application for inclusion of non- vitamin k antagonists
TRANSCRIPT
1
Application for inclusion of non-vitamin K antagonists oral anticoagulant (NOACs) for the treatment of non-valvular atrial fibrillation in the WHO Model List of Essential Medicines 2019
Biraj Karmacharya, Department of Community Programs, Dhulikhel Hospital Kathmandu University Hospital, Nepal
Abiodun Adeoye, Cardiovascular Unit, Department of Medicine, University College Hospital, Ibadan / College of Medicine, University of Ibadan, Ibadan, Nigeria; Director, Community Cardiovascular Research Unit, Elyon Heart Rehabilitation Centre Mariachiara Di Cesare, Department of Natural Science, School of Science and Technology, Middlesex University London, UK Ferdous Hakim, Research and Publication Unit, World Health Organization, Bangladesh Mark D. Huffman, Departments of Preventive Medicine and Medicine, Northwestern University's Feinberg School of Medicine and Food Policy Division, The George Institute for Global Health
Asim Katbeh, International PhD Programme in Cardiovascular Pathophysiology and Therapeutics, CardioPaTh Xinyi Leng, Department of Medicine & Therapeutics, The Chinese University of Hong Kong, Shatin, Hong Kong SAR Lis Neubeck, School of Health and Social Care, Edinburgh Napier University; Honorary Professor, the University of Sydney Susan Wakil School for Nursing and Midwifery, Charles Perkins Centre, Sydney Stephanie Partridge, Westmead Applied Research Centre and Prevention Research Collaboration, Faculty of Medicine and Health, The University of Sydney Pablo Perel, Department of Non-communicable Disease Epidemiology, London School of Hygiene and Tropical Medicine
Ezequiel Zaidel, Cardiology Department, Sanatorio Güemes University Hospital, Pharmacology Department, School of Medicine, University of Buenos Aires Coordinated and submitted by Mariachiara Di Cesare, Department of Natural Science, School of Science and Technology, Middlesex University London, UK Xinyi Leng, Department of Medicine & Therapeutics, The Chinese University of Hong Kong, Shatin, Hong Kong SAR Ezequiel Zaidel, Cardiology Department, Sanatorio Güemes University Hospital, Pharmacology Department, School of Medicine, University of Buenos Aires

2
List of acronyms. AF or NVAF Non-valvular Atrial Fibrillation CrCl Creatinine Clearance GI Gastrointestinal INR International Normalized Ratio NOACs non-vitamin K antagonists oral anticoagulants OAC Oral anticoagulant RWD Real-world data VKAs vitamin K antagonists
Classes of recommendations in guidelines – definitions. Class I Evidence and/or general agreement that a given treatment or procedure is
beneficial, useful, effective. Class II
Conflicting evidence and/or a divergence of opinion about the usefulness/efficacy of the given treatment or procedure.
Class IIa Weight of evidence / opinion is in favour of usefulness/efficacy Class IIb Usefulness/efficacy is less well established by evidence/opinion. Class III Evidence or general agreement that the given treatment or procedure is not
useful/effective, and in some cases may be harmful. Levels of evidence in guidelines – definitions. Level of evidence A Data derived from multiple randomized clinical trials or meta-analyses. Level of evidence B Data derived from a single randomized clinical trial or large non-
randomized studies. Level of evidence C Consensus of opinion of the experts and/ or small studies, retrospective
studies, registries.
3
GENERAL ITEMS 1. Summary statement of the proposal for inclusion, change or deletion.
We propose the inclusion of the non-vitamin K antagonists oral anticoagulant (NOACs) for the treatment of non-valvular atrial fibrillation (AF) in the WHO Model List of Essential Medicines based on high-quality evidence demonstrating their superiority to vitamin K antagonists (VKAs) in reducing stroke and systemic embolism, as well as the composite endpoint of stroke and systemic embolism, all-cause mortality, and major bleeding including intracranial haemorrhage.
AF is a major public health issue affecting almost 50 million people globally, with projected increases in the incidence and prevalence in the next three decades due to population growth, aging, and better survival among patients with AF, though major treatment gaps remain. Patients with AF have a high risk of hospital admission, stroke and premature death. Timely and effective diagnosis and management of atrial fibrillation is required to prevent the complications of AF.
Patients with AF who are treated with VKAs must be carefully monitored with frequent dose titration to achieve therapeutic dosing measured by International Normalized Ratio (INR) to minimize the risk of bleeding while also reducing the risk of thromboembolic events, including stroke. Vitamin K-rich foods, alcohol, medicines, and illness frequently interfere with patients’ ability to stay within their therapeutic range, which further compounds the challenges of constant monitoring. NOAC represents a paradigm shift in the treatment of AF for stroke prevention because they do not require routine INR testing and because they have far fewer interactions. NOACs show a favourable balance between efficacy and safety compared with VKAs, with significant reductions in stroke, intracranial haemorrhage, and mortality. As a result, major clinical practice guidelines around the world recommend NOAC over warfarin for initial treatment of AF for stroke prevention. As costs have substantially declined since the introduction of NOACs in 2009, these drugs represent an effective, cost-effective, and affordable alternative to VKA for patients with AF, especially for those with limited access to health care for whom routine INR monitoring is difficult.
This application supports access to NOACs for AF patients around the world.
2. Relevant WHO technical department and focal point (if applicable). None 3. Name of organization(s) consulted and/or supporting the application. Arrhythmia Alliance Hearts4Heart Nigeria Stroke Society Pan-African Society of Cardiology Stroke Investigative Research & Education Network World Heart Federation 4. International Nonproprietary Name (INN) and Anatomical Therapeutic Chemical (ATC) code of the medicine.
Dabigatran etexilate B01AE07 Rivaroxaban B01AF01 Apixaban B01AF02 Edoxaban B01AF03 5. Dose forms(s) and strength(s) proposed for inclusion; including adult and age-appropriate paediatric dose forms/strengths (if appropriate).
Dabigatran: Oral capsules of 110 mg and 150 mg twice daily Rivaroxaban: Oral tablets of 15 mg and 20 mg once daily Apixaban: Oral tablets of 2.5 mg and 5 mg twice daily Edoxaban: Oral tablets of 30 mg and 60 mg once daily
4
Dabigatran - Full dose recommended: 150 mg twice daily The RE-LY trial tested a high and low dose (110 mg and 150 mg twice daily, respectively) for
anticoagulation of patients with non-valvular AF for prevention of thromboembolism; however, recommendations from regulatory agencies differ:
• European Medicines Agency: Dose reduction (110 mg twice daily) recommended for patients ≥80
years (sequential dosing strategy accepted in different countries) or concomitant verapamil use, and dose reduction considered for patients at high risk of bleeding (creatinine clearance 30 to 50 ml/min and additional factors for bleeding) [1].
• Food and Drug Administration: 150 mg twice daily for patients with creatinine clearance greater than 30 ml/min . For patients with creatinine clearance (CrCl) >30 mL/min, the recommended dose of dabigatran is 150 mg twice daily. For patients with severe renal impairment (CrCl 15-30 mL/min), the recommended dose is 75 mg twice daily. Consider reducing the dose of dabigatran to 75 mg twice daily when dronedarone or systemic ketoconazole is co-administered with dabigatran in patients with moderate renal impairment (CrCl 30-50 mL/min). Avoid use of dabigatran and P-glicoprotein inhibitors in patients with severe renal impairment (CrCl 15-30 mL/min). Dabigatran is contraindicated in severe renal failure or dialysis [2].
Rivaroxaban - Full dose recommended: 20 mg once daily
The ROCKET-AF trial used the adjusted dose (15 mg once daily) for patients with non-valvular AF with CrCl 30-50 ml/min. For Japan, accepted doses are 15 and 10 mg daily, respectively (J-ROCKET) [3, 4]. Rivaroxaban is contraindicated in severe renal failure or dialysis. Apixaban - Full dose recommended: 5 mg twice daily
The ARISTOTLE trial used adjusted dose (2.5 mg twice daily) if two out of three criteria in patients with non-valvular AF: over 80 years, creatinine over 1.5 g/dL (133 mmol/l), or weight less than 60 kg [5]. Apixaban is contraindicated if serum creatinine is > 2.5 mg/dl or if the patient is on dialysis.
Edoxaban - Full dose recommended: 60 mg once daily The ENGAGE AF-TIMI trial tested a high and low dose (60 and 30 mg daily) and used an adjusted dose
(30 or 15 mg daily, respectively) in patients with non-valvular AF if CrCl 30 to 50 ml/min or if P-glicoprotein inhibitors used (verapmil or quinidine), or body weight less than 60 kg [6].
The Cockroft Gault formula was used in trials.
The European Society of Cardiology/European Heart Rhythm Association (ESC/EHRA) guidelines also suggest the use of Factor Xa inhibitors in patients with CrCl 15 to 30 ml/min (with caution), and apixaban, dabigatran and edoxaban in patients with mild hepatic failure (Child-Pugh B) [7]. Contraindications:
• Apixaban o Active bleeding, malignant neoplasm, oesophageal varices, recent brain surgery, recent GI
ulcer, recent intracranial hemorrhage, recent ophthalmic surgery, recent spine surgery, significant risk of major bleeding, vascular aneurysm.
o Avoid in pregnancy, breast feeding, severe hepatic impairment, if CrCl less than 15 ml/min.
• Edoxaban o Active bleeding, arteriovenous malformations, GI ulceration, hepatic disease, oesophageal
varices, recent brain surgery, recent GI ulcer, recent intracranial hemorrhage, recent ophthalmic surgery, recent spine surgery, uncontrolled severe hypertension, vascular aneurysm.
o Avoid in pregnancy, breast feeding, severe hepatic impairment (use cautiously in mild to moderate impairment), in end stage renal disease or patient undergoing dialysis.

5
• Rivaroxaban
o Active bleeding, in acute coronary syndrome –malignant neoplasm, oesophageal varices, recent brain surgery, recent GI ulcer, recent intracranial hemorrhage, recent ophthalmic surgery, recent spine surgery, significant risk of major bleeding, vascular aneurysm.
o Avoid in pregnancy, breast feeding, liver disease with coagulopathy, CrCl less than 15 ml/min.
• Dabigatran
o Active bleeding, do not use as anticoagulant for prosthetic heart valve, malignant neoplasm, oesophageal varices, recent brain surgery, recent GI ulcer, recent intracranial hemorrhage, recent ophthalmic surgery, recent spine surgery, significant risk of major bleeding, vascular aneurysm.
o Avoid in pregnancy, breast feeding, severe liver disease especially if prothrombin time really prolonged, CrCl less than 30 ml/min.
Table 1. Current market availability of NOACs.
Dabigatran Etexilate Rivaroxaban Apixaban Edoxaban Canada Capsules (110/150 mg) Tablets (10/15/20 mg) Tablets (2.5/5 mg) Tablets (15/30/60 mg) UK Capsules (75/110/150 mg) Tablets (2.5/10/15/20 mg) Tablets (2.5/5 mg) Tablets (15/30/60 mg) USA Capsules (75/150 mg) Tablets (10/15/20 mg) Tablets (2.5/5 mg) Tablets (15/30/60 mg) EU Capsules (75/110/150 mg) Tablets (2.5/10/15/20 mg) Tablets (2.5/5 mg) Tablets (15/30/60 mg) India Hard gelatine capsules
(75/110/150 mg) Tablets (15/20 mg) Tablets (2.5/5 mg)
Bangladesh Capsules (75/110 mg) Tablets (10/20 mg) Tablets (2.5/5 mg) Nepal Capsules (75/110/150 mg) Mexico Capsules (75/110/ mg) Tablets (10/15/20 mg) Tablets (2.5) Argentina Capsules (75/110/150 mg) Tablets (2.5/10/15/20 mg) Tablets (2.5/5 mg) Brazil Capsules (75/110/ mg) Tablets (10 mg) Tablets (2.5 mg) Tablets (30/60 mg)
Use of NOACs for venous thromboembolism (VTE) is not covered in this application but represents
another potential therapeutic target. 6. Whether listing is requested as an individual medicine or as representative of a pharmacological class.
The listing is as a representative of a pharmacological class: (□) Dabigatran Other NOACs include: Rivaroxaban Apixaban Edoxaban
The rationale for the choice of Dabigatran as square box: first NOACs licenced for marketing, more evidence available (10 years) in real world data, currently available in most countries compared to other NOACs, generic dabigatran already available in some countries (e.g. India). In addition treatments to reverse anticoagulation effects due to dabigatran exist (idarucizumab). TREATMENT DETAILS, PUBLIC HEALTH RELEVANCE AND EVIDENCE APPRAISAL AND SYNTHESIS 7. Treatment details (requirements for diagnosis, treatment and monitoring)
Atrial fibrillation (AF) is an atrial tachyarrhythmia characterised by predominantly uncoordinated atrial activation with consequent deterioration of atrial mechanical function. AF is classified as [8]:
• First diagnosed AF: AF that has not been diagnosed before, irrespective of the duration of the arrhythmia or the presence and severity of AF-related symptoms.

6
• Paroxysmal AF: Self-terminating, in most cases within 48 hours. • Persistent AF: AF that lasts longer than 7 days, including episodes that are terminated by
cardioversion, after 7 days or more. • Long-standing persistent AF: Continuous AF lasting for ≥1 year when it is decided to adopt a rhythm
control strategy. • Permanent AF: AF that is accepted by the patient (and physician) to be permanent with no plan for
rhythm control.
Diagnosis and assessment of atrial fibrillation [9] - Manual pulse palpation to assess for the presence of an irregular pulse in people presenting any of the
following symptoms: breathlessness/dyspnoea, palpitations, syncope/dizziness, chest discomfort, stroke/transient ischaemic attack;
- Electrocardiogram (ECG) in all people, whether symptomatic or not, in whom atrial fibrillation is suspected because an irregular pulse has been detected;
- In people with suspected paroxysmal atrial fibrillation undetected by standard ECG recording: 24-hour ambulatory ECG monitor in those with suspected asymptomatic episodes or symptomatic episodes less than 24 hours apart, and an event recorder ECG in those with symptomatic episodes more than 24 hours apart;
- Transthoracic echocardiography (TTE) in people with atrial fibrillation: for whom a baseline echocardiogram is important for long-term management; for whom a rhythm-control strategy that includes cardioversion (electrical or pharmacological) is being considered; in whom there is a high risk or a suspicion of underlying structural/functional heart disease (such as heart failure or based on the presence of heart murmur) that influences their subsequent management (for example, choice of antiarrhythmic drug); in whom refinement of clinical risk stratification for antithrombotic therapy is needed.
AF increases the risk of stroke and systemic embolism. Since the risk of AF-associated stroke is not
uniform and depends on patients’ ages, sex and other comorbidities, clinical risk scores have been formulated to stratify for prevention of stroke and untoward bleeding with thromboprophylaxis use. 7.1. Stroke risk stratification
In 2010, the CHA2DS2-VASc score was developed, validated, and demonstrated to be superior to the CHADS2 score [10] in identifying low-risk patients in whom anticoagulation was unlikely to confer benefit [11].
• C = congestive heart failure or left ventricular dysfunction (1 point) • H = hypertension (1 point) • A2 = age > 75 years old (2 points) • D = diabetes mellitus (1 point) • S2 = stroke or transient ischemic attack or thromboembolism (2 points) • V = vascular disease (prior myocardial infarction, peripheral artery disease, or aortic plaque) (1 point) • A = age 65-74 years old (1 point) • Sc = sex category (i.e. female gender) (1 point)
In the first publication of CHA2DS2-VASc score [11], the annual incidence rates of stroke or systemic
embolism were 0%, 0.6%, and 3% in scores 0, 1, and ≥2 , respectively. The CHA2DS2-VASc score has improved discrimination of patients with very low risk of stroke compared to CHADS2 score (annual incidence rates of stroke or systemic embolism were 1.4%, 2.4%, and 3.2%, for CHADS2 scores 0, 1, and ≥2, respectively). The CHA2DS2-VASc score’s C-statistic for predicting stroke or systemic embolism was 0.61 [95% CI, 0.51-0.69] compared with a C statistic of 0.56 [95% CI, 0.45-0.62] for the CHADS2 score. Further cohorts provided external validation of the CHA2DS2-VASc score and its improved performance, including nationwide cohorts from Denmark [12], Taiwan [13], the United Kingdom [14], and Sweden [15].
7
The CHA2DS2-VASc score is now recommended for risk stratification by major clinical practice guidelines such as the European Society of Cardiology (ESC), American College of Cardiology/American Heart Association (ACC/AHA), and the National Institute for Health and Care Excellence (NICE). 7.2. Bleeding risk assessment
Assessment of bleeding risk before starting anticoagulation among patients with AF is important. As for stroke risk stratification, several bleeding risk scores have also been developed and validated for clinical practice. However, bleeding risk scores should be used only to identify patients at risk for bleeding with the aim to have more regular review and follow-up, and importantly, to address reversible bleeding-related risk factors such as uncontrolled hypertension, labile INRs (for a warfarin user) and concomitant use of aspirin, NSAIDs or alcohol excess. The HAS-BLED score has been proposed as a simple clinical score to predict clinically relevant bleeding in AF patients [16].
• H = hypertension (1 point) • A = abnormal renal and liver function (1 point each) • S = stroke (1 point) • B = bleeding (1 point) • L = labile INRs (1 point) • E = elderly (age > 65 years old) (1 points) • D = drugs or alcohol (1 point each)
A HAS-BLED score ≥3 indicates a high risk of bleeding (≥3.74 bleeds per 100 Patient-years compared to less than 2% in HAS-BLED ≤2), and previous studies have demonstrated that the HAS-BLED score performed better than other bleeding scores.
8
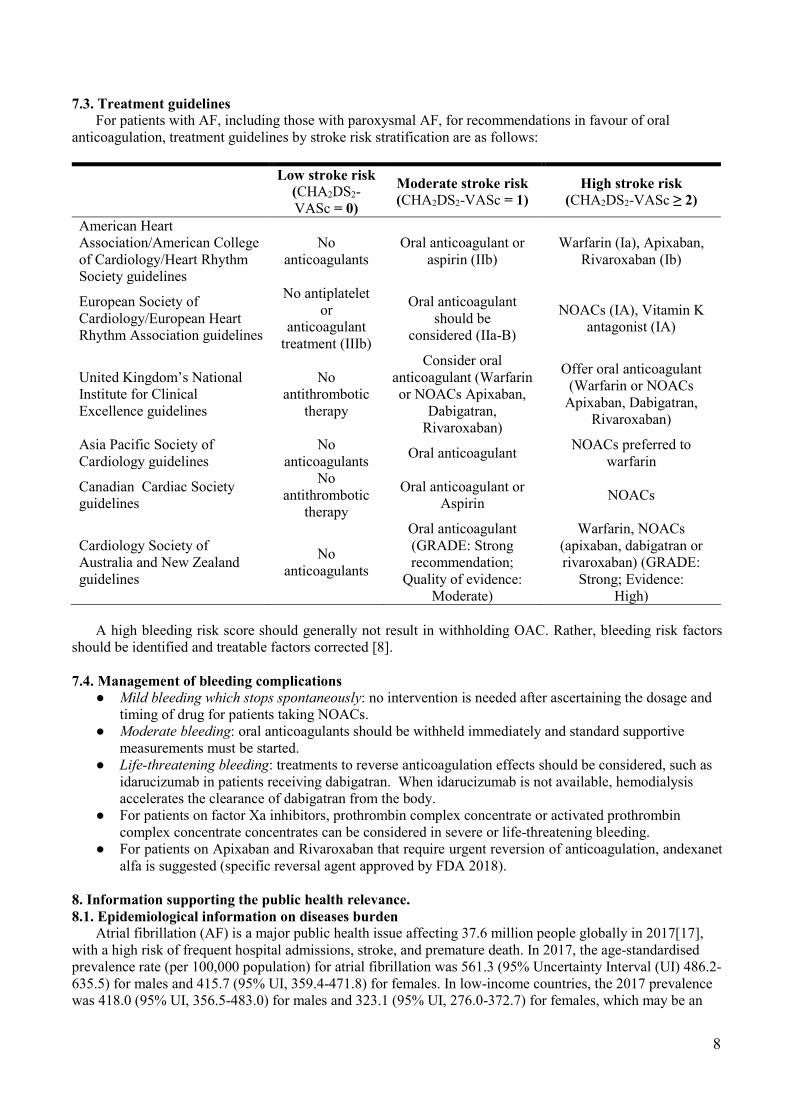
7.3. Treatment guidelines For patients with AF, including those with paroxysmal AF, for recommendations in favour of oral
anticoagulation, treatment guidelines by stroke risk stratification are as follows:
Low stroke risk
(CHA2DS2-VASc = 0)
Moderate stroke risk (CHA2DS2-VASc = 1)
High stroke risk (CHA2DS2-VASc ≥ 2)
American Heart Association/American College of Cardiology/Heart Rhythm Society guidelines
No anticoagulants
Oral anticoagulant or aspirin (IIb)
Warfarin (Ia), Apixaban, Rivaroxaban (Ib)
European Society of Cardiology/European Heart Rhythm Association guidelines
No antiplatelet or
anticoagulant treatment (IIIb)
Oral anticoagulant should be
considered (IIa-B)
NOACs (IA), Vitamin K antagonist (IA)
United Kingdom’s National Institute for Clinical Excellence guidelines
No antithrombotic
therapy
Consider oral anticoagulant (Warfarin or NOACs Apixaban,
Dabigatran, Rivaroxaban)
Offer oral anticoagulant (Warfarin or NOACs
Apixaban, Dabigatran, Rivaroxaban)
Asia Pacific Society of Cardiology guidelines
No anticoagulants Oral anticoagulant NOACs preferred to
warfarin
Canadian Cardiac Society guidelines
No antithrombotic
therapy
Oral anticoagulant or Aspirin NOACs
Cardiology Society of Australia and New Zealand guidelines
No anticoagulants
Oral anticoagulant (GRADE: Strong recommendation;
Quality of evidence: Moderate)
Warfarin, NOACs (apixaban, dabigatran or rivaroxaban) (GRADE:
Strong; Evidence: High)
A high bleeding risk score should generally not result in withholding OAC. Rather, bleeding risk factors
should be identified and treatable factors corrected [8]. 7.4. Management of bleeding complications
● Mild bleeding which stops spontaneously: no intervention is needed after ascertaining the dosage and timing of drug for patients taking NOACs.
● Moderate bleeding: oral anticoagulants should be withheld immediately and standard supportive measurements must be started.
● Life-threatening bleeding: treatments to reverse anticoagulation effects should be considered, such as idarucizumab in patients receiving dabigatran. When idarucizumab is not available, hemodialysis accelerates the clearance of dabigatran from the body.
● For patients on factor Xa inhibitors, prothrombin complex concentrate or activated prothrombin complex concentrate concentrates can be considered in severe or life-threatening bleeding.
● For patients on Apixaban and Rivaroxaban that require urgent reversion of anticoagulation, andexanet alfa is suggested (specific reversal agent approved by FDA 2018).
8. Information supporting the public health relevance. 8.1. Epidemiological information on diseases burden
Atrial fibrillation (AF) is a major public health issue affecting 37.6 million people globally in 2017[17], with a high risk of frequent hospital admissions, stroke, and premature death. In 2017, the age-standardised prevalence rate (per 100,000 population) for atrial fibrillation was 561.3 (95% Uncertainty Interval (UI) 486.2-635.5) for males and 415.7 (95% UI, 359.4-471.8) for females. In low-income countries, the 2017 prevalence was 418.0 (95% UI, 356.5-483.0) for males and 323.1 (95% UI, 276.0-372.7) for females, which may be an
9
underestimate due to lower diagnosis rates in low-income countries compared with other settings. In 2017, the estimated age adjusted disability-adjusted life years resulting from AF were 84.0 for males and 72.7 for females (per 100 000 population) [17]. Current projections suggest an expected increase in the incidence and prevalence of AF in the next three decades [18-20].
Effective, evidence-based treatments to prevent AF-related strokes exist. A 2007 systematic review, including 29 trials and over 28,000 participants, demonstrated that effective treatment with Vitamin K Antagonist (VKAs) oral anticoagulants reduce the risk of risk of stroke or systemic thromboembolic in people with AF by two-thirds (95% confidence interval [CI], 49% to 74%) [21]. However, patients treated with VKAs must be carefully controlled within a therapeutic range as measured by the International Normalised Ratio (INR) 2.0-3.0 to effectively reduce the risk of embolic stroke while minimizing bleeding risks [21]. Furthermore, dietary intake, alcohol, medications, and illness can all affect INR levels. Thus, treatment with VKA requires regular monitoring to ensure optimal time in therapeutic range, which is challenging for many patients and health systems. For example, the US Outcome Registry for Better Informed Treatment of Atrial Fibrillation (ORBIT-AF) including 5,210 patients with AF treated with VKA estimated that only 65% of time was spent in therapeutic range, with those at greatest risk of having a stroke being least likely to be within the therapeutic range [22]. Rates of time in therapeutic range are lower in LMICs [23]. A post-hoc analysis of the ORBIT-AF study showed the median time is spent in therapeutic range in middle-income countries varied between 46% to 65%, whereas in high-income countries it varied between 55% to 78% [24]. In addition, patient-specific characteristics were associated with lower likelihood of being therapeutic range, including factors such as lower income, frequent hospitalisation, and polypharmacy [25]. The laboratory monitoring and dose adjustment required by VKAs represent a major challenge in resource-limited settings. An analysis of management of AF in 46 countries using the RE-LY Atrial Fibrillation Registry has shown that the use of oral anticoagulation among patients with a CHADS2 score ≥2 was greatest in North America (66%) but was only 11% in China and that the mean time in the therapeutic range was 62% in Western Europe, 51% in North America, but only between 32% and 40% in India, China, Southeast Asia, and Africa [23].
Patient preferences for oral anticoagulants are important to ensure medication adherence and subsequent AF-related stroke and systemic embolism risk reduction. In a 2017 systematic review, 27 studies conducted in 12 different countries (n=7226) examined patient preferences towards OAC. Sixteen of the 27 studies compared OAC to no treatment [26]. The authors concluded that most studies show that patients are willing to accept bleeding risks if they can be assured of a certain threshold in stroke-risk reduction. However, within this systematic review, 11/27 publications (n=3737) examined preferences between warfarin and NOACs. Eight of 11 of the included studies, using either survey or discrete choice methodology, showed that patients prefer NOACs treatment based on convenience and reduced need for blood tests and fewer dietary restrictions when compared to warfarin. In the 3/11 studies where preference was for warfarin, all were conducted in high-income countries and among current anticoagulant users. The patients noted that they were anxious about the lack of laboratory testing and would prefer to be continued to be reviewed regularly by an oral anticoagulant clinic [26]. However, a 2016 Canadian survey suggests that the key influence in decision making about use of warfarin or NOACs is physician preference and bias for laboratory monitoring, which consequently influences the choices of the patients [27]. In Germany, experiment including 486 people with AF demonstrated that patients significantly preferred the attribute levels associated with NOAC use (in order of patients' importance) "once daily intake", "bridging necessary", "distance to practitioner of ≤1 km, "interactions with food/nutrition" and "need of INR controls/dose adjustment" [28].
In countries where access to regular monitoring of warfarin is limited by distance and accessibility the
consideration about regular monitoring is likely of lower importance compared to the ability to have an effective drug with fewer restrictions on lifestyle and easier convenience [29]. 8.2. Assessment of current use
NOACs are used as single therapy for stroke and systemic embolism prevention in patients with non-valvular AF. Data from the facility-based Global Anticoagulant Registry in the Field (GARFIELD-AF) from 35 countries, show a decrease in VKAs therapy (from 83% to 51%) and an increase in the NOACs use (from 4% to 37%) since 2010 (Figure 1) [30]. Similarly, in the National Cardiovascular Data registry Practice

10
INNovation And CLinical Excellence (NCDR PINNACLE) from US, the use of oral anticoagulant therapy increased from 52% to 61% after the introduction of NOACs since 2009 (Figure 2) [31].
Figure 1. Evolution in baseline treatment for patients enrolled in sequential cohort of GARFIELD-AF (source: www.af.garfieldresgistry.org)
Figure 2. Anticoagulant use by year/quarter [31]. 8.3. Target population
The target population includes patients with non-valvular AF who are at high risk of stroke (CHA2DS2-VASc >2). Some guidelines suggest use of NOACs in people with low-moderate risk of stroke (CHA2DS2-VASc=1). The Canadian and Australian guidelines suggest not including female sex in classifications. Patients with mechanical heart valves and those with moderate-to-severe mitral stenosis, mostly related to rheumatic heart disease, were excluded from randomized trials of NOACs, so for this proposal, non-valvular atrial fibrillation will refer to patients with atrial fibrillation without these conditions [7]. For countries with moderate to high prevalence of rheumatic heart disease, history of rheumatic disease, acute rheumatic fever, or cardiac murmurs, an echocardiogram should be performed to determine if the patient has rheumatic heart disease-related AF [32], based on the World Heart Federation guideline for diagnosis of rheumatic heart disease [33]. Currently an ongoing trial is testing the efficacy and safety rivaroxaban for rheumatic heart disease-related AF [34].
11
8.4. Likely impact of treatment on the disease NOACs reduce risk of stroke and systemic embolism, mortality, and bleeding in patients with non-
valvular AF. A 2016 modelling analysis evaluated possible trends of ischaemic stroke and death rates in AF patients comparing the scenario of unchanged oral anticoagulant use (45% of patients on VKA; 55% on NOACs) to a scenario of relative increase in NOAC use. In East Asia, NOACs uptake to 90% would help preventing 206,315 ischaemic strokes and 139,353 deaths over the period of 20 years from 2031 to 2050 when compared to the scenario of unchanged use of oral anticoagulants [35]. Similarly in Europe, the introduction of NOACs in 2010 has been estimated to have led to >88,000 fewer strokes, thromboembolisms, and deaths each year. If the prevalence rate of use of edoxaban were to increase from 11% in 2013 to 75% in 2030, then an additional 12,000 cases of stroke, thromboembolism, and death would be avoided annually [36]. 9. Review of benefits: summary of evidence of comparative effectiveness. 9.1. Summary of evidence of comparative effectiveness in RCTs
The efficacy and safety of each NOAC versus warfarin in preventing stroke and systemic embolism in non-valvular AF patients have been investigated in individual pivotal RCTs: the RE-LY [37], ROCKET-AF [3], J-ROCKET AF [4], ARISTOTLE [25], ENGAGE AF-TIMI 48 [6] trials. Please refer to Section 5 in this proposal for the NOAC and dose(s) investigated in each trial.
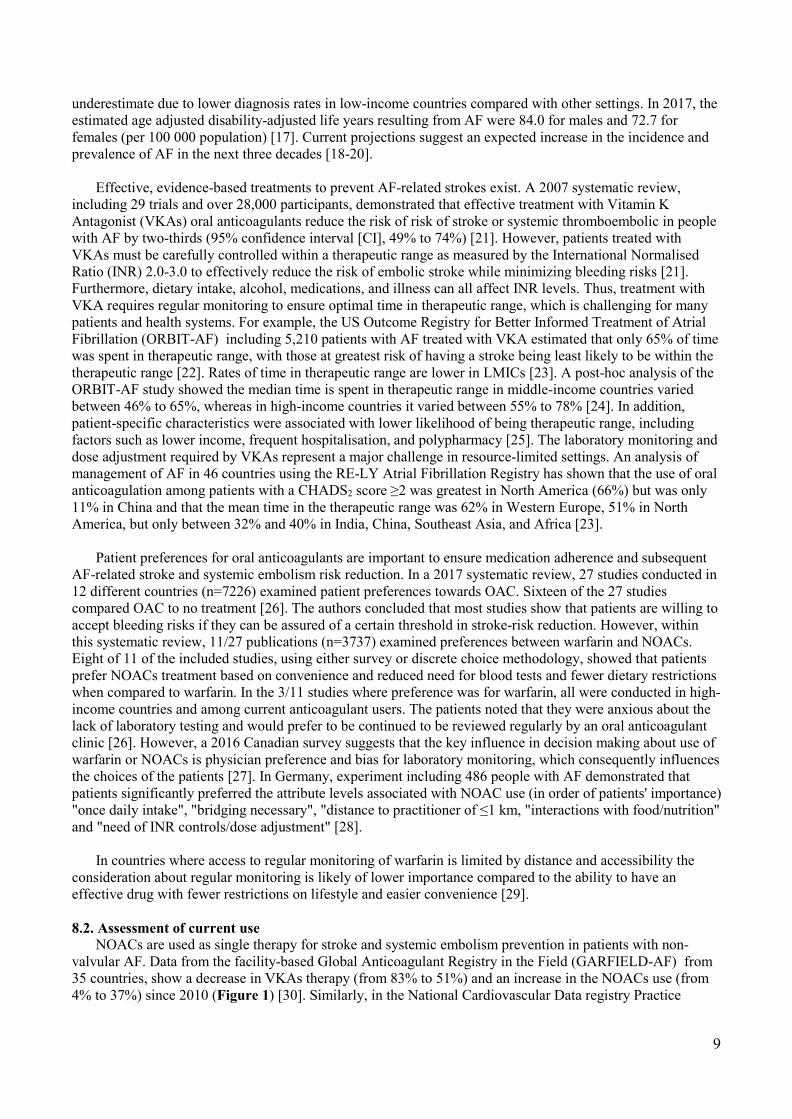
The overall efficacy and safety of NOACs versus warfarin in preventing stroke and systemic embolism in
non-valvular AF patients have been summarized in numerous systematic reviews and meta-analysis. For instance, Ruff et al. published a meta-analysis of 4 of the 5 RCTs [38]. We herein update the meta-analysis by adding data from the J-ROCKET AF trial [4]. In the 5 RCTs (59,819 patients), NOACs significantly reduced the risk of stroke and systemic embolism compared with warfarin in NVAF patients (RR 0.80, 95% CI 0.71-0.91; p=0.0003; Figure 3). A Grading of Recommendations, Assessment, Development and Evaluation (GRADE) Evidence Profile table for the effects of NOACs versus warfarin in preventing stroke and systemic embolism in RCTs is attached in Annex 1. The quality of evidence is high for NOACs in preventing stroke and systemic embolism compared to warfarin, given that the evidence was based on RCTs with low risk of bias with no downgrading for study limitations, indirectness of evidence, imprecision, heterogeneity, nor publication bias.
Figure 3. Forest plot showing the effect of NOACs versus warfarin in preventing stroke and systemic embolism in non-valvular AF patients based on data from 5 RCTs.
9.2. Summary of evidence of comparative effectiveness in real-world practice We also systematically searched in the literature and summarized existing evidence on the efficacy and safety of NOACs versus vitamin K antagonists in preventing stroke and systemic embolism in non-valvular AF patients in unselected populations (also known as real-world data). The primary efficacy outcome was stroke and systemic embolism, and the primary safety outcome was major bleeding as defined in each study. 9.2.1. Methods: Search strategy, study screening and selection
In September 2018, we searched PubMed and OVID (covering major databases of evidence-based medicine reviews, EMBASE, and MEDLINE), as well as the China Academic Journals Full-text Database and the Virtual Health Library Regional Portal for relevant primary studies and systematic reviews with full-text articles published in any language since 1 January 2009 until 13 September 2018. Briefly, the search terms

12
included non-vitamin k antagonist anticoagulants (NOAC), dabigatran, rivaroxaban, apixaban, edoxaban, vitamin k antagonist (VKA), warfarin, and nonvalvular atrial fibrillation (NVAF). We also manually searched references in pertinent review articles. The PICO structure for the analysis was:
Population: Patients with non-valvular AF Intervention: NOACs Comparison: VKA Outcome: Efficacy - stroke and systemic embolism; Safety – major bleeding
Inclusion criteria for a primary study were as follows: 1) studies reporting real-world data with a sample
size >1,000 participants; 2) any NOAC compared with VKAs (predominantly warfarin) in the efficacy and safety of preventing stroke and systemic embolism in NVAF patients. Studies reporting real-world data in our research included cohort studies, prospective registries, and retrospective analyses of insurance claims and electronic health records.
We reviewed the records retrieved from literature search to eliminate duplications and irrelevant articles, and selected the studies for qualitative and quantitative synthesis. For studies reporting data regarding the same NOAC in obviously overlapping study populations (in the same country/region), the one with the largest sample size or longest recruiting period was included for analysis. For an article with doubt regarding whether or not to be included in qualitative or quantitative analysis, agreement was achieved among three authors (X.L., E.Z., A.K.). 9.2.2 Methods: Data extraction and synthesis
We extracted relevant data from the primary studies and synthesized the data in Cochrane Review Manager (version 5.3). Random-effects models were used to estimate the efficacy and safety of each and all NOACs versus VKA (warfarin) in treating NVAF patients, presented in risk ratios (RR) and the 95% confidence intervals (CI). Publication bias of the primary studies was assessed by visual inspection of the funnel plot. Between-study heterogeneity was tested by the Cochran’s Q (χ2) and I2 statistics. Two-sided p values <0.05 and <0.10 were considered statistically significant, in estimation of the RRs, and between-study heterogeneity, respectively. Heterogeneity was not considered substantial when I2<50%. Summaries of evidence and assessment of evidence quality were conducted using the GRADE tool (https://gdt.gradepro.org/app).

13
9.2.3 Results: Study selection and description Figure 4 shows the flow chart for study screening and selection.
Figure 4. Flow chart for study screening.
Overall, 50 studies reported real-world data from a large range of countries, including (in alphabetical order): Canada (1 study) [39], Denmark (5 studies) [40-44], France (1 study) [45], Germany (1 study) [46], Hong Kong (1 study) [47], Israel (1 study) [48], Italy (2 studies) [49, 50], Japan (3 studies) [51-53], Malaysia (1 study) [54], New Zealand (1 study) [55], Norway (1 study) [56], South Korea (2 studies) [57, 58], Sweden (2 studies) [59, 60], Taiwan (4 studies) [61-64], the United Kingdom (1 study) [65], and the United States (11 studies) [66-75]. Other studies reported relevant real-world data in >1 countries or regions, as an individual study [30, 76] or as a systematic review [77-86]. Data were mostly from high- or middle-high-income countries or regions, while there were relatively less data from LMICs.

14
9.2.4 Results: Efficacy of NOACs versus VKA (predominantly warfarin) Of the 23 studies included in quantitative data synthesis, 12 studies reporting real-world data (n=520,859
patients) were analyzed for the primary efficacy outcome (stroke and systemic embolism; Figure 5). In these studies, NOACs were associated with a reduced risk of stroke and systemic embolism compared with warfarin in patients with non-valvular AF (RR 0.79, 95% CI 0.71-0.89; p<0.001). No apparent publication bias was observed by visual inspection of the funnel plot. There was substantial between-study heterogeneity (I2= 87%; p<0.001) for the effect of NOACs versus warfarin in preventing stroke and systemic embolism in patients with non-valvular AF in studies reporting real-world data. There were also significant between-study heterogeneities in meta-analysis below of the effects of each NOAC versus warfarin. Some of the key factors that would explain the heterogeneity are the definitions used to assign events, time of follow-up, study setting, and age of patients in each study.
Figure 5. Forest plot showing the efficacy of NOACs versus warfarin in preventing stroke and systemic embolism in patients with non-valvular AF based on data from studies reporting real-world data.
A GRADE Evidence Profile table for the effects of NOACs versus warfarin in preventing stroke and systemic embolism in real-world practice is attached in Annex 2; the quality of evidence is very low, given that the evidence was based on observational studies with heterogenous findings (I2=87%), but there was no downgrading for indirectness of evidence nor imprecision among these studies.
We also compared the efficacy of each NOAC versus VKAs (predominantly warfarin) separately in real-
world practice (Figures 6-8). In each comparison, the NOAC was associated with a significant lower risk of stroke and systemic embolism than warfarin, except that no real-world data were available regarding the associations between edoxaban versus warfarin and risks of stroke and systemic embolism. These data are reassuring that the application of NOACs into routine clinical practice show a similar direction and magnitude of effect as seen in randomized trials.
The GRADE Evidence Profile tables for the effects of each NOAC versus warfarin among patients with
non-valvular AF in studies reporting real-world data in preventing stroke and systemic embolism are attached in Annex 3-5. The quality of evidence is very low for dabigatran, rivaroxaban and apixaban, respectively, given that the evidence was based on observational studies with heterogenous findings (I2=86%, 82%, 91%), but there was no downgrading due to indirectness of evidence nor imprecision among these studies.

15
Figure 6. Forest plot showing the effect of dabigatran versus warfarin in preventing stroke and systemic embolism in NVAF patients based on data from studies reporting real-world data.
Figure 7. Forest plot showing the effect of rivaroxaban versus warfarin in preventing stroke and systemic embolism in NVAF patients based on data from studies reporting real-world data.
Figure 8. Forest plot showing the effect of apixaban versus warfarin in preventing stroke and systemic embolism in NVAF patients based on data from studies reporting real-world data. Results are similar with previous systematic reviews and meta-analyses [38, 86, 87]. 10. Review of harms and toxicity: summary of evidence of safety 10.1 Summary of evidence of safety in RCTs
As outlined in Section 9, the efficacy and safety of each NOAC versus warfarin in preventing stroke and systemic embolism in patients with non-valvular AF have been investigated in individual pivotal randomized trials, and the overall effects of NOACs versus warfarin have been reported in previous systematic reviews and meta-analyses. We updated the meta-analysis by Ruff et al. [38] by adding data from the J-ROCKET AF trial [4]. In the 5 RCTs (59,776 patients), NOACs were associated with a significantly lower risk of major bleeding compared with warfarin in NVAF patients (RR 0.86, 95% CI 0.74-0.99; p=0.04; Figure 9). A GRADE Evidence Profile table for the association between NOACs versus warfarin and risk of major bleeding in RCTs is attached in Annex 1; the quality of evidence is moderate, given that the evidence was based on RCTs with low risk of bias but inconsistent findings (I2=77%).

16
Figure 9. Forest plot showing the risks of major bleeding in non-valvular AF patients treated with NOACs versus warfarin based on data from 5 RCTs. 10.2. Summary of evidence of safety in real-world practice
The methods for literature search, study screening and selection, data synthesis, and evidence quality assessment are described in Section 9. 10.2.1. Results: Safety of NOACs versus VKA (predominantly warfarin)
Of the 23 studies included in quantitative data synthesis, 17 studies reporting real-world data (n=622,720 patients) were analyzed for the primary safety outcome (major bleeding; Figure 10). In these studies, NOACs were associated with a lower risk of major bleeding compared with warfarin in NVAF patients (RR 0.72, 95% CI 0.64-0.80; p<0.001). No apparent publication bias was observed by visual inspection of the funnel plot. A GRADE Evidence Profile table for the associations between NOACs versus warfarin and risks of major bleeding in studies reporting RWD is attached in Annex 2; the quality of evidence is very low, given that the evidence was based on observational studies with substantial heterogeneity (I2=90%), but there was no downgrading due to indirectness of evidence nor imprecision among these studies. Similar to the efficacy outcome, the direction and magnitude of the safety signal for NOACs compared with warfarin is similar in both randomized and non-randomized studies, which is reassuring for their widespread use.
Figure 10. Forest plot showing the risks of major bleeding in patients with non-valvular AF treated with NOACs versus warfarin based on data from RCTs and studies reporting real-world data.
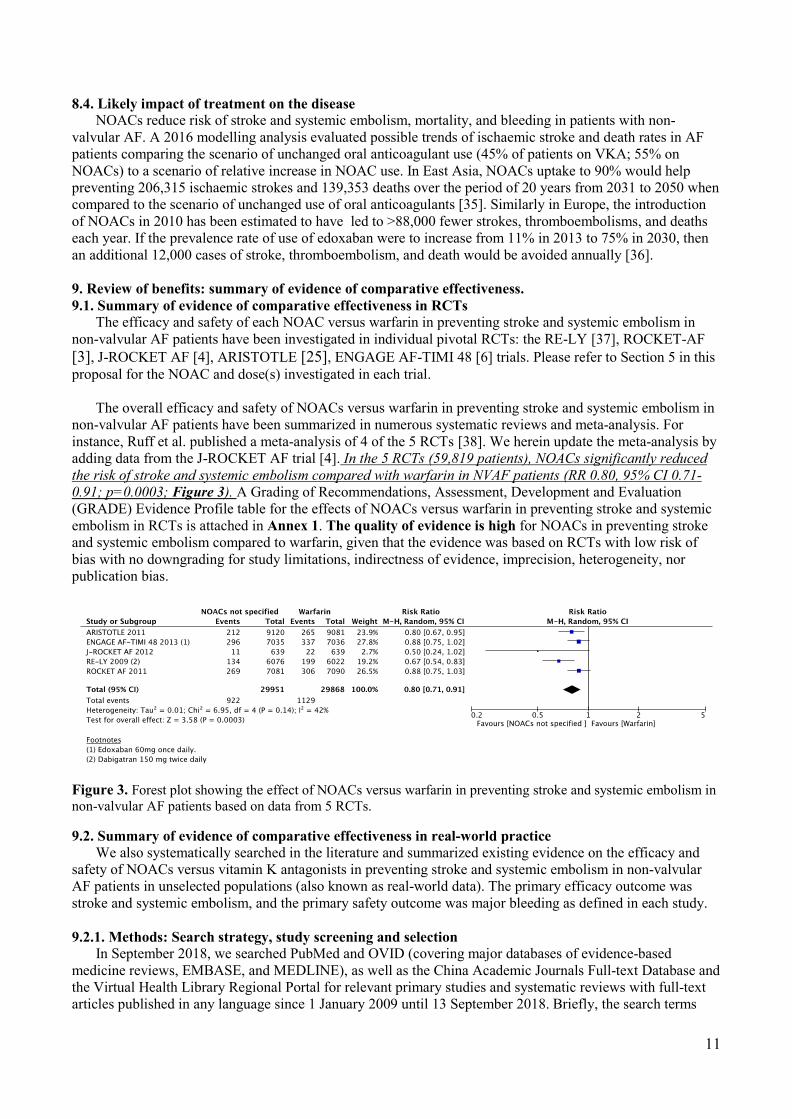
We also compared the safety of each NOAC versus VKAs (predominantly warfarin) separately in real-world practice (Figures 11-14). In each comparison, the risk of major bleeding associated with the NOAC was lower than in warfarin. The GRADE Evidence Profile tables for the associations between each NOAC versus warfarin and the risks of major bleeding in RCTs and in studies reporting RWD are attached in Annex 3-6. The quality of evidence is very low for dabigatran, rivaroxaban and apixaban, respectively, given that the evidence was based on observational studies with heterogenous findings (I2=79%, 91%, 77%), but there was no downgrading for indirectness of evidence nor imprecision among these studies. The quality of evidence is
17
moderate for edoxaban given that the evidence was based on observational studies with consistent findings without downgrading for indirectness of evidence nor imprecision among these studies.
Figure 11. Forest plot showing the risks of major bleeding in patients with non-valvular AF treated with dabigatran versus warfarin based on data from studies reporting real-world data.
Figure 12. Forest plot showing the risks of major bleeding in patients with non-valvular AF treated with rivaroxaban versus warfarin based on data from studies reporting real-world data.
Figure 13. Forest plot showing the risks of major bleeding in patients with non-valvular AF treated with apixaban versus warfarin based on data from a pivotal RCT and studies reporting real-world data.

18
Figure 14. Forest plot showing the risks of major bleeding in patients with non-valvular AF treated with edoxaban versus warfarin based on data from studies reporting real-world data. Results are similar with previous systematic-reviews and meta-analyses [38, 85-87]. 10.3. Safety of NOACs in elderly
A major public concern is the anticoagulation of elderly AF patients. Data from Prevention of thromboembolic events – European Registry in Atrial Fibrillation (PREFER-AF) registry shows anticoagulation is better than no anticoagulation for elderly > 75 years patients with net clinical benefit increasing among all aging subgroups [88]. A 2016 review by authors from McMaster University, including data from RCTs subgroups of patients over 75 years old, showed safety and efficacy of NOACs, except increased risk of bleeding with dabigatran at the higher (150 mg versus 110 mg) dose [89]. A whole country analysis of elderly AF patients from Taiwan demonstrated that NOACs as the best alternative for this population [90], and a US Medicare claims analysis from patients >75 years demonstrated apixaban had lower rates of stroke and bleeding than warfarin [91].
19
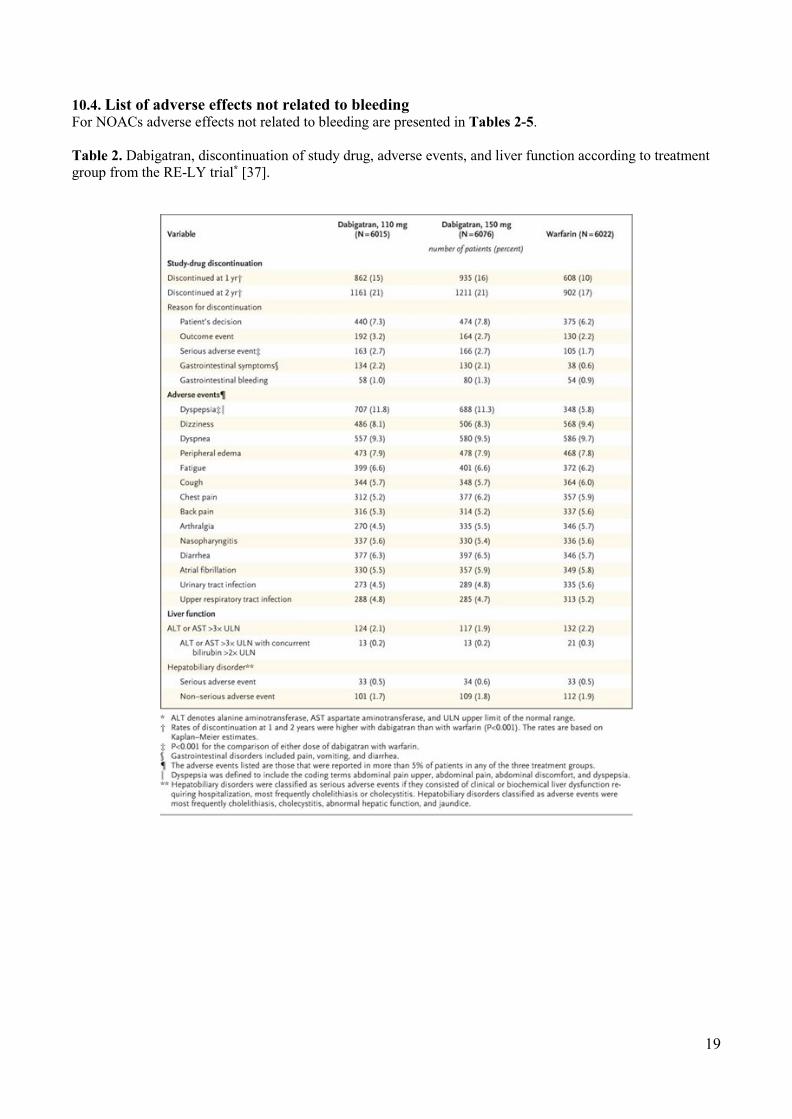
10.4. List of adverse effects not related to bleeding For NOACs adverse effects not related to bleeding are presented in Tables 2-5. Table 2. Dabigatran, discontinuation of study drug, adverse events, and liver function according to treatment group from the RE-LY trial* [37].

20
Table 3. Rivaroxaban adverse events from the ROCKET-AF trial* [3].
21
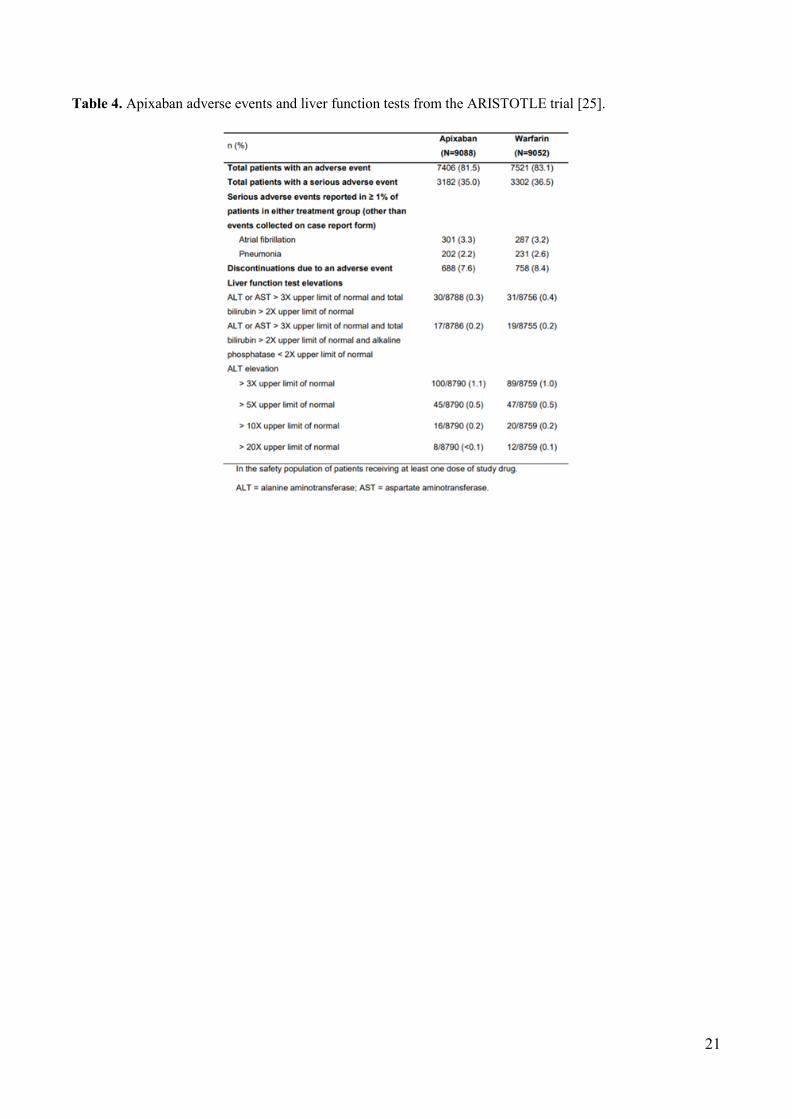
Table 4. Apixaban adverse events and liver function tests from the ARISTOTLE trial [25].
22
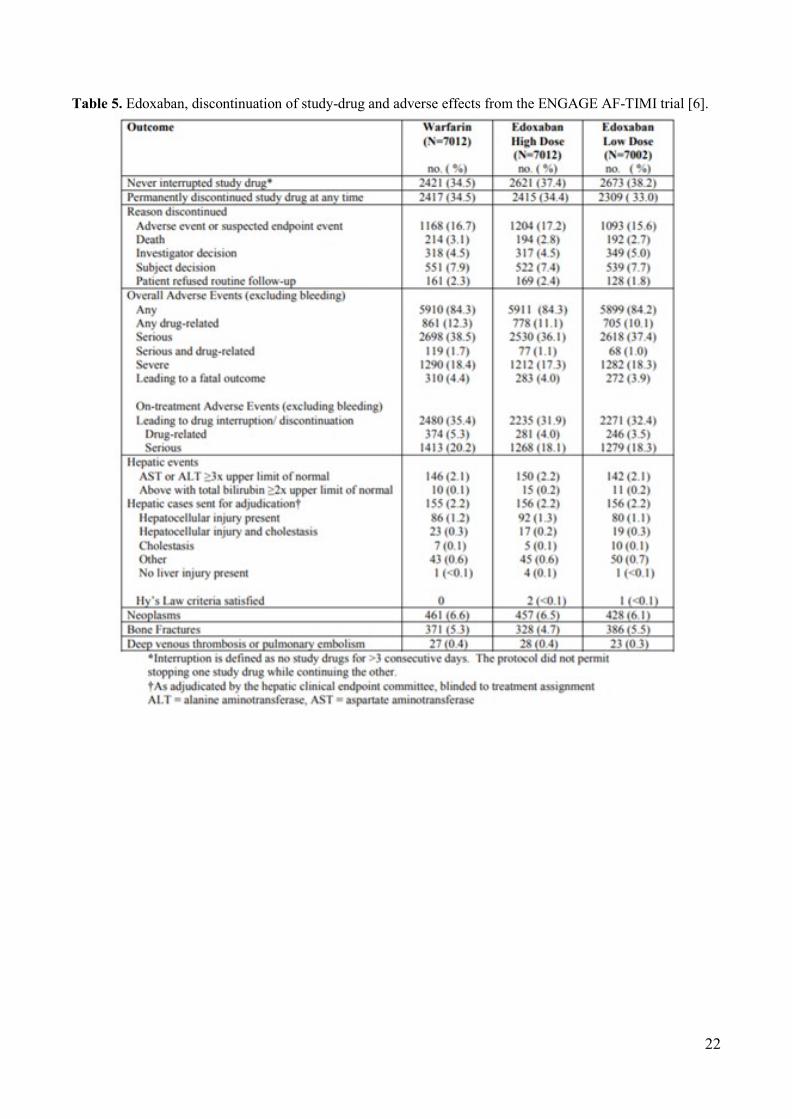
Table 5. Edoxaban, discontinuation of study-drug and adverse effects from the ENGAGE AF-TIMI trial [6].

23
11. Summary of available data on comparative cost and cost-effectiveness of the medicine. Table 6. Cost of NOACs per month in USD.
Country Costs per month in USD (if without insurance) Dabigatran Etexilate Rivaroxaban Apixaban Edoxaban
UK 150 mg twice daily: $64.91
20 mg once daily: $68.73
2,5 mg twice daily: $72.54
60 mg once daily: $67.55
USA 150mg twice daily: $300 (average retail price); $30-79 (if buying from international online pharmacies)
20mg once daily: $527 (average retail price); $47-195 (if buying from international online pharmacies)
5mg twice daily: $445 (average retail price); $64-192 (if buying from international online pharmacies)
60mg once daily: $397 (average retail price)
India 110 mg twice daily: $60.73 150 mg twice daily: $60.73
10 mg once daily: $57.19
5 mg twice daily: $61.08
Chile 150 mg twice daily: $67.51
20 mg once daily: $66.49
5 mg twice daily: $71.35
N/A
Argentina 150 mg twice daily: $121.22
20 mg once daily: $97.57
5 mg twice daily: $88.32
N/A
Brazil 150 mg twice daily: $76.78
20 mg once daily: $77.63
5 mg twice daily: $76.68
60 mg once daily: $66.96
China 110mg twice daily: $175 150mg twice daily: $222
20mg once daily: $742 5mg twice daily: $370 N/A
In other parts of this proposal, we reported the efficacy and safety of NOACs for stroke prevention among
patients with non-valvular AF. A key aspect for long term oral treatments is adherence, and food-drug and drug-drug interactions, necessary INR checking make VKAs a much less preferable class of drugs. Moreover, patients with non-valvular AF prefer NOACS over VKAs (see section 8.1). As a new group of drugs, their cost was expected to be higher than current treatment; however, different studies were developed to assess if the direct cost of replacing VKAs for NOACs would be offset by health costs related to stroke, bleeding, and their consequences.
A comprehensive 2016 systematic review (SR) of cost effectiveness analyses by Liberato and Marchetti [92] concluded that NOACS are cost effective in several countries, independent of their health system, direct costs of NOACs and VKAs, and costs of diseases. These authors defined a drug as cost effective when the incremental cost effectiveness ratio was below the willingness to pay value. For a critical appraise they used the International Society for Pharmacoeconomics and Outcome Research (ISPOR) checklist, and the mean ISPOR score was 33 (high quality). Most studies used a conventional Markov decision analysis model, and the rate of events was gathered from the RCTs of NOACs. We updated the systematic review (Annex 7), including 64 cost effectiveness analyses from 28 high- and middle-income countries from around the world. Most of them used same criteria, but newer cost effectiveness analyses from USA include costs from healthcare resource use and real world data from health systems to determine rate of stroke and bleeding rather than data solely from randomized trials. All studies to date demonstrate that NOACs are a cost effective strategy [93-156].
24
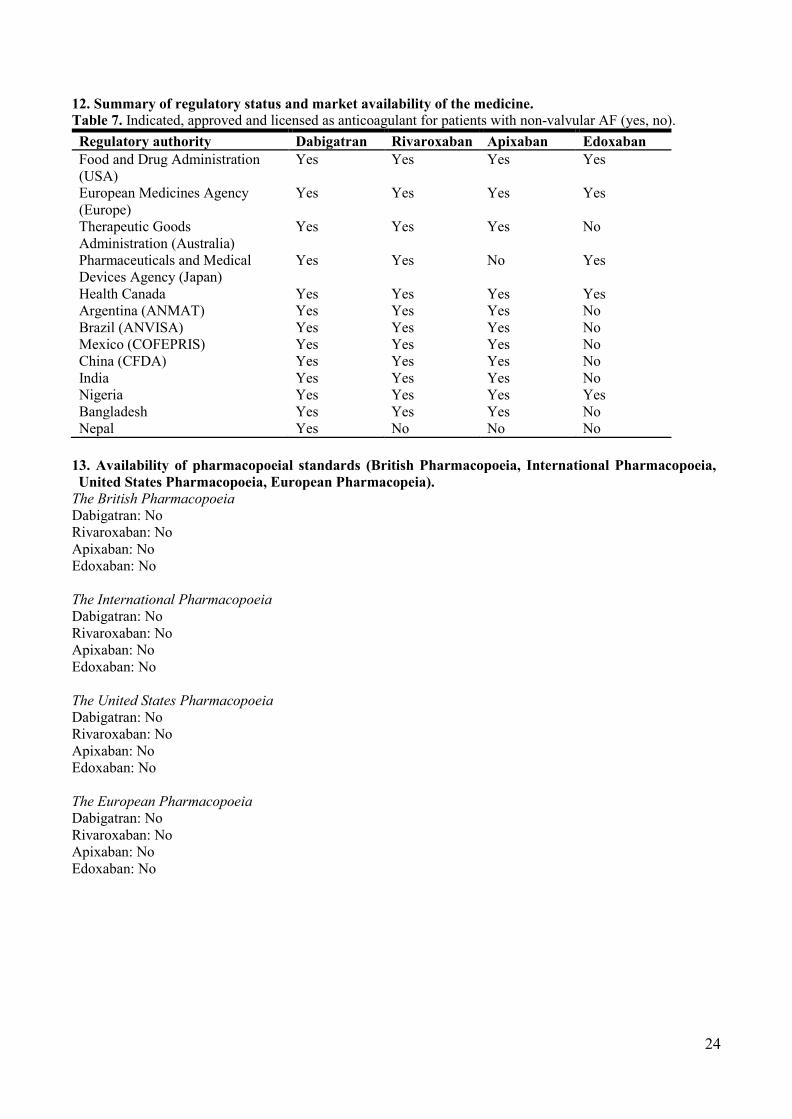
12. Summary of regulatory status and market availability of the medicine. Table 7. Indicated, approved and licensed as anticoagulant for patients with non-valvular AF (yes, no). Regulatory authority Dabigatran Rivaroxaban Apixaban Edoxaban Food and Drug Administration (USA)
Yes Yes Yes Yes
European Medicines Agency (Europe)
Yes Yes Yes Yes
Therapeutic Goods Administration (Australia)
Yes Yes Yes No
Pharmaceuticals and Medical Devices Agency (Japan)
Yes Yes No Yes
Health Canada Yes Yes Yes Yes Argentina (ANMAT) Yes Yes Yes No Brazil (ANVISA) Yes Yes Yes No Mexico (COFEPRIS) Yes Yes Yes No China (CFDA) Yes Yes Yes No India Yes Yes Yes No Nigeria Yes Yes Yes Yes Bangladesh Yes Yes Yes No Nepal Yes No No No
13. Availability of pharmacopoeial standards (British Pharmacopoeia, International Pharmacopoeia, United States Pharmacopoeia, European Pharmacopeia).
The British Pharmacopoeia Dabigatran: No Rivaroxaban: No Apixaban: No Edoxaban: No The International Pharmacopoeia Dabigatran: No Rivaroxaban: No Apixaban: No Edoxaban: No The United States Pharmacopoeia Dabigatran: No Rivaroxaban: No Apixaban: No Edoxaban: No The European Pharmacopoeia Dabigatran: No Rivaroxaban: No Apixaban: No Edoxaban: No

25
14. Reference list and in-text citations. 1. European Medicines Agency. Pradaxa [30 November 2018]. Available from: https://www.ema.europa.eu/en/medicines/human/EPAR/pradaxa. 2. US Food and Drug Administration. Pradaxa [30 November 2018]. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2012/022512Orig1s011_replace.pdf. 3. Patel MR, Mahaffey KW, Garg J, Pan G, Singer DE, Hacke W, et al. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N Engl J Med. 2011;365(10):883-91. 4. Hori M, Matsumoto M, Tanahashi N, Momomura S-i, Uchiyama S, Goto S, et al. Rivaroxaban vs. Warfarin in Japanese Patients With Atrial Fibrillation. Circulation J. 2012;76(9):2104-11. 5. Hohnloser SH, Hijazi Z, Thomas L, Alexander JH, Amerena J, Hanna M, et al. Efficacy of apixaban when compared with warfarin in relation to renal function in patients with atrial fibrillation: insights from the ARISTOTLE trial. Eur Heart J. 2012;33(22):2821-30. 6. Giugliano RP, Ruff CT, Braunwald E, Murphy SA, Wiviott SD, Halperin JL, et al. Edoxaban versus warfarin in patients with atrial fibrillation. N Engl J Med. 2013;369(22):2093-104. 7. Steffel J, Verhamme P, Potpara TS, Albaladejo P, Antz M, Desteghe L, et al. The 2018 European Heart Rhythm Association Practical Guide on the use of non-vitamin K antagonist oral anticoagulants in patients with atrial fibrillation. Eur Heart J. 2018;39(16):1330-93. 8. Kirchhof P, Benussi S, Kotecha D, Ahlsson A, Atar D, Casadei B, et al. 2016 ESC Guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Eur Heart J. 2016;37(38):2893-962. 9. NICE. Atrial fibrillation: management 2014. Available from: https://www.nice.org.uk/guidance/cg180. 10. Gage BF, Waterman AD, Shannon W, Boechler M, Rich MW, Radford MJ. Validation of clinical classification schemes for predicting stroke: results from the National Registry of Atrial Fibrillation. JAMA. 2001;285(22):2864-70. 11. Lip GY, Nieuwlaat R, Pisters R, Lane DA, Crijns HJ. Refining clinical risk stratification for predicting stroke and thromboembolism in atrial fibrillation using a novel risk factor-based approach: the euro heart survey on atrial fibrillation. Chest. 2010;137(2):263-72. 12. Olesen JB, Lip GY, Hansen ML, Hansen PR, Tolstrup JS, Lindhardsen J, et al. Validation of risk stratification schemes for predicting stroke and thromboembolism in patients with atrial fibrillation: nationwide cohort study. BMJ. 2011;342:d124. 13. Chao TF, Liu CJ, Wang KL, Lin YJ, Chang SL, Lo LW, et al. Using the CHA2DS2-VASc score for refining stroke risk stratification in 'low-risk' Asian patients with atrial fibrillation. J Am Coll Cardiol. 2014;64(16):1658-65. 14. Van Staa TP, Setakis E, Di Tanna GL, Lane DA, Lip GY. A comparison of risk stratification schemes for stroke in 79,884 atrial fibrillation patients in general practice. J Thromb Haemost. 2011;9(1):39-48. 15. Friberg L, Rosenqvist M, Lip GY. Evaluation of risk stratification schemes for ischaemic stroke and bleeding in 182 678 patients with atrial fibrillation: the Swedish Atrial Fibrillation cohort study. Eur Heart J. 2012;33(12):1500-10. 16. Pisters R, Lane DA, Nieuwlaat R, de Vos CB, Crijns HJ, Lip GY. A novel user-friendly score (HAS-BLED) to assess 1-year risk of major bleeding in patients with atrial fibrillation: the Euro Heart Survey. Chest. 2010;138(5):1093-100. 17. Institute for Health Metrics and Evaluation (IHME). GBD Compare Data Visualization Seattle, WA: University of Washington; [20 October 2018]. Available from: http://vizhub.healthdata.org/gbd-compare. 18. Krijthe BP, Kunst A, Benjamin EJ, Lip GY, Franco OH, Hofman A, et al. Projections on the number of individuals with atrial fibrillation in the European Union, from 2000 to 2060. Eur Heart J. 2013;34(35):2746-51.
26
19. Lip GYH, Brechin CM, Lane DA. The global burden of atrial fibrillation and stroke: a systematic review of the epidemiology of atrial fibrillation in regions outside North America and Europe. Chest. 2012;142(6):1489-98. 20. Miyasaka Y, Barnes ME, Gersh BJ, Cha SS, Bailey KR, Abhayaratna WP, et al. Secular trends in incidence of atrial fibrillation in Olmsted County, Minnesota, 1980 to 2000, and implications on the projections for future prevalence. Circulation. 2006;114(2):119-25. 21. Hart RG, Pearce LA, Aguilar MI. Meta-analysis: antithrombotic therapy to prevent stroke in patients who have nonvalvular atrial fibrillation. Ann Intern Med. 2007;146(12):857-67. 22. Pokorney SD, Simon DN, Thomas L, Fonarow GC, Kowey PR, Chang P, et al. Patients' time in therapeutic range on warfarin among US patients with atrial fibrillation: Results from ORBIT-AF registry. Am Heart J. 2015;170(1):141-8. 23. Oldgren J, Healey JS, Ezekowitz M, Commerford P, Avezum A, Pais P, et al. Variations in cause and management of atrial fibrillation in a prospective registry of 15,400 emergency department patients in 46 countries: the RE-LY Atrial Fibrillation Registry. Circulation. 2014;129(15):1568-76. 24. Connolly SJ, Pogue J, Eikelboom J, Flaker G, Commerford P, Franzosi MG, et al. Benefit of oral anticoagulant over antiplatelet therapy in atrial fibrillation depends on the quality of international normalized ratio control achieved by centers and countries as measured by time in therapeutic range. Circulation. 2008;118(20):2029-37. 25. Granger CB, Alexander JH, McMurray JJ, Lopes RD, Hylek EM, Hanna M, et al. Apixaban versus warfarin in patients with atrial fibrillation. N Engl J Med. 2011;365(11):981-92. 26. Wilke T, Bauer S, Mueller S, Kohlmann T, Bauersachs R. Patient Preferences for Oral Anticoagulation Therapy in Atrial Fibrillation: A Systematic Literature Review. Patient. 2017;10(1):17-37. 27. Oqab Z, McIntyre WF, Quinn KL, Lamb T, Quadros K, Yazdan-Ashoori P, et al. Resident Physicians Choices of Anticoagulation for Stroke Prevention in Patients With Nonvalvular Atrial Fibrillation. Can J Cardiol. 2016;32(6):824-8. 28. Bottger B, Thate-Waschke IM, Bauersachs R, Kohlmann T, Wilke T. Preferences for anticoagulation therapy in atrial fibrillation: the patients' view. J Thromb Thrombolysis. 2015;40(4):406-15. 29. Stambler BS, Ngunga LM. Atrial fibrillation in Sub-Saharan Africa: epidemiology, unmet needs, and treatment options. Int J Gen Med. 2015;8:231-42. 30. Camm AJ, Accetta G, Ambrosio G, Atar D, Bassand JP, Berge E, et al. Evolving antithrombotic treatment patterns for patients with newly diagnosed atrial fibrillation. Heart. 2017;103(4):307-14. 31. Marzec LN, Gosch KL, Chan PS, Ting HH, Shah ND, Maddox TM. Abstract 14902: The Introduction of Novel Oral Anticoagulants Has Improved Overall Oral Anticoagulation Rates in Atrial Fibrillation: Insights From the NCDR PINNACLE Registry. Circulation. 2015;132(Supp.3). 32. RHDAustralia (ARF/RHD writing group) National Heart Foundation of Australia and the Cardiac Society of Australia and New Zealand. Australian guideline for prevention, diagnosis and management of acute rheumatic fever and rheumatic heart disease (2nd edition). 2012. 33. Remenyi B, Wilson N, Steer A, Ferreira B, Kado J, Kumar K, et al. World Heart Federation criteria for echocardiographic diagnosis of rheumatic heart disease--an evidence-based guideline. Nat Rev Cardiol. 2012;9(5):297-309. 34. Gayle L. INVestIgation of rheumatiC AF Treatment Using Vitamin K Antagonists, Rivaroxaban or Aspirin Studies, Non-Inferiority (INVICTUS-VKA) 2018. Available from: https://clinicaltrials.gov/ct2/show/NCT02832544. 35. Bai Y, Guo SD, Shantsila A, Lip GYH. Modelling projections for the risks related with atrial fibrillation in East Asia: a focus on ischaemic stroke and death. Europace. 2018;20(10):1584-90.

27
36. Blann AD, Boriani G, Lip GY. Modelling projections for the uptake of edoxaban in an European population to 2050: effects on stroke, thromboembolism, and health economics perspectives. Europace. 2016;18(10):1507-13. 37. Connolly SJ, Ezekowitz MD, Yusuf S, Eikelboom J, Oldgren J, Parekh A, et al. Dabigatran versus Warfarin in Patients with Atrial Fibrillation. N Engl J Med. 2009;361(12):1139-51. 38. Ruff CT, Giugliano RP, Braunwald E, Hoffman EB, Deenadayalu N, Ezekowitz MD, et al. Comparison of the efficacy and safety of new oral anticoagulants with warfarin in patients with atrial fibrillation: a meta-analysis of randomised trials. Lancet. 2014;383(9921):955-62. 39. Yu AYX, Malo S, Svenson LW, Wilton SB, Hill MD. Temporal Trends in the Use and Comparative Effectiveness of Direct Oral Anticoagulant Agents Versus Warfarin for Nonvalvular Atrial Fibrillation: A Canadian Population-Based Study. J Am Heart Assoc. 2017;6(11). 40. Blann AD, Banerjee A, Lane DA, Torp-Pedersen C, Lip GYH. Net clinical benefit of edoxaban versus no treatment in a 'real world' atrial fibrillation population: A modelling analysis based on a nationwide cohort study. Int J Cardiol. 2015;201:693-8. 41. Gorst-Rasmussen A, Lip GY, Bjerregaard Larsen T. Rivaroxaban versus warfarin and dabigatran in atrial fibrillation: comparative effectiveness and safety in Danish routine care. Pharmacoepidemiol Drug Saf. 2016;25(11):1236-44. 42. Lamberts M, Staerk L, Olesen JB, Fosbol EL, Hansen ML, Harboe L, et al. Major Bleeding Complications and Persistence With Oral Anticoagulation in Non-Valvular Atrial Fibrillation: Contemporary Findings in Real-Life Danish Patients. J Am Heart Assoc. 2017;6(2). 43. Larsen TB, Skjoth F, Nielsen PB, Kjaeldgaard JN, Lip GY. Comparative effectiveness and safety of non-vitamin K antagonist oral anticoagulants and warfarin in patients with atrial fibrillation: propensity weighted nationwide cohort study. BMJ. 2016;353:i3189. 44. Staerk L, Fosbol EL, Lip GYH, Lamberts M, Bonde AN, Torp-Pedersen C, et al. Ischaemic and haemorrhagic stroke associated with non-vitamin K antagonist oral anticoagulants and warfarin use in patients with atrial fibrillation: a nationwide cohort study. Eur Heart J. 2017;38(12):907-15. 45. Maura G, Blotiere PO, Billionnet KBC, Ricordeau P, Alla F, Zureik M. Comparison of the Short- Term risk of bleeding and arterial thromboembolic events in nonvalvular atrial fibrillation patients newly treated with dabigatran or rivaroxaban versus Vitamin K antagonists A French nationwide propensity-matched cohort study. Circulation. 2015;132(13):1252-60. 46. Coleman CI, Antz M, Ehlken B, Evers T. REal-LIfe Evidence of stroke prevention in patients with atrial Fibrillation--The RELIEF study. Int J Cardiol. 2016;203:882-4. 47. Li WH, Huang D, Chiang CE, Lau CP, Tse HF, Chan EW, et al. Efficacy and safety of dabigatran, rivaroxaban, and warfarin for stroke prevention in Chinese patients with atrial fibrillation: the Hong Kong Atrial Fibrillation Project. Clin Cardiol. 2017;40(4):222-9. 48. Alnsasra H, Haim M, Senderey AB, Reges O, Leventer-Roberts M, Arnson Y, et al. Net clinical benefit of anticoagulant treatments in elderly patients with nonvalvular atrial fibrillation: Experience from the real world. Heart Rhythm. 2018;S1547-5271(18)30816-6. 49. Mayer F, Kirchmayer U, Coletta P, Agabiti N, Belleudi V, Cappai G, et al. Safety and Effectiveness of Direct Oral Anticoagulants Versus Vitamin K Antagonists: Pilot Implementation of a Near-Real-Time Monitoring Program in Italy. J Am Heart Assoc. 2018;7(6):e008034. 50. Ramagopalan S, Allan V, Saragoni S, Esposti LD, Alessandrini D, Perrone V, et al. Patient characteristics and bleeding events in nonvalvular atrial fibrillation patients treated with apixaban or vitamin K antagonists: real-world evidence from Italian administrative databases. J Comp Eff Res. 2018;7(11):1063-71. 51. Kohsaka S, Katada J, Saito K, Terayama Y. Safety and effectiveness of apixaban in comparison to warfarin in patients with nonvalvular atrial fibrillation: a propensity-matched analysis from Japanese administrative claims data. Curr Med Res Opin. 2018;34(9):1627-34. 52. Kohsaka S, Murata T, Izumi N, Katada J, Wang F, Terayama Y. Bleeding risk of apixaban, dabigatran, and low-dose rivaroxaban compared with warfarin in Japanese patients with non-valvular
28
atrial fibrillation: a propensity matched analysis of administrative claims data. Curr Med Res Opin. 2017;33(11):1955-63. 53. Yoshimura S, Koga M, Sato S, Todo K, Yamagami H, Kumamoto M, et al. Two-Year Outcomes of Anticoagulation for Acute Ischemic Stroke With Nonvalvular Atrial Fibrillation- SAMURAI-NVAF Study. Circulation J. 2018;82(7):1935-42. 54. Yap LB, Eng DT, Sivalingam L, Rusani BI, Umadevan D, Muhammad Z, et al. A Comparison of Dabigatran With Warfarin for Stroke Prevention in Atrial Fibrillation in an Asian Population. Clin Appl Thromb Hemost. 2016;22(8):792-7. 55. Nishtala PS, Gnjidic D, Jamieson HA, Hanger HC, Kaluarachchi C, Hilmer SN. 'Real-world' haemorrhagic rates for warfarin and dabigatran using population-level data in New Zealand. Int J Cardiol. 2016;203:746-52. 56. Halvorsen S, Ghanima W, Fride Tvete I, Hoxmark C, Falck P, Solli O, et al. A nationwide registry study to compare bleeding rates in patients with atrial fibrillation being prescribed oral anticoagulants. Eur Heart J Cardiovasc Pharmacother. 2017;3(1):28-36. 57. Cha MJ, Choi EK, Han KD, Lee SR, Lim WH, Oh S, et al. Effectiveness and Safety of Non-Vitamin K Antagonist Oral Anticoagulants in Asian Patients With Atrial Fibrillation. Stroke. 2017;48(11):3040-8. 58. Lee SR, Choi EK, Han KD, Jung JH, Oh S, Lip GYH. Edoxaban in Asian Patients With Atrial Fibrillation: Effectiveness and Safety. J Am Coll Cardiol. 2018;72(8):838-53. 59. Forslund T, Wettermark B, Andersen M, Hjemdahl P. Stroke and bleeding with non-vitamin K antagonist oral anticoagulant or warfarin treatment in patients with non-valvular atrial fibrillation: a population-based cohort study. Europace. 2018;20(3):420-8. 60. Sjogren V, Bystrom B, Renlund H, Svensson PJ, Oldgren J, Norrving B, et al. Non-vitamin K oral anticoagulants are non-inferior for stroke prevention but cause fewer major bleedings than well-managed warfarin: A retrospective register study. PLoS One. 2017;12(7):e0181000. 61. Chan YH, Kuo CT, Yeh YH, Chang SH, Wu LS, Lee HF, et al. Thromboembolic, Bleeding, and Mortality Risks of Rivaroxaban and Dabigatran in Asians With Nonvalvular Atrial Fibrillation. J Am Coll Cardiol. 2016;68(13):1389-401. 62. Chan YH, Yen KC, See LC, Chang SH, Wu LS, Lee HF, et al. Cardiovascular, Bleeding, and Mortality Risks of Dabigatran in Asians With Nonvalvular Atrial Fibrillation. Stroke. 2016;47(2):441-9. 63. Huang HY, Lin SY, Cheng SH, Wang CC. Effectiveness and Safety of Different Rivaroxaban Dosage Regimens in Patients with Non-Valvular Atrial Fibrillation: A Nationwide, Population-Based Cohort Study. Sci Rep. 2018;8(1):3451. 64. Lee HF, Chan YH, Tu HT, Kuo CT, Yeh YH, Chang SH, et al. The effectiveness and safety of low-dose rivaroxaban in Asians with non-valvular atrial fibrillation. Int J Cardiol. 2018;261:78-83. 65. Vinogradova Y, Coupland C, Hill T, Hippisley-Cox J. Risks and benefits of direct oral anticoagulants versus warfarin in a real world setting: cohort study in primary care. BMJ. 2018;362:k2505. 66. Abraham NS, Noseworthy PA, Yao X, Sangaralingham LR, Shah ND. Gastrointestinal Safety of Direct Oral Anticoagulants: A Large Population-Based Study. Gastroenterology. 2017;152(5):1014-22.e1. 67. Adeboyeje G, Sylwestrzak G, Barron JJ, White J, Rosenberg A, Abarca J, et al. Major Bleeding Risk During Anticoagulation with Warfarin, Dabigatran, Apixaban, or Rivaroxaban in Patients with Nonvalvular Atrial Fibrillation. J Manag Care Spec Pharm. 2017;23(9):968-78. 68. Coleman CI, Antz M, Bowrin K, Evers T, Simard EP, Bonnemeier H, et al. Real-world evidence of stroke prevention in patients with nonvalvular atrial fibrillation in the United States: the REVISIT-US study. Curr Med Res Opin. 2016;32(12):2047-53.
29
69. Graham DJ, Reichman ME, Wernecke M, Zhang R, Southworth MR, Levenson M, et al. Cardiovascular, bleeding, and mortality risks in elderly Medicare patients treated with dabigatran or warfarin for nonvalvular atrial fibrillation. Circulation. 2015;131(2):157-64. 70. Laliberte F, Cloutier M, Nelson WW, Coleman CI, Pilon D, Olson WH, et al. Real-world comparative effectiveness and safety of rivaroxaban and warfarin in nonvalvular atrial fibrillation patients. Curr Med Res Opin. 2014;30(7):1317-25. 71. Lauffenburger JC, Farley JF, Gehi AK, Rhoney DH, Brookhart MA, Fang G. Effectiveness and safety of dabigatran and warfarin in real-world US patients with non-valvular atrial fibrillation: a retrospective cohort study. J Am Heart Assoc. 2015;4(4):e001798. 72. Li XS, Deitelzweig S, Keshishian A, Hamilton M, Horblyuk R, Gupta K, et al. Effectiveness and safety of apixaban versus warfarin in non-valvular atrial fibrillation patients in "real-world" clinical practice. A propensity-matched analysis of 76,940 patients. Thromb Haemost. 2017;117(6):1072-82. 73. Lip GY, Pan X, Kamble S, Kawabata H, Mardekian J, Masseria C, et al. Major bleeding risk among non-valvular atrial fibrillation patients initiated on apixaban, dabigatran, rivaroxaban or warfarin: a "real-world" observational study in the United States. Int J Clin Pract. 2016;70(9):752-63. 74. Seeger JD, Bykov K, Bartels DB, Huybrechts K, Zint K, Schneeweiss S. Safety and effectiveness of dabigatran and warfarin in routine care of patients with atrial fibrillation. Thromb Haemost. 2015;114(6):1277-89. 75. Yao X, Abraham NS, Sangaralingham LR, Bellolio MF, McBane RD, Shah ND, et al. Effectiveness and Safety of Dabigatran, Rivaroxaban, and Apixaban Versus Warfarin in Nonvalvular Atrial Fibrillation. J Am Heart Assoc. 2016;5(6):e003725. 76. Monaco L, Biagi C, Conti V, Melis M, Donati M, Venegoni M, et al. Safety profile of the direct oral anticoagulants: an analysis of the WHO database of adverse drug reactions. Br J Clin Pharmacol. 2017;83(7):1532-43. 77. Raschi E, Bianchin M, Ageno W, De Ponti R, De Ponti F. Risk-Benefit Profile of Direct-Acting Oral Anticoagulants in Established Therapeutic Indications: An Overview of Systematic Reviews and Observational Studies. Drug Saf. 2016;39(12):1175-87. 78. Briere JB, Bowrin K, Coleman C, Fauchier L, Levy P, Folkerts K, et al. Real-world clinical evidence on rivaroxaban, dabigatran, and apixaban compared with vitamin K antagonists in patients with non-valvular atrial fibrillation: a systematic literature review. Expert Rev Pharmacoecon Outcomes Res. 2018;19:1-10. 79. Mumoli N, Mastroiacovo D, Tamborini-Permunian E, Vitale J, Giorgi-Pierfranceschi M, Cei M, et al. Dabigatran in nonvalvular atrial fibrillation: from clinical trials to real-life experience. J Cardiovasc Med. 2017;18(7):467-77. 80. Romanelli RJ, Nolting L, Dolginsky M, Kym E, Orrico KB. Dabigatran Versus Warfarin for Atrial Fibrillation in Real-World Clinical Practice: A Systematic Review and Meta-Analysis. Circ Cardiovasc Qual Outcomes. 2016;9(2):126-34. 81. Li G, Holbrook A, Jin Y, Zhang Y, Levine MA, Mbuagbaw L, et al. Comparison of treatment effect estimates of non-vitamin K antagonist oral anticoagulants versus warfarin between observational studies using propensity score methods and randomized controlled trials. Eur J Epidemiol. 2016;31(6):541-61. 82. Carmo J, Moscoso Costa F, Ferreira J, Mendes M. Dabigatran in real-world atrial fibrillation. Meta-analysis of observational comparison studies with vitamin K antagonists. Thromb Haemost. 2016;116(4):754-63. 83. Potpara TS. Dabigatran in 'real-world' clinical practice for stroke prevention in patients with non-valvular atrial fibrillation. Thromb Haemost. 2015;114(6):1093-8. 84. Deitelzweig S, Farmer C, Luo X, Li X, Vo L, Mardekian J, et al. Comparison of major bleeding risk in patients with non-valvular atrial fibrillation receiving direct oral anticoagulants in the real-world setting: a network meta-analysis. Curr Med Res Opin. 2018;34(3):487-98.
30
85. Deitelzweig S, Farmer C, Luo X, Vo L, Li X, Hamilton M, et al. Risk of major bleeding in patients with non-valvular atrial fibrillation treated with oral anticoagulants: a systematic review of real-world observational studies. Curr Med Res Opin. 2017;33(9):1583-94. 86. Ntaios G, Papavasileiou V, Makaritsis K, Vemmos K, Michel P, Lip GYH. Real-World Setting Comparison of Nonvitamin-K Antagonist Oral Anticoagulants Versus Vitamin-K Antagonists for Stroke Prevention in Atrial Fibrillation. A Systematic Review and Meta-Analysis. Stroke. 2017;48(9):2494-503. 87. Cameron C, Coyle D, Richter T, Kelly S, Gauthier K, Steiner S, et al. Systematic review and network meta-analysis comparing antithrombotic agents for the prevention of stroke and major bleeding in patients with atrial fibrillation. BMJ Open. 2014;4(6):e004301. 88. Patti G, Lucerna M, Pecen L, Siller-Matula JM, Cavallari I, Kirchhof P, et al. Thromboembolic Risk, Bleeding Outcomes and Effect of Different Antithrombotic Strategies in Very Elderly Patients With Atrial Fibrillation: A Sub-Analysis From the PREFER in AF (PREvention oF Thromboembolic Events-European Registry in Atrial Fibrillation). J Am Heart Assoc. 2017;6(7):e005657. 89. Kilickap M, Bosch J, Eikelboom JW, Hart RG. Antithrombotic Treatments for Stroke Prevention in Elderly Patients With Nonvalvular Atrial Fibrillation: Drugs and Doses. Can J Cardiol. 2016;32(9):1108-16. 90. Chao TF, Liu CJ, Lin YJ, Chang SL, Lo LW, Hu YF, et al. Oral Anticoagulation in Very Elderly Patients With Atrial Fibrillation: A Nationwide Cohort Study. Circulation. 2018;138(1):37-47. 91. Deitelzweig S, Luo X, Gupta K, Trocio J, Mardekian J, Curtice T, et al. Comparison of effectiveness and safety of treatment with apixaban vs. other oral anticoagulants among elderly nonvalvular atrial fibrillation patients. Curr Med Res Opin. 2017;33(10):1745-54. 92. Liberato NL, Marchetti M. Cost-effectiveness of non-vitamin K antagonist oral anticoagulants for stroke prevention in non-valvular atrial fibrillation: a systematic and qualitative review. Expert Rev Pharmacoecon Outcomes Res. 2016;16(2):221-35. 93. Ademi Z, Pasupathi K, Liew D. Cost-effectiveness of apixaban compared to warfarin in the management of atrial fibrillation in Australia. Eur J Prev Cardiol. 2015;22(3):344-53. 94. Amin A, Keshishian A, Vo L, Zhang Q, Dina O, Patel C, et al. Real-world comparison of all-cause hospitalizations, hospitalizations due to stroke and major bleeding, and costs for non-valvular atrial fibrillation patients prescribed oral anticoagulants in a US health plan. J Med Econ. 2018;21(3):244-53. 95. Andrikopoulos GK, Fragoulakis V, Maniadakis N. Economic evaluation of dabigatran etexilate in the management of atrial fibrillation in Greece. Hellenic J Cardiol. 2013;54(4):289-300. 96. Baron Esquivias G, Escolar Albaladejo G, Zamorano JL, Betegon Nicolas L, Canal Fontcuberta C, de Salas-Cansado M, et al. Cost-effectiveness Analysis Comparing Apixaban and Acenocoumarol in the Prevention of Stroke in Patients With Nonvalvular Atrial Fibrillation in Spain. Rev Esp Cardiol (Engl Ed). 2015;68(8):680-90. 97. Bergh M, Marais CA, Miller-Janson H, Salie F, Stander MP. Economic appraisal of dabigatran as first-line therapy for stroke prevention in atrial fibrillation. S Afr Med J. 2013;103(4):241-5. 98. Bonet Pla A, Gosalbes Soler V, Ridao-Lopez M, Navarro Perez J, Navarro Cubells B, Peiro S. [Dabigatran versus acenocumarol for the prevention of stroke in atrial fibrillation: budget impact analysis in one health department in Spain]. Rev Esp Salud Publica. 2013;87(4):331-42. 99. Canestaro WJ, Patrick AR, Avorn J, Ito K, Matlin OS, Brennan TA, et al. Cost-effectiveness of oral anticoagulants for treatment of atrial fibrillation. Circ Cardiovasc Qual Outcomes. 2013;6(6):724-31.

31
100. Chang AM, Ho JC, Yan BP, Yu CM, Lam YY, Lee VW. Cost-effectiveness of dabigatran compared with warfarin for stroke prevention in patients with atrial fibrillation--a real patient data analysis in a Hong Kong teaching hospital. Clin Cardiol. 2013;36(5):280-5. 101. Chang C-H, Yang Y-HK, Chen J-H, Lin L-J. Cost-effectiveness of dabigatran etexilate for the prevention of stroke and systemic embolism in atrial fibrillation in Taiwan. Thrombosis Research. 2014;133(5):782-9. 102. Chevalier J, Delaitre O, Hammes F, de Pouvourville G. Cost-effectiveness of dabigatran versus vitamin K antagonists for the prevention of stroke in patients with atrial fibrillation: a French payer perspective. Arch Cardiovasc Dis. 2014;107(6-7):381-90. 103. Chi NF, Wang Y, Chien LN, Chien SC, Ko Y. Health Care Costs and Utilization of Dabigatran Compared With Warfarin for Secondary Stroke Prevention in Patients With Nonvalvular Atrial Fibrillation: A Retrospective Population Study. Med Care. 2018;56(5):410-5. 104. Clemens A, Peng S, Brand S, Brueckmann M, Kansal A, Lim J, et al. Efficacy and cost-effectiveness of dabigatran etexilate versus warfarin in atrial fibrillation in different age subgroups. Am J Cardiol. 2014;114(6):849-55. 105. Costa J, Fiorentino F, Caldeira D, Ines M, Lopes Pereira C, Pinheiro L, et al. Cost-effectiveness of non-vitamin K antagonist oral anticoagulants for atrial fibrillation in Portugal. Rev Port Cardiol. 2015;34(12):723-37. 106. Coyle D, Coyle K, Cameron C, Lee K, Kelly S, Steiner S, et al. Cost-effectiveness of new oral anticoagulants compared with warfarin in preventing stroke and other cardiovascular events in patients with atrial fibrillation. Value Health. 2013;16(4):498-506. 107. Davidson T, Husberg M, Janzon M, Oldgren J, Levin LA. Cost-effectiveness of dabigatran compared with warfarin for patients with atrial fibrillation in Sweden. Eur Heart J. 2013;34(3):177-83. 108. Dorian P, Kongnakorn T, Phatak H, Rublee DA, Kuznik A, Lanitis T, et al. Cost-effectiveness of apixaban vs. current standard of care for stroke prevention in patients with atrial fibrillation. Eur Heart J. 2014;35(28):1897-906. 109. Ferrante JB. Costo-efectividad del Dabigatran en fibrilación auricular en Argentina. Hematologia. 2013;17(2):122-6. 110. Freeman JV, Zhu RP, Owens DK, Garber AM, Hutton DW, Go AS, et al. Cost-effectiveness of dabigatran compared with warfarin for stroke prevention in atrial fibrillation. Ann Intern Med. 2011;154(1):1-11. 111. Galindo-Suárez RM, Davila-Veites A, Olguin-Sánchez JF, Haddad A, del Angel- Martínez J, Muciño-Ortega E. Cost-Effectiveness Analysis of Apixaban in the Treatment of Atrial Fibrillation in Mexico. Value Health. 2013;16(7):A524. 112. García-Peña AA. Cost-effectiveness assessment of new oral anticoagulation drugs in patients with non-valvular atrial fibrillation. Rev Col Cardiol. 2016;4(2):87-95. 113. Giorgi MA, Caroli C, Giglio ND, Micone P, Aiello E, Vulcano C, et al. Estimation of the cost-effectiveness of apixaban versus vitamin K antagonists in the management of atrial fibrillation in Argentina. Health Econ Rev. 2015;5(1):52. 114. Gonzalez-Juanatey JR, Alvarez-Sabin J, Lobos JM, Martinez-Rubio A, Reverter JC, Oyaguez I, et al. Cost-effectiveness of dabigatran for stroke prevention in non-valvular atrial fibrillation in Spain. Rev Esp Cardiol (Engl Ed). 2012;65(10):901-10. 115. NICE technology appraisal guidance. TA249. Dabigatran etexilate for the prevention of stroke and systemic embolism in atrial fibrillation. [cited 2018 2 October]. Available from: https://www.nice.org.uk/guidance/ta249. 116. NICE technology appraisal guidance. TA256. Rivaroxaban for the prevention of stroke and systemic embolism in people with atrial fibrillation [cited 2018 1 October]. Available from: https://www.nice.org.uk/guidance/ta256.

32
117. NICE technology appraisal guidance. TA275. Apixaban for preventing stroke and systemic embolism in people with nonvalvular atrial fibrillation [cited 2018 1 October]. Available from: https://www.nice.org.uk/guidance/ta275. 118. Harrington AR, Armstrong EP, Nolan Jr PE, Malone DC. Cost-effectiveness of apixaban, dabigatran, rivaroxaban, and warfarin for stroke prevention in atrial fibrillation. Stroke. 2013;44(6):1676-81. 119. Hori M, Ikeda S, Okumura K, Matsuda S, Koretsune Y, Montouchet C, et al. Clinical and economic impact of rivaroxaban on the burden of atrial fibrillation: The case study of Japan. J Med Econ. 2016;19(9):889-99. 120. Jain R, Fu AC, Lim J, Wang C, Elder J, Sander SD, et al. Health Care Resource Utilization and Costs Among Newly Diagnosed and Oral Anticoagulant-Naive Nonvalvular Atrial Fibrillation Patients Treated with Dabigatran or Warfarin in the United States. J Manag Care Spec Pharm. 2018;24(1):73-82. 121. Janzic A, Kos M. Cost effectiveness of novel oral anticoagulants for stroke prevention in atrial fibrillation depending on the quality of warfarin anticoagulation control. Pharmacoeconomics. 2015;33(4):395-408. 122. Kamae I, Hashimoto Y, Koretsune Y, Tanahashi N, Murata T, Phatak H, et al. Cost-effectiveness Analysis of Apixaban against Warfarin for Stroke Prevention in Patients with Nonvalvular Atrial Fibrillation in Japan. Clin Ther. 2015;37(12):2837-51. 123. Kamel H, Easton JD, Johnston SC, Kim AS. Cost-effectiveness of apixaban vs warfarin for secondary stroke prevention in atrial fibrillation. Neurology. 2012;79(14):1428-34. 124. Kansal AR, Sorensen SV, Gani R, Robinson P, Pan F, Plumb JM, et al. Cost-effectiveness of dabigatran etexilate for the prevention of stroke and systemic embolism in UK patients with atrial fibrillation. Heart. 2012;98(7):573-8. 125. Kleintjens J, Li X, Simoens S, Thijs V, Goethals M, Rietzschel ER, et al. Cost-effectiveness of rivaroxaban versus warfarin for stroke prevention in atrial fibrillation in the Belgian healthcare setting. Pharmacoeconomics. 2013;31(10):909-18. 126. Kourlaba G, Maniadakis N, Andrikopoulos G, Vardas P. Economic evaluation of rivaroxaban in stroke prevention for patients with atrial fibrillation in Greece. Cost Eff Resour Alloc. 2014;12(1):5. 127. Krejczy M, Harenberg J, Marx S, Obermann K, Frolich L, Wehling M. Comparison of cost-effectiveness of anticoagulation with dabigatran, rivaroxaban and apixaban in patients with non-valvular atrial fibrillation across countries. J Thromb Thrombolysis. 2014;37(4):507-23. 128. Lanas F, Castro C, Vallejos C, Bustos L, de La Puente C, Velasquez M, et al. Latin American Clinical Epidemiology Network Series - Paper 2: Apixaban was cost-effective vs. acenocoumarol in patients with nonvalvular atrial fibrillation with moderate to severe risk of embolism in Chile. J Clin Epidemiol. 2017;86:75-83. 129. Langkilde LK, Bergholdt Asmussen M, Overgaard M. Cost-effectiveness of dabigatran etexilate for stroke prevention in non-valvular atrial fibrillation. Applying RE-LY to clinical practice in Denmark. J Med Econ. 2012;15(4):695-703. 130. Lanitis T, Cotte FE, Gaudin AF, Kachaner I, Kongnakorn T, Durand-Zaleski I. Stroke prevention in patients with atrial fibrillation in France: comparative cost-effectiveness of new oral anticoagulants (apixaban, dabigatran, and rivaroxaban), warfarin, and aspirin. J Med Econ. 2014;17(8):587-98. 131. Lee S, Anglade MW, Meng J, Hagstrom K, Kluger J, Coleman CI. Cost-effectiveness of apixaban compared with aspirin for stroke prevention in atrial fibrillation among patients unsuitable for warfarin. Circ Cardiovasc Qual Outcomes. 2012;5(4):472-9. 132. Lin J, Trocio J, Gupta K, Mardekian J, Lingohr-Smith M, Menges B, et al. Major bleeding risk and healthcare economic outcomes of non-valvular atrial fibrillation patients newly-initiated with oral anticoagulant therapy in the real-world setting. J Med Econ. 2017;20(9):952-61.
33
133. Lip GY, Kongnakorn T, Phatak H, Kuznik A, Lanitis T, Liu LZ, et al. Cost-effectiveness of apixaban versus other new oral anticoagulants for stroke prevention in atrial fibrillation. Clin Ther. 2014;36(2):192-210. 134. Mensch A, Stock S, Stollenwerk B, Muller D. Cost effectiveness of rivaroxaban for stroke prevention in German patients with atrial fibrillation. Pharmacoeconomics. 2015;33(3):271-83. 135. Monreal-Bosch M, Soulard S, Crespo C, Brand S, Kansal A. Comparison of the cost-utility of direct oral anticoagulants for the prevention of stroke in patients with atrial fibrillation in Spain. Rev Neurol. 2017;64(6):247-56. 136. Morais J, Aguiar C, McLeod E, Chatzitheofilou I, Fonseca Santos I, Pereira S. Cost-effectiveness of rivaroxaban for stroke prevention in atrial fibrillation in the Portuguese setting. Rev Port Cardiol. 2014;33(9):535-44. 137. Nshimyumukiza L, Duplantie J, Gagnon M, Douville X, Fournier D, Lindsay C, et al. Dabigatran versus warfarin under standard or pharmacogenetic-guided management for the prevention of stroke and systemic embolism in patients with atrial fibrillation: a cost/utility analysis using an analytic decision model. Thromb J. 2013;11(1):14. 138. Pepe Ribeiro de Souza C, Bolzachini Santoni N, Gomes de Melo T, Jansen de Oliveira Figueiredo M, da Costa Darrieux FC, Soares Piegas L, et al. Cost-Effectiveness and Cost-Utility Analyses of Dabigatran Compared with Warfarin in Patients with Nonvalvular Atrial Fibrillation and Risk Factors for Stroke and Systemic Embolism within Brazilian Private and Public Health Care Systems Perspectives. Value Health Reg Issues. 2015;8:36-42. 139. Pink J, Lane S, Pirmohamed M, Hughes DA. Dabigatran etexilate versus warfarin in management of non-valvular atrial fibrillation in UK context: quantitative benefit-harm and economic analyses. BMJ. 2011;343:d6333. 140. Pink J, Pirmohamed M, Lane S, Hughes DA. Cost-effectiveness of pharmacogenetics-guided warfarin therapy vs. alternative anticoagulation in atrial fibrillation. Clin Pharmacol Ther. 2014;95(2):199-207. 141. Pletscher M, Plessow R, Eichler K, Wieser S. Cost-effectiveness of dabigatran for stroke prevention in atrial fibrillation in Switzerland. Swiss Med Wkly. 2013;143:w13732. 142. Poulsen PB, Johnsen SP, Hansen ML, Brandes A, Husted S, Harboe L, et al. Setting priorities in the health care sector - the case of oral anticoagulants in nonvalvular atrial fibrillation in Denmark. Clinicoecon Outcomes Res. 2017;9:617-27. 143. Rognoni C, Marchetti M, Quaglini S, Liberato NL. Apixaban, dabigatran, and rivaroxaban versus warfarin for stroke prevention in non-valvular atrial fibrillation: a cost-effectiveness analysis. Clin Drug Investig. 2014;34(1):9-17. 144. Rognoni C, Marchetti M, Quaglini S, Liberato NL. Edoxaban versus warfarin for stroke prevention in non-valvular atrial fibrillation: a cost-effectiveness analysis. J Thromb Thrombolysis. 2015;39(2):149-54. 145. Shah A, Shewale A, Hayes CJ, Martin BC. Cost-Effectiveness of Oral Anticoagulants for Ischemic Stroke Prophylaxis Among Nonvalvular Atrial Fibrillation Patients. Stroke. 2016;47(6):1555-61. 146. Shah SV, Gage BF. Cost-effectiveness of dabigatran for stroke prophylaxis in atrial fibrillation. Circulation. 2011;123(22):2562-70. 147. Stevanovic J, Pompen M, Le HH, Rozenbaum MH, Tieleman RG, Postma MJ. Economic evaluation of apixaban for the prevention of stroke in non-valvular atrial fibrillation in the Netherlands. PLoS One. 2014;9(8):e103974. 148. Triana JJ, Castaneda-Cardona C, Parada L, Rosselli D. Cost-efectiveness of dabigatran in non valvular atrial fibrillation in Colombia. Value in Health. 2015;18 (3):A140-A1. 149. van Hulst M, Stevanovic J, Jacobs MS, Tieleman RG, Kappelhoff B, Postma MJ. The cost-effectiveness and monetary benefits of dabigatran in the prevention of arterial thromboembolism for patients with non-valvular atrial fibrillation in the Netherlands. J Med Econ. 2018;21(1):38-46.

34
150. Verhoef TI, Redekop WK, Hasrat F, de Boer A, Maitland-van der Zee AH. Cost effectiveness of new oral anticoagulants for stroke prevention in patients with atrial fibrillation in two different European healthcare settings. Am J Cardiovasc Drugs. 2014;14(6):451-62. 151. Vilain KA, Yang MC, Hui Tan EC, Wang K, Li H, Hsu WH, et al. Cost-Effectiveness of Edoxaban vs. Warfarin in Patients with Atrial Fibrillation Based on Results of the ENGAGE AF - TIMI 48 Trial: Taiwanese Perspective. Value Health Reg Issues. 2017;12:74-83. 152. Wang Y, Xie F, Kong MC, Lee LH, Ng HJ, Ko Y. Cost-effectiveness of dabigatran and rivaroxaban compared with warfarin for stroke prevention in patients with atrial fibrillation. Cardiovasc Drugs Ther. 2014;28(6):575-85. 153. Wisloff T, Hagen G, Klemp M. Economic evaluation of warfarin, dabigatran, rivaroxaban, and apixaban for stroke prevention in atrial fibrillation. Pharmacoeconomics. 2014;32(6):601-12. 154. Wouters H, Thijs V, Annemans L. Cost-effectiveness of dabigatran etexilate in the prevention of stroke and systemic embolism in patients with atrial fibrillation in Belgium. J Med Econ. 2013;16(3):407-14. 155. Wu Y, Feng J, Peng Y, Rong P, Li M, Zhou B. Cost-effectiveness of novel oral anticoagulants versus warfarin for stroke prevention in patients with non-valvular atrial fibrillation. Chin Hosp Pharm J. 2016;36(12):1003-7. 156. Zheng Y, Sorensen SV, Gonschior AK, Noack H, Heinrich-Nols J, Sunderland T, et al. Comparison of the cost-effectiveness of new oral anticoagulants for the prevention of stroke and systemic embolism in atrial fibrillation in a UK setting. Clin Ther. 2014;36(12):2015-28.