approach to interventional management of pulmonary embolism and the role of the multidisciplinary...
TRANSCRIPT

Approach to Interventional Management of Pulmonary Embolism and the Role of the
Multidisciplinary Team Approach
With credits also to:Richard N. Channick, M.D.Michael R. Jaff, M.D.Christopher Kabrhel, M.D.The MGH PERT Team
Kenneth Rosenfield, MD, MHCDSon behalf of MGH PERT collaborators

Kenneth Rosenfield, MD, MHCDSConflicts of Interest
• Consultant– Abbott Vascular– Capture Vascular– Cardinal Health– Contego– CRUZAR Systems– Endospan– Eximo– InspireMD– MD Insider– Micell– Shockwave– Silk Road– Surmodics– Valcare
• Research or Fellowship Support– Abbott Vascular– Atrium– NIH– InspireMD– Lutonix-Bard
• Board Member– VIVA Physicians (Not For
Profit 501(c) 3 Organization)• www.vivapvd.com
• Equity– CardioMEMs– Contego– Embolitech– Icon– Janacare– MD Insider– Micell– PQ Bypass– Primacea– Shockwave– Vortex

PE (and DVT): A national crisis!
• Severely under-recognized and undertreated
• Significant immediate and long-term sequelae
• High recurrence rate
• Treatments available that reduce mortality, morbidity and sequelae
Kearon C et al. Chest 2008; 133: 454S-545S.

Pulmonary Embolus: Why Worry??Consequences By Clinical Presentation
• Cardiac Arrest: 10-20%• Massive PE (SBP <90 mmHg): 4-6%• Submassive PE (stable
hemodynamics with RV dysfunction): 23-40%
• Submassive PE (stable hemodynamics w/o RV dysfunction)
• Recurrent PE• Untreated
Adapted from Fengler Am J of Emergency Medicine, 2009 27,84-95
mortality 66-95%22-53%
8-13%
1-4%
25%30%
How many other diseases have such terrible implications???

Have we made much progress since 1969?
5

Massive vs. Submassive PE
Massive PE •SBP<90mmHg or decrease > 40 mmHg from baseline for > 15 min •Inotropic support •Pulselessness •Persistent bradycardia (HR < 40 bpm)
Submassive PE•SBP≥90mmHg •RV dysfunction •RV dilatation ECHO or CT (RV/LV diameter > 0.9)
• BNP > 90 pg/mL
• EKG changes
• Myocardial necrosis: Troponin I > 0.4 ng/mL
Troponin T > 0.1 ng/mL
Jaff et al, Circulation 2011;123:1788Jaff et al, Circulation 2011;123:1788

Kucher et al, Circulation 2006 – ICOPER Registry
• 2454 consecutive patients with PE
• 108 patients with massive PE (SBP<90)
• Recurrent PE at 90 days
– Submassive PE: 7.6%
– Massive PE: 12.6%
ICOPER Study - Kucher et al Massive PE Circulation 2006.
52.4%*
14.7%
*2/3 from recurrent PE
Mortality
PE Outcomes – Massive and Submassive“…good justification to treat!”
REMARKABLY LITTLE PROGRESS IN 30 YEARS

“Treatment gap” in PE
8
• <5% of patients with PE receive “advanced therapy”, including those with clear indications (hypotension, RV dysfunction, biomarkers, etc.)
• Many more are eligible than receive• Reasons• Failure to recognize potential benefit and
integrate data in “real-time”• Fear of complications• Inability to respond rapidly (“systems” issues)• “Paralysis” in decision-making

Real World Case #1
• 66 year-old man with no signif past medical history noted dyspnea on exertion 5-6 days prior to presentation.
• Symptoms progressed – shortness of breath walking 20 feet
• Outside hospital PE-protocol CT extensive bilateral saddle PE
• Started on heparin and transferred to a tertiary referral hospital
• TTE at second hospital: large clot in right atrium confusion about best therapy
• Patient transferred to MGH
Troponin-T: 0.4 ng/mlNT-proBNP: 1975 pg/ml

PE-Protocol CT:
10

Transthoracic Echocardiogram: Still ImagesThrombus Across Pulmonic Valve
11
What would you do next?
Who makes the decision
and on what basis?

Management Alternatives
Acute PE
Anticoagulant MechanicalThrombolytic
Therapy
SystemicCatheter Directed
IVC Filter
MCS
~More likely with severity
Surgical Embolectomy
PercutaneousFragmentation
&Aspiration
Ultrasound-Assisted
Pharmaco-mechanical
How do we decide which therapy to apply in a given patient ???

13
Therapeutic Alternatives in Acute PE
• Anticoagulation– Unfractionated Heparin
• Continuous Intravenous• Full-Dose Subcutaneous
– Low-Molecular-Weight Heparin
– Direct Thrombin Inhibitors– Synthetic Pentasaccharide
Xa Antagonist– Warfarin
• Thrombolytic Therapy– Systemic (full or half-dose)– Catheter Directed (CDT)– Pharmacomechanical
Catheter-DirectedThrombolysis (P-CDT)
• Mechanical– Surgical Thrombectomy– Thrombo-aspiration
• Adjunct Rx– Extracorporeal support (ECMO)– RVAD– IVC Filter

Available Guidelines
Circulation 2011;123:1788.Chest 2012;141:419S.
“Management of submassive PE crosses the zone of equipoise, requiring the clinician to use clinical judgment.”
“In most situations of uncertain benefit of a treatment…we took the position of primum non nocere….given the certain risks of bleeding and less-certain benefits, thrombolysis is likely to be harmful. Selected patients without hypotension may benefit…”

Decision-making Beyond the Guidelines
• Guidelines offer few class I recommendations and do not cover all scenarios
– Paucity of data available for highest-risk patients
– Novel devices and approaches now available
• Expert multidisciplinary consultation essential (STEMI, Stroke,TAVR teams)
• Timely decision-making and intervention crucial
Circulation 2010;122:1124.Tex Heart Inst J 2013;40:5.

Which therapy to use???• Best treatment unknown
– No “standard approach”– No “Appropriate Use Criteria” for intervention
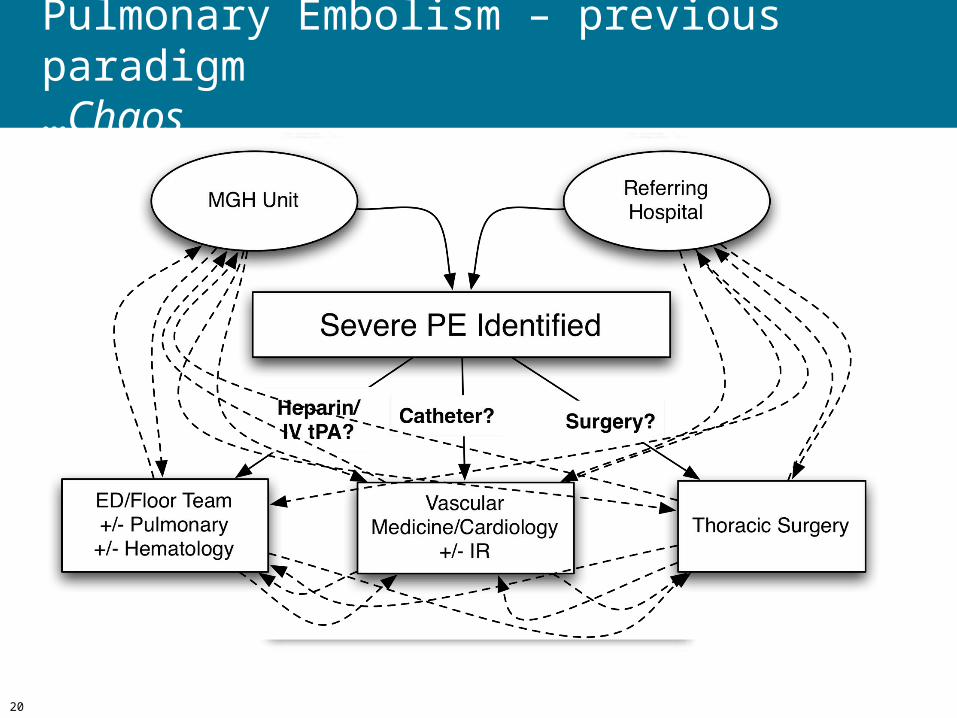
• Strategies “all over the map”… MGH experience as example: – Practice variation by medical service, location, size and
threat to patient, etc.– No standard algorithm or consistency in decision-making– No single “team” or “clearing-house”– No centralized locations for care or “centers of excellence”– No systematic evaluation of results
How do we decide whether to “intervene” and by what modality? Who decides? What is the endpoint?

Pulmonary Embolism Response Team
A Multidisciplinary Effort to Improve Care and Outcomes in Patients with PE
17

PERT: Pulmonary Embolism Response Team
• Goals: Improve patient outcomes with a collaborative, multidisciplinary team-based urgent consult to treat massive and submassive PE
• Functionality
– Modeled on rapid-response concept
– Multidisciplinary team of experts: convened via electronic meeting
– Evaluate and offer full range of available treatments
Chest 2013;144:1738

ED / ICU / Floor TeamPulmonary
Vascular Medicine/CardiologyCardiac Surgery
Pulmonary Embolism – previous paradigm…Chaos
20

Objectives• Respond expeditiously to treat patients with massive and
submassive PE
• Provide best therapeutic option(s) available for each patient
• Leverage the input of a multidisciplinary team of experts
• Coordinate care among services involved in care of PE
• Develop protocols for the full range of therapies available
• Collect data on clinical presentation, treatment efficacy, and outcomes (short and long-term)
…Fill unmet need and gap in knowledge base…
21
Pulmonary Embolism Response Team (PERT)

PERT Program Flow Map
Handoff totherapeutic site
ED
MGH floor
OSH
PERT fellow:HistoryPhysicalLabsEKG EchoCT-PE Massive
Surgery
Vortex
ECMO
LyticSubmassive
CDTAttending
Low Risk
Expeditious input and clinical judgment from multiple specialties to optimize therapy
A/C
ACTIVATE PERT MULTIDISCIPLINARY
TEAM
Electronic MeetingVascular MedicineCardiac SurgeryICU/Pulmonary
HematologyRad,Echo
22

Gotomeeting.com
Multidisciplinary Virtual Consultation• Leverage low- and no-cost
internal and commercially available tools
‒ Citrix® GoToMeeting web-based HDvideoconferencing
‒ Allows exchange ofscreen control
‒ Tracks meeting date, time and length
‒ Group email distribution lists
‒ Group paging

Back to our 66 y.o. man with Submassive PE and ?clot in transit…what to do?
• Multidisciplinary “gotomeeting”
– CT surgery, cardiology, vascular med, pulm critical care, hematology, ED, and anesthesiology
Decision made to proceed to catheterization laboratory for Vortex Angiovac
• Procedure under general anesthesia with TEE guidance
• Access: Percutaneous– Subclavian vein – triple lumen
– Right femoral vein – 26 F Dry-seal sheath
– Left femoral vein – 17 F Venous Return
– Left femoral artery (in case ECMO required)
25
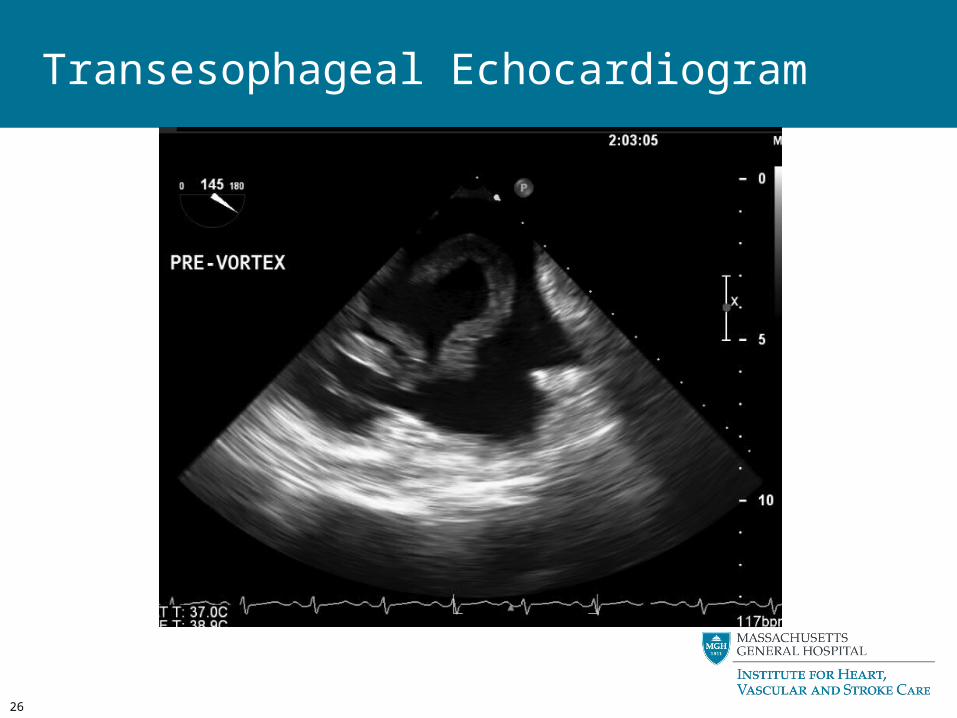
Transesophageal Echocardiogram
26
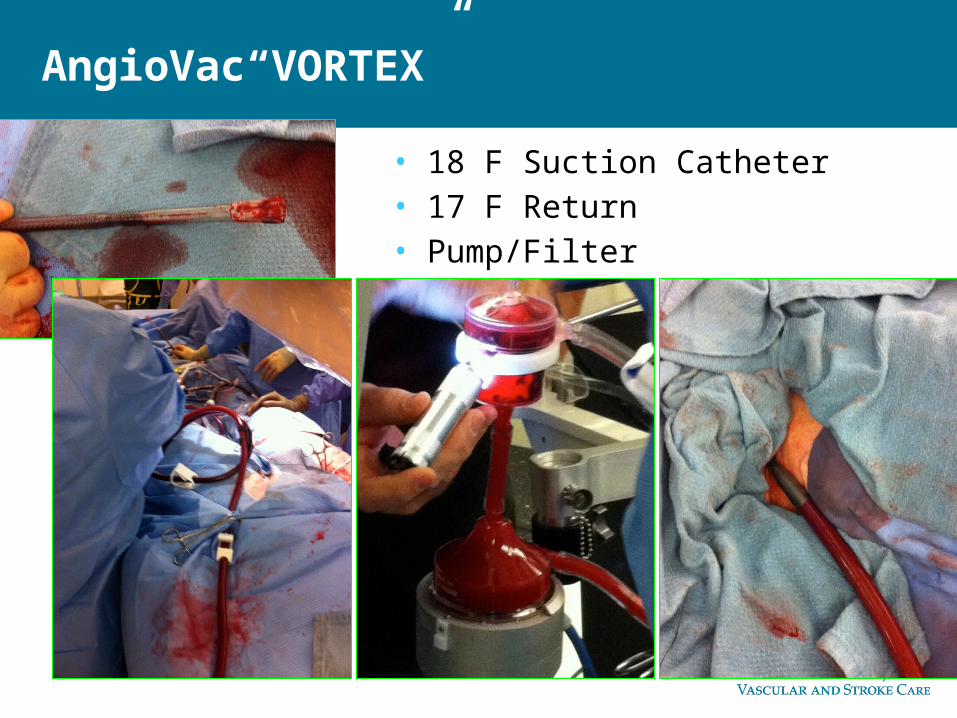
AngioVac“VORTEX”
• 18 F Suction Catheter• 17 F Return• Pump/Filter

Thrombus Extracted by Vortex AngioVac
28

Transesophageal Echocardiogram: Post Extraction
29

Pulmonary Angiography: Still Image
30

Post-VORTEX
• Plan to send to SICU for monitoring
• Sudden drop in BP to 60, requiring additional pressors
• Decision for thrombolysis of saddle PE’s
• Re-prepped and EKOS catheters placed bilaterally
31
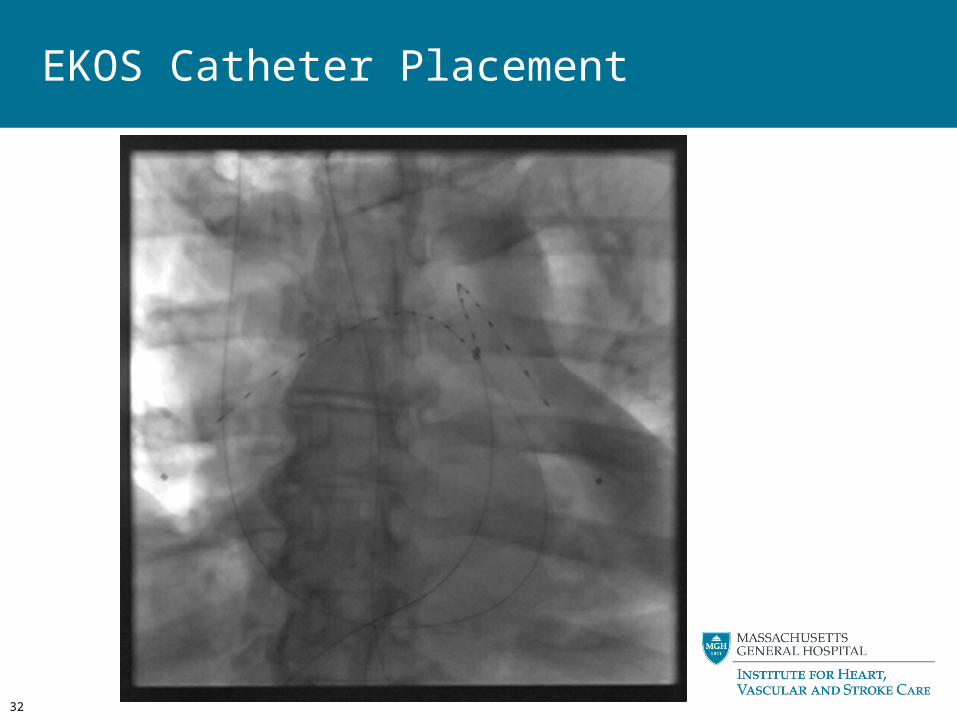
EKOS Catheter Placement
32

Post-procedure
• Initial 12 hours
– 2mg bolus tPA, then 1mg/hr via each EKOS x 4 hrs, then 0.5mg/hr x 6 hours
– Total dose 21mg
– Remained hypotensive/shocky requiring Epi @ 2-5, Phenylephrine @ 5-15, +/-Vasopressin
– RV function poor
• 14 hours post-procedure – Prop. d/c’ed and awoke, extubated, pressors stopped. BP 140, HR 80, O2 sat 100% on 2 L
• Home day 4
33

Emerging Technologies - “game-changers”?
• Ultrasound facilitated lysis – More rapid clot dissolution with lower dose of lytic agent?
• VORTEX Angiovac - En bloc thrombus aspiration– Rapid removal of offending clot percutaneously– Requires perfusionist & addl resources
• ECMO– Ability to support patient hemodynamically– “bridge” to definitive Rx
Will these change the paradigm completely?
How do we integrate these into existing treatments?
Underscores need for integrated, TEAM approach to PE
…with multi-disciplinary decision-making

PERT ActivationsOctober 2012 Launch through November 2015
35
333 Activations in 25 Months
OCT NOV DEC JAN FEB MAR APR MAY JUNE JULY AUG SEPT0
5
10
15
20
25
4
6
14
12
5
13
10
6
10
1720
13
17 17
10
13 13
1112
8
1417
1917
18 17
FY13 FY14 FY15

36
• Male: 56% Female: 45%
• Age range: 10 – 98 yrs‒ Median age: 62 yrs.
• Survival to discharge: 85%
• Interventions:59.8% Anticoagulation only
9.1% Catheter-direct thrombolysis
4.2% Surgery
2.8% IV systemic lysis
2.4% Mechanical support/ECMO
21.0% IVC filters
0.7% Vortex
AC Only
IVCF
IV Lysis
CDT
Vortex
ECMO
Surgery
PERT ActivationsOctober 2012 Launch to Present

PERT Consortium- Launch MeetingBoston, MA May 21, 2015
PERT
PERT
PERTPERTPERT
PERT
PERT
PERT
PERTPERT
PERTPERT
PERT
PERT
25+ Interested Centers
PERT
PERT
PERTPERT
PERT

38

Future of Vascular InterventionPulmonary Embolus Management• Summary
– PE still poorly understood; much to learn – New era: heightened awareness and
coordinated institutional approach to a complex, life-threatening problem
– OPTIMAL CARE WITH TEAM APPROACH!!PERT: a “model” program, demonstrating the power of interdisciplinary collaboration to streamline care, optimize outcomes for our patients, and enable development of better treatment paradigms for patients with PE
– PERT Consortium …Contact us if interested!!
