aortic aneurysm complicated with pyogenic spondylitis following vertebroplasty
TRANSCRIPT

predominant member of the genus,4,7 and all membersare biochemically heterogeneous. In 1982, Tsukamura dis-tinguished N. nova from the N. asteroides complex bio-chemically.3 A detailed description of N. nova as ahuman pathogen was published in 1991,8 and the first de-tailed clinical case of N. nova infection was reported in1993.5
The susceptibilities of each Nocardia species to antibi-otic agents were recently found to differ.6 This suggeststhat antibiotics for nocardia infection need to be appliedaccording to the individual species. Despite improvementin diagnostic techniques, surgery and chemotherapies, themortality rate of patients with nocardial brain abscess ismore than three times higher than that of patients withbrain abscess due to other bacteria.9 Isolating the individ-ual species of Nocardia would therefore be important forantibiotic treatment. Although N. nova is thought to ac-count for about 20% of the N. asteroides complex,8 thereare only a few clinical reports of infection by N. nova,which usually manifests as pneumonia or subcutaneousabscess.4,5 Our case is the first reported evidence that N.
nova can also cause brain abscess. A recent work, basedon current molecular taxonomy, has shown that whatwas previously referred to as N. nova actually comprisesa number of closely related species.10 More detailed iden-
tification of the Nocardia species may be necessary infuture.
References
1. Beaman BL, Burnside J, Edwards B, et al. Nocardial infections in theUnited States, 1972–1974. J Infect Dis 1976;134:286–9.
2. Khalini AH. Nocardial brain abscess: a case report. J Neurol
1982;227:115–20.3. Tsukamura M. Numerical analysis of the taxonomy of Nocardiae and
Rhodococci. Microbiol Immunol 1982;26:1101–19.4. Koibuchi T, Takahashi T, Nakamura T, et al. The first isolation of
Nocardia nova from an HIV-1 infected individual in Japan. J Infect
Chemother 2002;8:358–60.5. Monteforte JS, Wood CA. Pneumonia caused by Nocardia nova and
Aspergillus fumigatus after cardiac transplantation. Eur J Clin
Microbiol Infect Dis 1993;12:112–4.6. Mikami Y, Yazawa K. Susceptibility patterns of pathogenic Nocardia
to some selected antimicrobial agents and their usefulness in theidentification work in a clinical laboratory. Bull JFCC 1989;5:89–95.
7. Lerner PI. Nocardiosis. Clin Infect Dis 1996;22:891–903.8. Wallace Jr RJ, Brown BA, Tsukamura M, et al. Clinical and laboratory
features of Nocardia nova. J Clin Micobiol 1991;29: 2407–11.9. Mamelak A, Obana WG, Flaherty JF, et al. Nocardial brain abscess:
treatment strategies and factors influencing outcome. Neurosurgery
1994;35:622–31.10. Brown-Elliott BA, Brown JM, Conville PS, et al. Clinical and
laboratory features of the Nocardia spp. Based on current moleculartaxonomy. Clin Mircobiol Rev 2006;19:259–82.
doi:10.1016/j.jocn.2007.04.019
Aortic aneurysm complicated with pyogenic spondylitisfollowing vertebroplasty
Hyung-Jun Kwak a, Jung-Kil Lee a,*, Yeon-Seong Kim a, Kyung-Sub Moon a,Sung-Pil Joo a, Jae-Hyoo Kim a, Soo-Han Kim b, Won-Chae Chang b
a Department of Neurosurgery, Chonnam National University Hospital, 8 Hak-Dong, Dong-Ku, Gwangju, 501-757, South Koreab Department of Cardiovascular and Thoracic Surgery, Chonnam National University Hospital, Gwangju, South Korea
Received 11 April 2006; accepted 25 June 2006
Table 1Characteristics of the patient’s isolate in comparison to those of Nocardia species
Characteristic N. asteroides N. otitidiscaviarum N. brasiliensis Patient’s isolate
N. asteroides N. farcinica N. nova
CompositionCasein � � � � + �Xanthine � � � + �
SusceptibilityImipenem + + + � � +Kanamycin � � � + � �Tobramycin + � � + + �5-Fluorouracil � � + � � +
* Corresponding author. Tel.: +82 62 220 6602; fax: +82 62 224 9865.E-mail address: [email protected] (J.-K. Lee).
Case Reports / Journal of Clinical Neuroscience 15 (2008) 89–93 89
Abstract
Percutaneous vertebroplasty is a commonly used procedure for the treatment of painful vertebral fractures induced by osteoporosis ormetastatic disease. It is generally considered to be safe and effective. However, infectious complications can be serious. We present a patientin whom pyogenic spondylitis developed 3 months after vertebroplasty. During the debridement, profuse bleeding was encountered frominjury to the aorta and the patient was managed with primary closure. Two months after the initial surgery, an aortic aneurysm wasdetected. A wide resection of all infected tissue, including the bony lesion and aortic aneurysm was performed, and the descending thoracicaorta was replaced with a vascular graft. A titanium mesh cage filled with bone graft was employed for anterior reconstruction. Our patientillustrates that a life-threatening aortic aneurysm can indeed occur as an infectious complication of this minimally invasive procedure dueto the proximity of the aorta to the thoracolumbar vertebra. The spine surgeon should be aware of the possibility of aortic wall erosioncaused by long-standing spondylitis, and be prepared to manage an inadvertent injury to the aorta during surgical debridement.� 2006 Elsevier Ltd. All rights reserved.
Keywords: Aortic aneurysm; Complication; Spondylitis; Vertebroplasty
1. Introduction
Percutaneous vertebroplasty (PVP) using polymethyl-methacrylate (PMMA) has been well described for the
treatment of compression fractures of the thoracic andlumbar spine. Transpedicular vertebroplasty can be per-formed with a very low complication rate with excellentclinical outcome. Many studies have reported the incidenceof complications associated with cement extravasation andPMMA toxicities. Infectious complications are rare, andonly three cases of pyogenic spondylitis after PVT havebeen reported in the literature.1–3 It is less well appreciatedthat pyogenic spondylitis may spread to involve the aorta.In this paper, we present a rare case of pyogenic spondylitiscomplicated by aortic aneurysm, following PVP.
2. Case report
2.1. History
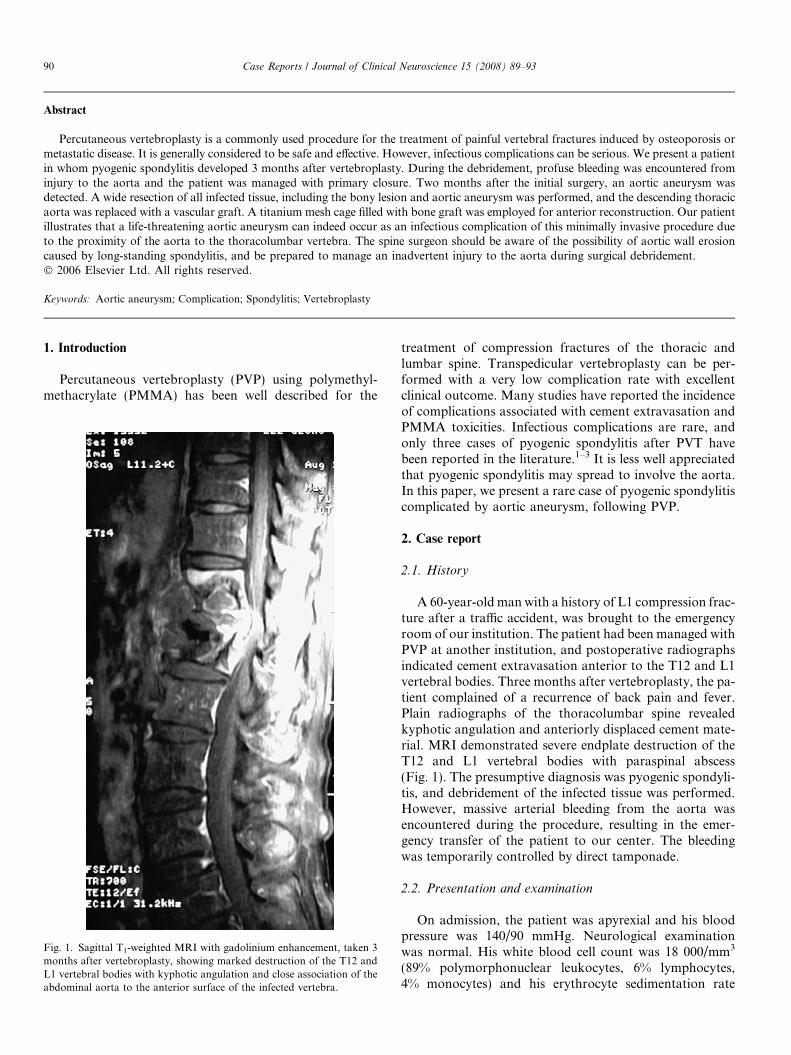
A 60-year-old man with a history of L1 compression frac-ture after a traffic accident, was brought to the emergencyroom of our institution. The patient had been managed withPVP at another institution, and postoperative radiographsindicated cement extravasation anterior to the T12 and L1vertebral bodies. Three months after vertebroplasty, the pa-tient complained of a recurrence of back pain and fever.Plain radiographs of the thoracolumbar spine revealedkyphotic angulation and anteriorly displaced cement mate-rial. MRI demonstrated severe endplate destruction of theT12 and L1 vertebral bodies with paraspinal abscess(Fig. 1). The presumptive diagnosis was pyogenic spondyli-tis, and debridement of the infected tissue was performed.However, massive arterial bleeding from the aorta wasencountered during the procedure, resulting in the emer-gency transfer of the patient to our center. The bleedingwas temporarily controlled by direct tamponade.
2.2. Presentation and examination
On admission, the patient was apyrexial and his bloodpressure was 140/90 mmHg. Neurological examinationwas normal. His white blood cell count was 18 000/mm3
(89% polymorphonuclear leukocytes, 6% lymphocytes,4% monocytes) and his erythrocyte sedimentation rate
Fig. 1. Sagittal T1-weighted MRI with gadolinium enhancement, taken 3months after vertebroplasty, showing marked destruction of the T12 andL1 vertebral bodies with kyphotic angulation and close association of theabdominal aorta to the anterior surface of the infected vertebra.
90 Case Reports / Journal of Clinical Neuroscience 15 (2008) 89–93

was 16 mm/h. The C-reactive protein level was elevated at15.7 mg/mL.
2.3. Operation and postoperative course
At operation, a perforation 0.7 · 0.7 cm, was detectedon the thoracic aorta near the celiac axis anterior to theT12 vertebra, and primary closure of the thoracic aortausing a synthetic patch reinforcement was performed. Aci-
netobacter baumannii was identified from a pus culture. Thepatient was treated with intravenous vancomycin for 8weeks, based on the results of an antibiotic sensitivity test.MRI of the thoracolumbar spine, obtained 2 months afterthe initial surgery, revealed extensive bony erosion, severekyphotic angulation, and a prevertebral round mass lo-cated at T12–L1, which displaced the aorta anteriorly.CT scans and three-dimensional CT angiograms clearlyvisualized an aortic aneurysm, 6.5 cm in size (Fig. 2). Weperformed a left retroperitoneal approach, and all infectedtissue, including the bony lesion and aortic aneurysm, werecarefully removed, and the descending thoracic aorta wasreplaced with a synthetic vascular graft. A titanium meshcage filled with autologous bone graft was used to fill thedebrided vertebral cavity. The patient did well postopera-tively, and was discharged on antibiotics. Plain radio-graphs, obtained 7 months after the surgery, revealedkyphotic angulation but relatively preserved alignmentwithout any evidence of recurrence of spondylitis (Fig. 3).
Fig. 2. T1-weighted sagittal MRI with gadolinium enhancement (a), obtained 2 months after insertion of the aortic synthetic patch reinforcement,demonstrating a prevertebral round mass at the T12–L1 level with extensive bony erosion of the T12 and L1 bodies. Three-dimensional CT (b) scan revealsa saccular aortic aneurysm.
Fig. 3. Follow-up lateral radiograph, taken 7 months after T12–L1 fusion,demonstrating kyphotic but relatively preserved alignment with a titaniummesh cage.
Case Reports / Journal of Clinical Neuroscience 15 (2008) 89–93 91

3. Discussion
Since PVP was developed, initially for the treatment ofaggressive spinal hemangiomas in 1987,4 it has becomeextensively applied to the treatment of the painful compres-sion fractures associated with osteoporosis and metastaticdisease. The goal of PVP is to provide pain relief andstrengthening of the vertebral body. PVP is generally consid-ered safe and effective, but is not completely free of compli-cations. Reported complications include cement leakageinto the spinal canal, neural foramen, and the venous sys-tem, complicated by pulmonary embolism.5–9 Complicationrates have been reported to range from <2% for osteoporoticcompression fractures to 10% for malignant tumors.5,10–14
Infectious complications are rare, but may be fatal.Meticulous protection of the surgical field from inoculationwith micro-organisms, as well as careful operative tech-nique, can greatly ameliorate the risk of spondylitis.5,12
The presence of foreign material increases the likelihoodof infection from contamination by relatively few bacteriaduring the operation.15 Some authors recommended mixingPMMA with antibiotics for prophylaxis.1,5,15,16 Shapiroet al.15 have reported a reduced infection rate with tobramy-cin-impregnated PMMA for cranioplasty, vertebral bodyreplacement and spinal fusion. A history of pre-existinginfection before PVP is also known to be an important fac-tor.1,2 To the best of our knowledge, only four cases of pyo-genic spondylitis after vertebroplasty have been previouslydescribed in the literature1–3 (Table 1). Yu et al.2 reportedpyogenic spondylitis following PVP in a patient with a uri-nary tract infection, which had been treated with intrave-nous antibiotics for 1 week prior to the operation. Theysuggested that the urinary tract infection may have inducedsystemic bacteremia, resulting in a high risk of operativecomplications. Walker et al. presented two cases of pyo-
genic spondylitis occurring after PVP, each of which in-volved a pre-existing urinary tract infection and previousdiscectomies for discitis.1 Kallmes et al. reported one infec-tion out of 63 vertebral bodies. In this case, the patient hadbecome severely immunocompromised due to high-dosesteroid therapy.16 Therefore, patients should be definitivelyscreened for systemic infection, and all possible infectioussources should be excluded or resolved before PVP. If anysigns of systemic infection are detected, the operationshould be delayed until the patient has completely recov-ered. When PVP is considered in patients who have recentlysuffered an infection, the use of a cement-antibiotic mixture,or of a prolonged antibiotics regimen, may be a reasonablechoice. In this patient, we are not aware of whether theinfectious source originated from the cement material orspread from systemic or skin infection. Further prospectivestudies will be required in order to determine the efficacy ofthe routine use of cement-antibiotic mixture.
The association of pyogenic spondylitis with infection ofthe aorta is rare, but potentially lethal. Doita et al.17 re-ported an aneurysm in the common iliac artery associatedwith pyogenic spondylitis. They emphasized that the infec-tion could extend to the contiguous aorta in vertebral spon-dylitis. As the infection progresses, the accumulation ofexudates under pressure within the vertebral body mayspread to the adjacent structures, with progressive bonydestruction. The aorta, which lies anteriorly to the thoraco-lumbar vertebra, may adhere to the vertebral body. Oncethe long-standing spondylitis and paraspinal abscess suffi-ciently erode the aortic wall, the infection eventually resultsin a small perforation, which may be obstructed temporar-ily by granulation tissue. It is not known if the aortic lesionis the result of direct infection of the posterior aortic wall,or ischemia or pressure necrosis due to compression fromleaked cement material. In the present patient, during the
Table 1Summary of cases of spondylitis after vertebroplasty reported in the literature
Authorsandyear
Age(yrs),Sex
Previous infectionhistory
Level ofvertebroplasty
Duration betweenvertebroplasty andinfection
Culturedorganism
Treatment
Yuet al.,2004
78, F Urinary tract infection T12 1 month No growth Anterior interbody fusion with a strut bone graftand posterior instrumentation
Walkeret al.,2004
64, F Calculus cholecystitis,urinary tract infection,meningitis
T11, T12 11 days Enterobacterspecies
T10–L1 fusion with titanium mesh cage and lateralinstrumentation, and supplemental posteriorinstrumentation from T8 to L3
49, F Discitis of T12–L1 L3 8 months CoagulasenegativeStapylococcus
aureus
L2–4 fusion with mesh cage and lateralinstrumentation, and supplemental posteriorinstrumentation from L2 to L5
Schmidet al.,2005
55,M
None L3–L5 7 days No growth Antibiotics only
Presentcase
60,M
None L1 3 months Acinetobacter
baumanni
Anterior interbody fusion with titanium mesh cage
92 Case Reports / Journal of Clinical Neuroscience 15 (2008) 89–93

subsequent debridement of the pyogenic spondylitis, with-out an awareness of this condition at the local hospital,profuse bleeding from the aorta occurred. Therefore, inad-vertently developed iatrogenic aortic injury, caused byinstruments or removal of cement material adherent tothe aortic wall, also cannot be excluded.
Whatever the cause, it is important to consider the pos-sibility of adhesion of the eroded aorta to the destroyedvertebral body during surgical debridement in pyogenicspondylitis, and wide resection of infected tissue shouldbe performed with great caution. Moreover, three-dimen-sional CT angiography can detect lesions of the aorta pre-operatively. The treatment of concurrent pyogenicspondylitis and an aortic aneurysm is more difficult thanthat of either condition alone.18,19 Even though we cannotbe certain whether the aortic pseudoaneurysm was directlyrelated to the infection of the vertebroplasty or simplybulged from the repair site of the intervening aorta, themost favorable outcome can be achieved when antimicro-bial therapy is combined with the extensive resection ofall infected tissues, paravertebral abscess, and bony lesions,as well as reconstruction of the aorta.
In summary, infectious complications after PVP can besevere. Sterile procedure preparations and careful operativetechnique are critical. Nonetheless, all possible infectioussources should be excluded prior to PVP. The spinesurgeon should be aware of the possibility of aortic wallerosion caused by long-standing spondylitis, and be pre-pared to manage an inadvertent injury to the aorta duringsurgical debridement.
References
1. Walker DH, Mummaneni P, Rodts Jr GE. Infected vertebroplastyReport of two cases and review of the literature. Neurosurg Focus
2004;17:E6.2. Yu SW, Chen WJ, Lin WC, et al. Serious pyogenic spondylitis
following vertebroplasty – a case report. Spine 2004;29: E209–11.3. Schmid KE, Boszczyk BM, Bierschneider M, et al. Spondylitis
following vertebroplasty: a case report. Eur Spine J 2005;14:895–9.
4. Galibert P, Deramond H, Rosat P, et al. Preliminary note on thetreatment of vertebral angioma by percutaneous acrylic vertebropl-asty. Neurochirurgie 1987;33:166–8.
5. Jensen ME, Evans AJ, Mathis JM, et al. Percutaneous polymethyl-methacrylate vertebroplasty in the treatment of osteoporotic vertebralbody compression fractures: technical aspects. AJNR Am J Neurora-
diol 1997;18:1897–904.6. Garfin SR, Yuan HA, Reiley MA. New technologies in spine:
kyphoplasty and vertebroplasty for the treatment of painful osteopo-rotic compression fractures. Spine 2001;26:1511–5.
7. Lieberman IH, Dudeney S, Reinhardt MK, et al. Initial outcomeand efficacy of ‘‘kyphoplasty’’ in the treatment of painfulosteoporotic vertebral compression fractures. Spine 2001;26:1631–8.
8. Padovani B, Kasriel O, Brunner P, et al. Pulmonary embolism causedby acrylic cement: a rare complication of percutaneous vertebroplasty.AJNR Am J Neuroradiol 1999;20:375–7.
9. Ratliff J, Nguyen T, Heiss J. Root and spinal cord compression frommethylmethacrylate vertebroplasty. Spine 2001;26:E300–2.
10. Barr JD, Barr MS, Lemley TJ, et al. Percutaneous vertebroplasty forpain relief and spinal stabilization. Spine 2000;25:923–8.
11. Chiras J, Depriester C, Weill A, et al. Percutaneous vertebral surgery.Techniques and indications. J Neuroradiol 1997;24:45–59.
12. Mathis JM, Barr JD, Belkoff SM, et al. Percutaneous vertebroplasty:a developing standard of care for vertebral compression fractures.AJNR Am J Neuroradiol 2001;22:373–81.
13. Mathis JM, Eckel TS, Belkoff SM, et al. Percutaneous vertebroplasty:a therapeutic option for pain associated with vertebral compressionfracture. J Back Musculoskel Rehab 1999;13:11–7.
14. Weill A, Chiras J, Simon JM, et al. Spinal metastases: indications forand results of percutaneous injection of acrylic surgical cement.Radiology 1996;199:241–7.
15. Shapiro SA. Cranioplasty, vertebral body replacement, and spinalfusion with tobramycin-impregnated methylmethacrylate. Neurosur-
gery 1991;28:789–91.16. Kallmes DF, Schweickert PA, Marx WF, et al. Vertebroplasty in the
mid- and upper thoracic spine. AJNR Am J Neuroradiol 2002;23:1117–20.
17. Doita M, Marui T, Kurosaka M, et al. Contained rupture of theaneurysm of common iliac artery associated with pyogenic vertebralspondylitis. Spine 2001;26:E303–7.
18. Reichle FA, Tyson RR, Soloff LA, et al. Salmonellosis and aneurysmof the distal abdominal aorta: case report with a review. Ann Surg
1970;171:219–28.19. Wilson SE, Gordon HE, Van Wagenen PB. Salmonella arteritis: a
precursor of aortic rupture and pseudoaneurysm formation. Arch
Surg 1978;113:1163–6.
doi:10.1016/j.jocn.2006.06.014
Case Reports / Journal of Clinical Neuroscience 15 (2008) 89–93 93