application of 4% chlorhexidine to the umbilical cord
TRANSCRIPT

REVIEW Open Access
Application of 4% chlorhexidine to theumbilical cord stump of newborn infants inlower income countries: a systematicreview and meta-analysisAklilu Abrham Roba1*† , Maleda Tefera1†, Teshager Worku1†, Tamirat Tesfaye Dasa1†, Abiy Seifu Estifanos2† andNega Assefa1†
AbstractThere are conflicting results from large randomized controlled trials in different populations regarding theeffectiveness of topical application of 4% chlorhexidine to the umbilical stump of newborn infants at reducingneonatal mortality. Meta-analysis and systematic review of trials performed in South Asia and Europe support 4%chlorhexidine application to reduce neonatal mortality, whereas trials performed in Sub-Saharan Africa do not. Theaim of this review is to determine the effectiveness of 4% chlorhexidine application to the umbilical stump ofnewborn infants born in lower income countries in order to reduce neonatal mortality when compared with usualcord care.Our search strategy included randomized trials published between January1st 2000 and September 4th, 2018, thatcompared 4% chlorhexidine with usual cord care (“dry cord care”). The outcome variable of interest was neonatalmortality. Pooled relative risks (RR) with 95% confidence intervals (CIs) using a random-effects model werecalculated. Nine trials were included, from six countries: Zambia, Tanzania, Bangladesh, Nepal, India and Pakistan,with a total of 257,153 participants. Five studies (N = 119,833) reported neonatal mortality. There was a 21%reduction in neonatal mortality among with 4% chlorhexidine application: pooled RR (95% CI) 0.79 (0.69–0.90), P =0.0005. The incidence of omphalitis was decreased by 35% with 4% chlorhexidine (6 studies, N = 108,263): pooledRR (95% CI) 0.65 (0.56–0.75), P = 0.00001. Chlorhexidine application delayed the umbilical cord separation time (4studies, N = 28,917): mean difference (95% CI) 2.71 (2.63–2.78) days.In conclusion, this systematic review found that topical application of 4% chlorhexidine to the umbilical cord stumpof newborn infants in lower income countries significantly reduces the incidence of neonatal mortality.Chlorhexidine also reduces the incidence of omphalitis, but prolongs umbilical cord separation time.
Trial registration: Systematic Review Registration: CRD42018109280.
Keywords: Chlorhexidine, Umbilical cord, Cord separation time, Omphalitis, Neonatal mortality, Newborn infants,Low-income countries, Lower-middle income countries
© The Author(s). 2019 Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, andreproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link tothe Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver(http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
* Correspondence: [email protected]†Aklilu Abrham Roba, Maleda Tefera, Teshager Worku, Tamirat Tesfaye Dasa,Abiy Seifu and Nega Assefa contributed equally to this work.1College of Health and Medical Sciences, Haramaya University, Harar, EthiopiaFull list of author information is available at the end of the article
Maternal Health, Neonatology,and Perinatology
Roba et al. Maternal Health, Neonatology, and Perinatology (2019) 5:16 https://doi.org/10.1186/s40748-019-0111-y
RETRACTED ARTIC
LE

IntroductionThe first 4 weeks after birth are critical for the survival ofnewborn infants. Worldwide, 2.6 million neonatal deathswere estimated to occur in 2016, which translates to ap-proximately 7000 deaths every day [1]. Omphalitis (infec-tion of the umbilical cord) is an important cause of illnessand death in newborn infants in developing countries [2].Harmful traditional practices during cord cutting or tying,and the application of different substances to the fresh um-bilical wound, may contribute to the entrance of infectiousmicro-organisms [3].Chlorhexidine digluconate is a broad-spectrum antiseptic
agent that is effective against a wide range of perinatal in-fectious microbials, as it strongly binds with their cell walland disrupts their osmotic equilibrium [4]. It has beenwidely used for hand washing, oral care and medical pur-poses for decades, including for cleansing the umbilicalcord and vaginal canal [5]. Because of its safety, efficacy,and low cost, chlorhexidine has been extensively evaluatedas a means of preventing vertically acquired (intrapartum)neonatal infection.A Cochrane review found that 4% chlorhexidine is ef-
fective to reduce neonatal mortality in settings with ahigh neonatal mortality rate (NMR) > 30/1000 live-births[6]. However, data is lacking on the effectiveness ofchlorhexidine in a setting where the NMR is < 30/1000live-births as well as for in-hospital deliveries [7, 8]. Glo-bally, there are two important questions: 1) do the bene-ficial effects of chlorhexidine application warrant achange in the current recommendation of “dry cordcare” (without chlorhexidine) in newborn infants [9]?,and 2) is the application of chlorhexidine as effective inthe hospital setting as it is in the community setting?.Three trials from South Asia (Nepal [10], Bangladesh [11]and Pakistan [12]) found a reduction in neonatal mortality,while studies from Sub-Saharan Africa (Zambia [13] andTanzania [14]) did not. No hospital-based studies have re-ported neonatal mortality [6].Equipment used for umbilical cord tying or cutting
may be a source of cord infection in newborn infants.One qualitative study in a rural community inEthiopia found that umbilical cords were being cutwith a razor, old blade, or even with a knife that wasalso used for cutting foodstuffs [3]. Cords were tiedwith a sewing thread, the thread from kerosenestoves, sisal thread, or thread or strips of cloth froma local blanket, traditional shawl or bed sheets. But-ter, petroleum jelly and hair lotion were being appliedto the cord [3]. Cord infections are associated withan increased risk of sepsis and neonatal mortality[15]. Therefore, in settings where exposure of the um-bilical cord to potentially invasive pathogens is high,interventions that promote hygienic practices and top-ical cord antisepsis are recommended [16].
The aim of this systematic review and meta-analysisis to determine the effect on neonatal mortality of 4%chlorhexidine application to the umbilical stump ofnewborn infants, compared with “dry cord care”, inlower income countries. Omphalitis and cord separ-ation time are secondary outcomes of interest.
MethodsThis Systematic review and meta-analysis was registeredin PROSPERO with registration number CRD42018109280.
Information sources and searching strategiesThe following databases were searched from January1st
2000 and September 4th, 2018: MEDLINE, PubMed,EMBASE, CINAHL, Web of Science direct (web of sci-ence core collection), Scopus, and Cochrane CentralRegister of Controlled Trials. In addition, we performed amanual search to retrieve unpublished studies and grey lit-erature via Google Scholar and other sources. We usedMeSH terms and search terms to construct a search stringfor each database that included terms ‘chlorhexidine’,‘neonate’, and ‘umbilical cord’. For example, the followingsearch strategy was used on PubMed: (“chlorhexidine glu-conate”[Supplementary Concept] OR “chlorhexidine”[-Mesh]) AND “infant, newborn”[Mesh]) AND “umbilicalcord”[Mesh] AND ((clinical trial [ptyp] OR controlledclinical trial [ptyp] OR randomized controlled trial [ptyp])AND “humans”[MeSH Terms]). To identify ongoing tri-als, we searched WHO trial registries in all three conti-nents. Latin America and the Caribbean region wereassessed through VHL regional portal using filtering (tw:((tw:(tw:((tw:(chlorhexidine)) AND (tw:(umbilical cord))AND (tw:(newborn))) AND (instance:"regional”)))) AND(instance:"regional”) AND (collection:(“06-national”) ANDdb:(“IBECS” OR “LILACS”) AND mj:(“umbilical cord” OR“chlorhexidine” OR “bacterial infections” OR “umbil-icus”))). After the searches, duplicate studies were re-moved, and remaining studies were screened for inclusionusing the title and abstract. Included studies were thenreviewed in full by two authors. Any differences in evalu-ation of studies were resolved by consensus of all authors.The PRISMA flow diagram [17] is shown in Fig. 1 and asummary of included studies in Table 1.
Eligibility criteriaWe included RCTs that had been conducted in com-munity or health facility settings, with individual orcluster randomization, and parallel or factorial de-signs. Studies that had been conducted in developingcountries, and compared the effect of single or mul-tiple topical applications of 4% chlorhexidine with“dry cord care” (applied nothing or soap and water
Roba et al. Maternal Health, Neonatology, and Perinatology (2019) 5:16 Page 2 of 9
RETRACTED ARTIC
LE

only), irrespective of duration of follow-up in the neo-natal period, were eligible. Studies that included alllive births irrespective of gestational age or birthweight, had been published and were accessible beforeSeptember 9th, 2018 and written in English were eli-gible. Studies that used other chlorhexidine strengths/concentrations, quasi-experimental studies, reviews,commentaries, editorials, and case series/reports wereexcluded.
Description of the outcomesThe outcome variables of interest were neonatal mor-tality, defined as death within the first 28 days of life;
omphalitis, defined as redness or swelling, with orwithout pus, in the skin surrounding the umbilicalcord stump; and the time of umbilical cord separ-ation, defined as the duration in days from birth tofull separation of the umbilical cord from the stump.
Risk of BiasTwo authors (AAR and TW) independently screenedand evaluated studies using the Cochrane Risk of BiasTool for Randomized Controlled Trials [22] (Table 2).Publication bias was explored using visual inspectionof the funnel plot. Besides, Egger’s regression test [23]was carried out to check the symmetry of the funnel
Fig. 1 Flow diagram showing literature search
Roba et al. Maternal Health, Neonatology, and Perinatology (2019) 5:16 Page 3 of 9
RETRACTED ARTIC
LE

Table 1 Summary table of trials
Study Design and Sample size Interventions Comparator Primary outcome/Otheroutcomes
Jamil,2018/Pakistan [20],Trial registration: Not found
Hospital-based RCT.I = 50C = 50T = 100
Chlorhexidine (liquid orgel form) were appliedonce daily for 7 days ortill umbilical cord falls off.
Dry cord care Presence of omphalitis wasrecorded as 38% in Drycare and 10% in thechlorhexidine group (p = 0.001)
Lyngdoh, D [18], 2018/ India,Trial registration: CTRI/2017/07/009146.
Hospital-based trialI = 35 (Chlorhexidine)C = 35 (Dry cord care)T = 105
He used chlorhexidine4% as well as humanbreast milk in interventionarm
Dry cord care 4% chlorhexidine is veryeffective in reducingpathogenic bacteriacolonization of the cord
Semrau, 2016/Zambia [13],Trial registration: NCT01241318
Cluster RCT.Ia=18,450Cb=19,308Tc=37,758
Topical application of4% chlorhexidine onceper day until 3 daysafter cord drop.
Clean dry cordcare
NMRd: 15·2/1000 live birth in IGe
NMR: 13·6/1000 live births CGf
Sazawal, 2016/Tanzania [14],Trial registration: NCT01528852
Community-based RCT.I = 18,015C = 18,896T = 36,911
4% chlorhexidine solutionto the cord every dayuntil 3 days after thecord had dropped off.
Dry cord care NMR: 10.5/1000 live birth in IGNMR: 11.7/1000 live births CG
Khairuzzaman, 2015/ Bangladesh [21],Trial registration: Not found
Hospital-based RCT. I =170C = 170T = 340
4% chlorhexidine solution Dry cord care The mean cord separationtime in newborns of IGwas significantly longerthan CG (7.44 ± 3.75 Vs4.83 ± 2.05 p < 0.001).
Mullany, 2013/Bangladesh [19],Trial registration: NCT00434408
Cluster-RCTI = 17,757C = 9624T = 27,381
Three arms IG:1)4% chlorhexidine,2) cleansing with soap andwater
Dry cord care. Cord separation time1) Single group: 6.9 ± 2.87 days,2) Multiple groups: 7.49 ± 3.08days3) Dry care: 4.78 ± 1.82 days
Sofi S, 2012/Pakistan [12];Trial registration: NCT00682006
2X2 factorial, cluster-RCT.I = 4867C = 4874T = 9741
Four arms1)4% chlorhexidine solutiononce daily up to 14 daysalong with soap andeducational messagespromoting hand washing.2) The chlorhexidine solutiononly and3) Hand washing only.
Dry cord care A reduction in NMR (RR = 0·62,95% CI 0·45–0·85); risk ofomphalitis (RR = 0·58, 95%CI 0·41–0·82; No effect ofhand washing for both outcomes
Arifeen, 2012/Bangladesh [11],Trial registration: NCT00434408
Community-based RCT.I = 19,608C = 9924T = 29,532
Three arms:1) Multiple 4% chlorhexidinecleansing2) Single 4% chlorhexidinecleansing
Dry cord care NMR = 22·5 per 1000 LB insingle chlorhexidine group,26·6 per 1000 LB amongmultiple chlorhexidine groupsand 28·3 per 1000 LB in drycord care group.
Mullany L, C,2006/Nepal&Bangladesh [10],Trial registration: NCT00109616
Cluster-RCT.I = 4924C = 5082T = 10,006
Three arms:1)4% chlorhexidine,2) cleansing with soap andwater
Dry cord care. Neonatal mortality was 24%lower in the chlorhexidinegroup (RR = 0·76,[95% CI 0·55–1·04]) than inthe DCC groupSevere omphalitis inchlorhexidine clusters wasreduced by 75% (incidencerate ratio 0·25, 95% CI 0·12–0·53.
aI InterventionbC ControlcT TotaldNMR Neonatal Mortality RateeIG Intervention GroupfCG Control Group
Roba et al. Maternal Health, Neonatology, and Perinatology (2019) 5:16 Page 4 of 9
RETRACTED ARTIC
LE

plot. Approximately symmetric funnel plots would in-dicate a “low risk” whereas asymmetric funnel plotswould indicate a “high risk” of publication bias. Dis-agreements were resolved by consensus with otherauthors.
Statistical analysisData synthesis and statistical analysis were carried out bythree authors (AAR, NA, and MT). Meta-analysis was con-ducted using Review Manager Version 5.3 software [24] forRelative Risk (RR) for neonatal mortality and omphalitis;mean difference (95% confidence interval [CI]) was used forcord separation time. Heterogeneity between studies wasexamined using the I2 statistic described by Higgins et al.[25] and p-value: P < 0.10 or I2 > 75% were considered asevidence of significant heterogeneity, which was exploredfurther by sensitivity analysis. Sub-group analysis was con-ducted between Sub-Saharan and South Asian countries aswell as studies of hospital and community settings.
ResultsStudy descriptionsA total of 12 RCTs were included in this systematic reviewand meta-analysis. The outcome of neonatal mortality wasreported in five RCTs, conducted in Zambia, Tanzania,Bangladesh, Nepal and Pakistan with a total of 119,973participants. Omphalitis was reported in six RCTs, con-ducted in Zambia, Tanzania, Bangladesh, Nepal andPakistan with a total of 108,263 participants.Four RCTs, from Bangladesh, India and Nepal with a
total of 28,917 participants, reported cord separationtime. Fig. 1.
Neonatal mortalityThe application of 4% chlorhexidine reduced the pooled in-cidence of neonatal mortality by 21% compared with drycord care (Fig. 2): pooled RR 0.79; 95% CI: 0.69–0.90; P =0.0004; random-effects model. There was minimal hetero-geneity between trials for this outcome (I2 = 44%, χ2 = 7.11,P = 0.13).
Fig. 2 Effect of 4% chlorhexidine application on neonatal mortality
Table 2 Risk of bias of included studies
Author, year Random sequencegeneration(selection bias)
Intention to treat(selection bias)
Blinding(performance bias)
Incompleteoutcome data(attrition bias)
Selective reporting(reporting bias)
An overall decision onthe quality of the study
Jamil,2018/Pakistan [20] Moderate unknown unclear High unknown Moderate risk of bias
Lyngdoh, D, 2018/India [18]
Moderate Moderate unknown Low Low Moderate risk of bias
Semrau, 2016/Zambia [13] Low Low Unclear Low Low Low risk of bias
Sazawal, 2016/Tanzania [14] Low Low Not blind Low Low Low risk of bias
Khairuzzaman, Md, 2015/Bangladesh [21]
Unclear Low Unclear Low Low Moderate risk of bias
Mullany, 2013/Bangladesh [19]
Low Low High Low Low risk of bias
Soofi S, 2012/Pakistan [12] Low Unclear Low Low Low Low risk of bias
Arifeen, 2012/Bangladesh [11]
Low Low Low Low Low Low risk of bias
Mullany L, C,2006/Nepal &Bangladesh [10]
Low Low Low Low Low Low risk of bias
Roba et al. Maternal Health, Neonatology, and Perinatology (2019) 5:16 Page 5 of 9
RETRACTED ARTIC
LE
Of the five studies, four [10–14] were conducted in acommunity setting, while one was conducted in hospitalneonatal intensive care unit [20]. Two studies were con-ducted in Sub-Saharan Africa of Zambia and Tanzania[13, 14], and three in South Asia, Nepal, Bangladesh andPakistan [10–12]. All except the Zambian study [13, 26]were conducted in countries with a high NMR > 30/1000live-births. All of the studies enrolled predominantly homedelivered newborn infants. The Tanzanian study recruitedparticipants from both the hospital and community (homebased) setting, with more than half of the participantsborn in hospitals [14]. In the Zambian study [13], 11·4% ofbirths in the chlorhexidine group and 16·1% of the drycord care group were born in hospitals [13]. Sub-groupanalysis based on geography found that 4% chlorhexidinereduced neonatal mortality by 43% in South Asia (RR[95% CI] 0.57 [0.42–0.76]) and 30% in Sub-Saharan Africa(RR [95% CI] 0.70 [0.67–0.74]) (Fig. 2).
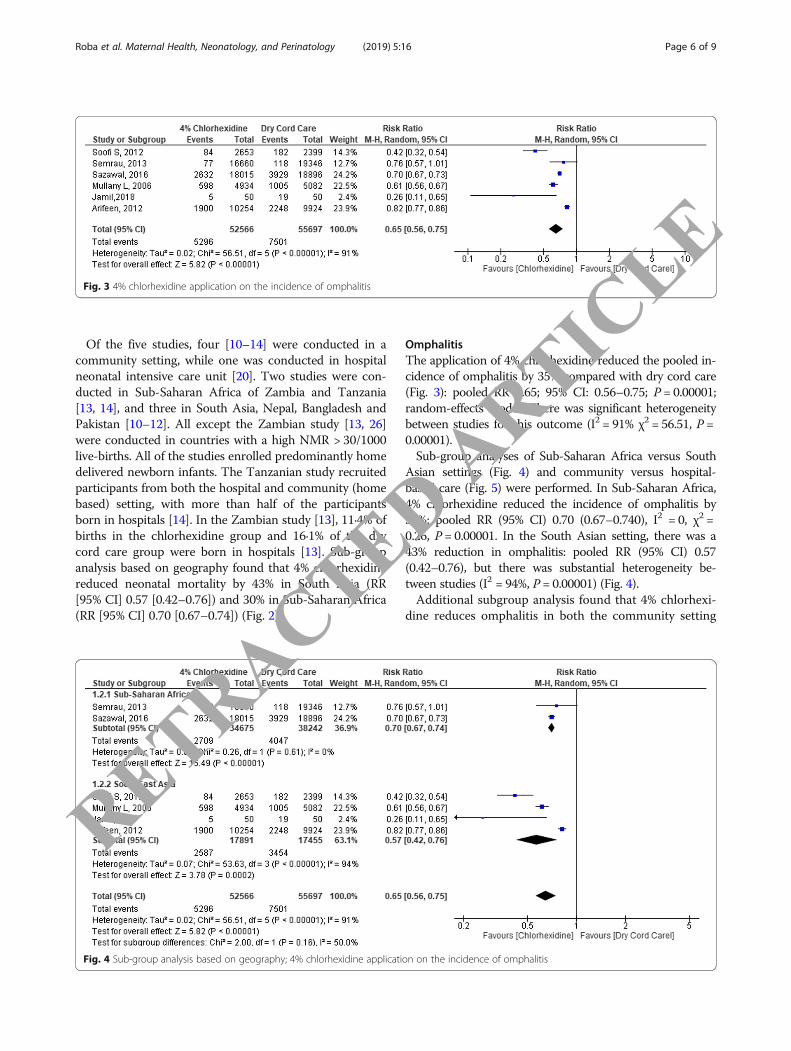
OmphalitisThe application of 4% chlorhexidine reduced the pooled in-cidence of omphalitis by 35% compared with dry cord care(Fig. 3): pooled RR 0.65; 95% CI: 0.56–0.75; P = 0.00001;random-effects model. There was significant heterogeneitybetween studies for this outcome (I2 = 91% χ2 = 56.51, P =0.00001).Sub-group analyses of Sub-Saharan Africa versus South
Asian settings (Fig. 4) and community versus hospital-based care (Fig. 5) were performed. In Sub-Saharan Africa,4% chlorhexidine reduced the incidence of omphalitis by30%: pooled RR (95% CI) 0.70 (0.67–0.740), I2 = 0, χ2 =0.26, P = 0.00001. In the South Asian setting, there was a43% reduction in omphalitis: pooled RR (95% CI) 0.57(0.42–0.76), but there was substantial heterogeneity be-tween studies (I2 = 94%, P = 0.00001) (Fig. 4).Additional subgroup analysis found that 4% chlorhexi-
dine reduces omphalitis in both the community setting
Fig. 4 Sub-group analysis based on geography; 4% chlorhexidine application on the incidence of omphalitis
Fig. 3 4% chlorhexidine application on the incidence of omphalitis
Roba et al. Maternal Health, Neonatology, and Perinatology (2019) 5:16 Page 6 of 9
RETRACTED ARTIC
LE
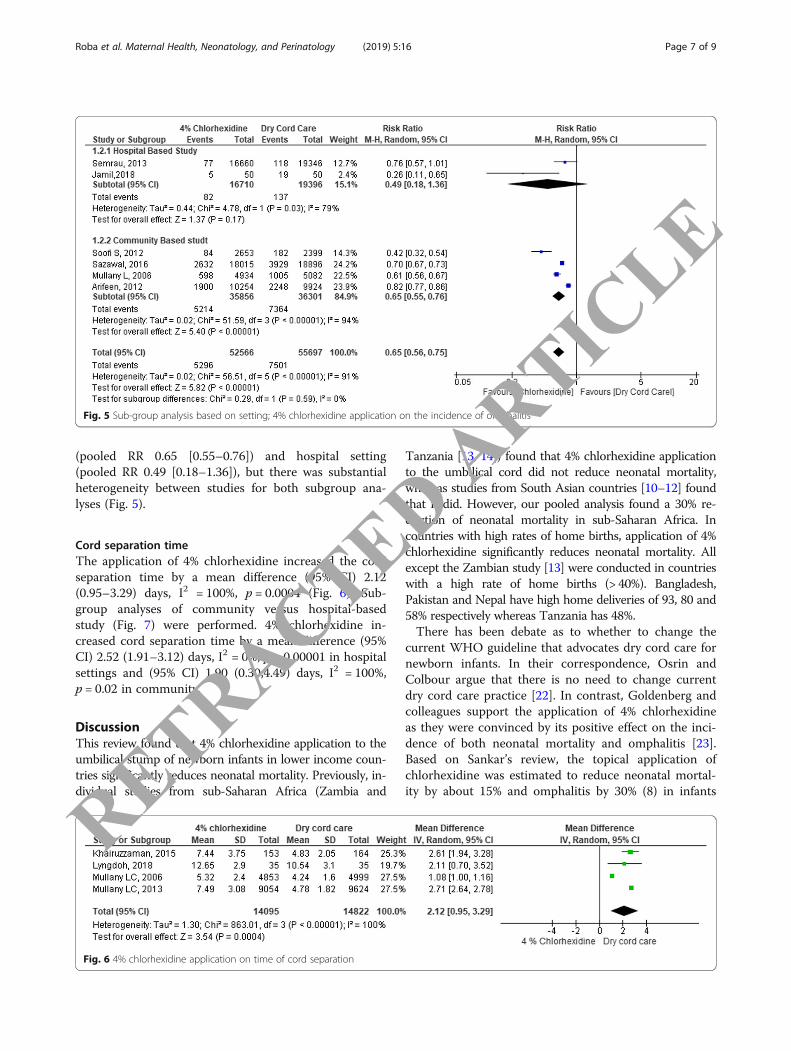
(pooled RR 0.65 [0.55–0.76]) and hospital setting(pooled RR 0.49 [0.18–1.36]), but there was substantialheterogeneity between studies for both subgroup ana-lyses (Fig. 5).
Cord separation timeThe application of 4% chlorhexidine increased the cordseparation time by a mean difference (95% CI) 2.12(0.95–3.29) days, I2 = 100%, p = 0.0004 (Fig. 6). Sub-group analyses of community versus hospital-basedstudy (Fig. 7) were performed. 4% chlorhexidine in-creased cord separation time by a mean difference (95%CI) 2.52 (1.91–3.12) days, I2 = 0%, p = 0.00001 in hospitalsettings and (95% CI) 1.90 (0.30,4.49) days, I2 = 100%,p = 0.02 in community.
DiscussionThis review found that 4% chlorhexidine application to theumbilical stump of newborn infants in lower income coun-tries significantly reduces neonatal mortality. Previously, in-dividual studies from sub-Saharan Africa (Zambia and
Tanzania [13, 14]) found that 4% chlorhexidine applicationto the umbilical cord did not reduce neonatal mortality,whereas studies from South Asian countries [10–12] foundthat it did. However, our pooled analysis found a 30% re-duction of neonatal mortality in sub-Saharan Africa. Incountries with high rates of home births, application of 4%chlorhexidine significantly reduces neonatal mortality. Allexcept the Zambian study [13] were conducted in countrieswith a high rate of home births (> 40%). Bangladesh,Pakistan and Nepal have high home deliveries of 93, 80 and58% respectively whereas Tanzania has 48%.There has been debate as to whether to change the
current WHO guideline that advocates dry cord care fornewborn infants. In their correspondence, Osrin andColbour argue that there is no need to change currentdry cord care practice [22]. In contrast, Goldenberg andcolleagues support the application of 4% chlorhexidineas they were convinced by its positive effect on the inci-dence of both neonatal mortality and omphalitis [23].Based on Sankar’s review, the topical application ofchlorhexidine was estimated to reduce neonatal mortal-ity by about 15% and omphalitis by 30% (8) in infants
Fig. 6 4% chlorhexidine application on time of cord separation
Fig. 5 Sub-group analysis based on setting; 4% chlorhexidine application on the incidence of omphalitis
Roba et al. Maternal Health, Neonatology, and Perinatology (2019) 5:16 Page 7 of 9
RETRACTED ARTIC
LE

born in settings that are comparable to those settings inour study. Sharif found a pooled reduction in neonatalmortality of 20% and in omphalitis by 60% [24].An important consideration before the introduction of
universal 4% chlorhexidine cord care in lower incomecountries is adverse effects of the therapy. Trials inGermany [27] and Pakistan [28] have shown chlorhexidineprevents skin erosion, irritation, omphalitis, erythema, um-bilical granuloma, purulence, bleeding, discharge andweeping of the navel. Another trial in Pakistanshowed there were no adverse effects [12], whereasthere are case-reports of adverse effects in pretermand low birth weight infants [29–33]. Ultimately, theamount of exposure to chlorhexidine that can be con-sidered safe is not known [34].The strength of our current meta-analysis is that the
studies included are RCTs from both community andhospital settings. It included seven large trials from twolarge continents: Asia and Africa. In general, the risk ofbias of the studies was low (Table 2). However, there aresome limitations of our results. Some of the studies in-cluded in the meta-analysis reported neonatal deathsfrom recruitment, whereas others excluded deaths onthe day of life associated with birth asphyxia. Some ofthe studies were not blinded, especially those from com-munity settings.
ConclusionTopical application of 4% chlorhexidine on the umbilicalcord of newborn infants born in lower income countries re-duces neonatal mortality by 21% and omphalitis by 35%.Chlorhexidine use delays cord separation time by about 2.5days in the hospital setting and 2 days in the community.The intervention is effective in both community-based aswell as health facility settings for the prevention of
omphalitis. We recommend guidelines consider including4% chlorhexidine application as routine practice in thesesettings.
AbbreviationsAAR: Aklilu Abrham Roba; CI: Confidence Interval; LB: Live Birth;MeSH: Medical Search Heading; MT: Maleda Tefera; NA: Nega Assefa;NMR: Neonatal Mortality Rate; RCT: Randomized Controlled trial; RR: RiskRatio; SSA: Sub-Saharan Africa; TTD: Tamirat Tesfaye Dasa; TW: TeshagerWorku
AcknowledgementsWe thank all individuals who contributed a lot for this by offering systematicreview and meta-analysis training. In addition, our deepest gratitude goes toBrett Manley, Associate editor of Maternal Health, Neonatology andPerinatology for unreserved effort to edit our document and OgbuduEmanuel for the language edition.
Authors’ contributionsAll authors contributed equally towards conceiving and designing the study,data extraction, analysis and interpretation and final approval of the manuscript.
Authors’ informationAll authors are from School of Nursing and Midwifery, College of Health andMedical Sciences, Haramaya University, Harar, Ethiopia except Abiy Seifu fromAddis Ababa University, School of Public Health, Department of ReproductiveHealth and Health Service Management.
FundingNot applicable.
Availability of data and materialsThe data that support the review findings of this study are available uponsubmitting a reasonable request to the corresponding author.
Ethics approval and consent to participateNot applicable.
Consent for publicationNot applicable.
Competing interestsThe authors declare that they have no competing interests.
Author details1College of Health and Medical Sciences, Haramaya University, Harar,Ethiopia. 2Department of Reproductive Health and Health Service
Fig. 7 4 Sub-group analysis based on Geography; 4% chlorhexidine application on cord separation time
Roba et al. Maternal Health, Neonatology, and Perinatology (2019) 5:16 Page 8 of 9
RETRACTED ARTIC
LE

Management, School Of Public Health, Addis Ababa University, Addis Ababa,Ethiopia.
Received: 10 January 2019 Accepted: 11 September 2019
References1. Neonatal mortality [https://data.unicef.org/topic/child-survival/neonatal-
mortality/]. Accessed 1 Mar 2019.2. Imdad A, Bautista RM, Senen KA, Uy ME, Mantaring JB 3RD, Bhutta ZA.
Umbilical cord antiseptics for preventing sepsis and death amongnewborns. Cochrane Database Syst Rev. 2013;Cd008635.
3. Amare Y. Umbilical cord care in Ethiopia and implications for behavioralchange: a qualitative study. BMC Int Health Hum Rights. 2014;14(1):12.
4. Davies A. The mode of action of chlorhexidine. J Periodontal Res Suppl.1973;12:68–75.
5. McDonnell G, Russell AD. Antiseptics and disinfectants: activity, action, andresistance. Clin Microbiol Rev. 1999;12(1):147–79.
6. Imdad A, Bautista RM, Senen KA, Uy ME, Mantaring JB 3rd, Bhutta ZA.Umbilical cord antiseptics for preventing sepsis and death amongnewborns. Cochrane Database Syst Rev. 2013;5:CD008635.
7. Osrin D, Colbourn T. Chlorhexidine and newborn omphalitis and mortality.Lancet Glob Health. 2017;5(3):E272–3.
8. Hodgins S. Chlorhexidine and newborn omphalitis and mortality. LancetGlob Health. 2017;5(3):E270–1.
9. Sankar MJ, Chandrasekaran A, Ravindranath A, Agarwal R. Umbilical cordcleansing with chlorhexidine in neonates: a systematic review. J Perinatol.2016;36(Suppl 1):S12–20.
10. Mullany LC, Darmstadt GL, Khatry SK, LeClerq SC, Katz J, Tielsch JM. Impactof umbilical cord cleansing with 4.0% chlorhexidine on time to cordseparation among newborns in southern Nepal: a cluster-randomized,community-based trial. Pediatrics. 2006;118(5):1864–71.
11. Arifeen SE, Mullany LC, Shah R, Mannan I, Rahman SM, Talukder MRR,Begum N, A-k A, Darmstadt GL, Santosham M, et al. The effect of cordcleansing with chlorhexidine on neonatal mortality in rural Bangladesh: acommunity-based, cluster-randomised trial. Lancet (British edition). 2012;379(9820):1022–8.
12. Soofi S, Cousens S, Imdad A, Bhutto N, Ali N, Bhutta ZA. Topical applicationof chlorhexidine to neonatal umbilical cords for prevention of omphalitisand neonatal mortality in a rural district of Pakistan: a community-based,cluster-randomised trial. Lancet. 2012;379(9820):1029–36.
13. Semrau KEA, Herlihy J, Grogan C, Musokotwane K, Yeboah-Antwi K, MbeweR, Banda B, Mpamba C, Hamomba F, Pilingana P, et al. Effectiveness of 4%chlorhexidine umbilical cord care on neonatal mortality in SouthernProvince, Zambia (ZamCAT): a cluster-randomised controlled trial. LancetGlob Health. 2016;4(11):e827–36.
14. Sazawal S, Dhingra U, Ali SM, Dutta A, Deb S, Ame SM, Mkasha MH, YadavA, Black RE. Efficacy of chlorhexidine application to umbilical cord onneonatal mortality in Pemba, Tanzania: a community-based randomisedcontrolled trial. Lancet Glob Health. 2016;4(11):e837–44.
15. Mir F, Tikmani SS, Shakoor S, Warraich HJ, Sultana S, Ali SA. Incidence andetiology of omphalitis in Pakistan: a community-based cohort study. J InfectDev Ctries. 2011;5(12):828–33.
16. Mullany LC, Darmstadt GL, Katz J, Khatry SK, Leclerq SC, Adhikari RK, TielschJM. Risk of mortality subsequent to umbilical cord infection amongnewborns of southern Nepal: cord infection and mortality. Pediatr Infect DisJ. 2009;28(1):17–20.
17. Stewart LA, Clarke M, Rovers M, Riley RD, Simmonds M, Stewart G, Tierney JF.Preferred reporting items for systematic review and meta-analyses of individualparticipant data: the PRISMA-IPD statement. JAMA. 2015;313(16):1657–65.
18. Lyngdoh D, Kaur S, Kumar P, Gautam V, Ghai S. Effect of topical applicationof human breast milk versus 4% chlorhexidine versus dry cord care onbacterial colonization and clinical outcomes of umbilical cord in pretermnewborns. J Clin Neonatol. 2018;7(1):25–30.
19. Mullany LC, Shah R, El Arifeen S, Mannan I, Winch PJ, Hill A, Darmstadt GL,Baqui AH. Chlorhexidine cleansing of the umbilical cord and separationtime: a cluster-randomized trial. Pediatrics. 2013;131(4):708–15.
20. Jamil A, Sajid M, Ishaq F, Mahmood R. Comparison of the frequency of omphalitisby applying chlorhexidine versus dry cord care. Pak Paediatr J. 2018;42(1):16–7.
21. Khairuzzaman M, Mannan MA, Matin A, Sarker MMA, Sarker NR, Mowla MG,Shahidullah M. Chlorhexidine cleansing of the umbilical cord and cord separationtime: A hospital based study in Bangladesh. J Sci Found. 2015;13(2):27–30.
22. Cochrane: Cochrane collaboration modified tool for assessing risk of bias forRCT’s, PART I and II. Appendix D. Cochrane risk of Bias tool.
23. Xiuquan Shi CN, Shi S, Wang T, Yang H, Zhou Y, Song X. Effect comparisonbetween Egger’s test and Begg’s test in publication Bias diagnosis in meta-analyses: evidence from a pilot survey. Int J Res Stud Biosci. 2017;5(5):14–20.
24. Shariff JA, Lee KC, Leyton A, Abdalal S. Neonatal mortality and topicalapplication of chlorhexidine on umbilical cord stump: a meta-analysis ofrandomized control trials. Public Health. 2016;139:27–35.
25. Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis.Stat Med. 2002;21(11):1539–58.
26. Zambia - Neonatal mortality rate [http://knoema.com/]. Accessed 1 Apr2019.
27. Kapellen TM, Gebauer CM, Brosteanu O, Labitzke B, Vogtmann C, Kiess W.Higher rate of cord-related adverse events in neonates with dry umbilical cordcare compared to chlorhexidine powder. Neonatology. 2009;96(1):13–8.
28. Saleem S, Rouse DJ, McClure EM, Zaidi A, Reza T, Yahya Y, Memon IA, KhanNH, Memon G, Soomro N, et al. Chlorhexidine vaginal and infant wipes toreduce perinatal mortality and morbidity: a randomized controlled trial.Obstet Gynecol. 2010;115(6):1225–32.
29. Kutsch J, Ottinger D. Neonatal skin and chlorhexidine: A burningexperience. Neonatal Netw. 2013;33(1):19–23.
30. Chapman AK, Aucott SW, Milstone AM. Safety of chlorhexidine gluconateused for skin antisepsis in the preterm infant. J Perinatol: official journal ofthe California Perinatal Association. 2012;32(1):4–9.
31. Vanzi V, Pitaro R. Skin injuries and chlorhexidine gluconate-based antisepsisin early premature infants: A case report and review of the literature. JPerinat Neonatal Nurs. 2018;32(4):341–50.
32. Bringue Espuny X, Soria X, Sole E, Garcia J, Marco JJ, Ortega J, Ortiz M,Pueyo A. Chlorhexidine-methanol burns in two extreme preterm newborns.Pediatr Dermatol. 2010;27(6):676–8.
33. Mannan K, Chow P, Lissauer T, Godambe S. Mistaken identity of skincleansing solution leading to extensive chemical burns in an extremelypreterm infant. Acta Paediatr. 2007;96(10):1536–7.
34. Sinha A, Sazawal S, Pradhan A, Ramji S, Opiyo N. Chlorhexidine skin or cordcare for prevention of mortality and infections in neonates. CochraneDatabase Syst Rev. 2015;(3):1–57. Art.No.: CD007835. https://doi.org/10.1002/14651858.CD007835.pub2.
Publisher’s NoteSpringer Nature remains neutral with regard to jurisdictional claims inpublished maps and institutional affiliations.
Roba et al. Maternal Health, Neonatology, and Perinatology (2019) 5:16 Page 9 of 9
RETRACTED ARTIC
LE