease in baseline oxyhemoglobin saturation by assisted coughing.
aOnly the TIV and NIV users required home visits plus MI-E, all of which resulted in correction of SpO2 baseline by somecombination of adjusting ventilator use and assisted coughing.
TIV, tracheostomy intermittent positive pressure ventilation; NIV, noninvasive intermittent positive pressure ventilation;MI-E, mechanical insufflation-exsufflation.
404 Vitacca et al. Am. J. Phys. Med. Rehabil. ● Vol. 89, No. 5, May 2010
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
210 Miguel Ramalho do Souto Gonçalves

inability to master the use of the Internet and
Webcams.21
Patients with severe bulbar-innervated muscle
dysfunction and those with only moderate dysfunc-
tion but without tracheostomy tubes are consid-
ered to have a poor prognosis.9 However, our re-
sults indicate that the severity of clinical
exacerbations as a result of airway secretion en-
cumbrance in such patients can be monitored and
secretion expulsion guided by oximetry. Normal-
ization of SpO2 baseline by aggressive assisted
coughing and MAC can avert hospitalization de-
spite continuous ventilatory support. This can only
be effective with trained care provider assistance.16
This is consistent with the findings of Bach et
al.12,22,23 who in one study demonstrated that an
uncorrected decrease in baseline SpO2 �95% re-
sulted in 33 of 35 patients with ALS dying or
requiring tracheotomy within 2 mos, but that
about one-half of such patients’ baseline SpO2s can
be temporarily normalized by MAC for about 11
mos.4 Thus, a motivated caregiver can often use
NIV and cough assistance to prevent acute respira-
tory failure for ALS as has also been described for
patients with Duchenne muscular dystrophy3,24
and other patient populations.16
Oximetry monitoring with on-demand medical
attention and MAC is a cost-saving alternative to
institutionalization and to continuous access to
MI-E. In one study in which the indication for
continuous home MI-E prescription was assisted,
peak cough flow �300 L/m as opposed to the mean
of 186 L/m (unassisted) peak cough flow in our
patients, the average period of time before MI-E
was needed to avert a hospitalization with contin-
uous rental was 11 mos.3 In our study, 56% of the
patients did not obtain MI-E at all, and those who
used it, did so for �20% of the total follow-up
period.
In conclusion, the telephone access and on-
demand MAC program increased both the patients’
and clinicians’ feelings of security for home man-
agement and was effective in averting hospitaliza-
tions for patients with ALS. Limitations of the
study are (1) lack of controls; (2) lack of quality-
of-life assessment; and (3) lack of outcomes com-
parisons with programs in which MI-E access is
continuous.
ACKNOWLEDGMENTS
We thank Mario Melazzini, who is a doctor,
patient, and profound human being, for his joy of
being alive. We also thank Millennium Respiratory
Services, Whippany, NJ, for their support in pro-
viding data.
TA
BLE
4H
ome
cost
sof
the
proj
ect
Item
sT
ota
lG
rou
pU
nit
ary
Cost
(€)
Tota
lC
ost
(€)
Gro
up
Wit
hR
espir
atory
Car
e(n
�27)
Su
bto
tal
Cost
(€)
Gro
up
Wit
hou
tR
espir
atory
Car
e(n
�12)
Su
bto
tal
Cost
(€)
MV
hom
eeq
uip
men
tco
sts
No
ven
tila
tor
use
(n�
11)
4860
day
s0
0N
ove
nt
(n�
5)
0N
ove
nt
(n�
6)
0N
IVu
sers
(n�
13)
4950
day
s4
19,8
00
NIV
(n�
11)
13,3
20
NIV
(n�
2)
6,4
80
TIV
use
rs(n
�15)a
5460
day
s30
163,8
00
TIV
(n�
11)
144,9
00
TIV
(n�
4)
18,9
00
Cal
lsto
TM
,n
1661
20
33,2
20
1359
27,1
80
302
6040
Hom
evi
sits
,n
66
68
4,4
88
66
4,4
88
00
MI-
Eac
tiva
tion
s,n
650
day
s16.3
3per
day
10,6
14
650
10,6
14
00
Pro
ject
’sto
tal
cost
231,9
22
200,5
02
31,4
20
Tota
lco
st/p
atie
nt
(mea
n�
SD
)5946
�7508
7426
�7940
2618
�5292
Cost
/Pat
ien
t/M
on
th(m
ean
�S
D)
403
�420
475
�445
239
�316
aD
uri
ng
foll
ow
-up,
thre
epat
ien
ts(t
wo
wit
hn
ove
nti
lato
ru
sean
do
ne
usi
ng
NIV
)u
nd
erw
ent
trac
heo
sto
my.
RT
,re
spir
atory
ther
apis
t;T
M,
tele
med
icin
e;M
I-E
,m
ech
anic
alin
suffl
atio
n-e
xsu
fflat
ion
(Co
ug
hA
ssis
t,P
hil
lip
sR
esp
iro
nic
s,P
itts
bu
rg,
CA
);M
V,
mec
han
ical
ven
tila
tion
.
www.ajpmr.com Cough Assistance in ALS 405
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 211

REFERENCES
1. Bach JR: Amyotrophic lateral sclerosis: Prolongation
of life by noninvasive respiratory aids. Chest
2002;122:92–8
2. Mustfa N, Walsh E, Bryant V, et al: The effect of
noninvasive ventilation on ALS patients and their
caregivers. Neurology 2006;66:1211–7
3. Gomez-Merino E, Bach JR: Duchenne muscular
dystrophy: Prolongation of life by noninvasive ven-
tilation and mechanically assisted coughing. Am J
Phys Med Rehabil 2002;81:411–5
4. Bach JR, Bianchi C, Aufiero E: Oximetry and indica-
tions for tracheotomy for amyotrophic lateral scle-
rosis. Chest 2004;126:1502–7
5. Mustfa N, Aiello M, Lyall RA, et al: Cough augmen-
tation in amyotrophic lateral sclerosis. Neurology
2003;61:1285–7
6. Servera E, Sancho J, Zafra MJ, et al: Alternatives to
endotracheal intubation for patients with neuromus-
cular diseases. Am J Phys Med Rehabil 2005;84:851–7
7. Sancho J, Servera E, Diaz J, et al: Efficacy of me-
chanical insufflation-exsufflation in medically stable
patients with amyotrophic lateral sclerosis. Chest
2004;125:1400–5
8. Winck JC, Goncalves MR, Lourenco C, et al: Effects
of mechanical insufflation-exsufflation on respira-
tory parameters for patients with chronic airway
secretion encumbrance. Chest 2004;126:774–80
9. Farrero E, Prats E, Povedano M, et al: Survival in
amyotrophic lateral sclerosis with home mechan-
ical ventilation: The impact of systematic respira-
tory assessment and bulbar involvement. Chest
2005;127:2132– 8
10. Krivickas LS, Shockley L, Mitsumoto H: Home care
of patients with amyotrophic lateral sclerosis (ALS).
J Neurol Sci 1997;152(suppl 1):S82–9
11. Vitacca M, Escarrabill J, Galavotti G, et al: Home
mechanical ventilation patients: A retrospective sur-
vey to identify level of burden in real life. Monaldi
Arch Chest Dis 2007;67:142–7
12. Bach JR, Intintola P, Alba AS, et al: The ventilator-
assisted individual. Cost analysis of institutionaliza-
tion vs rehabilitation and in-home management.
Chest 1992;101:26–30
13. Kollef MH, Ahrens TS, Shannon W: Clinical predic-
tors and outcomes for patients requiring tracheos-
tomy in the intensive care unit. Crit Care Med
1999;27:1714–20
14. Vitacca M, Bianchi L, Guerra A, et al: Tele-assistance
in chronic respiratory failure patients: A randomised
clinical trial. Eur Respir J 2009;33:411–8
15. Brooks BR, Miller RG, Swash M, et al: El Escorial
revisited: Revised criteria for the diagnosis of amyo-
trophic lateral sclerosis. Amyotroph Lateral Scler
Other Motor Neuron Disord 2000;1:293–9
16. Tzeng AC, Bach JR: Prevention of pulmonary mor-
bidity for patients with neuromuscular disease.
Chest 2000;118:1390–6
17. Bach JR: Mechanical insufflation-exsufflation. Com-
parison of peak expiratory flows with manually as-
sisted and unassisted coughing techniques. Chest
1993;104:1553–62
18. Sancho J, Servera E, Vergara P, et al: Mechanical
insufflation-exsufflation vs. tracheal suctioning via
tracheostomy tubes for patients with amyotrophic
lateral sclerosis: A pilot study. Am J Phys Med Re-
habil 2003;82:750–3
19. Wood KE, Flaten AL, Backes WJ: Inspissated secretions: A
life-threatening complication of prolonged noninvasive
ventilation. Respir Care 2000;45:491–3
20. Sancho J, Servera E, Diaz J, et al: Comparison of
peak cough flows measured by pneumotachograph
and a portable peak flow meter. Am J Phys Med
Rehabil 2004;83:608–12
21. Nijeweme-d’Hollosy WO, Janssen EP, Huis in ’t Veld
RM, et al: Tele-treatment of patients with amyotro-
phic lateral sclerosis (ALS). J Telemed Telecare
2006;12(suppl 1):31–4
22. Bach JR: A comparison of long-term ventilatory sup-
port alternatives from the perspective of the patient
and care giver. Chest 1993;104:1702–6
23. Bach JR, Barnett V: Ethical considerations in the man-
agement of individuals with severe neuromuscular dis-
orders. Am J Phys Med Rehabil 1994;73:134–40
24. Ishikawa Y, Bach JR, Komaroff E, Miura T, Jackson-
Parekh R. Cough augmentation in Duchenne mus-
cular dystrophy. Am J Phys Med Rehabil 2008;87:
726–30
406 Vitacca et al. Am. J. Phys. Med. Rehabil. ● Vol. 89, No. 5, May 2010
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
212 Miguel Ramalho do Souto Gonçalves

Study 9
Home mechanical cough assistance for acute
exacerbations in neuromuscular disease
Miguel R. Gonçalves, Mara Paneroni, João Bento, Debora Trainini, Luca Bianchi, João C. Winck and Michele Vitacca
(Respiratory Medicine, submitted)
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 213

Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
214 Miguel Ramalho do Souto Gonçalves

Home mechanical cough assistance for acute exacerbations in neuromuscular diseases. Miguel R. Gonçalves *, Mara Paneroni**, João Bento*, Debora Trainini**, Luca Bianchi **, João Carlos Winck* and Michele Vitacca**
* Lung Function and Ventilation Unit, Neuromuscular clinic, Pneumology Department, Faculty of
Medicine, S. João Hospital Porto, Portugal
** UO di Pneumologia Riabilitativa e Terapia Intensiva Respiratoria, Fondazione Salvatore
Maugeri IRCCS, Lumezzane (BS) Italy
Corresponding author:
Miguel R. Gonçalves Lung Function and Ventilation Unit – Pulmonary Medicine Department University Hospital of S. João Faculty of Medicine, University of Porto Address: Av. Prof. Hernani Monteiro, Porto, Portugal Phone: 00351 225512100 (extension 1042); [email protected] [email protected]
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 215

Abstract
Background: Mechanically assisted coughing (MAC) has been used successfully in hospital for
patients with neuromuscular disease (NMD), however, limited data exist on long-term home use.
Objective: To determine outcomes of home MAC for NMD patients using tracheostomy
mechanical ventilation (TMV) or noninvasive ventilation (NIV) during acute episodes.
Material and methods: The study was performed in two centers with NMD clinics. Forty six
NMD patients (14 females) continuously ventilator dependent (28 using NIV and 18 TMV) with a
mean age 51.3±22.3 years, were analyzed. Pulmonary function and cough efficacy were assessed
during routine evaluations. Hospitalization rates, avoided hospitalizations defined by normalization
of SpO2 within 24 hours by continuous ventilatory support and MAC, and resort to deep airway
suctioning were recorded. Treatment tolerance and side effects were also assessed.
Results: During 42±57 months of follow up, for 180 acute episodes, 146 hospitalizations were
avoided. Hospitalization rates for NIV users were significantly lower than for TMV users. Home
MAC during acute episodes normalized baseline SpO2 and decreased resort to deep airway
suctioning via tracheostomy tube per day. In all MAC sessions there were no complications.
Conclusion: Home MAC with oximetry feedback is effective and can avoid hospitalizations for
both NIV and TMV users.
Key words: Home mechanical ventilation, Mechanical assisted cough, Neuromuscular
disorders,
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
216 Miguel Ramalho do Souto Gonçalves

Introduction
Mechanical assisted cough (MAC) is the use of mechanical insufflation-exsufflation (MI-E)
(1) with an exsufflation-timed abdominal thrust. It can be applied via oral, oronasal interfaces or via
invasive airway tubes preferably with inflated cuffs (2). The physiological effects and efficacy of
MAC have been described for adults (1, 3-6) and children (7-8).
Patients with neuromuscular diseases (NMD) have respiratory muscle weakness and
impaired cough (9-10). For these patients, up to continuous use of noninvasive ventilation (NIV)
can maintain quality of life,(11) and markedly prolong survival (12) that is, nevertheless, punctuated
by respiratory tract infections (RTIs). Intercurrent RTIs are the main cause of morbidity, prolonged
hospitalizations, acute respiratory failure (ARF), intensive care admissions, and mortality (13-16).
The use of mechanically assisted coughing (MAC) has been reported to be effective in preventing
ARF and for avoiding hospitalizations in patients with Duchenne Muscular Dystrophy (DMD) (16).
In hospital application, MAC has been described as a first-line intervention for NMD
patients with ARF (2, 7, 17-20), however, its efficacy and optimal application in the home has not
been widely explored. The purpose of this study was to describe the outcomes of home MAC for
avoiding hospitalizations in NMD patients.
Material and Methods
The data were retrospectively gathered in two centers with NMD clinics and extending
home care organizations that include the provision of MAC. The study was approved by the
institutions’ review boards.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 217

Patients
A 4 year follow up observational analysis was performed for 46 totally ventilator dependent
patients (14 females) that included 33 with ALS and 13 with other NMDs (5 Duchenne muscular
dystrophy (DMD), 3 spinal muscular atrophy (SMA) type 1, 3 SMA type 2, 1 multiple sclerosis and
1 congenital muscular dystrophy) with mean age 51.3±22.3 years. Inclusion criteria were: NMD
diagnosis, baseline assisted cough peak flow (CPF) <270 L/min and continuous ventilator
dependence (> 20h per day) and decrease in SpO2 baseline below 95% during intercurrent episodes
of respiratory distress. Patients with lung disease, inability to cooperate and without dedicated
caregivers were excluded.
Measurements
Unassisted and assisted CPF were noted for NIV users and peak expiratory flow (PEF) noted
for TMV users. Spirometric (Vmax 229, Autobox, Sensormedics) recording of forced expiratory
volume in one second (FEV1) and forced VC (FVC) was noted. In TMV users, tracheotomy
pulmonary function tests were performed through the non-fenestrated tracheotomy tube with an
inflated cuff. All pulmonary function testing was done in sitting position according to standard
procedures(21).
Unassisted CPF was measured by having the patient cough forcefully through a standard
peak flow meter (miniRight, standard range Peak Flow Meter Clement Clarke International
England) connected to a facial mask. Assisted CPF involved the patient “air stacking” to approach
maximum insufflation capacity (22) using their volume-cycling ventilator or a manual resuscitator
and coughing into the peak flow meter as the abdominal thrust was applied at glottic opening (3).
Bulbar impairment and glottic dysfunction correlated with unassisted/assisted CPF ratio for NIV
users. Patients with a ratio =1 could not close the glottis and were considered to have severe
“bulbar” impairment (10, 13, 23).
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
218 Miguel Ramalho do Souto Gonçalves

Home oximetry feedback/MAC protocol
All patients and their caregivers attended a hospital-based educational program on lung
expansion techniques (air stacking), manual assisted coughing, and MAC with oximetry feedback.
MAC training included adjustment of settings on the Cough-Assist (Philips, Respironics, Inc,
Murrysville, PA) and use during practical clinical simulations, as well as training in awareness of
symptoms and signs of airway congestion that indicate need for MAC via oronasal mask or via
tracheostomy tube that had to be with an inflated cuff (2). The Cough-Assist and an oximeter
(Nonin 9500 oximeter Minneapolis Plymouth USA) was then provided for home use.
Secretion encumbrance that caused SpO2 to decrease to less than 95% despite continuous
full-setting ventilatory support in ambient air with dyspnea, that did not revert after manually
assisted coughing techniques, or, for patients with tracheotomy tubes, after several secretion
mobilization and suctioning sessions, indicated an acute episode and resort to MAC with settings
suggested by medical literature.(1, 3, 24) A effective MAC application by trained non-professional
caregivers (family members, private attendant) was the expulsion of airway secretions by MAC that
resulted in return of SpO2 to≥95%. A trained health care professional (respiratory therapist or
nurse) was always available 24h/day on free on-call to answer questions as well as to go to the
home to supervise MAC in difficult situations (25). Patients and caregivers were also instructed to
detect early signs of respiratory tract infections and instructed to contact our staff for medical
therapy.
Hospitalization avoidance was defined as MAC-engendered expulsion of mucus with
resulting normalization of SpO2 to values equal to baseline within 24 hours. Whenever dyspnea and
secretion encumbrance or SpO2 <95% persisted despite continuous ventilator use and aggressive
MAC (more than 4 sessions per hour), patients were instructed to go to Emergency Departments of
local hospitals. In addition, the TMV users were instructed to seek attention if requiring an increase
in the need for airway suctioning. These were the criteria established for hospital admission.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 219

Outcome Monitors
Numbers of: acute episodes of secretion encumbrance with desaturation indicating need for MAC,
hospitalizations, and avoided hospitalizations were analyzed and compared between NIV and TMV patient
groups. SpO2 baseline values during acute episodes were compared with pre-morbid baseline values and
values at recovery (after a 24h MAC application). For TMV patients, the number of deep airway suctionings
were also recorded both during the acute episode and at recovery. Tolerance and side effects were
monitored.
Statistical Analysis
Statistical analysis was performed by SPSS 15.0 software (SPSS, Chicago, I1, USA). Descriptive
data are reported as mean±SD. Comparisons between groups were done using the Mann-Whitney U-
test and differences between baseline, acute episode and recovery were compared using the
Wilcoxon rank test. A p value ≤ 0.05 was considered significant.
Results
During a follow up of 42±57 months, 46 subjects, that included, 28 (61%) NIV users and 18
(39%) TMV users, were studied. All had CPFs that satisfied the inclusion criteria. Demographic
data and clinical and functional characteristics are listed in table 1.
The home oximetry feedback/MAC protocol was used for a total of 180 (mean 3.9±2.9 per
patient) acute episodes of respiratory insufficiency due to secretion encumbrance during the follow
up of the study. During these episodes SpO2 significantly decreased in all patients in comparison
with baseline and significantly reverted in 24 hours after MAC (Figure 1). In TMV patients, during
the acute episodes, the number of deep airway suctionings significantly increased in comparison
with baseline and after MAC significantly decreased again in 24 hours to values similar to baseline
(Figure 2). Hospitalization data and outcomes are listed in table 2.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
220 Miguel Ramalho do Souto Gonçalves

During the follow up period 10 patients died (8 NMV and 2 TMV users), 4 suddenly and
presumably from cardiac arrhythmia (3 ALS and 1 SMA type 1), 3 with ALS from pneumonia, and 2 ALS
patients from stroke. All MAC sessions were well-tolerated and there were no complications related
to the treatment.
Discussion
The organization of home MAC access and patient compliance with it has already been
reported by our group for ALS patients (25). We have now reported data that focused on the clinical
effects of home MAC during acute episodes of secretion encumbrance in ALS and other NMD
patients. The results confirm that hospitalizations for ARF can be avoided for NMD patients by a
protocol of oximetry feedback for using ventilatory support and MAC in the home (12, 15-16, 26).
Moreover our findings support the clinical justification for availability and prescription of cough
assist devices and portable oximeters at home for this patient population, specially during
intercurrent RTI´s.
Provided that supplemental oxygen therapy be avoided, oximetry was critical since, once
artefact is ruled out, all desaturations indicated less than full ventilatory support (airflow leak or
inadequate ventilator settings), airway secretion congestion, and if the latter was not resolved by
MAC, persistent SpO2 decrease was caused by pneumonia or other persistent complications of
congestion(5, 15, 17, 27) Since all patients were continuously ventilator dependent during the
episodes, had the oxyhemoglobin desaturations and dyspnea not been reversed by MAC, they
would have had to have been hospitalized for problems related to upper respiratory tract infections
and inability to clear secretions. However, in our study, as a result of the protocol, 81% of the acute
episodes resolved without hospitalization.
These results are consistent with those reported by Gomes-Merino et al (16) that, with a similar
approach, described hospitalization avoidance and survival increase in a population with Duchenne muscular
dystrophy under NIV. Our study focused on other NMD diagnoses including having 71% ALS patients.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 221

Moreover, we found that, while the incidence of acute episodes was the same, the TMV users had
significantly more hospitalizations per desaturation episode than NIV users. This may be due specifically to
complications caused by the invasive tubes (28-30) and unrelated to MAC or by poorer bulbar-innervated
muscle function and airway protection mechanisms in the ALS population despite TMV with cuff
inflation(31-32)
Indeed, it is well known that the severely impaired bulbar-innervated muscle function in ALS
can render MAC ineffective (5, 12) via the upper airway and necessitate tracheostomy to be
effective (13, 32). Bach et al. described that persistent SpO2 < 95% in room air despite optimal use of NIV
and MAC, indicates need for tracheostomy in ALS patients (26) and presumably in patients with other NMDs
as well. In our study, MAC not only significantly improved SpO2 in all patients, it also significantly
decreased the number of airway suctionings in TMV patients. All TMV patients in this study had bulbar
muscle impairment and the fact that only 3 NIV users had bulbar impairment, may justify the good results of
MAC on reversion of desaturations at home.
The main requisite for home MAC prescription was the presence of adequate and motivated
patients and caregivers to learn the protocol from trained health care professionals. Our results
imply that the training and equipping be done early, before ARF occurs, and in the outpatient
setting as reported by Tzeng et al (15). Our results confirm that the caregiver can successfully use MAC
at home cough with oximetry feedback and can early detect possible acute episodes of secretion
encumbrance. However, according to our experience, to guarantee an optimal continuous support to the
caregiver, an easy access by phone to a heath care professional 2nd opinion, 24 h/day is strongly advised.
Limitations of the study include its retrospective nature with no control group, the small
number of patients and multiple diagnoses. Thus, we advise caution in the generalization of the
results.
In conclusion, it is possible and effective to manage episodes of acute respiratory
decompensation, related to secretion encumbrance, in continuously ventilator dependent NMD
patients in the home with patient and care provider training and equipping in a protocol of MAC
with oximetry feedback. This is true for patients dependent on either NIV or TMV.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
222 Miguel Ramalho do Souto Gonçalves

Table 1: Patient baseline characteristics
Patients, (n) 46
Age, years ± SD (range) 51±22 (1-83)
Gender M/F 32/14
Years of Onset* 5.7±5.6
Follow up after mechanical ventilation, months ± SD (range) 42±57 (6-300)
Bulbar/Non bulbar Involvement** 21/25
NIV users (n, %)
TMV users (n, %)
28 (61%)
18 (39 %)
VC, Liters (%) Tot – 1.0 ±0.5 (31±13%)
TMV users – 1.1 ±0.51 (34±10%)
NIV users – 0.97 ±0.52 (30±14%)
FVC/FEV1 (%) Tot - 88±12
TMV users - 86±12
NIV users - 88±13
Unassisted PCF, L/min (NIV users)
Assisted PCF, L/min (NIV users)
92±86
198±65
PEF, cmH20 (TMV users) 40±28
Legend: TMV – tracheostomy mechanical ventilation; NIV- noninvasive mechanical ventilation; Tot- Total
population;;VC - vital capacity; PCF – Peak Cough Flow; PEF . Peak Expiratory Flow; *from diagnosis; **from time
of entry in the study
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 223

Table 2 – Outcomes of Home MAC and hospitalization data
Patients under tracheostomy mechanical ventilation
(n=18)
Patients under noninvasive mechanical ventilation
(n = 28)
Total patients
(n=46)
Total home acute episodes of secretion encumbrance with MAC activation, nr
78 102 180
Home acute episodes of secretion encumbrance with MAC activation (per patient), mean±SD
4.3±3.7 3.6±2.3 3.9±2.9
Total Hospitalizations, nr 21 13 34 Hospitalizations (per patient), mean±SD 1.2±1.3 * 0.5±0.7 * 0.7±1.0 Avoided Hospitalizations, nr 57/78
(73%) 89/102 (87%)
146/180 (81%)
Legend: MAC – mechanical assisted cough; nr - number
* p < 0,05
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
224 Miguel Ramalho do Souto Gonçalves

Figure 1 – Oxygen saturation (SpO2) monitoring during baseline, acute epiosde and at recovery
(after MAC)
Legend: MAC – mechanical assisted cough
* p < 0,05- when comparing baseline to acute episode and acute episode to after MAC
*
*
*
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 225

Figure 2 – Number of deep airway suctionings in TMV patients during baseline, acute epiosde
and at recovery (after MAC)
Legend: MAC – mechanical assisted cough
* p < 0,05- when comparing baseline to acute episode and acute episode to after MAC
*
*
*
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
226 Miguel Ramalho do Souto Gonçalves

References
1. Winck JC, Goncalves MR, Lourenco C, Viana P, Almeida J, Bach JR. Effects of
mechanical insufflation-exsufflation on respiratory parameters for patients with chronic
airway secretion encumbrance. Chest. 2004 Sep;126(3):774-80.
2. Sancho J, Servera E, Vergara P, Marin J. Mechanical insufflation-exsufflation
vs. tracheal suctioning via tracheostomy tubes for patients with amyotrophic lateral
sclerosis: a pilot study. Am J Phys Med Rehabil. 2003 Oct;82(10):750-3.
3. Bach JR. Mechanical insufflation-exsufflation. Comparison of peak expiratory
flows with manually assisted and unassisted coughing techniques. Chest. 1993
Nov;104(5):1553-62.
4. Mustfa N, Aiello M, Lyall RA, Nikoletou D, Olivieri D, Leigh PN, et al. Cough
augmentation in amyotrophic lateral sclerosis. Neurology. 2003 Nov 11;61(9):1285-7.
5. Sancho J, Servera E, Diaz J, Marin J. Efficacy of mechanical insufflation-
exsufflation in medically stable patients with amyotrophic lateral sclerosis. Chest. 2004
Apr;125(4):1400-5.
6. Chatwin M, Ross E, Hart N, Nickol AH, Polkey MI, Simonds AK. Cough
augmentation with mechanical insufflation/exsufflation in patients with neuromuscular
weakness. Eur Respir J. 2003 Mar;21(3):502-8.
7. Miske LJ, Hickey EM, Kolb SM, Weiner DJ, Panitch HB. Use of the mechanical
in-exsufflator in pediatric patients with neuromuscular disease and impaired cough.
Chest. 2004 Apr;125(4):1406-12.
8. Fauroux B, Guillemot N, Aubertin G, Nathan N, Labit A, Clement A, et al.
Physiologic benefits of mechanical insufflation-exsufflation in children with
neuromuscular diseases. Chest. 2008 Jan;133(1):161-8.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 227

9. Perrin C, Unterborn JN, Ambrosio CD, Hill NS. Pulmonary complications of
chronic neuromuscular diseases and their management. Muscle Nerve. 2004
Jan;29(1):5-27.
10. Bach JR, Goncalves MR, Paez S, Winck JC, Leitao S, Abreu P. Expiratory flow
maneuvers in patients with neuromuscular diseases. Am J Phys Med Rehabil. 2006
Feb;85(2):105-11.
11. Mustfa N, Walsh E, Bryant V, Lyall RA, Addington-Hall J, Goldstein LH, et al.
The effect of noninvasive ventilation on ALS patients and their caregivers. Neurology.
2006 Apr 25;66(8):1211-7.
12. Bach JR. Amyotrophic lateral sclerosis: prolongation of life by noninvasive
respiratory aids, Chest. 2002 Jul;122(1):92-8.
13. Sancho J, Servera E, Diaz J, Marin J. Predictors of ineffective cough during a
chest infection in patients with stable amyotrophic lateral sclerosis. Am J Respir Crit
Care Med. 2007 Jun 15;175(12):1266-71.
14. Bach JR, Rajaraman R, Ballanger F, Tzeng AC, Ishikawa Y, Kulessa R, et al.
Neuromuscular ventilatory insufficiency: effect of home mechanical ventilator use v
oxygen therapy on pneumonia and hospitalization rates. Am J Phys Med Rehabil. 1998
Jan-Feb;77(1):8-19.
15. Tzeng AC, Bach JR. Prevention of pulmonary morbidity for patients with
neuromuscular disease. Chest. 2000 Nov;118(5):1390-6.
16. Gomez-Merino E, Bach JR. Duchenne muscular dystrophy: prolongation of life
by noninvasive ventilation and mechanically assisted coughing. Am J Phys Med
Rehabil. 2002 Jun;81(6):411-5.
17. Vianello A, Corrado A, Arcaro G, Gallan F, Ori C, Minuzzo M, et al.
Mechanical insufflation-exsufflation improves outcomes for neuromuscular disease
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
228 Miguel Ramalho do Souto Gonçalves

patients with respiratory tract infections. Am J Phys Med Rehabil. 2005 Feb;84(2):83-8;
discussion 9-91.
18. Goncalves M, Bach J. Mechanical Insufflation-exsufflation improves outcomes
for Neuromuscular disease patients with repiratory tract infections: " a step in the right
direction". Am J Phys Med Rehabil. 2005;84:89-91.
19. Servera E, Sancho J, Gomez-Merino E, Briones ML, Vergara P, Perez D, et al.
Non-invasive management of an acute chest infection for a patient with ALS. J Neurol
Sci. 2003 May 15;209(1-2):111-3.
20. Bach JR, Goncalves MR, Hamdani I, Winck JC. Extubation of patients with
neuromuscular weakness: a new management paradigm. Chest. 2010 May;137(5):1033-
9.
21. Quanjer PH, Tammeling GJ, Cotes JE, Pedersen OF, Peslin R, Yernault JC.
Lung volumes and forced ventilatory flows. Report Working Party Standardization of
Lung Function Tests, European Community for Steel and Coal. Official Statement of
the European Respiratory Society. Eur Respir J Suppl. 1993 Mar;16:5-40.
22. Kang SW, Bach JR. Maximum insufflation capacity. Chest. 2000 Jul;118(1):61-
5.
23. Suarez AA, Pessolano FA, Monteiro SG, Ferreyra G, Capria ME, Mesa L, et al.
Peak flow and peak cough flow in the evaluation of expiratory muscle weakness and
bulbar impairment in patients with neuromuscular disease. Am J Phys Med Rehabil.
2002 Jul;81(7):506-11.
24. Sancho J, Servera E, Marin J, Vergara P, Belda FJ, Bach JR. Effect of lung
mechanics on mechanically assisted flows and volumes. Am J Phys Med Rehabil. 2004
Sep;83(9):698-703.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 229

25. Vitacca M, Paneroni M, Trainini D, Bianchi L, Assoni G, Saleri M, et al. At
home and on demand mechanical cough assistance program for patients with
amyotrophic lateral sclerosis. Am J Phys Med Rehabil. 2010 May;89(5):401-6.
26. Bach JR, Bianchi C, Aufiero E. Oximetry and indications for tracheotomy for
amyotrophic lateral sclerosis. Chest. 2004 Nov;126(5):1502-7.
27. Bach JR, Ishikawa Y, Kim H. Prevention of pulmonary morbidity for patients
with Duchenne muscular dystrophy. Chest. 1997 Oct;112(4):1024-8.
28. Baydur A, Kanel G. Tracheobronchomalacia and tracheal hemorrhage in patients
with Duchenne muscular dystrophy receiving long-term ventilation with uncuffed
tracheostomies. Chest. 2003 Apr;123(4):1307-11.
29. Pignatti P, Balestrino A, Herr C, Bals R, Moretto D, Corradi M, et al.
Tracheostomy and related host-pathogen interaction are associated with airway
inflammation as characterized by tracheal aspirate analysis. Respir Med. 2009
Feb;103(2):201-8.
30. Markstrom A, Sundell K, Lysdahl M, Andersson G, Schedin U, Klang B.
Quality-of-life evaluation of patients with neuromuscular and skeletal diseases treated
with noninvasive and invasive home mechanical ventilation. Chest. 2002
Nov;122(5):1695-700.
31. Sancho J, Servera E, Banuls P, Marin J. Prolonging survival in amyotrophic
lateral sclerosis: efficacy of noninvasive ventilation and uncuffed tracheostomy tubes.
Am J Phys Med Rehabil. 2010 May;89(5):407-11.
32. Farrero E, Prats E, Povedano M, Martinez-Matos JA, Manresa F, Escarrabill J.
Survival in amyotrophic lateral sclerosis with home mechanical ventilation: the impact
of systematic respiratory assessment and bulbar involvement. Chest. 2005
Jun;127(6):2132-8.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
230 Miguel Ramalho do Souto Gonçalves

Study 10
Evolution of Noninvasive Management of End-Stage
Respiratory Muscle Failure in Neuromuscular Disease
Miguel R. Gonçalves, John R. Bach, Yuka Ishikawa, Eduardo Luis DeVito,
Francisco Prado, Pamela Salinas, Marie Eugenia Dominguez, Emilia Luna
Padrone, Mauro Vidigal-Lopes, Rita Guedes, Douglas McKim, Marcello
Villanova, Seong-Woong Kang, Emilio Servera, Jesús Sancho, Michel
Toussaint, Philippe Soudon, Michelle Chatwin, Anita K. Simonds, Martin
Bachmann, Michael Baumberger, Tsz-Kin Kwok, Konrad Bloch, David
Birnkrant, Juan Isquierdo, Ditza Gross, Louis Saporito, Brian Weaver,
Alice Hon, Bilal Saulat and João Carlos Winck,
(CHEST, in preparation for submission November 2010)
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 231

Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
232 Miguel Ramalho do Souto Gonçalves

Evolution of Noninvasive Management of End-Stage Respiratory
Muscle Failure in Neuromuscular Disease
Centers involved:
1- Miguel R. Gonçalves, João Carlos Winck, Department of Pulmonology,
University Hospital of S. João, Faculty of Medicine, University of Porto,
Portugal.
2- John R. Bach., Louis Saporito, Brian Weaver, Alice Hon, Bilal Saulat,
Department of Physical Medicine and Rehabilitation, UMDNJ-New Jersey
Medical School, University Hospital, Newark, N.J. USA
3- Yuka Ishikawa, National Organization Yakumo Hospital, Yakumo, Japan
4- Eduardo Luis DeVito, Instituto de Investigaciones Médicas Alfredo Lanari,
Facultad de Medicina, Universidad de Buenos Aires, Argentina.
5- Francisco Prado, Pamela Salinas, Universidad de Chile, Health Chilean
Ministry, Santiago, Chile.
6- Marie Eugenia Dominguez, Emilia Luna Padrone, Instituto National de
Enfermidades Respiratorias, Universidad National Autonoma de Mexico,
Mexico, D.F., Mexico.
7- Mauro Vidigal-Lopes, Rita Guedes, VentLar Home Care Program, FHEMIG,
Belo Horizonte, Brasil.
8- Douglas McKim, Respiratory Rehabilitation unit, Ottawa University Hospital,
Canada.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 233

9- Marcello Villanova, Neuromuscular Unit, Nigrisoli Hospital, Bologna, Italy
10- Seong-Woong Kang, Department of Rehabilitation Medicine, Gangnam
Severance Hospital, Seoul, South Korea.
11- Emilio Servera, Jesus Sancho Department of Pulmonology, Hospital Clínico
Valência, Spain
12- Michel Toussaint, Philippe Soudon, Center for home mechanical ventilation,
Indekaal Rehabilitation Hospital, Brussels, Belgium.
13- Michelle Chatwin, Anita K. Simonds, Sleep and Ventilation Unit, Royal
Brompton Hospital, London, UK.
14- Martin Bachmann, Asklepios Klinik Hamburg-Harburg, Germany
15- Michael Baumberger, Franz Michel, Centre Suisse des Paraplégiques,
Nottwil, Switzerland
16- Tsz-Kin Kwok, Tung Wah Hospital, Hong Kong, China
17- Konrad E.Bloch, Zurich, Switzerland.
18- David Birnkrant, Metro-Health Medical center, Case Western Reserve
University, USA
19- Juan Isquierdo, MedicalDiagnostic Inc., St. Petersburg, Florida, USA.
20- Ditza Gross, Telavive University Hospital, Israel
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
234 Miguel Ramalho do Souto Gonçalves
Abstract
From 20 centers in 18 countries, data are presented on 1623 nocturnal only
ventilated neuromuscular disease patients (NMD) that include amyotrophic lateral
sclerosis, Duchenne muscular dystrophy and spinal muscular atrophy type 1, in which
760 (47%) progressed to continuous full-setting noninvasive ventilation (NIV) over a
follow up of 15 years. A protocol of oximetry feedback using mechanically assisted
coughing and full-setting NIV permitted safe 229 safe extubations and 35 decanulations
of patients who could not pass spontaneous breathing trials (SBTs) before or after
extubation/decanulation. After the follow up period, 522 (69%) patients are still alive on
continuous full-setting NIV and tracheostomy was placed in a total of 140 (9%). An
expert panel reviewed recommendations of previous consensus and reviews on NIV use,
respiratory evaluations and assisted coughing in NMD to consider changes and updated
recommendations based on the evolution in practice patterns.
Introduction and Historical Perspective
Before 1953 noninvasive ventilation referred to the use of body ventilators like
the iron lung1. Despite their success for continuous ventilatory support, tracheostomy
positive pressure ventilation (TMV) became the standard for ventilatory support after a
1952 Danish polio epidemic for which there were few iron lungs2. Since TMV facilitated
mobilizing patients from iron lungs because positive pressure ventilators could be rolled
behind wheelchairs this invasive approach spread to the United States.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 235
Then in 1953 Dr. John Affeldt wrote, “…some of our physical therapists, in
struggling with (iron lung) patients, noticed that they could simply take the positive
pressure attachment, apply a small plastic mouthpiece..., and allow that to hang in the
patient's mouth….We even had one patient who has no breathing ability who has fallen
asleep and been adequately ventilated by this procedure, so that it appears to work very
well, and I think does away with a lot of complications of difficulty of using (invasive)
positive pressure. You just hang it by the patients and they grip it with their lips, when
they want it, and when they don't want it, they let go of it. It is just too simple."3.
Patients who were using body ventilators around the clock began using mouth
piece noninvasive intermittent positive pressure ventilation (NIV) during daytime hours.
Many then refused to go back to body ventilator use and used mouth piece NIV around-
the-clock. Losing the mouth piece during sleep could have meant death but there is no
indication that that ever happened4.
In 1956 Harris Thompson released a portable 28 lb. Bantam ventilator. The next
year it was noted, “If a patient is going to be left a respirator cripple with a very low VC,
a tracheotomy may be a great disadvantage. It is very difficult to get rid of a tracheotomy
tube when the VC is only 500 or 600 cc and there is no power of coughing, whereas, as
we all know, a patient who has been treated in a respirator (body ventilator) from the first
can survive and get out of all mechanical devices with a VC of that figure."5 Thus, it was
recognized that TMV could result in greater ventilator dependence because of
deconditioning, tube induced secretions, hyperventilation, bypassing upper airway
afferents, and possibly other factors6.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
236 Miguel Ramalho do Souto Gonçalves

In 1968 the lipseal interface came onto the market. Lipseals prevented loss of the
mouth piece during sleep and diminished air leakage, normalizing alveolar ventilation
during sleep even for patients with little or no measurable vital capacity (VC)4. Mouth
piece/lipseals were used up to continuously for long-term ventilatory support for 257
patients managed by Goldwater Memorial Hospital and by others scattered around the
country7 from 1968 through the advent of nasal NIV in 1987 when it was first recognized
that nasal NIV could provide full ventilatory support for a multiple sclerosis patient with
100 ml of VC8. Despite this no other centers reported using mouthpiece NIV for diurnal
ventilatory support in NMD until Servera et al. did so to avert intubations in 20059 and
Toussaint et al. for continuous support in 200610.
Once articles on nasal NIV proved its efficacy in long term ventilated patients
nasal and oro-nasal NIV were used in critical care11-12. Interfaces designed for treatment
with CPAP were modified for use with ventilator circuits. Nevertheless, most long-term
use of these interfaces was for “sleep disordered breathing” whereas inspiratory muscle
failure was not specifically addressed13-14. This was in part due to the fact that PaCO2
monitoring and assessment of inspiratory muscle failure were not included in
polysomnography that is programmed to interpret paradoxical chest wall motions as
obstructive and/or central apneas rather than from respiratory muscle dysfunction. This
may justify that neuromuscular disease (NMD) patients have been treated by nocturnal
continuous positive airway pressure (PAP) or low span (spans less than 10 cm H2O) bi-
level PAP, often referred to as “noninvasive ventilation” rather than by up to continuous
full setting NIV as they would eventually require with end-stage respiratory muscle
failure15.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 237

The use of CPAP and bi-level PAP has been reported in over 100 NMD papers
including in the 50 reviewed in this work, and in many it resulted in statistical
prolongation of life before continuous support became necessary and patients either
developed ARF and underwent tracheotomy or died16-17. Bi-level PAP at low spans were
considered inadequate for patients with little or no VC18-19. Bi-level PAP devices also do
not permit air stacking6, have low autonomy internal batteries20, and not always make
possible for infants to trigger21. Meanwhile, portable ventilators, rather than bi-level
devices, have been used by continuously NIV dependent patients for up to 56 years.
Airway secretion congestion, especially during intercurrent respiratory tract
infections (RTIs) can result in acute respiratory failure (ARF)22 and intubation, and with
failure to pass spontaneous breathing trials (SBTs), tracheotomy or death23. The ability
to increase cough flows by mechanically assisted coughing (MAC), available since 1993
facilitated long-term use of NIV by permitting patients to avert pneumonia and ARF22, 24-
25as well as for “unweanable” patients to be extubated without resort to tracheotomy26-27
Methodology
At the 69th Congress of the Mexican Society of Pulmonologists and Thoracic
Surgeons in April 2010, clinicians from centers who use NIV for full, long-term
ventilatory support submit their data for three diagnoses: Duchenne muscular dystrophy
(DMD), amyotrophic lateral sclerosis (ALS), and spinal muscular atrophy type 1 (SMA
1). Other centers were invited to send their data soon after. An expert panel considered
the evolution NIV reviews and consensus statements since 1993 and the importance of
complimentary interventions that permit long-term NIV as an alternative to TIV.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
238 Miguel Ramalho do Souto Gonçalves

Results
The data from 20 NMD centers in 18 countries on prolongation of life for NMD
patients as defined by continuous NIV dependence with little or no autonomous breathing
ability are in Tables 1-3. Data is presented as mean±SD for each center and the total data
display (all centers together) was performed using a mean correction factor for all the
items analyzed.
The centers with experience in extubation/decannulation of unweanable NMD
patients to NIV/MAC despite failing all SBTs, reported 229 safe extubations in DMD,
ALS and SMA1 patients and had 5 of 222 DMD, 52 of 139 ALS and 7 of 33 SMA 1
continuous NIV users undergo tracheotomy. Centers reported that 47% of ALS, 54% of
DMD and 39% of SMA 1 patients progressed to become continuously ventilator
dependent without being hospitalized or developing ARF.
Review of Evolution of NIV Reviews/Consensuses and Recommendations
Three members of the panel (MRG, JRB, AH) reviewed 50 consensuses and
Medline reviews from 1993-2010 with keywords for: NMD, DMD, ALS, SMA type 1,
NIV, respiratory management, respiratory care, long term ventilation, and ARF. The 50
NMD NIV references included 34 on various NMDs, 5 only on DMD, 5 on SMA 1, and
6 on ALS.
The literature was analyzed for the use over time of the following: oxygen
therapy, peak cough flow evaluation and augmentation, air stacking, low pressure (≤30
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 239

cmH2O) and high pressure (≥ 40 cm H2O) MAC, bi-level PAP used at both low and high
spans, NIV that includes nasal and mouthpiece NIV, part-time (<23 hours/day) and full-
time (>23 hours/day), oximetry feedback for NIV and MAC, elective tracheotomy
without meeting reported criteria for tracheotomy28, and extubation/decanulation of
unweanable patients to NIV. The importance of each was considered by the panel. Table
4 lists the reference papers and the evolution of intervention utilization over time.
Oxygen therapy
Avoidance of supplemental oxygen was recommended by 24 of the 50 papers and
its use ignored by the rest. Home oxygen therapy was strongly discouraged by
consensuses of 200429 and 201030. This panel concurred, recommending that
supplemental oxygen be used only for hospitalized patients when full-setting NIV and
MAC can not normalize (≥95%) oxyhemoglobin saturation (SpO2) and then only when
the patient can be readily intubated. Low flow oxygen has been reported to exacerbate
hypercapnia in NMD31. Most such patients who become CO2 narcotic do so receiving
oxygen rather than assisted ventilation. Besides decreasing ventilatory drive it appears to
exacerbate mouth leak of nasal NIV during sleep thereby exacerbating nocturnal
hypercapnia and renders oximetry less useful as a gauge of hypoventilation, airway
mucus congestion, atelectasis and pneumonia6, 22, 32. Oxygen supplementation, instead of
no treatment or assisted ventilation was reported to result in significantly more
pneumonias, hospitalizations, and hospitalization days31. Supplemental oxygen and
morphine are indicated for euthanasia such as in advanced bulbar-ALS patients who
satisfy criteria for but refuse tracheotomy33.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
240 Miguel Ramalho do Souto Gonçalves

Lung insufflation techniques: “air stacking”
Air stacking was cited in 21 of the 50 consensuses, in only 2 papers before 2002
but in 6 of 12 since 2009. Deep passive or active (air stacking) lung insufflation is
required to prevent chest wall contractures and lung restriction, to maximize cough peak
flows (CPF)34 and voice volume, promote lung growth, and prevent chest deformity in
children with NMD6. Air stacking involves the glottis holding consecutively delivered
air volumes (from a volume- cycled ventilator or a manual resuscitator) until maximum
possible lung inflation, the “maximum insufflation capacity” (MIC)35. The panel
unanimously recommended that NMD patients with VCs less than 80% of normal
practice daily air stacking and, if unable, passive maximal lung expansion. The MIC-VC
is also recommended as an objective, reproducible, quantitative measure of glottic
integrity36. For small children with paradoxical breathing who can not air stack,
nocturnal NIV can prevent pectus excavatum and promote lung growth and chest wall
development37-38
Evaluation and augmentation of cough peak flows (CPF)
Evaluation of CPF was cited in 25 of 50 papers, only one before 2000 but all but 5
since 2009. Measurement of unassisted and assisted CPF is useful to indicate introduction
of manually assisted coughing and MAC39. Manually assisted coughing consists of
maximal air stacking followed by a cough-timed abdominal thrust. These “assisted CPF”
are measured by peak flow meter and, when less than 270 to 300 L/m, indicate need for
access to MAC especially during intercurrent respiratory tract infections (RTI)40.The
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 241
panel unanimously recommended routine measurement of CPF and augmenting them
when they are less than 270 L/m.
Noninvasive Ventilation (NIV)
Three reviews and consensuses of respiratory management of NMD did not
mention NIV. Of the remaining 47, 11 recommended high span (IPAP, EPAP spans>10
cm H2O) bi-level PAP and 29 only low span PAP. Ten of 50 papers recognized the use
of NIV for full ventilatory support but none noted that tracheostomy could be avoided by
this when the patients are critically ill. In 1993 indication for tracheotomy was described
as need for NIV over 15 hours a day41. In that report, there was only one dissenting voice
who argued for continuous NIV use both in acute and chronic settings(the second author).
The use of some daytime mouth piece NIV was recommended in 16 of 47 papers
but despite this, its use has been reported in only four centers7, 9-10, 19. This panel
unanimously felt that low bi-level spans suboptimally rest inspiratory muscles and
insufficiently support patients with little or no VC. Further, since most of currently
available pressure- cycled units are limited to less than 40 cm H2O, they can be
inadequate for patients with poor pulmonary compliance. However, the panel
unanimously recommended that bi-level PAP be introduced to all patients symptomatic
for hypoventilation who can not air stack because of bulbar-innervated muscle
impairment of glottic closure as in bulbar ALS42. The panel also unanimously
recommended that volume cycling be used for all patients capable of air stacking unless it
caused excessive abdominal distension43-44. Nocturnal NIV can then be easily extended
through daytime hours as needed by switching from nocturnal nasal to diurnal mouth
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
242 Miguel Ramalho do Souto Gonçalves

piece NIV. When less than full support settings is used, tracheostomy or death becomes
inevitable.
Mechanically Assisted Cough
Mechanically assisted coughing (MAC) is defined as mechanical insufflation-
exsufflation (Cough Assisttm, Phillips Respironics, Inc.) (MI-E) with an exsufflation-
timed abdominal thrust. The MI-E delivers positive then negative pressures via an oro-
nasal interface or invasive airway tube to full clinical expansion then emptying of the
lungs45. Only 12 papers mentioned MI-E at what this panel considers effective absolute
pressures of >35 cm H2O46-48, 19 recommended low pressures, 3 noted no MI-E settings,
and 15 did not even mention MI-E. Only 3 papers29, 49-50 cited the importance of MAC,
that is, MI-E with an abdominal thrust. None cited the use of MAC via invasive airway
tubes, found to be so critical for extubation/decanulation of patients failing SBTs27.
MAC can also significantly decrease hospitalization rates24, 51. The panel unanimously
recommended that MAC be used, whether noninvasively or via invasive airway tube, for
all NMD patients with airway secretion congestion to prevent pneumonia and to facilitate
extubation/decanulation.
Extubation and Decannulation
Despite NIV and MAC, aspiration and intercurrent RTIs can result in pneumonia
and ARF and early tracheotomy has been proposed to “minimize respiratory
complications”52-54. Before 2010, no papers described the extubation or decanulation of
continuously ventilator dependent patients who could not pass SBTs before or after
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 243

extubation/decanulation. The conventional approach presupposes that ventilator weaning
is necessary for safe extubation. A 2010 publication reported successful extubation of
155 of 157 unweanable NMD patients in 2 centers using a protocol including extubation
to full setting NIV with the patients subsequently “weaning” themselves by taking fewer
and fewer mouth piece NIVs as needed, and using MAC to clear secretions27. Protocols
for decanulation of unweanable patients to NIV/MAC have also been described26, 55, with
advantages noted by patients for safety, convenience, appearance, comfort, speech, sleep,
swallowing, and general acceptability56. The panel unanimously recommended that all
NMD patients with some bulbar-innervated muscle function be extubated or offered
decanulation to full setting NIV and MAC with oximetry feedback. It appears that the
great majority of NMD patients for whom post-extubation assisted CPF attain 160 L/m
can be successfully extubated to full-setting NIV and MAC.
Tracheostomy
Tracheostomy for end-stage respiratory management was cited in 46 of 50 of the
papers. Conventional strategies recommend tracheotomy when continuous NIV is
required57, when intubated patients are unable to pass SBTs58, and electively, for
example, for impending surgery59. Even without ventilator use tracheostomies are often
retained because of lack of familiarity with MAC for clearing airway secretions60-61. This
is true despite long-term complications of tracheostomy mechanical ventilation (TMV)62.
In addition, patients using TMV tend to become and remain continuously ventilator
dependent whereas when extubated/decanulated to continuous NIV and having VCs of
250 ml or more, wean to nocturnal only NIV55; tracheostomy renders cough impossible
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
244 Miguel Ramalho do Souto Gonçalves

because glottic closure does not maintain thoraco-abdominal pressure and it results in air
leaks around the walls of the tube63. This panel unanimously recommended that
tracheotomy be indicated for all patients who aspirate so much saliva that SpO2 baseline
decreases and remains below 95% despite optimal NIV and MAC and that can not be
reversed by translaryngeal intubation over a 1 month period as has only been reported for
patients with ALS28.
Oximetry Feed-back Protocol
An oximetry, NIV/MAC protocol consists of using an oximeter for feedback to
maintain SpO2≥95% by full-setting NIV and aggressive MAC as needed22. The protocol
was recommended in 8 of 50 papers and in only 1 before 2003. Since supplemental
oxygen is avoided, patients and care providers are instructed that, once artifact is ruled
out, SpO2 below 95% is due to: hypoventilation with hypercapnia, airway secretion
congestion, and if not expeditiously managed, gross atelectasis or pneumonia28, 64. The
protocol is most important during RTIs and for extubation/decanulation27. If the baseline
SpO2 during RTIs decreases below 95% despite the protocol, the patient presents for a
formal evaluation. The panel unanimously agreed that, since it is impossible to develop
ARF with SpO2≥95% in ambient air, patients should be taught the protocol once CPF
can not exceed 270 to 300 L/m to prevent pneumonia and ARF, particularly during
intercurrent RTIs that can be managed at home24-25.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 245
Discussion
Mechanisms by which nasal or mouthpiece/lipseal NIV can improve the clinical
picture include: resting respiratory muscles and decreasing metabolic demand, increasing
tidal volumes and relieving hypercapnia, resetting chemoreceptors, opening atelectatic
areas, maintaining airway patency, improving ventilation/perfusion matching,
maintaining lung and chest wall range-of-motion and possibly compliance, improving
mucociliary clearance, and most importantly, by assisting, supporting, and substituting
for inspiratory muscle function6, 32.
This work keyed on three NMD diagnoses, however, continuous full-setting NIV
via mouth pieces had already been reported for 257 mainly post-polio survivors in 19937,
59 high level traumatic tetraplegics decanulated to full-setting NIV65-67 and patients with
non-Duchenne muscular dystrophies and other myopathies18, 68 All of the centers
reporting data in this study had long-term full-time NIV users with other diagnoses but it
was felt that limiting the data to these common and severe conditions would be more
practical and establish the point.
Nocturnal- only nasal NIV or bi-level PAP can at best marginally prolong life and
delay ARF. It can possibly do so by providing moderately deeper lung volumes to assist
in coughing. With advancing weakness, full-setting NIV can eventually be needed
continuously without requiring intubation and hospitalization, thereby avoiding ARF and
ultimately pressure by physicians to recommend tracheotomy.
Most conventionally managed patients develop ARF and die or undergo
intubation and tracheotomy due to airway congestion during RTIs22, the cause of 90% of
episodes of ARF for DMD patients without access to NIV and MAC24, 69. Suctioning
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
246 Miguel Ramalho do Souto Gonçalves

patients' airways via the nose or mouth is rarely effective and impairs breathing.
Whereas with “invasive suctioning” there is little chance of a suction catheter entering
the left mainstem bronchus, “noninvasive suctioning” using MI-E would not favor right
over left airway clearance63, 70.
Since MAC can only replace inspiratory and expiratory muscle function, it can
not be used to avert tracheotomy indefinitely if glottic dysfunction prevents air stacking
and airway protection to maintain baseline SpO2 (≥95%) as eventually occurs in
advanced bulbar ALS28, 42, 71. The patients who benefit most from MAC are those whose
bulbar muscle function is impaired but can maintain adequate airway patency but is
insufficient to permit optimal air stacking for assisted CPF over 250 to 300 L/m71.
The data presented suggest that reported “NIV failure” can result from inadequate
NIV interfaces, from inadequate ventilator settings, when MAC is not used, and when
mouth piece NIV is not used for air stacking or daytime support.
Whereas some recent consensuses recommend most of the interventions that this
panel considers important, all gave sufficient rationales to resort to tracheotomy for
advanced patients, largely because none reported extubating or decanulating unweanable
patients. Indeed, the 2010 DMD consensus30 was the first to make all of the
recommendations that this panel considered important, however, they concluded that
tracheostomy was appropriate when: preferred by the patient and clinician; NIV could not
successfully be used by the patient; when there was inability of “the local medical
infrastructure to support NIV”; for three extubation failures despite optimal use of NIV
and MAC; for aspiration of airway secretion to the extent that SpO2 remains below 95%
despite optimal use of NIV and MAC. However, this panel of 11 experts had only 4 with
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 247

any experience in continuous NIV including via mouthpiece and only one from a center
where NMD patients who failed SBTs are extubated without tracheotomy.
This is markedly different from this panel in which every member has continuous
long-term NIV users and at least 5 are from centers that routinely extubate and decanulate
“unweanable” NMD patients including 155 consecutive successful extubations of
unweanable NMD and SCI patients27. In addition, no one on this panel has ever noted
any patient who: “preferred” to undergo tracheotomy when they could be managed by
NIV and MAC. We suggest that only the patients not offered expert NIV/MAC “prefer”
tracheostomy. Other than for severely mentally retarded patients no one on this panel has
encountered a DMD patient who could “not successfully use NIV.” We are also unaware
of “inability of local medical infrastructure to support NIV” except in countries where
ventilator use is not funded. The centers that extubate unweanable DMD patients have
not yet had a DMD patient fail 3 extubations and, thereby, require tracheotomy. None on
this panel has witnessed a DMD patient aspirate so much saliva that the SpO2 remained
below 95% (or normal SpO2 for altitude) and thereby require a tracheostomy as per
tracheotomy indications for ALS28. Thus, while the 2010 panel’s NIV use
recommendations are comprehensive up to the point of requiring intubation30, this panel
suggests that with the ability to consistently extubate continuously ventilator dependent
DMD patients and others, resort to tracheotomy should be much less common. A basic
problem with the tracheotomy recommendations of the 2010 consensus is that they can
be interpreted by any clinician to justify tracheostomy rather than organizing a support
system of comprehensive instruction and training in NIV and MAC. Such a premise
perpetuates invasive care whereas noninvasive management is less costly, requires less
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
248 Miguel Ramalho do Souto Gonçalves

technology and skilled nursing, facilitates community care and quality of life, and is
invariably preferred by patients51.
For SMA 1 it is as yet unclear whether all will some day require tracheostomy
tubes for survival. Thus far, survival has been extended to up to age 17 using full-time
NIV for 16 years or more for children continuously NIV dependent since as young as 4
months of age72-73. There are now 5 such severely affected SMA 1 patients over age 15,
all with VCs less than 20 ml, and none with baseline SpO2 less than 95% because of
saliva aspiration. Thus, it is likely that at least some of these typically severe SMA1
patients will survive into adulthood without tracheostomy tubes despite continuous
ventilatory support since infancy. Despite these outcomes, consensuses of experts as
recently as 2009 report that 95% of SMA 1 children die before 18 months of age with a
mean age of death at 25 weeks74-75. Although acknowledging that NIV treated SMA 1
children can live much longer, in disbelief and without justification they dismissed this as
reflecting “less severely affected children”.
End of life and palliative care issues
Over a 6-year period, many journals published numerous papers on the futility of
managing ALS with palliative care without once referring to prolonging life by
NIV/MAC33, 76-80. The data from our 1623 NIV supported patients (that include 822 ALS)
suggest the inappropriateness of using palliative care precepts for properly equipped and
trained patients with adequate personal care support. A number of our DMD patients, for
example, are over age 40 and/or have depended on continuous NIV for over 20 years.
Unlike patients deciding about tracheotomy, few patients refuse NIV or MAC when
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 249

dyspneic from inspiratory or expiratory muscle insufficiency. Our panel unanimously
agreed that no properly trained and equipped patients that do not meet our criteria for
tracheotomy have ever chosen elective tracheotomy or to cease NIV/MAC and die.
Thus, it was unanimously felt that the use of the term “palliative respiratory care” for
NMD patients perpetrates the misconception that “NIV” is only for symptom relief rather
than to prolong life.
Conclusion
In conclusion, up to total failure of inspiratory and expiratory musculature without
severe bulbar-innervated muscle dysfunction is not indication for tracheotomy.
Tracheostomy ventilation has neither been demonstrated to be associated with better
survival nor better quality of life than full-setting NIV, and all patients having used both
TMV and NIV and who are decanulated prefer NIV overall as well as for speech,
swallowing, sleep, appearance, and security.303 The panel recommends against elective
tracheotomy for any NMD patient not meeting our criteria.116
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
250 Miguel Ramalho do Souto Gonçalves

Tab
le 1
– D
ata
on
Am
yo
tro
ph
ic L
ate
ral
Scl
erosi
s
Cen
ter
Nu
mb
er
PtN
IV
Ag
e p
tNIV
D
ura
tio
n
ptN
IV
Nu
mb
er
FtN
IV
Ag
e F
tNIV
D
ura
tio
n
FtN
IV
Cu
rren
t A
ge
Nu
mb
er
FtN
IV
no
Ho
sp
Sti
ll
Ali
ve
Ex
tub
ati
on
D
eca
nu
lati
on
D
eath
s T
MV
1
64
58.5
±12.
0 0.
9±1.
4 30
60
.9±1
0.4
2.3±
2.1
63±1
2.7
25
15
7 3
15
8
2
176
52.5
±5.6
0.
9±1.
1 10
9 53
.3±5
.3
0.8±
2.2
54.6
±5.7
34
67
15
6
42
44
4
62
58.0
±13.
4 1.
9±1.
9 20
57
.1±1
2.6
0.7±
0.6
61.4
±12.
2 4
35
0 0
27
7
7
23
55±1
4 1.
3±1.
6 11
55
±15
1±0.
9 60
±2
NK
2
4 1
9 5
8
83
56.1
±9.0
0.
9±0.
9 19
55
.5±9
.0
1.1±
2.1
NK
N
K
6 0
0 7
6
10
4 67
.8±6
.9
1.3±
0.8
4 69
.3±6
.6
2.0±
1.9
70.5
±8.4
N
K
1 0
0 3
1
11
78
59.5
±9.4
0.
9±1.
1 27
60
.3±1
.3
0.6 ±0.5
62
.2±9
.1
NK
14
0
0 13
6
13
120
64±2
4.2
NK
47
N
K
1,84
±0.8
N
K
NK
34
N
K
NK
86
7
16
13
59.3
±10.
4 1.
3±0.
8 13
59
.3±1
0.4
2.1±
2.5
NK
N
K
NK
0
0 N
K
NK
19
49
61.9
±13.
4 0.
9±1.
0 22
N
K
0.3±
0.7
70.4
±7.6
22
12
0
0 10
6
20
150
58.6
±24.
5 N
K
33
NK
23
.8
NK
N
K
29
0 0
4 6
Leg
end
– N
ptN
IV –
num
ber
of p
atie
nts
begi
nnin
g no
ctur
nal n
onin
vasi
ve v
enti
lati
on (
NIV
); A
ge p
tNIV
- ag
e w
hen
begi
nnin
g pa
rt-t
ime
(noc
turn
al)
NIV
; Dur
atio
n pt
NIV
-tim
e of
use
of
NIV
<20
ho
urs
per
day;
N f
tNIV
- n
umbe
r of
pat
ient
s pr
ogre
ssin
g to
>20
hr/
d ve
ntil
ator
dep
ende
nce;
Dur
atio
n ft
NIV
-dur
atio
n of
con
tinu
ous
NIV
sup
port
; Cur
rent
Age
-ag
e cu
rren
tly
or a
t tim
e of
dea
th;
Sti
ll A
live
-num
ber
of c
onti
nuou
sly
NIV
dep
ende
nt p
atie
nts
stil
l usi
ng c
onti
nuou
s N
IV; E
xt-N
umbe
r of
ext
ubat
ions
of
“unw
eana
ble”
pat
ient
s to
ful
l-se
ttin
g N
IV s
uppo
rt; D
ecan
-Num
ber
of
cont
inuo
usly
ven
tila
tor
depe
nden
t pat
ient
s de
canu
late
d to
NIV
; Dea
ths-
res
pira
tory
/tot
al; T
MV
– n
umbe
r of
pat
ient
s un
der
trac
heos
tom
y ve
ntil
atio
n; N
K –
not
kno
wne
d
Tota
l p
tNIV
– 8
22
pa
tien
ts
To
tal
ftN
IV –
335 p
ati
ents
Tota
l E
xtu
bati
on
s – 2
6
T
ota
l D
ecan
ula
tion
s – 1
0
Tota
l D
eath
s –
21
6 p
ati
ents
T
ota
l T
rach
eost
om
y –
96
Med
ian
Age
ptN
IV –
58,1
±12,6
yea
rs
Med
ian
Du
rati
on
ptN
IV -
1,0
±0
,8 y
ears
Med
ian
Age
ftN
IV -
56,2
±4,9
yea
rs
Nu
mb
erF
tNIV
noH
osp
- 8
5
Med
ian
Du
rati
on
ftN
IV -
3,4
±1
,3 y
ears
Cu
rren
t A
ge
– 5
9,3
±7,6
yea
rs
S
till
Ali
ve
– 1
86 f
tNIV
pati
ents
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 251

Tab
le 2
– D
ata
on
Du
chen
ne
Mu
scu
lar
Dyst
rop
hy
Cen
ter
Nu
mb
er
PtN
IV
Ag
e p
tNIV
D
ura
tio
n
ptN
IV
Nu
mb
er
FtN
IV
Ag
e F
tNIV
D
ura
tio
n
FtN
IV
Cu
rren
t A
ge
Sti
ll
Ali
ve
Nu
mb
er
FtN
IV
no
Ho
sp
Ex
tub
ati
on
D
eca
nu
lati
on
D
eath
s T
IPP
V
1
18
16.3
±4.6
3.
4±1.
8 14
20
.4±6
.3
5.4±
4.4
20.1
±9.2
11
12
7
2 3
0 2
12
0 20
.3±2
.8
2±2.
1 10
1 22
.3±5
.9
7±5.
9 30
.3±6
.1
87
23
29
9 14
0
3
88
18.9
±3.3
5.
4±3.
3 56
24
.7±4
.6
5.8±
3.4
31±5
.2
46
NK
8
2 10
0
4
28
20.5
±4.1
4.
7±3.
4 4
27.2
±6.2
2±
0.8
25.3
±4.5
1
0 0
1 4
1 5
38
12
.8±2
,9
25±1
4,6
2 12
±0,3
17
±22
14.9
±3
32
1 1
0 7
1
7
16
21±4
2±
1.6
9 25
±2
1.8±
1.3
25±1
5
NK
1
2 4
0 8
25
18
.3±4
3.
5±2.
4 11
21
.9±2
.4
5±4.
4 26
.9±4
.3
8 9
2 1
3 0
9
24
18±1
.6
9.9±
4.5
24
28.1
±4.6
4.
2±2.
8 32
.3±2
.8
24
24
0 0
0 0
10
10
22
.7±3
.2
1.7±
1.9
10
24.3
±4.1
4.
6±1.
6 28
.4±4
.6
10
10
0 4
0 0
11
9
18.7
±5.2
4.
6±2.
2 4
23.3
±6.5
4±
2.8
27±5
3
NK
0
0 1
1 1
2
100
18.9
±3.2
8.
3±4.
3 56
23
.6±3
.5
5.7±
3 28
.7±4
.2
23
38
1 0
33
12
13
16
2 17
±12.
9 N
K
51
NK
N
K
27.5
30
N
K
12
4 21
5
14
4
21.3
±3
5±3
4 25
±4
3.8±
1.4
28
2 N
K
0 0
2 0
15
6
22±2
.8
3±1.
1 6
25±2
.4
4.9±
3.2
29.9
±3.6
4
NK
0
0 2
0 1
6
3 20
±3.9
10
.0±5
.6
3 30
±4
2.4±
1.4
32.4
±3.9
3
3 0
0 0
0 1
7
36
20.8
±4.6
3.
3±1.
8 17
24
.5±4
.5
4.0±
2.6
28.2
±4.9
8
NK
0
0 4
7 1
8
13
19.8
±2.8
5.
7±2.
2 13
25
.5±4
.2
4.8±
3.6
30.8
±4.2
11
N
K
0 0
2 2
Leg
end
– N
ptN
IV –
num
ber
of p
atie
nts
begi
nnin
g no
ctur
nal n
onin
vasi
ve v
enti
lati
on (
NIV
); A
ge p
tNIV
- ag
e w
hen
begi
nnin
g pa
rt-t
ime
(noc
turn
al)
NIV
; Dur
atio
n pt
NIV
-tim
e of
use
of
NIV
<20
ho
urs
per
day;
N f
tNIV
- n
umbe
r of
pat
ient
s pr
ogre
ssin
g to
>20
hr/
d ve
ntil
ator
dep
ende
nce;
Dur
atio
n ft
NIV
-dur
atio
n of
con
tinu
ous
NIV
sup
port
; Cur
rent
Age
-ag
e cu
rren
tly
or a
t tim
e of
dea
th;
Sti
ll A
live
-num
ber
of c
onti
nuou
sly
NIV
dep
ende
nt p
atie
nts
stil
l usi
ng c
onti
nuou
s N
IV; E
xt-N
umbe
r of
ext
ubat
ions
of
“unw
eana
ble”
pat
ient
s to
ful
l-se
ttin
g N
IV s
uppo
rt; D
ecan
-Num
ber
of
cont
inuo
usly
ven
tila
tor
depe
nden
t pat
ient
s de
canu
late
d to
NIV
; Dea
ths-
res
pira
tory
/tot
al; T
MV
– n
umbe
r of
pat
ient
s un
der
trac
heos
tom
y ve
ntil
atio
n ; N
K –
not
kno
wne
d T
ota
l p
tNIV
– 7
00
pati
ents
To
tal
ftN
IV –
385
pati
ents
To
tal
Extu
ba
tio
ns
– 6
1
To
tal
Dec
an
ula
tio
ns
– 2
5
To
tal
Dea
ths
- 110
To
tal
Tra
cheo
stom
y –
29
M
edia
n A
ge
ptN
IV –
18.9
±4
.91
yea
rs
Med
ian
Du
rati
on
ptN
IV –
3.6
3±
2.7
yea
rs
Med
ian
Age
ftN
IV –
23
.8±
6.6
yea
rs
Nu
mb
er F
tNIV
no
Ho
sp –
120
M
edia
n D
ura
tion
ftN
IV –
5.5
6±
1.6
yea
rs
Sti
ll A
live
– 3
08
ftN
IV p
ati
ents
Cu
rren
t A
ge
- 28
,5±
4,2
yea
rs
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
252 Miguel Ramalho do Souto Gonçalves

Tab
le 3
– D
ata
on
Sp
ina
l M
usc
ula
r A
trop
hy t
yp
e 1
Cen
ter
Nu
mb
er
PtN
IV
Ag
e p
tNIV
D
ura
tio
n
ptN
IV
Nu
mb
er
FtN
IV
Ag
e F
tNIV
D
ura
tio
n
FtN
IV
Cu
rren
t A
ge
Nu
mb
er
FtN
IV
no
Ho
sp
Sti
ll
Ali
ve
Ex
tub
ati
on
D
eca
nu
lati
on
D
eath
s T
IPP
V
1
11
0.3±
0.3
0.2±
0.4
10
0,4±
0,2
2,4±
1.7
5.3±
3.1
7 6
8 0
4 3
2
76
0.4±
0.3
0.6±
0.1
22
0.9±
2.7
9.4±
3.5
10.3
±3.4
5
19
121
0 3
4
5
3 0.
5±0.
45
3.7±
4 4
0.6±
0.65
1.
8±0.
8 1.
2±0.
04
2 0
0 0
4 6
7
3 0.
7±0.
8 1.
4±2.
2 2
0,3±
0,1
0,1±
0 5±
5 N
K
2 0
0 1
2
13
7 0,
9 N
K
1 0,
1 0,
3 4.
8 N
K
0 13
0
7 0
16
1 0.
5 0.
4 1
0,5
4.5
5 N
K
1 0
0 0
0 L
egen
d –
N p
tNIV
– n
umbe
r of
pat
ient
s be
ginn
ing
noct
urna
l non
inva
sive
ven
tila
tion
(N
IV);
Age
ptN
IV-
age
whe
n be
ginn
ing
part
-tim
e (n
octu
rnal
) N
IV; D
urat
ion
ptN
IV-t
ime
of u
se o
f N
IV<
20
hour
s pe
r da
y; N
ftN
IV -
num
ber
of p
atie
nts
prog
ress
ing
to >
20 h
r/d
vent
ilat
or d
epen
denc
e; D
urat
ion
ftN
IV-d
urat
ion
of c
onti
nuou
s N
IV s
uppo
rt; C
urre
nt A
ge -
age
curr
entl
y or
at t
ime
of d
eath
; S
till
Ali
ve-n
umbe
r of
con
tinu
ousl
y N
IV d
epen
dent
pat
ient
s st
ill u
sing
con
tinu
ous
NIV
; Ext
-Num
ber
of e
xtub
atio
ns o
f “u
nwea
nabl
e” p
atie
nts
to f
ull-
sett
ing
NIV
sup
port
; Dec
an-N
umbe
r of
co
ntin
uous
ly v
enti
lato
r de
pend
ent p
atie
nts
deca
nula
ted
to N
IV; D
eath
s- r
espi
rato
ry/t
otal
; TM
V –
num
ber
of p
atie
nts
unde
r tr
ache
osto
my
vent
ilat
ion;
NK
– n
ot k
now
ned
Tota
l p
tNIV
– 1
01
pa
tien
ts
To
tal
ftN
IV –
40 p
ati
ents
Tota
l E
xtu
bati
on
s – 1
42
T
ota
l D
ecan
ula
tion
s – 0
Tota
l D
eath
s -
18
To
tal
Tra
cheo
stom
y –
15
M
ean
Age
ptN
IV –
0.4
3±
0.2
yea
rs
Mea
n D
ura
tio
n p
tNIV
- 0
.56
±0
.5 y
ears
M
ean
Age
ftN
IV –
0.6
8±
0.3
yea
rs
N
um
ber
FtN
IV n
oH
osp
- 1
4
Mea
n D
ura
tio
n f
tNIV
– 6
.0±
3.8
yea
rs
Cu
rren
t A
ge
– 7
.6±
2.4
yea
rs
Sti
ll A
live
– 2
8 f
tNIV
pati
ents
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 253

TABLE 4 - The Evolution of Consensus and Review Articles on Noninvasive Ventilation and Neuromuscular Disease.
Legend: Year - year of publication, O2 - oxygen avoidance, CPF – cough peak flow; AS- air stacking; MAC – mechanical assisted cough; lpMAC - mechanically assisted coughing with low pressure (<35); hpMAC – mechanical assisted coughing, high pressure (>35); lsp- low span BiPAP; hsp - high span BiPAP; MP – mouthpiece NIV, ptNIV - part-time NIV (up to 16 hours/day); ftNIV - full-time NIV (>20hours/day); TMV – tracheostomy mechanical ventilation;SpO2 feedback – protocol with oximetry feedback
Reference Year O2 avoidance
CPF AS MAC lpMAC hpMAC lsP HsP MP ptNIV ftNIV Extubation/Dednulation TMV SpO2 feedback
81 1993 X 41 1993 X X X X X X 17 1994 X X X 82 1995 X X X X X 50 1996 X X X X X X X X X X X 83 1997 X X X X 84 1997 X 85 1997 X X X 23 1998 X X X X X X X X 86 1998 X X X X X 87 2000 X X X X X 88 2002 X X X X X X X 57 2002 X X X X X X 89 2003 X X X X X 90 2003 X X X X X X X X 29 2004 X X X X X X X X X X X 91 2004 X X X X X X 92 2004 X X X X X X X X 93 2005 X X X X X 94 2005 X X X X X X X 95 2005 X X X X X 96 2006 X X X X X X X X X X 19 2006 X X X X X X X X 97 2006 X X X X X X X 98 2006 X X X X X X X X 99 2006 X X X X X X 100 2006 X X X X 58 2006 X X X 101 2006 X X X X X X X X 102 2007 X X X X X X 103 2007 X X X X X X X X X X 104 2007 X X X X X X X X X(Extubation) 105 2007 X X X 75 2007 X X X X X X X X 106 2008 X X X X X 107 2008 X X 108 2008 X X 109 2008 X X X 110 2009 X X X X X X X X 74 2009 X X X X X 111 2009 X X X X X X 112 2009 X X X 113 2009 X X X X X X X X 49 2009 X X X X X X X X X X 114 2009 X X X X X X 115 2009 X X X X X X 116 2009 X X X X 117 2009 X X X X X X X 118 2009 X X X X X X X X X
30 2010 X X X X X X X X X X X X
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
254 Miguel Ramalho do Souto Gonçalves

REFERENCES:
1. Bach J. The history of mechancial ventilation and respiratory
muscle aids. In: Bach JR (ed) Noninvasive Mechanical Ventilation.
Philadephia, Hanley & Belfus. 2002:45-72.
2. Bach J. A historical perspective on the use of noninvasive
ventilatory support alternatives. Am Rev Respir Dis 1996(22):161
181.
3. Round Table Conference on Poliomyelitis Equipment, Roosevelt
Hotel, White Plaines, New York City National Foundation for
Infantile Paralysis-March of Dimes, Inc. May 1953.
4. Bach JR, Alba AS. Sleep and nocturnal mouthpiece IPPV efficiency
in postpoliomyelitis ventilator users. Chest. Dec
1994;106(6):1705-1710.
5. Hodes H. Treatment of respiratory difficulty in poliomyelitis In:
Poliomyelitis: papers and discussion; presented at the third
international poliomyelitis conference, Lippincott, Philadelphia.
1955:91-113.
6. Bach JR. Update and perspectives on noninvasive respiratory
muscle aids. Part 1: The inspiratory aids. Chest. Apr
1994;105(4):1230-1240.
7. Bach JR, Alba AS, Saporito LR. Intermittent positive pressure
ventilation via the mouth as an alternative to tracheostomy for
257 ventilator users. Chest. Jan 1993;103(1):174-182.
8. Bach JR, Alba A, Mosher R, Delaubier A. Intermittent positive
pressure ventilation via nasal access in the management of
respiratory insufficiency. Chest. Jul 1987;92(1):168-170.
9. Servera E, Sancho J, Zafra MJ, Catala A, Vergara P, Marin J.
Alternatives to endotracheal intubation for patients with
neuromuscular diseases. Am J Phys Med Rehabil. Nov
2005;84(11):851-857.
10. Toussaint M, Steens M, Wasteels G, Soudon P. Diurnal ventilation
via mouthpiece: survival in end-stage Duchenne patients. Eur
Respir J. Sep 2006;28(3):549-555.
11. Brochard L, Isabey D, Piquet J, et al. Reversal of acute
exacerbations of chronic obstructive lung disease by inspiratory
assistance with a face mask. N Engl J Med. Nov 29
1990;323(22):1523-1530.
12. Carrey Z, Gottfried SB, Levy RD. Ventilatory muscle support in
respiratory failure with nasal positive pressure ventilation.
Chest. Jan 1990;97(1):150-158.
13. Ellis ER, Bye PT, Bruderer J, Sullivan C. Treatment of
respiratory failure during sleep in patients with neuromuscular
disease, positive pressure ventilation through a nose mask. Am
Rev Respir Dis. 1987;135:148-152.
14. Kerby G, Mayer L, Pingleton SK. Nocturnal positive pressure
ventilation via nasal mask. Am Rev Respir Dis. 1987;135(738-40).
15. Bach JR, O'Brien J, Krotenberg R, Alba AS. Management of end
stage respiratory failure in Duchenne muscular dystrophy. Muscle
Nerve. Feb 1987;10(2):177-182.
16. Wallgren-Pettersson C, Laing NG. 109th ENMC International
Workshop: 5th workshop on nemaline myopathy, 11th-13th October
2002, Naarden, The Netherlands. Neuromuscul Disord. Aug
2003;13(6):501-507.
17. Hotes LS, Johnson JA, Sicilian L. Long-term care, rehabilitation,
and legal and ethical considerations in the management of
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 255

neuromuscular disease with respiratory dysfunction. Clin Chest
Med. Dec 1994;15(4):783-795.
18. Bach JR. Continuous noninvasive ventilation for patients with
neuromuscular disease and spinal cord injury. Semin Respir Crit
Care Med. Jun 2002;23(3):283-292.
19. Benditt JO. Full-time noninvasive ventilation: possible and
desirable. Respir Care. Sep 2006;51(9):1005-1012; discussion
1012-1005.
20. Schonhofer B, Sortor-Leger S. Equipment needs for noninvasive
mechanical ventilation. Eur Respir J. Oct 2002;20(4):1029-1036.
21. Fauroux B, Leroux K, Desmarais G, et al. Performance of
ventilators for noninvasive positive-pressure ventilation in
children. Eur Respir J. Jun 2008;31(6):1300-1307.
22. Tzeng AC, Bach JR. Prevention of pulmonary morbidity for patients
with neuromuscular disease. Chest. Nov 2000;118(5):1390-1396.
23. Make BJ, Hill NS, Goldberg AI, et al. Mechanical ventilation
beyond the intensive care unit. Report of a consensus conference
of the American College of Chest Physicians. Chest. May
1998;113(5 Suppl):289S-344S.
24. Gomez-Merino E, Bach JR. Duchenne muscular dystrophy:
prolongation of life by noninvasive ventilation and mechanically
assisted coughing. Am J Phys Med Rehabil. Jun 2002;81(6):411-415.
25. Vitacca M, Paneroni M, Trainini D, et al. At home and on demand
mechanical cough assistance program for patients with amyotrophic
lateral sclerosis. Am J Phys Med Rehabil. May 2010;89(5):401-406.
26. Bach JR, Saporito LR. Criteria for extubation and tracheostomy
tube removal for patients with ventilatory failure. A different
approach to weaning. Chest. Dec 1996;110(6):1566-1571.
27. Bach JR, Goncalves MR, Hamdani I, Winck JC. Extubation of
patients with neuromuscular weakness: a new management paradigm.
Chest. May 2010;137(5):1033-1039.
28. Bach JR, Bianchi C, Aufiero E. Oximetry and indications for
tracheotomy for amyotrophic lateral sclerosis. Chest. Nov
2004;126(5):1502-1507.
29. Finder JD, Birnkrant D, Carl J, et al. Respiratory care of the
patient with Duchenne muscular dystrophy: ATS consensus
statement. Am J Respir Crit Care Med. Aug 15 2004;170(4):456-465.
30. Birnkrant DJ, Bushby KM, Amin RS, et al. The respiratory
management of patients with duchenne muscular dystrophy: a DMD
care considerations working group specialty article. Pediatr
Pulmonol. Aug 2010;45(8):739-748.
31. Bach JR, Rajaraman R, Ballanger F, et al. Neuromuscular
ventilatory insufficiency: effect of home mechanical ventilator
use v oxygen therapy on pneumonia and hospitalization rates. Am J
Phys Med Rehabil. Jan-Feb 1998;77(1):8-19.
32. Bach JR. Update and perspective on noninvasive respiratory muscle
aids. Part 2: The expiratory aids. Chest. May 1994;105(5):1538-
1544.
33. Maessen M, Veldink JH, van den Berg LH, Schouten HJ, van der Wal
G, Onwuteaka-Philipsen BD. Requests for euthanasia: origin of
suffering in ALS, heart failure, and cancer patients. J Neurol.
Jul 2010;257(7):1192-1198.
34. Kang SW, Bach JR. Maximum insufflation capacity: vital capacity
and cough flows in neuromuscular disease. Am J Phys Med Rehabil.
May-Jun 2000;79(3):222-227.
35. Kang SW, Bach JR. Maximum insufflation capacity. Chest. Jul
2000;118(1):61-65.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
256 Miguel Ramalho do Souto Gonçalves

36. Bach JR. Amyotrophic lateral sclerosis: predictors for
prolongation of life by noninvasive respiratory aids. Arch Phys
Med Rehabil. Sep 1995;76(9):828-832.
37. Bach JR, Bianchi C. Prevention of pectus excavatum for children
with spinal muscular atrophy type 1. Am J Phys Med Rehabil. Oct
2003;82(10):815-819.
38. Chatwin M, Bush A, Simonds AK. Outcome of goal-directed non-
invasive ventilation and mechanical insufflation/exsufflation in
spinal muscular atrophy type I. Arch Dis Child. Jun 23 2010.
39. Bach JR, Goncalves MR, Paez S, Winck JC, Leitao S, Abreu P.
Expiratory flow maneuvers in patients with neuromuscular
diseases. Am J Phys Med Rehabil. Feb 2006;85(2):105-111.
40. Bach JR. Mechanical insufflation-exsufflation. Comparison of peak
expiratory flows with manually assisted and unassisted coughing
techniques. Chest. Nov 1993;104(5):1553-1562.
41. Robert D, Willig TN, Leger P, Paulus J. Long-term nasal
ventilation in neuromuscular disorders: report of a consensus
conference. Eur Respir J. Apr 1993;6(4):599-606.
42. Farrero E, Prats E, Povedano M, Martinez-Matos JA, Manresa F,
Escarrabill J. Survival in amyotrophic lateral sclerosis with
home mechanical ventilation: the impact of systematic respiratory
assessment and bulbar involvement. Chest. Jun 2005;127(6):2132-
2138.
43. Boitano LJ, Benditt JO. An evaluation of home volume ventilators
that support open-circuit mouthpiece ventilation. Respir Care.
Nov 2005;50(11):1457-1461.
44. Bach JR. Bilevel pressure vs volume ventilators for amyotrophic
lateral sclerosis patients. Chest. Dec 2006;130(6):1949; author
reply 1949-1950.
45. Chatwin M. How to use a mechanical insufflator-exsufflator "cough
assist machine". Breathe. 2008;volume 4(June):321-325.
46. Winck JC, Goncalves MR, Lourenco C, Viana P, Almeida J, Bach JR.
Effects of mechanical insufflation-exsufflation on respiratory
parameters for patients with chronic airway secretion
encumbrance. Chest. Sep 2004;126(3):774-780.
47. Fauroux B, Guillemot N, Aubertin G, et al. Physiologic benefits
of mechanical insufflation-exsufflation in children with
neuromuscular diseases. Chest. Jan 2008;133(1):161-168.
48. Sancho J, Servera E, Marin J, Vergara P, Belda FJ, Bach JR.
Effect of lung mechanics on mechanically assisted flows and
volumes. Am J Phys Med Rehabil. Sep 2004;83(9):698-703.
49. Boitano LJ. Equipment options for cough augmentation,
ventilation, and noninvasive interfaces in neuromuscular
respiratory management. Pediatrics. May 2009;123 Suppl 4:S226-
230.
50. Dean S, Bach JR. The use of noninvasive respiratory muscle aids
in the management of patients with progressive neuromuscular
diseases. Respir Care Clin N Am. Jun 1996;2(2):223-240.
51. Bach JR, Intintola P, Alba AS, Holland IE. The ventilator-
assisted individual. Cost analysis of institutionalization vs
rehabilitation and in-home management. Chest. Jan 1992;101(1):26-
30.
52. Soudon P, Steens M, Toussaint M. A comparison of invasive versus
noninvasive full-time mechanical ventilation in Duchenne muscular
dystrophy. Chron Respir Dis. 2008;5(2):87-93.
53. Vianello A, Bevilacqua M, Arcaro G, Serra E. Prevention of
pulmonary morbidity in patients with neuromuscular disorders: a
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 257

possible role for permanent cricothyroid minitracheostomy. Chest.
Jul 1998;114(1):346-347.
54. Bach JR. Tracheostomy for advanced neuromuscular disease. Con.
Chron Respir Dis. 2007;4(4):239-241.
55. Bach JR, Goncalves M. Ventilator weaning by lung expansion and
decannulation. Am J Phys Med Rehabil. Jul 2004;83(7):560-568.
56. Bach JR. A comparison of long-term ventilatory support
alternatives from the perspective of the patient and care giver.
Chest. Dec 1993;104(6):1702-1706.
57. Shneerson JM, Simonds AK. Noninvasive ventilation for chest wall
and neuromuscular disorders. Eur Respir J. Aug 2002;20(2):480-
487.
58. Mehta S. Neuromuscular disease causing acute respiratory failure.
Respir Care. Sep 2006;51(9):1016-1021; discussion 1021-1013.
59. Birnkrant DJ, Pope JF, Eiben RM. Management of the respiratory
complications of neuromuscular diseases in the pediatric
intensive care unit. J Child Neurol. Mar 1999;14(3):139-143.
60. Baydur A, Kanel G. Tracheobronchomalacia and tracheal hemorrhage
in patients with Duchenne muscular dystrophy receiving long-term
ventilation with uncuffed tracheostomies. Chest. Apr
2003;123(4):1307-1311.
61. Biering-Sorensen M, Biering-Sorensen F. Tracheostomy in spinal
cord injured: frequency and follow up. Paraplegia. Sep
1992;30(9):656-660.
62. Epstein SK. Late complications of tracheostomy. Respir Care. Apr
2005;50(4):542-549.
63. Sancho J, Servera E, Vergara P, Marin J. Mechanical insufflation-
exsufflation vs. tracheal suctioning via tracheostomy tubes for
patients with amyotrophic lateral sclerosis: a pilot study. Am J
Phys Med Rehabil. Oct 2003;82(10):750-753.
64. Bach JR. Amyotrophic lateral sclerosis: prolongation of life by
noninvasive respiratory aids
Chest. Jul 2002;122(1):92-98.
65. Bach JR. New approaches in the rehabilitation of the traumatic
high level quadriplegic. Am J Phys Med Rehabil. Feb
1991;70(1):13-19.
66. Bach JR, Alba AS. Noninvasive options for ventilatory support of
the traumatic high level quadriplegic patient. Chest. Sep
1990;98(3):613-619.
67. Viroslav J, Rosenblatt R, Tomazevic SM. Respiratory management,
survival, and quality of life for high-level traumatic
tetraplegics. Respir Care Clin N Am. Jun 1996;2(2):313-322.
68. Bach JR, Wang TG. Noninvasive long-term ventilatory support for
individuals with spinal muscular atrophy and functional bulbar
musculature. Arch Phys Med Rehabil. Mar 1995;76(3):213-217.
69. Bach JR, Ishikawa Y, Kim H. Prevention of pulmonary morbidity for
patients with Duchenne muscular dystrophy. Chest. Oct
1997;112(4):1024-1028.
70. Garstang SV, Kirshblum SC, Wood KE. Patient preference for in-
exsufflation for secretion management with spinal cord injury. J
Spinal Cord Med. Summer 2000;23(2):80-85.
71. Sancho J, Servera E, Diaz J, Marin J. Efficacy of mechanical
insufflation-exsufflation in medically stable patients with
amyotrophic lateral sclerosis. Chest. Apr 2004;125(4):1400-1405.
72. Bach JR, Niranjan V, Weaver B. Spinal muscular atrophy type 1: A
noninvasive respiratory management approach. Chest. Apr
2000;117(4):1100-1105.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
258 Miguel Ramalho do Souto Gonçalves

73. Bach JR, Saltstein K, Sinquee D, Weaver B, Komaroff E. Long-term
survival in Werdnig-Hoffmann disease. Am J Phys Med Rehabil. May
2007;86(5):339-345 quiz 346-338, 379.
74. Roper H, Quinlivan R. Implementation of "the consensus statement
for the standard of care in spinal muscular atrophy" when applied
to infants with severe type 1 SMA in the UK. Arch Dis Child. Jul
6 2010.
75. Wang CH, Finkel RS, Bertini ES, et al. Consensus statement for
standard of care in spinal muscular atrophy. J Child Neurol. Aug
2007;22(8):1027-1049.
76. Albert SM, Murphy PL, Del Bene ML, Rowland LP. Prospective study
of palliative care in ALS: choice, timing, outcomes. J Neurol
Sci. Oct 31 1999;169(1-2):108-113.
77. Kuhnlein P, Kubler A, Raubold S, et al. Palliative care and
circumstances of dying in German ALS patients using non-invasive
ventilation. Amyotroph Lateral Scler. Apr 2008;9(2):91-98.
78. Kwiecinski H. [Symptomatic treatment and palliative care of ALS].
Neurol Neurochir Pol. 2001;35(1 Suppl):51-59.
79. Laaksovirta H. [Palliative care tailored according to the
symptoms of the ALS patient is an art form]. Duodecim.
2005;121(2):220-224.
80. Zimmerman EK, Eslinger PJ, Simmons Z, Barrett AM. Emotional
perception deficits in amyotrophic lateral sclerosis. Cogn Behav
Neurol. Jun 2007;20(2):79-82.
81. Hughes RA, Bihari D. Acute neuromuscular respiratory paralysis. J
Neurol Neurosurg Psychiatry. Apr 1993;56(4):334-343.
82. Corrado A, Gorini M, De Paola E. Alternative techniques for
managing acute neuromuscular respiratory failure. Semin Neurol.
Mar 1995;15(1):84-89.
83. AARC- Consenus statement. Noninvasive positive pressure
ventilation. Respir Care. 1997;42:365-369.
84. Teener JW, Raps EC. Evaluation and treatment of respiratory
failure in neuromuscular disease. Rheum Dis Clin North Am. May
1997;23(2):277-292.
85. Barthlen GM. Nocturnal respiratory failure as an indication of
noninvasive ventilation in the patient with neuromuscular
disease. Respiration. 1997;64 Suppl 1:35-38.
86. Bella I, Chad DA. Neuromuscular disorders and acute respiratory
failure. Neurol Clin. May 1998;16(2):391-417.
87. Gozal D. Pulmonary manifestations of neuromuscular disease with
special reference to Duchenne muscular dystrophy and spinal
muscular atrophy. Pediatr Pulmonol. Feb 2000;29(2):141-150.
88. Birnkrant DJ. The assessment and management of the respiratory
complications of pediatric neuromuscular diseases. Clin Pediatr
(Phila). Jun 2002;41(5):301-308.
89. Howard RS, Davidson C. Long term ventilation in neurogenic
respiratory failure. J Neurol Neurosurg Psychiatry. Sep 2003;74
Suppl 3:iii24-30.
90. Farrero E, Prats E, Escarrabill J. [Series 4: respiratory muscles
in neuromuscular diseases and the chest cavity. Decision making
in the clinical management of patients with lateral amyotrophic
sclerosis]. Arch Bronconeumol. May 2003;39(5):226-232.
91. Perrin C, Unterborn JN, Ambrosio CD, Hill NS. Pulmonary
complications of chronic neuromuscular diseases and their
management. Muscle Nerve. Jan 2004;29(1):5-27.
92. Wallgren-Pettersson C, Bushby K, Mellies U, Simonds A. 117th ENMC
workshop: ventilatory support in congenital neuromuscular
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 259

disorders -- congenital myopathies, congenital muscular
dystrophies, congenital myotonic dystrophy and SMA (II) 4-6 April
2003, Naarden, The Netherlands. Neuromuscul Disord. Jan
2004;14(1):56-69.
93. Simmons Z. Management strategies for patients with amyotrophic
lateral sclerosis from diagnosis through death. Neurologist. Sep
2005;11(5):257-270.
94. Mellies U, Dohna-Schwake C, Voit T. Respiratory function
assessment and intervention in neuromuscular disorders. Curr Opin
Neurol. Oct 2005;18(5):543-547.
95. Simonds AK. Ethical aspects of home long term ventilation in
children with neuromuscular disease. Paediatr Respir Rev. Sep
2005;6(3):209-214.
96. Kang SW. Pulmonary rehabilitation in patients with neuromuscular
disease. Yonsei Med J. Jun 30 2006;47(3):307-314.
97. Hess DR. Noninvasive ventilation in neuromuscular disease:
equipment and application. Respir Care. Aug 2006;51(8):896-911;
discussion 911-892.
98. Simonds AK. Recent advances in respiratory care for neuromuscular
disease. Chest. Dec 2006;130(6):1879-1886.
99. Panitch HB. Respiratory issues in the management of children with
neuromuscular disease. Respir Care. Aug 2006;51(8):885-893;
discussion 894-885.
100. Giannini A, Pinto AM, Rossetti G, et al. Respiratory failure in
infants due to spinal muscular atrophy with respiratory distress
type 1. Intensive Care Med. Nov 2006;32(11):1851-1855.
101. Kirk VG. Pulmonary complications of neuromuscular disease.
Paediatr Respir Rev. 2006;7 Suppl 1:S232-234.
102. Gregory SA. Evaluation and management of respiratory muscle
dysfunction in ALS. NeuroRehabilitation. 2007;22(6):435-443.
103. Simonds AK. Respiratory support for the severely handicapped
child with neuromuscular disease: ethics and practicality. Semin
Respir Crit Care Med. Jun 2007;28(3):342-354.
104. Birnkrant DJ, Panitch HB, Benditt JO, et al. American College of
Chest Physicians consensus statement on the respiratory and
related management of patients with Duchenne muscular dystrophy
undergoing anesthesia or sedation. Chest. Dec 2007;132(6):1977-
1986.
105. Annane D, Orlikowski D, Chevret S, Chevrolet JC, Raphael JC.
Nocturnal mechanical ventilation for chronic hypoventilation in
patients with neuromuscular and chest wall disorders. Cochrane
Database Syst Rev. 2007(4):CD001941.
106. Manzur AY, Kinali M, Muntoni F. Update on the management of
Duchenne muscular dystrophy. Arch Dis Child. Nov 2008;93(11):986-
990.
107. Hutchinson D, Whyte K. Neuromuscular disease and respiratory
failure. Pract Neurol. Aug 2008;8(4):229-237.
108. Weber M. Meeting report of European ALS Consortium (EALSC): 6th
European ALS congress research workshop and young investigators'
meeting. Amyotroph Lateral Scler. Oct 2008;9(5):318-320.
109. Ozsancak A, D'Ambrosio C, Hill NS. Nocturnal noninvasive
ventilation. Chest. May 2008;133(5):1275-1286.
110. Ambrosino N, Carpene N, Gherardi M. Chronic respiratory care for
neuromuscular diseases in adults. Eur Respir J. Aug
2009;34(2):444-451.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
260 Miguel Ramalho do Souto Gonçalves

111. Benditt JO. Initiating noninvasive management of respiratory
insufficiency in neuromuscular disease. Pediatrics. May 2009;123
Suppl 4:S236-238.
112. Radunovic A, Annane D, Jewitt K, Mustfa N. Mechanical ventilation
for amyotrophic lateral sclerosis/motor neuron disease. Cochrane
Database Syst Rev. 2009(4):CD004427.
113. Schroth MK. Special considerations in the respiratory management
of spinal muscular atrophy. Pediatrics. May 2009;123 Suppl
4:S245-249.
114. Racca F, Del Sorbo L, Mongini T, Vianello A, Ranieri VM.
Respiratory management of acute respiratory failure in
neuromuscular diseases. Minerva Anestesiol. Jan 2010;76(1):51-62.
115. Miller RG, Jackson CE, Kasarskis EJ, et al. Practice parameter
update: The care of the patient with amyotrophic lateral
sclerosis: multidisciplinary care, symptom management, and
cognitive/behavioral impairment (an evidence-based review):
report of the Quality Standards Subcommittee of the American
Academy of Neurology. Neurology. Oct 13 2009;73(15):1227-1233.
116. Panitch HB. The pathophysiology of respiratory impairment in
pediatric neuromuscular diseases. Pediatrics. May 2009;123 Suppl
4:S215-218.
117. Vazquez-Sandoval A, Huang EJ, Jones SF. Hypoventilation in
neuromuscular disease. Semin Respir Crit Care Med. Jun
2009;30(3):348-358.
118. Kennedy JD, Martin AJ. Chronic respiratory failure and
neuromuscular disease. Pediatr Clin North Am. Feb 2009;56(1):261-
273, xii.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 261

Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
262 Miguel Ramalho do Souto Gonçalves

Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 263

Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
264 Miguel Ramalho do Souto Gonçalves

GENERAL DISCUSSION
All 10 studies that were part of this thesis were clinical and had direct positive impact
on the patients studied in which NIV was insufficient due to secretion encumbrance.
The addition of new measurements (VRI, MI-LIC, DF, PCF-PEF) in the chronic setting
permitted the correct indication for lung expansion and air stacking techniques. MAC
was able to achieve adequate CPF to clear secretions and was crucial to invert the ARF
episode and avoid hospitalizations. Failure to provide adequate settings for effective
nocturnal ventilatory support, mouthpiece IPPV, and manually and mechanical assisted
coughing continue to make respiratory failure inevitable for the great majority this
patient population.
Acute Respiratory Failure
During acute critical care, in most patients, mechanical ventilation is a short-term
treatment used for up to 7 days to support or replace spontaneous breathing until the
cause of respiratory failure resolves or results in death. Patients who receive mechanical
ventilation for more than 7 days, when remain unweanable after 4 weeks of resolution
of the acute respiratory failure (ARF) episode, have been classified as chronic
ventilator-dependent patients(19). Intubated ventilator supported patients can develop
hypo- or hypercapnia, decreases in pulmonary function because of airway mucus, and
inspiratory muscle deconditioning.
When there is no need for an artificial airway, conventional extubation attempts follow
successful “spontaneous breathing trials (SBTs) and the passing of ventilator weaning
parameters(411). This may either cause anxiety because the patient is not ready to
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 265

breathe autonomously, or the schedule is too conservative, delaying respiratory muscle
reconditioning. Further, the use of pulse oximetry, which can signal the presence of
airway mucus encumberment as well as their elimination with treatment, is lost with
oxygen administration that is typically arbitrarily used in this setting. Some patients
with muscle weakness are unable to sustain spontaneous breathing effort and are
dependent on mechanical ventilation for life support. Some of them may be successfully
treated with partial time NIV (nocturnal and for daytime periods), but patients who
require continuous mechanical ventilation usually require more attention and support
that is most cases end in tracheostomy ventilation(415).
Until our study nr 1, there have been no studies that focused on extubation of adult
complete ventilator dependent NMD patients. (155, 190). A recent controlled post-
extubation respiratory failure study of 106 patients included 2 with pure restrictive
syndromes but none with NMD and all had passed SBTs despite hypercapnia. They
were extubated to either supplemental O2 alone or in conjunction with bi-level PAP at
spans of up to 14 cm H2O, pressures inadequate to sustain our patients(497). A meta-
analysis of 12 extubation studies to bi-level PAP demonstrated decreased mortality,
ventilator associated pneumonia, length of stay, and resort to tracheotomy, however
unweanable NMD patients were uniformly excluded in all papers(20). Eligibility for
extubation was based on “readiness for weaning” and failure of SBTs in 30 minutes or
more. The outcomes of these studies were important to justify extubation to NIV for
primarily lung/airways diseases patients with some autonomous breathing ability. For
such patients SpO2>90% is usually acceptable with or without supplemental oxygen.
Unlike all previous studies, patients included in study nr 1 had no ability to
autonomously sustain breathing before or after extubation with VCs as low as 0 ml, so
no control group extubation to O2 would be possible, ethical, or permissible by any
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
266 Miguel Ramalho do Souto Gonçalves

review board. For our patients long-term inability to maintain SpO2≥95% despite
continuous NIV and MAC in ambient air is the indication for tracheotomy(481).
The success of our protocol was not only from providing continuous full-setting NIV
via a variety of interfaces, but from frequent and aggressive MAC (up to every 30 min)
both pre- and post-extubation to expel secretions and maintain or return SpO2 over
95%. Such a regimen simulates the normal need to cough during episodes of
bronchitis/pneumonia. The aggressive use of MAC via the endotracheal tube was the
main intervention that resulted in normalization of SpO2 in ambient air, the most
important criterion for extubation.
In an earlier study of extubation to NIV, of possible independent variables including
extent of need for ventilatory support, age, VC, and maximum CPF measured at
extubation, only maximum CPF predicted extubation success or failure for 62
consecutive extubation/decannulation attempts on 49 consecutive self-directed NMD
patients (358). Thirty-four of the patients were continuously ventilator dependent both
pre- and post-extubation/decannulation. In that study none of the 15
extubation/decannulation attempts on those with maximum CPF below 160 L/m
succeeded as opposed to an 89% success rate in this study. The most likely reasons for
the difference between then and now are: baseline SpO2 criterion for extubation 92%
vs. 95% and thus the earlier patients had more residual airway secretions or lung disease
at extubation; 5% vs. 39% of patients with pre-extubation experience with NIV and
MAC; less hospital staff experience with NIV and MAC; 50 of 62 were decanulated
(not extubated); the patients were in various hospital locations; and MAC was used less
often and without family involvement (9, 462).
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 267

The 87% first attempt extubation success rate on patients with maximum CPF<160 L/m
study nr 1 is greater than the 82.4% (61 of 74) success rate reported for extubating
ventilator dependent infants with SMA type 1 according to an almost identical
protocol(498). The difference is most likely due to the ability of these patients, as
opposed to babies, to fully cooperate with NIV and MAC. The SMA 1 patients may
have also had more severe bulbar-innervated muscle dysfunction. Thus, while the
extubation success rates for our patients with CPF<160 L/m were higher than those for
a comparable infant population they were significantly less (89% vs. 100%) (p<0.05)
than for patients with assisted CPF≥160 L/m. Unmeasurable assisted CPF indicate
inability to close the glottis and are often associated with airway collapse (stridor) and
saliva aspiration that render MAC less effective.
An NIV/MAC protocol has already been demonstrated to have avoided over 100
hospitalizations for continuously NIV dependent NMD patients (63, 127, 481). Study
nr 1 considered unweanable NMD patients for whom an acute hospitalization and
intubation could not be or were not avoided.
In this study, patients were extubated when the following criteria were satisfied: no
supplemental oxygen requirement to maintain SpO2 greater than 94%, chest radiograph
abnormalities cleared or clearing, respiratory depressants discontinued, airway
secretions less than on admission, and any nasal congestion cleared. Thus, once the
patient is afebrile with a normal white blood cell count and the SpO2 is normal on room
air, the nasogastric tube is first removed to facilitate immediate post-extubation nasal
IPPV. MAC is then provided via the upper airway via an oral-nasal interface and the
oximetry feedback protocol is followed.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
268 Miguel Ramalho do Souto Gonçalves

The general notion that early tracheotomy after intubation somehow facilitates
ventilator weaning (436) should be reassessed for patients with NMD. In most
instances, upon extubation, patients with VC of 250 ml or more eventually weaned from
continuous to nocturnal-only aid by taking fewer and fewer mouth piece IPPVs. Thus,
the paradigm of weaning then extubation can be changed to extubation then weaning.
Employing noninvasive rather than invasive mechanical ventilation has also been
reported to decrease risk of ventilator associated pneumonia by 75% or greater(103,
499) and other subsequent complications associated with invasive airway tubes. Use of
mouth pieces rather than other interfaces for daytime ventilatory support also facilitated
speech, oral intake, comfort, and air stacking to deep lung insufflations to maintain
pulmonary compliance, (127, 362, 500) diminished atelectasis, and augmented
CPF(362). Nasal interface skin pressure was also avoided with mouthpiece use.
The main purpose of study nr 1 was not to facilitate ventilator weaning or to consider
long-term outcomes but simply to extubate unweanable NMD patients without
tracheotomy. It has already been suggested that extubation and decannulation can
facilitate ventilator weaning and quality of life(438). Likewise, over 10,000 patient-
years of continuous noninvasive ventilatory support has already been reported(9) and no
one has demonstrated greater outcomes or survival by invasive rather than by
noninvasive means for this patient population.
In study nr 2 we report 13 intubated and 7 tracheostomized SCI patients (above C5-C6,
ASIA A and B) completely ventilatory dependent that were all successfully extubated
and decanulated with specific protocols. It is has been described that 74% of ASIA A
SCI patients above the level of C5 required intubation(441) and the overall incidence of
tracheostomy in these cases was between 81 and 83%(442-443). The number of
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 269

respiratory complications during this phase contributes significantly to both hospital
length of stay and costs(444).
Guidelines for respiratory management after SCI were published in 2005 (501),
however these recommendations relied on evidence that did not pertain to the acute
ventilatory impairment of the SCI population. In 2006, Bach challenged the medical
community to decanulate high level SCI patients to NIV to avoid the complications of
tracheostomy, to facilitate training in glossopharyngeal breathing to increase
autonomous breathing ability and security in the event of ventilator failure, and to return
home (502) Study nr 2 is the first to accept this challenge.
In this study, besides successful extubation and decannulation of totally ventilator
dependent patients, after the protocol, only 9 (45%) of the total population used NIV at
discharge and all others weaned to autonomous breathing. The use of high delivered
NIV volumes has been reported to facilitate the weaning process and lessen risk of
respiratory complications(503) as well as result in increased VC and CPF for patients
who are extubated(487) or decanulated(358, 438, 504) and our results are consistent
with those studies. Moreover, it is not expected that continuous NIV can be a successful
alternative to invasive ventilation, if patients use only mask ventilation(492). Further,
for both groups, mouthpiece ventilation normalized speech, provided normal daytime
ventilation, permitted "air stacking" for lung expansion and assisted coughing, and
weaning(87, 438, 487).
Patients with high SCI are expected to be ventilator weaned with supplemental oxygen,
despite some combination of hypercapnia and airway mucus encumbrance. This effec-
tively is the main reason for patients to require reintubation(445) and tracheostomy(442)
that did not occur in any patient extubated in study nr 2. As in study nr 1, aggressive
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
270 Miguel Ramalho do Souto Gonçalves

use of MAC via translaryngeal and tracheostomy tubes was the main intervention that
may have improved pulmonary function (VC and CPF) and normalized SpO2 in
ambient air to satisfy the most important criterion for extubation/decannulation. Our
findings are consistent with those of Bach et al.(358, 505), however our patients were
all successfully extubated despite some having assisted CPF below 160l/min (at
extubation). This was possibly due to the more aggressive use of MAC up to every 15
min to maintain normal SpO2. Pillastrini et al.(506), too reported that mechanical in-
exsufflation aided in clearance of bronchial secretions and increased forced VC, forced
expiratory volume in 1 second, and peak expiratory flows for tracheostomized SCI
subjects. Vital Capacity and CPF also improved in our patients because of lung
expansion and secretions removal.
Decannulation protocols in long term mechanical ventilated patients have been
described in other studies (507-508), however these reports only consider decannulation
when ventilatory weaning was achieved and considered as failures the patients who
could not be weaned from the ventilator, without considering the use of NIV. Therefore
patients from study nr 2 would have been considered “unweanable” under current
recommendations (415, 431).Transition from tracheostomy to continuous NIV was
progressive and implied a specific protocol that included ventilation with a deflated cuff
for increasing periods until it could be tolerated throughout daytime hours and
overnight.
This “open system” ventilation(509) permitted the patients to improve their vocal cord
function that was essential for successful NIV training with a capped cuffless
fenestrated tube. In 2004 we reported that decannulation and conversion to NIV and
MAC can facilitate ventilator weaning of CMV dependent patients(438). It has also
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 271

been reported that decanulated patients invariably prefer NIV over return to
tracheostomy ventilation for safety, convenience, appearance, comfort, facilitating
effect on speech, sleep, and swallowing, and overall(439). Although there are studies
that report successful extubation and decannulation rates with the use of NIV and MAC
in high SCI patients (97, 358), study nr 2 is the first to compare the extubation with the
decannulation outcomes using the same protocol in this patient population.
In this study, both short –term and long term outcomes for the extubated patients were
better than for the decanulated patients. Thus, it appears preferable, in this patient
population, to prevent tracheotomy in the first place, whenever possible, rather than
decanulate later on. Certainly, patients with severe bulbar-innervated muscle
involvement, head injury, chest trauma, medical fragility, complicated courses including
the need for surgical procedures over a greater than 3 or 4 week period are best
managed by tracheotomy.
Data from study nr 2 also show that the extubated SCI patients had significantly shorter
ICU stays, were more quickly extubated than the decanulated patients decanulated, had
higher VC at 48 hours after tube removal, higher unassisted and assisted CPF at 48
hours and at 6 months after tube removal than those decannulated. This can be due to
the fact that extubated patients had significant less time on invasive ventilation with
consequent less respiratory muscle deconditioning, were somehow less severely
affected despite comparable VCs and ASIA levels at extubation, or had less risk of
upper airway instability and less secretion encumbrance or segmental atelectasis despite
the same CPF and normal SpO2. Moreover, the decanulated patients needed MAC to
clear airway secretions for longer periods of time as well as more time for NIV training
and tracheostomy site closure. The higher values of VC at 48 hours after extubation
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
272 Miguel Ramalho do Souto Gonçalves

explains the greater number of extubated patients discharged to the community with no
ventilatory support.
Although tracheostomy may have physiologic benefits over endotracheal tubes in terms
of reduced work of breathing(510)and permitting more efficient suctioning, over 90% of
the time suction catheters enter only the right mainstem bronchus resulting in 80% of
pneumonias occurring on the left lungs of these patients(511) and work of breathing is
readily compensated by providing pressure support during SBTs. There are no reports
of better outcomes with tracheostomy ventilation when compared to the NIV/MAC
protocols.
Improvement in VC, CPF and SpO2 following MAC has been reported (54, 60, 62, 84).
Studies 1 and 2 are consistent with those reports in acute setting with direct impact on
extubation and decannulation outcomes. A controlled study with a crossover design
controlled study would be needed to compare the effectiveness of noninvasive secretion
management (MAC) to invasive airway suctioning, however, due to the significant
efficacy of MAC in severe totally ventilator dependent patients with muscle weakness,
it would not be ethical to include this patient population in such trials.
In critical care, patients' mucociliary elevators are impaired by intubation. Thus, mucus
accumulation can greatly hamper ventilator weaning and the ability to remain extubated
and is one of the main reasons for patients to require reintubation. These effects are
exacerbated by the tendency of intubated patients to develop malnutrition often in part
due to the presence of the tube. Thus, it is not surprising that conventional extubation is
very significantly less often successful by comparison to extubation using respiratory
muscle aids. Early extubation, coupled with the use of noninvasive ventilatory support
has been used effectively in several critical ill populations to facilitate weaning(20, 114,
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 273

155), improve survival(161), decrease the incidence of ventilator-associated
pneumonia(103, 153) and reduce ICU length of stay(153, 161). However there is a
higher risk of NIV failure when applied in patients that develop ARF after extubation
and the evidence that supports its application is conflicting (159-160, 446).
The results found in the trial included in study nr 3 suggest that secretion management
with MI-E may work as an useful complement technique to treat patients who develop
ARF in the first 48 hours post-extubation. The efficacy of MI-E had a stronger impact
in preventing re-intubation in the group of patients that required NIV, justified by the
lower NIV failure rates in the patients that were submitted to MI-E. By contrast,
significant debate still exists concerning the precise indications and efficacy of NIV in
this patient population(512) without any mention to the problem of impaired airway
secretion.
The randomized controlled studies performed by Esteban et al (159). and Keenan et
al(160). concluded that NIV is not efficient in reducing re-intubation rates, duration of
invasive mechanical ventilation and ICU and hospital length of stay. None of these
studies showed improvement in survival in patients that used NIV other than SMT. In
contrary, the trials conducted by Nava et al.(190) and Ferrer et al.(155) found positive
outcomes with NIV in preventing ARF after extubation. Several reasons may explain
these differences. First, whereas the studies by Keenan et al(160) and Esteban et al(159)
applied NIV after patients had developed symptoms of respiratory failure, the studies by
Nava et al(190) and Ferrer et al(155) previously identified the high-risk patients and
applied NIV immediately after extubation. Because longer time from extubation to re-
intubation is associated with worse outcome(32), the delay in re-intubation correlates
with worse survival rates in patients who received NIV for established post-extubation
respiratory failure(159-160). Thus, the early application of NIV seems crucial to avoid
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
274 Miguel Ramalho do Souto Gonçalves
respiratory failure after extubation, and consequently re-intubation. Second, a
significantly higher proportion of patients with chronic respiratory disorders were
included in the studies that used early NIV in high risk patients, whereas the NIV post-
extubation respiratory failure trials enrolled only 10–11% of patients with chronic
pulmonary disease and used different definitions for post-extubation respiratory failure.
In our study, both experimental and control groups included 20% of patients with
chronic respiratory disorders, and all patients were closely monitored during the first 48
hours for early detection of signs and symptoms that indicated post-extubation
respiratory failure. As in the trials by Esteban et al.(159) and Keenan et al.(160) NIV
was only applied after the development of those symptoms according to specific
criteria. However, in our study NIV was applied in both study group patients and
controls and only MI-E application was considered an independent variable.
Secretion encumbrance and impaired airway clearance have been considered an
independent factor for extubation failure(513), and associated to NIV failure both in
persistent weaning(153) and in post-extubation failure(159) patients. While it is
relatively easy managing secretions through an endotracheal tube, it can be a serious
problem after extubation and specially during NIV. Deep airway suction suctioning
through the tube is a strategy most commonly used by nursing staff to manage
secretions while patients are on invasive MV, however it can more traumatic, difficult
to perform and often ineffective in extubated patients since it must be performed blindly
through the nose or the mouth.
It has been reported that conventional chest physical therapy for secretion management
does not increase the chances of weaning and extubation success (357). However,
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 275

critically ill patients may have normal mucociliary clearance but ineffective CPF which
itself has been associated with extubation failure (37, 358).
Study nr 3 randomly used MI-E (CoughAssistTM, Phillips Respironics International
Inc., Murrysville, Pa) pre- extubation via invasive tube and post-extubation through
oronasal interface at sufficient inspiratory and expiratory pressures (minimum of 40 to -
40 cm H2O) to fully expand and then fully empty the adult lungs in 6-8 seconds,
thereby expelling airway secretions while avoiding both hyper and hypoventilation.
The ability to use MI-E through the endotracheal tube immediately before extubation
was the main intervention that permitted the patients from the study group to minimize
the risk of post-extubation secretion encumbrance and, together with its 3 time daily
noninvasively application, may have had influence on the reduction of re-intubation and
NIV failure rates.
Although MI-E has been described as a very efficient technique in the acute setting for
patients with neuromuscular disease (NMD), in the treatment of respiratory failure due
to upper respiratory tract infections(246), to avoid intubation(27) and to facilitate
extubation, decannulation and prevent post-extubation failure(358, 438, 505), the
evidence supporting the role of this technique in this other critical ill patient population
is lacking. Indeed, study nr 3 is the first randomized controlled trial focused on MI-E
in critical care.
The fact that there is strong evidence on the efficacy of MI-E in critical ill patients with
NMD, and the authors´ positive experience with this technique in this patient population
(study nr 3), was the ethical reasons to exclude them from the study nr 3.
Potential limitations have to be taken into account when analyzing the differences
between the two groups. First, although there were no significant differences in baseline
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
276 Miguel Ramalho do Souto Gonçalves

characteristics at the entry of the study between the 2 groups patients from the
conventional extubation group had slightly more hypoxemic respiratory failure which
may have had impact on the NIV failure rate in this patient group, since NIV is more
likely to fail when severe hypoxia is present(156). Second, 6 controls and 4 study group
patients were re-intubated immediately with no indication for NIV. This fact was
associated with causes that could not be solved by MI-E, since cooperation with the
technique is crucial in extubated patients, fact that justified the best outcomes in patients
that required NIV.
Chronic Respiratory Failure
Numerical parameters such as respiratory rate (RR), Rapid Shallow Breathing Index,
maximal inspiratory pressure, and PaCO2 have been offered as indicators for nocturnal
NIV but have been unreliable(514). Although numerous unsubstantiated opinions have
also been given on indications for initiating nocturnal NIV, and current Medicare
guidelines for ventilator use mandate VC less than 50% of predicted normal, no
universally accepted objective parameters have yet been defined(18, 101, 515).
Decisions about ventilator use are largely based on the results of polysomnograms,
pulmonary function testing, and arterial blood gas samples. However, daytime arterial
blood gases may be normal despite symptomatic nocturnal hypoventilation. Indeed,
30% of patients hyperventilate from the pain of arterial puncture(516).
Polysomnograms do not distinguish apneas/hypopneas due to central and obstructive
events from those due to inspiratory muscle weakness(517). Further, conventional
pulmonary function testing is designed for patients with lung and airways diseases
rather than muscle weakness.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 277

Forced VC, flow and diffusion studies evaluated with the patient in the sitting position
reflect lung/airways disease. The VC measured with the patient supine is not part of
routine pulmonary function testing but better reflects diaphragm weakness. In a recent
study, supine VC less than 75% of predicted normal was 100% sensitive and specific
for predicting an abnormally low transdiaphragmatic pressure (Pdi)(518). Indeed,
patients can have VCs approaching normal when sitting but be less than 50% of normal
and have no ability to breathe when supine. The inaccuracy of considering VC alone,
especially in the sitting position, to indicate ventilator use has also been reported by
others(519).
Most often, asymptomatic patients with NMD are offered nocturnal continuous PAP or
low-span bi-level PAP on the basis of routine polysomnograms. This approach is valid
for treating central or obstructive apneas but not severe inspiratory muscle weakness
and hypoventilation for which high ventilator volumes and pressures are needed for
ventilatory support and muscle rest(10). The failure of skeletal muscle to continue to
generate a given tension is defined as muscle fatigue. When a patient is not able to
sustain the muscular work of breathing in the presence of increasing ventilatory load or
decreasing work capacity, muscle fatigue can occur and ventilatory assistance become
necessary. Bellemare and Grassino quantitated inspiratory muscle fatigue by measuring
the time elapsed between the onset of diaphragm contraction and the point at which a
target tension can no longer be sustained (Tlim)(456). In the case of the diaphragm,
there are two main factors influencing muscle fatigue or Tlim. The first is the Ti/Ttot or
duty cycle of the diaphragm. Since the diaphragm contracts mainly during inspiration,
it should fatigue more rapidly at any given tension if Ti/Ttot is abnormally increased.
The second is Pdi/PdiMax or the mean trans-diaphragmatic pressure swing developed
with each inspiration. The diaphragm should fatigue more rapidly at any given Ti/Ttot,
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
278 Miguel Ramalho do Souto Gonçalves

if the Pdi/PdiMax is greater than normal. They reported the relationship between Tlim
and TTIdi, that is, (Ti/Ttot) x (Pdi/PdiMax), and determined that Tlim = 0.1(TTIdi).
Thus, diaphragm endurance time could be predicted by the TTIdi. Determining TTIdi
requires placement of an esophageal balloon to measure Pdi and PdiMax. This makes it
impractical for general use. It has already demonstrated that Vt/VC can substitute for
Pdi/PdiMax because the more Vt approaches VC, the less the ability of inspiratory
muscles to sustain alveolar ventilation(520). Our data suggest that the VRI using
Vt/VC can supplement VC to help gauge the need for ventilator use by reflecting
ventilatory reserve.
In a previous study, Koga et al. described a breathing intolerance index (Ti/Ttot x
Vt/VC) in patients with lung/chest wall disease including 11 who were nocturnal-only
ventilator users, and in healthy subjects, and observed that it could be useful for
justifying ventilator use (520). In study nr 4 we proposed a Ventilator Requirment
Index (VRI) were we multiplied the Ti/Ttot x Vt/VC x respiratory rate (RR), to
determine whether this index could distinguish patients with NMDs with various levels
of inspiratory muscle dysfunction and need for ventilator use
An accurate index of extent of ventilator need can be important to justify the
prescription of one, two, or no ventilators. Patients with symptomatic hypoventilation
on the basis of inspiratory muscle dysfunction benefit from ventilator use at least during
sleep(89). These patients can use either pressure-cycled (BiPAPTM) or volume-cycled
machines. Likewise, two ventilators are required when a patient is continuously
ventilator dependent. Considering our data, anyone with NMD who appears to be
symptomatic for alveolar hypoventilation or who has a VC less than 50% or VRI
greater than 1.2 should have a trial of nocturnal NIV for symptomatic relief. Even 8 of
18 patients without obvious symptoms but with VC less than 50% or VRI greater than
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 279

1.2 felt sufficient benefit to go on using nocturnal NIV once introduced to it. Thus,
documentation of a VRI greater than 1.2 or a VC less than 50% is justification for the
prescription of a trial of part-time ventilator use. Once a patient requires ventilator use
greater than 20 hours day, a second ventilator should be prescribed provided that the VC
is less than 1000 ml or the VRI is greater than 2.5.
Maximum inspiratory pressures and maximum expiratory pressures are direct measures
of inspiratory and expiratory muscle strength. For patients with primarily ventilatory
impairment expiratory muscles are usually weaker than inspiratory muscles(521).
Expiratory muscle weakness not only decreases peak expiratory flows but it decreases
CPF(461). Routine pulmonary function testing includes the measurement of maximum
expiratory pressures and peak expiratory flow rates but not CPF(495, 522).
Cough peak flows are generally between 40 and 50% greater than peak expiratory flows
in normals as well as in patients with DMD(464). In severe bulbar ALS patients,
however, they may not be measurable because of inability to close the glottis(461).
Despite their importance, CPF have not yet been standardized.
Besides inspiratory and expiratory muscle weakness, CPF are also decreased by bulbar
muscle dysfunction that impairs glottic retention of an optimal breath, that impairs
glottic patency, vocal cord movement, and pharyngeal dilator function, and that leads to
aspiration of food or saliva. CPF are the best indication of the functional integrity of
bulbar musculature. They are also decreased by upper or lower airway obstruction,
anatomical or functional.
In study nr 5 we found that “dart flows” (DF) are significantly greater than CPF which
are, in turn, significantly greater than PEF for normals as well as for this group of
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
280 Miguel Ramalho do Souto Gonçalves

patients with NMD. The fact that CPF are normally greater than PEF in healthy people
as well as for patients with Duchenne muscular dystrophy has already been
reported(464). These three flow maneuvers are similar in that they are expiratory flows
measured at the mouth using a peak flow meter. However, each method of flow
generation requires different respiratory muscle groups.
With glottic closure, the greater transpulmonary pressures created by coughing
rather than by PEF maneuvers resulted in flows measured at the mouth being greater for
the former except for 12.8% of patients. However, cough efficacy is dependent on the
peak flow velocity which is greater as airways narrow during coughing, making
coughing more effective at expulsing airway secretions than huffing even though PEF
and CPF may be comparable when measured at the mouth(54). The reduction of the
cross sectional area of the airways during coughing is due to smooth muscle constriction
mediated by a vagal reflex (presumably preserved in these diseases), and due to
dynamic compression of the airways generated by the expiratory (transpulmonary)
pressure(523).The reduction in the cross sectional area of the airways increases fivefold
the velocity of gas and 25 fold the kinetic energy of the airstream. This explains why
the subgroup of 16 patients (12.8%) with CPF lower than PEF coughed rather than
huffed to expel secretions. Effective CPF and PEF share the need for deep lung
volumes, explaining their good correlation with VC and MIC.
The correlation of CPF with MIC or MIC, VC difference is explained by their
dependence on bulbar-innervated muscle (glottic) function. Whereas diminished CPF
and MIC-VC difference can be due to laryngeal dysfunction and are associated with
elevated risk of respiratory complications, DF usually exceed CPF and PEF. However,
DF are measured at the mouth but do not emanate from the airways and require little or
no inspiratory or expiratory muscle effort. DF, while also dependent on bulbar-
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 281

innervated muscles but not glottic function, do not appear to reflect risk of respiratory
complications. Inability to create measurable DF, however, is associated with
ineffective saliva control and drooling. These flows can also be confused with CPF if
the clinician is not careful to listen for glottic closure during CPF measurements. For
nine patients, seven with motor neuron disease, maximum DF were less than CPF.
Thus, different patterns of bulbar-innervated muscle dysfunction occur. In this way, DF
are similar to PEF since Wohlgemuth et al.(524) and Holcroft et al.(525) have pointed
out the need to caution their subjects from spitting during the measurement of PEF.
Although all of the flow maneuvers are dependent on effort and motivation, we
don’t think this was a confounding factor in our study since the three measures were
obtained in the same visit, in varying order, by the same examiner, and only the
maximum value of many attempts was recorded.
The techniques are simple and the peak flow meter required for measuring CPF and
PEF is very inexpensive and more widely available than spirometers required for
measuring VC and MIC. Assessment of both assisted and unassisted CPF is a
convenient method to objectify bulbar-innervated muscle function and respiratory
risk(364). A larger study is warranted to determine standard values of CPF and DF by
age, height, and weight. Peak flow meters with greater range should be developed to
more accurately measure the high range flows(526).
Like limb articulations and other soft tissues, the lungs and chest wall, too, require
regular motion to prevent chest wall contractures and lung restriction. As has been
recognized since at least 1952, this can only be achieved by air stacking, by providing
deep insufflations (via the upper airway or by "sighs" for patients using invasive
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
282 Miguel Ramalho do Souto Gonçalves

mechanical ventilation), or by nocturnal noninvasive ventilation for patients who cannot
cooperate with air stacking or insufflation therapy (83).
Kang and Bach also proved that the CPF value could be even higher if it is performed
through the Maximum Insufflation Capacity (MIC). The MIC is related to the
pulmonary compliance and with the pharyngeal and oropharingeal muscles function
(362). For most patients with NMD, while the VC decreases with time the MIC
increases for years before, however in ALS patients with bulbar impairment the
decrease of VC is proportional to the decrease of MIC (527)
The goal of conventional prescriptions for “range-of-motion” mobilization of extremity
articulations is to slow the development of musculoskeletal contractures for patients
with limb muscle weakness. However, the prevention of chest wall contractures and
lung restriction has only recently been addressed. In 2006, Lechtzin et al.(528) reported
the use of short-term noninvasive intermittent positive pressure ventilation (IPPV) to
increase pulmonary compliance for patients with amyotrophic lateral sclerosis (ALS).
Kang et al. demonstrated that lung volumes could be increased significantly over VC by
air stacking to approach MIC for patients with NMD. This resulted in significantly
increased (assisted) CPF that can decrease the risk of pneumonia. For patients such as
those with advanced bulbar ALS whose MIC equals VC, assisted CPF cannot be
increased by air stacking, and prognosis is poor(10).
Study nr 6 describes a simple technique that bypasses glottic function for providing
deep lung insufflations and for quantitating them as Lung Insufflation Capacity (LIC).
Patients with NMD often lose VC to the extent that they can expand their lungs to only
a small fraction of predicted volumes. For example, DMD patients’ VC decrease to
approximately 10% of predicted normal by age 20(529) and typical SMA type 1
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 283

patients’ VC have been reported to never exceed 250 ml(530), which, by age 10,
amounts to less than 10% of the predicted normal value(531). Incentive spirometry is,
therefore, useless because such patients’ tidal volumes approach their deepest breaths,
and these cannot exceed a small percentage of their insufflation capacity (IC). Likewise,
in reviews of studies in which inspiratory resistive exercise was performed by NMD
patients, no effect on VC, lung volumes, or maximum inspiratory or expiratory
pressures was reported(532). On the other hand, expanding the lungs well beyond IC by
air stacking or by single, deep insufflations permits greater lung distension, voice
volume, and CPF and can decrease atelectasis and loss of pulmonary compliance(364).
Our results show that the benefits can be greatest for the most advanced patients with
the lowest VC. The fact that lung expansion to LIC -VC trends inversely with VC,
whereas MIC -VC does not, indicates that, for the most advanced patients, it is
increasingly important to expand the lungs by passive insufflation rather than by air
stacking. In addition, MIC and LIC can increase with practice.
Inability to air stack no longer means that patients cannot simply and inexpensively
expand their lungs beyond IC. Study nr 6 demonstrates that like LIC-MIC, too, is an
objective, quantifiable, reproducible measure that (inversely) correlates with glottic
integrity. Glottic function is the most important aspect of bulbar-innervated muscle
function for NMD patients (364, 461)because it is most important for airway protection
and cough effectiveness and, therefore, permits the use of NIV to avoid otherwise
inevitable respiratory failure leading to death or tracheostomy with decreased quality of
life(63).
In this study, some patients were hypercapnic on presentation and had lungs stiff to the
extent that using a manual resuscitator to increase tidal volumes to normalize CO2
failed to do so and resulted in high airway pressures and chest discomfort. With regular
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
284 Miguel Ramalho do Souto Gonçalves
lung mobilization therapy and nocturnal NIV, however, five such patients became able
to renormalize CO2 when breathing autonomously without chest discomfort. This is
consistent with previous studies in which passive lung insufflation volumes were greatly
diminished for patients who were ventilated at constant pressures/volumes without
regular deep insufflations (468, 528). Patients supported by NIV at large delivered
volumes (1100–1500 ml) physiologically vary tidal volumes, can air stack to deep lung
volumes as a function of their bulbar innervated muscle integrity, and can better retain
lung distensibility(9). Thus, if pressure-cycled ventilators such as bi-level units (with
which air stacking is impossible) are used for nocturnal NIV, patients with diminished
VC should be equipped with a manual resuscitator or a volume cycled ventilator for air
stacking/maximal insufflations.
Home mechanical ventilation
Although only about 31% of ventilator users in acute hospitals have neuromuscular
ventilatory failure by comparison to 60% with cardiopulmonary disorders, because
neuromuscular ventilator users have a better prognosis and tend to use ventilators much
longer, they constitute over 50% of home mechanical ventilator users in the United
States(474)The population of home mechanical ventilator users has, in fact, more than
doubled since 1987(248) in Europe.
The vital use of manually assisted coughing was reported in only 18%, and MI-E in
only 5% of the clinics that prescribe respiratory care for patients with NMD(377).
Thus, failure to provide effective nocturnal ventilatory support, mouthpiece IPPV, and
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 285

assisted coughing continue to make respiratory failure inevitable for the great majority
of people with NMD.
Approaches to preventing peripheral airway secretion retention at home for patients
with NMD include the use of medications to reduce mucus hypersecretion or to liquefy
secretions, and facilitation of mucus mobilization. The latter can include manual or
mechanical chest percussion or vibration, direct oscillation of the air column, and
postural drainage. The goal is to transport mucus from the peripheral to the central
airways from where it can more easily be eliminated by manual assisted coughing and
mechanical assisted cough (MAC).
Home ventilated patients with NMD, however, do not have adequate inspiratory
and expiratory strength for sufficient cough flows. Thus, instead of overemphasizing
the effort-intensive use of secretion drainage techniques, these patients mostly need to
learn how to normalize their cough flows by using inspiratory and expiratory muscle
aids. Moreover, chest clapping also causes hypoxia so at times supplemental oxygen
needs to be administered(533).
Study nr 7 describes the indications of home MAC and its safety and compliance in
NMD patients. Oximetry feedback has proven usefulness by allowing to detect a sudden
decrease in SpO2 resulting from mucus plug (127, 481) Patients referred in this study
presented severe ventilatory failure and were on continuous mechanical ventilation
through noninvasive interfaces or tracheostomy.
The main condition for an efficacious home care after hospital discharge was the
presence of an adequate and motivated caregiver. In this study home basis MI-E was
centred in non-professional caregivers, with the support of a trained health care
professional in a home on-call regime. Moreover, it describes the importance of an
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
286 Miguel Ramalho do Souto Gonçalves

educational phase, introduced early to both patients and caregivers in the hospital, as
also proposed by Tzeng et al(127). Therefore, study nr 7 confirms that the caregiver,
when trained and motivated, can successfully use MI-E at home, and detect early signs
and symptoms of possible clinical respiratory worsening.
According to the methods applied in studies 5 and 6 of this thesis, bulbar muscle
function was evaluated, because severe bulbar dysfunction is responsible for
malfunction of the upper airway muscles, creating a dynamic collapse during the
exsufflation phase of MI-E, making this technique ineffective in this group of
patients(10, 60, 396). In this study ALS, which is the most common diagnosis,
represents a heterogeneous group: from non-bulbar with inadequate CPF to severe
bulbar requiring tracheostomy. The need of tracheostomy represents itself an extra
problem either concerning to its acceptance by the patients or associated to
tracheostomy related problems (local inflammation, increased secretions and
infections)(534-537).
Moreover, even though tracheostomy was proposed to all our severe bulbar patients,
some still rejected tracheostomy and preferred to continue with NIV and MAC protocol
at home. Bach et al have also reported that even severe bulbar ALS patients, can be
supported by combined used of VNI and MAC, delaying tracheostomy as long as the
SpO2 can be maintained above 95% in room air(481). However, these patients require a
close periodic monitoring in order to anticipate failure of non-invasive approach, so that
therapeutic options can be explored and discussed with patients and family, with the
intention that decisions can be made in advance rather than at the time of a respiratory
crisis(538).
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 287

In this study nr 7 each home MAC session consisted on 6 to 8 MI-E cycles at mean
pressures of 40 to -40 cmH2O, titrated according to patients’ tolerance. Chatwin et
al.(56) and Sivasothy et al.(539) have considered lower pressures to be more
comfortable and safe. However our settings are widely preferred for both comfort and
effectiveness and were also similar to those suggested by physiological studies.(57, 62,
365). Moreover, we had special attention on a careful individualized MI-E pressure
titration, trying to achieve maximal chest expansion, respecting comfort, which may
justify the tolerance and absence of complications.
According to patients and their caregivers there were few episodes in which home MAC
was not sufficient to deal with secretions encumbrance and emergency department visits
or hospitalizations were necessary. Other studies have already reported that NMD
patients dependent on NIV and using MAC guided by oximetry feed-back may be
safely managed at home without hospitalizations (10, 63, 127, 470).
We observed in study nr 7 that patients use home MAC according to their needs and
following oximetry feedback that consisted on using an oximeter for to maintain SpO2
greater than 94% by maintaining effective alveolar ventilation and airway secretion
elimination. Some patients used it daily and others intermittently during RTIs. This
study also showed that all patients with tracheostomy used MAC daily and more times a
day than patients under NIV, which used it more intermittently during RTIs. This fact
may be justified to local inflammation and increased secretions related to tracheostomy.
Study nr 7 showed that compliance of home MAC is different among NMD patients
and the organization of home care MAC programs in this population with severe
ventilatory impairment requires more study. Study nr 8 questioned that, although MAC
can be effective when continuously available at home (63, 127), expense can be
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
288 Miguel Ramalho do Souto Gonçalves

mitigated by on-demand rather than continuous access if on-demand MAC use can be
demonstrated to be effective. This study demonstrated that, for patients with ALS, a
program of telephone access, educational intervention, and on-demand home assisted
coughing interventions was shown to be feasible, very well accepted and resulted in
significant cost savings.
Although there are a number of studies that describe the efficacy of manual and
mechanical cough assistance techniques in hospital acute situations, until now there have
been no studies that focus directly on the feasibility and management of cough
assistance techniques at home for ALS patients. Only one previous ALS study used
continuous videoconferencing and telephone consultation for only four ALS patients. It
was also limited by the patients’ inability to master the use of the Internet and
Webcams(540).
Severe bulbar patients and moderate bulbar patients without tracheotomy had a poor
prognosis and high risk of death as previously noted(396). As in study nr 7, these
results also confirm that clinical worsening related to secretion encumbrance can be
detected by oximetry and SpO2 baseline normalized by MAC in the home setting for
ALS patients(481).
Study nr 8 also confirmed that respiratory care of advanced ALS is only effective if
families and care providers assist with oximetry and assisted coughing. Thus, a
motivated caregiver can successfully use at home cough assistance to prevent lung
pathology and hospitalizations. The higher number of avoided hospitalizations in the
patients with clinical worsening, that activated home MAC may suggest that this
approach can reduce and/or prevent respiratory infections with consequent reduction in
number of hospitalizations in ALS patients.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 289

When home visits are performed by a health care professional, the “on request” use and
rental of MI-E devices prescribed by a multidisciplinary team of experts, can offer a
clinical service together with a significant financial saving compared with continuous
care strategy prescription (to all ALS patients for all the days) of home cough assist
devices. This choice, up to now, is particularly costly and has not been demonstrated to
be the best approach to achieve a good cost/benefit. Oximetry monitoring with on-
demand professional attention and MAC is a cost-saving alternative that is not only
relevant for the European health care system but also for the American system where the
continuous prescription of MI-E is widely used even though most patients do not need
assisted coughing every day. Indeed, study nr 8 showed that 56% of the patients did
not need to use MAC and those who used it, did so for <20% of the total follow-up
period. Moreover we also confirmed in study nr 8, that ALS patients under
tracheostomy have more necessity to use MAC, justified by the higher number of
episodes of clinical worsening compared to the patients under NIV. We found also in
study nr 8, that this on-demand program adds considerably to the patients’ and
clinicians’ feelings of security in managing such patients at home with concomitant
positive outcomes and reduced costs.
After confirming in studies 7 and 8, the feasibility, patients´ compliance and better
organization of efficient home MAC access, in study nr 9, we reported data that
focused on the clinical effects of home MAC during acute episodes of secretion
encumbrance in ALS and other NMD patients, all totally ventilator dependent either
through NIV or by tracheostomy.
The results of study nr 8 confirm that hospitalizations for ARF can be avoided for
NMD patients by a protocol of oximetry feedback for using ventilatory support and
MAC in the home (10, 63, 127, 481). Moreover these findings support again the clinical
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
290 Miguel Ramalho do Souto Gonçalves

justification for availability and prescription of cough assist devices and portable
oximeters at home for this patient population, especially during intercurrent RTI´s.
Since all patients were continuously ventilator dependent during the episodes, had the
oxyhemoglobin desaturations and dyspnea not been reversed by MAC, they would have
had to have been hospitalized for problems related to upper respiratory tract infections
and inability to clear secretions. However, in study nr 9, as a result of the protocol,
81% of the acute episodes resolved without hospitalization.
These results are consistent with those reported by Gomes-Merino et al (63) that, with a
similar approach, described hospitalization avoidance and survival increase in a
population with Duchenne muscular dystrophy under NIV. Study nr 9 focused on other
NMD diagnoses including having 71% ALS patients. Moreover, we found that, while
the incidence of acute episodes was the same, the tracheostomy users had significantly
more hospitalizations per desaturation episode than NIV users. This may be due
specifically to complications caused by the invasive tubes (534, 537, 541) and unrelated
to MAC or by poorer bulbar-innervated muscle function and airway protection
mechanisms in the ALS population despite tracheostomy with cuff inflation(396, 542)
In our study, MAC not only significantly improved SpO2 in all patients, it also
significantly decreased the number of airway suctionings in the tracheostomy patients.
All tracheostomy patients in this study had severe bulbar muscle impairment and the fact
that only 3 NIV users had bulbar impairment, may justify the good results of MAC on
reversion of desaturations at home.
Our results in study nr 9 implied that the patient and caregiver training and home
equipping be done early, before acute respiratory failure (ARF) occurs, and in the
outpatient setting as reported by Tzeng et al (127). Our results confirm that the
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 291
caregiver can successfully use MAC at home cough with oximetry feedback and can
early detect possible acute episodes of secretion encumbrance.
According to the results of studies 7, 8 and 9, nasotracheal deep airway suctioning
should be the last resort considered for both NIV and tracheostomized NMD patients
with upper or lower airway secretion encumbrance. Even though indications for airway
suctioning have not been determined, patients with tracheostomy tubes are routinely
suctioned an average of 8 times a day and 30 or more times per day when they have
chest infections(47). At best, suctioning can clear only superficial airway secretions.
Suctioning misses mucus adherent between the tube and the tracheal wall and the left
main stem bronchus 54 to 92% of the time that can lead to a high incidence of left lung
pneumonias, potentially fatal mucus plugging, and perceived need for
bronchoscopies(511). Results from a survey indicate that 42% of institutions prescribed
cough assistance devices for outpatient use(543) in tracheostomized patients. Moreover
Garstang et al(399) reported that patients have a significant preference of mechanical
insufflation-exsufflation (MI-E) through the tube over deep suctioning as a mean of
removing secretions.
As a conclusion, to support the evidence of this line of research in the clinical practice,
study nr 10 analysed the historical evolution of practice regarding the use of
noninvasive mechanical ventilation (NIV) and complementary interventions for long-
term full-time noninvasive ventilatory support of patients with NMD and reported data
from different international centers that provide continuous NIV for this patient
population as an alternative to tracheostomy.
It has already been described that 55 to 90% of conventionally managed DMD patients
die from pulmonary cardio-complications between 16.2 and 19 years of age and
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
292 Miguel Ramalho do Souto Gonçalves

uncommonly after age 25(544). Studies have reported outcomes of tracheostomy IPPV
for patients who undergo prophylactic tracheostomy or who survive an initial episode of
respiratory failure and who subsequently undergo tracheostomy. Baydur et al.(545)
reported 7 DMD patients who received full-time tracheostomy, from the mean age of
22.3 to 28.5 years. Two of the 7 died from pneumonia and 5 of the 7 patients were
reported as having had pneumonia or recurrent pneumonias. Soudon et al.(546) reported
a 3.6 year mean survival for 23 tracheostomy IPPV users, most of whom had DMD.
Eagle et al. reported survival of 200 DMD patients as 19.5 years for those untreated and
24.8 years for those receiving tracheostomy IPPV(544).
In 80% of the NMD clinics in the U.S, patients are being offered nocturnal-only “low
span” NIV on the basis of polysomnograms(377). Many of these patients are found to
have nocturnal desaturations and frequent hypopneas. The hypopneas tend to be
associated with reduced chest wall movement or with chest wall paradox suggesting
non-central origin, that is, inspiratory muscle weakness(547-548). In DMD patients, the
use of “low span” NIV has been shown to prolong tracheostomy-free survival by a
matter of months-only with respiratory failure ultimately inevitable(549-551). Simonds
et al.(17) began it for 23 DMD patients with a one year survival of 85%, 2 year survival
of 73%; and a 5 year survival was less than 40% with at least 5 deaths due to respiratory
failure. As the VC decreases below 800 ml DMD patients often begin to rock back and
forth in their wheelchair to compress their abdomens during exhalation to increase their
tidal volumes. They also tend to develop hypercapnia during sleep at this point. They
eventually begin to use accessory breathing muscles and usually remain grossly
asymptomatic, though, until their VCs decrease below 450 ml and hypercapnia extends
into daytime hours. (552). This first occurs during sleep and eventually with the patient
awake. It is usually around this time that nocturnal NIV is indicated (553).
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 293

SMA type I is typically characterized by profound global weakness were early
respiratory failure is the major cause of morbidity and mortality and most children do
not survive beyond 2 years of age without specialised treatment(530). Oskoui et al.(554)
showed that survival of children with SMA type I from the international SMA register
born in 1995–2006 has increased compared with those born in 1980 –1994. They
concluded that this was due to more patients receiving ventilation (82% vs. 31%), MI-E
(63% vs. 8%) and supplementary feeding (78% vs. 40%).
There has been consensus and international statement on the standards of care in SMA
with specific reference to the management of infants in the with SMA type I(555-556).
These documents do not address care of infants with non severe SMA type 1. These
statements tend to ignore that clearly, as for patients with other NMDs, the survival of
many SMA type 1 patients with or without severe bulbar muscle involvement can be
prolonged by ventilatory support both by NIV or via indwelling tracheostomy tubes, as
long as respiratory muscle aids are provided.
Pulmonary complications and respiratory failure account for at least 84% of ALS
mortality(557). and death can occasionally occur in as little as 2 months from onset of
symptoms and can occur at the time of initial presentation to a physician(396).
In the U.S. less than 10% of ALS patients undergo tracheotomy(558). However, 80 to
97% of ALS tracheostomy continuous ventilator users are glad to have chosen
mechanical ventilation, are satisfied with their lives, and would use mechanical
ventilation over again if they had to(10, 559). Thus, tracheostomy can at times prolong
survival by 10 years or more. However, deterioration in physical functioning and in the
ability to communicate, limited family resources, and most importantly, lack of a
national personal attendant care policy, often make it difficult for ALS patients to be
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
294 Miguel Ramalho do Souto Gonçalves

managed in the community(538). In addition, as well as from airway mucus plugging,
much of the sudden death post-tracheotomy may be due to autonomic dysfunction(560).
From 20 centers in 17 countries, study nr 10 keyed on analyzing 1623 nocturnal only
ventilated NMD patients in which 760 (48%) progressed to continuous full-setting NIV
over a follow up of 15 years. A protocol of oximetry feedback using mechanically
assisted coughing (MAC) and full-setting NIV permitted 228 safe extubations and 35
decannulations of patients who could not pass spontaneous breathing trials (SBTs)
before or after extubation/decannulation. After the follow up period, 522 (69%) patients
are still alive on continuous full-setting NIV and tracheostomy was placed in a total of
140 (8%). This study focused only in patients with DMD, ALS and SMA type 1,
however, all of the centers reporting data in this study had long-term full-time NIV
users with other diagnoses but it was felt that limiting the data to these common and
severe conditions would be more practical and establish the point.
Mechanisms by which nasal or mouthpiece IPPV can improve the clinical picture
include: resting respiratory muscles and decreasing metabolic demand, increasing tidal
volumes and relieving hypercapnia, resetting chemoreceptors, opening atelectatic areas,
maintaining airway patency, improving ventilation/perfusion matching, maintaining
lung and chest wall range-of-motion and possibly compliance, improving mucociliary
clearance, and most importantly, by assisting, supporting, and substituting for
inspiratory muscle function. Although mouthpiece IPPV is being used for ventilatory
support since 1953 (42) very few studies reported its use for long-term management(1,
87, 90, 491-492).
Nocturnal-only nasal NIV or bi-level PAP can at best marginally prolong life and delay
ARF. It can possibly do so by providing moderately deeper lung volumes to assist in
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 295

coughing. With advancing weakness, full-setting NIV can eventually be needed
continuously without requiring intubation and hospitalization, thereby avoiding ARF
and ultimately pressure by physicians to recommend tracheotomy.
The data presented suggest that reported “NIV failure”(15, 561-562) in cooperative
NMD patients can result from inadequate NIV interfaces, from inadequate ventilator
settings, when MAC is not used, and when mouth piece IPPV is not used for air
stacking or daytime support.
Patients usually require daytime mouthpiece IPPV with the ventilator on the back of the
wheelchair and the mouth piece adjacent to the mouth once the VC is less than 350
ml(491). About 15% of patients eventually lose the ability to use mouthpiece IPPV
because of oro-motor weakness(44, 87). These patients typically prefer to use nasal
IPPV around-the-clock rather than undergo tracheotomy(563).
Other than for severely mentally retarded patients no center included in study nr has
encountered a DMD patient who could “not successfully use NIV.” Thus, while the
NIV recommendations from a recent consensus panel(529) are comprehensive up to the
point of requiring intubation, we suggest that with the ability to consistently extubate
continuously ventilator dependent DMD patients and others, resort to tracheotomy
should be much less common.
For SMA 1 it is as yet unclear whether all will some day require tracheostomy tubes for
survival. Thus far, survival has been extended to up to age 17 using full-time NIV for
16 years or more for children continuously NIV dependent since as young as 4 months
of age. According to study nr 10, one center reported 5 of such severely affected SMA
1 patients over age 15, all with VCs less than 20 ml, and none with baseline SpO2 less
than 95% because of saliva aspiration. Thus, it is likely that at least some of these
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
296 Miguel Ramalho do Souto Gonçalves

typically severe SMA1 patients will survive into adulthood without tracheostomy tubes
despite continuous ventilatory support since infancy.
Over a 6-year period, numerous papers published on the futility of managing ALS and
other NMD patients with palliative care without once referring to prolonging life by
NIV/MAC(166, 564-570). Palliative care can be defined as interventions for easing
pain, dyspnea, and other symptoms that accompany the dying process of patients with
terminal illnesses. However, publications fail to distinguish between “palliative care”
for terminal cancer and organ supporting interventions for neuromuscular diseases,
many of which cause end-organ failure of only one system, the neuromuscular system
and in particular, end-stage respiratory muscle failure(571).
The data from this thesis suggest the inappropriateness of using palliative care precepts
for properly equipped and trained patients with adequate personal care support. Some of
our NMD patients, for example, are over age 40 and/or have depended on continuous
NIV for over 20 years and numerous patients becoming continuously ventilator
dependent without hospitalization or intubation, demonstrates that death from end-organ
respiratory muscle failure is often avoidable without resort to invasive measures.
The pervading NMD respiratory paradigm is that diminishing VC bodes poorly for
prognosis. The use of NIV and MAC as described in this thesis, to prolong life by
continuous ventilatory support is contrary to current emphasis on invasive interventions
and high technology. Thus it is considered that tracheotomy is the only option for
prolonging survival and a crisis decision must eventually be made to "go on a respirator
(undergo tracheostomy) for the rest of your life" or die(572). This often leaves patients
and families feeling hopeless and depressed. Thus, conventional management strategies
are invasive and reactive rather than noninvasive and proactive, ignoring the problem
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 297

until ARF results in intubation or death. Since NMDs are considered to be terminal,
clinicians tend to do not prevent ARF or need for invasive airway tubes(166)
It was unanimously agreed upon by the centers involved in study nr 10 that no properly
equipped and trained NIV patients that do not meet our reported criteria for tracheotomy
has ever chosen to electively undergo tracheotomy or stop NIV/MAC and die. Thus, it
was unanimously felt that the use of the term “palliative respiratory care” for NMD
patients perpetrates the misconception that “noninvasive ventilation” is only useful for
symptom relief rather than to prolong life by continuous ventlatory support.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
298 Miguel Ramalho do Souto Gonçalves

CONCLUSIONS
- Intubated patients with NMD unable to pass spontaneous breathing trials achieve
successful extubation by using full NIV and MAC. Our extubation success rates
for these patients, suggest the avoidance of tracheotomy for ventilator dependent
NMD disease patients who have some residual bulbar-innervated muscle
function and who satisfy our extubation criteria. This ca now be offered even to
those with CPF less than 160 L/m.
- Considering the incidence of mortality and respiratory morbidity in the
population of high SCI patients managed by standard ventilatory invasive
techniques, we suggest that noninvasive methods of assisted ventilation and
coughing may facilitate both extubation and decannulation with significant
improvement on ventilatory dependence and pulmonary function and may
facilitate return home rather than prolonged institutionalization for weaning
attempts. Although some authors suggest a benefit on performing early
tracheostomy, we would like to suggest that for cooperative high level SCI
patients, an extubation protocol including full time NIV and MAC, can produce
better outcomes and avoid the necessity of tracheostomy.
- Our results recommend that MI-E devices for secretion clearance should be
included in an extubation protocol in specific subgroups of patients that may
require post-extubation NIV.
- The VRI as a simple, noninvasive index can be used as a complement and/or
alternative to VC in the evaluation of ventilatory impairment requiring
ventilatory assistance in NMD patients. Further validation of this index in other
populations and in the acute care setting as a weaning parameter is warranted.
- Cough Peak flows, PEF, and DF are useful measures of bulbar-innervated and
respiratory muscle function for patients with NMD, permitting greater
knowledge of the pattern of respiratory muscle compromise. It is important to
pay special attention to the technique of each flow measurement since DF can be
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 299

mistaken for CPF or PEF and respiratory risk can be underestimated. Effective
interventions to assist inspiratory and expiratory muscle function and the
accurate characterization of risk of respiratory complications depend on accurate
assessment of expiratory flow maneuvers.
- Regular lung insufflation, either by air stacking (to approach MIC) or by passive
lung insufflation (to approach LIC), is indicated for all NMD patients with
diminishing VC. Because the goal is to approach the predicted IC, passive
insufflation is used when the patient obtains a deeper volume in this manner than
by air stacking (i.e.when bulbar musculature is very weak).
- It is possible to manage severe NMD patients with inadequate airway clearance
on a home-based MAC regimen centred on trained non-professional caregivers.
This is valid for patients under NIV and for those requiring tracheostomy. MAC
should be considered as a useful complement to ventilatory support in these
patients at home.
- A telephone access and on-demand MAC program offers a technologic update to
increase both the patients’ and clinicians’ feelings of security for home
management and was effective in averting hospitalizations for patients with
ALS, with concomitant positive results in reducing home care costs.
- Home MAC use with oximetry feedback during respiratory infections can avoid
hospitalizations and effectively manage episodes of acute respiratory
decompensation, related to secretion encumbrance, in continuously ventilator
dependent NMD patients dependent on either NIV or tracheostomy.
- Since neither DMD, SMA, nor essentially any other NMD full time NIV users
appear to meet the same criteria established to indicate tracheotomy for patients
with advanced bulbar-ALS, these patients can be safely maintained using up to
continuous NIV with good survival outcomes. Assisted lung ventilation and
normal SpO2 can be maintained indefinitely during sleep as well as during
daytime hours for patients with little or no VC by using NIV at full ventilatory
support.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
300 Miguel Ramalho do Souto Gonçalves

RESUMO
Introdução
Um dos desenvolvimentos mais importantes na área da ventilação mecânica ao longo
dos últimos 15 anos foi o surgimento da ventilação não-invasiva (VNI) como uma
técnica crescente do arsenal terapêutico em cuidados intensivos. Além disso, tem sido
utilizada como terapêutica domiciliária em pacientes com insuficiência respiratória
crónica, de diferentes etiologias. De facto, a população sob ventilação mais do que
duplicou desde 1987.
Os argumentos para o uso da VNI dizem respeito principalmente às suas vantagens
sobre a ventilação mecânica invasiva, com redução significativa das complicações
relacionadas com cuidados intensivos, tais como trauma da via aérea superior,
pneumonia associada a ventilação mecânica e elevado nível de sedação. Para os
pacientes sob ventilação mecânica domiciliária a VNI tem vantagens sobre a ventilação
por traqueostomia, nomeadamente uma maior facilidade de adaptação do paciente e
cuidadores maior conforto menor com redução de custos.
Para pacientes totalmente dependentes do ventilador, com fraqueza muscular, a eficácia
da tosse está normalmente comprometida e a acumulação de secreções é frequente. O
manejo adequado de secreções com técnicas manuais ou mecânicas de tosse assistida
deve ser considerado antes do falhanço da VNI ser declarado.
São necessárias mais linhas de investigação com foco numa estratégia continuada de
cuidados respiratórios que incluem VNI optimizada e continua associada a tosse
assistida mecanicamente (TAM) em pacientes com fraqueza muscular e grave limitação
ventilatória, para justificar a aplicação de protocolos específicos que poderão melhorar a
sobrevida desta população
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 301

Objectivos
� Descrever as taxas de sucesso/falhanço na extubação de pacientes colaborantes
com fraqueza muscular, totalmente dependentes do ventilador, incapazes de
tolerar uma prova de ventilação espontânea, com um protocolo que inclui VNI
optimizada e continua e TAM numa unidade de cuidados intensivos (UCI)
� Descrever e comparar as taxas de sucesso na extubação e descanulação e seus
resultados em pacientes com lesão vértebro medular alta, orientados e totalmente
dependentes do ventilador com um protocolo que inclui VNI optimizada e
continua e TAM para manter SpO2 > 95% em ar ambiente
� Avaliar a eficácia da TAM como parte integrante de um protocolo de desmame
em pacientes que toleram a prova de ventilação espontânea, mas desenvolvem
falência respiratória pós extubação
� Determinar se um novo índex de requerimento ventilatório (IRV) poderá
contribuir para a distinção de pacientes com doença neuromuscular (DNM) com
vários níveis de disfunção dos músculos inspiratórios e dependência ventilatória
e verificar se este índex poderá acrescentar algo á eficácia da medida da
capacidade vital (CV) para indicar o suporte ventilatório
� Comparar os valores de pico fluxo da tosse (PFT), pico de fluxo expiratório
(PFE) e de um fluxo potencialmente simulador obtido através de uma propulsão
da língua e lábios (“dart flow”,DF) em indivíduos saudáveis e em pacientes com
DNM/patologia restritiva e correlacionar estes valores com a CV e a máxima
capacidade de insuflação ( CMI)
� Comparar a capacidade máxima de insuflação passiva (LIC) com a capacidade
de insuflação por “armazenamento de ar” (CMI) e com a CV, no sentido de
explorar relações entre estes valores e correlacioná-los com a função glótica e
PFT. Demonstrar os efeitos de insuflações diárias na LIC em MIC, bem como a
sua a importância na caracterização da severidade da doença.
� Descrever as indicações de TAM domiciliária e explorar a segurança, frequência
e eficácia em pacientes com DNM, totalmente ventilados por VNI ou por
traqueostomia
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
302 Miguel Ramalho do Souto Gonçalves
� Optimizar o protocolo de TAM domiciliário com monitorização de oximetria,
com a inclusão de uma consulta telefónica, no sentido de reduzir os custos e
evitar internamentos hospitalares em pacientes com DNM, totalmente ventilados
por VNI ou por traqueostomia
� Reportar dados de vários centros acerca da eficácia e resultados de uso continuo
de VNI em pacientes com distrofia muscular de Duchenne, esclerose lateral
amiotrófica e atrofia muscular tipo 1 ventilados cronicamente no seu domicilio e
avaliar a evolução das recomendações sobres esta matéria publicados nas
recentemente publicadas revisões e conferências de consenso.
Resultados
Taxa de sucesso na extubação á primeira tentativa com VNI e TAM foi de 95% (149
pacientes). Todas as tentativas de extubação em 98 pacientes com PFT assistidos ≥ 160
L / m foram bem sucedidas. A dependência de VNI contínua e autonomia ventilatória
prévia à intubação correlaciona-se com o sucesso da extubação (p <0,005). Seis dos oito
pacientes que inicialmente falharam a extubação foram bem sucedidos na tentativa
subsequente. Apenas dois pacientes com PFT assistidos imensuráveis foram submetidos
a traqueotomia.
Quando comparados com os pacientes com lesão vértebro-medular alta que foram
decanulados, os pacientes extubados apresentaram menor tempo de internamento em
UCI com menor tempo de duração do protocolo de VNI e TAM. Após o protocolo, CV,
PFT voluntário e assistido melhorou significativamente em todos os pacientes. Os
pacientes extubados apresentaram melhores valores de CV e PFT às 48h pós-extubação
e melhores valores de PFT aos 6 meses de follow up.
Setenta e cinco pacientes críticos (26 mulheres) com idades e índices de gravidade
similares, que toleraram com sucesso o desmame foram randomizados pré extubação
para receber tratamento convencional (grupo controlo) e para receber o mesmo
tratamento com a inclusão de TAM (grupo estudo) Nas 48 horas pós extubação, 20
pacientes do grupo controle (50%) e 14 pacientes do estudo (40%) utilizaram VNI.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 303

Pacientes do grupo de estudo tiveram uma significativa taxa mais baixa de re-intubação
em relação ao grupo de controlo, 6 (17%) vs 19 (48%), pacientes respectivamente.
Considerando apenas o subgrupo de pacientes que usaram VNI, as taxas de re-intubação
relacionados ao falhanço da VNI foram significativamente menores no grupo de estudo,
quando comparado ao grupo controle, 2 (6%) vs (33%) pacientes, respectivamente. O
tempo de internamento em UCI pós – extubação foi significativamente menor no grupo
de estudo (3,1 ± 2,5 vs 9,8 ± 6,7 dias).
O IRV superior a 1,2 foi atingido por 82 dos 91 pacientes que beneficiaram de
assistência ventilatória parcial. A CV inferior a 50% do normal previsto foi atingido por
82 dos 91 pacientes que beneficiaram de assistência ventilatória parcial. Tendo em
conjunto, um IRV superior a 1,2, e um VC inferior a 50% do normal previsto foi
atingido por 87 dos 91 pacientes. Da mesma forma, o IRV superior a 2,5 foi atingido
por 35 dos 42 pacientes que necessitaram de assistência ventilatória superior a 20
horas/dia em que se exigia um ventilador suplente. Uma CV inferior a 1000 ml foi
atingida por 36 de 42 pacientes. Tendo em conjunto um índice superior a 2,5 ou inferior
a 1000 VC ml foi atingido por 38 dos 42 pacientes que necessitaram de assistência
ventilatória superior a 20 horas/dia em que se exigia um ventilador suplente.
Para os pacientes com DNM, o DF foi significativamente maior do que PFT (p <0,01)
que, por sua vez, excedeu significativamente o PEF (p <0,05). 14 pacientes tiveram DF
inferior PFT. Treze desses 14 tinham a capacidade de armazenamento de ar (CMI>
CV), indicando maior comprometimento da boca e dos lábios do que dos músculos da
glote. Para 14 dos 88 pacientes com DNM, os valores de CMI não excederam a CV,
principalmente devido á incapacidade de encerrar a glote. PFT e PEF correlacionam-se
com a CV (r = 0,85 e 0,86, respectivamente), e com a CMI (r = 0,76 e 0,72,
respectivamente).
Em pacientes com DNM, os valores de CV, CMI e LIC foram de 1131 ± 744, 1712 ±
926 e 2069 ± 867 ml, respectivamente, e os valor por PFT voluntário e assistido foram
de 2,5 ± 2,0 e 4,3 ± 2,2 litros / seg, respectivamente, com todas as diferenças
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
304 Miguel Ramalho do Souto Gonçalves

estatisticamente significativas (P <0,001). CMI menos a CV correlacionou inversamente
com a LIC menos CMI (p <0,01) e, portanto, com a função glótica. Ambos os valores
de CMI e LIC aumentaram com a prática (p <0,001). Aumentos na LIC, foram maiores
para os pacientes com menor CV (p <0,05).
Pacientes com DNM usam TAM em casa diariamente ou de forma intermitente durante
as exacerbações agudas Todos os pacientes traqueostomizados usaram TAM
diariamente e mais vezes por dia do que pacientes sob VNI. Os cuidadores foram
considerados competentes e eficazes na aplicação de TAM em casa, com boa tolerância
e sem complicações.
Durante 42 ± 57 meses de seguimento, por 180 episódios agudos, 146 internamentos
foram evitados. As taxas de hospitalização para os pacientes sob VNI foram
significativamente inferiores do que para os traqueostomizados. TAM domiciliário,
durante os episódios agudos normalizou a SpO2 e diminuiu o nº diário de aspirações
profundas através do tubo de traqueostomia. O custo médio mensal por paciente para a
TAM domiciliário por demanda com consulta telefónica profissional, foi de € 403, que
representaram 420 € ou 59% menos do que o preço de uma prescrição contínua TAM
domiciliário.
Vinte centros de 17 países apresentaram 1492 pacientes com DNM ventilados
parcialmente durante a noite em que 713 (48%) evoluíram para suporte ventilatório não
invasivo contínuo durante um seguimento de 15 anos. Um protocolo de monitorização
por oximetria para a aplicação de TAM e VNI continua em ar ambiente permitiu 228
extubações bem sucedidas e 35 descanulações seguras de pacientes incapazes de passar
por provas de respiração espontânea. Após o período de seguimento, 493 (69%)
pacientes estão ainda vivos e em pleno uso contínuo de VNI. A traqueostomia foi
colocada em um total de 125 (8%) pacientes.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 305

Conclusões
� Um protocolo que inclui VNI continua e optimizada com TAM permite a
extubação segura de pacientes com fraqueza muscular devido a DNM e com
lesão vértebro-medular alta, que são incapazes de tolerar provas de ventilação
espontânea Embora alguns autores sugerem benefícios na realização da
traqueostomia precoce, resultados sugerem que, para pacientes com lesão
vértebro-medular com bom nível de cooperação, a extubação com a aplicação de
um protocolo que inclui VNI e MAC, pode produzir melhores resultados e evitar
a necessidade de traqueostomia.
� A aplicação de TAM para manejo de secreções aplicado em subgrupos
específicos de pacientes pode produzir melhores resultados da VNI para o
tratamento da insuficiência respiratória. pós-extubação
� A IRV pode ser usado como um complemento e / ou alternativas para a CV na
avaliação do comprometimento ventilatório e necessidade de assistência
ventilatória em pacientes com DNM.
� Picos de fluxo da tosse, PFE e DF são medidas úteis para avaliar a função da
musculatura bulbar em pacientes com DNM, permitindo um maior
conhecimento do padrão de comprometimento dos músculos respiratórios.
� Insuflação pulmonar regular seja por armazenamento de ar seja por insuflações
passivas são indicadas para todos os pacientes com DNM e CV
significativamente reduzido. Insuflação passiva é utilizada quando o paciente
apresenta comprometimento grave da musculatura bulbar.
� É possível manejar no domicílio a acumulação de secreções e exacerbações
agudas relacionadas, em pacientes com DNM, com um regime á demanda de
TAM centrado na formação e treino de cuidadores não- profissionais e com
acesso a consulta telefónica profissional. Este protocolo foi eficaz na prevenção
de hospitalizações em pacientes com esclerose lateral amiotrófica e outras DNM
totalmente ventilados seja por VNI contínua ou traqueostomia
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
306 Miguel Ramalho do Souto Gonçalves

� A ventilação pulmonar assistida e SpO2 normal pode ser mantida durante o sono, bem
como durante o dia em pacientes com DNM com pouca ou nenhuma CV usando VNI
em suporte ventilatório contínuo. A eficácia da VNI continua Resultados depende mais
da função da musculatura bulbar do que a capacidade vital.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 307

SUMMARY (Abstract)
Introduction
One of the most important developments in the field of mechanical ventilation over the
past 15 years has been the emergence of noninvasive positive pressure ventilation
(NPPV) as an increasing part of the critical care armamentarium. Moreover, it has been
effectively used for long term management in patients with chronic respiratory failure,
from different etiologies. Indeed, the population of home mechanical ventilator users
has, in fact, more than doubled since 1987.
The attraction for NPPV relates primarily to its advantages over invasive mechanical
ventilation with significant reduction of related critical care complications such as upper
airway trauma, ventilator associated pneumonia and high level of sedation. For patients
with long-term home mechanical ventilation, NPPV has advantages over tracheostomy
mechanical ventilation, including greater ease of administration, reduced need for
skilled caregivers, enhanced patient comfort, and lower costs.
For totally ventilator dependent patients with muscle weakness, cough is normally
impaired and secretion accumulation is frequent. Adequate secretion management with
manual or mechanical cough augmentation techniques might be advisable before NPPV
is declared failed or contraindicated in this population, both in acute and chronic
settings.
Research on a continuum strategy of care, from acute to chronic settings that include
NPPV coupled with mechanical assisted cough (MAC) in severely ventilatory impaired
patients with muscle weakness is warranted to support the application of specific
protocols that may improve survival in this patient population.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
308 Miguel Ramalho do Souto Gonçalves

Purpose
� Report extubation success/failure rates in cooperative, totally ventilator
dependent muscle weakness patients, unable to pass weaning trials, using a
protocol that include full, continuous NPPV and MAC in the intensive care unit.
� Report and compare extubation and decannulation success rates and outcomes of
self-directed, totally ventilator dependent patients with high spinal cord injury
using a management protocol that include full, continuous NPPV and MAC to
maintain SpO2≥95% in ambient air.
� Assess the efficacy of MAC as part of a weaning protocol for patients that pass
specific weaning trials but develop acute respiratory failure after extubation.
� Determine whether a new designed ventilator requirement index (VRI) could
distinguish patients with neuromuscular disease (NMD) with various levels of
inspiratory muscle dysfunction and ventilator dependence and if such an index
could add to the diagnostic efficiency of simple vital capacity (VC)
measurement in determining need for ventilator use.
� Compare cough peak flows (CPF), peak expiratory flows (PEF), and potentially
confounding flows obtained by lip and tongue propulsion (“dart flows”, DF) for
normals and for patients with neuromuscular disease/restrictive pulmonary
syndrome (NMD) and correlate them with vital capacity (VC) and maximum
insufflation capacity (MIC).
� Compare maximal passive lung insufflation capacity (LIC) with lung inflation
by air stacking MIC and with vital capacity (VC); to explore relationships
between these variables that correlate with glottic function and cough peak flows
(CPF); to demonstrate the effect of routine inflation therapy on LIC and MIC;
and to determine the relative importance of lung inflation therapy as a function
of disease severity.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 309

� Describe the indications of MAC treatment at home as well as, determine its
safety, compliance and efficacy within NMD patients under continuous NPPV
and tracheostomy.
� Establish an optimal MAC with oximetry feedback provision regimen at home,
with a telephone consultation to help reduce costs and avoid hospitalizations in
NMD patients under continuous NPPV and tracheostomy.
� Report multicentric data and outcomes of the use of NPPV for full, long-term
ventilatory support in Duchenne muscular dystrophy (DMD), amyotrophic
lateral sclerosis (ALS), and spinal muscular atrophy type 1 (SMA 1) and
consider the evolution of practice recommendations reported in reviews and
consensus statements
Results
First attempt extubation success rate with NPPV and MAC in was 95% (149 patients).
All 98 extubation attempts on patients with assisted cough CPF ≥ 160 L/m were
successful. Dependence on continuous NPPV and duration of dependence prior to
intubation correlated with extubation success (p<0.005). Six of 8 patients who initially
failed extubation succeeded on subsequent attempts and only two patients with no
measurable assisted CPF underwent tracheotomy.
When compared to high SCI patients that were decannulated, extubated patients had a
lower ICU length of stay with less time on NPPV and MAC protocol. After the
protocol, VC, unassisted and assisted CPF significantly improved in all patients.
Extubated patients had higher values of VC and CPF at 48h post-extubation and higher
values of CPF at a 6 month follow up.
Seventy five critical ill patients (26 females) with similar age and gravity successfully
weaned were randomized pre extubation to receive conventional post-extubation
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
310 Miguel Ramalho do Souto Gonçalves

treatment (control group) and to the same treatment with MAC (study group) In the 48
hours post extubation, 20 control patients (50%) and 14 study patients (40%) used
NPPV. Study group patients had a significant lower re-intubation rate than controls; 6
(17%) vs 19 (48%), patients respectively. Considering only the sub-group of patients
that used NIV, the re-intubation rates related to NIV failure were significantly lower in
the study group when compared to controls; 2(6%) vs (33%) patients respectively. Post
– extubation ICU length of stay was significantly lower in the study group (3.1± 2.5 vs
9.8± 6.7 days).
A VRI greater than 1.2 captured 82 of 91 patients who benefited from part-time
ventilatory assistance. A VC less than 50% of predicted normal captured 82 of 91
patients who benefited from part-time NPPV. Having an index greater than 1.2 or a VC
less than 50% of predicted normal captured 87 of 91 such patients. Likewise, a VRI
greater than 2.5 captured 35 of 42 patients who required ventilatory support greater than
20 hours per day and required a back-up ventilator. Having a VC less than 1000 ml
captured 36 of 42 such patients. Having an index greater than 2.5 or a VC less than
1000 ml captured 38 of 42 patients who required a back-up ventilator for full-time
ventilatory support.
For NMD patients, the DF were significantly greater than CPF (p<0.01) which, in turn,
significantly exceeded PEF (p<0.05). 14 patients had DF lower than CPF. Thirteen of
these 14 had the ability to air stack (MIC>VC) indicating greater compromise of mouth
and lip than of glottic muscles. For 14 of 88 NMD patients MIC values did not exceed
VC, mostly because of inability to close the glottis (inability to air stack). Nonetheless,
in 11 of these 14 patients the DF were within the standard deviation of the whole group,
thus, bulbar-innervated muscle dysfunction was not uniform. CPF and PEF correlated
with VC (r= 0.85 and 0.86, respectively), and with MIC (r=0.76 and 0.72, respectively).
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 311

In NMD patients, VC, MIC, and LIC were 1131 ±744, 1712±926, and 2069± 867 ml,
respectively, and, for unassisted and assisted CPF, they were 2.5±2.0 and 4.3±2.2
liters/sec, respectively, with all differences statistically significant (P<0.001). MIC
minus VC correlated inversely with LIC minus MIC (P <0.01) and, therefore, with
glottic function. Both MIC and LIC increased with practice (P <0.001). Increases in LIC
but not MIC over VC were greatest for patients with the lowest VC (P <0.05).
Patients with NMD used MAC at home either daily or intermittently during acute
exacerbations All tracheostomized patients used MI-E daily and more times a day than
patients under NPPV. Caregivers were competent and considered MAC effective at
home with good tolerance and no complications.
During 42±57 months of follow up, for 180 acute episodes, 146 hospitalizations were
avoided. Hospitalization rates for NPPV users were significantly lower than for
tracheostomy users. Home MAC during acute episodes normalized baseline SpO2 and
decreased resort to deep airway suctioning via tracheostomy tube per day. Mean
monthly cost per patient for on-demand home MAC with professional telephone
consultation, was €403, that represented 420€ or 59% less than the rental for continuous
home MAC prescription.
Twenty centers from 17 countries presented 1492 nocturnal only ventilated
neuromuscular disease (NMD) patients in which 713 (48%) progressed to continuous
full-setting noninvasive ventilation (NIV) over a follow up of 15 years. A protocol of
oximetry feedback using mechanically assisted coughing (MAC) and full-setting NIV
permitted safe 228 safe extubations and 35 decannulations of patients who could not
pass spontaneous breathing trials (SBTs) before or after extubation/decannulation. After
the follow up period, 493 (69%) patients are still alive on continuous full-setting NIV
and tracheostomy was placed in a total of 125 (8%).
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
312 Miguel Ramalho do Souto Gonçalves

Conclusions
� Continuous full setting NPPV and MAC permits safe extubation of NMD and
high SCI patients that are unable to pass spontaneous breathing trials Although
some authors suggest a benefit on performing early tracheostomy, we would like
to suggest that for cooperative high level SCI patients, an extubation protocol
including NPPV and MAC, can produce better outcomes and avoid the necessity
of tracheostomy.
� Secretion clearance with MI-E, applied in specific subgroups of patients may
produce better outcomes of NPPV to treat post-extubation respiratory failure.
� The VRI can be used as a complement and/or alternative to VC in the evaluation
of ventilatory impairment requiring ventilatory assistance in NMD patients.
� Cough Peak flows, PEF, and DF are useful measures of bulbar-innervated and
respiratory muscle function for patients with NMD, permitting greater
knowledge of the pattern of respiratory muscle compromise.
� Regular lung insufflation, either by air stacking (to approach MIC) or by passive
lung insufflation (to approach LIC), is indicated for all NMD patients with
diminishing VC. Passive insufflation is used when the patient has severe
impairment of the bulbar musculature.
� It is possible to manage secretion encumbrance and acute exacerbations at home
in NMD patients, with an on demand MAC regimen centred on trained non-
professional caregivers and telephone consultation. This was effective in
averting hospitalizations for patients with ALS and other NMD patients either
on continuous NPPV or tracheostomy
� Assisted lung ventilation and normal SpO2 can be maintained during sleep as
well as during daytime hours for patients with little or no VC by using NPPV at
full ventilatory support. Successful outcomes of continuous NPPV in NMD
patients depends more on the bulbar muscle function than on the vital capacity.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 313

References
1. Bach JR. Continuous noninvasive ventilation for patients with neuromuscular disease
and spinal cord injury. Semin Respir Crit Care Med. 2002 Jun;23(3):283-92.
2. Nava S, Hill N. Non-invasive ventilation in acute respiratory failure. Lancet. 2009 Jul
18;374(9685):250-9.
3. Ambrosino N, Foglio K, Rubini F, Clini E, Nava S, Vitacca M. Non-invasive mechanical
ventilation in acute respiratory failure due to chronic obstructive pulmonary disease:
correlates for success. Thorax. 1995 Jul;50(7):755-7.
4. Clini E, Sturani C, Rossi A, Viaggi S, Corrado A, Donner CF, et al. The Italian multicentre
study on noninvasive ventilation in chronic obstructive pulmonary disease patients. Eur Respir
J. 2002 Sep;20(3):529-38.
5. Cuvelier A, Muir JF. Noninvasive ventilation and obstructive lung diseases. Eur Respir J.
2001 Jun;17(6):1271-81.
6. Elliott MW. Noninvasive ventilation in COPD patients with chronic respiratory failure--
con. Monaldi Arch Chest Dis. 2000 Feb;55(1):58-61.
7. Hill NS. Noninvasive ventilation for chronic obstructive pulmonary disease. Respir Care.
2004 Jan;49(1):72-87; discussion -9.
8. Simonds AK, Elliott MW. Outcome of domiciliary nasal intermittent positive pressure
ventilation in restrictive and obstructive disorders. Thorax. 1995 Jun;50(6):604-9.
9. Bach JR. Update and perspectives on noninvasive respiratory muscle aids. Part 1: The
inspiratory aids. Chest. 1994 Apr;105(4):1230-40.
10. Bach JR. Amyotrophic lateral sclerosis: prolongation of life by noninvasive respiratory
aids
Chest. 2002 Jul;122(1):92-8.
11. Benditt JO. Initiating noninvasive management of respiratory insufficiency in
neuromuscular disease. Pediatrics. 2009 May;123 Suppl 4:S236-8.
12. Bourke SC, Tomlinson M, Williams TL, Bullock RE, Shaw PJ, Gibson GJ. Effects of non-
invasive ventilation on survival and quality of life in patients with amyotrophic lateral sclerosis:
a randomised controlled trial. Lancet Neurol. 2006 Feb;5(2):140-7.
13. Rideau Y, Delaubier A. Management of respiratory neuromuscular weakness. Muscle
Nerve. 1988 Apr;11(4):407-8.
14. Robert D, Willig TN, Leger P, Paulus J. Long-term nasal ventilation in neuromuscular
disorders: report of a consensus conference. Eur Respir J. 1993 Apr;6(4):599-606.
15. Shneerson JM, Simonds AK. Noninvasive ventilation for chest wall and neuromuscular
disorders. Eur Respir J. 2002 Aug;20(2):480-7.
16. Simonds AK. Recent advances in respiratory care for neuromuscular disease. Chest.
2006 Dec;130(6):1879-86.
17. Simonds AK, Muntoni F, Heather S, Fielding S. Impact of nasal ventilation on survival in
hypercapnic Duchenne muscular dystrophy. Thorax. 1998 Nov;53(11):949-52.
18. International Consensus Conferences in Intensive Care Medicine: noninvasive positive
pressure ventilation in acute Respiratory failure. Am J Respir Crit Care Med. 2001
Jan;163(1):283-91.
19. Make BJ, Hill NS, Goldberg AI, Bach JR, Criner GJ, Dunne PE, et al. Mechanical
ventilation beyond the intensive care unit. Report of a consensus conference of the American
College of Chest Physicians. Chest. 1998 May;113(5 Suppl):289S-344S.
20. Burns KE, Adhikari NK, Meade MO. Noninvasive positive pressure ventilation as a
weaning strategy for intubated adults with respiratory failure. Cochrane Database Syst Rev.
2003(4):CD004127.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
314 Miguel Ramalho do Souto Gonçalves

21. Hess DR. The evidence for noninvasive positive-pressure ventilation in the care of
patients in acute respiratory failure: a systematic review of the literature. Respir Care. 2004
Jul;49(7):810-29.
22. Brochard L. Mechanical ventilation: invasive versus noninvasive. Eur Respir J Suppl.
2003 Nov;47:31s-7s.
23. Ambrosino N. Ventilation techniques: invasive versus noninvasive. Monaldi Arch Chest
Dis. 1994 Dec;49(6):513-5.
24. Conti G, Marino P, Cogliati A, Dell'Utri D, Lappa A, Rosa G, et al. Noninvasive ventilation
for the treatment of acute respiratory failure in patients with hematologic malignancies: a pilot
study. Intensive Care Med. 1998 Dec;24(12):1283-8.
25. Nava S, Navalesi P, Conti G. Time of non-invasive ventilation. Intensive Care Med. 2006
Mar;32(3):361-70.
26. Polkey MI, Moxham J. Noninvasive ventilation in the management of decompensated
COPD. Monaldi Arch Chest Dis. 1995 Oct;50(5):378-82.
27. Servera E, Sancho J, Zafra MJ, Catala A, Vergara P, Marin J. Alternatives to
endotracheal intubation for patients with neuromuscular diseases. Am J Phys Med Rehabil.
2005 Nov;84(11):851-7.
28. Wysocki M, Tric L, Wolff MA, Gertner J, Millet H, Herman B. Noninvasive pressure
support ventilation in patients with acute respiratory failure. Chest. 1993 Mar;103(3):907-13.
29. Wood KA, Lewis L, Von Harz B, Kollef MH. The use of noninvasive positive pressure
ventilation in the emergency department: results of a randomized clinical trial. Chest. 1998
May;113(5):1339-46.
30. Wood KE, Flaten AL, Backes WJ. Inspissated secretions: a life-threatening complication
of prolonged noninvasive ventilation. Respir Care. 2000 May;45(5):491-3.
31. Esteban A, Alia I, Tobin MJ, Gil A, Gordo F, Vallverdu I, et al. Effect of spontaneous
breathing trial duration on outcome of attempts to discontinue mechanical ventilation.
Spanish Lung Failure Collaborative Group. Am J Respir Crit Care Med. 1999 Feb;159(2):512-8.
32. Epstein SK, Ciubotaru RL. Independent effects of etiology of failure and time to
reintubation on outcome for patients failing extubation. Am J Respir Crit Care Med. 1998
Aug;158(2):489-93.
33. Vitacca M, Ambrosino N, Clini E, Porta R, Rampulla C, Lanini B, et al. Physiological
response to pressure support ventilation delivered before and after extubation in patients not
capable of totally spontaneous autonomous breathing. Am J Respir Crit Care Med. 2001 Aug
15;164(4):638-41.
34. Ceriana P, Delmastro M, Rampulla C, Nava S. Demographics and clinical outcomes of
patients admitted to a respiratory intensive care unit located in a rehabilitation center. Respir
Care. 2003 Jul;48(7):670-6.
35. Esteban A, Anzueto A, Alia I, Gordo F, Apezteguia C, Palizas F, et al. How is mechanical
ventilation employed in the intensive care unit? An international utilization review. Am J Respir
Crit Care Med. 2000 May;161(5):1450-8.
36. Nava S, Ceriana P. Causes of failure of noninvasive mechanical ventilation. Respir Care.
2004 Mar;49(3):295-303.
37. Smina M, Salam A, Khamiees M, Gada P, Amoateng-Adjepong Y, Manthous CA. Cough
peak flows and extubation outcomes. Chest. 2003 Jul;124(1):262-8.
38. Nakagawa NK, Franchini ML, Driusso P, de Oliveira LR, Saldiva PH, Lorenzi-Filho G.
Mucociliary clearance is impaired in acutely ill patients. Chest. 2005 Oct;128(4):2772-7.
39. Chaisson KM, Walsh S, Simmons Z, Vender RL. A clinical pilot study: high frequency
chest wall oscillation airway clearance in patients with amyotrophic lateral sclerosis.
Amyotroph Lateral Scler. 2006 Jun;7(2):107-11.
40. Bellone A, Spagnolatti L, Massobrio M, Bellei E, Vinciguerra R, Barbieri A, et al. Short-
term effects of expiration under positive pressure in patients with acute exacerbation of
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 315

chronic obstructive pulmonary disease and mild acidosis requiring non-invasive positive
pressure ventilation. Intensive Care Med. 2002 May;28(5):581-5.
41. Vargas F, Bui HN, Boyer A, Salmi LR, Gbikpi-Benissan G, Guenard H, et al.
Intrapulmonary percussive ventilation in acute exacerbations of COPD patients with mild
respiratory acidosis: a randomized controlled trial [ISRCTN17802078]. Crit Care. 2005
Aug;9(4):R382-9.
42. Round Table Conference on Poliomyelitis Equipment, Roosevelt Hotel, White Plaines,
New York City National Foundation for Infantile Paralysis-March of Dimes, Inc. May 1953.
43. Bach J. A historical perspective on the use of noninvasive ventilatory support
alternatives. Am Rev Respir Dis 1996(22):161 81.
44. Bach JR, Alba AS, Bohatiuk G, Saporito L, Lee M. Mouth intermittent positive pressure
ventilation in the management of postpolio respiratory insufficiency. Chest. 1987
Jun;91(6):859-64.
45. Bach JR, Alba AS, Shin D. Management alternatives for post-polio respiratory
insufficiency. Assisted ventilation by nasal or oral-nasal interface. Am J Phys Med Rehabil. 1989
Dec;68(6):264-71.
46. Simonds AK. Home ventilation. Eur Respir J Suppl. 2003 Nov;47:38s-46s.
47. Bach JR, Rajaraman R, Ballanger F, Tzeng AC, Ishikawa Y, Kulessa R, et al.
Neuromuscular ventilatory insufficiency: effect of home mechanical ventilator use v oxygen
therapy on pneumonia and hospitalization rates. Am J Phys Med Rehabil. 1998 Jan-
Feb;77(1):8-19.
48. Clinical indications for noninvasive positive pressure ventilation in chronic respiratory
failure due to restrictive lung disease, COPD, and nocturnal hypoventilation--a consensus
conference report. Chest. 1999 Aug;116(2):521-34.
49. Simonds AK. Risk management of the home ventilator dependent patient. Thorax.
2006 May;61(5):369-71.
50. Vianello A, Bevilacqua M, Arcaro G, Serra E. Prevention of pulmonary morbidity in
patients with neuromuscular disorders: a possible role for permanent cricothyroid
minitracheostomy. Chest. 1998 Jul;114(1):346-7.
51. Vitacca M, Grassi M, Barbano L, Galavotti G, Sturani C, Vianello A, et al. Last 3 months
of life in home-ventilated patients: the family perception. Eur Respir J. 2009 Aug 28.
52. Vitacca M, Bazza A, Bianchi L, Gile S, Assoni G, Porta R, et al. Tele-assistance in chronic
respiratory failure: patients' characterization and staff workload of 5-year activity. Telemed J E
Health. 2010 Apr;16(3):299-305.
53. Vitacca M, Bianchi L, Guerra A, Fracchia C, Spanevello A, Balbi B, et al. Tele-assistance
in chronic respiratory failure patients: a randomised clinical trial. Eur Respir J. 2009
Feb;33(2):411-8.
54. Bach JR. Mechanical insufflation-exsufflation. Comparison of peak expiratory flows
with manually assisted and unassisted coughing techniques. Chest. 1993 Nov;104(5):1553-62.
55. Chatwin M. How to use a mechanical insufflator-exsufflator "cough assist machine".
Breathe. 2008;volume 4(June):321-5.
56. Chatwin M, Ross E, Hart N, Nickol AH, Polkey MI, Simonds AK. Cough augmentation
with mechanical insufflation/exsufflation in patients with neuromuscular weakness. Eur Respir
J. 2003 Mar;21(3):502-8.
57. Fauroux B, Guillemot N, Aubertin G, Nathan N, Labit A, Clement A, et al. Physiologic
benefits of mechanical insufflation-exsufflation in children with neuromuscular diseases.
Chest. 2008 Jan;133(1):161-8.
58. Goncalves M, Winck J. Exploring the potential of mechanical insufflation-exsufflation.
Breathe. 2008;volume 4(June):326-9.
59. Homnick DN. Mechanical insufflation-exsufflation for airway mucus clearance. Respir
Care. 2007 Oct;52(10):1296-305; discussion 306-7.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
316 Miguel Ramalho do Souto Gonçalves

60. Sancho J, Servera E, Diaz J, Marin J. Efficacy of mechanical insufflation-exsufflation in
medically stable patients with amyotrophic lateral sclerosis. Chest. 2004 Apr;125(4):1400-5.
61. Sancho J, Servera E, Vergara P, Marin J. Mechanical insufflation-exsufflation vs.
tracheal suctioning via tracheostomy tubes for patients with amyotrophic lateral sclerosis: a
pilot study. Am J Phys Med Rehabil. 2003 Oct;82(10):750-3.
62. Winck JC, Goncalves MR, Lourenco C, Viana P, Almeida J, Bach JR. Effects of mechanical
insufflation-exsufflation on respiratory parameters for patients with chronic airway secretion
encumbrance. Chest. 2004 Sep;126(3):774-80.
63. Gomez-Merino E, Bach JR. Duchenne muscular dystrophy: prolongation of life by
noninvasive ventilation and mechanically assisted coughing. Am J Phys Med Rehabil. 2002
Jun;81(6):411-5.
64. The Jerusalem Bible, The second book of the kings. Doubleday & Company, INC 1970(
).
65. Gordon A. History and evolution of modern resuscitation techniques. In Gordon AS
(ed): Cardiopulmonary Resuscitation Conference Proceedings, National Academy of Sciences,
Washington, DC. 1966;7:32.
66. Rendell Baker L. Principles in design and function of mechanical ventilators. Respir
Ther. 1979;9:63-9.
67. Ristagno G, Tang W, Weil M. Cardiopulmonary Resuscitation: From the Beginning to
the Present Day. Critical Care Clinics,.25(1):133-51.
68. Bach J. The history of mechancial ventilation and respiratory muscle aids. In: Bach JR
(ed) Noninvasive Mechanical Ventilation Philadephia, Hanley & Belfus. 2002:45-72.
69. Rodolph Matas T. The history and methods of intralaryngeal insuffation for the relief of
acute surgical pneumothorax with a description of the latest devices for the purpose. .
ransactions of the Southern Surgical and Gynecological Association. 1900;12(84):69-71.
70. Woollam C. The development of apparatus for intermittent negative pressure
respiration:1832-1918. Anaesthesia 1976;31(537-47).
71. Rendell Baker L. Principles in design and function of mechanical ventilators. Respir Ther
1979;9:63-9.
72. Anton S. Dictionary of the History of Medicine. Parthenon Publishing, Pearl River, NY.
1999;75.
73. Dalziel J. On sleep and an apparatus for promoting artificial respiration. Br Assoc
Advancement Sci. 1838;2(127).
74. Emerson J, Loynes J. The Evolution of Iron Lungs: Respirators of the Body Encasing
Type. J H Emerson Company, Cambridge, MA:. 1978.
75. . Drinker P, McKhann C. The iron lung: first practical means of respiratory support. .
JAMA. 1986;255(1476).
76. Gorham J. A medical triumph: the iron lung. Respir Care 1979;9(71).
77. The Council on Physical Medicine: Acceptability of the Fairchild Huxley cuirass
respirator. JAMA. 1950;143(1157).
78. The Council on Physical Medicine: The Monaghan Portable Respirator acceptance
report. JAMA. 1949;139(1273).
79. Spalding J, Opie L. Artificial respiration with the Tunnicliffe breathing jacket. Lancet.
1958;274:613-15.
80. Eve F. Actuation of inert diaphragm by gravity method. Lancet. 1932;2(995-97).
81. Bach JR. Ventilatory support alternatives to tracheostomy and intubation: current
status of the application of this technology. Conn Med. 1991 Jun;55(6):323-9.
82. Barach AL, Beck G, Smith W. Mechanical production of expiratory flow rates surpassing
the capacity of human coughing. Trans Assoc Am Physicians. 1953;66:315-24.
83. Barach AL, Beck GJ. Mechanical production of expiratory flow rates surpassing the
capacity of human coughing. Am J Med Sci. 1953 Sep;226(3):241-9.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 317
84. Barach AL, Beck GJ. Exsufflation with negative pressure; physiologic and clinical studies
in poliomyelitis, bronchial asthma, pulmonary emphysema, and bronchiectasis. AMA Arch
Intern Med. 1954 Jun;93(6):825-41.
85. Lassen H. The epidemic of poliomyelitis in Copenhagen,1952. Proc R Soc Med.
1954;47:67-71.
86. Hodes H. Treatment of respiratory difficulty in poliomyelitis In: Poliomyelitis: papers
and discussion; presented at the third international poliomyelitis conference, Lippincott,
Philadelphia. 1955:91-113.
87. Bach JR, Alba AS, Saporito LR. Intermittent positive pressure ventilation via the mouth
as an alternative to tracheostomy for 257 ventilator users. Chest. 1993 Jan;103(1):174-82.
88. Bach JR, Alba AS. Noninvasive options for ventilatory support of the traumatic high
level quadriplegic patient. Chest. 1990 Sep;98(3):613-9.
89. Bach JR, Alba AS. Management of chronic alveolar hypoventilation by nasal ventilation.
Chest. 1990 Jan;97(1):52-7.
90. Bach JR, Alba AS. Sleep and nocturnal mouthpiece IPPV efficiency in postpoliomyelitis
ventilator users. Chest. 1994 Dec;106(6):1705-10.
91. Delaubier A, Guillou C, Mordelet M, Rideau Y. [Early respiratory assistance by nasal
route in Duchenne's muscular dystrophy]. Agressologie. 1987 Jun;28(7):737-8.
92. Bach JR, Alba A, Mosher R, Delaubier A. Intermittent positive pressure ventilation via
nasal access in the management of respiratory insufficiency. Chest. 1987 Jul;92(1):168-70.
93. Sullivan CE, Issa FG, Berthon-Jones M, McCauley VB, Costas LJ. Home treatment of
obstructive sleep apnoea with continuous positive airway pressure applied through a nose-
mask. Bull Eur Physiopathol Respir. 1984 Jan-Feb;20(1):49-54.
94. McDermott I, Bach JR, Parker C, Sortor S. Custom-fabricated interfaces for intermittent
positive pressure ventilation. Int J Prosthodont. 1989 May-Jun;2(3):224-33.
95. Knoblauch A, Walther P. [Home ventilatory support--retrospective view and
perspectives]. Ther Umsch. 1990 Nov;47(11):885-9.
96. Bach JR. Alternative methods of ventilatory support for the patient with ventilatory
failure due to spinal cord injury. J Am Paraplegia Soc. 1991 Oct;14(4):158-74.
97. Bach JR. New approaches in the rehabilitation of the traumatic high level quadriplegic.
Am J Phys Med Rehabil. 1991 Feb;70(1):13-9.
98. Bach JR, Alba AS. Intermittent abdominal pressure ventilator in a regimen of
noninvasive ventilatory support. Chest. 1991 Mar;99(3):630-6.
99. Bach JR, Smith WH, Michaels J, Saporito L, Alba AS, Dayal R, et al. Airway secretion
clearance by mechanical exsufflation for post-poliomyelitis ventilator-assisted individuals. Arch
Phys Med Rehabil. 1993 Feb;74(2):170-7.
100. Carlucci A, Delmastro M, Rubini F, Fracchia C, Nava S. Changes in the practice of non-
invasive ventilation in treating COPD patients over 8 years. Intensive Care Med. 2003
Mar;29(3):419-25.
101. AARC- Consenus statement. Noninvasive positive pressure ventilation. Respir Care.
1997;42:365-9.
102. Confalonieri M, Calderini E, Terraciano S, Chidini G, Celeste E, Puccio G, et al.
Noninvasive ventilation for treating acute respiratory failure in AIDS patients with
Pneumocystis carinii pneumonia. Intensive Care Med. 2002 Sep;28(9):1233-8.
103. Girou E, Schortgen F, Delclaux C, Brun-Buisson C, Blot F, Lefort Y, et al. Association of
noninvasive ventilation with nosocomial infections and survival in critically ill patients. Jama.
2000 Nov 8;284(18):2361-7.
104. Jaber S, Delay JM, Chanques G, Sebbane M, Jacquet E, Souche B, et al. Outcomes of
patients with acute respiratory failure after abdominal surgery treated with noninvasive
positive pressure ventilation. Chest. 2005 Oct;128(4):2688-95.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
318 Miguel Ramalho do Souto Gonçalves

105. Rocco M, Dell'Utri D, Morelli A, Spadetta G, Conti G, Antonelli M, et al. Noninvasive
ventilation by helmet or face mask in immunocompromised patients: a case-control study.
Chest. 2004 Nov;126(5):1508-15.
106. Wysocki M, Tric L, Wolff MA, Millet H, Herman B. Noninvasive pressure support
ventilation in patients with acute respiratory failure. A randomized comparison with
conventional therapy. Chest. 1995 Mar;107(3):761-8.
107. Elliott MW, Aquilina R, Green M, Moxham J, Simonds AK. A comparison of different
modes of noninvasive ventilatory support: effects on ventilation and inspiratory muscle effort.
Anaesthesia. 1994 Apr;49(4):279-83.
108. Munoz X, Crespo A, Marti S, Torres F, Ferrer J, Morell F. Comparative study of two
different modes of noninvasive home mechanical ventilation in chronic respiratory failure.
Respir Med. 2006 Apr;100(4):673-81.
109. Nava S, Ceriana P. Patient-ventilator interaction during noninvasive positive pressure
ventilation. Respir Care Clin N Am. 2005 Jun;11(2):281-93.
110. Kacmarek RM. Noninvasive positive-pressure ventilation:the little things do make the
difference! Respir Care. 2003 Oct;48(10):919-21.
111. Fauroux B, Louis B, Hart N, Essouri S, Leroux K, Clement A, et al. The effect of back-up
rate during non-invasive ventilation in young patients with cystic fibrosis. Intensive Care Med.
2004 Apr;30(4):673-81.
112. Nava S, Fanfulla F, Frigerio P, Navalesi P. Physiologic evaluation of 4 weeks of nocturnal
nasal positive pressure ventilation in stable hypercapnic patients with chronic obstructive
pulmonary disease. Respiration. 2001;68(6):573-83.
113. Mehta S, Hill NS. Noninvasive ventilation. Am J Respir Crit Care Med. 2001
Feb;163(2):540-77.
114. Girault C, Daudenthun I, Chevron V, Tamion F, Leroy J, Bonmarchand G. Noninvasive
ventilation as a systematic extubation and weaning technique in acute-on-chronic respiratory
failure: a prospective, randomized controlled study. Am J Respir Crit Care Med. 1999
Jul;160(1):86-92.
115. Battisti A, Tassaux D, Janssens JP, Michotte JB, Jaber S, Jolliet P. Performance
characteristics of 10 home mechanical ventilators in pressure-support mode: a comparative
bench study. Chest. 2005 May;127(5):1784-92.
116. Nava S, Ambrosino N, Bruschi C, Confalonieri M, Rampulla C. Physiological effects of
flow and pressure triggering during non-invasive mechanical ventilation in patients with
chronic obstructive pulmonary disease. Thorax. 1997 Mar;52(3):249-54.
117. Nava S, Bruschi C, Rubini F, Palo A, Iotti G, Braschi A. Respiratory response and
inspiratory effort during pressure support ventilation in COPD patients. Intensive Care Med.
1995 Nov;21(11):871-9.
118. Fauroux B, Pigeot J, Polkey MI, Isabey D, Clement A, Lofaso F. In vivo physiologic
comparison of two ventilators used for domiciliary ventilation in children with cystic fibrosis.
Crit Care Med. 2001 Nov;29(11):2097-105.
119. Schonhofer B, Sortor-Leger S. Equipment needs for noninvasive mechanical ventilation.
Eur Respir J. 2002 Oct;20(4):1029-36.
120. Farre R, Navajas D, Prats E, Marti S, Guell R, Montserrat JM, et al. Performance of
mechanical ventilators at the patient's home: a multicentre quality control study. Thorax. 2006
May;61(5):400-4.
121. Drinkwine J, Kacmarek RM. Noninvasive positive pressure ventilation. Equipment and
techniques. Respir Care Clin N Am. 1996 Jun;2(2):183-94.
122. Chailleux E, Fauroux B, Binet F, Dautzenberg B, Polu JM. Predictors of survival in
patients receiving domiciliary oxygen therapy or mechanical ventilation. A 10-year analysis of
ANTADIR Observatory. Chest. 1996 Mar;109(3):741-9.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 319

123. Lien TC, Wang JH, Huang SH, Chen SD. Comparison of bilevel positive airway pressure
and volume ventilation via nasal or facial masks in patients with severe, stable COPD.
Zhonghua Yi Xue Za Zhi (Taipei). 2000 Jul;63(7):542-51.
124. Bach JR. Bilevel pressure vs volume ventilators for amyotrophic lateral sclerosis
patients. Chest. 2006 Dec;130(6):1949; author reply -50.
125. Boitano LJ, Benditt JO. An evaluation of home volume ventilators that support open-
circuit mouthpiece ventilation. Respir Care. 2005 Nov;50(11):1457-61.
126. Schonhofer B, Sonneborn M, Haidl P, Bohrer H, Kohler D. Comparison of two different
modes for noninvasive mechanical ventilation in chronic respiratory failure: volume versus
pressure controlled device. Eur Respir J. 1997 Jan;10(1):184-91.
127. Tzeng AC, Bach JR. Prevention of pulmonary morbidity for patients with neuromuscular
disease. Chest. 2000 Nov;118(5):1390-6.
128. Storre JH, Seuthe B, Fiechter R, Milioglou S, Dreher M, Sorichter S, et al. Average
volume-assured pressure support in obesity hypoventilation: A randomized crossover trial.
Chest. 2006 Sep;130(3):815-21.
129. Koyama T, Watanabe H, Kobukai Y, Makabe S, Munehisa Y, Iino K, et al. Beneficial
Effects of Adaptive Servo Ventilation in Patients With Chronic Heart Failure. Circ J. 2010 Jul 29.
130. Teschler H, Dohring J, Wang YM, Berthon-Jones M. Adaptive pressure support servo-
ventilation: a novel treatment for Cheyne-Stokes respiration in heart failure. Am J Respir Crit
Care Med. 2001 Aug 15;164(4):614-9.
131. Elliott MW. The interface: crucial for successful noninvasive ventilation. Eur Respir J.
2004 Jan;23(1):7-8.
132. Carrey Z, Gottfried SB, Levy RD. Ventilatory muscle support in respiratory failure with
nasal positive pressure ventilation. Chest. 1990 Jan;97(1):150-8.
133. Kwok H, McCormack J, Cece R, Houtchens J, Hill NS. Controlled trial of oronasal versus
nasal mask ventilation in the treatment of acute respiratory failure. Crit Care Med. 2003
Feb;31(2):468-73.
134. Anton A, Tarrega J, Giner J, Guell R, Sanchis J. Acute physiologic effects of nasal and
full-face masks during noninvasive positive-pressure ventilation in patients with acute
exacerbations of chronic obstructive pulmonary disease. Respir Care. 2003 Oct;48(10):922-5.
135. Navalesi P, Fanfulla F, Frigerio P, Gregoretti C, Nava S. Physiologic evaluation of
noninvasive mechanical ventilation delivered with three types of masks in patients with
chronic hypercapnic respiratory failure. Crit Care Med. 2000 Jun;28(6):1785-90.
136. Nava S, Navalesi P, Gregoretti C. Interfaces and humidification for noninvasive
mechanical ventilation. Respir Care. 2009 Jan;54(1):71-84.
137. Criner GJ, Travaline JM, Brennan KJ, Kreimer DT. Efficacy of a new full face mask for
noninvasive positive pressure ventilation. Chest. 1994 Oct;106(4):1109-15.
138. Bach JR. "Mask" ventilation doesn't have to be through the nose. Chest. 1992
Apr;101(4):1182-3.
139. Bach JR. Nasal ventilation is not the final word. Chest. 1993 Nov;104(5):1638-9.
140. Miyoshi E, Fujino Y, Uchiyama A, Mashimo T, Nishimura M. Effects of gas leak on
triggering function, humidification, and inspiratory oxygen fraction during noninvasive positive
airway pressure ventilation. Chest. 2005 Nov;128(5):3691-8.
141. Gonzalez J, Sharshar T, Hart N, Chadda K, Raphael JC, Lofaso F. Air leaks during
mechanical ventilation as a cause of persistent hypercapnia in neuromuscular disorders.
Intensive Care Med. 2003 Apr;29(4):596-602.
142. Mehta S, McCool FD, Hill NS. Leak compensation in positive pressure ventilators: a lung
model study. Eur Respir J. 2001 Feb;17(2):259-67.
143. Schettino GP, Tucci MR, Sousa R, Valente Barbas CS, Passos Amato MB, Carvalho CR.
Mask mechanics and leak dynamics during noninvasive pressure support ventilation: a bench
study. Intensive Care Med. 2001 Dec;27(12):1887-91.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
320 Miguel Ramalho do Souto Gonçalves

144. Lellouche F, Maggiore SM, Deye N, Taille S, Pigeot J, Harf A, et al. Effect of the
humidification device on the work of breathing during noninvasive ventilation. Intensive Care
Med. 2002 Nov;28(11):1582-9.
145. Nava S, Cirio S, Fanfulla F, Carlucci A, Navarra A, Negri A, et al. Comparison of two
humidification systems for long-term noninvasive mechanical ventilation. Eur Respir J. 2008
Aug;32(2):460-4.
146. Antonelli M, Conti G. Noninvasive positive pressure ventilation as treatment for acute
respiratory failure in critically ill patients. Crit Care. 2000;4(1):15-22.
147. Antonelli M, Pennisi MA, Montini L. Clinical review: Noninvasive ventilation in the
clinical setting--experience from the past 10 years. Crit Care. 2005 Feb;9(1):98-103.
148. Brochard L, Isabey D, Piquet J, Amaro P, Mancebo J, Messadi AA, et al. Reversal of
acute exacerbations of chronic obstructive lung disease by inspiratory assistance with a face
mask. N Engl J Med. 1990 Nov 29;323(22):1523-30.
149. Esteban A, Ferguson ND, Meade MO, Frutos-Vivar F, Apezteguia C, Brochard L, et al.
Evolution of mechanical ventilation in response to clinical research. Am J Respir Crit Care Med.
2008 Jan 15;177(2):170-7.
150. Meduri GU, Turner RE, Abou-Shala N, Wunderink R, Tolley E. Noninvasive positive
pressure ventilation via face mask. First-line intervention in patients with acute hypercapnic
and hypoxemic respiratory failure. Chest. 1996 Jan;109(1):179-93.
151. Carlucci A, Richard JC, Wysocki M, Lepage E, Brochard L. Noninvasive versus
conventional mechanical ventilation. An epidemiologic survey. Am J Respir Crit Care Med. 2001
Mar;163(4):874-80.
152. Demoule A, Girou E, Richard JC, Taille S, Brochard L. Increased use of noninvasive
ventilation in French intensive care units. Intensive Care Med. 2006 Nov;32(11):1747-55.
153. Ferrer M, Esquinas A, Arancibia F, Bauer TT, Gonzalez G, Carrillo A, et al. Noninvasive
ventilation during persistent weaning failure: a randomized controlled trial. Am J Respir Crit
Care Med. 2003 Jul 1;168(1):70-6.
154. Ferrer M, Esquinas A, Leon M, Gonzalez G, Alarcon A, Torres A. Noninvasive ventilation
in severe hypoxemic respiratory failure: a randomized clinical trial. Am J Respir Crit Care Med.
2003 Dec 15;168(12):1438-44.
155. Ferrer M, Valencia M, Nicolas JM, Bernadich O, Badia JR, Torres A. Early noninvasive
ventilation averts extubation failure in patients at risk: a randomized trial. Am J Respir Crit Care
Med. 2006 Jan 15;173(2):164-70.
156. Antonelli M, Conti G, Moro ML, Esquinas A, Gonzalez-Diaz G, Confalonieri M, et al.
Predictors of failure of noninvasive positive pressure ventilation in patients with acute
hypoxemic respiratory failure: a multi-center study. Intensive Care Med. 2001
Nov;27(11):1718-28.
157. Finlay G, Concannon D, McDonnell TJ. Treatment of respiratory failure due to
kyphoscoliosis with nasal intermittent positive pressure ventilation (NIPPV). Ir J Med Sci. 1995
Jan;164(1):28-30.
158. Burns KE, Adhikari NK, Meade MO. A meta-analysis of noninvasive weaning to facilitate
liberation from mechanical ventilation. Can J Anaesth. 2006 Mar;53(3):305-15.
159. Esteban A, Frutos-Vivar F, Ferguson ND, Arabi Y, Apezteguia C, Gonzalez M, et al.
Noninvasive positive-pressure ventilation for respiratory failure after extubation. N Engl J Med.
2004 Jun 10;350(24):2452-60.
160. Keenan SP, Powers C, McCormack DG, Block G. Noninvasive positive-pressure
ventilation for postextubation respiratory distress: a randomized controlled trial. Jama. 2002
Jun 26;287(24):3238-44.
161. Nava S, Ambrosino N, Clini E, Prato M, Orlando G, Vitacca M, et al. Noninvasive
mechanical ventilation in the weaning of patients with respiratory failure due to chronic
obstructive pulmonary disease. A randomized, controlled trial. Ann Intern Med. 1998 May
1;128(9):721-8.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 321

162. Masip J, Paez J, Merino M, Parejo S, Vecilla F, Riera C, et al. Risk factors for intubation
as a guide for noninvasive ventilation in patients with severe acute cardiogenic pulmonary
edema. Intensive Care Med. 2003 Nov;29(11):1921-8.
163. Bella I, Chad DA. Neuromuscular disorders and acute respiratory failure. Neurol Clin.
1998 May;16(2):391-417.
164. Cuomo A, Delmastro M, Ceriana P, Nava S, Conti G, Antonelli M, et al. Noninvasive
mechanical ventilation as a palliative treatment of acute respiratory failure in patients with
end-stage solid cancer. Palliat Med. 2004 Oct;18(7):602-10.
165. Nava S, Cuomo AM. Acute respiratory failure in the cancer patient: the role of non-
invasive mechanical ventilation. Crit Rev Oncol Hematol. 2004 Aug;51(2):91-103.
166. Freichels TA. Palliative ventilatory support: use of noninvasive positive pressure
ventilation in terminal respiratory insufficiency. Am J Crit Care. 1994 Jan;3(1):6-10.
167. Nava S, Cuomo A, Maugeri FS. Noninvasive ventilation and dyspnea in palliative
medicine. Chest. 2006 May;129(5):1391-2.
168. Confalonieri M, Parigi P, Scartabellati A, Aiolfi S, Scorsetti S, Nava S, et al. Noninvasive
mechanical ventilation improves the immediate and long-term outcome of COPD patients with
acute respiratory failure. Eur Respir J. 1996 Mar;9(3):422-30.
169. Brochard L, Mancebo J, Wysocki M, Lofaso F, Conti G, Rauss A, et al. Noninvasive
ventilation for acute exacerbations of chronic obstructive pulmonary disease. N Engl J Med.
1995 Sep 28;333(13):817-22.
170. Lightowler JV WJ, Elliott MW, Ram FSF. Non-invasive positive pressure ventilation to
treat respiratory failure resulting from exacerbations of chronic obstructive pulmonary
disease: Cochrane systematic review and meta-analysis. . BMJ
2003;326(25).
171. Keenan SP, Sinuff T, Cook DJ, Hill NS. Which patients with acute exacerbation of
chronic obstructive pulmonary disease benefit from noninvasive positive-pressure ventilation?
A systematic review of the literature. Ann Intern Med. 2003 Jun 3;138(11):861-70.
172. Plant PK, Owen JL, Parrott S, Elliott MW. Cost effectiveness of ward based non-invasive
ventilation for acute exacerbations of chronic obstructive pulmonary disease: economic
analysis of randomised controlled trial. BMJ. 2003 May 3;326(7396):956.
173. Keenan SP, Powers CE, McCormack DG. Noninvasive positive-pressure ventilation in
patients with milder chronic obstructive pulmonary disease exacerbations: a randomized
controlled trial. Respir Care. 2005 May;50(5):610-6.
174. Confalonieri M, Garuti G, Cattaruzza MS, Osborn JF, Antonelli M, Conti G, et al. A chart
of failure risk for noninvasive ventilation in patients with COPD exacerbation. Eur Respir J.
2005 Feb;25(2):348-55.
175. Domenighetti G, Gayer R, Gentilini R. Noninvasive pressure support ventilation in non-
COPD patients with acute cardiogenic pulmonary edema and severe community-acquired
pneumonia: acute effects and outcome. Intensive Care Med. 2002 Sep;28(9):1226-32.
176. Masip J, Roque M, Sanchez B, Fernandez R, Subirana M, Exposito JA. Noninvasive
ventilation in acute cardiogenic pulmonary edema: systematic review and meta-analysis. Jama.
2005 Dec 28;294(24):3124-30.
177. Winck JC, Azevedo LF, Costa-Pereira A, Antonelli M, Wyatt JC. Efficacy and safety of
non-invasive ventilation in the treatment of acute cardiogenic pulmonary edema - a systematic
review and meta-analysis. Crit Care. 2006 Apr 28;10(2):R69.
178. Gray A, Goodacre S, Newby DE, Masson M, Sampson F, Nicholl J. Noninvasive
ventilation in acute cardiogenic pulmonary edema. N Engl J Med. 2008 Jul 10;359(2):142-51.
179. Bellone A, Vettorello M, Monari A, Cortellaro F, Coen D. Noninvasive pressure support
ventilation vs. continuous positive airway pressure in acute hypercapnic pulmonary edema.
Intensive Care Med. 2005 Jun;31(6):807-11.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
322 Miguel Ramalho do Souto Gonçalves

180. Kosowsky JM, Storrow AB, Carleton SC. Continuous and bilevel positive airway
pressure in the treatment of acute cardiogenic pulmonary edema. Am J Emerg Med. 2000
Jan;18(1):91-5.
181. Nava S, Carbone G, DiBattista N, Bellone A, Baiardi P, Cosentini R, et al. Noninvasive
ventilation in cardiogenic pulmonary edema: a multicenter randomized trial. Am J Respir Crit
Care Med. 2003 Dec 15;168(12):1432-7.
182. Antonelli M, Conti G, Rocco M, Bufi M, De Blasi RA, Vivino G, et al. A comparison of
noninvasive positive-pressure ventilation and conventional mechanical ventilation in patients
with acute respiratory failure. N Engl J Med. 1998 Aug 13;339(7):429-35.
183. Keenan SP, Sinuff T, Cook DJ, Hill NS. Does noninvasive positive pressure ventilation
improve outcome in acute hypoxemic respiratory failure? A systematic review. Crit Care Med.
2004 Dec;32(12):2516-23.
184. Antonelli M, Conti G, Esquinas A, Montini L, Maggiore SM, Bello G, et al. A multiple-
center survey on the use in clinical practice of noninvasive ventilation as a first-line
intervention for acute respiratory distress syndrome. Crit Care Med. 2007 Jan;35(1):18-25.
185. Antonelli M, Conti G, Bufi M, Costa MG, Lappa A, Rocco M, et al. Noninvasive
ventilation for treatment of acute respiratory failure in patients undergoing solid organ
transplantation: a randomized trial. Jama. 2000 Jan 12;283(2):235-41.
186. Hilbert G, Gruson D, Vargas F, Valentino R, Gbikpi-Benissan G, Dupon M, et al.
Noninvasive ventilation in immunosuppressed patients with pulmonary infiltrates, fever, and
acute respiratory failure. N Engl J Med. 2001 Feb 15;344(7):481-7.
187. Girou E. Prevention of nosocomial infections in acute respiratory failure patients. Eur
Respir J Suppl. 2003 Aug;42:72s-6s.
188. Simonds AK. Streamlining weaning: protocols and weaning units. Thorax. 2005
Mar;60(3):175-82.
189. Epstein SK, Ciubotaru RL, Wong JB. Effect of failed extubation on the outcome of
mechanical ventilation. Chest. 1997 Jul;112(1):186-92.
190. Nava S, Gregoretti C, Fanfulla F, Squadrone E, Grassi M, Carlucci A, et al. Noninvasive
ventilation to prevent respiratory failure after extubation in high-risk patients. Crit Care Med.
2005 Nov;33(11):2465-70.
191. Esteban A, Anzueto A, Alía I, Gordo F, Apezteguía C, Pálizas F, et al. How is mechanical
ventilation employed in the intensive care unit? An international utilization review. Am J Respir
Crit Care Med. 2000;161:1450-8.
192. Esteban A, Anzueto A, Frutos F, Alía I, Brochard L, Stewart TE, et al. Characteristics and
outcomes in adult patients receiving mechanical ventilation: a 28-day international study.
JAMA. 2002;287:345-55.
193. Confalonieri M, Gorini M, Ambrosino N, Mollica C, Corrado A, Scientific Group on
Respiratory Intensive Care of the Italian Association of Hospital Pneumonologists. Respiratory
intensive care units in Italy: a national census and prospective cohort study. Thorax.
2001;56:373-8.
194. Lloyd-Owen SJ, Donaldson GC, Ambrosino N, Escarabill J, Farre R, Fauroux B, et al.
Patterns of home mechanical ventilation use in Europe: results from the Eurovent survey. Eur
Respir J. 2005;25:1025-31.
195. Lightowler JV, Wedzicha JA, Elliott MW, Ram FS. Non-invasive positive pressure
ventilation to treat respiratory failure resulting from exacerbations of chronic obstructive
pulmonary disease: Cochrane systematic review and meta-analysis. BMJ. 2003;326(7382):185.
196. Martin TJ, Hovis JD, Costantino JP, Bierman MI, Donahoe MP, Rogers RM, et al. A
randomized, prospective evaluation of noninvasive ventilation for acute
respiratory failure. Am J Respir Crit Care Med. 2000;161(3 Pt 1):807-13.
197. Portier F, Defouilloy C, Muir JF. Determinants of immediate survival among chronic
respiratory insufficiency patients admitted to an intensive care unit for acute respiratory
failure. A
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 323

prospective multicenter study. The French Task Group for Acute Respiratory Failure in Chronic
Respiratory insufficiency. Chest. 1992;101:204-10.
198. Robino C, Faisy C, Diehl J-L, Labrousse J, Guerot E. Effectiveness of non-invasive
poritive pressure ventilatio differs between decompensated chronic restrictive and obstructive
pulmonary disease patients. Intensive Care Med. 2003;29:603-10.
199. Banfi P, Redolfi S, Robert D. Home treatment of infection-related acute respiratory
failure in kyphoscoliotic
patients on long-term mechanical ventilation. Respir Care. 2007;52:713-9.
200. Winck JC, Gonçalves M. Muscles and lungs: fatal attraction, but time for intervention.
Monaldi Arch Chest Dis. 2005;63:121-3.
201. Conti G, Rocco M, Antonelli M, Bufi M, Tarquini S, Lappa A, et al. Respiratory system
mechanics in the early phase of acute respiratory failure due to severe kyphoscoliosis.
Intensive Care Med. 1997;23:539-44.
202. Sawicka EH, Spencer GT, Branthwaite MA. Management of respiratory failure
complicating pregnancy in severe kyphoscoliosis: a new use for an old technique? Br J Dis
Chest. 1986;80:191-6.
203. Elliott MW, Steven MH, Phillips GD, Branthwaite MA. Non-invasive mechanical
ventilation for acute respiratory failure. BMJ. 1990 Feb 10;300(6721):358-60.
204. Benditt JO. The neuromuscular respiratory system: physiology, pathophysiology, and a
respiratory care approach to patients. Respir Care. 2006;51:829-37.
205. Poponick JM, Jacobs I, Supinski G, DiMarco AF. Effect of upper respiratory tract
infection in patients with neuromuscular disease. Am J Respir Crit Care Med. 1997;156(2 Pt
1):659-64.
206. Farrero E, Prats E, Povedano M, Martinez-Matos JA, Manresa F, Escarrabill J. Survival in
amyotrophic lateral sclerosis with home mechanical ventilation: the impact of systematic
respiratory assessment and bulbar involvement. Chest. 2005;127:2132-8.
207. Bach JR, Ishikawa Y, Kim H. Prevention of pulmonary morbidity for patients with
Duchenne muscular dystrophy. Chest. 1997;112:1024-8.
208. Chen R, Grand'Masoin F, M.J. S, Ramsay DA, Bolton CF. Motor neuron disease
presenting as acute respiratory failure: a clinical and pathological study. J Neurol Neurosurg
Psychiatry. 1996;60:455-8.
209. de Carvalho M, Matias T, Coelho F, Evangelista T, Pinto A, Luís ML. Motor neuron
disease presenting with respiratory failure. J Neurol Sci. 1996;Aug;139 Suppl:117-22.
210. Lechtzin N, Wiener CM, Clawson L, Chaudhry V, Diette GB. Hospitalization in
amyotrophic lateral sclerosis: causes, costs, and outcomes. Neurology. 2001;56:753-7.
211. Bradley MD, Orrell RW, Clarke J, Davidson AC, Williams AJ, Kullmann DM, et al.
Outcome of ventilatory support for acute respiratory failure in motor neurone
disease. J Neurol Neurosurg Psychiatry. 2002;72:752-6.
212. Bach JR. Management of patients with neuromuscular disease. Philadelphia: Hanley &
Belfus; 2004.
213. Goncalves MR, Bach JR. Mechanical Insufflation-exsufflation improves outcomes for
Neuromuscular disease patients with repiratory tract infections. Am J Phys Med Rehabil.
2005;84:89-91.
214. Gonçalves MR, Winck JC, Nadais G, Almeida J, Marques JA. Acute respiratory failure in
Amyotophic lateral sclerosis: management with non-invasive respiratory aids. Eur Respir J.
2004;24 (Suppl 48):314s.
215. Vianello A, Bevilacqua M, Arcaro G, Gallan F, Serra E. Non-invasive ventilatory
approach to treatment of acute respiratory failure in neuromuscular disorders. A comparison
with endotracheal intubation. Intensive Care Med. 2000;26:384-90.
216. Vianello A, Corrado A, Arcaro G, Gallan F, Ori C, Minuzzo M, et al. Mechanical
insufflation-exsufflation improves outcomes for neuromuscular disease
patients with respiratory tract infections. Am J Phys Med Rehabil. 2005;84:83-8.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
324 Miguel Ramalho do Souto Gonçalves

217. Sancho J, Servera E, Marín J, Vergara P, Belda FJ, Bach JR. Effect of lung mechanics on
mechanically assisted flows and volumes. Am J Phys Med Rehabil. 2004;83:698-703.
218. Bach JR. Update and perspective on noninvasive respiratory muscle aids. Part 2: The
expiratory aids. Chest. 1994;105:1538-44.
219. Winck JC, Goncalves MR, Lourenco C, Viana P, Almeida J, Bach JR. Effects of mechanical
insufflation-exsufflation on respiratory parameters for patients with chronic airway secretion
encumbrance. Chest. 2004;126:774-80.
220. Servera E, Sancho J, Gomez-Merino E, Briones ML, Vergara P, Pérez D, et al. Non-
invasive management of an acute chest infection for a patient with ALS. J Neurol Sci.
2003;209:111-3.
221. Bach JR, Bianchi C, Aufiero E. Oximetry and indications for tracheotomy for
amyotrophic lateral sclerosis. Chest. 2004;126:1502-7.
222. Vianello A, Bevilacqua M, Arcaro G, Serra E. Prevention of pulmonary morbidity in
patients with neuromuscular disorders: a possible role for permanent cricothyroid
minitracheostomy. Chest. 1998;114:346-7.
223. Hanayama K, Ishikawa Y, Bach JR. Amyotrophic lateral sclerosis. Successful treatment
of mucous plugging by
mechanical insufflation-exsufflation. Am J Phys Med Rehabil. 1997;76:338-9.
224. Bach JR. Amyotrophic lateral sclerosis:predictors for prolongation of life by noninvasive
respiratory aids. Arch Phys Med Rehabil. 1995;76:828-32.
225. Oppenheimer EA. Treating respiratory failure in ALS: the details are becoming clearer. J
Neurol Sci. 2003;209:1-4.
226. Pearse RM, Draper A, Grounds RM. Non-invasive ventilation to avoid tracheal
intubation in a patient with Guillain-Barré syndrome. Br J Anaesth. 2003;91:913-6.
227. Seneviratne J, Mandrekar J, Wijdicks EF, Rabinstein AA. Noninvasive ventilation in
myasthenic crisis. Arch Neurol. 2008;65:54-8.
228. Agarwal R, Reddy C, Gupta D. Noninvasive ventilation in acute neuromuscular
respiratory failure due to myasthenic crisis: case report and review of literature. Emerg Med J.
2006;23:e6.
229. Hughes RA, Wijdicks EF, Benson E, Cornblath DR, Hahn AF, Meythaler JM, et al.
Supportive care for patients with Guillain-Barré syndrome. Arch Neurol. 2005;62:1194-8.
230. Mehta S. Neuromuscular disease causing acute respiratory failure. Respir Care.
2006;51:1016-21.
231. Lawn ND, Fletcher DD, Henderson RD, Wolter TD, Wijdicks EF. Anticipating mechanical
ventilation in Guillain-Barré syndrome. Arch Neurol. 2001;58:893-8.
232. Jackson AB, Dijkers M, DeVivo MJ, R.B. P. A demographic profile of new traumatic
spinal cord injuries: change and stability over 30 years. Arch Phys Med Rehabil. 2004;85:1740-
8.
233. Mansel JK, Norman JR. Respiratory complications and management of spinal cord
injuries. Chest. 1990;97:1146-52.
234. Cardenas DD, Hoffman JM, Kirshblum S, McKinley W. Etiology and incidence of
rehospitalization after traumatic spinal cord injury: a multicenter analysis. Arch Phys Med
Rehabil. 2004;85:1757-63.
235. Splaingard ML, Frates RC, Harrison GM, Carter RE, Jefferson LS. Home positive-
pressure ventilation-twenty years' experience. Chest. 1983;84:376-82.
236. Wicks AB, Menter RR. Long-term outlook in quadriplegic patients with initial ventilator
dependecy. Chest. 1986;90:406-10.
237. DeVivo MJ, Ivie CS. Life expectancy of ventilator dependent persons with spinal cord
injuries. Chest. 1995;108:226-32.
238. Bach JR, Alba A. Noninvasive options for ventilatory support of the traumatic high level
quadriplegic patients. Chest. 1990;98:613-9.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 325
239. Bach JR. Continuous noninvasive ventilation for patients with neuromuscular disease
and spinal cord injury. Semin Respir Crit Care Med. 2002;23:283-92.
240. Bach JR, Hunt D, Horton JA. Traumatic tetraplegia: noninvasive respiratory
management in the acute setting. Am J Phys Med Rehabil. 2002;81:792-7.
241. Bach JR, Goncalves M. Ventilator weaning by lung expansion and decannulation. Am J
Phys Med Rehabil. 2004;83:560-8.
242. De Jonghe B, Sharshar T, Lefaucheur JP, Authier FJ, Durand-Zaleski I, Boussarsar M, et
al. Paresis acquired in the intensive care unit: a prospective multicenter study. JAMA.
2002(288):2859-67.
243. Deem S. Intensive-care-unit-acquired muscle weakness. Respir Care. 2006;51:1042-52.
244. Latronico N, Guarneri B, Alongi S, Bussi G, Candiani A. Acute neuromuscular respiratory
failure after ICU discharge. Report of five patients. Intensive Care Med. 1999;25:1302-6.
245. Servera E, Sancho J, Zafra MJ, Marin J. Secretion management must be considered
when reporting success or failure of noninvasive ventilation. Chest. 2003 May;123(5):1773;
author reply -4.
246. Vianello A, Corrado A, Arcaro G, Gallan F, Ori C, Minuzzo M, et al. Mechanical
insufflation-exsufflation improves outcomes for neuromuscular disease patients with
respiratory tract infections. Am J Phys Med Rehabil. 2005 Feb;84(2):83-8; discussion 9-91.
247. Elliott M, Ambrosino N. Noninvasive ventilation: a decade of progress. Eur Respir J.
2002 Apr;19(4):587-9.
248. Lloyd-Owen SJ, Donaldson GC, Ambrosino N, Escarabill J, Farre R, Fauroux B, et al.
Patterns of home mechanical ventilation use in Europe: results from the Eurovent survey. Eur
Respir J. 2005 Jun;25(6):1025-31.
249. Winck J, Simonds AK. Indications, Definitions, Guidelines and Outcomes in Restriction
and Obstruction. In: Ventilatory Support for Chronic Respiratory Failure; Ed: N Ambrosino & R
Goldstein ,
Informa healthcare. 2008;Part V. Long term mechanical ventilation in the community (Chapter
19).
250. Aldrich TK. The patient at risk of ventilatory dependecy. Eur Respir J. 1989;Suppl
7:645s-51s.
251. McNicholas WT. Impact of sleep in COPD. Chest. 2000;117:48s-53s.
252. Anonymous. Clinical indications for noninvasive positive pressure ventilation in chronic
respiratory failure due to restrictive lung disease, COPD, and nocturnal
hypoventilation--a consensus conference report. Chest. 1999;116:521-34.
253. Nava S, Barbarito N, Piaggi G, De Mattia E, Cirio S. Physiological response to
intrapulmonary percussive ventilation in stable COPD patients. Respir Med. 2006;100:1526-33.
254. Vargas F, Bui HN, Boyer A, Salmi LR, Gbikpi-Benissan G, Guenard H, et al.
Intrapulmonary percussive ventilation in acute exacerbations of COPD patients with mild
respiratory acidosis: a randomized controlled trial[ISRCTN17802078]. Crit Care. 2005;9:R382-9.
255. Fletcher DD, Lawn ND, Wolter TD, Wijdicks EFM. Long-term outcome in patients with
Guillain-Barré syndrome requiring mechanical ventilation. Neurology. 2000;54:2311-15.
256. Miller RG, Rosenberg JA, Gelinas DF, Mitsumoto H, Newman D, Sufit R, et al. Practice
parameter: the care of the patient with amyotrophic lateral sclerosis (an evidence-based
review): report of the Quality Standards Subcommittee of the American Academy of
Neurology: ALS Practice Parameters Task Force. Neurology. 1999;52:1311-23.
257. Rutgers M, Lucassen H, Kesteren RV, Leger P. Respiratory insufficiency and ventilatory
support. 39th ENMC International Workshop, Naarden, The Netherlands, 26-28 January 1996.
European Consortium on Chronic Respiratory Insufficiency. Neuromuscul Disord. 1996;6:431-5.
258. Wallgren-Pettersson C, Bushby K, Mellies U, Simonds A, ENMC. 117th ENMC workshop:
ventilatory support in congenital neuromuscular disorders - congenital myopathies, congenital
muscular dystrophies, congenital myotonic dystrophy and SMA (II) 4-6 April 2003, Naarden,
The Netherlands. Neuromuscul Disord. 2004;14:56-69.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
326 Miguel Ramalho do Souto Gonçalves

259. Leigh PN, Abrahams S, Al-Chalabi A, Ampong MA, Goldstein LH, Johnson J, et al. The
management of motor neurone disease. J Neurol Neurosurg Psychiatry. 2003;74 Suppl 4:iv32-
iv47.
260. Jackson CE, Rosenfeld J, Moore DH, Bryan WW, Barohn RJ, Wrench M, et al. A
preliminary evaluation of a prospective study of pulmonary function studies and symptoms of
hypoventilation in ALS/MND patients. J Neurol Sci. 2001;191:75-8.
261. Butz M, Wollinsky KH, Wiedemuth-Catrinescu U, Sperfeld A, Winter S, Mehrkens HH, et
al. Longitudinal effects of noninvasive positive-pressure ventilation in patients with
amyotrophic lateral sclerosis. Am J Phys Med Rehabil. 2003;82:597-604.
262. Mellies U, Ragette R, Schwake C, Boehm H, Voit T, Teschler H. Daytime predictors of
sleep disordered breathing in children and adolescents with neuromuscular disorders.
Neuromuscul Disord. 2003;13:123-8.
263. Jackson CE, Lovitt S, Gowda N, Anderson F, Miller RG, The ALS care study group.
Factors correlated with NPPV use in ALS. Amyothophic Lateral Sclerosis. 2006;7:80-5.
264. Dougan CF, Connell CO, Thornton E, Young CA. Development of a patient-specific
dyspnoea questionnaire in motor neurone disease (MND): the MND dyspnoea rating scale
(MDRS). J Neurol Sci. 2000;180:86-93.
265. Medical Research Council. Committee on research into chronic bronchitis. Instructions
for use of the questionnaire on respiratory symptoms. In: Devon LW, editor. Holman1966.
266. Laberge L, Gagnon C, Jean S, Mathieu J. Fatigue and daytime sleepiness rating scales in
myotonic dystrophy: a study of reliability. J Neurol Neurosurg Psychiatry. 2005;76:1403-5.
267. Shahrizaila N, Kinnear WJM, Wills AJ. Respiratory involvement in inherited primary
muscle conditions. J Neurol Neurosurg Psychiatry. 2006;2006(77):1108-115.
268. Anonymous. ATS/ERS statement on Respiratory Muscle Testing. Am J Respir Crit Care
Med. 2002;166:518-624.
269. Gozal D. Pulmonary manifestations of neuromuscular disease with special reference to
Duchenne muscular dystrophy and spinal muscular atrophy. Pediatr Pulmonol. 2000;29:141-
50.
270. Varrato J, Siderowf A, Damiano P, Gregory S, Feinberg D, McCluskey L. Postural change
of forced vital capacity predicts some respiratory symptoms in ALS. Neurology. 2001;57:357-9.
271. Lechtzin N, Wiener CM, Shade DM, Clawson L, Diette GB. Spirometry in the supine
position improves the detection of diaphragmatic weakness in patients with amyotrophic
lateral sclerosis. Chest. 2002;121:436-42.
272. Fitting J-W, Paillex R, Hirt L, Aebischer P, Schluep M. Sniff nasal pressure: a sensitive
respiratory test to assess progression of amyotrophic lateral sclerosis. Ann Neurol. 1999;
46:887-93.
273. Morgan RK, McNally S, Alexander M, Conroy R, Hardiman O, Costello RW. Use of Sniff
nasal-inspiratory force to predict survival in amyotrophic lateral sclerosis. Am J Respir Crit Care
Med. 2005;171:269-74.
274. Chaudri MB, Liu C, Watson L, Jefferson D, Kinnear WJ. Sniff nasal inspiratory pressure
as a marker of respiratory function in motor neuron disease. Eur Respir J. 2000;15:539-42.
275. Hart N, Polkey MI, Sharshar T, Falaize L, Fauroux B, Raphael JC, et al. Limitations of sniff
nasal pressure in patients with severe neuromuscular weakness. J Neurol Neurosurg
Psychiatry. 2003;74:1685-7.
276. Perrin C, Unterborn JN, Ambrosio CD, Hill NS. Pulmonary complications in
Neuromuscular Diseases. Muscle & Nerve. 2004;29:5-27.
277. ATS Consensus Statement. Respiratory Care of the patients with Duchenne Muscular
Dystrophy. Am J Respir Crit Care Med. 2004(170):456-65.
278. Takano Y, Sakamoto O, Kiyofuji C, Ito K. A comparison of the end-tidal CO2 measured
by portable capnometer and the arterial PCO2 in spontaneously breathing patients. Respir
Med. 2003;97:476-81.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 327

279. Kotterba S, Patzold T, Malin JP, Orth M, Rasche K. Respiratory monitoring in
neuromuscular disease - capnography as an additional tool? Clin Neurol Neurosurg.
2001;103:87-91.
280. Pradal U, Braggion C, Mastella G. Transcutaneous blood gas analysis during sleep and
exercise in cystic fibrosis. Pediatr Pulmonol. 1990;8:162-7.
281. Janssens JP, Perrin E, Bennani I, de Muralt B, Titelion V, Picaud C. Is continuous
transcutaneous monitoring of PCO2 (TcPCO2) over 8 h reliable in adults? Respir Med.
2001;95:331-5.
282. Janssens JP, Howarth-Frey C, Chevrolet JC, Abajo B, Rochat T. Transcutaneous PCO2 to
monitor Noninvasive mechanical ventilation in adults. Assessment of a new transcutaneous
PCO2 device. Chest. 1998;113:768-73.
283. Aittokallio J, Virkki A, Aittokallio T, Saaresranta T, Polo-Kantola P, Polo O. Non-invasive
respiratory monitoring during wakefulness and sleep in pre- and
postmenopausal women. Respir Physiol Neurobiol. 2006;150:66-74.
284. Morielli A, Desjardins D, Brouillette RT. Transcutaneous and end-tidal carbon dioxide
pressures should be measured during pediatric polysomnography. Am Rev Respir Dis.
1993;148:1599-604.
285. Cuvelier A, Grigoriu B, Molano LC, Muir JF. Limitations of transcutaneous carbon
dioxide measurements for assessing long-term mechanical ventilation. Chest. 2005;127:1744-
8.
286. Heuss LT, Chhajed PN, Schnieper P, Hirt T, Beglinger C. Combined pulse
oximetry/cutaneous carbon dioxide tension monitoring during colonoscopies: pilot study with
a smart ear clip. Digestion. 2004;70:152-8.
287. Bendjelid K, Schutz N, Stotz M, Gerard I, Sutter PM, Romand J-A. Transcutaneous PCO2
monitoring in critically ill adults: clinical evaluation of a new sensor. Crit Care Med.
2005;33:2203-6.
288. Senn O, Clarenbach CF, Kaplan V, Maggiorini M, Bloch KE. Monitoring Carbon Dioxide
Tension and arterial oxygen saturation by a single earlobe sensor in patients with critical illness
or sleep apnea. Chest. 2005;128:1291-6.
289. Leger P, Bedicam JM, Cornette A, Reybet-Degat O, Langevin B, Polu JM, et al. Nasal
intermittent positive pressure ventilation. Long-term follow-up in patients with severe chronic
respiratory insufficiency. Chest. 1994 Jan;105(1):100-5.
290. Elliott MW, Simonds AK, Carroll MP, Wedzicha JA, Branthwaite MA. Domiciliary
nocturnal nasal intermittent positive pressure ventilation in hypercapnic respiratory failure
due to chronic obstructive lung disease: effects on sleep and quality of life. Thorax. 1992
May;47(5):342-8.
291. Sivasothy P, Smith IE, Shneerson JM. Mask intermittent positive pressure ventilation in
chronic hypercapnic respiratory failure due to chronic obstructive pulmonary disease. Eur
Respir J. 1998 Jan;11(1):34-40.
292. Jones SE, Packham S, Hebden M, Smith AP. Domiciliary nocturnal intermittent positive
pressure ventilation in patients with respiratory failure due to severe COPD: long-term follow
up and effect on survival. Thorax. 1998;53:495-8.
293. Meecham Jones DJ, Paul EA, Jones PW, Wedzicha JA. Nasal pressure support
ventilation plus oxygen compared with oxygen therapy alone in hypercapnic COPD. Am J
Respir Crit Care Med. 1995 Aug;152(2):538-44.
294. Lin CC. Comparison between nocturnal nasal positive pressure ventilation combined
with oxygen therapy and oxygen monotherapy in patients with severe COPD. Am J Respir Crit
Care Med. 1996;154:353-8.
295. Strumpf DA, Millman RP, Carlisle CC, Grattan LM, Ryan SM, Erickson AD, et al.
Nocturnal positive-pressure ventilation via nasal mask in patients with severe chronic
obstructive pulmonary disease. Am Rev Respir Dis. 1991;144:1234-9.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
328 Miguel Ramalho do Souto Gonçalves

296. Gay PC, Hubmayr RD, Stroetz RW. Efficacy of nocturnal nasal ventilation in stable,
severe chronic obstructive pulmonary disease during a 3-month controlled trial. Mayo Clin
Proc. 1996;71:533-42.
297. Casanova C, Celli BR, Tost L, Soriano E, Abreu J, Velasco V, et al. Long-term controlled
trial of nocturnal nasal positive pressure ventilation in patients with severe COPD. Chest.
2000;118:1582-90.
298. Clini E, Sturani C, Rossi A, Viaggi S, Corrado A, Donner CF, et al. The Italian multicentre
study on noninvasive ventilation in chronic obstructive
pulmonary disease patients. Eur Respir J. 2002;20:529-38.
299. Tuggey JM, Plant PK, Elliott MW. Domiciliary non-invasive ventilation for recurrent
acidotic exacerbations of COPD: an economic analysis. Thorax. 2003;58:867-71.
300. Bergofsky FH. Respiratory failure in disorders of the thoracic cage. Am Rev Respir Dis.
1979;119:643-69.
301. Pehrsson K, Bake B, Larsson S, Nachemson A. Lung Function in adult idiopathic
scoliosis: a 20 year follow up. Thorax. 1991;46:474-8.
302. Rom WN, Miller A. Unexpected longevity in patients with severe kyphoscoliosis.
Thorax. 1978;33:106-10.
303. Guilleminault C, Kurland G, Winkle R, Miles LE. Severe kyphoscoliosis, breathing and
sleep. The Quasimodo syndrome during sleep. Chest. 1981;79:626-30.
304. Gonzalez C, Ferris G, Diaz J, Fontana I, Nuñez J, Marin J. Kyphoscoliotic ventilatory
insufficiency. Effects of Long-term intermittent positive-pressure ventilation. Chest.
2003;124:857-62.
305. Ferris G, Servera-Pieras E, Vergara P, Tzeng AC, Perez M, Marin J, et al. Kyphoscoliosis
Ventilatory Insufficiency: noninvasive management outcomes. Am J Phys Med Rehabil.
2000;79:24-9.
306. Fuschillo S, De Felice A, Gaudiosi C, Balzano G. Nocturnal mechanical ventilation
improves exercise capacity in kyphoscoliotic patients with respiratory impairment. Monaldi
Arch Chest Dis. 2003 Oct-Dec;59(4):281-6.
307. Chailleux E, Farroux B, Binet F, Dautzenberg B, Polu JM. Predictors of survival in
patients receiving domiciliary oxygen therapy of mechanical ventilation. A 10 year analysis of
ANTADIR observatory. Chest. 1996;109:741-9.
308. Gustafson T, Franklin KA, Midgren B, Pehrsson K, Ranstam J, Strom K. Survival of
patients with kyphoscoliosis receiving mechanical ventilation or oxygen at home. Chest.
2006;130:1828-33.
309. Masa JF, Celli BR, Riesco JA, Sanchez de Cos J, Disdier C, Sojo A. Noninvasive positive
pressure ventilation and not oxygen may prevent overt ventilatory failure in patients with
chest wall diseases. Chest. 1997 Jul;112(1):207-13.
310. Andersen PM, Borasio GD, Dengler R, Hardiman O, Kollewe K, Leigh PN, et al. EFNS task
force on management of amyotrophic lateral sclerosis: guidelines for diagnosing and clinical
care of patients and relatives. Eur J Neurol. 2005;12:921-38.
311. Bourke SC, Bullock RE, Williams TL, Shaw PJ, Gibson GJ. Noninvasive ventilation in
ALS.Indications and effect on quality of life. Neurology. 2003;61:171-7.
312. Bourke SC, Tomlison M, Williams TL, Bullock RE, Shaw PJ, Gibson GJ. Effects of non-
invasive ventilation on survival and quality of life in patients with amyotophic lateral sclerosis:
a randomised controlled trial. Lancet Neurol. 2006;5:140-7.
313. Oppenheimer EA. Amyotrophic lateral sclerosis. Eur Respir Rev. 1992;2:323-9.
314. Cazzolli PA, Oppenheimer EA. Home mechanical ventilation for amyotrophic lateral
sclerosis: nasal compared to tracheostomy-intermittent positive pressure ventilation. J Neurol
Sci. 1996 Aug;139 Suppl:123-8.
315. Sivak ED, Shefner JM, Mitsumoto H, Taft JM. The use of non-invasive positive pressure
ventilation (NIPPV) in ALS patients. A need for imporved determination of intervention timing.
ALS. 2001;2:139-45.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 329

316. Bach JR. Amyotrophic Lateral Sclerosis. Prolongation of life by noninvasive respiratory
aids. Chest. 2002;122:92-8.
317. del Aguila MA, Longstreth WT, McGuire V, Koepsell TD, Van Belle G. Prognosis in
amyotrophic lateral sclerosis. Neurology. 2003;60:813-9.
318. Aboussouan LS, Khan SU, Meeker DP, Stelmach K, Mitsumoto H. Effect of Noninvasive
Positive -Pressure Ventilation on survival in Amyotrophic Lateral Sclerosis. Ann Intern Med.
1997;127:450-3.
319. Gruis KL, Brown DL, Schoennemann A, Zebarah VA, Feldman EL. Predictors of
Noninvasive ventilation tolerance in patients with amyotrophic lateral sclerosis. Muscle &
Nerve. 2005;32:808-11.
320. Cederbaum JM, Stambler N. Performance of the Amyotrophic Lateral Sclerosis
Functional Rating Scale (ALSFRS) in multicentre clinical trials. J Neurol Sci. 1997;152:51-9.
321. Kang SW, Bach JR. Maximum insufflation capacity: vital capacity and cough flows in
neuromuscular disease. Am J Phys Med Rehabil. 2000;79:222-7.
322. Suarez AA, Pessolano FA, Monteiro SG, Ferreyra G, Capria ME, Mesa L, et al. Peak flow
and peak cough flow in the evaluation of expiratory muscle weakness and bulbar impairment
in patients with neuromuscular disease. Am J Phys Med Rehabil. 2002;81:506-11.
323. Morton NE, Chung CS. Formal genetics of muscular dystrophy. Am J Hum Genet.
1959;11:360-79.
324. Baydur A, Gilgoff I, Prentice W, Carlson M, Fischer DA. Decline in respiratory function
and experience with longterm assisted ventilation in advanced duchenne's muscular
dystrophy. Chest. 1990;97:884-9.
325. Hukins CA, Hillman DR. Daytime predictors of sleep hypoventilation in Duchenne
muscular dystrophy. Am J Respir Crit Care Med. 2000;161:166-70.
326. Hahn A, Bach JR, Delaubier A, Renardel-Irani A, Guillou C, Rideau Y. Clinical implications
of maximal respiratory pressure dterminations for individuals with duchenne muscular
dystrophy. Arch Phys Med Rehabil. 1997;78:1-6.
327. Khan Y, Heckmatt JZ. Obstructive apnoeas in Duchenne muscular dystrophy. Thorax.
1994;49:157-61.
328. Suresh S, Wales P, Dakin C, Harris MA, Cooper DG. Sleep-related breathing disorder in
Duchenne muscular dystrophy: disease spectrum in the paediatric population. J Paediatr Child
Health. 2005;41:500-3.
329. Vianello A, Bevilacqua M, Salvador V, Cardaioli C, Vincenti E. Long-term nasal
intermittent positive pressure ventilation in advanced Duchenne's muscular dystrophy. Chest.
1994 Feb;105(2):445-8.
330. Curran FJ, Colbert AP. Ventilator management in Duchenne muscular dystrophy and
postpoliomyelitis syndrome: twelve years' experience. Arch Phys Med Rehabil. 1989;70:180-5.
331. Raphael JC, Chevret S, Chastang C, Bouvet F. Randomised trial of preventive nasal
ventilation in Duchenne muscular dystrophy. French Multicentre Cooperative Group on Home
Mechanical Ventilation Assistance in Duchenne de Boulogne Muscular Dystrophy. Lancet. 1994
Jun 25;343(8913):1600-4.
332. Muntoni F, Hird M, Simonds AK. Preventive nasal ventilation in Duchenne muscular
dystrophy. Lancet. 1994;344:340.
333. Phillips MF, Quinlivan RCM, Edwards RHT, Calverley PM. Changes in spirometry over
time as a prognostic marker in patients with Duchenne Muscular Dystrophy. Am J Respir Crit
Care Med. 2001;164:2191-4.
334. Ward S, Chatwin M, Heather S, Simonds AK. Randomised controlled trial of non-
invasive ventilation (NIV) for nocturnal hypoventilation in neuromuscular and chest wall
disease patients with daytime normocapnia. Thorax. 2005;60:1019-24.
335. Toussaint M, Steens M, Wasteels G, Soudon P. Diurnal ventilation via mouthpiece:
survival in end-stage Duchenne patients. Eur Respir J. 2006;28:549-55.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
330 Miguel Ramalho do Souto Gonçalves

336. Mellies U, Ragette R, Dohna Schwake C, Boehm H, Voit T, Teschler H. Long-term
noninvasive ventilation in children and adolescents with neuromuscular disorders. Eur Respir J.
2003;22:631-6.
337. Alba A, Solomon M, Trainor FS, editors. Management of respiratory insufficiency in
spinal cord lesions. Proceedings of the 17th Veteran's Administration spinal cord injury
conference, 1969; 1971: US Go 0-436-398vernment Printing Office.
338. Bach JR, Alba AS, Bohatiuk G, Saporito L, Lee M. Mouth intermittent positive pressure
ventilation in the management of postpolio respiratory insufficiency. Chest. 1987;91:859-64.
339. Bach JR, Alba AS. Sleep and nocturnal mouthpiece IPPV efficiency in postpoliomyelitis
ventilator users. Chest. 1994;106:1705-10.
340. Bach JR, S.M. S, Saporito LR. Interfaces for non-invasive intermittent positive pressure
ventilatory support in North America. Eur Respir Rev. 1993;3:254-9.
341. Baydur A, Gilgoff I, Prentice W, Carlson M, Fischer DA. Decline in respiratory function
and experience with long-term assisted ventilation in advanced Duchenne's muscular
dystrophy. Chest. 1990;97:884-9.
342. Baydur A, Layne E, Aral H, Krishnareddy N, Topacio R, Frederick G, et al. Long term
non-invasive ventilation in the community for patients with musculoskeletal disorders: 46 year
experience and review. Thorax. 2000 Jan;55(1):4-11.
343. Boitano LJ, Benditt JO. An evaluation of home volume ventilators that support open-
circuit mouthpiece ventilation. Respir Care. 2005;50:1457-61.
344. McKim DA, LeBlanc C. Maintaning an «Oral Tradition»: specific equipment
requirements for mouthpiece ventilation instead of tracheostomy for Neuromuscular Disease.
Respir Care. 2006;51:297-8.
345. Robert D, Willig TN, Leger P, Paulus J. Long-term nasal ventilation in neuromuscular
disorders: report of a consensus conference. Eur Respir J. 1993;6:599-606.
346. Ishikawa Y, Bach JR, Minami R. Cardioprotection for Duchenne Muscular Dystrophy.
Am Heart J. 1999;137:895-902.
347. Kohler M, Clarenbach CF, Boni L, Brack T, Russi EW, Bloch KE. Quality of life, physical
disability, and respiratory impairment in Duchenne muscular dystrophy. Am J Respir Crit Care
Med. 2005;172:1032-6.
348. Rubin BK. Physiology of airway mucus clearance. Respir Care. 2002 Jul;47(7):761-8.
349. Pryor JA. Physiotherapy for airway clearance in adults. Eur Respir J. 1999
Dec;14(6):1418-24.
350. Zahm JM, King M, Duvivier C, Pierrot D, Girod S, Puchelle E. Role of simulated
repetitive coughing in mucus clearance. Eur Respir J. 1991 Mar;4(3):311-5.
351. McCool FD, Rosen MJ. Nonpharmacologic airway clearance therapies: ACCP evidence-
based clinical practice guidelines. Chest. 2006 Jan;129(1 Suppl):250S-9S.
352. van der Schans CP, Postma DS, Koeter GH, Rubin BK. Physiotherapy and bronchial
mucus transport. Eur Respir J. 1999 Jun;13(6):1477-86.
353. Van der Schans C, Bach J, Rubin BK. Chest Physical Therapy: Mucus-mobilization
Techniques. in: Bach JR, ed Noninvasive mechanical ventilation. 2002;1st edition(Philadelphia:
Hanley&Belfus, Inc):259 - 84.
354. Bach JR. Prevention of morbidity and mortality with the use of physical medicine aids:
The obstructive and paralytic conditions. In: Bach JR, editor. Pulmonary Rehabilitation,.
Philadelphia, PA: Hanley & Belfus, Inc; 1996. p. 303-29.
355. Gomez-Merino E, Bach JR. Duchenne muscular dystrophy: prolongation of life by
noninvasive respiratory muscle aids. Am J Phys Med Rehabil. 2002;81:411-5.
356. Tzeng AC, Bach JR. Prevention of Pulmonary Morbidity for patients with
neurosmucular disease. Chest. 2000;118,:1390-6.
357. Templeton M, Palazzo MG. Chest physiotherapy prolongs duration of ventilation in the
critically ill ventilated for more than 48 hours. Intensive Care Med. 2007 Nov;33(11):1938-45.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 331

358. Bach JR, Saporito LR. Criteria for extubation and tracheostomy tube removal for
patients with ventilatory failure. A different approach to weaning. Chest. 1996
Dec;110(6):1566-71.
359. King M. Physiology of mucus clearance. Paediatr Respir Rev. 2006;7 Suppl 1:S212-4.
360. Pryor JA, Webber BA, Hodson ME. Effect of chest physiotherapy on oxygen saturation
in patients with cystic fibrosis. Thorax. 1990 Jan;45(1):77.
361. Poponick JM, Jacobs I, Supinski G, DiMarco AF. Effect of upper respiratory tract
infection in patients with neuromuscular disease. Am J Respir Crit Care Med. 1997 Aug;156(2
Pt 1):659-64.
362. Kang SW, Bach JR. Maximum insufflation capacity. Chest. 2000 Jul;118(1):61-5.
363. Servera E, Sancho J, Zafra MJ. [Cough and neuromuscular diseases. Noninvasive airway
secretion management]. Arch Bronconeumol. 2003 Sep;39(9):418-27.
364. Kang SW, Bach JR. Maximum insufflation capacity: vital capacity and cough flows in
neuromuscular disease. Am J Phys Med Rehabil. 2000 May-Jun;79(3):222-7.
365. Sancho J, Servera E, Marin J, Vergara P, Belda FJ, Bach JR. Effect of lung mechanics on
mechanically assisted flows and volumes. Am J Phys Med Rehabil. 2004 Sep;83(9):698-703.
366. Bach JR, Goncalves MR, Paez S, Winck JC, Leitao S, Abreu P. Expiratory flow maneuvers
in patients with neuromuscular diseases. Am J Phys Med Rehabil. 2006 Feb;85(2):105-11.
367. Plant PK, Owen JL, Elliot MW. Non-invasive ventilation in acute exacerbations of
chronic obstructive pulmonary disease: long term survival and predictors of in-hospital
outcome. Thorax. 2001;56:708-12.
368. van der Schans CP, Piers DA, Beekhuis H, Koeter GH, van der Mark TW, Postma DS.
Effect of forced expirations on mucus clearance in patients with chronic airflow obstruction:
effect of lung recoil pressure. Thorax. 1990 Aug;45(8):623-7.
369. Jones AP, Rowe BH. Bronchopulmonary hygiene physical therapy for chronic
obstructive pulmonary disease and bronchiectasis. Cochrane Database Syst Rev.
2000(2):CD000045.
370. Wolmer P, Ursing K, Midgren B, Eriksson L. Ineficiency of chest percussion in the
physical therapy of chronic bronchitis. Eur J Respir Dis. 1985(66):233-9.
371. Bach PB, Brown C, Gelfand SE, McCrory DC. Management of acute exacerbations of
chronic obstructive pulmonary disease: a summary and appraisal of published evidence. Ann
Intern Med. 2001 Apr 3;134(7):600-20.
372. Hubert J. Mobilisations du Thorax. Les edicions Medicales et Paramedicales de
Charleroi, Montignies-sur-Sambre, Belgium. 1989.
373. Bach JR, Ishikawa Y, Kim H. Prevention of the pulmonary morbidity for patients with
Duchenne Muscular Dystrophy. Chest. 1997;112:1024-8.
374. Sivasothy P, Brown L, Smith IE, Shneerson JM. Effects of manually assisted cough and
mechanical insufflation on cough flow of normal subjects, patients with chronic obstructive
pulmonary disease (COPD), and patients with respiratory muscle weakness. Thorax.
2001;56:438-44.
375. Bach JR. Mechanical lnsufflation-Exsufflation: Comparison of peak expiratory flows
with manually assisted and unassisted coughing techniques. Chest. 1993;104:1553-62.
376. Bach JR. Don't forget the abdominal thrust. Chest. 2004 Oct;126(4):1388-9; author
reply 9-90.
377. Bach JR, Chaudhry SS. Standards of care in MDA clinics. Muscular Dystrophy
Association. Am J Phys Med Rehabil. 2000 Mar-Apr;79(2):193-6.
378. Toussaint M, De Win H, Steens M, Soudon P. Effect of intrapulmonary percussive
ventilation on mucus clearance in duchenne muscular dystrophy patients: a preliminary report.
Respir Care. 2003 Oct;48(10):940-7.
379. Hess DR. The evidence for secretion clearance techniques. Respir Care. 2001
Nov;46(11):1276-93.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
332 Miguel Ramalho do Souto Gonçalves
380. Langenderfer B. Alternatives to percussion and postural drainage. A review of mucus
clearance therapies: percussion and postural drainage, autogenic drainage, positive expiratory
pressure, flutter valve, intrapulmonary percussive ventilation, and high-frequency chest
compression with the ThAIRapy Vest. J Cardiopulm Rehabil. 1998 Jul-Aug;18(4):283-9.
381. Varekojis SM, Douce FH, Flucke RL, Filbrun DA, Tice JS, McCoy KS, et al. A comparison
of the therapeutic effectiveness of and preference for postural drainage and percussion,
intrapulmonary percussive ventilation, and high-frequency chest wall compression in
hospitalized cystic fibrosis patients. Respir Care. 2003 Jan;48(1):24-8.
382. Newhouse PA, White F, Marks JH, Homnick DN. The intrapulmonary percussive
ventilator and flutter device compared to standard chest physiotherapy in patients with cystic
fibrosis. Clin Pediatr (Phila). 1998 Jul;37(7):427-32.
383. Trawoger R, Kolobow T, Cereda M, Giacomini M, Usuki J, Horiba K, et al. Clearance of
mucus from endotracheal tubes during intratracheal pulmonary ventilation. Anesthesiology.
1997 Jun;86(6):1367-74.
384. Nava S, Barbarito N, Piaggi G, De Mattia E, Cirio S. Physiological response to
intrapulmonary percussive ventilation in stable COPD patients. Respir Med. 2006
Sep;100(9):1526-33.
385. Bach JR. A historical perspective on the use of noninvasive ventilatory support
alternatives. Respir Care Clin N Am. 1996 Jun;2(2):161-81.
386. Hansen LG, Warwick WJ, Hansen KL. Mucus transport mechanisms in relation to the
effect of high frequency chest compression (HFCC) on mucus clearance. Pediatr Pulmonol.
1994 Feb;17(2):113-8.
387. van der Schans C, Prasad A, Main E. Chest physiotherapy compared to no chest
physiotherapy for cystic fibrosis. Cochrane Database Syst Rev. 2000(2):CD001401.
388. Scherer TA, Barandun J, Martinez E, Wanner A, Rubin EM. Effect of high-frequency oral
airway and chest wall oscillation and conventional chest physical therapy on expectoration in
patients with stable cystic fibrosis. Chest. 1998 Apr;113(4):1019-27.
389. Darbee JC, Kanga JF, Ohtake PJ. Physiologic evidence for high-frequency chest wall
oscillation and positive expiratory pressure breathing in hospitalized subjects with cystic
fibrosis. Phys Ther. 2005 Dec;85(12):1278-89.
390. Dolmage TE, De Rosie JA, Avendano MA, Goldstein RS. Effect of external chest wall
oscillation on gas exchange in healthy subjects. Chest. 1995 Feb;107(2):433-9.
391. Hansen LG, Warwick WJ. High-frequency chest compression system to aid in clearance
of mucus from the lung. Biomed Instrum Technol. 1990 Jul-Aug;24(4):289-94.
392. Jones A, Rowe BH. Bronchopulmonary hygiene physical therapy in bronchiectasis and
chronic obstructive pulmonary disease: a systematic review. Heart Lung. 2000 Mar-
Apr;29(2):125-35.
393. Lange DJ, Lechtzin N, Davey C, David W, Heiman-Patterson T, Gelinas D, et al. High-
frequency chest wall oscillation in ALS: an exploratory randomized, controlled trial. Neurology.
2006 Sep 26;67(6):991-7.
394. Gomez-Merino E, Sancho J, Marin J, Servera E, Blasco ML, Belda FJ, et al. Mechanical
insufflation-exsufflation: pressure, volume, and flow relationships and the adequacy of the
manufacturer's guidelines. Am J Phys Med Rehabil. 2002 Aug;81(8):579-83.
395. Bach JR, Smith WH, Michaels J, Saporito L, Alba AS, Dayal R, ., et al. Airway secretion
clearance by mechanical exsufflation for post-poliomyelitis ventilator-assisted individuals. Arch
Phys Med Rehab. 1993;74: 170-7.
396. Farrero E, Prats E, Povedano M, Martinez-Matos JA, Manresa F, Escarrabill J. Survival in
amyotrophic lateral sclerosis with home mechanical ventilation: the impact of systematic
respiratory assessment and bulbar involvement. Chest. 2005 Jun;127(6):2132-8.
397. Bach JR, Niranjan V, Weaver B. Spinal muscular atrophy type 1: A noninvasive
respiratory management approach. Chest. 2000;117:1100-5.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 333

398. Niranjan V, Bach JR. Noninvasive management of pediatric neuromuscular ventilatory
failure. Crit Care Med. 1998 Dec;26(12):2061-5.
399. Garstang SV, Kirshblum SC, Wood KE. Patient preference for in-exsufflation for
secretion management with spinal cord injury. J Spinal Cord Med. 2000 Summer;23(2):80-5.
400. Sancho J, Servera E, Vergara P, Marin J. Mechanical Insufflation-Exsufflation vs.
Tracheal Suctioning via Traqueostomy Tubes for Patients with Amyotrophic Lateral Sclerosis: a
pilot study. Am J Phys Med Rehabil. 2003;82:750-3.
401. Servera E, Sancho J, Gomez-Merino E, Briones ML, Vergara P, Perez D, et al. Non-
invasive management of an acute chest infection for a patient with ALS. J Neurol Sci. 2003 May
15;209(1-2):111-3.
402. Whitney J, Harden B, Keilty S. Assisted Cough: a new technique. Physiotherapy.
2002;88,(4):201-7.
403. Williams EK, Holaday DA. The use of exsufflation with negative pressure in
postoperative patients. Am J Surg. 1955;90::637-40.
404. Marchant WAF, R. Postoperative use of a CoughAssist device in avoiding prolonged
intubation. Br J Anaesth. 2002;89(4):644-7.
405. Bach JR. Cough in SCI patients. Arch Phys Med Rehabil. 1994 May;75(5):610.
406. Vianello AC, A; Arcaro,G; Gallan,F; Ori,C; Minuzzo,M; Bevilacqua,M. Mechanical
Insufflation-exsufflaton improves outcomes for neuromuscular disease patients with
respiratory tract infenctions. Am J Phys Med Rehabil. 2004;(in press).
407. Bach JR, Saporito LR. Criteria for successful extubation and tracheostomy tube removal
for patients with respiratory failure. Chest. 1996;110(6):1566- 71.
408. Bach J, Goncalves M. Ventilatory weaning by lung expansion and decannulation. Am J
Phys Med Rehabil. 2004;83:560-8.
409. Rello J, Paiva JA, Baraibar J, Barcenilla F, Bodi M, Castander D, et al. International
Conference for the Development of Consensus on the Diagnosis and Treatment of Ventilator-
associated Pneumonia. Chest. 2001 Sep;120(3):955-70.
410. De Jonghe B, Sharshar T, Lefaucheur JP, Authier FJ, Durand-Zaleski I, Boussarsar M, et
al. Paresis acquired in the intensive care unit: a prospective multicenter study. JAMA. 2002 Dec
11;288(22):2859-67.
411. Boles JM, Bion J, Connors A, Herridge M, Marsh B, Melot C, et al. Weaning from
mechanical ventilation. Eur Respir J. 2007 May;29(5):1033-56.
412. Meade M, Guyatt G, Cook D, Griffith L, Sinuff T, Kergl C, et al. Predicting success in
weaning from mechanical ventilation. Chest. 2001 Dec;120(6 Suppl):400S-24S.
413. Frutos-Vivar F, Ferguson ND, Esteban A, Epstein SK, Arabi Y, Apezteguia C, et al. Risk
factors for extubation failure in patients following a successful spontaneous breathing trial.
Chest. 2006 Dec;130(6):1664-71.
414. Capdevila X, Perrigault PF, Ramonatxo M, Roustan JP, Peray P, d'Athis F, et al. Changes
in breathing pattern and respiratory muscle performance parameters during difficult weaning.
Crit Care Med. 1998 Jan;26(1):79-87.
415. Carlucci A, Ceriana P, Prinianakis G, Fanfulla F, Colombo R, Nava S. Determinants of
weaning success in patients with prolonged mechanical ventilation. Crit Care. 2009;13(3):R97.
416. MacIntyre NR, Cook DJ, Ely EW, Jr., Epstein SK, Fink JB, Heffner JE, et al. Evidence-
based guidelines for weaning and discontinuing ventilatory support: a collective task force
facilitated by the American College of Chest Physicians; the American Association for
Respiratory Care; and the American College of Critical Care Medicine. Chest. 2001 Dec;120(6
Suppl):375S-95S.
417. Hotchkiss JR, Marini JJ. Noninvasive ventilation: an emerging supportive technique for
the emergency department. Ann Emerg Med. 1998 Oct;32(4):470-9.
418. Girault C, Briel A, Hellot MF, Tamion F, Woinet D, Leroy J, et al. Noninvasive mechanical
ventilation in clinical practice: a 2-year experience in a medical intensive care unit. Crit Care
Med. 2003 Feb;31(2):552-9.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
334 Miguel Ramalho do Souto Gonçalves

419. Caples SM, Gay PC. Noninvasive positive pressure ventilation in the intensive care unit:
a concise review. Crit Care Med. 2005 Nov;33(11):2651-8.
420. Esteban A, Anzueto A, Frutos F, Alia I, Brochard L, Stewart TE, et al. Characteristics and
outcomes in adult patients receiving mechanical ventilation: a 28-day international study.
Jama. 2002 Jan 16;287(3):345-55.
421. Pilcher DV, Bailey MJ, Treacher DF, Hamid S, Williams AJ, Davidson AC. Outcomes, cost
and long term survival of patients referred to a regional weaning centre. Thorax. 2005
Mar;60(3):187-92.
422. Martin TJ, Hovis JD, Costantino JP, Bierman MI, Donahoe MP, Rogers RM, et al. A
randomized, prospective evaluation of noninvasive ventilation for acute respiratory failure. Am
J Respir Crit Care Med. 2000 Mar;161(3 Pt 1):807-13.
423. Deem S, Lee CM, Curtis JR. Acquired neuromuscular disorders in the intensive care
unit. Am J Respir Crit Care Med. 2003 Oct 1;168(7):735-9.
424. Vassilakopoulos T, Petrof BJ. Ventilator-induced diaphragmatic dysfunction. Am J
Respir Crit Care Med. 2004 Feb 1;169(3):336-41.
425. Boczkowski J. Lung infection and the diaphragm: placing basic research in clinical
perspective. Am J Respir Crit Care Med. 2004 Mar 15;169(6):662-3.
426. Lacomis D, Petrella JT, Giuliani MJ. Causes of neuromuscular weakness in the intensive
care unit: a study of ninety-two patients. Muscle Nerve. 1998 May;21(5):610-7.
427. Divangahi M, Matecki S, Dudley RW, Tuck SA, Bao W, Radzioch D, et al. Preferential
diaphragmatic weakness during sustained Pseudomonas aeruginosa lung infection. Am J Respir
Crit Care Med. 2004 Mar 15;169(6):679-86.
428. De Jonghe B, Bastuji-Garin S, Sharshar T, Outin H, Brochard L. Does ICU-acquired
paresis lengthen weaning from mechanical ventilation? Intensive Care Med. 2004
Jun;30(6):1117-21.
429. Spitzer AR, Giancarlo T, Maher L, Awerbuch G, Bowles A. Neuromuscular causes of
prolonged ventilator dependency. Muscle Nerve. 1992 Jun;15(6):682-6.
430. Winck JC, Goncalves M. Muscles and lungs: fatal attraction, but time for intervention.
Monaldi Arch Chest Dis. 2005 Sep;63(3):121-3.
431. Epstein SK. Weaning the "unweanable": liberating patients from prolonged mechanical
ventilation. Crit Care Med. 2007 Nov;35(11):2640-1.
432. Covert CR, Brodie SB, Zimmerman JE. Weaning failure due to acute neuromuscular
disease. Crit Care Med. 1986 Apr;14(4):307-8.
433. Epstein SK. Etiology of extubation failure and the predictive value of the rapid shallow
breathing index. Am J Respir Crit Care Med. 1995 Aug;152(2):545-9.
434. Mehta S. Neuromuscular disease causing acute respiratory failure. Respir Care. 2006
Sep;51(9):1016-21; discussion 21-3.
435. Berney S, Bragge P, Granger C, Opdam H, Denehy L. The acute respiratory
management of cervical spinal cord injury in the first 6 weeks after injury: a systematic review.
Spinal Cord. 2010 Apr 20.
436. Blot F, Melot C. Indications, timing, and techniques of tracheostomy in 152 French
ICUs. Chest. 2005 Apr;127(4):1347-52.
437. MacDuff A, Grant IS. Critical care management of neuromuscular disease, including
long-term ventilation. Curr Opin Crit Care. 2003 Apr;9(2):106-12.
438. Bach JR, Goncalves M. Ventilator weaning by lung expansion and decannulation. Am J
Phys Med Rehabil. 2004 Jul;83(7):560-8.
439. Bach JR. A comparison of long-term ventilatory support alternatives from the
perspective of the patient and care giver. Chest. 1993 Dec;104(6):1702-6.
440. Jackson AB, Groomes TE. Incidence of respiratory complications following spinal cord
injury. Arch Phys Med Rehabil. 1994 Mar;75(3):270-5.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 335

441. Velmahos GC, Toutouzas K, Chan L, Tillou A, Rhee P, Murray J, et al. Intubation after
cervical spinal cord injury: to be done selectively or routinely? Am Surg. 2003 Oct;69(10):891-
4.
442. Harrop JS, Sharan AD, Scheid EH, Jr., Vaccaro AR, Przybylski GJ. Tracheostomy
placement in patients with complete cervical spinal cord injuries: American Spinal Injury
Association Grade A. J Neurosurg. 2004 Jan;100(1 Suppl Spine):20-3.
443. Romero J, Vari A, Gambarrutta C, Oliviero A. Tracheostomy timing in traumatic spinal
cord injury. Eur Spine J. 2009 Oct;18(10):1452-7.
444. Winslow C, Bode RK, Felton D, Chen D, Meyer PR, Jr. Impact of respiratory
complications on length of stay and hospital costs in acute cervical spine injury. Chest. 2002
May;121(5):1548-54.
445. Salam A, Tilluckdharry L, Amoateng-Adjepong Y, Manthous CA. Neurologic status,
cough, secretions and extubation outcomes. Intensive Care Med. 2004 Jul;30(7):1334-9.
446. Hilbert G, Gruson D, Portel L, Gbikpi-Benissan G, Cardinaud JP. Noninvasive pressure
support ventilation in COPD patients with postextubation hypercapnic respiratory
insufficiency. Eur Respir J. 1998 Jun;11(6):1349-53.
447. Perrin C, Unterborn JN, Ambrosio CD, Hill NS. Pulmonary complications of chronic
neuromuscular diseases and their management. Muscle Nerve. 2004 Jan;29(1):5-27.
448. Criner GJ, Brennan K, Travaline JM, Kreimer D. Efficacy and compliance with
noninvasive positive pressure ventilation in patients with chronic respiratory failure. Chest.
1999 Sep;116(3):667-75.
449. Leger P. Long-term ventilation in restrictive ventilatory disorders. Respir Care Clin N
Am. 2002 Dec;8(4):507-32, v.
450. Muir JF, Cuvelier A. Evaluation of candidates for long-term ventilation. Respir Care Clin
N Am. 2002 Sep;8(3):405-18, vi.
451. Kohler D. Noninvasive ventilation works in all restrictive diseases with hypercapnia
whatever the cause. Respiration. 2001;68(5):450-1.
452. Nauffal D, Domenech R, Martinez Garcia MA, Compte L, Macian V, Perpina M.
Noninvasive positive pressure home ventilation in restrictive disorders: outcome and impact
on health-related quality of life. Respir Med. 2002 Oct;96(10):777-83.
453. Servera E, Perez M, Marin J, Vergara P, Castano R. Noninvasive nasal mask ventilation
beyond the ICU for an exacerbation of chronic respiratory insufficiency. Chest. 1995
Dec;108(6):1572-6.
454. Simonds AK. Recent advances in respiratory care for neuromuscular disease. Chest.
2006;130:1879-86.
455. Bellemare F, Grassino A. Effect of pressure and timing of contraction on human
diaphragm fatigue. J Appl Physiol. 1982 Nov;53(5):1190-5.
456. Bellemare F, Grassino A. Force reserve of the diaphragm in patients with chronic
obstructive pulmonary disease. J Appl Physiol. 1983 Jul;55(1 Pt 1):8-15.
457. Ramonatxo M, Boulard P, Prefaut C. Validation of a noninvasive tension-time index of
inspiratory muscles. J Appl Physiol. 1995 Feb;78(2):646-53.
458. Mulreany LT, Weiner DJ, McDonough JM, Panitch HB, Allen JL. Noninvasive
measurement of the tension-time index in children with neuromuscular disease. J Appl Physiol.
2003 Sep;95(3):931-7.
459. Gozal D. Pulmonary manifestations of neuromuscular disease with special reference to
Duchenne muscular dystrophy and spinal muscular atrophy. Pediatr Pulmonol. 2000
Feb;29(2):141-50.
460. Sancho J, Servera E, Diaz J, Marin J. Predictors of ineffective cough during a chest
infection in patients with stable amyotrophic lateral sclerosis. Am J Respir Crit Care Med. 2007
Jun 15;175(12):1266-71.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
336 Miguel Ramalho do Souto Gonçalves

461. Suarez AA, Pessolano FA, Monteiro SG, Ferreyra G, Capria ME, Mesa L, et al. Peak flow
and peak cough flow in the evaluation of expiratory muscle weakness and bulbar impairment
in patients with neuromuscular disease. Am J Phys Med Rehabil. 2002 Jul;81(7):506-11.
462. Bach JR. Update and perspective on noninvasive respiratory muscle aids. Part 2: The
expiratory aids. Chest. 1994 May;105(5):1538-44.
463. Toussaint M, Boitano LJ, Gathot V, Steens M, Soudon P. Limits of effective cough-
augmentation techniques in patients with neuromuscular disease. Respir Care. 2009
Mar;54(3):359-66.
464. Ishikawa Y, Bach JR, Komaroff E, Miura T, Jackson-Parekh R. Cough augmentation in
Duchenne muscular dystrophy. Am J Phys Med Rehabil. 2008 Sep;87(9):726-30.
465. Braun SR, Giovannoni R, O'Connor M. Improving the cough in patients with spinal cord
injury. Am J Phys Med. 1984 Feb;63(1):1-10.
466. Hardy KA, Anderson BD. Noninvasive clearance of airway secretions. Respir Care Clin N
Am. 1996 Jun;2(2):323-45.
467. Nunn A, Gregg I. New regression equations for predicting peak expiratory flow in
adults. BMJ
1989;298:1068-70.
468. Bach JR, Kang SW. Disorders of ventilation : weakness, stiffness, and mobilization.
Chest. 2000 Feb;117(2):301-3.
469. Boitano LJ. Managing the patient with neuromuscular disease and respiratory
insufficiency. Respir Care. 2008 Nov;53(11):1434-5.
470. Bach JR. Amyotrophic lateral sclerosis: predictors for prolongation of life by
noninvasive respiratory aids. Arch Phys Med Rehabil. 1995 Sep;76(9):828-32.
471. Bach JR, Hon A. Amyotrophic lateral sclerosis: noninvasive ventilation, uncuffed
tracheostomy tubes, and mechanically assisted coughing. Am J Phys Med Rehabil. 2010
May;89(5):412-4.
472. Ozsancak A, D'Ambrosio C, Hill NS. Nocturnal noninvasive ventilation. Chest. 2008
May;133(5):1275-86.
473. Escarrabill J, Estopa R, Farrero E, Monasterio C, Manresa F. Long-term mechanical
ventilation in amyotrophic lateral sclerosis. Respir Med. 1998 Mar;92(3):438-41.
474. Goldberg AI. Noninvasive mechanical ventilation at home: building upon the tradition.
Chest. 2002 Feb;121(2):321-4.
475. Leger P, Laier-Groeneveld G. Infrastructure, funding and follow-up in a programme of
noninvasive ventilation. Eur Respir J. 2002 Dec;20(6):1573-8.
476. Vitacca M, Escarrabill J, Galavotti G, Vianello A, Prats E, Scala R, et al. Home mechanical
ventilation patients: a retrospective survey to identify level of burden in real life. Monaldi Arch
Chest Dis. 2007 Sep;67(3):142-7.
477. Vianello A, Bevilacqua M, Arcaro G, Gallan F, Serra E. Non-invasive ventilatory
approach to treatment of acute respiratory failure in neuromuscular disorders. A comparison
with endotracheal intubation. Intensive Care Med. 2000 Apr;26(4):384-90.
478. Goncalves M, Bach J. Mechanical Insufflation-exsufflation improves outcomes for
Neuromuscular disease patients with repiratory tract infections: " a step in the right direction".
Am J Phys Med Rehabil. 2005;84:89-91.
479. Lechtzin N, Rothstein J, Clawson L, Diette GB, Wiener CM. Amyotrophic lateral
sclerosis: evaluation and treatment of respiratory impairment. Amyotroph Lateral Scler Other
Motor Neuron Disord. 2002 Mar;3(1):5-13.
480. Mustfa N, Aiello M, Lyall RA, Nikoletou D, Olivieri D, Leigh PN, et al. Cough
augmentation in amyotrophic lateral sclerosis. Neurology. 2003 Nov 11;61(9):1285-7.
481. Bach JR, Bianchi C, Aufiero E. Oximetry and indications for tracheotomy for
amyotrophic lateral sclerosis. Chest. 2004 Nov;126(5):1502-7.
482. Krivickas LS, Shockley L, Mitsumoto H. Home care of patients with amyotrophic lateral
sclerosis (ALS). J Neurol Sci. 1997 Oct;152 Suppl 1:S82-9.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 337
483. Kollef MH, Ahrens TS, Shannon W. Clinical predictors and outcomes for patients
requiring tracheostomy in the intensive care unit. Crit Care Med. 1999 Sep;27(9):1714-20.
484. Mustfa N, Walsh E, Bryant V, Lyall RA, Addington-Hall J, Goldstein LH, et al. The effect
of noninvasive ventilation on ALS patients and their caregivers. Neurology. 2006 Apr
25;66(8):1211-7.
485. Bach JR, Ishikawa Y, Kim H. Prevention of pulmonary morbidity for patients with
Duchenne muscular dystrophy. Chest. 1997 Oct;112(4):1024-8.
486. Miske LJ, Hickey EM, Kolb SM, Weiner DJ, Panitch HB. Use of the mechanical in-
exsufflator in pediatric patients with neuromuscular disease and impaired cough. Chest. 2004
Apr;125(4):1406-12.
487. Bach JR, Goncalves MR, Hamdani I, Winck JC. Extubation of patients with
neuromuscular weakness: a new management paradigm. Chest. 2010 May;137(5):1033-9.
488. Benditt JO. Full-time noninvasive ventilation: possible and desirable. Respir Care. 2006
Sep;51(9):1005-12; discussion 12-5.
489. Bach JR. Why be limited to nocturnal noninvasive IPPV? Chest. 1997 May;111(5):1471-
2.
490. Hess DR. Noninvasive ventilation in neuromuscular disease: equipment and
application. Respir Care. 2006 Aug;51(8):896-911; discussion -2.
491. Toussaint M, Steens M, Wasteels G, Soudon P. Diurnal ventilation via mouthpiece:
survival in end-stage Duchenne patients. Eur Respir J. 2006 Sep;28(3):549-55.
492. Bach JR. Noninvasive ventilation is more than mask ventilation. Chest. 2003
Jun;123(6):2156-7; author reply 7.
493. Annane D, Orlikowski D, Chevret S, Chevrolet JC, Raphael JC. Nocturnal mechanical
ventilation for chronic hypoventilation in patients with neuromuscular and chest wall
disorders. Cochrane Database Syst Rev. 2007(4):CD001941.
494. Howard RS, Davidson C. Long term ventilation in neurogenic respiratory failure. J
Neurol Neurosurg Psychiatry. 2003 Sep;74 Suppl 3:iii24-30.
495. Teener JW, Raps EC. Evaluation and treatment of respiratory failure in neuromuscular
disease. Rheum Dis Clin North Am. 1997 May;23(2):277-92.
496. Kennedy JD, Martin AJ. Chronic respiratory failure and neuromuscular disease. Pediatr
Clin North Am. 2009 Feb;56(1):261-73, xii.
497. Ferrer M, Sellares J, Valencia M, Carrillo A, Gonzalez G, Badia JR, et al. Non-invasive
ventilation after extubation in hypercapnic patients with chronic respiratory disorders:
randomised controlled trial. Lancet. 2009 Sep 26;374(9695):1082-8.
498. Bach JR, Niranjan V, Weaver B. Spinal muscular atrophy type 1: A noninvasive
respiratory management approach. Chest. 2000 Apr;117(4):1100-5.
499. Kollef MH. Avoidance of tracheal intubation as a strategy to prevent ventilator-
associated pneumonia. Intensive Care Med. 1999 Jun;25(6):553-5.
500. Bach J, Bianchi C, Lopes M, Turi S, Felisari G. Lung Inflation by glossopharyngeal
breathing and "air stacking" in Duchenne Muscular Dystrophy. Am J Phys Med Rehabil.
2007;86:295-300.
501. Consortium for Spinal Cord Medicine. Respiratory management during the first five
days after spinal cord injury: a clinical practice guideline for health care professionals. available
from
http:\\wwwguidelinegov/summary/pdfaspxdoc_id=7198&stat=1&string=spinal+AND+injury.
2005.
502. Bach JR. Prevention of respiratory complications of spinal cord injury: a challenge to
"model" spinal cord injury units. J Spinal Cord Med. 2006;29(1):3-4.
503. Peterson WP, Barbalata L, Brooks CA, Gerhart KA, Mellick DC, Whiteneck GG. The
effect of tidal volumes on the time to wean persons with high tetraplegia from ventilators.
Spinal Cord. 1999 Apr;37(4):284-8.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
338 Miguel Ramalho do Souto Gonçalves

504. Viroslav J, Rosenblatt R, Tomazevic SM. Respiratory management, survival, and quality
of life for high-level traumatic tetraplegics. Respir Care Clin N Am. 1996 Jun;2(2):313-22.
505. Bach JR. Inappropriate weaning and late onset ventilatory failure of individuals with
traumatic spinal cord injury. Paraplegia. 1993 Jul;31(7):430-8.
506. Pillastrini P, Bordini S, Bazzocchi G, Belloni G, Menarini M. Study of the effectiveness of
bronchial clearance in subjects with upper spinal cord injuries: examination of a rehabilitation
programme involving mechanical insufflation and exsufflation. Spinal Cord. 2006
Oct;44(10):614-6.
507. Ceriana P, Carlucci A, Navalesi P, Rampulla C, Delmastro M, Piaggi G, et al. Weaning
from tracheotomy in long-term mechanically ventilated patients: feasibility of a decisional
flowchart and clinical outcome. Intensive Care Med. 2003 May;29(5):845-8.
508. Ross J, White M. Removal of the tracheostomy tube in the aspirating spinal cord-
injured patient. Spinal Cord. 2003 Nov;41(11):636-42.
509. Gregoretti C, Olivieri C, Navalesi P. Physiologic comparison between conventional
mechanical ventilation and transtracheal open ventilation in acute traumatic quadriplegic
patients. Crit Care Med. 2005 May;33(5):1114-8.
510. Diehl JL, El Atrous S, Touchard D, Lemaire F, Brochard L. Changes in the work of
breathing induced by tracheotomy in ventilator-dependent patients. Am J Respir Crit Care
Med. 1999 Feb;159(2):383-8.
511. Fishburn MJ, Marino RJ, Ditunno JF, Jr. Atelectasis and pneumonia in acute spinal cord
injury. Arch Phys Med Rehabil. 1990 Mar;71(3):197-200.
512. Agarwal R, Aggarwal AN, Gupta D, Jindal SK. Role of noninvasive positive-pressure
ventilation in postextubation respiratory failure: a meta-analysis. Respir Care. 2007
Nov;52(11):1472-9.
513. Khamiees M, Raju P, DeGirolamo A, Amoateng-Adjepong Y, Manthous CA. Predictors
of extubation outcome in patients who have successfully completed a spontaneous breathing
trial. Chest. 2001 Oct;120(4):1262-70.
514. Pierson DJ. Indications for mechanical ventilation in adults with acute respiratory
failure. Respir Care. 2002 Mar;47(3):249-62; discussion 62-5.
515. Wedzicha JA, Muir JF. Noninvasive ventilation in chronic obstructive pulmonary
disease, bronchiectasis and cystic fibrosis. Eur Respir J. 2002 Sep;20(3):777-84.
516. Cinel D, Markwell K, Lee R, Szidon P. Variability of the respiratory gas exchange ratio
during arterial puncture. Am Rev Respir Dis. 1991 Feb;143(2):217-8.
517. Bach J, Robert D, Leger P, Langevin B. Sleep fragmentation in Kyphoscoliotic individuals
with alveolar hypoventilation treated by NIPPV. Chest. 1995;107:1552-8.
518. Lechtzin N, Wiener CM, Shade DM, Clawson L, Diette GB. Spirometry in the supine
position improves the detection of diaphragmatic weakness in patients with amyotrophic
lateral sclerosis. Chest. 2002 Feb;121(2):436-42.
519. Jackson CE, Rosenfeld J, Moore DH, Bryan WW, Barohn RJ, Wrench M, et al. A
preliminary evaluation of a prospective study of pulmonary fuction studies and symptoms of
hypoventilation in ALS/MND patients. J Neurol Sci. 2001;191(75-8).
520. Koga T, Watanabe K, Sano M, Ishikawa Y, Bach JR. Breathing intolerance index: a new
indicator for ventilator use. Am J Phys Med Rehabil. 2006 Jan;85(1):24-30.
521. Braun NM, Arora NS, Rochester DF. Respiratory muscle and pulmonary function in
polymyositis and other proximal myopathies. Thorax. 1983 Aug;38(8):616-23.
522. Gregory SA. Evaluation and management of respiratory muscle dysfunction in ALS.
NeuroRehabilitation. 2007;22(6):435-43.
523. Irwin RS, Boulet LP, Cloutier MM, Fuller R, Gold PM, Hoffstein V, et al. Managing cough
as a defense mechanism and as a symptom. A consensus panel report of the American College
of Chest Physicians. Chest. 1998 Aug;114(2 Suppl Managing):133S-81S.
524. Wohlgemuth M, van der Kooi EL, Hendriks JC, Padberg GW, Folgering HT. Face mask
spirometry and respiratory pressures in normal subjects. Eur Respir J. 2003 Dec;22(6):1001-6.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 339
525. Holcroft CA, Eisen EA, Sama SR, Wegman DH. Measurement characteristics of peak
expiratory flow. Chest. 2003 Aug;124(2):501-10.
526. Sancho J, Servera E, Diaz J, Marin J. Comparison of peak cough flows measured by
pneumotachograph and a portable peak flow meter. Am J Phys Med Rehabil. 2004
Aug;83(8):608-12.
527. Bach JR, Mahajan K, Lipa B, Saporito L, Goncalves M, Komaroff E. Lung insufflation
capacity in neuromuscular disease. Am J Phys Med Rehabil. 2008 Sep;87(9):720-5.
528. Lechtzin N, Shade D, Clawson L, Wiener CM. Supramaximal inflation improves lung
compliance in subjects with amyotrophic lateral sclerosis. Chest. 2006 May;129(5):1322-9.
529. Birnkrant DJ, Bushby KM, Amin RS, Bach JR, Benditt JO, Eagle M, et al. The respiratory
management of patients with duchenne muscular dystrophy: a DMD care considerations
working group specialty article. Pediatr Pulmonol. 2010 Aug;45(8):739-48.
530. Schroth MK. Special considerations in the respiratory management of spinal muscular
atrophy. Pediatrics. 2009 May;123 Suppl 4:S245-9.
531. Bach JR, Baird JS, Plosky D, Navado J, Weaver B. Spinal muscular atrophy type 1:
management and outcomes. Pediatr Pulmonol. 2002 Jul;34(1):16-22.
532. DiMarco AF, Kelling JS, DiMarco MS, Jacobs I, Shields R, Altose MD. The effects of
inspiratory resistive training on respiratory muscle function in patients with muscular
dystrophy. Muscle Nerve. 1985 May;8(4):284-90.
533. Wong WP, Paratz JD, Wilson K, Burns YR. Hemodynamic and ventilatory effects of
manual respiratory physiotherapy techniques of chest clapping, vibration, and shaking in an
animal model. J Appl Physiol. 2003 Sep;95(3):991-8.
534. Baydur A, Kanel G. Tracheobronchomalacia and tracheal hemorrhage in patients with
Duchenne muscular dystrophy receiving long-term ventilation with uncuffed tracheostomies.
Chest. 2003 Apr;123(4):1307-11.
535. Durbin CG, Jr. Early complications of tracheostomy. Respir Care. 2005 Apr;50(4):511-5.
536. Epstein SK. Late complications of tracheostomy. Respir Care. 2005 Apr;50(4):542-9.
537. Pignatti P, Balestrino A, Herr C, Bals R, Moretto D, Corradi M, et al. Tracheostomy and
related host-pathogen interaction are associated with airway inflammation as characterized by
tracheal aspirate analysis. Respir Med. 2009 Feb;103(2):201-8.
538. Bach JR. Amyotrophic lateral sclerosis. Communication status and survival with
ventilatory support. Am J Phys Med Rehabil. 1993 Dec;72(6):343-9.
539. Sivasothy P, Brown L, Smith IE, Shneerson JM. Effect of manually assisted cough and
mechanical insufflation on cough flow of normal subjects, patients with chronic obstructive
pulmonary disease (COPD), and patients with respiratory muscle weakness. Thorax. 2001
Jun;56(6):438-44.
540. Nijeweme-d'Hollosy WO, Janssen EP, Huis in 't Veld RM, Spoelstra J, Vollenbroek-
Hutten MM, Hermens HJ. Tele-treatment of patients with amyotrophic lateral sclerosis (ALS). J
Telemed Telecare. 2006;12 Suppl 1:31-4.
541. Markstrom A, Sundell K, Lysdahl M, Andersson G, Schedin U, Klang B. Quality-of-life
evaluation of patients with neuromuscular and skeletal diseases treated with noninvasive and
invasive home mechanical ventilation. Chest. 2002 Nov;122(5):1695-700.
542. Sancho J, Servera E, Banuls P, Marin J. Prolonging survival in amyotrophic lateral
sclerosis: efficacy of noninvasive ventilation and uncuffed tracheostomy tubes. Am J Phys Med
Rehabil. 2010 May;89(5):407-11.
543. Schmitt JK, Stiens S, Trincher R, Lam M, Sarkarati M, Linder S, et al. Survey of use of the
insufflator-exsufflator in patients with spinal cord injury. J Spinal Cord Med. 2007;30(2):127-30.
544. Eagle M, Baudouin SV, Chandler C, Giddings DR, Bullock R, Bushby K. Survival in
Duchenne muscular dystrophy: improvements in life expectancy since 1967 and the impact of
home nocturnal ventilation. Neuromuscul Disord. 2002 Dec;12(10):926-9.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
340 Miguel Ramalho do Souto Gonçalves

545. Baydur A, Gilgoff I, Prentice W, Carlson M, Fischer DA. Decline in respiratory function
and experience with long-term assisted ventilation in advanced Duchenne's muscular
dystrophy. Chest. 1990 Apr;97(4):884-9.
546. Soudon P, Steens M, Toussaint M. A comparison of invasive versus noninvasive full-
time mechanical ventilation in Duchenne muscular dystrophy. Chron Respir Dis. 2008;5(2):87-
93.
547. Smith PE, Calverley PM, Edwards RH. Hypoxemia during sleep in Duchenne muscular
dystrophy. Am Rev Respir Dis. 1988 Apr;137(4):884-8.
548. Carroll N, Bain RJ, Smith PE, Saltissi S, Edwards RH, Calverley PM. Domiciliary
investigation of sleep-related hypoxaemia in Duchenne muscular dystrophy. Eur Respir J. 1991
Apr;4(4):434-40.
549. Fanfulla F, Berardinelli A, Gualtieri G, Zoia MC, Ottolini A, Vianello A, et al. The efficacy
of noninvasive mechanical ventilation on nocturnal hypoxaemia in Duchenne's muscular
dystrophy. Monaldi Arch Chest Dis. 1998 Feb;53(1):9-13.
550. Kinali M, Manzur AY, Mercuri E, Gibson BE, Hartley L, Simonds AK, et al. UK physicians'
attitudes and practices in long-term non-invasive ventilation of Duchenne Muscular Dystrophy.
Pediatr Rehabil. 2006 Oct-Dec;9(4):351-64.
551. Raphael JC, Chevret S, Annane D. Is early noninvasive mechanical ventilation of first
choice in stable restrictive patients with chronic respiratory failure? Monaldi Arch Chest Dis.
1999 Feb;54(1):90-7.
552. Toussaint M, Steens M, Soudon P. Lung function accurately predicts hypercapnia in
patients with Duchenne muscular dystrophy. Chest. 2007 Feb;131(2):368-75.
553. Ward S, Chatwin M, Heather S, Simonds AK. Randomised controlled trial of non-
invasive ventilation (NIV) for nocturnal hypoventilation in neuromuscular and chest wall
disease patients with daytime normocapnia. Thorax. 2005 Dec;60(12):1019-24.
554. Oskoui M, Levy G, Garland CJ, Gray JM, O'Hagen J, De Vivo DC, et al. The changing
natural history of spinal muscular atrophy type 1. Neurology. 2007 Nov 13;69(20):1931-6.
555. Wang CH, Finkel RS, Bertini ES, Schroth M, Simonds A, Wong B, et al. Consensus
statement for standard of care in spinal muscular atrophy. J Child Neurol. 2007
Aug;22(8):1027-49.
556. Roper H, Quinlivan R. Implementation of "the consensus statement for the standard of
care in spinal muscular atrophy" when applied to infants with severe type 1 SMA in the UK.
Arch Dis Child. 2010 Jul 6.
557. Miller RG, Rosenberg JA, Gelinas DF, Mitsumoto H, Newman D, Sufit R, et al. Practice
parameter: the care of the patient with amyotrophic lateral sclerosis (an evidence-based
review): report of the Quality Standards Subcommittee of the American Academy of
Neurology: ALS Practice Parameters Task Force. Neurology. 1999 Apr 22;52(7):1311-23.
558. Moss AH, Casey P, Stocking CB, Roos RP, Brooks BR, Siegler M. Home ventilation for
amyotrophic lateral sclerosis patients: outcomes, costs, and patient, family, and physician
attitudes. Neurology. 1993 Feb;43(2):438-43.
559. Moss AH, Oppenheimer EA, Casey P, Cazzolli PA, Roos RP, Stocking CB, et al. Patients
with amyotrophic lateral sclerosis receiving long-term mechanical ventilation. Advance care
planning and outcomes. Chest. 1996 Jul;110(1):249-55.
560. Lechtzin N. Respiratory effects of amyotrophic lateral sclerosis: problems and
solutions. Respir Care. 2006 Aug;51(8):871-81; discussion 81-4.
561. Ambrosino N. Noninvasive mechanical ventilation in acute on chronic respiratory
failure: determinants of success and failure. Monaldi Arch Chest Dis. 1997 Feb;52(1):73-5.
562. Ambrosino N, Carpene N, Gherardi M. Chronic respiratory care for neuromuscular
diseases in adults. Eur Respir J. 2009 Aug;34(2):444-51.
563. Bach JR, Bianchi C, Finder J, Fragasso T, Goncalves MR, Ishikawa Y, et al. Tracheostomy
tubes are not needed for Duchenne muscular dystrophy. Eur Respir J. 2007 Jul;30(1):179-80;
author reply 80-1.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
Miguel Ramalho do Souto Gonçalves 341

564. Kuhnlein P, Kubler A, Raubold S, Worrell M, Kurt A, Gdynia HJ, et al. Palliative care and
circumstances of dying in German ALS patients using non-invasive ventilation. Amyotroph
Lateral Scler. 2008 Apr;9(2):91-8.
565. Laaksovirta H. [Palliative care tailored according to the symptoms of the ALS patient is
an art form]. Duodecim. 2005;121(2):220-4.
566. Kwiecinski H. [Symptomatic treatment and palliative care of ALS]. Neurol Neurochir
Pol. 2001;35(1 Suppl):51-9.
567. Borasio GD. Palliative care in ALS: searching for the evidence base. Amyotroph Lateral
Scler Other Motor Neuron Disord. 2001 Mar;2 Suppl 1:S31-5.
568. Albert SM, Murphy PL, Del Bene ML, Rowland LP. Prospective study of palliative care in
ALS: choice, timing, outcomes. J Neurol Sci. 1999 Oct 31;169(1-2):108-13.
569. Mitsumoto H. Patient choices in ALS: life-sustaining treatment versus palliative care?
Neurology. 1999 Jul 22;53(2):248-9.
570. Birnkrant DJ, Noritz GH. Is there a role for palliative care in progressive pediatric
neuromuscular diseases? The answer is "Yes! J Palliat Care. 2008 Winter;24(4):265-9.
571. Maessen M, Veldink JH, van den Berg LH, Schouten HJ, van der Wal G, Onwuteaka-
Philipsen BD. Requests for euthanasia: origin of suffering in ALS, heart failure, and cancer
patients. J Neurol. 2010 Jul;257(7):1192-8.
572. Simonds AK. Living and dying with respiratory failure: facilitating decision making.
Chron Respir Dis. 2004;1(1):56-9.
Noninvasive ventilation and mechanical assisted cough: efficacy from acute to chronic care
342 Miguel Ramalho do Souto Gonçalves