aortic stenosis - home - american college of...
TRANSCRIPT

Aortic Stenosis:
Interventional Choice for a 70-year old-
SAVR, TAVR or BAV?
Interventional Choice for a 90-year old-
SAVR, TAVR or BAV?
Samin K Sharma, MD, FACC, FSCAI
Director Clinical & Interventional Cardiology
Zena and Michael a Weiner Professor of Medicine
Mount Sinai Hospital, NY

Aortic Stenosis
Normal 3-4 cm2
AS: - mild >1.5 cm2
- moderate 1.0-1.5 cm2
- severe <1.0 cm2
- critical <0.7 cm2
Etiology: Congenital: unicuspid
bicuspid
tricuspid
Acquired: rheumatic
calcific
cholesterolemia
rheumatoid
Aortic valve area:
5% at 70 yrs
10% at 80 yrs
18% at 90 yrs
Ross J, Braunwald E. Circulation 1968; 38: 61-67.

Interventional Choices for AS:
SAVR TAVR BAV
Sapien
CoreValve


Summary of Recommendations for AS:
Choice of Surgical or Transcatheter Intervention
Nishimura et al., J Thorac Cardiovasc Surg 2014;148:e1

Summary of Recommendations for AS:
Choice of Surgical or Transcatheter Intervention
Nishimura et al., J Thorac Cardiovasc Surg 2014;148:e1

Summary of Recommendations for AS:
Choice of Surgical or Transcatheter Intervention
Nishimura et al., J Thorac Cardiovasc Surg 2014;148:e1

Summary of Recommendations for AS:
Choice of Surgical or Transcatheter Intervention
Nishimura et al., J Thorac Cardiovasc Surg 2014;148:e1

Summary of Recommendations for AS:
Choice of Surgical or Transcatheter Intervention
Nishimura et al., J Thorac Cardiovasc Surg 2014;148:e1

Summary of Recommendations for AS:
Choice of Surgical or Transcatheter Intervention
Nishimura et al., J Thorac Cardiovasc Surg 2014;148:e1
BAV may provide palliative symptomatic benefit in these pts

Symptomatic Severe Aortic Stenosis
ASSESSMENT: High Risk AVR Candidate
3105 Total Patients Screened
PARTNER US Trial: Study Design
High Risk TA
ASSESSMENT:
Transfemoral
Access
TAVR
Trans
Femoral
Surgical
AVR
High Risk TF
Primary Endpoint: All Cause Mortality (1 yr)
(Non-inferiority)
TAVI
Trans
Apical
Surgical
AVR
1:1 Randomization 1:1 Randomization
VS VS Standard
Therapy
(usually BAV)
ASSESSMENT:
Transfemoral
Access
Not In Study
TAVR
Trans
Femoral
Primary Endpoint: All Cause Mortality
over length of trial (Superiority)
1:1 Randomization
VS
Total = 1058 patients
2 Parallel Trials High-surgical risk Gp
STS >10% Cohort A n= 700 In-operable
Gp Cohort B n=358
Yes No
Leon et al, NEJM 2010;363:1597

PARTNER Trial Cohort B: Time-to-Event Analysis
of Key Endpoints During 2 Years Follow-up
Makkar et al., NEJM 2012;366:1696
Rate of Death From Any Cause Rate of Re-hospitalization
20%
5yrs
94%
71%

PARTNER Trial Cohort A: Time-to-Event
Curves for Primary Endpoints at 3-Yrs
Kodali et al., NEJM 2012;366:1686
Death from Any Cause,
Intention-to-Treat Population
Death from Any Cause,
As-Treated Population

CoreValve Pivotal Trials Study Design
CoreValve US Pivotal Trials
Extreme Risk (Inoperable; STS mortality/morbidity >50%)
High Risk
Incremental STS mortality >15%
Iliofemoral Access
for 18 Fr Sheath
CoreValve
Iliofemoral
CoreValve
Non-
Iliofemoral
Randomization 1:1
N=790
SAVR CoreValve
Versus Yes No
N=487 N=147 N=392 N=388
Presented in ACC 2014 Presented in TCT 2013

CoreValve Extreme Risk Study: Primary Endpoints
N= 487
Popma et al, TCT 2013; JACC May 2014
1 Year Mortality Major Stroke

CoreValve High Risk Pivotal trial: Primary
Endpoint-- 1 Year All-cause Mortality
19.1%
4.5%
Surgical (N= 357)
14.2%
P = 0.04 for superiority
3.3%
TAVR (N= 390)
0 1 2 3 4 5 6 7 8 9 10 11 12 Months Post-Procedure
All-c
au
se
Mo
rta
lity
(%
)
Adams et al., N Engl J Med 2014;370:1790

CoreValve High-risk Pivotal Trial: 1-Year
Results
%
SAVR (n=357)
TAVR (n=390)
p=0.10
p=0.59
p=<0.001
p=0.004
p=0.03
p=<0.001
Adams et al., N Engl J Med 2014;370:1790
p=<0.001
Any stroke Major stroke AKI PPM Vasc MACCE Life-threatening/
compl disabling bleeding

159 86 70 44 31 15
163 91 71 46 31 15
Mean
Gra
die
nt
(mm
Hg
) V
alv
e A
rea (c
m²)
N =
EOA
Mean Gradient Error bars = ± 1 Std Dev
PARTNER Trial: Aortic Mean Gradient & Valve Area

0.0
0.5
1.0
1.5
2.0
0
10
20
30
40
50
ME
AN
GR
AD
IEN
T
(mg
) A
VA
(cm
2)
46±18
11.8±5.7 10±4.5 0.62±0.17
1.67±0.41 1.40±0.25
Baseline Post TAVR 5 Year
Mean Gradient Aortic Valve Area

Makkar et al., NEJM 2012;366:1696
Partner Trial Cohort B: TAVR for Inoperable
Severe Aortic Stenosis; Impact of Co-morbidities

What about Intermediate risk AS patients;
(defined as STS mortality risk of 4 to 8-10%)
Two Trials: PARTNER IIA (completed)
SURTAVI Trial (ongoing)

Severe AS Indication for AVR
Separate randomization for AS+CAD
Heart Team Discussion
• Europe: STS mortality risk score > 3% and < 8%
• US: STS mortality risk score > 4 and < 10%
Suitable for
Randomization 1:1 Randomization Non-randomization
Registries
TAVI AVR Control TAVI AVR
Medical
Management Primary Endpoint:
All cause Mortality
and Stroke at 2 yrs
CoreValve US Pivotal SURTAVI Trial: Design
Endpoint: All-cause Mortality at 2 yrs
VS
N = 1100
Yes No
N = 220
N = 220
VS
N = 1760

The PARTNER II Trial Study Design

The patient has the following:
CARDIAC STATUS NYHA Class IV
RISK FACTORS AND COMORBIDITIES History of CVA, previous CABG x4, chronic persistent A-Fib, s/p PPM Chronic Lung Disease/ COPD: Moderate FEV1: 1500cc %predicted: 55 Other: Frail, history of multiple GI bleeds, hyponatremia PREVIOUS CARDIAC INTERVENTIONS: CABG x4 in 1991, PCI x3 in remote and BAV in July 2013
Patient History
Age (years): 90
Gender: M
Height (ins): 72
Weight (Ibs): 160
Creatinine (mg) /dL: 1.03 Creatinine clearance (cc/min) : 60 BNP (pg/mL): 717 Coronary Art Disease: 3 Patent grafts Aortic Calcification: Severe

Echo Images: Annulus Measurement
22 Aortic annular size (mm)
0.41 Aortic valve area (cm2)
0.211 Aortic valve area index (cm2/m2)
48 Mean gradient (mmHg)
4.4 Peak velocity (m/sec)
52 LVEF (%)
Echo Image

CT Images: Annulus Measurements
CT Image
Ao Annulus mean diameter: 28.0 mm
32.6 x 23.4 Major x Minor aortic annulus diam
89.2 Aortic Annulus perimeter (28.4 x 3.14)
32.8 Max ascending Aorta diameter
35.8 – 39.3 Sinus of Valsalva diameter
23.5 – 30.5 Sinus of Valsalva height
29.5 – 30.9 Sinotubular Junction width (STJ)
(all in mm)

CT 3D Reconstructions

The patient has the following:
CARDIAC STATUS NYHA Class IV
RISK FACTORS AND COMORBIDITIES History of CVA, previous CABG x4, chronic persistent A-Fib, s/p PPM Chronic Lung Disease/ COPD: Moderate FEV1: 1500cc %predicted: 55 Other: Frail, history of multiple GI bleeds, hyponatremia PREVIOUS CARDIAC INTERVENTIONS: CABG x4 in 1991, PCI x3 in remote and BAV in July 2013
Patient History
Age (years): 90
Gender: M
Height (ins): 72
Weight (Ibs): 160
Risk Summary:
STS Score: 12% mortality
39% morbidity/mortality
Creatinine (mg) /dL: 1.03 Creatinine clearance (cc/min) : 60 BNP (pg/mL): 717 Coronary Art Disease: 3 Patent grafts Aortic Calcification: Severe

Treatment of Choice in this 90 Yr old AS pt
?Re-BAV
?SAVR
?TAVR
TAVR because
- 12% STS risk score making him
high risk for conventional SAVR
• Pt underwent 31mm CoreValve via RFA
percutaneous approach (using 2 perclose
sutures) under conscious sedation.




460 NSTEMI patients
460 NSTEMI patients
20 not ramdomized


Treatment of Choice in this 90 Yr old AS pt
?Re-BAV
?SAVR
?TAVR
TAVR because
- 12% STS risk score making him
high risk for conventional SAVR
• Pt underwent 31mm CoreValve via RFA
percutaneous approach (using 2 perclose sutures)
under conscious sedation.
• No complications, out of CCU next day and
discharged on post TAVR day 5.
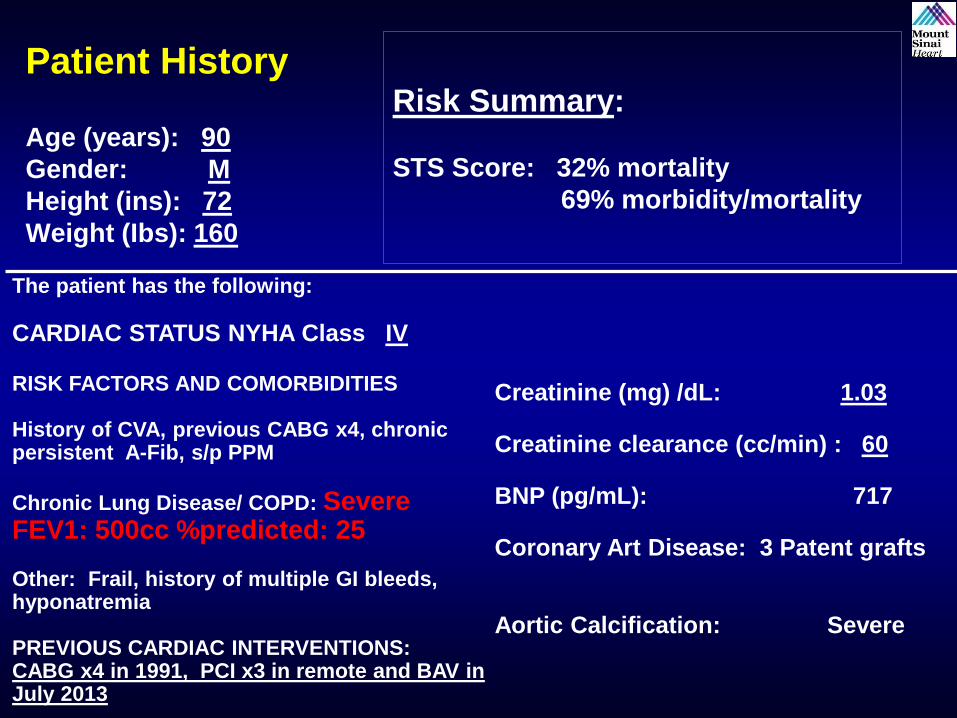
The patient has the following:
CARDIAC STATUS NYHA Class IV
RISK FACTORS AND COMORBIDITIES History of CVA, previous CABG x4, chronic persistent A-Fib, s/p PPM
Chronic Lung Disease/ COPD: Severe FEV1: 500cc %predicted: 25 Other: Frail, history of multiple GI bleeds, hyponatremia PREVIOUS CARDIAC INTERVENTIONS: CABG x4 in 1991, PCI x3 in remote and BAV in July 2013
Patient History
Age (years): 90
Gender: M
Height (ins): 72
Weight (Ibs): 160
Risk Summary:
STS Score: 32% mortality
69% morbidity/mortality
Creatinine (mg) /dL: 1.03 Creatinine clearance (cc/min) : 60 BNP (pg/mL): 717 Coronary Art Disease: 3 Patent grafts Aortic Calcification: Severe

Treatment of Choice in this 90 Yr old AS pt
?Re-BAV
?SAVR
?TAVR
Re-BAV because
- This pt with high comorbidity (FEV1 <500
cc) has extremely poor 1 year survival and
TAVR is unlikely to improve the long-term
survival
- BAV will provide palliative symptomatic
relief in these pts

The patient has the following: NYHA Class: III RISK FACTORS AND COMORBIDITIES previous CABG x4 in 2005, PAD Chronic Lung Disease/ COPD: Mild FEV1: 1900cc %predicted: 65 Other: No frailty PREVIOUS CARDIAC INTERVENTIONS PCI x2 last in 2/2013, recent cath showed patent all 3 grafts and patent PCI sites
Patient History Age (years): 71
Gender: M
Height (ins): 66
Weight (Ibs): 170
Creatinine (mg) /dL) 1.9 Creatinine clearance (cc/min) 30 BNP (pg/mL) 117 LVEF: 55% Aortic Calcification: Severe

Echo Images: Annulus Measurement

CT Images: Annulus Measurements

Iliofemorals

The patient has the following: NYHA Class: III RISK FACTORS AND COMORBIDITIES previous CABG x4 in 2005, PAD Chronic Lung Disease/ COPD: Mild FEV1: 1900cc %predicted: 55 Other: No frailty PREVIOUS CARDIAC INTERVENTIONS PCI x2 last in 2/2013, recent cath showed patent all 3 grafts and patent PCI sites
Patient History Age (years): 71
Gender: M
Height (ins): 66
Weight (Ibs): 170
Risk Summary:
STS Score: 4.5% mortality
8.2% morbidity/mortality
Creatinine (mg) /dL) 1.9 Creatinine clearance (cc/min) 30 BNP (pg/mL) 117 LVEF: 55% Aortic Calcification: Severe

Treatment of Choice in this 71 Yr old AS pt
?BAV
?SAVR
?TAVR
Pt was Randomized in the ongoing
Intermediate risk TAVR trial (SURTAVI)
because
- 4.5% STS risk score makes him ideal
for evaluation of TAVR vs. SAVR in
these intermediate risk AS pts
• Pt was randomized to SAVR and underwent
21mm Pericardial valve without complications.

The patient has the following in 8/2013: NYHA Class: IV and CCS class III angina on presentation to OSH with TnI 1.2U and transferred for treatment RISK FACTORS AND COMORBIDITIES previous CABG x4 in 1999 Chronic Lung Disease/ COPD: None FEV1: 2250cc %predicted: 95 Other: No frality PREVIOUS CARDIAC INTERVENTIONS Recent cath showed patent all 4 grafts with 80% stenosis of SVG to OM, LVEF 55%
Patient History Age (years): 78
Gender: M
Height (ins): 68
Weight (Ibs): 162
Creatinine (mg) /dL) 0.9 Creatinine clearance (cc/min) 70 BNP (pg/mL) 57 LVEF: 55% Aortic Calcification: Severe

ECG
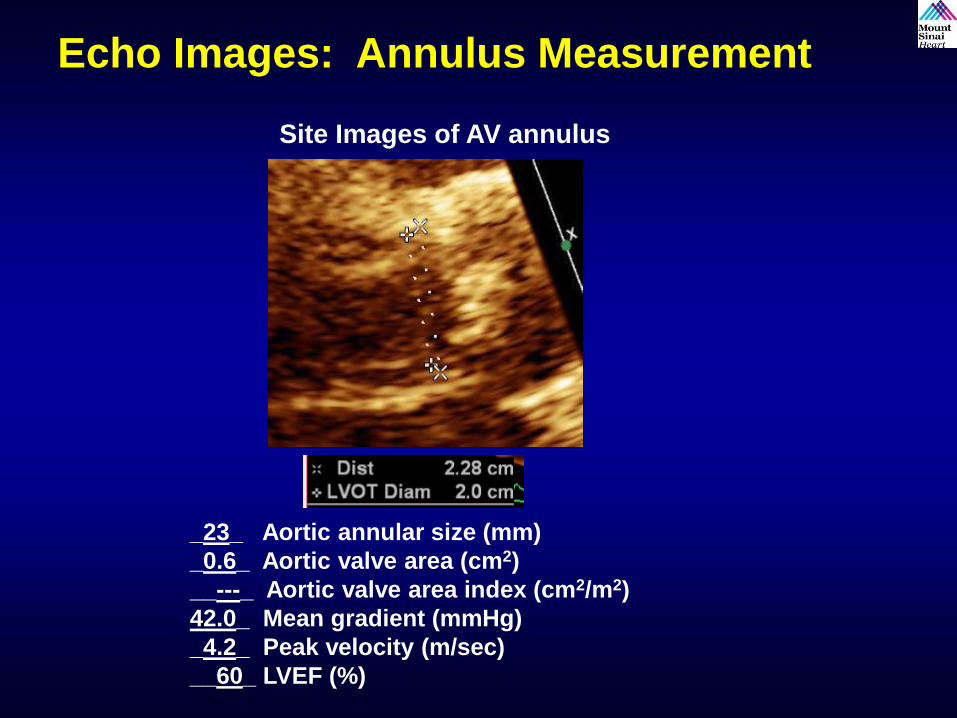
Echo Images: Annulus Measurement
Site Images of AV annulus
_23_ Aortic annular size (mm)
_0.6_ Aortic valve area (cm2)
__---_ Aortic valve area index (cm2/m2)
42.0_ Mean gradient (mmHg)
_4.2_ Peak velocity (m/sec)
__60_ LVEF (%)

CT Images: Annulus Measurements
Clinical Analyst’s Image
Ao Annulus mean diameter 26.1 mm
30.3 X 21.8_ Major x Minor aortic annulus diameter
82.9_ Aortic Annulus perimeter (26.4 x 3.14)
33.5 Max Ascending Aorta diameter
35.9 - 31.4 Sinus of Valsalva width
30.8-22.6 Sinus of Valsalva height (all in mm)
31.4 – 28.6 Sinotubular Junction width (STJ)

Hemodynamics: Baseline



460 NSTEMI patients
460 NSTEMI patients
20 not ramdomized


The patient has the following in 8/2013: NYHA Class: IV and CCS class III angina on presentation to OSH and transferred for treatment RISK FACTORS AND COMORBIDITIES previous CABG x4 in 1999 Chronic Lung Disease/ COPD: None FEV1: 2250cc %predicted: 95 Other: No frality PREVIOUS CARDIAC INTERVENTIONS Recent cath showed patent all 4 grafts with 80% stenosis of SVG to OM
Patient History Age (years): 78
Gender: M
Height (ins): 68
Weight (Ibs): 162
Creatinine (mg) /dL) 0.9 Creatinine clearance (cc/min) 70 BNP (pg/mL) 57 LVEF: 55% Aortic Calcification: Severe
Risk Summary:
STS Score: 2.8% mortality
4.2% morbidity/mortality

Treatment of Choice in this 78 Yr old AS pt
Presenting with CHF and NSTEMI/UA
?BAV+ PCI to SVG to OM
?SAVR+ CABG to OM
?TAVR+ PCI to SVG to OM
Pt was in CHF class IV and NSTEMI/unstable
angina. Had Heart Team discussion with CT
surgeon and recommended percutaneous
approach to stabilize the pt’s condition.





Treatment of Choice in this 78 Yr old AS pt
Presenting with CHF and NSTEMI/UA
?BAV+ PCI to SVG to OM
?SAVR+ CABG to OM
?TAVR+ PCI to SVG to OM
Pt was in CHF class IV and NSTEMI/unstable
angina. Had Heart Team discussion with CT
surgeon and recommended percutaneous
approach to stabilize the pt’s condition. Pt
then underwent BAV and BMS PCI to SVG to
OM. Did well and discharged home next day.

Treatment of Choice in this 78 Yr old AS pt
5 mths later for CHF Class III symptom
recurrence
?re-BAV
?SAVR
?TAVR
Pt had low STS risk (<4) score and
hence underwent conventional SAVR
using 23mm Pericardial valve without
any complications. No CABG needed
as BMS to SVG to OM was patent.
Risk Summary:
STS Score:
1.8% mortality
3.2% morbidity/mortality

Algorithm for Management of Severe AS: SAVR vs TAVR
Severe AS
Symptoms
No Yes
No Yes
LVEF <50%
Physically active
No Yes
Exercise Test
ressure below baseline
No Yes
Presence of risk factors and
low/intermediate individual surgical
risk
No Yes
Re-evaluate in 6 months SAVR
Contraindication
for AVR
No Yes
High risk for AVR Short life expectancy
Serious Comorbidity
STS >50%
No Yes No Yes
TAVR or SAVR
TAVR Med Rx
? BAV
Severe AS
No Yes
No Yes
LVEF <50%
Physically active
No Yes
Exercise Test
Symptoms or fall in blood
pressure below baseline
No Yes
Presence of risk factors and
low/intermediate individual surgical risk
No Yes
Re-evaluate in 6 months SAVR
No Yes
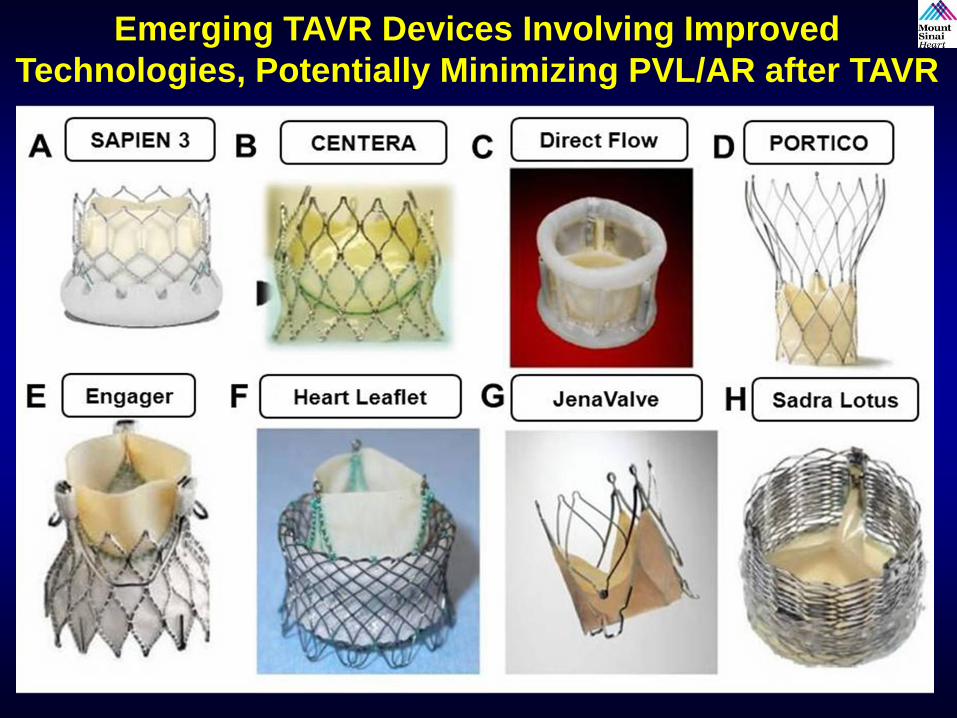
Emerging TAVR Devices Involving Improved
Technologies, Potentially Minimizing PVL/AR after TAVR

TAVR in Evolution (2014+)
Future Clinical Indications
• Valve-in-valve for bio-prosthetic aortic valve failure
• Intermediate (moderate) risk AS patients
• Asymptomatic severe AS
• Low flow-low gradient AS – impedance mismatch
• Aortic insufficiency; difficult with current
generation which is dependent on calcified native
AV to anchor the prosthesis